




Caring for Prisoners At Risk
Caring for Prisoners At Risk
Caring for Prisoners
A Gui
de fo
r Staff
At Ri
sk
Page 35 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 1
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Contents
The Department's Philosophy
Recognising risk—when to be concerned
Reception into a prison
Reviewing when things change
Mental health
Impact of a suicide or suicide attempt on staff
Special issues for youth offenders
Interviewing At Risk Prisoners
Page 1 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 34
Caring for Prisoners At Risk
Caring for Prisoners At Risk
4 Stage Listening Contd.
The Department’s Philosophy
Stage Four– Check how the action worked
Arrange another interview
The Department of Corrections acknowledges that
You can check quickly if the action plan worked
all prisoners by virtue of being in prison pose an
If the plan worked—fine. If not, you may need to explore why not, and
increased risk of self harm or suicide.
plan other options
The most important part of this stage of reworking the plan is to let the
Definition of At Risk
prisoner suggest options.
A prisoner who has been assessed as being “at risk” of harming
themselves..
\
Self harming behaviour (range of behaviours from cutting to
actions which are intended to lead to death)
5 Rules for Describing Interviews
Primary Principles
Everyone is responsible for the early identification of a prisoner’s at
risk status and for taking immediate action when such risks are
Focus on behaviour rather than the person
identified.
Focus on observations rather than inference
The level of risk presented by the prisoner should be minimised as
Focus on description rather than judgement
quickly and safely as possible.
Focus on the here and now rather than there and then
Key Principles of Policy
Focus on what is said rather than why it is said.
Care is central to everything we do and can only be achieved through
effective multi-disciplinary teamwork
Everyone in the prison community must take immediate action when
risk is identified
Decisions about At Risk Prisoners must be made by teams and not
individuals
All staff are required to be vigilant and recognise that a prisoner is in
crisis and their behaviour may unsettle other prisoners
Since assessment techniques alone are not enough to prevent
suicides, there is a need to create a context where prisoners feel safe
and confident to ask for help.
Page 33 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 2
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Current Statistics
4 Stage Listening
4-Stage listening is a model to help people to solve their own problems:
Between 2006 and 2009, there were 17 prisoner suicides in custody.
The stages are separate and you don’t have to go through all of them
At least 190 prisoner’s lives have been saved in the same period (this
number relates to self harm incidents where the individual would been
Often Stage 1 is enough—it will make people feel heard
unlikely to survive without intervention)
Sometimes it is better to refer a prisoner on for stages 2 & 3, and come
Hanging was the method most commonly used.
back for Stage 4
Over 70% used their bed sheets as ‘rope’
But sometimes we need to “seize the moment”.
Air ventilation grills were the most common hanging point
90% were committed in maximum or high security units—this is likely
Stage One—Explore the problem
to be linked to violent offenders, who are not afraid to act on these
tendencies, being more likely to commit suicide
Just listen actively while the prisoner talks (this may take longer than
most people allow)—use your listening skills
Male prisoners were more likely to take their own lives
Avoid questions as far as possible
Suicides were more likely to occur in the first six months of
incarceration. 35% were in remand; 65% sentenced
Use “follow-ons” and encouragements only to persuade the prisoner to
keep talking.
Prisoners with a history of suicide and self harm attempts are more
likely to take their own lives
While not totally definitive, prisoners aged 35-39 presented as the most
Stage Two – Focus And Share Perspectives
common age group, followed by 18-19, 20-24 and 25-29
Carry on listening actively
Both Maori and NZ European were equally represented in the suicides
Encourage the prisoner to focus on the most important parts of their
41% of suicides occurred during October and November
problem
11 of the 17 suicides were by prisoners who were drug users, either
e.g. give some information that would help them, or ask a few more
recreational or prescribed.
questions to get them thinking
Don’t advise or problem solve for them.
Stage Three – Help The Prisoner To Plan Action
Carry on listening actively
The pace may become more “business like” here
Encourage the prisoner to take the initiative in planning what they want
to do
You may have some suggestions, but don’t overdo it.
Page 3 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 32
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Suicide Risk After Self-Harm or
Attempted Suicide
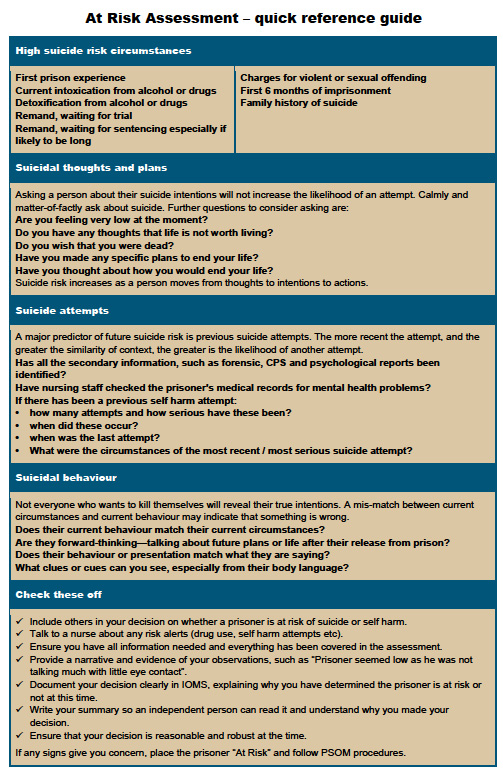
Recognising Risk—
When to be Concerned
Some people
Use self harm as a coping strategy with no plans of suicide
Assessment of At Risk Status
Use self harm as a way of communicating intense distress to others
Assessing suicidal risk is not an exact science especially within the prison
Suicide risk is higher in people who make a number of suicide attempts
setting, as prisoners can present with a number of predisposing factors such
with increasing frequency and increasing seriousness
as drug misuse and mental health problems.
The risk of suicide following a suicide attempt is 100 times that of the
Assessment is a dynamic process where levels of risk often change. All
general population.
prisoners are vulnerable to some degree and often give “clues” when they
are worried. Sometimes there are “cues” in their personal histories (the
predisposing factors), which can lead us to the view that they are especially
Listening Challenges
vulnerable. We need to be aware of these “clues and cues”.
Be aware of the challenges you need to overcome:
People who attempt or commit suicide often show distress or intent that can
be detected by observing, listening and asking. Be aware that some may
(other) prisoners putting demands on you
conceal their intent. Consider what the person says and does.
Sorting out practicalities
Having to do At Risk assessments in a very short time
Distress signals—ask the person about them
Being tempted to listen “so far and no further”
Coming up with advice or a practical solution and stop listening.
Characteristics of Prison Increasing the Risk of Suicide
Authoritarian environment
When helping someone, try listening for longer
No apparent control over future
Relax
Isolation from friends, family, community
Slow down
Shame of imprisonment
Offer time
Dehumanising effects of imprisonment
Use active listening.
Fears
Staff insensitivity to arrest and imprisonment
Take time to listen before you:
Negative expectations about short term / long term future
Offer practical help
Sense of hopelessness
Discuss what the prisoner should do
Ask about suicidal intentions (but get to this when appropriate).
Page 31 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 4
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Behaviours to watch for
Factors
Crying, emotional outbursts
Recent suicide attempt
Factor which make suicide more likely
Giving away possessions
Immediate intention to carry out suicide
Withdrawal from social contact
Specific plan of suicide
Self neglect (e.g. not eating)
Choice of violent method of suicide e.g. hanging
Not planning for release
Access to means of committing suicide
Increase in frequency or lethality of self harm
Plans for death e.g. will changes, family farewells
Alcohol / Drug abuse
Recent escalation of:
Irrational behaviour, out of touch with reality
Suicidal behaviour e.g. self harm
Recklessness / fighting
Help seeking behaviour e.g. seeing the chaplain
Hostile rejections of help
Current symptoms of mental disorder
Thoughts
Past high-risk suicide attempt
“There’s no point…”
Likelihood of bad news—’the last straw’
“I can’t take it any more.”
A self imposed deadline passes without the good news the prisoner
hoped for.
“I wish I were dead.”
“Everyone would be better off without me.”
Factors which make suicide less likely
“I just want it to be over.”
Looking forward to future events
“Nothing will ever get better.”
A statement from the prisoner that he/she will not commit suicide if an
“There’s no future for me.”
event occurs. However, this lowers immediate risk only. Beware if the
event is not under the prisoner’s control e.g. “I will not commit suicide if
my wife comes back to me before I go to court.”
Fear of:
Death
Being left physically / mentally damaged
Attempt having no effect on family / friends
No-one to look after children / significant others
No access to means of suicide.
Page 5 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 30
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Avoid Ambiguous Questions
Feelings expressed
Desperate
Angry
Some people are not direct enough in their questioning because they feel too
embarrassed or awkward asking about suicide plans for fear of giving the
Sad
person the idea.
Ashamed
You cannot plant the idea if it was not there before
Hopeless
Prisoners who are feeling suicidal are more likely to be comfortable
Worthless
talking about it if you are comfortable asking them
Lonely
Most reveal suicide intent when questioned directly by a sympathetic
interviewer
Disconnected
Only a minority of people deny suicidal intent when in fact they are
Powerless
planning suicide.
Physical changes
Ambiguous questioning may receive an unclear answer e.g. “Have you
Lack of interest / pleasure in everything
thought about doing something silly?”
Lack of physical energy for no apparent reason
A “yes” response may be interpreted as suicidal ideation when in fact
the prisoner may have been thinking of escape or picking a fight
Disturbed sleep
Your idea of “something silly’ may not be what the prisoner thinks on
Change / loss of appetite, weight
as “something silly”
Increase in minor illness
So be clear and direct.
Situations / triggers
Relationship problems
Recent suicide of someone close to them
Violence, bullying or fear of these
Parole refusal or other knock back
Longer sentence than expected
Page 29 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 6
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Times of Heightened Risk
Explore Hopelessness
First 24 hours of confinement
Intoxication/withdrawal
Hopelessness is the best predictor of suicide. Hopelessness is:
Waiting for trial
Characterised by feelings that the current situation is not only
Pre / Post Court appearances
intolerable right now, but will never improve in the future
Sentencing, especially if sentence likely to be harsh
“Do you think your life could ever get better?”
Impending release
Often associated with helplessness.
Night and weekends – times when staff numbers likely to be lower
Bad news from family, friends, community
Explore whether the prisoner believes anybody can help to improve the
current situation
First 30 days after imprisonment or movement to new facility
If a prisoner describes a degree of hopelessness or helplessness, or if
For pre-trial offenders, 60 days after imprisonment
you have reason to believe a prisoner to be suicidal, you should
4-5 years for long term sentenced violent offenders
specifically ask about thoughts of suicide
Periods of isolation
Does the prisoner have anything to look forward to? While prisoners
who look forward to an event are less likely to commit suicide in the
immediate future, be careful when prisoners plan to live until they have
seen through a particular event e.g. birthday, before committing
suicide.
Wishes to be Dead
Active wishes to kill oneself are more serious than passive wishes to be dead
e.g. “I just wish I could just go to sleep and not wake up”.
Specific Plans for Suicide
Has the prisoner had thoughts about harming or killing him / herself?
Are these thoughts fleeting or persistent?
Does the prisoner have any specific plans e.g. how, where, when,
etc.?
Page 7 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 28
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Clarification of Current Problems
Making an Initial Response
Find out and clarify problems over the last few months and the last 24 hours.
(In the Residential Unit)
You should check if there are problems relating to the following that the
prisoner has not spontaneously mentioned:
Relationship with partner, other family members, friends
Talk to the person. Ask them about what you are concerned about.
Comment on behaviour: “You’re looking really low. Is anything
Social isolation
wrong?”. Ask about events: “You were in court today weren’t you. How
Bereavement
did it go?” Give broad openings: “Tell me about it…. You look like you
need to talk things over with someone.”
Separation
Take time to listen. Talking about a problem is a strength, not a
Legal, including current court / police proceedings
weakness.
Physical health
Do not feel you need to solve the problem—support is delivered by a
Use of illicit drugs / alcohol
good team, not just an individual.
Mental health.
Check out how bad the person is feeling.
If you suspect the prisoner might be thinking of suicide, ask them as
directly as possible: “Are you thinking about suicide?” Or “Is it so bad
Specific Questioning About Suicidal
you are thinking of killing yourself?”
Intent
If there is risk, don’t leave the person alone. Alert other staff—custodial
and Health.
Begin a Review Risk Assessment.
Asking someone about suicidal thoughts will not plant an idea that was
not there before
Be aware that some people may conceal their
Most people who are contemplating suicide feel relieved to be able to
talk about it
intent. Consider both what the person says and
You cannot assess suicide risk without specific questioning
also what they do.
Specific information will help if you need to refer the prisoner to other
professionals—it may even speed up the process.
Talking about suicide with someone will give them the opportunity to:
Express their feelings
Give them a sense of relief
Discover a reason to live
Talking about suicide will not cause someone to do it.
Page 27 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 8
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Demonstrate acceptance of the prisoner
Non-verbal communication encourages the prisoner to speak:
Nodding
Saying “uh-huh”
Eye contact (be aware of cultural norms though)
Reflect or paraphrase what the prisoner says and empathise. This
helps the prisoner speak about difficult issues:
“I can see that things have been very difficult for you lately”
Clarify ambiguities
Sometimes prisoners do not express themselves very clearly. Clarify a
prisoner’s subjective experience:
“What exactly do you mean by ‘wound up’?”
Summarise
Go over what has been discussed and ask if it is correct. This:
Enables the prisoner to correct any misconceptions or factual
inconsistencies
Shows the prisoner you have been listening
Shows you are taking the problems seriously
Gives some hope to the prisoner that his/her situation can improve.
Page 9 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 26
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Questioning Style
Start off with open questions i.e. questions that get the prisoner talking
Reception into a Prison
Avoid ‘why’ questions at first—these can involve opinion rather than
fact
Avoid questions that can be answered with only ‘yes’ or ‘no’. These
Assessment Tools
have the effect of shutting the prisoner down
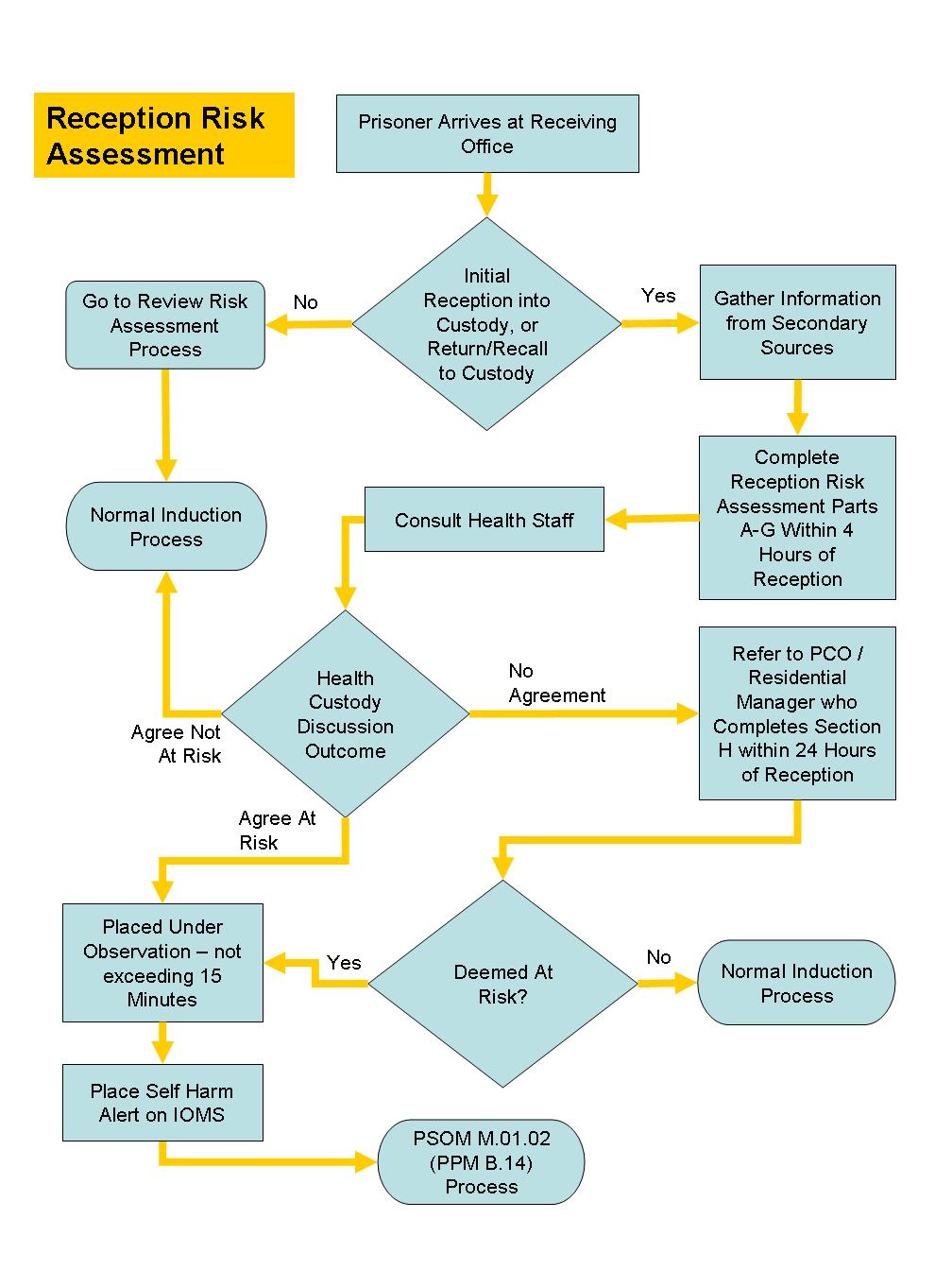
Reception Risk Assessment
Listen more than you question—the prisoner should do most of the
talking at first
Reception Risk Assessment
Once the prisoner speaks about specific problems, ask direct
questions to obtain the information needed
The Reception Risk Assessment is designed to assess the at risk
status of prisoners newly arrived at a prison. It will be administered by
Use closed questions—able to be answered with ‘yes’ or ‘no’ - only to
Receiving Office staff.
clarify facts.
The policy for its use and application is in the Prison Operations
Manual (POM) in section M.05.01.
Pick up verbal and non-verbal cues
Pay attention to:
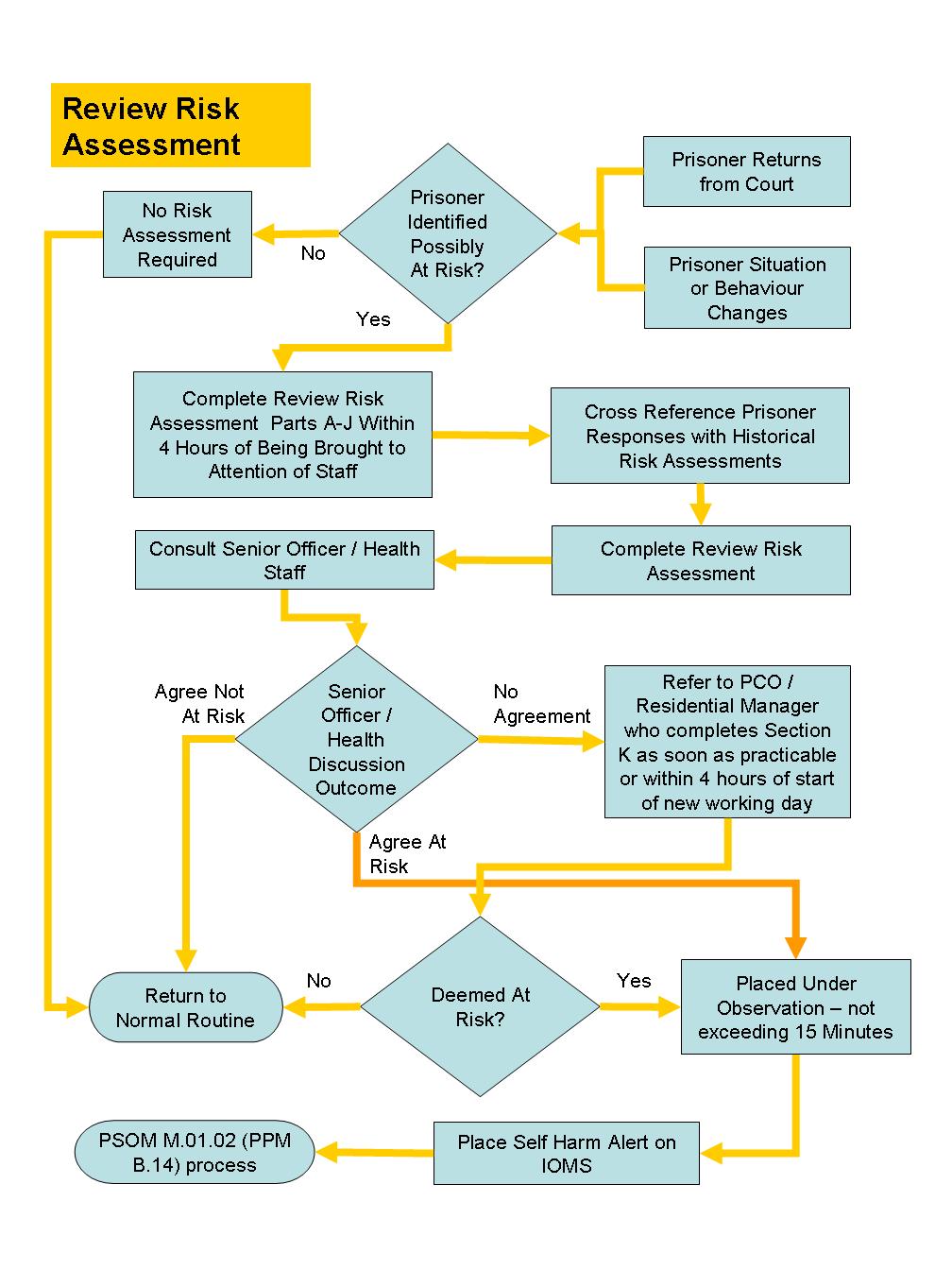
Review Risk Assessment
Key words or phrases that refer to emotional topics and social
The Review Risk Assessment is designed to assess the at risk status
information:
of prisoners already incarcerated at a prison. It will be administered by
Receiving Office staff only when a prisoner returns from court. In all
“I have been feeling very wound up lately”
other instances, it will be administered by Unit custody staff.
Non-verbal signs of possible emotional disorder:
The policy for its use and application is in the Prison Operations
Tearfulness
Manual (POM) in section M.05.02.
Signs
Agitation
Restlessness
Pacing
Lack of eye contact (be aware of cultural norms though)
Slouched posture.
Page 25 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 10
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Interviewing At Risk Prisoners
Establishing rapport
Questioning style
Pick up verbal and non-verbal cues
Demonstrate acceptance of the prisoner
Clarify ambiguities
Summarise
Establishing Rapport
“Active Listening” means:
Introduce yourself by name
Explain what will happen, why, and how long it will take
Interview the prisoner in a quiet setting, if possible
Arrange the seating appropriately—try to be on the same level
Maintain eye contact
Beware of looking excessively at notes or the computer
Be aware of cultural norms about eye contact
Use the prisoner’s name
Keep the pace of the interview unhurried and not challenging
Page 11 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 24
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Reviewing When Things Change
Assessment Tools
Review Risk Assessment
Review Risk Assessment
The Review Risk Assessment is designed to assess the at risk status
of prisoners already incarcerated at a prison. It will be administered by
Receiving Office staff only when a prisoner returns from court. In all
other instances, it will be administered by Unit custody staff.
The policy for its use and application is in the Prison Operations
Manual (POM) in section M.05.02
Page 23 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 12
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Special Issues for Youth Offenders
Introduction
Youth present a special set of conditions which can lead to suicide or self
harm.
The experience of incarceration may be particularly difficult for youth
offenders who are separated from their families and friends. Distressed
young prisoners are especially dependent on supportive relationships with
the staff. Therefore, separating and isolating young prisoners may lead to
additional risk for suicidal actions, which can happen at any time of their
confinement.
Youth offenders who are placed in adult correctional facilities should be
considered to be at particularly high risk of suicide.
An important note for recognition of risk in young people—depressed mood
may present as irritable mood.
Another consideration is that many young people are impetuous and may not
show any indication of their intention to self harm or suicide. Getting them to
talk about how they are feeling is a way of getting them to reveal what actions
they may be contemplating.
Page 13 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 22
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Mental Health
Introduction
One of the risk factors for suicide is having a mental health illness. The
World Health Organisation estimates that 90% of all suicide victims have
some kind of mental health condition, often depression or substance abuse.
Suicide is a major cause of premature death amongst people with mental
illness.
Mental Health in Prison
There is a many types of mental health disorders in a prison setting. These
can include:
Schizophrenia
Bipolar Affective disorder (previously known as Manic Depression)
Depression
Anxiety disorders like:
Phobias
Obsessive compulsive disorder (OCD)
Generalised anxiety disorder (GAD)
Post traumatic stress disorder
Alcohol and drug dependence or abuse can co-exist with a mental illness..
Treatment of a mental illness can reduce suicide risk. Suicide tendency can
be treated with therapy and medication. Early intervention and effective
management appear to reduce the risk over time.
Page 21 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 14
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Schizophrenia
Schizophrenia causes severe disruption to a person’s thought process.
Impact of Suicide or
Suicide Attempts on Staff
People with Schizophrenia often experience delusions or hallucinations, in
particular auditory hallucinations. Schizophrenia distorts the way a person
Introduction
thinks, feels or perceives things. This may lead to a withdrawal from reality.
Stress reactions in staff following a suicide or suicide attempt are common
Symptoms of schizophrenia may include:
and are normal reactions to an abnormal event.
Changes in personality and thought process
Common Stress Reactions
He or she has difficulty separating what is real from what is not
Constant thoughts of the suicide incident
Can become isolated and withdrawn
Reluctance to go back to the place it occurred in
Deterioration in personal hygiene and how they relate to others.
Tension
A numbness to surroundings
Acute symptoms of schizophrenia:
Inability to eat or sleep
Bizarre delusions
Constant tiredness
Exaggerated religious beliefs
Apathy, depression
Paranoid ideals
Irritability, outbursts of anger
Hallucinations
Extreme withdrawal
What to do to minimise the effects of stress
Sleep disturbance
Recognise that stress is a normal reaction
Threats of harm to self or others
Accept that taking care of yourself is a strength, not a weakness
Disruptive, aggressive, suspicious behaviour.
Talk about the experience with a colleague, friend, family member or
PIRT team
Take part in debriefing sessions
Get back to your normal routine as soon as possible. Time out from
working with prisoners can sometimes be more helpful than time off
work
Get enough sleep and regular exercise, and eat a healthy diet
Be more careful when driving or operating machinery. Accidents are
more common after severe stress
Call your PIRT team or EAP.
Page 15 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 20
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Six Resiliency Factors
Depression
Resilience is the process of adapting well to adverse situations. These
Many people who attempt suicide have experienced depression which may
factors contribute to counteracting the negative impact of the adverse
also be the result of another mental illness. Types of depression include
situations:
major depression, bipolar affective disorder and dysthymic disorder.
Pro-social bonding
Clear and consistent boundaries
Symptoms of depression may include:
Life skills
Lethargic or lack energy
Poor concentration and memory
Caring and support
Changes in appetite—a considerable loss or gain in weight
High expectations
Disturbed sleep
Meaningful participation
Denial
Average or above intelligence.
Thoughts of suicide—thoughts of worthlessness or extreme guilt
Reduced level of interest or pleasure in most or all activities.
Major Depression
This is a major mental illness where the person experiences a drop in mood,
energy and initiative. They may become so depressed that they consider or
attempt suicide. The potential serious consequences of untreated
depression and the success of treatment make this an important mental
illness to identify.
Bipolar Affective Disorder
Bipolar which means Bi – two; and polar – directly opposite in tendency or
nature. The person’s mood can cause extremes from deep lows
(depression) to highs (mania).
Symptoms of bipolar disorder (mania) may include:
Increased physical activity
Becoming interfering or intrusive
Making elaborate and grand plans
Spending lavishly and foolishly
Writing endless letters of complaint
Reacting violently if beliefs are challenged
Page 19 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 16
Caring for Prisoners At Risk
Caring for Prisoners At Risk
Hallucinations
Symptoms of bipolar disorder (depressive) may include:
The person may hear, smell, taste or feel something that has no basis in
Lethargic – no energy
reality. This may include the following:
Feeling worthless and or helpless
Visual
Changes in appetite
seeing and talking to others.
Difficulty sleeping
Tactile
Poor memory
feeling insects under the skin.
Thoughts of suicide
Auditory
Anxious or irritable.
voices instructing the person to carry out certain actions.
Psychosis
Obsessive Compulsive Disorders
Psychosis describes a severe form of mental illness that disorganises and
Obsessive compulsive disorder or OCD is an anxiety disorder. Persistent
changes the whole personality. People begin to say and do things that other
thoughts, impulses and images that cause anxiety and stress.
people cannot accept as normal. Reality becomes distorted, judgement and
reasoning deteriorate, and mood becomes abnormal experiencing
Behaviours that act to reduce the stress include:
hallucinations.
Continual hand washing
Symptoms of psychosis may include:
Checking routines
Delusions
Repetitive praying
Hallucination
Repetitive counting.
Delusions
Three types of delusional behaviour are:
Grandeur
the person may believe that they are impossibly rich, talented,
powerful or titled.
Persecution, paranoid
the person may believe they are being spied on, poisoned,
sexually assaulted, talked about, or having thoughts inserted or
removed from their mind.
Hypochondriac
related to bodily functions, for example can’t swallow, have
cancer.
Page 17 © Department of Corrections
Version 2 August 2010
Version 2 August 2010
© Department of Corrections Page 18
Document Outline