Office of the Associate Minister of Transport
Chair
Cabinet Economic Growth and Infrastructure Committee
ADDITIONAL MEASURE TO ADDRESS DRUG-DRIVING
Proposal
1.
I propose that New Zealand introduce an additional drug testing process for drivers who are
suspected of either having committed a driving offence or have been involved in a motor
vehicle crash. The testing process would be an oral fluid screening test at the roadside. The
new testing process would be available alongside the current impairment testing process.
Executive summary
2.
The road toll for the year to 2 November 2016 is 271, which is 9 higher than for the same
period last year. While it is still too early to determine the factors that may have contributed to
the increase, this emphasises the need for a continued Government focus on interventions
that are likely to reduce road trauma. Addressing drug-driving is an important objective.
3.
The Government has previously considered the effectiveness of the drug-driving enforcement
regime, and has received several reports on drug-driving (for example, EGI Min (12) 7/2, EGI
Min (10) 4/5 and EGI-16-MIN-0059 refer). The Ministry of Transport (the Ministry) reviewed
the extent of New Zealand’s drug-driving problem and the effectiveness of the current drug-
driving enforcement model. This drug-driving review originates from the Safer Journeys Action
Plan 2013-15, which includes investigating opportunities to strengthen the existing drug-
driving enforcement model.
4.
The review estimated that the drug-driving problem has a social cost of between $96.8 million
and $731.4 million per annum, with a central estimate of $250.5 million. The central estimate
translates to approximately 23 deaths, 112 serious injuries, and 304 minor injuries per year.
The social cost was estimated using several sources, such as New Zealand crash data,
studies of New Zealand deceased drivers and international research.
5.
The Ministry reported its findings on the review to me on 31 July 2015. In response, I am
recommending changes to the drug-driving enforcement regime to help minimise the harm
resulting from drug-driving.
6.
The current drug-driving testing regime is an impairment-based approach. It relies on a Police
officer forming good cause to suspect a driver has used a drug or drugs before carrying out a
behavioural test to determine if the driver is impaired. An evidential blood test is then required
to secure a conviction. The behavioural test is called the Compulsory Impairment Test (CIT).
It consists of pupil dilation, standing on one leg and walk and turn assessments. The
combination of the need to find good cause and the practicalities of carrying out the CIT mean
that few tests are carried out. There is little deterrence value in the current approach.
Page 1 of 29
8j3h8arqdt 2019-06-17 11:30:20
7.
To help reduce drug-driving, I recommend a new drug-driving testing process be introduced.
This process would allow the Police to use oral fluid screening devices to drug test drivers
following an incident. This process would be applied where drivers are suspected of having
committed a driving offence or have been involved in a motor vehicle crash. The Police officer
would not need to first establish good cause to suspect a driver has used a drug or drugs
before testing the driver for drugs. The screening process would be carried out at the
roadside.
8.
The new regime would allow a much larger number of drug tests to be conducted, which
would help deter drug-driving.
9.
Under the proposed process, drivers would be required to undergo an oral fluid screening
test. If that first test were positive, a second oral fluid test would be undertaken. If the second
test were positive, an evidential blood test would be taken. The presence of drugs in the blood
sample would be sufficient evidence for an offence. Each oral fluid test would take around 3-5
minutes to complete.
10.
I propose that the drugs to be detected under the oral fluid testing regime (‘specified drugs’)
be approved by Order in Council. This allows the range of drugs to be changed should
technological developments allow for more drugs to be detected, or if the patterns of drug use
change. Initially, I propose oral fluid screening for THC (the active ingredient in cannabis),
methamphetamine and MDMA (ecstasy).
11.
A limitation of oral fluid screening devices is that they can only test for a limited number of
drugs. Consequently, Police officers would still have access to the impairment testing process
in cases where other drugs are involved, if they first form good cause to suspect a driver has
used a drug or drugs.
12.
Unlike the impairment testing process, oral fluid screening cannot determine whether a driver
is impaired. As a result, I propose an infringement offence for those drivers tested under this
presence-based testing process. This does not involve a criminal conviction. A driver would
receive a $200 infringement fee plus 50 demerit points.
13.
Once fully implemented, the regime would cost around $9 million per annum (with 45,000
tests carried out per annum). Most costs would fall to the Police. Additional costs to the Police
would not be able to be met within existing resources. Funding would need to be made
available by a variation to the Road Policing Programme under the National Land Transport
Programme. First year funding can be provided by reprioritising funds from within the National
Land Transport Fund. Funding for subsequent years will need to be accommodated within the
road policing activity class in the upcoming Government Policy Statement on land transport
2018.
Current drug-driving problem
14.
The Ministry estimates that drug-driving has a social cost of between $96.8 million and $731.4
million per annum, with a central estimate of $250.5 million. The central estimate translates to
approximately 23 deaths, 112 serious injuries, and 304 minor injuries per year. By
comparison, in 2015, there were 78 alcohol-related deaths, 403 serious injuries and 1,189
minor injuries.
15.
Three data sources were used to estimate the scale of the drug-driving problem: data from
New Zealand’s Crash Analysis System (CAS) that includes all traffic crash data reported by
the Police, data from the United Kingdom, and a 2014 New Zealand Environmental Science
and Research (ESR) study of drivers killed in road crashes.
Page 2 of 29
8j3h8arqdt 2019-06-17 11:30:20
16.
Unlike alcohol, there is no comprehensive data showing the relationship between the dosages
of various drugs, the level of impairment and crash risk. The World Health Organisation notes
a meta-analysis that compiled information from 66 studies showed an increase in the risk of
crashes for 11 different drugs1. However, it is not possible to disaggregate the social cost and
attribute it to particular drugs and dosages, when taken on their own or in combination with
others.
Empirical evidence of drug-driving in New Zealand
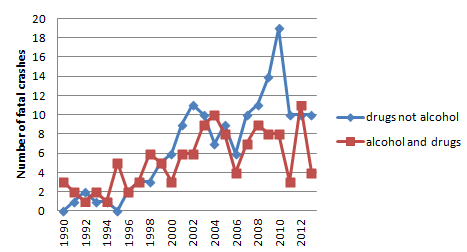
17.
CAS data shows the number of fatal crashes occurring where a driver has consumed drugs.
Although the numbers are small and subject to fluctuations, Figure 1 below outlines that the
number of fatal crashes occurring where drivers have consumed drugs is now higher than in
the 1990s.
Figure 1 – Fatal crashes with drugs (or combined with alcohol) 1990-2013
18.
An ESR study of at-fault deceased drivers found that of 1,046 deceased driver blood samples
analysed, 500 (48 percent) of the deceased drivers had alcohol or other drugs in their blood
that may have impaired their ability to drive safely. Of the 500 drivers, 92 (18 percent) had
used cannabis alone, 142 (28 percent) had used a combination of alcohol and cannabis, and
127 (25 percent) had used some other combination of drugs. While the study does not prove
that the deceased drivers were impaired by drugs when they crashed, it does indicate that
they had used drugs within the 24 hour period before the crash. In this study, ESR tested for
the active ingredient in cannabis. It did not test the blood samples for inactive drug
compounds that can remain detectable in blood samples for days or weeks later.
19.
Another ESR study analysed blood samples taken from 1,999 drivers who had an evidential
blood sample taken as part of the alcohol testing process (but had not been injured in a
crash). The samples were screened for evidence of the use of a limited range of drugs other
than alcohol. The analysis found that 35 percent had used cannabis as well as alcohol, and 2
percent had used alcohol and some other drug.
1
Global Status Report on Road Safety 2015; World Health Organization: p.40
Page 3 of 29
8j3h8arqdt 2019-06-17 11:30:20
20.
There are several studies pointing to the prevalence of the use of certain drugs generally and
in driving. The Ministry of Health’s 2007/08 New Zealand Alcohol and Drug Use Survey found
the most commonly used recreational drugs in the 12 months before the survey were
cannabis (14.6 percent), BZP party pills (5.6 percent), MDMA (2.6 percent), and
amphetamines (2.1 percent). In that year, buying BZP party pills was legal, so the number of
people using BZP has likely dropped since then.
21.
In 2014, the Ministry introduced a new question about driving while affected by drugs with or
without alcohol, to the Ministry’s Public Attitudes to Road Safety survey. Nine percent of
participants said they had driven while affected by prescription or pharmacy drugs, including 2
percent combined with alcohol. Four percent said they had driven while affected by other
drugs (whether legal or not), including 2 percent combined with alcohol.
22.
The Ministry of Health’s Cannabis Use 2012/13: New Zealand Health Survey found that 11
percent of adults reported using cannabis in the 12 months before the Survey. Of this 11
percent, 36 percent of cannabis users reported driving under the influence of cannabis in the
last 12 months. This equates to around 133,000 adults. Men were 1.5 times more likely than
women to report they had driven under the influence of cannabis.
Drug-driving enforcement regimes have three elements: the criteria for testing, the testing
process, and the sanctions
23.
The three main elements of any drug-driving enforcement regime are:
23.1. Element 1: the criteria the Police apply at the front-end of the process to determine
which drivers will be tested
23.2. Element 2: the testing process the Police follow once they have decided to test a
driver
23.3. Element 3: the legal process and sanctions that apply to drivers who fail the drug
testing process and are therefore considered to have committed a drug-driving
offence.
24.
For the three elements outlined, the different approaches that can be implemented for each
are discussed in the sections below.
Element 1: Possible criteria to determine which drivers to test
25.
There is a spectrum of possible criteria, or circumstances, under which a Police officer could
be permitted to test drivers for drugs. The criteria represent a threshold that must be crossed
before a test can be carried out. A high threshold can limit the number of tests that can be
undertaken. The two ends of the spectrum are outlined below.
Non-random (good cause to suspect) testing
26.
This is the current criterion used for New Zealand’s drug testing regime and requires a Police
officer to form good cause to suspect a driver has used a drug or drugs before testing them.
Using this criterion to initiate testing has the advantage of ensuring drivers are not
unreasonably detained or tested.
Page 4 of 29
8j3h8arqdt 2019-06-17 11:30:20
27.
The Police state that there is a high evidentiary threshold for establishing good cause to
suspect and that establishing good cause to suspect can be difficult for the Police. A Police
officer must explicitly identify a reason to suspect a driver has potentially used drugs. This
threshold means that it is likely that there are a number of drug impaired drivers who are not
being tested and sanctioned. It also limits the size of any deterrent effect arising from the
testing process as only a small number of drivers meet the threshold and can be tested.
Random testing
28.
Random testing lies at the opposite end of the spectrum. Under a random testing regime, a
Police officer could stop and drug test any driver who is driving a motor vehicle on a public
road. No reason is needed, such as good cause to suspect the driver has used a drug or
drugs.
29.
While Police officers can randomly test drivers for alcohol, they cannot randomly test them for
drugs. In practical terms, random drug testing would involve stopping drivers at checkpoints
and compulsorily testing them. Under random testing regimes, it is important that drivers are
not held up for an undue amount of time and roadside tests are undertaken promptly to
ensure reasonable numbers of drivers can be processed.
30.
Random testing is promoted as best practice for increasing deterrence because it is the best
way to increase public perception of the risk of being caught. However, it may limit rights
outlined in the New Zealand Bill of Rights Act 1990 (NZBORA), such as the right not to be
subjected to arbitrary detention, unreasonable search and seizure, and the right to be
presumed innocent until proven guilty. The justification for restricting these rights will depend
on whether what is proposed is a proportionate and rational response to the problem being
addressed.
Element 2: Possible drug testing approaches that could be conducted on drivers
31.
There are two main approaches to drug testing that can be used on drivers: behavioural
impairment-based testing and presence-based testing. Both of these methods have
advantages and disadvantages. These testing methods are outlined below.
An impairment-based approach
32.
The advantage of an impairment-based approach is that a behavioural test is used to
demonstrate that drivers are impaired. This is the approach currently used in New Zealand for
drug-driving enforcement. The behavioural test used is called the Compulsory Impairment
Test (CIT). If a driver’s performance on the CIT is unsatisfactory, they may be required to
undergo a blood test. The presence of a ‘qualifying drug’ confirms an offence has been
committed. Qualifying drugs are found in the schedules of the Misuse of Drugs Act 1975.
Prescription medicines are also qualifying drugs. The list of qualifying drugs is long and this
approach addresses the use of a wide range of drugs that can impair driving. The impairment
testing process is also effective in dealing with drivers who have used a number of different
drugs.
33.
Impairment testing relies on a Police officer observing behavioural indicators associated with
drug use rather than toxicological analyses of bodily samples, such as blood, to detect the
presence of drugs. The CIT is only able to detect physical forms of impairment that are
directly observable (for example, gross motor dysfunction). Drivers with more subtle forms of
impairment (for example, cognitive impairment) are likely to be missed.
Page 5 of 29
8j3h8arqdt 2019-06-17 11:30:20
34.
There are limitations to the number of CITs that can be undertaken due to the time it takes to
conduct the test and the Police resource required to be taken off the front line to carry it out at
a Police station. The Police will not conduct a CIT at the roadside due to safety issues. The
option of redesigning the CIT has not been investigated, as the current process is considered
best practice.
35.
For these reasons, the number of CITs undertaken each year is low. Police advise that
around 200 tests are not satisfactorily completed per annum, but do not hold data on how
many CITs are conducted overall. A high proportion (90 percent) of blood samples taken after
an unsatisfactory CIT test are positive for the presence of a qualifying drug or drugs. From
November 2009 to December 2013, 1,004 blood tests were taken, of which 903 tested
positive for at least one qualifying drug. The CIT is robust in that it does not over-refer those
drivers who have not taken drugs, for unnecessary blood tests.
A presence-based approach and oral fluid roadside screening
36.
The main alternative to impairment-based testing is to test for the presence of drugs in bodily
fluids without a need to demonstrate that a driver is impaired. Drugs can be detected in a
number of bodily fluids, including blood, urine, and oral fluids. However, unlike alcohol, there
is a less straightforward relationship between the presence of drugs in a driver’s system and
their ability to drive. Consequently, many countries operate a zero tolerance policy in
presence-based regimes.
37.
Presence-based testing can avoid the need to conduct a cumbersome behavioural test.
Therefore, it opens up the possibility of testing a significantly greater number of drivers
because presence-based tests can be carried out at the roadside. Oral fluid testing is
regarded as the most practical and the least invasive method for roadside screening
purposes.
38.
Oral fluid screening could, therefore, be a useful additional tool for the Police to increase the
numbers of tests conducted. There are limitations. Current oral fluid screening devices can
only test for a limited number of drugs and cannot determine the amount of a drugs in a
person’s system. Further, each oral fluid test can take 3-5 minutes.
39.
As well, the result of an oral fluid screening test is not reliable enough to be used for evidential
purposes. While the accuracy of oral fluid screening devices has improved over recent years,
available devices can still produce false positive results (this is where the device incorrectly
indicates the presence of a drug). Newer devices that have recently come on to the market
have addressed the main source of false positives which are due to operator handling errors.
Nonetheless, some false positives can still arise from cross-reactivity of certain substances in
the mouth. Consequently, any failed oral fluid test result at the roadside would have to be
verified by a confirmatory blood test carried out later by an approved forensic laboratory.
40.
Oral fluid testing devices are available, and used in other countries for roadside screening of
drivers. A number of states in Australia operate random oral fluid screening programmes. For
example, Victoria has operated an oral fluid screening programme for over a decade.
Element 3: Possible sanctions for drug-driving
41.
The sanctions that are applied for drug-driving have an effect on deterring this behaviour
especially when combined with other factors such as increasing public perception of the risk
of being caught. The level of the sanction must be credible to signal the community’s
unwillingness to tolerate this form of driving behaviour and proportionate to the nature and
severity of the offending.
Page 6 of 29
8j3h8arqdt 2019-06-17 11:30:20
Criminal penalties
42.
New Zealand’s current penalties for drug impaired driving are criminal penalties that are
imposed by the courts following conviction for the offence. These penalties are aligned to the
court-imposed penalties that apply for drink-driving which is warranted by the demonstrated
impairment involved. These penalties send appropriate signals to the public about drug-
driving. However, the disadvantage of court-imposed penalties is that they impose costs on
the Justice sector to apply and administer the penalties.
Infringement penalties
43.
Infringement offences apply to less serious offences. As they are generally dealt with outside
the court system, they do not result in criminal convictions. They are easier and less costly to
administer. While infringements create a risk that the offending is not taken seriously enough,
they can be made more severe by the addition of demerit points.
New drug-driving enforcement regime needs to increase deterrence
44.
The key to reducing the prevalence of fatal and injury crashes, which involve drugs, is lifting
the level of enforcement. Australian research shows that, as the driver testing rate increases,
the percentage of drivers who are killed because of drug-driving reduces. The reason for this
relationship is that more testing creates a deterrent effect.
45.
Deterrence relies primarily on highly visible Police enforcement and drivers’ perceptions of the
likelihood of being caught, as well as the consequences that follow for a drug driver. Publicity
in the form of advertising also supports the enforcement efforts and, over time, assists to
shape public attitudes that drug-driving is unacceptable.
46.
The current impairment-based testing regime will not deliver enough tests to achieve
significant improvements in road safety outcomes. Therefore, the status quo option of
retaining impairment testing as the only drug-driving testing regime has not been considered
further in this paper. In my view, introducing a presence-based approach using roadside oral
fluid drug testing is the only viable solution for a significant increase in the scale of the drug
screening of drivers currently undertaken. A key decision is the criterion that should be
applied before a Police officer can conduct an oral fluid test.
Four oral fluid testing enforcement regimes have been considered
47.
I have considered four oral fluid testing options. Both the testing process and the penalty
applied to a drug-driver would be the same for each of the four options. The element that sets
each of these options apart, is the criterion that would enable a Police officer to undertake the
testing process. Because each option employs different criteria for initiating testing, the
perceived likelihood of being tested, and therefore the deterrent effect, would vary.
Page 7 of 29
8j3h8arqdt 2019-06-17 11:30:20
48.
The four options are:
48.1. Option 1: Oral fluid drug testing under the current good cause to suspect criterion (a
Police officer has discretion to choose the testing path)
48.2. Option 2: Oral fluid drug testing without good cause to suspect (random testing
carried out at high risk times)
48.3. Option 3: Oral fluid drug testing following a suspected driving offence or a motor
vehicle crash (post-incident testing)
48.4. Option 4: Oral fluid drug testing following a motor vehicle crash (post-crash testing)
49.
Officials considered several drug-driving enforcement regimes, which are described in the
accompanying Regulatory Impact Statement.
Features of oral fluid testing common to all options
50.
Before discussing each of the oral fluid testing options in detail, there are several features that
are common to all of the options.
Impairment-based drug testing to remain available
51.
Oral screening devices can only detect the presence of a limited number of drugs. Therefore,
Police officers would still have access to the impairment testing process under each option.
Double oral fluid testing process required
52.
The best method for mitigating the risk of false positives is for a second oral fluid screening
test to be undertaken at the roadside if a driver fails the first test. If the driver failed the second
oral fluid test, a blood sample would be taken for evidential purposes. Blood testing remains
the most accurate method for identifying a broad range of drugs, is conclusive, and provides
no false positives.
Infringement offence proposed
53.
As a presence-based approach, the oral fluid testing process would not require the Police to
prove impairment. A presence-based offence could lead to drivers who do not present a road
safety risk being sanctioned. Unlike alcohol, there is insufficient research available that clearly
documents the relationship between dosages of various drugs and their impacts on crash risk
and levels of impairment. A good understanding of these relationships would be necessary to
set legal driving limits for drugs. The limitations of proving impairment have been previously
discussed.
54.
To mitigate the risk of unimpaired drivers receiving criminal penalties, an infringement offence
provides a suitable sanction for showing the presence of drugs only, and recognises that
impairment has not been demonstrated. While some drivers who were not impaired may be
sanctioned, the presence-based approach will detect more impaired drivers who are currently
evading enforcement action under the current impairment regime.
55.
An infringement offence would also have a much lower impact on Justice sector costs.
Page 8 of 29
8j3h8arqdt 2019-06-17 11:30:20
56.
Criminal penalties would remain for drivers who are convicted following an impairment test.
Retaining criminal penalties will continue to send the message that driving while impaired on
drugs is unacceptable.
Collection of data
57.
All options would allow the collection of additional information on the use of specified drugs by
drivers who are stopped and tested under the oral fluid testing regime. This information would
be useful to inform future policy development relating to drug-driving enforcement.
Option 1: Introducing oral fluid testing under the current good cause to suspect criterion (not
recommended)
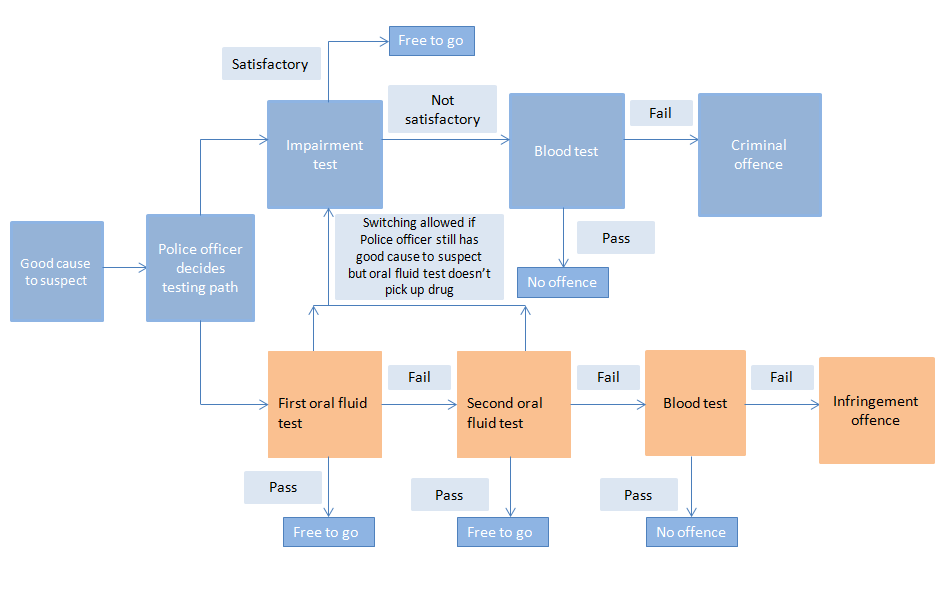
58.
Under Option 1, a Police officer would need to determine that they have good cause to
suspect a driver has used a drug or drugs before conducting any further drug tests. The
Police would then have a choice to initiate either an oral fluid testing process, or follow the
impairment testing process. If the impairment testing path was chosen, the process and
penalty would be the same as under the current impairment regime. The diagram below
outlines the process that could be followed under this regime.
59.
Option 1 has been assessed using a feasible number of tests the Police would be able to
conduct. It is estimated that the current number of tests undertaken for the existing
impairment testing path would remain at the existing rate of approximately 200 each year. For
oral fluid tests, the number able to be undertaken has been estimated at 1,000 tests, which is
five times the number of CITs currently undertaken each year currently. The Police question
whether delivering 1,000 tests per year is attainable due to the good cause to suspect
threshold.
Page 9 of 29
8j3h8arqdt 2019-06-17 11:30:20
60.
While a higher number of tests would be preferable, this regime is based on the Police
identifying sufficient numbers of drivers to test. The main disadvantage of Option 1 is that
introducing oral fluid drug testing under the current good cause to suspect criterion is unlikely
to have an increased deterrent effect and, therefore, will not achieve any significant road
safety benefits.
61.
If oral fluid testing were introduced alongside the impairment testing process, either a criminal
or infringement path would be decided before any test is undertaken. This could lead to a
situation where two people, both impaired, may face different legal consequences based on
the type of test administered by the Police officer at the time.
62.
Once a Police officer had formed good cause to suspect, they would have discretion over
which testing path to apply to a driver. There may be issues of fairness if a Police officer could
switch between testing processes once started given the same threshold applies to both
processes. There is also a risk of legal challenges concerning the criteria the officer used to
follow the impairment testing process rather than oral fluid testing process. This is due to the
difference in the severity of the applicable sanctions.
63.
This potential inconsistency is difficult to reconcile. If oral fluid testing is introduced,
infringement penalties are preferable, as impairment is not demonstrated. Downgrading the
criminal penalty for the impairment testing path has not been considered as this might send a
message that driving while impaired on drugs is not a serious offence.
64.
Option 1 raises a number of issues, without providing a satisfactory deterrent effect.
Option 2: Oral fluid drug testing without good cause to suspect drug use (random testing)
targeted to risk (not recommended)
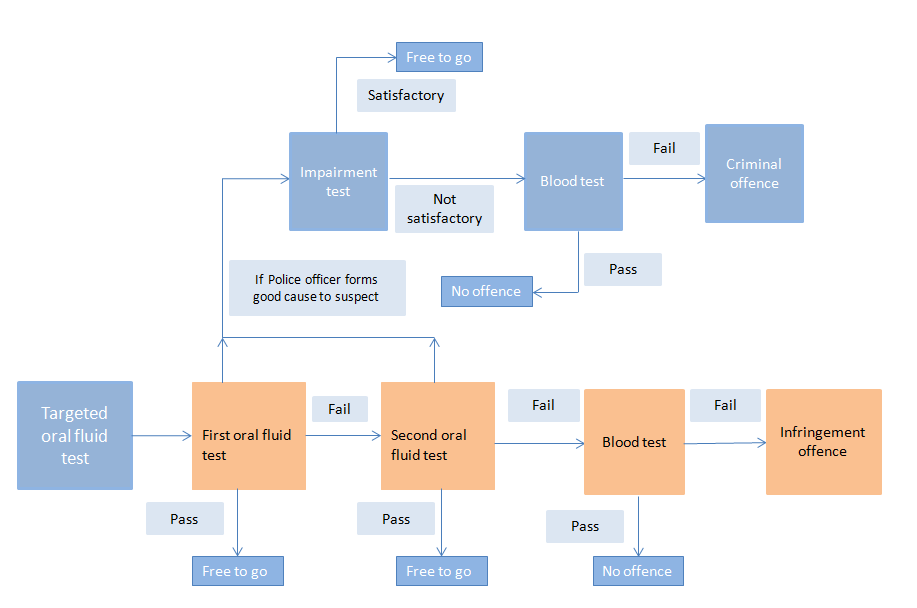
65.
Under Option 2, oral fluid drug testing would be undertaken by officers using a targeted
deployment model. This will consist of training specific road policing groups, such as Highway
Patrol and Strategic Traffic Units to administer the tests in a targeted way. There would be a
specific emphasis on targeting high risk driving behaviours, such as fleeing drivers, illegal
street racing, or night-time speeding, at high risk times and places. Either checkpoints or
mobile vehicle stops would be used. The diagram below outlines the process that would be
followed under this approach.
Page 10 of 29
8j3h8arqdt 2019-06-17 11:30:20
66.
In an operational setting, a Police officer might first undertake an alcohol screening test before
undertaking an oral fluid screening test for drugs. However, an oral fluid test would not follow
all alcohol breath tests. In addition, the Police officer would have the ability to require the
driver to undertake an oral fluid test without first having taken an alcohol breath test.
67.
In order to implement this option, enabling legislation would need to allow a Police officer to
stop any driver who is driving a motor vehicle on a public road and drug test them, without first
needing good cause to suspect the driver has taken drugs.
68.
The New Zealand Automobile Association (AA) surveyed its members in 2009. This survey
found that 89 percent of the members surveyed supported introducing roadside saliva testing
for drugs. However, the survey did not explain the process that is involved with oral fluid drug-
screening tests nor the time it would take to screen a driver’s oral fluid for drugs. The AA
advises that this level of support remains consistent with a rolling survey that it conducts
quarterly, where members are asked if they support or oppose introducing a saliva based
drug test to detect drug-driving. In the last survey of around 900 members, 83.9 percent
expressed support.
Option 3: Introducing oral fluid drug testing following an incident comprising either a
suspected driving offence or a driver’s involvement in a motor vehicle crash (preferred
option)
69.
Rather than randomly testing drivers, Option 3 would allow the Police to screen the oral fluids
of drivers following an incident where they had presented themselves as a potential road
safety threat. An incident would comprise either a suspected driving offence, or a motor
vehicle crash. Eligible driving offences would consist of offences relating to driving that are
enforced by a Police officer. Parking offences and owner liability offences such as speed
camera and toll offences would be excluded.
Page 11 of 29
8j3h8arqdt 2019-06-17 11:30:20
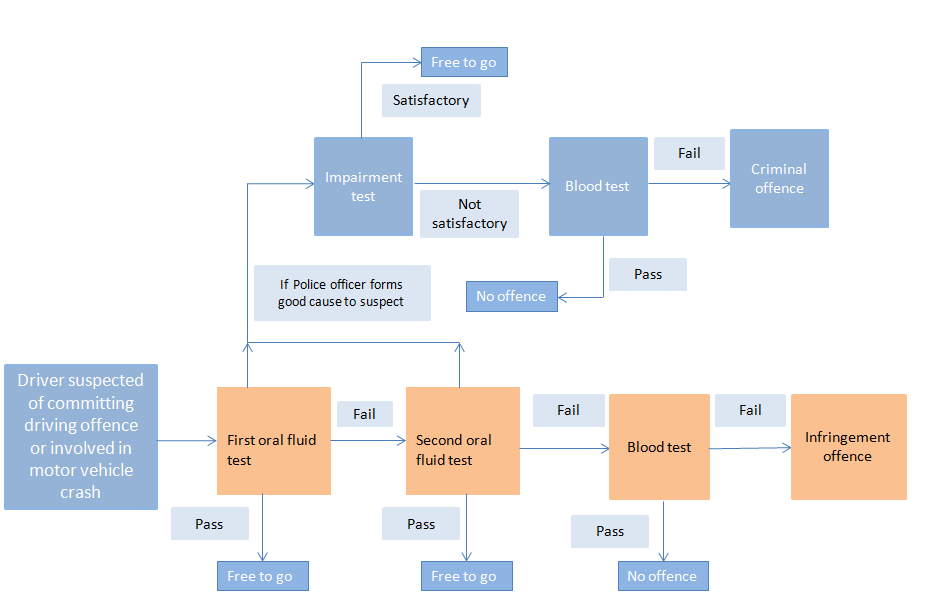
70.
The following diagram outlines the process that would be followed under this approach.
71.
This would be a useful additional tool for the Police where there has been a crash because it
is often not possible to carry out an impairment test, even where a Police officer has good
cause to suspect drug use. Drivers may be injured, in a state of shock or emotional distress,
which could affect their ability to perform the impairment test. In these circumstances,
requiring them to undergo a CIT would be inappropriate. The Police find that they are seldom
able to use impairment testing for crash-involved drivers.
72.
Post-accident drug testing is a common approach following workplace accidents where
people are involved in safety sensitive roles, and by the Police in other jurisdictions following
motor vehicle crashes.
73.
Drivers suspected of committing driving offences and those involved in motor vehicle crashes
would provide a much wider pool of potentially drug impaired drivers compared to those who
are tested through the current drug-driving enforcement regime. Higher levels of testing will
increase both the perceived and actual risk of being caught while driving after having taken
specified drugs. It is expected to have a greater deterrent value than is offered under the
current regime.
74.
The Police have indicated that the oral fluid testing under this option would also be
undertaken by specific road policing groups, such as Highway Patrol and Strategic Traffic
Units, who would be specifically trained to administer the tests.
Page 12 of 29
8j3h8arqdt 2019-06-17 11:30:20
Option 4: Introducing oral fluid drug testing following a motor vehicle crash (not
recommended)
75.
Option 4 is a subset of Option 3 and would introduce oral fluid drug testing for drivers
following a motor vehicle crash. Each year, over 50,000 drivers are involved in motor vehicle
crashes that Police attend and record. This provides a suitable potential number of tests to be
undertaken to have a deterrent effect.
76.
In an operational setting, it is likely that a Police officer would first undertake an alcohol
screening test before undertaking an oral fluid test for drugs. However, a drug test would not
follow all alcohol tests. In addition, a Police officer will have the ability to require the driver to
undertake an oral fluid test without first having taken an alcohol breath test. The Police officer
may not perform either an alcohol screening test or a drug screening test if the particular
circumstances do not warrant testing.
77.
Because oral fluid drug testing following a motor vehicle crash is a subset of Option 3, it would
provide similar benefits. The deterrent effect on this option is expected to be slightly less than
under Option 3 because it would employ a narrower criterion for initiating testing and,
therefore, the perceived likelihood of being caught would be lower.
Post-incident oral fluid testing for drugs (Option 3) should be introduced
78.
I propose that Cabinet agree to introduce post-incident oral fluid drug testing for drivers
(Option 3). This would allow Police officers to undertake the oral fluid testing process after a
suspected driving offence or after a motor vehicle crash. This is my preferred option because
it will:
78.1. increase the perceived likelihood of being caught and have a deterrent effect,
minimising the harm caused by drug-driving. This option has a good benefit cost ratio
of 5:1 over 10 years
78.2. allow a Police officer to drug test drivers who have already presented themselves as
a potential road safety threat and sanction them if they have used drugs. This is less
intrusive on individual rights under the NZBORA when compared to random testing
78.3. allow a significant amount of data to be collected on the number of tests taken and
the outcome of those tests, which will further develop the evidence base and help
decision making in the future.
79.
The impairment testing process and penalties would remain in place if a Police officer has
good cause to suspect a driver has taken, and is impaired by drugs.
80.
I note that the accompanying Regulatory Impact Statement (RIS) prepared by the Ministry
supports random testing. While random testing has a slightly higher benefit cost ratio, I
believe that the post-incident testing achieves much the same outcome but with a smaller
impact on individual rights under the NZBORA.
Page 13 of 29
8j3h8arqdt 2019-06-17 11:30:20
Other matters relating to the testing process and sanctions
Specified drugs
81.
I propose that the drugs that can be identified using an oral fluid test be specified by Order in
Council. This provides Cabinet oversight. It also preserves flexibility to add or subtract drugs
to accommodate changing patterns of drug use or allow for the introduction of new devices
that can test for a wider range of drugs.
82.
The number of drugs that can be detected by existing oral fluid screening devices is limited.
For example, the devices used by most Australian states can only detect THC (the active
ingredient in cannabis), methamphetamine, and MDMA.
83.
Based on current knowledge, it is likely that the three drugs that would be initially specified
under this regime would be the same as those in Australia: THC, methamphetamine, and
MDMA. This is due to the risk these drugs pose to road safety, and the availability of a reliable
and cost effective screening device. THC and methamphetamine are the two most commonly
detected illicit drugs in blood samples taken from drug drivers in New Zealand. MDMA is not
readily available in New Zealand.
84.
Roadside oral fluid drug testing will only detect THC for a few hours after cannabis has been
used. The exact time can vary, depending on the amount and potency of the cannabis used
and the individual’s metabolism. Inactive THC residue in the body of a driver from cannabis
use in previous days or weeks will not be detected by an oral fluid screening test.
Approval process for new devices
85.
The process for approving oral fluid screening devices needs to be flexible. The Police need
to be able to take advantage of any new technology that improves the accuracy of results,
expands the range of drugs that can be detected, minimises delays to motorists, or reduces
costs.
86.
Therefore, I propose that the Minister of Police approve the preferred device(s) by Notice in
the
New Zealand Gazette, after consulting with the Minister of Science, the Minister of Justice
and the Minister of Transport.
Infringement penalty
87.
There would be one infringement offence notice applied per failed blood test even if more
than one specified drug were to be detected in the same blood sample.
88.
I propose the same infringement penalty that drivers who commit low level alcohol offences
receive under the alcohol testing regime (see Table 1).
Table 1: Drink-driving infringement offences and penalties
Offence
Penalty
Drivers under the age of 20 with between 0 and 150
$200 infringement fee and 50 demerit points
micrograms (mcg) of alcohol per litre of breath
Drivers aged 20 and over with breath alcohol levels
$200 infringement fee and 50 demerit points
between 250 and 400mcg of alcohol per litre of breath
Page 14 of 29
8j3h8arqdt 2019-06-17 11:30:20
89.
As driver licences are suspended for 3 months after 100 or more demerit points have been
accumulated within a two-year period, 50 demerit points is a strong deterrent. There is a risk
that this level of penalty may be considered too severe because, unlike low level alcohol
offences, the correlation with impairment is less clear.
Different consequences of the oral fluid testing and impairment testing processes
90.
Operating the oral fluid testing regime and the impairment regime together could produce
quite different legal consequences for a driver. For example, a driver subjected to the oral
fluid test would receive an infringement offence. However, they could be charged with a
criminal offence if they were tested under the impairment regime, although there is a higher
evidentiary threshold for the impairment testing process. This potential inconsistency in
consequences is difficult to reconcile because it is desirable to retain the impairment testing
process alongside the presence-based testing process.
91.
To mitigate this potential inconsistency, I propose allowing the Police, under certain
conditions, to switch from the oral fluid testing process to the impairment testing process. A
switch could be made, if after starting the oral fluid testing process, a Police officer formed
good cause to suspect a driver had used drugs. For example, a driver passed the first oral
fluid testing process but admitted to the Police they had taken drugs or they appeared to be
under the influence of drugs. This would allow a driver to face the more serious criminal
penalty if they are impaired, regardless of which testing process the officer started with. Also,
the risk of an impaired driver avoiding a sanction would be reduced when they had used a
drug that the oral fluid screening device could not detect.
92.
A switch to the impairment testing process should not be permitted once the driver has failed
two oral fluid screening tests. This would avoid the oral fluid testing process being regarded
as capricious or unreasonable. In addition, a Police officer would not be able to switch to the
oral fluid testing process once the impairment testing process had been started.
93.
While a switch to the impairment process would be available, the Police advise that it may not
be regularly used for crash-involved drivers. The Police rarely use the impairment test for
drivers involved in crashes even when they have good cause to suspect the driver had used
drugs. If the driver is injured or is in a state of shock or emotional distress following a crash, it
would be inappropriate to require them to undergo a CIT.
Drivers hospitalised following a crash who show the presence of drugs
94.
If a driver is taken to hospital, or a doctor’s surgery because of a motor vehicle crash, I
propose that Police officers be able to require the person to provide a blood sample. The
sample would be tested for the presence of a specified drug. If a specified drug is detected,
the driver would have committed an infringement offence.
95.
This approach will ensure that drivers, who are involved in a crash and cannot undergo the
oral fluid testing process as a result of any injuries received, can be sanctioned.
Page 15 of 29
8j3h8arqdt 2019-06-17 11:30:20
96.
However, this approach will cause an inconsistency with an existing offence under section 58
of the Land Transport Act 1998. Under section 58 of the Land Transport Act, it is a criminal
offence if the person’s blood is taken in hospital or a doctor’s surgery and contains evidence
of a Class A drug2 (which is usually methamphetamine). If the hospitalised driver tests positive
for a Class A drug, they will continue to be liable for the existing criminal offence. By
comparison, a hospitalised driver whose blood tested positive for THC, would be liable for an
infringement offence only.
Medical defence
97.
Section 64(1A) of the Land Transport Act currently allows a medical defence to a drug-driving
prosecution. I propose a similar medical defence for the new offence detected by the roadside
oral fluid testing process. This defence would apply where a court is satisfied that a person
has consumed a specified drug in accordance with a current and valid prescription written for
them by a health practitioner, and has complied with the instructions for using the drugs from
a health practitioner or manufacturer of the drug.
98.
It is possible for people to be prescribed medicinal cannabis, such as the Sativex mouth
spray, for specified conditions if their medical specialist obtains the appropriate approvals. In
time, the Government may decide to extend the list of specified drugs to include other
controlled drugs (such as opiate-type drugs) that are available under prescription for
treatment purposes.
Detailed legal requirements
99.
To operate effectively, the enabling legislation will require appropriate driver obligations and
Police powers to enforce those obligations. These include driver obligations to undergo the
testing process, and actions the Police can take in situations where a driver fails or refuses to
comply, or fails to remain for the testing process. The law needs to provide appropriate
protections for drivers in the form of defences and rights such as the right to seek an
independent analysis of a blood sample by a private analyst. It also needs to allow Police
officers, in the interests of public safety, to forbid drivers to drive for a period where a driver
has failed the testing process or who has refused or failed to undergo it.
100.
The recommendations specify these detailed requirements, which have been modelled on the
relevant requirements of existing alcohol and drug testing provisions.
Review of the regime after three years
101.
I recommend that the Ministry be directed to review the adequacy of the penalties in deterring
offending after a period, with contributions from other relevant agencies. This issue would be
included in a broader review of the new regime’s efficacy and impacts on individuals, and
whether the regime reflects international best practice. It would take place once three years of
data about the regime are available.
102.
In order to enable a review to be undertaken, the Police would need to collect and record
appropriate data on number of tests undertaken and the results.
2 as specified in Schedule 1 of the Misuse of Drugs Act 1975
Page 16 of 29
8j3h8arqdt 2019-06-17 11:30:20
Implementation of oral fluid testing for drugs
Number and delivery of tests
103.
A regime designed to create a deterrence effect requires a large number of tests. The
proposed presence-based drug-driving testing regime can deliver a large number of tests cost
effectively.
104.
The proposed regime would be phased in over a 3 year period, reaching 45,000 oral fluid
tests per year. I propose that 15,000 oral fluid drug tests be funded in the first year, increasing
to 30,000 tests in the second year and 45,000 tests in the third and subsequent years.
105.
The proposed rollout of screening tests allows the Police to phase in the new testing regime,
and make adjustments as necessary. The Police will determine the most efficient and
effective method of delivery for targeting drug-driving risk, allowing the method to adapt to
address new risks as they develop.
Implementation date
106.
It may take some time to begin testing following enabling legislation being enacted. The
Police would need to develop their operational requirements, find a suitable oral fluid
screening device via a competitive tendering process, and have the new device approved for
use. The Police would also need to develop and implement a programme to train Police
officers to use the device. If the legislation were enacted by the end of May 2017, I would
expect an implementation date of 1 December 2017 at the earliest.
Stakeholder engagement
107.
The Ministry held a stakeholder workshop in May 2015. Attendees included a range of
government departments, treatment providers, university academics, and several interest
groups such as the AA and the New Zealand Drug Foundation. Thirty stakeholder groups
were invited to this workshop, and four provided written feedback on the proposals.
108.
Stakeholders expressed a view that drug-driving affects all ages, and involves both
prescription and illicit drugs. The low number of drug tests under the current regime also
concerned them. Some stakeholders were concerned about presence-based testing, as the
mere presence of a drug or drugs in a bodily fluid sample does not mean a person is
impaired.
109.
There was no consensus on the best way forward. Some stakeholders favoured adopting the
Victorian regime while others were opposed due to inconsistencies of this regime with the
NZBORA.
110.
If Cabinet agrees to changes to the Land Transport Act, there would be further public
engagement at Select Committee. As noted previously, surveys by the AA` suggest good
support for oral fluid drug testing among its members.
Additional issue - amendments to the definition of ‘qualifying drug’ in the Land Transport
Act 1998
111.
Under the Land Transport Act, a person may not drive or attempt to drive a motor vehicle
while impaired, with that person’s blood containing evidence of a qualifying drug. This is the
existing impairment-based offence under section 57A of the Land Transport Act.
Page 17 of 29
8j3h8arqdt 2019-06-17 11:30:20
112.
The Land Transport Act’s current definition of a qualifying drug includes controlled drugs
specified in Schedule 1, Schedule 2, and Parts 1, 4 and 7 of Schedule 3 of the Misuse of
Drugs Act, benzodiazepine drugs in Part 5 of the Misuse of Drugs Act, and prescription
medicines. This definition excludes some drugs in Schedule 3 of the Misuse of Drugs Act that
may impair drivers. There is no justification, on road safety grounds, to exclude them.
113.
I propose that the definition of a qualifying drug be amended to include all of the drugs listed
in Schedule 3 of the Misuse of Drugs Act, except for Part 6. Amending the definition will add
all drugs in Part 2 (such as codeine) and the remaining drugs in Part 5 of Schedule 3 of the
Misuse of Drugs Act to the definition of qualifying drug. This amendment will only relate to
offences detected and prosecuted under the impairment-based regime and will not apply to
specified drugs detected through the oral fluid testing process.
114.
I also propose adding the drugs in Part 3 of Schedule 3 of the Misuse of Drugs Act. Most are
not used as medicines in New Zealand, except for pholcodine, which is available in cough
mixtures and can be abused. Part 6 of Schedule 3 relates to preparations and mixtures, and
is not relevant to driving. The Appendix lists the drugs I propose adding to the definition of a
qualifying drug.
115.
This will assist in future proofing the Land Transport Act if any adjustments are made to
Schedule 3 of the Misuse of Drugs Act. The proposed amendment will not remove any of the
drugs that are currently qualifying drugs for the section 57A offence.
Consultation
Minister of Transport
116.
The matters covered in this paper fall within my delegated portfolio responsibilities. The
Minister of Transport has been consulted on these proposals, and he agrees with the
submission of this paper.
Departments and agencies consulted
117.
The Police, Ministry of Justice, the Department of Corrections, the Ministry of Health, the New
Zealand Transport Agency (NZTA) and the Accident Compensation Corporation participated
in the reference group for the drug-driving review and provided feedback on the Ministry’s
drug-driving review paper as well as this Cabinet paper. Other departments consulted on this
paper were the Treasury, Te Puni Kōkiri, the Ministry of Social Development and the ESR.
118.
The Department of the Prime Minister and Cabinet was informed of this paper.
Comments from Departments
The Police
119.
While Police prefer Option 2 (targeted random testing), as the way to achieve significant road
safety gains in the long term, Police also support the paper’s preferred option of post-incident
testing (Option 3) as an initial measure.
120.
Police note that the current proposed level of testing of 15,000 oral fluid tests in the first year
would represent approximately 5 percent of the approximately 300,000 traffic events that the
Police attend each year. Although this will not deliver the general deterrent value associated
with high levels of visible testing – as is the case with random breath testing - it will deliver
some specific deterrent value as a pragmatic interim step towards achieving full random drug
testing.
Page 18 of 29
8j3h8arqdt 2019-06-17 11:30:20
121.
Police’s future intention is to deliver the oral fluid testing using a targeted deployment model.
This will consist of training specific road policing groups such as highway patrol (who target
rural highways) and strategic traffic units (who target urban localities) to administer the tests in
a targeted way – with a specific emphasis on targeting high risk driving behaviours (e.g.
fleeing drivers, illegal street racing, night-time speeding, and speeding commercial vehicles)
at high risk times.
122.
Police do not support the Option 1 of having ‘good cause to suspect’ as the point of initiation
for an oral fluid testing regime. It offers no practical value in terms of increasing the deterrent
effect or delivering any significant improvements to road safety outcomes. Specifically, Police
have identified that establishing good cause to suspect for the purposes of the current CIT
regime involves difficulties with making an appropriate assessment at the roadside to form
good cause to suspect, and satisfying the court that an assessment of good cause to suspect
was properly made. Unlike alcohol, where there is a definite odour and physical impairment,
such as slurring of speech there is lack of physical signs of impairment associated with many
drugs. Police also have concern about confusion arising from using the same initiation criteria
(good cause to suspect) for parallel regimes having distinct processes and outcomes.
123.
Police wish to highlight that the current good cause to suspect criteria is currently identifying
very small numbers of potentially impaired drivers, and having an oral fluid test as well as the
CIT will not significantly increase the number of drivers tested.
124.
Police agree that the proposed regime will need to be met by a variation to the Road Policing
Programme under the National Land Transport Programme.
Ministry of Justice
125.
The Ministry of Justice prefers Option 1, which would retain the current good cause to suspect
threshold and allow the Police officer to determine which testing pathway to follow. It
disagrees with the view that the current good cause to suspect threshold is too onerous a
threshold to meet for search and seizure (requiring a driver to provide samples of oral fluids
for drug testing). It is unaware of any evidence (including case law) demonstrating that the
good cause to suspect threshold would be unworkable in practice. Further, it believes that the
historically low numbers of tests is more closely related to the difficulty of carrying out the CIT,
rather than the need to meet the good cause to suspect threshold.
126.
The Ministry of Justice also believes that the good cause to suspect threshold as the criterion
for drug testing drivers could be used as a threshold for the other options. It believes that oral
fluid testing could be undertaken at check-points using good cause to suspect as the
threshold for testing. The Ministry of Justice has also provided input to the human rights
section in relation to NZBORA issues.
127.
The Ministry of Justice notes, although the fines that result from Option 3 are not significant in
terms of total volume, existing cost pressures mean that additional collection and enforcement
costs cannot be met within existing baselines. This will be especially so if the number of fines
imposed is significantly higher than those estimated.
Ministry of Health
128.
The Ministry of Health raised concerns that Option 3 (the preferred option) would give the
Police too much discretion to drug test drivers. This relates to drivers who are suspected of
having committed a driving offence or been involved in a crash. It notes the disproportionate
impact of current discretionary enforcement of drug offences on certain populations,
particularly Maori.
Page 19 of 29
8j3h8arqdt 2019-06-17 11:30:20
129.
The Ministry of Health considers the proposed regime is inconsistent with New Zealand's
National Drug Policy 2015 to 2020. It is proposed to sanction drivers for having used drugs, in
the absence of evidence to demonstrate any road safety risk associated with their drug use.
Treasury
130.
Treasury considers the post-incident testing proposal is an improvement on the previously
proposed random drug testing regime. However, Treasury continues to have concerns in
relation to the proposal to introduce additional measures to drug test drivers, including:
130.1. the costs associated with implementation, or where these costs will fall, is not
outlined in the paper, and this uncertainty creates risks in terms of the on-going costs
to the Crown for the implementation as well as difficulties in assessing the costs and
benefits of this proposal
130.2. public consultation on this proposal has not been undertaken, which is problematic
given the significance of this proposal, the potential NZBORA implications and the
number of people it could impact
130.3. the relative priority and urgency of the introduction of additional measures for drug
testing drivers is not clear. This is due to a lack of clarity in terms of the extent of the
problem as well as this proposal not being placed within the broader strategy to
improve road safety.
131.
Therefore, Treasury recommends delaying decisions on this proposal until work is undertaken
to address the concerns outlined above. Depending on the outcome of this further work, the
Ministry may wish to report back to Cabinet with an updated proposal for drug testing drivers
and seek agreement to undertake public consultation on the updated proposal.
Financial implications
132.
The proposed oral fluid testing regime will result in costs for the Crown. These costs are
worthwhile because they will reduce the social cost of drug impaired driving. Changes to the
testing regime for drug-driving will require either additional Crown funding or existing funding
to be reprioritised from elsewhere.
133.
The additional costs and savings to the Crown were estimated as part of the Ministry’s cost-
benefit analysis (CBA). Table 2 below outlines the estimates of total additional costs for the
first 3 years of the oral fluid drug testing regime.
Page 20 of 29
8j3h8arqdt 2019-06-17 11:30:20
Table 2: Potential additional costs for introducing oral fluid drug testing (GST exclusive)
Cost in year 1
Cost in year 2 Cost in year 3
(15,000 tests)
(30,000 tests)
(45,000 tests)
$m
$m
$m
Police
2.82
5.64
8.47
One-off costs to Police (training
0.33
0.00
0.00
and education)
NZTA
0.00
0.00
0.01
One-off costs to NZTA (system
1.55
0.00
0.00
change costs, advertising and
promotion)
Ministry of Justice
0.06
0.13
0.19
Department of Corrections
0.01
0.01
0.01
Total
4.77
5.78
8.68
134.
The final cost of the regime will depend on the detail of the statutory regime eventually
enacted by Parliament and the results of the procurement processes undertaken by the Police
to obtain oral fluid testing devices.
135.
Under the oral fluid testing regime, the majority of the added costs fall on the Police, due to
the process involved with testing drivers for drugs. These costs include the cost of purchasing
drug screening devices and the cost of taking and analysing evidential blood samples.
However, the Police state that some of these costs may be overestimated.
136.
Drug-driving and drink-driving enforcement costs are met from the National Land Transport
Fund under the Road Policing Programme of the National Land Transport Programme. The
Road Policing Programme (approximately $300 million per annum) would need to be varied to
accommodate the new regime. The Police state that new funding will need to be provided for
new costs, such as the purchase of equipment. The Police currently spend around $42 million
per annum on alcohol and drug-driving enforcement, with most of this money being spent on
alcohol enforcement. Diverting existing drink-driving enforcement funding to drug testing could
risk undermining drink-driving enforcement.
137.
Additional funding required by the Police for the first year of the regime can be provided by
reprioritising funds within the National Land Transport Fund to the Road Policing Programme.
The Minister of Transport will seek a recommendation from the NZTA regarding a variation to
the Road Policing Programme. Any variation to the Road Policing Programme will be
approved by the Minister of Transport and the Minister of Police, and will be achieved within
the funding bands set out in the Government Policy Statement on land transport.
138.
Ongoing costs to the Police after the first year of the regime will need to be accommodated
within the Road policing activity class in the Government Policy Statement on land transport
2018.
139.
The NZTA has stated that there would not necessarily be cost impact from drivers incurring
demerit points from the infringement offence included as part of the preferred option.
However, it states that there may be cost impacts if the new offence led to significantly more
people being suspended, due to drivers having additional demerit points added to their record
due to drug-driving. The cost of administering the demerit point system (and suspensions) is
funded through the driver licence reinstatement fee people pay after being suspended.
Page 21 of 29
8j3h8arqdt 2019-06-17 11:30:20
140.
I propose that the NZTA, in conjunction with the Ministry, review the driver licence
reinstatement fee for drivers to ensure the fee is sufficient to cover the increased volume of
licence suspensions.
141.
If Cabinet agrees to the merit of these policy proposals, I recommend that the Ministry, in
conjunction with the NZTA, the Police, the Ministry of Justice and the Department of
Corrections, submit a budget bid seeking appropriate funding, where required.
142.
It is planned that enabling legislation will be passed by May 2017. The proposed regime could
be implemented 6 months after that enactment date (see the section below on legislative
implications). However, this will require funding to be secured before this date. Funding bids
would need to be submitted before Budget 2018 against the between Budget contingency in
order for the regime to be implemented by December 2017.
Human rights implications
143.
Introducing a presence-based testing regime is likely to engage several rights affirmed and
protected by the NZBORA. These include the rights to be secure against unreasonable
search and seizure (section 21), not to be arbitrarily arrested or detained (section 22), and to
be presumed innocent until proved guilty (section 25(c)).
144.
All of the options are likely to interfere, to some extent, with the rights under NZBORA. The
restriction on these rights is likely to be more extreme under Option 2 (the random testing
option) than the other options. Option 1 (retaining good cause to suspect the use of drugs
threshold) is likely to have the least impact on restricting NZBORA rights.
145.
Increasing road safety by preventing the deaths and injuries caused by drug-driving is an
important public policy objective that may justify limiting rights in order to achieve it. The more
closely aligned the basis for testing drivers with the objective of testing (removing threats to
road safety), the more acceptable the testing regime. Justification requires that the chosen
means of attaining the objective be both rational and proportionate.
146.
Considerations include:
146.1. Is there evidence of a clear causal link between introducing a presence based testing
regime and deterrence of drug-driving (a rational connection)?
146.2. Have less intrusive alternatives been considered, and would they be capable of
sufficiently deterring drug-driving (a proportionate response)?
147.
The Ministry of Justice has previously expressed concerns that a sufficiently strong evidential
base has not been presented to justify limiting people’s rights, in particular, in relation to
random testing.
148.
The need to establish reasonable grounds to detain and search a person is an important
procedural safeguard in preventing unreasonable detentions and searches. This may affect
both people who are not drug-driving and people who have trace amounts of drugs in their
systems, but are not impaired in their driving. Either group could unreasonably be subject to
temporary detainment and an invasive search, or to a false positive leading to further
consequences.
Page 22 of 29
8j3h8arqdt 2019-06-17 11:30:20
149.
The key policy questions for Cabinet to consider and be satisfied upon are:
149.1. Is there strong evidence that presence based testing deters drug-driving significantly
more than other methods of deterring drug-driving?
149.2. If so, does that evidence of effectiveness at deterring drug-driving justify arresting
and detaining people who may pose no actual road safety risk?
150.
The Ministry of Justice notes that a final assessment of the consistency of the proposals with
the NZBORA would usually be undertaken by the Attorney-General once the approved
proposals have been drafted. This will not occur, however, if the existing Land Transport
Amendment Bill is used. As the Bill is currently before the Transport and Industrial Relations
Committee, any new proposals added to the Bill will not be scrutinised for consistency with
the NZBORA.
Legislative implications
151.
The Land Transport Act will need to be amended to introduce the drug testing proposal
agreed to by Cabinet. Consequential amendments will also be needed to the Land Transport
(Offences and Penalties) Regulations 1999 to specify the infringement fee and demerit points
for the presence-based offence. An Order in Council will be needed to approve the specified
drugs for the oral fluid testing process. The Minister of Police will also need to approve the
oral fluid screening device(s) by Notice in the
New Zealand Gazette.
152.
There may be an opportunity to include the preferred proposal in the Land Transport
Amendment Bill, which is currently with the Transport and Industrial Relations Committee.
Meeting the time lines for the Committee’s work on the Bil wil be chal enging and undue
delays should be avoided. The Committee is likely to need extra time to seek public
submissions, which could impact on the Bil ’s report back date.
153.
Introducing the proposal in the existing Land Transport Amendment Bill will mean that the
preferred proposal will avoid proper scrutiny for NZBORA consistency. The Ministry of Justice
considers this is undesirable, and another legislative vehicle would be more appropriate to
introduce a drug-driving regime.
Regulatory impact analysis
154.
The Regulatory Impact Analysis (RIA) requirements apply to the proposal in this paper and a
Regulatory Impact Statement (RIS) has been prepared and is attached.
155.
The Regulatory Impact Analysis Team at the Treasury (RIAT) has reviewed the RIS and CBA
prepared by the Ministry and considers that the RIS does not meet the quality assurance
criteria.
156.
The RIS contains useful information, but RIAT does not consider the preferred option, or other
proposals in the Cabinet paper follow convincingly from the analysis. The RIS summarises the
available evidence from New Zealand and overseas, discussing a range of options to
implement testing. The RIS acknowledges that little data exists on the extent of drug-driving in
New Zealand or the extent to which impairment caused by drug-driving causes harm. The RIS
acknowledges that the analysis of a drug-driving problem is subject to a range of unknowns
and uncertainties.
Page 23 of 29
8j3h8arqdt 2019-06-17 11:30:20
157.
The argument for the preferred option is driven strongly by the CBA results and the objective
to “deter drivers from driving drugged”. RIAT considers little weight should be given to the
CBA given the RIS acknowledges considerable uncertainty about the magnitude of the
problem (drug-impaired drivers causing harm).
158.
The preferred option advanced by officials in the RIS differs from recommendation 4 in the
Cabinet paper. While this is not a problem in itself, the RIS only provides detailed impact
analysis on officials’ preferred option, meaning the impacts of other options, including the
Cabinet paper recommendations are unclear. In particular, RIAT is concerned that the RIS
does not outline the implementation feasibility of undertaking 45,000 oral fluid tests per year
within 3 years without random testing.
159.
The options in the RIS have not been subject to public consultation. This is concerning given
the proposed change could impact a large number of people. The analysis of the “public
acceptability” objective is not convincing, although the RIS does acknowledge the lack of
consultation.
160.
RIAT considers there is a stronger case supporting the option to delay a decision on offences
or infringements until public consultation is carried out; more data on the underlying problem
is collected; and testing technology is developed further (acknowledging, for example, the
high but declining incidence of false positives).
Gender implications
161.
The Ministry conducts an annual survey named Public Attitudes to Road Safety. A new
question about driving while affected by drugs with, or without, alcohol was introduced in
2014. Six percent of males responding to this survey said they had driven while affected by
‘other drugs' with or without alcohol, compared to two percent of females. This suggests that a
greater percentage of males than females would be affected by the introduction of a
presence-based drug-driving testing regime.
Disability perspective
162.
There are no disability implications arising from this paper.
Publicity
163.
I intend to issue a media statement if Cabinet agrees to the recommendations in this paper. I
also intend to release publicly relevant documents including this paper and the Ministry’s CBA
and RIS once the announcement has been made.
164.
A communications plan will be developed by the Ministry, in consultation with the NZTA and
the Police to ensure the public is aware of the changes and the reasons for them.
Recommendations
165.
The Associate Minister of Transport recommends that the Committee:
Process for specifying drugs and devices for oral fluid testing process
1.
note that the likely specified drugs that will be tested for as part of the oral fluid testing
process will be THC (the active ingredient in cannabis), methamphetamine, and MDMA
(ecstasy)
Page 24 of 29
8j3h8arqdt 2019-06-17 11:30:20
2.
agree that the drugs that can be tested for as part of the oral fluid testing process be
specified by Order in Council
3.
agree that the Minister of Police may approve a device or devices for the purposes of oral
fluid screening tests, after consulting with the Minister of Science, the Minister of Justice and
the Minister of Transport, by notice in the
New Zealand Gazette
Oral fluid testing process
4.
agree to introduce an oral fluid drug testing regime where an enforcement officer can stop
and administer an oral fluid screening test to any driver who is suspected of having
committed a driving offence or has been involved in a motor vehicle crash, without first
needing good cause to suspect that the driver has consumed a drug or drugs
5.
agree that
a
driving offence for the purposes of initiating the oral fluid testing process will be
restricted to driving offences that are enforced by a Police officer, and will exclude parking
offences and owner liability offences, such as speed camera or toll offences
6.
agree that the oral fluid drug testing process be made available alongside the current
impairment testing process and involve the following elements:
i.
a roadside oral fluid screening test for any drugs that are specified by the Governor-
General by Order in Council for the purpose of the test
ii.
a second oral fluid screening test if the driver produces a positive test result for any of
the specified drugs
iii.
an evidential blood test if the second oral fluid test is positive for any of the specified
drugs
7.
agree that, up until the start of the second oral fluid test, Police officers are able to switch
from the oral fluid testing regime to the impairment testing process, if they form good cause
to suspect the driver has used a drug or drugs
8.
agree,
once a Police officer has started the second oral fluid test, they must wait until a
result is shown on the oral fluid screening device before making any decision to switch to the
impairment testing process; if the result is positive, the Police officer must continue with the
oral fluid testing process; and, if the result is negative, the Police officer may switch to the
impairment testing process if they had formed good cause to suspect the driver has used a
drug or drugs
9.
agree that, once a Police officer has started, or switched to, the impairment testing regime,
they cannot switch to the oral fluid testing process
10.
agree that drivers who fail or refuse to undergo the first oral fluid screening test when
requested, or who have a positive result on the first test, be required to undergo a second
oral fluid screening test
11.
agree that drivers who fail or refuse to undergo the second oral fluid screening test when
requested, or who have a positive result on the second test, be required to undergo an
evidential blood test
12.
agree to create an offence for drivers who fail or refuse to permit a blood sample to be
taken, where drivers would face the same penalties as drivers failing or refusing to permit a
blood sample to be taken under section 60(1) of the Land Transport Act 1998
13.
agree that Police officers have the power to arrest without warrant, any driver who refuses to
accompany a Police officer for the purposes of the roadside oral fluid testing process, or fails
or refuses to remain for the test, or for the result of the test to become available
Page 25 of 29
8j3h8arqdt 2019-06-17 11:30:20
14.
agree that the penalties for refusing to accompany a Police officer for the purposes of the
oral fluid screening process, or failing or refusing to remain for the test or for result of the test
to become available, are the same as those that currently apply under the current drug-
driving impairment regime
15.
agree to replicate or apply, where appropriate, the procedures (including obligations, powers
and penalties) set out for the existing alcohol and drug testing regimes
Medical defence
16.
agree to create a medical defence for the offences detected by the oral fluid testing process
that would allow a driver a defence if they had consumed a specified drug in accordance
with a current and valid prescription written for that person and had complied with
instructions from a health practitioner or the manufacturer of the drug
Testing drivers in a hospital or doctor’s surgery
17.
agree that a person who is under examination, care, or treatment at a hospital or doctor’s
surgery, as a result of an incident or accident involving a motor vehicle, must supply a blood
sample to be taken for the purposes of testing for the presence of a specified drug or drugs
18.
agree, if the person whose blood is taken in a hospital or a doctor’s surgery shows the
presence of a specified drug, they will be liable for the infringement offence agreed to under
recommendation 20, unless the drug detected is a drug listed in Schedule 1 of the Misuse of
Drugs Act 1975, in which case they would qualify for the existing offence under section
58(1)(b) of the Land Transport Act 1998
Police powers to forbid a driver to drive in the interests of public safety
19.
agree that, in the interests of public safety, a Police officer may exercise all or any of the
powers in section 121 of the Land Transport Act 1998, including forbidding a driver to drive if
the result of the second oral fluid screening test the driver has undergone appears to be
positive for any specified drug, or the person fails or refuses that second oral fluid screening
test
Offence and penalties for driving with a specified drug in blood
20.
agree to create an infringement offence for driving or attempting to drive a motor vehicle on
a road if they have any one or more of the specified drugs in their blood sample irrespective
of whether the specified drugs detected in their blood sample is the same specified drug or
drugs that were detected in the oral fluid screening tests
21.
agree that the infringement offence incur an infringement fee of $200 and 50 demerit points
22.
agree to reproduce, where appropriate, the enforcement procedures, powers and penalties
set out for the current alcohol and drug testing regimes
Other matters
23.
direct the Ministry of Transport, with contributions from the relevant Justice sector agencies,
to provide the Minister of Transport, the Minister of Police and the Minister of Justice with an
assessment of the effectiveness of the oral fluid testing process in the drug-driving regime,
including the adequacy of the penalties in deterring offending, once 3 years of data are
available
24.
direct the
Ministry of Transport and the Police to collect relevant data to support the review,
including the number of tests undertaken and the results of those tests
Page 26 of 29
8j3h8arqdt 2019-06-17 11:30:20
Financial and operational implications
25.
agree to implement the new oral fluid drug testing regime over 3 years with 15,000 drug
tests being funded in the first year, rising to 30,000 tests in the second year, and 45,000
tests in the third and subsequent years
26.
note that the proposal to introduce oral fluid drug testing of drivers will have significant cost
implications for the Police, and these would need to be met by a variation to the Road
Policing Programme under the National Land Transport Programme
27.
note that additional funding required by the Police for the first year of the regime can be
provided by reprioritising funds within the National Land Transport Fund to the Road Policing
Programme and this will be achieved within the funding bands set out in the Government
Policy Statement on land transport
28.
note that the Minister of Transport will seek a recommendation from the New Zealand
Transport Agency regarding a variation to the Road Policing Programme
29.
note that the Ministers of Transport and Police will approve any variation to the Road
Policing Programme
30.
note that the Ministers of Finance and Police will need to agree any change to the Police
appropriation for the Road Policing Programme and the Ministers of Finance and Transport
will need to agree the corresponding reduction in the National Land Transport Fund Vote:
Transport appropriation
31.
note that costs to the Police after the first year of the regime will need to be accommodated
within the Road policing activity class in the upcoming Government Policy Statement on land
transport 2018
32.
note the proposal to introduce random drug testing of drivers will have cost implications for
the New Zealand Transport Agency, the Justice system, the Accident Compensation
Corporation and the Department of Corrections
33.
agree that where additional funding is required, the Ministry of Transport, in conjunction with
the New Zealand Transport Agency, the Police, the Ministry of Justice and the Department
of Corrections, will submit a bid seeking funding before Budget 2018, against the between
Budget contingency
34.
direct the New Zealand Transport Agency, in conjunction with the Ministry of Transport, to
review the driver licence reinstatement fee that applies for drivers after being suspended, to
ensure the fee is sufficient to cover the increased volume of licence suspensions
Human rights implications
35.
note that introducing a presence-based regime is likely to engage several rights affirmed
and protected by the New Zealand Bill of Rights Act 1990 including the rights to be secure
against search and seizure (section 21), not to be arbitrarily arrested or detained
(section 22) and to be presumed innocent until proved guilty (section 25(c))
36.
note that if the agreed proposals are included in the Land Transport Amendment Bill, which
is being considered by the Transport and Industrial Relations Committee, there will be no
opportunity for these proposals to undergo scrutiny by the Attorney-General for consistency
with the New Zealand Bill of Rights Act 1990
Page 27 of 29
8j3h8arqdt 2019-06-17 11:30:20
Legislative implications
37.
note that the Land Transport Act 1998 will need to be amended to introduce the drug testing
proposal agreed to by Cabinet
38.
note that
consequential amendments will also be needed to the Land Transport (Offences
and Penalties) Regulations 1999 to specify the infringement fee and demerit points for the
presence-based offence
39.
note that the drugs for the oral fluid testing process will be specified by Order in Council and
that the Minister of Police will need to approve the oral fluid screening device(s) by Notice in
the
New Zealand Gazette
40.
agree that the definition of a qualifying drug in the Land Transport Act 1998 be amended to
include all of the drugs listed in Schedule 3 of the Misuse of Drugs Act 1975, except for Part
6 of Schedule 3
41.
agree to include the necessary amendments in the Land Transport Amendment Bill currently
before the Transport and Industrial Relations Committee if possible
42.
note that, if the proposals are included in the Land Transport Amendment Bill, the Transport
and Industrial Relations Committee may need extra time to call for public submissions
43.
invite the Associate Minister of Transport to issue drafting instructions to give effect to the
relevant recommendations above, including any necessary consequential savings and
transitional provisions
44.
authorise the Associate Minister of Transport to make decisions, consistent with the overall
policy decisions in this paper, on any issues that may arise during the drafting process
Publicity
45.
note that a communications plan will be developed by the New Zealand Transport Agency in
consultation with the Police to ensure the public is aware of the changes and the reasons for
them
46.
note I plan to:
i.
issue a media statement announcing Cabinet’s decisions
ii.
publish relevant documents on the Ministry of Transport’s website once the
announcement has been made, which include this paper and its accompanying
Regulatory Impact Statement and the Ministry of Transport’s cost benefit analysis
Hon Craig Foss
Associate Minister of Transport
Dated:
Page 28 of 29
8j3h8arqdt 2019-06-17 11:30:20
Appendix - Drugs in Schedule 3 of the Misuse of Drugs Act 1975 to be added to the definition
of a ‘qualifying drug’ in the Land Transport Act 1998
Part 2:
Codeine (3-methylmorphine)
Dihydrocodeine
Propoxyphene (α-4 (N, N-dimethylamino)-1, 2-diphenyl-3-methyl-2-propionoxybutane)
Part 3:
Acetyldihydrocodeine
Ethylmorphine (3-ethylmorphine)
Nicocodine (6-nicotinylcodeine)
Nicodicodine (6-nicotinyldihydrocodeine or nicotinic acid ester of dihydrocodeine)
Norcodeine (
N-demethylcodeine)
Pholcodine (morpholinylethylmorphine)
Propiram (
N-(1-methyl-2-piperidinoethyl)-
N-2-pyridylpropionamide)
Part 5:
Amfepramone (2-(diethylamino) propiophenone)
Aminorex
Barbital (5,5-diethylbarbituric acid)
Clorazepate
Ethchlorvynol (ethyl-2-chlorovinylethynyl-carbinol)
Ethinamate (1-ethynylcyclohexanol carbamate)
Mazindol (5-(4-chlorophenyl)-2, 5-dihydro-3H-imidazo [2, 1-a]-isoindol-5-ol)
Meprobamate (2-methyl-2-propyl-1,3-propanediol dicarbamate)
Methylphenobarbital (5-ethyl-1-methyl-5-phenylbarbituric acid)
Methylprylon (3,3-diethyl-5-methylpiperidine-2,4-dione)
Pemoline
Phenobarbital (5-ethyl-5-phenylbarbituric acid)
Phentermine (2-amino-2-methyl-1-phenylpropane)
Pipradrol (1,1-diphenyl-1-(2-piperidyl)methanol)
SPA ((−)-1-dimethylamino-1,2-diphenylethane)
Page 29 of 29
8j3h8arqdt 2019-06-17 11:30:20