Final report AO-2013-010: Aérospatiale AS350B2 ‘Squirrel’, ZK-IMJ,
collision with parked helicopter, near Mount Tyndall, Otago, 28 October 2013
The Transport Accident Investigation Commission is an independent Crown entity established to
determine the circumstances and causes of accidents and incidents with a view to avoiding similar
occurrences in the future. Accordingly it is inappropriate that reports should be used to assign fault or
blame or determine liability, since neither the investigation nor the reporting process has been
undertaken for that purpose.
The Commission may make recommendations to improve transport safety. The cost of implementing
any recommendation must always be balanced against its benefits. Such analysis is a matter for the
regulator and the industry.
These reports may be reprinted in whole or in part without charge, providing acknowledgement is made
to the Transport Accident Investigation Commission.

Final Report
Aviation inquiry AO-2013-010
Aérospatiale AS350B2 ‘Squirrel’, ZK-IMJ,
collision with parked helicopter
near Mount Tyndall, Otago
28 October 2013
Approved for publication: June 2017
Transport Accident Investigation Commission
About the Transport Accident Investigation Commission
The Transport Accident Investigation Commission (Commission) is a standing commission of inquiry and
an independent Crown entity. It is responsible for inquiring into maritime, aviation and rail accidents
and incidents for New Zealand, and co-ordinating and co-operating with other accident investigation
organisations overseas. The principal purpose of its inquiries is to determine the circumstances and
causes of the occurrences with a view to avoiding similar occurrences in the future. Its purpose is not to
ascribe blame to any person or agency or to pursue (or to assist an agency to pursue) criminal, civil or
regulatory action against a person or agency. The Commission carries out its purpose by informing
members of the transport sector and the public, both domestically and internationally, of the lessons
that can be learnt from transport accidents and incidents.
Commissioners
Chief Commissioner
Jane Meares
Deputy Chief Commissioner
Peter McKenzie, QC
Commissioner
Stephen Davies Howard
Commissioner
Richard Marchant
Commissioner
Paula Rose (from May 2017)
Key Commission personnel
Chief Executive
Lois Hutchinson
Chief Investigator of Accidents
Captain Tim Burfoot
Investigator in Charge
Peter R Williams
General Manager Legal & Business Services
Cathryn Bridge
Email
[TAIC request email]
Web
www.taic.org.nz
Telephone
+ 64 4 473 3112 (24 hrs) or 0800 188 926
Fax
+ 64 4 499 1510
Address
Level 11, 114 The Terrace, PO Box 10 323, Wellington 6143, New Zealand
Important notes
Nature of the final report
This final report has not been prepared for the purpose of supporting any criminal, civil or regulatory
action against any person or agency. The Transport Accident Investigation Commission Act 1990
makes this final report inadmissible as evidence in any proceedings with the exception of a Coroner’s
inquest.
Ownership of report
This report remains the intellectual property of the Transport Accident Investigation Commission.
This report may be reprinted in whole or in part without charge, provided that acknowledgement is
made to the Transport Accident Investigation Commission.
Citations and referencing
Information derived from interviews during the Commission’s inquiry into the occurrence is not cited in
this final report. Documents that would normally be accessible to industry participants only and not
discoverable under the Official Information Act 1982 have been referenced as footnotes only. Other
documents referred to during the Commission’s inquiry that are publicly available are cited.
Photographs, diagrams, pictures
Unless otherwise specified, photographs, diagrams and pictures included in this final report are
provided by, and owned by, the Commission.
Verbal probability expressions
The expressions listed in the following table are used in this report to describe the degree of probability
(or likelihood) that an event happened or a condition existed in support of a hypothesis.
Terminology
Likelihood of the
Equivalent terms
occurrence/outcome
(Adopted from the Intergovernmental
Panel on Climate Change)
Virtually certain
> 99% probability of occurrence
Almost certain
Very likely
> 90% probability
Highly likely, very probable
Likely
> 66% probability
Probable
About as likely as not
33% to 66% probability
More or less likely
Unlikely
< 33% probability
Improbable
Very unlikely
< 10% probability
Highly unlikely
Exceptionally unlikely
< 1% probability

The accident scene, with ZK-IMJ in the foreground and ZK-HAE in the background
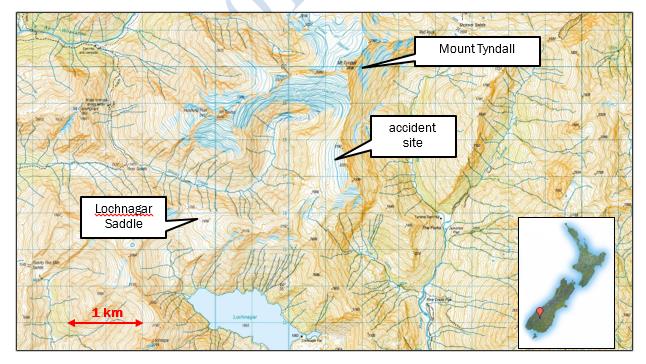
Location of the accident
link to page 10 link to page 11 link to page 12 link to page 13 link to page 14 link to page 15 link to page 15 link to page 17 link to page 17 link to page 18 link to page 19 link to page 20 link to page 20 link to page 21 link to page 22 link to page 22 link to page 23 link to page 24 link to page 25 link to page 25 link to page 25 link to page 27 link to page 27 link to page 27 link to page 28 link to page 28 link to page 29 link to page 30 link to page 30 link to page 31 link to page 32 link to page 33 link to page 33 link to page 34 link to page 35 link to page 36 link to page 36 link to page 36 link to page 36 link to page 37
Contents
Abbreviations ..................................................................................................................................................... ii
Glossary ............................................................................................................................................................ iii
Data summary .................................................................................................................................................. iv
1. Executive summary ................................................................................................................................... 1
2. Conduct of the inquiry ............................................................................................................................... 2
3. Factual information ................................................................................................................................... 3
3.1.
Narrative .................................................................................................................................... 3
3.2.
Injuries to persons .................................................................................................................... 5
3.3.
Damage to aircraft .................................................................................................................... 5
3.4.
Personnel information .............................................................................................................. 6
3.5.
Aircraft information ................................................................................................................... 7
Weight and balance .................................................................................................................. 8
3.6.
Meteorological information ...................................................................................................... 8
3.7.
Wreckage and impact information ........................................................................................... 9
3.8.
Medical and pathological information .................................................................................. 10
3.9.
Survival aspects ..................................................................................................................... 10
3.10.
Organisational and management information ..................................................................... 11
3.11.
Other occurrence.................................................................................................................... 12
4. Analysis ................................................................................................................................................... 13
4.1.
Introduction ............................................................................................................................ 13
4.2.
The possibility of the pilot misjudging the separation ......................................................... 13
4.3.
The possibility of a loss of visual reference .......................................................................... 15
First approach ........................................................................................................................ 15
Second approach ................................................................................................................... 15
4.4.
The possibility of a loss of control ......................................................................................... 16
Helicopter defect .................................................................................................................... 16
Performance limit ................................................................................................................... 17
4.5.
The possibility of a medical or psychological condition ....................................................... 18
Medical condition ................................................................................................................... 18
Potential psychological condition .......................................................................................... 19
4.6.
Summary of potential causes ................................................................................................ 20
5. Safety issues .......................................................................................................................................... 21
Flight-following ....................................................................................................................... 21
Disembarking while rotors are turning ................................................................................. 22
6. Findings .................................................................................................................................................. 23
7. Safety actions ......................................................................................................................................... 24
General ................................................................................................................................................ 24
Safety actions addressing safety issues identified during an inquiry ................................................. 24
Safety actions addressing other safety issues ..................................................................................... 24
8. Recommendation ................................................................................................................................... 25
link to page 37 link to page 37 link to page 38 link to page 39 link to page 40 link to page 41 link to page 41
General ................................................................................................................................................ 25
Recommendation ................................................................................................................................... 25
9. Key lessons ............................................................................................................................................. 26
10. Citations .................................................................................................................................................. 27
Appendix 1: Weight and balance calculation ............................................................................................... 28
Appendix 2: Ironic processes of mental control – Key points from research on unwanted outcomes .... 29
References.............................................................................................................................................. 29
link to page 16 link to page 17 link to page 18
Figures
Figure 1
The parked helicopter as seen on the go-around from first approach .............................. 4
Figure 2
The helicopter after the accident (with de-fuelling kit alongside) ...................................... 5
Figure 3
Typical damage to the main rotor blades of the parked helicopter ................................... 6
Final Report AO-2013-010 | Page i
Abbreviations
CAA
Civil Aviation Authority of New Zealand
Commission
Transport Accident Investigation Commission
ELT
emergency locator transmitter
kg
kilogram(s)
m
metre(s)
the pilot
the pilot of ZK-IMJ, which collided with the parked helicopter
the senior pilot
the pilot of ZK-HAE, the parked helicopter
Page ii | Final Report AO-2013-010
Glossary
airworthiness directive a mandatory instruction, issued by the CAA, to ensure the continued
airworthiness of an aircraft or component
blowing snow
loose snow present after fresh snow has fallen, especially if the temperatures
are cold and the snow has not yet bonded. Loose snow obscures ground
references when rotors are in ground effect (see below)
bright-out
a phenomenon caused by excessive reflection of sunlight off the snow surface,
resulting in a lack of depth perception, most common when the sun is high in
the sky and the snow is fresh
centre of gravity
the single point in an object through which the weight (force of gravity) acts
collective lever
the control that changes the pitch angle of a helicopter’s main rotor blades by
the same amount and at the same time, which changes the total rotor thrust,
usually to effect a climb or descent
cyclic stick
the control that changes the pitch angle of a helicopter’s main rotor blades at
the same point of their rotation cycle, which causes the rotor disc (see below)
to tilt in the direction in which the pilot has put the stick. The helicopter then
moves in that direction
elevation
height above mean sea level
flare
to apply aft cyclic, which produces a rearward rotor thrust component that
slows a helicopter
flight-following
the process of maintaining awareness of an aircraft’s position and intentions so
that a timely response can be made in the event of an incident or the aircraft
being overdue
go-around
to discontinue a landing approach and re-circuit for another attempt
ground effect
a helicopter is ‘in ground effect’ when the downwash from the main rotor
strikes the surface and generates an increase in pressure, which effectively
creates a cushion of air that reduces the power required to hover. The effect
reduces as the helicopter moves away from the surface, with the result that
more power is required. At a height equivalent to approximately half of the
rotor diameter, there is little effect and the helicopter is then ‘out of ground
effect’
Mayday
the internationally recognised signal sent by an aircraft or vessel that is in
distress and needs immediate assistance. The call includes the aircraft
identification, its location and the assistance required
rotor disc
the area swept by a helicopter’s rotor blades each revolution
Final Report AO-2013-010 | Page iii
Data summary
Aircraft particulars
Aircraft registration:
ZK-IMJ
Type and serial number:
Aérospatiale AS350B2, 9057
Number and type of engines:
one Turbomeca ‘Arriel’ 1D1 turbo-shaft
Year of manufacture:
2002
Operator:
The Helicopter Line Limited
Type of flight:
air transport – scenic
Persons on board:
seven
Pilot’s licence:
commercial pilot licence (helicopter)
Pilot’s age:
52
Pilot’s flying experience:
7,327 flight hours total, 1,454 hours on helicopters, of
which 465 hours were on the Aérospatiale AS350
Date and time
28 October 2013, 15081
Location
near Mount Tyndall, Otago
latitude:
44°33.1´ south
longitude: 168° 37.9´ east
Injuries
one serious, six minor
Damage
destroyed
1 Times in this report are New Zealand Daylight Time (universal co-ordinated time + 13 hours) and expressed in the
24-hour format.
Page iv | Final Report AO-2013-010
1.
Executive summary
1.1.
On 28 October 2013 a party of 12 tourists was taken in two AS350 Squirrel helicopters
operated by The Helicopter Line from Queenstown aerodrome to a snowfield approximately two
kilometres southeast of Mount Tyndall in Otago province. The first helicopter landed. The
second helicopter was about to land but the pilot carried out a go-around. During the go-around
the helicopter came close to colliding with the main rotors of the parked helicopter.
1.2.
On the second approach the helicopter drifted towards the parked helicopter and its tail
contacted the main rotor blades of the parked helicopter. The blades severed the lower vertical
stabiliser and part of the tail rotor of the airborne helicopter. The rest of the tail rotor assembly
and vertical stabiliser detached immediately.
1.3.
The helicopter was uncontrollable without the tail rotor assembly. It spun rapidly a number of
times before climbing slightly then crashing about 70 metres in front of the parked helicopter.
The pilot received a serious injury and all of his passengers received minor injuries.
1.4.
The Transport Accident Investigation Commission (Commission) found that blowing snow very
likely contributed to the near collision during the go-around, but it was unable to determine the
cause of the collision. The Commission made findings that excluded technical, helicopter
performance and other environmental factors as causes of the collision. The possibility that the
pilot misjudged his approach, causing the accident, could not be excluded. There was no
evidence to suggest that the pilot had a medical condition that contributed to the accident, but
that possibility could not be excluded.
1.5.
The Commission identified the following safety issues during the inquiry:
when pilots do not inform their flight-following organisations of changes to their routes or
destinations, any search and rescue action that is required could be delayed or
misdirected
the widespread practice of allowing passengers to leave and return to a helicopter parked
on snow while the rotors are turning is hazardous.
1.6.
A recommendation was made to the Director of Civil Aviation that he ensure that helicopter
operators who conduct snow landings address in their safety management systems the hazard
of passenger disembarkation and embarkation during snow landings while the rotors are
turning.
1.7.
The key lessons identified during the inquiry into this occurrence were:
transport operators should keep formal records of concerns about operational staff and
how they are dealt with. Record keeping is consistent with the safety management
system goal of improving system quality
pilots should ensure that they inform their flight-following organisations of any changes to
their operating areas or destinations.
Final Report AO-2013-010 | Page 1
2.
Conduct of the inquiry
2.1.
At 1630 on 28 October 2013 the Civil Aviation Authority (CAA) informed the Transport Accident
Investigation Commission (Commission) of the accident. The Commission opened an inquiry
that day.
2.2.
Before the Commission’s investigators arrived on site early in the afternoon of 29 October
2013, the Commission gave permission for both helicopters to be de-fuelled and for the cabin
of the parked helicopter to be stripped in preparation for removal from the site. Investigators
examined both helicopters briefly on site, ahead of a forecast deterioration in the weather. The
helicopters were lifted by helicopter to Wanaka later that day.
2.3.
Both helicopters were examined at Wanaka before the helicopter that had been parked during
the collision was returned to the operator. The landing helicopter, ZK-IMJ, was taken to the
Commission’s technical facility in Wellington.2
2.4.
Between 29 October and 1 November 2013 investigators interviewed the operations manager
and chief pilot of The Helicopter Line Limited (the operator), the pilot of the parked helicopter,
and the passengers who had been in ZK-IMJ. Other witnesses were interviewed by phone in
November 2013.
2.5.
The pilot of ZK-IMJ was not fit to be interviewed until 4 December 2013. Owing to the nature of
his injury, the interview was conducted in the presence of a medical rehabilitation specialist.
The Commission’s medical consultant reviewed the pilot’s medical records made before and
after the accident.
2.6.
On 4 September 2014 the investigator in charge re-interviewed the operations manager and the
chief pilot.
2.7.
The documented policies and procedures of the operator, the training records it held for the
pilot and the maintenance records for the helicopter were reviewed during the investigation.
2.8.
There were no fatalities among the passengers, all of whom were from the People’s Republic of
China. New Zealand was not obliged by Annex 13, Aircraft Accident and Incident Investigation,
to the Convention on International Civil Aviation to notify China of the accident. However, the
New Zealand Ministry of Foreign Affairs and Trade and a Chinese consular official were
informed of the accident and investigation.
2.9.
France, the State of Manufacture of the helicopter and the engine, did not formally participate
in the initial investigation, but an expert from the manufacturer assisted with a further review of
the wreckage on 27 January 2016.
2.10. On 14 December 2016 the Commission approved a draft report for circulation to interested
persons for comment. Written submissions were received from three interested persons. The
Commission considered the submissions and in May 2017 circulated an amended draft report
to two interested persons for comment.
2.11. Written submissions on the amended draft report were received from both interested persons.
The Commission considered the submissions, and changes made as a result of those
submissions have been included in the final report.
2.12. On 28 June 2017 the Commission approved the final report for publication.
2 Except for the landing skids, which, after inspection, were removed for convenience and returned to the operator.
Page 2 | Final Report AO-2013-010
3.
Factual information
3.1.
Narrative
3.1.1. On Monday 28 October 2013 a Squirrel helicopter registered ZK-IMJ (the helicopter) was
assigned to the pilot who had the accident later that day (the pilot). At 0910 he departed on his
first flight of the day, taking six passengers from the operator’s main base at Queenstown
aerodrome for a ‘snow landing experience’ in mountains to the north.3 The flight returned to
Queenstown at 1012.
3.1.2. At 1036 the pilot carried out a passenger flight to Milford Sound, where the helicopter was shut
down for two hours. While at Milford Sound the pilot had a light lunch. On the return flight they
landed briefly in deep, fresh snow near the Humboldt Glacier, before arriving at Queenstown at
1413.
3.1.3. At 1448 the pilot departed Queenstown in company with another Squirrel4 to take a tour group
for a scenic flight and snow landing in the Lochnagar Saddle area, south of Mount Tyndall. Each
helicopter had six passengers. The pilot led the way. At 1504 he radioed the Queenstown base
to say they were landing at Lochnagar Saddle. However, the more experienced pilot (the senior
pilot) of the second helicopter radioed that the snow looked better further north. The senior
pilot then took the lead and flew to the expansive snowfield above Snowy Creek, also referred to
as the Tyndall Glacier.
3.1.4. The senior pilot said he made a shallow approach because he was alert to the possibility of a
slight tailwind and of the main rotor downwash causing ‘blowing snow’.5 A video taken by a
front-seat passenger in the helicopter that later crashed (ZK-IMJ) (the video) showed that the
lead helicopter came to a hover before landing, with no discernible blowing snow. The senior
pilot said the wind appeared to be calm.
3.1.5. The pilot of ZK-IMJ made an approach to the right of the parked helicopter. The video showed
that initially there was adequate lateral separation from the parked helicopter. None of the
passengers spoke English as a first language, but one said that the pilot was talking to them
over the intercom as they approached to land, and that his voice was steady and did not
suggest that he had any concerns.
3.1.6. The video showed that there was blowing snow as the helicopter came within about 20 metres
(m) of the parked helicopter. On the video the visibility decreased to the extent that detail of the
parked helicopter was barely visible, but a still photograph taken at the same time was much
clearer (see Figure 1).6
3.1.7. Instead of landing, the pilot carried out a go-around7 and, according to the senior pilot, radioed
that this was because he had been too high on the approach. The video showed the helicopter
moving towards the parked helicopter in blowing snow, then turning left to cross closely in front
of it. The senior pilot said he rebuked the pilot for flying too close to his helicopter, but the pilot
did not reply.
3.1.8. The re-circuit took about one minute. The video record stopped when the helicopter was
approximately 50 m from the parked helicopter, and did not show the collision.8 The senior
pilot said the helicopter was about 10 m behind his tail when it began moving towards him. He
3 Times are taken from the air traffic control and Rescue Coordination Centre New Zealand logs where available;
otherwise they are from the operator’s log.
4 Another Aérospatiale AS350B2, serial number 3625, registered ZK-HAE.
5 The operator described blowing snow as “loose snow present after fresh snow has fallen, especially if the
temperatures were cold and the snow has not yet bonded together, obscures ground reference when rotors are in
ground effect”. (The Helicopter Line, Operations Manual, section 5.26, Snow landings affected by weather
phenomena.)
6 The still photograph had a greater pixel count than a standard video camera.
7 In a go-around the pilot discontinues a landing approach and re-circuits for another attempt.
8 It was likely that the video recorder memory buffer was affected by the impact.
Final Report AO-2013-010 | Page 3

saw little or no blowing snow on the second approach, although some of the passengers said
they saw it. One of them said the helicopter was “swaying”, which made him think it was windy.
3.1.9. The helicopter continued to move towards the parked helicopter until its lower vertical stabiliser
and tail rotor hit the main rotor blades of the parked helicopter. The tail rotor assembly and
vertical fin separated from the helicopter and fell in front of and to the right of the parked
helicopter.
Figure 1
The parked helicopter as seen on the go-around from first approach
(Still photograph taken by a passenger)
3.1.10. Without a tail rotor, the helicopter climbed slightly and spun rapidly before tipping forward. It
came to rest on its right side about 70 m in front of the parked helicopter. There was no fire.
3.1.11. Because of the location the senior pilot could not contact the Queenstown base directly by radio
to advise it of the accident. He shut down his helicopter’s engine, told his passengers to remain
seated and went to the crashed helicopter. He shut down the engine on the crashed helicopter
and provided first aid to the passengers, but the pilot was unresponsive.
3.1.12. The senior pilot returned to his helicopter, broadcast a Mayday call9, to which there was no
response, and activated the emergency locator transmitter (ELT) for his helicopter. The search
and rescue satellite system detected the ELT signal at 1514 and notified the Rescue
Coordination Centre New Zealand at 1521. The Rescue Coordination Centre called the operator
at about 1523 to advise that an ELT alert had been received from the parked helicopter.
3.1.13. The senior pilot, in the meantime, alternated between helping the injured and going back to his
helicopter to broadcast further Mayday calls. At about 1530 a pilot many kilometres away
heard one of the Mayday calls and relayed it to air traffic control. At approximately 1555 the
first rescue helicopter arrived at the site.
9 Mayday is the internationally recognised signal sent by an aircraft or vessel that is in distress and needs
immediate assistance. The call includes the aircraft identification, its location and the assistance required.
Page 4 | Final Report AO-2013-010

3.1.14. The accident occurred in daylight at approximately 1508, on a broad snow shelf at the head of
Snowy Creek, southeast of the Tyndall Glacier. The elevation (height above mean sea level) was
approximately 2,050 m.
3.2.
Injuries to persons
3.2.1. The pilot received a severe brain injury and some minor fractures, and was in hospital for 39
days. The brain injury caused him a lengthy period of post-traumatic amnesia. He was
subsequently unable to recall the accident and had limited recall of the two months prior to the
accident.
3.2.2. All of the passengers in the helicopter were injured. Three passengers required hospital
treatment, with two of them remaining in hospital for two nights.
3.2.3. No-one in the parked helicopter was injured.
3.3.
Damage to aircraft
3.3.1. The helicopter came to rest on its right side (see Figure 2). The main rotor blades were
attached but had shattered from striking the snow while under power. The tail assembly had
fallen about 15 m in front of and to the right of the parked helicopter. The severed lower
vertical stabiliser was located, but the removed section of tail rotor blade was not found. The
front-left cabin door was detached in the ground impact.
Figure 2
The helicopter after the accident (with de-fuelling kit alongside)
3.3.2. The visible damage to the parked helicopter was confined to the outermost half-metre of each
of the three main rotor blades (see Figure 3). The main rotor head and main transmission were
subjected to shock loading when the main rotor struck the airborne helicopter, and had to be
replaced.
Final Report AO-2013-010 | Page 5

Figure 3
Typical damage to the main rotor blades of the parked helicopter
3.4.
Personnel information
3.4.1. The pilot had obtained a private pilot licence (aeroplane) in 1982 and a commercial licence in
1984. His flying career had primarily involved seasonal scenic flying, mainly in aeroplanes. This
had included ski planes, on which he had logged more than 1,100 snow landings, and float
planes.10 He had logged approximately 5,870 aeroplane hours, with his last aeroplane flight
being in July 2012. He held a C-category aeroplane instructor rating.
3.4.2. The pilot had begun helicopter training in 1999 on the Robinson R22. He had been issued with
a private pilot licence (helicopter) in 2000 and a commercial pilot licence (helicopter) in 2001.
He had obtained a type rating for the Hughes 500 in 2001 and for the Robinson R44 and the
Bell 47G in 2002. He had flown helicopters only occasionally at first and logged no helicopter
flying between July 2002 and May 2004. He had obtained a night rating in July 2005, but then
followed another gap in flying until October 2006 when he flew a few frost-protection flights in a
Robinson R44. He had logged no helicopter flying between November 2006 and June 2008.
3.4.3. In October 2008, when the pilot had 140 hours of helicopter experience, he had been hired by a
scenic flying company in Rotorua to fly a Robinson R44. The company had given him 3.5 hours
of dual instruction and 5.7 hours of command under supervision before allowing him to be a
pilot in command. He had obtained an AS350 Squirrel type rating with that company in
November 2011. During the next 10 months he had flown the Squirrel and the R44
intermittently, as well as a float plane.
3.4.4. In September 2012, when he had accrued approximately 1,050 hours of helicopter time, The
Helicopter Line had hired him as a full-time Squirrel pilot. He had flown 6.8 hours under
training before being approved to act as a pilot in command. His training had included 2.65
10 The first entry in the only logbook of aeroplane flying made available had been in May 2005, by which time the
pilot had accrued 5,000 hours.
Page 6 | Final Report AO-2013-010
hours of mountain flying instruction. The record of his final route check noted that he had
performed “multiple landings in challenging blowing snow and flat light conditions”.
3.4.5. Although the pilot had had experience in ski-plane operations, the operator’s policy had
required him to be based on the West Coast of the South Island to gain more experience of
helicopter operations on snow. The operator’s records indicated that his training progress had
been satisfactory. According to the operator, the pilot’s colleagues generally thought him to be
a steady pilot with “solid skill and judgement”.
3.4.6. In February 2013 the pilot had returned to the Queenstown base and been upgraded to B
category in the internal competency scheme then in use by the operator. The B category
permitted a pilot to use any landing site, although all flying remained under the supervision of a
Lead Pilot.
3.4.7. The pilot’s total helicopter experience at the date of the accident was 1,454 hours, of which
465 hours had been on the Squirrel. His logbook showed that he had landed many times in the
Lochnagar Saddle area, but recorded only one landing at the Tyndall Glacier.
3.4.8. The operator’s chief pilot said that in August 2013 fellow pilots had expressed concern that the
pilot had misjudged his separation from another helicopter while on a photographic flight, and
that he had made a landing approach that was unnecessarily fast. The chief pilot said that he
had responded by briefing the pilot on general flying standards, but he had not formally
recorded the concerns or the action taken.
3.4.9. The chief pilot had been an observer on the pilot’s next flight crew competency check flight,
conducted on 22 August 2013. The pilot had passed the check, but the chief pilot had
remained concerned that the pilot, like some other pilots at the time, had let his standards slip
and was displaying a degree of complacency.
3.4.10. Subsequently the pilot had flown a snow experience flight in the company of the chief pilot in a
second Squirrel. The chief pilot said that he “could find no fault with [the pilot’s] flying or
airmanship” on that occasion. As a result, and after favourable comments from others about
the pilot’s flying standard, the chief pilot had considered that the previous specific performance
issues had been rectified.
3.4.11. The counselling by way of the briefing from the chief pilot and the monitoring by way of the
observed check flight were not recorded in the pilot’s personal file. The operator had no other
record of the pilot having received counselling or needing specific retraining. The chief pilot
said that it was not unusual for operational or management issues that arose with pilots to be
dealt with and not recorded, but he agreed later that the concerns and the action taken in this
case ought to have been recorded.
3.4.12. The pilot and his family and associates considered him to be very healthy, fit and active, and
with no known concerns. The night before the accident he had gone to bed before 2130.
Those who saw him on the day of the accident said he had appeared fit to fly.
3.4.13. The senior pilot of the parked helicopter had been employed by the operator for more than 20
years and had more than 10,600 hours of helicopter experience. He was the Lead Pilot at the
Queenstown base and had authorised the flights that ended with the accident. He was very
familiar with the snowfield used. He said he had chosen his landing site so that the pilot of the
second helicopter would have ample room to choose his own, suitable landing site.
3.5.
Aircraft information
3.5.1. The Aérospatiale11 AS350B2 Squirrel helicopter was a higher-gross-weight version of the
original model designed and manufactured in France in 1974. It was certified to carry a pilot
and up to five passengers, but a supplemental type certificate was later approved that allowed
11 The company was later named Eurocopter, and at the time of this report was known as Airbus Helicopters.
Final Report AO-2013-010 | Page 7
the replacement of the single passenger seat next to the pilot with a two-place seat. The six-
passenger configuration was widely used for air transport flights.
3.5.2. The helicopter had been imported from Australia, on lease to the operator, and entered into the
New Zealand aircraft register on 26 August 2013. An airworthiness certificate in the standard
category had been issued on 30 August 2013. The certificate was non-terminating as long as
the helicopter was maintained and operated in accordance with Civil Aviation Rules. The
helicopter had been maintained in accordance with the approved maintenance programme.
There had been no recorded maintenance defects since 16 September 2013.
3.5.3. The helicopter had flown 37 hours since it was imported, and had accrued 3,055.2 hours at the
time of the accident. The next scheduled maintenance was a 100-hour check due at 3,118.4
hours.
3.5.4. The Turbomeca ‘Arriel’ 1D1 turbo-shaft engine had accrued 3,338.15 total hours at the time of
the accident.
3.5.5. The helicopter was equipped with a Garmin GNS 430 satellite navigation system, a model that
did not store recoverable data.
3.5.6. The helicopter was equipped with a Kannad 406 AF-H model ELT, appropriate to helicopter
installation. The ELT had been inspected and tested in accordance with the applicable
requirements in August 2013, but it did not activate during the accident.
3.5.7. The helicopter was not fitted, and was not required to be fitted, with a flight recorder.
Weight and balance
3.5.8. The operator had standard loading plans for its scenic flights. Its operational documentation12
stated that if passengers were seated in accordance with a standard plan, the helicopter would
comply with the limitations for all-up weight and centre of gravity position.13
3.5.9. The standard loading plan used a standard weight of 80 kilograms (kg) for each passenger.
That weight, which had been determined by the operator after conducting a CAA-approved
survey, avoided the need to weigh each passenger.
3.5.10. The operator had a computer program that could be used to calculate the weight and centre of
gravity position of a loaded helicopter. The program displayed pictorially the centre of gravity
position with reference to the allowable range of centre of gravity positions and would generate
an alert if a weight limit were breached.
3.5.11. The operator’s procedures14 stated that a weight and balance calculation was not required for
any flight that was loaded in compliance with a standard loading plan. The accident flight was
loaded in compliance with a standard plan for scenic flights.
3.5.12. The procedures also stated that pilots were not required to calculate separately the helicopter’s
weight and balance if a standard loading plan were used and the passengers were seated
according to the plan.
3.6.
Meteorological information
3.6.1. The accident occurred on the first fine day after two days of heavy snowfall. The passenger
video confirmed the excellent flying conditions.
3.6.2. There was no cloud and little or no wind at the time of the accident. The senior pilot said that
the wind rose to between five and eight knots from the south while they waited for rescue. The
12 The Helicopter Line Operations Manual, 9.1, Passenger weights and passenger loading; and form Ops 30 B2.
13 The centre of gravity is the single point in an object through which the weight (force of gravity) acts.
14 The Helicopter Line Operations Manual, 9.2, Weight & Balance Calculations & Passenger Manifests.
Page 8 | Final Report AO-2013-010
pilots of the rescue helicopters said that the wind was not more than a slight breeze. They said
the temperature was between zero and plus five degrees Celsius, and the air pressure 1,013
hectopascals.
3.6.3. The helicopters approached the landing site on a northerly heading, which put the sun high and
to the left of the approach direction.
3.7.
Wreckage and impact information
3.7.1. The accident occurred on a large snowfield above Snowy Creek, at an elevation of 2,050 m on
the south side of Mount Tyndall. The field had unobstructed approaches from the southeast,
and sloped down from right to left when viewed from the approach direction used.
3.7.2. The geometry of the collision was estimated from the senior pilot’s recollection and by
measuring the angles at which the helicopter’s lower vertical fin and one tail rotor blade had
been severed. As the landing skids, the lowest part of the helicopter, were not struck by the
main rotor of the parked helicopter, the helicopter must have been to the front right of the
parked helicopter at the instant of collision.
3.7.3. The helicopter came to rest on its right side approximately 70 m in front of the parked
helicopter, heading 90 degrees left of the approach direction.
3.7.4. The cabin was intact, although some seat squabs had been removed and used to support the
occupants while they waited for rescue. The buckling of the passenger bench seat supports
and a ground scar from a main rotor blade strike indicated that the helicopter had hit heavily on
its left side before it rolled on to its right side. The windscreen right pillar was broken near the
grab handle used by pilots when getting into and out of their seat.
3.7.5. The senior pilot had turned off the battery and fuel when he first got to the helicopter. The
hydraulic switch on the collective lever15 was in the guarded (on) position, as was normal.
3.7.6. Two of the three main rotor blades were visible; the third was buried in the snow. The main
rotor head was shattered and the blades buckled, which indicated that the engine had been
delivering high power when the rotor blades hit the snow.
3.7.7. The engine compressor and turbine showed evidence of having been operating at impact. The
power-demand anticipator for the fuel control unit, which was cable driven by collective lever
movement, operated correctly.
3.7.8. The circumstances of the accident and the damage to the main and tail rotors provided clear
evidence that the engine had been delivering high power prior to the collision. So the engine
was not examined further. The helicopter manufacturer agreed with that reasoning.
3.7.9. The tail boom was almost completely severed where it attached to the cabin. The horizontal
stabilisers were largely undamaged, except the left stabiliser had a tear and bend that had very
likely been caused by a main rotor blade.
3.7.10. At Wanaka, the correct movement of the main rotor flight controls was confirmed from the
pilot’s seat to the swash plate. The tail rotor drive was continuous from the transmission to the
point where the tail boom separated. The tail rotor drive shaft aft of the break showed evidence
of having been under power when it broke. The tail rotor drive was thereafter continuous to the
point where the tail rotor assembly had detached. The continuity and correct movement of the
yaw pedals were shown, allowing for the break in the tail boom. The tail rotor pitch change
movement was correct.
3.7.11. There was no leakage of fluid from any component of the hydraulic system that powered the
flight controls. The hydraulic pump drive belt was in good condition and the pump turned. The
15 Collective lever is the control that changes the pitch angle of a helicopter’s main rotor blades by the same
amount and at the same time, which changes the total rotor thrust, usually to effect a climb or descent.
Final Report AO-2013-010 | Page 9
hydraulic system filter bypass indicator was not ‘popped’, indicating that the filter was not
blocked. All visible damage was assessed as being a result of the crash.
3.7.12. While the wreckage was at Wanaka, the warning and caution annunciator panel and the Garmin
GNS 430 integrated communications, navigation and GPS receiver were removed from the
instrument panel for further examination. No useful information was obtained from this.
3.7.13. The visible damage to the parked helicopter was confined to the outermost half-metre of each
main rotor blade. However, later examination determined that the main transmission and mast
needed replacement.
3.8.
Medical and pathological information
3.8.1. The pilot had most recently completed an examination for a CAA medical certificate on 5
September 2013. The issued certificate included a requirement that he have half-spectacles
readily available for near-vision correction.
3.8.2. The pilot had informed the CAA medical examiners that he took medication for occasional
severe hay fever, but he was reportedly not affected by it on the day of the accident. Although a
very low level of a non-sedative hay fever medication16 was detected in a blood sample taken
after the accident, medical opinion17 was that the medicine would have been taken more than
24 hours before the accident and that the pilot was very unlikely to have been affected by any
potentially adverse side effects.
3.8.3. The operator had a drugs and alcohol policy that permitted random testing, and post-incident
testing of staff with their consent. The pilot had passed a random test in June 2013. An
analysis of blood and urine samples taken when the pilot was admitted to hospital did not
detect any alcohol or illicit drugs.18
3.8.4. The Commission’s medical consultant19 reviewed the notes held by the pilot’s general
practitioner at the time of the accident and assessed them as containing nothing of potential
relevance to the accident. The consultant also reviewed the hospital records pertaining to the
injuries the pilot received and his treatment.
3.9.
Survival aspects
3.9.1. The passengers were from China and only a few of them understood English. The operator’s
staff had given the passengers a pre-flight safety briefing in English, supplemented with briefing
cards written in Chinese. However, some passengers said that they still had not understood the
briefing. The Commission has recognised previously the difficulty for transport operators of
ensuring that non-English-speaking passengers receive meaningful pre-trip safety briefings.20
3.9.2. The safety briefing that was given included information on the survival and emergency
equipment carried on board, which was sufficient to support seven people for 72 hours.
3.9.3. The first passenger to escape after the crash said that her seat belt had been adjusted tightly
and was hard to undo with the helicopter on its side. She could not free the pilot, whose belt
was too tight. In helping the others out, she noted that their seat belts were loosely fastened. It
was not determined whether some passengers had had loose seat belts from the start of the
flight or they had loosened them subsequently.
3.9.4. The senior pilot was concerned that his own passengers should remain protected in his
helicopter until he had assessed the situation. He asked if any of them had first aid training,
16 Levrix brand.
17 That of the pathologist and the Commission’s medical consultant.
18 The analysis considered that drugs would have been administered to the pilot after the accident.
19 Dr Rob Griffiths MB, ChB(Hons), FAFPHM, FAFOM, MMP, DIH, DipAvMed, FFOM(RCP), FACASM, FACOEM.
20 Commission report 2008-207, Commercial jet boat Kawarau Jet No. 6, roll-over, confluence of the Kawarau and
Shotover Rivers, 25 September 2008.
Page 10 | Final Report AO-2013-010
but he was not understood. None of his passengers was involved in helping the injured. The
first aid kits and survival packs from both helicopters were used as required.
3.9.5. The Rescue Coordination Centre was alerted to the accident at 1521.21 No ELT signal was
received from the crashed helicopter.22 An aircraft maintenance engineer who arrived on site
while the rescue was underway said the ELT remote control switch in the cockpit of the crashed
helicopter was in the ‘armed’ position, but the indicator light was not flashing, which meant that
no signal was being transmitted. The engineer moved the remote switch to ‘on’, saw the light
flash and then left the switch armed.
3.9.6. Later testing showed that the six-axis activation switch was satisfactory, but there was no output
on the primary frequency of 406 megahertz. The cause of this was not determined. The output
of the secondary frequency of 121.5 megahertz was satisfactory.
3.9.7. The operator provided flight-following23 with its trained staff at the Queenstown base, but the
accident was in an area with poor radio contact. Thirty minutes without communication was
allowed before the Overdue Aircraft procedure was to be initiated. That limit was reached at
about the time that the Rescue Coordination Centre informed the operator of the beacon alert.
3.10. Organisational and management information
3.10.1. The Helicopter Line had been incorporated in 2002 and was one company in a group that
provided a range of services to tourists, including helicopter and aeroplane flights. At the time
of the accident the company operated from three primary bases and two satellite bases in the
South Island with a fleet of 20 helicopters, mainly the AS350 Squirrel, and 31 pilots, including
five on a casual basis.
3.10.2. The operations manager was responsible for the overall conduct of air operations and their
supporting ground operations. The chief pilot was responsible for crew training and competency
assessments and maintaining operating standards. The chief pilot at the time had been
appointed in March 2013.
3.10.3. The operations manager stated that the operator’s three biggest operational risks were:
roll-over while landing in flat-light conditions
heli-skiing operations
a mid-air collision, due to the number of aircraft in popular tourist areas.
These were aggregated under the heading ‘Accidents-aviation’ in the operator’s risk register,
with generic risk controls that included standard operating procedures, checks and training.
The operations manager said that the pilot categorisation scheme was another control that
was intended to mitigate these risks.
3.10.4. The operator’s procedures listed approximately 30 off-base landing sites, with brief notes on the
physical attributes of the sites and any precautions to be taken when using them.24 The list did
not include the snowfield where the accident occurred, nor any site on the Lochnagar Saddle
where the pilot had initially chosen to land. The two areas were within the concession area
granted to the operator by the Department of Conservation, which managed the region.25
3.10.5. On 17 October 2013 the operator had completed the CAA’s re-certification process, which
recurred every five years and required 100% compliance with the applicable Civil Aviation Rules.
The operator had recognised that its organisational changes in the previous four years could
21 The unique identification of ELTs meant that it was initially thought that the parked helicopter had crashed.
22 The ELT was a Kannad 406 AF-H model.
23 Flight-following is the process of maintaining awareness of an aircraft’s position and intentions so that a timely
response can be made in the event of an incident or the aircraft being overdue.
24 The Helicopter Line, Line Station Procedure, section QTN 1.2, Queenstown helibase procedures – bases,
helipads and landing areas.
25 The operator added details for a Lochnagar Saddle landing site, but not for the snowfield, in June 2014.
Final Report AO-2013-010 | Page 11
have created new risks, but the CAA’s routine surveillance had not disclosed any significant
operational concerns. The CAA’s most recent audit prior to the re-certification had been
completed on 26 November 2012 and made two minor maintenance-related findings.
3.11. Other occurrence
3.11.1. On 9 January 2014 another of the operator’s Squirrel helicopters was about to land on the
Richardson Glacier when the skid contacted the snow, causing the helicopter to roll on to its
side.26,27 The helicopter was destroyed, but the pilot28 and four passengers were uninjured.
3.11.2. That accident occurred at an altitude of 2,286 m on a relatively level glacial snowfield. The
stated weather conditions were unlimited visibility with negligible cloud and no wind. Snow
had fallen the previous day and contributed to bright conditions.
3.11.3. According to the pilot’s report, as he had been about to land the surface became less visible in
the bright light and because of blowing snow moving ahead as the helicopter slowed. The pilot
had lost sight of his reference points, so he commenced a go-around. As he did so the landing
skids contacted the snow, causing the machine to roll over abruptly.
26 The Commission was notified of the accident, but decided not to open a separate inquiry.
27 CAA occurrence number 14/52.
28 This was not the pilot involved in the 28 October 2013 accident.
Page 12 | Final Report AO-2013-010
4.
Analysis
4.1.
Introduction
4.1.1.
The accident occurred in weather conditions that fellow pilots said were “perfect”. The pilot
was familiar with the helicopter, the type of operation and the general area where they landed.
The accident was very unusual in that it was preceded by a near-collision during the prior go-
around.
4.1.2.
The pilot’s injury prevented his recalling the flight. Therefore the evidence of the senior pilot
and the video taken by a passenger were invaluable for the analysis. The senior pilot was
seated on the right side of the parked helicopter and had a clear view of the helicopter during
the go-around, the last 30 m of the second approach, and the collision.
4.1.3.
The analysis considers the following possible causes of the collision:
a. the pilot might have misjudged the approaches and separation
b. the pilot might have lost visual reference with the other helicopter
c. the pilot might have lost control because:
1) of a helicopter defect or
2) a helicopter performance limit was reached
d. the pilot might have been affected by a medical or psychological condition.
4.1.4.
In addition, the following two safety issues identified during this inquiry are discussed:
when pilots do not inform their flight-following organisations of changes to their routes or
destinations, any search and rescue action that is required could be delayed or
misdirected
the widespread practice of allowing passengers to leave and return to a helicopter parked
on snow while the rotors are turning is hazardous.
4.2.
The possibility of the pilot misjudging the separation
4.2.1.
The landing site that the pilot chose initially was very likely where he had landed that morning,
because a passenger on that flight said they had landed on a ridge, not a wide snowfield.
Although the pilot had logged only one landing at the Tyndall Glacier, it was possible that he
had made other landings there but had logged them as Lochnagar Saddle. The flight was a
standard snow experience flight, for which pilots had flexibility as to where to land. Landing on
such an expansive snowfield, with another helicopter as a focal point, should not have been
demanding for one of the operator’s B-category pilots. Given these circumstances, the lack of
a description of the Lochnagar Saddle and Tyndall Glacier landing sites in the operator’s
procedures at the time was almost certainly not a factor in the accident.
4.2.2.
It was very unlikely that the pilot would have minded the senior pilot taking the lead prior to
arriving at the landing site. It could not be determined how often the pilot had followed
another helicopter to a snowfield landing. The operator had not specified a procedure for
landing multiple helicopters at a single landing area, except that, for snow landings, all of the
helicopters had to have landed before any passengers would be allowed to disembark. There
was no prescribed minimum spacing between parked helicopters. The chief pilot said the rule
of thumb was one and a half rotor diameters between the rotor discs29, and that rule
appeared to have been generally followed. As the main rotor diameter of the AS350 Squirrel
was 10.7 m, the rule would give nearly 27 m between the centres of adjacent landing sites.
4.2.3.
By comparison, the recommended minimum distance between the centres of adjacent landing
sites at a heliport intended to serve Squirrel helicopters was 14.6 m (CAA, 2007). The
concrete landing pads at the operator’s Queenstown base were a minimum of 14 m apart.
29 A rotor disc is the area swept by a helicopter’s rotor blades each revolution.
Final Report AO-2013-010 | Page 13
Therefore the pilot’s normal ‘picture’ of a close, adjacent helicopter was of one that was only
14 m away, on a clearly defined landing site. He was sufficiently experienced in operations
onto unmarked landing sites, such as snowfields, and into confined areas that it should have
been second nature to ensure a safe separation.
4.2.4.
Having another helicopter land first gives the following pilot a clear reference point in an
otherwise unmarked landing area, and early warning of a blowing snow problem. These
advantages enable the following pilot to ensure a safe separation from the one ahead.
4.2.5.
There was plenty of space for the helicopter to land to the right of the parked helicopter,
without encroaching on the steeper upslope further to the right. The parked helicopter was an
excellent visual reference to assist the pilot in judging his rate of closure and spacing.
4.2.6.
The initial alignment of the pilot’s first approach appeared well spaced, but the senior pilot
thought it was too fast if the pilot intended to land alongside his helicopter. The senior pilot
might have interpreted the blowing snow as a sign that the pilot had had to slow abruptly from
a high speed. However, other experienced pilots of the operator considered the pilot’s
approaches, as seen on the video, to be at an appropriate angle and speed.
4.2.7.
A go-around is usually an undemanding manoeuvre in a helicopter, but the pilot might have
been annoyed with himself for having had to do so. Whether this or the rebuke by the senior
pilot was a factor in the subsequent accident was discussed with the Commission’s consultant
psychologist.30 In his opinion, if the pilot had been in a negative frame of mind he could have
had a degraded ability to focus on the landing and simply misjudged the second approach.
However, the chief pilot was of the opinion that it was in the pilot’s nature to have accepted
the rebuke and to have responded positively.
4.2.8.
There were aspects of the pilot’s performance during the go-around and the accident itself
that were similar to the misjudgements reported two months earlier (see paragraph 3.4.9).
This is a strong indication that this accident might have been the result of the pilot having
made similar misjudgements, although the pilot could not recall any such events or having
been reprimanded for such a concern. The reported errors in judgement were serious and the
operator ought to have had a written record of them and any remedial training that had taken
place.
Findings
1. The pilot’s training and the monitoring of his performance were in accordance
with the operator’s training policy and procedures.
2. In the absence of any other explanation, the possibility that the pilot had
reverted to his previously reported behaviour and misjudged his approach
could not be excluded.
3. The operator’s standard of record keeping for this pilot’s training and
performance monitoring did not meet generally accepted best practice.
4. The weather and snow conditions were favourable and the parked helicopter
provided an excellent visual reference for the pilot to ensure a safe
separation.
5. It could not be determined whether the senior pilot’s rebuke adversely
affected the pilot’s concentration or spatial judgement on the following
approach.
30 Keith McGregor, BSc, MNZPsS, CMIOP.
Page 14 | Final Report AO-2013-010
4.3.
The possibility of a loss of visual reference
4.3.1.
The operator’s operations manual guided pilots in coping with ‘bright-out’31, blowing snow and
a lack of spatial reference. The manual stated that pilots should make an initial approach and
plan to go around unless conditions clearly allowed a landing. The manual further
recommended that:
In conditions of reduced surface visibility the pilot should not continue an
approach without visual reference to the snow surface unless reference can be
achieved by the presence of objects such as flags, rocks, helicopters…
First approach
4.3.2.
The surface of the deep, powder snow was easily discerned. The senior pilot said that he had
not encountered blowing snow when he landed, and none could be seen in the video. His
approach had been terminated without an obvious flare.32
4.3.3.
It was very likely that as the pilot of the following helicopter was reducing his speed, the rotor
downwash lifted the surface snow. The blowing snow was not so dense as to obscure the
parked helicopter, but it may have made the rotor disc of the parked helicopter difficult to
discern.
4.3.4.
The accident pilot watched the video five weeks after the accident and commented that the
blowing snow on the first approach appeared to be “not too bad”. A photograph taken by a
rear-seat passenger showed the parked helicopter more clearly than the video did, and was
very likely more representative of what the pilot saw.33
4.3.5.
The operator’s management pilots considered that the amount of blowing snow raised on the
first approach would have been easily within the pilot’s capabilities and experience to see
through and land safely. The fact that he did not land was not especially significant, but it
indicated that he made a conscious decision to go around. The senior pilot said that after the
pilot began the go-around the pilot had transmitted what sounded like “too high”. The audio
on the passenger video was analysed but the pilot’s comments could not be determined.
4.3.6.
A go-around from this position required a climb straight ahead before making a left turn away
from the rising terrain. The pilot misjudged when he had passed the parked helicopter and
could turn left. It was very likely that he did not realise that he had converged towards the
parked helicopter during the approach. In addition, the blowing snow may have been dense
enough that he could not discern the edge of the parked helicopter’s rotor disc.
Finding
6. It was very likely that the pilot carried out the go-around because he lost his
depth perception and sight of the other helicopter in blowing snow.
Second approach
4.3.7.
The passengers in the helicopter said that the blowing snow at the end of the second
approach was worse than on the first approach, but the senior pilot disagreed. Although the
video stopped before the accident, the senior pilot watched the approach of the helicopter,
which he said was similar in angle and speed to the first approach. The senior pilot saw the
31 Bright-out was described as “a phenomenon caused by excessive reflection of sunlight off the snow surface,
resulting in a lack of depth perception, most common when the sun is high in the sky and the snow is fresh”. (The
Helicopter Line, Operations Manual, section 5.26, Snow landings affected by weather phenomena.)
32 In a flare the pilot applies aft cyclic, which produces a rearward rotor thrust component that slows a helicopter.
33 Because the still photograph had a greater pixel count than that of a standard video camera.
Final Report AO-2013-010 | Page 15
helicopter almost come abeam before it seemed to turn towards him and a collision became
imminent.
4.3.8.
The attitude of the helicopter at the point of collision could not be determined accurately
without knowing whether the main rotor disc of the parked helicopter was level. However, it
was more likely than not that the parked helicopter’s disc was level, in readiness for the
passengers’ disembarkation. If so, the airborne helicopter was in a more-or-less-level attitude
at the time of the collision, as determined by the angle at which its vertical stabiliser was
severed. A level attitude suggests that the pilot was not flaring the helicopter to reduce speed,
or accelerating for another go-around or banking significantly to the left. The landing skids,
which are more than half a metre below the lowest point of the tail, were not hit by the rotor
disc, which indicated that the helicopter did not directly overfly the parked helicopter.
4.3.9.
The environmental conditions in this accident had some similarities to the accident on the
Richardson Glacier a few months later (see paragraph 3.11.1): the relatively high altitude;
clear and bright conditions; fresh, flat snow; and blowing snow as the helicopter was about to
land. However, in the accident near Mount Tyndall the pilot had the parked helicopter as a
strong visual reference during both approaches.
Findings
7. It was unlikely that blowing snow significantly affected the pilot’s view of
the parked helicopter during the second approach.
4.4.
The possibility of a loss of control
4.4.1.
The pilot’s flying, judging from the video, was smooth. That, and the absence of any radio
communication from him to the contrary, indicated strongly that the helicopter’s technical
performance was normal. No performance limitation was identified. The passengers’
evidence did not indicate that the pilot was distracted or that anything interfered with his
control during either approach.
Helicopter defect
4.4.2.
There was nothing in the passenger video, which began prior to the passengers boarding at
Queenstown, to suggest that there was a technical problem or that the pilot had difficulty at
any stage with controlling the helicopter.
4.4.3.
The helicopter behaviour, in climbing and spinning after the tail rotor assembly separated, was
evidence of ample power being delivered to the transmission at the time of the collision. An
expert from Airbus Helicopters confirmed that the damage to the main rotor system was
strong evidence that the rotor had been under high power when the helicopter struck the
ground. For these reasons the engine was not subjected to further examination.
4.4.4.
The flight controls moved correctly, and continuity of the collective, cyclic and tail rotor
controls was shown as far as impact damage allowed. The hydraulic system (which powered
the flight control servo actuators) had no obvious defects and was not tested further.
Finding
8. No technical defect was found that might have contributed to the close go-
around or to the collision.
Page 16 | Final Report AO-2013-010
Performance limit
4.4.5.
Three of the key parameters that affect an aircraft’s performance are:
its total weight
the altitude
the air temperature.
The location of the centre of gravity primarily affects stability and controllability.
4.4.6.
The empty weight of the helicopter was recorded in the helicopter logbook as 1,327.7 kg. The
fuel load on departure from Queenstown was 50% of tank capacity, or 213 kg.34 Using the
assumptions of the operator’s standard loading plan35, the take-off weight of the helicopter
was later calculated to be 2,129 kg, which was under the maximum permitted weight of 2,250
kg.
4.4.7.
No-one calculated the weight or the centre of gravity position before the flight, because one of
the operator’s procedures waived the requirement when using a standard loading plan. Had
the weight and balance calculator been used, the pictorial display would have indicated that
the centre of gravity was ahead of the forward limit.
4.4.8.
The passengers were not weighed before the flight or after the accident. However, they were
observed to be lightly framed and generally of short stature. Therefore, their average weight
was very likely to have been less than the operator’s standard weight of 80 kg. Using
hypothetical passenger weights of up to 75 kg, the take-off weight was re-estimated as 2,079
kg, with the centre of gravity on the forward limit. Allowing for fuel used during the flight, the
weight at the time of the accident was estimated to have been 2,037 kg, with the centre of
gravity then behind the forward limit (and therefore within limits) (see Appendix 1).
4.4.9.
According to the flight manual, at a landing weight of 2,037 kg and with an air temperature of
plus five degrees Celsius, the helicopter could have hovered out of ground effect36 at a
pressure altitude of 2,700 m, which was about 650 m above the accident site. This hover
capability showed that there would have been adequate power and control for the normal
manoeuvres associated with landing and take-off at the lower altitude of the accident site.
4.4.10. Although the helicopter weight and centre of gravity position were likely to have been within
limits for this flight, the operator’s procedures risked pilots taking off with their helicopters
outside permissible limits. For example, if six passengers of standard weight were carried with
a standard 60% fuel load and a pilot weighing 95 kg, the centre of gravity would remain ahead
of the forward limit, even with the maximum possible ballast carried in the rear of the
helicopter. If pilots checked the weight and balance calculator for every flight, they would be
alerted to the actual balance condition.
4.4.11. Therefore, the operator’s standard loading plans did not guarantee that the weight and centre
of gravity position would be within permissible limits. As the operator’s procedures waived a
calculation of weight and balance when a standard loading plan was used, and did not require
pilots to verify weight and balance if a standard loading plan was used, it was very likely that
potential loading errors could go undetected.
4.4.12. The pilot-in-command of an aircraft is required37 to assess the weight and balance information
and to ensure that the aircraft will remain for the duration of the flight within the limits
34 The fuel quantity indicator scale showed intervals of 10%. Fuel weights are for a specific gravity of 0.79.
35 Except 75 kg was used for each front-seat passenger in order to comply with the seat weight limit.
36 A helicopter is ‘in ground effect’ when the downwash from the main rotor strikes the surface and generates an
increase in pressure, which effectively creates a cushion of air that reduces the power required to hover. The
effect reduces as the helicopter moves away from the surface, with the result that more power will be required. At
a height equivalent to approximately half of the rotor diameter, the effect is considered to be nil and the helicopter
is then ‘out of ground effect’.
37 Civil Aviation Rule 135.305 (b).
Final Report AO-2013-010 | Page 17
specified in the flight manual. The procedures used by the operator in 2013 meant that its
pilots often did not assess this information, and instead relied on the implied guarantee that
the standard loading plans would keep them within the limits.
4.4.13. The CAA, in allowing the use of standard passenger weights, emphasised that flight manual
limitations must be observed.38 The operator has since amended its procedures to require an
actual weight and balance calculation for every flight.
4.4.14. Experience with the Squirrel helicopter had shown that care was needed to ensure that the
centre of gravity was not ahead of the forward limit when a dual seat was fitted and six
passengers were carried.39 On 27 November 2015, in an action unrelated to this accident,
the CAA issued an airworthiness directive40 that required the actual weight and balance to be
calculated before every flight of a Squirrel helicopter when people or cargo occupied the two-
place front seat.41
Findings
9. The helicopter’s weight and centre of gravity position were estimated to
have been within flight manual limits at the time of the accident.
10. The operator’s procedures regarding the use of standard loading plans did
not ensure compliance with the Civil Aviation Rule that on all occasions
helicopters are to be flown within the limitations published in the flight
manual. In this case the use of the standard loading plan did not cause or
contribute to the accident.
4.5.
The possibility of a medical or psychological condition
4.5.1.
There was no obvious explanation for an experienced pilot, performing a routine and familiar
flight in a serviceable helicopter under ideal weather conditions, having a serious collision risk
twice in a short space of time. The possibility that the pilot misjudged the separation between
the helicopters because of a medical or psychological condition was considered.
Medical condition
4.5.2.
The medical notes held by the CAA and the pilot’s general practitioner contained nothing to
suggest that a pre-existing medical condition could have been a factor. His use of hay fever
medication was considered not pertinent, and tests for illicit drugs and alcohol were negative.
4.5.3.
A passenger on the morning snow landing flight to the Lochnagar Saddle area said that they
thought the pilot had been “good, safe and secure, and aware of everything”. A passenger on
the later Milford Sound flight knew the pilot and said his demeanour had been “okay”, with
nothing unusual noted. None of the passengers on the accident flight, and none of the staff
who saw the pilot during the day, said they had noticed anything of concern about the pilot.
4.5.4.
Before departing Queenstown on the accident flight, the pilot was wearing a cap with
sunglasses resting above the peak. It is not known whether he was wearing the sunglasses at
the time of the accident. During the approaches to the Tyndall Glacier, the sun would have
been ahead and above, and slightly to the left. Without sunglasses, glare from the bright snow
38 See, for example, Advisory Circular 119-4, page 15.
39 See, for example, Commission report 94-023, Aérospatiale AS350B, ZK-HWV, collision with terrain, near Fox
Glacier, 29 October 1994.
40 An airworthiness directive is a mandatory instruction, issued by the CAA, to ensure the continued airworthiness
of an aircraft or component.
41 Airworthiness Directive DCA/AS350/128 Forward two-place seat – Operating limitations. Where weighing
passengers was not practical (e.g. when uplifting passengers in remote locations), it was permissible to use each
passenger’s declared weight plus 6 kg.
Page 18 | Final Report AO-2013-010
could have been a problem. However, the parked helicopter would have provided a good
contrast with the snow.
4.5.5.
The pilot’s vision had been checked at a routine CAA medical examination less than two
months previously. The requirement that he have half-spectacles available was a common
age-related requirement, primarily for reading charts and manuals, and not pertinent to this
flight. Therefore it was unlikely that he had a vision problem at the time of the accident.
4.5.6.
The accident pilot did not advise the senior pilot that he was unwell or having any difficulty
flying the helicopter. During the go-around, the pilot was reported to have said only that he
had misjudged his approach angle; that he was too high. He did not respond to the senior
pilot’s rebuke for coming too close. Had the pilot been affected by a medical condition that
prevented him making a radio call, it would have been very unlikely that he could have made a
steady approach to land.
4.5.7.
The video did not show the last 10 seconds or so before the collision, but what was recorded
suggested that the pilot was in full control of the helicopter on both approaches. Some
passengers said it was “windy” or that the helicopter was “rocky” or “swaying” on the second
approach, but the senior pilot said it was not windy. The passengers may have mistaken
blowing snow – and possibly the normal vibration that is felt when a helicopter slows down –
as an indication of wind.
4.5.8.
If the passengers’ recall of events was not confused by the collision, their description of a
“rocky” or “swaying” approach could have meant the pilot was over-controlling. However, the
senior pilot observed the impending and actual collision and did not see any evidence of over-
controlling.
4.5.9.
Some neurological disturbances, such as a severe migraine or a transient ischaemic attack
(‘mini-stroke’), can cause impairment or be ongoing risks of incapacitation (CAA, 2010). It can
be difficult to prove that such an event has occurred, because there might not be any
‘artefact’, or physical evidence. However, in the opinion of the pilot’s rehabilitation medical
consultant, apart from the traumatic head injury, “there was no discrepancy in his
presentation to suggest that there was any other medical/neurological diagnosis that had
occurred around the time of the crash”.
Finding
11. There was no evidence to suggest that the pilot had a medical condition
that contributed to the accident, but that possibility cannot be excluded.
Potential psychological condition
4.5.10. Having been unable to identify any direct cause of the accident, the Commission considered
the possibility of an obscure psychological factor.
4.5.11. The investigation considered whether the pilot might have tried so hard to stay clear of the
parked helicopter on the second approach that he experienced an ‘ironic process of mental
control’. The theory of this psychological effect, which might cause a person to do exactly
what they were trying to avoid, is summarised in Appendix 2. An example that illustrates the
theory is a cyclist hitting an obstruction that they were trying strenuously to avoid.
4.5.12. The possible relevance of the theory is as follows. The pilot would have been aware that the
go-around was delaying the snow experience for both groups of passengers. One would
expect him to have wanted to complete the go-around quickly and to make a tidy landing near
the parked helicopter. If he had been overly intent on making a ‘perfect’ landing close to the
other helicopter, he might have tried too hard to avoid getting too close and, ironically, flown
into it.
Final Report AO-2013-010 | Page 19
4.5.13. However, the circumstances did not fit the theory well. Ironic effects require some adverse
mental load. The go-around might have created some time pressure and the pilot may have
felt driven to make a better approach, but those pressures were unlikely to have been of
sufficient intensity or duration to provoke an ironic effect.
4.5.14. A further reason to doubt the applicability of this theory comes from Wegner’s view on the role
of ‘automaticity’ in resisting ironic effects (Wegner, 1994, p.48). Even an experienced pilot
must give close attention to the desired touchdown point and prevailing conditions, but the
manipulation of the controls to achieve the landing is essentially an automatic skill. The pilot
was very familiar with landing in confined areas and on landing sites with the minimum
separation from adjacent sites (for example, at the operator’s base). It was very unlikely that
he would have been trying ‘too hard’ to land close to the parked helicopter when the parked
helicopter provided a highly visible point of reference and there was ample space.
4.6.
Summary of potential causes
4.6.1.
The analysis considered the following potential causes of the collision:
a. misjudgement by the pilot of his separation from the parked helicopter
b. loss of visual reference with the other helicopter
c. loss of control because of a helicopter defect or because a performance limit was
reached
d. the pilot being affected by a medical or psychological condition.
4.6.2.
The pilot was experienced in flying onto unmarked landing sites, such as snowfields, and into
confined areas such that it should have been second nature for him to ensure a safe
separation. The landing site was expansive and the parked helicopter was an excellent visual
reference. The pilot clearly misjudged his spacing twice, but only the first instance could be
explained.
4.6.3.
The first helicopter landed without raising any blowing snow, which might have misled the pilot
into not reducing his speed sufficiently early on his first approach. When the pilot did go
around because of the blowing snow his helicopter raised, he did not discern the parked
helicopter’s rotor disc and turned too soon, passing close in front of it.
4.6.4.
No evidence was found of a mechanical problem with the helicopter, or of its performance
being adversely affected. No medical reason was identified to explain the pilot’s actions. An
obscure psychological effect was considered unlikely to have been a contributing factor.
4.6.5.
The fact that within three months the operator had two accidents during snow landings did not
necessarily indicate that the operator’s standards or training were inadequate. Snow landings
are inherently hazardous and the operator’s pilots were trained to anticipate blowing snow
and to perform go-arounds if they lost essential visual references. The nature of helicopter
operations means that they routinely operate close to other aircraft and structures. Therefore
it is reasonable to assume that pilots will normally maintain a safe separation from other
helicopters and structures throughout every approach and landing.
Finding
12. The cause of the collision was not determined.
Page 20 | Final Report AO-2013-010
5.
Safety issues
5.1.
The following safety issues were identified during this inquiry:
when pilots do not inform their flight-following organisations of changes to their routes
or destinations, any search and rescue action that is required could be delayed or
misdirected
the widespread practice of allowing passengers to leave and return to a helicopter
parked on snow while the rotors are turning is hazardous.
Flight-following
5.2.
The failure of an ELT on a crashed aircraft to transmit a signal, or for the signal to be not
heard, can have potentially fatal consequences. If the alarm is not raised some other way,
which fortunately did happen in this case, search and rescue action will not begin until the
operator determines that the flight is overdue.
5.3.
Therefore it is imperative that a flight-following system have accurate information regarding
the route, destination and intended actions of a flight being monitored. An unannounced
change to the information that was last advised could result in a search of the wrong area. In
this case the pilot radioed the operator’s base that the two helicopters were about to land at
the Lochnagar Saddle, but the actual landing took place about three kilometres away. The
Commission has highlighted this as a key lesson arising from this investigation.
5.4.
The poor reliability of ELTs is a global issue. However, the varied circumstances of aircraft
crashes mean that 100% reliability might never be achieved. Severe damage, fire or an
obstructed or broken antenna are common reasons for signals not being received after a
crash.
5.5.
Apart from manufacturers improving the reliability of their ELTs, operators could reduce the
consequences of un-alerted accidents in remote sites by fitting GPS flight tracking devices.
Tracking devices have proved their worth time and again when ELTs have failed. At the time,
the operator had flight trackers fitted to some of its helicopters, but neither of the helicopters
involved in this accident had one fitted.42
5.6.
The Commission drew attention to the benefits of flight tracking devices and the poor
reliability of ELTs when it recommended to the Director of Civil Aviation on 26 February 2014
that he43:
encourage the use of flight tracking devices, especially for use in aircraft operating in
remote areas around New Zealand (005/14)
continue to support the international work underway to improve the crash survivability
of ELTs and to include GPS information in the data transmitted by such devices
(006/14).
On 5 March 2014 the CAA replied, in part:
(005/14) In our draft recommendation response 31 January 2014, the Director
commented that the CAA provide for the fitment of Flight Tracking Devices (FTDs) by
operators and this can be achieved in accordance with the relevant provisions of AC 43-
14. The CAA will continue to encourage operators to fit FTDs in this manner. The CAA
considers the action sufficient to satisfy the closure of the Commission’s
recommendation
(006/14) In the same response letter, the Director commented that the CAA already
supports in principle the ICAO [International Civil Aviation Organization] and
42 Since April 2014 the operator had installed flight tracking devices in all of its helicopters, and all of its operating
bases had dedicated monitoring screens.
43 Inquiry report 11-003, in-flight break-up, ZK-HMU, Robinson R22, near Mount Aspiring, 27 April 2011.
Final Report AO-2013-010 | Page 21
manufacturers’ efforts to improve the crash survivability of ELTs and accuracy of
position reporting. The work is ongoing and in this context the CAA requests that the
recommendation be closed.
5.7.
Both safety recommendations remain open. The Commission has also promoted the benefits
of flight tracking devices in its Watch List item: Technologies to track and locate.44
Disembarking while rotors are turning
5.8.
Although not a factor in this accident, a further safety issue identified during the inquiry was
the widespread practice of allowing passengers to leave and return to helicopters parked on
snow while the rotors are turning. Frequently the pilot will also disembark to guide the
passengers while they move under the main rotor disc. There is a serious risk to people on
the ground if a helicopter has settled into fresh snow or it breaks through an apparently hard
surface crust. Should this happen the clearance between the rotor disc and people walking
beneath could reduce sufficiently for someone to be struck by the rotor blades.
5.9.
The risk persisted in spite of the operator, in common with other operators, having taken steps
to reduce it by fitting snowshoes to helicopter landing skids and by training pilots in the correct
snow landing techniques.
5.10.
The Director of Civil Aviation informed the Commission of proposed Civil Aviation Rules that, if
passed, could address the hazard of leaving helicopters unattended with the rotors turning
under power.45 However, there is no certainty that the proposed rules will be implemented.
5.11.
Therefore, the Commission recommended that the Director of Civil Aviation ensure that
helicopter operators that conduct snow landings address in their safety management systems
the hazard of passenger disembarkation and embarkation during those landings while the
rotors are turning.
44 See www.taic.org.nz/Watchlist2016/Technologiestotrackandtolocate/tabid/297/language/en-NZ/Default.aspx.
45 Notice of Proposed Rule Making (NPRM 17-02), Small Issues Rules Amendment.
Page 22 | Final Report AO-2013-010
6.
Findings
6.1.
The pilot’s training and the monitoring of his performance were in accordance with the
operator’s training policy and procedures.
6.2.
In the absence of any other explanation, the possibility that the pilot had reverted to his
previously reported behaviour and misjudged his approach could not be excluded.
6.3.
The operator’s standard of record keeping for this pilot’s training and performance monitoring
did not meet generally accepted best practice.
6.4.
The weather and snow conditions were favourable and the parked helicopter provided an
excellent visual reference for the pilot to ensure a safe separation.
6.5.
It could not be determined whether the senior pilot’s rebuke adversely affected the pilot’s
concentration or spatial judgement on the following approach.
6.6.
It was very likely that the pilot carried out the go-around because he lost his depth perception
and sight of the other helicopter in blowing snow.
6.7.
It was unlikely that blowing snow significantly affected the pilot’s view of the parked helicopter
during the second approach.
6.8.
No technical defect was found that might have contributed to the close go-around or to the
collision.
6.9.
The helicopter’s weight and centre of gravity position were estimated to have been within flight
manual limits at the time of the accident.
6.10. The operator’s procedures regarding the use of standard loading plans did not ensure
compliance with the Civil Aviation Rule that on all occasions helicopters are to be flown within
the limitations published in the flight manual. In this case the use of the standard loading plan
did not cause or contribute to the accident.
6.11. There was no evidence to suggest that the pilot had a medical condition that contributed to the
accident, but that possibility cannot be excluded.
6.12. The cause of the collision was not determined.
Final Report AO-2013-010 | Page 23
7.
Safety actions
General
7.1.
The Commission classifies safety actions by two types:
(a)
safety actions taken by the regulator or an operator to address safety issues identified
by the Commission during an inquiry that would otherwise result in the Commission
issuing a recommendation
(b)
safety actions taken by the regulator or an operator to address other safety issues that
would not normally result in the Commission issuing a recommendation.
Safety actions addressing safety issues identified during an inquiry
7.2.
On 27 November 2015 the CAA issued an airworthiness directive that required the weight and
balance to be calculated before every flight of a Squirrel helicopter when people or cargo
occupied the two-place front seat.46
Safety actions addressing other safety issues
7.3.
None identified.
46 Airworthiness Directive DCA/AS350/128 Forward two-place seat – Operating limitations.
Page 24 | Final Report AO-2013-010
8.
Recommendation
General
8.1.
The Commission may issue, or give notice of, recommendations to any person or organisation
that it considers the most appropriate to address the identified safety issues, depending on
whether these safety issues are applicable to a single operator only or to the wider transport
sector. In this case a recommendation has been issued to the Director of Civil Aviation, with
notice of the recommendation given to the New Zealand Helicopter Association.
8.2.
In the interests of transport safety, it is important that recommendations are implemented
without delay to help prevent similar accidents or incidents occurring in the future.
Recommendation
8.3.
A safety issue identified during the inquiry was the widespread practice of allowing passengers
to leave and return to helicopters parked on snow while the rotors are turning. Frequently the
pilot will also disembark to guide the passengers while they move under the main rotor disc.
There is a serious risk to people on the ground if a helicopter has settled into fresh snow or it
breaks through an apparently hard surface crust. Should this happen the clearance between
the rotor disc and people walking beneath could reduce sufficiently for someone to be struck
by the rotor blades.
8.4.
On 25 May 2017 the Commission recommended that the Director of Civil Aviation ensure that
helicopter operators who conduct snow landings address in their safety management systems
the hazard of passenger disembarkation and embarkation during those landings while the
rotors are turning. (009/17)
8.5.
On 11 July 2017 the Director of Civil Aviation replied:
In accordance with the provisions of Civil Aviation Rules Part 119: Air Operator –
Certification, helicopter operators have until 1 February 2021 to introduce a
Safety Management System. Given that timeline, the Director accepts the
recommendation and will ensure that when operators’ Safety Management
Systems are certificated all significantr aviation risks are identified and managed.
Final Report AO-2013-010 | Page 25
9.
Key lessons
9.1.
Transport operators should keep formal records of concerns about operational staff and how
they are dealt with. Record keeping is consistent with the safety management system goal of
improving system quality.
9.2.
Pilots should ensure that they inform their flight-following organisations of any changes to
their operating areas or destinations.
Page 26 | Final Report AO-2013-010
10.
Citations
CAA. (2007, April 27).
Chapter 3 - Physical characteristics. Retrieved from Advisory Circular AC139-8,
Aerodrome
Design:
Heliports:
http://www.caa.govt.nz/assets/legacy/Advisory_Circulars/AC139_8.pdf
CAA. (2010, Deecember).
MIS 011 Strokes and Transient Ischaemic Attacks. Retrieved from CAA :
http://www.caa.govt.nz/assets/legacy/medical/Med_Info_Sheets/MIS011.pdf
Wegner, D. M. (1994). Ironic processes of mental control.
Psychological Review, Vol.101, No.1, 34-52.
Wegner, D. M., Ansfield, M., & Pilloff, D. (1998). The putt and pendulum: ironic effects of the mental
control of action.
Psychological science, Vol.9, No.3, May 1998.
Final Report AO-2013-010 | Page 27
Appendix 1: Weight and balance calculation
These calculations use passenger weights that are closer to their probable weights than the standard
80 kg used then by the operator.
Take-off from Queenstown
AS350 W&B
Weight
Arm
Moment
Pilot
85
1.55
131.75
Dual front
140
1.55
217
Rear pax
290
2.54
736.6
Side locker
2
3.2
6.4
Fuel 50%
213
3.48
741.24
Survival kit
17
4.6
78.2
Boot
4
4.6
18.4
Total load
751
1,929.59
Empty helo
1,328
3.532
4,689.44
TOTAL depart
2,079
3.184
6,619.03
[Forward limit at this weight is ~3.184]
Arrival at landing site
AS350 W&B
Weight
Arm
Pilot
85
1.55
131.75
Dual front
140
1.55
217
Rear pax
290
2.54
736.6
Side locker
2
3.2
6.4
Fuel 40%
171
3.48
595.08
Survival kit
17
4.6
78.2
Boot
4
4.6
18.4
Total load
709
1,783.43
Empty helo
1,328
3.532
4,689.44
TOTAL land
2,037
3.178
6,472.87
[Forward limit at this weight is ~3.175]
Reference: AS350B2 flight manual, section 2.1, page 2.
Page 28 | Final Report AO-2013-010
Appendix 2: Ironic processes of mental control – Key points from research on
unwanted outcomes
Wegner (1994) proposes the theory of ‘ironic processes of mental control’ to explain why people
sometimes make the error of doing exactly that which they are trying to avoid. These errors are more
likely to happen under mental load (such as stress, time pressure, distraction). An example of an ironic
error is when efforts to fall asleep result in wakefulness.
The theory suggests that when we consciously try to produce a desired thought or action, we also
unconsciously monitor for the unwanted thought or action. The purpose of this ‘ironic monitoring’ is to
ensure that we actively avoid the unwanted state.
As Wegner explains (Wegner, 2009, p.48), “The conscious search for distractions and the unconscious
search for the unwanted thought work together to achieve suppression – the conscious search doing
the work and the unconscious search checking for errors”. Mental load, such as stress or distraction,
can impair the conscious effort to produce the wanted state. But the unconscious search for errors
requires less effort and therefore remains less affected when mental load increases. So the search for
errors continues and, through the process of cognitive priming, can produce the very state to be
avoided.
LoRusso (2009, p.4) cites research providing evidence for the theory of ironic processes in several
areas of mental control: the control of sleep (Ansfield, Wegner & Bowser, 1996), the control of anxiety
(Koster, Rassin, Crombez & Naring, 2003), when trying to relax when under stress (Wegner, Broome &
Blumberg, 1997) and in mood control (Wegner, Erber & Zanakos, 1993).
Less research has been found in the area of ironic effects of the mental control of action, although
some has been conducted in relation to sporting performance. For example, Wegner, Ansfield and
Pilloff (1998) conducted an experiment involving golf putting, and concluded that “distraction can
undermine motor control to produce not only erroneous movement, but precisely the least wanted
movement” (p.199). LoRusso (2009), who used tennis players as subjects, concluded that “trying not
to perform some action under pressure can bring about those exact unwanted actions” (p.ix).
Being relaxed and avoiding distractions helps to avoid counter-intentional effects. Wegner also
suggests that the “automatization” of the operating process raises the resistance to ironic effects
(Wegner, 1994, p.48). Skilled behaviour follows training and repeated practice in intentional actions to
the point that they become automatic. The actions become easier and require less thought and the
results are more accurate (fewer errors). However, when conscious attention is given to exactly what
one is doing during an otherwise automatic action, the error count often increases. Wegner suggests
that when attention is given to the details of an action, it becomes intentional rather than automatic,
and as a result the resistance to errors is lost.
An alternative to the theory of ironic processes is that of overcompensation. De la Peña, Murray and
Janelle (2008, cited in Toner, Moran & Jackson, 2013) propose the “implicit compensation hypothesis”.
Toner et al. (2013) contrast the two theories. They explain that the theory of ironic processes of mental
control suggests that an instruction not to act in a particular way may result in that very action being
taken, especially under cognitive load; however, the implicit overcompensation hypothesis predicts that
instructions to avoid a behaviour lead to the opposite action regardless of cognitive load. Toner et al.
(2013) concluded from their research (using golfers as subjects) that unskilled players were more likely
to overcompensate than more experienced players.
Transport Accident Investigation Commission research, 26 February 2014
References
LoRusso, J. E. (2009).
Ironic Processes of Mental Control of Action in Tennis. (MS, Master of Science),
Florida State University. Retrieved from http://diginole.lib.fsu.edu/etd/1037.
Toner, J., Moran, A. P. & Jackson, R. (2013). The effects of avoidant instructions on golf putting
proficiency and kinematics
. Pre-publication version of article published in
Psychology of Sport
and Exercise, 14(4), 501-507. Retrieved from
Final Report AO-2013-010 | Page 29
http://researchrepository.ucd.ie/bitstream/handle/10197/4295/Toner,_Moran_%26_Jackson_
2013.pdf?sequence=1.
Wegner, D. M. (1994). Ironic processes of mental control.
Psychological Review, 101(1), 34-52.
Wegner, D. M. (2009, 3 July 2009). How to think, say, or do precisely the worst thing for any occasion.
Science, 325, 48-50.
Wegner, D. M., Ansfield, M. & Pilloff, D. (1998). The putt and the pendulum: ironic effects of the
mental control of action.
Psychological Science, 9(3), 196-199.
Page 30 | Final Report AO-2013-010

Recent Aviation Occurrence Reports published by
the Transport Accident Investigation Commission
(most recent at top of list)
Addendum to final Mast bump and in-flight break-up, Robinson R44, ZK-IPY, Lochy River, near
report
Queenstown, 19 February 2015
AO-2015-002
Interim Report
Collision with terrain, Eurocopter AS350-BA, ZK-HKW, Port Hills, Christchurch, 14
AO-2017-001
February 2017
AO-2013-011
Runway excursion, British Aerospace Jetstream 32, ZK-VAH, Auckland Airport,
2 November 2013
AO-2014-006
Robinson R44 II, ZK-HBQ, mast-bump and in-flight break-up, Kahurangi National
Park, 7 October 2014
Interim Report
Collision with terrain, Robinson R44, ZK-HTH, Glenbervie Forest, Northland, 31
AO-2016-007
October 2016
AO-2014-004
Piper PA32-300, ZK-DOJ, Collision with terrain, Near Poolburn Reservoir, Central
Otago, 5 August 2014
AO-2015-002
Mast bump and in-flight break-up, Robinson R44, ZK-IPY, Lochy River, near
Queenstown, 19 February 2015
AO-2013-008
Boeing 737-300, ZK-NGI, Loss of cabin pressure, near Raglan, Waikato,
30 August 2013
AO-2013-003
Robinson R66, ZK-IHU, Mast bump and in-flight break-up, Kaweka Range,
9 March 2013
AO-2014-002
Kawasaki BK117 B-2, ZK-HJC, Double engine power loss, Near Springston,
Canterbury, 5 May 2014
AO-2013-006
Misaligned take-off at night, Airbus A340, CC-CQF, Auckland Airport, 18 May 2013
AO-2010-009
Addendum to Final Report: Walter Fletcher FU24, ZK-EUF, loss of control on take-off
and impact with terrain, Fox Glacier aerodrome, South Westland, 4 September 2010
AO-2012-002
Airbus A320 ZK-OJQ, Bird strike and subsequent engine failure, Wellington and
Auckland International Airports, 20 June 2012
AO-2013-005
In-flight loss of control, Robinson R22, ZK-HIE, near New Plymouth, 30 March 2013
AO-2013-007
Boeing 737-838, ZK-ZQG, stabiliser trim mechanism damage, 7 June 2013
Price $16.00
ISSN 1179-9080 (Print)
ISSN 1179-9099 (Online)