

133 Molesworth Street
PO Box 5013
Wellington 6140
New Zealand
T+64 4 496 2000
21 February 2025
Erika Whittome
By email: [FYI request #29836 email]
Ref:
H2025059434
Tēnā koe Erika
Response to your request for official information Thank you for your request under the Official Information Act 1982 (the Act) to the Ministry of
Health – Manatū Hauora (the Ministry) on 22 January 2025 for information regarding COVID-19
science updates. You requested:
“I am requesting information from August 2021 until November 2021 which used to be
published on your website as "covid science updates" and "Covid Insights" reports
For example
https://www.health.govt.nz/system/files/documents/pages/csu_03_august_2021_voc_key
_info_summary_guillan_barre_syndrome_after_covid-19_vaccination.pdf
and COVID-19 Science Updates Science and Insights 19 Oct 2021 "COVID-19 Delta
variant secondary" attack rates, August-October 2021.
Would you please share all of these "CSU"s and "Insight reports" from Aug 2021 until the
end of November 2021”
The following documents have been identified in scope of your request and are released to you
in full:
• 3 August 2021 COVID-19 Science Updates
• 10 August 2021 COVID-19 Science Updates
• 13 September 2021 COVID-19 Science Updates
• 23 September 2021 COVID-19 Science Updates
We apologise for any confusion or loss of information. Our investigation into the matter revealed
that the whole Ministry website was updated last year and the page links for these reports broke
as a result. We are working to reinstate the page. Please note that the links may be different
when the page is reinstated.
I trust this information fulfils your request. If you wish to discuss any aspect of your request with
us, including this decision, please feel free to contact the OIA Services Team on:
[email address].

Under section 28(3) of the Act, you have the right to ask the Ombudsman to review any
decisions made under this request. The Ombudsman may be contacted by email at:
[email address] or by calling 0800 802 602.
Please note that this response, with your personal details removed, may be published on the
Manatū Hauora website at
: www.health.govt.nz/about-ministry/information-releases/responses-
official-information-act-requests. Nāku noa, nā
Dr Kristie Carter
Group Manager, Intelligence Surveillance and Knowledge Public Health Agency | Te Pou Hauora Tūmatanui
Page 2 of 2

 Document 1
COVID-19 Science Updates
CSU 46
13 September 2021
Document 1
COVID-19 Science Updates
CSU 46
13 September 2021
1. No evidence that COVID-19 vaccination is associated with increased risk of miscarriage
Evidence that the Pfizer COVID-19 vaccine is safe during pregnancy has been growing. At the same time,
it has become clearer that COVID-19 infection during pregnancy is associated with an increased risk of
developing severe disease
(link). This report reviews the data from two studies
(link, link), that evaluate
the risk of miscarriage in people who received a COVID-19 vaccine during pregnancy. Both studies show
that the rate of miscarriage is similar for vaccinated and unvaccinated pregnant people, and that there is
1982
no evidence that the COVID-19 vaccine is associated with an increased risk of miscarriage during
pregnancy.
ACT
• Shimabukuro
et al, reported on the safety of receiving the mRNA COVID-19 vaccine for pregnant
people
(link). The study included 3,958 pregnant people in the US enrolled in the ‘v-safe’
pregnancy registry. Registry participants had received an mRNA vaccine (Pfizer or Moderna) at
some point during their pregnancy. Participants were asked questions relating to pregnancy
outcomes, such as pregnancy loss or live birth, and neonatal outcomes such as rate of preterm
birth and size for gestational age. Participants were followed for 10-12 weeks post-vaccination.
•
INFORMATION
The rate for miscarriage, as with most pregnancy outcomes, was evaluated against all completed
pregnancies. However, because the Shimabukuro
et al study reported only 10-12 weeks of
follow-up after vaccination, not all the pregnancies evaluated in the study were complete.
Therefore, in order to estimate the rate of miscarriage, authors evaluated the outcomes from
the completed pregnancies only.
OFFICIAL
• There were 827 completed pregnancies. Of those, there were 712 births, 104 miscarriages, 1
stillbirth, and 10 other outcomes, e.g., ectopic pregnancy. Therefore, the rate of miscarriage was
THE
104/827 or 12.6%, similar to the background rates for unvaccinated individuals; the background
rate for miscarriage for pregnancies in the general population is about 12.5 to 18.7%
(link).
• Most of the individuals were vaccinated in the 3rd trimester (86%), however, and it is reasonable
UNDER
to want to estimate the rate of miscarriage for people vaccinated in the first and second
trimester. There were 96 (8.5%) miscarriages reported in the 1st trimester, and the remaining 8
(0.5%) occurred in the 2nd trimester.
• An incorrect method for estimating the rate of miscarriage, but one that has circulated on social
media, is to count the number of miscarriages among the 127 individuals who were
vaccinated in
RELEASED
their 1st or 2nd trimester and who completed their pregnancies within 3 months of that date (the
maximum follow-up time of the study). However, most pregnancies completed within 3 months
of the 1st or 2nd trimesters are not full-term births, by definition. The analysis
should include all
women followed to full-term or the end of their pregnancies, and then determine of those who
had miscarriages, rather than selecting only those whose pregnancy ended within the study’s
follow-up period (3 months), as this generates a selection bias to include more miscarriages in
the analysis.
Context and disclaimer. This update contains topical talking points, science advice and research – it is intended as a high-level overview. The topics herein are
assembled ‘at pace’ often under urgency and may be based on reports that are not peer-reviewed. Both the content and ‘comment’ components of this
briefing represent science commentary at a single point in time – information herein may or may not align with Ministry of Health positions or priorities.

 Document 1
COVID-19 Science Updates
Document 1
COVID-19 Science Updates
• In total, there were 2,846 pregnant people who were vaccinated in their 1st and 2nd trimesters,
and the vast majority of the pregnancies (96%) were still ongoing at the end of the follow-up
period (3 months). The remaining 127 (4%) pregnancies were completed within 3 months
following vaccination in the 1st or 2nd trimester. This means that almost no completed full-term
births are included in the 127 simply because the study does not have sufficient follow-up time.
Hence, it is not surprising that of the 127 pregnancies completed within 10-12 weeks of the first
and second trimesters, 104 (82%) were recorded as a miscarriage.
• A second study was performed that was able to follow almost all pregnant people from the 1st
and 2nd trimester until completion of the pregnancy, either to full term or other pregnancy
1982
outcome. Therefore, this study did not have the bias associated with limited follow-up time. The
researchers followed 2,456 pregnant people from vaccination with a COVID-19 vaccine in the
ACT
first and second trimesters until completion of their pregnancies. All participants in the study
received a mRNA COVID-19 vaccine before 20 weeks’ gestation
(link). The risk of miscarriage
from 6–19 weeks’ gestation until the completion of the pregnancy was 14.1% (95% CI:
12.1,16.1%), consistent with background rates. This shows that when pregnant people are
vaccinated in the first or second trimesters, and we can follow the individuals until we know the
outcomes of all the pregnancies, that the rate of miscarriage is no higher or lower than in
unvaccinated pregnant people.
INFORMATION
Comment: There is no evidence that the COVID-19 vaccine is associated with an increased risk of
miscarriage during pregnancy. In general, the benefits of COVID-19 vaccination outweigh the risks from
COVID-19.
OFFICIAL
THE
UNDER
RELEASED
2 of
2
Context and disclaimer. This update contains topical talking points, science advice and research – it is intended as a high-level overview. The topics herein are
assembled ‘at pace’ often under urgency and may be based on reports that are not peer-reviewed. Both the content and ‘comment’ components of this
briefing represent science commentary at a single point in time – information herein may or may not align with Ministry of Health positions or priorities.
link to page 6

 Document 2
COVID-19 Science Updates
CSU 47
23 September 2021
Document 2
COVID-19 Science Updates
CSU 47
23 September 2021
1. Risk of hospitalisation and severe outcomes from COVID-19 in children: Evidence from the Delta wave
in the US
On 03 September 2021, the US CDC published two reports on hospitalisation rates in children
(link, link).
A hallmark feature of the COVID-19 pandemic has been the dramatically higher incidence of severe
disease and mortality among older adults, however, COVID-19 still causes severe disease in children,
albeit with a much lower incidence. In addition, there is growing evidence that the Delta variant results in
1982
a higher rate of hospitalisation than for previous variants
(link, link). This CSU characterises the disease
burden on children aged 0-17 years old in the US. Note that in the US, children aged 12 and over have
been eligible to be vaccinated with the Pfizer COVID-19 vaccine since May 2021.
ACT
The first analysis
(link) was based on the Coronavirus Disease 2019 – Associated Hospitalization
Surveillance Network (COVID-NET), a consortium of over 250 hospitals in the US that conducts
population-based surveillance for laboratory-confirmed hospitalisations of COVID-19. Medical charts for
all COVID-19 paediatric admissions were abstracted by trained reviewers.
• Authors found that from 01 March, 2020–14 August, 2021, the overal cumulative incidence of
COVID-19–associated hospitalisations was 49.7 per 100,000 children and adole
INFORMATION scents aged 0-17
years. Unlike adults, the risk was ‘U-shaped’ with respect to age: the risk was highest for 0-4 year
olds (69.2 admissions per 100,000) and 12-17 year-olds (63.7), but lower for 5-11 year olds
(24.0).
• The rise in prevalence of the Delta variant coincided w
OFFICIAL ith an increased number of
hospitalisations. The weekly COVID-19-associated hospitalisation rates rose from 0.3
hospitalisations per 100,000 in 0-17 year-olds in the weeks 12 June-03 July, to 1.4 per 100,000 in
THE
the week ending 14 August.
• Mechanical ventilation and in-hospital mortality (but not ICU admission) tended to increase as
Delta became prevalent: based on 3,116 paediatric admissions for which there were complete
UNDER
clinical data, the risks of mechanical ventilation and in-hospital mortality were 6.1%, and 0.7%,
respectively, from 01 March to 19 June, and increasing to 9.8%, and 1.8%, for the period 20 June
to 31 July. The proportion of ICU admissions remained fairly stable over the same time periods,
comprising 26.5% and 23.2% of hospital admissions, respectively.
• There were 68 adolescents (12-17 year-olds) for whom vaccination status was available. Of
RELEASED
those, only 9 were partially or fully vaccinated. Unvaccinated adolescents were more likely to be
hospitalised, however, meaningful conclusions cannot be drawn from such a small sample.
A second study
(link) compared the incidence of COVID-19 and COVID-19 outcomes in 0-17 year-olds
prior to the introduction of Delta (August 2020 – June 2021), and during the current Delta wave (July-
August 2021).
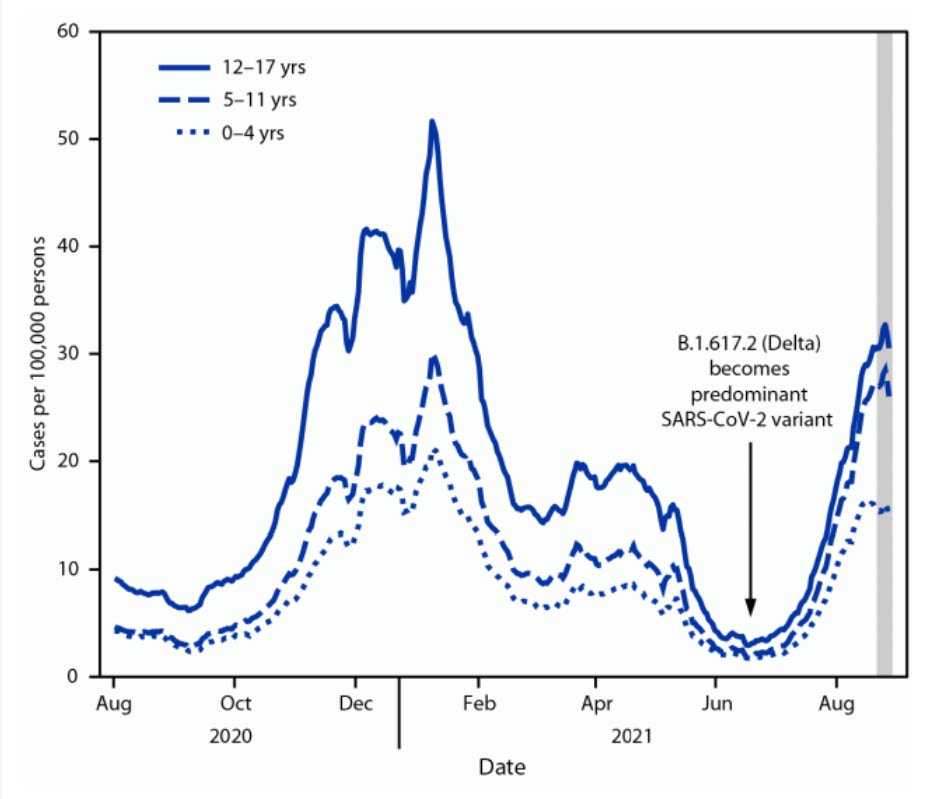
• The incidence increased for al age groups from June to August 2021 (see
Figure 1)
Context and disclaimer. This update contains topical talking points, science advice and research – it is intended as a high-level overview. The topics herein are
assembled ‘at pace’ often under urgency and may be based on reports that are not peer-reviewed. Both the content and ‘comment’ components of this
briefing represent science commentary at a single point in time – information herein may or may not align with Ministry of Health positions or priorities.

 Document 2
COVID-19 Science Updates
Figure 1. Average daily COVID-19 case incidence among persons aged 0–17 years, by age group — United States, 01 August,
2020–27 August, 2021 (Source: CDC’s case-based COVID-19 surveillance system, accessed August 30, 2021.
Document 2
COVID-19 Science Updates
Figure 1. Average daily COVID-19 case incidence among persons aged 0–17 years, by age group — United States, 01 August,
2020–27 August, 2021 (Source: CDC’s case-based COVID-19 surveillance system, accessed August 30, 2021.
https://www.cdc.gov/nndss/action/covid-19-response.html )
1982
ACT
INFORMATION
OFFICIAL
THE
• Regions with low vaccination coverage in the general population tended to have higher rates of
COVID-19-related emergency department (ED) visits and hospital admission in 0-17 year-olds,
compared to regions with high
UNDER coverage. For example, the region with the lowest vaccination
coverage in the general population (with coverage of 49.9%) had 3.4 times the COVID-19 ED
visits and 3.7 times the rate of COVID-19 hospital admissions in 0-17 year-olds as the region with
highest vaccination coverage (coverage of 72.2%). However, there are other confounding factors
in that the states with the lowest vaccination coverage also tend to be located in the southern
US, have lower socio-economic indicators, and poorer health outcomes generally.
RELEASED
• With regard to severity, the proportion of hospitalised cases in 0-17 year olds that were admitted
to the ICU was 10-25% prior to Delta (August 2020 to June 2021) and 18-20% in July and August
2021. Based on 1,790 hospitalisations with data on disease severity, in-hospital mortality was
0.4% (8 deaths). Median length of stay in the ICU for 0-17 year olds was 2-3 days. Of the 63 ICU
admissions in children in July-August 2021, 27% were aged 0-4, 27% were 5-11, and 46% were
12-17 years.
2 of
3
Context and disclaimer. This update contains topical talking points, science advice and research – it is intended as a high-level overview. The topics herein are
assembled ‘at pace’ often under urgency and may be based on reports that are not peer-reviewed. Both the content and ‘comment’ components of this
briefing represent science commentary at a single point in time – information herein may or may not align with Ministry of Health positions or priorities.

 Document 2
COVID-19 Science Updates
Document 2
COVID-19 Science Updates
• Authors commented that the increased risk of hospitalisation during the Delta wave may be due
to more severe disease associated with Delta (as has been suggested by
UK and
Danish data, but
not supported in a study from
Norway) or due to increased overall transmission from Delta, i.e.,
that more transmission results in a greater number of hospital admissions overall.
• Authors also noted that testing rates in children and adolescents are lower than for adults, and
therefore COVID-19 cases tend to be underreported in this age group.
Comment:
Children can experience severe outcomes from COVID-19 including hospitalisation and ICU admission. As
1982
with adults, vaccination of both the eligible adolescents and coverage in the wider population can reduce
those risks. The Delta variant appears to increase both the rate of COVID-19 overall and the risk of
ACT
hospitalisation, although once hospitalised, the proportion requiring ICU admission appeared to remain
static (23-26%) as Delta became prevalent. Notably, the risks from COVID-19 appear to be age-
dependent within children and adolescents: very young children (0-4 years) and older children (12-17
year olds) are at higher risk of hospitalisation compared to 5-11 year olds. Vaccines for children aged 5-
11 may be available in the US in late 2021 or early 2022, with Pfizer announcing on 20 September that
they wil be submitting their phase 2/3 clinical trial data for children aged 5-11 ‘as soon as possible’.
Other factors, such as the capacity of the healthcare systems and better recognition of early signs of
INFORMATION
deterioration may also factor into changing rates of hospitalisation over time, independent of the
variant.
OFFICIAL
THE
UNDER
RELEASED
3 of
3
Context and disclaimer. This update contains topical talking points, science advice and research – it is intended as a high-level overview. The topics herein are
assembled ‘at pace’ often under urgency and may be based on reports that are not peer-reviewed. Both the content and ‘comment’ components of this
briefing represent science commentary at a single point in time – information herein may or may not align with Ministry of Health positions or priorities.

 Document 3
COVID-19 Science Updates
CSU 44
03 August 2021
Document 3
COVID-19 Science Updates
CSU 44
03 August 2021
1. Summary of key information from recent weekly Variants of Concern Updates
The Science and Technical Advisory team within the COVID-19 Directorate of the Ministry produces a weekly
review of evidence on Variants of Concern (VOC) and Variants Under Investigation (VUI) in the weekly
Variants of Concern Update. All updates are publicly available on the COVID-19 Science New
s (link)
webpage on the Ministry of Health website.
1982
Summary of key information from the recent updates:
ACT
• The ongoing active global pandemic gives the virus opportunities to replicate and mutate: while
there is an active pandemic globally, the opportunity for the emergence of new variants exists.
• Variants of concern (VOC) are variants that pose a greater threat to peoples’ health and
management of the pandemic, due to increased transmissibility, causing more severe disease,
and/or ability to evade immune responses or vaccines. Variants with preliminary evidence
suggesting that they may become a VOC, are initially designated a Variant Under Investigation (VUI)
while they are being evaluated.
INFORMATION
• In the previous six weeks there has been a continuous increase in the global spread of the Delta
(B.1.617.2) variant, which has a transmission advantage over other variants. A notable exception is
some South American countries (Peru, Chile) where the VUI Lambda (C.37) has overtaken other
circulating lineages, including Alpha (B.1.1.7) and Gamma (P.1) as the dominant variant.
OFFICIAL
• The Delta variant with the added mutation K417N is known informal y as “Delta plus”. Mutation
K417N is potentially associated with im
THE mune escape. Public Health England (PHE) has reported a
very small number of cases with “Delta plus” as of 23 July. Of note, data on this variant is generally
not collected separately but included along with Delta.
• WHO expect Delta to continue t
UNDER o displace other variants and to become the dominant VOC
worldwide in the coming months.
• In Aotearoa New Zealand, Delta is the predominant VOC identified in cases at our border in recent
weeks.
What do we know about Delta?
RELEASED
Transmissibility
• Epidemiological evidence from secondary attack rates, household transmission studies, and growth
rate modelling all support increased transmissibility.
• The basic reproductive number R0 for Delta is estimated to be at least 5.5-6.5, meaning that on
average each person transmits Delta to another 5-6 people.
Context and disclaimer. This update contains topical talking points, science advice and research – it is intended as a high-level overview. The topics herein are
assembled ‘at pace’ often under urgency and may be based on reports that are not peer-reviewed. Both the content and ‘comment’ components of this
briefing represent science commentary at a single point in time – information herein may or may not align with Ministry of Health positions or priorities.

 Document 3
COVID-19 Science Updates
Document 3
COVID-19 Science Updates
• An outbreak study in Guandong China indicated that Delta is associated with very high viral loads –
1000 times higher on the first PCR positive test compared with the previously dominant variant in
that region -- and a shorter median incubation time of 4 days, compared to approximately 6 days for
the prior variant.
Severity of Disease
• PHE data estimated that Delta is associated with 2.3 times the risk of hospitalisation compared to
Alpha. Fortunately, PHE data indicate that the case fatality rate for Delta remains low (0.2%). Data
reported for risk of death with Alpha varies: PHE’s most recent case fatality rate for Alpha is
approximately 1.8%, noting that this data is based on the wave from December 2020.
1982
Vaccine effectiveness (VE)
ACT
• The Pfizer vaccine is effective against symptomatic Delta infection when two doses are given: PHE
reported 33% protection after one dose, 88% protection after two doses against symptomatic
infection. Similar results have been reported in Denmark and Canada. In contrast, Israel’s Ministry of
Health reported a vaccine effectiveness against symptomatic disease of 64%. This result was
reported in a press release, but the difference may be due to a methodological differences that do
not fully account for the confounding in the observational data.
• The AstraZeneca vaccine is less effective against symptomatic Delta infection wh
INFORMATION en two doses are
given compared to Pfizer but still provides protection: Public Health England reported 30%
protection after one dose, 67% protection after two doses against symptomatic Delta infection.
• A separate analysis from Public Health England (but typical of other estimates) showed two doses of
the Pfizer vaccine offered 96% protection against hospit
OFFICIAL alisation due to the Delta variant. The
AstraZeneca vaccine provided 92% protection against hospitalisation due to the Delta variant in the
same Public Health England analysis.
THE
Horizon scanning
• Recent data from England shows infection rates in healthcare workers are increasing. The cause is
unclear but contributing factors
UNDER may include one or more of: waning immunity for AstraZeneca
and/or Pfizer vaccines; immune escape properties of variants; increasing prevalence of COVID-19 in
England due to Delta. Further updates wil continue to report on this as data emerges.
Comment:
The predominant variant o
RELEASED f SARS-CoV-2 is Delta and looking ahead it is prudent to plan for outbreaks
assuming Delta will be the variant responsible. Delta has increased transmissibility compared to the
previously dominant Alpha variant. It also appears to have higher viral loads, a shorter incubation period,
and shows some degree of immune escape (even though mRNA vaccines appear to largely maintain their
effectiveness against symptomatic disease) compared to previous variants. The shorter incubation period
has implications for the contact tracing timelines and the speed with which public health measures.
2 of
4
Context and disclaimer. This update contains topical talking points, science advice and research – it is intended as a high-level overview. The topics herein are
assembled ‘at pace’ often under urgency and may be based on reports that are not peer-reviewed. Both the content and ‘comment’ components of this
briefing represent science commentary at a single point in time – information herein may or may not align with Ministry of Health positions or priorities.

 Document 3
COVID-19 Science Updates
Document 3
COVID-19 Science Updates
2. Guillan Barré Syndrome after COVID-19 Vaccination
Events of Guillain-Barré syndrome (GBS) have been observed after vaccination with AstraZeneca and
Johnson and Johnson (J&J)/Janssen COVID-19 vaccines internationally. On 13 July 2021, the US Food and
Drug Administration (FDA) added a warning regarding GBS for the J&J vaccine. The European Medicines
Agency (EMA) added a similar warning to the AstraZeneca vaccine and is continuing to assess GBS with
regard to the J&J vaccine, as of 14 July 2021. GBS is a rare autoimmune neurological disorder affecting the
peripheral nervous system.
• GBS can range from a very mild case with brief weakness to complete paralysis and death. Most
1982
people recover from even the most severe cases of GBS but some may be left with residual
weakness. The most common precipitating cause is a respiratory or gastrointestinal viral infection.
ACT
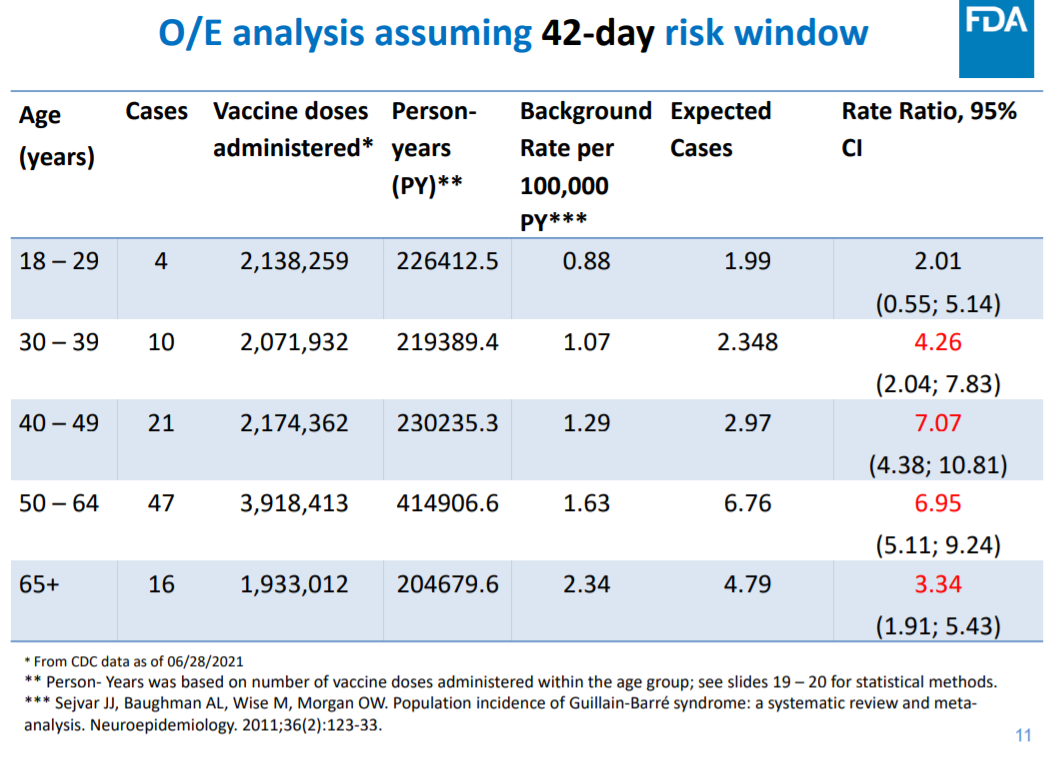
• The background risk of GBS increases with age from a rate of approximately 0.9 per 100,000 person-
years for 18 – 29 year-olds, to 2.3 per 100,000 person-years for those 65 years and over
(link and
Table 1)
• The US CDC’s Advisory Committee on Immunization Practice (ACIP) analysed 100 preliminary
reports, reported to the VAERS (Vaccine Adverse Event Reporting System) up to 30 June 2021.
During the data col ection period, approximately 12.2 million doses of the J&J vaccine were
INFORMATION
administered in the US, for a crude rate of 8.1 per million doses
(link). Of these 100 cases, 95% were
serious, 61% occurred in males, and there was one death attributed to GBS. When stratified by age,
the risk was significantly elevated for those over the age of 30: people aged 30-39 had
approximately 4 times the risk of GBS post-vaccination with the J&J vaccine; people aged 40-49 and
50-64 years had approximately 7 times the risk of GBS (s
OFFICIAL ee Table 1)
Table 1 Background rates, expected numbers of cases and observed numbers of cases of GBS by age (ACIP)
THE
UNDER
RELEASED
3 of
4
Context and disclaimer. This update contains topical talking points, science advice and research – it is intended as a high-level overview. The topics herein are
assembled ‘at pace’ often under urgency and may be based on reports that are not peer-reviewed. Both the content and ‘comment’ components of this
briefing represent science commentary at a single point in time – information herein may or may not align with Ministry of Health positions or priorities.
link to page 11

 Document 3
COVID-19 Science Updates
Document 3
COVID-19 Science Updates
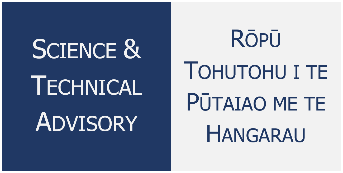
• The rate of GBS in those receiving the Pfizer or Moderna mRNA vaccines was approximately 8 times
lower than the rate for Janssen (se
e Table 2).
Table 2 Crude reporting rates of GBS for mRNA vaccines and Janssen vaccine in the US (ACIP)
1982
ACT
• The EMA’s Pharmacovigilance Risk Assessment Committee (PRAC) reviewed 227 reported cases of
GBS through 27 June 2021, after administration of the AstraZeneca vaccine
(link). Approximately
51.4 million doses of AstraZeneca vaccine had been administered through 20 June, for an
approximate rate of 4.4 per million doses.
INFORMATION
• As of 27 June 2021, 15 cases of GBS after vaccination with the J&J COVID-19 vaccine were reported
from the EU/EEA to the Eudravigilance database
(link). Approximately 7 million doses were
administered in the EU/EEA in a similar period, through 20 June 2021, which corresponds to a crude
rate of 2.1 per million doses.
• The WHO released a statement
(link) regarding the risk o
OFFICIAL f GBS after COVID-19 vaccination on 25th
July 2021, which is consistent with comments made by the US and EU agencies. The WHO
recommend that individuals receiving t
THE he Janssen or AstraZeneca COVID-19 vaccine are made
aware of the possible association with GBS, but that there is no evidence that GBS is associated with
mRNA vaccines.
UNDER
Comment:There is some previous evidence to suggest that influenza vaccination is linked to GBS. For
example, researchers found that over the 2010-2011 influenza season in Italy, there was a 2-fold relative
increase in the risk of GBS for vaccinated compared to unvaccinated individuals
(link). However, an
association has not been reported for other vaccination programs. It is possible that because the enormous
size of the COVID-19 vaccination, which has no precedent, and the increased safety monitoring associated
with COVID-19, researcher
RELEASED s are able to identify associations between vaccination and extremely rare events.
Interestingly, the pathophysiology of GBS is based on the development of auto-antibodies (against the
myelin sheath of the peripheral nervous system), which is similar to the proposed mechanism for the
vaccine induced thrombocytopaenic thrombosis (VITT), observed after vaccination using adenoviral vector
vaccines; VITT is associated with platelet-activating antibodies against platelet factor 4 (PF4). However, it is
important to keep in mind that the risk of these potential complications from the vaccine is tiny compared
to the benefits of vaccination in preventing disease and death from COVID-19.
4 of
4
Context and disclaimer. This update contains topical talking points, science advice and research – it is intended as a high-level overview. The topics herein are
assembled ‘at pace’ often under urgency and may be based on reports that are not peer-reviewed. Both the content and ‘comment’ components of this
briefing represent science commentary at a single point in time – information herein may or may not align with Ministry of Health positions or priorities.

 Document 4
COVID-19 Science Updates
CSU 45
10 August 2021
Document 4
COVID-19 Science Updates
CSU 45
10 August 2021
1. COVID-19 Mortality in Children
The risk of death from COVID-19 is low for children compared to adults, but not zero. Here we review
several estimates for the risk of mortality from COVID-19 for children, reported in countries that have
experienced large numbers of COVID-19 cases in children: the US, England and the EU (see Table 1).
Table 1 Mortality rates for COVID-19 cases for children and adolescents (case fatality rate is the proportion of cases that result in
death; infection fatality rate is the proportion of SARS-CoV-2 infections that result in death). Rates are cumulative from the start
1982
of the pandemic in each country
Source
Gender
Age
Deaths
Cases
Mortality
Methodology ACT
(years)
Risk, Deaths
per 10,000
Casesa
0-4
175
619,091
2.8
An estimate of case fatality rate
US CDC
(CFR), i.e., the risk of death for
5-11
128
1,186,893
1.1
(link)
children with COVID-19. Data
All
12-15
139
1,069,780
1.3
updated 07 August 2021. Reporting
Cited 07
INFORMATION
August 2021
methodology for cases differs by
16-17
99
735,032
1.3
state.
0-4
4
56,739
0.7
aEstimates of mortality risk for the
English data are given as the
Male
10-14
5
142,653
0.4
infection fatality rate (IFR), i.e., the
OFFICIAL
15-19
27
207,112
1.3
risk of death for children infected
with SARS-CoV-2; The CFR was not
Public
0-4
6
53,907
1.1
THE
provided. IFR was calculated using
Health
10-14
8
143,000
0.6
number of deaths within 28 days of
England
positive test. Numerator includes
(link)
any individual with at least one
UNDER
Cited 08
positive COVID-19 test result,
Female
August 2021
either lab-reported or lateral flow
15-19
10
228,668
0.4
device. Positive rapid lateral flow
tests not confirmed with PCR test
are not included. Data updated 08
August 2021.
RELEASED
Male
<10
<5
7,635
1.3-5.2*
Estimate of case fatality rate (CFR).
*Range of values based on N=1-4
10-19
<5
13,833
0.7-2.9*
ECDC (link)
cases possible where the exact
Female
<10
<5
6,983
1.4-5.7*
number of cases was not available.
Cited 01
August 2021
Data period ending 01 August
2021.Reporting methodology
10-19
0
14,562
0
varies by country.
Context and disclaimer. This update contains topical talking points, science advice and research – it is intended as a high-level overview. The topics herein are
assembled ‘at pace’ often under urgency and may be based on reports that are not peer-reviewed. Both the content and ‘comment’ components of this
briefing represent science commentary at a single point in time – information herein may or may not align with Ministry of Health positions or priorities.

 Document 4
COVID-19 Science Updates
Document 4
COVID-19 Science Updates
• The mortality risk for children with COVID-19 (CFR) ranges from approximately 1-3 in 10,000 for
most subgroups. As expected, the IFR is lower; the IFR estimates from England range between
about 0.4-1.3 deaths per 10,000 infections.
• Furthermore, a recent study in England reviewed all deaths in children (<18 years) who had
reported a positive test for SARS-CoV-2 infection from March to February 2021
(link). After
clinical review, COVID-19 was determined to be the cause of death in 25 children. Of those, 15
had a pre-existing life-limiting health condition. However, the study did
not report the case or
infection fatality rate (and so cannot be compared to the estimates in the Table). Instead, using
the total population aged <18 years in England, the authors estimated that the overall mortality
1982
risk due to SARS-CoV-2 infection was approximately 2 per million.
Comment:
ACT
In children, death due to COVID-19 is rare: approximately 1 to 3 deaths occur per 10,000 COVID-19 cases
in children. These estimates do not account for hospitalisation or comorbidity due to COVID-19. Also,
these rates are cumulative throughout the entire pandemic, and do not account specifically for the Delta
variant, which appears to be associated with more severe disease. Mortality risk is important for
evaluating the benefit-risk calculation involved in the decision to immunise children. Based on Pfizer’s
clinical trial data for 12-15 year-olds (N=1,131 randomised to vaccine and 1,129 to placebo), the vaccine
INFORMATION
efficacy for symptomatic disease was 100%. As with adults, the personal protection from vaccination
should be considered in addition to any population protection via a reduction in overall transmission.
OFFICIAL
THE
UNDER
RELEASED
2 of
2
Context and disclaimer. This update contains topical talking points, science advice and research – it is intended as a high-level overview. The topics herein are
assembled ‘at pace’ often under urgency and may be based on reports that are not peer-reviewed. Both the content and ‘comment’ components of this
briefing represent science commentary at a single point in time – information herein may or may not align with Ministry of Health positions or priorities.