Released under the Official Information Act 1982
Version 5.01
25 March 2026
VACCINATION
TREATMENT PROTOCOLS
Approval Details
This publication is issued under the authority of:
SIGNED ON ORIGINAL
Version 5.01
LTCOL RJ Duncan
Date: 25 March 2026
Chief Medical Officer
1
link to page 2 link to page 4 link to page 4 link to page 4 link to page 4 link to page 4 link to page 4 link to page 4 link to page 5 link to page 5 link to page 5 link to page 5 link to page 5 link to page 6 link to page 7 link to page 7 link to page 7 link to page 8 link to page 8 link to page 8 link to page 8 link to page 8 link to page 9 link to page 9 link to page 9 link to page 9 link to page 9 link to page 13 link to page 14 link to page 18 link to page 21 link to page 24 link to page 27 link to page 29 link to page 33 link to page 34 link to page 37 link to page 39 link to page 41 link to page 43 link to page 45 link to page 47 link to page 50 link to page 52 link to page 54 link to page 57
Released under the Official Information Act 1982
Version 5.01
25 March 2026
CONTENTS
CONTENTS ................................................................................................................................................................... 2
Specifications of the Vaccination Treatment Protocols ................................................................................................ 4
Purpose of the Vaccination Treatment Protocols........................................................................................................... 4
Scope ........................................................................................................................................................................... 4
Authority of the Issuer .................................................................................................................................................. 4
Conflict ......................................................................................................................................................................... 4
Review ......................................................................................................................................................................... 4
Audit ............................................................................................................................................................................ 4
NZDF VTP approved vaccines ........................................................................................................................................ 5
Application ................................................................................................................................................................... 5
Patients who qualify for care under the VTP .............................................................................................................. 5
Authorised VTP Users ............................................................................................................................................... 5
Authority for vaccination administration ....................................................................................................................... 5
Administration process ................................................................................................................................................. 6
Precautions .................................................................................................................................................................. 7
Consent ........................................................................................................................................................................ 7
Section 29 Medicines .................................................................................................................................................... 7
Off-label use ................................................................................................................................................................. 8
Site of administration ................................................................................................................................................... 8
Simultaneous live vaccines............................................................................................................................................ 8
Stand-down period ....................................................................................................................................................... 8
Adverse reactions ......................................................................................................................................................... 8
Variance in regime ........................................................................................................................................................ 9
Delayed completion of course ...................................................................................................................................... 9
High-risk vaccines ......................................................................................................................................................... 9
Recording vaccinations ................................................................................................................................................. 9
Vaccine prescription format .......................................................................................................................................... 9
Vaccine MSOs: BASELINE PROGRAMME .................................................................................................................... 13
COVID-19 Vaccine ....................................................................................................................................................... 14
Hepatitis A Vaccine ..................................................................................................................................................... 18
Hepatitis B Vaccine ..................................................................................................................................................... 21
Measles, Mumps and Rubella Vaccine......................................................................................................................... 24
Poliomyelitis Vaccine .................................................................................................................................................. 27
Tetanus-Diphtheria-Pertussis Vaccine (Tdap) .............................................................................................................. 29
Vaccine MSOs: ENHANCED PROGRAMME .................................................................................................................. 33
Cholera Vaccine .......................................................................................................................................................... 34
Dengue Disease Vaccine ............................................................................................................................................. 37
Herpes (Varicella) Zoster Vaccine ................................................................................................................................ 39
Human Papilloma Virus Vaccine .................................................................................................................................. 41
Influenza Vaccine........................................................................................................................................................ 43
Japanese Encephalitis Vaccine (Primary option) .......................................................................................................... 45
Japanese Encephalitis Vaccine (Alternative option) ..................................................................................................... 47
Meningococcal A, C, W-135 and Y Vaccine .................................................................................................................. 50
Meningococcal B Vaccine............................................................................................................................................ 52
Rabies Vaccine ............................................................................................................................................................ 54
Tick Borne Encephalitis (TBE) Vaccine ......................................................................................................................... 57
2
link to page 60 link to page 62 link to page 63 link to page 65
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Typhoid Vaccine ......................................................................................................................................................... 60
Other MSOs ............................................................................................................................................................... 62
Adrenaline .................................................................................................................................................................. 63
Record of Amendments ............................................................................................................................................. 65
3
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Specifications of the Vaccination Treatment Protocols
Purpose of the Vaccination Treatment Protocols
1.
The purpose of this Vaccination Treatment Protocols (VTP) is to authorise New Zealand
Defence Force (NZDF) credentialled and authorised healthcare personnel (NZDF Vaccinators: see
para 19 for definition) who are not
medical practitioners, to administer vaccines, in order to deliver
timely and clinically appropriate pharmaceutical treatments to NZDF personnel, and in some
circumstances non-NZDF personnel, in the absence of an NZDF, or other, affirmed prescriber.
2.
The VTP is a legal Medicine Standing Order in accordance with th
e Medicines Act 1981 and the
Medicines (Standing Orders) Regulations 2002.
Scope
3.
The VTP scope is in accordance with
DHR 13 NZDF Healthcare Providers’ Delegated Scopes of
Practice, Part 4, Chapters 1 and 2.
4.
The VTP applies to NZDF personnel employed to provide health support to NZDF-directed
outputs and who have an authority to practice issued by the Chief Medical Officer to administer
specific medications to NZDF and Foreign Nations’ uniformed personnel under that authority to
practice.
Authority of the Issuer
5.
The VTP is issued by the Chief Medical Officer (the Issuer), under the delegated authority of the
Surgeon General and
Defence Force Order (DFO) 18 Defence Health.
6.
The original copies of all medicine prescriptions are signed by th
e Issuer and held in the
Defence Health Directorate.
Conflict
7.
The VTP is not to be construed as prevailing over any relevant Act of Parliament, or regulations
made under it, or any Defence Force Order.
8.
Any conflict between the VTP and any other orders, rules, instructions or procedures issued
within the NZDF should be reported to the Issuer immediately.
Review
9.
The VTP is to be reviewed and reissued annually (including the individual medicine
prescriptions). The reissued VTP must be re-published prior to the expiry of the previous VTP.
10. The VTP applies until it is replaced, in part or whole, by a new order or until it is cancelled in
writing by the Issuer.
11. Amendments will be made and promulgated, if identified during the annual review or at any
other time and approved by the Issuer.
12. VTP review process is outlined in
DHR 13, Part 1
Treatment Protocols.
Audit
13. The use of the VTP is to be audited annually, in accordance with
DHR 13, Parts 1 and 4, to
ensure compliance with the VTP direction. Corrective actions will be taken where issues have been
identified during the audit.
4
Released under the Official Information Act 1982
Version 5.01
25 March 2026
14. A representative sample of VTP encounters, not requiring
countersignature must be reviewed
monthly to ensure compliance with the VTP.
15. The VTP audit process is outlined in DHR 13, Part 1.
NZDF VTP approved vaccines
16. All vaccines administered through the VTP are listed in the
Defence Medicines List (DML). Only vaccines included in the VTP can be administered by NZDF Vaccinators under the authority of
the VTP. Vaccines not included in the VTP can be administered if prescribed by a medical
practitioner.
Application
Patients who qualify for care under the VTP
17. NZDF Vaccinators, on duty, may provide healthcare to the patient groups in accordance with
DFI 18.1 Health Services, Part 4, Chapter 3
Access to NZDF Health Services.
18. Under certain circumstances, the Issuer may grant an
Applied Practice Permit (refer to
DHR 13, Part 5) to allow NZDF Vaccinators to administer vaccines to a patient or patients who do not qualify
for care under DFI 18.1, Part 4, Chapter 3.
Authorised VTP Users
19. The Issuer is responsible for determining which healthcare providers are granted an
authority
to practice under the VTP within the NZDF.
20. Only NZDF vaccinators are authorised to administer vaccines under the VTP.
Authority for vaccination administration
21. Baseline programme vaccines are able to be administered, using this VTP as the authority, to
patients with—
a.
incomplete NZ National Immunisation Schedule (NIS) vaccination schedule courses; or
b.
incomplete or absent NZDF baseline programme vaccine courses.
22. Enhanced programme vaccines are able to be administered if authorised by a medical
practitioner and specified in an Authorising Document (these include, but are not limited to, OPORD,
OPINST, EXORD, EXINST, the JSOP Vaccination for Overseas Posting and the High Readiness
Nominal Roll).
23. Meningococcal ACWY, meningococcal B and influenza (in season) vaccines are able to be
administered to ab initio trainees using this VTP as the authority.
24. Personal choice vaccines (eg influenza, Herpes zoster and HPV vaccines) are able to be
administered, using this VTP as the authority, to patients who request them and fulfil the eligibility
criteria.
25. Unless prescribed by a medical practitioner for a specific patient, all vaccinations given by
Defence Force personnel are to be given in accordance with the NZDF VTP. The VTP are based on
manufacturers’ recommendations and the Ministry of Health Immunisation Handbook, with variance
only by exception due to operational requirements.
26. The Defence Health Information System (DHIS) is to be used to assist the NZDF vaccinator in
determining which vaccinations are required for each individual.
5
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Authority to Administer Vaccines
Vaccine
Baseline
Enhanced
Enhanced Programme
Programme
Programme
Authorisation
COVID-19
Primary course
Booster dose
Patient choice
NZDF divers
Authorising document
Hepatitis A
-
-
Hepatitis B
-
-
Measles, Mumps & Rubella
-
-
Poliomyelitis
Primary course
Booster dose
Authorising document
Tetanus, Diphtheria, Pertussis
Primary course
Other booster
Authorising document
10 yearly booster
doses
Post-exposure
Cholera
-
Authorising document
Dengue Disease
Authorising document
Herpes (Varicella) zoster
-
Patient choice
Human Papilloma Virus
-
Patient choice
Influenza
-
Ab initio trainees
Patient choice
NZDF divers
Authorising document
Japanese Encephalitis Virus
-
Authorising document
Meningococcal ACWY
-
Ab initio trainees
Individuals aged ≤25 years who
are in their first 12 months of
living in shared service
accommodation
Authorising Document
Meningococcal B
-
Ab initio trainees
Individuals aged ≤25 years who
are in their first 12 months of
living in shared service
accommodation
Authorising Document
Rabies
-
Authorising document
Tick Borne Encephalitis (TBE)
-
Authorising document
Typhoid
-
Authorising document
Administration process
27. Minimum staffing and equipment requirements for vaccination must be met in order for NZDF
vaccinators to conduct vaccinations. These requirements are to be in accordance with the current
edition of the Immunisation Handbook.
6
Released under the Official Information Act 1982
Version 5.01
25 March 2026
28. The process for administering vaccines within the NZDF is shown in the NZDF Vaccination
Process Chart in
DHR 31 Applied Clinical Practice - Medical, Part 4, Chapter 2
Vaccine Administration.
29. All vaccines within this VTP are to be administered by a NZDF Vaccinator using the NZDF
patient consent process, and the administration is to be fully documented.
30. Patients are to be counselled about the vaccine they are receiving and are also to be
encouraged to read the relevant Patient Information Leaflet.
Precautions
31. Appropriate medical treatment and supervision must always be available in case of
anaphylactic reactions.
32. Approval from a medical practitioner is to be obtained before a vaccine is given if any of the
precautions identified in the specific vaccine prescription are present.
33. Syncope can occur during vaccination as a response to the needle injection. Ensure measures
are in place to avoid injury from faints.
34. If bleeding occurs at the site of vaccination, firm pressure is to be applied to injection site,
without rubbing, for at least 2 minutes.
Consent
35. Informed consent is to be gained and recorded in the DHIS, prior to vaccine administration.
The informed consent process is detailed in
DHR 30 Applied Healthcare: Health and Disability Services, Part 1, Chapter 2
Informed Consent for Health Service Provision. If the DHIS is unavailable,
an
MD1188 Written Consent for Vaccinations is to be used to record written consent. A copy of the
MD1188 is to be scanned into the DHIS as soon as practicable.
36. MD1188 must be completed if the identified primary vaccination schedule is not used.
37. Service personnel have the right to refuse vaccination. If a service person exercises this right, a
medical practitioner is to be informed. The medical practitioner is then to discuss the possible
consequences of that decision with the patient in accordance with
DHR 31, Part 4, Chapter 1
NZDF
Vaccination.
Section 29 Medicines
38. Medications go through an assessment and approval process before they can be supplied in
New Zealand. This is to ensure that the medicines supplied meet the required standards of quality
and are effective. In certain circumstances, the NZDF may need to prescribe a medicine that has not
yet been approved; these medicines are covered under section 29 of the Medicines Act 1981 and are
frequently referred to as ‘section 29 medicines’.
39. The VTP contains some vaccinations that have not yet been approved. VTP Users who
administer section 29 medicines must do the following—
a.
Advise the patient that the vaccine they are being administered has not yet been
approved for use in New Zealand. If the patient declines the vaccine, VTP issuers should
speak with a medical practitioner to identify an alternative medicine.
b.
Ensure the patient understands that the NZDF may be asked to provide the medicine
manufacturer or importer and Medsafe with information about the supply of section 29
medicines to identifiable individuals. Document this conversation in the patient notes.
c.
Gain patient consent to accept this medicine. Patients can also speak with a medical
practitioner if they would like more information about section 29 medicines.
7
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Off-label use
40. When medications go through the New Zealand approval process, they are assigned approved
indications.
41. The VTP contains some vaccinations with indications different from their approved indications.
These are annotated ‘Off-Label’.
42. NZDF Vaccinators administering Off-Label vaccinations are to do the following—
a.
Advise the patient that the vaccine they are being issued is safe for use and has been
shown to be effective but it has not been approved for that indication in New Zealand.
b.
Gain patient consent to accept this vaccination. Patients can also speak with a medical
practitioner if they would like more information about Off-Label use of medicines.
Site of administration
43. The VTP prescriptions specify the site of administration of the individual vaccines.
44. The administration of two vaccines at the same site is not recommended. Separate limbs are to
be used if possible. When it is necessary for two vaccines to be given in the same limb, the injection
sites should be separated by at least 2 cm.
Simultaneous live vaccines
45. Multiple vaccines, including live virus vaccines, may be given at the same time.
46. There are concerns about an impaired immune response if two live vaccines are not given at
the same time, but are given within four weeks of each other. Therefore, if two live vaccines are not
given at the same time, they are to be given at least four weeks apart.
Stand-down period
47. All patients must be kept under close observation for 20 minutes (or the length of time
specified in the MSO) following vaccination.
48. Stand down following any vaccination is for a minimum period of 12 hours for aircrew and
48 hours for divers, unless specific directed times are stated within the vaccine prescription.
Personnel must be symptom free from any side effects before returning to duties.
49. VTP
Users treating aircrew should also be aware of, and understand, the rules in
DHR 37
Applied Healthcare: Occupational Medicine, Part 2
Aviation Medicine, Chapter 2
Aircrew - Prescribing
Medicines.
Adverse reactions
50. Adverse reactions can occur despite vaccines being extensively tested for safety and efficacy.
Adverse reactions might be intensified if multiple vaccines are given at the same time.
51. Two terms are used to describe spontaneous reports in the context of vaccination:
a.
An adverse event is any undesirable event experienced by a person, which may or may
not be causally associated with the vaccine.
b.
An adverse reaction is any undesirable effect resulting from a vaccine (ie they are
causally associated).
52. Any adverse reaction is to be recorded in the DHIS. An explanation should be recorded in the
Vaccination Care Plan and in the medical notes of the DHIS.
53. Any serious or unexpected adverse event following vaccination should be reported to the
Medical Assessor, Centre for Adverse Reactions Monitoring, PO Box 913, Dunedin. Reporting details
are outlined in the latest edition of the Immunisation Handbook.
8


Released under the Official Information Act 1982
Version 5.01
25 March 2026
Variance in regime
54. No variance to the VTP is permitted by VTP Users.
55. Any variance from the NZDF VTP prescriptions must be prescribed by a medical practitioner
prior to vaccine administration.
56. Medical practitioner direction is to be obtained when a situation arises that is not covered by
the VTP.
57. When any vaccine is prescribed by a medical practitioner—
a.
the medical practitioner must ensure that—
clear verbal direction is provided; and
the NZDF Vaccinator is capable of administering the prescribed vaccine; and
b.
both the NZDF Vaccinator and responsible medical practitioner must document the
directions provided to the NZDF Vaccinator by the medical practitioner in the patient’s
DHIS records.
Delayed completion of course
58. Where there is a delay in completing a course of vaccinations, refer to a medical practitioner.
High-risk vaccines
59. There are some vaccinations with high-risk profiles that are to be given only by a registered
health practitioner, ie an NZDF Vaccinator qualified registered nurse, or a medical practitioner.
Currently, there are no high-risk vaccines in the NZDF VTP.
Recording vaccinations
60. The NZDF Vaccinator is responsible for ensuring all vaccines administered are recorded in the
appropriate Vaccination Care Plan in DHIS, on the same day vaccination occurs, preferably at the
time of vaccination.
61. All vaccines administered to patients are to be recorded into the DHIS. This is to include—
b.
date given;
c.
assessment and treatment details of the patient;
d.
any monitoring of follow-up treatment (if required);
e.
facility where the vaccine was administered;
f.
batch number and expiry date of the vaccine; and
g.
site of administration.
Vaccine prescription format
62. VTP users must read the prescriptions of every vaccine they are considering to use. The
Vaccine Table below outlines the information available for all vaccines and the actions that NZDF
Vaccinators need to take.
63. The vaccine prescriptions do not include all possible drug interactions, cautions or side effects.
The information contained reflects the scope of practice of NZDF personnel, the environments in
which care is typically provided and the typical NZDF population demographics. This means that
information related to children and elderly is not usually included. Refer to th
e NZ Formulary for a
more comprehensive list of interactions and their clinical significance, cautions and side effects.
9
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Vaccine
(programme – baseline or enhanced)
Full vaccine name
Available Products
Outlines the vaccines available with the following information:
NZDF Vaccinator action:
Trade Name
Check the vaccine name, strength and expiry date
Ingredients and strength
Presentation (eg suspension; powder; solution)
Appearance of initial product
Indication
Outlines the VTP indication
Authorisation
Indicates the authorisation for enhanced programme vaccines or enhanced
NZDF Vaccinator action:
use of vaccines
Ensure appropriate authorisation for administration of
the vaccine is present
Dosage and Route
Outlines:
NZDF Vaccinator action:
of Administration
any instructions on reconstitution / preparation of the vaccine
Prepare the vaccine in accordance with specific
required prior to administration.
instructions (if required)
Appearance when reconstituted if applicable
Ensure the schedule of the vaccine is being adhered to
the primary vaccination course with dose, route, and frequency /
Ensure all NZDF specific requirements are followed
number of doses to be administered.
the booster dose regimen, if applicable.
NZDF specific requirements to be considered prior to the
administration of each vaccine.
If more than one product is available the instructions for each specific
vaccine will be given.
Some vaccines may have more than one indication, these will be clearly
separated with the relevant information.
10
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Contraindications
Lists other medications and/or circumstances when a vaccine must not
NZDF Vaccinator action:
be administered.
Exclude all contraindications before administering
All vaccines have the following contraindications:
Do not administer the vaccine if any contraindication
o Known hypersensitivity to any component of the vaccine or other
applies
rabies vaccines including hypersensitivity to neomycin or other
antibiotics of the same class (aminoglycoside)
o Hypersensitivity after previous vaccination with rabies vaccines
o Acute systemic illness with fever over 38°C
Precautions
Outlines significant precautions associated with the vaccine.
NZDF Vaccinator action:
All injectable vaccines have the following precautions:
Consult with a medical practitioner prior to
o Appropriate medical treatment and supervision should always be
administration of the vaccine if any precaution is present.
available in case of anaphylactic reactions.
o Thrombocytopenia or a bleeding disorder
Any precautions concerning the vaccine’s administration during
pregnancy or breastfeeding will be highlighted.
Occupational
Lists any occupational considerations, eg occupational restrictions.
NZDF Vaccinator action:
Considerations
All vaccines have the following occupational considerations:
Alert patient of any occupational considerations such as
o NZDF Aircrew are to be stood down for 12 hours following
driving, flying, diving, swimming, working at height,
administration.
operating machinery and/or weapons use.
o NZDF Divers are to be stood down for 48 hours following
Inform patient of stand down requirements
administration.
o Personnel must be symptom free from any side effects before
returning to duties.
Side Effects
Lists expected consequences of medicine administration (as most
NZDF Vaccinator action:
appropriate to the NZDF population)
Warn patient of possible side effects
Explain how to avoid/reduce the side effects occurring
and what to do if they do occur
11
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Significant Drug
Lists significant drug interactions
NZDF Vaccinator action:
Interactions
All vaccines have the following general interaction statements:
Consult medical practitioner prior to administration if
o Immunosuppressive medicines may reduce the response to the
patient is taking any listed drugs concurrently.
vaccine – refer to medical practitioner
If the patient is on an unfamiliar medicine, consult the
o Separate injection sites / limbs and separate syringes must be used if
latest version of Stockley’s alerts (via the NZ Formulary
other medicines, including vaccines, are to be given at the same time.
link). If red or amber, consult a medical practitioner.
o Many medicines have multiple interactions with non-DML
medicines. If the patient is on a medicine with which you are unfamiliar,
consult the latest version of Stockley’s interaction (via
https://about.medicinescomplete.com/publication/stockleys-
interactions-checker/). If red or amber, consult a medical practitioner.
Special Notes &
Lists any special information for the vaccinator.
NZDF Vaccinator action:
Additional
Follow any instructions provided
Information
Information for
Lists any specific information to tell the patient, in addition to the
NZDF Vaccinator action:
patients
general advice provided post-vaccination.
Counsel the patient about the specific information and
encourage them to read the patient information leaflet.
Scope authorised
States who is authorised to administer this vaccine
NZDF Vaccinator action:
to administer this
Administer vaccine only if the medicine is within your
medicine
authorised scope.
Countersigning
States the countersignature requirements
NZDF Vaccinator action:
If countersignature required, task to appropriate medical
practitioner as soon as practical. The medical practitioner
must countersign no later than 48 hours after having
been tasked the countersign request.
Clinical
States what clinical documentation is required in addition to that
NZDF Vaccinator action:
Documentation
specified in the ‘Recording Vaccinations’ section
Complete any additional documentation
12
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Vaccine MSOs: BASELINE PROGRAMME
13
link to page 17
Released under the Official Information Act 1982
Version 5.01
25 March 2026
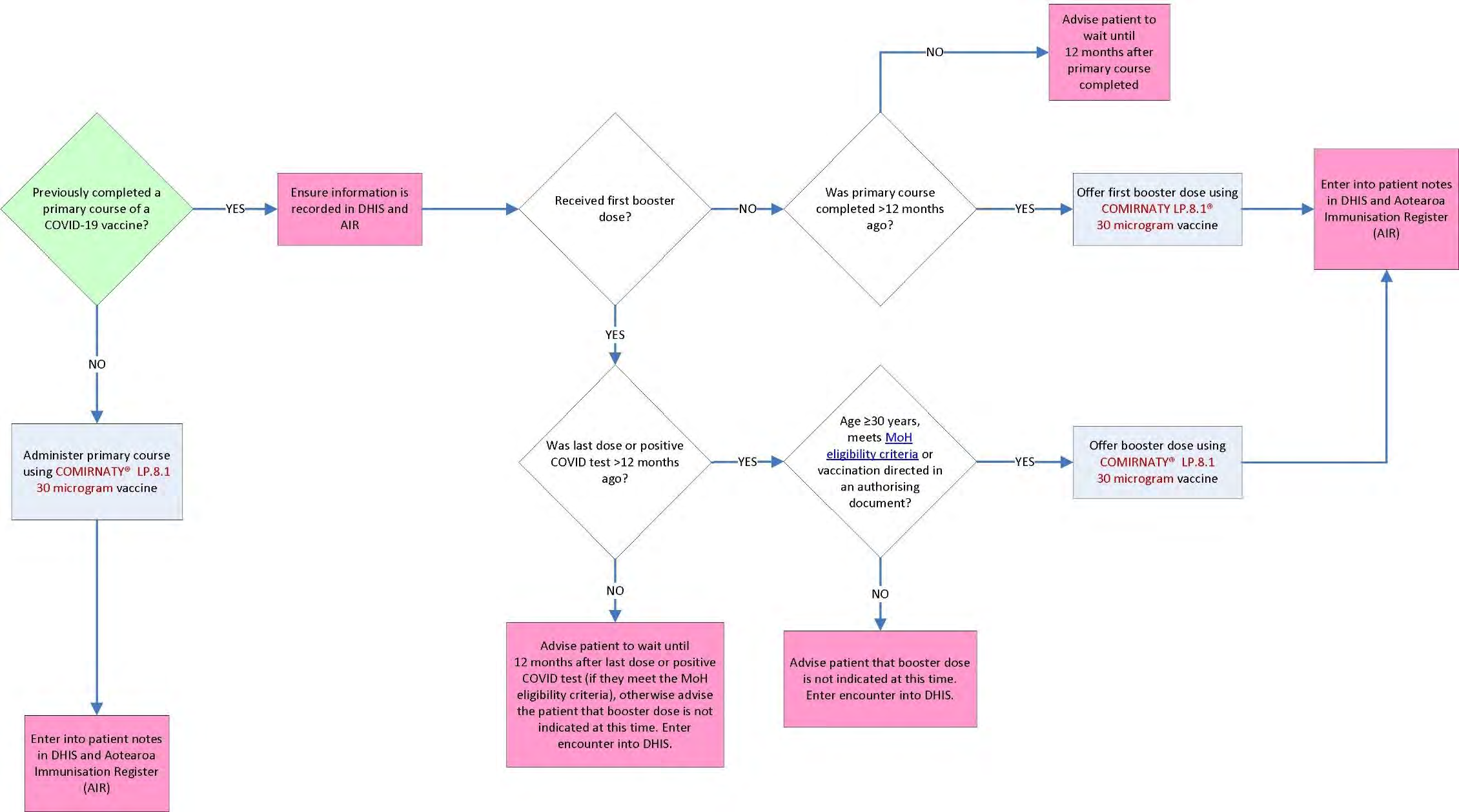
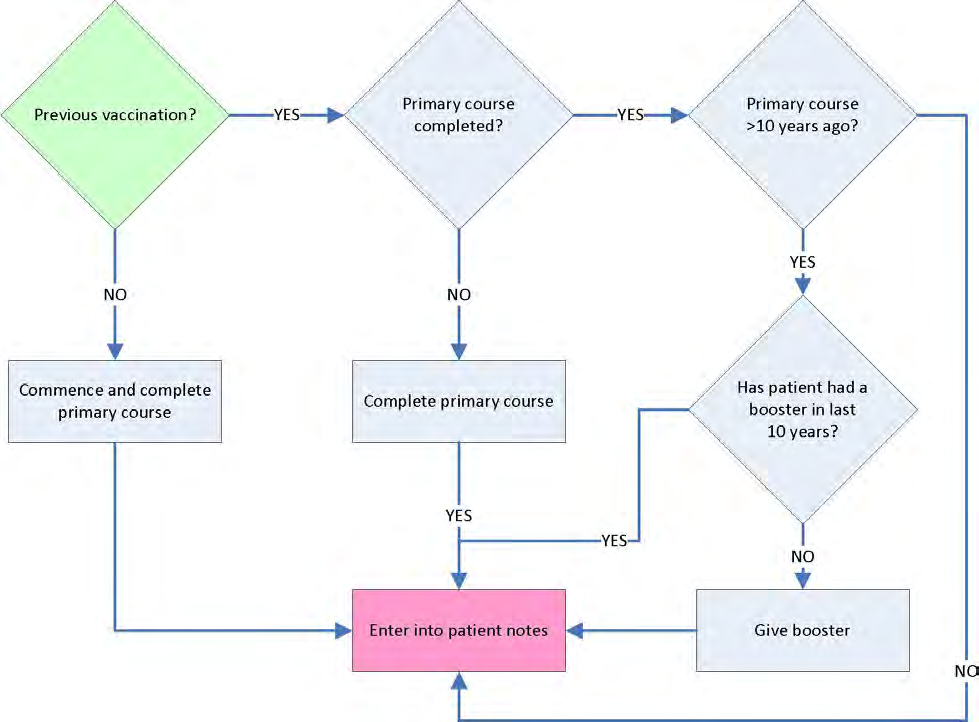
COVID-19 Vaccine
(Baseline programme – primary course)
(Enhanced programme – all booster doses)
mRNA COVID-19 Vaccine (nucleoside modified)
Available Product
Comirnaty® LP.8.1 COVID-19 mRNA Vaccine 30 microgram
Presented as a single-dose prefilled syringe of 0.3 mL white to off white
suspension
NO DILUTION is required.
Each 0.3 mL dose contains: 1 dose of vaccine LP.8.1 Comirnaty®
Indication
Active immunisation against COVID-19
See COVID-19 Vaccine Algorithm below.
Authorisation
Booster dose: Patient choice in accordance with current
Ministry of Health
criteria, NZDF divers (se
e DHR 37 Applied Healthcare: Occupational
Medicine, Part 1, Chapter 2
Diving Medical Standards) or authorising
document (eg from a J1H Annex H)
Dosage and Route
WARNING: DO NOT DILUTE PRIOR TO USE.
of Administration
Comirnaty® LP.8.1 30 microgram vaccine is to be used for both primary
course and booster doses.
1x Prefilled one dose (0.3 ml) 30 mcg for Primary Dose
1x Prefilled one dose (0.3 ml) 30 mcg for Booster Dose
Pre-filled syringes are supplied thawed and
must not be shaken, it should
appear as a white to off-white suspension. Do not use if discoloured or
particles are visible.
Remove the tip cap and attach an appropriate needle for intramuscular
injection and administer the entire volume of the syringe by intramuscular
injection (deltoid area recommended) according to the algorithm.
see
Contraindications
Known hypersensitivity to any component of the vaccine
Hypersensitivity after previous vaccination with Comirnaty® vaccine
Acute systemic illness with fever over 38°C
Previous episode of myocarditis or pericarditis
Precautions
Appropriate medical treatment and supervision should always be
available in case of anaphylactic reactions.
Thrombocytopenia or a bleeding disorder including anticoagulant
therapy
Known allergy to other vaccines
Pregnancy
Breastfeeding
Previous cardiac condition
Previous adverse event after a COVID‐19 vaccination
14
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Occupational
NZDF Aircrew are to be stood down for 48 hours following
Considerations
administration.
NZDF Divers are to be stood down for 48 hours following
administration.
Personnel must be symptom free from any side effects before
returning to duties.
Side Effects
Local reaction at site of injection (pain, inflammation, redness)
Nausea
Diarrhoea
Vomiting
Headache
Fatigue
Myalgia
Arthralgia
Fever
Chills
Rarely, the following adverse effects have been reported:
Myocarditis, myopericarditis, pericarditis
The incidence of these side effects appears higher in males under 40 years
old, and shortly after the second dose of the vaccine; however, this rate
may decline with longer dose-intervals and with additional doses after the
second. Cases are usually mild. If symptoms occur, seek medical
practitioner advice.
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine
Interactions
– refer to medical practitioner
All NIS vaccines can be given at the same time as Comirnaty® vaccines.
Separate injection sites/limbs and separate syringes must be used if
other medicines, including vaccines, are to be given at the same time.
Many medicines have multiple interactions with non-DML medicines. If
the patient is on a medicine with which you are unfamiliar, consult the
latest version of Stockley’s interaction (via
https://about.medicinescomplete.com/publication/stockleys-
interactions-checker/). If red or amber, consult a medical practitioner.
Special Notes &
Influenza vaccination is highly recommended and can be given at the
Additional
same time as COVID-19 vaccines.
Information
Operational enhanced vaccines can be given at same time as COVID-19
vaccines
Information for
There have been very rare reports of myocarditis and pericarditis
patients
occurring shortly after receiving the Comirnity® vaccine. Seek
immediate medical attention if you start to get:
o Chest pains or if your existing chest pain gets worse
o Discomfort or heaviness in your chest
o Shortness of breath or difficulty breathing
o An abnormal heartbeat or a racing fluttering feeling or a feeling of
skipped heartbeats
15
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Patients are to be advised as with any vaccine may not protect all
vaccine recipients. Individuals may not be fully protected until 7 days
after their dose of Comirnaty®.
Encourage the patient to read the Patient Information Leaflet.
Scope authorised
Current NZDF Vaccinators (medics and registered nurses) who also
to administer this
achieve the additional IMAC 3-hour COVID online course
medicine
Countersigning
Countersignature not required
Clinical
All relevant information is to be recorded in the Aotearoa Immunisation
Documentation
Register (AIR) and, for NZDF uniformed staff, in the patient’s DHIS
record (Profile).
16
Released under the Official Information Act 1982
Version 5.01
25 March 2026
COVID-19 Vaccine Algorithm
17
Released under the Official Information Act 1982
Version 5.01
25 March 2026
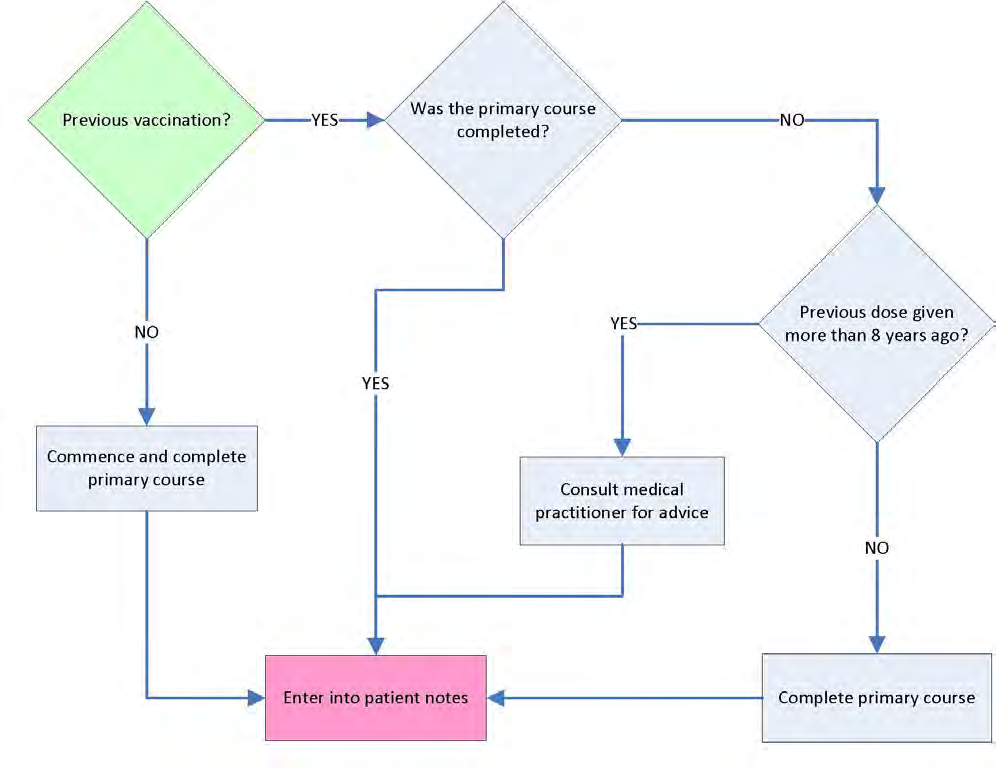
Hepatitis A Vaccine
(Baseline Programme)
Inactivated Hepatitis A Vaccine (adsorbed)
Available Products
Havrix 1440®
Each 1 mL dose contains:
Inactivated hepatitis A virus: 1,440 ELISA units
Cloudy white suspension for injection. Storage may cause the vaccine to appear as a fine white
deposit with a clear colourless supernatant.
Avaxim®
Each 0.5 mL dose contains:
Hepatitis A virus: 160 antigen units
Cloudy, white suspension for injection.
18
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Indication
Active immunisation against Hepatitis A
Dosage and Route of Shake well before use. Once shaken, both vaccines should be a slightly opaque, cloudy, white
Administration
suspension. Discard the vaccine if it does not have this appearance.
Havrix 1440®
Primary vaccination
Administer the required number of doses of 1 mL by intramuscular injection (deltoid area
recommended) to complete the following schedule:
First dose:
on day 0
Second dose:
between 6 and 12 months after the first dose.
CAUTION: Do not give the second dose earlier than 6 months after the first dose.
Note: If the primary course was started less than eight years ago, but not completed within the
12-month period, complete the primary course by administering the second dose. If the
primary course was started more than eight years ago, consult a medical practitioner for
advice.
Booster
No booster required following completion of the primary vaccination course.
Avaxim®
Primary vaccination
Administer the required number of doses of 0.5 mL by intramuscular injection (deltoid area
recommended) to complete the following schedule:
First dose:
on day 0
Second dose:
between 6 and 36 months after the first dose.
CAUTION: Do not give the second dose earlier than 6 months after the first dose.
Note: If the primary course was started less than eight years ago, but not completed within the
12-month period, complete the primary course by administering the second dose. If the
primary course was started more than eight years ago, consult a medical practitioner for
advice.
Booster
No booster required following completion of the primary vaccination course.
Contraindications
Known hypersensitivity to any component of the vaccine or other hepatitis A vaccines
Hypersensitivity after previous vaccination with hepatitis A vaccines
Acute systemic illness with fever over 38°C
Precautions
Thrombocytopenia or a bleeding disorder
Hypersensitivity to neomycin or other antibiotics of the same class (aminoglycoside)
Pregnancy – refer to medical practitioner
Breastfeeding – refer to medical practitioner
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
19
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Side Effects
Local reactions (including pain, inflammation, redness)
Headache
Fatigue
Irritability
Nausea, vomiting, loss of appetite
Mild fever
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria, anaphylaxis)
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
Interactions
practitioner.
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult Stockley’s alerts
(available through the NZ Formulary).
Information for
Encourage the patient to read the Patient Information Leaflet.
patients
Scope authorised to
Current NZDF Vaccinator
administer this
medicine
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
One dose provides sufficient immunity in order to deploy. The second dose must not be given
information
earlier than 6 months or later than 8 years after the first dose. If longer than 8 years, the primary
course should be restarted.
Havrix 1440® and Avaxim® can be used interchangeably to complete a two-dose primary course.
20
Released under the Official Information Act 1982
Version 5.01
25 March 2026
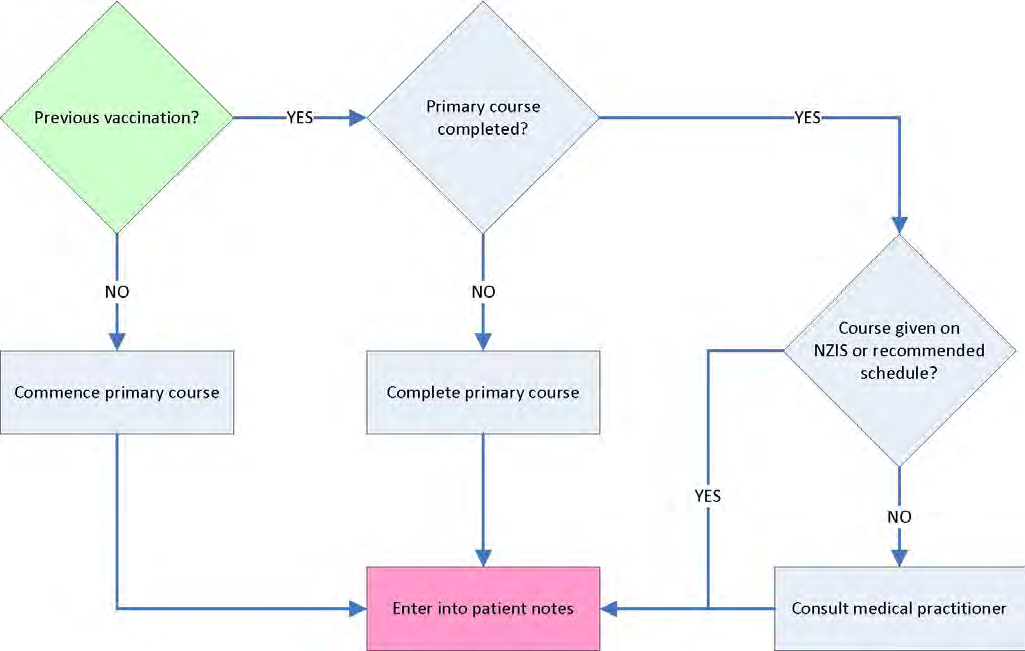
Hepatitis B Vaccine
(Baseline Programme)
Inactivated Hepatitis B Vaccine (adsorbed)
Available Product
Engerix-B®
Each 1 mL dose contains:
Hepatitis B surface antigen: 20 mcg.
Cloudy white suspension for injection. Storage may cause the vaccine to appear as a fine
white deposit with a clear colourless supernatant.
Indication
Active immunisation against Hepatitis B
21
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Dosage and Route of
Shake well before use. Once shaken, the vaccine should appear as a slightly opaque, white
Administration
suspension.
Primary vaccination
Administer the required number of doses of 1 mL by intramuscular injection (deltoid area
recommended) to complete the following schedule:
First dose:
on day 0
Second dose:
1 month later
Third dose:
6 months from date of the first dose
Note: If the primary course has been started but not completed, administer the
required number of doses to complete the primary course without repeating prior
doses.
Note: An alternative two-dose hepatitis B vaccine catch-up schedule of monovalent
hepatitis B vaccine at 0 and 6 months has been available for adolescents aged
10–15 years. Where members have received this schedule when aged between
10–15 years, they do not require a third hepatitis B vaccination.
Booster dose
No booster required following completion of the recommended primary vaccination course.
Contraindications
Known hypersensitivity to any component of the vaccine or other hepatitis B vaccines
Hypersensitivity after previous vaccination with hepatitis B vaccines
Acute systemic illness with fever over 38°C
Precautions
Thrombocytopenia or a bleeding disorder
Chronic liver disease
HIV
Pregnancy
Breastfeeding
Occupational Considerations
NZDF Aircrew are to be stood down for 12 hours following administration.
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
Side Effects
Local reactions (including pain, inflammation, redness)
Nausea
Vomiting
Diarrhoea
Abdominal pain
Malaise
Rash
Loss of appetite
Irritability
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria, anaphylaxis)
Significant Drug Interactions
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
practitioner.
22
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult
Stockley’s alerts (available through the NZ Formulary).
Information for patients
Encourage the patient to read the Patient Information Leaflet.
Scope authorised to
Current NZDF Vaccinator
administer this medicine
Countersigning
Countersignature not required
Additional Clinical
If an accelerated schedule is approved by a medical practitioner, it must be documented
Documentation
in the patient’s care plan, including the booster dose at 12 months.
Additional information
The interpretation of hepatitis B serology depends upon the person’s vaccination history.
Measurement of anti-HBs antibody levels after a documented course of three hepatitis B
vaccines is not authorised unless the person has known risk factors (seek MO advice) or
requires documented immunity for occupational or deployment reasons.
Even if anti-HBs antibodies are positive after the first or second dose in unvaccinated
individuals, the primary course must be completed.
Accelerated Schedules
CAUTION: May only be given after consultation, approval and under the
authority of a prescription from a medical practitioner.
There are two approved Accelerated Schedules:
Schedule 1: three doses of 1 mL by intramuscular injection (deltoid area
recommended) according to the following schedule, followed by a booster dose of
1 mL:
o First dose:
on day 0
o Second dose:
7 days later
o Third dose:
21 days from the date of the first dose
o Booster dose:
12 months from the date of the first dose
Schedule 2: three doses of 1 mL by intramuscular injection (deltoid area
recommended) according to the following schedule, followed by a booster dose of
1 mL:
o First dose:
on day 0
o Second dose:
1 month later
o Third dose:
2 months from the date of the first dose
o Booster dose:
12 months from the date of the first dose
23
Released under the Official Information Act 1982
Version 5.01
25 March 2026
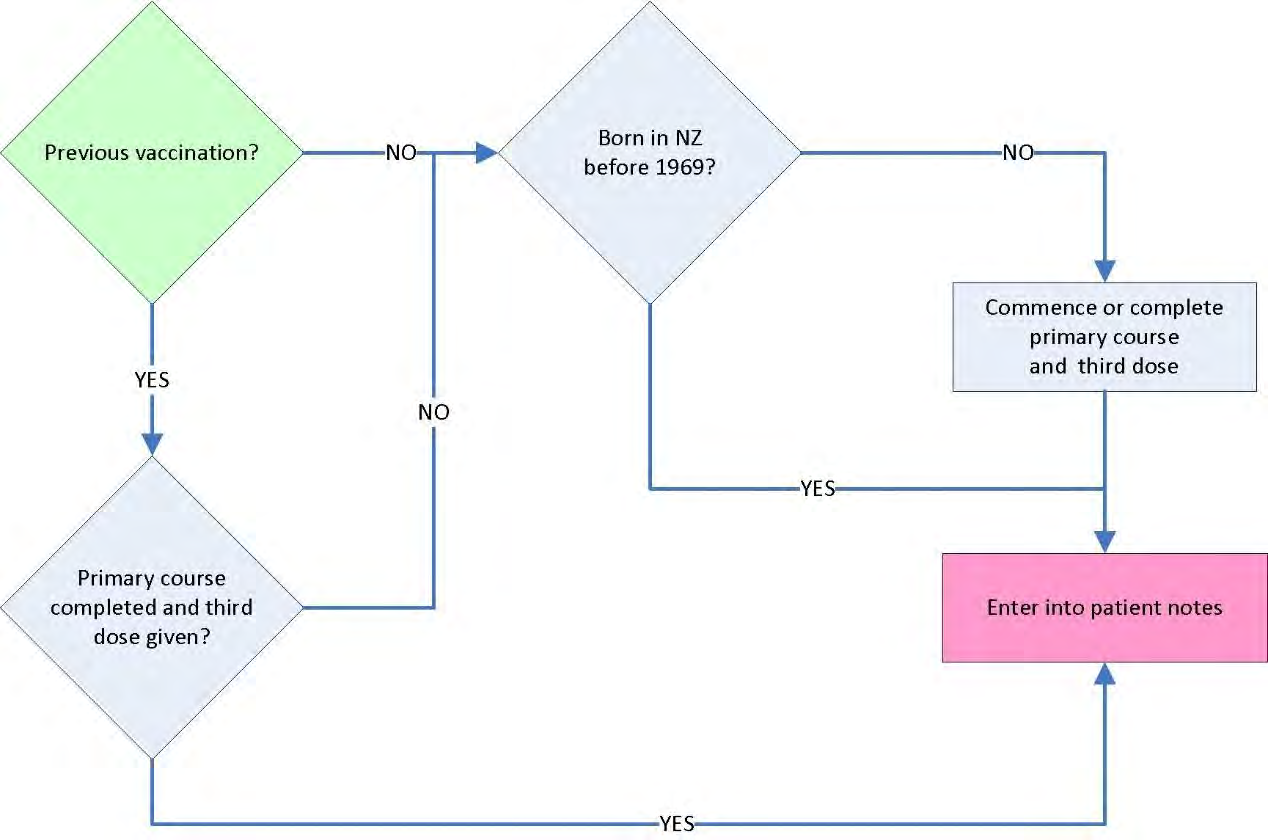
Measles, Mumps and Rubella Vaccine
(Baseline Programme)
Live trivalent attenuated Measles, Mumps and Rubella Vaccine
Available Product
Priorix®
Each 0.5 mL of the reconstituted vaccine contains not less than:
Measles virus (Schwarz): 1000 CCID50 units
Mumps virus (Jeryl Lynn, strain RIT 4385): 5000 CCID50 units
Rubella virus (Wistar RA 27/): 1000 CCID50 units.
There are two components to the Priorix vaccine:
the vaccine – a whitish to slightly pink powder in a glass vial
the diluent – a clear, colourless liquid in a glass pre-filled syringe or ampoule
Indication
Active immunisation against measles, mumps and rubella
Dosage and Route of To prepare one dose of Priorix—
Administration
Add entire volume of diluent to vial of vaccine powder.
Shake the mixture well until all powder is dissolved.
Vaccine solution should be a clear peach to fuchsia pink colour.
If not used immediately, the vaccine solution can be stored between +2°C to +8°C for up to
8 hours.
24
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Primary vaccination
Administer the required number of doses of 0.5 mL by intramuscular injection (deltoid area
recommended) to complete the following schedule:
First dose:
on day 0
Second dose:
at least 4 weeks after first dose
Note: If the primary course has been started but not completed, administer the required
number of doses to complete the primary course without repeating prior doses.
Booster dose
An additional third dose is to be administered at least 6 months following primary vaccination.
Contraindications
Known hypersensitivity to any component of the vaccine including neomycin
Hypersensitivity after previous vaccination with measles, mumps or rubella containing vaccines
Acute systemic illness with fever over 38°C
Pregnancy
Immunosuppression
Administration of another live vaccine (including BCG) within the previous four weeks, unless
given concurrently
Blood or immunoglobulin transfusions during the previous 11 months
Precautions
Thrombocytopenia or a bleeding disorder
Hypersensitivity to eggs
Breastfeeding – refer to medical practitioner
Females of childbearing age should be comprehensively counselled about the risks of becoming
pregnant
within one month of vaccination.
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
Side Effects
Local reactions (including pain, inflammation, redness)
Fever and/or mild rash 6–12 days post immunisation (measles component)
Fever and/or mild swelling under the jaw 10–14 days after immunisation (mumps component)
Fever, mild rash and/or swollen glands 2–4 weeks after immunisation
Temporary joint pain 2–4 weeks after immunisation
Significant Drug
Priorix® is a live attenuated vaccine and must be given one month before, or after,
Interactions
administration of other live vaccines.
Priorix must not be administered to patients taking immunosuppressive medicines.
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult Stockley’s
alerts (available through the NZ Formulary).
Information for
Encourage the patient to read the Patient Information Leaflet.
patients
Some side effects may take up to 4 weeks to occur.
Scope authorised to
Current NZDF Vaccinator
administer this
medicine
25
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
Patients born in New Zealand before 1969 do not require MMR vaccination.
information
Refer to latest version of Immunisation Handbook if two doses of MMR have not been
previously administered.
The vaccine can be administered safely to patients who have had an anaphylactic reaction to
food containing eggs.
26
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Poliomyelitis Vaccine
(Baseline / Enhanced Programme)
Inactivated Poliomyelitis Vaccine
Available Product
IPOL®
Each 0.5 mL dose contains:
Poliovirus type 1 (Mahoney): 40 D Antigen Units (DAgU)
Poliovirus type 2 (MEF-1): 8 DAgU
Poliovirus type 3 (Saukett): 32 DAgU
Suspension for injection. Clear, colourless.
Indication
Active immunisation against poliomyelitis
Dosage and Route of Shake well before use.
Administration
Primary vaccination (Baseline Programme)
Administer the required number of doses of 0.5 mL by subcutaneous injection (deltoid area
recommended) to complete the following schedule:
First dose:
on day 0
Second dose:
8 weeks after the first dose
Third dose:
8 weeks after the second dose
Note: If the primary course has been started but not completed, administer the required
number of doses to complete the primary course without repeating prior doses.
Authorisation for booster dose: Authorising Document
Booster dose (Enhanced Programme)
Administer 0.5 mL by subcutaneous injection (deltoid area recommended)
Note: A booster dose is indicated only if at least 10 years after primary course.
Contraindications
Known hypersensitivity to any component of the vaccine or other poliomyelitis vaccines
Hypersensitivity after previous vaccination with IPOL® or other poliomyelitis vaccines
Acute systemic illness with fever over 38°C
Precautions
Thrombocytopenia or a bleeding disorder
Pregnancy – refer to medical practitioner
Hypersensitivity to neomycin, streptomycin sulfate, polymixin B sulfate or other antibiotics of
the same class
Immunosuppression
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
27
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Side Effects
Local reactions (including pain, inflammation, redness)
Generally feeling unwell or tired
Irritability, restlessness and sleepiness
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria, anaphylaxis)
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
Interactions
practitioner
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult Stockley’s
alerts (available through the NZ Formulary).
Information for
Encourage the patient to read the Patient Information Leaflet.
patients
Scope authorised to
Current NZDF Vaccinator
administer this
medicine
Countersigning
Countersignature not required
Clinical
An International Certificate of Vaccination and Prophylaxis will be raised on deployment where
Documentation
required.
Additional
Nil additional information
information
28
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Tetanus-Diphtheria-Pertussis Vaccine (Tdap)
(Baseline Programme)
Combined Tetanus-Diphtheria-Acellular Pertussis Vaccine
Available Product
Boostrix®
Each 0.5 mL dose contains:
Tetanus toxoid: 20 International Units (IU)
Diphtheria toxoid: 2 IU
Bordetella pertussis acellular antigens
pertactin: 2.5 micrograms
pertussis toxoid: 8 micrograms
filamentous haemagglutinin: 8 micrograms
Cloudy white suspension for injection. Storage may cause the vaccine to appear as a fine
white deposit with a clear colourless supernatant.
Indication 1
Active immunisation against Tetanus, Diphtheria and Pertussis
Dosage and Route of
Shake well before use. Once shaken, the vaccine should appear as a white cloudy
Administration
suspension.
29
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Primary vaccination (unapproved indication)
Administer the required number of doses of 0.5 mL by intramuscular injection (deltoid
area recommended) to complete the following schedule:
First dose:
on day 0
Second dose:
4–6 weeks after the first dose
Third dose:
4–6 weeks after the second dose
Note: If the primary course has been started but not completed, administer the
required number of doses to complete the primary course without repeating prior
doses.
Booster (Baseline Programme 10 yearly booster)
Administer 0.5 mL by intramuscular injection (deltoid area recommended) every
10 years after the primary course is completed.
Authorisation for Enhanced Programme booster: Authorising Document
Booster (Enhanced Programme)
Administer 0.5 mL by intramuscular injection (deltoid area recommended).
Indication 2
Active immunisation against Pertussis during each pregnancy
Dosage and Route of
Shake well before use. Once shaken, the vaccine should appear as a white cloudy
Administration
suspension.
Administer a single dose of 0.5 mL by intramuscular injection (deltoid area
recommended).
Note: Recommended to be given from 16 weeks gestation of every pregnancy,
preferably in the second trimester
Indication 3
Tetanus prone wound1 and more than 5 years since last booster.
Dosage and Route of
Shake well before use. Once shaken, the vaccine should appear as a white cloudy
Administration
suspension.
Administer a single dose of 0.5 mL by intramuscular injection (deltoid area
recommended).
1 Te Whatu Ora Health New Zealand. Immunisation Handbook 2024, version 4. 21.5.6
Prevention of tetanus following
injury
30
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Contraindications
Known hypersensitivity to any component of the vaccine or other tetanus, diphtheria
or pertussis vaccines
Hypersensitivity after previous vaccination with tetanus, diphtheria or pertussis
vaccines
Acute systemic illness with fever over 38°C
Previous encephalopathy of unknown aetiology, occurring within 7 days following
previous vaccination with pertussis-containing vaccine
Previous transient thrombocytopaenia or neurological complications following a
previous immunisation against diphtheria and/or tetanus
Precautions
Thrombocytopenia or a bleeding disorder
Temperature of ≥40°C or collapse or shock-like state (hypotonic-hyporesponsive
episode) within 48 hours of previous pertussis vaccination
Convulsions with or without fever, occurring within 3 days of previous pertussis
vaccination
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
Side Effects
Local reactions (including pain, inflammation, redness)
Headache
Nausea & vomiting
Myalgia or arthralgia
Fatigue
Influenza-like symptoms
Malaise
Fever
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria,
anaphylaxis)
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to
Interactions
medical practitioner.
Many medicines have multiple interactions with non-DML medicines. If the patient is
on a medicine with which you are unfamiliar, refer to a medical practitioner or
consult Stockley’s alerts (available through the NZ Formulary).
Special Notes including
Encourage patient to read Patient Information Leaflet.
information for patients
Scope authorised to
Current NZDF Vaccinator
administer this medicine
Countersigning
Countersignature not required
Clinical Documentation
No additional documentation required
31
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Additional information
Pertussis protection for military partners of pregnant women, or those with
newborns, should be considered if they have not had a dose in the previous 10 years
and must be on medical practitioner prescription
When Tdap vaccine is administered for the prevention of tetanus following injury
(indication 3), consider whether medical practitioner consultation for wound
assessment is clinically indicated.
Note: Refer to latest version of the Immunisation Handbook (Prevention of
tetanus following injury) and IMAC Guidelines for the management of tetanus-
prone wounds.
https://www.immune.org.nz/diseases/tetanus
32
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Vaccine MSOs: ENHANCED PROGRAMME
33
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Cholera Vaccine
(Enhanced Programme)
Oral Cholera Vaccine (inactivated bacteria and recombinant toxin)
Preparation
Dukoral®
Each dose contains:
Vibrio cholerae 01 Inaba classic strain (heat-inactivated): ca. 31.25 × 109 bacteria
Vibrio cholerae 01 Inaba El Tor strain (formalin-inactivated): ca. 31.25 × 109 bacteria
Vibrio cholerae 01 Ogawa classic strain (formalin-inactivated): ca. 31.25 × 109 bacteria
Vibrio cholerae 01 Ogawa classic strain (heat-inactivated): ca. 31.25 × 109 bacteria
Recombinant cholera toxin B subunit: 1 mg
There are two components to the Dukoral vaccine:
the vaccine – a whitish oral liquid suspension in a glass vial
the buffer – a white to off-white effervescent powder in a sachet
Indication
Active immunisation against Cholera
Authorisation
Authorising Document
34
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Dosage and Route
To prepare one dose of Dukoral—
of Administration
Dissolve effervescent powder in approximately 150 mL of cool water to make the buffer
solution.
Shake the vaccine vial gently and add the vaccine suspension to the buffer solution.
Mix well and use within two hours of preparation.
Primary vaccination
Administer the required number of doses orally, to complete the following schedule:
First dose:
on day 0
Second dose:
1–6 weeks after the first dose.
CAUTION: If more than 6 weeks have elapsed between doses, the primary course
must be restarted.
Contraindications
Known hypersensitivity to any component of the vaccine or other cholera vaccines
Hypersensitivity after previous vaccination with cholera vaccines
Acute systemic illness with fever over 38°C
Acute gastrointestinal illness
Precautions
Appropriate medical treatment and supervision should always be available in case of
anaphylactic reactions.
Thrombocytopenia or a bleeding disorder
Pregnancy
Breastfeeding
Dukoral® contains approximately 1.1 g sodium per dose, caution in patients on a controlled
sodium diet.
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
Side Effects
General stomach discomfort, including pain, cramps, gurgling and bloating
Malaise
Fatigue
Headache
Loss of/poor appetite
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
Interactions
practitioner.
Food and drink should be avoided for 1 hour before and after vaccination.
Chloroquine and hydroxychloroquine – concurrent administration should be avoided. Therapy
should be started no sooner that 8 days after vaccination with oral cholera vaccine.
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult Stockley’s
alerts (available through the NZ Formulary).
Information for
Food and drink should be avoided 1 hour before and 1 hour after vaccination.
patients
The vaccine does not provide full protection. It is important to adhere to standard health
protection measures to avoid cholera and other causes of traveller’s diarrhoea.
35
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Scope authorised
Current NZDF Vaccinator
to administer this
medicine
Countersigning
Countersignature required
Clinical
No additional documentation required
Documentation
Additional
Vaccination should be completed at least one week prior to exposure.
information
Only water is be used to dissolve the effervescent powder.
Booster doses:
o are indicated only if patient is under conditions of repeated or continued exposure to the
Vibrio cholerae organism.
o may only be given under the authority of a prescription from a medical practitioner.
36
link to page 7
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Dengue Disease Vaccine
(Enhanced Programme)
Live, Attenuated Tetravalent Dengue Disease Vaccine
Available Product
QDenga®
After reconstitution, each 0.5 mL dose contains:
Dengue virus serotype 1 (live, attenuated) ≥ 3.3 log10 plaque-forming units (PFU)/dose
Dengue virus serotype 2 (live, attenuated) ≥ 2.7 log10 PFU/dose
Dengue virus serotype 3 (live, attenuated) ≥ 4.0 log10 PFU/dose
Dengue virus serotype 4 (live, attenuated) ≥ 4.5 log10 PFU/dose
Powder and solvent solution for injection. Prior to reconstitution, the vaccine is a white to
off-white coloured freeze dried powder (compact cake). The solvent is a clear, colourless solution.
Indication
Active immunisation against Dengue Disease
Authorisation
Authorising Document
Dosage and Route of Completely reconstitute the vaccine with the solvent before use.
Administration
Primary vaccination
Administer the required number of doses of 0.5 mL by subcutaneous injection (deltoid area
recommended) to complete the following schedule:
First dose: on day 0
Second dose: after at least 3 months if remaining in a dengue endemic area
Note: Wherever possible, QDenga® vaccine should be given no less than 14 days prior to travel to
dengue endemic region
Note: This is an unappro
ved Section 29 medicine, so informed consent is required.
Booster dose
No booster dose is authorised
Contraindications
WARNING: Patients with a hypersensitivity reaction after the first dose should
not be given a
second dose.
Known hypersensitivity to any component of the vaccine
Congenital or acquired immune deficiency, including those receiving immunosuppressive
therapy such as systemic corticosteroids
Individuals with HIV infection
Pregnancy
Breastfeeding
Acute severe febrile illness
Precautions
Women of childbearing potential should avoid pregnancy for at least one month following
vaccination
If administered at the same time as other injectable vaccines, administer at different injection
sites
37
link to page 7
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 72 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
As symptoms of vaccine viraemia may be indistinguishable from dengue infection, the first
dose should be given no less than 14 days prior to travel into a dengue endemic region
wherever possible.
Side Effects
Local reactions (including pain, inflammation, redness)
Viraemia. Clinical studies observed viraemia in 49% of recipients who had not been infected
with dengue before. Vaccine viraemia started in the second week post-vaccination and on
average lasted four days with symptoms of headache, arthralgia, myalgia and rash. Viraemia
was rare after the second dose.
Headache
Myalgia
Malaise
Asthenia
Fever
Significant Drug
Where patients have received treatment with immunoglobulins or blood products, delay
Interactions
vaccinating for three months to avoid neutralisation of the attenuated vaccine.
Immunosuppressant medication may reduce the effectiveness of the vaccine.
Information for
This is an unapprov
ed Section 29 medicine.
patients
Encourage patients to read the Patient Information leaflet
Warn patients of possible viraemia after the first dose
Scope authorised to
Current NZDF vaccinator
administer this
medicine
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
None
information
38
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Herpes (Varicella) Zoster Vaccine
(Enhanced Programme)
Varicella Zoster Virus Recombinant Glycoprotein E Antigen Vaccine
Available
Shingrix®
Preparation
Each 0.5 mL dose contains:
Varicella Zoster Virus glycoprotein E: 50 micrograms
AS01B liposome-based adjuvant containing two immunostimulants:
Quillaja saponaria (soapbark tree) saponin fraction 21 (QS-21): 50 micrograms
Detoxified lipopolysaccharide fraction 3-O-desacy-4’-monophosphoryl liquid from
Salmonella minnesota: 50 micrograms
There are two components to the Shingrix® vaccine:
the vaccine – white powder in a glass vial
the suspension – opalescent, colourless to pale brownish liquid in a glass vial
Indication
Active immunisation against herpes zoster and prevention of post-herpetic neuralgia
Authorisation
Patient choice for patients aged 65 years (the second dose can be administered at age 66 years if
the first dose was given at 65 years)
Note: Patients who do not meet the above authorisation criteria and request the vaccine
are to be referred to a medical practitioner.
Dosage and Route of To prepare one dose of Shingrix®—
Administration
Add entire contents of suspension vial to vial of vaccine powder.
Shake the mixture gently until all powder is dissolved.
Vaccine solution should be an opalescent, colourless to pale brownish colour.
If not used immediately, the vaccine solution can be stored between +2°C to +8°C for up to
6 hours.
Primary vaccination
Administer the required number of doses of 0.5 mL by intramuscular injection (deltoid area
recommended) to complete the following schedule:
First dose:
on day 0
Second dose:
between 2 and 6 months after the first dose
Booster dose
No booster required following completion of the recommended primary vaccination course.
Contraindications
Known hypersensitivity to any component of the vaccine
Confirmed anaphylactic reaction to other Herpes zoster vaccines
Acute systemic illness with fever over 38°C
Precautions
Thrombocytopenia or a bleeding disorder
39
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
Side Effects
Local reactions (including pain, inflammation, redness)
Myalgia and arthralgia
Fainting (especially in younger patients), dizziness
Headache
Malaise
Fatigue
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria, anaphylaxis)
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
Interactions
practitioner.
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult Stockley’s
alerts (available through the NZ Formulary).
Information for
Encourage patient to read Patient Information Leaflet.
patients
Scope authorised to
Current NZDF Vaccinator
administer this
medicine
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
Nil
Information
40
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Human Papilloma Virus Vaccine
(Enhanced Programme)
Human Papillomavirus 9-valent, Recombinant, Adsorbed Vaccine
Available
Gardasil 9®
Preparation
Each 0.5 mL dose contains:
Human Papillomavirus 6 L1 protein: 30 micrograms
Human Papillomavirus 11 L1 protein: 40 micrograms
Human Papillomavirus 16 L1 protein: 60 micrograms
Human Papillomavirus 18 L1 protein: 40 micrograms
Human Papillomavirus 31 L1 protein: 20 micrograms
Human Papillomavirus 33 L1 protein: 20 micrograms
Human Papillomavirus 45 L1 protein: 20 micrograms
Human Papillomavirus 52 L1 protein: 20 micrograms
Human Papillomavirus 58 L1 protein: 20 micrograms
Cloudy white suspension for injection. Storage may cause the vaccine to appear as a fine white
deposit with a clear colourless supernatant.
Indication
Active immunisation against Human Papilloma Virus
Authorisation
Patient choice for patients meeting the MoH funding eligibility criteria
Note: Patients who do not meet the MoH funding eligibility criteria and request the vaccine
are to be referred to a medical practitioner.
Dosage and Route of Shake well before use.
Administration
Primary vaccination
Administer the required number of doses of 0.5 mL by intramuscular injection (deltoid area
recommended) to complete the following schedule:
First dose:
on day 0
Second dose:
2 months after the first dose
Third dose:
6 months after the first dose
Note: If the primary course has been started but not completed, administer the required
number of doses to complete the primary course without repeating prior doses.
Note: An alternative two-dose schedule of HPV vaccine, given at 0 and 6–12 months, is
recommended for individuals who receive the first dose before their 15th birthday. Where
members have received this schedule, they do not require a third HPV vaccination.
Booster dose
No booster required following completion of the recommended primary vaccination course.
Contraindications
Known hypersensitivity to any component of the vaccine or other Human Papilloma Virus
vaccines
Hypersensitivity after previous vaccination with Human Papilloma Virus vaccines
Acute systemic illness with fever over 38°C
41
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Precautions
Thrombocytopenia or a bleeding disorder
Pregnancy – vaccination should be delayed until completion of pregnancy
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
Side Effects
Local reactions (including pain, inflammation, redness)
Myalgia and asthenia
Fainting (especially in younger patients)
Headache
Malaise
Fever
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria, anaphylaxis)
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
Interactions
practitioner.
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult Stockley’s
alerts (available through the NZ Formulary).
Information for
Encourage patient to read Patient Information Leaflet.
patients
Scope authorised to
Current NZDF Vaccinator
administer this
medicine
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
Refer to a medical practitioner:
information
o if the primary vaccination schedule cannot be adhered to. The following should be
considered with an alternate schedule:
The second dose must be administered at least one month after the first dose.
The third dose must be administered at least three months after the second dose.
o if patients not meeting the MoH funding eligibility criteria request the vaccine.
42
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Influenza Vaccine
(Enhanced Programme)
Quadrivalent Inactivated Split Virion Influenza Vaccine
Available
Influvac® Tetra (2026 egg-based vaccine)
Preparation
Each 0.5 mL dose contains:
A/Missouri/11/2025 (H1N1)pdm09-like virus
A/Singapore/GP20238/2024(H3N2)-like virus
B/Austria/1359417/2021-like virus
B/Phuket/3073/2013-like virus
Indication
Active immunisation against influenza
Authorisation
Ab initio trainees
Patient choice
NZDF divers (see
DHR 37 Applied Healthcare: Occupational Medicine, Part 1, Chapter 2
Diving
Medical Standards)
Authorising Document
Note: Recommended for all NZDF personnel and strongly recommended for healthcare
providers, pregnant persons, persons over 65 years of age, Māori/Pasifika persons over
55 years of age, persons with chronic health conditions (such as asthma, diabetes or a heart
or lung condition), recruits and all NZDF uniformed personnel.
Dosage and Route of Shake before use. After shaking, the vaccine should appear as an even suspension.
Administration
Primary vaccination
If the patient has not received that year’s seasonal influenza vaccine, administer one dose of
0.5 mL by intramuscular injection (deltoid area recommended).
Booster dose
No booster required following completion of the primary vaccination course.
Contraindications
Known hypersensitivity to any component of the vaccine or other influenza vaccines
Hypersensitivity after previous vaccination with influenza vaccines
Acute systemic illness with fever over 38°C
Precautions
Thrombocytopenia or a bleeding disorder
History of Guillain-Barre syndrome
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
Side Effects
Local reactions (including pain, inflammation, redness)
43
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Headache
Malaise
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria, anaphylaxis)
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
Interactions
practitioner.
13-valent pneumococcal conjugate vaccine – increased risk of fever following concomitant
administration.
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult Stockley’s
alerts (available through the NZ Formulary).
Information for
Encourage the patient to read the Patient Information Leaflet.
patients
Scope authorised to
Current NZDF Vaccinator
administer this
medicine
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
The influenza strains in the vaccine change every year. Content can be verified from the
information
manufacturer’s datasheet.
Egg allergy, including anaphylaxis, is not a contraindication or precaution.
The standard 15-minute observation period may be shortened to 5 minutes if the
individual meets all
IMAC criteria (see ‘Waiting after receiving a 2026 influenza
vaccination’ under ‘Schedule and administration’) and is briefed by the healthcare
provider as per IMAC advice.
See als
o FLU2026 Winter Preparedness Kit: Vaccination for Flu, COVID-19 and other
respiratory viruses.
44
link to page 7
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Japanese Encephalitis Vaccine (Primary option)
(Enhanced Programme)
Live Attenuated Japanese Encephalitis Vaccine
Available Product
IMOJEV®
Powder and Diluent for Suspension for Injection
Diluent is a 0.4% Sterile Sodium Chloride Solution
Each dose contains: Monovalent Live Attenuated Viral Vaccine Japanese Encephalitis
virus:
4.0–5.8 log PFU (plaque-forming units)
The powder is a white to creamy white homogenous cake which might be retracted from
the sides of the vial. After reconstitution
IMOJEV® is a colourless to amber suspension.
Indication
Active immunisation against Japanese Encephalitis (Primary JEV vaccine option for the
NZDF)
Authorisation
Authorising Document (to include High Readiness Nominal Roll)
Dosage and Route
Using aseptic technique, reconstitute
IMOJEV® by injecting all the 0.4% sodium chloride
of Administration
solution into the freeze-dried vaccine, using one of the needles provided in the carton.
Swirl the vial gently. After the vaccine is completely dissolved, draw up a 0.5-ml dose of the
reconstituted suspension with the same syringe.
For injection, fit the syringe with the second needle provided in the package.
Vaccination
Administer a single injection of reconstituted vaccine 0.5 mL by subcutaneous injection
(deltoid area recommended)
Note: This is an unapproved,
Section 29 medicine so informed consent is required.
Booster dose
There is no need for a booster dose after the administration of a single dose of IMOJEV®
Contraindications
Hypersensitivity after previous vaccination with any Japanese Encephalitis Vaccine
Known hypersensitivity to any component of the vaccine
Administration of another live vaccine (including BCG) within the previous four weeks, unless
given concurrently
Immunosuppression
Pregnancy
Breastfeeding
Acute systemic illness with fever over 38°C
45
link to page 7
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Blood or immunoglobulin transfusions during the previous 3 months
Precautions
None
Occupational
Ideally, the vaccine should be given at least 28 days prior to potential exposure to JEV. If a
Considerations
person is travelling to a JE endemic area and they will enter within 28 days of receiving their
vaccination, they and their command chain are to be made aware of their reduced protection
status.
NZDF Aircrew are to be stood down for 12 hours following administration.
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
Side Effects
Local reactions (including injection site pain, inflammation, redness)
Headache
Fatigue
Malaise
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to
Interactions
medical practitioner
Many medicines have multiple interactions with non-DML medicines. If the patient is
on a medicine with which you are unfamiliar, refer to a medical practitioner.
Information for
This is an unapproved,
Section 29 medicine.
patients
Women should avoid pregnancy for 28 days after vaccination.
Encourage the patient to read the Patient Information Leaflet.
Scope authorised to
Current NZDF Vaccinator
administer this
medicine
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
IMOJEV® can be used as a booster to previous JE-Vax and Green Cross courses if they
information
have an ongoing risk of JE virus exposure and require vaccination.
Where patients have previously received JESPECT® and require a booster dose, using JESPECT®
for the booster dose is the preferred option. However, IMOJEV® may be used as an alternative
where needed.
IMOJEV® can be co administered with any other vaccine including the seasonal influenza
vaccine
46
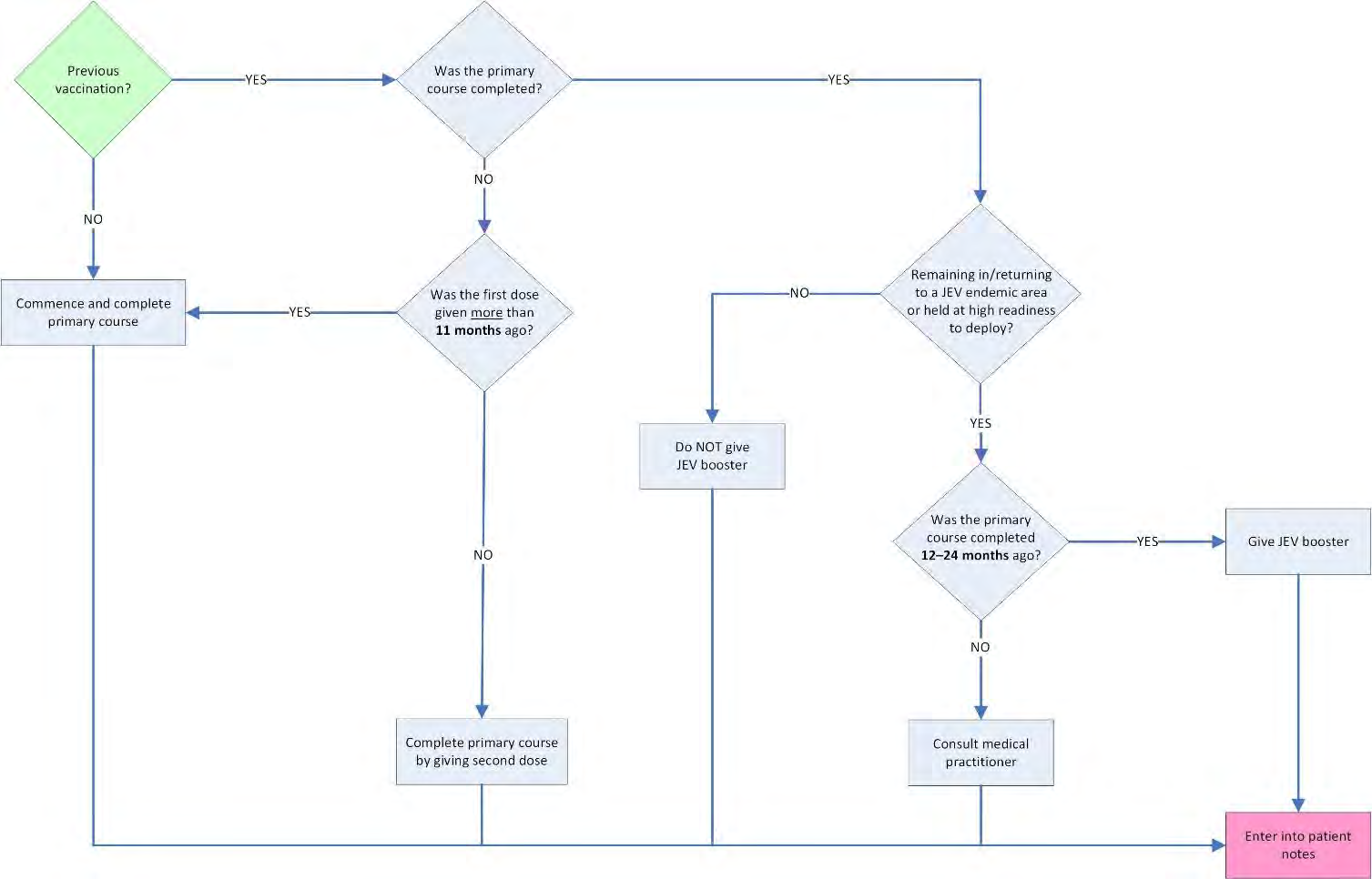
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Japanese Encephalitis Vaccine (Alternative option)
(Enhanced Programme)
Inactivated Japanese Encephalitis Vaccine (adsorbed)
Available Product
Jespect®
Each 0.5 mL dose contains:
Japanese encephalitis virus (purified, inactivated): 6 antigen units (AgU)
Cloudy white suspension for injection. Storage may cause the vaccine to appear as a fine white
deposit with a clear colourless supernatant.
Indication
Active immunisation against Japanese Encephalitis (Alternative JEV vaccine option for the NZDF)
Authorisation
Authorising Document (to include High Readiness Nominal Roll)
47
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Dosage and Route of Shake well before use. Once shaken, the vaccine should appear as a white cloudy suspension.
Administration
Primary vaccination
Administer the required number of doses of 0.5 mL by intramuscular injection (deltoid area
recommended), to complete the following schedule:
First dose:
on day 0
Second dose:
on day 28
Notes:
1. If the second dose is delayed, it can be given up to 11 months after the first dose;
otherwise, the primary course is to be restarted.
2. If the primary course cannot be completed within the required time period, consult
with a medical practitioner.
Booster dose
A booster dose of 0.5 mL by intramuscular injection (deltoid area recommended) can be given
between 12 and 24 months following completion of the primary vaccination for those individuals
remaining in or returning to a JEV endemic area or held at high readiness to deploy. The
authorising document for those held at high readiness to deploy is to be the High Readiness
Nominal Roll. This booster provides immunity for a further 10-year period.
Contraindications
WARNING: Patients with a hypersensitivity reaction after the first dose
should not be given a second dose.
Known hypersensitivity to any component of the vaccine
Hypersensitivity after previous vaccination with Jespect®
Acute systemic illness with fever over 38°C
Precautions
Thrombocytopenia or a bleeding disorder
Immunosuppression
Pregnancy – refer to medical practitioner
Breastfeeding – refer to medical practitioner
Occupational
The primary course should be completed at least 7 days prior to potential exposure to JEV. If a
Considerations
person is travelling to a JE endemic area and is unable to complete the primary course or they
will enter within 7 days of receiving their primary course, they and their command chain are to
be made aware of their unknown protection status.
NZDF Aircrew are to be stood down for 12 hours following administration.
NZDF Divers are to be stood down for 72 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
Side Effects
Local reactions (including pain, inflammation, redness)
Nausea
Headache
Influenza-like illness
Myalgia
Rash
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria, anaphylaxis)
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
Interactions
practitioner
48
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult Stockley’s
alerts (available through the NZ Formulary).
Information for
Encourage the patient to read the Patient Information Leaflet.
patients
Scope authorised to
Current NZDF Vaccinator
administer this
medicine
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
Jespect® can be used as a booster to previous JE-Vax and Green Cross courses.
information
Jespect® is indicated only for use in persons 18 years of age and older.
Jespect® is marketed in the US, Europe, Canada, Hong Kong and Singapore under the trade
name IXIARO® and in Australia and New Zealand as Jespect®
An accelerated course of JEV vaccine may be used only after consultation, approval and under
the authority of a prescription from a medical practitioner.
49
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Meningococcal A, C, W-135 and Y Vaccine
(Enhanced Programme)
MenACWY-D quadrivalent meningococcal conjugate vaccine
MenACWY-T quadrivalent meningococcal conjugate vaccine
Preparations
Menactra® (MenACWY-D)
Each 0.5 mL dose contains:
Meningococcal polysaccharide Group A: 4 micrograms
Meningococcal polysaccharide Group C: 4 micrograms
Meningococcal polysaccharide Group Y: 4 micrograms
Meningococcal polysaccharide Group W-135: 4 micrograms
Diphtheria toxoid protein: 48 micrograms
Clear to slightly turbid solution for injection
MenQuadfi® (MenACWY-T)
Each 0.5 mL dose contains:
Meningococcal polysaccharide Group A: 10 micrograms
Meningococcal polysaccharide Group C: 10 micrograms
Meningococcal polysaccharide Group Y: 10 micrograms
Meningococcal polysaccharide Group W-135: 10 micrograms
Tetanus toxoid protein: 55 micrograms
Clear, colourless solution for injection
Indication
Active immunisation against meningococcal disease caused by
Neisseria meningitidis serogroups
A, C, W-135 and Y
Authorisation
Ab initio trainees aged <25 years who have not received a previous MenA,C,W,Y vaccine in the last
4 years
Individuals aged ≤25 years who are in their first 12 months of living in shared service
accommodation who have not received a previous MenA,C,W,Y vaccine in the last 4 years
Authorising Document: no booster to be given within 5 years of any previous MenA,C,W,Y vaccine
Dosage and Route of Shake gently before use.
Administration
CAUTION: Check whether patient has received a previous MenA,C,W,Y vaccine and
refer to Authorisation.
Primary vaccination
Administer one dose of 0.5 mL by intramuscular injection (deltoid area recommended).
Booster
Refer to Authorisation for booster direction
50
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Contraindications
Known hypersensitivity to any component of the vaccine or other Meningococcal A, C, W-135
and Y vaccines
Hypersensitivity after previous vaccination with Meningococcal A, C, W-135 and Y vaccines
Acute systemic illness with fever over 38°C
Precautions
Thrombocytopenia or a bleeding disorder
Pregnancy
Breastfeeding
13-valent Pneumococcal conjugate vaccine (PCV13) administration in last four weeks
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
Side Effects
Local reactions (including pain, inflammation, redness)
Arthralgia / myalgia
Gastrointestinal disturbances
Anorexia
Chills/fever
Headache
Malaise
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria, anaphylaxis)
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
Interactions
practitioner
PCV13 – administration of PCV13 and MenACWY-D should be separated by at least four weeks
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult Stockley’s
alerts (available through the NZ Formulary).
Information for
Encourage the patient to read the Patient Information Leaflet.
patients
Scope authorised to
Current NZDF Vaccinator
administer this
medicine
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
information
51
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Meningococcal B Vaccine
(Enhanced Programme)
Meningococcal B Recombinant, Adsorbed Vaccine
Available Product
Bexsero®
Each 0.5 mL dose contains:
Neisseria meningitidis Group B NHBA fusion protein:
50 micrograms
Neisseria meningitidis Group B NadA protein:
50 micrograms
Neisseria meningitidis Group B fHbp fusion protein:
50 micrograms
Neisseria meningitidis Group B outer membrane vesicles:
25 micrograms
Clear, colourless suspension for injection. Storage may cause the vaccine to appear as a fine white
deposit with a clear colourless supernatant.
Indication
Active immunisation against meningococcal disease caused by
Neisseria meningitidis serogroup B
Authorisation
Ab initio trainees
Individuals aged ≤25 years who are in their first 12 months of living in shared service
accommodation
Authorising Document
Dosage and Route of Shake well before use to form a uniform suspension.
Administration
Primary vaccination
Administer the required number of doses of 0.5 mL by intramuscular injection (deltoid area
recommended), to complete the following schedule:
First dose:
on day 0
Second dose:
at least 8 weeks after first dose
Booster dose
No booster required following completion of the primary vaccination course
Contraindications
Known hypersensitivity to any component of Bexsero®
Hypersensitivity after previous vaccination with Bexsero® or other meningitis B vaccines
Acute systemic illness with fever over 38°C
Precautions
Thrombocytopenia or a bleeding disorder
Pregnancy
Breastfeeding
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
52
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Side Effects
Local reactions (including pain, inflammation, redness)
Headache
Nausea
Myalgia
Arthralgia
Rash
Generally feeling unwell or tired
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria, anaphylaxis)
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
Interactions
practitioner.
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult Stockley’s
alerts (available through the NZ Formulary).
Information for
Encourage the patient to read the Patient Information Leaflet
patients
Scope authorised to
Current NZDF Vaccinator
administer this
medicine
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
The safety and efficacy of Bexsero® in patients over 50 years of age have not been established.
information
53
link to page 8
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Rabies Vaccine
(Enhanced Programme)
Inactivated Rabies Virus Vaccine
Available Products
Verorab Inactivated Rabies Vaccine (Verorab)®
Each 0.5 mL dose of the reconstituted vaccine contains:
Inactivated Wistar rabies virus strain: 3.25 International Units
There are two components to the Verorab vaccine:
the vaccine – a white homogenous pellet
the diluent – 0.4% sodium chloride solution in a pre-filled syringe which when constituted
forms a uniformly clear and colourless solution.
Rabipur®
Each 1 mL dose of the reconstituted vaccine contains:
Inactivated rabies virus: 2.5 International Units
There are two components to the Rabipur vaccine:
the vaccine – lyophilised powder in a glass vial
the diluent – diluent in ampoule
Indication
Active immunisation for
pre-exposure prophylaxis against Rabies
Authorisation
Authorising Document
Dosage and Route of To prepare one dose of rabies vaccine—
Administration
Add the entire volume of diluent to the vial of vaccine powder.
Gently swirl the vial to avoid foaming.
Reconstituted Verorab should be uniformly clear and colourless.
Reconstituted Rabipur should be clear to slightly opalescent and colourless to slightly pink.
Primary vaccination
Administer the required number of doses of 0.5 mL of Verorab or 1 mL of Rabipur by
intramuscular injection (deltoid area recommended) to complete the following schedule:
First dose:
on day 0
Second dose:
on day 7
Note: The above two-dose regimen is unapproved
(off-label use), so informed consent is
required.
Note: Immunocompromised individuals are to be referred for medical practitioner
assessment and consideration of a three-dose regimen.
Note: If the primary course cannot be completed within the required time period, consult
with a medical practitioner.
54
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Booster
Administer 0.5 mL of Verorab or 1 mL of Rabipur by intramuscular injection (deltoid area
recommended).
Note: A third dose (booster) is required where a two-dose regimen was given and an individual is
planning another visit to an endemic area more than 3 years after the initial two doses. No further
booster doses are required following a three-dose regimen.
Contraindications
Known hypersensitivity to any component of the vaccine or other rabies vaccines including
hypersensitivity to neomycin or other antibiotics of the same class (aminoglycoside)
Hypersensitivity after previous vaccination with rabies vaccines
Acute systemic illness with fever over 38°C
Precautions
Thrombocytopenia or a bleeding disorder
Immunosuppression
Pregnancy – refer to medical practitioner
Breastfeeding – refer to medical practitioner
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
Side Effects
Local reactions (including pain, inflammation, redness)
Myalgia and asthenia
Arthralgia
Lymphadenopathy
Influenza-like symptoms
Headache
Malaise
Fever
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria, anaphylaxis)
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
Interactions
practitioner
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult Stockley’s
alerts (available through the NZ Formulary).
Information for
Encourage the patient to read the Patient Information Leaflet.
patients
Scope authorised to
Current NZDF Vaccinator
administer this
medicine
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
Post-exposure prophylaxis:
information
o Consists of local treatment of a wound, initiated as soon as possible after an exposure. This
is followed by administration of rabies vaccine with or without immunoglobulin depending
55
Released under the Official Information Act 1982
Version 5.01
25 March 2026
upon the category of exposure to the suspected rabid animal and the patient’s
immunisation status.
o Administration of rabies vaccine for post-exposure prophylaxis may be conducted only
under the authority of a prescription from a medical practitioner.
Booster doses:
o may be required for high risk exposure groups, for example those undertaking animal
control activities, veterinarians or force health protection personnel; and
o may be given only after consultation, approval and under the authority of a prescription
from a medical practitioner.
56
link to page 7
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Tick Borne Encephalitis (TBE) Vaccine
(Enhanced Programme)
Inactivated TBE Virus Vaccine
Available Products
TicoVac™ (FSME-IMMUN)
Each 0.5 mL dose of the vaccine contains 2.4 mcg of inactivated TBE virus.
The TicoVac™ vaccine is a pre-mixed suspension in a single use pre-filled syringe for intramuscular
injection.
Encepur®
Encepur® is not to be used for the initial two doses of vaccination. It is interchangeable with
TicoVac™ for third and booster doses.
Indication
Active immunisation for
pre-exposure prophylaxis against TBE.
Authorisation
Authorising Document
Dosage and Route of To prepare one dose of TBE vaccine—
Administration
Bring the vaccine to room temperature before administration.
Shake well to mix the vaccine suspension.
The vaccine should be a homogeneous off-white, opalescent suspension.
The vaccine should be inspected visually for particulate matter and discolouration prior to
administration.
Do not administer if particulate matter or discolouration remains after shaking.
Primary vaccination
Administer the required doses of 0.5 mL of TicoVac by intramuscular injection (deltoid area
recommended) to complete the following schedule:
First dose:
on day 0
Second dose: 1–3 months after first dose
Accelerated schedule may be authorised and given no earlier than day 14
Third dose: 5–12 months after second dose if continued exposure expected
Note: This is an unappro
ved Section 29 medicine, so informed consent is required.
Note: Immunocompromised individuals are to be referred for medical practitioner assessment.
Note: If the first two doses cannot be completed within the required time period, consult with a
medical practitioner.
57
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Booster
Administer 0.5 mL of TicoVac™ or Encepur® by intramuscular injection (deltoid area
recommended).
Note: A booster is required where the primary regimen was given and an individual remains in or
is planning another visit to an endemic area more than 3 years after the third dose was
administered. After the first booster dose, boosters need to be administered only every 5 years
until age 60 years, then 3 yearly thereafter (subject to continued exposure risk).
Contraindications
Known hypersensitivity to any component of the vaccine or other TBE vaccines
Hypersensitivity after previous vaccination with TBE vaccines
Acute systemic illness with fever over 38°C
Precautions
Thrombocytopenia or a bleeding disorder
Immunosuppression
Pregnancy – refer to medical practitioner. Insufficient human data on risk. In the context
of NZDF vaccination, consider defer future doses subject to deployments
Breastfeeding – refer to medical practitioner. Human data not available. In the context of
NZDF vaccination, consider defer future doses subject to deployments.
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
Side Effects
Local reactions (including pain, inflammation, redness)
Myalgia and asthenia
Arthralgia
Lymphadenopathy
Influenza-like symptoms
Headache
Malaise
Fever
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria, anaphylaxis)
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
Interactions
practitioner
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult
Stockley’s alerts (available through the NZ Formulary).
Information for
Encourage the patient to read the Patient Information Leaflet.
patients
Scope authorised to
Current NZDF Vaccinator
administer this
medicine
58
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
Vaccination against TBE should include a minimum of the initial 2 doses, with these
information
2 doses completed at least one week prior to potential exposure to TBE.
Completion of the primary course (ie the third dose) may need to occur in location once
deployed
It is important that the initial 2 doses, at least, are the same vaccine (e.g. TicoVac)
Encepur is the other commonly available vaccine in Europe, and is considered
interchangeable with TicoVac, for third and booster doses.
In most cases, the third dose should still be administered after return to New Zealand if
there is a chance the person will deploy to a TBE endemic region in the future.
Authorisation to administer TBE vaccine includes completing the full 3-dose schedule,
even if the third dose is administered after return to New Zealand.
Vaccine effectiveness (VE) after only two initial doses is around 95.3% at 5 months (VE
expressed as % of people who are seropositive after 2 doses). This is valid if the second
dose was administered on or after 21 days. Therefore a 2 dose regimen is considered
appropriate for a one-off deployment for a period no greater than 5 months after the
second dose.
59
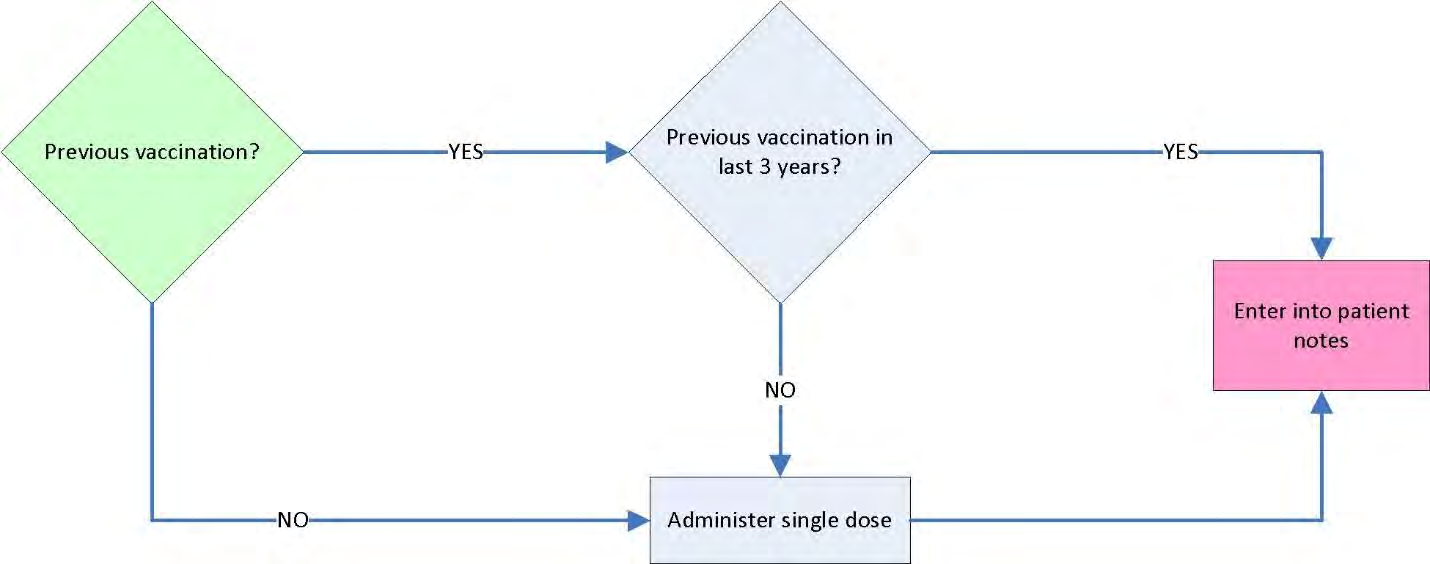
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Typhoid Vaccine
(Enhanced Programme)
Typhoid Vi Polysaccharide Vaccine
Preparation
Typhim Vi®
Each 0.5 mL dose contains:
Salmonella typhi Vi polysaccharide: 25 micrograms
Clear, colourless solution for injection
Indication
Active immunisation against Typhoid fever
Authorisation
Authorising Document
Dosage and Route
Primary vaccination
of Administration
Administer a single dose of 0.5 mL by intramuscular injection (deltoid area recommended).
Booster dose
Administer a single dose of 0.5 mL by intramuscular injection (deltoid area recommended).
Contraindications
Known hypersensitivity to any component of the vaccine or other typhoid vaccines
Hypersensitivity after previous vaccination with typhoid vaccines
Acute systemic illness with fever over 38°C
Precautions
Thrombocytopenia or a bleeding disorder
Pregnancy
Breastfeeding
Occupational
NZDF Aircrew are to be stood down for 12 hours following administration.
Considerations
NZDF Divers are to be stood down for 48 hours following administration.
Personnel must be symptom free from any side effects before returning to duties.
60
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Side Effects
Local reactions (including pain, inflammation, redness)
Myalgia and asthenia
Headache
Malaise
Fatigue
Hypersensitivity reactions (including bronchospasm, angioedema, urticaria, anaphylaxis)
Significant Drug
Immunosuppressive medicines may reduce the response to the vaccine – refer to medical
Interactions
practitioner.
Many medicines have multiple interactions with non-DML medicines. If the patient is on a
medicine with which you are unfamiliar, refer to a medical practitioner or consult Stockley’s
alerts (available through the NZ Formulary).
Information for
Encourage the patient to read the Patient Information Leaflet.
patients
Scope authorised
Current NZDF Vaccinator
to administer this
medicine
Countersigning
Countersignature not required
Clinical
No additional documentation required
Documentation
Additional
Vaccination with Typhim Vi® should occur at least 2 weeks prior to potential exposure to the
information
Salmonella typhi organism.
Typhim Vi® provides protection against the risk of infection related to
Salmonella typhi, but
gives no protection against
Salmonella paratyphi A or B or against non-typhoidal Salmonellae.
61
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Other MSOs
62
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Adrenaline
(a-dren-a-lin)
sympathomimetic
Adrenaline 1 mg in 1 mL Injection
Indication
Anaphylactic shock following vaccination
Dosage and Route
Administer 0.5 mg (0.5 mL of the adrenaline 1 mg in 1 mL injection)
of Administration
intramuscularly (preferably in the upper outer thigh) immediately.
Repeat every 5–15 minutes as needed whilst awaiting medical assistance.
Available Product
1 mg in 1 mL ampoule
Contraindications
• There are no contraindications to adrenaline administered for anaphylaxis.
Precautions
• Myocardial ischaemia
• Tachydysrhythmias
• Hypercalcaemia
• Hypokalaemia
• Sulfite allergy
Occupational
• None
Considerations
Side Effects
• Tachydysrhythmias
• Myocardial ischaemia/infarction
• Hypertension
• Nausea; vomiting
• Tremor, anxiety, sweating
• Cold extremities
• Hyperglycaemia
Significant Drug
• Beta-blockers (eg propranolol, metoprolol, atenolol)—severe anaphylaxis
Interactions
may not respond to adrenaline; refer to a medical practitioner
• Tricyclic antidepressants (eg amitriptyline, nortriptyline, clomipramine)—
refer to a medical practitioner
• Mono-amine oxidase inhibitor antidepressants (eg tranylcypromine,
moclobemide)—refer to a medical practitioner
Information for
• None
Patients
Special Notes
• US name: Epinephrine
• Adrenaline 1 mg in 1 mL injection is also known as adrenaline 1:1,000 injection.
• Injection may contain sulfites.
Scope authorised
Current NZDF Vaccinator
to administer this
medicine
Countersigning
• No countersignature required
63
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Clinical
• Report to Ministry of Health MedSafe
Centre for Adverse Reactions to Medicines
Documentation
(CARM)
• This is a healthcare incident. See
DHR 02 Applied Health Regulation, Part 5, Chapter 2
Healthcare Incident Management Processes
64
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Record of Amendments
Version
Issue Date
Details of Change
Authority
2.00
1 December 2022
Initial Issue of Revised Format Vaccine SO
LTCOL R Duncan
2.01
01 February 2023
Addition of MenQuadfi to Meningococcal ACWY
LTCOL R Duncan
prescription
Inclusion of 2023 Seasonal Influenza vaccine
2.02
05 April 2023
Inclusion of COVID-19 vaccine
LTCOL R Duncan
2.03
27 September 2023
Changes to the Authorisations for the
LTCOL R Duncan
Meningococcal A, C, W-135 and Y Vaccine and
the Meningococcal B Vaccine
2.04
11 October 2023
Minor formatting changes not affecting intent
LTCOL R Duncan
Addition of catch-up programme to
Authorisation for the Meningococcal B Vaccine
2.05
05 December 2023
Replace the COVID-19 Immunisation Register
LTCOL R Duncan
(CIR) with the Aotearoa Immunisation Register
(AIR) in the COVID-19 MSO
3.00
07 February 2024
Name change from VSO to VTP and full review of
LTCOL R Duncan
contents.
Minor formatting changes not affecting intent.
Change in timeframe for recommended pertussis
protection for military partners of pregnant
women or those with newborns.
3.01
07 March 2024
Updated Influenza vaccine to 2024 product.
LTCOL R Duncan
Updated COVID-19 booster vaccine. Added
hyperlink to MOH booster eligibility criteria.
3.02
10 April 2024
Updated COVID-19 vaccine primary course and
LTCOL R Duncan
flowchart.
Added option of shorter observation period for
individuals after receiving an influenza vaccine if
they meet IMAC criteria.
3.03
02 August 2024
Added third indication for tetanus vaccination.
LTCOL R Duncan
Replaced Merieux Inactivated Rabies Vaccine
with Verorab Inactivated Rabies Vaccine.
65
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Version
Issue Date
Details of Change
Authority
3.04
04 September 2024
Added a section on off-label use.
LTCOL R Duncan
JEV vaccine MSO: added a booster dose.
Hepatitis B vaccine MSO: added note on
situations where a third dose is not required.
HPV vaccine MSO: added note on situations
where a third dose is not required.
Tdap vaccine MSO: amended the ‘Additional
note’ regarding Indication 3 to direct that
medical practitioner consultation for wound
assessment be considered where clinically
indicated.
Rabies vaccines MSO: added notes regarding the
two-dose regimen and added a booster dose.
3.05
06 November 2024
Added ‘NZDF divers’ as a group authorised to
LTCOL R Duncan
receive boosters for COVID vaccine and influenza
vaccine, in accordance with DHR 37.
Removed information about the 2023 influenza
vaccine.
As per DHR37, after receiving vaccinations, divers
are to be stood-down from diving for a period of
48 hours (with the exception of the Japanese
Encephalitis Vaccine, which requires a 72-hour
stand-down).
4.00
05 February 2025
Annual full review of contents.
LTCOL R Duncan
Updated COVID-19 vaccine MSO and flowchart.
4.01
12 March 2025
Updated Influenza vaccine to 2025 product.
LTCOL R Duncan
4.02
07 May 2025
Changes to the Authorisations for the
LTCOL R Duncan
Meningococcal A, C, W-135 and Y Vaccine
Removal of booster dose caution from the
Typhoid Vaccine
4.03
16 July 2025
Addition of Section 29 information
LTCOL R Duncan
Addition of third dose for the MMR vaccine
Addition of TBE vaccine MSO
4.04
10 September 2025
Addition of Dengue Disease Vaccine MSO
LTCOL R Duncan
4.05
03 October 2025
Addition of Adrenaline MSO
LTCOL R Duncan
5.00
04 February 2026
Removal of ‘Previous diagnosis of Guillain Barre
LTCOL R Duncan
Syndrome’ from the list of precautions in the
Meningococcal A, C W-135 and Y vaccine MSO
Change to the clinical documentation statement
in the Poliomyelitis Vaccine MSO
66
Released under the Official Information Act 1982
Version 5.01
25 March 2026
Version
Issue Date
Details of Change
Authority
5.01
25 March 2026
Update of the influenza vaccine MSO
LTCOL R Duncan
Update of the COVID-19 vaccine MSO
Addition of the IMOJEV® MSO
Minor changes to the Jespect® MSO
67
Document Outline