OIA H2026081053 - Appendix 1
A COVID-19 Vaccine Safety Surveil ance Strategy for
New Zealand
Framework Proposal for discussion
Associate Professor Michael Tatley
New Zealand Pharmacovigilance Centre – University of Otago
This document has been prepared with contributions from:
s 9(2)(g)(ii)
- Medsafe
s 9(2)(g)(ii)
– IMAC
s 9(2)(g)(ii)
– Auckland University
s 9(2)(g)(ii)
– Otago University
under the Official Information Act 1982
Released
28 September 2020
Michael Tatley – NZPhvC / University of Otago
OIA H2026081053 - Appendix 1
A COVID-19 Vaccine Safety Surveil ance Strategy for New Zealand
Table of Contents
Context ................................................................................................................................................. 1
A COVID-19 Vaccine Safety Surveillance Strategy for New Zealand ..................................................... 1
Elements of a COVID-19 Safety Surveillance System: ...................................................................... 1
Passive Reporting of Adverse Events Following Immunisation .................................................... 1
Active Monitoring of Adverse Events Following Immunisation.................................................... 2
Hospital surveillance .................................................................................................................... 3
1982
Defining Adverse Events of Special Interest (AESI) ....................................................................... 4
Establishing historical baselines for AESIs .................................................................................... 5
Act
Hospital Surveillance Focal Areas ................................................................................................. 5
Mortality monitoring .................................................................................................................... 5
Vaccine safety surveillance oversight and coordination .............................................................. 5
Supporting Pacific Island Neighbours ........................................................................................... 7
Critical Practical Considerations for Developing a COVID-19 Vaccine Safety Surveillance
Information
Strategy ........................................................................................................................................ 8
References .......................................................................................................................................... 10
Appendix 1.......................................................................................................................................... 11
Official
The KIWIvax smartphone based technology to monitor AEFI’s ..................................................... 11
Appendix 2.......................................................................................................................................... 17
the
COVID-19 vaccine Adverse Events of Special Interest .................................................................... 17
under
Released
2 September 2020
Michael Tatley - NZPhvC / University of Otago
OIA H2026081053 - Appendix 1
A COVID-19 Vaccine Safety Surveillance Strategy for New Zealand
Context
The COVID-19 pandemic has caused unprecedented havoc globally, with major impact devastating
every aspect of society, health, lifestyle and the economy. Although fundamental public health practices
remain core to limiting the spread of the pandemic, the development and use of a vaccine is recognized
as critical to a path to increasing stability and eventual achievement of a new normality.
The urgency of the pandemic crisis has given rise to extraordinary initiatives in vaccine development,
compressing the usually decades long pathway into months to a year or two. Multiple vaccine
strategies are in varying stages of development, some of which already are at the point of early Phase III
trials. Whilst this accelerated vaccine development will be able to address and identify vaccine safety
issues, the trade-off from this approach will be the forgoing of the truly large-scale robust safety studies
that have been undertaken historically. Whilst NZ vaccine licensure will be dependent on positive Phase
III clinical trial evidence, these will still not be able to identify rare events, or events that may be
1982
confined to individuals or groups that were not well represented in phase III international trials. It is
unlikely that any Phase III clinical trials will be undertaken in NZ.
Act
Therefore, it is imperative that a NZ COVID-19 vaccine safety surveillance strategy is put in place to
identify safety issues with COVID-19 vaccines in use in the broader population to inform decisions
about continued use, or to reassure the population of the safety of the vaccine(s) and that its safety is
being closely monitored.
NZ operated a highly successful and comprehensive vaccine safety surveillance strategy for the delivery
of the new MeNZB vaccine (the Meningococcal Vaccine Strategy – MVS) over the period 2004-2006/7.
Information
This approach garnered international interest and accolade for its robust methodology and ability to
support decision making and reassure public safety of the vaccine.1-3
Unfortunately, once the epidemic was under control, the infrastructure and institutional knowledge and
personnel were disbanded and largely lost. However, the approach has been well documented and
Official
some of the personnel with system knowledge and elements of the infrastructure are still available,
although some of the personnel perform other roles today. Of importance is that there has been
the
significant progress in NZ in electronic approaches to linked datasets and data analysis which will allow
more cost effective and efficient surveillance.
The proven MVS approach provides an ideal template on which to base a COVID-19 Vaccine Safety
under
Surveillance Strategy (
decide an appropriate acronym), customizing it to account for the current era.
A COVID-19 Vaccine Safety Surveil ance Strategy for New Zealand
The purpose of the Safety Surveillance Strategy will be to inform Public Health safety decision making
about the safety of COVID-19 vaccine(s), how a vaccine’s risk-profile may influence its utilization,
Released
including potentially withdrawing a vaccine from further roll-out. Overall, a Safety Surveillance Strategy
will also serve to reassure the public that stringent monitoring of vaccines that are in use is being
undertaken.
Elements of a COVID-19 Safety Surveil ance System:
Passive Reporting of Adverse Events Following Immunisation
Spontaneous Reporting Program
New Zealand has had a long and successful history of Adverse Events Following Immunisation (AEFI)
monitoring as a component of its Pharmacovigilance system.4 This is provided through the Centre for
25 September 2020
s 9(2)(g)(ii) – NZPhvC / University of Otago
Page
1 of
18
OIA H2026081053 - Appendix 1
A COVID-19 Vaccine Safety Surveillance Strategy for New Zealand
Adverse Reactions Monitoring (CARM) within the New Zealand Pharmacovigilance Centre (NZPhvC) at
the University of Otago, which delivers national pharmacovigilance services for the Ministry of Health.
CARM is New Zealand’s national centre receiving voluntary reports from health professional and the
public of AEFI’s, as well as adverse reactions to medicines. The CARM system has been in operation
since 1965, is well supported with NZ having one of the highest rates per capita of reporting to national
monitoring program globally. Vaccines account for about 40% of all reports to CARM. Reports to CARM
are reviewed by specialist clinical assessors and are recorded into a national database. Standardized
terms are assigned to the events documented in each report using the World Health Organization
(WHO) Adverse Reaction Terminology dictionary structured to group related terms by System Organ
Class to facilitate pattern identification. The clinical review further determines the severity,
seriousness, outcome and the likelihood of causal association to the vaccine for each report in line with
WHO protocols. Co-medications and co-morbidity are also recorded.
Enhanced Spontaneous Reporting
Whilst spontaneous reporting has been the cornerstone of NZ’s system for over 50 years with high
1982
rates of reporting, particularly for vaccines, enhancing spontaneous reporting in the circumstances of
new products where there is limited safety information has been applied successfully to gather more
data. During the MeNZB vaccination strategy over 2004-6 reporters were encouraged to lower their
Act
threshold for reporting of any adverse event to CARM, resulting in a 2-fold increase in vaccine reports
over the previous years that were already the highest by double of the next highest country member
(Australia), of the WHO Program for International Drug Monitoring of which NZ was a founding
member in 1968. These additional reports of the same high quality clinical case narrative classic of NZ
AEFI and Adverse Drug Reaction reports to CARM, provide valuable additional data to inform the safety
evaluation of the vaccine and illustrates the commitment of NZ Health Professionals to supporting
pharmacovigilance.
Information
Enhanced spontaneous reporting of AEFI’s both by providers and the public should be encouraged for
COVID-19 vaccines to expand the database to support evaluation of the vaccine’s safety profile.
Enhanced reporting would require further resourcing utilizing the spectrum of communication
channels including social media for promotion and marketing to both vaccinators and vaccinees
Official
Active Monitoring of Adverse Events Following Immunisation
KIWIvax
the
NZ AEFI monitoring has been passive (i.e. reliant on voluntary reporting) and is subject to
underreporting. In addition to underreporting, passive reporting systems are further limited by
reporting biases and the lack of denominators.
To overcome this, the NZPhvC, working alongside the Immunization Advisory Centre (IMAC), is in the
under
process of finalising the development of KIWIvax, an automated real time SMS-smartphone-based
technology system that will enable the identification of AEFI’s directly from vaccinees who are actively
followed up after vaccination through a series of simple questions initiated from a post vaccination
SMS. KIWIvax consists of a program (SMART vax) loaded onto a Medical Practice’s computer system
and extracts data from the Practice Management System (PMS). Medtech32 currently accounts for
approximately 80% of PMS’s in NZ.5 The data from this interaction auto-populates a database which is
Released
analysed by customised software that generates a diversity of reports, graphics or customised queries
for the purposes of monitoring safety profile of the vaccines monitored.
The development of KIWIvax has become possible due to collegial collaboration between the NZPhvC
and the Australian developers of the innovative SMARTvax/AusVaxSafety system, which has achieved
uptake across all Australian States and Territories and shown to be successful in monitoring the safety
profile of vaccines used in Australia and also in supporting research projects.6-8
SMARTvax/AusVaxSafety has been customised to suit the needs for New Zealand vaccine safety
monitoring to become a New Zealand SMARTvax/KIWIvax. This development was initiated and well
underway prior to the COVID-19 pandemic to support the monitoring of routine schedule and/or other
vaccines in use in New Zealand. It is suited to the monitoring of any vaccine and ideally suited to
monitor COVID-19 vaccine(s) that may be brought into use.
25 September 2020
s 9(2)(g)(ii) – NZPhvC / University of Otago
Page
2 of
18
OIA H2026081053 - Appendix 1
A COVID-19 Vaccine Safety Surveillance Strategy for New Zealand
This approach, discussed in more detail in Appendix 1, sends an SMS message to the vaccinee extracted
from the Practice Management System (PMS) of the medical practice where the vaccination was
administered by means of a dedicated SMARTvax software application. Medical Practice approval
authorises the loading of the SMARTvax software. The message which is sent 3 days after the
vaccination event (for routine vaccines), enquires whether there had been an adverse event of any type
after the vaccination by simply requiring a ‘Yes’ or ‘No’. For COVID-19 vaccines the timing of the initial
message will be revisited according to the vaccine platform type in use. In the event of a ‘Yes’, the
vaccinee is invited to complete a survey by responding to a series of targeted questions/options about
the nature of the AEFI. The system also includes an option to report further details relating to events
that are of a more serious nature and enable direct follow-up with the vaccinee to establish further
detail. Responses are reported back to the Medical Practice’s PMS patient file to facilitate clinical follow-
up in the event of an event of concern. The SMARTvax software uploads an anonymized copy of the
interaction to a cloud-based database which houses the analytical software that enables reports,
graphics and queries to be performed. Since the denominators are known (all SMS’s sent – ‘Yes’, ‘No’
and non-responses), rates of AEFI events can be determined. The SMARTvax at the time of the Cloud
1982
database upload also sends a copy of the interaction to the NZPhvC database which complements
passive (spontaneous/voluntary/enhanced) reporting to enable a comprehensive overview of all
Act
sources of AEFI’s to be performed.
KIWIvax offer advantages in reaching the entire vaccine cohort, supporting the automated population
of AEFI databases for analysis and can free-up resources that can then be more usefully directed to
follow-up serious, clinically significant or unusual AEFI of concern or interest. More than 80% of NZ’ers
own a Smartphone.9 The KIWIvax system provides opportunities to achieve greater efficiencies in
resource utilisation and further improve AEFI surveillance. Utilizing this technology will enable far
wider reach than the current modalities of reporting which are limited to the conscious decision to
report an AEFI online or to a health provider for onward notification to the NZPh
Information vC.
KIWIvax variation for non-PMS systems
SMARTvax has been designed to operate in a PMS Medical Practice environment in
interfacing/interrogating PMS-specific structures and data fields. Vaccines that are administered in
other clinical settings (Pharmacy or Community Vaccination Clinics), do not use similar computer
Official
bound PMS systems or use cloud based software systems. SMARTvax currently is not compatible with
non-computer Patient Management Systems. The Australian developers are in the final stages of
the
designing a variation of the way the SMARTvax component of this system operates for application
outside of the typical PMS systems used in medical practices. This system is being designed to operate
in the context of pharmacy-based or community vaccination clinics, but with the same SMS interaction
feeding the Cloud and NZPhvC database. The NZPhvC collaboration with the Australian developers
under
extends to incorporating an appropriately customised variation of this SMARTvax version in New
Zealand. This variation will use the core SMS messaging identical to the PMS version, but likely involve
the Pharmacy/Community Vaccination Clinics, or in New Zealand the NIR, notifying the NZPhvC of the
vaccination including the vaccinee’s mobile contact number. The NZPhvC will house the SMARTvax
software and initiate the SMS interaction, receive the responses and upload an anonymized copy to the
Cloud database.
Released
Hospital surveillance
The Passive and Active safety surveillance elements are likely to provide early real time safety data that
due to their targeted focus beyond traditional routine methods may be considered adequate
surveillance for NZ’s COVID-19 vaccines monitoring. However, it is possible that some AEFI’s may be
of sufficient severity/seriousness to result in hospital admission or will require Emergency Department
consultation. It may also be possible that the vaccine properties/composition could result in
unintended events resulting in hospitalisation, not immediately recognised as vaccine-related, but
potentially predicted from the anticipated immune response.
By the time NZ will access COVID-19 vaccines for roll-out it is likely that even with the concerns around
accelerated Phase III trials there will have been many tens of thousands of trial participants globally
25 September 2020
Michael Tatley – NZPhvC / University of Otago
Page
3 of
18
OIA H2026081053 - Appendix 1
A COVID-19 Vaccine Safety Surveillance Strategy for New Zealand
providing a significant baseline of safety reassurance. This, together with safety surveillance data
collectively from other countries accounting for probable substantial uptake of vaccine ahead of NZ will
provide a further measure of safety reassurance. Despite this, the accelerated development and safety
study windows and the diversity of vaccine platforms, the rapid pandemic deployment into population
characteristics and underlying conditions potentially not represented in the trials or roll-out elsewhere
requires that NZ undertake additional surveillance of hospital attendances for reassuring the safety of
the vaccine(s) in use.
It is critical that vaccinees who are hospitalised in a close temporal window following vaccination
(timing/duration dependant on the type of vaccine), or who develop an Adverse Event of Special
Interest (AESI), which are a subset of AEFI’s of particular concern, are carefully reviewed to determine
if the admission event may be related to the vaccine. This will further support the early identification of
AEFI’s of potential concern.
There is expected to be a resource limitation in being able to review every hospital admission to
determine if they had received a COVID-19 vaccine within a close temporal window. Whilst we could
1982
consider adopting similar approaches from the MeNZB MVS surveillance strategy of the early 2000’s
which reviewed every hospital attandance who had received a vaccine within the previous 7 days, there
are significant challenges to considering the MeNZB approach in the COVID-19 vaccine context:
Act
The MeNZB MVS hospital surveillance strategy was a highly resource intensive approach with
long lead times to training and preparation and focussed on a considerably smaller cohort of
vaccinees (sequential geographic rollout and <19 years) than is expected to be the case for
COVID-19 vaccine uptake. This would not be feasible for COVID-19 vaccines
The MVS approach was confined to 3 major hospitals manually reviewing daily/weekly patients
admission notes to determine those that met criteria (age/AESI/unusual events) who were then
cross checked with the NIR to identify those who had been vaccinated. The logistics of this for
Information
COVID-19 vaccines would be immense.
Manual review of admission notes was required because an ICD diagnostic code was only
assigned on discharge, such that if ICD codes were relied upon for case identification, an event
of interest could be missed for days or even weeks.
Official
Unlike the COVID-19 vaccines, the MeNZB vaccine had by comparison only limited Phase III
trials, relying on bridging to similar vaccine trials and rollout of related vaccines in other
the
countries. By the time NZ brings COVID-19 vaccines into NZ use, these vaccines will have
substantial Phase III safety data already alongside real-world rollout AEFI knowledge.
The key component of the MeNZB Hospital Surveillance Strategy revolved around analysing the AESI’s
or unusual events which were laboriously identified with great urgency due to the relative absence of
under
safety data by comparison to COVID-19 vaccine(s). A COVID-19 Hospital Surveillance Strategy can still
focus on identifying AESIs as a key component, but be less reliant on absolute real time event
identification.
The following components of a Hospital Surveillance Strategy for COVID-19 for NZ are possible:
Defining Adverse Events of Special Interest (AESI)
Global initiatives are currently underway to identify AESI’s and their associated case definitions. The
Released
CEPI organisation (Coalition for Epidemic Preparedness Innovation) has contracted the international
Brighton Collaboration to harmonize the safety assessment of COVID-19 vaccines via its Safety Platform
for Emergency Vaccines (SPEAC) project.10 New Zealand vaccinologists are participating in this
process, including through the Global Vaccine Safety Data Network project. The current list of AESI’s,
case definitions and related resources developed to date are included in Appendix 2. This list is likely to
be dynamic with the most current list/case definitions expected to be applied in analyses pertaining to
AESI’s. This list is expected to be a baseline standardised list that NZ surveillance will actively monitor.
Historical/background levels of AESI’s provide an important baseline from which to determine if
vaccine-related AESI’s contributes excess risk and is an activity that should be initiated in NZ. The WHO
Global Advisory Committee on Vaccine Safety have called for countries to prepare baseline rates of
AESIs prior to deploying COVID-19 vaccines.
25 September 2020
Michael Tatley – NZPhvC / University of Otago
Page
4 of
18
OIA H2026081053 - Appendix 1
A COVID-19 Vaccine Safety Surveillance Strategy for New Zealand
It will be important to ensure that the definitions of the AESI’s can be matched against relevant ICD
discharge codes or ICD code groups to enable interrogation to extract cases that meet the AESI
definition. An appropriate validation project should be completed to reassure that appropriate ICD
codes can be identified to support AESI case extraction.
Establishing historical baselines for AESIs
NZ can utilise the international list of AESIs to set up a monitoring system prior to the entry of vaccines
in the country so there is an established historical baseline of population prevalence of these defined
events.
Hospital Surveillance Focal Areas
Hospitalisation due to Adverse Events of Special Interest
All hospital attendances that result in an ICD code(s) that aligns with an AESI and regardless of the
patient’s vaccination status should be identified to support analytical comparisons of observed events
1982
against expected/historical levels and between vaccinated and unvaccinated individuals to identify
excess events potentially attributable to COVID-19 vaccination. A system supporting rapid regular
review/analysis (e.g. weekly/monthly) should be developed and implemented. Act
Capturing all potential hospital attendances with Adverse Events of Special Interest
Since ICD codes are only assigned on discharge, knowledge of AESI definitions should be promoted
amongst clinicians who should be encouraged to identify patients who meet these definitions and that
the discharge system ensures that an accurate ICD code is expeditiously assigned. A mechanism for
identifying patients who are admitted and managed as a possible AESI, but not yet discharged should be
established to include these patients in analyses of Hospital AESI;’s who might otherwise only be
identified much later.
Information
Hospitalisation due to other serious and/or unusual events
Clinicians should be encouraged to identify any serious and/or unusual events in vaccine recipients that
may help to inform new AESI’s. Cases with these criteria should be reviewed to determine the presence
of excess numbers, unusual demographic distribution, or an unusual clinical picture.
Official
Mortality monitoring
the
In order to further support the identification of all possible clinical outcomes of a serious nature that
may represent a potential association with the COVID-19 vaccine(s), close to real-time, review of the
Mortality Register will be a useful activity. A mechanism should be established to enable NHI data
linkage from the National Immunisation Register with the Mortality Register to identify through
under
electronic matching, those deaths that have occurred within 90 days following COVID-19 vaccination.
A weekly/monthly review of the matches should be reviewed by personnel with appropriate expertise
and advising those matches with AESI’s to an appropriately constituted Mortality/Clinical Review
Committee that should be established. The Mortality Review Committee’s role will be to determine the
presence of a potential pattern of association with vaccination, with reports of any findings of an
association to be added to the review of other safety findings.
Released
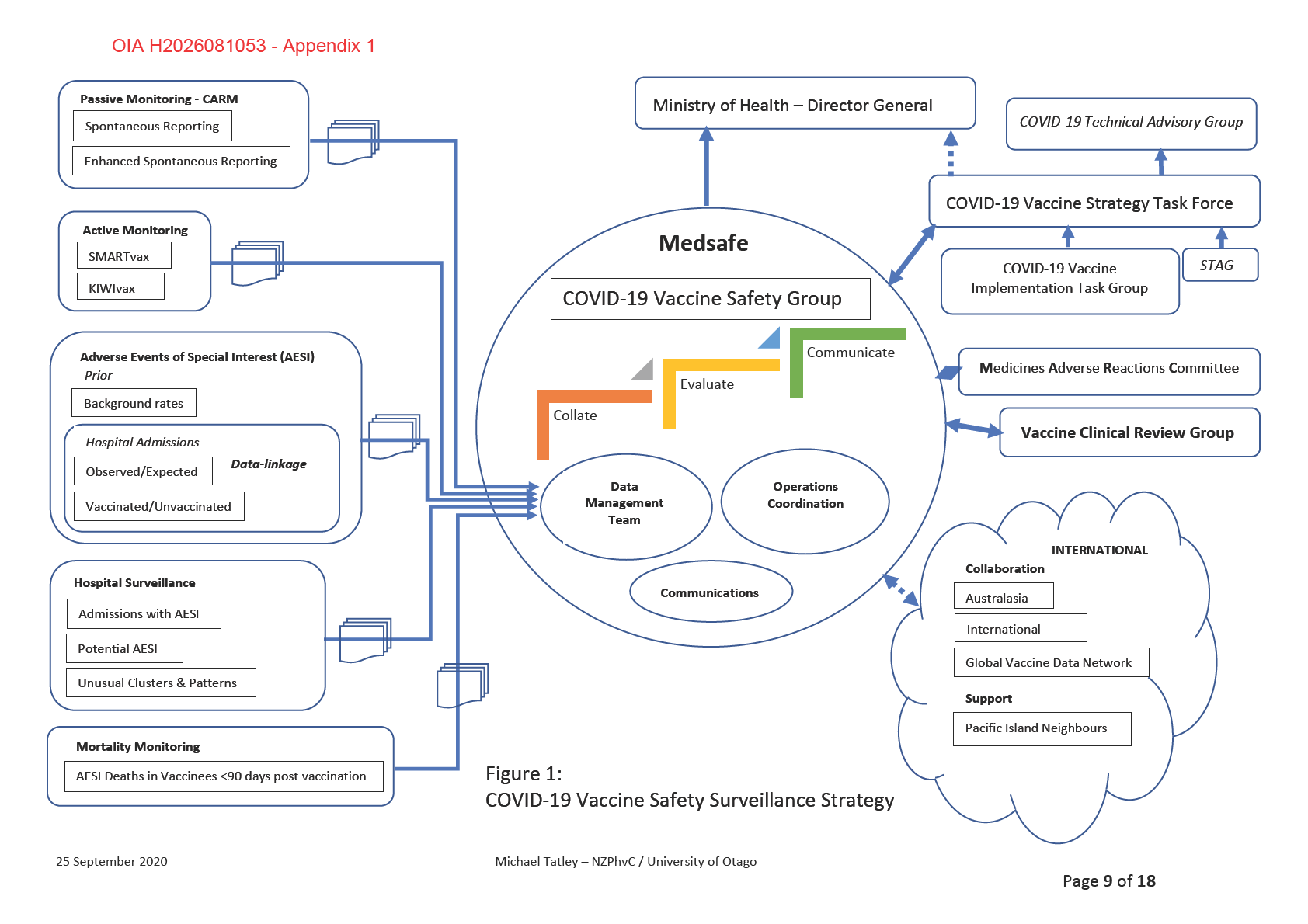
Vaccine safety surveillance oversight and coordination
In order to provide oversight and coordination across the diverse safety surveillance components, the
following structures are proposed: (Figure 1)
COVID-19 Vaccine Safety Surveillance Group
As Medsafe is the Regulatory body within the Ministry of Health legislated to regulate medicines
(including vaccines) which embraces safety aspects, there should be an appropriately skilled and
resourced group within Medsafe to provide leadership and coordination of the activities and
components specific to supporting vaccine safety surveillance elements/components. This COVID
Vaccine Safety Surveillance Group should ensure that networks with and access to people with
25 September 2020
Michael Tatley – NZPhvC / University of Otago
Page
5 of
18
OIA H2026081053 - Appendix 1
A COVID-19 Vaccine Safety Surveillance Strategy for New Zealand
appropriate skills and expertise are established within the Ministry of Health and/or nationally to
support its work. These diverse areas include Public Health/Infectious diseases, Epidemiology,
Biostatistics, Database management & analysis, Project management, Training of health personnel (to
support surveillance elements), Networking and Communication. Access to expertise and expert advice
in Clinical Medicine, Rare diseases, Immunology/Vaccinology or other disciplines of importance to
support analysis and review activities will also be required.
This group should serve as the hub towards which all relevant safety data is directed to and
accumulated to support analyses that will be used to inform findings of and advice in regard to the
safety of COVID-19 vaccines in use in New Zealand to support decision making and communication.
This group will interface with other relevant groups such as the newly constituted COVID-19 Strategy
TAG, COVID-19 Vaccine Strategy Group, Science and Technical Advisory Group (STAG), COVID -19
Vaccine Implementation Task Group and the Immunisation Program.
Analytical methods
Whilst descriptive statistics and frequentist approaches are likely to be key methods of
1982
characterising the vaccinated population and associated AEFI’s/AESI’s, strategies such as
illustrating observed versus expected numbers of events and risk interval analyses/person-
Act
time-at-risk and any other analytical approach is expected. Collaboration with international
partners to ensure harmonisation of methods will be important.
Data analysis, Networking and Reporting
Opportunity should be sought within the data management and analytical activities of the group
to network and/or collaborate with other experts, individuals or groups in order to strengthen
the ability to ensure that all opportunities are utilised to identify issues of safety concern and
provide appropriate communication. Expertise from within the New Zealand will include
academics/research groups in epidemiology, pharmacoepidemiology, vaccino
Information logy, as well as
expertise in Immunisation Advisory Centre (IMAC), the ESR. These groups may provide support
in communication or undertake independent, complimentary or collaborative research. Regular
reports and updates on findings should be produced supporting the science findings from
surveillance. These reports also add evidence of transparency and reassure public safety on the
Official
findings and rigour of the surveillance system.
International collaboration
the
Since all countries will be focused on identifying safety issues of concern of the COVID-19
vaccine and many other countries, groups and initiatives are underway, there will be beneficial
advantage through networking to identify and/or share findings. Opportunities and
mechanisms to engage in collaboration should be actively encouraged. Trans-Tasman
under
collaboration offers advantages due to the existing collegial connections, further strengthened
through the use in New Zealand of SMARTvax/KIWIvax, an NZ customised version of the
Australian SMARTvax/AusVaxSafety, provides an ideal platform to share/compare data using
an almost identical approach. Other international groups include the Global Vaccine Data
Network (GVDN), which is co-directed and coordinated from New Zealand as the host country.
The GVDN has 17 partner countries across the globe whose focus includes the development of
common data models as well as the collective expertise of many of the world’s foremost experts
Released
in vaccine safety and vaccine pharmacoepidemiology. NZ should also explore collegial
relationships with other research groups and initiatives in other countries including the
Coalition for Epidemic Preparedness Innovations (CEPI).11
25 September 2020
Michael Tatley – NZPhvC / University of Otago
Page
6 of
18
OIA H2026081053 - Appendix 1
A COVID-19 Vaccine Safety Surveillance Strategy for New Zealand
MARC – Providing Vaccine Safety Oversight
There is distinct advantage in utilising a group that is outside of Government such as the Medicines
Adverse Reactions Committee (MARC) to provide vaccine safety oversight and advice for the new-to-NZ
COVID-19 vaccine(s) that will be used on wide scale in NZ. This is especially important in the context of
the rapid development and clinical trial processes for the COVID-19 and the need to reassure the NZ
public and those that are vaccine hesitant that there is an objective scientific review of the safety
evidence of the COVID-19 vaccines that is independent of Government and political influence. MARC is
constituted with experts in diverse clinical fields providing advice to Medsafe based on clinical
evaluation of safety information presented to it for consideration. It may be appropriate to enhance the
spectrum of expert advisors to MARC to specifically support COVID-19 vaccine review for the duration
that this may be necessary. This group can review all safety-related surveillance data, request data and
provide expert independent advice on the safety of COVID-19 vaccines in use, including the ability to
recommend the suspension of any vaccine in use should its findings identify issues of sufficient gravity
to warrant such an action to avoid excess vaccine-associated morbidity of concern or mortality.
1982
COVID-19 Vaccine Clinical Review Group
It will be essential to have access to clinical expertise to support the review of complex, serious or
Act
severe AEFI and those AESI that are attributed to COVID-19 vaccination to determine or asses their
causal association to inform vaccine safety evaluation decision-making and advice. Currently a group
with such a function for vaccines in current use exists – an informally constituted group of clinicians,
pharmacovigilance and regulatory personnel - the Vaccine Safety Expert Advisory Group (VSEAG). This
group of peers provides a forum for consideration and discussion of cases of clinical importance, or
complexity, their potential further investigation or management, causal association and implications for
the vaccinee or use of the vaccine. For COVID-19 vaccines, due to their new technology platforms and
COVID-19 disease profiles, an appropriate group should be established, which could include
Information
supplementing the VSEAG and formalising it, or establishing a new dedicated COVID-19 Clinical Review
Group.
Supporting Pacific Island Neighbours
Official
Whilst the focus of a COVID-19 Vaccine Safety Surveillance Strategy is targeted on developing and
implementing a system to ensure the safe use of new vaccines for New Zealanders, our Pacific Island
neighbours have less well developed and resource
the d health systems. Consequently, they may be less able
to establish a vaccine safety surveillance system. NZ has expressed its commitment to support access
to COVID-19 vaccines for the South Pacific12 and hence there is a high likelihood that the same or
similar COVID-19 vaccines will be delivered to our Pacific neighbours. NZ would be in a good position
to assist or facilitate Pacific Island Count
under ries in their vaccine safety surveillance, with use of many of the
suggested approaches listed above.
This could be COVID-19 Vaccine Safety Surveillance-specific, or form part of a wider initiative around
Medicine Security, including some existing early initiatives on strengthening Pharmacovigilance of
Vaccines in Immunisation Programmes and/or Medicines used in these countries. Collaboration with
the WHO’s Western Pacific Regional Office and its networks should also be encouraged to ensure that
any NZ vaccine safety surveillance contribution is complementary to and in alignment with Regional
Released
strategies.
The NZPhvC/Otago University has been invited to participate in recent WHO Western Pacific Regional
Office (WHO-WPRO) National Regulatory Authority (NRA) workshops since 2018 on Health Systems
Strengthening initiatives for the region with special focus on the Pacific Island Countries. A Concept
Proposal on Strengthening Pharmacovigilance Systems as a component in support of broader Medicines
regulatory Strengthening has gained the interest of WHO-WPRO, Pacific Island Countries (PIC) and
MFAT. The NZPhvC/Otago University was invited to present a concept proposal for COVID-19 Vaccine
Safety Surveillance for the PIC’s at a September 2020 WHO-WPRO NRA meeting. This proposal centered
around introducing and establishing Passive Monitoring systems with the support of NZ expertise in
Pharmacovigilance/ Vaccine Safety Surveillance based on the model of Health Systems Strengthening
25 September 2020
Michael Tatley – NZPhvC / University of Otago
Page
7 of
18
OIA H2026081053 - Appendix 1
A COVID-19 Vaccine Safety Surveillance Strategy for New Zealand
proposal referred to earlier. WHO-WPRO has arranged meetings, workshops and possible
implementation strategies and pathways scheduled for November 2020. Through this initiative a
pathway to support PIC’s and further inform Regional and Global knowledge on the safety of COVOD-19
vaccines will have been established.
Critical Practical Considerations for Developing a COVID-19 Vaccine Safety Surveillance Strategy
• Lead times and infrastructural obstacles
The MeNZB MVS setting-up in the early 2000’s illustrated that long lead times were
required to develop and implement its operational components. This was partly due to
its novel nature and complexity of establishing the components, but also due to
inefficiencies in inter departmental co-operation as well as in resolving legislative and
regulatory obstacles to enable the implementation of systems. Initiatives for developing
and finalising a NZ COVID-19 Vaccine Safety Surveillance Strategy therefore need to
commence urgently to allow sufficient time to address challenges that will inevit
1982ably
present.
• Adequate resourcing
Act
The elements presented in this proposal, or any COVID-19 Vaccine Safety Surveillance
Strategy, cannot be successfully undertaken as part of ongoing service delivery or
operational activities. Not only would any strategy require funding/resourcing of at
least some new elements that did not previously exist, or will require resources to be
redirected from other areas that in turn would need to be filled to ensure service
continuity, but some components will face increased workload that will need additional
funding/resource support. An example of the latter pertains to the passive monitoring
Information
by CARM for the MeNZB that resulted in a more than 2-fold increase in report workload
in a system already operating at the limits of its capacity.
• Institutional knowledge and National Expertise
Although the members of the MeNZB MVS team were unfortunately disbanded around
Official
2007/8 when the MeNZB epidemic had declined, some key members of this group are
still accessible working in other areas of the Ministry of Health. They represent an
immense wealth of institutiona
the l and practical knowledge on developing, implementing
and addressing the operational challenges that were overcome and could be avoided, or
provide helpful advice for a COVID-19 vaccine strategy. Key members of this MVS team,
or at least the Director of the MVS, would be of indispensable value in being included in
developing a COVID-19 Va
under ccine Safety Surveillance Strategy, the Strategy infrastructure,
or at the very least in an advisory role.
National experts or groups with expertise in areas that can be of value in supporting the
elements of an NZ COVID-19 Vaccine Safety Surveillance Strategy should be identified
and invited to contribute individually, institutionally, organisationally, or in
collaboration with other groups. These include expertise areas such as Epidemiology,
Pharmacoepidem
Released iology, Vaccinology, Rare and Infectious Diseases etc.
25 September 2020
Michael Tatley – NZPhvC / University of Otago
Page
8 of
18
1982
Act
Information
Official
the
under
Released
OIA H2026081053 - Appendix 1
References
1. Holst J, Oster P, Arnold R, et al. Vaccines against meningococcal serogroup B disease containing outer
membrane vesicles (OMV): lessons from past programs and implications for the future.
Hum Vaccin
Immunother 2013;9(6):1241-53. doi: 10.4161/hv.24129 [published Online First: 2013/07/17]
2. McNicholas A, Galloway Y, Stehr-Green P, et al. Post-marketing safety monitoring of a new group B
meningococcal vaccine in New Zealand, 2004-2006.
Hum Vaccin 2007;3(5):196-204. doi:
10.4161/hv.3.5.4458 [published Online First: 2007/07/31]
3. Tatley MV, Kunac DL, McNicholas A, et al. The Intensive Vaccines Monitoring Programme (IVMP): an
electronic system to monitor vaccine safety in New Zealand.
Vaccine 2008;26(22):2746-52. doi:
10.1016/j.vaccine.2008.03.017 [published Online First: 2008/04/24]
4. Kunac DL, Harrison-Woolrych M, Tatley MV. Pharmacovigilance in New Zealand: the role of the New
Zealand Pharmacovigilance Centre in facilitating safer medicines use.
N Z Med J 2008;121(1283):76-
89. [published Online First: 2008/10/09]
5. NZHIT. Overview of the software applications landscape across New Zealand’s health system prepared
1982
for the NZ Health & Disability Sector Review Panel 2019.
6. Glover C, Crawford N, Leeb A, et al. Active SMS-based surveillance of adverse events following
immunisation with influenza and pertussis-containing vaccines in Australian pregnant w
Act omen using
AusVaxSafety.
Vaccine 2020 doi: 10.1016/j.vaccine.2020.04.056 [published Online First: 2020/06/06]
7. Leeb A, Regan AK, Peters IJ, et al. Using automated text messages to monitor adverse events following
immunisation in general practice.
Med J Aust 2014;200(7):416-8. doi: 10.5694/mja13.11166
[published Online First: 2014/05/06]
8. Regan AK, Blyth CC, Mak DB, et al. Using SMS to monitor adverse events following trivalent influenza
vaccination in pregnant women.
Aust N Z J Obstet Gynaecol 2014;54(6):522-8. doi: 10.1111/ajo.12266
[published Online First: 2014/10/14]
9. Hughes C. Smartphone users in New Zealand as of 2019: Statista.com; 2020 [Available from:
Information
https://www.statista.com/statistics/680711/new-zealand-mobile-social-media-
penetration/#:~:text=Mobile%20phone%20market,country%20in%20the%20same%20year.
accessed 13 July 2020.
10. Law B, Sturkenboom M. D2. 3 priority list of adverse events of special interest: COVID-19.
SPEAC 2020
11. Coalition_for_Epidemic_Preparedness_Innovation_(CEPI). Coalition for Epidemic Preparedness
Official
Inniovation 2020 [Available from: https://cepi.net/ accessed 17 September 2020.
12. Ministry_of_Health. COVID-19: Vaccine strategy 2020 [updated 03 September 2020. Available from:
https://www.health.govt.nz/our-work/diseases-and-conditions/covid-19-novel-coronavirus/covid-
the
19-current-situation/covid-19-vaccine-strategy accessed 09 September 2020.
13. World Health O. Global manual on surveillance of adverse events following immunization. 2016
update ed: World Health Organization 2014:109 p.
14. World Health Organization.Department of Immunization VaB. Global vaccine safety blueprint.
under
Geneva2012.
15. Westphal DW, Williams SA, Leeb A, et al. Continuous active surveillance of adverse events following
immunisation using SMS technology.
Vaccine 2016;34(29):3350-5. doi:
10.1016/j.vaccine.2016.05.015 [published Online First: 2016/05/22]
16. Ateudjieu J, Stoll B, Nguefack-Tsague G, et al. Vaccines safety; effect of supervision or SMS on reporting
rates of adverse events following immunization (AEFI) with meningitis vaccine (MenAfriVac): a
randomized controlled trial.
Vaccine 2014;32(43):5662-8. doi: 10.1016/j.vaccine.2014.08.012
Released
[published Online First: 2014/08/28]
17. Cashman P, Moberley S, Dalton C, et al. Vaxtracker: Active on-line surveillance for adverse events
following inactivated influenza vaccine in children.
Vaccine 2014;32(42):5503-8. doi:
10.1016/j.vaccine.2014.07.061 [published Online First: 2014/08/01]
18. AusVaxSafety. AusVaxSafety 2020 [Available from: http://www.ncirs.org.au/our-work/ausvaxsafety
accessed 17 September 2020.
25 September 2020
Michael Tatley – NZPhvC Univ of Otago
Page
10 of
18
OIA H2026081053 - Appendix 1
Appendix 1
The KIWIvax smartphone based technology to monitor AEFI’s
INTRODUCTION
Immunisation is one of the most impactful, effective and successful public health interventions
worldwide. Immunisations have saved lives and maintained the health of populations through
protection from vaccine preventable diseases. Vaccines in use today have excellent safety
profiles, but occasionally Adverse Events Following Immunisation (AEFI) do occur.13 Most of
these AEFI are non-serious, mild and of short duration, but in rare instances serious AEFI’s
associated with significant health impacts have occurred. Whilst some of these very rare serious
effects have been due to the vaccine, most on further review are found to be coincidental. Since
vaccines are administered to healthy individuals, especially very young children and often in
1982
regions where the diseases they are preventing have become rare or unknown, the public
tolerance for any AEFI is extremely low. The family’s or vaccinee’s fear of the potential for an
AEFI can result in reluctance or hesitancy about vaccination and compounded by
Act
misinformation, create confusion and anxiety which can affect vaccination uptake. This can lead
to unnecessary susceptibility to vaccine preventable diseases that threaten the lives of
individuals, or more widely, the community or country.
Surveillance and monitoring of AEFI’s is therefore a crucial component of National
Immunisation Programme strategy.14 15 Immunisation programmes need to be backed by
reliable safety monitoring measures and to be able to respond to public concerns about vaccine
safety. AEFI monitoring as a component of pharmacovigilance provides information on
Information
prevailing patterns of AEFIs, most of which are expected transient local or systemic immune
responses that manifest clinically in a small proportion of vaccine recipients. AEFI monitoring
also can identify serious, unexpected or unusual AEFIs, all of which can be followed up and
investigated to identify whether they are attributed to the vaccine and paving the way for
identification of potential safety issues and enabling changes in practice as rapidly as possible.
Official
AEFI monitoring informs and supports ongoing Benefit-Risk evaluation of all vaccines and
provides reassurance to the public that the safety of vaccines has great importance, translating
the
to maintaining public trust and confidence in the uptake of vaccines.
New Zealand (NZ) has had a long and successful history of AEFI monitoring as a component of
its Pharmacovigilance system.4 This is provided through the Centre for Adverse Reactions
Monitoring (CARM) within the New Zealand Pharmacovigilance Centre (NZPhvC) at the
under
University of Otago, which delivers national pharmacovigilance services for the Ministry of
Health. NZ AEFI monitoring has been passive (i.e. reliant on voluntary reporting) and is subject
to underreporting. In addition to underreporting, passive reporting systems are further limited
by reporting biases and the lack of denominators. To overcome this, at the time of introducing
the NZ-specific MeNZB vaccine in 2004, NZ introduced a novel Intensive Vaccine Monitoring
Programme (IVMP).3 This included an active monitoring system that involved an automated
Released
system that extracted vaccination event details from selected Primary Care medical practice
Practice Management Systems (PMS) as well as extracting all vaccinee visits to the medical
practice for a 6-week period post-vaccination. This enabled the construction of a post-vaccine
event profile. The IVMP was a resource intensive system, not sustainable for long term ongoing
monitoring or the monitoring of multiple vaccines. Although Web-based and Smartphone AEFI
reporting Apps were brought into use by the Pharmacovigilance system in subsequent years,
they remained subject to underreporting, bias and in particular vaccinee awareness that a post-
vaccination safety monitoring system was in place.
25 September 2020
Michael Tatley – NZPhvC Univ of Otago
Page
11 of
18
OIA H2026081053 - Appendix 1
Recent international approaches to improve ease of reporting have included the use of SMS
smartphone technology.7 8 15-17 This approach sends an SMS message to the vaccinee/caregiver
from the PMS from the medical practice where the vaccination was administered. The message
which is sent a few days after the vaccination event, enquires whether there had been an
adverse event of any type after the vaccination by simply requiring a ‘Yes’ or ‘No’. In the event of
a ‘Yes’ the vaccinee is invited to complete a survey by responding to a series of targeted
questions/options about the nature of the AEFI. Responses are recorded in a database and since
the denominators known, rates of AEFI events can be determined. Systems also include options
to report further details relating to events that are of a more serious nature and enable direct
follow-up with the vaccinee to establish further detail. These SMS systems offer advantages in
reaching the entire vaccine cohort, supporting the automated population of AEFI databases for
analysis and can free-up resources that can then be more usefully directed to follow-up serious,
clinically significant or unusual AEFI of concern or interest. More than 80% of NZ’ers own a
Smartphone.9 Utilizing this technology will enable far wider reach than the current modalities of
reporting which are limited to the conscious decision to report an AEFI online or to a health
1982
provider for onward notification to the NZPhvC.
Adopting SMS smartphone AEFI reporting provides opportunities to achieve greater efficiencies
Act
in resource utilisation and further improve AEFI surveillance. This is not only important for the
monitoring of current routine childhood, seasonal influenza and travel vaccines in a social
environment that is increasingly influenced by vaccine sceptics, but also provides a firm
foundation on which to monitor the COVID-19 vaccines on the horizon which will have a very
uncertain safety profile. There is an urgency to set up the functionality of such a system prior to
the arrival of expected COVID-19 vaccine/s
A SMS smartphone-based monitoring system, SMARTvax, which was initially developed for a
Information
medical practice group in Perth, Australia in 2010 to monitor adverse events following the
seasonal influenza vaccine7 achieved great success and has gone on to become the core
technology of the nationwide AusVaxSafety implemented in all Australian states and
territories.8 17 18 The utility of SMARTvax as the SMS smartphone interface tool and
AusVaxSafety as the overall system analysing the database repository that SMARTvax
Official
populates, has repeatedly demonstrated its ability to support diverse vaccine safety studies.9 11
In collaboration with the developers of SMARTvax the NZPhvC has initiated the customisation
the
and development of a NZ-specific version of SMARTvax and is working alongside the
Immunization Advisory Centre (IMAC) to optimised ensure optimized and culturally sensitive
system interfaces. . SMARTvax is known to be compatible with multiple PMS software in use in
Australia including Medtech32, the PMS with the largest share in NZ at 80%.5
under
The endpoint will be an NZ SMS smartphone AEFI technology tool supporting ‘KIWIvax’, an NZ
vaccine monitoring approach that would have been demonstrated to be able to interact with the
most widely used practice management software application in NZ (Medtech32) and ready for
piloting to support NZ AEFI monitoring for any of the national schedule vaccines, and eventually
a COVID19 vaccine rollout.
Proposed Operation
Released
KIWIvax system will use the New Zealand-customised version of the SMARTvax tool to interface
with the vaccinee/caregiver stimulated by the recording of a vaccine administration in the
Practice Management System. The information generated from the interaction will be messaged
to the medical practice’s PMS and uploaded to the database in the New Zealand
Pharmacovigilance Centre (New Zealand’s National Centre for the monitoring of adverse
reactions) and form part of the national dataset of AEFI’s. An anonymised version of the data
will be stored on a cloud-based server, which will also hold the software to produce the
analytical outputs and dashboard graphics which will form the basis of KIWIvax, a new
dynamic, near real-time vaccine monitoring and surveillance system.
25 September 2020
Michael Tatley – NZPhvC Univ of Otago
Page
12 of
18
OIA H2026081053 - Appendix 1
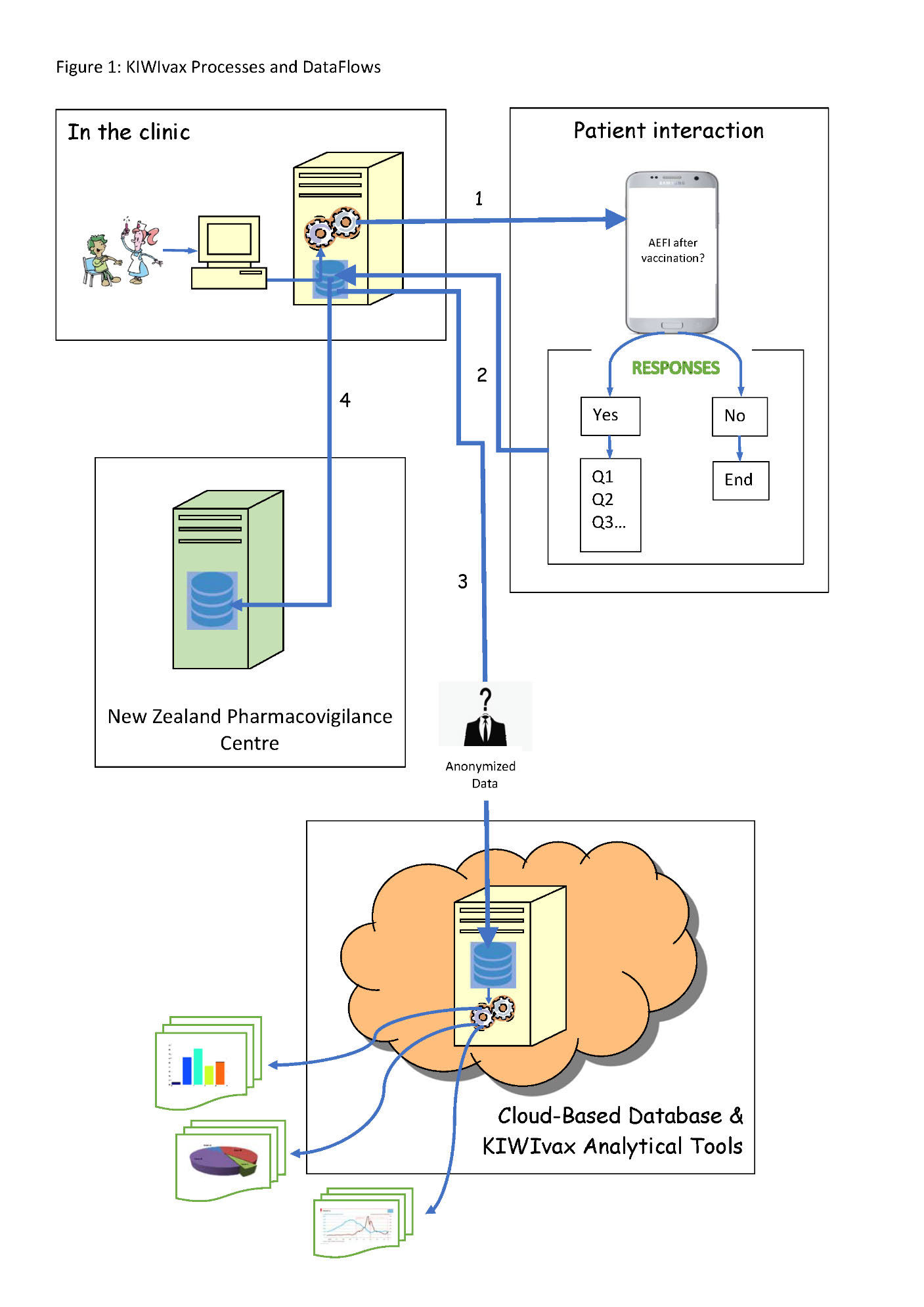
The KIWIvax System: (Figure 1)
• SMARTvax will be installed on individual medical practices Practice Management Systems
(PMS). Permission and approval will be required by each medical practice.
• Registering of a vaccine administration for a patient in the PMS will at 3 days post-vaccination
generate a message to the vaccinee/caregiver with a standard text enquiring if any AEFI has
occurred in the period since the vaccination.
• The message will offer 3 possible responses:
• ‘YES’ - this will prompt an invitation to a survey with a series of questions and options
to choose common AEFI’s, some of which will open expandable trees, questions around
severity as well as options to provide free text for more detail, or to notify unlisted
AEFI’s. An optional will also be provided to contact the NZPhvC to discuss the AEFI’s
with the clinician.
• ‘NO’ - will acknowledge that no event occurred and that in the event of a further
vaccination there will be further contact.
1982
• ‘OPT OUT’ - - will terminate further interaction with an appropriate text message
• All SMS’s will form the basis of a denominator for analysis with the various AEFI responses
Act
supporting the numerator.
• All data from the interaction will be stored in three locations:
• on the database of the patient’s medical practice from which the SMS originated
• an upload from the medical practice database:
- onto an NZPhvC server in line with privacy requirements and subject to the
same data security provisions operating in the NZPhvC.
- of anonymised data to a Cloud-based server housing the analytical software to
enable national analyses.
Information
• Data on the Cloud-based server will be analysed to produce NZ-appropriate analysis and
graphics that will form the basis of KIWIvax.
SMARTvax development to date
• A collaboration has been established between the NZPhvC
Official and the SMARTvax developers to
customise SMARTvax for NZ.
• Confirmed that SMARTvax can interrogate and link to the New Zealand Medtech32 data
the
libraries and identifiers.
• Identified additional NZ-specific data fields that SMARTvax must interrogate, refer to, or
incorporate for NZ monitoring.
• Verified that the SMARTvax customisations to initiate SMS messaging and return responses
under
using mobile numbers identified from data fields in a test version of Medtech32 are functional
SMARTvax/KIWIvax development in progress
• Configuration of SMARTvax to upload SMS data interactions from the medical practice PMS to
the NZPhvC database
• Configuration of the NZPhvC database to receive incoming uploads from the medical practice
and develop protocols fo
Released r related data management
• Establishing an NZ Cloud-based database to receive and store the data received from the
SMARTvax tool interrogation/interaction generated from the medical practice.
• Customisation of the NZ Cloud-based database interrogation analysis and statistical
output/dashboards that will become the KIWIvax utility.
• Beta-testing the functionality of the technological tools in a real world medical practice
environment for a small number of vaccinees.
• Establishing collaboration with Māori Iwi and Runanga to ensure that the tool and its
operations and intended interfaces with vaccinees and providers are culturally appropriate
through involvement at appropriate stages in the development of KIWIvax.
25 September 2020
Michael Tatley – NZPhvC Univ of Otago
Page
13 of
18
OIA H2026081053 - Appendix 1
• Consideration of ethical aspects that need to be addressed to inform a New Zealand ethics
approval in anticipation of a working customised SMARTvax and KIWvax technology being
finalised. Two key dimensions of ethics considerations are those of (a) the ethics of
interrogating patient level details from the medical practices PMS required by SMARTvax and
(b) vaccinee/caregiver opt in/opt out considerations.
• Plan and implement a trial of the KIWIvax system in a real-world environment in a PHO
setting for a 3-6 month period to evaluate its functionality, acceptability and utility in
supporting vaccine safety surveillance.
• Consider requirements, workload and resource implications for the possible integration of
SMARTvax into other non- Medtech32 practice management systems.
1982
Act
Information
Official
the
under
Released
25 September 2020
Michael Tatley – NZPhvC Univ of Otago
Page
14 of
18
OIA H2026081053 - Appendix 1
1982
Act
Information
Official
the
under
Released
25 September 2020
Michael Tatley – NZPhvC Univ of Otago
Page
15 of
18
OIA H2026081053 - Appendix 1
References
1. World Health O. Global manual on surveillance of adverse events following immunization. 2016 update
ed: World Health Organization 2014:109 p.
2. World Health Organization.Department of Immunization VaB. Global vaccine safety blueprint.
Geneva2012.
3. Westphal DW, Williams SA, Leeb A, et al. Continuous active surveillance of adverse events following
immunisation using SMS technology.
Vaccine 2016;34(29):3350-5. doi:
10.1016/j.vaccine.2016.05.015 [published Online First: 2016/05/22]
4. Kunac DL, Harrison-Woolrych M, Tatley MV. Pharmacovigilance in New Zealand: the role of the New
Zealand Pharmacovigilance Centre in facilitating safer medicines use.
N Z Med J 2008;121(1283):76-
89. [published Online First: 2008/10/09]
5. Tatley MV, Kunac DL, McNicholas A, et al. The Intensive Vaccines Monitoring Programme (IVMP): an
electronic system to monitor vaccine safety in New Zealand.
Vaccine 2008;26(22):2746-52. doi:
10.1016/j.vaccine.2008.03.017 [published Online First: 2008/04/24]
6. Ateudjieu J, Stoll B, Nguefack-Tsague G, et al. Vaccines safety; effect of supervision or SMS on reporting
1982
rates of adverse events following immunization (AEFI) with meningitis vaccine (MenAfriVac): a
randomized controlled trial.
Vaccine 2014;32(43):5662-8. doi: 10.1016/j.vaccine.2014.08.012
[published Online First: 2014/08/28]
Act
7. Cashman P, Moberley S, Dalton C, et al. Vaxtracker: Active on-line surveillance for adverse events
following inactivated influenza vaccine in children.
Vaccine 2014;32(42):5503-8. doi:
10.1016/j.vaccine.2014.07.061 [published Online First: 2014/08/01]
8. Leeb A, Regan AK, Peters IJ, et al. Using automated text messages to monitor adverse events following
immunisation in general practice.
Med J Aust 2014;200(7):416-8. doi: 10.5694/mja13.11166
[published Online First: 2014/05/06]
9. Regan AK, Blyth CC, Mak DB, et al. Using SMS to monitor adverse events following trivalent influenza
vaccination in pregnant women.
Aust N Z J Obstet Gynaecol 2014;54(6):522-8. doi: 10.1111/ajo.12266
Information
[published Online First: 2014/10/14]
10. Hughes C. Smartphone users in New Zealand as of 2019: Statista.com; 2020 [Available from:
https://www.statista.com/statistics/680711/new-zealand-mobile-social-media-
penetration/#:~:text=Mobile%20phone%20market,country%20in%20the%20same%20year.
accessed 13 July 2020.
Official
11. AusVaxSafety. AusVaxSafety- an NCIRS collaboration 2020 [Available from:
http://www.ausvaxsafety.org.au/ accessed 15 July 2020.
12. NZHIT. Overview of the software applications landscape across New Zealand’s health system
the
prepared for the NZ Health & Disability Sector Review Panel 2019.
13. Nowlan M, Willing E, Turner N. Influences and policies that affect immunisation coverage-a summary
review of literature.
N Z Med J 2019;132(1501):79-88. [published Online First: 2019/08/30]
under
Released
25 September 2020
Michael Tatley – NZPhvC Univ of Otago
Page
16 of
18
OIA H2026081053 - Appendix 1
Appendix 2
COVID-19 vaccine Adverse Events of Special Interest
The rapid development of COVID-19 vaccine candidates and accelerated clinical trial timelines
and relatively limited sample sizes exposes risks in being able to fully reassure the safety of
these vaccines.1,2 This highlights the critical importance of vaccine safety surveillance strategies
to detect both common and rarer post-vaccination adverse events in the wider real-world
exposed population. This is all the more critical since no DNA or RNA vaccines have been
licensed in humans to date2 adding further weight to the need to ensure that the AEFI
monitoring for these vaccines is as comprehensive as possible. Potential safety concerns include
vaccine-mediated disease enhancement syndrome (observed with other RSV vaccines)2, as well
as other events that may be potentially attributable to the characteristics of the vaccine, the
nature of the immune response to the vaccine antigens, or even the disease itself. These events
form a distinct subset of AEFI’s referred to as Adverse Events of Special Interest (AESI’s).
1982
An Adverse Events of Special Interest is defined as:
‘An adverse event of special interest (serious or non-serious) is one of scientific and medical
Act
concern specific to the sponsors product or program, for which ongoing monitoring and
rapid communication by the investigator to the sponsor could be appropriate. Such an
event might require further investigation order to characterise and understand it.
Depending on the nature of the event, rapid communication by the trial sponsor to other
parties (e.g., regulators) but also be warranted.’3
Discussions and consensus groups have highlighted the importance of considering COVID-19
disease enhancement syndrome and the need to identify AESI’s. Initiatives are currently
Information
underway through SPEAC (Safety Platform for Emergency Vaccines) funded by CEPI4 (Coalition
for Epidemic Preparedness Innovations). SPEAC have developed a Priority List of Adverse
Events of Special Interest: COVID-19, organising candidate AESI’s in three groups:3
1. AESI relevant to a broad range of vaccines
Official
Neurologic
Generalized convulsion
Guil ain-Barré Syndrome (GBS)
the
Acute disseminated encephalomyelitis (ADEM)
Hematologic
Thrombocytopenia
Immunologic
Anaphylaxis
Vasculitides
under
Other
Serious local/systemic AEFI
2. AESI relevant to one or more specific COVID-19 vaccine platforms
Neurologic
Aseptic meningitis
Encephalitis / Encephalomyelitis
Released
Transverse myelitis
Immunologic
Arthritis
Other
Myocarditis
25 September 2020
Michael Tatley – NZPhvC Univ of Otago
Page
17 of
18
OIA H2026081053 - Appendix 1
3. AESI relevant to a specific target disease
Immunologic
Enhanced disease following immunization
Multisystem inflammatory syndrome in children
Respiratory
Acute respiratory distress syndrome (ARDS)
Cardiac
Acute cardiac injury including:
• Microangiopathy
• Heart failure and cardiogenic shock
• Stress cardiomyopathy
• Coronary artery disease
• Arrhythmia
• Myocarditis, pericarditis
Hematologic
Coagulation disorder
• Deep vein thrombosis
• Pulmonary embolus
• Cerebrovascular stroke
1982
• Limb ischemia
• Hemorrhagic disease
Act
Renal
Acute kidney injury
Gastrointestinal
Liver injury
Guil ain Barré Syndrome
Neurologic
Anosmia, ageusia
Meningoencephalitis
Chilblain-like lesions
Dermatologic
Single organ cutaneous vasculitis
Information
Erythema multiforme
References:
Official
1. Kochhar S, Salmon DA. Planning for COVID-19 vaccines safety surveillance.
Vaccine 2020;38(40):6194-
98. doi: 10.1016/j.vaccine.2020.07.013 [published Online First: 2020/07/10]
2. Lambert P-H, Ambrosino DM, Andersen SR, et al. Consensus summary report for CEPI/BC March 12-13,
the
2020 meeting: Assessment of risk of disease enhancement with COVID-19 vaccines.
Vaccine
2020;38(31):4783-91. doi: 10.1016/j.vaccine.2020.05.064 [published Online First: 2020/05/25]
3. Law B, Sturkenboom M. D2. 3 priority list of adverse events of special interest: COVID-19.
SPEAC 2020
4. Coalition_for_Epidemic_Preparedness_Innovation_(CEPI). Coalition for Epidemic Preparedness
under
Inniovation 2020 [Available from: https://cepi.net/ accessed 17 September 2020
Released
25 September 2020
Michael Tatley – NZPhvC Univ of Otago
Page
18 of
18