GOV-045703
From:
[Out of Scope]
@matai.org.nz>
Sent:
Tuesday, 16 December 2025 10:36 am
To:
[Out of Scope]
Subject:
Re: Tūārai quarterly report - Brain injury and concussion
[Out of Scope]
.
Definitely keen on that coffee
.
From: [Out of Scope]
@acc.co.nz>
Date: Tuesday, 16 December 2025 at 10:31 AM
To: [Out of Scope]
@matai.org.nz>
Subject: RE: Tūārai quarterly report - Brain injury and concussion
Thanks [Out of Scope] – me too re: [Out of Scope] [Out of Scope]
[Out of Scope]
That’s great what you have provided thanks [Out of Scope] and how about we have a coffee date in the new year my shout
From: [Out of Scope]
@matai.org.nz>
Sent: Tuesday, December 16, 2025 9:28 AM
To: [Out of Scope]
@acc.co.nz>
Subject: Re: Tūārai quarterly report - Brain injury and concussion
Kia ora [Out of Scope]
Sorry if the quick email, [Out of Scope]
.
It was so lovely to see you at the symposium and I really appreciate your kind words. It’s always hard putting your
story out there and hoping it resonates somehow.
Re: the reporting, how’s this?
Ngā mihi,
[Out of Scope]
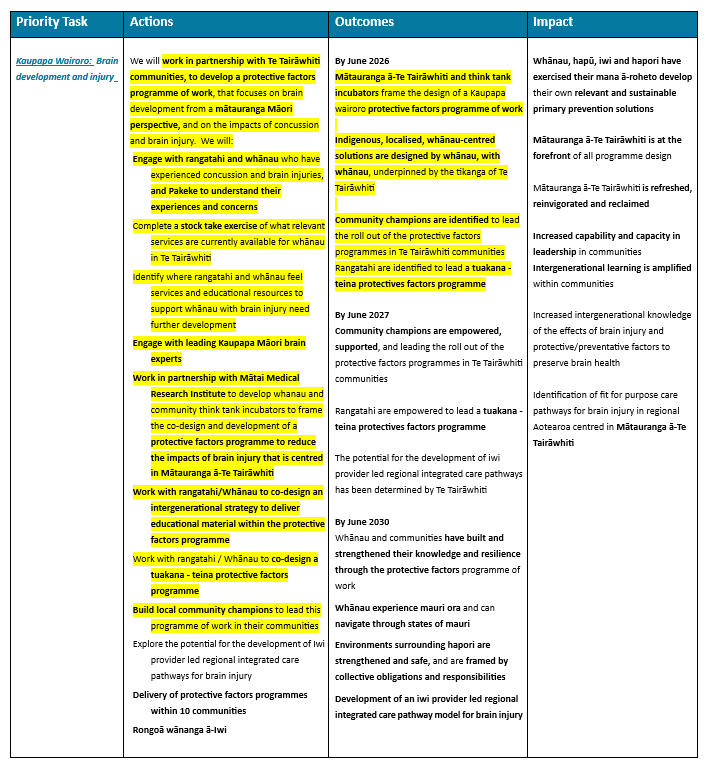
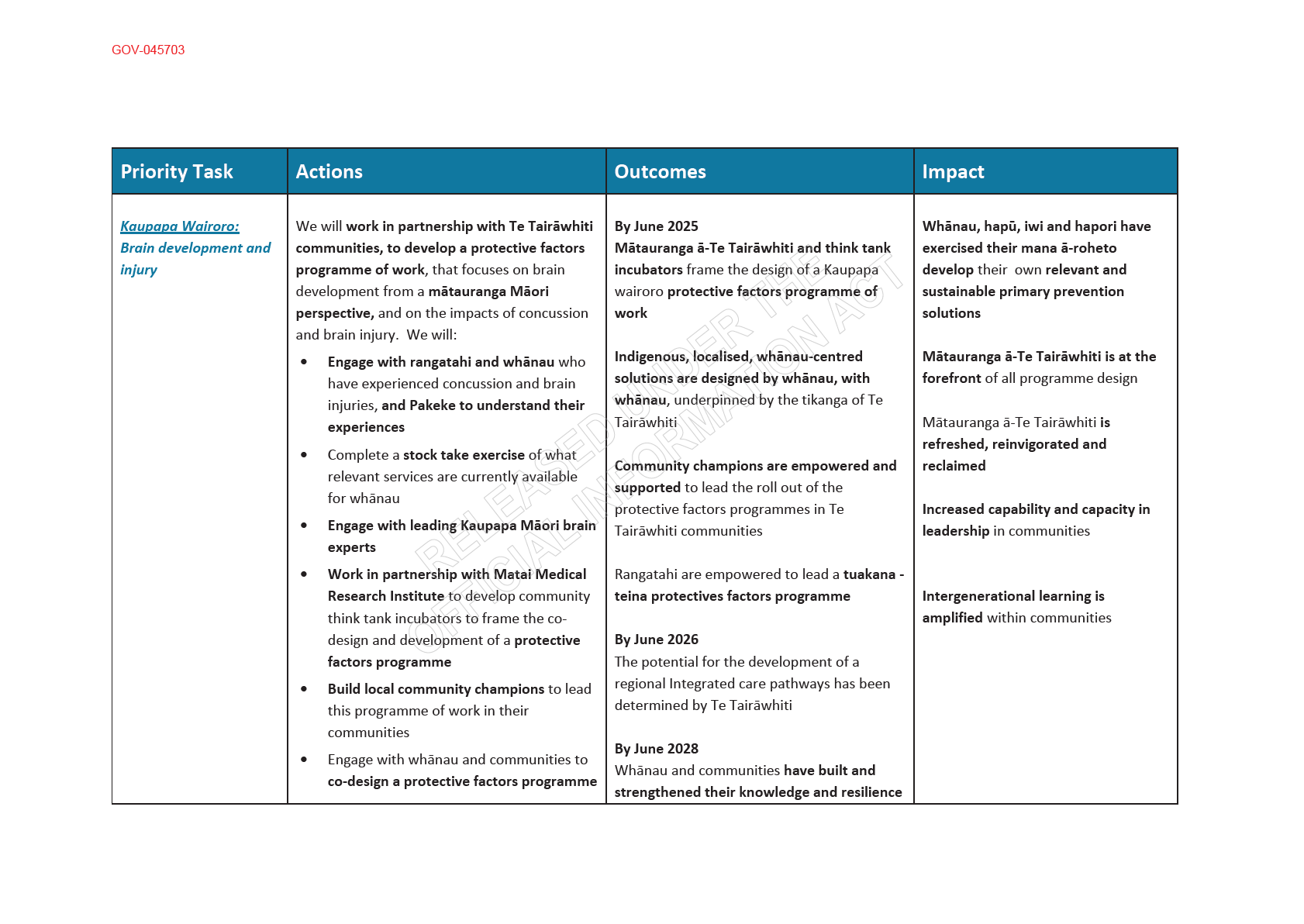
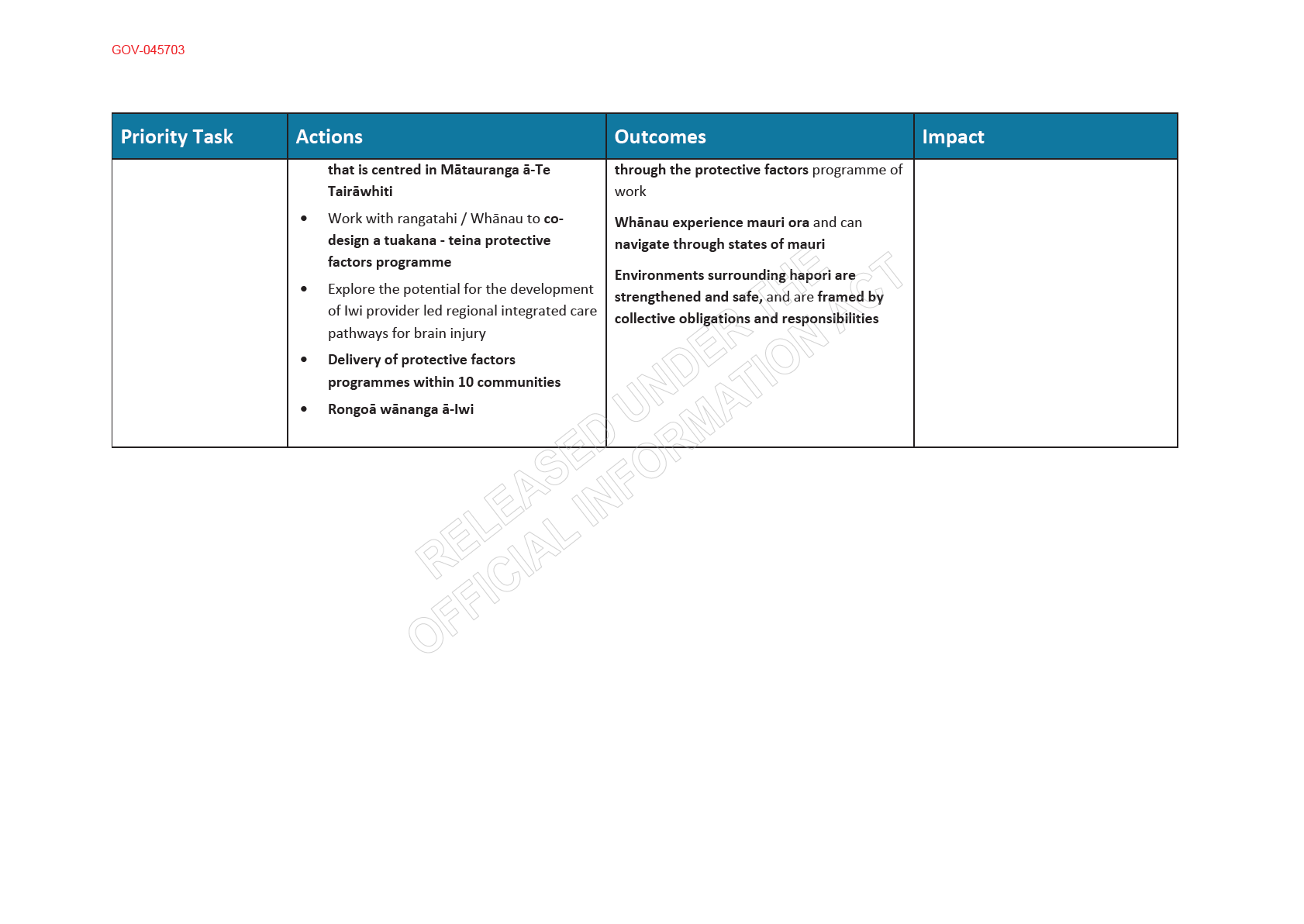
Kaupapa Wairoro: Brain Development and Injury
Community engagement and knowledge-sharing have been central to progress under Kaupapa Wairoro. A major
highlight was the Mātai Symposium, which brought together more than 60 national and international
speakers and over 300 attendees across Saturday and Sunday. The symposium provided a significant forum for
open kōrero on brain development, concussion, and brain injury, weaving together mātauranga Māori, lived
experience, clinical practice, and research evidence. Strong attendance from whānau, clinicians, researchers,
1
GOV-045703

GOV-045703
From:
[Out of Scope]
@matai.org.nz>
Sent:
Wednesday, 12 March 2025 6:29 am
To:
[Out of Scope]
Cc:
Tuterangi Nepe-Apatu
Subject:
Re: Kaupapa Wairoro Brain development and injury
Attachments:
Kaupapa Wairoro Brain development and injury_Mātai.docx
Mōrena [Out of Scope]
Apologies for the delay.
Please find attached our up-dated table for the Kaupapa Wairoro.
Ngā mihi,
[Out of Scope]
Kaiwhakahaere/Chief Operations Officer
Mātai Medical Research Institute
466 Childers Road
PO Box 359, Gisborne 4010
New Zealand
P [Out of Scope]
W www.matai.org.nz
From: [Out of Scope]
@acc.co.nz>
Date: Thursday, 6 March 2025 at 9:19 AM
To: [Out of Scope]
@matai.org.nz>
Cc: [Out of Scope]
@matai.org.nz>
Subject: RE: Kaupapa Wairoro Brain development and injury
Mōrena - No worries
From: [Out of Scope]
@matai.org.nz>
Sent: Thursday, March 6, 2025 9:12 AM
To: [Out of Scope]
@acc.co.nz>
Cc: [Out of Scope]
@matai.org.nz>
Subject: Re: Kaupapa Wairoro Brain development and injury
Kia ora [Out of Scope]
1

GOV-045703
I hope you’re having a great week.
Just letting you know I haven’t forgotten this. Should have this to you by Friday PM.
Ngā mihi,
[Out of Scope]
Kaiwhakahaere/Chief Operations Officer
Mātai Medical Research Institute
466 Childers Road
PO Box 359, Gisborne 4010
New Zealand
P [Out of Scope]
W www.matai.org.nz
From: [Out of Scope]
@acc.co.nz>
Date: Monday, 24 February 2025 at 3:38 PM
To: [Out of Scope]
@matai.org.nz>
Subject: Kaupapa Wairoro Brain development and injury
As promised
Disclaimer:
"This message and any attachments may contain confidential and privileged information. If you believe
you have received this email in error, please advise us immediately by return email or telephone and
then delete this email together with all attachments. If you are not the intended recipient, you are not
authorised to use or copy this message or any attachments or disclose the contents to any other
person."
2
GOV-045703
From:
[Out of Scope]
@matai.org.nz>
Sent:
Monday, 16 June 2025 11:13 am
To:
[Out of Scope]
Subject:
Re: Data
Importance:
High
Hey [Out
of Scop
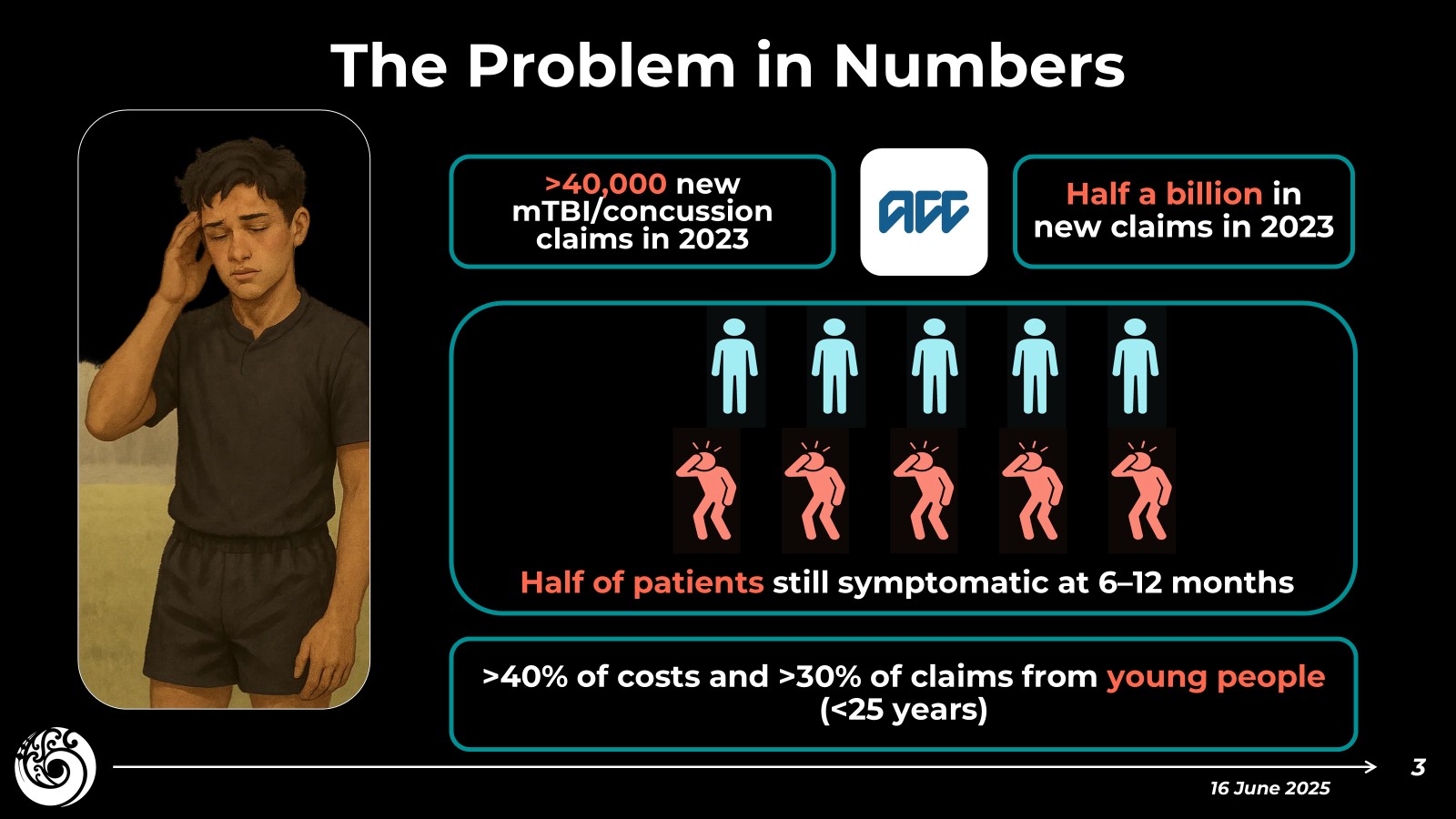
Want to have a quick look at the screenshots of these slides for my talk next week. Still need to add the
referencing. Numbers are based on the spreadsheets you sent through. Main one I want to clear is the ½ billion
claim costs of mTBI/concussion in 2023 to ACC. Here's how I came up with this:
1. Since generally sports-related injuries are 20% of all brain injuries. I multiplied the 80 million figure for
sports related injuries by 5 equalling 400 million
2. I used the findings of Te Ao 2014 that said the costs of mTBI/concussion are three times that
of moderate/severe in NZ. So I took the active costs of all injuries in 2023 (866 million) divided by four, and
multiplied the result by three for an estimate of ~650 million.
3. I split the difference between these two estimates to land at half a billion.
I have to submit my final slides by this Wednesday. So if you want me to update this let me know.
[Out
of Scop
1

GOV-045703
[Out of Scope]
, PhD.
Senior Research Fellow
Honorary Research Fellow, Anatomy & Medical Imaging, University of Auckland
Neurological Foundation First Fellowship
Mātai Medical Research Institute
466 Childers Road
PO Box 359, Gisborne 4040
New Zealand
M [Out of Scope]
W www.matai.org.nz
From: [Out of Scope]
@matai.org.nz>
Sent: Wednesday, June 11, 2025 13:42
To: [Out of Scope]
@acc.co.nz>
Subject: Re: Data
Thanks.
Another quick question. Can you share any data on the # of cases and cost of cases of all mTBI (not just sports-
related)? If not, I think I can reverse engineer an estimate from the data you provided by applying the findings from
the attached paper to the current data.
[Out of Sco
From: [Out of Scope]
@acc.co.nz>
Sent: Monday, June 9, 2025 10:43
To: [Out of Scope]
@matai.org.nz>
Subject: RE: Data
Yes. That was the address I used. I will just hang on to it until you come to Wellington.
2


GOV-045703
[Out
of Scope]
, (She/Her)
Injury Prevention Partner - Sport and TBI, ACC
| Mobile +[Out of Scope] |
Targeted Investment-0580 | Wellington - Justice Centre
ACC |
| Wellington 6011 | New Zealand
ACC Website | ACC Newsroom | Facebook | Instagram | LinkedIn | YouTube | TikTok
From: [Out of Scope]
@matai.org.nz>
Sent: Monday, 9 June 2025 10:39 am
To: [Out of Scope]
@acc.co.nz>
Subject: Re: Data
Thank you.
I didn't send it back so there must have been an issue with delivery. The address was 466 Childers Road, right?
[Out
of Scop
From: [Out of Scope]
@acc.co.nz>
Sent: Monday, June 9, 2025 10:27
To: [Out of Scope]
@matai.org.nz>
Subject: RE: Data
No problem.
Answer below.
On Friday I received the Sports Med presentation gift of thanks back in the post. It was a ‘Return to Sender’. Did
you yu send it back or did it not reach you? It just aid on the envelope ‘unclaimed’.
3


GOV-045703
[Out
of Scope]
, (She/Her)
Injury Prevention Partner - Sport and TBI, ACC
| Mobile +[Out of Scope] |
Targeted Investment-0580 | Wellington - Justice Centre
ACC |
| Wellington 6011 | New Zealand
ACC Website | ACC Newsroom | Facebook | Instagram | LinkedIn | YouTube | TikTok
From: [Out of Scope]
@matai.org.nz>
Sent: Monday, 9 June 2025 10:20 am
To: [Out of Scope]
@acc.co.nz>
Subject: Re: Data
Thanks so much for this. Just to clarify if I report the ~ $80 million costs from 2024 in Copy of AR-8078 Sports-
Related Concussion Data.xlsx is that cost specific to just 2024? Yes
Also, to clarify the # of claims on 2024. Is the active claims number (13,593) inclusive of the 12,045 new claims in
2024 meaning 1,548 existing claims rolled into 2024 from previous years. This is correct and the $80m cost above
covered the active claims. Or is the total number of claims >25,000 for 2024?
[Out
of Scop
From: [Out of Scope]
@acc.co.nz>
Sent: Friday, June 6, 2025 10:17
To: [Out of Scope]
@matai.org.nz>
Subject: Data
[Out of Scop,
4


GOV-045703
Good to chat yesterday.
A few differ ent cuts of data attached for you to have a look at and pick out whatever is useful. These have all been
signed out for external use.
I will put something in for the morning of 25 June – I will be on touch on that.
[Out of
Scope]
, (She/Her)
Injury Prevention Partner - Sport and TBI, ACC
| Mobile +[Out of Scope] |
Targeted Investment-0580 | Wellington - Justice Centre
ACC |
| Wellington 6011 | New Zealand
ACC Website | ACC Newsroom | Facebook | Instagram | LinkedIn | YouTube | TikTok
Disclaimer:
"This message and any attachments may contain confidential and privileged information. If you believe
you have received this email in error, please advise us immediately by return email or telephone and
then delete this email together with all attachments. If you are not the intended recipient, you are not
authorised to use or copy this message or any attachments or disclose the contents to any other
person."
5
link to page 26 link to page 26 link to page 26 link to page 26 link to page 26 link to page 26 link to page 26 link to page 26 link to page 26
link to page 26 link to page 27 link to page 26 link to page 26 link to page 27 link to page 26 link to page 26 link to page 27 link to page 27 link to page 26 link to page 27 link to page 27 link to page 27 link to page 27 link to page 27 link to page 27 link to page 27 link to page 27 link to page 27 link to page 26 link to page 27 link to page 27 link to page 27 link to page 27 link to page 26 link to page 27 link to page 15
CTE in the Sydney
GOV-045703 Brain Bank
BRAIN COMMUNICATIONS 2022: Page 3 of 17 | 3
neuronal and astrocytic phosphorylated tau pathology lo-
evidence of CTE-NC, using a strict definition of CTE-NC,
cated in
a perivascular distribution in the sulcal depths was
in their
cases.30
indicative of CTE-NC.
18 Other supportive features proposed
We have assessed cortical regions of 636 neurodegenera-
from both this study and a subsequent consensus study in
tive disease and normal healthy control cases in the Sydney
2021
19 are the presence of neuronal tau in superficial cortical
Brain Bank to ascertain the prevalence of CTE-NC using
layers and the CA2 and CA4 regions of the hippocampus,
both the first and second consensus criteria.
18,19 A subset
subcortical neuronal and astrocytic tau and tau grains.
of cases was identified with a history of TBI with or without
Non-tau pathological supportive features include TAR
loss of consciousness and a small proportion of these cases
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
DNA binding protein 43 (TDP-43) positive inclusions and
also had a history of contact sport played regularly at the
neurites in the medial temporal lobe, macroscopic changes
professional or club level. We provide evidence of low preva-
consisting of cortical and subcortical brain atrophy, enlarge-
lence of CTE-NC, even in cases with history of TBI.
ment of the 3rd ventricle, cavum septum pellucidum and
mammillary body
atrophy.10,18,19 Four progressive stages
of pathological severity were described in 2013,
10 but these
Materials and methods
were not validated in the 2016 consensus
study18 or the
most recent 2021 consensus study
19 and as such they are
Case recruitment
not a feature of the current diagnostic guidelines. Instead, a
Cases were recruited through prospective brain donor pro-
pathology severity grade has been proposed that charac-
grammes with a focus on ageing and neurodegeneration. As
terizes a case as ‘low’ or ‘high’ CTE-NC based on the distri-
such, they are representative of patients with neurodegenera-
bution of neuronal tau throughout cortical and subcortical
tive conditions and healthy controls in our local region of
regions.
19
NSW, Australia. The Sydney Brain Bank has ethical approval
It is not clear how much CTE-NC is required to manifest
from the University of New South Wales, Australia, to collect,
clinical disease, and both cardinal and supportive pathologic-
characterize, store and distribute human brain tissue for the
al features of CTE-NC (neuronal tau and TDP-43-positive
purpose of medical research. The broad case types can be
inclusions and neurites) are widely seen in other
seen
in Table 1. All cases were screened based on current pub-
neurodegenerative conditions and the normal aged brain.
lished neuropathological diagnostic criteria
31–
44 and using a
Multiple studies have shown that not all cases with a history
standardized panel of histologically and immunohistochemi-
of repetitive mild neurotrauma in sports display CTE-NC.
cally stained neuroanatomical regions. The routine screening
Using the first consensus diagnostic recommendations,
18
comprises sections sampled from (i) superior frontal,
CTE-NC was reported in 66–87% of former professional
American football
players,20 Scottish soccer and Rugby
players
21 and English professional soccer players.
22 Other
Table 1 Primary neuropathological diagnosis (n = 636)
studies of former professional athletes have shown lower per-
and presence of CTE-NC
centages of CTE-NC (48–50%) in professional Canadian
Sample
%
Mean CTE-NC
football and ice hockey players.
23,24 However, all of the
Case type
size
Males
age
(%)
above studies of former athletes are not population-based,
Alzheimer’s disease
176
52.3 77 ± 14
1.1
with potential bias in those coming to post-mortem brain
neuropathologic change—
examination. Indeed, studies analysing brain bank cohorts
intermediate and high
have reported much lower levels of CTE-NC (12–31.8%)
Lewy body disease (dominant
111
68.5 80 ± 7
0
in individuals with a history of participation in contact
movement disorder)
sports.25,26 CTE-NC has also been found in a routine neuro-
Lewy body disease (dominant
35
74.3 80 ± 9
2.9
dementia)
pathology service in Canada in individuals with a history of
Multiple system atrophy
22
54.5 70 ± 8
0
head injury with or without substance abuse
27 and a brain
Frontotemporal lobar
52
51.9 69 ± 9
0
bank population in the UK in individuals without a known
degeneration with TDP-43
history of head injury and no neurological
symptoms.28
Motor neuron disease
55
63.6 64 ± 12
0
There have been few large-scale investigations of CTE-NC
Progressive supranuclear palsy
55
58.2 77 ± 7
0
Corticobasal degeneration
16
62.5 71 ± 11
0
and most studies in neurodegenerative brain bank cohorts
Pick’s disease
8
62.5 74 ± 5
0
were performed before the development of the first consen-
Globular glial tauopathy
12
58.3 73 ± 11
0
sus criteria.
18 These studies have reported varying percen-
Rare diseases, including
27
59.3 81 ± 16
0
tages of CTE-NC. A large-scale study of 450 decedents
frontotemporal dementia
who did not participate in youth sports found 3% of cases
with FUS, neuronal
intranuclear inclusion disease
had CTE-NC,
25 while another found a higher rate of
Huntington’s disease
15
73.3 62 ± 17
0
11.9% in 268 cases.
28 In a large community-based sample
Cerebrovascular disease
29
55.2 88 ± 10
0
of 532 cases, only three cases (0.6%) had CTE-NC and
Healthy aged controls
21
42.9 86 ± 9
0
none of these cases had a known history of head injury
Chronic traumatic
2
100
79 ± 2
100
with loss of consciousness or participation in contact
encephalopathy
neuropathologic change
sports.29 Another community-based study found no
link to page 15 link to page 15 link to page 26 link to page 27 link to page 26 link to page 27 link to page 26 link to page 27 link to page 27 link to page 27
4 | BRAIN COMMUNICATIONS
GOV-045703
2022: Page 4 of 17
H. McCann
et al.
pre-central, inferior temporal and anterior cingulate gyri; (ii)
Disorders and Stroke/National Institute of Biomedical
hippocampus,
entorhinal gyrus and amygdala; (iii) midbrain,
Imaging and Bioengineering (NINDS/NIBIB) consensus cri-
pons and medulla and (iv) caudate, putamen and cerebellar
teria,
18,19 tissue blocks were retrospectively sampled from
dentate. These regions were stained with haematoxylin and eo-
the middle frontal gyrus, superior and middle temporal gyrus
sin, modified Bielschowsky silver and antibodies to detect
and inferior parietal gyrus and included as many sulcal
phospho-tau, ß-amyloid, p62, α-synuclein and TDP-43 pro-
depths as possible. A subset of 90 cases were sampled bilat-
teins. Additional sampling and staining were performed where
erally, where both formalin-fixed brain hemispheres were
indicated by clinical presentation or gross observations of ab-
available, to ascertain whether there was significant patho-
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
normalities during macroscopic examination. Where a case
logical asymmetry. These included cases representative of
had evidence of more than one neuropathology meeting criteria
the neurodegenerative cohort, including sporadic and famil-
for neurodegenerative disease, the dominant neuropathology
ial intermediate and high Alzheimer’s disease neuropatholo-
was listed as the primary diagnosis (
Table 1). More than one
gic change, sporadic and familial Lewy body disease,
type of pathology, and diagnosis, was common.
cerebrovascular disease and genetic frontotemporal lobar
Two cases had already been identified as having CTE-NC
degeneration with TDP-43. Paraffin-embedded sections
as the primary diagnosis during our routine neuropathologic-
were cut on a rotary microtome at 10 µm thickness and
al screen. A total of 636 cases were screened. The majority of
stained with a primary antibody to detect phospho-PHF
cases were sporadic in origin (
n = 507), although some had
tau (AT8, 1:1500, cat #MN1020, Thermo Scientific,
either a known genetic mutation or a familial history consist-
Rockford, IL, USA) using a BenchMark GX autostainer
ent with a dominantly inherited disorder (
n = 129,
see Table 1
and an Optiview Detection kit (cat# 760-700 Roche
for case types, numbers, gender and age distributions).
Diagnostics).
Clinical diagnosis of neurodegenerative disease and injury
Cases that were identified as having CTE-NC then had a
were collected prospectively from recruitment via clinical
full set of regions stained according to the 2016 and 2021
notes or questionnaires completed by the participant, their
NINDS/NIBIB consensus criteria.
18,19 Where possible, bilat-
next-of-kin or their clinician. Any history of TBI was collected
eral regions were examined from the cortex, hippocampus,
retrospectively at the time of recruitment via specific ques-
amygdala, basal ganglia, thalamus, midbrain with substantia
tions, including whether there had ever been a head injury,
nigra, pons with locus coeruleus, medulla oblongata, cere-
the year the head injury was sustained and further details of
bellar cortex, cerebellar dentate nucleus, hypothalamus
head injury. Additional information regarding sporting car-
and mammillary body. Pathology staging was performed
eer or military service was obtained retrospectively from pub-
based on both 2013 criteria (staging from one to four)
10
licly available obituaries. As a rule, we did not know whether,
and the 2021 (low or high)
19 NINDS/NIBIB consensus
or the extent to which, cases participated in contact, collision
criteria.
or combat sports during adolescence or early adulthood;
therefore, these cases are underestimated. However, a small
Microscopic analysis
number of people had a documented history of participation
in combat (e.g. boxing) or collision (e.g. rugby) sports. These
Using a Zeiss Axioscope A1 brightfield microscope, three in-
individuals had participated in either organized senior club le-
vestigators (one clinical neuropathologist and two research
vel or professional sport. In total, 109 cases were identified as
neuropathologists with over 50 years of collective experience
having a previous TBI (17.1% of the cohort) and of these 17
in neurodegenerative pathologies) assessed the presence of
(15.6%) had documented TBI-related loss of consciousness.
tau-immunopositive neurons and astrocytes and noted their
Seven of the 109 TBI cases (6.4%) also had a documented his-
distribution within each tissue section, specifically whether
tory of contact sport participation. We did not systematically
they were situated in the sulcal depth in a perivascular ar-
collect (or have access to) information relating to the severity
rangement—described as ‘around small vessels’ in the cur-
of TBI, whether it was associated with structural findings on
rent NINDS/NIBIB consensus diagnostic criteria.
19
neuroimaging, the functional deficits associated with the in-
According to the current 2021 consensus criteria, the min-
jury or the extent to which the person recovered, clinically,
imum threshold for the neuropathological diagnosis of
from the injury. Information on number of TBIs and duration
CTE-NC is the presence of a single pathognomonic lesion
of loss of consciousness was also not systematically collected,
in the cortex, and that lesion consists of phosphorylated
therefore, cases were broadly dichotomized as having a his-
tau aggregates in neurons, with or without glial tau in thorn-
tory of TBI or not.
shaped astrocytes, at the depth of a cortical sulcus around a
small blood vessel. The presence of thorn-shaped or granu-
lar/fuzzy astrocytes indicating ageing-related tau astroglio-
Tissue sampling and
pathy
(ARTAG)40
was assessed in these regions
immunohistochemistry for analysis of
morphologically (not through co-labelling with an astrocytic
CTE-NC
marker) and the distribution noted, specifically whether it
was situated in subpial, subependymal, white matter or cor-
In order to detect the pathognomonic cortical lesions accord-
tical regions and whether the arrangement was perivascular.
ing to the 2016 and 2021 National Institute on Neurological
Investigators showed 93.3% agreement when identifying
link to page 27 link to page 27 link to page 15 link to page 18 link to page 18 link to page 15 link to page 26 link to page 18 link to page 27 link to page 18 link to page 27 link to page 27 link to page 19 link to page 20 link to page 26 link to page 20
CTE in the Sydney
GOV-045703 Brain Bank
BRAIN COMMUNICATIONS 2022: Page 5 of 17 | 5
CTE-NC, pathology almost meeting criteria for CTE-NC
hippocampus required to stage according to the 2021 con-
and ARTAG
(Cohen’s kappa = 0.865, indicating almost per-
sensus criteria.
19
fect agreement).
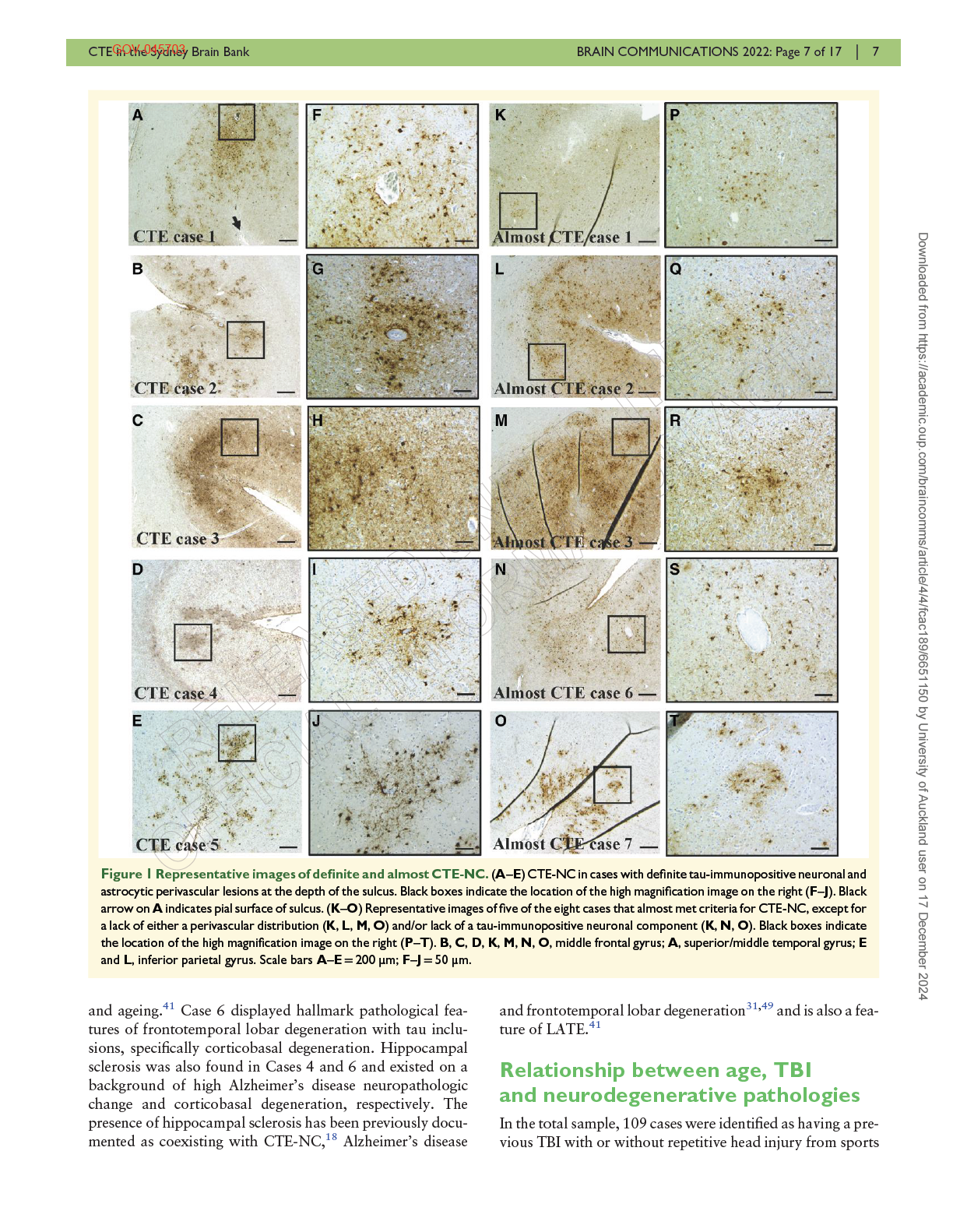
The severity of CTE-NC ranged from one focal lesion
(Case 2), to isolated focal lesions in two separate sampled re-
Statistical analysis
gions (Case 1), to multiple foci in all three sampled cortical
regions (Cases 3–5). CTE-NC was found in the middle front-
A multivariate ordinal regression model with multivariate lo-
al and superior/middle temporal gyri in four of the five cases,
git link, as implemented in the mvord R
package,45 was used
with lesions in the inferior parietal gyrus found in three cases.
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
to assess the effect of TBI, age (mean centred average), gen-
Of the two cases with bilateral samples, one had bilateral le-
der and post-mortem delay on pathological features of com-
sions in the middle frontal gyrus and left-sided lesions in the
mon neurodegenerative diseases: amyloid plaques (A Score
superior/middle temporal and inferior parietal gyri (Case 4).
0–3), neurofibrillary tangles (B Score 0–3), Lewy pathology
The other had left-sided lesions only in the middle frontal
(LB Stage 0–6), the presence of cortical ARTAG (yes/no)
and superior/middle temporal gyri (Case 1). The perivascular
and limbic-predominant age-related TDP-43 encephalop-
sulcal depth lesions were noted to consist of predominantly
athy (LATE) (yes/no). The presence or absence of CTE-NC
astrocytic tau and very sparse neuronal tau, a feature that
(either as a primary,
n = 2 or secondary diagnosis,
n = 3)
has recently been noted by others
46 (Fig. 1).
was not included in the analysis because the number of cases
was too low.
Clinical characteristics of cases with
Data availability
CTE-NC
The clinical profiles of these cases can be seen in
Table 3.
The data that support the findings of this study are available
Four of the five cases were males, with the ages of all cases
from the corresponding author upon reasonable request.
ranging from 74 to 92. In three cases the disease duration
was relatively rapid at <5 years, while two other cases had
Results
longer disease durations of 8 and 15 years. The age of symp-
tom onset ranged from 63 to 90 years of age. Most cases (ex-
Prevalence of CTE-NC
cept Case 4) had a clinical diagnosis consistent with a
dominant dementia phenotype, with or without a movement
Of the 636 cases screened, five showed tau-immunopositive
disorder component. None of the cases had cognitive impair-
neuronal and astrocytic pathology located in a strictly peri-
ment or movement disorders in other family members sug-
vascular arrangement in the sulcal depths, definitively meet-
gestive of familial disease or had known gene mutations
ing current criteria for CTE-NC.
19 This included two cases
for neurodegenerative disease.
that had already been identified during routine screening,
According to the current National Institute of
giving an overall frequency of 0.79% of cases with
Neurological Disorders and Stroke Consensus Diagnostic
CTE-NC in our brain bank cohort (
Table 1). Of the five cases
Criteria for traumatic encephalopathy
syndrome,16 only
identified, two had a primary diagnosis of Alzheimer’s dis-
Case 3 in retrospect would have met criteria for traumatic
ease neuropathological change and one case had limbic
encephalopathy syndrome (see
Table 3). These criteria are
Lewy body disease
(Table 2). All cases had TDP-43 path-
listed below.
ology in the medial temporal lobe consistent with LATE.
1. A history of substantial exposure to repetitive head
The two cases with a primary diagnosis of CTE-NC also
impacts, either through high contact or collision
had hippocampal sclerosis and one case had a small subcor-
sports with a minimum 5-year history, or other
tical infarct. Varying severity of ß-amyloid pathology was
non-sport-related risks for which risk thresholds have
found in all cases, including those where the primary diagno-
not yet been established. There were three cases that
sis was CTE-NC (Cases 3 and
4, Table 2). No cases meeting
met this criterion (Cases 3–5). One played Australian
strict neuropathological criteria for CTE-NC were found in
rugby league at the club level for 20 years and two
any other disease group (
Table 1).
others had a boxing history.
The staging of CTE-NC varied from Stage 1 to 4 using the
2. Presence of cognitive impairment, including deficits in
2013 staging
criteria10 (Table 2). Only Cases 2, 3 and 4 could
episodic memory and/or executive dysfunction and/or
be reliably staged according to the 2021 consensus criteria,
19
neurobehavioural features significantly different from
as they did not have a coexisting tauopathy
(Table 2). While
baseline. There were four cases that met this criterion
we attempted to apply the 2021 staging to the remaining two
(Cases 1, 2, 3 and 5), although in three cases (Cases 1, 2
cases, they were all identified as having high CTE-NC due to
and 5) cognitive impairment can be explained by neuro-
the presence of neuronal tau throughout all cortical layers,
pathologically confirmed Alzheimer’s disease or Lewy
all sectors of the hippocampal formation, and subcortically
body disease (see Point 4 below).
in the amygdala, mammillary bodies and thalamus. Thus,
3. A progressive worsening of symptoms over the course of
we were unable to distinguish the neuronal tau restricted
at least 1 year in the absence of continued exposure to TBI
to the upper cortical layers and CA2/CA4 sectors of the
or mild repetitive neurotrauma. There were three cases
link to page 26 link to page 19 link to page 27 link to page 22 link to page 27 link to page 27 link to page 27
6 | BRAIN COMMUNICATIONS
GOV-045703
2022: Page 6 of 17
H. McCann
et al.
that appeared to meet this criterion (Cases 3–5), although
one had a comorbid diagnosis of Alzheimer’s disease
(Case 5).
sclerosis
sclerosis
AD-NC
4. Symptoms must not be fully accounted for by other disor-
LBD
traumatic
ders, although a comorbid diagnosis of another neurode-
diagnosis
LBD
infarct
AD-NC
generative disease, neurobehavioural or substance abuse
chronic
Neuropathological
disorder can be present and does not exclude a traumatic
High
Limbic
LATE
CTE-NC
Neocortical
LATE
CTE-NC
CTE-NC
Striatal
Hippocampal
LATE
CTE-NC
Hippocampal
LATE
Intermediate
LATE
CTE-NC
encephalopathy syndrome diagnosis.
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
of
5. Supportive features include a delayed onset of several
staged
staged
CTE-NC,
of
years after repetitive head injury ends; motor symptoms
2021
such as Parkinsonism, dysarthria and ataxia; and psychi-
reliably
pathologies
reliably
pathologies
C0–C3;
atric features such as anxiety, apathy, depression and
staging
be
the presence
be
presence
paranoia. Delayed symptom onset was only applicable
not
to
not
to
(6)
(8)
(10)
CTE
to the three cases with a history of participation in combat
due
coexisting
due
coexisting
Could
High
High
High
Could
and collision sports (Cases 3–5). Parkinsonism was re-
CERAD score,
ported in Case 3, cerebellar signs in Case 4 and mood dis-
score,
order in Case 5.
3
1
4
3
4
CTE
2013
staging
C
injury.
The above criteria are intended to be used in a research set-
ting to facilitate investigations into the clinical features asso-
brain
fit
B0–B3;
ciated with CTE-NC. Provisional levels of certainty of
not
CTE-NC are graded as suggestive, possible, probable and
cortex
2
3
3
2
definite.
16
criteria
traumatic
TDP-43
pathology
stage
Stage
Stage
Stage
distribution,
TBI,
entorhinal
only—does
staging
Cases almost meeting criteria for
LATE
In
LATE
LATE
LATE
tangle
disease;
CTE-NC
V
VI
0
0
0
body
In addition to the five cases meeting strict consensus criteria
Lewy
body
stage
for CTE-NC, there were eight cases that almost met criteria
neurofibrillary
Lewy
as they displayed astrocytic tau pathology that concen-
trated in an irregular pattern in the sulcal depth.
score,
score
C2
C1
C1
C0
C2
B
However, these cases either lacked clear evidence of
C
(neuritic
plaques)
tau-immunopositive neurons or the pathology was not
A0–A3;
strictly perivascular (
Fig. 1). These cases, therefore, met
the criteria for
ARTAG.40 All eight cases met criteria for ei-
encephalopathy; LBD,
ther intermediate or high Alzheimer’s disease neuropatho-
score
B3
B1
B3
B3
B2
logic change and four also met criteria for Lewy body
distribution,
B
tangles)
TDP-43
disease, brainstem predominant Stage IV to neocortical
(neurofibrillary
plaque
Stage VI. These cases were predominantly male (seven
males and one female) and their ages ranged from 69 to
age-related
86 years old. Although two had disease durations shorter
β-amyloid
than 5 years, the other five cases had longer disease dura-
A3
A2
A1
A1
A3
tions ranging from 8 to 20 years
(Table 4). The age of
A score
-amyloid
plaques)
score,
(β
A
symptom onset ranged from 55 to 76 years, which was
somewhat younger than the definite CTE-NC cases.
limbic-predominant
change;
All cases displayed a dementia dominant phenotype. None
4
8
2
2
of the cases had cognitive impairment or movement disorder
CTE-NC
15
LATE,
Disease
in other family members suggestive of familial disease or any
duration
(years)
known gene mutations for neurodegenerative disease, in-
with
change;
cluding Case 4, which had a disease onset at 55 years old.
neuropathologic
Three cases had a positive history of single TBI (Cases 6–8)
cases
Gender
Female
Male
Male
Male
Male
and one of these also had a professional sport background
of
at
disease
as a soccer player for more than 5 years (Case 6). One case
89
74
78
81
92
Age
death
neuropathologic
had been a boxer in his youth for an unknown time period
Details
(Case 5).
2
Alzheimer’s
1
2
3
4
5
LATE was found in all cases and is commonly seen in as-
sociation with Alzheimer’s disease neuropathologic
Case
number
Case
Case
Case
Case
Case
AD-NC,
encephalopathy
change,
31 Lewy body pathology,
47 small vessel disease
48
Table
link to page 27 link to page 26 link to page 27 link to page 27 link to page 27
link to page 20
8 | BRAIN COMMUNICATIONS
GOV-045703
2022: Page 8 of 17
H. McCann
et al.
of
Lewy
and
or
Clinical
disease
(per
real
by
by
not
known
injury.
known
injury.
duration
no
boxing
TES.
criteria
TES
subcortical
no
body
no
cognitive
of
intermediate
head
confirmed
head
confirmed
for
sclerosis,
with
for
features
Short
by
change
explained
explained
had a
(TES)
criteria,
and Lewy
criteria,
criteria,
criteria
case
Duration
criteria
disease
repetitive
repetitive
disorder
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
clinically.
meet
of
features
meet
of
features
explained
, this
hippocampal
meet
meet
traumatic encephalopathy
unknown.
disease
3
syndrome
not
not
general
not
not
history
Clinical
neuropathologically
Alzheimer’s
history
Clinical
neuropathologically
body
Table
infarct,
LATE)
neurobehavioural
detected
movement
progression.
career
features
Alzheimer’s
neuropathological
Meets
Does
Does
Meets
Does
Does
of
age
head
score
11
85;
no
age
of
of
delay
tremor
mood
(years)
applicable
or
applicable
since
injury;
age
Yahr
cognitive
features
was
onset
delay
years;
depression
delay
not
not
symptoms
history of
and
5-year
2
90
onset
repetitive
motor
head
a
cerebellar
and depression
-motor
there
no
rigid
years
years
age
no
Parkinsonism
upper limb
treated for
-psychiatric
onset
onset
depression
mild
medication
Hoehn
least
80
3
medicated
at
many
many
Supportive
-delayed
because
history of
injury;
psychiatric
because
repetitive
Akinetic
Parkinsonism
73,
of
onset;
years;
54,
onset;
with
component
self-reported
age
onset;
disorder
with
and behavioural
therapy
Delayed
Delayed
Yes,
Yes,
Yes,
11
to
2
26
years
years
over
4
8
decline
years,
over
15
MMSE
from
Disease
over
over
cognitive
progression
obvious
over
movement
disorder
years
progression
decline
years;
down
25
Yes,
Yes,
Cognitive
No
Slight
of
and/
age
age
age
this
Clinical
at
rating
problems
clinical
and
87.
1
on
of
90.
dementia
predated
short-term
from
change;
impairment,
age
dementia
memory
found
impairment
impairment
and hallucinations
instability
features
loss
rating
2
impairment from
impairment from
Clinical
of
inappropriate
not
disorder
neurobehavioural
increased
behaviour
71.
Clinical
79
or
cognitive
cognitive
85,
memory
dementia
66,
confusion
age
rating
anger,
behaviours diagnosed
63.
3
age
testing
diagnosed at
Emotional
mood
diagnosis
syndrome.
Cognitive
Memory
Memory
Mild
Self-reported
Mild
5
to
and
have
have
years.
for
TBI
sport
rugby
to
to
20
known
of
unknown.
of
club
for
consciousness
boxer,
consciousness
boxer
Not
known
of
known
of
loss
traumatic encephalopathy
contact
participation
isolated TBI and
isolated TBI and
isolated TBI and
History
former
player
Not
loss
former
duration
Not
loss
former
years.
have
consciousness
TES,
No
No
Yes,
Yes,
Yes,
injury;
CTE-NC
with
with
with
bodies
bodies/
with
limb
cerebellar
Clinical
diagnosis
Lewy
Lewy
Alzheimer’s
disease
disease/
Parkinsonism
tremor
mild
component
disease
traumatic brain
Dementia
Dementia
Alzheimer’s
Upper
Alzheimer’s
cases
TBI,
of
4
8
2
2
15
Disease
duration
(years)
details
examination;
at
89
74
78
81
92
state
Age
death
Clinical
3
1
2
3
4
5
mini-mental
Female
Male
Male
Male
Male
Case
number
Case
Case
Case
Case
Case
Table
MMSE,
link to page 22 link to page 23 link to page 23 link to page 23 link to page 24 link to page 24 link to page 23 link to page 27 link to page 27 link to page 19 link to page 27 link to page 27 link to page 28
CTE in the Sydney
GOV-045703 Brain Bank BRAIN COMMUNICATIONS 2022: Page 9 of 17 | 9
(17.1% of the cohort), and three (2.8% of the 109) were
frequency of CTE-NC (0.6%) in 532 individuals from a simi-
identified
as having CTE-NC. All three of these cases were
lar community-based cohort of ageing and neurodegenera-
also high exposure former athletes; CTE-NC was not identi-
tion in the USA
29 and a large-scale study reporting no
fied in any cases with a single TBI alone. Of the eight cases
CTE-NC in 310 cases from Europe.
30 There was not a single
that almost met criteria for CTE-NC, four had an isolated
case of CTE-NC in individuals with a documented history of
TBI and two of these also had a history of contact sport par-
a TBI alone; rather, three of the cases had TBI in addition to
ticipation (
Table 4).
high exposure to repetitive head impacts in collision and
We used a multivariate ordinal regression model to deter-
combat sports and two cases had no known history of neuro-
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
mine how age (mean centred), gender, post-mortem delay
trauma (TBI or repetitive head impacts in sports). All five
and TBI are associated with the presence and severity of in-
cases had coexisting pathology, and three cases had neurode-
dividual pathologies, specifically ß-amyloid (A Score 0–3),
generative diseases diagnosed clinically and neuropathologi-
neurofibrillary tangles (B Score 0-3), Lewy body pathology
cally (Alzheimer’s disease and Lewy body dementia). There
(Lewy body Stages 0–6), cortical ARTAG (presence or ab-
were eight cases (1.3% of the brain bank cohort) that almost
sence) and LATE (presence or absence). All cases with a
met criteria for CTE-NC because they displayed astrocytic
strong family history of disease or a known genetic mutation
tau pathology that concentrated in an irregular pattern in
were removed from this analysis because these are known
the sulcal depth and in some cases could be considered to
drivers of disease and could confound our analysis. This
be ‘around small vessels’, but these cases either lacked clear
left a total of 507 cases for analysis
(Table 5).
evidence of tau-immunopositive neurons or they were not
Post-mortem delay was not a significant predictor of
seen in a more strict and definitive perivascular arrangement
ß-amyloid pathology (A Score
P = 0.77), neurofibrillary tan-
(
Fig. 1). Of these eight ‘CTE-like’ cases, 100% had ARTAG,
gles (B Score
P = 0.1), Lewy pathology stage (
P = 0.19) or
LATE and Alzheimer’s disease neuropathologic change
cortical ARTAG (
P = 0.77). However, a greater post-
(intermediate or high). The results of our study and others
mortem delay was associated with a lower likelihood of hav-
suggest that CTE-NC is rare in the general population.
ing LATE (
P = 0.03), which may the reflect loss of TDP-43
antigenicity post-mortem. Gender was not a significant pre-
dictor of ß-amyloid pathology (A Score
P = 0.28), neurofib-
Observations on the CTE-NC lesion
rillary tangles (B Score
P = 0.91), Lewy pathology stage
and applying the CTE-NC consensus
(
P = 0.15) or LATE (
P = 0.75). However, as expected, males
criteria
were more likely to have cortical ARTAG than females, with
24% of males having ARTAG compared with only 10% of
Thorn-shaped astrocytes consistent with ARTAG were ob-
females (
P = 0.00003, see
Table 6 for relative risks).
served in 100% of our cases with CTE-NC. However, cur-
As expected, age was a significant predictor of most path-
rent NINDS/NIBIB CTE consensus criteria
19 consider
ologies, showing that for every unit increase in this variable
subpial and subcortical astrocytic tau to be part of
the odds of having a higher ß-amyloid stage (A score) in-
CTE-NC, despite being indistinguishable from ARTAG.
creased by 4.3% (
P ≤ 0.0000001), neurofibrillary tangle
Indeed, both are composed of 4R tau and share identical
stage (B score) increased by 3.4% (
P = 0.00002), and the
morphology.
50–52 Increased astrogliosis and degeneration
odds of having cortical ARTAG and LATE increased by
of astrocytes (beaded and broken processes) have been iden-
3.3% (
P = 0.001) and 9.4% (
P < 0.0000001), respectively.
tified in association with CTE-NC, particularly in the white
Age was not a significant predictor of Lewy body pathology
matter, which reportedly do not correlate to the amount of
in this older adult group (
P = 0.1, see
Table 6 for relative
astrocytic tau,
53 suggesting that another mechanism of astro-
risks).
cytic dysfunction might be operative. Furthermore, single
TBI was not significantly associated with increased
nucleus RNA-seq has shown that white matter astrocytes
ß-amyloid stage (
P = 0.06), Lewy pathology stage (
P = 0.7)
in CTE-NC have transcript profiles consistent with neuroin-
or cortical ARTAG (
P = 0.06). However, the odds of having
flammation and dysfunctional metabolism, suggesting white
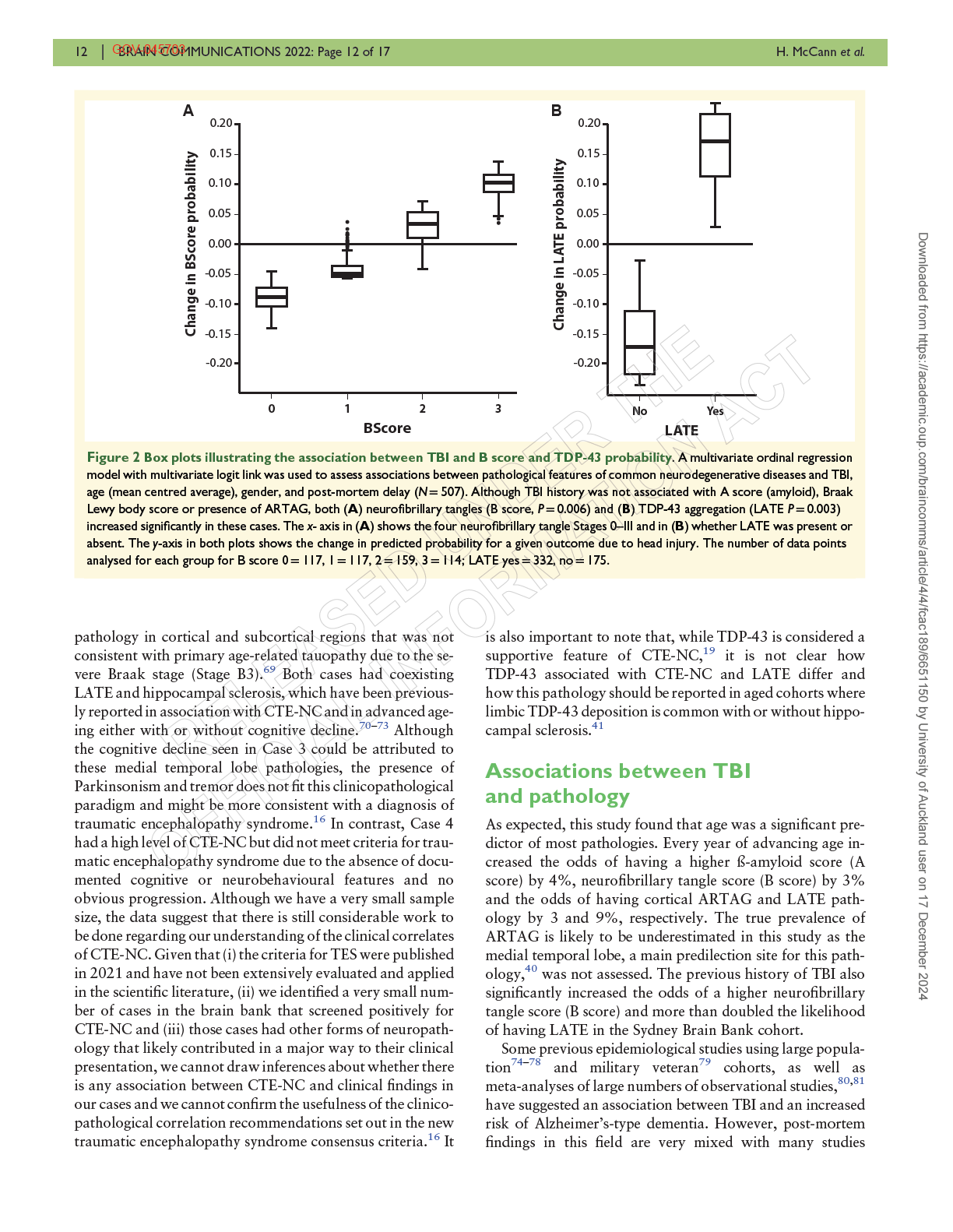
a higher neurofibrillary tangle (B) score increased by 79% in
matter pathology may be an important differentiating fea-
the TBI group (
P =
0.006, Fig. 2A), and TBI was associated
ture between ARTAG and
CTE-NC.54 Interestingly, it was
with a 148% increased likelihood of having LATE (
P =
noted in the two cases with a primary pathological diagnosis
0.003,
Fig. 2B and Table 6).
of CTE-NC (Cases 3 and 4) that white matter thorn-shaped
astrocytes were widespread, being present in every region ex-
amined with the exception of the cerebellum. This frequency
Discussion
of pathology was not observed in any of the other cases ex-
amined. The presence of astrocytic tau in all cases of
This is one of the largest studies examining the neuropathol-
CTE-NC and also those cases almost meeting criteria indi-
ogy of CTE published to date. In the Sydney Brain Bank, of
cates it is likely to co-occur with the pathognomonic
the 636 cases screened, only five were identified as having
CTE-NC lesion, regardless of whether it is considered a sup-
CTE-NC, illustrating a strikingly low prevalence (0.79%).
portive or separate feature. Future studies should prioritize
This is consistent with a recent study reporting a low
our understanding of the differences and similarities between
link to page 27 link to page 26 link to page 26 link to page 26 link to page 27 link to page 28 link to page 26 link to page 27 link to page 27 link to page 27 link to page 28 link to page 28 link to page 27 link to page 27 link to page 28 link to page 26 link to page 27 link to page 28 link to page 28
10 | BRAIN COMMUNICATIONS
GOV-045703
2022: Page 10 of 17 H. McCann
et al.
Table 4 Cases almost meeting criteria for CTE-NC with coexisting pathologies
History of TBI and contact
Disease
Case number
Age at death
sport participation
Gender
duration (years)
Main neuropathologies
Case 1
79
No
Male
7
High AD-NC
Moderate small vessel disease
ARTAG
LATE
Case 2
69
No
Male
5
High AD-NC
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
ARTAG
LATE
Case 3
72
No
Male
4
High AD-NC
Brainstem predominant LBD
ARTAG
LATE
Case 4
75
No
Female
20
High AD-NC
Moderate small vessel disease
Hippocampal sclerosis
ARTAG
LATE
Case 5
80
Yes, isolated TBI and previous boxer
Male
11
High AD-NC
(unknown duration)
Limbic LBD
ARTAG
LATE
Case 6
72
Yes, isolated TBI and professional soccer Male
10
Corticobasal degeneration
for 5 years
Intermediate AD-NC
Hippocampal sclerosis
ARTAG
LATE
Case 7
76
Yes, isolated TBI
Male
8
Neocortical LBD
Intermediate AD-NC
ARTAG
LATE
Case 8
86
Yes, isolated TBI
Male
10
High AD-NC
Limbic LBD
ARTAG
LATE
AD-NC, Alzheimer’s disease neuropathologic change; ARTAG, ageing-related tau astrogliopathy; LATE, limbic-predominant age-related TDP-43 encephalopathy; LBD, Lewy body
disease; TBI, traumatic brain injury.
astrocytic tau in ARTAG and CTE-NC to better understand
identified as having
CTE-NC,20 and despite the proposed
the relationship between these pathologies. Determining the
differential distribution of neuronal tau in both
relative significance of astrocytic versus neuronal tau in the
Alzheimer’s disease and CTE-NC, the 2021 NINDS/NIBIB
CTE-NC lesion would also be of importance, particularly
CTE consensus
criteria19 does not address cases with coex-
as we and
others46 have reported the dominance of perivas-
isting neurofibrillary tangle pathology equal to or greater
cular sulcal depth astrocytic tau.
than Braak Stage IV, where tangles appear in the neocor-
Our experience of applying the NINDS/NIBIB consensus
tex.58 This level of Alzheimer’s disease neuropathologic
criteria and assessing various anatomical regions for patho-
change is seen not only in Alzheimer’s disease but also in
logical change supports the concept of predilection sites for
cases of normal ageing, making any attempt at staging diffi-
CTE-NC, such as the middle frontal
gyrus,10 but also super-
cult in aged cohorts. Previous immunohistochemical and
ior/middle temporal gyri and inferior parietal gyri. However,
biochemical studies have shown that neuronal tau in both
staging CTE-NC proved more problematic. Indeed, the 2013
CTE-NC and Alzheimer’s disease neurons consists of 3R
staging
criteria10 have already been shown not to be consist-
and 4R tau that undergo common post-translational modifi-
ent when used in a consensus situation in
201618 or 2021,
19
cation.
10,52,59–62 Transcriptome analysis has also shown
despite reported associations with age at death, presence of
similar changes in protein phosphatase expression in
dementia and years of American football
play55 in a research
CTE-NC and Alzheimer’s
disease.63 However, a proteomic
setting. Furthermore, the 2016 and 2021 consensus criteria
study has found that Alzheimer’s disease and CTE-NC share
acknowledge that disease staging on the background of a co-
<25% homology between their insoluble proteomes, with
existing neurodegenerative disease,
18,19 which is common in
many of the proteins identified specifically in CTE-NC also
older individuals with
CTE-NC,20,21,56,57 requires further
being increasingly expressed as disease stage progresses.
64
investigation. Indeed, Alzheimer’s disease is one of the
Electron cryo-microscopy has been used to reconstruct the
most frequently seen neurodegenerative diseases in cases
tau filaments in both CTE-NC and Alzheimer’s disease and
link to page 28 link to page 27 link to page 27 link to page 27 link to page 27 link to page 27 link to page 27 link to page 28 link to page 28 link to page 28 link to page 28 link to page 27 link to page 27
CTE in the Sydney
GOV-045703 Brain Bank BRAIN COMMUNICATIONS 2022: Page 11 of 17 | 11
Table 5 Sporadic case types classified according to their
Table 6 Odds ratios with 95% confident intervals for
primary
neuropathological diagnosis used for
gender, post-mortem delay, age and TBI on individual
regression analyses
pathologies using multinomial regression
Number
%
Mean
Pathology
OR (95% CI)
P-value
Case type
of cases
males
age
A score (amyloid)
Alzheimer’s disease neuropathologic
129
57.6
80 ± 12
Gender
1.21 (0.85–1.71)
0.28
change—intermediate and high
Post-mortem delay
0.99 (0.99–1.01)
0.77
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
Lewy body disease (dominant
99
67.4
80 ± 7
Age
1.04 (1.03–1.06)
0.
0000001
movement disorder)
TBI
1.49 (0.98–2.29)
0.06
Lewy body disease (dominant
34
78.1
81 ± 9
B score (tau)
dementia)
Gender
1.02 (0.72–1.44)
0.91
Multiple system atrophy
21
52.4
70 ± 8
Post-mortem delay
0.99 (0.99–1)
0.1
Frontotemporal lobar degeneration
24
60.0
71 ± 9
Age
1.03 (1.01–1.05)
0.
00002
with TDP-43
TBI
1.79 (1.18–2.72)
0.
006
Motor neuron disease
41
64.6
67 ± 11
Braak Lewy body score
Progressive supranuclear palsy
53
56.6
77 ± 7
Gender
0.76 (0.52–1.10)
0.15
Corticobasal degeneration
13
53.8
73 ± 11
Post-mortem delay
0.99 (0.98–1)
0.19
Pick’s disease
8
62.5
74 ± 5
Age
1.01 (0.99–1.03)
0.11
Globular glial tauopathy
10
60.0
76 ± 10
TBI
1.09 (0.69–1.71)
0.7
Rare diseases, including
23
50.0
83 ± 15
ARTAG
frontotemporal dementia with
Gender
0.29 (0.16–0.52)
0.
00003
FUS, neuronal intranuclear
Post-mortem delay
0.99 (0.98–1.01)
0.77
inclusion disease
Age
1.03 (1.01–1.05)
0.
001
Cerebrovascular disease
29
55.2
88 ± 10
TBI
1.73 (0.97–3.07)
0.06
Healthy aged controls
21
42.9
86 ± 9
LATE
Chronic traumatic encephalopathy
2
100.0
79 ± 2
Gender
1.07 (0.67–1.71)
0.75
neuropathologic change
Post-mortem delay
0.98 (0.98–0.99)
0.03
Age
1.09 (1.07–1.12)
<0.
00000001
TBI
2.48 (1.35–4.54)
0.
003
The change in relative risk represents a unit change in each independent variable. Bold
has found a hydrophobic cavity exclusively in CTE-NC cases
values indicate statistical significance. ARTAG, ageing-related tau astrogliopathy; LATE,
which does not associate with tau, suggesting possible differ-
limbic-predominant age-related; OR, odds ratios; TDP-43, TAR DNA binding protein
43; TBI, traumatic brain injury.
ent mechanisms of tau aggregation.
65 These studies provide
the necessary groundwork to identify possible key differ-
ences between neuronal tau in Alzheimer’s disease, primary
age-related tauopathy and CTE-NC that may be used in a
Clinicopathological correlation and
neuropathological setting to decipher the true extent of
CTE-NC on the background of ageing and neurodegenera-
applying the new consensus criteria
tive tauopathies.
for traumatic encephalopathy
In this study, we identified a subset of cases that almost
syndrome
met criteria for CTE-NC except for no clear evidence of
neuronal tau and/or a definitive perivascular arrangement
In other brain bank cohorts, CTE-NC has been previously
of the lesion. These cases were mostly male and half had a
reported in individuals with Parkinson’s disease, progressive
known history of TBI with or without or participation in
supranuclear palsy and multiple system
atrophy,28,57 where
sports associated with repetitive head injury. Others have
frequent falls are a common
feature.66,67 However, we did
previously noted similar cases with ‘CTE-like’ pathology
27
not identify a single case of CTE-NC in these disease groups,
or with ‘features of CTE’
26 or ‘components of
CTE’30 and
which included 188 participants. As falls are reported to be
suggested they may be attributed to either restrictive sam-
the most common cause of head injury in the older popula-
pling or may be indicative of early-stage CTE-NC that
tion,
68 our findings are inconsistent with speculation that
does not yet meet staging criteria. The current 2021 consen-
falls in later life might cause CTE-NC. These findings sup-
sus criteria recommend that further regions be blocked bilat-
port a previous brain bank study indicating that isolated
erally in cases of high suspicion
19; however, despite our
TBIs are not associated with
CTE-NC.25
additional analysis of superior frontal, inferior temporal, an-
Three of the five cases that we identified with CTE-NC had
terior cingulate and primary motor cortex, we still did not
a primary neuropathological and clinical diagnosis of
identify any strictly perivascular neuronal lesions in these
Alzheimer’s disease and/or Lewy body disease. Two of these
cases. Our findings, and those of
others,46 indicate the pres-
cases (Cases 1 and 2) had relatively sparse foci of CTE-NC in
ence of sulcal depth, perivascular thorn-shaped astrocytes is
the cortical regions examined, supporting the notion that
a consistent feature of CTE-NC and further research is re-
CTE-NC was not likely the cause of dementia in indivi-
quired to better determine the significance of this pathology
duals.21 In contrast, Cases 3 and 4 had more widespread
in the context of CTE-NC.
CTE-NC in all cortical regions examined and extensive tau
link to page 28 link to page 26 link to page 26 link to page 27 link to page 27 link to page 27 link to page 28 link to page 28 link to page 28
link to page 28 link to page 27 link to page 27 link to page 28 link to page 29 link to page 29 link to page 29 link to page 29 link to page 27 link to page 27 link to page 27 link to page 26 link to page 27 link to page 26 link to page 27 link to page 26 link to page 29 link to page 27 link to page 27 link to page 27 link to page 29
CTE in the Sydney
GOV-045703 Brain Bank
BRAIN COMMUNICATIONS 2022: Page 13 of 17 | 13
reporting no association between TBI and Alzheimer’s
cases, as recommended in both the first and second
disease neuropathological change, including CERAD
NINDS/NIBIB consensus criteria. Bilateral sampling is re-
score,82–
84 Thal
phase83 and Braak
stage.82–84 Postupna
commended, if possible, in order to detect patchy or isolated
et al.
29 additionally quantified the levels of paired helical fila-
CTE-NC, particularly in cortical regions.
18,19 In line with
ment tau, ß-amyloid 1–42, α-synuclein, phosphorylated
many neurodegenerative brain banks we endeavour to
TDP-43 as well as markers of inflammation (Iba1 and glial fi-
supply both fresh frozen and formalin-fixed specimens
brillary acidic protein) in various brain regions of a large post-
from cases where asymmetry of pathology is not a barrier
mortem cohort and found no association between TBI and
to achieving a clear neuropathological diagnosis. Of the
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
these measures. However, in a subset of cases with more care-
636 cases analysed only 90 were sampled bilaterally to assess
fully matched control samples and more detailed analysis,
symmetry of CTE-NC. Of the cases with CTE-NC or ‘almost
higher levels of hippocampal tau were found in individuals
CTE-NC’ with bilateral samples, 50–60% had unilateral le-
with a history of TBI with loss of consciousness,
29 which is
sions only. It is therefore possible we may have undetected
more consistent with the findings from our study. Other
cases with CTE-NC due to the largely unilateral sampling.
post-mortem studies also report that TBI is associated
However, all cases identified as having unilateral pathology
with greater tau and ß-amyloid pathology and greater
had less extensive and more isolated CTE-NC, which is likely
phosphorylation-independent TDP-43.
85 Furthermore, im-
to be
asymptomatic.10
aging studies illustrate that tau protein accumulates following
Finally, we did not determine the influence of genetic risk
a single TBI in civilians and military service members and in
factors such as ApoE4 or tau haplotype on pathologies and
former high exposure athletes in multiple brain
regions86–
90
did not record the age at injury and the time between TBI
and changes seen on tau imaging are consistent with the spa-
and death, which may all influence post-mortem study out-
tial distribution of tau pathology seen
post-mortem.89
comes. Indeed, the presence of an ApoE4 allele has been
shown to align with higher cortical grey matter positron
Study limitations
emission tomography tau uptake, suggesting that individuals
with this genotype may be more likely to accumulate tau
A significant limitation of this study is that we did not system-
pathology.
94 Future, prospective, longitudinal studies com-
atically collect information regarding previous contact sport
bining clinical, genetic and post-mortem outcomes will pro-
participation. However, Australians are traditionally active in
vide the crucial information required to definitively address
organized sports from a young age, with an estimated 13%
this area of considerable public concern.
of the population participating in one or more of the four
main contact sport codes in
2017,91 and more than double
Conclusions and future directions
the amount of men playing these sports than
women.92 It is
therefore likely that we have underestimated the prevalence
Emerging research appears to agree that single head injury is not
of mild TBI and repetitive head injury through exposure to con-
associated with CTE-NC and many studies, including ours, in-
tact sport participation in this population. That said, if we as-
dicate the frequency of this pathology in the general population
sume that substantially more people had a personal history of
is likely low.
26,29,30 Our data support a potential role for TBI in
playing contact and collision sports, this reinforces our finding
accelerating the formation of age-related pathologies such as
that CTE-NC is rare in the general population including in
neurofibrillary tangles and LATE. It is unknown whether these
those who played sports in their youth. Additionally, the reli-
changes represent early neurodegeneration underlying various
ance on recall for the reporting of TBI and sporting history,
forms of dementia, and post-mortem study outcomes in this
and the non-standardized methods of data collection, particu-
area are still very conflicting, indicating that many factors are
larly loss of consciousness, is a limiting factor in this study. A
likely to be contributing in this complex scenario. Further stud-
large meta-analysis of 15 studies and 25 134 adults reported
ies are also required to better determine the relative contribution
that 12% of the adult general population has a history of TBI
of neuronal and astrocytic tau to the pathognomonic lesion of
with loss of consciousness.
93 We reported TBI in 17.1% of
CTE-NC, how to conceptualize the subset of cases that almost
our total cohort and TBI with loss of consciousness in just un-
meet criteria for CTE-NC, and to address age-related and
der 3% of this cohort, suggesting this may have been under-
Alzheimer’s disease coexisting neuronal tau pathology in this
reported. Additionally, our definition of TBI for this study
context. The COllaborative Neuropathology NEtwork
was intentionally broad, allowing us to identify the largest sam-
Characterizing ouTcomes of TBI (CONNECT-TBI) initiative
95
ple of cases that might be at risk for CTE-NC.
has been established to address these issues, among others, and
Another limitation was our approach to screening. First,
will provide an international multi-institutional effort to fill
similar to past studies that screened large populations of
these knowledge gaps.
cases,
26,29,30 we examined tissue from the small number of
cortical regions considered to be most valuable to detect
CTE-NC.18,19 Given that CTE-NC can be sparse, isolated,
Acknowledgements
and located nearly anywhere in the cortex, it is possible
that some cases harboring this pathology were not detected.
The authors would like to thank Francine Carew-Jones and
Second, both cerebral hemispheres were not screened in all
Christin Weissleder for their invaluable assistance with tissue
link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14 link to page 14
14 | BRAIN COMMUNICATIONS
GOV-045703
2022: Page 14 of 17 H. McCann
et al.
sampling and immunohistochemistry. We thank Peter
References
Humburg from Stats Central, Mark Wainwright Analytical
Centre, UNSW for support with the statistical analysis. We
1. Martland HS. Punch drunk.
J Am Med Assoc 1928;91:1103–1107.
https://doi.org/10.1001/jama.1928.02700150029009
would also like to thank the brain donor programmes, the
2. Critchley M. Punch-drunk syndromes: The chronic traumatic en-
brain donors and their families for their generous gift to re-
cephalopathy of boxers. In: Maloine, ed.
Hommage a Clovis
search and assistance with clinical history. The Sydney
Vincent. Imprimerie Alascienne; 1949:131–145.
Brain Bank is supported by Neuroscience Research
3. Grahmann H, Ule G. Diagnosis of chronic cerebral symptoms in
Australia.
boxers (dementia pugilistica & traumatic encephalopathy of box-
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
ers).
Psychiatr Neurol (Basel) 1957;134(3–4):261–283. https://
doi.org/10.1159/000138743
Funding
4. Millspaugh JA. Dementia pugilistica.
US Nav Med Bull 1937;35:
297–303.
This work was funded by The Brain Foundation and
5. Omalu BI, Bailes J, Hammers JL, Fitzsimmons RP. Chronic trau-
Neuroscience Research Australia. G.M.H. is a National
matic encephalopathy, suicides and parasuicides in professional
Health and Medical Research Council Leadership Fellow.
American athletes: The role of the forensic pathologist.
Am J
Forensic Med Pathol 2010;31(2):130–132. https://doi.org/10.
1097/PAF.0b013e3181ca7f35
Competing interests
6. Omalu BI, DeKosky ST, Minster RL, Kamboh MI, Hamilton RL,
Wecht CH. Chronic traumatic encephalopathy in a national
A.J.G. serves as a scientific advisor for HitIQ, Ltd. He has a
football league player.
Neurosurgery 2005;57(1):128–134. discus-
sion
128–134.
https://doi.org/10.1227/01.NEU.0000163407.
clinical practice in neuropsychology involving individuals
92769.ED
who have sustained sport-related concussion (including cur-
7. Goldstein LE, Fisher AM, Tagge CA,
et al. Chronic traumatic en-
rent and former athletes). He has been a contracted concus-
cephalopathy in blast-exposed military veterans and a blast neuro-
sion consultant to Rugby Australia since July 2016. He has
trauma mouse model.
Sci Transl Med 2012;4(134):134ra160.
received travel funding or been reimbursed by professional
https://doi.org/10.1126/scitranslmed.3003716
8. McKee AC, Daneshvar DH, Alvarez VE, Stein TD. The neuropath-
sporting bodies, and commercial organizations for discuss-
ology of sport.
Acta Neuropathol 2014;127(1):29–51. https://doi.
ing or presenting sport-related concussion research at meet-
org/10.1007/s00401-013-1230-6
ings, scientific conferences, workshops and symposiums.
9. McKee AC, Robinson ME. Military-related traumatic brain injury
Previous grant funding includes the NSW Sporting Injuries
and neurodegeneration.
Alzheimers Dement 2014;10(Suppl 3):
Committee, the Brain Foundation (Australia), an
S242–S253.
10. McKee AC, Stern RA, Nowinski CJ,
et al. The spectrum of disease in
Australian-American Fulbright Commission Postdoctoral
chronic traumatic encephalopathy.
Brain 2013;136(Pt 1):43–64.
Award, an NHMRC early research career fellowship, a
https://doi.org/10.1093/brain/aws307
Hunter New England Local Health District, Research,
11. Omalu B, Hammers JL, Bailes J,
et al. Chronic traumatic encephal-
Innovation and Partnerships Health Research &
opathy in an Iraqi war veteran with posttraumatic stress disorder
Translation Centre and Clinical Research Fellowship
who committed suicide.
Neurosurg Focus 2011;31(5):E3. https://
doi.org/10.3171/2011.9.FOCUS11178
Scheme, and the Hunter Medical Research Institute
12. Stewart W, McNamara PH, Lawlor B, Hutchinson S, Farrell M.
(HMRI), supported by Jennie Thomas, and the HMRI, sup-
Chronic traumatic encephalopathy: A potential late and under re-
ported by Anne Greaves. G.L.I. serves as a scientific advisor
cognized consequence of rugby union?
QJM 2016;109(1):11–15.
for NanoDx® Inc., Sway Operations, LLC, and Highmark,
https://doi.org/10.1093/qjmed/hcv070
Inc. He has a clinical and consulting practice in forensic
13. Buckland ME, Sy J, Szentmariay I,
et al. Chronic traumatic enceph-
neuropsychology, including expert testimony, involving in-
alopathy in two former Australian national rugby league players.
Acta Neuropathol Commun 2019;7(1):97. https://doi.org/10.
dividuals who have sustained mild TBIs (including athletes).
1186/s40478-019-0751-1
He has received research funding from several test publishing
14. Pearce AJ, Sy J, Lee M,
et al. Chronic traumatic encephalopathy in a
companies, including ImPACT Applications, Inc., CNS Vital
former Australian rules football player diagnosed with Alzheimer’s
Signs, and Psychological Assessment Resources (PAR, Inc.).
disease.
Acta Neuropathol Commun 2020;8(1):23. https://doi.org/
He has received research funding as a principal investigator
10.1186/s40478-020-0895-z
15. Montenigro PH, Baugh CM, Daneshvar DH,
et al. Clinical subtypes
from the National Football League, and salary support as a
of chronic traumatic encephalopathy: Literature review and pro-
collaborator from the Harvard Integrated Program to pro-
posed research diagnostic criteria for traumatic encephalopathy
tect and improve the Health of National Football League
syndrome.
Alzheimers Res Ther 2014;6(5):68. https://doi.org/10.
Players Association Members. He has received research
1186/s13195-014-0068-z
funding from the Wounded Warrior Project™. He has re-
16. Katz DI, Bernick C, Dodick DW,
et al. National institute of
neurological disorders and stroke consensus diagnostic criteria for
ceived unrestricted philanthropic support from ImPACT
traumatic encephalopathy syndrome.
Neurology 2021;96(18):
Applications,
Inc.,
the
Mooney-Reed
Charitable
848–863. https://doi.org/10.1212/WNL.0000000000011850
Foundation, the National Rugby League, the Boston Bolts
17. Omalu B, Bailes J, Hamilton RL,
et al. Emerging histomorphologic
and the Spaulding Research Institute. None of the above en-
phenotypes of chronic traumatic encephalopathy in American ath-
tities were involved in the study design, collection, analysis,
letes.
Neurosurgery 2011;69(1):173–183. discussion 183. https://
doi.org/10.1227/NEU.0b013e318212bc7b
interpretation of data, the writing of this article or the deci-
18. McKee AC, Cairns NJ, Dickson DW,
et al. The first NINDS/NIBIB
sion to submit it for publication. No other authors have any
consensus meeting to define neuropathological criteria for the
competing interests.
diagnosis
of
chronic
traumatic
encephalopathy.
Acta
link to page 14 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 17 link to page 17 link to page 18 link to page 18 link to page 19 link to page 21 link to page 21 link to page 21 link to page 21
CTE in the Sydney
GOV-045703 Brain Bank
BRAIN COMMUNICATIONS 2022: Page 15 of 17 | 15
Neuropathol 2016;131(1):75–86. https://doi.org/10.1007/s00401-
35. Dickson DW, Rademakers R, Hutton ML. Progressive supranuclear
015-1515-z
palsy: Pathology and genetics.
Brain Pathol 2007;17(1):74–82.
19. Bieniek KF, Cairns NJ, Crary JF,
et al. The second NINDS/NIBIB con-
https://doi.org/10.1111/j.1750-3639.2007.00054.x
sensus meeting to define neuropathological criteria for the diagnosis of
36. Ahmed Z, Doherty KM, Silveira-Moriyama L,
et al. Globular glial
chronic traumatic encephalopathy.
J Neuropathol Exp Neurol 2021;
tauopathies (GGT) presenting with motor neuron disease or fronto-
80(3):210–219. https://doi.org/10.1093/jnen/nlab001
temporal dementia: An emerging group of 4-repeat tauopathies.
20. Mez J, Daneshvar DH, Kiernan PT,
et al. Clinicopathological evalu-
Acta Neuropathol 2011;122(4):415–428. https://doi.org/10.1007/
ation of chronic traumatic encephalopathy in players of American
s00401-011-0857-4
football.
JAMA 2017;318(4):360–370. https://doi.org/10.1001/
37. Brettschneider J, Del Tredici K, Toledo JB,
et al. Stages of pTDP-43
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
jama.2017.8334
pathology in amyotrophic lateral sclerosis.
Ann Neurol 2013;74(1):
21. Lee EB, Kinch K, Johnson VE, Trojanowski JQ, Smith DH, Stewart
20–38. https://doi.org/10.1002/ana.23937
W. Chronic traumatic encephalopathy is a common co-morbidity,
38. Vonsattel JP, Myers RH, Stevens TJ, Ferrante RJ, Bird ED,
but less frequent primary dementia in former soccer and rugby
Richardson
EP
Jr.
Neuropathological
classification
of
players.
Acta Neuropathol 2019;138(3):389–399. https://doi.org/
Huntington’s disease.
J Neuropathol Exp Neurol 1985;44(6):
10.1007/s00401-019-02030-y
559–577. https://doi.org/10.1097/00005072-198511000-00003
22. Ling H, Morris HR, Neal JW,
et al. Mixed pathologies including
39. Ahmed Z, Asi YT, Sailer A,
et al. The neuropathology, pathophysi-
chronic traumatic encephalopathy account for dementia in retired
ology and genetics of multiple system atrophy.
Neuropathol Appl
association football (soccer) players.
Acta Neuropathol 2017;
Neurobiol 2012;38(1):4–24. https://doi.org/10.1111/j.1365-2990.
133(3):337–352. https://doi.org/10.1007/s00401-017-1680-3
2011.01234.x
23. Schwab N, Wennberg R, Grenier K, Tartaglia C, Tator C, Hazrati
40. Kovacs GG, Ferrer I, Grinberg LT,
et al. Aging-related tau astrogliopa-
LN. Association of position played and career duration and chronic
thy (ARTAG): Harmonized evaluation strategy.
Acta Neuropathol
traumatic encephalopathy at autopsy in elite football and hockey
2016;131(1):87–102. https://doi.org/10.1007/s00401-015-1509-x
players.
Neurology 2021;96(14):e1835–e1843. https://doi.org/10.
41. Nelson
PT,
Dickson
DW,
Trojanowski
JQ,
et
al.
1212/WNL.0000000000011668
Limbic-predominant age-related TDP-43 encephalopathy (LATE):
24. Hazrati LN, Tartaglia MC, Diamandis P,
et al. Absence of chronic
Consensus working group report.
Brain 2019;142(6):1503–1527.
traumatic encephalopathy in retired football players with multiple
https://doi.org/10.1093/brain/awz099
concussions and neurological symptomatology.
Front Hum
42. Sone J, Mori K, Inagaki T,
et al. Clinicopathological features of
Neurosci 2013;7:222. https://doi.org/10.3389/fnhum.2013.00222
adult-onset neuronal intranuclear inclusion disease.
Brain 2016;
25. Bieniek KF, Ross OA, Cormier KA,
et al. Chronic traumatic enceph-
139(Pt 12):3170–3186. https://doi.org/10.1093/brain/aww249
alopathy pathology in a neurodegenerative disorders brain bank.
43. Ferrer I, Vidal N. Neuropathology of cerebrovascular diseases.
Acta Neuropathol 2015;130(6):877–889. https://doi.org/10.1007/
Handb Clin Neurol 2018;145:79–114. https://doi.org/10.1016/
s00401-015-1502-4
B978-0-12-802395-2.00007-9
26. Bieniek KF, Blessing MM, Heckman MG,
et al. Association between
44. Esiri MM, Wilcock GK, Morris JH. Neuropathological assessment of
contact sports participation and chronic traumatic encephalopathy:
the lesions of significance in vascular dementia.
J Neurol Neurosurg
A retrospective cohort study.
Brain Pathol 2020;30(1):63–74.
Psychiatry 1997;63(6):749–753. https://doi.org/10.1136/jnnp.63.6.749
https://doi.org/10.1111/bpa.12757
45. Hirk R, Hornik K, Vana L. Mvord: An
R package for fitting multi-
27. Noy S, Krawitz S, Del Bigio MR. Chronic traumatic
variate ordinal regression models.
J Stat Softw 2020;93(4):1–41.
encephalopathy-like abnormalities in a routine neuropathology ser-
https://doi.org/10.18637/jss.v093.i04
vice.
J Neuropathol Exp Neurol 2016;75(12):1145–1154. https://
46. Arena JD, Johnson VE, Lee EB,
et al. Astroglial tau pathology alone
doi.org/10.1093/jnen/nlw092
preferentially concentrates at sulcal depths in chronic traumatic en-
28. Ling H, Holton JL, Shaw K, Davey K, Lashley T, Revesz T.
cephalopathy neuropathologic change.
Brain Commun 2020;2(2):
Histological evidence of chronic traumatic encephalopathy in a large
fcaa210. https://doi.org/10.1093/braincomms/fcaa210
series of neurodegenerative diseases.
Acta Neuropathol 2015;130(6):
47. Agrawal S, Yu L, Nag S,
et al. The association of Lewy bodies with
891–893. https://doi.org/10.1007/s00401-015-1496-y
limbic-predominant age-related TDP-43 encephalopathy neuro-
29. Postupna N, Rose SE, Gibbons LE,
et al. The delayed neuropatho-
pathologic changes and their role in cognition and Alzheimer’s de-
logical consequences of traumatic brain injury in a community-
mentia in older persons.
Acta Neuropathol Commun 2021;9(1):
based sample.
Front Neurol 2021;12:624696. https://doi.org/10.
156. https://doi.org/10.1186/s40478-021-01260-0
3389/fneur.2021.624696
48. Agrawal S, Yu L, Kapasi A,
et al. Limbic-predominant age-related
30. Forrest SL, Kril JJ, Wagner S,
et al. Chronic traumatic encephalop-
TDP-43 encephalopathy neuropathologic change and microvascu-
athy (CTE) is absent from a European community-based aging co-
lar pathologies in community-dwelling older persons.
Brain
hort while cortical aging-related tau astrogliopathy (ARTAG) is
Pathol 2021;31(3):e12939. https://doi.org/10.1111/bpa.12939
highly prevalent.
J Neuropathol Exp Neurol 2019;78(5):398–405.
49. Ihara R, Vincent BD, Baxter MR,
et al. Relative neuron loss in hip-
https://doi.org/10.1093/jnen/nlz017
pocampal sclerosis of aging and Alzheimer’s disease.
Ann Neurol
31. Hyman BT, Phelps CH, Beach TG,
et al. National institute on
2018;84(5):741–753. https://doi.org/10.1002/ana.25344
aging-Alzheimer’s association guidelines for the neuropathologic
50. Lopez-Gonzalez I, Carmona M, Blanco R,
et al. Characterization of
assessment of Alzheimer’s disease.
Alzheimers Dement 2012;8(1):
thorn-shaped astrocytes in white matter of temporal lobe in
1–13. https://doi.org/10.1016/j.jalz.2011.10.007
Alzheimer’s disease brains.
Brain Pathol 2013;23(2):144–153.
32. Mackenzie IR, Neumann M, Bigio EH,
et al. Nomenclature and
https://doi.org/10.1111/j.1750-3639.2012.00627.x
nosology for neuropathologic subtypes of frontotemporal lobar de-
51. Ferrer I, Garcia MA, Gonzalez IL,
et al. Aging-related tau astroglio-
generation: An update.
Acta Neuropathol 2010;119(1):1–4. https://
pathy (ARTAG): Not only tau phosphorylation in astrocytes.
Brain
doi.org/10.1007/s00401-009-0612-2
Pathol 2018;28(6):965–985. https://doi.org/10.1111/bpa.12593
33. Mackenzie IR, Neumann M, Baborie A,
et al. A harmonized classi-
52. Arena JD, Smith DH, Lee EB,
et al. Tau immunophenotypes in
fication system for FTLD-TDP pathology.
Acta Neuropathol 2011;
chronic traumatic encephalopathy recapitulate those of ageing
122(1):111–113. https://doi.org/10.1007/s00401-011-0845-8
and Alzheimer’s disease.
Brain 2020;143(5):1572–1587. https://
34. Dickson DW, Bergeron C, Chin SS,
et al. Office of rare diseases neu-
doi.org/10.1093/brain/awaa071
ropathologic criteria for corticobasal degeneration.
J Neuropathol
53. Hsu ET, Gangolli M, Su S,
et al. Astrocytic degeneration in chronic
Exp Neurol 2002;61(11):935–946. https://doi.org/10.1093/jnen/
traumatic encephalopathy.
Acta Neuropathol 2018;136(6):
61.11.935
955–972. https://doi.org/10.1007/s00401-018-1902-3
link to page 21 link to page 22 link to page 22 link to page 22 link to page 22 link to page 22 link to page 22 link to page 22 link to page 22 link to page 22 link to page 22 link to page 23 link to page 23 link to page 23 link to page 23 link to page 24 link to page 24 link to page 24 link to page 24 link to page 24 link to page 24 link to page 24 link to page 24 link to page 24 link to page 24 link to page 24 link to page 24 link to page 24 link to page 25 link to page 25 link to page 25 link to page 25 link to page 25 link to page 25
16 | BRAIN COMMUNICATIONS
GOV-045703
2022: Page 16 of 17 H. McCann
et al.
54. Chancellor KB, Chancellor SE, Duke-Cohan JE,
et al. Altered oligo-
72. Kapasi A, Yu L, Boyle PA, Barnes LL, Bennett DA, Schneider JA.
dendroglia and astroglia in chronic traumatic encephalopathy.
Acta
Limbic-predominant age-related TDP-43 encephalopathy, ADNC
Neuropathol
2021;142(2):295–321.
https://doi.org/10.1007/
pathology, and cognitive decline in aging.
Neurology 2020;95-
s00401-021-02322-2
(14):e1951–e1962.
https://doi.org/10.1212/WNL.0000000000
55. Mez J, Daneshvar DH, Abdolmohammadi B,
et al. Duration of
010454
American football play and chronic traumatic encephalopathy.
Ann
73. Wilson RS, Yu L, Trojanowski JQ,
et al. TDP-43 pathology,
Neurol 2020;87(1):116–131. https://doi.org/10.1002/ana.25611
cognitive decline, and dementia in old age.
JAMA Neurol 2013;70-
56. McKee AC, Gavett BE, Stern RA,
et al. TDP-43 proteinopathy and
(11):1418–1424. https://doi.org/10.1001/jamaneurol.2013.3961
motor neuron disease in chronic traumatic encephalopathy.
J
74. Nordstrom A, Nordstrom P. Traumatic brain injury and the risk
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
Neuropathol Exp Neurol 2010;69(9):918–929. https://doi.org/10.
of dementia diagnosis: A nationwide cohort study.
PLoS
1097/NEN.0b013e3181ee7d85
Med 2018;15(1):e1002496. https://doi.org/10.1371/journal.pmed.
57. Koga S, Dickson DW, Bieniek KF. Chronic traumatic encephalop-
1002496
athy pathology in multiple system atrophy.
J Neuropathol Exp
75. Fann JR, Ribe AR, Pedersen HS,
et al. Long-term risk of de-
Neurol
2016;75(10):963–970.
https://doi.org/10.1093/jnen/
mentia among people with traumatic brain injury in
nlw073
Denmark: A population-based observational cohort study.
58. Braak H, Braak E. Neuropathological stageing of Alzheimer-related
Lancet Psychiatry 2018;5(5):424–431. https://doi.org/10.1016/
changes.
Acta Neuropathol 1991;82(4):239–259. https://doi.org/
S2215-0366(18)30065-8
10.1007/BF00308809
76. Guo Z, Cupples LA, Kurz A,
et al. Head injury and the risk of AD in
59. Cherry JD, Kim SH, Stein TD,
et al. Evolution of neuronal and glial
the MIRAGE study.
Neurology 2000;54(6):1316–1323. https://doi.
tau isoforms in chronic traumatic encephalopathy.
Brain Pathol
org/10.1212/WNL.54.6.1316
2020;30(5):913–925. https://doi.org/10.1111/bpa.12867
77. Gardner RC, Burke JF, Nettiksimmons J, Kaup A, Barnes DE, Yaffe
60. Kanaan NM, Cox K, Alvarez VE, Stein TD, Poncil S, McKee AC.
K. Dementia risk after traumatic brain injury vs nonbrain trauma:
Characterization of early pathological tau conformations and phos-
The role of age and severity.
JAMA Neurol 2014;71(12):
phorylation in chronic traumatic encephalopathy.
J Neuropathol
1490–1497. https://doi.org/10.1001/jamaneurol.2014.2668
Exp Neurol 2016;75(1):19–34. https://doi.org/10.1093/jnen/
78. Iacono D, Raiciulescu S, Olsen C, Perl DP. Traumatic brain injury
nlv001
exposure lowers age of cognitive decline in AD and non-AD condi-
61. Schmidt ML, Zhukareva V, Newell KL, Lee VM, Trojanowski JQ.
tions.
Front Neurol 2021;12:573401. https://doi.org/10.3389/
Tau isoform profile and phosphorylation state in dementia pugilis-
fneur.2021.573401
tica recapitulate Alzheimer’s disease.
Acta Neuropathol 2001;
79. Barnes DE, Byers AL, Gardner RC, Seal KH, Boscardin WJ, Yaffe K.
101(5):518–524. https://doi.org/10.1007/s004010000330
Association of mild traumatic brain injury with and without loss of
62. Lucke-Wold B, Seidel K, Udo R,
et al. Role of tau acetylation in
consciousness with dementia in US military veterans.
JAMA Neurol
Alzheimer’s disease and chronic traumatic encephalopathy: The
2018;75(9):1055–1061. https://doi.org/10.1001/jamaneurol.2018.
way forward for successful treatment.
J Neurol Neurosurg 2017;
0815
4(2):140.
80. Li Y, Li Y, Li X,
et al. Head injury as a risk factor for dementia and
63. Seo JS, Lee S, Shin JY,
et al. Transcriptome analyses of chronic trau-
Alzheimer’s disease: A systematic review and meta-analysis of 32
matic encephalopathy show alterations in protein phosphatase ex-
observational studies.
PLoS One 2017;12(1):e0169650.
pression associated with tauopathy.
Exp Mol Med 2017;49(5):
81. Fleminger S, Oliver DL, Lovestone S, Rabe-Hesketh S, Giora A.
e333. https://doi.org/10.1038/emm.2017.56
Head injury as a risk factor for Alzheimer’s disease: The
64. Cherry JD, Zeineddin A, Dammer EB,
et al. Characterization of de-
evidence 10 years on; a partial replication.
J Neurol Neurosurg
tergent insoluble proteome in chronic traumatic encephalopathy.
J
Psychiatry 2003;74(7):857–862. https://doi.org/10.1136/jnnp.74.
Neuropathol Exp Neurol 2018;77(1):40–49. https://doi.org/10.
7.857
1093/jnen/nlx100
82. Sugarman MA, McKee AC, Stein TD,
et al. Failure to detect an as-
65. Falcon B, Zivanov J, Zhang W,
et al. Novel tau filament fold in
sociation between self-reported traumatic brain injury and
chronic traumatic encephalopathy encloses hydrophobic molecules.
Alzheimer’s disease neuropathology and dementia.
Alzheimers
Nature 2019;568(7752):420–423. https://doi.org/10.1038/s41586-
Dement 2019;15(5):686–698. https://doi.org/10.1016/j.jalz.2018.
019-1026-5
12.015
66. Wielinski CL, Erickson-Davis C, Wichmann R, Walde-Douglas M,
83. Robinson AC, Davidson YS, Horan MA, Cairns M, Pendleton N,
Parashos SA. Falls and injuries resulting from falls among patients
Mann DMA. No association between head injury with loss of con-
with Parkinson’s disease and other parkinsonian syndromes.
Mov
sciousness and Alzheimer disease pathology—Findings from the
Disord 2005;20(4):410–415. https://doi.org/10.1002/mds.20347
University of Manchester longitudinal study of cognition in normal
67. Brown FS, Rowe JB, Passamonti L, Rittman T. Falls in progressive
healthy old age.
Int J Geriatr Psychiatry 2019;34(8):1262–1266.
supranuclear palsy.
Mov Disord Clin Pract 2020;7(1):16–24.
https://doi.org/10.1002/gps.5129
https://doi.org/10.1002/mdc3.12879
84. Crane PK, Gibbons LE, Dams-O’Connor K,
et al. Association
68. Thompson HJ, McCormick WC, Kagan SH. Traumatic brain injury
of traumatic brain injury with late-life neurodegenerative conditions
in older adults: Epidemiology, outcomes, and future implications.
J
and neuropathologic findings.
JAMA Neurol 2016;73(9):
Am Geriatr Soc 2006;54(10):1590–1595. https://doi.org/10.1111/j.
1062–1069. https://doi.org/10.1001/jamaneurol.2016.1948
1532-5415.2006.00894.x
85. Johnson VE, Stewart W, Smith DH. Widespread tau and amyloid-
69. Crary JF, Trojanowski JQ, Schneider JA,
et al. Primary age-related
beta pathology many years after a single traumatic brain injury in
tauopathy (PART): A common pathology associated with human
humans.
Brain Pathol 2012;22(2):142–149. https://doi.org/10.
aging.
Acta Neuropathol 2014;128(6):755–766. https://doi.org/
1111/j.1750-3639.2011.00513.x
10.1007/s00401-014-1349-0
86. Robinson ME, McKee AC, Salat DH,
et al. Positron emission tom-
70. Dickson DW, Davies P, Bevona C,
et al. Hippocampal sclerosis: A
ography of tau in Iraq and Afghanistan veterans with blast neuro-
common pathological feature of dementia in very old (> or = 80
trauma.
Neuroimage Clin 2019;21:101651. https://doi.org/10.
years of age) humans.
Acta Neuropathol 1994;88(3):212–221.
1016/j.nicl.2019.101651
https://doi.org/10.1007/BF00293396
87. Gorgoraptis N, Li LM, Whittington A,
et al. In vivo detection of
71. Nelson PT, Schmitt FA, Lin Y,
et al. Hippocampal sclerosis in ad-
cerebral tau pathology in long-term survivors of traumatic brain in-
vanced age: Clinical and pathological features.
Brain 2011;134(Pt
jury.
Sci Transl Med 2019;11(508):eaaw1993. https://doi.org/10.
5):1506–1518. https://doi.org/10.1093/brain/awr053
1126/scitranslmed.aaw1993
link to page 25 link to page 25 link to page 25 link to page 25 link to page 25 link to page 25 link to page 25 link to page 25
CTE in the Sydney
GOV-045703 Brain Bank
BRAIN COMMUNICATIONS 2022: Page 17 of 17 | 17
88. Takahata K, Kimura Y, Sahara N,
et al. PET-detectable tau path-
92. Eime R, Charity M, Harvey J, Westerbeek H. Five-year changes in
ology correlates with long-term neuropsychiatric outcomes in pa-
community-level sport participation, and the role of gender strat-
tients with traumatic brain injury.
Brain 2019;142(10):
egies.
Front Sports Act Living 2021;3:710666. https://doi.org/10.
3265–3279. https://doi.org/10.1093/brain/awz238
3389/fspor.2021.710666
89. Barrio JR, Small GW, Wong KP,
et al. In vivo characterization of
93. Frost RB, Farrer TJ, Primosch M, Hedges DW. Prevalence of trau-
chronic traumatic encephalopathy using [F-18]FDDNP PET brain
matic brain injury in the general adult population: A meta-analysis.
imaging.
Proc Natl Acad Sci U S A 2015;112(16):E2039–E2047.
Neuroepidemiology 2013;40(3):154–159. https://doi.org/10.1159/
https://doi.org/10.1073/pnas.1409952112
000343275
90. Stern RA, Adler CH, Chen K,
et al. Tau positron-emission tomog-
94. Vasilevskaya A, Taghdiri F, Burke C,
et al. Interaction of APOE4 al-
Downloaded from https://academic.oup.com/braincomms/article/4/4/fcac189/6651150 by University of Auckland user on 17 December 2024
raphy in former national football league players.
N Engl J
leles and PET tau imaging in former contact sport athletes.
Med 2019;380(18):1716–1725. https://doi.org/10.1056/NEJMoa
Neuroimage Clin 2020;26:102212. https://doi.org/10.1016/j.nicl.
1900757
2020.102212
91. Football participation stabilises with more women playing. Roy
95. Smith DH, Dollé JP, Ameen-Ali KE,
et al. COllaborative
Morgan. 2018. Accessed 22 November 2021. http://www.
Neuropathology NEtwork Characterizing ouTcomes of TBI
roymorgan.com/findings/7539-women-in-football-december-
(CONNECT-TBI).
Acta Neuropathol Commun 2021;9(1):32.
2017-201803230556
https://doi.org/10.1186/s40478-021-01122-9
GOV-045703
From:
[Out of Scope]
Sent:
Thursday, 22 February 2024 8:46 pm
To:
[Out of Scope]
Subject:
Re: Follow-up
Kia Ora [Out
and
of Scope
thank you [Out of Scope] for the introduction.
My name is [Out of Scope]
and my role is head of health partnerships at ACC. Which includes our
health commissioning and contract management.
It would be good to catch up and understand more about your work in concussion / TBI.
Let's organise a time to catch up in the near future.
Nga mihi nui
[Out of Scope]
Get Outlook for iOS
From: [Out of Scope]
@acc.co.nz>
Sent: Thursday, February 22, 2024 7:31 AM
To: [Out of Scope]
@matai.org.nz>
Cc: [Out of Scope]
@acc.co.nz>
Subject: RE: Follow-up
Kia ora [Out
of Scop
All good man. Another connection would be great thanks. I’ll get someone from our Health Partnerships team to follow
up with you if that’s ok
Nga mihi
[Out
of Scope]
Deputy Chief Executive - Prevention & Partnerships, ACC
ACC cares about the environment – please don’t print this email
unless it is really necessary. Thank you.
From: [Out of Scope]
@matai.org.nz>
Sent: Wednesday, February 21, 2024 5:57 PM
To: [Out of Scope]
@acc.co.nz>
Subject: Follow-up
1
GOV-045703
From:
[Out of Scope]
@matai.org.nz>
Sent:
Wednesday, 24 September 2025 2:00 pm
To:
[Out of Scope]
Subject:
Re: few updates for the Tūranga Health Tūārai report on how things have progressed
for the kaupapa Wairoro programme of work during the July – September quarter
Kia ora [Out of Scope]
Mātai hosted an interactive Careers in Science Day for over 150 Year 12–13 students from Gisborne Boys’ High
School, Manutuke School, Wairoa College, Ngā Uri a Māui, Campion College, Gisborne Girls’ High
School, and Lytton High School. The kaupapa was simple: bring health science to life through kanohi-ki-te-
kanohi experiences. Students rotated through hands-on stations run by Mātai, and with support from Tōnui
Collab, the Auckland Bioengineering Institute, Health NZ Tairāwhiti, FACT—First Aid & CPR Training, TBI
Health, and Geneva Health, meeting researchers, technologists, and clinicians. The feedback was clear, science
isn’t “just a lab coat”; it connects to sport, creativity, physics, dentistry, and real jobs, and many tauira said it
helped them see why people choose these pathways.
Throughout the day, rangatahi heard from local and national scientists, including Dr [Out of Scope] (concussion
research) and PhD student [Out of Scope], who emphasised whānau-centred motivations for science and its impact
for communities up the coast. [Out of Scope] , a former Gisborne Girls’ High School student now completing
her PhD at Mātai on symptoms that follow brain injury, explained that the brain has ~86 billion neurons controlling
movement, senses, thinking, memory, and automatic functions like breathing, and that everyday choices
(including drug use and screen time) influence neuronal activity. Her doorway demo, pressing arms against a
frame for 30 seconds, then stepping away to see them lift on their own as neurons keep firing briefly, made the
science click. Demonstrations like instrumented mouthguards with the Gisborne Boys’ High School 1st
XV showed how research and sport intersect in everyday life.
The energy and kōrero from students and kaiako set the tone for ongoing engagement, inviting whānau to connect
again at the A&P Show, the Tairāwhiti Brain & Health Symposium (War Memorial Theatre, 28 Nov), and the
next Mātai open day (29 Nov).
Ngā mihi,
[Out of Scope]
From: [Out of Scope]
@acc.co.nz>
Date: Wednesday, 24 September 2025 at 12:59 PM
To: [Out of Scope]
@matai.org.nz>, [Out of Scope]
@turangahealth.co.nz>
Subject: few updates for the Tūranga Health Tūārai report on how things have progressed for the
kaupapa Wairoro programme of work during the July – September quarter
Kia ora [Out of Scope]
Can we get a few updates from you for the Tūranga Health report that goes to ACC on how things have progressed
for the kaupapa Wairoro programme of work during the July – September quarter? Can either just send through a
paragraph or two or can just drop in the empty column below.
1
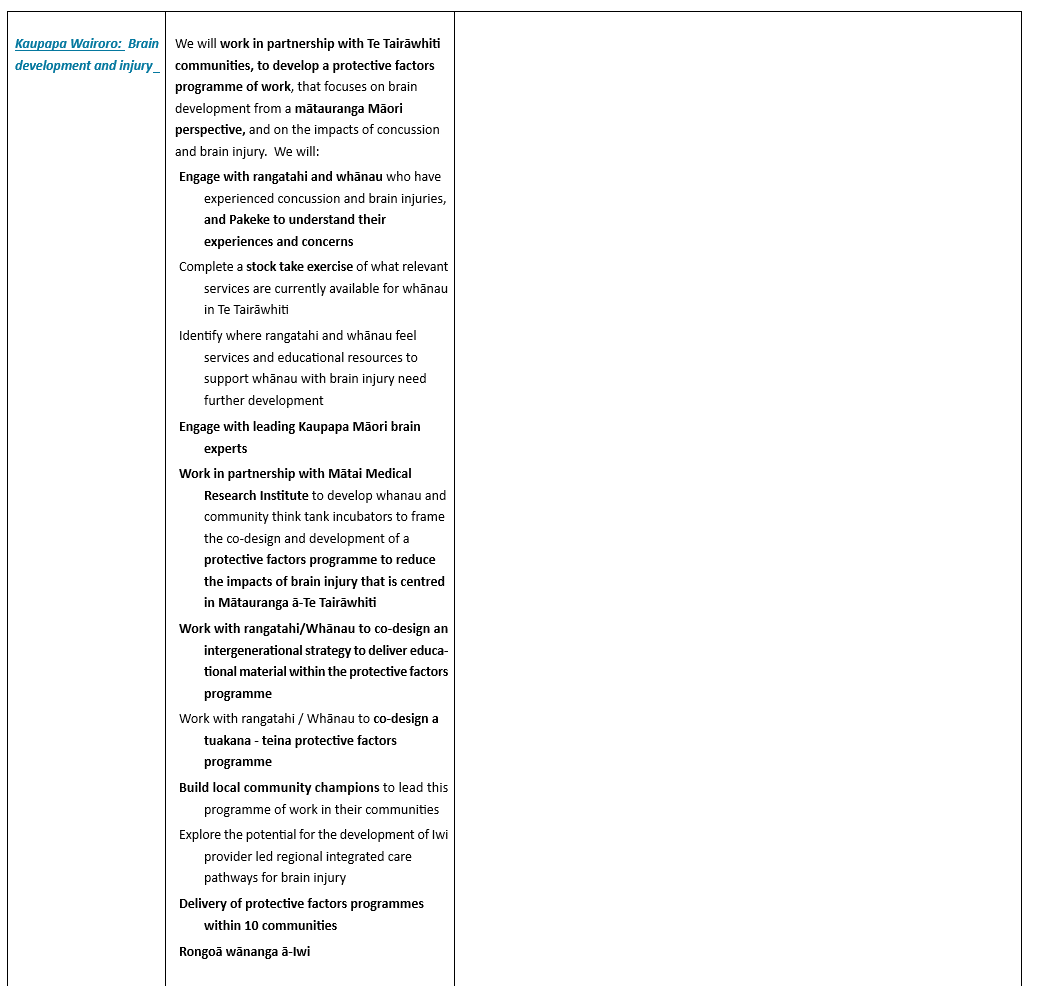
GOV-045703
GOV-045703
Disclaimer:
"This mess
age and any attachments may contain confidential and privileged information. If you believe
you have received this email in error, please advise us immediately by return email or telephone and
then delete this email together with all attachments. If you are not the intended recipient, you are not
authorised to use or copy this message or any attachments or disclose the contents to any other
person."
3