
133 Molesworth Street
PO Box 5013
Wellington 6140
New Zealand
15 November 2022
T+64 4 496 2000
Sebastian
By email: [FYI request #16691 email]
Ref:
H2022014883
Tēnā koe Sebastian
Response to your request for official information
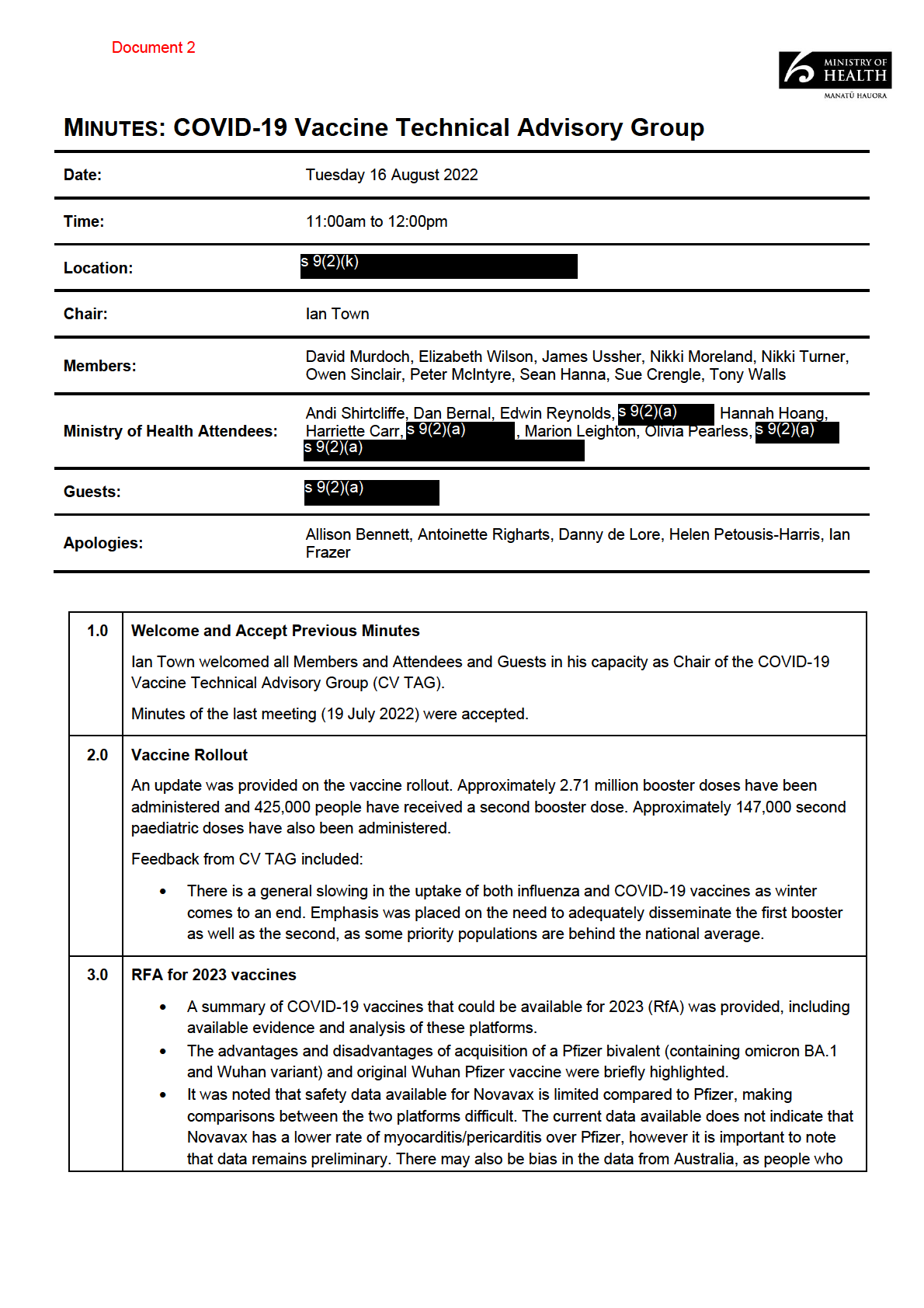
Thank you for your request under the Official Information Act 1982 (the Act) to Manatū
Hauora (the Ministry of Health) on 17 October 2022 for information regarding the COVID-19
Vaccine Technical Advisory Group (CV TAG). Each part of your request is responded to
below:
For the COVID-19 Vaccine Technical Advisory Group I would like to request copies of:
All meeting minutes dated since 22 June 2022
Manatū Hauora has identified four sets of relevant CV TAG minutes within scope of this part
of your request. All documents are itemised in Appendix 1 and copies of the documents are
enclosed. Where information is withheld under section 9 of the Act, I have considered the
countervailing public interest in releasing information and consider that it does not outweigh
the need to withhold at this time.
All memos or reports they have produced since 22 June 2022
All CV TAG memos within this timeframe are publicly available at:
www.health.govt.nz/about-ministry/leadership-ministry/expert-groups/covid-19-vaccine-
technical-advisory-group-cv-tag. CV TAG does not produce reports. Therefore, this part of
your request for is refused under section 18(e) of the Act.
I trust this information fulfils your request. Under section 28(3) of the Act, you have the right
to ask the Ombudsman to review any decisions made under this request. The Ombudsman
may be contacted by email at:
[email address] or by calling 0800 802 602.
Nāku noa, nā
Dave Henderson
Interim Group Manager, Intelligence, Surveillance and Knowledge Public Health Agency | Te Pou Hauora Tūmatanui
Appendix 1: List of documents for release
#
Date
Document details
Decision on release
1
19 July 2022
COVID-19 Vaccine TAG Minutes Some information withheld
under the following sections
of the Act:
•
section 9(2)(a) to
protect the privacy of natural
persons.
•
section 9(2)(k) to
prevent the disclosure or use
of official information for
improper gain or advantage.
2
16 August 2022
COVID-19 Vaccine TAG Minutes
3
13 September 2022 COVID-19 Vaccine TAG Minutes
4
11 October 2022
COVID-19 Vaccine TAG Minutes
Page 2 of 2
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
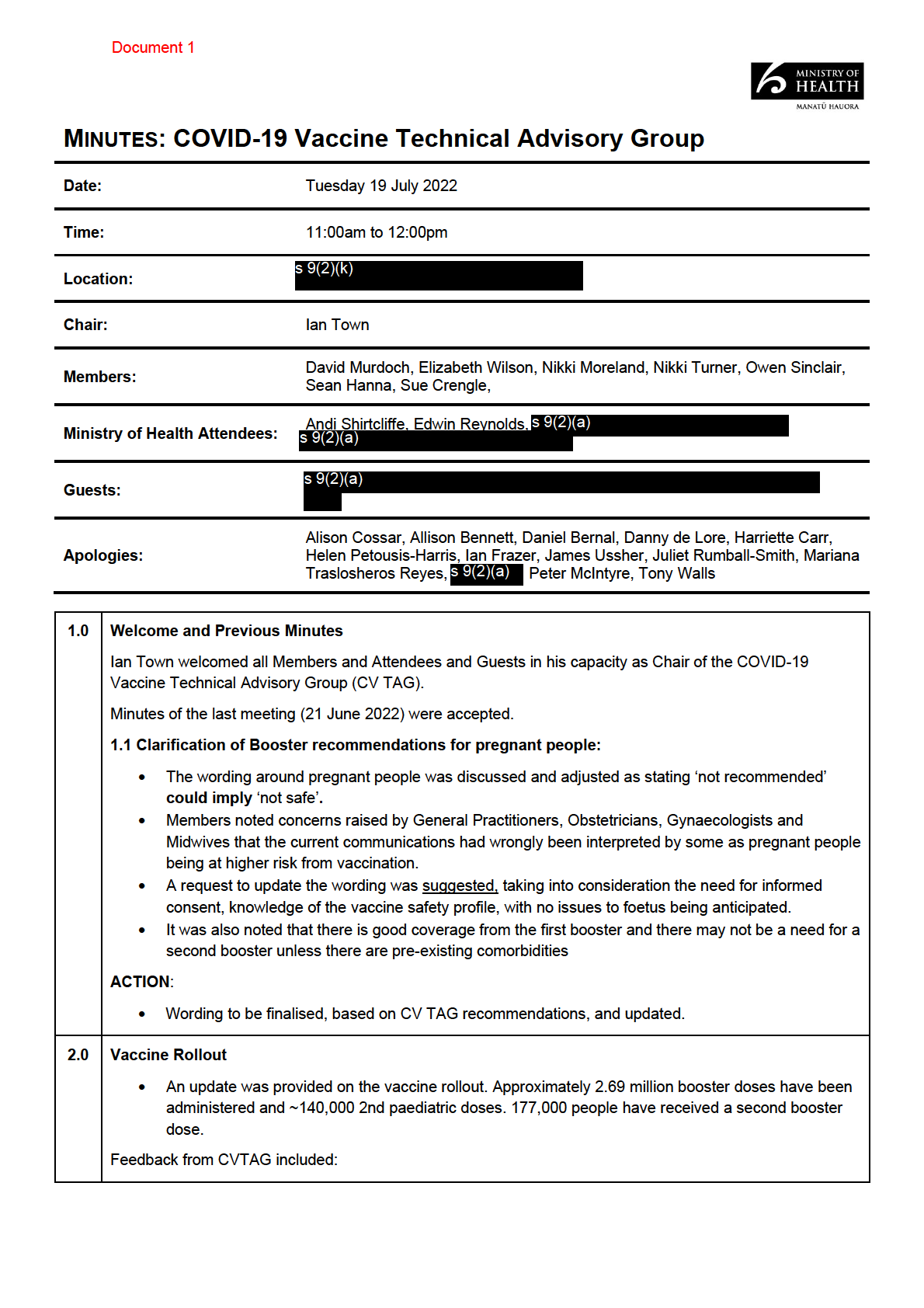
Document 1
•
A member noted the lower uptake in influenza vaccinations for the over 65’s in the Asian population
and requested more data if available. In addition to this, data on uptake from disabled people is also
desired.
•
Members expressed concern in the uptake of vaccination among Pacific Peoples.
ACTION:
•
Collate data on flu vaccination uptake in the following groups: 65+, Asian and disabled people.
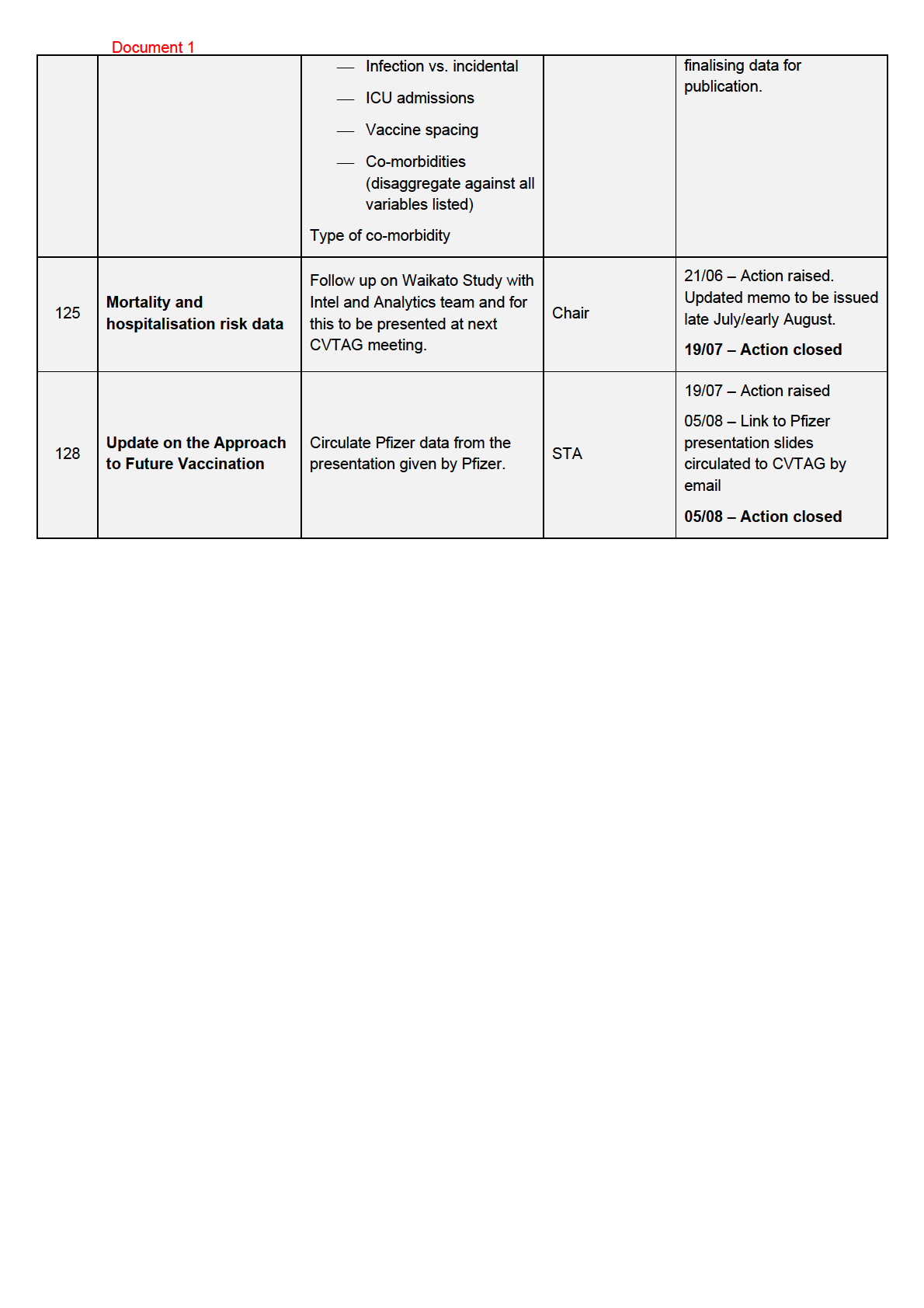
3.0 Mortality and Hospitalisation Risk Data
•
An update on the mortality and hospitalisation risk data was provided. The data showed that mortality
and hospitalisations are increasing for those aged 60 years and over and there have been a
substantial number of infections in those aged 65 years and over compared to first wave.
•
The mortality risk in age-adjusted populations was found to be 2.4 times higher in Māori and 3.6
times higher in Pacific Peoples than other ethnicities.
•
Unvaccinated people were 3 times more at risk of death than boosted individuals. Co-morbidi
1982ty and
high deprivation were also highly associated with mortality.
•
Vaccination was strongly associated with a lower-case fatality risk. 50% of al deaths in 20-to-60-
ACT
year-olds could have been avoided if boosted.
Feedback from CVTAG included:
•
Members commented on the value of this data in a New Zealand setting and its importance to
support the vaccination campaign. Members emphasised that this should be used to strengthen the
communications on vaccine effectiveness.
ACTION:
INFORMATION
•
A breakdown of the mortality and hospitalisation risk data was requested, broken down by disability,
and age, with a comparison to influenza by age and ethnicity.
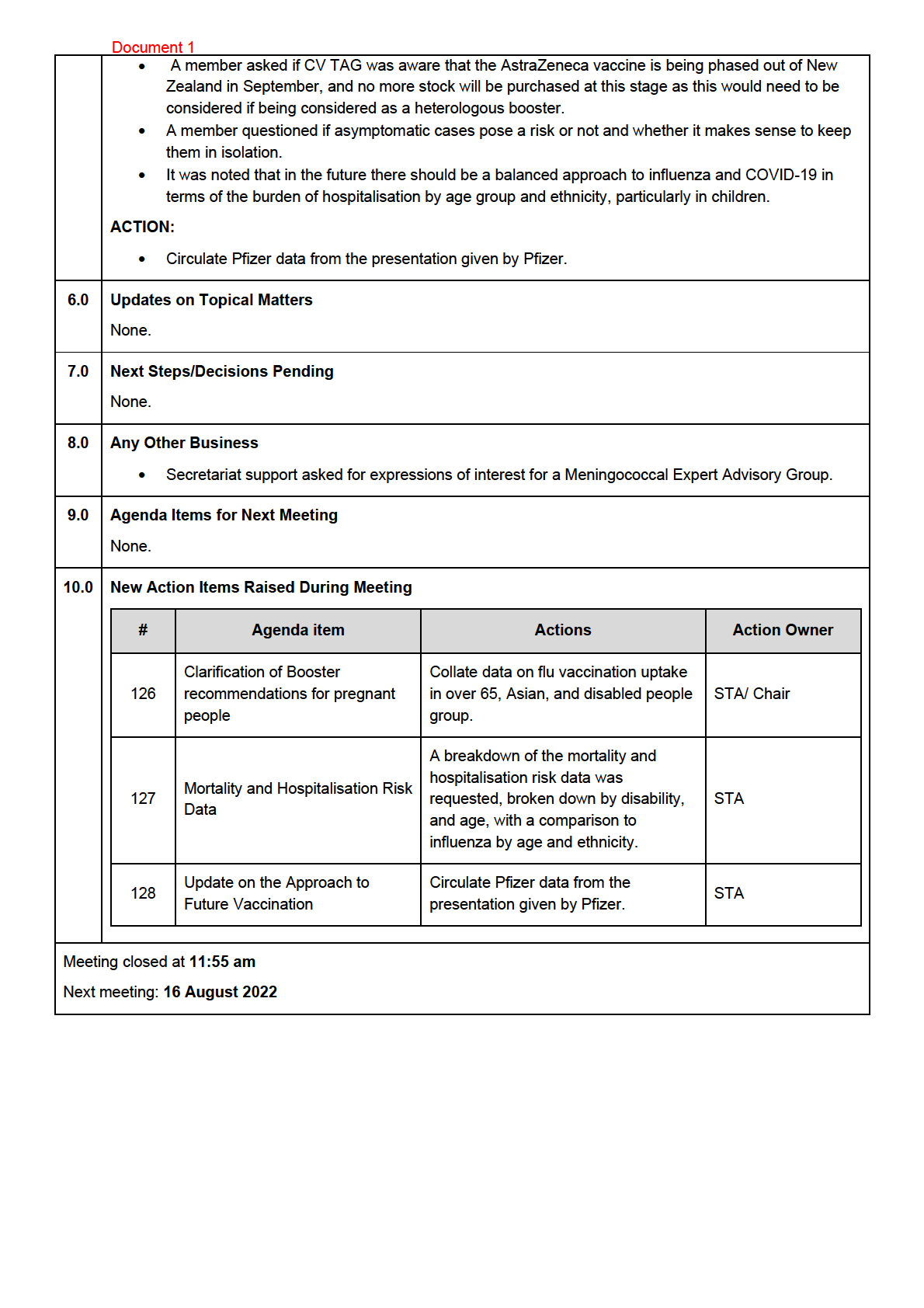
4.0 Booster Uptake Data
•
An update on booster uptake adjusted for COVID-19 infection in the previous 3 months was
OFFICIAL
provided. The data showed a minimal difference between groups adjusted for infection compared to
no adjustment.
•
There was concern about Māori aged
THE 50 to 65, as only 76% have received a booster from those
eligible (78% if excluding people who have tested positive in the last 3 months).
Feedback from CVTAG included:
•
Roll out of second boosters has influenced increasing uptake of first booster doses and paediatric
UNDER
second doses.
•
There stil needs to be more effort directed towards increasing booster uptake among Māori and
Pacific Peoples.
5.0 Update on the Approach to Future Vaccination
•
A verbal update of
RELEASED the status of the Future Vaccination plan was given. The cabinet paper wil outline
the approach for the next 12 months. This wil include 2 key elements: the vaccination approach for
2023 and the vaccination approach for 2024.
Feedback from CVTAG included:
•
The Chair noted that the 2024 vaccination taskforce wil include a wider group to include research
scientists, vaccine manufacturers and international perspectives.
•
A member noted that heterologous boosting may have a role in the coming months, noting that
beyond 6 months, immunity waning against severe symptoms in younger populations may occur.
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
hav
Document 2 e already presented with myocarditis from Pfizer may be more routinely recommended
Novavax for their next dose.
Feedback from CV TAG included:
• Members noted there is little gain for a bivalent BA.1 vaccine as the cases in New Zealand are
predominantly (~85%) BA.5. It would be more suitable for a BA.4/BA.5 bivalent vaccine if that is
to become available.
• One member raised the option of BA.4/BA.5 bivalent vaccines (once available) to be used to
target high-risk groups.
• One member noted concerns of increasing reactogenicity of Novavax per dose.
• There was discussion of the role that heterologous boosting may play in the future, in particular
the potential advantage of Novavax as a heterologous booster, following a primary course of
Pfizer. However, it was noted that currently data are scarce for supporting this.
• Further uptake of future vaccines remains a concern. A combined COVID-19 and influenza
vaccine may have a large impact on the uptake of both flu and COVID-19 vaccination rates, as
these rates are becoming a growing concern as “COVID-19 fatigue” sets in.
1982
• Additional consideration for the document:
o
there needs to be consideration on whether it is worth waiting for BA.4 or BA.5 vaccines,
ACT
bearing in mind global supply and order of country priority
o
it should be considered whether these variant specific vaccines would be for all groups or
just those at higher risk
o
real world clinical data is stil needed but recommendations can be made on what is
currently known from the limited studies available
• Further details on the Waikato study were requested as this is being extended to include additional
hospitals. The breakthrough infection data could provide valuable insight on vaccine efficacy
considering the circulating variants and the hybrid immunity landscape of New Zealand.
INFORMATION
Action: Chair to follow up with data for the Waikato study when this becomes available and report back
to CV TAG
4.0 Novavax in 12–17-year-olds
An overview of the evidence for first doses of Novavax in 12
OFFICIAL –17-year-olds was presented.
Data are currently scarce, however, data available shows there is similar immunological responses and
trial-based efficacy of 12–17-year-olds com
THE pared to 18-25-year-olds vaccinated with Novavax. There is
no comparison with Pfizer. Safety data including data on myocarditis/pericarditis are still limited but
appear similar to Pfizer.
Feedback from CV TAG included:
UNDER
• A member noted that this is not a high-risk group, however, having an additional option available
over Pfizer is valuable.
• Concern was noted surrounding the results of the limited myocarditis data available to date.
Noting that while this is of concern, Novavax should stil be made available for this age group for
those that choose to have it, albeit not “recommended”. Pfizer remains the preferred vaccine for
COVID-19.
RELEASED
• It was noted that considering the current data, there is a selection bias as individuals who present
with myocarditis from a Pfizer vaccination, are routinely recommended Novavax as their next
dose in Australia.
• More long-term and local data on myocarditis is needed to examine the outcomes and long-term
effect it has on people.
• For those seeking Novavax as a booter in this age group can obtain it via prescription with
informed consent.
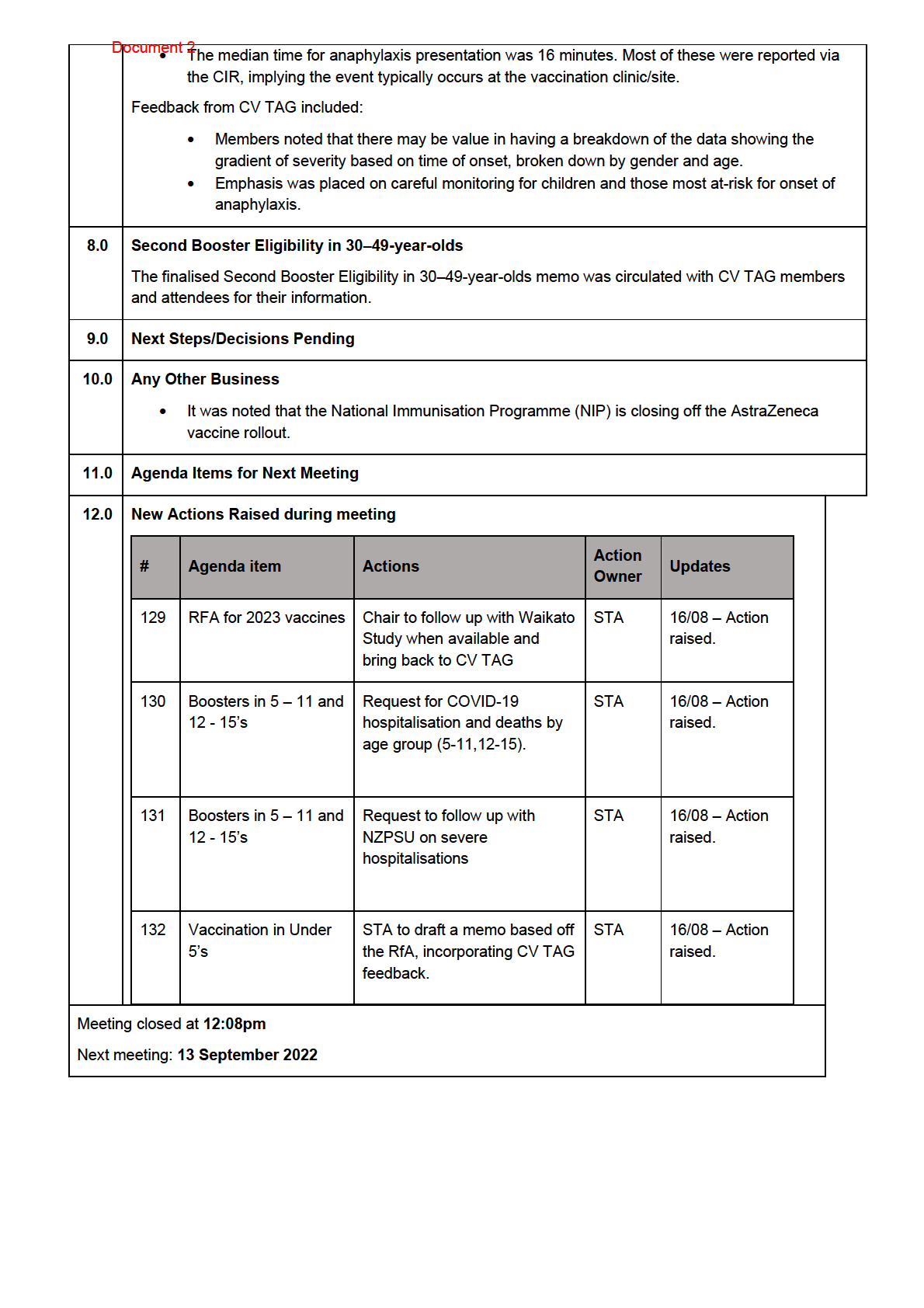
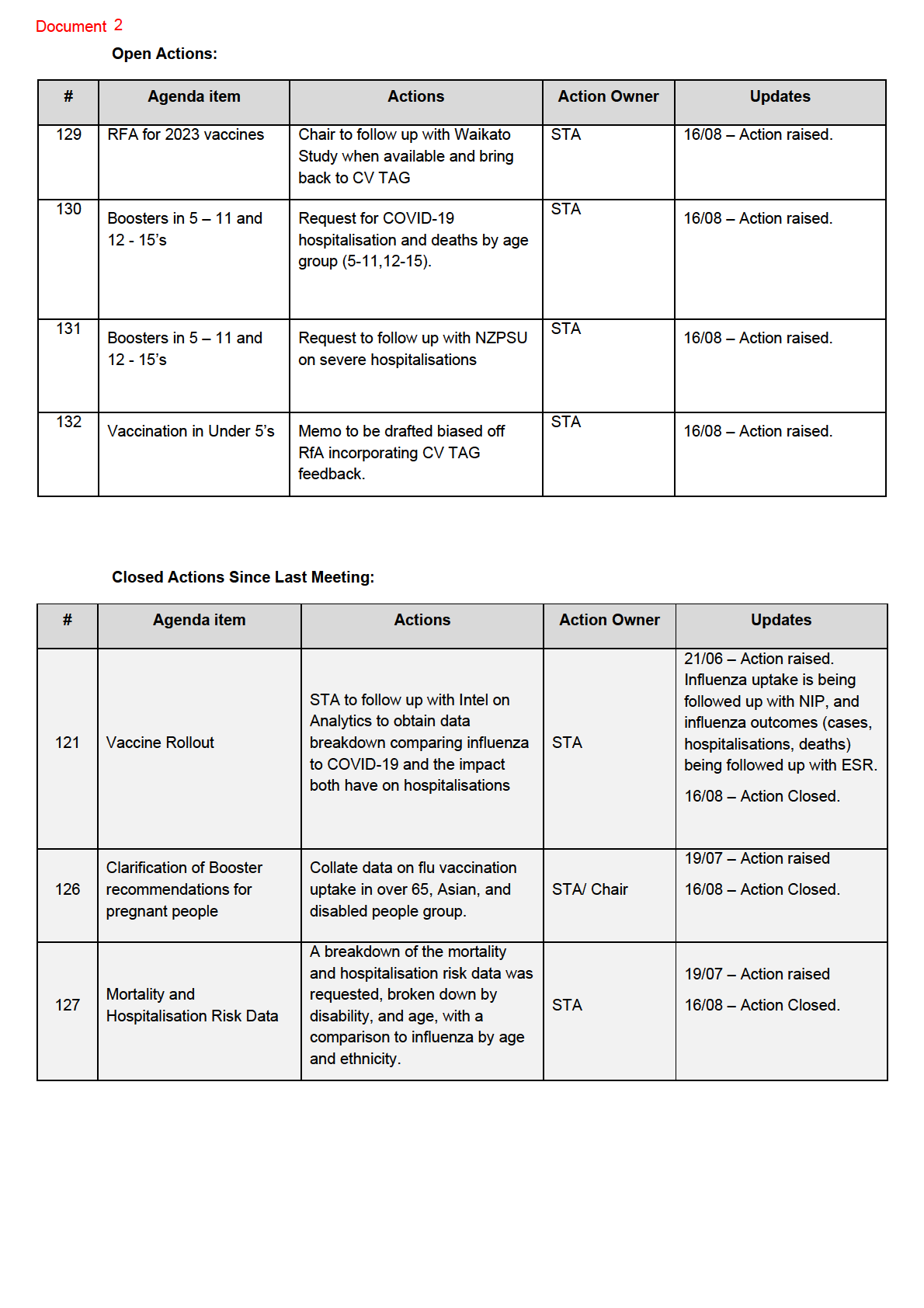
5.0 Boosters in 5 – 11 and 12 - 15’s
• T
Document 2here was a brief verbal discussion on boosters in children aged 5 - 11 and 12 - 15. No new
significant evidence has arisen in this area, CV TAG agreed that boosters in this age group are
not necessary at this time.
• A CV TAG member noted that NZ data on morbidity and mortality in 5 – 11 and 12- to 15-year-
olds would better inform decisions for this age group. This wil also provide a better understanding
on what effect vaccination has in 5 – 11- and 12–15-year-olds with high-risk conditions and how
many if any are being hospitalised and at what rate.
Action: Request for COVID-19 hospitalisation and deaths by age group (5-11,12-15).
Action: Request to follow up with The New Zealand Paediatric Surveil ance Unit (NZPSU) on severe
hospitalisations in these age groups
6.0 Vaccination in Under 5’s
A submission for the use of the paediatric Pfizer vaccine in children aged 6 months to 4 years is expected
to Medsafe this month. A summary of the RfA covered the latest national and international data on
1982
mortality and hospitalisation in this age groups as wel as peak body advice.
Use of both Moderna and Pfizer vaccines for this age group were covered in the RfA, however, the use of
ACT
Moderna is not in consideration at this stage.
Feedback from CV TAG included:
• Members noted that this is more associated with a policy decision and reaffirmed that
vaccinations in under-fives is not clinically recommended at this time, particularly given the low
risk of adverse outcomes from COVID-19 infection for this age group and likely high proportion of
prior exposure given the recent outbreaks in New Zealand.
• It was raised whether this vaccine should be made available for children most at –risk (i.e.,
INFORMATION
severely immunocompromised). It was noted that this may need to be considered at a later stage.
• Members noted that there is some public concern from parents of under-fives. This indicates a
need for publicly available data to show that this age group is relatively unaffected by severe
outcomes from COVID-19 and not subject to an increase in mortality compared to older age
groups.
• As there are observed delivery challenges in at-ris
OFFICIAL k groups, an influenza vaccine uptake
comparison in this age group could be useful in determining the effectiveness of under-five’s
COVID-19 vaccine rol out.
THE
• The lack of information and data on transmission in under-fives were noted, along with what
impact vaccination wil have on this.
• It was noted that a further break down of the hospital data from “under 9’s” is needed, however,
there is limited data due to severe illness being uncommon in this age group.
UNDER
Action: STA to draft a memo based off the RfA, incorporating CV TAG feedback.
7.0 Change in Post-vaccine Observation Time and the Detection of Anaphylaxis
Data and the impacts of the reduction in post-vaccination observation time from 20 minutes to 15 was
presented. This focussed on the rates of anaphylaxis along a time scale over 12 months.
RELEASED
• Al cases were reviewed by the medical assessors at CARM and the study was conducted using
the Brighton criteria.
• In a six-month period (with a 20 minute observation) 2.7 mil ion vaccinations were given, 31
people showed signs of anaphylaxis (1 in 90,000). 71% of which occurred during the 20 minute
observation period.
• In the next six-month period (with a 15 minute observation) there were more vaccinations given
and more cases of anaphylactic response, but at a lower proportion of all vaccinations, resulting
in a rate of 1 in 100,000 however only 47% of cases occurred in the 15 minutes observation
period. No deaths were reported.
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 3
Action: Stratified analysis of mortality broken down into those who had co-morbidities compared to
those without.
4.0 Influenza hospitalisation data
Hospitalisation data of severe acute respiratory il ness associated with influenza and COVID-19 was
presented.
Feedback from CV TAG included:
•
Accumulated data might not present peaks of hospitalisations caused by influenza
•
Need to consider peaks of ED presentations, along with hospitalisations
Action: Additional influenza data was requested for children under the age of 1 year and children aged
1-5 years, broken down by ethnicity, by month and in comparison to COVID-19 and ED presentations
5.0 Update on second boosters
The Chair advised that there has been no change to the age threshold for Māori to access second
1982
boosters. Current discussions in other countries about bivalent vaccines wil likely be reviewed in NZ
over summer in preparation for autumn 2023.
ACT
Feedback from CV TAG included:
•
The need to consider COVID-19/flu combination vaccines as part of service delivery
6.0 Update on COVID-19 Strategic Vaccine Taskforce
The Taskforce wil pause for the moment and members wil be kept informed about the strategy focus.
The activities of CV-TAG are expected to continue in the current form until the end of the year, before
INFORMATION
transitioning to the TAG for the National Immunisation Programme (NIP). This TAG wil be focused on
providing operational and technical recommendations on immunisation.
Airfinity wil be presenting on future vaccine platforms and technologies, with CVTAG members invited
for the next meeting
OFFICIAL
7.0 NZPSU Data on severity of COVID-19 among children
Data from the New Zealand Paediatric Surveil ance Unit (NZPSU) on admissions of children aged 0-15
THE
years to intensive care units (ICU) between 1 January and 30 June 2022 were presented.
Severe COVID-19 led to 29 ICU and PIMS-TS / MIS-C (Paediatric inflammatory Multisystem Syndrome
temporally associated with SARS-CoV-2) (Multisystem Inflammatory Syndrome in Children) admissions
and two deaths (COVID-19 secondary diagnosis).
UNDER
Feedback from CV TAG included:
•
Consideration into the role of obesity as a factor for admissions to ICU.
8.0 Update on Medsafe myocarditis Study
A Medsafe staff member gave a status update of the study which includes people aged 12+ years who
RELEASED
experienced a case of myocarditis or pericarditis after receiving any dose of COVID-19 vaccine. Cases
were identified through the Centre for Adverse Reactions Monitoring (CARM) and will be fol owed up for
a minimum of three months after onset of il ness.
The recruitment phase has finished and results from the consumer survey (n=300, response rate of
68%) are expected by end of October; the health care professionals survey (n=143, response rate of
49%) is expected follow afterwards.
An additional sub-analysis based on CDC criteria wil be performed to make results internationally
comparable.
Prescriber alert for Nuvaxovid issued by Medsafe
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED