Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
help with ‘Stamp it Out’ and ‘Prepare for It’ pillars e.g. through model ing, contact tracing and testing
protocols, emerging technologies, and ensuring that debate around Alert Level responses is grounded
in what wil be effective.
The A3 does not include the ‘Manage the Impacts’ pillar but this wil be a focus slightly further down the
track e.g. readiness of health system infrastructure and the workforce, how we best engage
communities for equity, access and learnings.
Internal discussion ongoing as to how to best represent and integrate vaccine activity into the
Elimination Strategy.
Fine-tuning the Elimination Strategy wil be an ongoing area of work over the next month and wil be
brought back to a future TAG meeting for further discussion (or via email).
TAG members were asked to provide feedback on fine-tuning the Elimination Strategy based on the
provided overview.
ACT 1982
TAG feedback included:
• It is timely to focus on revisiting the Elimination Strategy
• Sense of complacency as vaccines roll out is one of many threats
• Shift to require pre-travel testing likely to have had a small but useful impact. The Ministry is
developing a trend report tracking arrivals.
• A common difficulty is not having enough evidence, or not putting processes in place to try to
INFORMATION
collect evidence e.g. by conducting pilot studies. The complex distributed MIQ environment has
made the evaluation of changes chal enging.
Pillar 1: Keep it Out
• There could be a strong role for model ing in Pil ar 1. Including variables such as numbers of
travellers, duration of quarantine, R, incorporating changes with new variants etc.
• The current focus seems to be on ‘keeping it out’ of the community, but not necessarily MIQ.
Would like improved understanding of the cases coming into New Zealand and how they are
being acquired, e.g. before flight vs on flight. More in depth case studies are needed.
• Ministry attendees noted that in-depth Public Health assessments are carried out but where the
virus was acquired is difficult to determine. Information from case investigations, EpiSurv and
genetic sequencing is being pul ed together to help answer these questions.
• Even with detailed source investigations – determining exactly source/ transmission route is not
always possible.
• Every incident of potential in facility transmission is investigated through an incident review
process which has been standardised in recent weeks.
• Suggestion to shift focus in border management to more offshore settings – for example,
Australia has significantly reduced the allowed number of arrivals. NZs high numbers of arrivals
RELEASED UNDER THE OFFICIAL
makes us vulnerable.
• The Pullman cluster and Christchurch cases last year demonstrate that post-isolation
requirements need to be reconsidered.
• Management of quarantine free travel zones – if people from ‘quarantine free zones’ are in
contact with people from other countries in airports, there is still a potential risk
Document 1
Group was reassured that a very wide range of options/suggestions for improving border controls was
being explored at pace.
Aspirational goal of having no cases arrive in NZ is highly desirable – suggestion to require quarantining
in airport hotel or home in origin country prior to travel. Suggestion to carry out research – e.g. ask a
sample of people about what would make it easier to alter their pre-travel behaviour. Noting it seems
logical to focus on the people incoming on flights rather than the whole NZ population. Chair noted that
such measures are extremely hard to impose/ensure compliance, and that overseas hotels may be a
potential transmission risk.
Pillar 2: Prepare for It
• Feedback from community providers: concern that overall rates of community testing have
dropped – need for continued vigilance should be highlighted.
ACT 1982
• It was noted that the Surveil ance Strategy is going to be careful y reviewed
• The UK experience indicates new variants may have arisen in a chronically infected individual so
understanding genetic variation, particularly in the spike protein wil help inform vaccine choices
and understanding of whether vaccine updates are needed
• Would like to see greater alignment between genomic epi modelling and TPM modelling
• This Pil ar should include reference to ‘correlates of protection’ – we need to understand what the
correlates of protection are post-vaccination, and how to test for them (e.g. we may need a
INFORMATION
certain level of antibody response to deem that a person is protected from infection). It is possible
that some people arriving into the country who have been vaccinated may stil not be protected
from infection.
• Current messaging abut testing – e g. get tested when you have compatible symptoms, stay
away from work –puts the onus on the individual. It may be beneficial to also have onus on
workplaces to support this
Members were asked to send further feedback to TAG Secretariat.
3.0
Update on Vaccines
The COVID-19 Vaccine Programme is an end-to-end sub-directorate within the COVID-19 Health
System Response Directorate, with over 100 people working on planning for acquiring, storage and
distributing vaccines.
The initial 50,000 Pfizer vaccine doses are expected to arrive in the next 2-3 weeks.
Rollout wil begin across North Island MIQ facilities, fol owed by healthcare workers and age residential
care staff. The South Island roll-out wil run about a week later.
Medsafe has provisional y approved Pfizer vaccine. The Ministry and the COVID-19 Vaccine TAG has
advised that the vaccine is considered safe to deploy.
RELEASED UNDER THE OFFICIAL
Questions about other vaccines continue to be worked on, but we are not expecting delivery of these
until later in the year. NZ has advanced purchased a total of 18 mil ion doses – if they all land, there wil
be a surplus. There is a proposal to consider how these might be re-distributed.
Dr Collin Tukuitonga wil soon be vising the Cook Islands to carry out a site assessment for vaccine
rollout, to be supported by New Zealand and Australia logistics.
TAG feedback included:
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
Caroline
60
Any Other Business
Circulate the Rainbow Chart the TAG
McElnay
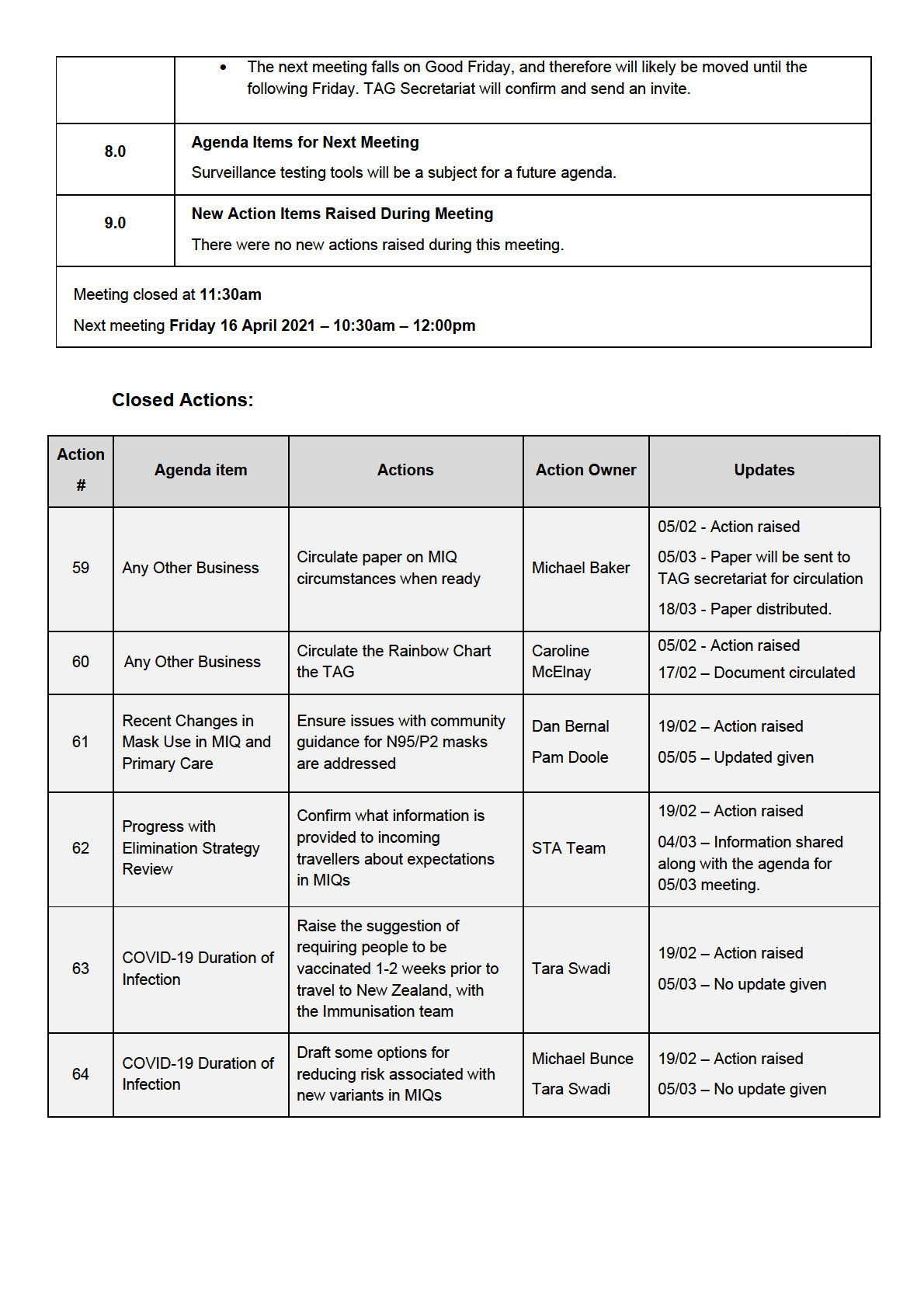
Meeting closed at
11:30am
Next meeting
Friday 19 February 2021 – 10:30am – 12:00pm
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
• Sir Peter Gluckman’s recently published commentary was mentioned, which contains thoughtful
questions for what COVID-19 means for New Zealand in the future (TAG secretariat wil
circulate).
• The Director-General of Health and the Chief Science Advisor are to be interviewed by the
IPPR Committee co-chaired by Rt Hon Helen Clarke
• Last week the PM, Ministers and Ministry staff met with business leaders in Auckland to provide
insights and commentary on the management of COVID-19 and impacts on business/the
economy
• An in-depth dive into the potential of using saliva testing as a screening tool is underway. Note
that the NZMN is having a special meeting about saliva testing on Monday – can see the
appeal of saliva testing for surveil ance purposes. Wil report back to TAG.
3.0
Recent Changes in Mask Use in MIQ and Primary Care
An update was provided on changes in MIF/Qs in terms of the use of N95/P2 masks.
ACT 1982
• Change has resulted from a number of factors, including: emergence of new variants with
possibly increased transmissibility; further consideration of the risk in confined spaces where
some staff are interacting with returnees; growing evidence of transmission of COVID-19 via
aerosolised particles, particularly in closed spaces with poor ventilation. Al these factors were
considered by several stakeholders, who agreed that a change was indicated for staff with
close interactions with returnees.
TAG Feedback included:
• There needs to be some clarification of the new community mask guidance. Communications to
INFORMATION
GPs and urgent medical care facilities (about changes allowing use of N95/P2 for these
facilities in specific contexts) was not as clear as it could have been.
• Importance of proper fit testing – and clarifying who pays for it
• Eventually the guidance wil need to evolve so it is related to risk, site and function, and not
profession-specific
4.0
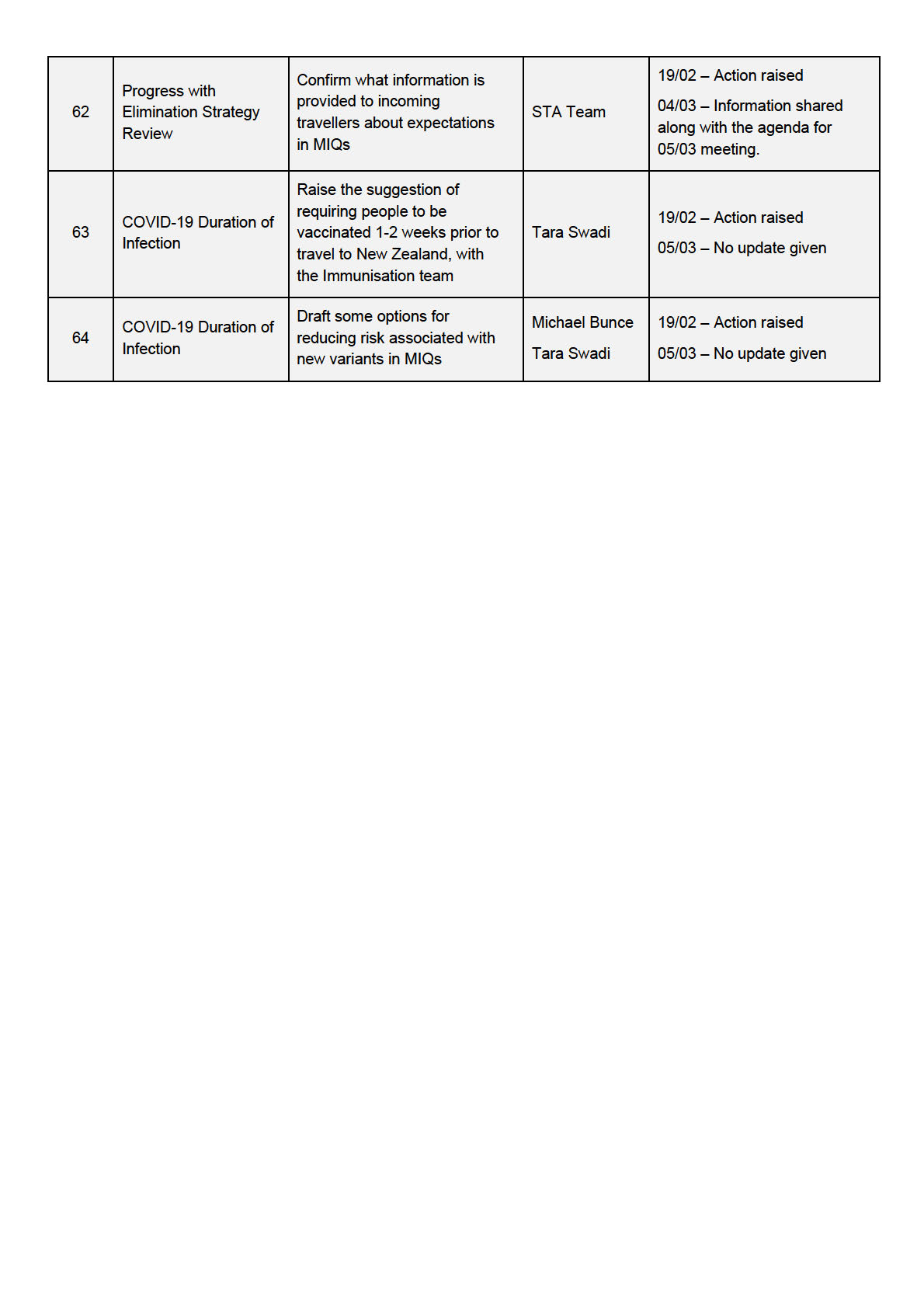
Progress with Elimination Strategy Review
Stephen Harris thanked the group for fol owing up after the last meeting with specific and useful
feedback and welcomed further communications of ideas.
The Weekly Update (‘Horizon Scan’) is intended to be a mechanism for providing regular feedback
to Ministers and to each other about what is going on across the whole of government sphere.
Unfortunately, a Ministerial strategy session had to be postponed this week due to the outbreak, so
have been unable to engage Ministers as hoped.
TAG Feedback included:
• The A3 is a useful and concise visual layout
• For ‘Keep it out’ – a query was raised if there was an overall decline in the number of incoming
people testing positive, and could this be a consequence of pre-departure testing
RELEASED UNDER THE OFFICIAL
o A report is being put together on the positivity numbers and rates at different time points
and in relation to testing regimes and wil be interested to see if PDT has reduced the influx
of cases. This report wil be shared with the group once completed.
o The Chair agreed that the risk to New Zealand is proportional to the number of incoming
cases. The Ministry is interested in monitoring trends, though this is not easily available as
the way information is col ected requires several data feeds to be integrated.
Document 1
• Manage the Impact - would like to see something about equity outside impacts on small
business.
o Equity is going to become more and more prominent across all the pil ars – one of the ‘load
bearing cables’ of the elimination strategy.
o There is a new Māori advisor in the Policy Team
• For Keep it Out pil ar – could there be an explicit bullet point about communications pre-travel,
regarding what the Ministry wants people to do during the week prior to travel and during travel
before they arrive in New Zealand, aiming to minimize their risk of acquiring COVID-19 which
then manifests after arrival?
In the next few weeks there wil be a gear shift in the way the Elimination Strategy is addressed.
Within the directorate, there is a dedicated team of half a dozen people who wil meet and parcel
out areas of particular focus for revolving pairs, who wil go out and consult with people, eliciting
information and further granularity. This wil represent a shift to a more proactive mode. More
ACT 1982
regular dialogue with TAG members individual y and as a group is anticipated, to give some
confidence around the evolving uncertainties.
• Michael Baker to provide a written commentary directly to Stephen Harris and Chair on
potential Alert levels (and steps proposed)
• Intended approach in the medium and longer term is a fundamental question that wil guide
activity this year
INFORMATION
George Whitworth from DPMC introduced another part of the Elimination Strategy work, which is
currently underway, repeating the COVID-19 scenarios exercise. This involves considering different
scenarios we may need to prepare for in the next 6-18 months, using health, social and economic
lenses and carrying out foresight analyses to help AoG navigate challenges and make decisions
with a longer timeframe in mind Some draft material wil be shared with TAG for the next meeting.
Welcomed input from the group, particularly any under-appreciated aspects/ risks.
5.0
Surveil ance Update
An update was provided on the Surveil ance Strategy:
• Late 2020 there was a review of the Surveil ance Plan, which resulted in some terminology
being changed slightly. New documents have been available on the Ministry of Health website
since late January
• The Surveil ance Strategy provides a high-level understanding of what we are trying to do, roles
of different organisations, and a list of guidance documents. It is intended to be reviewed at
least every 6 months
• Sitting under this is the Testing Plan, which is reviewed more frequently, to ensure we are
carrying out the best type of testing to answer questions in the current context
• Testing guidelines are put out by the Testing Operations team and are updated every couple of
RELEASED UNDER THE OFFICIAL
weeks, providing guidance as to exactly who needs to be tested and who needs to isolate while
awaiting test results
• Over the last couple weeks the focus has been pul ing together a surveil ance update into the
Testing Plan - tabulating who wil be tested in particular epidemiological contexts, (e.g. no
comm transmission/ small amount of community transmission/ widespread transmission) and
which kinds of test technologies might be used (where they fit in different contexts and are most
usefully deployed). Once this document is finalised, wil be moving into process of looking
Document 1
closely at all components of the Surveil ance Strategy and how they need to change as we
have a partially vaccinated population.
• A lot depends on the what we think about whether people who are vaccinated are less
infectious
• A suite of documents is being prepared, and these wil be circulated for information to TAG
• Recent experiences have shown us that regional responses can be useful. For example,
repeatedly negative tests from sewerage sampling in Northland helped provide reassurance
that there was no undetected community transmission occurring
6.0
Update on Vaccines and Immunisation
• COVID-19 vaccines are a hot topic in the media
• A large team is are working on the rol out. The first New Zealander is to be vaccinated on
Friday 19th – a smal group of vaccinators
• Working with Northern DHBs, Māori and Pacific providers to provide an integrated rollout.
ACT 1982
• Noted that the programme wil be easier in the controlled environment of MIQs compared to
community rol out
• Over the next 4-6 weeks, vaccines wil be delivered to MIQ workers across the North Island and
then to Canterbury – wherever there is an MIQ. Al workers, family and whanau wil be offered
the vaccine
• Tier 1 wil receive the Pfizer vaccine, which is stored in freezers in Auckland and Christchurch
• After Tier 1 rol out, vaccines wil be offered to a wider group health care wor
INFORMATION kers etc
• There has been an active period of discussion with Pacific and Māori leaders over the last
couple of days about the potential to bring forward access to vaccines for these populations, in
addition to the age and vulnerability criteria
• The rollout to the general population is expected from mid-year. A large amount of work is
going into this rollout, with the scale and logistical challenges being unprecedented.
• The Ministry of Health is also focused on literature about effectiveness and safety of vaccines,
information about variants, and potential for vaccines to be adjusted for new variants.
• There is a specific COVID-19 Vaccine TAG, but TAG wil also be kept informed and may be
asked questions, or there may be things that the group would like to raise.
Discussion from the group:
• It was noted that perceptions about the efficacy of the different vaccines wil need to be
carefully managed. The Chair noted that Minister Verrall is fol owing developments
• The Ministry of Health is very aware of the need to ensure that no-one feels they are getting a
‘lesser’ vaccine.
• A question was raised as to whether vaccinati
RELEASED UNDER THE OFFICIAL on of border workers is being accompanied by
increased frequency of testing.
o The Minister has said there wil be no reduction in testing
o Discussions are underway regarding whether more frequent saliva testing may have a role
to ramp up assurances.
Document 1
• Comment that it is great that the Pfizer vaccine is being rolled out to MIQ staff in an early timely
way. Even though there is limited information about potential impact on transmission, it is likely
that there wil be a significant effect.
• Suggestion for some better communications about reactogenicity with this vaccine (e.g.
headache, fatigue, and fever are common). This may help everyone take this in their stride
rather than generate mistruths
o It was noted that information sheets for MIQ workers and managers are being fine-tuned
and trying to front foot this issue. The Ministry is in daily contact with border Chief
Executives
• Question raised as to how public perceptions/ acceptability of vaccine are tracking, as news of
both vaccine success and news about side effects are common. Wil there be a larger ongoing
study?
o The Ministry of Health has commissioned Horizons Research to do a fortnightly survey on
vaccine attitudes, which are critical y important. The first results were released yesterday in
ACT 1982
a Q&A media session
o The Ministry of Health also has team monitoring social media chat and responding to
questions and comments
7.0
COVID-19 Duration of Infection
Background: The UK variant accounts for about 50% of cases coming into New Zealand. There is
solid evidence that it is more transmissible. There is mixed evidence about viral load – it typically
appears to be higher, but there is a large natural variation. Some viral loads are extremely high,
representing 2-16 x more viral RNA.
INFORMATION
A pre-print from Harvard was provided to TAG for background reading. It described a cohort of 65
patients who underwent daily surveil ance to investigate infection dynamics and duration. Only 7
were genotyped as B.1.1.7 (under-powered for the variant). It reported that duration of infection is
potentially longer with UK variant compared to wildtype (though virus culture was not carried out, so
we don’t real y know if the viral loads are synonymous with infectious particles). The study is
underpowered for the variant, but the underpinning methods appear solid. The preliminary
indication that B.1.1.7 samples have higher viral loads is consistent with other recent reports. In
contrast, the preliminary conclusion that B.1.1.7 necessitates longer periods of isolation is not
consistent with the science advice coming out of the UK which has not observed (or reported) the
need for extended isolation periods.
The question for TAG was how solid the evidence should be for a higher viral load before changes
are recommended. The main significant implication is the duration of infection and whether we need
to change the recovered case definition – i.e. Is 10 days stil adequate, especially considering that
exit screening is not carried out for people who have tested positive? Is there any indication of a
need to extend quarantine for those who test positive, especial y for those with variants? Noting
also fails on genome sequencing are common, which also raises the question of whether any
change in policy should apply to all who test positive.
RELEASED UNDER THE OFFICIAL
TAG feedback included:
• There is good evidence for a higher viral load
• People are most infectious around the time symptoms develop, or just before, so the first week
of infection is likely to be the most problematic
• Using symptoms for de-escalating IPC can be very inaccurate
• Extending isolation to 14 days after symptoms develop could be a good idea
Document 1
• Risk stratification – not helpful putting everyone under same restrictions (e.g. people who are
historic cases)
• Recommend avoiding re-testing people, as a lot of people have ‘long tails’ of RNA detection but
would no longer be infectious
• Another paper is contradictory, showing variant cases are positive for less time
• The one-week period after people leave MIQ needs to be thought about more actively
• s 9(2)(f)(iv)
s 9(2)(f)(iv)
ACT 1982
8.0
Māori Health Perspectives
Focus at the moment is on vaccines. Likely to take a similar approach to Native Americans, framing
the vaccine as ‘your right to good health’
9.0
Pacific Health Perspectives
INFORMATION
A program of engagement is underway for Pacific peoples using established networks and
providers
10.0
Any Other Business
11.0
Agenda Items for Next Meeting
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
2.0
Ministry of Health Update
• The current outbreak has been interesting in that the virus has not behaved in the way
that the B.1.1.7 variant was expected to, leading to questions on how dynamics of New
Zealand’s community context may differ.
• The Ministry of Health has provided advice to Cabinet, and announcements on alert
levels are expected this afternoon.
• The extraordinary effort of those in Auckland was acknowledged, supported by contact
tracing efforts from PHU col eagues around New Zealand.
• Investigations into the origins of the outbreak continue with no source yet identified.
3.0
Definition of Contacts
Background:
• The outbreak has been well covered in the media in terms of the contacts, and the
ACT 1982
metrics used to monitor the operational management of the outbreak
• A review had occurred earlier of the contact categories, which previously was limited to
‘close’ or ‘casual’ contacts. The Ministry of Health wanted to apply the lessons learned
from prior outbreaks in the review process and developed this new technical document in
November 2020.
• Definitions of contact categories have been recently be expanded to five categories with
contacts categories ranging from ‘no contact’ to ‘close plus’.
• The document is used by the Ministry of Health and Public Health Units
INFORMATION to guide the
assessments made by Medical Officers of Health when assessing groups of contacts,
articulating what needs to happen for each type of contact category. The technical
guidance is used in advice given to contacts and by Healthline to provide consistency
across the health system, though adapting it to accessible language has been a
challenge.
A precautionary approach was taken given the knowledge that this was the B.1.1.7
variant, that the variant may have longer incubation periods, and that there were few
population-level controls at the time. A decision was made therefore to not change the
management but to re-categorise people from Kmart as ‘close’ or ‘close plus’. The
framework continues to be used by Public Health Units for their guidance.
• Once this cluster is contained, there wil be an in-depth epidemiological review of the
framework looking at secondary attack rates, the impact of recategorisation on
management, and the impact on public health and contact tracing services.
TAG feedback included:
• It was noted and acknowledged that the recategorization had an impact on workload.
• The group agreed it was useful to have more categories than just casual and close.
• It was noted the ‘close plus’ category needed some clarity, as household contacts of
RELEASED UNDER THE OFFICIAL
close contacts would be considered at risk.
o The key distinction here is that it is a second order contact and isolation category
(and therefore households are also in isolation). This is useful early on in an
outbreak when there may be second or third chains of transmission.
• A query was raised on how many days prior to symptoms contact tracers go back, as
going back 5 days would find exposures and trace origins.
Document 1
o Contact tracers go back 48 hours prior to symptoms to look for exposures. When
there is no obvious source, a source investigation is also undertaken which goes
back 14 days, however this is done by another team, so one team looks back
and one team looks forward.
• Discussions of this virus having a “long tail” were queried. It is the infectious period for
which there is more evidence on it being longer, not the incubation period.
o It was noted that what was more important to note here was the delay in getting
tested by some, who had symptoms for 4-5 days before being tested. The
atypical symptoms also contributed to this delay and therefore issues were
aggregated. This led to the alert level change as a precautionary measure.
• There have been some issues with translating the new contact categories into other
languages and stil capturing the subtle differences.
• The strong community response and high-testing uptake within South Auckland was
acknowledged.
ACT 1982
4.0
Elimination Strategy Update
It was noted that Policy and DPMC had been diverted from this due to the alert level changes,
however an ongoing review is occurring of the Elimination Strategy and updates are iterative.
Work is stil underway, and a more formal and comprehensive update wil be provided at the
next meeting.
5.0
Refinements to the Alert Level Options
A paper presenting possible refinements to alert level options was presented t
INFORMATION o the group. The
Director-General of Health has asked to be updated on the group’s thinking and is keen for
feedback on the nuances within levels and for a risk-based response.
The motivations behind the report were threefold:
• To better manage outbreaks, as having four levels was argued to be weighted towards
lockdown with little room to control spread below that. The paper expands Level 2 to be
able to control community transmission without lockdown.
• To incorporate new knowledge, evidence, and experience, in relation to transmission,
masks, and superspreading aspects and what we know that a smal group of people tend
to contribute to the majority of cases of onward transmission.
• Focus is also needed on equity and acknowledging the hardship many communities have
faced over the past year.
The suggested refinements use alert levels to complement contract tracing and public health
efforts to avoid lockdowns, and to provide more nuance to ensure that levels are distinctly
different.
Discussion from the group:
• The government has chosen to weave additional sub-controls into levels before, however
these have been ad hoc thus far therefore it is difficult to see the broader framework.
RELEASED UNDER THE OFFICIAL
• The emphasis on strong public health messaging must also continue, for example on
cough etiquette and hand hygiene.
• IPC controls also need to increase in other residential facilities where there are risks of
outbreaks, therefore there was a suggestion of adding further setting-specific advice.
• There was some concern that the messaging would create confusion regarding large
gatherings. Within this model we would cycle through alert levels more quickly, and this
would be disruptive for planning of larger gatherings such as sport events.
Document 1
o It was argued there is minimal evidence on the effectiveness of putting numbers
on gatherings, with studies finding little in the way difference related to absolute
size, and therefore focus should be on making sure environments are managed
sufficiently with ventilation, or by being outdoors.
• A question was raised on how this would change with wider vaccination rollout and
knowledge of community immunity, and how further cases would be managed.
• A question was raised on when the best time would be to bring new levels or nuances in.
o It was argued that now may be the best time as people are paying attention due to
the outbreak, and as we come down it is important that vigilance is maintained and
there are some options provided that have their basis in science.
• It was also argued that we already do have seven levels though they were just neve
defined (e.g. level 0 as normal activity and no public health treat, and level 2.5), therefore
this would make the status quo more meaningful.
• The government is committed to a framework with Alert Levels 1 to 4, and therefore any
change would need to be expressed within that framework.
• Aspects such as inter-region travel restrictions need further consideration.
ACT 1982
• Any changes would have implications for hospitals, as it has taken some time to set up
systems and achieve consistency across the country.
Any further feedback or observations can go directly to Dr Amanda Kvalsvig
([email address]) for incorporation into the report and to further develop thinking.
The team may come back with another version.
The Ministry of Health wil need to provide advice to the Director-General of Health on the report,
and they wil consult with the authors as the advice is prepared.
INFORMATION
6.0
Long-Term Strategy - Business Engagement
• Three weeks ago, the PM, Ministers and Ministry of Health staff met with business
leaders in Auckland to provide insights and commentary on the management of COVID-
19 and impacts on business/ the economy.
• An article has been shared with the group from Sir David Skegg, Sir Peter Gluckman,
and others from the COVID-19 Working Group to the International Science Council, an
international think tank looking at future scenarios for the COVID-19 pandemic.
• It is an appropriate time to be having these discussions as the vaccination rol out
begins and therefore the commentary is well-timed.
• Efforts are underway to engage with the business community more widely.
• The sector is keen to hear what scenarios the government is considering, as this wil
have implications for the way businesses plan, for example in relation to the borders,
travel, and tourism.
• DPMC wil be coordinating this work.
TAG feedback included:
• Opportunities for incremental improvements should be identified and rol ed out, ensuring
RELEASED UNDER THE OFFICIAL
the system is flexible, versatile, and road-tested for the future.
• There was a call for a public health agency to take us into the future, with concern that
other crises wil divert attention from the learnings.
• There is a wil ingness to involve the private sector and get ideas from economic leaders
into the mix on how business can be managed going forward.
7.0
Māori Health Perspectives
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
alert levels could be integrated into existing levels and language, similar to the Level 2.5
option.
Discussion from the group:
•
A question was raised on whether there would be any further investigation into the
source of the Papatoetoe High School cluster and whether serology testing would shed
more light. A question was also raised on whether serology testing of staff at the
Sheraton Four Seasons was conducted.
o A decision was made not to investigate the source further and not to pursue
serology testing within the School or Sheraton. The time and workload required
to obtain blood samples was not deemed to be a risk proportionate response.
o Kits using finger pricks and laboratory ELISA testing are being considered to
enable a more rapid response, though currently their sensitivity is lower than
rapid POC testing from blood samples. There wil likely be a role for serology in
the future when looking at the impact on people with previous infection or
vaccination.
ACT 1982
•
It was argued that this year is the year for legacy and investments, and now is the best
time to make changes for an enduring approach that is more versatile and responsive to
change.
•
Clarification was requested on the functions of the new expert advisory group set up by
the Minister to assist with quality assurance, led by Sir Brian Roche. The group has not
formally been convened yet.
INFORMATION
3.0
Elimination Strategy Update
•
Apologies have been sent by Stephen Harris, George Whitworth. Their team has been
heavily focussed on travel free zones as intentions to open a travel bubble with Australia
have been brought forward. The implications of this for border management wil feed
into the elimination strategy conversation.
•
Work continues on the Elimination Strategy, along with the request from business
leaders for being part of the strategic approach. Each of these wil come together in the
coming months with the Prime Minister planning to give an update during parliamentary
recess after Easter.
4.0
Vaccine Rollout
The Chair provided an update:
•
Virtually al MIQ staff have now been administered their first dose, and second doses are
underway.
•
There has been some difficulty getting interest in vaccination from families of the MIQ
workers.
•
Different DHBs are at various stages of planning for the wider rollout. For example, Capital
RELEASED UNDER THE OFFICIAL
and Coast DHB only have two MIQ facilities with one not in use, they have already started
vaccinating frontline healthcare workers.
•
Regarding the supply chain, larger amounts of the Pfizer vaccine are not expected until
May/June, with the more general rollout stil expected to be from July onwards. Attempts
are underway to try to bring these larger deliveries forward.
•
Janssen have asked if New Zealand would like its contracted delivery brought forward. A
process of complementary rollout could occur with dual effort for both vaccines and the
Janssen vaccination could be given in a wider variety of contexts (e.g. pharmacies) as it
Document 1
only requires a single dose though stil has good efficacy. It is currently in the final stages
of consideration by Medsafe and a discussion of complementary rol out of the vaccines wil
occur.
•
The Director General and Chair were interviewed by the Health Select Committee on
vaccine targets. The current advice remains that we should try to vaccinate as many
people as possible, however there remains pressure from some MPs for a vaccination
target.
•
Studies are underway to monitor vaccine effectiveness among children. The Ministry of
Health is monitoring developments, but this could provide an additional target population,
initially 12 to15 year old.
•
The high-risk categories used for flu vaccine prioritisation are being considered for COVID-
19 vaccinations with some additions specific to COVID.
Discussion from the group:
•
The borders may not open until everyone is vaccinated, and therefore a question was
raised as to whether it may be better to vaccinate those who are high-risk later once ther
ACT 1982e
is broader population immunity and high antibody levels.
o It was noted that the calls for vulnerable populations to be vaccinated are a higher
priority
o The Prime Minister is taking a precautionary approach to border openings,
carefully calibrating opening against communication, and the trust and partnership
with different states and territories in Australia. Australian Health Authorities have
been quick to push pause, however once confidence builds and there is trust in
the ability to track and trace cases then less interruptions may occur. The Ministry
INFORMATION
of Health is working hard to develop these protocols.
•
There has been unease among GPs and in primary care on the scale and burden that
vaccine rollout will have on routine care. It was argued that clarity and guidance is needed
on expectations and roles. If we vaccinate two mil ion people in the next four months, that
is four mil ion vaccination events, on top of the 1.5 mil ion flu vaccination events, and
therefore the impact of the system wil be large. A question was also raised about the
necessity to separate out the flu vaccination from COVID-19 vaccination by two weeks,
and whether this could be changed to reduce the number of vaccination events and
burden on the system.
o The need to separate the flu vaccination from the COVID-19 vaccination is under
active review by IMAC and the Public Health team, noting that there is a workload
issue.
o Work is underway to harmonise communications and connections between the
Ministry of Health and DHBs, within DHBs, and with primary care. This has been
raised in CIVP Steering Group and it is agreed that clarity is needed with the
general population asking questions too.
•
A question was also raised on whether flu vaccinations wil be used this year, and what the
Ministry of Health’s position on this is.
o The flu vaccination programme wil go ahead.
RELEASED UNDER THE OFFICIAL
•
A question was raised about how population immunity is modelled and whether this was
part of any upcoming work.
o It was argued that the policy of ‘zero tolerance’ is unsustainable if borders open.
o It was noted that there are likely to be regional variations in uptake and protection
which wil create vulnerabilities if there are outbreaks in pockets of the community
where vaccine coverage is not high. In these instances, the Ministry of Health is
Document 1
relying upon local knowledge of DHB and community colleagues to identify
particular strategies.
o The Ministry of Health is continuing to use language of population protection and
population immunity over herd immunity.
• Questions were also raised on how vaccine rollout wil be adapted with the emergence of
new variants globally, as transmission is likely to continue for some time in other countries
with large populations and low vaccine accessibility.
o s 9(2)(b)(ii)
o s 9(2)(b)(ii)
• A question was raised about whether the goal remains to protect New Zealand from
importing cases, and if so, then whether it might be possible to prioritise vaccinations
among people going on short-term overseas trips.
ACT 1982
o An ‘exit vaccination’ strategy is being actively considered, not only for sports
teams as well as with MFAT staff being deployed overseas.
• Clarification was requested on the current state of a national immunisation register.
o A new national register is currently in design, with it being revamped from being a
basic database to a national immunisation solution. This wil be a legacy
investment from the COVID-19 vaccination response. Currently the back
integration with NHI numbers and inter-operational requirements between DHBs
and with primary care are being addressed, as the Ministry of H
INFORMATION ealth wants to
leverage existing infrastructure
• Clarification was also requested on what are the medium (next one to two years) to long-
term strategies for the Ministry of Health, whether elimination wil remain a focus, whether
eradication may be pursued, or whether it is accepted that the virus may become endemic.
It was argued that the public health impact must be minimised.
o The Ministry of Health is continuing to pursue the elimination strategy would be
most sensible, though this wil need to be considered by Ministers.
o Information from overseas on the extent to which vaccinations provide protection
from transmission is being monitored as vaccination rol out continues.
o Work is required to manage expectations and shift the dialogue slightly, as the
opening of borders wil inevitably result in an increase in cases. This must be
accepted as a risk that can be managed, alongside building confidence that any
cases that do emerge wil be identified and isolated, and that ongoing chains of
transmission are prevented as the system becomes more agile. Similarities were
noted regarding how New Zealand handles measles.
5.0
Māori Health Perspectives
No update given.
RELEASED UNDER THE OFFICIAL
6.0
Pacific Health Perspectives
No update given.
7.0
Any Other Business
• Work on the national strategic direction and the ability of the government to apply
learnings, adapt advice, and become more efficient are ongoing, and wil continue to be
discussed in future meetings.
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
may have less frequent exposures but may stil have exposures with significant risk of
transmission.
• Protocols for border workers may also be applicable to some healthcare workers.
Vaccine rol out
• The vaccine rollout has been a chal enge. Overal , the coverage for Tier 1 has been good.
The vaccine workforce wil require further development, and this has a high priority.
• The recent development of coagulation disorders associated with the AstraZeneca
vaccine has caused major disruptions of vaccination programmes around the world.
• It was noted that Australia has announced that there is likely to be a delay to full
immunisation of the population which wil not now occur this year as planned.
• In New Zealand, the final approval of the Janssen vaccine has been delayed pending
further information from the company about blood clotting issues.
TAG Feedback
ACT 1982
• Concern was raised from the primary care sector regarding an apparent lack of
communication regarding the vaccine rollout. This has been escalated to the Programme
leads.
• There was discussion regarding employment of non medical y / health trained personnel
undertaking vaccination and concerns that this could undermine confidence in the
vaccination programme.
• Regarding the clotting problem with AstraZeneca, it was noted that there wil be intense
competition for the Pfizer vaccine, and that pre-ordered doses may not
INFORMATION be delivered. The
possibility of individuals who want to travel purchasing vaccines was raised.
• Messaging regarding the side effect of vaccines was discussed. Two points were raised.
The first related to the way in which the details of the complications were presented to the
public, via the media. Although there have been cases of cerebral venous sinus
thrombosis, the rate of these complications is stil very low. Presenting absolute numbers
is more alarming than presenting rates per mil ion or percentages (i.e., no denominators
are being given) Although it is possible that there wil be some complications identified
with the Pfizer vaccine, it would be difficult to provide this information proactively without
causing public concern.
• The national immunisation solution which is being tested currently and wil eventually
replace the current national immunisation register.
• There was some general discussion regarding the relationship between the vaccine
rollout and changes to border controls.
3.0
Elimination Strategy
• The Chair shared in confidence a slide of the draft plan for moving to open borders. The
information was stil at a high level and wil be presented in more detail as the issues are
worked through.
RELEASED UNDER THE OFFICIAL
• There was discussion regarding the goal with regards to elimination or accepting ongoing
circulation of the virus, with the recognition that it was not yet possible to determine which
outcome could or would be pursued. It was also noted that this is more a global than NZ
or Australasian decision.
4.0
Review on Alert Levels
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
s 9(2)(f)(iv)
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
s 9(2)(f)(iv)
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
s 9(2)(f)(iv)
ACT 1982
INFORMATION
4.0
Māori Health Perspectives
• No update given
5.0
Pacific Health Perspectives
• No update given
6.0
Any Other Business
RELEASED UNDER THE OFFICIAL
• None noted
7.0
Agenda Items for Next Meeting
• None noted
8.0
New Action Items Raised During Meeting
• No actions raised during 30 April 2021 meeting
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
• It was commented that surveil ance testing advice is not fit for purpose anymore. Feedback from GPs
is that patients are presenting late in respiratory il ness as they do not want to have to isolate. New
Zealand would benefit from pushing a surveil ance programme that emphasises getting tested on
day 1-2 of respiratory il ness, using masks, social distancing, and use of the COVID-19 Tracer app,
rather than advising people to isolate. This would make it more accessible because the current
isolation recommendation is being ignored by the general population. Work needs to be done on ‘fit
for purpose’ advice, as surveil ance strategy has not been updated since last year.
• The surveil ance plan is being reviewed.
Vaccine rol out
• The Chair gave an update on the vaccine rollout. It was noted that Melbourne pivoted their rollout
quickly.
• New Zealand is very dependent on Pfizer at the moment. Pfizer’s Global Al ocation Model wil run on 1
June, and we wil know then how we wil receive the next shipment towards the 450,000 doses
ACT 1982
ordered. Supply chain issues have prompted a shift in communications by the government to note
Group 4 can now be expected to start from the end of July.
• Discussions are occurring on how to onboard other vaccines, which are a work in progress and there
is no current rollout plan for these.
TAG feedback included:
• A comment was raised on the confusion in the community and among GPs about Group 3.
INFORMATION
o Communication about delivery and access can only be started when we know how much
vaccine we have on shore, otherwise there is a risk of further confusion. The actual criteria for
who is in Group 3 has now being clarified, and there wil be greater communication and clarity
over the next week or two.
• A comment was raised wondering if it would be helpful for the criteria for Group 3 to harmonise with
the influenza criteria, and whether there was sufficient different to warrant separate criteria for both.
o Communications are being actively worked on and tidied up by clinical col eagues in the
Ministry.
• A comment was raised about when there might be approval of the vaccine for 12-16-year olds.
o Medsafe is considering the recent data from Pfizer
2.0 Science Updates
Products and Services on Ministry of Health webpage
(https://www.health.govt.nz/our-work/diseases-and-conditions/covid-19-novel-coronavirus/covid-19-resources-
and-tools/covid-19-science-news)
• An overview was provided on how the Ministry has been trying to make their work more accessible
with the creation of a Science News page. It is hoped it could be helpful to practitioners in the health
RELEASED UNDER THE OFFICIAL
sector. The Ministry hopes to share more with TAG on the breadth of the work being done to raise
awareness, but to also seek input from TAG members in these pieces of work.
• Kōrero Pūtaiao/Science Chat is where the team tackles topics that could be coming up in GP or
pharmacies to generate informed discussion. It is meant to not be too technical but not overly lay. The
next one coming out wil be on saliva testing.
• COVID-19 Science Update: A summary of the latest science and opinion. The next topic uploaded will
be on airborne transmission, and more wil be coming soon.
Document 1
• Variants of Concern Update: A short high-level summary of what is happening with the new variants
emerging. Ful report with references is also available and has detailed information on each VOC.
• The Pātaka Knowledge Hub was also shared to show TAG the internal Ministry science outputs which
collates key facts and figures about the virus. The Ministry will try to make this available through a
secure link to TAG members, and work is being with IT to enable this.
• Thanks was given to al in TAG who assisted the Ministry team with this and who responded quickly
when things needed peer review. The expansion of the Science and Technical Advisory Team meant
good progress was being made to summarise the science quickly and effectively, and it is hoped that
increasingly the team can support the wider public being informed too.
3.0
Elimination Strategy/Reconnect Aotearoa New Zealand An update on the Elimination Strategy and progress on Reconnect Aotearoa New Zealand was
provided:
• It has been four weeks since TAG was last provided an update on this work, and there has been
ACT 1982
intensive work to progress it since then.
• The Prime Minister is the now the lead Minister on the Reconnecting Aotearoa New Zealand work
because reconnection touches all portfolios. The PM wil be taking a paper to Cabinet in June to
explain what work is being done to ease border restrictions. The Melbourne situation reminds us that
the pathway to reconnection is not always straight and there wil be pauses along the way.
• The Reconnection framework was drafted alongside the Elimination Strategy. The paper that wil be
taken to Cabinet will also update on where the Elimination Strategy is currently and how it has
evolved. The Reconnection framework and Elimination Strategy are considered t
INFORMATION o be joint and
presented together, with a single narrative document that links policy and operations and enables
support of public conversations.
TAG feedback included:
• A question was raised about forward planning with Australia and how New Zealand can plan in
conjunction with what they are doing.
o Ministry colleagues join the Australian Public Health Committee meetings, and New Zealand
is a key partner in the conversations about risk assessment. The reciprocity of conversations
and bilateral risk assessment has been constructive and collegial and enables faster decision
making
• It was noted that for incoming travel ers, most of the cases at the border are picked up at day 0/1 and
it is unknown what proportion are asymptomatic or symptomatic. More information on this would be
helpful. It was proposed that one area of research could be testing for antibodies with a cohort of
incoming travellers, and that onshore research could be helpful. The pre-departure testing protocol
would also need to be reviewed for its sensitivity in picking up cases.
o Finger prick antibody and serology tests may mean this is a possibility, and this was
considered useful analysis.
RELEASED UNDER THE OFFICIAL
• It was noted that New Zealand is stil in the phase of preventing circulating virus (i.e. elimination) and
interrupting transmission. From a health and economic perspective, there have been advantages to
this even though we are uncertain about the long-term goal. It is currently impossible to know what the
‘final state’ wil look like as much more data and insight is needed.
o The Ministry of Health is advising caution, slow steps and to wait for further evidence before
decisions are made, especially after setbacks in Australia, Singapore, and Taiwan.
Document 1
• A question was raised asking if there has there been any research on community and hospital
preparedness.
o Resurgence plans need to be reviewed. There is a tension and high workload as the same
people rolling out the vaccine are the ones planning for resurgence. The Chair acknowledges
this concern and has asked senior leadership to look into these areas
Action: Draft a proposal for researching serology testing at the border.
Science Questions underpinning the Reconnecting Framework
• An overview was provided on the science questions underpinning the framework and how they fit in,
and what wil be assessed.
• The Risk Assessment Framework lists the levers that could be pul ed based on the science. It looks at
science questions categorised by context e.g. international/ border/ overseas, MIFQ, or community.
• Feedback was requested from TAG members to identify gaps in the science questions currently being
ACT 1982
answered.
TAG feedback included:
• It was noted that https://outbreak.info/ is a great resource for looking at VOCs. The emergence of
VOCs wil be heavily dependent on global prevalence of infection and rates of transmission.
• The ESR vaccination model and TPM vaccine model show promise for addressing the questions
under the ‘vaccination’ section. The models are similar and seem to be reaching similar conclusions.
INFORMATION
This wil enable decisionmakers to examine the effects of a range of things including the emergence
of VOCs with different R0 values, vaccine efficacy against disease and transmission, varying number
of infected individuals coming across the bo der, different vaccine roll-out strategies etc
• It was noted that for contact tracing, an assessment of close contacts and whether vaccination
changes their contact management wil need to occur, and this should take into account whether
people from high risk and unvaccinated groups wil require other restrictions.
• A question was raised on whether the Government is closer to developing a research and
development strategy.
o It was noted that there has not been any progress on this topic to date.
• It was noted that the resilience of health workforce needs to be captured within the framework, and
that this was an opportunity to catch system errors. Human behaviour is major risk factor that is not
being reviewed. Manpower and training of primary and secondary care health workforce is lacking.
o TAG members were informed that the Ministry now has a Manager leading Behavioural
Insights within the Science and Insights group. The Manager is just starting and wil be taking
a stronger lead on this. Wil try to bring them to TAG to expand on their work further.
• It was suggested that a broader discussion is needed on therapeutics, where there is a role for
national clinical guidance/ clinical guidelines.
RELEASED UNDER THE OFFICIAL
o There needs to be a degree of administrative infrastructure and a mandate to do this work,
which is currently done through professional networks. The Ministry also hopes for this
dialogue to occur. Initial policy conversations are occurring with Pharmac. Leadership and
administrative support would be needed from the Ministry, Pharmac and specialist bodies.
This wil be added to the Action Plan to work through.
• The Chair requested TAG members to take a deeper look at the shared documents and send
responses to TAG Secretariat.
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
• There was also an issue raised that the evidence-base for the recommendations for
vaccination in pregnancy had not been circulated to the primary health care services. To
be checked and actioned fol owing the meeting.
s 9(2)(f)(iv)
4.0
ACT 1982
5.0
Surveil ance Strategy Update
• An update about the surveil ance strategy was presented to TAG. The revised surveil ance
INFORMATION
strategy includes five main components 1. identify cases for public health management, 2.
evaluate the effectiveness of public health response 3, generate knowledge about disease
risks and patterns 4, monitor to ensure equity and 5. engender public and stakeholder
confidence and participation in the response. An additional component, ‘Identify and
monitor the conditions to enable reconnecting Aotearoa New Zealand’ is to be added. This
update outlined some of the planning around the intent to ful y review the strategy now,
noting several new additions since the previous strategy, but also to develop the review
into more of a rolling nature over six-week cycles. The team will circulate initial drafts for
TAG comment.
TAG feedback included:
• TAG members noted the changes and the approach. It was recommended that the
wording be updated so that each of the objectives are defined as an action.
6.0
Māori Health Perspectives
• No update given
7.0
Pacific Health Perspectives
• No update given
RELEASED UNDER THE OFFICIAL
8.0
Any Other Business
Recent COVID-19 exposure event in Wel ington
• An update on the outbreak case investigations underway in Wel ington was provided by
the Director of Public Health. At this stage all tests from contacts have returned as
negative. The case had been partly vaccinated and it has been confirmed that the SARS-
CoV-2 was the delta variant.
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 1
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL

Document 2
MINUTES: Technical Advisory Group COVID-19
Date:
Friday 23 July 2021
Time:
10.30 am – 12:00 pm
s 9(2)(k)
Location:
Chair:
Ian Town
Bryan Betty, Erasmus Smit, Michael Baker, Nigel French, Nigel Raymond, Sally
Members:
Roberts, Virginia Hope
ACT 1982
Ministry of Health Attendees:
Daniel Bernal, Sarah Mitchell
Guests:
James Harris; Richard Jaine, Susan Morpeth
Shanika Perera, Andi Shirtcliffe, Anja Werno, Collin Tukuitonga, Matire Harwood
Apologies:
Caroline McElnay, Emma Hickson, Jeremy Tuohy
INFORMATION
Welcome and Previous Minutes
1.0
Dr Ian Town welcomed all members, attendees, and guests in his capacity as Chair of the COVID-
19 Technical Advisory Group.
Minutes of the last meeting (25 June 2021) were accepted subject to the following corrections:
Item 3.0 There was also an issue raised that the evidence base for the recommendations for
vaccination in pregnancy had not been circulated to the primary health care services. there were no
references posted on the Ministry of Health website for positions taken such as the COVID-19
vaccine for pregnancy, and it was requested for references to be put on the website so there was
easy access clinicians. To be checked and actioned following the meeting.
Item 4.0 There was ongoing discussion about the vaccination settings and the epidemiological
behaviour of the virus, in particular the increased transmissibility of the Delta variant, which may
dictate what options are practical.
Ministry of Health Update on COVID-19 Response
2.0 RELEASED UNDER THE OFFICIAL
The Chair provided an update on the Ministry of Health COVID-19 Response. The topics included:
•
Quarantine Free Travel with Australia – announcement due today
•
On the topic of the process for Reconnecting Aotearoa New Zealand, the Ministry is
providing advice to DPMC in this space and the SPHAG is also advising the Government.
•
Saliva testing is now being rolled out for some of the border workforce, currently as an
evaluation pilot in Christchurch. Saliva testing may soon be an alternative option to
nasopharyngeal or combined oropharyngeal/ nasal swab tests for border workers.
TAG feedback included:
Document 2
•
There was a question about whether saliva testing is going to become mandatory, noting
that it seems very few people want to participate.
•
The Chair noted that there have been a range of issues with communications and
engagement with border workforce agencies and their unions, but this has improved since
the requirement for a nasal swab as well the saliva testing was removed.
Science Updates
3.0
Three COVID Science Updates (CSUs) were included with the agenda.
•
CSU 40 included the topics of additional doses of COVID-19 vaccine to improve vaccine
efficacy in people who are immunocompromised.
•
CSU 41 on fleeting contact stepwise explains the differences between Alpha and Delta
variants and delves into the idea of fleeting contact.
•
CSU 42 covers therapeutics that are available, or close to being available, for COVID-19,
1982
and categorises them into ‘likely to be beneficial, ‘showing promise’ or ‘unsupported by
current evidence’. The topic of therapeutics is one of the most common enquiries from the
ACT
public and others, so this CSU is helpful as a basis for a standard response.
TAG feedback included:
•
Having access to these Science Updates was welcomed
•
There are some RCTs of therapeutics (such as nafamostat) taking place in New Zealand
which should be kept on the radar
o
It was noted that the Science and Technical Advisory are evaluating a horizon scanning
INFORMATION
product from the UK on therapeutics. Will need to make sure New Zealand trials are
included and highlighted.
•
A question was raised about whether there is an active PHARMAC group looking at
therapeutics for approval.
o
The Chair noted that a therapeutics group is in the process of being established and will
OFFICIAL
probably be hosted by the Ministry with representation from PHARMAC and Medsafe.
•
There was a suggestion to change the settings on the COVID tracing app (currently thought
THE
to be set at 15 minutes) in light of the potential for shorter encounters to result in
transmission.
o To be actioned by STA
UNDER
Reconnect Aotearoa New Zealand (RANZ) Science Round-up 4
4.0
Details of the 4th RANZ Science Round-up were included with the agenda. Scientific confidence
about different sub-topic areas is increasingly shifting into ‘moderate’ and ‘high’ categories. It was
noted that the Science Round-up cycles into the fortnightly policy roundup, to help link the evidence
RELEASED
base for particular approaches they may be considering.
TAG feedback included:
• TAG feedback on the science round-up was generally positive noting that topics are usually
driven by requests for health advice.
Surveillance Strategy
5.0
A thorough review of the surveillance strategy has been completed and is now in the final stages of
editing. The intention is to review more frequently in the months ahead. This will likely involve a shift
Document 2
from the 6-monthly cycle to a 12-weekly cycle. TAG members were thanked for reviewing the
documents and providing detailed comments.
TAG feedback included:
•
Te Tiriti o Waitangi and equity should be separated as there is currently mixed messaging.
•
Refugees are a key group missing from this document.
•
Suggestions of an Australian academic/response advisor to critique the strategy.
Māori Health Perspectives
6.0
No update given
Pacific Health Perspectives
7.0
No update given
1982
Any Other Business
8.0
•
ACT
Previous TAG feedback regarding increasing mask wearing and scanning of QR codes was
relayed to senior officials and government. The Ministry have been asked to provide further
Alert Level advice.
•
There was a comment that we will need to revisit laboratory capacity, noting that the most
we could test during the August cluster was 25,000 a day and this was not sustainable.
o ESR to continue this discussion with Ministry of Health testing leads.
INFORMATION
•
TAG highlighted the need for a R&D strategy with potential for formal evaluation and review
to guide on improved use of resources in future
o
The Chair noted this is greatly needed. Some evaluations and small pilot studies
OFFICIAL
looking at implementation and grants from HRC have taken place, but a wider strategy
is lacking. There are conversations with the manager of Science and Insights as to how
this might develop. It was also noted that the funding of a long-term study on COVID-19
THE
outcomes will be announced soon.
o
Some data is being gathered through border worker testing, but this is more set up for
monitoring and compliance than for research.
UNDER
•
It was noted that ESR is working towards a generic HDEC in order to do more studies in
MIFs and MIQs, so that focused question amendments can be bolted on to the HDEC
approval
RELEASED
•
Feedback was relayed from the sector about the complexities of general practice getting
involved in the vaccine rollout, noting that now is a key time to seek to address these issues
if possible.
o
The Chair agreed that as vaccination of Group 4 gets underway, a wider engagement
of pharmacy and primary care teams will be needed. The CVIP team has oversight of
this.
Agenda Items for Next Meeting
9.0
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 4
MINUTES: COVID-19 Technical Advisory Group
Date:
Friday 12 November 2021
Time:
10.30 am – 12:00 pm
s 9(2)(k)
Location:
Chair:
Ian Town
1982
Anja Werno, Bryan Betty, Michael Baker, Nigel French, Nigel Raymond, Sally
Members:
Roberts, Shanika Perera, Virginia Hope
ACT
Ministry of Health Attendees:
Andi Shirtcliffe, Daniel Bernal, Jeremy Tuohy, Sarah Mitchell
Guests:
Steve Waldegrave
Collin Tukuitonga, Erasmus Smit, Matire Harwood, Caroline McElnay, Emma
Apologies:
Hickson
INFORMATION
Welcome and Previous Minutes
1.0
Dr Ian Town welcomed all members, attendees, and guests in his capacity as Chair of the COVID-
19 Technical Advisory Group.
OFFICIAL
Minutes of the last meeting (22 October 2021) were approved.
Ministry of Health Update on COVID-19 Response
2.0
THE
•
The Chair presented some slides using data and modelling for Auckland and Northland
•
Shows pattern of continued increase in cases at 150-200 daily. Includes assumptions
about protective vaccine effects as vaccine numbers increase by about 6000 per day
UNDER
•
With opening of retail, we may see cases climb further
•
With this outbreak, less cases have been progressing to ICU, possibly due to the younger
cohort and increased vaccination levels. The occupancy is still relatively low in Auckland
metro ICUs
•
The modelling includes some raw predictions around beds and ICUs
RELEASED
•
Noted that testing and contract tracing capacity are at breaking point, and a more risk-
based approach for these is needed
•
Community based care programmes and protocols are being developed using complex
algorithms and risk assessment.
TAG feedback included
•
In Auckland and Waikato, Public Health are stretched, with flow on effects to GPs.
Document 4
• There is an issue with lack of clarity regarding the risk vaccinated vs unvaccinated
patients pose to staff and other patients in primary care, and how masking affects this.
-
The Chair noted that a protocol on this topic for secondary care has just been
finished, and that this would be followed up for primary care
ACTION: confirm with the Chief Clinical Officer for Primary Care and COG that work is underway
to support this request for primary care.
• Raised concern about the vaccine exemptions and how it was announced - an
announcement was made, and then 3-4 weeks passed before there was a process in
place.
-
The Chair noted that the vaccine order has been re-written and the exemption
process posted. The new order is to be Gazetted on Monday.
• With regard to the PowerPoint slide shown, the projections look quite encouraging in
terms of the number of cases levelling off over time. However, it was questioned whether
1982
some factors had been considered, such as relaxation of restrictions around social
mixing, waning of immunity post-vaccination, and the impact of boosters.
ACT
-
The Chair noted these are complex interactions, and further input from TAG would be
welcome. Also noted that NZ data has informed some contract tracing decisions.
• There was a comment that it would now be a good time to socialise what endemicity
would mean for New Zealand. Even some health professionals are surprised to learn that
literally every person will have to encounter the virus at some point. This message needs
to be familiarised. We need awareness that this is something our immune systems will
need to see on a fairly regular basis.
INFORMATION
-
The Chair noted that this should be a key topic for the next TAG meeting to allow
time for more in-depth discussion.
• It was noted that other areas may be able to learn from Auckland’s experience. Several
anecdotes given in example of this.
OFFICIAL
Science Updates
3.0
Not discussed due to time constraints. Future science topic priorities for the Science and Technical
THE
Advisory will be discussed at a later meeting.
4.0
Protection Framework Processes
•
UNDER
An overview was given of the developing strategic thinking about how we take account of
the proposed traffic light system to make sure this works in the context of broader public
health measures.
• Key questions proposed and TAG input sought: when exactly the shift will occur (likely
early-mid December); how to protect the most vulnerable; how to keep the health system
sustainable; how boundaries should work; and how contact tracing, testing case
RELEASED
management and isolation should be managed.
• A key question is how vulnerability should be defined and how vulnerable communities
should be protected as the virus spreads. The Ministry of Health suggests a composite of
indicators that balance vaccination, access to healthcare, deprivation, age profile – and to
not just rely on the traffic light system.
TAG Feedback included:
• The benefits of limiting infection should not be underestimated. For example, the impact of
long COVID is a big unknown that could profoundly alter the risk equation
Document 4
• Some were very concerned about the prospect of opening Auckland soon and emphasised
the benefits of delaying the spread of SARS-CoV-2, especially to more vulnerable areas.
-
The Ministry of Health is also concerned about Aucklanders travelling, and is advising
strongly on the need to protect more vulnerable communities.
• The need to retain the ability to enact measures above and beyond the red level, such as
lockdowns, was emphasised
-
The group was reassured that the Ministry of Health is putting forward strong advice
about the importance of being able to move to lockdowns if necessary.
• The new system should take account of likely future events, such as flu season next
winter, as well as a legacy point of view
• Therapeutics in hospital appear moderately good at preventing people needing ICU. In the
community however, therapeutics are likely to have a more modest effect, at least in the
short term (due to factors such as price, likely small deliveries, and difficulties getting the
1982
treatment to people).
• There was a recommendation to make the need to minimise harm across the system more
ACT
central to the strategy (more than just reducing hospitalisations associated with COVID-
19), and the community sector should be better represented.
• One option to alleviate the pressure on primary care could be to have COVID-19 specific
treatment centres available in the community, where people who don't require
hospitalisation, but may only require 24-48 hours of close observation, can be looked after.
• There was feedback that when strategy is being developed, it needs to be better
connected to operational planning and the reality of services on the ground. Before a
INFORMATION
change to a whole new system and opening of borders, there is a need to lock in some of
this operational planning.
-
The Ministry of Health is unable to influence the decision to open before Christmas,
so the focus is on trying to prepare to minimise potential harm. It was acknowledged
OFFICIAL
that strategy in isolation from operations is not meaningful. Guidance is needed from
the government on targets, definition of vulnerability, etc, and then it will be essential
to ensure that connections with key people locally are being made to enable
THE
community level planning
• There is some evidence that vaccination rates pick up as COVID-19 becomes a more
tangible threat to communities
UNDER
-
There is some complexity around this, for example in Northland there was a jump in
vaccinations originally but this dropped off second time around. This may particularly
occur in communities that have a deep distrust of government
• There would need to be thought about how geographically adjacent areas would work
together when at different colours (e.g. with workforces across areas)
•
RELEASED
Managing demand of testing will be critical going forward. We are currently over-testing
and should think about focusing on really important areas that give best value for money
and allow the system to operate speedily
-
It was agreed that there is a need to focus resources tightly and this work is
underway
• It was noted that there is a lag between the number of cases and the impact on
hospitalisations and deaths. It would not be wise to just wait until we are at crisis point
before moving to lockdowns – has thought been given to the triggers that should be used
to determine moving to stronger measures?
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 4
before publishing on Ministry
website.
confirm with the Chief
Ministry of Health
Clinical Officer for Primary
77 Update on COVID-19
Care and COG that work is
STA
12/11 – Action raised
Response
underway to support this
request for primary care.
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 5
MINUTES: COVID-19 Technical Advisory Group
Date:
Friday 10 December 2021
Time:
10.30 am – 12:00 pm
s 9(2)(k)
Location:
Chair:
Ian Town
1982
Anja Werno, Bryan Betty, Erasmus Smit, Matire Harwood, Michael Baker, Nigel
Members:
French, Nigel Raymond, Sally Roberts, Shanika Perera
ACT
Andi Shirtcliffe, Caroline McElnay, Daniel Bernal Emma Hickson, Jeremy Tuohy,
Ministry of Health Attendees:
Sarah Mitchell
Guests:
Steve Waldegrave
Apologies:
Collin Tukuitonga, Virginia Hope
INFORMATION
Welcome and Previous Minutes
1.0
Dr Ian Town welcomed all members, attendees, and guests in his capacity as Chair of the COVID-
19 Technical Advisory Group.
OFFICIAL
Minutes of the last meeting (12 November 2021) were approved.
Ministry of Health Update on COVID-19 Response
THE
2.0
The Chair and the Director of Public Health gave an update on the COVID-19 Response:
•
The national management of COVID continues to evolve rapidly, particularly in relation to
reconnecting New Zealand.
UNDER
•
The R value is currently below one, and community transmission in Auckland is stable or
decreasing. However, some communities such as Māori and Pacific and those in
extended households have continued to experience higher rates of disease than other
communities. Waikato cases have seeded from Auckland connections. Cases outside
Auckland are usually connected and have been able to be contained.
•
RELEASED
We have seen benefits of a highly vaccinated population and good contact tracing
responses. However, there are some populations who are not highly vaccinated. Māori
vaccination rates are rising.
•
The programme for care of COVID in the community has been implemented extremely
quickly. It is a major change shifting the emphasis from MIQ to home isolation and
management. It has been noted that this adds a large burden on primary care. There have
been some communication issues, and instances of people not getting the care they need
promptly. MSD will be assisting with the community programme to help with support to
Document 5
families isolating at home, including provision of advice, food, and access to other
services.
• There is a lot at stake with the community programme – Auckland has thousands of people
monitoring at home. Additional call centres have been set up to ensure regular checks and
that action is taken in a timely way when needed.
• An audit of the first 35 COVID patients being managed in primary care has been
undertaken. The majority were unvaccinated and had multiple generations living at home,
so the infection spread quickly. Those who were vaccinated had less severe disease and
didn’t require hospitalisation. There was less spread into households where cases or
contacts were vaccinated. Oximeters were difficult to obtain, but some were donated.
Supporting patients through primary care felt manageable and it was seen as positive to
be able to provide wrap around care and check in with patients.
• There has been a strong push for first and second vaccination doses to be administered to
1982
people who may not have had access at a suitable vaccination site. Equity leads at the
Ministry have made significant progress specially to ensure that funding is flowing to
providers.
ACT
• There have been worrying reports of individual medical practitioners issuing fake/
unfounded vaccine exemptions. The Medical Council and Police are investigating these
reports.
• The Ministry is still working through residual high court procedures addressing opposition
to the use of the vaccine. The STA team is supporting these proceedings through detailed
affidavits.
TAG feedback included:
INFORMATION
• Concern was raised about the emergence of the Omicron variant, and initial evidence
about immune escape. The current evidence is limited. However, booster doses will likely
be necessary to provide good protection.
• The successful transition to the traffic light system was noted
OFFICIAL
• The scope of the traffic light system seems quite limited in terms of advice about indoor
environments it covers. For example, holiday accommodation (and temporary
THE
accommodation in general) is not covered. This could be a real issue over summer. The
Alert Levels covered all transmission settings.
• With the Auckland boundary about to open, it would be helpful to have more detailed
guidance available to enable people to stay safe while travelling.
UNDER
• Rapid Antigen Tests are becoming available, though they have questionable performance
compared with PCR. It was suggested that RATs should be available for testing children
under 12 tested before visiting vulnerable relatives.
• It was noted that one of the most vulnerable populations are people with alcohol and drug
dependency. Their vaccination rates are lower than for Māori, but there is no explicit
RELEASED
strategy for them. This is an extremely difficult group to reach, and they don’t have a
strong voice.
-
The Chair noted that most of these issues have been raised, and the vaccine program
has several strategies around using tailored efforts to engage with those yet to be
vaccinated.
• A question was raised about whether work has been done to predict the speed of spread
to areas of low vaccination.
Document 5
• A question was raised about whether there have been thoughts to remove the term ‘HIS
criteria’ from the nomenclature – it has implications for high-risk patients and PPE
requirements. Primary care is still awaiting PPE advice for vaccinated vs unvaccinated
patients, and what the approach to children should be as COVID becomes more widespread.
Advice is not clear on these issues and should consider the many types of GP set ups.
The Chair agreed that vaccination reach and coverage has exceeded expectations. There is
now a big push to schedule boosters and catch up on other vaccines, especially measles.
• COVID-19 therapeutics seem moderately effective in hospital but not so useful in the
community.
Science Updates
3.0
• The emergence of Omicron is concerning, and the Ministry is closely following
developments.
1982
• Four papers about neutralisation studies have been published.
• Vaccine escape is a theoretical concern. Neutralisation studies give some indication of
ACT
potential risk, but performance of the vaccine in the real world, even against Delta, has
been better than predicted. T cell immunity also helps to protect against severe disease.
• Health risk assessments are being carried out to consider what measures need to be in
place. Recent advice given by the Ministry is to reduce the number of countries designated
as very high risk (currently 9 southern African countries), and to consider shortening pre-
departure testing timeframes to within 48 hours of travel for PCR and within 24 hours for
RAT. This is considering the apparent increased transmissibility of Omicron.
INFORMATION
• New Zealand is fortunate to still have MIQ in place. However, it is anticipated that
Omicron will reach New Zealand from a country that has not been designated very high
risk, so the advice has been to take a more universal approach and make sure MIQ
facilities are completely on point with protocols.
TAG feedback included:
OFFICIAL
• Agreement that it is a relief we still have functioning border controls. A question was raised
about whether Omicron would alter plans to relax border controls early next year which are
THE
unlikely to be compatible with prevention of community transmission of Omicron.
• If travel volumes are small, preventing the arrival of Omicron into the community should be
manageable, but if they are large, then any variant is likely to arrive. Therefore, should the
policy of home isolation may need to be be reconsidered.
UNDER
-
The Chair noted that the Reconnecting Aotearoa New Zealand work is impacted by
concerns about Omicron. There are unlikely to be decisions until the New Year, as
successful implementation of the Protection Framework and preparing for summer in
the sector will be top priorities. Parliament stops sitting at the end of next week.
• Further assessments will be undertaken next week about what other factors need to be
RELEASED
considered for RNZ, especially with Australia, which is the first link due to happen. An
update on testing was given. Omicron has two lineages: BA.1 and BA.2. Australia has
been trying to identify new community infections very quickly by looking for the S gene
target dropout. However, not all Omicron variants have this deletion.
• A key factor determining vaccine effectiveness is time since vaccination. New Zealand
currently has a well-protected population. Current evidence indicates that Omicron has
significant vaccine escape compared to previous variants. In association with waning
vaccine immunity, the proportion of individuals susceptible to Omicron by winter could be
very high in the absence of either natural infection or further vaccination
Document 5
• A statement from a German expert indicates they are very worried, and notes without
exposure to the virus you lose the opportunity for natural boosting and generating
immunity to multiple antigens. If we want the virus to become endemic, we need to be
exposed to it.
-
The Chair commented that the case for allowing widespread exposure has been made
by a few experts based on the assumption that the disease will be mild, and the
community will rapidly develop natural immunity.
• The importance of getting rapid genome sequencing of all cases in MIQ to detect new
variants arriving at the border was emphasised. All recent cases in MIQ have been Delta,
which is encouraging.
-
It was questioned whether MIQs could be used for people with mild disease but high
risk of deteriorating, or those who for social reasons we aren’t sure they can be
monitored safely.
1982
-
It was noted that the experience of trying to get extra healthcare interventions into
MIQs has been difficult, and so this would not be an option.
ACT
What Endemicity Would Mean for New Zealand
4.0
The Chair gave some opening statements for this topic:
• There are important differences between elimination and tight suppression, and how these
play out in a highly vaccinated population. We haven’t seen the explosive outbreaks we
might have feared in pre-vaccine area.
• We are heading towards new territory every day and needing to keep ahead of the
INFORMATION
science. It was noted that politicians have repeatedly made decisions that are even more
cautious than Ministry advice, and it seems likely they will continue with tight suppression if
possible.
TAG feedback included:
• The best approach is a significant source of debate.
OFFICIAL
• Thus far, countries that have taken a precautionary approach, such as New Zealand, have
been very successful.
THE
• Some TAG members felt we should avoid SARS-CoV-2 circulating widely now, and noted
a relevant editorial in the NZMJ.
• However, on the other hand it is possible that allowing the virus to circulate could be the
UNDER
best biological way of managing it. However, some felt there was significant uncertainty
associated with this idea.
• The biggest gap in our knowledge is with long COVID. Even if 1-2% of cases have ongoing
health impacts, we would be more inclined to want to eliminate the virus.
• Some TAG members felt we do not have enough knowledge to identify an optimal strategy
RELEASED
and the cautious approach is still preferable.
•
COVID-19 Protection Framework
5.0
TAG members were thanked for their extremely helpful advice this year, and an overview of the
COVID-19 Protection Framework (CPF) and processes was given:
• The Government’s strategy with the CPF is based on high levels of vaccination, and the
premise that the vaccine will reduce transmission and severity of illness.
Document 5
• The CPF itself is not the full spectrum of measures we had with the alert levels. It stops at
about the equivalent of alert level 2.5.
• The overarching objective is to minimise hospitalisations and deaths. Important facets of
this include suppressing SARS-CoV-2 spread, protecting the health system, protecting at-
risk communities, and continuing non-COVID healthcare.
• The Ministry of Health’s COVID-19 Protection Framework Assessment Committee meets
fortnightly to advise on traffic light settings. The Assessment Committee includes members
with not only medical and virological expertise, but also significant knowledge about the
communities involved, which enriches the assessment.
• DHB representatives also attended the second assessment, which provided additional
detail about what is going on across regions.
• The CPF focuses on whether the health system can cope rather than eliminate the virus. A
range of measures have been incorporated into a table to aid assessment.
1982
• The outcomes of the first and second traffic light assessments by the CPF Assessment
Committee were similar. The Government chose an even more cautious approach.
ACT
• Considerations when recommending ‘colours’ for regions include vaccination rates overall,
and for Māori in particular; self-assessments by DHBS; location of cases and current
setting; suggested colour if all things were rated equal; suggested colour given specific
contexts, e.g., the Auckland boundary about to open and upcoming significant changes in
terms of travel. All factors are put together to provide a basis for robust discussion.
• The CPF does not exclude the possibility that localised lockdowns may still be required but
there would be a very high bar to do so (e.g., if there are very high hospitalisations and/or
INFORMATION
deaths, or if it becomes evident that Omicron causes very severe disease as well as being
very transmissible). This is unlikely to happen over the holiday period, but the tools are
there if needed.
• The aim is to improve the methodology of assessments over time. The first assessment
used lag rather than lead indicators and did not have as much quality control due to time
OFFICIAL
constraints. The second assessment introduced the notion of lead indicators e.g., housing
disadvantage, and case numbers could be predicting hospitalisations and deaths. It was
THE
informed by DHBs providing a richer set of information, with lots more background on how
they were feeling.
• A CPF Expert Assurance Group (CPF EAG) has been set up to ensure the methodology
used by the CPF Assessment Committee is more robust and repeatable. They will meet
UNDER
every 6-7 weeks.
• It was noted that Cabinet wanted advice on a regional basis but did not specify how this
should be defined. Various parts of Government use different boundaries (e.g., DHBs vs
territorial authorities, etc). For the assessment, the aim is to investigate more granular
levels of data (at least territorial authorities) because there is variation at local levels that
may not be obvious at regional levels.
RELEASED
TAG feedback included:
• The traffic light system is narrow scope in terms of indoor environments e.g., it does not
cover temporary accommodation and holiday motorhome parks. Is there a plan to expand
scope?
• It was noted that the CPF itself is owned by DPMC, and the Ministry of Health provide
public health advice. The Ministry has been working closely with DPMC to help clarify
some of the detail. A review of the performance of the CPF has been initiated, but it is
unlikely to provide feedback before the summer holidays Feedback from TAG can be sent
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 6
MINUTES: COVID-19 Technical Advisory Group
Date:
Friday 10 February 2023
Time:
10.30 am – 12:00 pm
s 9(2)(k)
Location:
Chair:
Nicholas Jones
1982
Members:
Anja Werno, Bryan Betty, Erasmus Smit, Michael Baker, Michel e Balm, Nigel
Raymond, Sally Roberts, Virginia Hope
ACT
Ministry of Health Attendees: Andi Shirtcliffe, Brooke Hollingshead, Chris Hedlund, Jane Pryer, Jeremy Tuohy,
Kirsten Beynon, Pete Hanl,
Guests:
Stephen Glover, Carolyn Clissold, Antoinette Righarts
Nigel French, Col in Tukuitonga, Matire Harwood, Shanika Perera, Peter
Apologies:
Abernethy, Fiona Cal aghan, Shama Kukkady
INFORMATION
1.
Welcome and Accept Previous Minutes
Dr Nicholas Jones welcomed al members, attendees, and guests in his capacity as Chair
of the COVID-19 Technical Advisory Group (COVID-19 TAG).
OFFICIAL
The minutes of the last meeting (Friday 2 December 2022) were accepted.
THE
2.
Trends and Insights
Infection cases were less than expected in model ing.
Variants of Concern
UNDER
A link to the latest SARS-CoV-2 Variants of Concern (VoC) on the Ministry’s website was shared prior
to the meeting. While the variants in circulation have not changed substantial y, the expected rise in
XBB.1.5 has not materialised yet.
Feedback from members included:
•
The lack of a single global y dominant variant and differences in circulating
variants i
RELEASED n other countries result in a more complex situation. However, unless
one variant takes over (like Omicron did), the differences between emerging and
converging mutations are not significant enough to deviate resources from other
important issues such as antimicrobial resistance (AMR) and invasive Group A
streptococcus (IGAS).
3.
PHRA update
The Chair informed the TAG that the Public Health Risk Assessment committee discussed the
opening of Chinese borders alongside the transition away from their elimination policy. It was
decided that instead of requiring pre-departure test from only one specific country, passengers
Document 6
are asked to test voluntarily upon arrival.
Point of care testing order, case isolation and face mask use were discussed, and all three
requirements were recommended to be kept in place.
The current risk is considered to be low and expected to remain low for the next two months.
However, there is no standard way of describing risk at the moment.
Feedback from members included:
• Since the Chinese population is relative naive, it is not expected that new variants will
emerge during the first wave.
POCT order:
• How long wil regulatory function be retained? How wil significant stock of testing kits
in NZ be managed?
1982
• Current order only covers COVID-19 tests, however, multiplex devices testing for
influenza and RSV should also be considered (triple target space for it in primary
care).
ACT
Case isolation:
• How will asymptomatic people or people who might not self-test to avoid self-isolation
be accounted for?
• Can isolation period be safely reduced from 7 to 5 days? A more realistic/pragmatic
approach needs to consider people who are asymptomatic or do not test/report to
avoid isolation
• What would the provisions look like when isolation is no longer mandatory and what
INFORMATION
impacts wil this have on financial aid.
Face mask:
• Several members commented on issues arising from the fact that the current mask
mandate applies to visitors only, not for patients in health settings.
• Distinction between visitors and patients can lead
OFFICIAL to tensions, especialy in settings
such as pharmacies, hospitals and primary care. Therefore, in general practice the
effect of the existing mandate is to result in everyone being required to wear a mask.
THE
• Can the mandate for visitors be reviewed? The mandate is often not being applied
well, and visitors remove masks as soon as they enter the patient’s room.
• Can there be more flexibility for health care workers (HCW) by moving away from a
general recommendation to the individual’s responsibility to assess the situation? It
was stated that HCW ar
UNDER e already making their own decisions regarding mask use.
• Feedback from HCW on recommendations to wear masks included:
o that the risk is perceived as being low and
o mask use can negatively impact on communication (such as the doctor-
patient relationship or communication with children, elderly, or patients with
mental health issues)
• Communication regarding mask use needs to be clearer, and balancing the pros and
RELEASED
cons of mask use need to be considered
• While some organisations/institutions in health care settings want to set up their own
rules, others prefer the government to provide guidance which makes it easier to
impose.
• Nosocomial rate of COVID-19 infections, such as how many people come up with
COVID-19 on day 6 after hospital admission to hospital, would be helpful to inform
decisions on mask use. However, finding the source of infection (visitor, staff, other
patients) is not available and data extremely hard to obtain.
• It needs to be acknowledged that mask use is a complex matter and whatever
Document 6
outcome a revision wil bring, there wil be people vocally expressing their
concerns/non-approval in response to it.
ACTION:
• Hospitalisation rates based on ethnicity (JT wil ask Sidd Mehta)
• Delay between admission and diagnosis of COVID (JT to ask Antoinette)
• IPC guidelines should be tied in the review of the next risk assessment (Michelle)
4. Future of COVID-19 TAG and Terms of Reference
The Chair informed members that before continuing with the discussions of the future of
the COVID-19 TAG, the Public Health Agency (PHA) Deputy Director-General is
considering the needs for a Technical Advisory Group for the PHA more general y,
particularly focusing on communicable and infectious diseases.
1982
5. Policy choices for the ongoing management of COVID-19
ACT
The COVID-19 Policy group manager presented the current strategic approach and
choices for the ongoing management of COVID-19 which wil be presented to Cabinet in
April 2023. The management wil shift from an all-of-government response to increasingly
considering COVID-19 alongside other health issues. This coincides with the decision to
longer have a separate ministerial portfolio for COVID-19.
The strategic framework wil be revisited to provide a clear narrative of how COVID-19 wil
be managed. Preparedness, protection, resilience and stability wil be broad principles of
the overarching strategy to ensure equitable outcomes, protect those most at ris
INFORMATION k and
manage pressures on health system, so that al parts of the system can continue to
operate effectively.
The three key measures will be:
• Vaccination: actively encouraging people to stay up to date
OFFICIAL
• Antivirals: broad eligibility criteria to reduce serious outcomes when people are
infected and to reduce the number of hospital admissions
THE
• Case isolation
Feedback from the members:
UNDER
• The upcoming change in COVID-19 funding for GPs and primary should be
monitored careful y. This change wil result in reverting a currently very proactive
system to a reactive system where the onus is completely on the patient to initiate
contact.
• To avoid singular thinking, the changes should reflect systemwide interconnection
and allow for lateral thinking. s 9(2)(g)(i)
RELEASED
• The role of antivirals should be considered careful y when planning making
access to antivirals as broad as possible. Generally, vaccines are more effective
than antivirals and the focus should remain on vaccines. A large UK study among
25,000 people of moderate risk shows that antivirals did not alter hospitalisation
number, however, they shortened the period of viral shedding and reduced some
symptoms.
•
Ideally other infectious diseases would be treated more like COVID-19 instead of
Document 6
treating COVID-19 like other infectious diseases. Finding a middle ground would
improve the default options applied to other respiratory pathogens.
•
One member suggested that although vaccines and antivirals can help minimise
the consequences of infection, the strategy should still aim at minimising infections.
This raises the questions whether transmission should be key objective (reduce
population transmission vs transmission of the more vulnerable population)
•
Surveillance systems should provide integrated information on disease burden,
equity of access and use of interventions. Sentinel sites could help provide high
quality information.
•
The COVID-19 strategy needs to link back to the nationwide immunisation
strategy. This is an opportunity to focus more heavily on other vaccine preventable
diseases to make the space future proof.
•
Access to PCR test for elderly people is retained (RATs can provide false negative
results if not used correctly).
1982
•
Preparedness should involve having good IPC teams in the centre and the regions
(where not in place at beginning of COVID-19)
ACT
6.
Reinfection evidence update
A representative from the Science and Technical Advisory team provided updated
information regarding the risks of reinfection.
The risk of serious outcomes is decreased in people who have had a previous infection,
but protection is greater if an individual has been vaccinated and has experienced
INFORMATION
previous infection (hybrid immunity).
Severe outcomes wil continue to occur in those with multiple comorbidities.
OFFICIAL
7.
Patient care guidelines from WHO
While WHO continues to strongly recommends mask use in community settings in high-
THE
risk situations, recommendations regarding case isolation have been updated: people who
are asymptomatic should isolate for 5 days, those with symptoms should isolate for a
maximum of 10 days with RATs used to reduce the period of isolation.
Feedback from members included:
UNDER
•
Since RATs have proven to be more predictive of infectivity than symptoms, de-
emphasising symptoms and testing to release makes sense. However, the current
New Zealand system of 7 days is simple and allows communication to be clear
and less confusing.
•
If the current New Zealand isolation requirements are to change, clarity of the
message i
RELEASED s important.
•
Limited evidence on pre-symptomatic, asymptomatic or non-compliant
transmission makes it hard to determine how effective isolation of compliant
symptomatic individuals alone is in the reduction of transmission.
•
Transmission risk is dynamic, i.e., with low incidence of infection in community,
some places as general practice waiting rooms might not be places of high risk.
•
People infected with COVID-19 should not be pushed to return to work despite
strained work force coverage.
Updated IPC guideline
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED