MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 25 FEBRUARY 2015, IN THE TE WAIORA ROOM,
DHBADMINISTRATIONBUILDING, MCLEOD STREET, HASTINGS
AT 1.06 PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana
Dan Druzianic
Peter Dunkerley
Diana Kirton
Helen Francis
Andrew Blair
Jacoby Poulain
Denise Eaglesome
Barbara Arnott
Apologies:
Heather Skipworth
In Attendance:
Chief Executive Officer
Members of the Executive Management Team
Chris McKenna and John Gommans (Co-Chairs HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council)
Members of the public
Media
Minutes
Brenda Crene
KARAKIA
Ngahiwi Tomoana opened the meeting with a Karakia.
DEPUTATION
The Chair welcomed Thomas O’Neill (Food Workers Union) and Linda Mitchell who provided
a deputation to the Board around proposed changes to the provision of food within DHBs
nationally. They were supported by staff from HBDHB Nutrition and Food Service.
Following the presentation and hand-out provided, the Chair thanked the presenter and
supporters, advising the Board had their first discussion on the HBL Food Business Case
earlier in the day. He acknowledged staff had received very little information to date.
The Board would value engagement with staff and stakeholders. A copy of the “business
case” will be provided with the commercially sensitive aspects removed. This will allow
HBDHB staff to familiarise themselves with the detail and allow for a six week period of
consultation.
What is proposed is a national model, and HBDHB will take steps to refine the model to
ensure impact on our organisation is minimised, in particular the area affecting staff.
There were four things to consider:
1. Impact of our own staff.
2 Do not want a national solution to impact on the quality of meals
3 Concerned to make sure that local producers are considered, as Hawke’s Bay is a food
producing province.
4 Must be cost effective.
February 2015
Section 1
1
Action:
Management to prepare a shortened version of the Business Case for
distribution to staff and other stakeholders and ensure a six week
consultation process is put in place. The Board will further discuss
once this process has been completed.
BOARD MEETING RESUMES
The Chair advised of Heather Skipworth’s apology for the meeting.
DECLARATIONS OF INTEREST
One change was noted to the Interest Register by Diana Kirton with no interests advised in
any of the items to be discussed on the day’s agenda.
The Interests register would be updated removing Diana as a member of the Hawke’s Bay
Medical Research Foundation.
Action
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 17 December 2015, were confirmed as a correct
record of the meeting.
Moved:
Barbara Arnott
Seconded:
Peter Dunkerley
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
All actions 1-4 had been actioned.
BOARD WORK PLAN
The Board Work Plan for March 2015 was noted, including the Workshop scheduled for
Wednesday 4 March.
The farewell for Warrick on the evening of 15th March for Board members and partners was
noted.
Board Evaluation detail would be issued the week commencing 2 March. To ensure timelines
are met, this section would take two weeks. It was important to be timely with this
information to ensure the evaluation report would be available for 25 March (11.00am)
The HB Health Sector Leadership Forum has been moved to 22nd April.
CHAIR’S REPORT
There were five retirements acknowledged with letters being issued from the Chair
acknowledging years of high quality service to the community of Hawke’s Bay.
Years Service
Helanie Pocknall
Registered Nurse
Surgical
21
Susan Marshall
Call Centre Operator
Planning Informatics & Finance
21
Rata Maxwell
Cook
Oral Rural & Community
12
Catherine Williams
Registered Nurse
Acute & Medical
18
Public Health Medicine
Dr Lester Calder
Specialist
Population Health
11
• The letter of expectation dated 17 December 2014, had been received from the Minister
of Health Johnathon Coleman. Key points noted were: fiscal discipline in management;
strong clinical leadership and engagement; greater integration between primary and
secondary care being vital. Also the National Health Targets require continued focus as
well as efforts focusing on morbidity and continued physical activity to keep communities
healthy. The Minister wants to see the NZ Health Strategy refreshed.
2
• A letter dated 17 December had been received from the Minister requesting information
on Family Violence and Sexual Violence Services and Activities. Work was underway to
provide a stocktake of government funded services that respond in Hawke’s Bay which
includes: core services; business as usual; funding or contracted services and internal
programmes.
• A further letter from the Minister dated 12 February 2015, provided ministerial consent and
approval to enter into a cooperative arrangement and borrowing facility. This was a
technical requirement to progress health shared services, specifically the National
Infrastructure Platform should DHBs resolve to do so.
• A letter dated 10 February 2015 had been received from the Ministry of Health around
Mental health and addiction non-governmental organisations (NGOs) “Fair Funding”
campaign, informing DHBs of the next steps. HBDHB had responded 12 months ago to
concerns raised by the Trust at the time.
• An email dated 10 February, had been received from Audit New Zealand advising Chrissie
Murray had been appointed as Auditor of HBDHB. Chrissie would be invited to attend the
FRAC and Board meetings on 25 March 2015
(Action).
• The Governor General of NZ had accepted an invitation to unveil the new naming stone
of Hawke’s Bay Fallen Soldiers’ Memorial Hospital on June 11th. Chair Kevin Atkinson
would not be available this day and Ngahiwi Tomoana as Deputy Chair would attend in
his absence.
• Quarter Two Health Target 2014/15 results published by the Ministry comparing all DHBs and
PHOs were summarised:
Hospital:
Shorter stays in hospital Emergency Departments HB 17/20 nationally; Improved access to
Elective Surgery 16/20 ( Note: HBDHB has delivered 100% of YTD contracted volume); Faster
Cancer Treatment 14/20; Increased Immunisation 1st/20; Better Help for Smokers to Quit 5/20
and More Heart and Diabetes to Quit 12/20.
Reports this calendar year show a dramatic improvement in elective surgery and ED shorter
stays are significantly better.
The
PHO continues to perform well with Increased Immunisation HB PHO at 9/36 compared
with PHOs nationally; Better Help for Smokers to Quit 11/36; and More Heart and Diabetes
Checks at 19/36.
CHIEF EXECUTIVE OFFICER’S REPORT
The CEO welcomed Rika Hentschel (of Women Child & Youth Services) who had been
appointed as Acting Chief Operating Officer (COO) for two months.
Appointment of the new COO, Sharon Mason (of Southern DHB) was announced recently and
would take up her role in the latter part of April around the same time Andrew Phillips
commences as Director of Allied Health. Both would be in attendance at the April Board
meeting.
The AIM 24/7 project is working as intended; good progress with elective surgery targets and
comfortable we will achieve to plan.
The Length of stay in hospital has been dropping. Asked whether there had been any concerns
regarding quality of care as a result of this rationalisation? A paper to FRAC provided no signal
of adverse consequences. Patients like to move on quickly from Hospital and positive impacts
on both patients and staff have been observed. There appeared to be no impact on providers
due to the higher focus on discharges?
The AIM 24/7 project is half way through and presently focused on the front door of the hospital.
Faster Cancer streams: it was a little early to determine this as a new target as we are still
coming to grips with reporting and ensuring data was comprehensive and accurate. However
moving forward we are confident of delivering this by July 2016.
3
Other areas include the solid financial performance; progress with Project Dane; the good work
being done on Te Ara Whakawaiora, working with the PHO, and Performance Framework with
a solid start to the calendar year.
The Deputy Chair noted the positive language used in reporting. We often see performance
drop during the transformational process, however we were now seeing an upturn.
Overall a positive financial and soundly based performance has been achieved.
FINANCIAL PERFORMANCE REPORT FOR MONTH OF JANUARY 2015
Tim Evans (GM of Planning, Infomatics and Finance) advised a favourable variance of $224
thousand for January, with a cumulative favourable year to date variance of $380 thousand.
This was achieved after restoring the contingency to $3 million by reversing the $250 thousand
used from the fund in December.
An overview of the report was provided with particular note made:
• We have experienced high personnel costs with case weight activity 21% higher than
planned.
• It was satisfying to see improved access to elective surgery with discharges above plan
for January, leaving us in a much improved position. Outsourced surgery was down as
were IDFs over which we have less control.
• More surgeons had been appointed recently and we are undertaking a review of all
surgical specialties.
• Financial flows around oncology were discussed. The relationship of funds flowing has
been uneven. Need to see a viable cancer centre at Mid Central but also need to rectify
imbalances and simplify the process, not chase payments.
The Countdown Kids Hospital Appeal was very successful with the Acting COO providing some
background to this national programme (between 10 DHBs), with resulting fundraising
successfully undertaken. As the appeal amount exceeded the $150k management delegation,
management sought the Boards approval to spend the $164,437 raised on clinical equipment.
FRAC had discussed this earlier in the day and recommended that the approval be given.
RESOLUTION
That the Board:
•
Approve the expenditure of $164,437 on clinical equipment from the Countdown Kids
Hospital Appeal special fund.
Moved
Dan Druzianic
Seconded
Ngahiwi Tomoana
Carried
REPORT AND RECOMMENDATIONS FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
Review of the Clinical Council Report from the meeting held on 11 February 2015 was provided
by Chris McKenna (co-Chair). In particular the following was noted:
• Keen oversight on electives programmes and had received a very positive presentation
from the COO and Service Director Becky Olson.
• Received an update on Palliative Care services and planning, progressing meetings and
approach.
• Council members were very engaged in the prioritisation process, a new experience for
many on Council who were now working with management in this area.
4
Hawke’s Bay Health Consumer Council
Graeme Norton, Chair of the Consumer Council tabled a report to the Board from the meeting
held on 12 February 2015.
A presentation on the Palliative Care Services was received. This resulted in plans to pull a
consumer reference group together for Palliative Care.
The project for Person and Whānau centred care had been discussed at their meeting recently.
It was surprising how closely this aligned with the Engaging Effectively with Maori courses
being provided to all HBDHB staff and others. Cultural competence courses such as this could
well be referred to as “Person and Whānau Centred Care”. This was all about effectively
engaging with people/patients.
Health literacy would be coming to Council in April as will the HBL food services business case
for consideration by both Consumer and Clinical Councils.
Consumer Stories to the Board were queried. This would be followed up.
Action.
Maori Relationship Board (MRB) meeting held 11 February 2015
In Heather Skipworth’s absence, as Acting Chair of MRB for the meeting, the following
feedback was summarised.
• There had been lengthy discussion on the survey tool around consumer experience from
cultural perspective.
• One quarter of the organisation had attended the Engaging Effectively with Maori course.
A review around the course delivery time(s) to enable staff to attend was being considered.
It was hoped Governance groups and committees commit to attend this Course.
• Bariatric Surgery - the bigger picture was conveyed by the CEO to MRB. A plan to address
obesity needs to be put in place. Caroline updated the Intersector Leadership Group on
equity which was endorsed by the group.
• Regarding Obesity all evidence points to children and even younger than school age being
the focus of healthy eating programmes. There has been a requirement in schools for
healthy eating which appears to have slipped
• MRB will hold a meeting on 19 March meeting to understand issues for Maori providers in
community. Denise Eaglesome asked whether Wairoa providers would be attending. This
would be checked and Denise advised accordingly
Action Tracee Te Huia
• Merging the Maori Health Plan with the Annual Plan was planned this year. It was
important not to dilute either but we now have mechanisms in place and feel confident this
can be achieved.
Will Ministry and the Maori directorate accept, may be up for debate but we are up for that
challenge. We are being watched by a number of organisations (as the leaders in this
area) and are sure we will are well placed to combine plans due to the performance
programmes set up.
Pasifika Health Leadership Group (PHLG)
Barbara Arnott conveyed detail from the PHLG meeting held on 16 February 2015.
There had been discussion about primary sector (PHO) representation on PHLG and also
around community engagement.
Tim Hutchins (contracted to the DHB) had shared some stories which highlighted his work in
providing services to the 5,000 plus Pacific community.
Central Region Pacific Collective: This Collective has a contract with the Ministry of Health
to service Wellington and the Central Region including Hawke’s Bay. The Collective supports
existing Pacific providers as well as non-Pacific providers who deliver services to the Pacific
5
population. A steering group that will govern this work is currently being established with the
Collective seek a representative from Hawke’s Bay. This is being considered by the PHLG.
Due to the size of the Pasifika population base in HB, there is uncertainty as to whether this is
a good option.
HBDHB do not reach benchmark for Pasifika in HB and felt there was a greater need for direct
funding for additional workforce navigator-type roles, as the Pacifica community is growing in
number with no win-win at present. Looking for something similar to Whānau Ora.
PHLG were pleased to be invited to attend Board Meetings in May and November 2015.
INFORMATION/DISCUSSION
Transform and Sustain Projects
Tim Evans provided an overview of the detail provided highlighting and acknowledging the
slow uptake of the Video Conferencing technology (explaining it had stalled). This area would
receive focus as staff and clinicians need to embrace this new avenue technologically to
provide health care.
Accountability Planning Update
Tim Evans and Paul Malan (Planning Manager) provided a presentation on planning
requirements for 2015. Presentation appended. A matrix was issued to provide an overview
of the aligning aspects of the plan.
MONITORING
Te Ara Whakawaiora / Diabetes – More Heart and Diabetes Checks
Liz Stockley (as Indicator Champion) supported by Victoria Speers, spoke to the report for the
“increased engagement of Maori with a primary care provider” specifically around more heat
and diabetes checks.
The report was taken as read, with discussion summarised including:
• There was general discussion and feedback around after hours services with only some
practices open.
It was noted Wairoa GPs did not offer after hours services and services were very limited
on a Saturday. A mobile nurse in the Wairoa Health Centre out of hours was seen as a
good option if advertised widely. This would be investigated –
Action.
• Attendance at practices in primary health care was at 80%.
Monitoring progress on uptake was explained as was the difficulties during a visit to have
many health requirement monitored (given limited time for both parties). Therefore specific
accessible clinics appears to be the best approach.
The Board were pleased to be advised of an excellent result for the Health Hawke’s Bay PHO,
who achieved top cervical screening for Maori in the country, being the first to achieve the
target of 80%.
Te Ara Whakawaiora / Diabetes – Smokefree
Dr Caroline McElnay (Director Population Health and Health Equity Champion), introduced
Shari Tidswell (Population Health Advisor).
Referring to page 78 of the report, targets were generally being met but there is a need to
embed performance and make an “impact on smoking rates” which is where the focus will
be.
Offering effective cessation is crucial. Tobacco control plan available.
6
• Ngahiwi Tomoana asked whether the same approach taken for DNAs (already in place)
should be utilised with antismoking campaign messaging and support included. More
aggressive work needs to be done in this area.
• What is offered at the moment was not working for young pregnant Māori women. Needs
to go wider as it is extremely difficult for the young especially to quit smoking in their home
environments, with cigarettes often supplied by their peers.
Performance Framework Exceptions (Quarter 2 October-December 2014)
Tim Evans provided a brief overview which focussed on the achievements, Areas of Progress
and Areas of Focus.
Human Resource KPIs Quarter 2 (Oct-Dec 2014)
John McKeefry (GM Human Resources)
An overview of the report was provided.
Staff turnover had risen slightly but was not of concern. For 12 months to 31 December 2014
HBDHB were the lowest out of the 6 mid-sized DHBs.
Accrued Annual Leave has been a challenge but is being proactively managed.
There was some general discussion around sick leave. Management were asked whether
there was monitoring and/or awareness of staff stress levels with all the changes occurring
within services. In response, staff surveys (fairly recently undertaken) had not highlighted a
problem and from a benchmark perspective HBDHB do not appear to be out of line with other
DHBs for sick leave.
Other sick leave areas discussed were around the ageing workforce, accrued sick leave
entitlements and sick leave taken due to a sick dependant (which is reported separately).
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public
Excluded.
RECOMMENDATION TO EXCLUDE THE PUBLIC
RESOLUTION
That the Board exclude the public from the following items:
22.
Confirmation of Minutes of Board Meeting dated 17 December 2014
- Public Excluded
23.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
24.
Board Approval of Actions exceeding limits delegated by CEO
25.
Chair’s Report
Reports and Recommendations from Committee Chairs
26.
Finance Risk and Audit Committee – 25 February 2015 (tabled)
Moved Helen Francis
Seconded
Peter Dunkerley
Carried
7
The public section of the Board Meeting closed 3.22pm
Signed:
Chair
Date:
8
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 25 MARCH 2015, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.12 PM
Present:
Kevin Atkinson (Chair)
Dan Druzianic
Peter Dunkerley
Diana Kirton
Helen Francis
Andrew Blair
Jacoby Poulain
Heather Skipworth
Barbara Arnott
Denise Eaglesome (by Video Conference)
Apologies:
Ngahiwi Tomoana
In Attendance:
Chief Executive Officer
Members of the Executive Management Team
Chris McKenna (Co-Chair HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council)
Chrissy Murray of Audit NZ
Members of the public
Media
Minutes
Brenda Crene
KARAKIA
Heather Skipworth opened the meeting with a Karakia.
DECLARATIONS OF INTEREST
Several changes were advised for the Interest Register:
Heather Skipworth advised that she was a member of a Trust that has been awarded a
Green Prescription contract by the HBDHB.
Diana Kirton advised her appointment to the HB Power Consumers Trust from October 2014.
No interest was advised in any of the items to be discussed on the day’s agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 25 February 2015, were confirmed as a correct
record of the meeting.
Moved:
Dan Druzianic
Seconded:
Barbara Arnott
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Actions 1 (Interest Register); 2 (Invitation) and 4 (Representation) had been actioned.
Action 3: Consumer Stories: The intention to share consumer stories with the Board
monthly would commence in May 2015.
Action 5 Out of hours cover for Wairoa – Liz Stockley to update in April.
April 2015
Section 1
1
BOARD WORK PLAN
The Board Work Plan for May through August 2015 was noted.
Action: Members noted a discussion on HBL would be held at the April Board
Meeting
A reminder to board members of the forthcoming HB Health Sector Leadership Forum being
held on Wednesday 22 April. The doors will open at the Napier Sailing Club at 8.30am with
the day commencing at 9.00am. HB Intersector Leadership Group members have been
invited to attend again this year.
CHAIR’S REPORT
There were no long service retirements to acknowledge since the previous Board Meeting.
The Chair expressed thanks to the management team and other staff for the enlightening
workshop and hospital tour held on 4 March.
Quarter 2 health targets from MoH had been received and HBDHB had performed well across
most of the indicators.
It was of concern to note that four of the six DHBs in the central region have changes in CEO’s
imminent or acting CEO’s in place.
The Chair attended a Grey Power meeting in March by invitation. As part of the address
statistics were provided to Grey Power highlighting that those over 75 are regularly the
recipients of hip and knee replacements. They found the statistics very helpful as many had
felt the opposite was occurring. Grey Power members accepted the need for those who did
not meet the threshold for surgery to be reviewed regularly by their GP, but raised a point that
these review costs were a barrier for many.
The Chair asked management (DHB/PHO) to take a look at options that may support those in
need with a voucher system suggested as an example (one per year).
Action:
Management of DHB/PHO to “look at” providing assistance to the elderly (or
those in need) on “HBDHB waiting lists for surgery” to attend a GP
appointment for a review. A response would be provided to the Board in due
course.
CHIEF EXECUTIVE OFFICER’S REPORT
Dr Kevin Snee provided an overview of his report and was pleased with target results for the
indicators measured. Service Performance in ED had largely been maintained as had Elective
Surgery.
PHO enrolment: gap between DHB funded population and PHO enrolled population was noted
with work being undertaken in this area. The question to be asked do we have the GP capacity
to provide a service to the unenrolled. The issue being availability in the right place at the right
time. This area was further discussed under the Te Ara Whakawaiora indicators.
FINANCIAL PERFORMANCE REPORT FOR MONTH OF FEBRUARY 2015
Tim Evans (GM of Planning, Infomatics and Finance), provided a brief overview of the report
for February advising a favourable variance of $41 thousand which increased the year to date
favourable variance to $421 thousand. The DHB remains in a strong position at this time with
the forecast remaining unchanged for the $3 million surplus projected in the budget.
2
REPORT AND RECOMMENDATIONS FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
Review of the Clinical Council Report from the meeting held on 11 March 2015 was provided
by Chris McKenna (co-Chair). In particular the following was noted:
Specimen labelling errors were discussed. Members were advised that intensive work was
being undertaken in this area. The majority of testing is in the low risk category with all DHBs
across NZ struggle in this area.
An overview of AIM 24/7 was provided to GPs followed by a tour of the hospital in early March.
The group were impressed about the improving patient flow and access to specialty advice
through AAU.
Hawke’s Bay Health Consumer Council
Graeme Norton, Chair of the Consumer Council tabled a report to the Board from the meeting
held on 12 March 2015.
In addition to the report Graeme advised workload was raised, and meetings with individual
consumer members are taking place. Through this process suggestions have been made
around doing things differently.
Particular note was made about Mental Health and Addiction Service DNAs and the need to
follow up on missed appointments within the service. There would be conversations around
the method of engagement as what is presently occurring is not necessarily reaching those in
need. The Acting COO had received detail and would follow this up with the service.
Maori Relationship Board (MRB) Workshop held 11 March 2015
In Ngahiwi Tomoana’s absence, Heather Skipworth provided feedback from the workshop held
with providers on Wednesday 11 March. It was felt this had been a very valuable exercise.
Feedback on the Te Ara Whakawaiora indicators were also received and noted, together with
comments from Consumer and Clinical Councils which have been fed back to the service(s).
Comments from MRB around cardiovascular targets were noted.
Leadership Forum Workshop Agenda
Ken Foote (Company Secretary) outlined the programme developed for the Forum being held
on 22 April 2015, and the endeavour to ensure elements of continuity with the focus on
inequity.
MONITORING
Te Ara Whakawaiora / Cardiovascular Disease
In Dr Gommans absence, Chris McKenna introduced Dr Keith Dyson (Cardiologist) to speak
to these indicators.
• National data collection has now been implemented in DHBs with many having difficulties
reaching the MoH target(s).
• Results are varied, there are constant turnover of Junior Doctors who have differences of
opinion on who should complete the data collection.
• Locally we are limited and only undertake diagnostics two mornings per week.
Although Wellington provides an excellent service, with the complexity of transfers we will
always struggle to meet the targets.
• Dr Dyson was on the Regional TAS Committee (in Wellington) and he can raise any issues
with the Wellington cardiologists from time to time. When there are breaches discussions
have historically been held between the respective Chief Operating Officers at the time.
3
• Interventional cardiology is not in “secondary centres” (like Hawke’s Bay), however there
is a realisation that this can be done safely, as is occurring in the UK. A coherent strategic
regional plan would be very helpful, including timing and how it fits in with the broader
regional model.
• Nelson as a province broke away and now have their own interventional cardiologists with
local access every day of the week.
• The cost to set up would be approximately $1.8m and would require a specific clinical skill
set. Through succession planning this may be considered but it would take time. This may
lend itself better to regional collaboration.
• There are private clinics doing interventional cardiology in main centres.
• There could be an opportunity to evaluate a Private/Public partnership.
• If interventional cardiology was DHB owned, private sessions may be undertaken on
Saturday mornings as income for the DHB (as is the case in Nelson). It was noted that
most are now doing “acute” cardiology, so private health insurance(s) may not cover
intervention.
Te Ara Whakawaiora / Culturally Competent Workforce
Chris McKenna (CNO) and John McKeefry (GM HR Services) were in attendance
It was very pleasing to note there had been 49% attendance to the Engaging Effectively with
Maori seminars.
A pleasing reduction in the gap of those employed in health, identifying themselves as Maori
was noted being down to 33 in February 2015. There was some discussion around placement
of Maori nurse graduates. Hawke’s Bay has the highest rating of the mid-sized DHBs in the
country for employment of Maori and much is attributed to the very good working relationship
between the DHB and EIT. Over 50% of students are Maori with many having been nurtured
through from school into a degree programme.
Low vacancy rates for roles in general practice (is a problem nationally), however that is offset
with a rise in aged residential care vacancies. Chris McKenna advised of the need to work with
the NGOs and rotate around public health nursing under supervision.
The report was well received.
Te Ara Whakawaiora / PHO Enrolment
Victoria Speers was in attendance for Liz Stockley (CEO Health Hawke’s Bay) Champion of
this target for Maori.
Following an overview there was further discussion around patients who were not enrolled with
a GP practice for varying reasons. It was generally agreed we may not have the GP capacity
in areas because we do not understand the distribution of those not enrolled. Victoria would
look into mapping this detail and cross reference with other methods, including census data
and provide feedback in due course.
Action.
FOR INFORMATION
WW1 Commemorative Event
Ken Foote (Company Secretary) advised the commemorative event timing had been aligned
to the Governor General’s availability to officiate on 11 June 2015. The programme includes
the reopening and rededication of the Chapel and renaming of the Hospital to “Hawke’s Bay
Fallen Soldiers’ Memorial Hospital”, and includes the unveiling of the foundation stone.
4
Health Literacy Information Paper
Ken Foote had provided the Board with some background information on Health Literacy. The
Alliance Leadership Team would consider a report the following week, prepared by their Focus
Group. The outcome would be advised with the Leadership team overseeing the development
of a programme going forward.
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public
Excluded.
RECOMMENDATION TO EXCLUDE THE PUBLIC
RESOLUTION
That the Board exclude the public from the following items:
18.
Confirmation of Minutes of Board Meeting dated 25 February 2015
- Public Excluded
19.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
20.
Board Approval of Actions exceeding limits delegated by CEO
21.
Chair’s Report
- HBL Transition
- Combined Board’s Symposium
22.
Annual Plan / Budget Update
Reports and Recommendations from Committee Chairs
22.
Finance Risk and Audit Committee – 25 March 2015 (tabled)
Moved Peter Dunkerley
Seconded
Diana Kirton
Carried
The public section of the Board Meeting closed 2.37pm
Signed:
Chair
Date:
5
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 29 APRIL 2015, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.08PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana
Dan Druzianic
Peter Dunkerley
Diana Kirton
Helen Francis
Andrew Blair
Jacoby Poulain
Heather Skipworth
Denise Eaglesome
Apologies:
Barbara Arnott
In Attendance:
Chief Executive Officer
Members of the Executive Management Team
John Gommans (Co-Chair HB Clinical Council)
Sharon Mason and Andrew Phillips (new to the executive team)
Graeme Norton (Chair, HB Health Consumer Council) arrived 2.30pm
Members of the public
Media
Minutes
Brenda Crene
KARAKIA
Ngahiwi opened the meeting with a Karakia.
A welcome was extended to Sharon Mason (Chief Operating Officer) and Andrew Phillips (Director of
Allied Health) who had recently joined the Executive Management Team (EMT).
DECLARATIONS OF INTEREST
A wording change was noted on the Interests Register for the Chair of Unison Networks Limited and
Trustees of HB Power Consumers Trust which hold all shares in Unison Networks Limited.
Action: The wording change would reflect “Unison has a lease agreement with HBDHB for a
generator which is located at Hawkes Bay Fallen Soldiers’ Memorial Hospital” and
would be incorporated on the Interest Register for Kevin Atkinson, Diana Kirton and
Helen Francis respectively.
No interest was advised in any of the items to be discussed on the day’s agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 25 March 2015, were confirmed as a correct record of the
meeting.
Moved:
Dan Druzianic
Seconded:
Andrew Blair
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Action 1: Consumer Stories will be heard at future board meetings and has been included on the
workplan. Remove action.
Action 2: Out of hours cover for Wairoa – Liz Stockley verbal update in April. As Liz was not present
the action was deferred until the May meeting.
Action 3: Interest Register changes completed – remove action
Action 4: Chair’s action from the Greypower meeting, ongoing.
Action 5: GP Capacity: Mapping unenrolled people in the wider community - ongoing.
BOARD WORK PLAN
The Board Work Plan for May noted.
Action: Board member apologies for future meetings will be noted on the workplan.
Apologies were advised for the following months:
August - Jacoby Poulain
September - Helen Francis and Denise Eaglesome
October - Helen Francis and Dan Druzianic
Board members would like more input into the workplan and would discuss/confirm topics outside the
meeting which would be relayed to management, ensuring there was adequate preparation time.
CHAIR’S REPORT
The Chair advised of the following retirements, with a letter being sent conveying the Board’s best
wishes and thanks for extended years of devoted service.
Years of
Name
Area
Service
Lesley Olsen
Older Persons & Mental Health
14
Patricia Orme
Acute & Medical
37
Lorraine Gregory
Facilities & Operational Support
19
Lynne Pinker
Oral Rural & Community
29
CHIEF EXECUTIVE OFFICER’S REPORT
Dr Kevin Snee provided an overview of his report including highlights of the shortest stays in ED
(currently 96%); improved access to elective surgery (confident to achieve with focussed planning);
faster cancer treatment (change in reporting requirements by MoH) an explanation of this change would
be provided to the Board in May. In short, HBDHB were doing better overall (65%), however the
recording area needs some focus.
Better help for smokers to quit resulted in the error mentioned last month being worked through.
Estimated at 89.52% shows an incredible effort has been made by the PHO in achieving this target.
The CEO was very pleased to see good representation by Intersector agencies at HB Health Sector
Leadership on 22nd April.
FINANCIAL PERFORMANCE REPORT FOR MONTH OF MARCH 2015
Tim Evans (GM of Planning, Informatics and Finance), was in attendance for the March report advising
an adverse variance of $218 thousand decreasing the year to date favourable variance to $203
thousand.
• Good activity and year end forecast
• There had been a valuation of hospital land and buildings undertaken (a standard requirement).
Seven years ago there was a plan to replace many of the buildings. This has progressed at a much
2
Minutes of HB District Health Board 29 April 2015
slower pace. The valuation of the assets saw a rise of $40m (a balance sheet item only). The DHB
would be disadvantaged by extra depreciation as a consequence. However this would be mostly
offset by extending the life of the assets.
• The
Mental Health building project report was positive in all areas
A NGO based recovery and respite care contract was developed by end of March, with Te
Taiwhenua seeking a five bed respite. The outcome of consultation with neighbours would be
known in May, and if successful acute services should be up and running in July.
Community resilience programs are occurring in Napier/Hastings
Acute Intensive program is happening on the current site.
Emergency mental health services are working in well with ED processes presently.
Recovery centres in the community are now focusing on more life skills based services and this is
proving successful. The change was initially hard for many clients and their families to accept but
due to good management, the new regime appears to be working well.
Action: A presentation on the Recovery Centres transition was requested by the Board in
4-5 months’ time, to provide comfort that what was planned is happening in the
community.
This would be included on the Board Workplan.
REPORT AND RECOMMENDATIONS FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
Dr Gommans as Co-Chair of Council highlighted several areas, including the HB Clinical Research
Committee who had recently issued their first Annual Report (available on the HBDHB website). The
Committee were comfortable with quality and governance of the research known about within Hawke’s
Bay; however there did appear to be research approved by other organisations which have health
implications, and there was a need to ensure appropriate processes were in place.
Clinical Council were supportive of the Patient Experience Strategy presented.
The HBL Food Services business case was not supported by Council as clinical quality of the food to
be provided could not be assured. There was not only a social impact there was also an environmental
impact of transporting the goods. Freeze heated food was not conducive with good health. It was
agreed an electronic food ordering system would be useful.
Hawke’s Bay Health Consumer Council
Pressures on consumer members to represent on varying pieces of work across the health sector was
reviewed by the Chair in one on one discussions with consumer council members. Feedback
highlighted suggestions for Council to operate differently going forward and that consumer engagement
should be part of ‘business as usual’ across the sector. Members generally wanted to focus on two or
three areas areas where they could make a difference and develop agendas which were more
conducive. Time would be taken to discuss and shape prior to taking this back to Council.
The Board noted the HBL food services business case (as presented) was not supported by
Consumer Council.
Māori Relationship Board (MRB)
Chair of MRB, Ngahiwi Tomoana provided an overview of areas of discussion including Health Equity
Update, HQSC Inpatient Experience Survey tool; Implementation of the Patient Experience Strategy;
Pipeline of Māori participating in the Incubator program at secondary school through to tertiary training
and the non-support of the HBL Food Services Summary Business Case.
Summary of comments and discussion follows:
• Better utilisation of service providers’ time with the co-design of new contracts was raised, with more
emphasis on time with whānau and less time on the paperwork.
• The Health Equity update highlighted health target outcomes for young pregnant Māori women
appeared to be getting worse.
• The HQSC inpatient experience survey tool (a national programme) had been discussed and
concerns were raised by MRB which would be relayed to the MoH by QIPS.
• Patient Experience Strategy Implementation recommendations were not endorsed by MRB who felt
this should be community owned not clinically generated.
• Work in the Incubator programme through secondary school to tertiary was discussed with renewed
focus on the barriers including keeping students in the science courses which are crucial when
taking a medical pathway.
• MRB did not support the HBL Food Services Summary Business Case presented. They did
however support the provision of Māori Kai on the hospital food menu. This was being raised with
the Nutrition and Food Services Manager.
HB Health Sector Leadership Forum held 22 April 2015
Good attendance overall with relevant topics, very real engagement and genuine intent to make a
difference. Attendance from the Intersector Leadership Group was appreciated however there was a
slight concern that representation from Clinical Council, MRB and the PHO was lower than expected.
Some positive feedback had been received regarding the Forum, its direction, value, willingness and
passion of the participants.
Action: It was agreed a survey would be provided to attendees to ascertain what they got out
of the day and comment on future formats.
A game changer will be “
health literacy” which Dan Druzianic felt needs to be whole of community
approach with input from the Intersector Leadership Group. Many do not get the concept of health
literacy. Denise Eaglesome suggested to involve the local Principals Association in this work as they
can drive change at grass roots level – they will have a chairperson and this would be the best group
to align with instead of the Ministry of Education (which is nationally driven).
DISCUSSION AND MONITORING
Annual Plan/Budget Update
A verbal update was provided by Paul Malan (Planning Manager) who advised on feedback received
from MoH on the HBDHB Annual Plan (including Māori Health Plan).
There would be discussion with the Ministry on structures around the required Alliance Leadership and
Service Alliance teams to ensure MoH understanding. Alignment with Transform and Sustain and the
inclusion of a visual with Health equity report has been included.
The process ahead will require HBDHB to submit amended sections to the reviewers for approval.
Once all areas are green or by 26 May, a second draft of the entire plan will be submitted to the National
Health Board. To ensure the most up to date version of the Plan was submitted to the Board for
consideration at the May Board Meeting, it was agreed this would be issued on the Friday prior, for
review over the weekend.
No changes had been advised around the Regional Services Plan however a late request to all DHBs
for a response to Hepatitis C to be included in the RSPs at a high level.
4
Minutes of HB District Health Board 29 April 2015
Health Equity Update
Dr Caroline McElnay was in attendance for the Board review of her report. The main focus of the
update was to get this out there and as a result many presentations have been made to the community
by request.
We now need to move on, identify priorities being the ones HBDHB/PHO can lead and drive to the next
stage with other priorities identified sitting with the Intersectoral Leadership Group.
Smoking: We are preparing a
Strategy on Tobacco which is an opportunity as nationally there is a
review being undertaken. The group identified little traction with young Māori women and this group will
be focused on locally.
Obesity: We are also preparing a
Strategy on Obesity which will go back to Intersector Leadership
Group as HBDHB/PHO cannot deal with this large issue. Youth do not buy most of the food that comes
into their homes. How do you deal with this becomes an area of education and health literacy. Activity
and becoming fit normally leads to better nutritional outcomes. Nutritional education at primary school
should focus on 5, 6 and 7 year olds. By High School patterns have often been formed and High school
students should receive a refresher on nutrition as they can likely influence parents purchasing and the
students go on to have families themselves.
Alcohol: Is an area with no lead identified and rests with the Intersector Group.
HBDHB identified five areas to lead: Smoking, Obesity, Heart Disease and Diabetes Management;
Primary care access and Monitoring.
At a local Government level, a model for an economic development strategy now includes
representation from the DHB as the biggest employer in Hawke’s Bay.
Annual Māori Health Plan Q2
Tracee TeHuia (GM Māori Health) provided a brief overview of the quarter two results and urged
everyone to continue to monitor Te Ara Whakawaiora targets to ensure progress.
Traction was being gained in the cervical screening area. Learning how we are linking in with the Māori
community to deliver the services and also co-designing services to ensure further traction is gained.
There will be a presentation on Screening in May.
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
RECOMMENDATION TO EXCLUDE THE PUBLIC
RESOLUTION
That the Board exclude the public from the following items:
18.
Confirmation of Minutes of Board Meeting dated 25 March 2015
- Public Excluded
19.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
20.
Board Approval of Actions exceeding limits delegated by CEO
21.
Chair’s Report
22.
Strategic Relationships Central Region DHBs
23.
Electronic Board and Committee Papers
Report and Recommendation from Committee Chair
24.
Finance Risk and Audit Committee – 29 April 2015 (tabled)
Moved Diana Helen
Seconded Peter Dunkerley
Carried
The public section of the Board Meeting closed 2.50.pm
Signed:
Chair
6
Minutes of HB District Health Board 29 April 2015
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 24 JUNE 2015, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.00PM
Present:
Kevin Atkinson (Chair)
Dan Druzianic
Peter Dunkerley
Diana Kirton
Barbara Arnott
Helen Francis
Jacoby Poulain
Heather Skipworth
Denise Eaglesome
Apologies:
Ngahiwi Tomoana and Andrew Blair
In Attendance:
Chief Executive Officer
Members of the Executive Management Team
John Gommans (Co-Chair HB Clinical Council)
Jill Lowry (Nurse Director)
Graeme Norton (Chair, HB Health Consumer Council)
Minutes
Brenda Crene
KARAKIA
Denise Eaglesome opened the meeting with a Karakia.
APOLOGIES
Ngahiwi Tomoana’s apology was noted and the board acknowledged the recent sad loss of his
mother, with sympathy expressed for the family. Andrew Blair was in the Chatham Islands
representing the Board in the hand back of the Chatham’s health services to Canterbury DHB to
administer.
INTEREST REGISTER
No changes to the Interest Register were advised and there were no board member interests advised
in any of the items to be discussed on the day’s agenda.
A
WELCOME was extended to Jill Lowry (Nurse Director) who was in attendance as acting for Chris
McKenna.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 27 May 2015, were confirmed as a correct record of the
meeting.
Moved:
Dan Druzianic
Seconded:
Peter Dunkerley
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Action 1: Te Ara Whakawaiora / More Heart and Diabetes Check: Following a suggestion a mobile
nurse be stationed at the Wairoa Health Centre out of hours. An alternative to this
suggestion was being progressed, according to the written response received from the
PHO included in the board papers. Remove Action.
Action 2: This action resulted from a Greypower meeting the Chair had attended:
Page 1 of 6
A scoping exercise to assess the costs of GP visits was underway including discussions
with the PHO on how such a scheme could be administered. A full proposal would be
worked up.
This was originally raised around surgery (hips and knees) for those over 65 years who are
regularly expected to regularly return to their GPs (for required reviews). The cost of GP
visits is high for retirees to bear, but is a requirement to remain within the system for
publically funded surgery. It was noted several options exist and this could be done
through other agencies eg, WINZ.
Action:
This item will be carried forward to the July meeting with the PHO and
Mary Wills addressing this on behalf of Tim Evans who will be on leave at
the time.
Action 3: GP Capacity to provide a service to the unenrolled.
Mapping unenrolled people in the wider community. The PHO can map at a high level (not
by location). Efforts will continue with a high focus on high needs through a number of
initiatives with general practice, ED, WINZ and MSD. This work remains ongoing –
therefore the action will be removed.
Action 4: Interest Register – completed – remove action.
Action 5: remains for August around the presentation of a follow up on Obesity - the next steps.
Action 6: Denise Eaglesome advised at a meeting held 9 June, that Wairoa District Council (WDC)
confirmed their support for “Fluoridisation”. Community consultation will follow with a need
to ensure the community are better informed.
Action:
Denise will ensure the Wairoa District Council respond officially to Dr
Caroline McElnay Director of Population Health (HBDHB) with clarity
around their expectations.
BOARD WORK PLAN
The Board Work Plan for July was noted, including the Combined Board Symposium in Masterton on
16-17 July.
CHAIR’S REPORT
The Chair advised the following retirements, with a letter being sent conveying the Board’s best wishes
and thanks for their extended years of devoted service.
Years of
Name
Job Title
Service
Service
Lynne Wall
Clinical Nurse Manager
Acute & Medical
20
Annette Wixon
Care Associate
Director of Nursing
15
In summary, the Chair mentioned the following:
• HB Helicopter Rescue Trust: At a recent meeting the rotation of trustees was discussed. Andy
Train would be retiring as Chairman and trustee. By consensus, following a recruitment process,
Robert Pattullo was appointed as a new trustee. Due to the high calibre of the applicants seeking
appointment to the Trust, there was a need to ensure their interest was retained and revisited in
the future. The Trust will nominate a Chairperson and, if they deem necessary could appoint an
outside Chair.
• A letter had been received from the Minister on the quarter three health targets, reflecting HBDHB
and the PHO had made considerable efforts and had delivered significant improvements.
• The Chair will be providing quarterly updates to the Minister on progress with the Mental Health
project.
Page 2 of 6
CHIEF EXECUTIVE OFFICER’S REPORT
Dr Kevin Snee provided an overview of his report. In addition to achieving targets HBDHB are financially
sustainable, remaining positive about achieving the $3.0m projected surplus.
Targets: The ‘Shorter Stays in the Emergency Department’ target will be reach 95% in June (being at
94% in May) this is reflective of the great work being undertaken within DHB services. Due to improved
access to Elective Surgery this year compared to last, we now have the flexibility to deal better with in
hospital patient flow. Better help for smokers to quit (within the Hospital) is on plan, with a Tobacco
Control plan being presented to the Board in July.
Appended to the CEOs report was a letter (addressed to Kevin Atkinson as Board Chair) from the Office
of Hon Dr Jonathan Coleman. This letter congratulated the HBDHB for the considerable efforts made
to deliver system improvements with the achievement of 5/6 health targets for the hospital, and 3/3
targets for the PHO. It was heartening to receive comments from the Ministry’s target champions for
quarter three, which were appended to the letter.
HBDHB said farewell to the Chatham Islands (on 24 June) with the handover of health services to
Canterbury DHB.
FINANCIAL PERFORMANCE REPORT
Tim Evans provided an overview of the May financial report for the 11th month of the financial year,
advising of an unfavourable variance of $130 thousand, decreasing the year to date favourable variance
to $42 thousand. The monthly review of the forecast has not changed the $3 million surplus projected
in the budget, however the forecast remains tight.
The Mental Health Unit is relatively on track and under budget considering there is a full redesign of
mental health services occurring simultaneously. Recruitment has been progressing for mental health
positions with only two remaining to be filled.
Accrued leave was raised and discussed at the FRAC meeting earlier in the day. Sharon Mason
advised annual leave planning would be refreshed as a regular item in health services meetings. It was
noted the issue has been acknowledged and there is a plan to manage.
REPORT FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
Dr Gommans as Co-Chair of Council highlighted several areas being:
The development Collaborative Clinical Pathways was progressing with the transition to business as
usual. A “Pilot” for the Diabetes Pathways would commence in four General Practices across HB in
the near future.
We must continue to ensure that we have the consumer perspective embedded in business as usual.
It is far too easy for clinicians to decide what best practices however partnering with consumers is
crucial to the successful implementation of Clinical Pathways.
Health Literacy framework development. It was acknowledge that several on council were concerned
consumers had not been included in the initial framework establishment phase.
Hawke’s Bay Health Consumer Council
Graeme Norton, Chair advised he had included the Consumer minutes for the Board’s information to
highlight the robust conversations and challenging meetings held with the goal being to move Consumer
Council forward, working in a way that differs from the present.
Council talks regularly about the need to put patients and whānau at the centre but sense there is a
long way to go yet. This is all about a culture shift and having clinicians and staff working very differently
and look through a different lens when it comes to patients/consumer.
This work has been placed within the Quality Improvement and Patient Safety area and the appointment
and with the new Consumer Services Manager being a pivotal role in achieving this. Council also needs
to take advantage of the new Director of Allied Health, Andy Phillips who has a wealth of experience in
co-creation and will also be pivotal to assist in changing ways/existing systems from within. The
Page 3 of 6
intention is there but at the shop floor engagement is often not occurring as well as we should be. A
very welcome addition is having Clinical and Consumer representatives attending each other’s
meetings.
It is evident that other DHBs are interested in viewing Hawke’s Bays Clinical and Consumer Council to
understand the structure and effectiveness of each.
Māori Relationship Board (MRB)
Board Member and member of MRB Denise Eaglesome provided brief summary of areas of interest
including: DNAs; Menus; the Incubator programme and Health Literacy – Framework Establishment.
It was noted MRB had endorsed the addition of a Health Literacy component to the DNA project to
enable Kaitakawaenga’s DNA the ability to educate and empower patients and their whānau about their
health and treatment, as well as navigate effortlessly through the health system.
“The Health Literacy – Framework Establishment” paper presented was managed through the HB
Health Alliance Team and therefore was not considered. This recommendation should be passed on to
the Focus Group/HB Health Alliance team for consideration when the Health Literacy Project is formed.
DISCUSSION
Suicide Prevention – Postvention Plan
Dr Caroline McElnay introduced Penny Thompson (Suicide Prevention Co-ordinator) who provided
insight and took questions from members on the detail presented:
• Where in the process are consumers and whānau involved, as it should be at all levels including
the governance level?
o Agreed this should be looked at. In hindsight the top tier did not have as much consultation.
It is included in the report but needs to be expressed in a clear and concise way.
• Typo noted re: Kai Piki Te Ora runs out of Te Kupenga … typo should read “
Incorporated”.
• The challenge is for those in need who are sent home with no follow up plan, subsequently commit
suicide and a week later a follow up letter arrives, referring to matters prior to the suicide occurring.
On discharge the Police expressed their concerned around no consistent/planned and timely follow
up. Communication between the services is an issue raised consistently.
o Plans are underway to improve the follow up process, including tighter communications with
Police.
• Maori response team – raised at Intersectoral group? Who is the local response team in Wairoa?
How will this work.
o WAGG and Intersectoral Group is work in progress.
o Intersectoral plans have been developed from scratch over an 18 month period. Presently
waiting for guidance through courts and inquests, and have asked the Coroner to review
systems in place in Hawke’s Bay. A response is expected in August.
o The good news is we have come a long way towards achieving our goal.
• A very proactive plan but always room for improvement.
• Feedback had been received from the Ministry of Health and had been incorporated into the Plan
presented to the Board. The document was close to what would be presented.
• A whānau member was quite receptive to assist in the suicide areas and provide insight into
prevention. Does this include victims and their families?
o A future intention. Some already have the youth component within their organisation. Like
to see that increased over time.
Board members supported the Plan and would welcomed follow-up and feedback when available.
MONITORING
Te Ara Whakawaiora – First Specialist Assessment Did Not Attend
Page 4 of 6
Sharon Mason, Chief Operating Officer introduced and welcomed Denal Meihana (Service Manager
Maori Health) and two Kaitakawaenga DNA staff to the meeting.
Significant work had been done in this area, and as “specialties” had increased, a dip in the success
rate had been noted, however that was now on the rise. A lot of focus will continue to be placed on
‘patient focused bookings’.
Sharon advised the DNA processes will be fully reviewed with a new sponsor and project manager
appointed. We do need to be careful when redesigning systems across services, so as not to redesign
the same system in a different way. This is the reason behind the appointment of a new team with a
new lens, to ensure it will be done differently and effectively. Present constraints need to be questioned
and reconsidered as well.
There are many and varying reasons why people are unable to attend their appointments with no
standard theme appearing. In summary comments included:
• Some consumers receive letters that contain too much information around their appointment,
being left confused. Others receive no information and have no idea why they need to go to a
hospital clinic, especially if they have waited for a long time.
• Some have a lack of understanding about their illness with no comprehension of urgency ie.,
health literacy.
• The content of letters sent to consumers, had been evaluated previously, however this needs
to be reviewed across all services/specialties.
• The hospital post through DX mail. If someone changes their address they more often than not
inform NZ post who do not advise DX mail. NZ post do not redirect DX mail.
•
Query around ethnicity categorisation and collation of statistics for DNAs?
In response there were three categories of ethnicity to identify yourself, if within one of those
categories an individual identifies as Maori they are then included in statistics as a “Maori” uf
the DNA. However, if they do not DNA they remain in their original first choice category which
may well not be Maori.
Action:
Ethnicity Categorisation and Collation of Statistics for DNAs, this method
could account for 20% or more DNAs for Maori and this needs to be
clarified.
The board were looking forward to further progress and thanked those present advising this work was
really valuable.
Consumer Story
The Consumer Story was the first of many to be relayed to improve patient experiences and learnings
where improvements can be made. The story had been shared with the team on how to improve the
service area/surroundings with some changes having already been made. Overload of information at
the outset of a patient’s visit, has been considered and changes made. Private versus public patient
processes were being looked at, as there appeared to be a problem in this instance.
The Chair advised that segregation of chemo patients was an issue 15 years ago.
It was conveyed this was work in progress with a need to systematically and pragmatically work through
what can practically be achieved. This includes a review of how we use our facilities, structuring use in
a different way and splitting services etc to take the clinical risk away from some susceptible patients.
This review could well include how many repeat patients are being seen that actually should be going
back to their GPs.
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
Page 5 of 6
RECOMMENDATION TO EXCLUDE THE PUBLIC
RECOMMENDATION
That the Board exclude the public from the following items:
17.
Confirmation of Minutes of Board Meeting dated 27 May 2015
- Public Excluded
18.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
19.
Board Approval of Actions exceeding limits delegated by CEO - Nil
20.
Chair’s Report
21.
Reports and Recommendations from Committee Chair(s)
- Finance Risk and Audit Committee – 24 June 2015 (tabled)
Carried
Th
e public section of the Board Meeting closed 2.50pm
Signed:
Chair
Date:
Page 6 of 6
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 27 MAY 2015, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.09PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana
Dan Druzianic
Peter Dunkerley
Diana Kirton
Barbara Arnott
Helen Francis (arrived at 1.30pm)
Andrew Blair
Jacoby Poulain
Heather Skipworth
Denise Eaglesome (by video conference)
Apologies:
-
In Attendance:
Chief Executive Officer
Members of the Executive Management Team
John Gommans (Co-Chair HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council)
Members of staff from Nutrition and Health Service for agenda item 11.
Media
Minutes
Brenda Crene
KARAKIA
Ngahiwi opened the meeting with a Karakia.
INTEREST REGISTER
Notification of two inclusions on the Interest Register were made for:
Action: Denise Eaglesome: Coordinator for a Health Contract, Wairoa College Rugby Academy.
Barbara Arnott:
Daughter, Danielle Everett is Commercial Manager Food for Health
Benefits Limited.
Due to the above interest being declared, Barbara Arnott would abstain from discussions/
decisions relating to Agenda Item 11, the Health Benefits Limited Food Services Proposal.
No other interest was advised in any of the items to be discussed on the day’s agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 29 April 2015, were confirmed as a correct record of the
meeting.
Moved:
Dan Druzianic
Seconded:
Peter Dunkerley
Carried
Page 1 of 8
MATTERS ARISING FROM PREVIOUS MINUTES
Action 1: Out of hours cover in Wairoa – ongoing.
Action 2: The Chair’s action from the Greypower meeting – ongoing.
Action 3: GP Capacity: Mapping unenrolled people in the wider community - ongoing.
The other items had been actioned.
BOARD WORK PLAN
The Board Work Plan for June was noted.
No board member advised of their absence for any Board meetings other than those already noted.
The Symposium in July had been confirmed with organisers and accommodation booked. Several
board members were unable to attend and two would be attending one day.
CHAIR’S REPORT
The Chair advised the following retirements, with a letter being sent conveying the Board’s best wishes
and thanks for their extended years of devoted service.
Years of
Name
Area
Service
Service
Aurelia Peterson
Clinical Nurse Specialist
Women Children & Youth
13
Robyn Price
Registered Nurse
Acute & Medical
19
Dianne James
Administration Coordinator
Oral Rural & Community
16
Project Facilitator Theatre
31
Joan Plowman
Productivity
Surgical
Other areas raised by the Chair included:
•
Special Commemoration Event on11 June 2015
The Chair reminded members of the special commemorative event on 11 June on the Hospital site
to rededicate the refurbished Chapel and formerly recognised the correct name of the Hospital as
the “Hawke’s Bay Fallen Soldiers’ Memorial Hospital”.
Detail of how the morning would unfold was advised which included the arrival of the Governor
General, officials, church leaders and invited guests for the memorial events.
Commemorative Gift to the Hawke’s Bay District Health Board
A large framed picture was gifted to the Board by Ken Foote (Company Secretary of HBDHB and
Brig [Rtd] ONZM, ED***). Ken and his family felt it fitting to dedicate the picture to mark this
commemorative event which represents NZ “fallen soldiers” over the past 100 years or so.
The Board thanked Ken and the Foote family for their very kind gesture and assured safe keeping
of the treasured picture which would be placed in a prominent position within the Hospital.
•
Encouraging target results for Hawke’s Bay
HBDHB were included in the Health and Disability report (over a 6 month period), recording the
least number of complaints nationally. On review it showed no systemic problem in any one service
area.
It was also very encouraging to receive the report “How is my DHB performing”, as Hawke’s Bay
met 5 out of the 6 target areas being one of three DHBs to do so. The area missed was faster
cancer treatment (a new indicator), mainly due to issues associated with data capture.
Hawke’s Bay was one of seven DHBs in NZ forecasting breakeven or better for the financial year
ended 30 June 2015.
The management team and staff were congratulated on the excellent results
Page 2 of 8
• The Chair advised also that the PHO achieved targets in every category despite the challenges
along the way. This was a significant result and congratulations were extended to the CEO of
Health Hawke’s Bay, Liz Stockley and her team. An overview of recent activity was provided.
CHIEF EXECUTIVE OFFICER’S REPORT
Dr Kevin Snee provided an overview of his report. In addition to achieving targets we are financially
sustainable (with $3m surplus projected) with the DHB being able to invest in services it has not been
able to in the past.
ED performance was at 95% for the quarter with the service responding much better to the changes
made; Elective surgery was at/or above plan and hopeful to achieve plan by year end; Faster Cancer
treatment (a new target) has some bedding down to do.
Other areas touched on included: Obesity; Cervical screening of Maori community; HR KPIs (with
improving representation of Māori in the health sector workforce); together with several Health Benefits
papers presented to the Board for consideration.
FINANCIAL PERFORMANCE REPORT
Tim Evans provided an overview of the April financial report advising a small unfavourable variance of
$33 thousand, decreasing the year to date favourable variance to $172 thousand.
The last of the Inter District Flows (IDFs) are below plan. There is comfort we will reach the elective
volumes and remain confident of achieving the planned surplus of $3.0m.
The cost reduction programme has gone well. Capital spend is $5.4m behind plan. Employee workforce
indicators show headcount above budget but are well controlled. Case weight discharges were above
budget in April however are close to plan overall.
There was a presentation to FRAC on the Mental Health unit. Not only are the DHB building a new
facility but also changing and transforming the mental health services in Hawke’s Bay which is great for
HB.
There has been continuing pressure on residential care and community support which has been partly
funded by additional income as we are investing in services to assist older people.
DECISION
National Infrastructure Platform (NIP)
Gina McEwen, Head of Information Services, was in attendance.
A national proposal has been developed to consolidate the DHB’s 40 data centres and associated
infrastructure technology into a lower cost NIP. This will provide a reliable, scalable platform for the
DHBs future IT requirements. DHBs need to do more for less while keeping pace with IT innovations.
Originally the costings for Hawke’s Bay DHB were too high, with little benefit in the timelines envisaged.
This has been reworked with the original proposition unchanged. What is on the table will see Hawke’s
Bay DHB in a favourable position, with long term benefits. We are talking significant infrastructure here
and changing into a model on data storage.
The Board thanked those involved in taking this to a workable reality. It was noted there were still
several DHBs to review the proposal, however the majority of DHBs are supporting this.
An additional clause was included in the recommendation provided, which delegated authority to the
CEO or nominee.
Page 3 of 8
RESOLUTION
That the Board
Approves the Health Benefits Limited (HBL) Detailed Business Case – National Infrastructure
Platform (NIP) Programme (version 2.0, dated 23 September 2014).
The Board approves delegation to the Chief Executive Officer (or nominee) authority to enter into
an agreement with Health Benefits Limited on behalf of Hawke’s Bay District Health board for the
provision of NIP services on a national basis.
Moved
Kevin Atkinson
Seconded Dan Druzianic
Carried
Health Benefits Limited Food Services Proposal
Barbara Arnott left the room prior to this discussion, as noted earlier under the “Interests Register”.
The Board, at its February meeting had endorsed wide ranging consultation on the Health Benefits
Limited (HBL) Food Services business case. A summary business case with a considerable amount of
supporting documentation was made available to stakeholders from 31 March 2015.
The Chair acknowledged that extensive consultation had occurred on this proposal. He acknowledged
the presence of staff from HBDHB’s Nutrition and Food Service as well as representatives from the
Service and Food Workers’ Union.
It was advised that the HB Clinical Council, HB Health Consumer Council and Māori Relationship Board
were unanimously unsupportive of the HBL proposal to outsource the food service (within the hospital
including meals on wheels).
The four key themes of concern emerging from Consultation included:
•
Concern expressed that outsourced services would lead to reduced quality, impact on patients
and concerns regarding the move away from cook fresh versus cook chill/cook freeze.
•
There will be limited benefits with no positive net present value benefits in the first three years.
The estimated $3.91m benefits over 15 years, leading to concerns that given the disruption and
change is not worth it.
•
Potential negative impact on local suppliers and local jobs.
•
Reduction of eight fulltime equivalent (FTE) roles.
In summary of general discussions the following was agreed:
• The Board did not support the Business Case as presented.
• Of the 6 recommendations put forward, the Board unanimously felt it could not support items 4, 5
and 6, around monitoring/cost benefit analysis following implementation by HBL of other DHBs who
sign up to the business case. Accordingly, items 4, 5 and 6 were removed from the resolution below.
• The final note included in the recommendation would remain and be amended to include the words
“internal review” ie, “HBDHB will undertake an internal review of its food services costings and food
service provision across the district including Wairoa and Central Hawke’s Bay”.
RESOLUTION
That the Board:
1.
Note the attached:
HBL Information paper (Appendix 1) and note as attached to the Information paper:
Page 4 of 8
a. Hawke’s Bay District Health Board (HBDHB) respondent summary table (
Appendix A)
b. HBDHB table of feedback and analysis (
Appendix B)
c. HBDHB table of feedback summary (
Appendix C)
2.
Note the feedback from MRB, Clinical and Consumer Councils does not support HBDHB
implementing the business case.
3. Do not support the implementation of the HBL Food Services business case at the HBDHB at this
time.
Note that HBDHB will undertake an internal review of its food services costings and food service
provision across the district including Wairoa and Central Hawke’s Bay.
Moved
Kevin Atkinson
Seconded Andrew Blair
Carried
REPORT FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
Dr Gommans as Co-Chair of Council highlighted several areas being:
• The development of Clinical Pathways has been and will continue to move forward, regardless of
the time taken by Medtech to resolve full software functionality. Although the quantum of pathways
produced is not high it will not be difficult to change routine pathways developed by others for
common conditions, localising them to build momentum. Transition of the Clinical Pathways Project
to business as usual is in progress with Council receiving a paper in June, including the formation
of a governance group to oversee the next step.
• The Urgent Care Alliance (UCA) is a sizeable Project which commenced at the beginning of 2015.
The UCA report directly to Clinical Council through their Chair, Graeme Norton. A very large
stakeholder reference group (of 30 people) is in place, is working and we look forward to seeing the
results of this collaborative approach to urgent care in Hawke’s Bay.
Hawke’s Bay Health Consumer Council
Graeme Norton, Chair handed out “Engaging with Consumers – HBDHB Stocktake” a snap shot of
consumer engagement across HB and putting people at the centre. This will assist Council to best
align and focus its efforts across the health sector.
Māori Relationship Board (MRB)
Chair of MRB, Ngahiwi Tomoana provided brief summary of areas of interest including:
• Ngahiwi acknowledge that across the DHB funding was well contained with real savings being
made, whilst at the same time it was heartening to see health targets for Maori continuing to
improve. It is great to see unfamiliar territories becoming the norm and that is a huge incentive for
the Maori Relationship Board members to see these improvement for Māori Health.
• Obesity is acknowledged and understood as a real issue for Maori, with a multitude of contributing
factors.
• A Mission Statement is what defines the DHB, however MRB feel an “action” Mission Statement
should be considered.
• Challenges with retaining Maori nurse enrolments for Bachelor of Nursing Studies was being
investigated as the attrition rate seemed to be high.
Page 5 of 8
• Did Not Attend title change was requested by MRB, as it implied an onus of blame on the individual.
This is being investigated by the GM Maori Health.
• It is very pleasing to hear the HBL Food proposal would not be implemented in Hawke’s Bay with
the MRB having been unanimously unsupportive of the proposal.
Pasifika Health Leadership Group (PHLG)
A warm welcome was extended to the Pasifika Leadership Group Chair, Caren Rangi, who
acknowledged Barbara Arnott as strong advocate for the group. Caren provided an overview since the
Group’s establishment in 2013. Caren advised it was pleasing to be successful with the funding bid for
Pasifika Health and keen to see this applied to assist Pasifika people to navigate through the health
system.
Pasifika Health has had some great examples of health successes in immunisation and breast
screening. It was noted they are not an add-on to Māori Health but PHLG were are very grateful for
the support of Maori Health to Talalelei’s role.
The ability to address the HBDHB Bard was important to the PHLG, and Caren thanked them for the
opportunity and would return again in November.
DISCUSSION
Annual Planning Update
A copy of the latest Annual Plan had been issued to board members on Friday 22nd May via email,
seeking comment prior to the Plan being submitted to the National Health Board on 26 May. There had
been no significant areas of concern raised in preparation of the plan.
This second draft review would be undertaken which would come back, or be advised by CTAS with
non-negotiable changes. Sign off of the Annual Plan and Regional Services Plan is expected by the
end of June 2015.
Planning Manager, Paul Malan was thanked for his efforts in putting the plan(s) together over past
years with a more simplified process in place now.
RESOLUTION
That the Board:
1. Endorse the 2nd DRAFT Annual Plan
2. Note the Annual Plan has been submitted to the National Health Board on 26 May 2015 as “not
yet board approved‟.
3. Approve the process for finalising the plan
4. Delegate authority to any two members of the Board to sign the Executive Summary and
Statement of Performance Expectations, as required by section 141(3) of the Crown Entities Act
2004
5. Delegate authority to Chairman of the Board and to the Chief Executive Officer to sign the Annual
Plan on behalf of Hawke’s Bay District Health Board as required in terms of section 9(2) of New
Zealand Public Health and Disability (Planning) Regulations 2011
Moved:
Kevin Atkinson
Seconded: Helen Francis
The Regional Services Plan was also endorsed by the Board.
Page 6 of 8
RESOLUTION
That the Board:
• Endorse the 2nd FINAL Regional Services Plan Draft
• Note the FINAL RSP Draft was submitted to the National Health Board on 26 May 2015 as “not
yet board approved”
• Approve finalisation process.
• Delegate authority to the Chairman of the Board and the Chief Executive to sign the final Plan
on behalf of Hawke’s Bay District Health Board.
Moved:
Kevin Atkinson
Seconded: Helen Francis
Transform and Sustain Projects Overview
The overview report was received.
MONITORING
Te Ara Whakawaiora Obesity Strategy
Dr Caroline McElnay and Shari Tidswell were in attendance advising an approach to curbing Obesity,
was this item placed on the agenda for the Intersector Group meeting on 22 June. It was acknowledged
that Health is only a part of the puzzle and only so much can be done to drive change from within the
health sector. The majority of focus needs to come from sectors within the community.
The Board supported the strategic direction outlined in the report including the recommendations from
the target champion on page(s) 4/222 with additional resource secured from the recent funding round.
Action:
Directional recommendations only had been received within the Obesity Strategy
document. The Board requested the group to come back in the very near future
and say what exactly will be done. (Caroline McElnay / Shari Tidswell)
From general discussions the following detail was summarised:
• Would like to see more focus on whānau and NGOs to work closely with Iron Maori. Activity and
healthy eating is infectious. Iron Maori come up with a plan? Have programmes in school and
prisons etc.
• Staff being motivated and enabled to do physical exercise is infectious to their wider families also.
This is where employers can help.
• It was noted Wairoa employers were being encouraged to provide gym memberships.
Te Ara Whakawaiora Ambulatory Sensitive Hospitalisations
Ambulatory sensitive hospitalisations are hospital admissions for conditions which could potentially be
prevented by early access to treatment in care.
Inequities in skin infections and dental conditions were higher than would be ideal, with Kohanga Reo
and public nursing assisting in this area. It was pleasing to see Rotavirus promoted in HB and been
promoted nationally.
Ngahiwi Tomoana was concerned at the slow uptake by Maori, particularly the younger age groups with
more traction needed in these areas. The CEO of Health HB, Liz Stockley advised that basing this work
within Iwi was working positively, instead of being driven by the PHO or DHB. Nevertheless there was
a need for focus to push this forward.
Page 7 of 8
Denise advised of the pending discussion/decision around fluoridation of the Wairoa water supply.
Board members indicated their support for fluoridisation.
HR KPIs Q3 (Jan-March 2015)
An overview of the quarterly report had been received with several points noted within the report by the
GM HR Services
Performance Framework Exceptions Q3
The performance report was received and performance highlights for Achievements; Areas of Progress
and Areas of Focus were noted (page(s) 5/ 250).
Taku Wahine Purotu – Screening Challenge This report was provided for the Board’s information, containing a description of a very successful
programme, especially from a communication and relationship building perspective. Page(s) 4/277
highlighted that Hawke’s Bay has made steady progress to close the equity gap showing the least
disparity of all twenty DHBs for cervical screening. An excellent result.
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
RECOMMENDATION TO EXCLUDE THE PUBLIC
RECOMMENDATION
That the Board exclude the public from the following items:
24.
Confirmation of Minutes of Board Meeting dated 29 April 2015
- Public Excluded
25.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
26.
Board Approval of Actions exceeding limits delegated by CEO (late paper)
27.
Chair’s Report
28.
Integrated Pathology Services
Report and Recommendation from Committee Chair
29.
Finance Risk and Audit Committee – 27 May 2015 (tabled)
Carried
Th
e public section of the Board Meeting closed 3.15pm
Signed:
Chair
Date:
Page 8 of 8
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 29 JULY 2015, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.00PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana (arrived at 2.30pm)
Dan Druzianic
Peter Dunkerley
Andrew Blair
Diana Kirton
Barbara Arnott
Helen Francis
Jacoby Poulain
Heather Skipworth
Denise Eaglesome
Apology
Nil
In Attendance:
Chief Executive Officer
Members of the Executive Management Team
John Gommans and Chris McKenna (Co-Chairs, HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council) arrived 2.15pm
Minutes
Brenda Crene
KARAKIA
Tracee Te Huia opened the meeting with a Karakia.
APOLOGIES
Several late.
INTEREST REGISTER
One change had been advised to change the Interest Register for Andrew Blair, effective 8 August
2015.
Action Brenda
Peter Dunkerley wanted to ensure Board members knew he had no involvement or interest in the
Pharmacy he once owned that it was being renamed as a Radius Pharmacy.
No board member advised interest in any of the items to be discussed on the day’s agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 24 June 2015, were confirmed as a correct record of the
meeting.
Moved:
Dan Druzianic
Seconded:
Barbara Arnott
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Action 1: This action resulted from a Greypower meeting the Chair had attended. A response has
been deferred until August.
Action 2: Obesity Strategy: the next steps will be revealed in August.
Action 3: Wairoa Fluoridation: In hand – remove action.
Action 4: DNA Ethnicity, the COO reported categorisation had been corrected, reducing the DNA
rates for Maori by 3.9%. Remove action.
Page 1 of 8
BOARD WORK PLAN
The Board Work Plan for August was noted including the Risk Management and Health and Safety
Workshop on 19th August.
Papers deferred from the August were: Stage 4 Renal Business Case (now September); Transform
and Sustain Health Promotion Plan (September) and the Community Pharmacy Services Position
paper (October).
CHAIR’S REPORT
The Chair advised the following retirement, a letter would be sent conveying the Board’s best wishes
and thanks to Sue for her extended years of devoted service, with the Board and Executive team in
particular acknowledging the high calibre of work produced.
Years of
Name
Job Title
Service
Service
Sue Ward
Portfolio Manager Referred Services
Planning Informatics and Finance
32
In summary, the Chair mentioned the following:
• Members of the HBDHB were nominated for a Pharmacy Guild Award (relating to their work with
the Clinical Facilitation Programme). The winner(s) of this Award will be announced in Auckland
on 8 September 2015. The group nominations include: Billy Allan, Anne Denton, Sue Ward and
other Health HB members.
• The Chair and CEO of Mid Central DHB will visit HBDHB on 9/10 September and attend the
Clinical and Consumer Council meetings during their visit.
There was strong interest at the Combined Boards Symposium (16/17 July) on HBDHBs
restructured committees and the move to a Clinical and Consumer Council model, in addition to a
reduced Board Governance structure.
• The MoH provided approval for the Maori Health Plan 15/16 with congratulations to Hawke’s Bay’s
outstanding rating in the SUDI section. Congratulations were extended by the Board to Tracee Te
Huia (GM Maori Health) and her team, for the excellent work done overall with the Plan achieving
the highest ranking nationally.
• Survey by Association of Salaried Medical Specialists (ASMS) placed HBDHB as top in the country
(with 57%) of professional individuals surveyed locally who felt HBDHB encouraged clinical
leadership.
There has been an incredible amount of work undertaken and Chief Medical Officer – Hospital, Dr
Gommans attributes a lot of this to the structure, medical and clinical leadership, including Allied
Health and sees all levels of the organisation from bottom up working together. DHB staff see us
“walking the talk”.
• Julie Patterson CEO of Whanganui District Health Board thanked HBDHB for loaning them the
dental health unit during their devastating flood.
CHIEF EXECUTIVE OFFICER’S REPORT
In recognition of Maori Language Week, the CEO opened as follows:
“E aku nui, aku rahi
Tēnā koutou, tēnā koutou, tēnā tātau katoa
E kore te tangata e pakari i runga i te waimarino
Ko taku toa, he toa takitini
Nā tō rourou, nā taku rourou
Ka ora te iwi
Tēnā koutou, tēnā koutou, tēnā tātau katoa”
Page 2 of 8
The CEO acknowledged EIT’s support to the DHB in learning Te Reo and stressed the need to
understand the language and culture to better understand the people we serve.
Dr Kevin Snee provided an overview of his report. He was particularly pleased with the unaudited
surplus of $3.054 million for the financial year ended June. This will be the fifth consecutive year with
Hawke’s Bay being the only DHB in country who have delivered surpluses five years running. This
allows planning with a greater degree of confidence to deliver improved services, with significant
investments having already been made.
The Waikato DHBs “
identity theft” matter recently reported in the media was discussed with the
board members seeking reassurance from the HR Manager around the processes in place at the
HBDHB:
Action
The Board were advised management had a high level of confidence with clinical
and non-clinical staff vetting processes, however an internal review would be
undertaken to ensure the system was robust considering this was a deliberate
identity theft attempt. This review would go to the Finance Risk and Audit
Committee.
Action:
In Primary Care, the CEO of Health Hawke’s Bay advised they do ensure that GPs
are registered, however she would ensure all GP Practice Managers are met with
individually to ensure sound employment vetting processes are in place.
Assistance will be provided to individual practices, if required.
The CEO touched on other areas covered in the report including: Consumer Story; Tobacco Control;
Te Ara Whakawaiora: Smoking; Tobacco Control Plan. Maori Annual Health Plan 2015-16.
FINANCIAL PERFORMANCE REPORT
Tim Evans (GM PIF) provided an overview of the June financial report for the 12th month of the financial
year, advising of a favourable variance of $12 thousand, with an unaudited projected surplus of $3.054
million for the year end. It was very satisfying to achieve the savings programme and also the elective
surgery target. Inter District Flows (IDF) outflow wash up for year-end remain outstanding.
The Chair of the Finance Risk and Audit Committee advised it had been another very pleasing year for
the HBDHB from a financial perspective.
The Board Chair congratulated management on this draft year end result.
REPORT FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
Dr Gommans as Co-Chair of Council highlighted several areas and mentioned the Tobacco Control
Plan and the Endoscopy Services presentation later in the day.
The fifth Annual HB Clinical Council Meeting would be held on 12 August which would include a
Workshop. Council has moved on from the inaugural structure and time will be set aside to review the
foundation documents to better reflect change to best meet clinical governance and community needs
going forward.
Hawke’s Bay Health Consumer Council
The Chair of Council, Graeme Norton provided an overview including: DNA/Patient Focused Bookings
and Council’s desire to ensure a very good model was incorporated throughout the system as best
practice; Tobacco Control Plan: looking forward being part of the co-design of services and wondered
whether there was an opportunity to understand what was working well from a future contract
perspective; Consumer Council had undertaken a Review with a draft plan prepared for the next 12
months. He indicated a closer working relationship with Clinical Council around person centred care,
jointly through leadership. Consumer Council now aligns with the new QIPS team and acknowledged
the support being provided by the new Consumer Engagement Manager now in place.
Page 3 of 8
Māori Relationship Board (MRB)
Helen Francis provided a brief overview of areas of interest including: Maori Health Plan Monitoring
Tool created by Dr George Gray; Programme Incubator support offered by MRB; Feedback on Tobacco
Control Plan and raised suicides in Flaxmere, and MRBs desire to make a difference through a
collective approach with a plan to workshop the topic in August.
Dr Gray provided accolades to Tracee Te Huia and her team for the excellent results achieve for Maori.
The tool he developed has been picked up by Primary Care as well.
The emergence of the Patient focussed bookings to curb DNAs was discussed and it was
acknowledged that health literacy forms part of the big picture in ensuring we have a robust system
developed across services to curb DNAs
The Board Chair felt when receiving MRB reports, that whilst the report is about actions, we may not
have been capturing these in discussions and consequently minuting them as actions. A review had
been undertaken recently around this with the only unquantified action relating to MRBs request for
governance member attendance at Cultural Perspectives Training ie, “Engaging Effectively with Maori”.
It was pleasing that 18 students were enrolled in Incubator Programme in Wairoa for 16 September at
Wairoa College. There were schools not offering science but HBDHB have been proactive in this area.
If this could be focused on further it would overcome the issues.
FOR DISCUSSION
Organisational Development - presentation
Kate Coley and John McKeefry jointly addressed the Board.
This programme has been in place for many years and is focused around culture, capability and
capacity within the health sector to ensure the right people are in the right places at the right time.
Key initiatives include talent management and a new transformational leadership programme as well
as others noted below:
• Where we are at:
Transform and Sustain launched in late 2013. Vision and Values already in place.
Organisational Development (OD) programme redeveloped to support Transform and Sustain
Culture is changing to patient centred, empowered bottom up team’s
Teams transforming to align to Vision and Transform and Sustain
AIM 24/7, Mental Health rebuild, Maternity review, Electives productivity, EngAGE – all examples of
Transform and Sustain culture change
ASMS survey – ranked HBDHB most positive in terms of distributed Clinical Leadership.
• Where we need to be to develop a culture centred on the patient and out staff:
Empower our Managers/Clinical leaders with their teams to develop their own outcomes aligned to Vision
and Transform & Sustain and deliver these outcomes – bottom up approach
Improve clinical participation in management and governance across Hawke’s Bay Health sector – being
leaders at all levels
Ensure clinicians are supported to providing high quality and safe patient care (from bedside to
boardroom)
Ensure Managers and Clinical Leaders have necessary time, skills (training) and support
Ensure all staff have time, skills (training) and leadership, support
Improve staff engagement to deliver Triple Aim outcomes
Have a healthy and safe work environment
Have an open, learning organisation
Live our Values
A copy of the presentation would be provided to members via Diligent.
Actioned
Page 4 of 8
Consumer Story
Kate Coley conveyed a consumer story, reading from a letter received from the wife of a patient
following multiple admissions to hospital. The gentleman had recently died. This letter presented
some positives and some negatives relating to the patients care and family needs, and raised the
issue of effective care for complex patients.
Hospital clinicians and staff have reflected on how and why they do what they do, highlighting that
things can be done better including better ward based management processes. This letter coincided
with work already in progress such as the need to have continual readmissions back to the “original
team”. It also highlighted the strength of the role that “Sarah” played focusing on the needs of the
patient and their family. This role has now been expanded to other wards with the question of how we
take this across services – especially for the complex needs patients. “Sarah” is in a sense up-skilling
ward staff. A system across Hospital and Community care needs to result as one of many initiatives
being looked at.
MONITORING
Te Ara Whakawaiora – Smoking
Dr Caroline McElnay and Shari Tidswell provided a brief overview of the detail provided advising the
work that will occur to increase performance of this indicator. It was noted considerable activity and
promotion of smoke free had been undertaken to get to this point - with the focus now being on primary
care and maternity.
The
Tobacco Strategy paper leads more into the activities which follows overlaps.
Surveys of the smoking amongst young people are used in future predications and there is concern
statistics were plateauing not decreasing. There is still a huge difference by ethnicity with smoking
commencing in adolescence. Young Maori women surveyed showed 60% had tried; and 30% were
regular smokers by age 15. In comparison, there were
very low smoking rates in young Pakeha
women of the same age.
We can learn by sharing knowledge with other DHBs but Hawke’s Bay needs its
own strategy which
pulls together local providers to get the shift to target specific issues. An operational plan had been
provided with the report which at the outset was acknowledged had a number of gaps. Filling those
gaps and putting them into a strategy for Hawke’s Bay was the next step.
Action:
The Board agreed a Tobacco Control Strategy was required and Dr McElnay
agreed this would come back to the Board in three months ie. October Board
Meeting.
Action:
The Board Agreed that the Tobacco Control Strategy be submitted as an agenda
item for the Intersectoral Forum, once it was complete.
A local Council has an online presence around Smokefree environments and the community are able
to make submissions through the following links:
http://www.napier.govt.nz/assets/Documents/smokefree-policy-june2015-draft.pdf
http://www.napier.govt.nz/our-council/consultations/have-your-say/draft-smokefree-policy/
HBDHB Annual Maori Health Plan Quarter 3 (Jan-March 2015) Dashboard
The areas of achievement; areas of progress and the challenges were noted by the Board.
Now looking at “exception” reporting for the 2015/16 year, as recommended by Dr George Gray.
The Te Ara Whakawaiora programme has been revitalised, seeking stronger recommendations to
accelerate improvements.
The trending tool provided/shared is and will continue to make a huge difference in understanding real
time information across DHBs nationally. Other DHBs are learning from Hawke’s Bay presently.
In referring to the Quarter 3 dashboard (provided) Hawke’s Bay has made fantastic progress being
the best performing DHB in NZ with the lowest disparity. Areas requiring focus include Diabetes and
Page 5 of 8
Oral health caries free, which is a high rate of admissions for young Maori children and very high
DNAs within Oral health services.
For Oral health, a number of known issues are being worked through including: model of care,
community hubs (also a non-Maori problem), patient centred booking system issues, health literacy.
It was noted by the GM Maori Health that there were gold standard systems in place in Hawke’s Bay
but people were not attached to them.
FOR DECISION
Maori Relationship Board member
Patrick Le Geyt recently resigned from the Maori Relationship Board (MRB). In accordance with the
Terms of Reference Ngati Kahungunu Iwi Inc (NKII) were requested to nominate a replacement. NKII
have advised that Ana Apatu is that nominee. It was recommended that the Board approves Ana’s
appointment.
RESOLUTION
That Ana Apatu be appointed to the Māori Relationship Board, to replace Patrick Le Geyt.
Moved
Helen Francis
Seconded
Denise Eaglesome
Carried
Improved Endoscopy Services
Sharon Mason (COO) presented members of the team involved in bringing the business case to the
Board: Paula Jones, Malenya Taylor, Tony McKee, Trent Fairey, Malcolm Arnold and Guy Vautier.
An overview conveyed endoscopy and gastroenterology services at HB Hospital were currently
managed very close to capacity and the service would find it impossible to cope with the additional
work arising from mandatory bowel screening.
The additional volumes anticipated over the next three years is
2015-2016
2016-2017
2017-2018
Short fall between outpatient clinics currently
being held and demand hours required
388
416
888
Converted into four hour clinic sessions
97
104
222
*2017-2018 includes 506 hrs of outpatient clinics (127 sessions) required as a consequence
of the bowel screening programme.
Shortfall between the current elective
endoscopy theatre sessions held and demand
hours required
146
190
586*
Converted into four hour sessions
37
48
147
*2017-2018 includes 380 hrs of endoscopy theatre time (95 sessions) required as a
consequence of the bowel screening programme.
Following extensive investigations and hard work by all concerned, the proposed case for approval
was presented. Summarised comments included:
• Have been optimising current theatre slots, already including Saturdays. It was noted the additional
MoH funding provided concluded on 30 June (from a one off incentive).
• Partner with Royston: It was noted there were implications through Health and Safety for the DHB
to lease space at Royston. However, Royston offered extra lists (utilising a DHB Doctor) and this
had been successfully trialled - with IT ensuring the information went into HBDHB information
system (which could occur in the interim during build).
Page 6 of 8
• Expanding the workforce by raising awareness amongst nurses to undertake relevant training is a
priority.
• The development of nurse training (50:50) within the Royston environment would be extremely
beneficial and needs to be investigated.
Action:
Agreed the CEO engage with the Acurity Executive nationally, to assist ongoing
local discussion to achieve a mutually acceptable outcome.
• Extending to Radiology, and CT scanning was discussed. It was agreed that CT colonoscopy was
more timely and safer, however there were risks of undetected issues which may become cancer
in future. Bowel cancer screening is crucial for early detection and once the MoH’s stance is known
we will evaluate how to provide that service. It was confirmed HB radiology have the capability to
undertake CT colonography also.
• Those who visited Endoscopy Auckland found the trip very valuable.
In response to a question “Are we over engineering sterile and clean environments; and mechanical air
pressure needs?” – the board were advised, the standards are mandatory when building a new
specialised facility.
Following general discussion the following Resolution was agreed.
RESOLUTION
That the Board:
1. Approve this business case subject to the financial discussion in the Public Excluded section
of this Board meeting.
2. Note previous Business Case approval pathway.
3. Note transitional arrangements to meet increasing demand and colonoscopy wait-time targets
for duration of construction and implementation phase. Request management provide the
Board with quarterly updates on the overall project, including any design or system changes.
4. Note
the private sector partnership approach.
5. Note
that in parallel, the development of options in partnering with a private provider via a
request for purchase (RFP) process will occur to utilise latent capacity in the third procedure
room.
6. Note that the Financials and commentary on the visit to Endoscopy Auckland are in the
Public Excluded section for commercial sensitivity reasons.
Moved
Helen Francis
Seconded
Diana Kirton
Carried
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
Page 7 of 8
RECOMMENDATION TO EXCLUDE THE PUBLIC
RECOMMENDATION
That the Board exclude the public from the following items:
21.
Improved Endoscopy Services – Commercial Financials
22.
Confirmation of Minutes of Board Meeting dated 24 June 2015
- Public Excluded
23.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
24.
Board Approval of Actions exceeding limits delegated by CEO
25.
Chair’s Report
26.
Reports and Recommendations from Committee Chair(s)
- Finance Risk and Audit Committee 29 July 2015
Carried
Th
e public section of the Board Meeting closed 3.50pm
Signed:
Chair
Date:
Page 8 of 8
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 26 AUGUST 2015, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.00PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana
Dan Druzianic
Peter Dunkerley
Andrew Blair
Diana Kirton
Barbara Arnott
Helen Francis
Heather Skipworth
Denise Eaglesome
Jacoby Poulain
Apologies
Nil
In Attendance:
Chief Executive Officer
Members of the Executive Management Team
Chris McKenna and John Gommans (Co-Chairs, HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council) arrived 2.15pm
Minutes
Brenda Crene
KARAKIA
Ngahiwi opened the meeting with a Karakia.
APOLOGIES
Nil
INTEREST REGISTER
No board member advised interest in any of the items to be discussed on the day’s agenda.
There was one change notified for the interest register. Heather Skipworth advised the Te
Timatanga Ararau Trust had been awarded a Green Prescription Contract signed earlier in the
year.
Actioned
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 29 July 2015, were confirmed as a correct record of the
meeting.
Moved:
Dan Druzianic
Seconded:
Barbara Arnott
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Action 1: This action from a Greypower resulted from a meeting the Chair had attended earlier in
the year. Advised this matter would be taken forward as part of the Orthopaedic Pathway
review. The PHO will contribute to how this may work, however it is dependent on the
Pathway redesign process. Remove action
Action 2: Implementation Obesity Strategy: the next steps will be provided to the Board in October
Page 1 of 6
Action 3: Internal reviews on staff vetting processes were underway within the health sector in HB.
Action removed, as this item has been included on the FRAC workplan.
Action 4: Tobacco Control Strategy will come to the Board in November. Remove action as this
has been included on the workplan.
Action 5: Improved Endoscopy – CEO engaging with Acurity executive nationally. The CEO will
report back on this meeting. Remove action.
BOARD WORK PLAN
The Board Work Plan for September was noted.
Helen Francis and Denise Eaglesome were confirmed as apologies for the September meeting.
CHAIR’S REPORT
There were no retirements advised for August 2015.
The Chair noted an endorsement was required for the appointment of a new HB Clinical Council
member, advising the CEOs of HBDHB and Health HB had approved the appointment of Dr David
Rodgers (as GP representative), replacing Dr Hannes Meyer on Council.
RESOLUTION
The Board endorsed the appointment of Dr David Rodgers as GP representative on Council,
replacing Dr Hannes Meyer who had retired by rotation.
Moved
Kevin Atkinson
Seconded
Helen Francis
Carried
In summary, the Chair noted the following:
• Performance HBDHB compared nationally for quarter 4 of 2014/15 was conveyed with Shorter
stays in ED at target of 95%; Improved access to Elective Surgery HB 102% vs 100% target;
Faster Cancer Treatment 67% vs target of 85% (a new target with a number of DHBs are
struggling with – have until June 2016 to reach
); Increased Immunisation –noting HB was
number one in the country with 96% vs target of 95%; Better help for smokers to Quit HB at
85% vs target of 90%; and More Heart and Diabetes Checks had reached the 90% target.
More focus to improve Better help for Smokers to Quit was advised, with more nurses utilised.
The CEO advised misleading positive results have not been not helpful with several DHBs
finding the same.
• A letter received from Ngati Kahungunu Iwi Inc, confirmed Heather Skipworth’s appointment as
interim chair of the Maori Relationship Board for the next 3-4 months.
• The Central Region Regional Services Plan 2015/16 had been signed off by the Minister.
CHIEF EXECUTIVE OFFICER’S REPORT
The CEO advised of a reasonably positive start to the financial year.
Issues highlighted in his report included:
• Shorter stays in ED – noting whilst still behind target, we are in a much better position than last
year. In July 2014 the hospital was in gridlock, a major incident process had been activated and
services were struggling to cope. AIM 24/7 has made a significant difference but still a lot to do.
• Elective surgery performance ahead of target.
Page 2 of 6
• Faster cancer treatments appear well below target. New definitions and identifying the right
number of cases causing issues for a lot of DHBs.
• Transform and Sustain projects generally progressing will. RHIP (CRISP), continues to be slow
but indications are that this will soon pick up.
FINANCIAL PERFORMANCE REPORT
Tim Evans (GM PIF) provided a financial overview for July, advising a favourable variance of $91
thousand.
Early indications are that health target expectations relating to volumes by specialty will place cost
pressures on surgical services this year. Surgical services budgets are being revisited, and options
for mitigating any issues arising from the likely changes to elective services funding are being
investigated.
Savings have mostly been phased evenly throughout the year, putting pressure on the first few
months, as savings plans are developed and implemented. This has created a shortfall in July,
however that shortfall has been offset by favourable variances in other areas including vacancies
and lower payments to other providers.
Comments summarised as follows:
• 115% in electives, Finance are concerned we are being over ambitious and this will have an
impact in finances.
• Terminology for elective surgery types is being widened.
• Technical question raised in FRAC from table on page 12 of the report regarding a significant
move in “crown equity and reserves” actual vs budget, related to a timing issue.
• The new mental health project continues on target.
• A query around Dental Health contracts in Wairoa? Advised these were for children, not adults.
• When will the end of year financial result for 2014/15 be finalised? Advised still awaiting the
MoH elective wash-up which does not have a deadline. We are holding $3.0m surplus as
almost certain but will not be in a position to confirm until the September meeting.
• The projected surplus for 2015/16 has been increased to $3.99m. This relates to a MoH
initiative providing an extra $25m to DHBs. HB do not intend to spend this extra funding in an
operational sense therefore will be in a position at financial year end (2016) to move this
increase in funding into capital investment.
In return for the additional funding MoH want three years of surpluses. This last minute gift from
treasury has high expectations attached and a letter was being prepared in response.
The following resolution writing off outstanding debt was approved.
RESOLUTION
That the Board
Approve the write-off of $31,366.73 of outstanding debt considered uncollectable as outlined
in the report.
Moved:
Peter Dunkerley
Seconded:
Dan Druzianic
Carried
REPORT FROM COMMITTEE CHAIRS
It was advised visits by Chairs and CEOs of various DHBs were planned on 9 and 10 September
and they would be attending both the Clinical and Consumer Council meetings.
Page 3 of 6
Action.
In preparation for the visitors, TORs, minutes and reports to the Board for the
prior two meetings of both Councils, would be provided.
Hawke’s Bay Clinical Council
Dr John Gommans commented on Council extended meeting held on 12 August 2015, as outlined
in the report to the Board. In summary: Preparation of the Quality Accounts were underway for
Board endorsement in December 2015; A joint meeting had been held between the Pilot Group
and the Clinical Pathways development group, with an operational group now being set up.
Clinical Council’s Annual general meeting took place following the ordinary meeting, with an
invitation extended to a wider group. This was a chance to reflect over the past five years of
Council (acknowledging the health sector was in a very different and positive place today) and
included a Workshop.
Action: An overview of Council’s Annual Meeting Workshop will be provided to the Board.
Good relationships are being formed between Clinical and Consumer Council, with a joint meeting
of the Councils being held in October.
With Dr Gommans involvement with Clinical Council since 2010, he had advised his intention to
step down as co-Chair of Council but would continue as a member, with the replacement Chair
being Dr Mark Peterson who would co-Chair alongside Chris McKenna.
The Board complimented John on his outstanding leadership over the five year period he had been
co-Chair of Council and the excellent service Council had provided to the Board.
Hawke’s Bay Health Consumer Council
Council Chair, Graeme Norton advised of the Consumer Council review was underway, including
the TOR which would come through to the Board in due course.
• A joint meeting between HB Health Consumer Council and HB Clinical Council is planned for
October which sends a strong collaborative signal to the health sector and community.
• A recruitment process for a representative on the HQSC Consumer Network resulted in several
Consumer Council members putting themselves forward for appointment.
• A suggestion to have the Consumer Story earlier in the Board Meeting was conveyed.
Graeme took the opportunity to thank Dr John Gommans (co-Chair) of HB Clinical Council for his
tireless efforts over past years. He advised that Consumer Council has been in place for two years
and it had been very helpful indeed to have John’s guidance during this formative time.
Māori Relationship Board (MRB)
Board members in attendance at the workshop on Suicide conveyed the Workshop had been
excellent with good actions/outcomes conveyed for review.
• The question is how do we improve and make this happen as there was no single answer, or a
right or wrong answer?
• It was acknowledged Suicide Prevention/Postvention needs more momentum and whanau
engagement in the process. There is nothing in the workplan referring to a Maori/Pasifika type
model?
• The MRB chair was asked to bring back more aspects for consideration as the community
wants things to happen.
Action: What funding is linked to this aspect of work for Suicide? CFO would investigate
and advise the connections.
Page 4 of 6
Alliance Leadership Team Meetings
Action: In future a summary on Alliance matters will be included in HBDHB Board reports.
Barbara Arnott as the HBDHB Board representative on the Alliance Leadership Team presented a
summary and generally updated the Board on the work of the Alliance.
FOR DISCUSSION
Consumer Story
Kate Coley provided two consumer stories relating to the Assessment Treatment and
Rehabilitation Ward (AT&R) in the hospital. Both stories were powerfully positive.
The Board were very grateful to receive such wonderful feedback about the service and asked to
have their sincere thanks and gratitude passed on to the AT&R ward.
Action:
a)
A letter of thanks from the Board to AT&R, will be prepared to be
signed off by the Chair.
b)
Letters also acknowledging the writers. Action Kate Coley
c)
In future Consumer Stories will be place higher on the Board agenda.
Action Brenda Crene
MONITORING
Performance Framework Exceptions Q4 Apr-Jun 2015
Tim Evans provided an overview of the report provided including: Performance Highlights;
Achievements; Areas of Progress and Areas of Focus.
A copy of the HBDHB Performance Framework Results Q4 was also included.
There was some discussion around performance relating to the Pacific population – noting that this
had more to do with the changing ‘numbers’ of our Pacific population. Despite this it was
acknowledged the Pacific population generally, do have issues accessing health services. Some
form of navigator service would help significantly.
It was also acknowledged that the Diabetes management target is unachievable and not
particularly relevant given it does not measure the difference, or the gains we have made, it just
measures against the target. The DHB should consider this as part of the annual performance
framework in future years.
Transform and Sustain Projects Overview
Tim Evans (GM Planning, Finance and Informatics) provided an overview of the diagram presented
giving a one glance view of where projects were using the traffic light system.
This can be cross referenced with a more detailed FRAC overview report.
Issues highlighted included:
• Limited project activity has been shown in area 2. Transform Patient Involvement (through
Consumer Council); 4. Transforming multiagency working through the Intersector Leadership
Forum and Intersector Leadership Group 11. Transforming Business Models through
interdistrict flow optimisation.
• Issue with Regional Health Informatics Programme (RHIP) – now under new management and
being led forward. Presently a review is underway to take this joint venture forward. Have high
hopes it will take reasonable shape in the near future.
• Area with some risk is in transforming Primary Health Care which may be reflecting the state we
are in at present.
Page 5 of 6
Human Resource KPIs Q4
John McKeefry GM Human Resources provided an overview of the report provided.
• Sick leave as at June was sitting at a similar level as for the previous year.
• Leading nationally across DHBs in the leave statistics.
Action:
The Board would like to see expectations and Plan over the next 12-24
months. With the report showing how we are achieving against this plan.
Effective from the next quarter report Q1 2015/16
Action:
Maori and non-Maori staff : Questions were posed as to how ethnicity is
counted where staff may identify with more than one, whether it is positions
that are counted or people, and generally how the process works. GM HR will
provide board members with a full explanation of this.
• New occupational and patient safety KPI to FRAC in future.
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
RECOMMENDATION TO EXCLUDE THE PUBLIC
RECOMMENDATION
That the Board exclude the public from the following items:
18.
Improved Endoscopy Services – Commercial Financials
19.
Confirmation of Minutes of Board Meeting dated 29 July 2015
- Public Excluded
20.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
21.
Board Approval of Actions exceeding limits delegated by CEO
22.
Chair’s Report
23.
Reports and Recommendations from Committee Chair(s)
- Finance Risk and Audit Committee 26 August 2015
Carried
Th
e public section of the Board Meeting closed 2 .50pm
Signed:
Chair
Date:
Page 6 of 6
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 28 OCTOBER 2015, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.05PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana
Peter Dunkerley
Andrew Blair
Diana Kirton
Barbara Arnott
Heather Skipworth
Jacoby Poulain
Denise Eaglesome
Apologies
Helen Francis and Dan Druzianic
In Attendance:
Kevin Snee (Chief Executive Officer)
Members of the Executive Management Team
Chris McKenna (Chair, HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council)
Members of the public and media
Minutes
Brenda Crene
KARAKIA
Ngahiwi opened the meeting with a Karakia.
APOLOGIES
As noted above.
INTEREST REGISTER
No changes to the Interest Register were notified and there were no Board interests declared in
any of the items on the agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 30 September 2015, were confirmed as a correct record
of the meeting.
Moved:
Ngahiwi Tomoana
Seconded:
Peter Dunkerley
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Action 1:
Implementation Obesity Strategy – As consultation detail needed to be collated, this
report would be presented to the Board in November 2015.
BOARD WORK PLAN
The Board Work Plan for November was noted with mention the Transform and Sustain Health
Promotion Plan had been removed.
Page 1 of 8
A reminder was conveyed regarding the forthcoming Health Awards function being held on 26
November.
CHAIR’S REPORT
• The Chair advised the following retirements, with a letter being sent conveying the Board’s best
wishes and thanks for their extended years of devoted service.
Years of
Name
Area
Service
Service
15
Joan Greaney
Service Coordinator
Older Persons & Mental Health
32
Joy Senior
Clinical Nurse Specialist
Oral Rural & Community
27
Oianah Ellsion
Manager Booking & Administration Support
Facilities & Operational Support
15
Patricia Sunley
Cook
Facilities & Operational Support
• Health Partnerships Limited newly appointed Chair had visited and spent time with HBDHB
Chair and senior managers. These meetings were positive and well received.
• Cranford Hospice had advised of the appointment of Janice Twyford Jones as their new CEO,
who would commence on 16 November 2015.
CHIEF EXECUTIVE OFFICER’S REPORT
On presenting this report matters highlighted included:
• Elective surgery was ahead of target at 104% compared with a target of 100%.
• The “Consumer Focussed Booking Project” was progressing well.
• Rheumatic Fever Plan had been requested by the MoH to provide assurance that HBDHB have
systems in place. A description of what HB does is not often expected in responses to the MoH,
however it was advised that Hawke’s Bay are leading the way nationally in managing/alleviating
Rheumatic Fever. To a large extent this is due to ‘Say Ahhh’ which is one of the best
programmes in the country. Even though Hawke’s Bay is classified as a high prevalence area
due to social and ethnicity factors, our figures are now aligned with a “low prevalence “area.
• The Maori Annual Health Plan dashboard tells a good story and we are seeing some significant
improvements in HB, including a drop in teenage pregnancy (from over 20% to around 10%).
The Chair acknowledged the Annual Māori Health Plan reflected exceptional results for Maori
health in Hawke’s Bay. It was very disappointing the media perspective was not balanced in a
recent article in HB Today (26 October 2015), entitled ‘
Stark inequality’ seen in Maori health’ and
‘
MP: DHB must support indigenous health drives’.
FINANCIAL PERFORMANCE REPORT
Matters highlighted by the CFO included:
• The result for September was unfavourable with an unfavourable result year to date of $289k.
2016/17 is anticipated to be a tight year financially with areas of turbulence, however the CFO
felt there was no need for any action to be taken at this time.
• Capital spend is ahead of plan, mainly due to a catch up for the mental health unit build which is
due for completion in January 2016.
• Presently the DHB is running more in-house theatre activity and relying less on outsourcing.
• The Financial Improvement Programme was tracking well.
Page 2 of 8
CONSUMER STORY
A consumer story on the experiences of a melanoma patient waiting for and receiving surgery was
shared. Areas of concern had been reviewed and recommendations discussed with service(s)
staff. A lot of work has been done to ensure processes are streamlined. It has been very beneficial
to utilise such consumer experiences to make service/.systems improvements.
The areas raised in the story were not about the service and manner of the people/staff, it was
more about systems/processes, delays and waste.
Feedback from Consumer and Clinical Council (mid-month) was not dissimilar to the Board.
The following
suggestion was noted:
• MRB patient stories are a little different from the stories heard at the Board. Suggested it would
be nice to bring some of MRB’s stories through to the Board, Clinical and Consumer Councils.
REPORT FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council and HB Health Consumer Council joint meeting
Chris McKenna and Graeme Norton as the respective chairs of the above meeting, provided an
update to the Board.
Both councils found the joint meeting very engaging and full of active conversations with the focus
on streamlining processes to improve the patient journey. Consumer members were complimented
for their vigour and questioning and Clinical Council enjoyed the robustness of discussions.
Contributions around the Rheumatic Fever paper was noted with a strong signal, especially from
Consumer Council that this was a social issue which could benefit from stronger consumer
engagement. It was understand the MoH had been quite prescriptive in their request in August,
however it was acknowledged there was a bigger picture.
The health sector workforce and skills were highlighted and briefly discussed.
Māori Relationship Board (MRB) - verbal
Acting Chair Heather Skipworth provided an update to the Board. Although no meeting had been
held during the month, papers had been reviewed by members. A report was tabled and had
been uploaded on to Diligent prior to the meeting for review. Of note was the DHB Maori health
profiles for 2015 and the endorsement of the Rheumatic Fever Prevention Plan issued to the MoH
on 20 October.
FOR DECISION
Committee Structure and Meeting Schedule for 2016
It was recommended the Board complete a review the Committee Structure and the draft meeting
schedule for 2016 provided. HBDHB has undergone some major changes in committee structures
over past years which appears to have bedded down. The board’s views on how the new structure
was working received favourable comments as summarised:
• Confirmed the present structure was very effective and helped support culture change.
• Leadership of Clinical and Consumer Council was commended as outstanding.
• It was noted the meeting schedule provided was consistent with 2015 and worked well.
RECOMMENDATION
That the Board
1. Confirm the current governance committee structures and processes
2. Approve the attached Meeting Schedule for 2016.
Adopted
Page 3 of 8
Matters raised for consideration/Action:
• Consider taking the duplication of papers out as meeting agendas are often full.
• Clinical and Consumer Council Chair will socialise combined meetings and timings.
• Consumer Council and MRB Chair will socialise combined sessions or more formally attending
each other’s meetings in future.
Central Technical Advisory Services Annual General Meeting
The Board received the Notice of Meeting, Minutes of the 2014 CTAS AGM and noted the Draft
Annual Report for the year ended 30 June 2015, and adopted the following recommendation:
RECOMMENDATION
That the Board
Appoint Kevin Atkinson as the HBDHB representative to attend the TAS Annual General Meeting
to be held Monday 7 December 2015, with another Board Member or the Kevin Snee appointed
as his Alternate.
Adopted
Action:
Advise CTAS of the outcome (Company Secretary)
Allied Laundry Ltd AGM
The Board received the Notice of Meeting for Allied Laundry and passed adopted the following
recommendation:
RECOMMENDATION
That the Board
•
Note the Chairman’s Report and the Financial Statements for Allied Laundry Services Ltd
(Allied) for the year ended 30 June 2015.
•
Appoint Ken Foote as the HBDHB Shareholder representative to attend the Allied Annual
General Meeting to be held on Tuesday 24 November 2015, with David Richie appointed as
his Alternate.
Adopted
Action:
Advise Allied of the outcome (Company Secretary)
The Chair of Allied Laundry, Ken Foote advised members that Hutt Valley and Capital and Coast
DHB were soon to become shareholders of Allied Laundry. A formal report will be issued to
shareholders’ in due course with a view to restructure of the company on 1 March 2016. This
would see Allied managing all linen requirements for six Central Region DHBs plus Taranaki DHB.
The Minister of Health had approved that Hutt Valley and Capital and Coast can buy shares.
Presently Allied were waiting for approval to borrow the funds necessary to purchase plant from
Germany.
Te Matau ā Māui Health Trust – Trustee Appointment
With background provided and the Trustee Appointment Schedule dated March 2016 made
available the Board adopted the following recommendation:
Page 4 of 8
RECOMMENDATION
That the Board
Re-appoint Leanne Hutt as the Central Hawke’s Bay resident trustee on Te Matau a Maui Health
Trust, for a three year term from March 2016
Adopted
Action:
Advise Te Matau a Maui Trust and Leanne Hutt of the outcome (Co-Sec)
FOR DISCUSSION
“Customer Focused Booking Project”
Sharon Mason (COO), introduced Carleine Receveur Senior Change Manager (and Project
Sponsor).
Did Not Attend appointment projects have received a lot focus in the past and the good work that
had preceded this was acknowledged. Success factors are to reduce Did Not Attends (those not
turning up for appointments); ensure full clinic utilisation; see a reduction in waiting times at the
appointment, and increasing customer satisfaction levels.
The Customer Focused Booking Project had been recently formed with the customer at the centre.
Hutt Valley DHB had been through a process several years earlier and shared their learnings with
HBDHB in mid-October which included their customer focused on-line booking system which they
had developed. This was shown to a significant group at the time and received robust discussion
from many perspectives.
Board members viewed a presentation of Hutt’s on-line booking system “UBOOK” with interest,
and it had been ascertained that the system could easily sit on HBDHB IS platform.
A very positive message was relayed to get this moving forward.
A business case will follow.
Refreshed Rheumatic Fever Prevention Plan
In Dr Caroline’s absence Katie Kennedy (Women, Children and Youth Portfolio) was introduced by
Kevin Snee. The plan had been produced by request for the MoH, not from within the DHB to
comprehensively address our needs! As noted earlier, Hawke’s Bays incidence or Rheumatic
Fever (RF) is that of a “low prevalence” area, due mainly to the success of the “Say Ahhh”
programme.
The Ministry are looking to withdraw funding when they see programmes nationally are working
which may be as early as June 2017.
In summary:
• It was noted Wairoa did not have high instances of RF.
• MRB feel confident with the programme going forward, however do seek consultation with Maori
on RF. A letter of support from MRB had been included with the report as Appendix 5.
• Through Community Awareness we will be informed and we move with that.
The Plan was submitted to the Ministry of Health on 20 October in draft form, subject to final DHB
Board endorsement on 28 October 2015.
RECOMMENDATION
That the Board
Endorse the Refreshed Rheumatic Fever Prevention Plan.
Adopted
Page 5 of 8
MONITORING
Te Ara Whakawaiora / Obesity Local Indicator 2015/16
Obesity is the second leading risk to health in New Zealand. Medium and long-term costs of not
addressing obesity are very high, as obesity leads to a range of diseases with high health sector
costs.
Shari Tidswell was in attendance for Dr Caroline McElnay and the report was taken as read, with
discussion summarised including:
• The target set by the MoH at 75% or greater for all four year olds recording a healthy weight.
Locally we have 25% of children at a healthy weight, however are missing those who were
under weight.
• The most influential focus to target the young is through gestation and breast feeding which
filters through, however this will take time.
• Good at engaging with communities, can we spread more than one message at one time? This
is about wellbeing and fits well with “Best Start in Life”. Those delivering the messages are
integrating and up skilling. We now have a more integrated approach on the ground.
• “Healthy Conversations” is being introduced to HB. This is about having wide ranging
motivational conversations that are meaningful to change behaviours.
• Kahungunu Hikoi Whenua family’s wellbeing who have a whanau health plan – there has
already been indicators and examples that address this. This is about a range of factors, not a
single symptom focus!
The following
suggestion was noted:
• This would be a good workshop topic for HB Health Consumer Council and the Maori
Relationship Board. It was also suggested as helpful to have those already delivering the
programmes involved.
Annual Māori Health Plan 2014/15 Dashboard for Q4
The Chair conveyed he was very disappointed about the recent Hawke’s Bay Today article as
Hawke’s Bay, from a health perspective for Maori, is leading the way nationally.
The GM Māori Health thanked the Board for their support for the focus which has enabled
improvements in Māori health in HB. From the work done by Dr Caroline McElnay, a good outcome
is now being seen in the gap in the quantity of life for Maori compared with non-Māori had
decreased.
HB are in a very good place with Iwi and Post Settlement Groups; and have an established
Memorandum of Understanding, whereas others around the country are struggling with iwi
relationships.
• Highlight that MRB focus has been on child health and access to primary care. 99% seen in HB
in schools programmes showing we have a good representation of children in HB accessing
services.
• Working with Kohanga Reo’s which had not been previously possible has changed and we are
now seeing the Kohanga children for checks.
• Rate of cervical screening best in the country but not as good with breast screening (ie, a
regional screening service into HB with location of the service being an issue).
• Positive progress is being made quarter by quarter.
• The targets have changed and HBDHB pushed to have no differentiation between Maori and
non-Maori.
• “Iron Māori” has changed family lives regarding health and nutrition. Alongside the health
programmes you must have health literacy, noted as being the biggest driver in deprivation!
Page 6 of 8
FOR INFORMATION
Mental Health Recovery Centre Transition - Presentation
Allison Stevenson and Dr Simon Shaw introduced Deborah Grace the Chairperson of the Mental
Health Partnership Advisory Group (PAG). With the rebuild of the mental health centre imminent in
2014, the model of care was also to be addressed for the unit and the community. In mid 2015
PAG was officially formed and what evolved from differences of opinion, led to positive outcomes
for all concerned. Once users were able to accept the community centres would close, the groups
focus was on what the future may look like and that became the turning point in this excellent
example of co-design that transpired. An extraordinarily positive outcome was achieved for all
concerned.
There were now two community centres, providing a different range of services and community
involvement (than before) which are successfully operating, in Napier “Manaia House” and in
Hastings “Te Puawaitanga”.
Annual Plan approvals
A letter from the Minister of Health was received on 25 September 2015, noting he had approved
and signed the HBDHB 2015/16 Annual Plan for three years. Incorporated in this approval was
the: Statement of Intent 2015-2019; Statement of Performance Expectations 2015/16; and the
Māori Health Plan 2015 (approved by the Director National Health Board and Deputy Director
General Māori Health on 13 July 2015).
The Board noted this approval and the provision of the final plans and reports.
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
Page 7 of 8
RESOLUTION TO EXCLUDE THE PUBLIC
RESOLUTION
That the Board exclude the public from the following items:
25.
Confirmation of Minutes of Board Meeting
- Public Excluded
26.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
27.
Board Approval of Actions exceeding limits delegated by CEO
28.
Chair’s Report
29.
Reports and Recommendations from Committee Chair(s)
- Finance Risk and Audit Committee (tabled)
30.
Strategic Relationships Central Region DHBs
Moved:
Diana Kirton
Seconded:
Barbara Arnott
Carried
The public section of the Board Meeting closed 3.35pm
Signed:
Chair
Date:
Page 8 of 8
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 30 SEPTEMBER 2015, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.00PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana
Dan Druzianic
Peter Dunkerley
Andrew Blair
Diana Kirton
Barbara Arnott
Heather Skipworth
Jacoby Poulain
Apologies
Helen Francis, Denise Eaglesome, Kevin Snee (CEO)
In Attendance:
Tim Evans (Acting Chief Executive Officer)
Members of the Executive Management Team
Chris McKenna and John Gommans (Co-Chairs, HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council) arrived at 2.15pm
Minutes
Annie Quinlivan
KARAKIA
Ngahiwi opened the meeting with a Karakia.
APOLOGIES
Tim Evans the Acting CEO advised that Kevin Snee was on leave, therefore he would be standing
in for him until 9 October 2015. In addition, Chris McKenna would be standing in for Sharon Mason
who was on sick leave, and Peter Kennedy would be Acting Chief Financial Officer.
INTEREST REGISTER
No board member advised interest in any of the items to be discussed on the day’s agenda.
Andrew Blair advised that he had recently been appointed by the Minister of Health as Chair of the
Southern Partnership Group. He had also been appointed as Advisor to the Hawke’s Bay
Orthopaedic Group Limited. Both of these appointments had been included on the Interest Register.
ANNOUNCEMENTS BY THE CHAIR
The Chair advised that it has just been announced that he had sold his business (IMS) to MYOB.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 26 August 2015, were confirmed as a correct record of
the meeting.
Moved:
Dan Druzianic
Seconded:
Barbara Arnott
Carried
Page 1 of 7
MATTERS ARISING FROM PREVIOUS MINUTES
Action 1:
MRB’s Suicide Workshop – Caroline McElnay advised that there is funding attached to
the Strategic Plan for this issue but as this was a new area of work for the organisation,
specific funding needed to be identified. Implications of having future workshops with
MRB support needed to be investigated but feedback from the community was that the
workshops were useful.
Action 2:
HR KPIs – Maori and non-Maori staff – GM HR advised the Board that any staff member
who identified themselves as Maori would be counted as Maori in the statistics. This
approach was consistent with the Ministry of Health Ethnicity Data protocol.
BOARD WORK PLAN
The Board Work Plan for October was noted. It was noted that both Helen Francis and Dan
Druzianic would be away.
It was also noted that the HB Health Sector Leadership Forum was being held on 7 October. Those
able to attend were asked to advise the Company Secretary, Ken Foote.
Action
CHAIR’S REPORT
1.
Endorsement of Appointments: The Chair advised the Board on the recent appointment of
Sarah de la Haye to the Consumer Council and Deb Higgins to the Clinical Council both for a
term of three years. The Board of Health HB had been advised of both appointments.
2.
Approval of the HBDHB Annual Plan: A letter had been received from the Minister of Health,
the Hon Dr Jonathan Coleman advising the approval of the 2015/16 HBDHB Annual Plan.
3.
Visit from Chair of Health Partnerships Limited: The Chair of Health Partnerships would be
visiting HBDHB on Friday 9 October to discuss the relationship between HPL and the HBDHB.
Acting CEO Tim Evans will be in attendance at that meeting, and all Board members are
welcome to be involved in that discussion.
4.
Received Health and Disability Commissioner’s report for January to June 2015.
5.
Ministry of Health Quarter 4 report: The MoH Quarter 4 Health Target report had been
received. The Minister requested that two of the targets required stronger improvement.
These were “Faster Cancer Treatment” and “Better Help for Smokers to Quit in Primary Care”.
CHIEF EXECUTIVE OFFICER’S REPORT
The Acting CEO presented the report. Issues highlighted in his report included:
• Performance struggling with shorter stays in ED. One of the drivers was the significant increase
in ED presentations – a 13% increase.
• Elective surgery continues to improve
• Faster Cancer Treatment – an improvement was needed for those people that had been identified
as high risk.
• Contingency remains unused on target
• Consumer Stories – this was a new focus to enable the DHB to see the “business” through the
eyes of the consumers/patients and as a result, improved processes would be instigated because
of these learnings.
• Board Delegations Policy – this had been to FRAC earlier in the day and the Contracts Manager,
Ashton Kirk would be speaking to this later in the agenda.
• Te Ara Whakawaiora / Culturally Competent Workforce – an improvement in that HBDHB were
now at 12.27% which was getting close to the target of 12.97%. The Engaging Effectively with
Page 2 of 7
Maori courses had been well received by staff and the PHO had had a good uptake in staff
attending the course. Unfortunately the plan to have all staff attend this course by December
2015 would be delayed.
• Te Ara Whakawaiora / More Heart and Diabetes Checks. This report had two separate
components – Diabetes and CVD Risk Assessment and was largely focused on primary care.
• Ministry of Health Quarter 4 report: The quarter four health target results had been finalised and
the HBDHB had done well in five of the health targets. However improvement needed to be
achieved for Faster Cancer Treatment and Immunisation coverage.
FINANCIAL PERFORMANCE REPORT
Comments were summarised as follows by the Acting Chief Financial Officer, Peter Kennedy:
•
A favourable variance of $9,000 with no contingency utilised.
•
A review of the surgical services budget was in progress.
•
Tracking better for year end result.
•
Mental Health rebuild – current indications are that this is going to come in on time and under
budget.
•
Maternity Unit refurbishment was going well and the roof was now on.
RESOLUTION
That the Board
Delegate authority to approve the annual report and sign the letter of representation to the
auditors, to the Chair of the Board and the Deputy Chair of the Board.
Moved:
Barbara Arnott
Seconded:
Peter Dunkerley
Carried
CONSUMER STORY
An email which had been received from a patient’s wife was read out at the meeting. This person
felt it important to provide the HBDHB with some feedback after her husband’s two experiences in
ED. Kate Coley (Director Quality Improvement & Patient Safety) gave a presentation to the Board
on what was currently being undertaken within ED to better reflect the needs of the
patients/consumers coming into ED. This was part of the AIM 24/7 project to look at ED front of
house.
Analysis has been done through both patient and staff surveys, as well as looking at the foot traffic
and journey of a patient when they were in the ED environment. Sixty people had been interviewed
so that the process and experience of these patients could be understood.
The staff survey had been undertaken, the following results emerged:
82% -
it is not clear to patients who they should talk to
86%
-
not told how long they might have to wait
86%
-
not able to discuss why there were coming into ED because of lack of privacy
18%
-
the front entrance – provides a positive impression as a hospital.
Other comments regarding the current configuration of ED front of house were as follows:
Page 3 of 7
•
ED is used as a thoroughfare. 134 patients came into ED and 148 people came through ED
doors and then moved somewhere else.
•
On average patients were moved a dozen times because of the processes currently in place.
The Project Team would be looking at the design of the ED waiting area, manage the issue of lack
of privacy and clinical space, reduce the number of patient movements and reduce the confusion for
patients of what the process was when in ED.
This was presented to both the Clinical and Consumer Councils, EMT and feedback from these three
groups had been incorporated into the business case.
Some of the issues to be addressed were:
•
ED is for ED patients only.
•
Additional of triage rooms required so more privacy for the patient.
•
More space for people brought in by ambulance
•
Signage to be streamlined
•
Review of processes thereby reducing the amount of time a patient is moved
Work is due to start November 2015 and finish February/March 2016.
REPORT FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
Dr Mark Peterson provided an update to the Board from the Clinical Council. In summary this
included:
•
The Central Region CEO’s and Chairs attended both Clinical and Consumer Council meeting
on 9 and 10 September 2015. Interest was shown from this group to introduce a similar
structure to other DHB’s.
•
Redesign of the Musculoskeletal Service – a paper was presented on the implementation of
the review and fundamental redesign of musculoskeletal and orthopaedic services. The
Clinical Council endorsed and supported this review.
•
Clinical Council Workshop Summary – a summary of this workshop held on 12 August was
presented to the Board.
•
Clinical Council Terms of Reference – a revised Terms of Reference was endorsed and
approved by the Clinical Council.
Hawke’s Bay Health Consumer Council
Council Chair, Graeme Norton spoke to the report which was included in the Board agenda.
Issues presented in the report included the following:
•
Partnership Advisory Group: first year celebration was recently held.
•
MRB focus on Suicide Prevention / Postvention: endorsement from the Consumer Council on
the focus of suicide prevention
•
Report on Implementation of the HBDHB Obesity Strategy
•
Travel Plan Survey – the Consumer Council were involved in the process of developing this
survey.
•
Consumer Council Terms of Reference and Annual Plan updated and approved.
•
Graeme Norton co-presented at APAC with John Gommans on effective and collaborative
working of both Consumer and Clinical Council.
Page 4 of 7
Māori Relationship Board (MRB)
Acting Chair Heather Skipworth provided an update to the Board on the September MRB meeting.
In summary the issues raised were as follows:
•
Acknowledgement given to Kevin Snee on his excellence in use and leadership of Te Reo
Maori.
•
New Mortuary opening
•
Wairoa Health Needs Assessment
•
Rheumatic Fever Plan.
•
Implementation of the Obesity Strategy
•
Cultural Training.
BOARD DELEGATION POLICY
Hawke’s Bay District Health Board is required under the New Zealand Public Health and Disability
Act 2000 to have a Board Delegations Policy. The current policy was identified as needing review.
A revised draft policy was presented to FRAC and the Board in January 2015 and the Board
approved this draft.
The Board Delegations Policy also required the approval of the Ministry of Health. The Ministry of
Health reviewed the January 2015 policy as approved by the Board. Feedback from the Ministry
and recommendations to include the obligations under relevant legislation were included. FRAC
considered the revised Board Delegations Policy in August 2015 and recommended it be approved
by the Board in September 2015.
RESOLUTION
The Board
Approve the Board Delegation Policy for signing by the Ministry of Health on behalf of the
Minister.
Moved:
Dan Druzianic
Seconded:
Andrew Blair
Carried:
URGENT CARE ALLIANCE UPDATE
This update provided a summary of the work of the Urgent Care Alliance since the last quarterly
update in June 2015. It was intended that these reports provide a more in-depth overview in addition
to the monthly progress reports that are regularly received by EMT/Clinical Council.
The Board noted the report.
Page 5 of 7
ANNUAL LEAVE
The purpose of this Board report was to outline the recent and planned initiatives to reduce annual
leave and other leave balances.
Discussion on the difficulty of requiring clinical staff to take time off from their job was considered.
The issue of locums coming to work for the HBDHB while on annual leave from another DHB was
also deliberated on, as was the complications involved for clinicians to have annual leave and being
able find cover for their role eg., on-call etc.
The Board endorsed management actions to reduce the accrued annual leave liability.
ALLIANCE LEADERSHIP TEAM
A summary of the notes from a meeting for the HB Health Alliance Leadership Team was included
in the Board agenda. Updates on the following issues were covered:
•
Development of primary care networks
•
Urgent care update
•
Health promotion update, and
•
Youth health update
MONITORING
Te Ara Whakawaiora / Culturally Competent Workforce
John McKeefry spoke to the report
The report was taken as read, with discussion summarised including:
•
The 2014/15 year saw a reduction in the gap between actual representation and target. The
year started with a new target of 12.97% and a gap of 59 and ended with 12.27% and a gap
of 20.
•
There had been an overall increase in the past 12 months of 1.44% of employees who
identified as Māori with 12.27% at 30 June 2015 compared to 10.83% as 30 June 2014. Over
the last 5 years there had been a significant increase with 8.74% identifying as Māori in June
2010 compared to 12.27% in June 2015.
•
To date 1088 current staff members (38.2%) have completed the ‘Engaging Effectively with
Māori’ training, with a further 158 staff booked to attend.
Te Ara Whakawaiora / Diabetes – More Heart and Diabetes Checks
Liz Stockley (as Indicator Champion) spoke to the report. The report was taken as read.
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
RECOMMENDATION TO EXCLUDE THE PUBLIC
Page 6 of 7
RECOMMENDATION
That the Board exclude the public from the following items:
21.
Confirmation of Minutes of Board Meeting
- Public Excluded
22.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
23
Board Approval of Actions exceeding limits delegated by CEO
24.
Chair’s Report
25.
Reports and Recommendations from Committee Chair(s)
- Finance Risk and Audit Committee (tabled)
Moved:
Barbara Arnott
Seconded:
Diana Kirton
Carried
Th
e public section of the Board Meeting closed 3.15pm
Signed:
Chair
Date:
Page 7 of 7
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 25 NOVEMBER 2015, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.08PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana (arrived at 1.40pm)
Peter Dunkerley
Andrew Blair
Diana Kirton
Barbara Arnott
Heather Skipworth
Jacoby Poulain
Denise Eaglesome
Helen Francis
Dan Druzianic
Apologies
Nil
In Attendance:
Kevin Snee (Chief Executive Officer)
Members of the Executive Management Team
Chris McKenna (Chair, HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council)
Members of the public and media
Minutes
Brenda Crene
KARAKIA
Heather Skipworth opened the meeting with a Karakia.
APOLOGIES
Apology for lateness had been received from Ngahiwi Tomoana
INTEREST REGISTER
No changes to the Interest Register were notified and there were no Board member interests
declared in any of the items on the agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 28 October 2015, were confirmed as a correct record of
the meeting.
Moved:
Andrew Blair
Seconded:
Barbara Arnott
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Item 2:
The Board wish to ensure the following are picked up by the respective Council’s and
Committees in 2016:
• Combined Clinical and Consumer Meeting – advised three meetings will be
staggered throughout the year, as and when required.
• Combined Consumer and MRB Workshop around “Obesity” to be considered.
• Suggested to include MRB consumer stories at the Board Meeting / and Vice versa.
Page 1 of 7
Item 1: Actioned
BOARD WORK PLAN
The Board Work Plan for December was noted.
The A3 project update Transform and Sustain dashboard had been included on the FRAC agenda
on this occasion.
An initial discussion around the Transport/Travel would be held in the public excluded section of
this meeting, with the intention to provide the full strategy to the December Board meeting.
CHAIR’S REPORT
• The Chair advised the following retirements, with a letter being sent conveying the Board’s best
wishes and thanks for their extended years of devoted service.
Years of
Name
Area
Service
Service
Arnett McCleallan
Kitchen Assistant
Facilities & Operational Support
20
Lynn Barton
Receptionist - Outpatient
Facilities & Operational Support
17
• A draft of the NZ Health Strategy document had been released by the Ministry, with national
consultation occurring. Details on forthcoming meetings are available on request.
• A Risk Management Consultant (Chris Peace) was undertaking a Risk Management Review
and interviews with respective management and staff. The Chair advised this was going well
and expressed his thanks to Ken Foote for managing this process. The Board look forward to
receiving the draft report when available.
• MoH Health Targets had been released with the only area to drop back being shorter stays in
ED, down from 95% to 92%. This is due to a rise numbers through ED which is similar to the
levels experienced during winter.
• The Chair confirmed the Symposium for Central Region DHBs would be held in Masterton on
20 and 21 July 2016. This date would be included on the 2016 workplan.
Action.
CHIEF EXECUTIVE OFFICER’S REPORT
On presenting this report, matters highlighted included:
• MoH have been interested in HBDHB’s theatre utilisation asking other DHBs to link in to view
how the productivity has been achieved, noting there have been big changes in culture,
disciplines, and management. Surgical directorate should be congratulated.
• Problem with ESPI compliance which has financial penalties for ongoing non-compliance.
• Smokers in primary care now over 12 months, instead of 15 months. Now showing as a
percentage of all smokers in enrolled population who have been asked if they want to cease
smoking, whereas previously everyone who entered clinics were asked.
• Diabetes checks are progressing well.
• Financially we are in good shape with the deficit advised earlier having reduced.
• Catch-up in orthopaedic services and a range of extended options. .
• Transform and sustain project detail was included in the FRAC paper. Noted no red flags as
the CRISP project had moved to amber.
Page 2 of 7
FINANCIAL PERFORMANCE REPORT
Matters highlighted by the CFO included:
• The result for October was a favourable variance of $414 thousand, with the year to date result
$124 thousand favourable with no contingency used, other than that allocated to surgical
Directorate.
• Hawke’s Bay is unique amongst DHBs and consider/monitor strategies in financial terms in
relation to resource deployment. What gets measured gets done …which is reflected in the
figures provided on page 2 of the report.
• The Blessing of the new Mental Health Unit was held in November and everyone was very
impressed. “A long journey but fabulous destination”
Action:
A tour of “Nga Rau Rakau” (the Mental Health Unit
) in December was queried.
This would be followed up by the COO and advised accordingly.
CONSUMER STORY
The story related to a very independent elderly person who resided in an aged residential care
facility from the age of 88. At age 90 this person who had shown signs of deterioration, had fallen
badly resulting in a broken femur. The outcomes from this review resulted in a number of learnings
and quality improvements, which have been shared within the hospital and other facilities.
Educating and talking to the person and their whanau is key to alleviating accidents, this was part
of the patient rounding (strong evidence based system) brought in.
REPORT FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
The report provided an overview of the: Quality Accounts (presentation) in a more graphic format;
Serious and Adverse Events; Delivery of our Future Musculoskeletal and Orthopaedic Service;
Regional Tobacco Strategy for Hawke’s Bay 2015-2020; the Health Literacy Business Case and an
Information Systems Function Review – with consultants.
Regarding Bilingual Signage, Council agreed there needed to be more work done on this and the
options simplified, with support in principle for the MRB’s recommendation, however there would
be exceptions when Māori would not be suitable in the first instance.
Fetal Alcohol Spectrum Disorder (FASD):
Council received a presentation on FASD. In HB each year there are approximately 2,000 births,
this likely results in 20 children each year being affected (in a variety of ways) by FASD (and this
figure is noted as conservative). From a diagnostic point of view with a small but developing group
here in HB, are able to diagnose through a multidisciplinary team. We are leading nationally in this
area and if FASD is picked up early we can minimise the level of disability children can suffer.
Education and raising awareness within the community is crucial with comments summarised
below:
• There is no safe time for a pregnant woman to drink!
• Messaging on the back of buses is being considered “If you don’t know, Don’t drink”.
• A visual comparison of an unaffected alongside an affected brain of a child with FASD, is
empowering.
• This is not about how to educate – but where to educate – with the person delivering being key.
• Information provided to schools showing the ugly facts stops many and encourages strong
messages to be relayed by children to their families. Many in Wairoa stopped smoking through
this method.
• GP service detail/advertising suggested to capture quicker.
Page 3 of 7
• Zero tolerance needs to be conveyed to the community, but this is really about all aspects of
health and wellbeing: alcohol, smoking, drugs and obesity.
HB Health Consumer Council
An overview of Council discussions was summarised, with focus on:
Bilingual signage with the outcome from the Consumer meeting differing from that of MRB and
Clinical Council. Consumer Council’s preference was to see this explored further, being mindful of
the timelines to have the Mental Health signage in place in the New Year.
The Board as a whole had not yet received the Bilingual Signage paper although it had been
reviewed through board member participation at MRB.
The Board asked management to respond, considering the respective Committee views. It was
noted this was already in hand with discussion/presentation(s) scheduled to Committees in
December.
Other areas considered by Consumer Council included a very lively one hour Workshop with a
MoH representative on the “NZ Health Strategy”. A feedback document has subsequently been
provided to DHB planning and the MoH representative who attended.
Māori Relationship Board (MRB)
MRB’s report to the Board included an overview of the following: Regional Tobacco Strategy for
Hawke’s Bay 2015-2020; Locality Networks Planning; and IS functions consultation.
Also received was a presentation on Fetal Alcohol Spectrum Disorder; and Bilingual Signage with
the proposed changes to signage and display not supported, resulting in the following
recommendations which were noted by the Board.
RECOMMENDATION
That the Board
Note MRBs recommendations following the Fetal Alcohol Syndrome Disorder presentation and
the Bilingual Signage report as follows:
• Alcohol & Drugs as well as FASD be added as a priority to the Annual Māori Health Plan for
2016-17.
• Te Reo Māori to appear before English, that both internal and external signage follow the
same format and that the policies; Signage and Display (HBDHB/OPM/095) and Te Reo
Māori Translation (HBDHB/OPM/113) are amended to reflect MRBs recommendations
before final approval and sign-off.
FOR DISCUSSION / DECISION
Regional Tobacco Strategy for HB 2015-2020
With the strategy provided, the discussion with board members that follows reinforced the amount
of work that had been undertaken with a very wide range of partners and stakeholders including
year 9 college students with their own agenda.
In summary
• Messaging was crucial as people do not smoke and drink alone, especially young Maori
pregnant women with 50% of 27 year old Maori women smoking, having commenced the habit
through family influence.
• Do agree with incentivised programs.
• Good actions but they do not wrap around the whole whānau!
Page 4 of 7
Action:
It was agreed the strategy would be reviewed yearly with an update to be
provided to the Board in November 2016 (which would be included on the
workplan).
Congratulations to the team, well done.
RECOMMENDATION
That the Board
Note the content of this report and endorsed the draft Regional Tobacco Strategy for Hawke’s
Bay 20115-2020
Adopted
Delivery of our Future Musculoskeletal and Orthopaedic Service
The report provided by Dr Andy Phillips was well received by the Board.
A triple aim based approach to look at the provision of an efficient needs based service in this area
with a phased approach to resolving pain and disability arising from musculoskeletal conditions in
patients within our community. Although in three stages, the paper provided focused on stage one:
Reduction of pain and disability by providing non-surgical treatments for hip and knee; non-surgical
treatment option for spine; clarity around prioritisation for orthopaedic surgery and more consistent
scoring practices; reducing delay between FSA and referral to the waiting list (being given
certainty); options for those not meeting the threshold for surgery; better patient clarity about the
hip and knee elective surgical pathway and the basis on which they have been accepted/declined
for surgery; and increase surgical capacity to meet delivery of major joint replacements.
The board advised they have a higher level of confidence in this area following the receipt of this
report and adopted the following recommendation.
RECOMMENDATION
That the Board:
Endorse the phased approach to resolving pain and disability arising from musculoskeletal
conditions in patients within our community.
Adopted
Improving Patient Flow (ED six hour performance)
Dr Gommans and Emma Foster provided a presentation to the Board, summarised below.
A number of system and process changes have occurred within ED over time, including much
better use of resources. This has resulted in shorter stays in ED (ie, 95% April-June 2015)
Improvements included:
•
ED Observation Beds: moved 4 beds from AAU into ED with increased utilisation and reduced
LOS.
•
Medical Day Unit: next to AAU, day cases now in MDU
•
AAU: changed model of care
–
Acute Physician takes GP calls 0800-1700 Monday - Friday
–
Duty SMO in AAU: supporting team & ‘pull’ from ED/GP
–
Additional Medical Registrar and House Officer resource in AAU (shift one inpatient
ward team to AAU)
Page 5 of 7
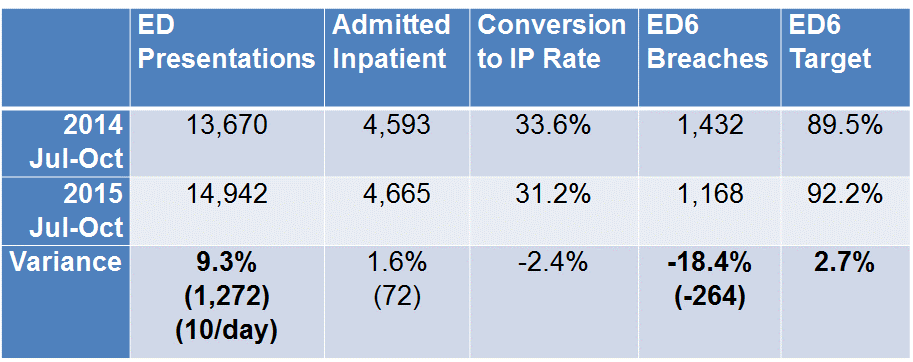
–
Additional evening Medical Registrar in ED/AAU Mon- Fri
–
Second weekend Medical Registrar in ED/AAU
•
General Medicine: changed inpatient model of care
–
Ward-based Medical Teams
–
Doctors now participate in ward Multi-Disciplinary Team
–
‘Rapid (Board) Rounds’ for discharge planning
•
Nurse led ‘criteria based’ discharging for weekends
–
RN completion of Discharge Summary
•
Inter-Professional Practice (IPP) trialled on A1
–
move from multiple assessments by Multi-Disciplinary Team members to shared skill-
set for IPP model.
–
IPP initial assessment tool created and trialled.
–
Shared education sessions to start next month.
Demand in ED for the winter months of 2015 (ie, July-October 2015) saw higher throughput than
the preceding year (2014) resulting in a drop in the target level (ie, 95% July-Oct 2015)
It was advised the actions above appear to have dealt with last year’s problems, now we are
having to deal with higher volumes ongoing, as the winter set back is continuing to pose a more
persistent problem for ED.
This project is now moving into Stage 2 with staff and others buying into the ongoing problem
which has brought about a bottom up approach resulting in a noticeable culture change to date.
Emma Foster was thanked for her work on this project and members were advised she was
leaving the DHB in December to take on a new venture.
MONITORING
Performance Framework Exceptions Q1 Jul-Sept 15
Performance Highlights included:
• Achievements: More heart and Diabetes checks; improved access to elective surgery; and Wait
Time for diagnostic services.
• Areas of Progress: Faster Cancer Treatment; and Stroke Services.
• Areas of Focus: Shorter days in ED; Better help for smokers to quit in primary care; Mental
Health Services, percentage of child and you with a transition discharge plan; Diabetes
Management; Improving wait time for diagnostics.
Page 6 of 7
Human Resource KPIs Q1 Jul-Sept 15
Matters within the report were highlighted and discussed with extended discussion around leave
balances.
Leave balances (for staff) has been a national issue for some time. The Central Region DHBs are
picking this up as a priority focus. HBDHB will be refining policy to be as directive as possible and
it is likely the fifty highest leave balance “offenders” would likely be reported to EMT periodically.
The Board received more confidence with the intense focus being placed on ensuring leave was
taken.
FOR INFORMATION
HB Health Alliance Meeting Summary
Alliance member Barbara Arnott was available for questions, noting 2015 had been very slow,
hopefully 2016 will see more matters/issues for consideration.
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
RESOLUTION TO EXCLUDE THE PUBLIC
RESOLUTION
That the Board exclude the public from the following items:
21.
Confirmation of Minutes of Board Meeting
- Public Excluded
22.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
23.
Board Approval of Actions exceeding limits delegated by CEO
24.
Chair’s Report
25.
Reports and Recommendations from Committee Chair
- Finance Risk and Audit Committee
36.
Introducing the Travel Plan - Presentation
Moved:
Helen Francis
Seconded:
Dan Druzianic
Carried
The public section of the Board Meeting closed 3.37pm
Signed:
Chair
Date:
Page 7 of 7
MINUTES OF THE BOARD MEETING
HELD ON WEDNESDAY 16 DECEMBER 2015, IN THE TE WAIORA ROOM,
DHB ADMINISTRATION BUILDING, MCLEOD STREET, HASTINGS
AT 1.00PM
Present:
Kevin Atkinson (Chair)
Ngahiwi Tomoana (arrived at 1.40pm)
Peter Dunkerley
Andrew Blair
Diana Kirton (arrived at 2.00pm)
Barbara Arnott
Jacoby Poulain
Denise Eaglesome
Helen Francis
Dan Druzianic
Apologies
Heather Skipworth
In Attendance:
Kevin Snee (Chief Executive Officer)
Members of the Executive Management Team
Dr Mark Peterson (Chair, HB Clinical Council)
Graeme Norton (Chair, HB Health Consumer Council)
Members of the public and media
Minutes
Brenda Crene
KARAKIA
Ngahiwi Tomoana opened the meeting with a Karakia.
APOLOGIES
Apology for lateness had been received from Diana Kirton
INTEREST REGISTER
A short term interest advised by email on 14 December by Diana Kirton had been included in the
Interest Register presented in the board papers.
Subsequently two interests were included for Andrew Blair on 17 December 2015.
No board member had an interest in any of the items on the Agenda.
CONFIRMATION OF PREVIOUS MINUTES
The minutes of the Board meeting held on 25 November 2015, were confirmed as a correct record
of the meeting.
Moved:
Barbara Arnott
Seconded:
Peter Dunkerley
Carried
MATTERS ARISING FROM PREVIOUS MINUTES
Item 1:
The following will occur during 2016 therefore the actions will be removed for the following:
Combined Clinical and Consumer Meeting (three meetings staggered throughout the year,
as and when required); Obesity discussions were in hand; May consider including MRB
consumer stories at the Board Meeting / and vice versa.
Item 2: Workplan updates – actioned.
Page 1 of 7
Item 3:
Mental Health Facility Tour – actioned.
BOARD WORK PLAN
The Board Work Plan for January was noted. A planning workshop will be held in January and an
updated detail workplan developed soon after for 2016.
CHAIR’S REPORT
• The Chair advised the following retirements, with a letter being sent conveying the Board’s best
wishes and thanks for their extended years of devoted service.
Years of
Name
Area
Service
Service
Julia MacKenzie
Registered Nurse
Acute & Medical
35
Carole Reese
Receptionist - Inpatient
Facilities & Operational Support
29
Liz Lack
Care Associate
Women Children & Youth
27
47 years
Maureen Fau
Uniform Co-ordinator
Facilities & Operational Support
overall
Maureen Fau had been working for the DHB for 47 years albeit with a break in service. An article
in the Leader was provided at the board meeting for members to view.
• Allied Laundry Limited: Ministerial approval had been received for Allied Laundry to enter into a
loan facility to purchase equipment, subject to shareholder approval.
The Chair put forward the following recommendation for approval:
RECOMMENDATION
That HB District Health Board, as a shareholder in Allied Laundry, gives approval for Allied
Laundry Services Limited to enter into a $2.550m (including overdraft) loan facility with the Bank
of New Zealand for the purposes of purchasing plant and equipment.
Moved
Dan Druzianic
Seconded Barbara Arnott
Carried
• A letter from the Ministry had been received around targets acknowledging the good work
undertaken.
• HBDHB’s financial result topped DHBs nationally for 2014/15 and the board acknowledged this
result and the extraordinary amount of hard work by all concerned to achieve this.
CHIEF EXECUTIVE OFFICER’S REPORT
The report was taken as read acknowledging:
• A drop in the target was noted for ‘shorter stays in ED’. High ED attendances were being
experienced around the country. A drop of 9.3% was experienced in the ‘Improved access to
Elective Surgery’. Results were encouraging for Faster Cancer treatment, immunisation and
better help for smokers to quit.
• Financial performance was well placed, five months into the financial year.
• It was noted the Travel Plan business case presented was far broader than just about parking,
we are looking for a long term sustainable solution.
Page 2 of 7
FINANCIAL PERFORMANCE REPORT
Matters highlighted by the CFO included:
• The pleasing financial result for November showed a favourable variance of $51 thousand, with
the year to date result at $175 thousand favourable with no contingency used other than $1m
transferred to surgical services and $90 thousand contributed to the corporate 3.0% savings plan.
• The debt write off of $22 thousand to November (authorised by GM PIF), had been itemised.
Reorganisation of Non-Financial Reporting
A presentation was received on the Reorganisation of Non-Financial Reporting, to better reflect the
strategic differences in the roles of the two committees; to connect appropriately to different
audiences for non-financial performance; to monitor the impact of Transform and Sustain as well
as the process of implementation.
The proposed changes would see:
• The Non-Financial Performance Framework Dashboard being replaced by the HBDHB Quarterly
Monitoring Dashboard.
• The Transform and Sustain Programme Overview being replaced with the Transform and
Sustain Strategic Dashboard.
The Board approved the proposed new reporting structure as follows:
Report
Current
Proposed
Reporting
Reporting
HBDHB Non-Financial Performance Framework
Dashboard
EMT, Board
EMT
HBDHB Non-Financial Exceptions Report
EMT, Board
EMT, Board
Transform & Sustain Project Overview and
Detailed Project Report
EMT, Board
EMT, FRAC
Transform & Sustain Programme Overview
Report
EMT, FRAC
EMT, FRAC
Hawke’s Bay DHB Quarterly Performance
Monitoring Dashboard
CHAIR, CEO
EMT, Board
Transform and Sustain Dashboard
Not Provided
EMT, Board
CONSUMER STORY
A patient story around difficulties experienced in ED was relayed. This highlighted the need for the
changes already identified and occurring in ED or planned for implementation in the near future.
REPORT FROM COMMITTEE CHAIRS
Hawke’s Bay Clinical Council
Bilingual Signage: Council supported the principles presented, advising the main decision makers
in this process were Consumer Council and MRB.
Travel Plan: Council were happy to endorse the business case to implement the “Go Well” Travel
Plan (option 3).
Urgent Care Year End Report and the additional expressions of interest, request for proposal
timelines (phase one of the programme) was in progress with feedback being sought on the
proposed options. Council endorsed the report and approved the options.
Collaborative Clinical Pathways: A query as to whether the development was progressing fast
enough. In response, what had been experienced to date was in-line with others around the country
Page 3 of 7
who were introducing Clinical Pathways. The focus now is to ensure implementation occurs with
consumer input to ensure person centred care is aligned.
Other areas reviewed and supported were the Quality Accounts and Medicines Reconciliations, with
acknowledgement of the monitoring reports provided.
HB Health Consumer Council
An overview of Council discussions was summarised with the Chair advising his update had been
provided to outline matters and issues occurring outside of normal Consumer Meetings.
Council strongly supported the Bilingual Signage principles with most vying for option B, however
were happy to leave the final aspects to the process that follows to MRB and relevant staff.
The “Go Well” Travel Plan had been endorsed by Consumer Council.
The Quality Accounts had been reviewed and Council members were happy with this document,
noting there were final tweaks being made up until submission to Health Quality and Safety
Commission. The Urgent Care Year End Report was noted and endorsed.
Māori Relationship Board (MRB)
The report was received for the Special Meeting of MRB held the week prior. It was noted MRB had
endorsed the Bilingual Signage principles with several additions noted.
The Travel Plan business case received and feedback provided along with MRB endorsement,
noting several areas for consideration.
Ngahiwi noted that the late inclusion of the PHLG report had created last minute technical issues for
reporting presentation. He pointed out that that MRB and PHLG were quite separate Committees
and there were no intentions to merge them.
Pasifika Health Leadership Group (PHLG)
The Pasifika Group’s meeting had been held the week of the Board meeting. Barbara Arnott (an
attendee at all PHLG meetings as Chair of CPHAC), spoke to the report and advised she supported
an increase in Pacific Navigators. Five were being sought and it was felt some of these may be
provided from other intersector organisations eg, Ministry of Social Development. If there was an
increased focus on Pasifika people’s health (consisting of just over 5,000 people in HB), a very
speedy improvement could be made.
It was noted PHLG felt an Intersector Project was required to address health and social issues for
Pacific People in HB. They also alluded to changes in the TOR and meetings, with several taking
place within the community.
The Board noted the issues raise in the Report.
FOR DECISION
Quality Accounts 2014/15
Kate Coley (DQIPS) provided a presentation on the latest version of the Quality Accounts which
had been reviewed by EMT, MRB and endorsed by Clinical and Consumer Counci,l noting there
were still some minor tweaks to be made prior to issue.
The board were impressed with document which took on a different format to prior years (2013 and
2014).
Action:
If board members wished to provide feedback directly
to [email address] they were most welcome, noting this document
would be issued to HQSC pre-Christmas.
Page 4 of 7
Travel Plan Business Case
Sharon Mason (COO) introduced Andrea Beattie (DHB) and Louise Baker (Opus Consultants).
Also in support was a representative from the HB Regional Council.
In 2013, the Board declined a ‘Paid Parking’ proposal because they were concerned it would
impact negatively on patients and staff, and may be seen as a revenue generating exercise with
‘profits’ derived by a commercial operator going out of the district.
In 2014 the Facilities Management Team were tasked to revisit parking and transport in a more
holistic way, taking into consideration the following objectives to:
•
Improve access to facilities for low income families
•
Promote exercise
•
Reduce the carbon footprint and
•
Increase the availability of car parks
As a result of this review the following options had been considered with preference for Option 3.
1. Do Nothing
2. Travel Plan, no charging - fewer sustainable options
3. Travel Plan with ‘gold-coin’ charging to fund sustainable transport FAVOURED
4. Build More Parks.
Board members individually supported option 3. The HB Regional Council representative present,
advised they were to review services in early 2016 to fully consider a viable transport service given
the goals of the HBDHB for the HB community.
The capital cost and operational budget detail was explained to members
RESOLUTION
That the Board note the feedback from the respective Council’s; and approve:
• The business case to implement the “Go Well” Travel Plan (Option 3) from 1 July 2016.
• The implementation of parking charges from 1 February 2017 to sustainably fund the Travel
Plan.
• The 2016/17 capital and operational budgets as set out in the business case.
Adopted
Action:
a)
The Board sought an update on progress prior to implementation
(timing to be advised by COO in due course)
b)
A request by a board member for regular reporting following
implementation including a focus on monitoring for inequity.
Bilingual Signage - Presentation
Sharon Mason (COO) introduced Andrea Beattie who provided a presentation which took on board
feedback from Council’s and MRB during November. Sharon and Andrea’s leadership was noted,
given the tight timeframes.
As a result of feedback generally some
“basic principles” were formulated for consideration
:
A commitment to incorporate bilingual signage around the HBDHB hospital and health facilities
Te Reo Māori placed first, followed by English.
Rationale - preservation of language, reducing inequalities (improving Māori health is about
making services and the environment more inviting for Māori so they’l actually feel ok about
coming here to receive services)
Page 5 of 7
Either Te Reo Māori above with English below, or both languages side-by-side (decision
required – see examples appended)
Font to be bold, upright roman style (no italics)
Signage contents to simple, clear and consistent, using plain English terms
Applies to new signage; transition of existing signage to new form will be phased through capital
projects.
The Board agreed and approved the above principles and advised they would leave the final look
and feel of signage to the experts. Over time, as signage is replaced it would be updated with the
new signage. This sends a supportive message acknowledging Te Reo Māori and Kahungunu Reo
strategy to the HB community.
MONITORING
Urgent Care Year End Report and Update
The report provided noted progress made by the Urgent Care Alliance and the Urgent Care
Stakeholder Group. The report summarised the progress to date of the Urgent Care Project that
was established and is led by the Urgent Care Alliance Leadership Team. It sets out a series of
options for key priorities and indicates the Urgent Care Alliances intentions over the coming year.
Note the additional document provided showed a high level work in progress timeline for an
expression of interest and request for proposal process for the Urgent Care Project.
Te Ara Whakawaiora Breast and Cervical Screening and the Annual Maori Health Plan
Dashboard Q1 July-Sept 2015 were reviewed relative to their respective areas and progress/or
otherwise noted.
GENERAL BUSINESS
There being no further discussion, the Chair accepted a motion to move into Public Excluded.
RESOLUTION TO EXCLUDE THE PUBLIC
Page 6 of 7
RESOLUTION
That the Board exclude the public from the following items:
22.
Confirmation of Minutes of Board Meeting
- Public Excluded
23.
Matters Arising from the Minutes of Board Meeting
- Public Excluded
24.
Board Approval of Actions exceeding limits delegated by CEO
25.
Chair’s Report
Reports and Recommendations from Committee Chair
26.
Finance Risk and Audit Committee
27.
Hawke’s Bay Clinical Council
Moved:
Diana Kirton
Seconded:
Helen Francis
Carried
The public section of the Board Meeting closed 3.07pm
Signed:
Chair
Date:
Page 7 of 7
Document Outline