MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 24 FEBRUARY 2016, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.02PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana
Peter Dunkerley
Andrew Blair
Diana Kirton (from 1.36pm)
Barbara Arnott
Jacoby Poulain
Heather Skipworth
Denise Eaglesome
Helen Francis
Dan Druzianic
Apologies
Nil
In Attendance:
Kevin Snee (Chief Executive Officer)
Members of the Executive Management Team
Dr Mark Peterson and Chris McKenna (as co-Chairs of HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council)
Members of the public
Minutes
Brenda Crene
KARAKIA
Ngahiwi Tomoana opened the meeting with a Karakia.
APOLOGIES
Diana Kirton apologised for lateness.
INTEREST REGISTER
There were no interests advised at the meeting.
Barbara Arnott asked to have an interest removed from the Register, relating to her daughter’s
employment with Health Benefits Limited.
Actioned
No board member had an interest in any of the items on the Agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 16 December 2015, were confirmed as a correct record
of the meeting.
Moved:
Barbara Arnott
Seconded:
Dan Druzianic
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Item 1:
The Quality Accounts had been finalised – and the action would be removed.
Item 2:
Travel Plan Business Case: The Board had requested progress updates with regular
reporting to include a focus on monitoring for “inequity”. Advised the ToR initiates the
Page 1 of 7
project’s start up with reports coming to the Board soon after. These have been
included on the detailed workplan. This action would be removed.
BOARD WORK PLAN
The Board Work Plan was noted.
CHAIR’S REPORT
• The Chair advised of the following retirements, with a letter being sent conveying the Board’s
best wishes and thanks for their extended years of devoted service.
Years of
Retired or
Name
Area
Service
Service
retires on
Sue Van Dam
Registered Nurse
Older Persons & Mental Health
10
24-Jan-16
Margaret Ansell
Clinical Coder
Facilities & Operational Support
22
5-Feb-16
• During December the Letter of Expectations for 2016/17 had been received outlining the
forthcoming year. An overview of funding expectations were shared.
• The Chair advised a Privacy Self-Assessment would need to be completed by the end of
March 2016.
• Health Target results had been released by the MoH and results were conveyed to members.
• Liz Stockley advised the last quarter’s results for smoking cessation advice had been poor and
the reasons which had attributed to the decline. She understands practices have been very
proactive in this area, with issues more attributed to the capture/recording of the required
detail. The key is whether patients are ready to give up smoking. There is an expectation this
quarters results would improve.
CHIEF EXECUTIVE OFFICER’S REPORT
The CEO’s report was taken as read, acknowledging:
• The new Mental Health facility was officially opened on 23rd February by the Minister of Health,
following which a number of initiatives were shared with Dr Coleman.
The Chair commended staff and management highly within the Mental Health service for the
seamless movement of patients from the old facility to the new. A wonderful job done. Allison
Stevenson was present at the meeting for this acknowledgement and was requested to pass
this on to all staff involved.
• ED was coping and in a better place than previously and we are hopeful to achieve target in
the near future.
• Orthopaedic patients now receiving better intervention, including alternative initiatives.
• The key problems in the month of January were patients waiting longer than four months for
First Specialist Appointments and elective surgery; together with patients receiving smoking
advice in primary care. Anticipate these will be on track for the targetted expectations.
• Regarding Faster Cancer Treatment – there is work to be done and if the problem(s) continue,
a report will be provided to the Board.
• Immunisation of children: It was the first time HB had not met the target, with 35 infants not
fully up to date with their immunisations between Sept-Dec 2015 (ie, Q2).
The pattern was reviewed and tended to indicate a blip, for no specific reason. An overview of
the system(s) in place was relayed to the Board. Some parents choose to decline vaccinations
but do change their minds. It was important to ensure conversations around immunisations
were continued with families. The results within HB were similar to the rise seen nationally.
Page 2 of 7
• A dip in the financial result for December had corrected itself in January with a favourable
outcome at the end of January 2016 (refer to the finance section).
• Health and Social Care networks outlines a strategy on how we can bring organisations
together to respond to the needs of the community. Effort will be required to take this forward.
Need to ensure consumers are fully involved from the outset.
FINANCIAL PERFORMANCE REPORT(S)
The Financial reports for December 2015 and January 2016 were reviewed with matters
highlighted in the respective reports.
• As mentioned. a dip in the financial result for December corrected itself in January with an
overall favourable variance of $128 thousand.
• The Financial Performance Summary provided an analysis of factors driving the favourable
variance to date.
• Overall we were very close to budget, however it will be testing to achieve the budgeted
surplus for this financial year (ending 30 June 2016).
The message conveyed by the CFO was not to take anything on that is too challenging for the
remainder of this financial year.
It was noted a number of the Central Region DHBs were tracking significantly below their
respective plans. It was a tribute to a lot of good work being done within the HBDHB to find
ourselves in a positive position.
CONSUMER STORY
No specific Consumer Story was conveyed, however feedback from customers who had
experiences with booking staff and receptionists within DHB services, were shared with Board
members.
Ensuring positive customer service interactions was recognised as crucial to an efficient and
pleasurable customer journey. Advised that customer training is planned for staff with feedback
that staff are delighted.
Consumer Council prefer to no longer receive consumer stories as part of their monthly agendas.
They felt, as initiators of these stories, they could best support consumer outcomes in other ways.
REPORT FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
The report advised commentary on the Health literacy strategic review which mentioned that,
across the sector we needed to focus on eliminating technical/medical jargon for consumers and to
focus more on ensuring consumers truly understood. Consistency in this area needs to be applied
across the whole health sector.
Other areas overviewed included Clinical Governance Structures (consultation); Council member
portfolios of interest; the successful Respiratory Pilot; and the Health and Social Care Networks
strategic direction which would ultimately improve the health outcomes for our community, and was
supported by Council.
Hawke’s Bay Consumer Council
The Health Literacy Review saw some rigorous discussion by consumer members who had been
constantly told they needed to get more literate!. The question is how literate is the health sector!
The health literacy strategic review and the development of the framework for health literacy within
HB health sector will address this.
Page 3 of 7
Health and Social Care Networks passed through the Consumer Meeting quickly with the direction
of travel supported. In week following the Consumer Meeting however, some members felt the
paper had been produced without consumer input and they advised they were prepared to roll their
sleeves up and make a strong contribution going forward. This was noted by the report writer(s)
The Consumer Council structure in HB: Word has spread with most of the Central Region DHBs
looking to implement something similar. The resulting structures may not be the same but
Consumer Council members were looking forward to supporting and feeding into joint work for the
region.
Māori Relationship Board (MRB)
The report provided included: Whanau Ora, Living Wage in HB; the MRB workplan; Maori Bachelor
of Nursing Students; MRB representation on Clinical Council; Health Literacy Review; as well as
Health and Social Care Networks. The content of the report was conveyed by MRB’s Chair and
suggestions made were acknowledged and noted by the HBDHB Board.
• Living Wage in HB: MRB challenged the DHB to implement the living wage within HBDHB, as
they felt a large number of Maori were affected. In response the CFO advised there were a
range of possibilities to be considered, one option may be to lift the skills, leading to improved
service delivery. He noted any change would also affect a wider group of staff in care facilities.
He was not saying let’s do it … but there were far wider implications to be considered first.
• Meetings and Workplan: MRB sought 10 meetings per year (outside Leadership Forum
attendance) and members were keen to prioritise their own workplan – reducing to no more
than six items. MRB’s priorities in 2016-17 were Smoking, Obesity, Alcohol and other drugs
and young mothers and Children.
• MRB sought representation on Clinical Council. It was noted MRB was a governance body
whereas Clinical Council were a management body reporting to the CEO. A discussion would
be held to consider.
• Health and Social Care Networks
: MRB endorsed the content of this Programme Brief pending
consideration for MRBs feedback and input the strategic direction.
Denise Eaglesome advised that Wairoa had discussed HSCN. In this regard there needs to be
pre Intersectoral workshops with Wairoa needs to be Wairoa led and DHB enabled.
Suggested that Wairoa be the first to hold an Intersectoral Wairoa Workshop with wider
community DHB and MSD to promote leadership. It was noted there was also a HB Health
Consumer Council member based in Wairoa.
FOR DISCUSSION AND INFORMATION
Health and Social Care Networks
Liz Stockley (leading this work) was supported by Kevin Snee and outlined the detail and intent of
Health and Social Care Networks, advising keenness to discuss in more detail at the forthcoming
Health Sector Leadership Forum.
The introduction of the programme was seen as a key initiative focused on improving the health
and wellness of our population. It will be a significant programme of activity and of associated
change management, requiring support at all organisational levels. We are, therefore, seeking
support from the DHB Board to begin this journey.
As noted above Wairoa would be a great starting point and the community already have
considerable leadership.
Page 4 of 7
Action:
RECOMMENDATION
It was noted the Council’s and MRB had supported the direction of travel for Health and
Social care networks, therefore the Board were happy that management proceed with
this concept (taking on board all comments raised/made) and were asked to keep the
Board updated with progress periodically with timeline(s) advised for workplan(s).
Adopted
MONITORING REPORTS
Human Resource (HR) KPIs Q2 Oct-Dec 2015
Innovation in on-line leave management systems is being looked at with a view to move towards a
closed loop system, with no gaps in leave captured and leave approved.
Accidents were higher than target at 119 vs 90 for the quarter. This was being focused on to raise
awareness.
Action: Māori staff representation in the workforce:
This has moved little in the last quarter, an action plan needs to be produced.
Suggested actions for consideration and noting by HR:
•
Suggest including a Maori representative on specific interview panel panels.
•
Escalate queries relating to appointments by hiring managers to have them explain
their actions to either their Executive Manager or to the CEO.
•
Include competencies /targets in all position profiles.
Te Ara Whakawaiora / Access (ASH Rates 0-4 & 45-64 years)
Te Ara Whakawaiora Ambulatory Sensitive Hospitalisation rate targets have shown some
improvements, both in terms of Māori admission rates and also in terms of the comparative rates
between Māori and the total population.
This is particularly the case for the 0-4 age group. Rates for the 45-65 age group continue to show
significant disparity, though rates have improved.
• Asthma a concern in Maori children vs non-Maori yet there are more levers now to reduce
asthma incidence (through appropriate long term prevention/treatment). Noted some may be
viral.
• Dental: Robin Whyman will be presenting to the board in the near future.
• Jacoby Poulain asked how were
“key messages delivered to families” when most were at
home?
Action: Mark Peterson to arrange for an update to be provided.
• Improved diagnosis of heart attacks shows with good management you can either prevent or
reduce severity in primary care.
• Since Wairoa is an isolated area, what would health inequities there look like? Inequities’
would be narrower but it would be a useful exercise to do.
Page 5 of 7
HBDHB Non-Financial Exceptions Report for Q2 Oct-Dec 2015
Our overall performance on Elective Surgery is running just above 100%. Heart and diabetes
checks are at 90.3%, which is above target for the fourth successive quarter. We are making
progress on Faster Cancer Treatment (continuing upward trend towards achieving this target).
Shorter stays in ED shows improvement. The result for Acute Coronary Syndrome Services (high
risk patients receiving an angiogram within three days) was 68.7%, which is an 18% improvement
on the previous quarter.
There were significant changes made in the run up to Christmas and working with cardiology to
change their rosters. Working with Capital and Coast regarding patient transfers. Regional
Cardiology group networking progressing. Regional review of cardiac services would be
beneficial.
Monitoring Dashboard Quarter 1 2015/16 (provided by Ministry of Health)
The report received related to Q1 (July-Sept 2015), a significant time lag!
It was understood that patient portals were being progressed. A process was in place and 50% of
patients now have access to the portal. However, the number enrolled and using the portal was
quite low.
HBDHB Transform & Sustain Strategic Dashboard Q2 Oct-Dec 2015
This new report to the Board aims to deal with the impact rather than the process of our Transform
& Sustain strategy. Three ‘vital sign’ indicators for: service quality (what our consumers say about
us); population health (the gap between Māori and Non Māori death rates under 50 years old),
and; use of resources (PHO break even, DHB make target surplus) are each supported by seven
representative indicators.
Comments during discussions included:
• Probably need to do more analysis as to what this means in future.
• Not a comprehensive list of everything being measured.
• Delivers the triple aim and should be measuring quality of care, efficiencies and around
population health. Patient experience survey.
This is work in progress which will lead to healthier lives.
Page 6 of 7
RESOLUTION TO EXCLUDE THE PUBLIC
RESOLUTION
20.
Confirmation of Minutes of Board Meeting
- Public Excluded
21.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
22.
Board Approval of Actions exceeding limits delegated by CEO
23.
Chair’s Report
24.
Allied Laundry Services Ltd Report to Shareholding DHBs
25.
Preliminary Budget - Presentation
Reports and Recommendations from Committee Chairs
26.
HB Clinical Council
27.
Finance Risk and Audit Committee
Moved:
Peter Dunkerley
Seconded:
Dan Druzianic
Carried
The public section of the Board Meeting closed 3.35pm
Signed:
Chair
Date:
Page 7 of 7
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 30 MARCH 2016, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.00PM
Present:
Kevin Atkinson (Chair)
Peter Dunkerley
Diana Kirton
Barbara Arnott
Jacoby Poulain
Denise Eaglesome
Dan Druzianic
Apologies
Ngahiwi Tomoana, Andrew Blair, Heather Skipworth and Helen Francis
In Attendance:
Kevin Snee (Chief Executive Officer)
Members of the Executive Management Team
Dr Mark Peterson (Co-Chair, HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council)
Members of the public and media
Minutes
Brenda Crene
KARAKIA
Denise Eaglesome opened the meeting with a Karakia.
APOLOGIES
Apologies were noted from Ngahiwi Tomoana, Heather Skipworth, Andrew Blair and Helen
Francis
INTEREST REGISTER
Action
Diana Kirton asked that Eve be removed as an Interest on the Register as her
placement had been brief.
No board member advised of any interest in the items on the Agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 24 February 2016, were confirmed as a correct record of
the meeting.
Moved:
Peter Dunkerley
Seconded:
Barbara Arnott
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Item 1:
Health & Social Care Networks: Timelines had been included on the workplan.
Remove action.
Item 2:
Human Resources – Maori Staff representation in the workforce: the points noted in the
action status had been provided by HR Manager. Remove action.
Item 3:
Te Ara Whakawaiora / Access: In considering aspects of the report provided, Jacoby
Poulain received a response to her query regarding information to those in the home,
which was mainly through public health nurses. Remove action
Page 1 of 7
BOARD WORK PLAN
The Board Work Plan was noted.
The Surgical Wait List Flow noted on the workplan was to be moved out one month as data was
being sought.
Action
A Refresh of Transform and Sustain had been drafted and would receive wide consultation. This will
be a topic for discussion at the HB Health Sector Leadership Forum on 17 May. It was noted that
Clinical and Consumer Council as well as MRB were to consider the draft in April.
CHAIR’S REPORT
• The Chair advised the following retirements, with a letter being sent conveying the Board’s best
wishes and thanks for their extended years of devoted service.
Years of
Name
Role
Service
Service
Retires
Tony McKee
Facilities Manager
Facilities & Operational Support
14
31-Mar-16
Jenny O'Sullivan
Midwife
Women Children & Youth
21
31-Mar-16
Dr Rob Armstrong Respiratory Physician
Acute & Medical
26
1-Apr-16
Noeline Paenga
Medical Secretary
Facilities & Operational Support
21
1-Apr-16
• Kate Coley (Director QIPS) had been instrumental in preparing a response to the “privacy
assessment” ie, a maturity assessment based on criteria and expectations established and rated
across nine key principles. The Board were advised HBDHB generally sat in the middle of the
defined area. An action plan will be developed from this assessment.
The Board Chair and CEO signed off the assessment document during the meeting which was
provided to Kate.
The privacy assessment and audit process take place again in early 2017.
• The Chair referred to a Health Quality and Safety Commission (HQSC) book entitled “Governing
for Quality” which focused on governance, quality and safety and included a section on how
board members should go about assessing quality and safety.
Kate Coley and Ken Foote advised of their intention to bring a report to the Board in July 2016
entitled “Governing for Quality”.
The Board indicated their interest to have a two hour Quality Workshop also. This would be
investigated and timeline(s) advised as part of the Governing for Quality piece of work.
• MoH funding for the DHB in the 2016/17 year had increased 3.96% (based on the population).
The largest increase in funding went to Northland.
• A health workforce review was referred to by the Chair. A key point noted by the Board was the
aging workforce (with 45.4% of nurses being over 50 years of age).
• Board members were pleased to see there had been an increase in the number of qualified
support workers.
CHIEF EXECUTIVE OFFICER’S REPORT
The CEO’s report was taken as read and is summarised as follows:
• An overview of the performance targets was provided.
• Improvements in ED should enable HBDHB to be better placed heading into winter. From June
onwards, initiatives will be in place which will result in further improvements.
Page 2 of 7
• Smoking cessation in primary care had seen a small improvement and will likely to be close to
target by the end of the next quarter. Liz Stockley provided some detail around the work
occurring.
• The MoH Q2 results were appended to the CEO’s report which showed problems in ED and the
smoking target.
• The financial result for February was positive.
Following the CEO’s report a new 8 minute Induction and Recruitment video was played to board
members. The two minute version will be included on the website.
FINANCIAL PERFORMANCE REPORT
The Financial report for February 2016, was reviewed with the month yielding a favourable variance
of $55 thousand, with the year-to-date result at $136 thousand favourable (for month nine).
The forecast for the 30 June 2016 year remains at the $3.990 million budgeted surplus. It was noted
that 0.99m was MoH funding provided but not to be spent.
• Only the year to date part of the $1.0 million transferred to Surgical Services and the $90
thousand contributed to the corporate 3% savings plan, had been released from contingency.
• Elective surgery was 5.5% above plan after adjusting for prior period entries, and 1.5% ahead of
the health target year to date, with 81% provided in-house in comparison to the planned 75%.
• Capital spend was close to the budget with employee numbers lower than planned.
• Case weighted discharges were well placed and were a good indicator.
• There is room for error with the need to continue to work hard to achieve the anticipated budget.
• The CFO advised a Budget update around the effect of spends by category would follow the
prioritisation process, with Clinical Council in May.
Action: Ensure this is included on the board agenda for May.
CONSUMER STORY
Difficulties experienced by a well-known leader in the community (as he prepared for surgery)
highlighted challenges which will hopefully be alleviated as a new orthopaedic pathway is developed.
HBDHB Customer Service Manager, Jeanette Rendle sought out and was put in touch with Henare
O’Keefe. She was wanting to know how consumers felt about orthopaedic services. Henare has
since volunteered to become involved (with system changes) from a consumer perspective because
of his experiences.
The co-design of service(s) will focus on consumer outcomes. These outcomes may not be exactly
what consumers want (due to financial constraints) but outcomes must be communicated in a way
that shows respect and ensures everyone is valued.
REPORT FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
Dr Mark Peterson spoke to the Council report to the Board which included the Davanti IS review.
He noted clinicians were impatient in this area and have been for some time. Council were generally
supportive but had an element of scepticism as IS were not proactive and existing systems were
seen as barriers not enablers.
The mobility action plan had been reviewed with the aim to support people with musculoskeletal
conditions to fulfil their health potential and increase independence, through improved access to
Page 3 of 7
high quality advice, assessment, diagnosis and treatment. Ministry funding was available and would
be applied for to assist with costs in this area.
Urgent Care Alliance – expressions of interest had closed and there was now enough interest to be
able to put together a request for proposal. The goal being to establish a model in primary care that
would reduce pressure within the hospital (specifically ED). A behavioural/culture change in this
area would not happen quickly.
Action:
Clinical Council were asked how far advanced was the Hepatitis C Clinical
Pathway as this would likely be a priority for the Ministry? This should be kept
on the radar and an update provided to the board.
Hawke’s Bay Health Consumer Council
Graeme Norton reiterated the wishes of Council to focus on where they can make a difference with
their goal to see the consumer voice included in every aspect of the health system.
• Obesity and Youth received focus during their meeting earlier in the month.
• Council were now working with the population health team and strengthening confidence that
what was being done would work.
• The Chair emphasised how the Consumer Relationship Manager’s role was now starting to link
through and supporting consumer focus in a more managed way.
Māori Relationship Board (MRB)
Denise Eaglesome spoke to the report in the absence of Ngahiwi Tomoana and Heather Skipworth.
She advised some MRB members appeared to be frustrated with progress and the lack of focus on
equity. There was mention MRB were adamant that if staff wanted to report or present to MRB they
must first use the HEAT tool to identify how their work was going to reduce inequity. MRB highlighted
the important of DHB needing a formal process for this to occur across all governance groups as it
is one of the overall priorities.
Board members felt this was more about communications coming through in the reporting provided.
Was there a need to review the MRB structure?
It appears MRB want to know how they can deliver their role more effectively, with some confusion
surrounding their role within the DHB. The DHB (in 2013) removed DSAC, CPHAC and HAC from
their meeting structure but MRB remained.
Since the restructure it was noted:
• MRB now has five HBDHB board members, previously two.
• MRB have always had strong advocacy at the HBDHB Board table.
• MRB members may not realise it but there is a lot of Maori input elsewhere in the health system
(across the sector). This may not always be visible in the reporting they receive.
It appears MRB may be advocating for what is not visible. They may feel a lack of response to
comments raised.
The CEO advised from where he was sitting HBDHB were doing better than anywhere else in NZ
for Maori health. The Trendly data is what is generating other DHBs to look at what we are doing
here in HB. The CEO stated that he has asked the GM Maori Health to provide a report to MRB on
where DHB is doing well in Maori Health. This will be provided to the April meeting.
It must be remembered that most of the levers for improvement(s), sit outside the health system,
hence there is such a high focus on multiagency (Intersectoral) work which will ultimately make the
biggest impact.
The author of the HB Health Equity report advised this was presently being reviewed as part of its
yearly cycle.
Page 4 of 7
Action:
Kevin Snee will meet with MRB members in April to discuss issues.
Whanau Ora was raised as something the DHB needed to better define. P LeGeyt is developing
this further following the workshop in March.
Pasifika Health Leadership Group (PHLG)
As an introduction, Barbara Arnott advised this followed on from discussions in December 2015.
PHLG feel the need to have more navigators within the health system, to help the growing population
of Pasifika in HB. These people come from many different islands, speak various languages, and
have different cultures and values.
Collectively the six members of Pasifika Health Leadership Group believe the navigators are the
best option to reduce inequity and enhance communication.
Barbara introduced
Tim Hutchins of Pasifika Navigation Service who provided a snapshot of
consumer stories relating to his work with Pacific families.
• A variety of situations have occurred which have needed to be dealt with in very different ways
because of the wide ranging cultures and languages of the Pasifika people. Their needs have
often been overwhelming.
• The Navigator role has also been utilised in the ED setting also, focusing on reducing ED visits
by pasifika people who have used it as a GP service. The main issues have been communication
(language barriers) and the fact that health services mostly run during normal working hours
making it difficult for those working to attend.
• Tim advised he has had a heavy workload and had worked with 950 families. His original contract
was for Rheumatic Fever.
Another navigator has since been employed at Totara Health.
It was suggested a more holistic approach is required with a review of navigators (for Maori and
Pasifika people). Look at what exists now and include nurses/district nurses into the equation as
they are, in a sense, navigators also. Services need to be utilised in a more coordinated and cost
effective manner.
A funding bid had been prepared for consideration.
The Board thanked those in attendance and wished them luck with their bid.
FOR DECISION
NZ Health Partnerships Ltd
NZ Health Partnerships Ltd was incorporated in 2015 to take over many of the functions and
activities previously undertaken by Health Benefits Ltd. NZ Health Partnerships is a multi-parent
Crown subsidiary that is led, supported and owned by New Zealand’s 20 DHBs and has been
established to enable DHBs to collectively maximise shared service opportunities for the national
good. On consideration the Board approved the following Resolution.
RESOLUTION
That as a shareholder of NZ Health Partnerships Ltd, the Hawke’s Bay District Health Board
approved the Company’s:
• Statement of Intent – 1 July 2015 to 30 June 2019
• Statement of Performance Expectations – 1 July 2015 to 30 June 2016; and
• Annual Plan 2015/16
Moved
Dan Druzianic
Seconded
Peter Dunkerley
Carried
Action:
Ken Foote to provide the response to NZ Health Partnerships.
Page 5 of 7
FOR INFORMATION
Draft HBDHB Annual Plan and SOI 2016/17 - Draft v1.1
Changes to the Annual Plan since 2015/16 were outlined noting the Minister was seeking a refreshed
Statement of Intent (SOI) in this year’s Annual Plan. The refresh is focused on incorporating the NZ
Health Strategy themes and how we measure the implementation and impact of Transform and
Sustain.
The areas of increased Focus; less Focus and local Maori Priorities were relayed to members.
Any feedback on the plan would be provided directly t
o [email address] • The draft has been through the various Committees and through various other stakeholder
groups
• It was noted the final draft was due in May 2016
• A query from the Chair related to page 59 of the plan. It was felt that HBDHBs position on food
services and laundry services should be better defined. Carina noted this point at the meeting.
• Advanced Care planning was now included in the Plan (although not in the version provided)
Thanks were conveyed to Carina for a job well done.
Draft Central Region Regional Service Plan
The draft document provided outlined the Central Region’s Plan developed collaboratively by the six
DHBs in the Central Region reflecting strong focus on co-design principles across regional work. In
2016/17 the focus across the region would be on improving health outcomes and reducing disparities
for Maori as well as working on the implementation of the five themes within the NZ health strategy
through integration, regional collaboration and reducing silos.
MONITORING REPORTS
Te Ara Whakawaiora / Breastfeeding
Caroline McElnay introduced Nicky Skerman and Katie Kennedy (as Authors of the report).
It was acknowledged that Hawke’s Bay had yet to meet the Ministry’s target for breastfeeding across
age bands and ethnicities, with breastfeeding rates for Māori being consistently lower than other
ethnicities. A review of how best to improve breastfeeding rates by supporting mothers/whānau
more intensively, starting specifically in the first at six weeks of a child’s life, is underway.
An active discussion followed, resulting in the following action.
Action:
The Board wish to understand what other DHBs are doing and also to see
where HB is benchmarked (including reasons and relative demographics).
This will be included in the CEO’s report when the information is available.
Annual Maori Plan Dashboard for Q2 (October to December 2015)
The Trendly tool has enabled better management ie., best practice where HB can learn from.
It was heartening to see the achievements made and the board were advised where results were
not as good (ie., the challenging areas) had been incorporated into the Annual plan.
Areas of progress noted were more heart and diabetes checks and breast screening.
The challenging areas were Breastfeeding rates; Post natal Maori women smoke free; Immunisation
rates; Maori under the Mental Health Act; and the Maori Workforce (with 2% below target of the
14.3% target).
Not yielding results as fast as would like in some areas but the focus is working with the person, not
the disease, and see how we can reach the whole family at one time in a more co-ordinated way.
Page 6 of 7
There being no general business the Board moved to the public excluded section of the meeting.
RESOLUTION TO EXCLUDE THE PUBLIC
RESOLUTION
22.
Confirmation of Minutes of Board Meeting
- Public Excluded
22.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
23.
Board Approval of Actions exceeding limits delegated by CEO
24.
Chair’s Report
25.
Information Services Function Review
Reports and Recommendations from Committee Chairs
26.
Finance Risk and Audit Committee
27.
HB Clinical Council
Moved:
Dan Druzianic
Seconded:
Diana Arnott
Carried
The public section of the Board Meeting closed 3.25pm
Signed:
Chair
Date:
Page 7 of 7
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 27 APRIL 2016, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.05PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana
Andrew Blair
Peter Dunkerley
Diana Kirton
Barbara Arnott
Helen Francis
Heather Skipworth
Jacoby Poulain
Denise Eaglesome
Apologies
Dan Druzianic
In Attendance:
Kevin Snee (Chief Executive Officer)
Members of the Executive Management Team
Chris McKenna and Mark Peterson (Co-Chair, HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council)
Members of the public and media
Minutes
Brenda Crene
KARAKIA
Heather Skipworth opened the meeting with a Karakia.
APOLOGIES
Nil
INTEREST REGISTER
No changes to the interests register were advised
No board member advised of any interest in the items on the Agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 30 March 2016, were confirmed as a correct record of
the meeting.
Moved:
Barbara Arnott
Seconded:
Peter Dunkerley
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Item 1:
Budget Update following the Prioritisation Process – Verbal update to the Board in May
Item 2:
Hepatitis C Clinical Pathway timing: Ongoing update in May
Item 3:
Meeting with MRB Members: The CEO attended MRB’s workshop and discussions
were captured in the report from MRB for April.
Item 4:
NZ Health Partnerships recommendations were conveyed accordingly: remove action
Page 1 of 9
Item 5
TAW / Breastfeeding demographics information in CEOs report: Ongoing - with update
expected in September 2016
BOARD WORK PLAN
The Board Work Plan was noted and would be updated at least to calendar year end.
The Board Chair noted the large number of agenda items listed for the May Board meeting.
Action:
EMT will review the workplan.
CHAIR’S REPORT
• The Chair advised the following retirements, with a letter being sent conveying the Board’s best
wishes and thanks for their extended years of devoted service.
Years of
Name
Role
Service
Service
Retires
Jennie Butler
Dental Therapist
Oral Rural & Community
47
14-Apr-16
Jane Harding
Registered Nurse
Surgical
19
29-Apr-16
• The NZ Health Strategy was launched (over 2 days) in mid April. Attendees found it interesting
from an innovation point of view. Advised there were adverse childhood experiences and
childhood development ideas to follow up on.
There appeared to be a very close similarlarity to the HBDHB’s Transform and Sustain. It
would appear that HBDHB’s strategy is three years ahead of the Ministry.
CHIEF EXECUTIVE OFFICER’S REPORT
The CEO’s had recently received news that HBDHB were top nationally for ‘hand hygiene’. The
target was now 80% with Hawke’s Bay achieving 89%. Well done to all those who have supported
in achieving this milestone.
Regional Health Information Programme (RHIP)
The CEO’s report contained a recommendation for the Board’s consideration. Detail around the
topic had been discussed extensively at the Regional Governance Group Meeting and it was time
to move forward with certainty and implement the programme.
While financial detail is still being refined the population based funding formula share of an
additional spend of $8.3m for the region to complete the programme, would mean $1.7m over
three years programme for Hawke’s Bay (which can be funded).
Barbara Arnott requested that HBDHB’s contribution of $1.7m (as was included in the report) be
noted in the resolution. This was agreed.
RESOLUTION
That the Board
1) Note the contents of this report.
In relation to Regional Health Information Programme (RHIP):
2)
That the Chairs and CEs reconfirm the commitment of the RHIP Programme vision as per their
commitment on 15 October 2015.
3)
Agree to Deploy (build, implement and operate), the RIS, Clinical Portal (Core and Enhanced),
Healthcare Practitioner Index, Regional WAN and Infrastructure to all 6 DHBs.
4)
Agree that the Programme of deployment to other DHBs, following Whanganui's deployment,
Page 2 of 9
will be subject to:
a) The successful implementation and go live of the current planned phase of the Programme
(recommendation 2 above) within the current allocated Programme budget.
b) That there is a Post Implementation review of the Clinical Portal Implementation to ensure it
is a sound base upon which to build the Enhanced Portal
c) That there is a review of the proposed Enhanced Portal design and functionality against the
existing Portal functionality as a reference to ensure it will provide additional value
d) That there is continued independent review of the Programme.
5)
Agree to deploy the Interim Regional Operating Model as agreed to support the Whanganui
deployment as above.
6)
Note that the Interim Service Model will need to be developed to meet the regional needs as
other DHBs come onto the regional solution.
7)
Agree to have WebPAS build and available for local implementation / uptake, initially by first
Whanganui in 2016, followed by MidCentral / Wairarapa and then the remaining DHBs (timing
and sequence to be advised).
8)
Agree to the commitment of funding of up to $8.3M (in addition to the $56.2M already
committed) to support the above recommendations, noting that any additional funds to be
invested will be accompanied by a revised cash flow, accommodating where possible each
DHB’s funding availability and constraint
9)
Note that some Chairs and CEs will need to seek Board approval for this additional funding and
will do so before 30 April 2016.
10)
Note that HBDHB’s contribution would be $1.7 (as noted in the report).
Moved
Peter Dunkerley
Seconded
Heather Skipworth
Carried
Action Admin:
Ensure the Resolution is provided to CTAS.
Flouridation
The governments intention for DHBs to now make decisions around fluoridation was agreed a
sensible move, as DHBs are far better placed than council’s to make decisions on oral health.
Indications are that since Central Hawke’s Bay had removed fluoride from their water supply, their
dental statistics have detrioriated.
The balance of the CEO’s report was taken as read, noting the positive financial result.
FINANCIAL PERFORMANCE REPORT
The Financial report for March 2016, was reviewed showing a favourable variance of $52 thousand
with a year to date result of $187 thousand favourable. Only the year to date part of the $1.0
million was transferred to Surgical Services and the $90 thousand contributed to the corporate 3%
savings plan, have been released from contingency. Members were advised the $2m contingency
was still available.
For clarification the $3.990million budgeted surplus includes $.99m funding provided to HBDHB by
the MoH.
Clarification around Pharmac may see a claw back by Ministry of our savings.
Other areas of the report were summarised as follows:
• Good and bad offsetting each other does show a certain amount of volatility. Need to get
budget work finished to enable spending in targeted areas to commence/continue.
• IDFs remain uncertain at this time.
Page 3 of 9
• Strategic resource redeployment. We are now investing more resource into population health
and community care and not as much into the hospital. With quarter 3 of the financial year
behind us, it shows there has been a signficiant shift equating to nearly $1m.
• The quality and financial improvement plan is sitting 13% below target. Movement in budgets
is taking effect in this area.
• No HR issues.
Overall we are close enough to the end of the financial year to feel confident of reaching the
financial target at year end.
CONSUMER STORY
Kate Coley provided feedback on changes made in-house to date and an update on stories
shared:
Services out of villa 6: A small project has been looking at accommodation pressures (ie, variety of
services run out of the villa). Separation of “oncology” cancer patients in particular, due to their
immunity issues has always been supported by the board.
ED front of house structural changes had been delayed, with work commencing at the end April
2016. Already, processes around triage have been changed/adapted. The EngAGEe Orbit team
has been in place since February with a huge impact on reducing the number of frail elderly that
would normally have been admitted through ED. Support in ED with wrap around services being
provided to get them back home as soon as practical, has seen a 50% reduction in admissions.
Complaints in ED had dropped by 50%, with several complimentary stories shared at the meeting.
Customer service training has been provided to an array of staff, with complaints around the first
interaction dropping considerably. This is being rolled out to Primary Care as well.
REPORT FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
Dr Mark Peterson spoke to the report to the Board from Council’s meeting held on 13 April 2016:
• Clinical Council considered Business Cases for Investment in 2015/16. All three were
endorsed. These proposals had been previously approved pending the provision of the
business cases.
• Best Start Healthy Eating (Draft): Council endorsed and were very supportive of the direction of
travel and looked forward to reviewing the final document.
A discussion around changing the paper to Healthy Lifestyles as opposed to Healthy Eating
was raised. However it was noted the focus was healthy eating and more benefits come from
this as opposed to exercise.
• The “Prioritisation Process” was underway with individual Council members already reviewing
the detail (of the cases put forward). The extended Council meeting on 11 May will incorporate
the prioritisation process and the Board will be updated accordingly (at their 25 May meeting).
MRB will have the opportunity to review the prioritisation detail at their meeting on 12 May, and
provide their comments to the Board.
• There will be an MRB representative attending Clinical Council meetings in the same capacity
as the Chair of Consumer Council. No name had been put forward as yet.
• Asked whether Clinical Council had considered or discussed Faster Cancer Treatment, the
response was they had not. It was advised this was being monitored closely and there will be
action.
Page 4 of 9
Hawke’s Bay Health Consumer Council
Graeme Norton advised the outcomes of their meeting held on 14 April 2016.
•
Older Persons Panel – a self-elected sub group of six (of Consumer Council) was now working
with Mental Health, Older Persons and Options to establish a working panel to provide
consumer engagement on various aspects of service development and delivery.
•
Health and Social Care Networks – a sub group will work with GM Primary Care to ensure
robust engagement of consumers in network development.
Following on from presentation in February – had a meeting and a subgroup was put in place.
•
Draft Best Start Healthy Eating (Obesity Strategy) was reviewed and felt the strategy had
received good community engagement – essential as the community need to own this. The
final is scheduled to come to the Board in May. This has been a very healthy process with
valuable in depth contribution by consumer members.
•
Consumer Engagement Principles and Framework: the work done to date can now be used as
the basis for a discussion with Clinical Council.
Māori Relationship Board (MRB)
Ngahiwi Tomoana (Chair) provided an overview of the Workshop held on 13 April 2016:
The content included in the MRB report to the Board was noted.
MRB had reflected on their performance and were delighted with the results shared at the
workshop, noting teen pregnancies were down, and there was in increase in systemic heart
disease and smoking checks. MRB discussed how they could make further improvements
resulting in even more success.
Members examined the Maori Health Service Review. Want to take a leadership role and
determine if the whanau health service was to the whole whanau, rather than individuals.
• The Obesity strategy was an example of how this can be modelled. Pilot testing a whanau
based model of service delivery.
• Now seeing behavioural changes in dealing with Maori, starting to show results.
• Asked whether MRB was fit for purpose? Was MRB the best model? Some felt they should be
more analytical.
Kevin Atkinson advised there was a good relationship between MRB, HBDHB and Iwi. The
number of HBDHB board members on MRB had increased over recent years. Did MRB think it
should be just a Māori advisory board?
Ngahiwi advised he was unsure but felt that what was likely required, was a change in “focus”.
HBDHB Board members on MRB relayed the following comments:
-
Certainly have a better understanding of the issues and feel enlightened to a different
perspective.
-
Felt some areas get to the board a little late. Māori like to discuss things in more depth so
timing is an issue.
-
Relayed that MRB members feel advice in some cases was not implemented.
Questioning a group effectiveness? MRB are not alone in this review, as PHLG and the
HBDHB Board look inwardly and wonder if they make a difference also. MRB are going
through a questioning period at present.
From Barbara Arnott’s experience this is all to do with “focus”.
Maybe Tracee TeHuia and Adele White (CEO NKII) could have a discussion.
Page 5 of 9
Action: Kevin Atkinson asked that he and Ngahiwi Tomoana be included in the
discussion with Tracee and Adele.
• Everyone is trying hard to work together. The CEO felt the discussion at MRB was a really
constructive and very worthwhile. We have come a long way and there is a lot of good
information available and we can now benchmark ourselves against other DHBs. We have the
best relationship throughout the 20 DHBs nationally, and this was acknowledged at the
Workshop.
• Consumer Council had consciously shifted how it worked as they felt constantly burdened.
They now focus intently on their pre-meeting agendas and only discuss where they can make
the biggest impact. Need to get a good quality of depth to be able to give good advice.
• Talk about things - then get the discussion into a form that will ensure there are workable
actions helps!
• It was suggested the HEAT tool be applied to all papers, not just for MRB. Otherwise we will
not know whether the recommendaitons are worthwhile. This would help improve efficiencies
around meetings and would put the committees in a better position to review the strategy.
FOR INFORMATION AND DISCUSSION
Transform and Sustain Refresh Draft
Tim Evans took the Board through the paper provided.
• As we have moved through the Transform and Sustain process over the past three years or so,
it has progressed and we are now seeing a reduction in projects. Therefore priorities have
been worked through the executive team (in line with the triple aim) to bring forward project
work that will ensure further required change continues to occur
• Following are the topics of focus agreed to by the Executive team:
⇒ Person and Whānau Centred Care (people as partners in their healthcare)
⇒ Health and Social Care Networks (creating strong primary and community care clusters)
⇒ Whole of Public Sector delivery (delivering effectively with public sector partners)
⇒ Information System connectivity (and improved outpatient process)
⇒ Financial Flows and models (incentivising and funding the right behaviours)
⇒ Organisational Development Investing in Staff and changing culture (equipping our staff
for a changing world)
Now is the time for consultation and discussion with wider stakeholders and this was presently
planned to occur in fairly tight timelines.
• Those attending the HB Health Sector Leadership Forum Workshop will be exposed to this
detail to enable discussion/feedback on 17 May 2016. The draft paper had already been
through Consumer, MRB and Clinical Council.
• The Board noted the reasoning and process thus far and again, the Chair noted the HBDHB
Transform and Sustain detail to date, contained a lot of similarities with the National Plan ie,
the NZ Health Strategy.
It was noted that work had already commenced in some of these ‘new’ priority areas, particularly
Person & Whanau Centred Care and Heatlh and Social Care Networks.
Barbara Arnott advised that the Pasifika Health Leadership Team were meeting on 9 May, and
were grappling as to where they could make a significant difference. Barbara provide detail to
PHLG and expect PHLG them to feed questions into the process.
Timelines: The Leadership Forum Workshop detail will feed into the final Transform and Sustain
document which will come through the advisory committees through to the Board for their 29 June
Meeting Note: this was already included on the respective work plans.
Page 6 of 9
From the timeline provided in the report, it appears the projects were to be co-design documented
and agreed by 30 June 2016.
DHB Elections 2016
Pre-election resolutions required with detail provided in the report prepared by Ken Foote. The only
change to the resolution below as approved in 2013, is the change in Electoral Officer
RESOLUTION
That the Board
• Appoints Warwick Lampp from Electionz.com as the HBDHB Electoral Officer.
• Resolves that the names of candidates on the voting documents be arranged in alphabetic
order of surname.
• Requests the DHB elections communications programme includes the promotion of
nominations as well as encouragement to vote.
• Advertise and conducts “information evenings” for potential candidates (in Hastings and
Napier) prior to nominations being opened.
Moved
Barbara Arnott
Seconded
Diana Kirton
Carried
1.
Key dates relating to the elections include:
13 July
First Public Notice of Election
15 July
Nominations Open / Roll Open for Inspection
12 August
Nominations Close / Electoral Roll Closes
19 August
Public Notice of Candidates
16 September
Delivery of Voting Documents
8 October
Election Day / Voting Closes at Noon
13 October
Official Result Declaration
5 December
New Board comes into office
Electronic Papers Post Implementation Report
Electronic Board papers were introduced in July 2015 through the use of Diligent Boards
application on Surface Pro devices. Given the number of issues that have arisen, a post
implementation review was initiated and recently completed. The report, an independent
assessment, was provided.
Following receipt of the report the Steering Group consisting of Ken Foote, Gina McEwen and
Brenda Crene, considered the contents with Steering Group comments now included against the
recommendations on pages 14 –17 of the report.
A range of comments on the device and application were relayed at the meeting which mirrored
feedback within the report.
The biggest downfall with the device for users of the DHB surface pro devices was the short
battery life, however an independent using his own surface pro for work purposes within the DHB
advised there was no issue (from his perspective) and found the device very good.
Diligent initially was set up for iPad use (Internationally) and more recently developed the app for
Windows 8.1 (the DHB opted to wait for). The diligent app for iPads is very easy to download onto
owned devices for user log in, as usual.
Page 7 of 9
Several agreed the device provided had more functionality than desired, for others not enough (as
the device had been stripped and was not fully functional). This set up (within the DHB network)
had caused a lot of problems for some.
There is now an option to restore full functionality to the surface pro devices and have the Diligent
App easily accessible by the normal user password, (without DHB network password access).
NOTE: If training is an issue, it was advised that Diligent Training is easy to access through the
0800 number 24/7/365. Ken Foote undertook his training via this method and uses most aspects
of functionality extensively. He is happy to sit with anyone and provide assistance, if requested.
If retaining the Surface Pro device we must ensure members have the Diligent App easily
accessible (if the device is re-set to original).
The Chair advised he is keen to have the Central Region on Diligent.
PRESENTATION
Living our Values/Behaviours
The presentation by John McKeefry was received by the Board who requested a copy of the
slides.
Actioned.
Areas covered in the presentation included: What does success look like? Current Status; Values
and Behaviours as well as a number of Actions to be undertaken; including the Promotional
approach – rebranding.
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
RESOLUTION TO EXCLUDE THE PUBLIC
RESOLUTION
That the Board
Exclude the public from the following items:
19.
Confirmation of Minutes of Board Meeting
- Public Excluded
20.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
21.
Board Approval of Actions exceeding limits delegated by CEO
22.
Chair’s Report
Reports and Recommendations from Committee Chairs
23.
Finance Risk and Audit Committee
24.
HB Clinical Council
Moved:
Peter Dunkerley
Seconded:
Diana Kirton
Carried
Page 8 of 9
The public section of the Board Meeting closed 3.16pm
Signed:
Chair
Date:
Page 9 of 9
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 29 JUNE 2016, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.00PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana
Dan Druzianic
Andrew Blair
Peter Dunkerley
Diana Kirton
Helen Francis
Heather Skipworth
Jacoby Poulain
Denise Eaglesome
Apologies
Barbara Arnott
In Attendance:
Kevin Snee (Chief Executive Officer)
Members of the Executive Management Team
Chris McKenna and Mark Peterson (Co-Chairs, HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council)
Members of the public and media
Minutes
Brenda Crene
KARAKIA
Ngahiwi Tomoana opened the meeting with a Karakia.
APOLOGIES
Our hearts are with Barbara Arnott who lost her dear mother.
INTEREST REGISTER
Denise Eaglesome would email a change to the Interest Register through.
Action.
No board member advised of any interest in the items on the Agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 25 May 2016, were confirmed as a correct record of the
meeting.
Moved:
Peter Dunkerley
Seconded:
Diana Kirton
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Item 1:
Te Ara Whakawaiora / Breastfeeding: The additional detail requested would be
included in reporting presented to the Board in September – ongoing.
Item 2:
Re MRB discussions - Progress update provided when available.
Item 3:
Smoke Free in Primary Care: included in CEO’s report and on Clinical Council
agenda. Remove action.
Page 1 of 10
Item 4:
Health Partnerships – Food Services Agreement: actioned and item to be
removed.
Item 5:
MRB’s Recommendations: Healthy populations team were to consider. Advised at
implementation plans are integrated, however they are kept separate in the planning
phase to ensure focus is maintained.
Response to be provided from HPT.
Item 6:
Best Start Healthy Eating and Activity: actioned and item would be removed.
Item 7:
Transform and Sustain Strategic Dashboard: reporting change in progress.
Remove action.
Item 8:
HBDHB Non-Financial Exceptions Report Q3: compliments passed on. Remove
action.
Item 9:
MoH Dashboard for HBDHB Q2: to July meeting, has been included on the workplan.
Remove action
Item 10:
Maori Staff Employed: reporting change communicated for TAW (monitoring) paper to
FRAC in July, prior to circulation to the committees. Work was progressing on a Maori
staffing strategy and The Acting Chair of MRB asked for a preview prior to release.
Action.
BOARD WORK PLAN
On the Workplan provided for July, it was noted that the HB Integrated Palliative Care Draft paper
had been moved to August leaving a fairly light Board agenda for July. The Chair asked
management to review the light agenda and maybe include a further item(s).
Action
27 July
Consumer Story
Kate Coley
Transform and Sustain Refresh
Tim Evans
Final HBDHB Annual Plan 16/17 SOI (on Diligent & Website)
Tim Evans
HB Intersectoral Group Regional Plan TBC
Kevin Snee
Under 19 mental health wait target presentation
Sharon Mason
CHAIR’S REPORT
• The Chair advised the following retirements, with a letter being sent conveying the Board’s best
wishes and thanks for their extended years of devoted service.
Years of
Name
Role
Service
Service
Retires
Barbara
Quality Improvement & Patient
McPherson
Infection Control Advisor
Safety
27
24-Jun-16
Project Management Office
Peggy Kersley
Manager
Human Resources
25
30-Jun-16
Medical Officer in
Dr Richard Loan
Psychiatry
Older Persons & Mental Health
24
29-Jun-16
Dr Philip Baker
Neurologist
Acute & Medical
33
1-Jul-16
Larraine Field
Registered Nurse
Surgical
10+
26-Jun-16
• MoH advises 2.2m NZs have been immunised against influenza thus far in 2016
• Pharmac’s funding decisions was conveyed, including the recent treatment announcement for
two hepatitis C drugs.
Page 2 of 10
• A letter of thanks had been received from an Australian thanking the DHB and staff sincerely for
the prompt and efficient care received from HB hospital and staff.
• Letter from former staff member who had recently spent time in hospital and wished to thank
Dr John Gommans and staff for the wonderful care and service.
• Financial position nationally: the Chair noted that 16 of 20 DHBs in NZ had projected surplus at
the beginning of the 2016/16 financial year. As at 30 April there were only 7 of the 20 in a
projected surplus situation.
• Thanks were conveyed to team and staff for delivering and maintaining continuous surpluses.
CHIEF EXECUTIVE OFFICER’S REPORT
The CEO provided an overview of his report summarised as follows:
• Regarding Asset Management: it is pleasing to note the life span of clinical equipment in HBDHB
has been found to be in better condition than most other DHBs.
• Poor performance in ED with winter woes and the Hospital is under pressure.
• A presentation will be provided shortly around the relationship between ED and AAU 8%
attendances increased in May. The PHO are working with us around strategies in primary care
and also the top 200 “frequent flyers” to ensure packages of care are put in place. There will be
a visit from MoH in the near future around specialising in acute demand area.
• An overview of other areas was provided along with the encouraging financial performance,
however the high cost patient alluded to the Board had not been resolved.
• HBDHB are playing a full role in addressing inequities and those that are amenable to health
interventions are doing fairly well.
• Pharmacy services in the community: as part of a national initiative this is moving towards the
likelihood of having more flexible contracts.
• The CRISP programme of IS work was also live regionally, and moving ahead now with a degree
of confidence.
• In summary, we have made good progress across a range of key strategic priorities whilst
continuing to deliver sound performance across a range of indicators. There remains some room
for improvement in some areas.
• Ngahiwi Tomoana was pleased advising that many areas were looking very positive.
FINANCIAL PERFORMANCE REPORT
The Financial report for May 2016, was reviewed showing a favourable variance of $95 thousand
with a year to date result of $110 thousand favourable. Forecast remains on track for a $3.990m
surplus.
In Summary:
• Inter District Flows (IDFs) remain unknown.
• Elective surgery doing well with increased in-house services.
• A little behind in efficiencies (-16%) on planned activity. However there is unplanned work
occurring with savings resulting.
• Capital spend a little behind but not significant as we carry this over years for large projects.
• Employee numbers are contained.
• One high cost case alluded to the board last month, has yet to be resolved.
Page 3 of 10
CONSUMER STORY
Jeanette Rendle (Consumer Engagement Manager) provided a heartfelt story around excellent
and caring support provided by DHB staff and the impact that had on a families experience.
The CEO advised what happened was a great example of staff living our values, however the
question was whether a rest home situation may have been the best option.
FOR INFORMATION
2016 ELECTIONS AND BRIEFING FROM ELECTORAL OFFICER
Ken Foote, Company Secretary introduced the Electoral Officer (EO) Warwick Laamp who
provided an overview of the up and coming elections process
A consistent approach across the country is being taken with the key areas being:
• 15 July: candidate hand-outs will be available for issue.
• Candidate briefing sessions are planned and potential candidates encouraged to attend.
• Nominations close Friday 12 August.
• There are no controls around timing for campaigning and potential candidates may commence
at any time
• With Social Media more prevalent, care is definitely needed in this area. It was noted that a
candidate cannot use DHB resources in campaign material, and no DHB social media channels
are to be used for campaigning. Candidates are not able to have HBDHB logo appearing on any
of their material and they need to be mindful and make sure they understand what their social
media footprint is, and care is needed if responding to posts. The DHB will delink if this occurs.
• It will be business as usual during the election period 8 July to 8 October. This means elected
member details may remain on the DHB website but not be more prominent.
• DHB staff must ensure neutrality and have a similar set of protocols to ensure no conflicts occur.
• The EO strongly recommends HBDHB staff do not nominate or second candidate nominations.
REPORT FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
Dr Mark Peterson spoke to the report relating to the Council Meeting held 8 June 2016. A
recommendation for the Board to approve a new investment prioritisation was adopted as follows:
RECOMMENDATION
That the Board
Approve $26,000 during 2016/17 (June-December 2016) from the new investment prioritisation
contingency to investigate the recommendations of the Coroner’s report into four suicides in
Flaxmere.
Adopted
It was noted that Council supported the following initiatives at their meeting:
• Food Service team investigating and implementing the recommendations.
• The Mobility Action Programme and RFP to MoH.
• Target Champions Dr Robin Whyman’s recommendations for Oral Health.
Page 4 of 10
• The Board Chair noted the strong message around fluoridation advising that if and when we
have received all detail around fluoride, together with the authority to act, then we could
consider moving with some urgency.
Hawke’s Bay Health Consumer Council
Graeme Norton Chair of Council advised the outcomes of their meeting held on 9 June 2016 in
summary:
• The Youth Health Strategy was supported. At times it is hard to see how strategies are merged
into others at implementation, as it is not often covered in the paperwork. However the strands
connecting to whatever services that flow, need to be carefully managed.
• Positive framework – comment on health equity and framing in the positive. Enabling equity
rather than eliminating inequity as we see this as an opportunity. Frame positive lasts longer. If
framed negatively hard to keep energy levels up.
• The Mobility Action Programme plan was supported. This had been developed to support the
RFP for pilot funding.
• National Consumer Council collective had first teleconference last week. There are four
Consumer Council’s operating at present, with others in the planning stage. A number of DHBs
are really struggling to provide this commitment to form Consumer Councils. Graeme expressed
he was keen for the Board Chair, CEO as well as the Co-chairs of Clinical Council to voice the
value of Consumer Council, as many need confidence to get this over the line.
Pasifika Health Leadership Group
Talalelei Taufale Pacific Health Development Manager was in attendance and addressed the board
around the Pasifika dashboard. This is part of the national plan for improving health outcomes for
Pacific people in NZ and the Pasifika Health Leadership Group had adopted the dashboard as the
foundation to measure and review improvements for their people. The framework compared other
DHBs in NZ and HB performed well.
The Areas of Progress and the Challenges were noted and the layout of the dashboard was
discussed. Board members advised they were happy with the 20 indicators and the format used.
This report would be provided every six months.
RECOMMENDATION
That HBDHB Board:
1. Adopt the health priorities as per the Ministry of Health Ala Mo’ui Pathways to Pacific Health
2014-2018 as the Pasifika health priorities for HBDHB.
2. Report six monthly progress to the HBDHB using the Ala Mo’ui dashboard with local
commentary provided.
Adopted
Māori Relationship Board (MRB)
Heather Skipworth (Acting Chair) provided an overview of the meeting held 8 June 2016:
• Maori Staff target was noted in the recommendations as MRB wish to push the target higher.
• Heather advised MRB would like to see the Maori Staff Strategy prior to issue to FRAC
Action. • Regarding the Health Equity Report provided, MRB were happy with this and like Consumer
Council, MRB want to celebrate the successes.
• The Te Ara Whakawaiora Fluoride aspect of the recommendation was not adopted by MRB as
they wanted to hear what the concerns were first. There will always be those campaigning
against fluoride and we need to be courteous.
Page 5 of 10
• MRB were pleased to see Suicide Prevention funding approved.
Ngahiwi Tomoana was keen for HBDHB to be a flagship employer.
Advised that management will look at doing significantly better but not sure whether the 25% target
was realistic.
Outside of health, Iwi are working with growers to encourage their uptake of permanent Maori
workers (vs utilising those from overseas). Through government agencies, Iwi and training
organisations, our people are targeting areas to bring new jobs. This would involves up skilling and
training potential employees.
The Board noted all nine of
MRB’s recommendations (in italics below) regarding priority actions
required to further reduce health inequality in Hawkes Bay and requested the CEO to further
investigate and report back on these.
Action
2.
Approve the following as priority actions required to further reduce health inequity in Hawke’s
Bay:
a)
Raise the target to Increase Māori Staff from 10% year-on-year to 25% over a five year
period
b)
Present the strategy to Increase Māori staff to MRB before going to the Finance, Risk
and Audit Committee (FRAC).
c)
Review the current HBDHB hiring protocols and processes
d)
Review the conviction policy for the HBDHB and whether a conviction that is old, is
relevant now
e)
Broaden the scope of the target to all disciplines, not just medical, nursing and allied
health
f)
Shift the responsibility of achieving the target to Hiring Managers setting KPIs for
monitoring
g)
Senior Management monitor the progress of the target and provide monthly updates
identifying why the target was achieved, or not achieved
h)
Train Hiring Managers to efficiently and effectively use the Managers Toolkit
i)
Māori Health Service involved in the recruitment processes from the development of
position profiles, shortlisting and interview stages with a member of the team becoming
a compulsory member of all hiring/selection panels
3.
MRB did not approve recommendation number 4 of the Te Ara Whakawaiora: Oral Health
paper but instead approved the following actions:
a)
Target Champion to present information about the benefits and side effects of
Fluoridation to get a clearer understanding of Fluoridation
b)
HBDHB champion sugar free beverage events and challenge all other organisations to
do the same.
The Board noted items 3. a) and b) appeared practical
.
• Ask DHB for water only in schools, as this message would be better coming through a health
organisation. Now have healthy eating approved. Are looking at sugar free beverages for
schools and events. The Chair asked this request be passed on.
Action for consideration.
• DHB to consider food wastage and look at providing to homeless. This would be looked into.
Action for consideration.
Page 6 of 10
FOR DECISION
FOOD SERVICES OPTIMISATION REVIEW
Sharon Mason introduced Gavin Carey-Smith and Jill Foley who provided an overview and the
request for the board to support implementation of the recommendations contained in the report.
The capital involved would come through a separate process.
A discussion around software with members advised the team were investigating a number of
suppliers and options used presently in NZ. If this is connected with what HBL are doing it would be
looked at but we do need to go with the best option for us.
Following discussion the following recommendation was adopted.
RECOMMENDATION
That the Board:
1.
Note the contents of this report.
2.
Support the Food Service team in investigating and implementing the recommendations.
3.
Note capital applications that arise from recommendations below will be put through the
capital plan process for approval.
Adopted
YOUTH HEALTH STRATEGY 2016-19
Dr Caroline McElnay introduced Nicky Skerman (Population Health Strategist
Women, Children and
Youth).
The development of this strategy had been through a rigorous process to get to this point. Going
forward – go back to youth consulted with and identify leaders in those groups with the intention of
doing some training around governance for those identified (likely 6 in total).
Feedback included
• We have the most vulnerable whanau here in HB yet nothing was mentioned. Many whanau are
now young solo mums with high risk factors. Feel this is an omission which needs addressing.
Feel the solution lies there as well as with the gangs. Young mums in Wairoa need to be part
of 16 to 19 year old group.
• Jacoby supported Ngahiwi as this should be applicable to all youth but there are polar differences
across our community. Rex Tumu holds a forum for Rangatahi – those who want to advocate
for themselves. If taking about Flaxmere 50% are single mums under 25 years old. Good
opportunities to create synergies.
• What about a partnership with secondary schools?
• Focus on positive development of all youth (the whole young person) is not just about picking
out the most vulnerable.
Nicky advised the priorities would be driven by the young people around the table who would be
from all ethnicities and situations.
• Nice if this group could report back regarding change. They should ID priorities and who
stakeholders should be and produce an action plan. How to structure youth services going
forward and what we want from them.
• Board were very supportive and interested to see how this strategy develops and adopted the
following recommendation with comments raised provided to Nicky Skerman.
Page 7 of 10
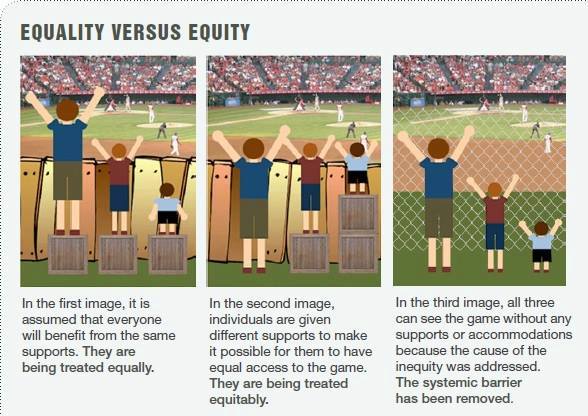 RECOMMENDATION
That the Board:
RECOMMENDATION
That the Board: Endorse the Youth Health Strategy 2016-19.
Adopted
An Update on the Youth Health Strategy 2016-19 would be provided to the Board in July 2017 (this
was already on the detailed workplan).
FOR DISCUSSION
SUICIDE PREVENTION AND POSTVENTION PLAN
Dr Caroline McElnay introduced Penny Thompson who provided and overview of this update on
progress against the plan submitted in 2015.
Discussion summarised:
• What are the main challenges? Had not done as much community consultation as should have
been done as this needs to be monitored on an ongoing basis with agencies.
• Police advise that social media was the biggest driver of suicide.
FACEBOOK this month is now actively involved and is monitoring their site closely. They
acknowledge they have a role to play. Also newspapers are naming and shaming.
• An overview of the extra work Penny would be involved with as a result of the Coroner’s report
was provided. 1st establish a working group to ensure all agencies/networks are linked.
• Set up an interagency governance group. Go first – sit there at a senior level.
HEALTH EQUITY UPDATE REPORT 2016
Dr Caroline McElnay provided an update (as Health Equity Champion) for the sector, which was well
received by the Board.
In summary:
• The report provided a snapshot of 18 indicators compared with 49 indicators (nationally). This
sub-set was grouped to show how HBDHB was doing.
Of the 18 indicators compared: Health equity was achieved in 1 indicator; Good progress in 3;
could do better in 9; with no change/or worse in 5 indicators.
Insight into Iron Maori and how this
programme provides health benefits
was provided.
The board were asked, how should we be
tackling?
• Behaviour and risk
• Social and economic factors
• Healthcare
Were there more areas we should add? In
response, could add “sport”.
Guardian impact of sport in schools was
mind boggling. There were examples of
schools that don’t and do focus on sport.
Page 8 of 10
When Caroline McElnay returns from three months sabatical, she will continue her work in this
area.
MONITORING
TE ARA WHAKAWAIORA / ORAL HEALTH
Sharon Mason introduced Dr Robin Whyman (Director of Oral Health Services)
• Under 5 year old caries free indicator is now being used increasingly. Worldwide there is a
growing body of evidence of the decay picture in children and the increasing their move into
adulthood.
• While there has been some improvement over past years (10% or so), we have not moved the
inequity. Nationally this is a challenge.
• We now obtain our targeted children through a quadruple integrated approach with Well Child
therefore are not chasing mums to enrol their children.
• Jacoby a board member and first time Mum, was not contacted in the child’s first year. Need to
address the wider cohort rather than those not turning up.
• Improving in the dental practice areas, however we need to make sure we have early prevention.
Nationwide awareness campaign – engaged soon including messaging will be helpful.
• The timeframe for fluoridation under DHBs (instead of Councils) was unknown, however a
legislative change was planned within this government’s term.
• There are real benefits for fluoridisation however the bigger picture needs to be understood.
Robin Whyman would advise when more information was to hand around bullet point four
(below).
• Denise sought Robin’s help with the Wairoa Council.
RECOMMENDATION
T hat the Board:
1. Note the contents of this report
2. Adopted the Target Champions recommendations for Oral Health as follows:
• That Maori health provider contracts are changed to focus on engagement of hard to
reach whanau with oral health services in the early pre-school years (by June 2017)
•
That Community Oral Health Services achieve the preventative practice targets (by
December 2017)
•
To implement Maternal Nutrition Programme activities and implement healthy
eating/sugar reduction programmes/policies as planned in the Best Start: Healthy Eating
and Activity Plan (Reported annually until 2020)
• That Hawke’s Bay DHB implements community water fluoridation as soon as necessary
legislative changes enabling the DHB to act are in place.
Yet to be confirmed, dependent upon legislative changes.
Adopted
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
Page 9 of 10
RESOLUTION TO EXCLUDE THE PUBLIC
RESOLUTION
That the Board
Exclude the public from the following items:
22.
Confirmation of Minutes of Board Meeting
- Public Excluded
23.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
24.
Board Approval of Actions exceeding limits delegated by CEO
25.
Chair’s Report
26.
Integrated Pharmacist Services in the Community
27.
Regional Development Strategy
Reports and Recommendations from Committee Chairs
28.
Finance Risk and Audit Committee Report
Moved:
Dan Druzianic
Seconded:
Peter Dunkerley
Carried
The public section of the Board Meeting closed 4.45 pm
Signed:
Chair
Date:
Page 10 of 10
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 25 MAY 2016, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.03PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana
Andrew Blair
Dan Druzianic
Peter Dunkerley
Diana Kirton
Barbara Arnott
Helen Francis
Heather Skipworth
Jacoby Poulain
Apology
Denise Eaglesome
In Attendance:
Kevin Snee (Chief Executive Officer)
Members of the Executive Management Team
Chris McKenna and Mark Peterson (Co-Chairs, HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council)
Members of the public and media
Minutes
Brenda Crene
KARAKIA
Ngahiwi Tomoana opened the meeting with a Karakia.
APOLOGIES
An apology was noted from Denise Eaglesome.
INTEREST REGISTER
No changes to the interests register were advised.
No board member advised of any interest in the items on the Agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 27 April 2016, were confirmed as a correct record of the
meeting.
Moved:
Barbara Arnott
Seconded:
Diana Kirton
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Item 1:
Budget Update and Investment Prioritisation was included on the board agenda for
discussion (agenda item 16) – action item removed.
Item 2:
Clinical Pathway for HepC – status update provided. Item can be removed
Item 3:
Te Ara Whakawaiora – Breastfeeding – ongoing, detail expected in September.
Item 4:
Workplan for May – amended following EMT discussion. Item can be removed
Page 1 of 12
Item 5:
Regional Health Improvement program – actioned. Item can be removed.
Item 6:
MRB discussions – verbal update from Tracee TeHuia that the meeting had been
delayed, pending a replacement within NKII’s Health Portfolio.
Ongoing
Item 7:
Transform and Sustain refresh topics – actioned, item can be removed
Item 8:
Living our Values / Behaviours presentation issued to board members, remove action.
BOARD WORK PLAN
The Board Work Plan was noted out to March 2017 with several additions as follows:
27 July
Consumer Story
Kate Coley
Draft - Developing a Person Whanau Centred Culture
Kate Coley
Annual Organisational Development Plan/Programme
John McKeefry
Draft - HB Integrated Palliative Care
Tim Evans / Mary Wills
HB Intersectoral Group Regional Plan TBC
Kevin Snee
Health Equity Report
Caroline McElnay
Transform and Sustain Refresh
Tim Evans
Te Ara Whakawaiora / Oral Health
Robin Whyman
CHAIR’S REPORT
The Chair advised the following retirements, with a letter being sent conveying the Board’s best
wishes and thanks for their extended years of devoted service.
Years of
Name
Role
Service
Service
Retired / Retires
Pauline Gordon
Care Associate
Surgical
16
3-Apr-16
Merehira Edwards Registered Nurse
Surgical
35
2-May-16
Facilities &
Kathy Simmons
Health Records Associate
Operational Support
22
18-May-16
Facilities &
Barbara Stewart
Receptionist - Outpatient
Operational Support
15
31-May-16
•
Published statistics “How is my DHB performing?” for 3rd quarter of 2015/16:
The HB Today had published “How is my DHB performing?” with Hawke’s Bay reflecting well
for: Immunisation at 96% (cf target of 95%); Improved Access to Elective Surgery at 102%
(which was above the 100% target); and on target at 90% for Better Heart and Diabetes
Checks.
Those below in Hawke’s Bay included: Shorter stays in ED at 1% below target; Better help for
smokers to quit (below for PHO enrolled patients); and Faster Cancer Treatment (FCT).
FRAC had discussed the detail around the new FCT target, how it was measured, and
anomalies around early detection.
With added focus in this area, improvements were expected in the near future.
•
Smoke Free:
The Chair expressed his concern at the low target achieved for “Helping Smokers to Quit” (in
the Primary Care setting). HB had achieved 78%, well below the 90% target. There had been
a noticeable drop in this major MoH target and this needed to be turned around immediately.
Management and the PHO were challenged to at least reach the middle of the pack in the very
near future. The Board wanted to hear how this was going to be achieved.
Page 2 of 12
Nicola Ehau (Manager Innovation & Development for Health Hawke’s Bay Ltd) was in
attendance and provided an overview on the areas of focus for smoke free which should see
the target achieved by the end of June 2016. Resources within the PHO and DHB were
working alongside each other to assist and encourage practices to achieve targets with their
support.
A question was asked around how other PHOs (nationally) achieved the results they had. In
most, if not all cases results were achieved by providing additional resources. Every PHO had
a different approach, in Auckland there were active smoking champions out in the community.
The concept was similar even though the structure was different.
The end goal is to have smoke free become part of “business as usual” for all general practices
in Hawke’s Bay.
Action CEO:
HBDHB CEO would now include a smoke free update
in his report monthly.
Action Clinical Council co-Chairs: Clinical Council will ensure added focus is placed on
smoke free in primary care.
Dr Mark Peterson advised the real challenge was that this was a 15 month rolling target, with
2,000 being the base contacted consistently. Practices are not in that place yet.
•
The Chair noted an extra $39m for
Pharmac had been advised.
•
The MoH had extended the term of the
Commissioner at Southern DHB, until 2019.
•
MoH had announced a new role in Pharmacy. A new technician will help free up
pharmacists to spend more time with patients. Pharmacists will still be responsible clinically
for correct prescriptions.
•
Advised the
MoH had disestablished the National Health Committee and the National
Health Board and the Ministry of Health would take over the functions performed by these
groups.
•
Health Partnerships Limited (HPL) were asking DHBs to reconsider participation in the
Food
Services Agreement. This would be a key topic at following weeks Forum in Wellington.
HPL seek to achieve the greatest level of participation as possible and the Chair wanted to be
assured that HBDHB Board were still comfortable with the decision not to participate. Board
members advised the Chair they were fully supportive and had no intention to review their
decision.
Action:
HBDHB’s CEO would advise that HBDHB Board remain strongly in favour of
their past decision, and did not wish to reconsider HPLs Food Services
Agreement.
CHIEF EXECUTIVE OFFICER’S REPORT
In presenting his report, the CEO noted in particular:
• Food Services Optimisation Review around quality and efficiency which has been undertaken
and may require some capital investment. An update will be provided in June. Electronic
ordering had been noted in an earlier review.
• Targets: a drop had been noted for shorter stays in ED for the month, as well as faster cancer
treatment (further discussed later in the meeting). Better help for smokers to quit in the Hospital
had dropped but was above target by 2.6%; with More heart and diabetes checks down .5%
below the target of 90%.
• Hawkes Bay’s financial performance is good, compared to the rest of the country.
• An overview of the papers included on the agenda was provided, noting good progress.
Page 3 of 12
FINANCIAL PERFORMANCE REPORT
The financial result for April 2016, was an unfavourable variance of $173 thousand with a year to
date a favourable result of $15 thousand cumulative. This included contingency of $250 thousand
released to cover the rest of the elective surgery costs. As well as an additional $100 thousand
transferred to Surgical Services and $90 thousand contributed to the corporate savings plan (3%).
Overall this left $166 thousand of the contingency for the remaining two months of the financial year
ended July 2016.
Not an easy month but believe HBDHB are still on track to reach year end surplus target.
CONSUMER STORY
Kate Coley (Director of QIPS) provided board members an insight into a patient’s experience (in
day surgery) as well as the experience of the patient’s support person. The need for timely
effectively communication with a stressed and anxious family member was noted, in contrast to
the person receiving surgery who found the journey relaxed and comfortable.
The outcome of this story will see improvements made to internal processes in the day surgery
area.
REPORT FROM COMMITTEE CHAIRS
Combined Hawke’s Bay Clinical Council and HB Health Consumer Council Report
This follows the joint meeting held on 11 May 2016.
Clinical Council considered their own agenda for the first part of this meeting, with Consumer
members joining thereafter. This was the second joint meeting held with a collaborative spirit evident
which was reflected in the constructive discussions. Several more joint meetings were likely during
2016.
The Healthy Eating and Activity plan reflected good co-design with consumer members. The same
process had been used for the Youth Health Strategy with very positive feedback on the work done
to date. The final report on this strategy is expected in June.
Customer Focused Booking Programme was now planned to include a much wider focus as the
customers don’t just need a good booking system, they need more flexibility. Appointments are now
often required outside normal working hours 8am to 5pm (5 days per week). A more holistic and
flexible system will take more time to develop and implement.
Best Start: Healthy Eating and Activity was well received with strong support.
An update on the Travel Plan was provided with good progress being made. This will be a big culture
change for staff.
Reappointments to HB Health Consumer Council
With approval noted by the CEO’s of HBDHB and Health HB; and the associated background
provided to board members, the following resolution was endorsed.
Page 4 of 12
RESOLUTION
That the Board endorse the CEO’s approval to reappoint the following members of Consumer
Council for a further term of two years.
James Henry
Malcolm Dixon
Leona Karauria
Rosemary Marriott
Terry Kingston
Tessa Robin and
Heather Robertson
Moved
Helen Francis
Seconded
Barbara Arnott
Carried
Māori Relationship Board (MRB)
Heather Skipworth (Deputy Chair) provided an overview of the Meeting held on 12 May 2016 and
noted the term “obesity” had already been largely been removed from the May reports which was
very pleasing to see.
The following was put forward for the Board’s consideration
RECOMMENDATION
That the Board
1.
Note the content of this report, and
2.
Consider MRBs advice and recommendations regarding the Best Start: Healthy Eating
and Activity Plan Final, as follows:
•
The term ‘Obesity’ be removed where practical within the plan. MRB understands
full exclusion may not be achievable because the plan is a public document and that
‘obesity’ is a clinical term
•
Refrain from using the term ‘Obesity’ within the community to eliminate the
stigmatising of children and youth
•
Linking the Best Start: Healthy Eating and Activity Plan, Youth Health Strategy and
Suicide Prevention Plan together to achieve an integrated approach. The strategies
convey similar messages but are not connecting together.
Endorsed
Pasifika Health Leadership Group (PHLG)
Barbara Arnott provided an overview from the PHLG meeting held on Monday 9 May 2016.
Barbara advised it was very pleasing to see the bid for two Pasifica navigators was successful
(pending board approval).
PHLG have come of age and it had taken a long time for them to understand how they could make
a real difference. The Pasifika people have a range of cultures and language differences which at
times has been overwhelming. Pacific people is the fastest growing area in our population in HB
and accessing health services is paramount. Many have not been to, or lived in NZ before.
Page 5 of 12
Pacific health has benefitted from the navigator/facilitation role(s) however two more Pasifica
navigators will be very well received to ensure timely access to health services.
FOR DECISION
Final Draft HBDHB annual Plan 2016/17, and the
Final Draft of the Central Region Regional Services Plan 2016/17
The final drafts were received and distributed to board member on 24 May, the day prior to the Board
meeting for members to review.
The process for approval was a little cumbersome to ensure MoH timelines were met. The reports
provided were not in final form however but do require approval subject to further changes which
would be incorporated into the plan by 30th May.
Carina Burgess (the author) advised areas that could change, were clearly identified in the reports
provided and outlined in the cover report.
Following discussion the recommendation was approved.
RESOLUTION
That the Board:
•
Approve the Final HBDHB Annual Plan 2016/17 and Central Regional Services Plan 2016/17
subject to any minor changes that may occur from the final feedback received by MoH on 13th
June.
•
Note the HBDHB Māori Health Plan is incorporated into the HBDHB Annual Plan 2016/17.
•
Delegate(s) Kevin Atkinson and one other board member to review and approve minor
changes and sign the final documents prior to 17th June.
Moved
Dan Druzianic
Seconded
Andrew Blair
Carried
The process from here includes:
Any changes from EMT/Board incorporated into Final Draft Annual Plan, Māori Health Plan and Regional
30th May
Services Plan, Submitted to MOH and loaded onto Diligent
Final Draft HBDHB Annual Plan to the Board
2nd June
Final Drafts to Māori Relationship Board (MRB)
8th June
Feedback on Final Draft of Annual Plan, Māori Health Plan and Regional Service Plan from MOH
13th June
Delegated Board Members to review, approve and sign Final Plans
16th June
Final Annual Plan and Regional Service Plan due to MOH
17th June
Final HBDHB Māori Health Plan 2016/17 due to MOH
30th June
Best Start: Healthy Eating and Activity
Shari Tidswell (Team Leader/Health Promotion Advisor) provided an overview to board members,
acknowledging the feedback received from the committees during the month.
The Plan provided an evidenced-based approach to increasing healthy weights for children in
Hawke’s Bay which will be delivered with community partners (in order to support whānau
engagement) and integration with existing programmes.
The Board noted the three advisory committees had recommended the Best Start: Healthy Eating
and Activity plan be adopted.
Page 6 of 12
Comments included:
• MRB’s Deputy Chair Heather Skipworth was happy to see the term “obesity” used sparingly in
the document presented to the Board, and was happy to hear the team were very clear about
not over utilising the term obesity in the community.
• From personal experience, a member advised there appeared to be very little information
available on maternal nutrition.
Shari noted there was a referral pathway and midwives needed to be further reminded in this
area.
• It was noted the biggest single influencing factor on a child’s diet was their parent(s). There
was very little reference in the document o parents/carers or to GPs (who support families and
provide referrals). In response -
B4 school checks were in place and providers asked about what tools help.
Healthy first food discussions with mums.
For older aged children gaps occurred in accessing primary care. These are limited but
want to develop other programs eg, through green prescription and active families, which is
a referral pathway through Primary care.
The CEO advised HB has a role in leadership and will need to advocate for changes nationally and
locally to develop an environment which supports healthy lifestyle changes.
HB will be reporting against the target B4 School checks as a measure against national target.
Action:
A full review against plan for Best Start Healthy Eating and Activity was agreed to
come back through the Committees to the Board in May 2017. This would be included
on the detailed workplan.
RECOMMENDATION
That the Board:
1. Noted committee feedback.
2. Approved the Best Start: Healthy Eating and Activity Plan.
3. Agreed a full review against plan, would be provided in May 2017
Adopted
Budget Update and Investment Prioritisation
An update was provided by FRAC’s Chair Dan Druzianic (who referred members to page 23 of the
FRAC report) and put forward a FRAC Recommendation for Board approval.
Board members who had not attended the FRAC meeting were asked if there were any queries on
any aspects of the proposed resolution they wished to discuss.
RESOLUTION
That the Board
1.
Approve the budget to make annual savings of $13 million for the 2016/17 financial year
($10.3 million to balance expected unavoidable commitments and demands and $2.7
million for new investment)
Page 7 of 12
2.
Approve Option 2 (Net Expenditure – PBFF) be adopted in terms of moving and
measuring strategic resource deployment and for savings allocations.
3.
Endorse the process undertaken by Clinical Council to prioritise the requests for new
investment.
4.
Note the
comments from the Māori Relationship Board
5.
Approve Clinical Council’s recommendations and savings options for new investments
totalling $2m.
Moved
Dan Druzianic
Seconded
Peter Dunkerley
Carried
FOR INFORMATION / DISCUSSION
Travel Plan Update
Andrea Beattie provided a video outlining proposed travel options for staff. Parking has been an
ongoing problem for a number of years (for the public) and a wide range of innovative ideas and
options shown in the video related to staff hoping to reduce their travel to the hospital site. Options
included: car-pooling, extra cycle stands, covered areas and extra showers, reconfiguring car parks,
as well as the Regional Council altering and increasing bus transport options at peak times (including
park and ride). Overall the plan is to encourage exercise and alternative means of travel to work,
and to free up parking for the community.
The “Go Well” travel plan project formally kicks off from 1 July, with this promotional video initiating
conversations with both internal and external stakeholders.
Discussion included:
• Had the Hastings District Council been approached suggesting the introduction of angle parking
in McLeod Street? Advised this had not been taken any further at this time.
• Good communications need to be ensured for staff around showering facilities, bike parks etc.
• Benchmarking – how do we ensure we have made a difference (over time) following
implementation?
In response, we do have a mechanism to compare with a year later. A survey undertaken has
provided a “base” snapshot (by those who filled it in). This would be re-done again in future.
The Chair was pleased with progress, and looked forward to the project formally commencing on 1
July 2016. The next Travel update would be provided in August.
Customer Focused Booking
Carleine Receveur the project lead introduced her paper and acknowledged the feedback to date
from MRB and Clinical and Consumer Council.
This was about putting the customer at the heart of the booking process and changing the interaction
we have with our customers. In the past we have disempowered our population and have appeared
as dictatorial around appointments/bookings to suit the clinics rather than the customers. This
project starts from the very beginning by re-defining bookings and re-engaging with staff and
customers and co-designing a system that works for everyone.
Due to complexities uncovered during the course of the project, Customer Focussed Bookings has
become a “programme of work” under which project(s) or work streams have been put in place. To
this end a project entitled “Clinical Scheduling and Booking” is recommended to be put in place as
a pre-requisite to ensure standardised processes are in place before implementing “UBook”.
Page 8 of 12
The following was summarised:
• Need to be careful with data security, with IS working to ensure this is not compromised.
• 80% of rescheduling has occurred for DHB related reasons. This is a priority area for the project
and because of this timeframes are in ‘amber’
• Booking staff need to interact well across specialties and some innovative training has been
undertaken with favourable outcomes. Quality around bookings has improved and risks have
since reduced.
• The work done on the DNA Project had raised issues and these have been noted and absorbed
into the work being done. Work continues with Maori in co-designing systems/approaches that
work.
• Presently plan to have the booking system in place and running by the end of 2016 with the
Ophthamology area being first.
In discussion:
• Does “UBook” allow for early evening appointments? In response - if a speciality sets this up
as such this will be achievable. The system will provide for whatever specific specialty booking
times are.
• Are other DHBs looking at “UBook”? The MoH have supported Hutt Valley’s “UBook” system as
very innovative. Hutt are working with HBDHB first.
• What other software products have been looked at? There is presently nothing else on the
market that is comparable.
• Can “UBook” be linked to the GO WELL travel times. It is well understood that those booking
themselves take responsibility (to travel and attend times they have booked). This frees up the
booking staff to focus on areas where they are most needed which may well include considering
travel time details when booking for customers.
RECOMMENDATION
That the Board:
• Note the contents of this report.
• That due to the complexity and depth of work involved in clinic scheduling, Customer
Focused Booking is shifting from a project to a programme. Under this umbrella programme
a discreet project for Clinic Scheduling and Booking is being developed.
Adopted
Timelines Follow:
Activity
Timeframe - 2016
Download UBook files into test environment
March - May
Internal testing of UBook by bookers and administration staff
June - July
Further IT development (e.g. integration into Webpas)
Aug - Sept
Robust testing in the external environment
Sept - Oct
Further developments / testing / troubleshooting
Oct - Nov
Training, communications
Nov
Go Live (with speciality)
Dec
Information Service Function Review Update
Tim Evans (GM PIF) provided an update on progress following a presentation to the Board (which
had including Davanti personnel) in March 2016.
Page 9 of 12
The board were advised the Steering Group had been appointed and the Terms of Reference was
with EMT.
Advice was being received from HR and the GM PIF had gone through the initial structure with
everyone to obtain ideas on shape and issues aired. He advised the Davanti proposal milestones
(as had been advised earlier) had been reset to meet the DHBs expectations and KPIs would be
developed to show progress and improvements were being made which would come through the
steering group. Technical support was being provided to the Project Sponsor.
The Board had reviewed progress and the next steps, understanding there was an expectation the
project would take six months.
The Board were asked for their thoughts around the update and planning to date.
Due to the sensitive nature of some of the issues to be discussed, the Board
moved into Public Excluded (refer to Resolution to Exclude).
The public board meeting then reconvened following the discussion.
MONITORING
Transform and Sustain Strategic Dashboard Q3 Jan-Mar 16
The framework is a tool to convey specific areas where poor performance and/or progress are
indicated. Tim Evans advised he wished to handle this reporting in a different way and use the
dashboard as a framework by taking subjects/projects and managing the workload to FRAC. He
felt this would be a more powerful tool.
The Board were happy with this approach.
Actions GM PIF:
As a result of the board’s agreement, under-performing dashboard
measures will be developed.
HBDHB Non-Financial Exceptions Report Q3; and MoH Dashboard Q2
Tim Evans drew attention to the Achievements, Areas of Progress and Areas of Focus. The latter
being our focus to hit target: on better help for pregnant women to quit smoking; faster cancer
treatment; and children without dental caries at five years of age.
The Chair referred to the comments included within the report and passed compliments on to those
who do this work.
Action
Tim Evans to relay the board’s thanks to the comment writers for the HBDHB
Non-Financial Exceptions Report.
Monitoring Dashboard for Quarter 2 (Oct-Dec 2015) provided by the MoH
HBDHB’s only red highlight was for “under 19 year olds mental health waits” in spite of active work
in this area.
Action:
Sharon Mason advised that more information on the under 19 Mental Health
waits is expected and would be presented at the July Meeting.
Annual Maori Health Plan Q3 Jan-March 2016 Dashboard
Tracee TeHuia (GM Maori Health) spoke to the dashboard provided.
The board were advised there had been a conversation around comparative reporting with the
suggestion the Annual Maori Health Plan dashboard be presented in the same format/template as
the Non-Financial Exceptions Report; but relay what was happening within the ethnicities. Need
to provide a picture of the HB population to enable better understanding.
Page 10 of 12
It was pleasing to note the good conversations around the proposed new UBook (customer
booking) system due commence at the end of the calendar year.
Good responses had been received around change proposal for the DHB Māori Health Service.
Dr Gommans focus on clinicians attending the “engaging effectively with Maori” training was
commended. Five of the doctors had commented the training has been beneficial to them.
Great to see an excellent result for quick access in angiograms in the last quarter.
The new Te Ara Whakawaiora programme for 2016/17 has now been signed off and reporting will
be coming through the committees to the Board from the target champions.
Human Resource KPIs Q3
John McKeefry provided a brief overview of the report provided, with the main focus being on the
Maori staff employed target. We do know that of all applicants, 9% are Māori with 15% of Maori
being shortlisted which is encouraging. Of resignations received in the three months to 31 March
2016, only one person of 89 identified as Maori through the exit interview process.
This year our Māori staff employed target plateaued, despite active efforts. We cannot be complacent
even though HB are doing better in this areas, than most DHBs.
Action:
The following comments would be considered by HR and GM Maori Health
• HR are strongly recommending that Maori health services staff be included on interview panels,
including Allied Health also.
• Can exit interviews by made compulsory for Maori staff who had resigned, to better understand
their reasons for leaving (and apply the learnings gained). It was suggested such exit interviews
may be undertaken by a Maori Health Service staff members by way of a chat. Privacy issues
need to be considered.
• Do the DHB go out to various campuses to recruit (for Maori)? Other than sensitiveness around
the Human Rights Act, it was acknowledged it could be an area of focus (outside of EIT and
medical grads).
Deputy Chair Ngahiwi Tomoana advised there are a lot of Maori with transferable skills. Health is
the biggest employer in HB. A lot of graduates ask how they can come back to help their people,
however the focus is often not on health. Ngahiwi
personally felt there were a several areas that
could be focused on:
Communication Strategy: Go out to the Maori communities, schools, iwi, community and
conduct a drive to become a health professional, or health worker.
Focus on present Māori employees and get their stories into the community. Drive this
as the place to work.
We have passive recruitment presently. It was noted that Iwi have not been proactive in the area of
health employment either – this can be done in partnership!
Action:
Te Ara Whakawaiora: Culturally Competent Workforce is currently due through
the committees in August 2016.
This is being reported in two parts a) HBDHB staff who are Maori; and b) HBDHB
staff who have completed Treaty on-line training.
1. It was agreed the TAW Culturally Competent Workforce report would go to
FRAC (in July) prior to going through the Committees (in August). This would
be altered on the detailed workplan and TAW schedule.
2. As part of the Maori staff recruitment Campaign develop a “Communication
Strategy” in partnership with Iwi to drive the employment of Maori.
HR and
Comms.
Page 11 of 12
Te Ara Whakawaiora - Cardiovascular
Dr John Gommans spoke to the paper noting the indicator had been met locally and by ethnicity.
Overall a good result. Regional data is included as HB is a long way from the tertiary centre
(Wellington). HB do undertake procedures here but need to prioritise patients to Wellington.
A Cardiology Review TOR being drafted presently (Sharon), with no immediate change to the service
in the very near future.
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
RESOLUTION TO EXCLUDE THE PUBLIC
RECOMENDATION
That the Board
Exclude the public from the following items:
19.
Information Service Function Review (part)
26.
Confirmation of Minutes of Board Meeting
- Public Excluded
27.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
28.
Board Approval of Actions exceeding limits delegated by CEO
29.
Chair’s Report
Reports and Recommendations from Committee Chairs
30.
Finance Risk and Audit Committee
31.
HB Health Consumer Council and Clinical Council
32
Maori Relationship Board
The public section of the Board Meeting closed 4.12 pm
Signed:
Chair
Date:
Page 12 of 12
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 27 JULY 2016, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.00PM
Present:
Kevin Atkinson (Chair)
Dan Druzianic
Andrew Blair
Peter Dunkerley
Diana Kirton
Barbara Arnott
Helen Francis
Heather Skipworth
Jacoby Poulain
Denise Eaglesome
Apology
Ngahiwi Tomoana
In Attendance:
Kevin Snee (Chief Executive Officer)
Members of the Executive Management Team
Dr John Gommans for HB Clinical Council
Graeme Norton (Chair, HB Health Consumer Council)
Members of the public and media
Minutes
Brenda Crene
KARAKIA
Heather Skipworth opened the meeting with a Karakia.
APOLOGY
Noted above from Ngahiwi Tomoana who was in talks with Ministers around the Regional
Economic Strategy.
INTEREST REGISTER
No changes to the interests register were advised and no board member advised of any interest in
the items on the Agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 29 June 2016, were confirmed as a correct record of the
meeting.
Moved:
Dan Druzianic
Seconded:
Peter Dunkerley
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Item 1:
Te Ara Whakawaiora/Breastfeeding: Will be included in the CEO’s report in
September. Action remains.
Item 2:
Discussion with NKII to be held in September. Remove action.
Item 3:
MRB Recommendations: Nick Jones to respond.
Page 1 of 5
Those raised in June had been addressed by HR under action item 4 and also under
item 5.
Item 4:
Maori Staff Employed – paper provided to FRAC 27 July for consideration entitled
“TAW / Culturally Competent Workforce” will be provided to the Board in August.
Remove action.
Item 5:
Actioned
Item 6:
Ensure board agenda remains consistent (removing peaks and troughs).
Noted, remove action.
Item 7:
Unnecessary to note interests for member Denise Eaglesome - remove action.
BOARD WORK PLAN
The Board Work Plan was noted and would be updated at least to calendar year end.
The papers in italics have been deferred.
31 Aug
Consumer Story
Kate Coley
Draft Quality Accounts
Kate Coley
Travel Plan update – verbal
Sharon Mason
Annual Organisational Development Plan/Programme now Nov
John McKeefry
Community Based Pharmacy Services in HB - Strategic Direction
Billy Allan
HB Integrated Palliative Care (Draft) now Sept
Mary Wills
Final HBDHB Annual Plan 16/17 SOI (on Diligent & Website)
Monitoring
HBDHB Non-Financial Exceptions Report Q4 Apr-Jun 16
Tim Evans
Annual Maori Health Plan Q4 Apr-Jun 2016
Tracee TeHuia
Transform and Sustain Strategic Dashboard Q4 Apr-Jun 16
Tim Evans
Human Resource KPIs Q4
John McKeefry
Te Ara Whakawaiora: Culturally Competent Workforce includes
John McKeefry
Maori Staffing
Te Ara Whakawaiora: Mental Health and Alcohol & Other Drugs
Allison Stevenson
CHAIR’S REPORT
• The Chair advised the following retirements, with a letter being sent conveying the Board’s best
wishes and thanks for their extended years of devoted service.
Years of
Name
Role
Service
Service
Retired
Forbes Bennett
Intensivist
Acute & Medical
38
20-Jun-16
Pamela Walker
Medical Typist
Facilities & Operational Support
14
30-Jun-16
• John McKeefry’s GM Human Resources resignation was acknowledged (effective end of
August 2016). The Board thanked John sincerely for his contribution over the past seven
years and wished him well for the future.
• Liz Stockley GM Primary Care and CEO of Health HB, had tendered her resignation earlier
in July, effective at the end of October 2016.
• Congratulations were extended to Jacoby Poulain on the birth of her son during the month.
• During the month the Minister of Health advised the free flu vaccine would be extended for a
further month.
Page 2 of 5
• The Minister had endorsed the Central Region’s Regional Service Plan for 2016/17, advising
he planned to strengthen the role of RSPs in future.
• The National Health IT Board were disbanded and the MoH have replaced them with a new
“Digital Advisory Board”.
CHIEF EXECUTIVE OFFICER’S REPORT
The CEO provided an overview of his report which included the end of year performance targets and
advised the financial unaudited result was better than planned. At this stage HBDHB were a
standout financially, on a population basis.
The Regional Economic Strategy had been launched that morning with ministers in attendance.
There had been a number of announcements regarding investments to support infrastructure. The
detail will be brought to the Board in August, noting we have an important part to play going forward.
Presently in the process of securing consultation on the social inclusion strategy.
FINANCIAL PERFORMANCE REPORT
The Financial Report for June 2016, showed a favourable variance of $266 thousand for the month,
with a year end result of $376 thousand favourable with all contingencies used. This was a
provisional, unaudited figure.
Technical adjustments (also made by the rest of the region’s DHBs) included: reducing RHIP costs
to capital operating costs by $687 thousand; anticipating raised capital definition to $2m which
resulted in a number of assets being fully depreciated, and increased operating costs by $448
thousand. The savings programme came in at 85% $8.7m of the $10.2m target. IDFs remain work
in progress, with Capital spend behind plan by $4.2m.
The Board expressed thanks to the team and staff for achieving the financial result to date.
NATIONAL PATIENT EXPERIENCE SURVEY RESULTS 2015-16
Kate Coley provided an overview of the presentation provided.
In summary:
Only a 21% response rate was received with a slight increase in Maori respondents (50 people, 15%
- compared to 38 people, 11% last year) and youth 15–24 years (7.6%) (last year 4.8%).
We scored positively across all four domains (communication, coordination, partnership and
physical and emotional needs). In several areas we tracked higher than the NZ average. During
the survey we captured 503 positive words and 140 negative.
The plan now is to undertake a “local experience survey” and develop a “quarterly quality
dashboard” to enable us to identify themes, trends and improvements made.
REPORT FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
Council supported the following at their 13 July Meeting:
• The purpose and principles paper and business case for the establishment of Health & Social
Care networks.
• The implementation plan for Clinical Governance Committees Structure
• The development of a position statement on reducing alcohol related harm.
• Ongoing work of the last days of life care planning
• The principles of the Transform & Sustain refresh and next steps.
Page 3 of 5
Dr John Gommans attended on behalf of the co-chairs and specifically mentioned Health and Social
Care Networks and Council’s support for Executive Management Team’s recommendation to move
forward with Wairoa and Central HB in the first instance.
John advised he was now on leave for several months which included Council’s AGM being held in
August.
Hawke’s Bay Health Consumer Council
Council supported the following at their 14 July 2016 meeting:
• The purpose and principles paper and business case for the establishment of Health &
Social Care networks. Come such a long way and he felt consumers had been heard.
• The development of a position statement on reducing alcohol related harm.
• The principles of the Transform & Sustain Refresh but with some strong recommendations
around integration of the 6 priorities.
In summary the Consumer Chair noted:
• Consumer members on steering groups still sense and experience siloed behaviours. The
need to ensure a joint approach will ensure the goal of an integrated whole is achieved.
• Feel it is important to focus on what else is occurring out there (locally and nationally) and
not try to reinvent the wheel.
• Suggested the Health Awards be “alcohol free” in support of Iwi who have made similar
decisions around their functions and gatherings.
Māori Relationship Board (MRB)
Heather Skipworth (Acting Chair) provided an overview of their meeting held on 13 July 2016:
MRB wish to understand fluoridation prior to legislation being passed.
The workforce target: MRB are taking a leading role and solutions are being worked through that
can make significant improvements.
Heat Tool is not applied across all papers provided to MRB. Presently the tool is being piloted and
will come to MRB for endorsement shortly.
The Chair sought feedback from board members at the table who were part of MRB.
Board members responded positively about the value of MRB and that they felt much better informed
and aware of Maori health issues, as a result of participating in discussions of MRB.
FOR DISCUSSION / DECISION
TRANSFORM & SUSTAIN REFRESH
Tim Evans (GM PIF) spoke to the report provided.
We are presently half way through a five year programme and need to ensure we have the capacity
and focus on the right areas. The priorities list had been reaffirmed as well as focus on prior lessons
learned. Kate Rawstron the new Project Office Manager had provided advice and guidance which
had been taken on board.
PRESENTATION
UNDER 19 MENTAL HEALTH WAIT TARGET (0 to 19 year olds)
Allison Stevenson (Service Director) and Dr Simon Shaw spoke to the presentation they provided.
The paper related to target PP8 – The percentage of 0-19 year olds referred for non-urgent mental
health or addiction services seen within 3 weeks (by a mental health service provider), 0 to 19 years.
Page 4 of 5
This target had not been achieved (trending at around 60% of the 80% target). This resulted in a
review of the service and within a three week period, the target had lifted to 96% of the 80% target.
Action:
Several board members felt there may be unidentified and unmet mental health
needs within the community for those under 19 years of age. Denise and
Heather to provide [email address] with detail.
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
RESOLUTION TO EXCLUDE THE PUBLIC
RESOLUTION
That the Board
Exclude the public from the following items:
17.
Confirmation of Minutes of Board Meeting
- Public Excluded
18.
Matters Arising from the Minutes of Board Meeting - nil
- Public Excluded
19.
Board Approval of Actions exceeding limits delegated by CEO - nil
20.
Chair’s Report
Reports and Recommendations from Committee Chairs
21.
Finance Risk and Audit Committee Report
22.
HB Clinical Council
Moved:
Helen Francis
Seconded:
Diana Kirton
Carried
The public section of the Board Meeting closed 2.30 pm
Signed:
Chair
Date:
Page 5 of 5
Document Outline