Document 1.
Guide to accessing funding for Long-Term Support
Services for people with disabilities and chronic
health conditions
Version 1.1
January 2016
Page 1 of 30
Guide History [to be completed]
1.1 Document Location
This document is only valid on the day it was printed.
The source of the document wil be found at this location –
[insert folder structure]
1.2 Revision History Date of this revision:
Date of next revision:
Revision
Previous
Summary of Changes
Changes marked
date
revision date
First issue
1.3 Approvals
This document requires the fol owing approvals.
Name
Signature
Title
Date of Issue Version
1.4 Distribution
This document has been distributed to:
Name
Title
Date of Issue
Version
Page 2 of 30
link to page 1 link to page 1 link to page 5 link to page 6 link to page 6 link to page 6 link to page 6 link to page 7 link to page 7 link to page 7 link to page 8 link to page 8 link to page 9 link to page 10 link to page 10 link to page 10 link to page 12 link to page 13 link to page 15 link to page 15 link to page 15 link to page 15 link to page 16 link to page 16 link to page 18 link to page 18 link to page 18 link to page 18 link to page 18 link to page 19 link to page 19 link to page 20 link to page 20 link to page 20
Table of Contents
Guide to accessing funding for Long-Term Support Services for people with disabilities and chronic
health conditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Abbreviations used in this document . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
1.0
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
1.1
Overview. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
1.2
Guiding principles for access to long term support services . . . . . . . . . . . . . . . . . . . . . . . . 6
1.3
Eligibility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
2.0
LTS-CHC & DSS Client Groups and criteria for funding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.1
LTS-CHC Funding Pool . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.1.1
Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.1.2
Eligibility criteria for the LTS-CHC client group . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
2.1.3
Examples of very high need for long-term support services . . . . . . . . . . . . . . . . . . . . 8
2.1.4
Exclusions for LTS-CHC funding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.2
DSS Funding Pool . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.2.1
DSS client group . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.2.2
Applying the definitions of physical, sensory and intel ectual disability . . . . . . . . . . . 10
2.2.3
Other eligible groups . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.2.5
Exclusions for DSS funding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.0
Joint Funding. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
3.1
Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
3.2
Change of Funder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
3.3
Shared arrangements for people with DSS eligible disabilities and other conditions . . . 15
3.4
Resolving funding responsibility between DSS and DHBs . . . . . . . . . . . . . . . . . . . . . . . 16
3.5
LTS-CHC and DSS National Resolution Panel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
4.0
Support services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
4.1
Home Based Support Services (HBSS) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
4.2
Carer Support (including residential respite services) . . . . . . . . . . . . . . . . . . . . . . . . . . 18
4.3
Environmental Support Services (ESS) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
4.4
Community Residential Support Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
4.5
Advanced personal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
4.6
Access to DHB funded community support services . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
5.0
Process for Accessing Long-Term Support Services for People with Chronic Health
Conditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
5.1
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Page 3 of 30
link to page 20 link to page 22 link to page 22 link to page 22 link to page 22 link to page 24 link to page 24 link to page 24 link to page 24 link to page 24 link to page 25 link to page 25 link to page 25 link to page 25 link to page 26 link to page 27 link to page 27 link to page 28 link to page 29 link to page 30
5.2
The NASC process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Appendix 1 – Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
The Government’s definition of a ‘person with a disability’ for the purpose of accessing
disability support services [CAB (94) M 3/5 (1a)] . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Definitions in ‘Support for Independence for People with Disabilities: a New Deal’ . . . . . . . . . 22
Appendix 2 – Close in Interest Criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Criteria for Allocating Clients aged 50-64 to a DHB Funder . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Relationship to ‘Close in Interest’ for Aged Residential Care . . . . . . . . . . . . . . . . . . . . . . . . . 24
Clients to be considered against these criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
The Criteria [Draft pending DHB CEO and MoH sign off] . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Who wil make this determination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Responsibility for undertaking the initial needs assessment. . . . . . . . . . . . . . . . . . . . . . . . . . 25
Dispute Resolution . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Risk Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Appendix 3 – Conditions not currently classified by the Ministry of Health as a disability . . . . . . . 27
Exclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Appendix 4 – [Check for name of appendix] . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Appendix 5A – [Check for name of appendix]. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Appendix 6 – The referral/screening information form for LTS-CHC clients . . . . . . . . . . . . . . . . . 30
Page 4 of 30
Abbreviations used in this document
Abbreviation
Ful Name
ACC
Accident Compensation Corporation
CHC
Chronic Health Conditions
DHB
District Health Board
DSS
Disability Support Services
ESS
Environmental Support Services
HBSS
Home Based Support Services
LTS
Long Term Support
ICF
World Health organisation International Classification of Functioning,
Disability and Health
MoH
Ministry of Health
NASCs
Needs Assessment Service Coordinators
Page 5 of 30
1.0 Introduction
1.1 Overview
The purpose of this document is to give guidance to relevant parties on the provision of Long
Term Support to eligible people, and to support District Health Boards (DHBs) and Disability
Support Services (DSS) Needs Assessment Service Coordinators (NASCs) in decisions on
which funding pool is used.
1.2 Guiding principles for access to long term support services
The New Zealand Public Health and Disability Act, the New Zealand Disability Strategy and
the World Health organisation International Classification of Functioning, Disability and
Health (ICF) provide the basis for Ministry of Health (MoH) and DHB activity.
Principles underpinning access to long-term support services
1. Access to support services should be based on need, not diagnosis
2. Responsiveness to clients’ needs is timely and appropriate
3. National y consistent policy, procedures and analysis supports innovation and local
solutions
4. Accountability for funding support services is simple and clear, regardless of age
5. [Equity statement].
Actions/principles underpinning the ways in which the Ministry of Health and DHBs wil
work together 1. Clear, understandable statements about who services are delivered are available in
order to ensure a consistent approach to funding decisions is able to be applied.
2. Sharing of data to enable future planning.
1.3 Eligibility
People eligible for Long Term Support – Chronic Health Conditions (LTS-CHC) or Disability
Support Services (DSS) funding for long term conditions:
a. Must be eligible for a ful range of publical y funded health and disability services
under the Eligibility Direction.
b. Do not have an injury that is likely to meet Accident Compensation Corporation
(ACC) cover and entitlement criteria under the Accident Compensation Act 2014.
In order to receive funded household management services clients require a Community
Services Card.
Page 6 of 30
link to page 7
2.0 LTS-CHC & DSS Client Groups and criteria for
funding
2.1 LTS-CHC Funding Pool
The LTS-CHC Funding Pool is targeted at people with chronic health conditions and very high
need for long-term support services who do not meet current eligibility criteria for MoH
funded DSS or DHB funded long-term support services.
While eligible clients wil have very high support needs, some wil be receiving much of this
support from relatives or whanau.
2.1.1 Definitions
Chronic health condition
For the purposes of establishing eligibility for LTS-CHC funding a chronic health condition is:
a. Either a progressive health condition where the person has a functional impairment
that is expected to last for at least six months or to increase over time as a direct
result of the condition;
b. Or a health condition lasting at least six months where the level of functional
impairment can be ameliorated by periodic or ongoing treatment, for example
drugs, therapy, or surgery;
c. And the condition is not currently classified by the MoH as a disability (see
exclusions in
Appendix 3).
The majority of people who meet the criteria of high need for long-term support services wil
have more than one chronic health condition. This can include non-injury related brain
damage such as Alzheimer’s, Korsakoff’s or a tumour. One or more of the conditions could
be a mental health condition, however, the LTSD-CHC fund wil only fund support services
where the principal need for those services results from a physical condition (including non-
injury related brain damage).
The LTS-CHC fund does not fund support services for people predominately or solely
disabled as a result of one or more mental health conditions.
Examples of co-existing health conditions that eligible clients could have include
schizophrenia, depression or drug or alcohol dependence.
DHB funded long-term support services DHB funded long-term support services are defined as a range of services DHBs fund for
people over the age of 65 and for people aged 50 to 64 who have been assessed as ‘close in
interest’ to older people (see
Appendix 2 for the close in interest criteria).
1
1 DHBs interpret the close in interest criteria differently. Issues relating to differing DHB interpretations of the
close in interest criteria wil be addressed as part of the longer-term work to resolve funding responsibility for
Page 7 of 30
link to page 8
2.1.2 Eligibility criteria for the LTS-CHC client group
Clients eligible for LTS-CHC funding are people who meet all of the following criteria:
a. Are aged under 65;
b. Are currently not eligible for MoH funded disability support services or DHB funded
long-term support services;
c. Have one or more chronic health conditions(s) that is/are expected to continue for
six months or more (provided in definition in section 1.2);
d. Have very high need for long-term support services. Very high need is defined as
requiring assistance
2 with activities of daily living at least daily to remain safely in
their own home or needing residential care. The person’s wel being and functional
status is deteriorating, their needs are increasing and safety issues are becoming
apparent. The person has limited opportunity to participate in age appropriate
activity. The person is assessed as needing support daily, but some or most of it may
be provided by family, whānau or friends. The LTS-CHC would fund any additional
formal support services needed;
e. Do not have an informal support system (family whānau) or the caregiver is under
considerable pressure and their ability to support the person is compromised;
f. Are not currently receiving MoH funded disability support services or long-term
support services funded by a DHB (regardless of the funding source).
People who have received equipment or housing or vehicle modifications funded from the
Environmental Support Services (ESS) budget are not excluded if they meet al other criteria.
2.1.3 Examples of very high need for long-term support services
Examples of very high support need include (but are not limited to) situations where failure
to provide long-term support services may result in the person:
a. Being at risk of inappropriate or premature admission to residential or acute care
because of concern about their safety in their current living situation; or
b. Experiencing delayed discharge from hospital because of concerns about their safety
without assistance at least 5 days a week (either in their own home or in residential
care); or where
c. Residential care is the only realistic option
this group of people. For the Interim Funding Pool (IFP) the interpretation of the close in interest criteria wil
be that in operation in each DHB as at June 2006.
2 Assistance refers to physical hands-n care. For children this refers to significantly higher levels of care than
would usual y be expected for the child’s age.
Page 8 of 30
This could be because (for example) the person:
a. Has a recent history of falling;
b. Needs assistance with daily self-care;
c. Is unable to transfer (eg get in or out of bed without assistance);
d. Is confused and at risk of harm. The confusion can be the result of non-injury related
brain damage such as Alzheimer’s, Korsakoff’s the effects of psychotropic drugs or a
tumour, but not mental health conditions such as schizophrenia or depression;
e. Needs night time monitoring.
People meeting the eligibility criteria for LTS-CHC funding who have a condition resulting
from drug or alcohol abuse wil continue to access necessary mental health services related
to the addiction or resultant behaviour problems.
People with fluctuating need for support services eg people with chronic fatigue syndrome,
who have periods of marked change in the level of support they need are eligible for
LTS-CHC funding if, over a 12 month period they are expected to meet the very high needs
criteria for at least half of the time. Given the variable level of support needed such clients
would be expected to have more frequent reassessments (eg three to six monthly).
2.1.4 Exclusions for LTS-CHC funding
People not eligible for LTS-CHC funding include those:
a. Whose need for support services is for less than six months;
b. Who meet the access criteria for ACC funding;
c. Who meet the access criteria for MoH funded DSS (see section on joint funding and
Appendix 3);
d. Who meet the access criteria for the relevant DHBs long-term support services (see
section on joint funding and definition Section 1.2 and
Appendix 4);
e. Who do not meet the eligibility criteria for having a chronic health condition and
very high need for long-term support services. This includes people requiring ESS,
but not meeting the very high need threshold.
Page 9 of 30
link to page 10
2.2 DSS Funding Pool
2.2.1 DSS client group
The MoH DSS client group consists of people who:
a. Present for assessment for DSS before the age of 65;
b. And have a physical, intel ectual, or sensory disability or a combination of these
which is likely to:
i.
Remain even after provision of equipment, treatment and rehabilitation
ii.
Continue for at least six months, and
iii.
Result in a need for ongoing support.
c. And do not meet the exclusion criteria (refer Section 2 for MoH DSS funding
exclusions).
In addition the MoH funds ESS for a broader group of people (refer to Section 4
paragraph 4.3). This includes those outlined above; people with disabilities associated with
aging and people aged under 65 with disabling chronic health conditions.
A person’s diagnosis is a factor in determining eligibility for MoH funded DSS but is not the
main determinant. It provides a guide as to whether a person is:
a. Likely to have, or likely to develop (in the case of young children), a physical,
intel ectual and/or sensory disability and also whether the person is likely to have
ongoing support needs mainly due to this disability.
b. Likely to have primarily personal health needs that could be significantly ameliorated
by treatment and/or likely to require ongoing clinical intervention.
2.2.2 Applying the definitions of physical, sensory and intel ectual disability
The fol owing outlines the sub-groups within the broader MoH DSS client group accessing
individualised services. Impairments under each sub-group are accompanied by examples of
conditions that may result in these types of impairments but this is not intended to be a
diagnostic ‘in’ and ‘out’ list.
Physical disability
The MoH DSS client group with physical disabilities accessing individualised services includes
people with impaired limb function affecting independence in activities of daily living and/or
mobility
3
3 This group includes people with chronic medical conditions who, fol owing active treatment and
rehabilitation, are assessed as having a long-term physical disability and an ongoing support need where
physical disability (as opposed to physical incapacity) is the primary reason for support.
Page 10 of 30
link to page 11 link to page 11 link to page 11
Physical disability may be due to (but is not limited to):
a. Partial/total absence or loss of limbs (eg at birth or fol owing amputation as a result
of diabetes);
b. Structural impairments of limbs (eg achondroplasia);
c. Paralysis (eg hemiplegia fol owing a stroke or brain tumour; paraplegia due to spina
bifida, tetraplegia due to debulking of a spinal tumour);
d. Reduced muscle strength (eg fol owing guil ain-barré);
e. Ataxi
a4 (eg with cerebral palsy or multiple sclerosis)
f. Muscle wasting (eg with muscular dystrophy or motor neurone disease)
g. Muscle tone abnormalities (eg due to acquired brain injury not covered by ACC)
h. A limited range of movement (eg juvenile rheumatoid arthritis, osteoarthritis).
Some impairments arising from significant skeletal malformations (eg severe scoliosis)
may also meet the physical disability eligibility criteria, depending on the nature of the
resulting impairment.
Sensory disability
The MoH DSS client group with sensory disabilities accessing individualised services includes
people with the fol owing types of long-term sensory impairments that are generally not
responsive to treatment and affect independence in activities of daily living and/or mobility
5
a. Blind;
b. Deaf;
c. Deaf-blind;
d. Significant visual impairment;
e. Significant hearing impairment
f. Significant other sensory loss (eg no taste or touch – rare)
6
Intel ectual disability
The MoH DSS client group with intellectual disabilities accessing individualised services
includes people with intel ectual disability present at birth or general acquired before aged
18 (eg due to Angelman’s syndrome, microcephaly or meningitis).
4 Ataxia is a lack of muscle coordination during voluntary movement, such as walking or pricking up objects,
generally due to disorders in the brain or spinal cord.
5 This group includes people with chronic medical conditions who, fol owing active treatment are assessed as
having a long-term sensory disability and an ongoing support need where sensory disability is the primary
reason for support (eg blind due to diabetes).
6 Note sensory impairment does not include hypersensitivity or perceptual impairments such as auditory
processing disorder.
Page 11 of 30
link to page 12
A NASC may request a specialist assessment to confirm a person has an intel ectual
disability. This may include a cognitive assessment (general y, an IQ test score of up to 70
indicates a limitation in intel ectual functioning) and standardised assessment of adaptive
behaviour in the areas of conceptual skills, social skills and practical skills.
Eligibility for MoH funded Intellectual Disability Compulsory Care and Rehabilitation services
is legislatively mandated (Section 7 of the Intellectual Disability (Compulsory Care &
Rehabilitation) Act 2003 refers).
Eligibility for MoH funded DSS contract for people with intellectual disability is outlined in
the ‘
Operational Guideline for the Assessment of Intel ectual Disability to Access Disability
Support Services Contract for People with Intel ectual Disability in New Zealand 2009’7
Where a person has been assessed as eligible for DSS on the basis of a physical or sensory
disability and the person has a co-existing significant intellectual impairment that was
acquired at age 18 or older and is not covered by another funder (eg ACC), the MoH may
fund the ful package of support.
2.2.3 Other eligible groups
There are certain other groups that the MoH funds support services for whose impairments
do not strictly meet the DSS definition of physical, sensory or intellectual disability. Their
inclusion generally reflects long-standing practice.
Disability in young children where presence of a physical, sensory and/or intel ectual
disability is not yet confirmed.
The MoH funds DSS for children who are medical y stable and have significantly delayed
physical, intel ectual and/or sensory development (often global development delay) for
whom there are indicators of likely long-term physical intellectual and/or sensory disabilities
and where clinical/rehabilitative intervention is not expected to significantly reduced the
need for long-term support. Eligibility is on an interim basis until a long-term disability
(usual y an intel ectual disability) with associated ongoing support need is confirmed
(general y by age seven).
Disability associated with acquired brain injury and certain neurological conditions.
The MoH funds DSS for some people who have acquired brain injuries and certain
neurological conditions that do not result in a physical or sensory disability.
This includes some people who, after treatment and rehabilitation, have long-term
significant cognitive impairment (eg due to multiple sclerosis, a stroke, or a benign brain
tumour). Clinical reports will generally be required to support the referral to NASC. Eligibility
decisions take into consideration the age of the person, whether the person has any
significant co-existing medical conditions and the nature of the person’s support need.
The MoH does not fund DSS for people who require support:
a. Due to cognitive impairment arising from a mental il ness or addiction or due to the
consequences of treatment for these conditions (eg people with Korsakoff’s
7 This guideline is included in the NASC Managers’ Manual
Page 12 of 30
link to page 13 link to page 13 link to page 13
psychosis or other substance induced brain damage);
b. Solely due to behavioural problems.
2.2.5 Exclusions for DSS funding
DSS does not fund support services for people with conditions or situations covered by other
funders including:
a. Support to address short-term needs ie less than six months duration eg fol owing
surgery or medical events
8 (DHBs Personal Health);
b. Support for people who first present for assessment for long-term support at age 65
or over (DHBs Health of Older People – CAB Min (03) 5/5 refers);
c. Support for people who first present for assessment for long-term support between
ages 50 and 65 who are clinically assessed by a DHB clinician or needs assessor as
being ‘close in interest’ to older people
9 (DHBs Health of Older People – CAB Min
(03) 5/5 refers)
d. Aged residential care for MoH DSS clients who have been reassessed by a DHB
needs assessor as requiring this service (DHBs Health of Older People – CAB Min
(03) 5/5 refers);
e. Support for people who first present for assessment for long0term supports before
the age of 65 whose support need is due to impairments that do not meet DSS
operational definition of physical, sensory or intellectual disability (DHBs LTDS-CHC);
f. Support for ‘medically fragile children’ – children with high health needs and/or
multiple impairments whose health status has not yet stabilised and for whom a
physical, sensory and/or intel ectual disability with associated ongoing support
needs has not been identified (DHBs Personal Health / LTS – CHC Primary Care);
g. Support for needs arising primarily from physical incapacity (eg shortness of breath,
fatigue or pain) due to chronic health conditions (DHBs Personal Health / LTS – CHC
Primary Care);
h. Support for additional care needs arising from a condition in the pal iative stage
10;
8 This includes ‘topping up’ existing MoH DSS support package for MoH DSS clients in these situations
9 People with long-term conditions more commonly experienced by older people and requiring integrated
health and disability support services. Refer to
Appendix 2.
10 This includes specialist palliative care services for people receiving MoH DSS funding.
Page 13 of 30
link to page 14 link to page 14 link to page 14 link to page 14 link to page 14
i. Support for needs arising from a mental il ness and/or addiction
11 including
physical, sensory and cognitive impairments attributable to this underlying
condition eg tardive dyskinesia due to long-term use of psychotriopic medication,
cognitive impairment due to alcohol or other substance abuse, impaired mobility
due to alcohol related peripheral neuropathy or functional difficulties due to
conversion disorder (DHBs Mental health and Addiction / LTS-CHC, Primary care)
12;
j. Support services needed primarily as a result of dementia or substance abuse (DHBs
Health of Older People / Mental Health of Older People / LTS-CHC, Primary Care);
k. Support services needed primarily as a result of behavioural problems (eg
associated with Foetal Alcohol Syndrome or substance abuse) except where the
person has a co-existing disability that meets DSS eligibility criteria
13 (some services
are funded by other government agencies such as the Ministry of Education, in
other situations this is a funding gap);
l. Support due to an injury that meets ACCs cover and entitlement criteria under the
Accident Compensation Act 2001
14;
m. Support for situations covered by other central government agencies such as the
Ministry of ?Education and the Ministry of Education and the Ministry of Social
Development (including the Child, Youth and Family Services)
15;
n. Support needs solely due to social/environmental factors (eg a dysfunctional home
environment). (Some services are funded by other government agencies such as the
Ministry of Education, in other situations this is a funding gap).
11 Responsibility for planning and funding disability support services for people with psychiatric disabilities was
devolved to DHBs in 2001 (CAB Min (01) 12/12 refers). Al residual contracts and funding were devolved in
2003 (CAB Min (03) 23/8 refers).
12 People who have a mental il ness and/or addiction and a co-existing physical, sensory or intellectual
disability that meets MoH DSS eligibility criteria may receive both DHB and MoH DSS funded support.
13 Where a person has behavioural issues due to an acquired brain injury or certain degenerative neurological
conditions (eg Huntington’s disease) secondary to a co-existing physical, sensory or intel ectual disability, MoH
DSS may fund the ful support package.
14 Refer footnote 3.
15 Some people wil receive support from both MoH DSS and other agency(ies).
Page 14 of 30
3.0 Joint Funding
3.1 Overview
Some clients will meet the eligibility criteria of both DSS and LTS-CHC and other funding.
Prior to June 2011 any person who was eligible for DSS or other DHB funded services was
not eligible for LTS-CHC funding. Recognising that this presents situations where a person
receives less support than they need, it was agreed that joint funding would be available
where a person’s situation is complex (eg support needs are very high due to a combination
of multiple health conditions and disabilities and a complex social situation) and significant
input is required from to or more funders (general y a high cost support package).
A pragmatic approach to joint funding wil be adopted, whereby funders wil agree on a
case-by-case basis what contribution each funder makes. Normal y joint funding wil be
possible where two funders purchase the same service that the eligible person required. The
NASC must determine that the person meets the eligibility criteria for both funders. In
extraordinary cases it may be possible that three funders are involved but these wil be
exceptional situations.
One funder wil assume responsibility for paying for services while the matter is being
resolved.
3.2 Change of Funder
A person’s health and disability status can change over time. There are some situations
where the health and support needs of a person who is accessing long-term support services
change to the extent that the funder of their supports needs to change.
3.2.1 Principles governing a change of funder
A client whose condition has changed to the extent that he/she no longer meets the current
funder’s eligibility and/or access criteria will continue to receive long-term support services
funded by that funder until arrangements have been agreed with an alternative funder and
have been put in place.
In order to change funders, a person must meet the eligibility and access criteria of the
proposed future funder.
The assessment of changed need requiring a change of funder wil be based on clinical and
functional assessment. The agency receiving the referral for long-term support services is
entitled to request additional clinical information to confirm this assessment.
3.3 Shared arrangements for people with DSS eligible disabilities and other
conditions
Joint funding or shared service arrangements may apply where a person assessed as needing
formal support:
a. Meets MoH DSS eligibility and access criteria; and
Page 15 of 30
b. Has a personal health condition, chronic health condition, condition in the pal iative
stage, mental il ness and/or addiction, and/or injury.
Where a person has support needs arising from both a DSS eligible disability type and a co-
existing condition or situation for which another funder (eg DHB, ACC or Ministry of
Education) has support funding responsibility, the MoH wil negotiate joint funding or shared
service arrangements with the relevant other funder. The MoH contributes to the person’s
support package by funding the DSS required as a result of the DSS eligible disability.
In complex situations where the cause of impairment is unclear (eg injury vs acquired) or a
person has multiple impairments/causes of impairments, the MoH works with other funders
to determine a pragmatic joint funding / shared services arrangement to support prompt
access to essential supports (eg 50/50 split or inter-funder transfer through the Crown
Funding Agreement). Further work is needed across funders to agree consistent and efficient
pathways for resolving funding responsibility in these situations.
3.4 Resolving funding responsibility between DSS and DHBs
Where there is disagreement between funders over whether a person’s support needs are
the funding responsibility of the MoH or a DHB, it is important that the interests of the
person needing support are protected in the first instance.
The fol owing resolution procedures apply:
a. Any disagreement about access to MoH or DHB funded services wil be resolved in
the first instance by discussion between the relevant needs assessment services.’
b. Where resolution cannot be achieved through discussion between MoH and DHB
needs assessment services, the first level of escalation wil be to the operational
management with the MoH DSS Group and to the DHB Portfolio Manager;
c. Where resolution cannot be achieved through the involvement of the DHB and DSS,
the dispute can be escalated to the LTS-CHC & DSS National Resolution Panel.
3.5 LTS-CHC and DSS National Resolution Panel
The role of the LTS-CHC and DSS National Resolution Panel is to:
1. Consider and make decisions on complex applications where the funding stream is
unclear between DSS and DHBs as to how the client’s needs are funded.
2. Use case studies to establish national policy / precedents / guidelines for future
clients around funding decisions.
3. Notify the relevant MoH contracted NASC and Disability Support Team of new
approvals.
The panel meets under the direction of the 20 DHBs and MoH DSS. Either party may refer
cases to the panel.
Page 16 of 30
Prior to referral to the panel, all parties must have explored all options to resolve the
funding for a difficult and complex client situation.
Al relevant information is submitted for the Panel to consider. Prior to referral all a parties
must be aware of the application and its contents, and have been given the opportunity to
provide further information, as required.
Both parties enter the process in good faith with a commitment to finding a solution, and
agree to abide by the decision of the Panel.
Page 17 of 30
4.0 Support services
Some support services are in short supply in some locations. Consequently assessed need
does not guarantee access to services. Where the most appropriate service is not available,
alternative options should be considered. The services that can be purchased are described
below.
4.1 Home Based Support Services (HBSS)
HBSS is a range of support services contracted by the DHB that enable clients to remain at
home (eg personal care, household management).
4.2 Carer Support (including residential respite services)
This is a subsidy for support services needed to assist the unpaid ful time carer of client to
take a break from caring for that person. (This subsidy can be used for carer support coming
into the home or to provide respite in a residential care facility). The need for, and the
quantum of Carer Support is assessed and approved according to the MoH Carer Support
Guidelines (see
Appendix 2). Most specialised respite services for medically fragile children
are available in some parts of New Zealand through the Medically Fragile Children service
specification.
4.3 Environmental Support Services (ESS)
ESS is funded for those clients who are not eligible for MoH DSS funded ESS. People who
meet the LTS-CHC access criteria, but whose family choose to provide all of the care they
need, can stil access ESS if this is an essential component of their support needs.
A person may access ESS either if it is an essential component of their support package, or if
the person would require assistance with activities of daily living at least once a day for five
days a week without ESS. This applies even if provision of ESS reduces the need for
assistance with activities of daily living below the threshold for the ‘high needs’ access
criterion (see Section 1.3.1).
ESS may be:
a. Equipment, such as wheelchairs, hoists, walking aids and equipment to help with
communication and vision;
b. Housing modifications, such as door widening, handrails, ramp access and level
access showers to enable effective use of the above equipment;
c. Vehicle modifications such as hand controls.
4.4 Community Residential Support Services
These are residential support services for younger people who need 24 hour support that
can be provided within aged residential care services or residential services provided for
people with physical disabilities.
Page 18 of 30
4.5 Advanced personal care
Those clients who require advanced personal cares wil have this support provided through
the Specialist Community Nursing Services or District Nursing service specification.
4.6 Access to DHB funded community support services
Many clients receiving community-based long-term services wil need, and be eligible for,
DHB funded health services. DHB funded health services include community health nursing
and al ied health services, meals on wheels, continence and stomal supplies, short term loan
equipment and equipment to administer medial treatment such as home oxygen,
ventilators, home dialysis etc. DHB funded services also include Mental Health Community
and Recovery Support Services.
A person needing these services should be referred to them at the same time as they are
going through the process to determine eligibility for LTS-CHC or DSS funding.
Page 19 of 30
link to page 20
5.0 Process for Accessing Long-Term Support Services for People
with Chronic Health Conditions
5.1 Introduction
LTS-CHC NASCs are al ocated a budget based on the size and demographic characteristics of
the population they cover.
16
5.2 The NASC process
The DHBs manage the LTS-CHC fund, using existing systems and processes wherever
appropriate. NASC Roles and Responsibilities are covered in Section 3 of
‘The Operational
manual for Needs Assessment and Service Coordination Managers, May 2005’. This includes
compliance with the Privacy Act 1993. The NASC Process Flow Chart on page 32 of that
Manual has been modified to cover the additional steps that wil be required for LTS-CHC
clients (see
Appendix 5A).
5.2.1 Referral Process
Triage at the point of referral wil determine the appropriate agency to refer to.
The receiving NASC wil acknowledge receipt of the referral
[include a Flow Chart – Triage]
Where the initial referral is to a DHB Mental Health NASC – if the person does not meet the
eligibility criteria for accessing mental health funding and they have co-existing medical
conditions the Mental Health NASC wil refer people aged 50 and over to the DHB older
persons’ NASC for assessment of whether they meet the criteria for ‘close in interest’ to
colder people (DHB funded services). If they do not, the process is the same as for people
under the age of 50. People under the age of 50 wil be referred to the NASC for assessment
for eligibility for either MoH funded DSS or for the LTS-CHC fund. To meet the eligibility
criteria for LTS-CHC funding the person’s primary need for support services must result from
a physical condition (including non-injury related brain damage). The LTS-CHC fund does not
fund support services for people predominantly or solely disabled as a result of a mental
health condition.
Referral assessed for funding are to be from health practitioners, as the status of the clients’
health conditions and capabilities (functional, cognitive and social) needs to be clearly
documented. This includes any specialised heath assessments. If the original referral is from
a non-health practitioner or a self-referral then the MoH contracted NASC wil need to
obtain permission from the client to ask the client’s primary health practitioner to submit a
referral in order to verify the status of the client’s chronic health condition.
16 It should be noted that, in some cases the NASC notional budget wil cover more than one DHB population.
Page 20 of 30
Health practitioner includes:
a. PHO practitioners eg General Practitioners, Car Plus practice nurses;
b. Hospital. Medical Specialists;
c. Community Health Nurses;
d. DHB Allied Health Professionals (including social workers).
The Referral/Screening information Form for LTS-CHC clients is provided in
Appendix 6 [Need to check if DHBs al use the same form – if not remove this reference and refer to
local process or policy]. The first two pages of the Referral/Screening form may be
completed by the referrer and submitted to the screening NASC along with necessary clinical
summaries, assessments and reports to support the application for long-term support
services. Wherever possible the Referral/Screening form should be completed as a word
document that can be emailed. The third page is to be completed by the screening NASC.
5.2.2 Assessment and development of support packages
The LTS-CHC NASC undertakes the Needs Assessment using national assessment guidelines
and support package al ocation tol s so that national consistency is assured.
The NASC wil col ate and document al information needed to make a decision for needs
assessment and service coordination for each approved client. Documentation wil include
an assessment of health needs and a health management plan developed by the relevant
referrer/health agency (as appropriate). For people being discharged from hospital, this
could take the form of a discharge plan.
Specialised assessments
The documentation wil also include appropriate, relevant clinical information and any
specialised assessments that are needed. Specialised assessments could include:
a. Occupational therapy;
b. Physiotherapy
c. Social work;
d. Continence;
e. Mental Health;
f. Psychological;
g. Dementia;
h. Cognitive;
i. Speech language therapy;
j. Environmental Support Services.
Specialised assessments that are currently funded by a DHB wil continue to be funded by
the DHB.
Page 21 of 30
link to page 22
Appendix 1 – Definitions
The Government’s definition of a ‘person with a disability’ for the purpose of
accessing disability support services [CAB (94) M 3/5 (1a)]
‘A
person with a disability is a person who has been identified as having a physical,
psychiatric, intel ectual, sensory or age-related disability (or a combination of these), which is
likely to continue for a minimum of six months and result in the reduction of independent
function to the extent that ongoing support is required.
Where a person has a disability which is the result of a personal injury by accident which
occurred on or after 1 April 1974, it should be determined whether they are eligible for cover
under the Accident Rehabilitation and Compensation Act 1992.
Where a person’s level of independent function is reduced by a condition which requires
ongoing supervision from a health professional (eg in the case of rental dialysis), that person
is considered to have a personal health need rather than a disability. Where a person has
both a disability and a personal health need, the services provided to address those needs are
disability support services and personal health services respectively’
Subsequent to this definition being agreed by Cabinet, Cabinet decided to transfer
responsibility for some disability groups to DHBs. Funding responsibility for DSS for people
with psychiatric disability transferred to DHBs in 2001 and for people with age-related
disability in 2003
17. The latter group included:
a. People who first present for assessment for DSS at age 65 and over: and
b. People aged between 50 and 65 who are clinical y assessed as ‘close in interest’ to
older people (having poorer health and disability status than the general population
and conditions/disabilities normally acquired at age 65 and over.
[Jan W Notes for the fol owing that this is not a group. Al DSS age etc has devolved to DGB
and Mental Health with DHB. This is a descriptor of al funded by Vote Heath]
Definitions in ‘Support for Independence for People with Disabilities: a New
Deal’
[Minister of Social Welfare and Minister of Health 1992. Support for Independence for
People with Disabilities: A new Deal. Wellington: Parliament Buildings]
‘
Physical disability – reduced physical capacity (for example, through loss or impaired use of
limbs).
Sensory disability – impairment of the senses (mostly sight and hearing).
Intellectual disability – permanently impaired learning ability (usually from birth) which
prevents or inhibits people from developing the range of physical and social skil s usual y
found in a person of that age.
17 Note: This devolution also included residual MoH funded long-term support services for people with
personal health conditions, mental il nesses and pal iative care needs.
Page 22 of 30
Psychiatric disability – disability arising from continuous or intermittent disorders related to
thinking, feeling, volition, or behaviour (for example, schizophrenia, severe chronic
depression, or long-term addition to alcohol and drugs.
Age-related disability – physical, intel ectual or psychiatric conditions related to the onset of
old age. This includes conditions that can affect younger people, such as Alzheimer’s disease
or stroke, but which are more often found amongst older people’.
Page 23 of 30
link to page 24
Appendix 2 – Close in Interest Criteria
Criteria for Allocating Clients aged 50-64 to a DHB Funder
Background
These criteria were developed by a representative group of District Health Board, Ministry of Health
and Needs Assessment and Service Coordination agency stakeholders to assist in operationalising
Cabinet’s decision that ‘
people between 50 and 65 who have been clinical y assessed by a District
Health Board and/or needs assessor as ‘close in interest’ to persons aged 65 and over, and who
require access to disability support services wil be funded by a District Health Board.18
The intention is to ensure that people who acquire conditions more commonly associated with
ageing earlier than the general population, and whose needs are best met by DHBs integrated health
and disability services for older people, have access to these services.
Relationship to ‘Close in Interest’ for Aged Residential Care These criteria are not related to the assessment for ‘close in interest’ for aged residential care. This
determination wil continue to be made according to the current process ie, on the basis of a
geriatrician/psychogeriatician’s clinical judgement and NASC assessment processes. Al clients
assessed as requiring aged residential care in this age range wil be DHB funded from
1 October 2003.
Clients to be considered against these criteria Clients who will be assessed against these criteria will be those who:
a. Present to a Needs Assessment and Service Coordination agency for the first time between
ages 50 and 65;
b. And are assessed as meeting the DSS definition for disability;
c. And are assessed as needing community based disability support services.
The Criteria [Draft pending DHB CEO and MoH sign off]
The client meets the DSS definition of disability, and
Either
Has three or more advanced chronic conditions with multiple comorbidities
Or
Has a vulnerable state of health arising from a complex interaction of medical and social problems
(may be considered to be ‘frail’)
And
18 DHBs interpret the close in interest criteria differently. Issues relating to differing DHB interpretations of the
close in interest criteria wil be addressed as part of the longer-term work to resolve funding responsibility for
this group of people. For the Interim Funding Pool the interpretation of the close in interest criteria wil be that
in operation in each DHB as at June 2006.
Page 24 of 30
Requires integrated health and disability support services and close health management to ensure
health is maintained at an optimal level.
The assessment process wil include consideration of the client’s and his/her family’s perspectives on
the client’s needs, goals and where these may be best met.
Who wil make this determination The determination of which funding stream the client should be al ocated to wil be made by the
NASC Needs Assessor/Service Coordinator informed by appropriate clinical input. Which clinicians
are appropriate to provide this input wil be a local DHB decision.
Responsibility for undertaking the initial needs assessment
For NASC agencies that cross age ranges (Central and Midland Regions), the NASC agency wil
determine on the basis of the referral who within their team carries out the initial assessment.
For NASC agencies in regions which have separate younger peoples’ (lifelong disability) and older
peoples” NASC agencies (Southern and Northern regions), clients may present initial y to either the
MoH or DHB funded NASC agency.
The NASC agency receiving the initial referral wil screen the referral and where the information is
provided is explicit enough to clearly indicate the funding stream, then the referral wil either be
accepted and an assessment arranged by the agency receiving the referral or directed to the
relevant NASC agency providing for that client group.
Where the information provided does not clearly indicate which funding stream the client should be
al ocated to, the NASC agency which receives the referral wil undertake the initial needs
assessment.
Where the outcome of the assessment is that the person appears to fit the criteria and the younger
peoples’ NASC carried out the initial assessment, the assessment wil be forwarded to the older
peoples’ NASC agency. The older peoples’ NASC service coordinator wil then review the information
provided and seek clinical input to confirm this person should be al ocated to a DHB funder.
Dispute Resolution
It is anticipated that situations where NASC agencies disagree over which funding stream the client
should be al ocated to (which wil be rare) but where this occurs, the NASC assessor/service
coordinator should raise this with their Manager. Where the respective NASC Managers are unable
to reach agreement, this issue should be escalated to the DHB Planning and Funding team (for older
peoples’ NASCs) and to the MoH DSS Operational Team (for younger peoples’ NASCs).
Evaluation
These criteria wil be evaluated once they have been operational for six months.
The evaluation wil include:
a. Whether the criteria are workable ‘on the ground’;
b. Identification of any boundary/interface issues arising in applying the criteria;
c. Actual volumes/$ against devolved volumes/$.
Page 25 of 30
Risk Management
The risk management arrangements in place for the devolution of DSS funding wil apply to this
client group. The new national y consistent data requirements put in place for NASC from
1 October 2003 wil enable reports to be generated on this client group including numbers by DHB
area, ethnicity, primary and secondary impairments/conditions contributing to clients’ support
needs, services clients are accessing and funding associated.
Page 26 of 30
Appendix 3 – Conditions not currently classified by the Ministry of
Health as a disability
Exclusions
[no content as yet]
Page 27 of 30
Appendix 4 – [Check for name of appendix]
[Page 4 notes : Who meet the access criteria for the relevant DHBs long-term support services (see
section on joint funding and definition Section 1.2 and
Appendix 4);]
[no content as yet]
Page 28 of 30
Appendix 5A – [Check for name of appendix]
[page 20 notes The NASC Process Flow Chart on page 32 of that Manual has been modified to cover
the additional steps that wil be required for LTS-CHC clients (see Appendix 5A)]
[no content as yet]
Page 29 of 30
Appendix 6 – The referral/screening information form for LTS-CHC
clients
[Need to check if DHBs al use the same form – if not remove this reference and refer to local
process or policy].
[no content as yet]
Page 30 of 30

Document 2.
NEEDS ASSESSMENT
SERVICE
COORDINATION
(NASC)
Health of Older People and Long-Term
Chronic Health Conditions
GUIDELINES TO SUPPORT
NATIONAL CONSISTENCY
2025
Document Owner
Version Endorsed by
Date endorsed
Date due for
Date
0
formal review
reviewed
Nati onal Ageing Well Team
1.1
Ageing Well
April 2025
April 2026
June 2025
Out of scope
Steering
Group
link to page 34 link to page 34 link to page 34 link to page 34 link to page 35 link to page 36 link to page 36 link to page 36 link to page 36 link to page 36 link to page 36 link to page 37 link to page 37 link to page 37 link to page 38 link to page 38 link to page 38 link to page 38 link to page 38 link to page 38 link to page 38 link to page 38 link to page 39 link to page 39 link to page 39 link to page 39 link to page 39 link to page 39 link to page 39 link to page 40 link to page 41 link to page 41 link to page 41
 1 Contents
Overview ..................................................................................................
1 Contents
Overview .................................................................................................. Error! Bookmark not defined.
1.1
Document Purpose ................................................................................................................ 3
1.2
NASC Role and Responsibilities .............................................................................................. 3
1.3
Underlying Principles of NASC ................................................................................................ 3
1.4
Māori Health .......................................................................................................................... 3
1.5
Service Function .................................................................................................................... 4
2
Access .................................................................................................................................... 5
2.1
Eligibility Criteria for Health of Older Persons and LTS NASC Service ......................................... 5
2.2
Service Inclusions .................................................................................................................. 5
2.3
Consent ................................................................................................................................ 5
2.3.1
Consent for clients without capacity ............................................................................... 5
3
Assessment, Review and Re-assessment ................................................................................. 5
3.1
Review ................................................................................................................................... 6
3.2
Reassessment ....................................................................................................................... 6
3.3
Discharge .............................................................................................................................. 6
4
Various Funding Streams ......................................................................................................... 7
4.1
Transition Between Funding Streams ...................................................................................... 7
4.2
Dual Funding ........................................................................................................................................... 7
5
Guidelines for Prioritisation ..................................................................................................... 7
5.1
Prioritisation .......................................................................................................................... 7
5.2
Very High-Risk Clients ............................................................................................................ 7
5.3
Referral Information ............................................................................................................... 7
5.4
Timeframes ........................................................................................................................... 7
6
interNASC transfer principles .................................................................................................. 8
7
interRAI Assessment ............................................................................................................... 8
8
Cultural Considerations .......................................................................................................... 8
8.1
Culturally Appropriate Assessment Model (CAAM) ................................................................... 8
9
Allocating Home and Community Support Services (HCSS) ....................................................... 8
9.1
Current Context (fee for service and restorative casemix bulk funded HCSS models) ................. 8
9.2
Access .................................................................................................................................. 8
9.3
Restorative HCSS - Casemix Model Overview .......................................................................... 9
9.4
Paid Family Carer ................................................................................................................. 10
10 Allocating Respite .................................................................................................................. 10
10.1
Purpose ............................................................................................................................... 10
1
link to page 41 link to page 42 link to page 42 link to page 42 link to page 42 link to page 42 link to page 42 link to page 43 link to page 43 link to page 43 link to page 44 link to page 44 link to page 44 link to page 44 link to page 45 link to page 45 link to page 45 link to page 45 link to page 45 link to page 45 link to page 45 link to page 45 link to page 46 link to page 46 link to page 47 link to page 48 link to page 49 link to page 51 link to page 52 link to page 52 link to page 56 link to page 57 link to page 59 link to page 60 link to page 60 link to page 62
 10.2
Criteria ................................................................................................................................ 10
10.3
Respite Options ................................................................................................................... 11
10.3.1
Residential Care ............................................................................................................... 11
10.3.2
Residential Respite in Secure Care ................................................................................ 11
10.3.3
Day Programmes .............................................................................................................. 11
10.3.4
Carer Support ................................................................................................................... 11
11 Individualised Funding (IF) ...................................................................................................... 11
12 Admission to ARC ................................................................................................................... 12
12.1
Pathway to Permanent Residential Care ................................................................................ 12
12.2
Determining ARC Level of Care ............................................................................................. 12
12.3
Short Term Residential Care ................................................................................................. 13
12.4
Residential Care Subsidy ...................................................................................................... 13
12.5
Residential Support Subsidy ................................................................................................. 13
12.6
Residential Care Loan .......................................................................................................... 13
12.7
Key Information in Relation to the ARRC Contract .................................................................. 14
12.7.1
Change of Level of Care .................................................................................................. 14
12.7.2
Appeals Process .............................................................................................................. 14
12.7.3
Premium Room Charges ................................................................................................. 14
12.7.4
Notification for One Hospital-level Resident to be Cared for in a Rest Home Service
Area (NOHRRA) ................................................................................................................ 14
12.7.5
Continuation of Payments during Resident Temporary Absence in ARC - Hospital and
10.2
Criteria ................................................................................................................................ 10
10.3
Respite Options ................................................................................................................... 11
10.3.1
Residential Care ............................................................................................................... 11
10.3.2
Residential Respite in Secure Care ................................................................................ 11
10.3.3
Day Programmes .............................................................................................................. 11
10.3.4
Carer Support ................................................................................................................... 11
11 Individualised Funding (IF) ...................................................................................................... 11
12 Admission to ARC ................................................................................................................... 12
12.1
Pathway to Permanent Residential Care ................................................................................ 12
12.2
Determining ARC Level of Care ............................................................................................. 12
12.3
Short Term Residential Care ................................................................................................. 13
12.4
Residential Care Subsidy ...................................................................................................... 13
12.5
Residential Support Subsidy ................................................................................................. 13
12.6
Residential Care Loan .......................................................................................................... 13
12.7
Key Information in Relation to the ARRC Contract .................................................................. 14
12.7.1
Change of Level of Care .................................................................................................. 14
12.7.2
Appeals Process .............................................................................................................. 14
12.7.3
Premium Room Charges ................................................................................................. 14
12.7.4
Notification for One Hospital-level Resident to be Cared for in a Rest Home Service
Area (NOHRRA) ................................................................................................................ 14
12.7.5
Continuation of Payments during Resident Temporary Absence in ARC - Hospital and
Social Leave (bed extensions) ........................................................................................ 14
12.7.6
Exiting ARC ....................................................................................................................... 15
13 Appendices ............................................................................................................................ 15
Appendix 1: HCSS Casemix service response ........................................................................... 16
Appendix 2: Client Funding pathways ........................................................................................ 17
Appendix 3: interNASC transfer principles ................................................................................ 18
Appendix 4: interRAI Assessment Types .................................................................................... 20
Appendix 5: SAT screening questionnaire .................................................................................. 21
Appendix 6: Individualised Funding – Purchasing Guidelines .................................................. 22
Appendix 7: Checklists for Entry to Care .................................................................................... 25
Appendix 8: Determining a Resident Subsidy Type ................................................................... 27
Appendix 9: Applying ARRC clause A13 to Premium Room Charges ....................................... 28
Appendix 10: Approving continuation of payments during resident temporary absence in
ARC .......................................................................................................................... 29
Appendix 11: Key Terms and Processes ........................................................................................ 31
2

1.1 Document Purpose
The purpose of these guidelines is to foster consistency among NASCs nationwide. This is a living
document, and Ageing Well will work with NASC on any changes moving forward.
The document also acts as a repository of approved nationally consistent ageing well policy which
supports the desired shift across Health NZ to deliver services and funding in a more consistent
manner.
The document will be formally reviewed in 12 months. Any significant changes made in the interim
will be communicated to NASC via Ageing Well.
1.2 NASC Role and Responsibilities
The role of the Need Assessment Service Co-ordination (NASC) is to work with older people and
those with long term chronic health conditions to help identify their needs and outline what
support services are available. NASC support goal setting and enable access to Health New
Zealand - Te Whatu Ora funded support services and assist with accessing other supports as
required.
NASC focus should remain on making evidence-based clinical decisions that optimise client
outcomes. Maintaining objective clinical reasoning is essential to ensure decisions are
consistently justified. The use of interRAI provides the framework for making clinically informed
decisions.
1.3 Underlying Principles of NASC
The principles underpinning assessment and provision of support are:
• Clients are encouraged and supported to maximise independence, enabled to continue to
participate and contribute to their own wellbeing, their families and the wider New
Zealand community. Factors influencing the ability to access services and participate in
their community include health status, income and access to other resources such as
transport.
• Service processes are transparent and equitable for the population and their whānau.
• Clients are assessed using appropriate assessment tools to ensure people get the care
that they require.
1.4 Māori Health
NASC will work within the Pae Ora framework of Pae Tū: Hauora Māori Health Strategy.
Pae ora reflects a holistic, indigenous worldview and includes three interconnected elements:
mauri ora, whānau ora and wai ora. Improvements must be made across each of these elements
for Māori to live with good health and wellbeing. Meeting our obligations under Te Tiriti o Waitangi
will ensure Māori can live longer, healthier, and more independent lives.
Pae Tū enhances and builds on the momentum of both He Korowai Oranga: Māori Health Strategy
and Whakamaua: Māori Health Action Plan 2020–2025. It reaffirms the vision of ‘pae ora – healthy
futures for Māori’, and the four outcomes set out in Whakamaua, which provide an important
focus for collective action:
3

• Outcome 1: Whānau, hapū, iwi and Māori communities can exercise their authority to
improve their health and wellbeing
•
Outcome 2: The health system is fair and sustainable, and delivers more
•
equitable outcomes for Māori
•
Outcome 3: The health system addresses racism and discrimination in
•
all its forms
•
Outcome 4: The inclusion and protection of mātauranga throughout the
NASC policies and practices will demonstrate measurable benefit to Māori, including
demonstration of:
•
service that will equitably and directly deliver on Māori health priorities,
•
workforce training focused on the delivery of services to Māori including understanding of
Māori principles/tikanga (for example CAAM), and
•
client and whānau feedback on how they believe the NASC has delivered in relation to
Māori values and beliefs.
1.5 Service Function
• Triage incoming referrals according to prioritised need
• Manage waitlists
• Conduct culturally appropriate Needs Assessments to identify specific needs (see section
8.1)
• Identify client needs via appropriate assessments (utilising interRAI for those over 18) and
provide options for services
• Explore options with the person/carer and coordinate services tailored to individual needs
• Review as required
• Manage residential care placements in accordance with Entry to Care guidelines
• Maintain an updated register of contracted service providers and distribute service
information to clients
• Liaise with community agencies and services
• Reassess needs in response to significant changes in need and/or circumstances
• Collaborate with individuals and their support network to enhance independence
• Offer advice, information and support to individuals, families and the community
• Ensure a clear whānau support plan is in place, in line with aged care funding and service
provision
• Identify, review and refer needs to other appropriate services (e.g. National Travel
Assistance, Total Mobility Scheme and other clinical services such as district nurses,
allied health) as appropriate
• Support applications for and referrals to Equipment and Modification Service (EMS)
funding
• If identified as a need, arrange meetings between individuals, their support network, and
service providers
• Work in partnership with key aged care service (e.g. HCSS and ARC) providers in providing
effective and sustainable services for clients
• Escalate any issues related to contractual obligations or direct impact on funding to
Health NZ funder.
4
link to page 36

2 Access
2.1 Eligibility Criteria for Health of Older Persons and LTS NASC Service
Eligibility for NASC services is outlined
in Health and Disability Services Eligibility Direction 2011.
Being eligible grants individuals the right to be considered for publicly funded health or disability
services if they meet the access criteria, which may be provided fully funded or at a subsidised
cost. Eligibility for foreign nationals is primarily determined by immigration status.
2.2 Service Inclusions
Referrals can be received from a clinical or community service, including self-referral. To be
accepted for assessment, the client will have a functional need related to age, or, a long-term
chronic health condition with very high need
s1. Clients under the age of 65 would be eligible for
service under health if their disability is related to health-related needs.
If the client presents for the first time after the age of 65 and has a physical, intellectual, or
sensory disability then they do not meet DSS inclusion criteria as per the ‘New Deal in 1992’
cabinet paper and would therefore be health funded.
If a person qualifies for funded support by a different funding stream (e.g. ACC), it is expected that
that funder will fund their support services.
2.3 Consent
The assessor will seek informed consent from the person or person entitled to make decisions on
their behalf, at the time of triage in adherence to the Code of Health and Disability Services
Consumers’ Rights 1996 and other relevant legislation (see link to section 12 Legislation). Consent
will be regularly revisited at times while the client is in contact with the service.
2.3.1 Consent for clients without capacity
If the client’s enduring power of attorney (EPOA) for Personal care (health) and welfare has been
activated, or there is a welfare guardian appointed by the court, this person must provide consent
on behalf of the client. EPOA documentation and activation must be documented on interRAI and
a copy held on file by both the NASC and if the person is in residential care, the provider.
If there is uncertainty regarding the persons capacity to make personal care and welfare
decisions, and there is no enacted (activated) EPOA or court order appointment around welfare
guardianship, then this will need to be referred to the persons GP or another appropriate health
professional, for assessment and follow up to ensure the NASC process can progress.
3 Assessment, Review and Re-assessment
All people over 65 accessing support are required to have had a comprehensive clinical
assessment using the suite of interRAI tools to enable appropriate support in the home or
residential care environment and improve outcomes for clients.
1 Very high need for this service is defined as: - requiring assistance with activities of daily living at least daily to remain
safely in their own home - the person’s wellbeing and functional status is deteriorating, their needs are increasing and
safety issues are becoming apparent
5

All people 18-65 accessing support are required to have had a comprehensive clinical age-
appropriate assessment to enable appropriate support in the home or residential care
environment and improve outcomes for clients.
Currently an interRAI assessment for under 18 is not available in NZ, therefore an alternative
appropriate assessment tool should be used for those aged 0-18.
3.1 Review
A review is where the individual support plan is reviewed to ensure service delivery is meeting the
client’s current support needs. The client will receive a review if:
• There has been a change in need; or
• Clinical judgement indicates a review is necessary; or
• A request for review is received and is clinically indicated; or
• The client is due for a review as per the agreed review schedule.
A client or their authorised agent may at any time request a review if the service is not meeting
their needs.
3.2 Reassessment
A reassessment refers to when the client requires a new assessment using an interRAI (or another
tool for people under 18) assessment tool. A client will be reassessed if:
• There has been a significant change in need, and the existing assessment no longer
accurately reflects the client’s needs; or
• The client requires entry into Age Residential Care and
o the current assessment is more than six months old; or
o the assessment does not accurately reflect the client’s need.
Review and reassessment target timeframes for districts delivering the new restorative bulk
funded casemix is described in Appendix 1. This may not be relevant to a number of NASC
agencies who are not operating in regions and districts where this new casemix models have been
adopted.
3.3 Discharge
A client may be discharged from NASC for one or more of the following reasons:
• Needs are being met by a different service/funder (e.g. ACC)
• Relocated out of a geographic region (if the client is remaining in Aotearoa, see Inter NASC
Transfer and associated principles)
• The client is deceased
• If someone has improved to the point of not currently requiring services, the client can be
made inactive on interRAI but not discharged.
Note - support may have been declined by the client for various reasons, or they have decided
they no longer wish to receive support; however, they may continue to be active on the NASC
caseload.
6

4 Various Funding Streams
Appendix 2 provides information about Client Funding pathways.
4.1 Transition Between Funding Streams
Client clinical status is determined based on the driving cause of the need, rather than age. A
client supported by the long-term chronic health conditions, disability or mental health funding
streams will not automatically be transitioned onto the HOP funding stream when they turn 65,
unless their primary needs become an age-related need. This should be a clinical decision as to
when the transition should occur based on the presence of any age-related needs.
4.2 Dual Funding
Some clients have complex needs, which may be impractical to support via a single funding
stream. In cases where the client meets criteria across multiple funding areas, joint funding or
shared service arrangements may be required. An example of an appropriate case where dual
funding would be necessary would be if a client meets MSD DSS eligibility and access criteria (i.e.,
a person is eligible for DSS assessment and support) and has additional age-related needs.
In complex situations where the cause of impairment is unclear (e.g. injury vs acquired) or a
person has multiple impairments/causes of impairments, NASCs and other support services and
funders need to determine a pragmatic joint funding/shared services arrangement to support
prompt access to essential supports. Close working relationships with other services and funders
are required to determine this agreement.
It is acknowledged that cases requiring possible dual funding are challenging and there is
currently no formal process described for decision making. If a client's funding pathway is
unclear, the NASC should engage with other funding streams and the Health NZ funder to discuss
individual cases.
5 Guidelines for Prioritisation
5.1 Prioritisation
Clients’ assessment and service coordination should be prioritised based on need and safety.
5.2 Very High-Risk Clients
NASCs must make every effort to ensure placement or support allocation is in place promptly and
in consideration of the associated risks. In case of limited provider availability, NASC should
consider options such as a multiple provider packages and engage support from Health NZ
funder.
5.3 Referral Information
NASCs will make the decision on prioritisation based on the initial information received; if not
possible, more information will be gathered from the referrer. The allocation of prioritisation
should be changed as more information is gathered.
5.4 Timeframes
The target timeframes for assessment and coordination should be based on your agreed district or
regional prioritisation processes. For a change of level of care in ARC, refer to section 12.7.1.
7

6 interNASC transfer principles
Each NASC will have their own detailed inter-NASC transfer process, however, it is expected that
NASC will follow the agreed interNASC transfer principles described in Appendix 3.
7 interRAI Assessment
All Health NZ Health of Older People assessments are completed on the nationally mandated
web-based electronic assessment tool, interRAI. It is recommended that interRAI assessments
are also used for people with Long Term Chronic Health Condition interRAI where appropriate.
interRAI assessments offer a standardised, comprehensive approach to evaluating individuals'
health and social needs. These assessments facilitate person-centered care planning, enhance
communication among healthcare professionals, and support quality improvement initiatives.
Additionally, interRAI assessments contribute valuable data for research and policy development
in healthcare. Below is a list of validated interRAI assessment types. For a full description of the
description of each assessment type see Appendix 4.
• Contact Assessment (CA)
• Home Care Assessment (HC)
• Long Term Care Facility Assessment (LTCF)
• Acute Care Assessment Tool (AC)
• Palliative Care Assessment Tool (PC)
• Community Health Assessment (CHA)
8 Cultural Considerations
8.1 Culturally Appropriate Assessment Model (CAAM)
A culturally appropriate assessment model (CAAM) that is responsive to and aligned with Te Ao
Māori was developed to contribute to achieving equitable access to health services and health
outcomes. The CAAM integrates tikanga, whakawhānaungatanga and manaakitanga principles,
offering a framework for interRAI Home Care assessments for Māori. Aligning with Te Ao Māori,
CAAM enhances access to equitable health services and outcomes, while bolstering mātauranga
Māori within the health and disability system. This model complements the interRAI assessment
process. Whilst not mandatory, NASC assessors and leaders are encouraged to complete this
training.
9 Allocating Home and Community Support Services (HCSS)
9.1 Current Context (fee for service and restorative casemix bulk funded HCSS models)
Health NZ is aiming to move to a nationally consistent restorative bulk funding model for HCSS.
Some districts have traditional fee-for-service (FFS) funding arrangements, and some districts
have restorative bulk funding models.
9.2 Access
The eligible population is initially screened using a Service Allocation Tool (SAT) (see Appendix 5)
to determine whether a client is complex or non-complex and which type of interRAI tool is
appropriate to assess the client. The pathways for complex and non-complex clients vary,
8

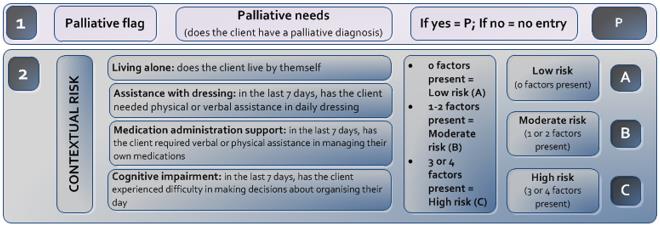
including the assessment type used and whether the interRAI assessment is undertaken by either
NASC or the HCSS provider.
Should the client answer yes to any of the screening questions in Appendix 5, then the client is
placed into the complex category and will receive an HC interRAI. If not, then they are placed into
the non-complex category and a CA will be carried out. If local practice in your district is for the
referrer to complete the SAT tool and there are concerns about the client's complexity pathway,
this can be flagged by either the provider or the NASC and changed accordingly.
On completion of the SAT tool a contextual risk rating will be assigned as described in Figure 1. The
calculated risk score will be included in the referral to the HCSS provider to determine the service
response time required in the National HCSS Service Specification. If providers in the service
region have not transitioned to the National HCSS Service Specification, please use the risk
assignment process as determined by the existing contractual requirements with relevant
providers.
Figure 1: Contextual Risk Rating Tool
9.3 HCSS Restorative, casemix, bulk funded model - overview
The National HCSS restorative bulk funded model uses the University of Auckland (UoA) Casemix
methodology to form groups of people with similar needs. These groups or “cases” collectively
form a “casemix” which describes the range of different groups with similar levels of assessed
needs. The casemix informs a bulk funding payment arrangement which enables providers to
deliver a flexible service response.
The client Casemix is determined using the interRAI assessment outcomes scores. The Casemix
algorithms enable HCSS providers to identify high-level client goals and service response
expectations. See Appendix 1 for the Casemix service response model included in the revised
National HCSS Service Specification.
HCSS providers will work in partnership with clients and their whānau and support networks to
develop and agree goals and document these in the clients’ individual support plan. Providers will
deliver services to facilitate achievement of the agreed client’s goals. NASC will re-assess the
client depending on the complexity allocated by Casemix level.
9

9.4 Paid Family Carer
All people eligible for HCSS can choose to have a whānau or family member, or any carer of their
choice provide this care. The carer is employed by a HCSS provider to deliver the agreed services
to their chosen client who may be a whānau or family member. A whānau or family member can
become a paid carer if they are:
•
16 years or over,
•
physically able to perform the necessary tasks, and
•
available to attend to the person according to their care plan.
The allocation is as per usual HCSS guidelines to cover essential tasks such as showering and
dressing and does not include items such as supervision.
For more information see the website
here.
10 Allocating Respite
10.1 Purpose
The purpose of respite care is to provide temporary relief to unpaid carers while ensuring that the
client utilising respite services has their needs met. How respite is utilised is unique to the
situation of individual clients and carers. Respite can be allocated via the following means:
• Facility-based respite care (e.g. a short-term stay at an Aged Residential Care (ARC)
facility)
• Day Programmes (including in home day respite)
• Carer Support (purchasing of items and/or services)
10.2 Criteria
Respite should be allocated for clients who have at least one full-time carer. The amount of respite
allocated should be guided by the need required by the carer. This should be informed by the
amount of unpaid support the carer provides. In addition to the quantity of support, the intensity
of support required, and risk of carer stress should also be considered. Funded respite options
vary across New Zealand, and allocation should be based on the options available in each
region/district.
Clients who live alone are not typically eligible for residential respite unless in exceptional
circumstances. This could include accessing short-term residential care to avoid admission to
hospital or permanent residential care, or to facilitate timely discharge from hospital (if funding is
available in your region).
In some regions the NASC may allocate day programmes to individuals for reasons for social
isolation and loneliness.
10

10.3 Respite Options
10.3.1 Residential Care
Clients and their full-time carers/whānau can access residential respite for the client for a period
agreed with the facility. Clients/carers should be made aware at the time of allocation that the
ability to use this form of respite is subject to bed availability at ARC facilities. Clients and
carers/whānau are responsible for monitoring the usage of any funded allocated respite.
10.3.2 Residential Respite in Secure Care
Facility-based short-term care (or respite) delivered in a secure facility should only be arranged for
clients with an enacted EPOA or welfare guardian. This must be supported by an appropriately
qualified physician.
In an emergency situation where, secure care is required and an activated EPOA is not in place,
NASC should use their discretion when considering admission to secure care e.g., the client or
their carer is at risk. Admission in these circumstances should be for a time-limited period and
must be agreed with the main carer, family or whānau, and the provider. This must be agreed with
an appropriately qualified physician under an approved legal framework. The Health and Disability
Commissioner (Code of Health and Disability Services Consumers’ Rights) Regulations 1996,
clause 7.4 is an example of this.
10.3.3 Day Programmes
Day programmes are organised group activities in the community that provide respite for full-time
carers or support social relationships. Clients living alone who are at risk of social isolation or
loneliness may also be eligible for day activities. Respite in a person’s home is also available in
some districts.
10.3.4 Carer Support
Carer Support is a subsidy to partially reimburse full-time carers for the cost of care and support
associated with taking a break from care duties. It should be clearly explained that carer support
is not designed to employ a person formally and is a contribution to the costs of having someone
(or something i.e., equipment) help relieve a carer. The purchasing guidelines for Carer Support
can be found
here.
11 Individualised Funding (IF)
Individualised Funding (IF) is a model of funding that gives individuals and their families more
control over the support services they receive. This approach offers flexibility in choosing and
managing support workers or service providers based on personal needs and preferences. The
funding is held by a contracted host agency, and the person or their agent is the employer and
takes on all employment responsibilities.
Situations where IF may be appropriate include, but are not limited to, clients in the following
scenarios:
• Option of employment of family or whānau to provide care through an arrangement where
an HCSS provider is unavailable to employ the whānau/family member as per section
8.3.4
11

• Living in a remote area where support services would be difficult to access
• Has specific requirements relating to the provision of their care, which would be difficult
to fulfil via traditional support services (e.g. cultural or religious requirements).
It is important to note that IF should only be allocated to clients with suitable support networks
(whānau, friends, acquaintances) who are available to provide support or have the capability to
employ support workers.
IF should not be allocated to clients who do not have either:
• Capacity to manage their allocated IF budget, or
• At least one suitable person to act as an agent/employer for their budget
IF is not available in all district/regions, therefore any discussions for IF for a client should be
discussed immediately with Regional Planning, Funding and Outcomes teams to ensure that
either a) IF is available in the district/region b) the client would meet the criteria for IF.
The purchasing guidelines for IF can be found in Appendix 6.
12 Admission to ARC
ARC is crucial in supporting individuals who need assistance with daily activities due to age-
related conditions, long term chronic health conditions or disabilities.
12.1 Pathway to Permanent Residential Care
Entering aged residential care in New Zealand involves a pivotal decision for clients and their
family and whānau. It is guided by health needs and assessed using the HC interRAI assessment
tool. This tool considers factors such as health status, mobility, cognition, and daily living skills to
determine the appropriate level of care required. The assessment should be no older than six
months old as per requirements of the national ARRC agreement and should accurately reflect the
client’s needs.
The decision to enter residential care marks a significant transition, impacting quality of life and
requiring careful consideration of medical requirements, social support, and personal preferences
to ensure the chosen facility effectively meets the resident's needs.
12.2 Determining ARC Level of Care
If an assessment indicates the need for residential care, and a client/their legal agent decides to
transition into care, the Entry to Care guidance tool (see Appendix 7) should be used to determine
level of care. These checklists should be used in conjunction with clinical judgment. The checklist
helps understand the interRAI data to support this decision.
The least restrictive level of care should be considered and trialled before higher levels. The four
levels of care are:
• Rest Home
• Continuing Care (previously known as hospital)
• Dementia
• Psychogeriatric / Hospital Specialised
12

12.3 Short Term Residential Care
Alongside the use of short-term residential care for respite, short periods in residential care may
be utilised for avoidance of acute admission or a period of recovery post-acute admission. Follow
your local process for short term residential care placement.
Age Residential Care Funding
NASC is responsible for determining eligibility for entry into ARC under the ARRC agreement, as
well as what level of care. This determination may require input from other clinicians depending on
care level i.e., a Psycho-Geriatrician for psychogeriatric care.
12.4 Residential Care Subsidy
The residential care subsidy provides a contribution towards the cost of residential care services
for eligible individuals. Eligibility is determined by the Ministry of Social Development (MSD) and is
means tested based on income, and assets. A
needs assessment certificate within the MSD
subsidy application form, as well as the funding authorisation must be completed by the NASC if
the person discloses that they intend to apply for a subsidy. For more information see
here.
12.5 Residential Support Subsidy
If the person is under 65 and their condition is not age-related, e.g. cancer, obesity, or other illness
and / or the person's needs would not fit with those in age residential care, then they should be
considered under Long Term Chronic Conditions. A funding authority
form must be completed by
NASC for clients requiring this subsidy.
People requiring residential care due to a chronic illness may receive a residential support subsidy
(rather than a Residential Care Subsidy—10.4). The facility applies for the support subsidy, so no
Residential Care Subsidy form is required.
NASCs are responsible for informing the facility about this requirement and should provide a copy
of the paperwork and advise the facility of their obligation to complete the residential support
subsidy form. If the form is not completed, MSD will not be aware that the client is in care, and
they will continue to receive their benefit (if they have one), and the facility will not get paid that
portion.
NASC should contact the designated Health NZ ARC contract manager for more information
about which ARC facilities have long-term chronic conditions contracts.
12.6 Residential Care Loan
The Residential Care Loan in New Zealand offers financial assistance to individuals who require
residential care but do not qualify for the residential care subsidy due to higher income or asset
levels. It covers the cost of accommodation and care services in aged residential facilities and is
repaid from the individual's estate after their death. The loan helps make ARC services accessible
to those with differing financial situations, with terms and conditions, including possible interest
charges, set by the government. NASC are responsible for completing the
needs assessment
certificate to access the Residential Care Loan within the Residential Care Subsidy Form, as if
they were applying for a subsidy. For more information se
e here.
See Appendix 8 to determine a Resident Subsidy Type.
13

12.7 Key Information in Relation to the ARRC Contract
12.7.1 Change of Level of Care
Under the ARRC contract, NASC have 5 days (or 10 days in an exceptional circumstance) to
approve requests for a change of level of care from the date of the request. Facilities should not
transfer clients without funding authority from NASC unless in exceptional or emergency
circumstances.
12.7.2 Appeals Process
Under the ARRC contract, providers have the right to appeal the decision on the change of level of
care assessment outcome. Providers must inform NASC of this and the reasons for their
disagreement, and NASC will decide whether to reconsider the decision or if such a decision is to
be final.
12.7.3 Premium Room Charges
If a resident wishes to be admitted to a Standard Room at a facility but a Standard Room or a
Premium Room for which Premium Room Services are not charged is not available, and there is
not an available bed within 10km of the preferred facility, then that provider is required to admit
the person with no additional charges. Note it is the preferred facility’s responsibility to find an
alternative standard bed within 10km if the client has requested admission to that facility. NASC
should contact the Health NZ ARC contract manager for any support with a provider to invoke this
clause. See Appendix 9 for how this clause within the ARRC contract is to be applied.
12.7.4 Notification for One Hospital-level Resident to be Cared for in a Rest Home Service Area
(NOHRRA)
Aged care providers are required to notify Health NZ when managing or intending to manage one
hospital-level care resident in a rest home area. This request may come to the NASC and should
be forwarded to the Health NZ funder.
For more information, see Health NZ website here
- Notification for one hospital-level resident in a
rest home service area – Health New Zealand | Te Whatu Ora.
12.7.5 Continuation of Payments during Resident Temporary Absence in ARC - Hospital and
Social Leave (bed extensions)
Under the ARRC agreement, residents are entitled to maintain funding for their bed for up to 21
days when they are in hospital, or up to 14 days for a temporary absence for social leave. Funding
for subsidised residents should always be approved if the client remains in the hospital for over 21
days. If the client is deemed not to be returning to their previous level of care, then the provider
and sector operations should be notified and the client exited from the bed. For private payers,
not in receipt of a subsidy, this is subject to their admission agreement between them and the
ARC provider. See Appendix 10 for National guidelines for approving continuation of payments
during resident temporary absence in ARC.
14

12.7.6 Exiting ARC
Residents may move between facilities should their needs change and they are no longer be able
to be supported by that facilities level of care. The funding authority form should always be dated
from the date of the departure/entry.
In instances where a person wishes to return home from residential care, it is possible to have
HCSS re-instated or engaged to support the transition. They may need to discuss with the provider
if their individual admission agreement has a notice period clause within the agreement.
For more information on the ARRC agreement, contact Health NZ contract managers or see online
agreement here for more informati
on here.
13 Appendices
1. HCSS Casemix service response
2. Client Funding Pathways
3. interNASC transfer principles
4. interRAI Assessment Types
5. Service Allocation Tool (SAT) screening questionnaire
6. Individualised Funding – Purchasing Guidelines
7. Checklists for Entry to Care
8. Determining a Resident Subsidy Type
9. Applying ARRC clause A13 to premium room charges
10. Approving continuation of payments during resident temporary absence in ARC
11. Key Terms and Processes
15
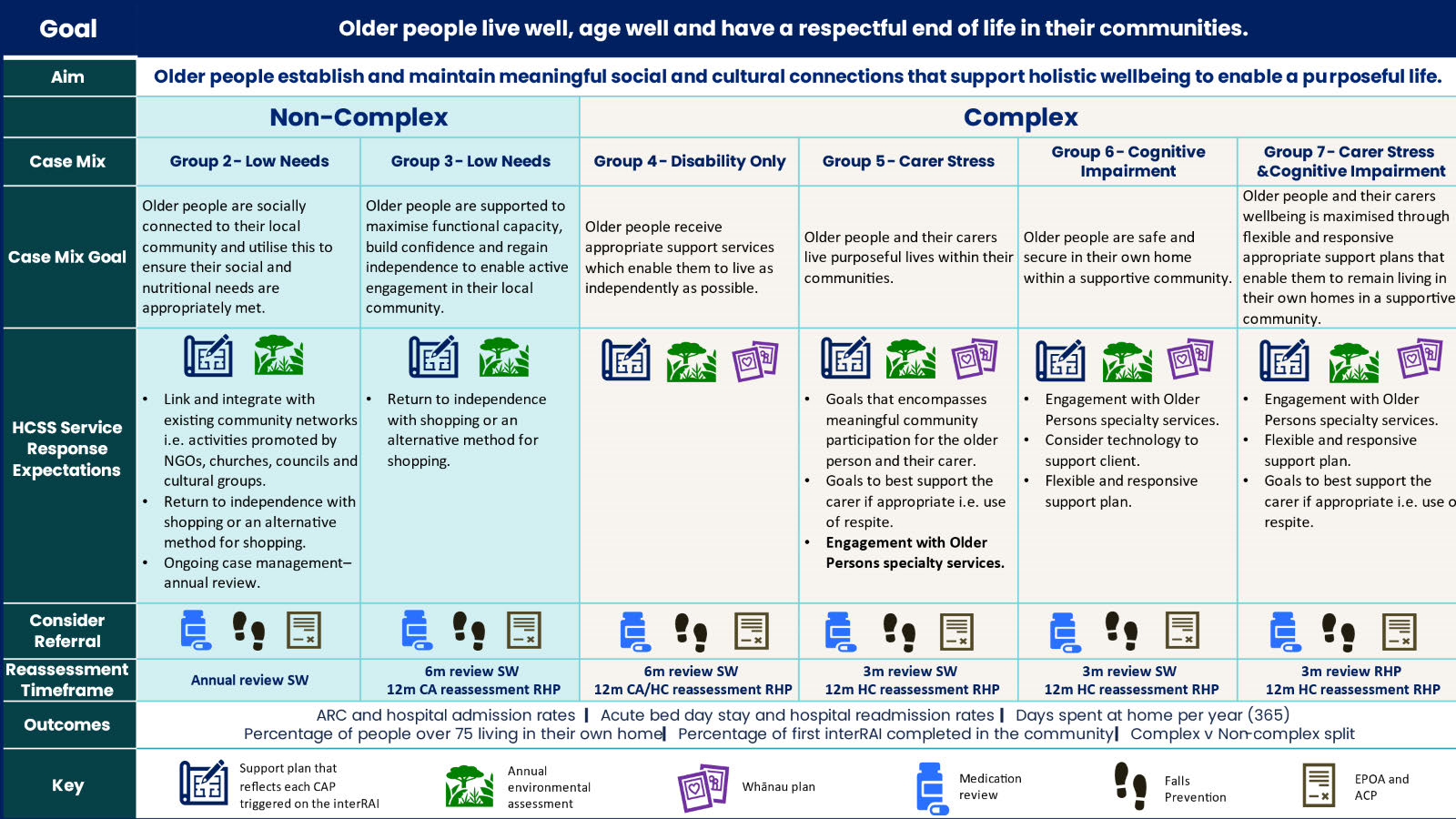
Appendix 1: HCSS Casemix service response
Restorative service model and assessment time frames for bulk funded Casemix regions operating under the revised 2025 National HCSS Service
Specification. If you re in a region that hasn’t transitioned, please refer to local contractual agreements.
Reassessment timeframes are desired best practice and may not be achievable within NASC current resourcing.
16

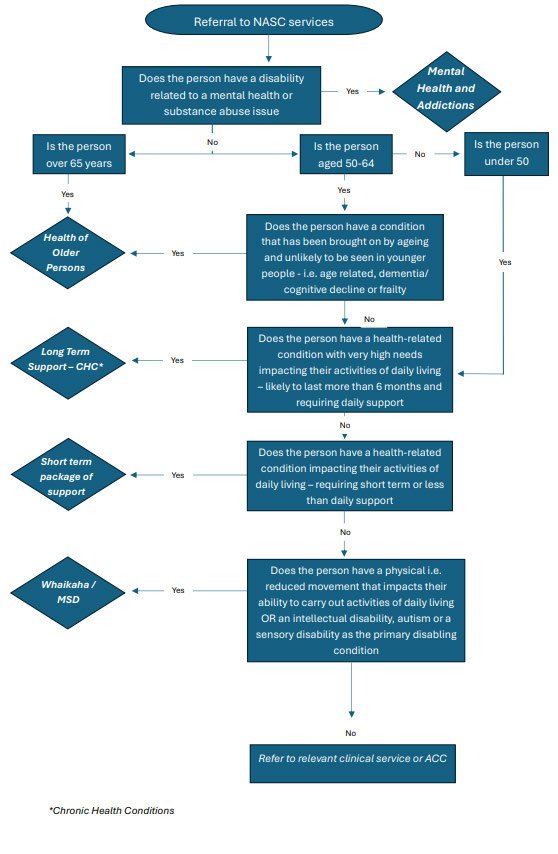
Appendix 2: Client Funding pathways
Client Funding Categorisation Pathways Flowchart
17
link to page 49

Appendix 3: interNASC transfer principles
National Principles for inter-NASC client transfers for aged care services
Overarching principles for HOP/LTS geographical inter-NASC Transfer
• People can access the services they require and are enabled to move between districts/
regions. Especially for services documented in the Service Coverage Schedu
le2.
• People have the right to options and should not be denied moving between districts
regardless of the residential care occupancy of each region i.e., beds should not be
blocked for ‘local people only’.
• NASCs receiving clients should respect the assessment and clinical decisions made by
transferring NASC colleagues.
• The transfer process should not negatively impact a person's desire to move districts and
impact on the preferences of them or their whānau to move.
• Minimum expectations should be met for all client transfers.
Minimum expectations
The transferring (i.e. sending NASC) takes responsibility for appropriate communication, including
adequate information provision (e.g. interRAI assessment, clinical information if required), and
ensuring the appropriate process of transfer steps is completed. For residential care, this
includes a HC or PC assessment that is no less than 6 months old prior to transfer. This could
include consideration of specialty service ‘handovers’ between Older Persons Mental Health or
similar.
The transferring NASC should endeavour to communicate to the receiving NASC the
intention of the client to transfer districts prior to the physical transfer.
Both transferring and receiving agencies respect the wishes of the individuals and
whānau/ families and make this central to decision-making.
The receiving NASC accepts the decision made by the transferring NASC regarding the
package of care allocated (including the level of care) if those services are available in that
area. The inter-NASC transfer process does not include an approval or denial option by
NASCs.
For ARC specifically, NASCs may run a prioritisation process (including a waitlist for
people in hospital, the community or another level of care in an ARC facility) to manage
admissions to ARC against bed availability. This can be based on client and carer need
and/or to enable hospital flow. However, this process cannot supersede instances where
an agreement has already been reached between an ARC facility and a client/their family
to admit a resident from out of district which would result in an inter-NASC transfer.
Should the receiving NASC have considerable concerns with the decisions made by the
transferring NASC, this should be escalated to the Regional Ageing Well Managers to
inform opportunities for national consistency.
If the receiving NASC believes the care level allocated to the client does not reflect the current
interRAI assessment and supporting documentation, the receiving NASC should still accept the
2 Accountability arrangements | Ministry of Health NZ
18

person at that level of care, however, communicate with the facility and the client/family this may
change upon the next assessment. Where there is significant concern about the allocated level of
care (e.g. secure care), the receiving NASC should discuss this with the client, their whānau and
the new facility.
The transferring NASC should inform clients prior to transferring that the receiving NASC
may not have all available services as per the previous district. In facility respite is an
example of this. A grandparenting approach could be considered for services where they
are available.
Process
Each NASC will have their own detailed inter-NASC transfer process, however, it is
expected that Minimum Information to be Provided as Applicable by ‘transferring’ NASC.
The transferring NASC is to attach their inter-NASC transfer form and follow the minimum
expectations.
The process should be completed in a timely manner. Information will be transferred to
another NASC within five working days of the transfer request being received (as per
national NASC service specifications). Ideally all information is transferred prior to client
moving districts unless exceptional circumstances apply.
Minimum information to be provided as applicable by ‘sending / transferring’ NASC.
1. Current interRAI assessment demonstrating a need for support.
2. Sign off by appropriately qualified medical practitioner supporting the need for
secure care
3. Referral to receiving district mental health team if required including confirmed
capacity status.
4. Evidence that client and whānau are supportive of transfer
5. Any further information supporting the geographical choice
6. Clear evidence of legal status including:
a) Are Enduring Power of Attorney (EPOA) established
b) If established, are they activated
c) Is welfare guardianship established
d) Is there a PPPR pending
7. Information on any additional supports that may be required including
a) Bariatric equipment
b) Extra HCA support for settling period
c) Infection control considerations
d) Information on any other co-morbidities including addiction management.
8. Identification of facility and evidence of facility willingness to accept.
Minimum process of transfer steps to be completed
9. Check with receiving NASC as to availability of beds in relation to local hospital
discharges and awaiting community admissions currently in process prior to
speaking to any facilities.
10. Minimum 5 business days’ notice ahead of physical transfer
11. NASC support continuity of clinical care ensuring client handover, where possible
i.e., medication prescription and administration.
19

Appendix 4: interRAI Assessment Types
All community and age residential care assessments are completed via the nationally mandated
web-based electronic assessment tool, interRAI. interRAI assessments offer a standardised,
comprehensive approach to evaluating individuals' health and social needs. They facilitate
person-centric care planning, enhance communication among healthcare professionals and
support quality improvement initiatives. Additionally, interRAI assessments contribute valuable
data for research and policy development in healthcare.
Contact Assessment (CA)
A contact assessment serves as an initial screening tool that offers essential clinical information
to guide decisions regarding the necessity and priority for a further comprehensive Home Care
assessment (HC). It is primarily used for the ongoing evaluation of individuals with non-complex
needs who reside within the community.
Home Care Assessment (HC)
The HC interRAI assessment tool is utilised for comprehensive and systematic evaluation of
individuals receiving home care services.
Periodic reassessments are crucial to monitor changes in the client's health status over time.
Assessment findings guide the development of personalised care plans, facilitate communication
among care providers, and ensure documentation of client information in health records.
Long-Term Care Facility Assessment (LTCF)
LTCF assessments are conducted by aged residential care facility staff. They focus on evaluating
residents' needs and determining their needs within the context of their long-term placement. As
per the ARRC agreement, LTCF assessments should be completed within 21 days of entry into
aged residential care when a resident’s needs have changed and every 6 months thereafter.
Acute Care Assessment Tool (CA)
The Acute Care assessment tool should be used for clients in an inpatient ward. It should be used
to determine immediate care needs. Then, the client should either be discharged home with a
package of support or placed into short-term residential care awaiting assessment for either
permanent care placement or home-based supports.
Palliative Care Assessment Tool (PC)
The Palliative Care Assessment Tool (PC) should be used when a person is identified as needing
palliative care or end-of-life care services. It helps assess and document the specific needs of
individuals requiring such specialised care, ensuring appropriate and tailored support and
services are provided to them.
Community Health Assessment (CHA)
The Community Health Assessment (CHA) is used to assess individuals' health and social care
needs across various settings, from independent residences to assisted living. Although not used
extensively in New Zealand, the CHA may be more appropriate than the Home Care assessment
tool (HC) when individuals require a broader assessment scope, have complex health needs,
particularly mental health needs, or when integration with other healthcare services using the
interRAI system is necessary.
20

Appendix 5: SAT screening questionnaire
Lead Issue
Screening Question
•
Cognitive
Does the client have a cognitive impairment that affects their everyday life
impairment
through a decreased ability to think, concentrate, remember ideas and
make safe decisions?
•
Progressive
Does the client have a progressive neurological condition such as
neurological
Parkinson’s Disease, Multiple Sclerosis or Huntington’s Disease that
condition
requires daily support?
•
Carer stress
Is the client’s carer unable to continue caring for the client or feeling
overwhelmed or distressed, and/or there are abuse and neglect concerns?
•
Dressing
Does the client require ongoing/long-term physical assistance with daily
dressing of their lower body? (does not include application or removal of
compression hosiery).
•
Medication
Does the client require ongoing/long-term verbal or physical assistance in
Management
managing their own medications?
•
Mood
Does the client have fluctuating anxiety, low mood, other mental illness, or
experience chronic pain that significantly impacts daily living?
Should the client answer yes to any of the screening questions, then the client is placed into the
complex category and will receive an HC interRAI. If not, then they are placed into the non-
complex category and a CA will be carried out.
21

Appendix 6: Individualised Funding – Purchasing Guidelines
Background
These purchasing guidelines set out Health New Zealand / Te Whatu Ora’s (Health NZ)
expectations and requirements on the use of individualised funding (IF) packages. The guidelines
are to ensure that fiscally responsible arrangements are in place to support the use of public
funds and that IF allocations are applied in the manner intended.
The IF Host Provider is required to review payment claims against the guidelines and escalate any
claims, which are outside the scope or contrary to the guidelines to their Commissioning manager
in Health NZ.
Criteria
There are three criteria that must be met in order to use IF for support.
Criterion 1: The purchase fits with the purpose of the funding
The IF packages are intended to enable people who have been assessed by NASC (Needs
Assessment Service Coordination) as requiring Home and Community Support Services (HCSS) to
manage and direct their own HCSS.
Health NZ currently allocates up to three categories of HCSS:
• personal care – services to assist with activities of daily living e.g. personal hygiene,
toileting, transfers and mobility, feeding and medication oversight
• household management – services to assist with domestic arrangements e.g. cleaning,
laundry and meal preparation
• respite – services to provide the full time carer with a break.
IF claims must be for services within the categories listed above and must be in line with any
requirements specified in the person’s care plan.
Criterion 2: The purchase aligns with the Support Plan
HCSS purchased by a person must align with the goals of their Support Plan. NASC ensures the
person’s goals are documented in the Support Plan, which then guides the development of the
Individual Service Plan (ISP).
Criterion 3: The purchase is cost effective
The following requirements are to ensure a cost effective approach:
• support must be at a market related price and within the allocated budget
• services that are already wholly or partly funded by Whaikaha, ACC or other public
organisations cannot be purchased using the IF allocation
• a claim must not exceed a person’s IF allocation (usually allocated for a one-year period).
The IF Host Provider will monitor IF claims and highlight with the individual when their
year to date expenditure extrapolated will exceed their allocation prior to the time period
expiry date; thus allowing time for the individual to take remedial action. If remedial
action is not taken the case will be escalated to Health NZ.
Other considerations
Administration costs
Health NZ acknowledges that there is an increased level of responsibility with managing and
coordinating an individual’s care including employment and management of support workers
/caregivers as well as administrative tasks to facilitate these arrangements.
People are able to elect the level of administrative support they require from the IF Host Provider
with the fees for this paid for at an agreed rate from the individual’s IF allocation. A person can
22

also claim, from their IF allocation, actual and reasonable administration costs that they incur in
managing their support arrangements, provided these are direct costs from an external source
(e.g. employment advertisement costs).
Where a person has engaged a whānau/family member or close associate to support them with
management and administration, they may elect to award that person an honorarium (to cover
incidentals) of up to $300 per annum, from their IF allocation. Where a support package is fewer
than 12 months, the value will be calculated on a pro-rata basis.
Evidence of expenditure
Evidence of expenditure to support claims for payment must be provided to the IF Host Provider.
This will include timesheets for staff or contractors, receipts and invoices. Health NZ may request
to inspect these records at any time.
Legal obligations
People receiving an IF support package must ensure that they comply with all relevant legal
obligations including, but not limited to, employment, health and safety, Kiwi Saver, ACC, pay
equity and immigration.
Claims outside the scope of these guidelines
If a person wishes to purchase goods and services outside the scope of these guidelines, the IF
Host Provider shall seek clarification from Health NZ on whether the proposed claim can be paid
from the person’s IF allocation before any purchases are made. Health NZ will consider the
request and respond to the IF Host provider in a timely manner with its decision, which the IF Host
Provider will then convey to the individual making the request; all decisions will be final.
Retrospective payments for non-approved purchases will not be reimbursed.
Exclusion criteria
The IF allocation cannot be used to purchase goods, services and utilities that the person would
reasonably be expected to pay for if they did not require HCSS:
• utilities e.g. electricity, gas, water, phone
• general household fittings, furniture and whiteware goods
• standard electrical goods and consumer products
• food, groceries and other common household goods e.g. cleaning products, hygiene
products
• supplies for support workers e.g. tea, coffee, hygiene products
• mortgage payments, rent or rental assistance
• general vehicle purchase, modifications, maintenance
• house, contents, life or other insurance
• tickets to movies, shows, sporting events
• repayment of personal debt
• donations to charitable or church organisations
• personal travel expenses
• CCS disability parking cards
• alcohol, tobacco, nicotine products
• professional services unrelated to HCSS or management of the IF arrangement
• complementary therapies and non-government funded or subsidised health treatment or
pharmaceuticals.
In addition to the above, the IF allocation cannot be used to:
• pay the primary caregiver to provide respite care
• purchase anything illegal
• purchase assessed health services that are funded elsewhere.
23

It is the responsibility of the person (or their delegate), with the support of the IF Host Provider, to
ensure that all purchases meet these guidelines.
A person can contact the NASC if there are any queries relating to these purchasing guidelines
and how they apply to the individual’s situation.
Version
Endorsed by
Date endorsed
Date due for review
1
Ageing Well Steering Group
April 2024
24

Appendix 7: Checklists for Entry to Care
Rest Home and Hospital Levels of Care
Rest Home Level
Observations
To consider a client for entry to care, both of the following should be met:
• Client has had an interRAI assessment completed within the last six months (as
per policy) which accurately reflects the current need, and resulted in the need for
residential care
• All options to safely support the client in the home environment with the use of
community-based or natural support have been exhausted
interRAI Indicators
Answer
•
Minimum 4/5 of indicators 1-5 plus indicator 6, as per below: •
Exception: If no carer present, exclude indicator 3.
3/4 remaining indicators required, plus indicator 6. 1 CAP: Behaviour
• Not triggered
2 CAP: Institutional Risk (HC only)
• Triggered
ONLY APPLICABLE IF CLIENT HAS A CARER
Question P2A: Informal helper(s) is unable to
3 continue in caring activities (HC only)
•
OR
Yes
Question P2B: Primary informal helper expresses
feelings of distress, anger, or depression (HC only)
4 Outcome Scale: Aggressive Behaviour
• Score 0-6
5 Outcome Scale: Fracture Risk
• Score 4-8
6
Rest Home Level Care only:
•
Outcome Scale: ADL Long Form
Score 5-11
Hospital Level
•
As above for Rest Home Level Care, excluding indicator 6 and 3 if applicable •
PLUS at least one of the following:
7 Outcome Scale: Functional Hierarchy
• Score 5+
Outcome Scale: ADL Long Form (HC only)
• Score 12+
8 Outcome Scale: ADL Hierarchy (LTCF only)
• Score 3+
25
 Dementia and Psychogeriatric Levels of Care
Dementia Level Care
Observations
To consider a client for entry to secure care, all of the following should be met:
Dementia and Psychogeriatric Levels of Care
Dementia Level Care
Observations
To consider a client for entry to secure care, all of the following should be met:
• Client has had an interRAI assessment completed within the last six months
which accurately reflects current need, and resulted in the need for residential care
• All options to safely support the client in the home environment with the use of
community-based or natural support have been exhausted
• Client has been assessed as requiring secure care by an appropriately qualified
Physician
• Enduring Power of Attorney enacted OR Welfare Guardianship activated
interRAI Indicators
Answer
•
HC: Minimum 5/7 indicators •
Exception: If no carer present, exclude indicator 3.
4/6 remaining indicators required
•
LTCF: Minimum 2/4 indicators
1 CAP: Behaviour
• Triggered
2 CAP: Institutional Risk (HC only)
• Triggered
Question P2A: Informal helper(s) is unable to
continue in caring activities (HC only)
3
OR
• Yes
Question P2B: Primary informal helper expresses
feelings of distress, anger, or depression (HC only)
4 Outcome Scale: Cognitive Performance score (CPS)
• Score 3+
5 Outcome Scale: Fracture Risk
• Score 4+
6 Outcome Scale: Communication
• Score 4+
7 Outcome Scale: MAPLe (HC only)
• Score 4+
Psychogeriatric Level Care
•
As above for Rest Home Level Care, excluding indicator 3 if applicable •
PLUS at least one of the following:
8 Outcome Scale: Aggressive Behaviour
• Score 6+
Outcome Scale: ADL Long Form (HC only)
• Score 12+
9 Outcome Scale: ADL Hierarchy (LTCF only)
• 3+
26

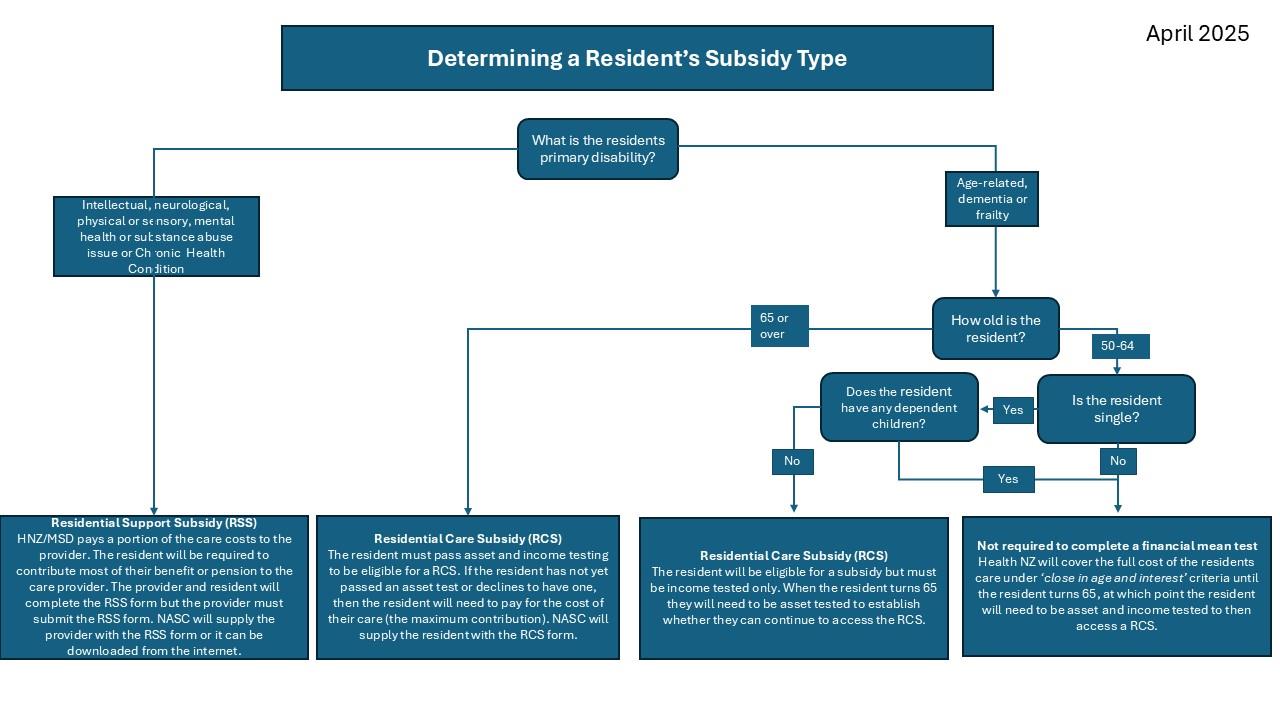
Appendix 8: Determining a Resident Subsidy Type
27

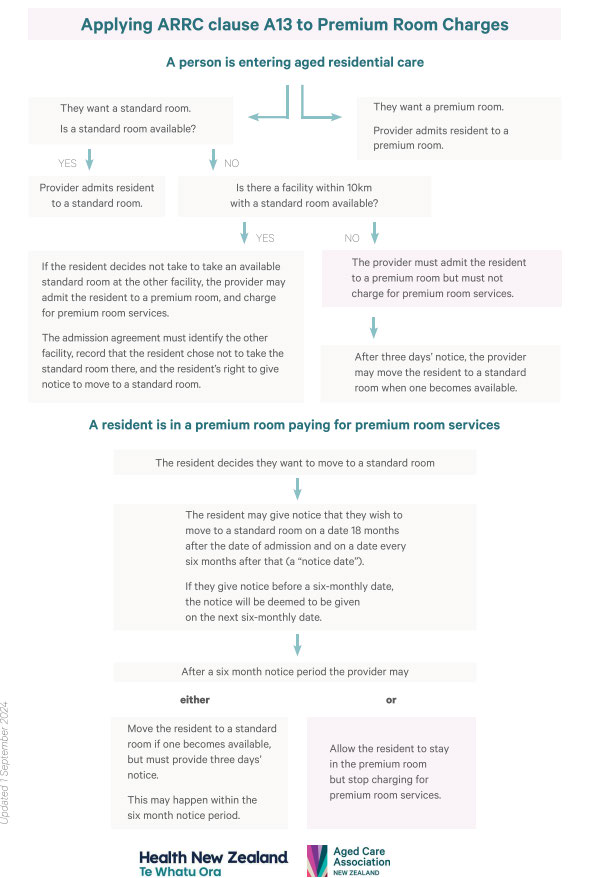
Appendix 9: Applying ARRC clause A13 to Premium Room Charges
28

Appendix 10: Approving continuation of payments during resident temporary absence in ARC
National guidelines for approving continuation of payments during resident temporary absence in ARC
Background
The National Age-Related Residential Care (ARRC) Agreement requires approval for payments to
continue when a resident is temporarily absent from a facility. Clause A7 of the ARRC Agreement
states:
A7.
PAYMENT DURING TEMPORARY ABSENCE
A7.1 Where a Subsidised Resident leaves your Facility temporarily, as long as the Person's bed
is held for that Subsidised Resident during his or her absence, and is not used by another
Subsidised Resident, we will continue to make payments for that Subsidised Resident on
the following basis:
a. Hospitalisation: Where a Subsidised Resident is admitted to hospital for treatment or to
undergo an assessment, we will continue to make payments in full for up to 21 days (or for
any longer period that the NASC Service may recommend) in any one of our financial
years.
b. Temporary Absences: Where a Subsidised Resident is away from your Facility with
family/whānau or friends, we will continue to make payments in full for up to 14 days at
any one time, and up to 28 days in total (or a greater number of days in total, if you obtain
our agreement in advance) in any one of our financial years.
Approval guidance
ARC facilities are responsible for keeping track of days any resident is temporarily absent from the
facility over the course of a financial year. It is their responsibility to make application to NASC /
Funder for continuation of payment when the resident will, or has, exceeded these days. For
clarity, a day of absence is defined as a day when the resident is not in the facility for the entire
day.
The overarching principle that should direct any decision making is that the ARC facility is the
person’s home.
1. Approving temporary absence for hospitalisation
When an ARC resident is in hospital, it is expected that their room will be held for them, with their
belongings intact. Therefore, it is appropriate that Health NZ will continue to provide funding to a
facility if the client remains in hospital for over 21 days in any one financial year. Additionally, their
room should not be used to temporarily accommodate other residents.
Continuation of funding should only be declined if:
• It is expected that the resident’s change in condition means their care needs will not be able
to be met at the current facility
• It is expected that the resident will die in the hospital
This criteria should be utilised to ensure that Health NZ and the resident are not continuing to pay
for care unnecessarily when they will not return to the facility and ensure that other people have
access to this bed.
2. Approving ‘other’ temporary absence
There are times when a resident wishes to be absent from a facility to spend time with family/
whānau or friends for a period of time greater than the maximum time permitted under the ARRC
agreement clause A7.1(b). As this is the person’s home it is expected that these periods should be
reviewed on an individual basis and the following factors taken into consideration
-
what is the purpose of the time away from the facility – short trips or one long trip
29

-
does this support the overall well-being of the resident
-
is the request in advance of the period of leave sought
The application for continuation of payment under these circumstances provides an opportunity
for NASC to consider if residential care is the most appropriate option for this resident and
whether other community-based options would better meet their needs. If it determined that the
person could be managed appropriately within the community setting, then requests could be
declined.
Operational process
The current process for making a request is different across the country however all requests are
sent to Health NZ via the NASC or the Funding team. The variation can present difficulties for the
Health NZ teams as well as the ARC providers, especially those who have facilities across
multiple districts. In future all requests should be submitted on a form available on the Health NZ
website and there will be a common pathway for submission.
For private payers, not in receipt of a subsidy, this is subject to their admission agreement
between them and the ARC provider.
30

Appendix 11: Key Terms and Processes
Service Term or
Definition or process description
Process
Person
The use of the term “People” or “Person” refers to people living in the
community who are referred to the NASC to receive the services
described in this specification.
Referral
A formal request to the NASC to determine if a person is eligible for the
services described in this specification.
Initial Client Visit
The first face to face visit where assessment / plan of service discussed,
and individual support plan agreed
Service Allocation
Also abbreviated to ‘SAT’. It is a screening tool that comprises six
Tool
questions to determine client complexity and service level access.
Casemix
This is a system that classifies people into groups with similar levels of
assessed need and resource utilisation.
Casemix allocation
The process by which clinical assessors determine which Casemix
group a client belongs to, based on the outcomes of either the Contact
or Home Care Assessment.
interRAI
A comprehensive clinical assessment, which focuses on a person’s level
Assessment
of functional ability. It is specifically designed to show the assessor
opportunities for improvement and/or any risks to the person’s health,
which then forms the basis of a care plan. The interRAI assessment tools
used within this service are the Contact and Home Care assessments.
Re-assessment
Provider and NASC assessors are required to complete repeat
assessments of clients as clinically indicated or as set out in the Review
and Reassessment regimes.
Service
The first day that the support service is delivered into the home of a
Implementation
client by a support worker implementing the requirements of the
individual support plan.
Natural Supports
the resources inherent in the community, including personal
associations and relationships, that enhance the wellbeing and security
of clients. Natural supports usually involve family members, friends,
neighbours and acquaintances. Some clients have few natural supports
and may need support to develop these connections.
Individual Support
The Providers develop client centred goal-based individual support
Plan
plans in partnership with clients. The purpose of the Individual support
plan is to provide clear guidance to support staff about:
• activities they need to complete to support clients to achieve set
goals
• what needs to be escalated to the attention of the RHP
• the estimated time it should take for them to complete the activities
of the individual support plan and expected time between reviews.
• hazards are identified and describe how they are mitigated
• the contingency plan in the case of emergencies
The support plan is owned by the client, can be made available to be
shared with the wider support team.
Restorative support May include:
Activities to support independence with:
• bathing or showering
31
 Service Term or
Definition or process description
Process
Service Term or
Definition or process description
Process
• personal grooming, for example shaving, brushing teeth
• toilet access and use
• transfers, in accordance with manual handling guidelines
• dressing and undressing
• application of creams and lotions, following guidelines where
applicable.
Any activities that support independent maintenance of a safe and
sanitary personal living environment. This may include restorative
activities supported to vacuum, clean kitchen and bathroom areas
following supported hygiene or food preparation, and support to
maintain clean bedding and laundry during activities of daily living such
as getting up and getting dressed.
This does not include, cleaning of windows, high cleaning, outdoor
maintenance, cleaning of any additional rooms, dusting, cleaning of
ornaments and additional cleaning considered beyond that required to
maintain ‘safe and sanitary’ living conditions.
Stop and Watch
An early warning communication tool that supports workers and/or
whānau. It can be used to alert the service co-ordinator if they notice
something different in a resident’s daily care routine.
Flexible service
Services are planned in such a way that enables flexible service delivery.
delivery
Support can be increased if the client is temporarily unwell or reduced if
they regain functional ability. A client does not need to be reassessed or
have a change in Casemix allocation because of the short-term nature of
the flex.
Client service
Reviews are scheduled when the individual support plan is developed.
review
The purpose of the review is to evaluate and measure client progress
against SMART goals, observe if there are any clinical indications for a
further assessment or greater Interdisciplinary team input. The outcome
of a review may require the individual support plan to be modified or
redeveloped.
Following a review, the service allocation may:
• remain the same with same service allocation
• remain the same but with a change to the mix of services
• be decreased with a decrease in service time and support activities
provided
• be increased with an increase in resource allocation
• be discontinued with Provider initiating a formal discharge process
• be insufficient, indicating there is a need for a re-assessment. The
Provider will flex the service as appropriate to ensure the client is
safe and supported until the reassessment occurs.
Needs Assessment These organisations are funded by HNZ Regions. Their roles are to
and Service Co-
determine service eligibility, assess the person’s support needs, make
ordination (NASC)
service allocations and co-ordinate support services to meet those
needs. NASC co-ordinate such services, but do not themselves provide
32
 Service Term or
Definition or process description
Process
Service Term or
Definition or process description
Process
the services. They manage referrals to Providers and other
Interdisciplinary team members including primary care.
Case management
Case management is a client and whānau centred collaborative process
of assessment, planning, coordination, evaluation and advocacy that
sees the client’s wider health and social sector team take an integrated
approach to service delivery. A designated lead RHP who
understands the client’s wider health and social needs is nominated by
the clients integrated healthcare team and acts as the key point of
contact to facilitate the client/whānau to navigate the wider healthcare
team. The lead RHP may be, but is not limited to, a Provider RHP, NASC
assessor, primary care nurse or dementia navigator.
Service
Service coordination is about planning a person’s care based on their
coordination
goals and support needs and sharing information with everyone who
(NASC)
helps to care for the person. It is performed collaboratively with a person
and their whānau and likely includes all of the following:
• educating and supporting the person and their carer
• helping the person access community care and support services
• talking with health and community care providers
• planning what services might be needed in the future
Service co-
Service co-ordination activities carried out by Provider staff including
ordinator (Provider)
• matching support staff with required competency and level of
training to meet the complexity needs of the client;
• Acting as a conduit between clients, support staff, registered health
professionals and external agencies;
• Completing activities of client case management;
• Assisting in the recruitment, employment, management and training
of support workers,
• rostering and scheduling staff;
• developing and maintaining relationships with referring agencies,
and
• monitoring and reviewing the quality of service provision including
completion of some client reviews.
These activities are incorporated into staff roles so that quality services
can be delivered efficiently to optimise resource utilisation and to
ensure enough service flexibility to address regional needs (for example.
rurality)
Registered Health
The Health Practitioners Competence Assurance Act 2003 (the Act)
Professional
provides a framework for the regulation of health practitioners to protect
the public where there is a risk of harm from professional practice.
Registered health professionals (RHP) may include; physiotherapists,
occupational therapists, registered nurses and social workers.
In this service the RHP is responsible for delivering services on behalf of
a service Provider. This includes the provision of direct care or support
services to the client and covers all staff who are employed or
contracted. Activities completed by the provider RHP may include:
• interRAI assessments,
• case management including facilitating an integrated approach to
client support from primary and secondary care.
33
 NEEDS ASSESSMENT AND SERVICE
Protocol
COORDINATION (NASC)
CPM.M5.16
CLINICAL PRACTICE
MANUAL
PURPOSE
NEEDS ASSESSMENT AND SERVICE
Protocol
COORDINATION (NASC)
CPM.M5.16
CLINICAL PRACTICE
MANUAL
PURPOSE
It is the Te Whatu Ora – Health New Zealand Hauora a Toi Bay of Plenty Mental Health &
Addiction Service’s (MH&AS) policy intent that al tāngata whaiora / service users requiring
psychiatric disability support have access to services promoting recovery and resilience that
are co-ordinated to meet their individual needs and goals.
OBJECTIVE
• To ensure tāngata whaiora / service users’ needs have been identified and prioritised using
a comprehensive assessment approach.
• To provide regionally-funded community and residential support services in a responsive
and timely manner.
• To ensure tāngata whaiora / service users, families / whānau and the clinical teams all
have accurate and current information about mental health disability support services.
• To meet requirements of the Ngā paerewa Health & Disability Service and contractual
obligations with the funding authority for the provision of needs assessment and service
co-ordination.
EXCLUSIONS
There are no exclusions
STANDARDS TO BE MET
1. Needs Assessment
1.1
When a tāngata whaiora / service user meets the criteria for Psychiatric Disability
Support Services, then it is the treating clinical team’s responsibility (with the tāngata
whaiora / service user’s consent) to initiate the referral to NASC
1.2
The criteria for referral is
a)
diagnosis of mental health and / or addictions disorder,
b)
established treatment and clinical team assigned, and
c)
evidence of requirement for community support for at least 3 months duration.
If these criteria are not met, consideration will be made on a case-by-case basis
(such as the severity of the functional or occupational impairments, and / or the need
for discharge planning from acute services).
1.3
At the time of referral, the tāngata whaiora / service user will be able to elect to be
assessed by a NASC worker within Community Mental Health Services or Kaupapa
/ Maori Health Providers.
1.4
The appropriate NASC Referral Form will be completed by the tāngata whaiora /
service user’s clinician (e.g., Case Manager) and forwarded to the NASC Team
Leader or Administrator.
1.5
NASC will screen the referral and will liaise with the referrer if not appropriate or if
further information is required. If declined, NASC will notify the referrer, and where
possible will assist the referrer / tāngata whaiora / service user to identify
alternatives.
Issue Date:
Sep 2022
Page 1 of 5
NOTE: The electronic version of
Review Date:
Sep 2023
Version No: 6
this document is the most current.
Any printed copy cannot be
Protocol Steward: Team Leader,
Authorised by: Chief Medical Officer
assumed to be the current version.
NASC, MH&AS
 NEEDS ASSESSMENT AND SERVICE
Protocol
COORDINATION (NASC)
CPM.M5.16
CLINICAL PRACTICE
MANUAL
NEEDS ASSESSMENT AND SERVICE
Protocol
COORDINATION (NASC)
CPM.M5.16
CLINICAL PRACTICE
MANUAL
1.6
Allocation to a Needs Assessor will be made within 3 days of receiving the referral,
and a comprehensive needs assessment in a timely manner. Referrals from acute
inpatient services will be prioritised and undertaken as soon as practicable.
1.7
NASC will inform the tāngata whaiora / service user of the needs assessment and
service co-ordination process and include full information about their rights and
responsibilities.
1.8
Needs Assessment includes:
a)
Utilising an appropriate Support Needs Assessment form to identify and
prioritise a tāngata whaiora / service user’s needs and goals, including their
health, daily living, and financial, housing, employment, recreational, social
and cultural needs (see Appendix).
b)
Additional assessment tools that are deemed necessary to obtain a
comprehensive and holistic summary of a tāngata whaiora / service user’s
needs.
c)
A review of the tāngata whaiora / service user’s clinical file, taking into
consideration treatment approaches used, risk and relapse prevention
strategies, and community management plans.
d)
Obtaining collateral information from clinical service provider, community
agencies, and family / whānau members.
e)
Other forms of assessment can be used where appropriate (including OT /
Functional Assessments, Psychology testing, Behavioural Support reports),
and referrals for Specialist Assessments will be considered when the tāngata
whaiora / service user has high and complex needs.
1.9 Relevant whānau /family, provider agency staff and significant others will be
included in the process as appropriate.
1.10 Copies of completed documentation are provided to the tāngata whaiora / service
user, relevant service provision agencies and filed on the tāngata whaiora / service
user’s clinical notes.
2. Service Co-ordination
2.1 NASC is responsible for ensuring the process of service co-ordination is conducted
and documented.
2.2 Service co-ordination will be undertaken in collaboration with the tāngata whaiora /
service user and where appropriate their family / whānau members, and information
and access to independent advocacy services will be provided if required.
2.3 Service Co-ordination activities will include
a)
Identifying the most suitable support service(s) required to meet the tāngata
whaiora / service user’s prioritised needs and goals. Where possible, the
person will be offered a choice of support options and / or services and may
need to be assisted to select their preferences.
b)
Processing all referral documentation, including the Community Support
Service Referral Form (see Appendix), and the completion of funding
documentation and forms as required by the service provider and / or Ministry
of Health.
c)
Arranging referrals for further specialist assessments and treatments as
recommended within Needs Assessment report (e.g., Support Net, Drug and
Alcohol counselling).
d)
Liaising with relevant members of the clinical team, nominated service
provider(s), and the tāngata whaiora / service user and their family / whānau
in the development of a Shared Support Plan (SSP).
Issue Date:
Sep 2022
Page 2 of 5
NOTE: The electronic version of
Review Date:
Sep 2023
Version No: 6
this document is the most current.
Any printed copy cannot be
Protocol Steward: Team Leader,
Authorised by: Chief Medical Officer
assumed to be the current version.
NASC, MH&AS
 NEEDS ASSESSMENT AND SERVICE
Protocol
COORDINATION (NASC)
CPM.M5.16
CLINICAL PRACTICE
MANUAL
NEEDS ASSESSMENT AND SERVICE
Protocol
COORDINATION (NASC)
CPM.M5.16
CLINICAL PRACTICE
MANUAL
e)
Where no service can be provided, or the co-ordinated supports do not
adequately meet the needs of the tāngata whaiora / service user, NASC will
record this and notify the appropriate person(s) (MH&AS Business Leader,
Clinical Director, and / or Planning & Funding). The use of Packages of Care
(POC) or Flex-Funds arrangements will be considered in accordance with the
guidelines i
n protocol CPM.M5.2 Packages of Care.
3. Liaison and Review
3.1 A review of the tāngata whaiora / service user’s Shared Support Plan will occur at 3
monthly intervals as per
protocol CPM.M5.30 Treatment Plan. NASC will attend the
SSP meetings and contribute to the development of these as necessary in order to
meet the needs and goals identified in the current Needs Assessment document.
3.2 NASC will liaise regularly with the clinical team / Case Manager, Service Provider,
the tāngata whaiora / service user and their family / whānau (where appropriate) to
ensure the support provided is appropriate to meet the individual’s needs.
3.3 NASC will complete a review of the tāngata whaiora / service user’s needs and
support provision within 3 months after the initial placement, and thereafter as
required.
3.4 A full re-evaluation of the person’s needs to be completed using the comprehensive
assessment at least yearly, or for those in residential support services and / or with
high and complex needs 6-monthly.
3.5 If reviews or reassessment are required outside of these schedules, it is
responsibility of the clinical team and / or Service Provider to notify NASC.
4. Inter–NASC Requests / Co-ordination
4.1 When required to send or receive referrals between Te Whatu Ora districts / regions,
NASC will operate with other Te Whatu Ora NASC teams in accordance with the
Best Practice Guidelines recommended by NASCA (see Appendix).
4.2 When referring, NASC will provide all necessary information required, including a
current comprehensive Needs Assessment. Receiving NASCs will work with the
tāngata whaiora / service user and their family / whānau to identify and arrange
suitable support options and will then complete the service co-ordination process.
4.3 Service Co-ordination will only be finalised and processed once the corresponding
transfer of care / referral is made between the appropriate clinical teams. Once the
tāngata whaiora / service user is receiving the support services, ongoing liaison and
review will become the responsibility of the receiving NASC.
5. Service Planning / Development
5.1 NASC will maintain an up-to-date directory of all mental health / community support
services, and advise tāngata whaiora / service user’s, family / whānau, and clinical
teams of service options and availability.
5.2 Access to support services will be provided in a responsive and timely manner, and
when barriers or delays are encountered, NASC will work to address these with
Service Providers, MH&AS Management and / or Planning & Funding.
5.3 NASC will monitor the allocation and use of regionally funded supported services to
ensure that resources are used appropriately, efficiently, and timely.
5.4 NASC will inform MH&AS Management and Planning & Funding if there are unmet
needs or service delivery gaps. Research projects and / or service improvement
initiatives will be undertaken in collaboration with all relevant stakeholders.
Issue Date:
Sep 2022
Page 3 of 5
NOTE: The electronic version of
Review Date:
Sep 2023
Version No: 6
this document is the most current.
Any printed copy cannot be
Protocol Steward: Team Leader,
Authorised by: Chief Medical Officer
assumed to be the current version.
NASC, MH&AS
 NEEDS ASSESSMENT AND SERVICE
Protocol
COORDINATION (NASC)
CPM.M5.16
CLINICAL PRACTICE
MANUAL
NEEDS ASSESSMENT AND SERVICE
Protocol
COORDINATION (NASC)
CPM.M5.16
CLINICAL PRACTICE
MANUAL
5.5 MH&AS will have service level agreements and Memorandums of Understanding
with contracted providers, and NASC will work with Planning & Funding to monitor
the provision of these.
REFERENCES
•
Ngā Paerewa Health and Disability Services Standard. NZS 8134:2021
• Standards for Needs Assessment for People with Disabilities. Ministry of Health (June
1994).
• Needs Assessment & Service Coordination Service Specification, Tier Level 3. Ministry
of Health (April 2009).
• Notification of Needs Assessment and Service Coordination Form (Ministry of Health)
ASSOCIATED DOCUMENTS
•
NASC Referral Form
•
Support Needs Assessment Form
•
Community Support Service Referral Form
•
Shared Support Plan
•
Te Whatu Ora Hauora a Toi Bay of Plenty Clinical Practice Manual protocol CPM.M5.30
Treatment Plan
•
Te Whatu Ora Hauora a Toi Bay of Plenty Clinical Practice Manual protocol CPM.M5.17
Discharge from Mental Health & Addictions Services
•
Te Whatu Ora Hauora a Toi Bay of Plenty Clinical Practice Manual protocol CPM.M5.2
Packages of Care.
Issue Date:
Sep 2022
Page 4 of 5
NOTE: The electronic version of
Review Date:
Sep 2023
Version No: 6
this document is the most current.
Any printed copy cannot be
Protocol Steward: Team Leader,
Authorised by: Chief Medical Officer
assumed to be the current version.
NASC, MH&AS
 NEEDS ASSESSMENT AND SERVICE
Protocol
COORDINATION (NASC)
CPM.M5.16
CLINICAL PRACTICE
MANUAL
Appendix 1: Procedure
PSYCHIATRIC DISABILITY SUPPORT
TASK
ACTION
WHO
NEEDS ASSESSMENT AND SERVICE
Protocol
COORDINATION (NASC)
CPM.M5.16
CLINICAL PRACTICE
MANUAL
Appendix 1: Procedure
PSYCHIATRIC DISABILITY SUPPORT
TASK
ACTION
WHO
Requirement for Community Support Services identified
in collaboration with tāngata whaiora / service user, and
family / whānau where appropriate. Referral discussed
Case Manager / MDT
in clinical meeting, and NASC Referral Form completed
Referral
with tāngata whaiora / service user consent.
Referral screened and Needs Assessor allocated within
NASC
3 days. Declined referrals discussed with referrer.
Comprehensive needs assessment conducted using
the appropriate Support Needs Assessment tool.
Needs Assessment
NASC
Other
supporting
information
gathered
where
appropriate,
including
clinical
file,
specialist
assessments, and family / whānau perspective.
Recommendations and service provider options
discussed with tāngata whaiora / service user, clinical
team, and family / whānau (where appropriate). Where
possible, tāngata whaiora / service user is able to select
preferred support options.
NASC
Service
Co-ordination
Referral documentation collated and forwarded to the
nominated Service Provider(s). Where required
relevant Ministry of Health documentation is completed
and lodged.
Acceptance / decline of referral requested within 5
Support Provider
working days.
The initial Shared Support Planning meeting arranged
with key stakeholders to clarify prioritised needs, and to
NASC
confirm roles and responsibilities. Initial plan developed
from Needs Assessment.
Shared
Support
Within 1 month of entry to service, supports are
Planning
reviewed, and recommended changes agreed. Shared
Support
Provider
/
Support Plan (SSP) document updated and signed by
Case Manager
key stakeholders.
SSP meeting is arranged 3 monthly, with stakeholders
Support Provider
notified and invited to appointment.
Regular contact with Support Provider, the tāngata
whaiora / service user and their family / whānau to
NASC / Case Manager
monitor that planned support is meeting the needs as
identified in the Needs Assessment.
Liaison & Review
Support Needs are reviewed 6-monthly for those in
residential support services and / or with high and
NASC
complex needs, otherwise re-assessments done at
least yearly.
Issue Date:
Sep 2022
Page 5 of 5
NOTE: The electronic version of
Review Date:
Sep 2023
Version No: 6
this document is the most current.
Any printed copy cannot be
Protocol Steward: Team Leader,
Authorised by: Chief Medical Officer
assumed to be the current version.
NASC, MH&AS
link to page 70
 Service Term or
Definition or process description
Process
Service Term or
Definition or process description
Process
• writing and review of support services and individual support plans,
• direction, delegation and supervision of non-regulated staff.
Support Worker
Provider staff who help patients at home with tasks such as showering
and dressing, housework such as cleaning, ironing, meal preparation
and assistance, medication oversight. They may support clients with
rehabilitation, supporting strength and balance and walking exercises,
and attendance at social groups.
Interdisciplinary
A team of health professionals from different disciplines and workplaces
Team (IDT)
work together with the client, to undertake assessments, diagnosis, and
plan interventions through goal setting and the creation of an individual
support plan.
The client and their whānau and carers are involved in discussions as
appropriate.
Interdisciplinary
The interdisciplinary review is provided for clients needing High-Cost
review
Intensive Support packages: clients in any Casemix group that require
intensive support packages over 21 hours will have an interdisciplinary
review arranged by the NASC. Review will occur monthly for unstable
and three monthly for stable.
Medication Support
Provider support staff assist and/or prompt a client to self-administer
medicines as prescribed and as documented in the individual support
plan.
Medication
The Provider has determined that the client is unable to safely
Administration
administer their own medication and does not have reliable whānau
support to assist them. The support staff physically assists the client to
safely administer medication as per the individual support plan
developed by the Registered Nurs
e3.
Risk assessment
Process undertaken to determine the level of risk associated with
support provision.
A Risk Assessment Framework supports HNZ NASC and contracted
Providers with this process. The risk framework can be found in the
Tier
One Community Health, Transitional and Support Services (HNZ funded)
service specification.
Integrated
HCSS services are required to operate an integrated management
Management
framework composing strategic and operational integrated management
Framework
groups consisting of representatives from contracted providers, allied
health, primary health care NASC and HNZ DISTRICT HCSS contract
managers. More detail is provided in the HCSS Operations Manual.
Te Ara Whakapiri
Te Ara Whakapiri: Principles and guidance for the last days of life
outlines the essential components and considerations required to
promote quality care at the end of life for all adults in New Zealand.
3 Draft Medication Guidelines for the HCSS Sector 2017
34
Document Outline