 CORPORATE OFFICE
CORPORATE OFFICE
Level 1
32 Oxford Terrace
Telephone: 0064 3 364 4160
Christchurch Central
Fax: 0064 3 364 4165
CHRISTCHURCH 8011
[email address]
8 May 2018
J Baker
Email: [FYI request #7707 email];
Dear J Baker,
RE Official Information Act request CDHB 9844
I refer to your email dated 24 April 2018 requesting the following information under the Official Information Act
from Canterbury DHB.
Many of our people in the community undergo treatment for gallstones and cholecystitis
Treatment options includes elective gallbladder surgery commonly known as cholecystectomy (laparoscopic
cholecystectomy)
Information to include but not exclusive to:
•
Patient treatment information handout / fact sheet brochures
•
Patient informed consent form or forms
•
Elective surgery consent form or forms
•
Post cholecystectomy wound care, recovery and diet information
•
And any other handout information provided to clients
Include also if possible published and revision dates.
Please provide a copy of ALL the information you provide to clients (public heath consumers) during the clinical
assessment, cholecystectomy (laparoscopic) preoperative informed consent and surgery admission process.
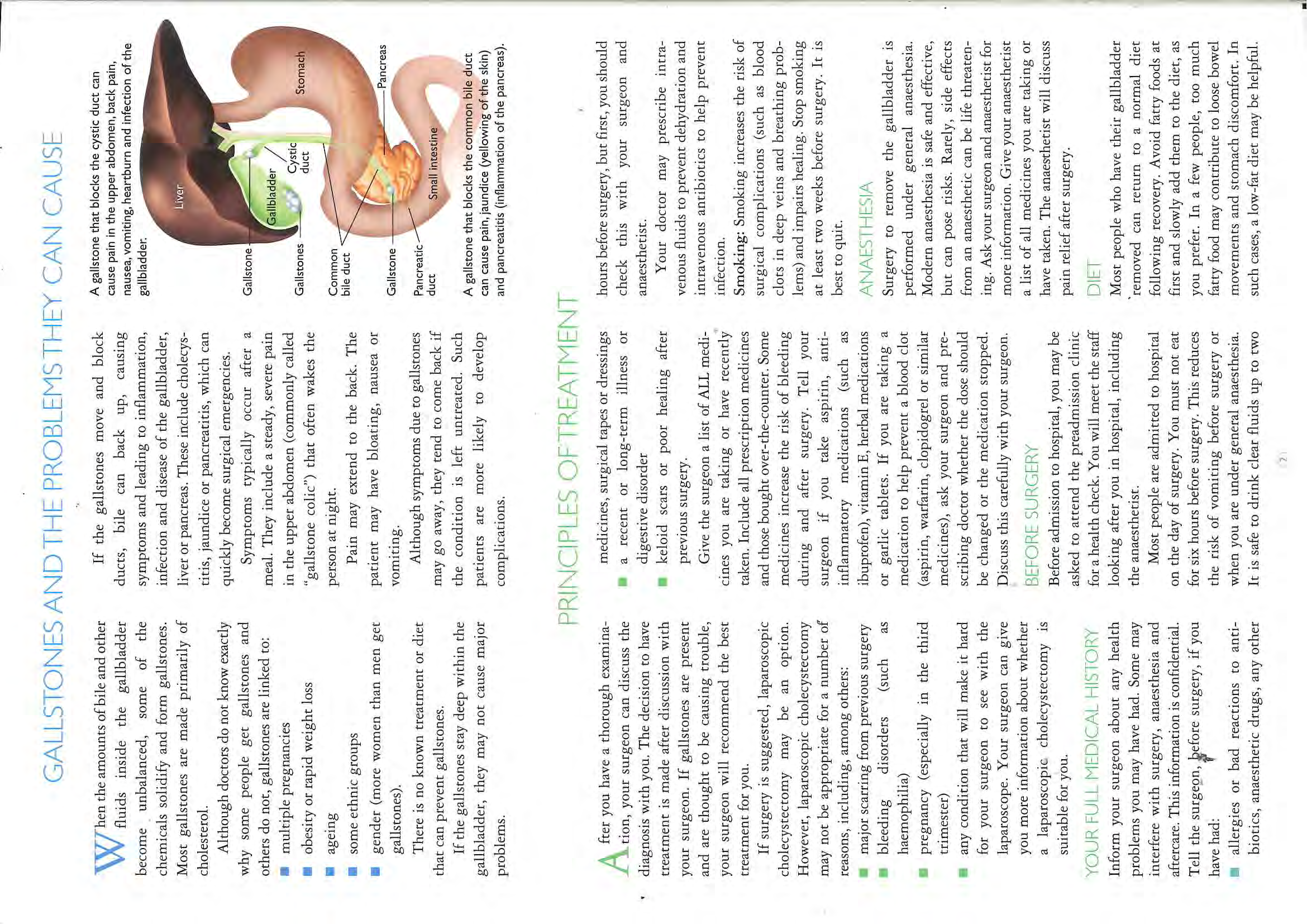
A cholecystectomy is the surgical removal of the gallbladder, which is commonly performed to treat gallstones.
Occasionally it is also performed as part of a bowel, pancreatic or hepatobiliary cancer surgery or as a result of
trauma. Usually the surgery is performed laparoscopically via small incisions, however in some instances it may be
required to be an open procedure, resulting in a large incision.
Patients needing this surgery can be referred by their General Practitioner to be seen in Outpatients, where the
history, examination and discussion about the surgery takes place. They are then given a copy of the Royal
Australasian College of Surgeons (RACS) ‘Laparoscopic Gall Bladder Surgery’ pamphlet. On occasion they may be
given a ‘Reducing the Risk of Blood Clots’ or a ‘Patient Controlled Analgesia’ pamphlet if this is clinically indicated.
Alternatively patients may be admitted acutely to the Surgical Admissions and Review Area (SARA), with Acute
Cholecystitis, and may be offered an Acute Cholecystectomy if appropriate. Patients admitted to the SARA unit
are given further information brochures including ‘Ward 16 – Patient Information - Surgical Assessment and
Review Area ’, ‘Acute Surgery’ and ‘Laparoscopic Cholecystectomy’ (which includes wound care and dietary
advice). If the procedure is converted to an open procedure, patients are given a pamphlet on ‘Managing at Home
after Abdominal Surgery’. Inpatients may also be given a RACS (Royal Australasian College of Surgeons)
‘Laparoscopic Gall Bladder Surgery’ pamphlet.
Consent paperwork for the procedure is completed on a standardised Canterbury DHB ‘Request for Treatment by
Operation / Procedure’ form. For elective procedures this occurs either in the Outpatients Department or Day of
Surgery Admissions (DOSA) unit on the day of admission. For inpatients this is completed in the SARA unit. When
completing the consent form the Medical Team are required to advise the patients, and document both the
benefits and the risks of the procedure.
On discharge, patients are given individual discharge advice by the Surgical team which is reiterated by Nursing
staff, regarding when to see their GP, how to manage their wounds and resuming normal levels of activity. This is
also documented on their discharge summary.
There is also extensive information provided on the Canterbury HealthInfo website under ‘Gallbladder and
Gallstones’ which can be found at:
https://www.healthinfo.org.nz/; this information is written by clinical advisers
and is publically available.
Some Canterbury DHB patients have their elective surgery contracted out to St Georges Hospital or Southern Cross
Hospital. Each hospital has their own consent, admission and discharge information paperwork and they are
responsible for the provision of any patient information given to the patients.
Patient information pamphlets are reviewed regularly to ensure they remain current. We have recently completed
a review of our patient information and are confident they remain best practice. Please find attached the
following:
Appendix 1 Ward 16 – Patient Information Surgical Assessment and Review Area – Oct 2017
Appendix 2 Acute Surgery –May 2016
Appendix 3 Laparoscopic Cholecystectomy - February 2018
Appendix 4 Managing at Home after Abdominal Surgery –August 2010
Appendix 5 Request for Treatment by Operation / Procedure – October 2017 –
Appendix 6 Royal Australasian College of Surgeons –Laparoscopic Gallbladder Surgery – August 2014.
Appendix 7 Reducing the Risk of Blood Clots – June 2010
Appendix 8 Patient Controlled Analgesia – November 2014
I trust that this satisfies your interest in this matter.
Please note that this response, or an edited version of this response, may be published on the Canterbury DHB
website.
Yours sincerely
Carolyn Gullery
General Manager
Planning, Funding & Decision Support
 Welcome to Ward 16/SARA
We strive for excellence in our communication and team work, to deliver patient
Welcome to Ward 16/SARA
We strive for excellence in our communication and team work, to deliver patient
and family/whanau focused health care with enthusiasm and a sense of passion,
providing a supportive, approachable and fun environment
Ward 16
A
We are one of three general surgical wards and we specialise in upper
R
A
Gastrointestinal and Hepaticobiliary Surgeries.
S
t
We care for patients who have come in acutely and electively for surgery, as well
16/
as those needing management of acute surgical conditions
ard
tmen
We also have the Surgical Assessment Review Area on ward 16
W
ar
to
Surgical Assessment Review Area (SARA)
ep
We are an acute specialised unit where patients with acute surgical conditions
me
y D
have their initial assessment.
co
er
rg
Your assessment will be carried out initially by nurses and doctors. Where
el
W
required, tests and investigations will then be performed or requested. There are
Su
sometimes delays in these, we appreciate your patience.
We are a short stay area, once assessed, if deemed needing to stay you will be
moved to another ward as soon as a bed is available
On arrival all patients are nil by mouth, until specified otherwise by the surgical
team. Eating and drinking may cause a delay in procedures.
We are not always able to find a cause of some ongoing pain with a reasonable
line of investigations in an acute setting and sometimes it may be assessed as
appropriate for further assessments or investigations to be carried out by your
GP in an outpatient setting.
There is a senior nurse in-charge in SARA morning, afternoon and at night who
is responsible for ensuring a smooth patient journey. They are available to speak
with you or your family/whanau about any concerns.
What if my family want to ring?
Telephone Christchurch Hospital switchboard on;
(
03) 3640 640 and ask for Ward 16 or SARA or extension 89160
Visiting hours Ward 16: 11.00 – 1.00 pm and 3.00 – 8.00 pm
Visiting or telephone calls are discouraged outside of these times to enable cares,
assessments and patient rest.
Please do not be offended if nursing staff ask visitors to leave during these times.
SARA: 8.00 am and 8.00 pm, please talk to the nursing staff if any questions.
Ref: 0170
Authorised by: CNM, Ward 16
Oct 2017
Please tell us if you have an
Enduring Power of Attorney (EPOA)
Advanced Care Plan (ACP)
Health Passport
Or any specific needs or requirements for us to be able to provide care for you
Interdisciplinary Team
Doctors, nurses, pharmacists, physiotherapists, occupational therapists, social workers, dietitians, ward
assistants, ward clerks, chaplains & Māori health. Patients are assessed on arrival and throughout
admission for interdisciplinary assessment. If you wish to speak to any member of the team, please let
us know.
Charge Nurse Manager (CNM)
The CNM is responsible for the day to day ward management and is available to discuss any general
enquiries.
Nurses
We have a nursing team of highly skilled professionals that strive to ensure each patient receives a high
standard of care. Student nurses may also be working with Registered Nurses as part of their training.
Clinical Nurse Specialist and Clinical Nurse Educator
As a teaching hospital we have Specialist Nurses who support the nursing staff.
Medical Staff
You are admitted under a surgical consultant, who has a team of doctors working with them.
Morning ward round usually occur 0800 and 1000, this is when you are assessed by the team and a
plan for the day is made, this plan may change across the day. We aim to keep you fully informed with
treatment and test results as we receive them.
Hospital Aides
Support the nursing staff and assist in the general running of the ward.
Ward Clerk
The voice and face of the ward when you arrive or ring up.
Patient Privacy
Your name will be written above your bed, outside your room and on the White Board in the corridor.
Please let your nurse know if you do not want your name displayed.
Patient Identification
During your stay you will be asked to give your name, date of birth and sometimes address many times.
This is to keep you safe, making sure that the Right Patient gets the Right Drug or test and procedure.
Teaching
We are a teaching hospital and have student health professionals who may spend time with you. If you
do not wish to have students involved in your care, please let your team know. This will not affect your
care in any way
Your Rights
Your rights are guaranteed by law. This is known as the Code of Health and Disability Services
Consumers’ Rights. There is a leaflet available in your area outlining your rights. There is an
Interpreter Service available on request.
Valuables
We encourage you to leave valuables at home. The Canterbury District Health Board and the ward take
no responsibility for loss or damage.
Ref: 0170
Authorised by: CNM, Ward 16
Oct 2017
Smoke Free
The CDHB has a smoke free policy and smoking is not permitted in any building or on the grounds.
All patients are asked if they smoke and advice and smoking cessation support is offered.
Please ask for a Quit Pack for yourself or family or visit www.quit.org.nz.
Electronic Devices:
Free WIFI is available
We ask
you to respect other patients privacy when using any electronic device and to keep devices on
silent / vibrate mode.
Day Room
This is for patients and family/whanau to relax and watch TV, you will find it at the end of the ward
Education
Health Education is an important part of your care and recovery. We will provide you with clear and
concise information, by talking with you and your family/whanau and sharing written information to
support this discussion
Have your say
We encourage patients and families to tell us about their experience in hospital. There are blue boxes
throughout the hospital to place written feedback. A National Survey may be emailed to you a week
after discharge from hospital, we would appreciate you to completing this.
What if I experience pain?
Please let staff know if you are in pain at any time, no matter how busy we seem.
We will ask you to score your pain between 0 (no pain) and 5 (worst pain possible) this helps staff
assess for the most appropriate treatment and medication.
What if I feel sick or vomit?
This can happen when you are ill and/or after surgery or anaesthesia.
If you feel sick you may not be able to eat, which will slow down your recovery. Please tell us if you feel
sick so we can get you treatment.
What if I am constipated?
Constipation can occur while you are in hospital because you are less active, and may eat and drink
less. Some medicines, such as codeine and morphine can also cause constipation.
We may suggest that you take laxatives to prevent or treat constipation while in hospital.
Concerns?
If you or your family have any questions or concerns about anything mentioned in this pamphlet please
talk to us.
For more information about:
your health and medication, go to www.healthinfo.org.nz
hospital and specialist services, go to www.cdhb.health.nz
Ref: 0170
Authorised by: CNM, Ward 16
Oct 2017
Ref: 0170
Authorised by: CNM, Ward 16
Oct 2017
 Acute Surgery
Acute Surgery Patient information - General Surgical Wards
The following information is a guide to your care while in hospital.
Your care may vary depending on your surgery and surgeon’s
instructions.
What is an Acute Surgery List?
s
You require an operation and have been booked on the Acute Surgical List. The acute
ard
surgical list is made up of any number of patients who require unexpected operations
y
W
of varying degrees of urgency. You
must not eat or drink anything whilst waiting on this
er
ical
list, including chewing gum or boiled sweets. We advise against smoking.
rg
rg
u
Su
S
When will this Surgery Occur?
te
ral
e
Your admitting surgeon will communicate with the operating theatre to schedule your
u
c
n
operation and will give you an estimated time for the surgery. However it is not
A
Ge
possible to be specific about this time because patients at Christchurch Hospital are
operated on according to the urgency of their condition, i.e. life-threatening conditions
must go to theatre first. Therefore this acute list can be subject to sudden changes
when serious cases arrive in the Emergency department. Also some acute operations
can be unpredictable and may take longer than anticipated.
Please be aware that it is generally not possible for an operation to be scheduled
immediately and occasionally a patient may need to be rescheduled at short notice
whilst an urgent patient is dealt with. Whilst every effort is made to get patients’
surgery completed in a timely fashion, such situations are unavoidable and your
understanding is appreciated.
You will be advised as soon as a time is scheduled for the operation.
This may only be a few minutes before you are due to go to theatre
so it is important that you let the nursing staff know if you need to
leave the Ward at any time.
Your nurse will prepare you for theatre as soon as you are booked on the acute list.
Depending on anticipated waiting times, you may also be transferred to a Ward prior to
going to theatre. Your belongings will be transferred to that Ward where you will return
to after surgery. Please send valuables home with your family if possible.
Who will perform my Operation?
Patients who are admitted acutely will be assigned a surgical team that is on duty for
that day. This consists of a Consultant, Senior Registrar, Junior Registrar, House
surgeon and possibly a trainee intern or medical student. You may not meet this entire
team until doctors rounds the following day. Your surgery will likely be performed by a
Registrar and overseen or assisted by the Consultant, depending on complexity.
Ref:2058
Authorised by: Director of Surgical Nursing Services
May 2016
When Will I Be Able to Eat and Drink?
To safely have a general anaesthetic, you may not eat for 6 hours before surgery, water may be
permitted for up to 2 hours before but check with your nurse. The anaesthetist may give specific
instructions that differ from this. Food and fluids will be restarted as soon as it is safe to do so after your
surgery depending on the surgeons instructions, again please check with your nurse.
If you eat and drink during this time, the operation will have to be delayed, possibly until the
following day.
You may require intravenous fluids to avoid dehydration whilst fasting. Your nurse will continue to
monitor you regularly, if your condition changes during this time your nurse will ask for the doctor to
review you and your plan of care may change, you may be pushed forward for surgery more urgently or
you may be cancelled or postponed. There can be many variables with an acute illness so your
patience is appreciated.
We understand that waiting for surgery is a stressful time for you and your family and will
endeavour to keep you informed. We encourage you to ask questions at any time.
General Surgical Wards
Christchurch Hospital
Phone (03) 364 0640
For more information about:
your health and medication, go to www.healthinfo.org.nz
hospital and specialist services, go to www.cdhb.health.nz
Ref:2058
Authorised by: Director of Surgical Nursing Services
May 2016

Laparoscopic Cholecystectomy
Patient information - General Surgical Wards
s
The following information is a guide to your care while in hospital, and includes
y
ard
important discharge information. Your care may vary depending on your surgery and
m
W
surgeon’s instructions.
ic
p
ical
rg
u
What is a cholecystectomy?
sco
ystecto
o
S
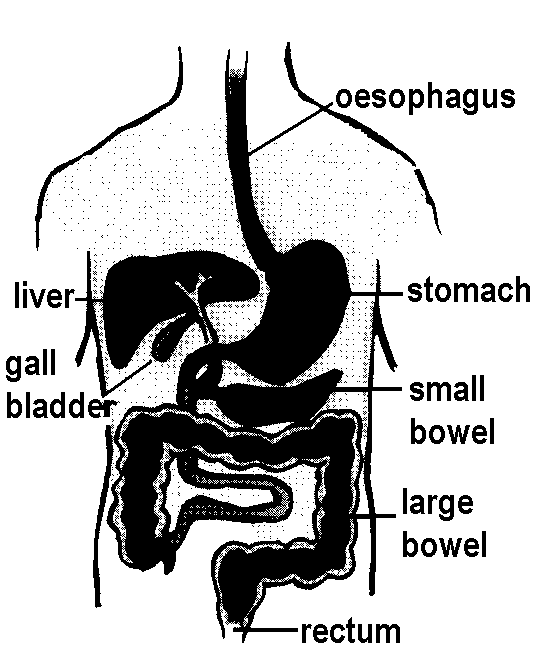
It is the surgical removal of the gallbladder. The gallbladder is a small pear shaped
ar
lec
ral
e
organ attached to the underside of your liver. The gallbladder stores bile, produced by
o
ap
h
n
the liver. Bile aids digestion by breaking down fats in the foods you eat. Your gallbladder
L
C
Ge
is not essential for healthy digestion, as bile will continue to flow from the liver to the
small intestines.
When the amount of bile and other liquids in your gallbladder become unbalanced,
some solidify and form gallstones. If the gallstones move and block the bile ducts the
gallbladder, liver and pancreas may get infected or diseased and your doctor may
decide to remove your gallbladder.
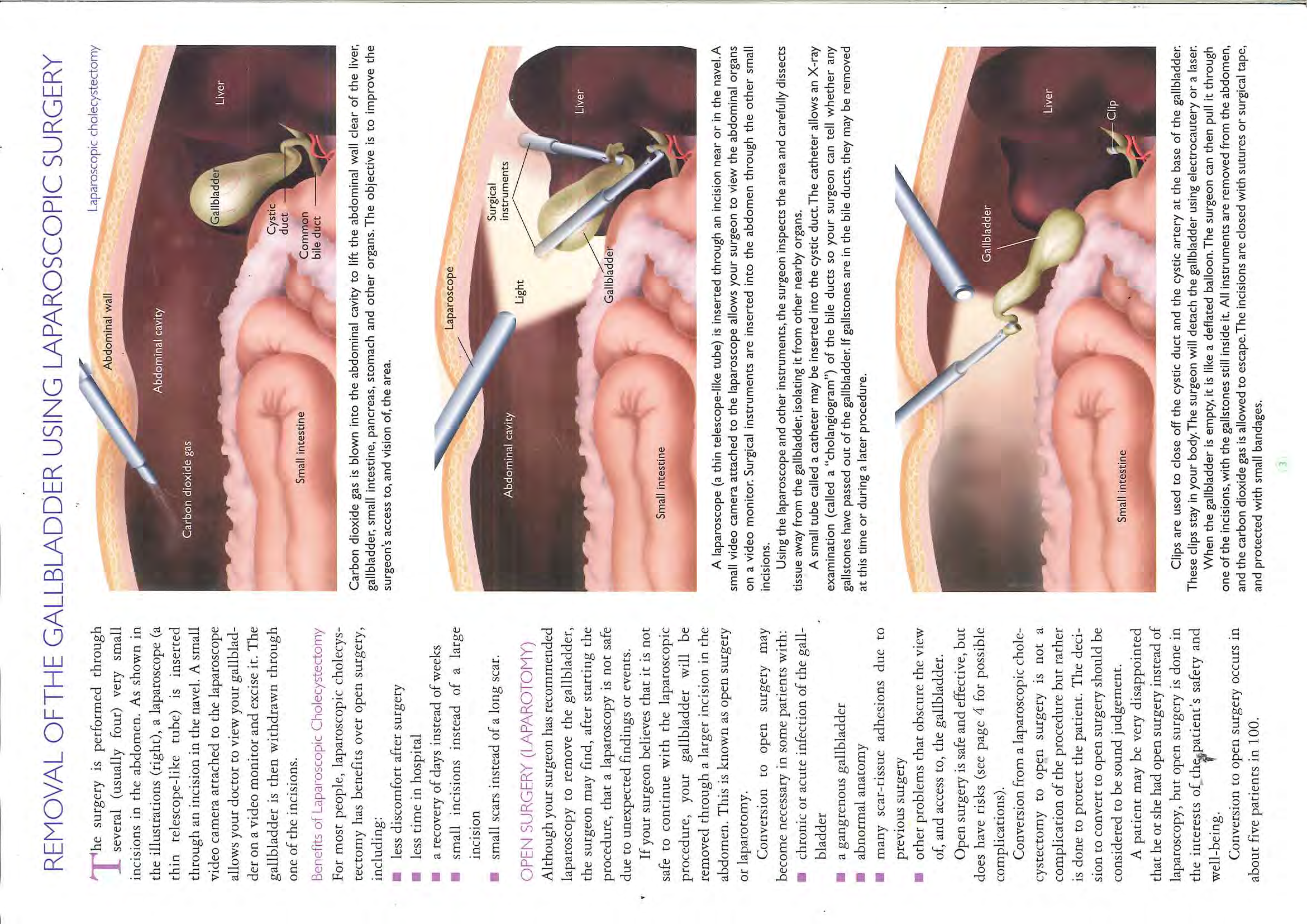
What is a laparoscopic cholecystectomy?
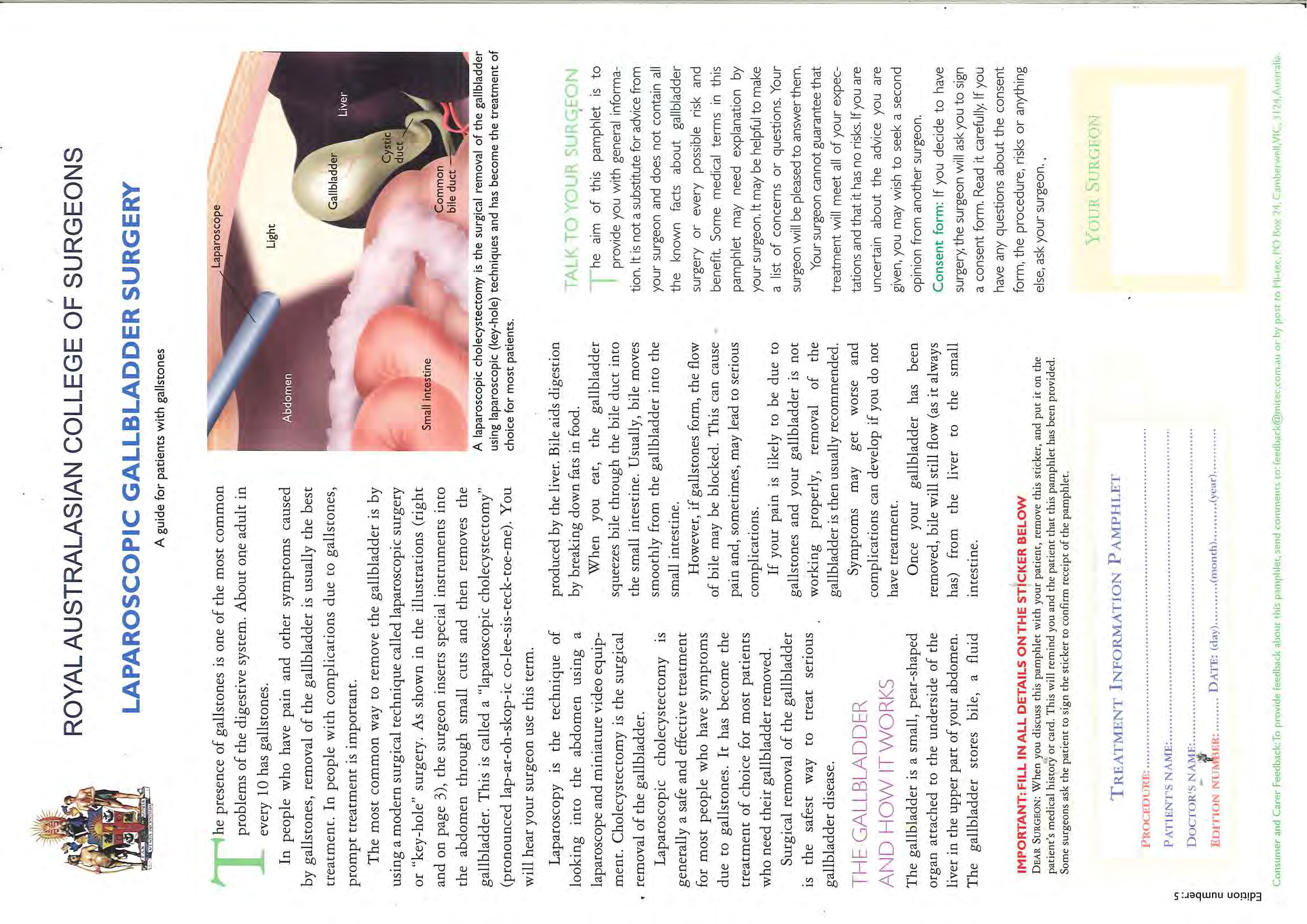
This is the surgical method of removing the gallbladder using a keyhole technique. Your
surgeon will make 3-4 small cuts on your stomach and inserts a telescope and a light
through these holes to locate and remove your gallbladder.
Sometimes during the operation, the surgeon may need to change from a keyhole
technique to an open technique. This is called an
open cholecystectomy. This results in
a larger wound and you may require a longer stay in hospital.
How long will I be required to stay in hospital?
Your nurse will encourage you to get up and get back to normal activity as soon as
possible. Most patients are able to go home within 12-24 hours. You will feel tired
afterwards and you should allow your body the time it needs to rest and recover. Most
people can return to work and mild activity within 4-10 days. Avoid heavy lifting for four
weeks after surgery to allow your stomach muscles to heal.
When can I eat and drink?
You will be able to eat and drink as soon as you feel able. You may suffer some nausea
(this is common), which may be managed with some oral medications. Please advise
your nurse if you feel nauseated.
Having had gallbladder surgery you may wish to restrict your intake of fatty foods,
however this is not a requirement.
Will I experience pain after the procedure?
You may experience moderate pain in the first 24-48 hours. You will be offered regular
Ref: 2051
Authorised by: Director of Surgical Nursing Services
February 2018
oral pain relief while in hospital, please tell your nurse if you start to feel sore. You will receive a script
on discharge if you require on going pain relief.
What is shoulder tip pain?
This is something you may or may not experience following your surgery. It is caused by small bubbles
of the gas (used to inflate your stomach) rising up beneath your diaphragm. This causes referred pain
to occur in your shoulder blades. This pain usually eases within 36 hours and can be managed with
pain relief and mobility.
How do I manage my wound?
You will have 3-4 small wounds on your stomach, each covered with an adhesive tape dressing. The
tape usually stays in place for 7-10 days, but can be removed if they become dirty. Please note:
If you
required an open cholecystectomy, you will have an additional wound approximately 6 cm in length.
This wound may have some minor bruising around it for the next week or so.
The stitches are all dissolvable and may take up to 3 weeks to dissolve. Do not be alarmed if you
discover any small ends coming through your skin, simply trim these off with scissors after a few days
at skin level.
You may shower as normal, it does not matter if your wounds get wet. Pat dry.
Sometimes wounds can become infected. If you note redness, discharge or experience increased pain,
please seek medical assistance.
When should I see my GP?
We recommend that you see your GP in one week, when we expect the specimen report to be
available. Your GP will discuss with you any concerns or abnormalities, which is unusual. We expect
the report to simply show that your gallbladder was inflamed.
During your visit ask your GP to check your wounds and also ask any questions you have.
If you have any questions that cannot be answered, we are more than happy to see you in our
outpatient clinic. However, we do not routinely follow up patients after cholecystectomy.
Please contact your GP if you:
develop a fever
develop yellow skin or eyes
experience increased stomach pain or distension
experience on going diarrhoea
experience persistent nausea or vomiting
notice your wound becoming red, inflamed or discharging
If you have any concerns please contact your
General Surgical Wards
G.P. or, outside business hours, contact the
Christchurch Hospital
after-hours surgery
In case of an emergency, call 111
Phone (03) 364 0640
For more information about:
your health and medication, go to www.healthinfo.org.nz
hospital and specialist services, go to www.cdhb.health.nz
Ref: 2051
Authorised by: Director of Surgical Nursing Services
February 2018


 Managing At Home After Abdominal Sur-
Managing At Home After Abdominal Sur-
gery
Patient information - Department Occupational Therapy
Ideas for Managing at Home after your
Abdominal Surgery
py
After your abdominal surgery you will find that your
ra
abdomen is tender, especially when reaching,
fter
The
bending or lifting objects. It is recommended that after
A
your surgery you do not lift anymore than 2-3kg. Any
y
onal
me
ti
a
more than this and it will cause strain on your wound.
o
er
H
rg
up
This booklet provides some useful tips on how to
t
c
manage your pain during the everyday tasks that you
A
Su
g
al
do. You may find that some ideas work better than
in
in
others or you may already have ways that work for
ag
n
o
rtment Oc
you.
an
d
b
An Occupational Therapist will discuss with you the
M
A
Depa
aids that you require. Most equipment is available for
short-term loan from the Occupational Therapy Department. Should you have any
problems
relating to daily living activities, an Occupational Therapist will advise and/or
recommend practical assistance where necessary.
Always follow the advice of you Consultant, Surgeon or General Practitioner.
Dressing
Sitting to get dressed decreases the distance to reach your feet for putting on
shoes/socks.
An easireach may help with dressing lower limbs if it is too painful to bend over to
reach your feet.
Sock aids can be used for putting on socks, so you do not have to bend to reach
your feet.
Long handled shoe horns.
Wear slip on shoes or use elastic laces to prevent having to tie shoelaces.
Move frequently worn clothes into drawers that are
of
waist height
Ref:2472
Authorised by: Clinical Manager, Occupational Therapy
August 2010
 Showering
Showering
Using long handled brushes and toe wipers can assist washing lower body.
Sitting on a shower stool or bathboard to shower will make it easier and safer when reaching to wash
legs.
Place shampoos, conditioners and body wash at waist level
If having difficulty drying your feet, place a towel on the floor and rub your feet on it. You can then get
another person to pick it up or you could use your easireach.
Toilet
You may find getting on and off the toilet painful, particularly if the toilet is low and you need to lean
forward to get off the toilet. You may find a raised toilet seat or an over toilet frame useful.
Laundry
Wash clothes regularly so carrying large amounts of wet clothes is avoided.
Only carry small amounts of wet washing at a time e.g. 2-3kg.
Use a laundry basket on wheels, or place your washing basket on a stool, so
you don’t have to reach to the ground to pick up clothes
or place your washing
basket on a chair at the washing line to avoid repetitive bending.
Adjust your washing line so you do not have to excessively stretch to reach it.
If your washing line causes excessive reaching, use a clothes horse instead to
hang washing on.
Bed
If you have difficulty or find it painful moving and getting out of bed. An Occupational Therapist can give
advice about techniques on making the process easier. There is also equipment available such as bed
loops which may help.
Kitchen
Move food/plates/pots to waist height so reaching and bending are eliminated.
Slide heavy objects along the bench whenever possible rather than lifting them.
Place frequently used items on higher shelves in the fridge.
Driving
Ask your doctor when you will be able to resume driving as it will depend on the type of surgery that
you have had (e.g. laparoscopic or open surgery). You may find it comfortable to place a small pillow
on your stomach to stop the seatbelt from rubbing or pressing against your wound.
If you have any concerns or queries please do not hesitate to con-
tact the
OCCUPATIONAL THERAPY DEPARTMENT
For more information about:
your health and medication, go to www.healthinfo.org.nz
hospital and specialist services, go to www.cdhb.health.nz
Ref:2472
Authorised by: Clinical Manager, Occupational Therapy
August 2010
(Attach Label here or Complete Details)
Page 1 of 2
(Attach Label here or Comp N
let A
e M
D E
et :_
ail_
s__
) _______________________________________________ NHI:__________
R
Request for Treatment
NAME:___________________________________________________ NHI:__________
GENDER: ____ DOB:______________ AGE:______
b
y WAR
OpD:__
er ______
ati ___
on ___
/ __
E
GENDER: ____
DOB:______________
AGE:______
WARD:________________
Procedure
Q
U
REQUEST FOR TREATMENT BY OPERATION / PROCEDURE
E
AGREEMENT FOR BLOOD OR BLOOD PRODUCT TRANSFUSION
I,
S
Health
Pro
fe R
ss e
i q
o ues
nal t and agree that the following operation/procedure (specify side by
writing RIGHT or LEFT or BILATERAL)
T
(Print Name)
(Print Designation)
whose signature appears below has advised me that I / my child / my ward may require a blood or blood product transfusion.
(delete as appropriate)
F
Having had the opportunity to ask questions and discuss the possible risks and benefits and the alternatives to a blo od or blood
O
produ be
ct p
traer
n f
s or
fu m
si ed
on o
w n
i m
th e
hi /
m m
/h y
e c
r, hi
I ld /
AG ward
REE / DO NOT AGREE to blood products EXCEPT:
(delete as appropriate)
R
I understand that if found essential, further or alternative operative/procedural measures may be undertaken during the
being c
aour
dm s
i e
ni o
st f
e the
red oper
to m at
e i/on/
m p
y r
coc
hil e
d d/ure.
my ward should the use of such products be deemed necessary.
In the course of the p
(r
doc
ele e
tess
a so
af
pm
pr y
op rm
iata
ek
)ing the decision to request this operation/procedure to be undertaken, one or more
T
of the fol owing methods was used to give me the details and information I expected and required.
(Tick appropriate
NZ Blood Service leaflet given to patient
Yes
R
boxes)
S
igned: Verbal discussion
Surgical Consultation letter
E
Hand drawings/diagrams
(Patient / Parent / Other)
Anatomical model, bone specimen
(Date)
A
Illustrations from a surgical textbook or journal
Implant or device to be inserted
Signed:
T
Printed handout/pamphlet
(affix deta
( chab
Health le l
Profabe
e
l
ssio b
na e
l) low)
Video, CD Rom, DVD
(Date)
The showing of X-ra
If
y
bl s/s
oo c
d ans
or beith
lo e
od r a
p s film
rodu s
ct o
s r o
a n
re a
not require O
d, th
c e
ror
s (s
s p
oec
ut ify
a )
nd write N/A
M
computer (PACS)
DECISION TO TREAT MADE BY ATTENDING MEDICAL PRACTITIONER
E
and in so doing, I was informed of both benefits and risks including possible rare but serious risks, these benefits and
The de rciisskis
o ninc
to ludi
un ng:
dertake a procedure or administer blood or blood product to a patient who is unable to provide consent or for
N
who m t here is no legal representative is ultimately the responsibility of the doctors caring for the patient. However, it is the
Canterbury District Health Board’s policy to consult, where practical, members of the patient’s family, significant others an d/or
T
any one else with a legitimate interest in the care of the patient in order to help determine what the patient’s wishes might be.
I,
Dr
(Print Doctor’s Name)
(Print Designation)
hereby certify that the condition of
(Print Patient’s Name)
is such that consent cannot be obtained prior to:
By Health
Professional
(Print Name)
(Print Designation)
which I further certify is, in my opinion, in her/his best interests.
This health professional whose signature appears below has explained to me the reasons for and other alternative
treatments to this operation/ procedure. I have had adequate opportunity to ask questions and have received all the
In reaching this opinion, I have taken into account information provided to me by others with an interest in her/his welfare, the
information that I want. I understand that I am welcome to ask for more information if I wish. I acknowledge that an
signature of one of whom appears below as witness.
assurance has not been given that the operation/procedure wil be performed by a particular health professional, but
that person wil
A , howev
ND / O er
R , hav
(d e
ele a
teppr
as opr
appr iat
opre
ia te
ex
)perience.
In
reaching this opinion I have consulted with colleagues, the signature and name of one of whom appears below as witness.
Blood Testing: I agree to a blood sample being taken from me if a healthcare worker is directly exposed to my blood
Sign
or
ed: other body fluids during the course of this operation/procedure and I am unable to provide specific consent at or
shortly after the time of expos
(
ur
Doct e
or) due to the effect of anaesthesia or other drugs. Any sample taken wil only be te
( ste
Dat d
e)
Proof A
for such transmissible diseases that might be a risk to the healthcare worker, e.g. hepatitis B, hepatitis C and HIV.
Sign
I
ed: understand that I wil be informed if any such testing is undertaken and wil be advised of the results have been re-
assured that
( m
Heal y
th d
P e
roc
f i
e sion
ssion aw
l i
wl n
itneot hav
ss – sig e
n a
anny
d
prinf
int luen
nam c
e) e on whether or not my operation/procedur
( e
Desiw
g i
n l
a p
tio r
noc
) eed:
(Date)
Yes No
Signed:
(Patient’s witness – sign and print name)
(Relationship to patient)
(Date)
Body Tissues, Body Parts or Prostheses: Do you have any specific requirements for the return or disposal of
body tissue, body parts or prostheses?
Q
NOTE S
FOR STAFF
Yes (complete Tissue Return and Disposal Form C230007)
Procedure to be followed when the patient or legal guard
No
Not applicable
ian cannot/is not available to provide consent:
M
In these situations, medical staff can undertake those measures which are in their opinion necessary and in the patient’s best interests to save
life or prevent permanent physical and mental injury and/or to prevent prolonged unavoidable pain and suffering, provided that:
R
1.
S
R
ign
eas
ed:
onable at tempts have been made to obtain consent taking the clinical situation and the time avail able
into consideration.
0
2.
They
are in a position to document justification for proceeding without obtaining consent.
(Patient / Parent / Other)
(Date)
3.
Where time permits the specialist having overall responsibility for the patient is aware of the proposed action.
0
4.
Where appropriate and where time permits, the specialist-in-charge has sought a second opinion from another medical practitioner with
Signed:
appropriate ex perience.
2
In non-urgent situations, reasonable steps must be taken to ascertain what the patient’s informed choice might be in the given circumstances.
(Health Professional)
(Date)
This may necessitate seeking opinion from others having an interest in the welfare of the patient. In this regard staff are referred to Right 7(4)
A
of the Code of Health and Disability Services Consumers’ Rights.
CONSENT FOR BLOOD OR BLOOD PRODUCT TRANSFUSION LOCATED OVERLEAF
125627
Ref. 1747
Page 2
1of 2
Authorised by: Chief of Surgery
August 2017
Page 1 of 2
(Attach Label here or Complete Details)
Request for Treatment
NAME:___________________________________________________ NHI:__________
by Operation /
GENDER: ____ DOB:______________ AGE:______ WARD:________________
Procedure
AGREEMENT FOR BLOOD OR BLOOD PRODUCT TRANSFUSION
Health
Professional
(Print Name)
(Print Designation)
whose signature appears below has advised me that I / my child / my ward may require a blood or blood product transfusion.
(delete as appropriate)
Having had the opportunity to ask questions and discuss the possible risks and benefits and the alternatives to a blo od or blood
product transfusion with him/her, I AGREE / DO NOT AGREE to blood products EXCEPT:
being administered to me / my child / my ward should the use of such products be deemed necessary.
(delete as appropriate)
NZ Blood Service leaflet given to patient
Yes
Signed:
(Patient / Parent / Other)
(Date)
Signed:
(Health Professional)
(Date)
If blood or blood products are not required, cross out and write N/A
DECISION TO TREAT MADE BY ATTENDING MEDICAL PRACTITIONER
The decision to undertake a procedure or administer blood or blood product to a patient who is unable to provide consent or for
whom there is no legal representative is ultimately the responsibility of the doctors caring for the patient. However, it is the
Canterbury District Health Board’s policy to consult, where practical, members of the patient’s family, significant others an d/or
anyone else with a legitimate interest in the care of the patient in order to help determine what the patient’s wishes might be.
I,
Dr
(Print Doctor’s Name)
(Print Designation)
hereby certify that the condition of
(Print Patient’s Name)
is such that consent cannot be obtained prior to:
which I further certify is, in my opinion, in her/his best interests.
In reaching this opinion, I have taken into account information provided to me by others with an interest in her/his welfare, the
signature of one of whom appears below as witness.
AND / OR
(delete as appropriate)
In reaching this opinion I have consulted with colleagues, the signature and name of one of whom appears below as witness.
Signed:
(Doctor)
(Date)
Proof A
Signed:
(Health Professional witness – sign and print name)
(Designation)
(Date)
Signed:
(Patient’s witness – sign and print name)
(Relationship to patient)
(Date)
NOTES FOR STAFF
Procedure to be followed when the patient or legal guardian cannot/is not available to provide consent:
In these situations, medical staff can undertake those measures which are in their opinion necessary and in the patient’s best interests to save
life or prevent permanent physical and mental injury and/or to prevent prolonged unavoidable pain and suffering, provided that:
1.
Reasonable attempts have been made to obtain consent taking the clinical situation and the time available into consideration.
2.
They are in a position to document justification for proceeding without obtaining consent.
3.
Where time permits the specialist having overall responsibility for the patient is aware of the proposed action.
4.
Where appropriate and where time permits, the specialist-in-charge has sought a second opinion from another medical practitioner with
appropriate experience.
In non-urgent situations, reasonable steps must be taken to ascertain what the patient’s informed choice might be in the given circumstances.
This may necessitate seeking opinion from others having an interest in the welfare of the patient. In this regard staff are referred to Right 7(4)
of the Code of Health and Disability Services Consumers’ Rights.
Ref. 1747
Page 2 of 2
Authorised by: Chief of Surgery
August 2017
 Reducing the Risk of Blood Clots
Reducing the Risk of Blood Clots
Patient information - Department General Surgery
Why you need to know about clots
d
o
o
ry
If a blood clot forms in your leg (deep vein thrombosis), it can affect blood flow, and
B
f
may cause severe pain and swelling. It may also cause permanent damage to your
o
urge
leg. If a blood clot forms, some of it may travel through your veins to your lungs and
l S
isk
block their blood supply (pulmonary embolism). Without blood, your lungs cannot send
R
ra
ne
oxygen to the rest of your body. You may have trouble breathing or, in rare cases, you
e
may die.
th
g
n
Studies have shown that treatment will reduce the chance of you developing a blood
ci
u
rtment Ge
clot. The following list shows the main things that put you at risk of developing a blood
ts
ed
lo
clot in the leg or lung:
R
C
Depa
Hip or knee replacement
Prolonged surgery
Stroke
Heart Failure
Cancer
Severe lung disease
Severe infection or inflammation
Having a previous blood clot in the leg or lung
What your health care team will do
At your pre-admission appointment or at the time of admission, the risk of a blood clot
forming in your legs or lungs will be assessed. Your level of risk will depend on:
Your age
Your type of surgery
Any other health problems you have had in the past
Ask your doctor or nurse about your level of risk for developing a blood clot. If you are
at risk, your health care team will discuss treatment options with you. Treatment may
include:
Wearing compression stockings
Using a compression pump on your lower legs during surgery
Taking tablets or injections to help prevent a blood clot
Gently exercising your feet and legs while in bed
Getting out of bed and walking as soon as possible
Ref:2475
Authorised by: Saxon Connor Consultant
June 2010
Some of these treatments may not be suitable for some people. If you are at high risk, your
healthcare team may recommend more intensive treatment.
Ask your doctor or nurse what treatments they recommend for you.
What you can do to reduce the risk of blood clots forming
While you are in hospital you should:
1. Make sure you get any tablets or injections your doctor has prescribed to reduce your risk
2. Keep your compression stockings on
3. Read the patient information pamphlet on TED stockings
4. Avoid sitting or lying in bed for long periods
5. Walk as often as your doctor advises
6. Drink plenty of fluid if allowed.
Before you leave hospital, ask your doctor or nurse what to do when you go home. Find out:
How long to wear your compression stockings
Whether you must use any medicines
What physical activity you need to do
Whether you have to avoid alcohol
What else you and your family can do to reduce the risk of a blood clot.
What to watch for
If you experience any of the following while you are in hospital, call a nurse immediately:
Pain or swelling in your legs
Pain in your lungs or chest
Difficulty breathing
If you have any of these signs after you have left hospital, telephone your doctor immediately or go
straight to the Emergency Department (Ph: 364 0270). In the case of an emergency dial 111 for an
ambulance
Acknowledgement:
Adapted from
Stop the Clot Programme, National Institute of Clinical Studies, Australia, April 2009
For more information about:
your health and medication, go to www.healthinfo.org.nz
hospital and specialist services, go to www.cdhb.health.nz
Ref:2475
Authorised by: Saxon Connor Consultant
June 2010



Patient Controlled Analgesia
Patient information - Department of Anaesthesia
www.healthinfo.org.nz
What is a PCA?
a
a
PCA stands for ‘Patient Controlled
si
t
lled
e
Analgesia’. It is a special pump that gives you
o
esi
tr
g
sth
pain relief (analgesia) when you want it.
en
n
al
e
a
o
n
Pati
C
A
n
A
Who gets a PCA?
This will depend on the type of surgery you are
having. Your Anaesthetist will talk to you about this.
How does a PCA pump work?
The pump contains strong pain relief (e.g. morphine, fentanyl).
The pump is connected to a drip which goes into a
vein in your hand or arm. When you press the
green button, the pump delivers pain relief to you
through the drip.
You control how much pain relief you get by
pressing the button when you need it.
The pain relief takes about five minutes to work.
How do I use a PCA?
You will be shown how to use your PCA before it is given to you by your nurse.
Press the button on the PCA when you are sore, or five minutes before doing
something that will cause pain or discomfort like moving or getting out of bed.
To help you know when the next dose is available, the green button will light up when
it is ready to press.
To prevent an overdose, you must not let anyone else press the button!
Ref. 131
Authorised by: Acute Pain Management Service Clinical Coordinator
November 2014
 What if my pain relief doesn’t work?
What if my pain relief doesn’t work?
If your pain is not being helped by your PCA, please tell your nurse. Your nurse and the Acute Pain
Management Service will oversee your pain relief.
How safe is PCA?
Your PCA has safety features to stop you overdosing on pain relief and it is programmed to release a
safe amount of pain relief each hour.
Nurses will be closely monitoring you while you use the PCA.
Do not press the PCA button if you are comfortable or sleepy, and don’t let others press the button.
Can I become addicted?
Strong pain killers can be addictive however when taken for pain after surgery, this risk is very small.
Are there any side effects?
All medications can produce side effects. Possible side effects include nausea, vomiting, constipation,
drowsiness, difficulty concentrating, hallucinations, itchiness and difficulty passing urine.
Please let your nurse know if you get any side effects so you can be treated for them quickly. If you
have questions or problems with your PCA tell your nurse. Rarely your breathing can be slowed down to
a dangerous level however you will be monitored for this.
How long will I have a PCA?
This will depend the amount of pain you have after your surgery. Your nurse and the Acute Pain
Management Service will oversee this.
Finally….
We think the PCA will suit you. It lets you control your pain because you know best how you feel.
Ref. 131
Authorised by: Acute Pain Management Service Clinical Coordinator
November 2014
Document Outline