

133 Molesworth Street
PO Box 5013
Wellington 6140
New Zealand
T+64 4 496 2000
25 February 2026
Elspeth Baker-Verves
By email: [FYI request #33059 email]
Ref: H2025076281
Tēnā koe Elspeth
Response to your request for official information
Thank you for your request under the Official Information Act 1982 (the Act) to the Ministry of
Health – Manatū Hauora (the Ministry) on 30 November 2025 for information regarding ADHD
Hui Actions, Data Survey Funding, and Coordination Progress. I wil respond to each part of
your request below.
The Ministry notes that you have made multiple requests on the same topic (H2025076364,
H2025076972, H2025076445, and H2025076277 refers), which has resulted in some overlap
in subject matter across the documents identified. To avoid unnecessary repetition or
reproduction of the same material, these are instead referenced in the appropriate releases in
Appendix 1.
Please provide the following information, with specific reference to the Ministry’s
memorandum ‘Aide-Mémoire: ADHD Actions, Dependencies and Milestones
(H2024050133)’:
1. Funding for ADHD Data Survey
a. Has funding been approved or allocated for the ADHD data survey referenced in the
Aide-Mémoire?
b. If yes, please provide the amount, the funding source within Vote Health, and the
financial year(s) in which it is allocated.
c. If funding has not been approved, please provide all correspondence, budget bids, or
internal discussion documents relating to efforts to secure funding.”
The Ministry can confirm that funding has been approved and allocated. In September 2024,
the Minister for Mental Health, Hon Matt Doocey, announced ongoing funding for the delivery of
mental health and addiction prevalence studies. See the announcement here:
www.beehive.govt.nz/release/peer-mental-health-service-launched-further-support-planned.
The Ministry also communicated this funding publicly here:
www.health.govt.nz/news/new-
funding-for-child-and-youth-mental-health-survey.
The funding sources for the study are previously uncommitted mental health and addictions
funding, which the Government has commit ed to allocating towards the Child and Youth Mental
Health Study on an ongoing basis. This funding of $2 mil ion per annum is not time limited.
2. Progress on Data Survey (Design 2025 – Collection 2026 – Reporting 2027)
a. Has the 2025 design phase commenced, and if so, who is leading or contracting this
work?
The design phase commenced in 2025. National Research Bureau (NRB), a New Zealand-
based research company specialising in conducting national surveys, wil collect the data
through interviews with members of the public. The Universities of Otago and Auckland are
designing the study and questionnaire and providing mental health support to participants. This
information is publicly available here:
www.health.govt.nz/statistics-research/surveys/child-and-
youth-mental-health-study. As such, section 18(d) of the Act applies to this part of your request.
b. What milestones have been achieved to date?
Milestones that have been achieved to date include:
• established key leadership and technical roles to deliver the first iteration of the Child
and Youth Mental Health Study.
• establishment of a Governance Group, Expert Advisory Group and Youth Advisory
Group to guide the development and implementation of the study.
• completing a procurement process and contracting a provider to design and implement
the study.
• confirmation of objectives for the first iteration of the study.
• planning the methodology of the study.
c. Is the timeline for 2026 collection and mid-2027 data release stil current?
The Ministry can confirm that these estimated timeframes are stil correct. We anticipate
fieldwork beginning in April 2026 and initial results being published by the Ministry in July 2027.
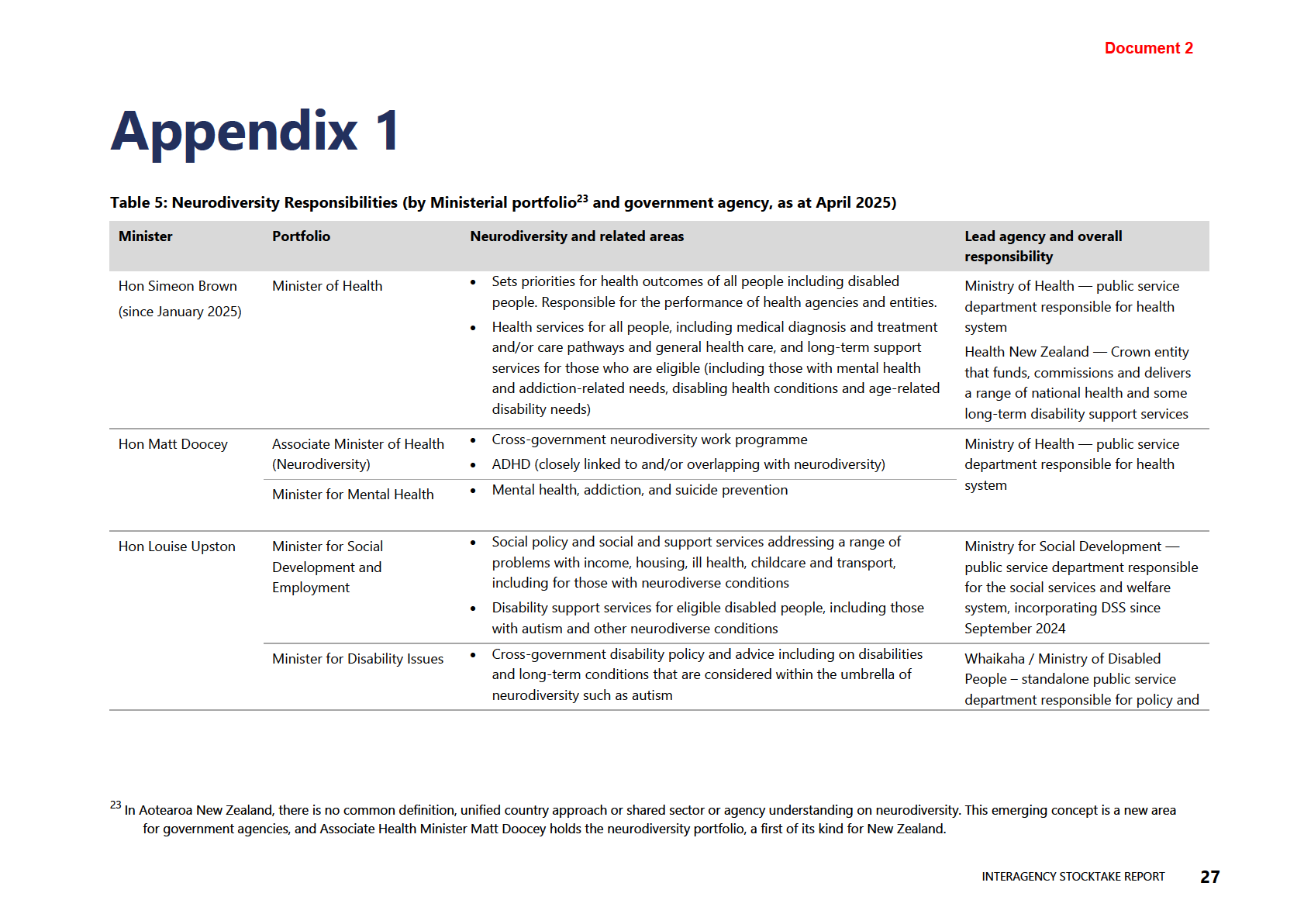
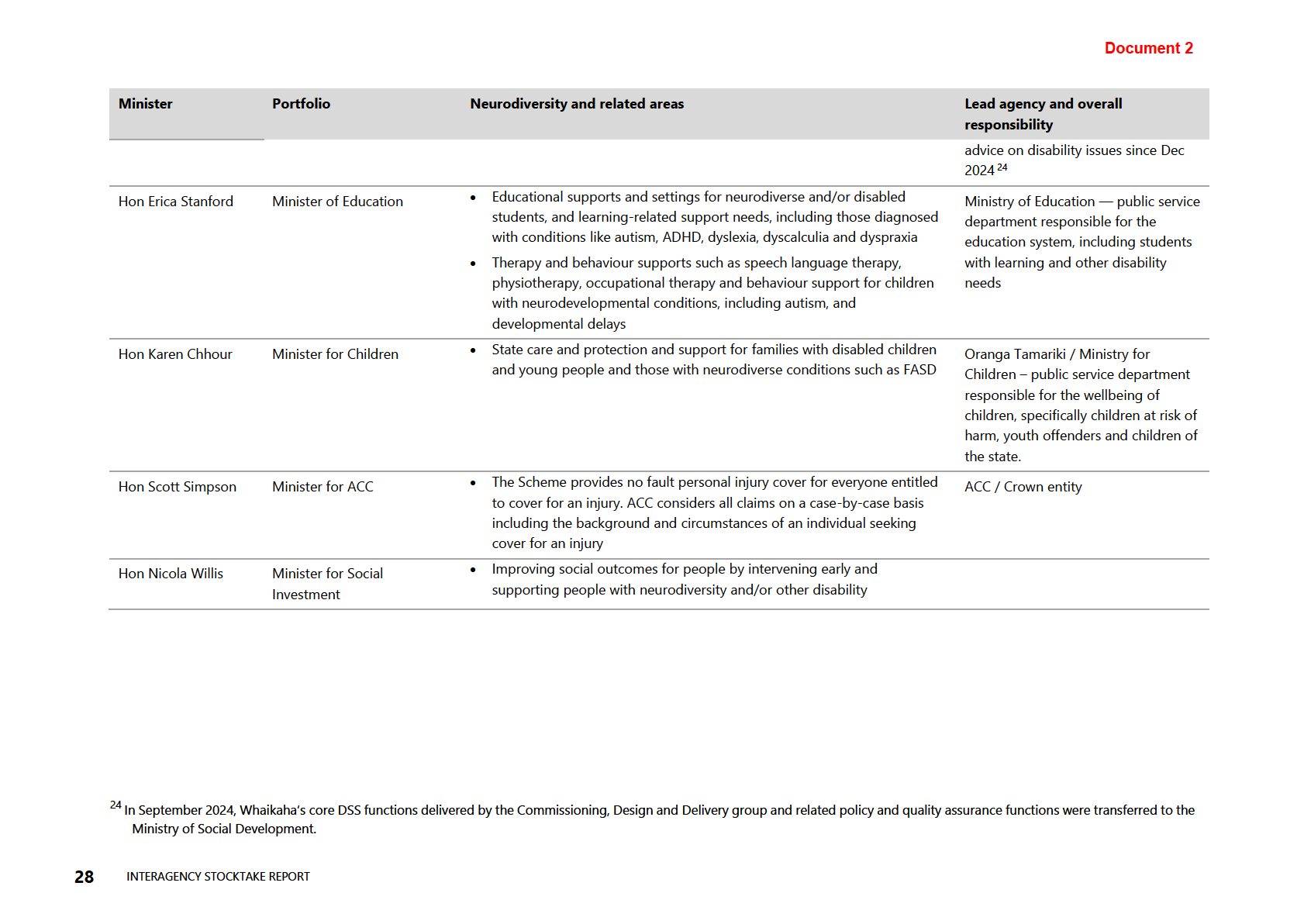
3. Cross-Agency Neurodiversity Group Stocktake
a. Has the cross-agency neurodiversity group’s stocktake of ADHD-related supports and
screening tools been completed?
b. If yes, please release the stocktake report or summary findings.
c. If not, please provide the expected completion date and the lead agency responsible.
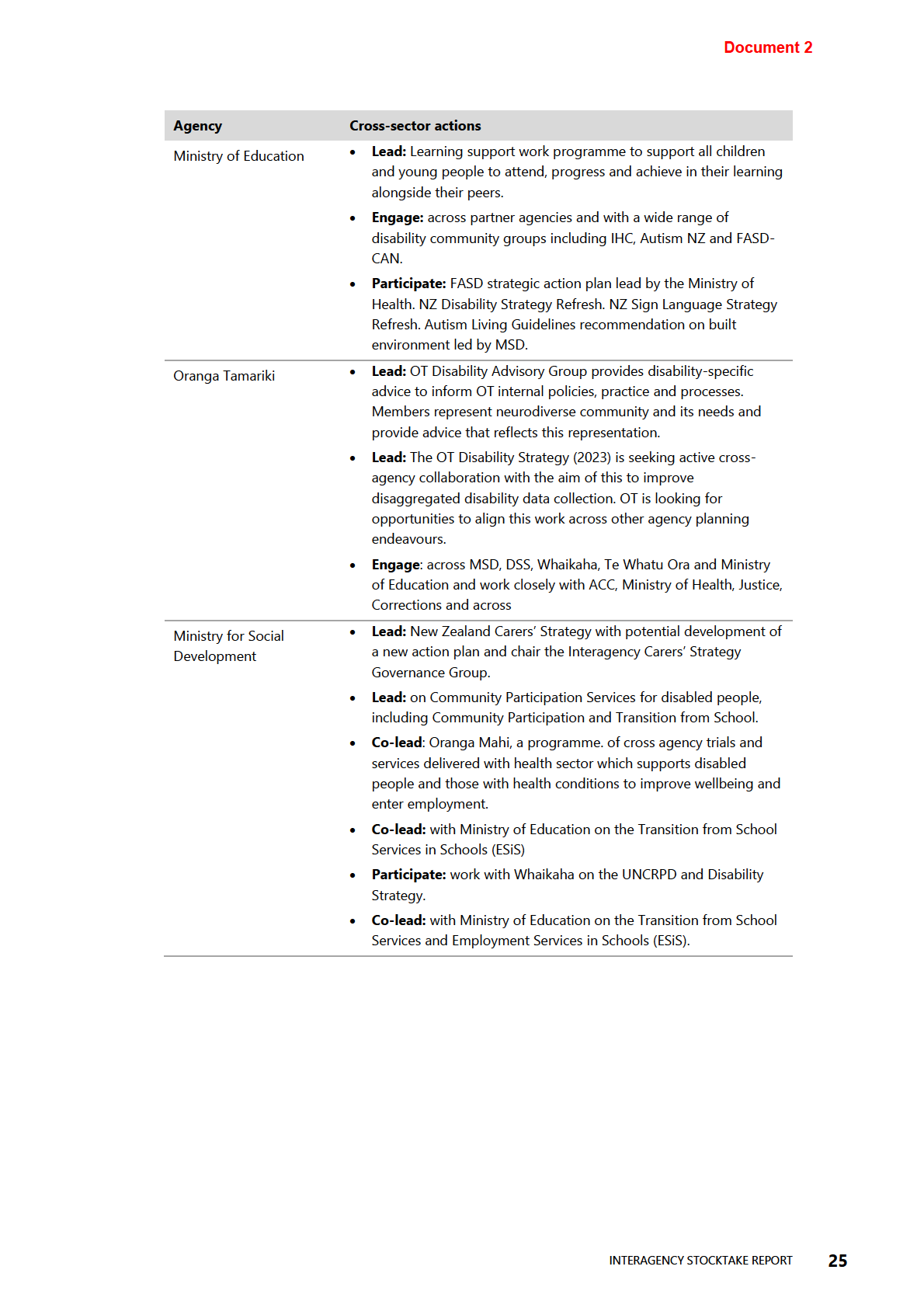
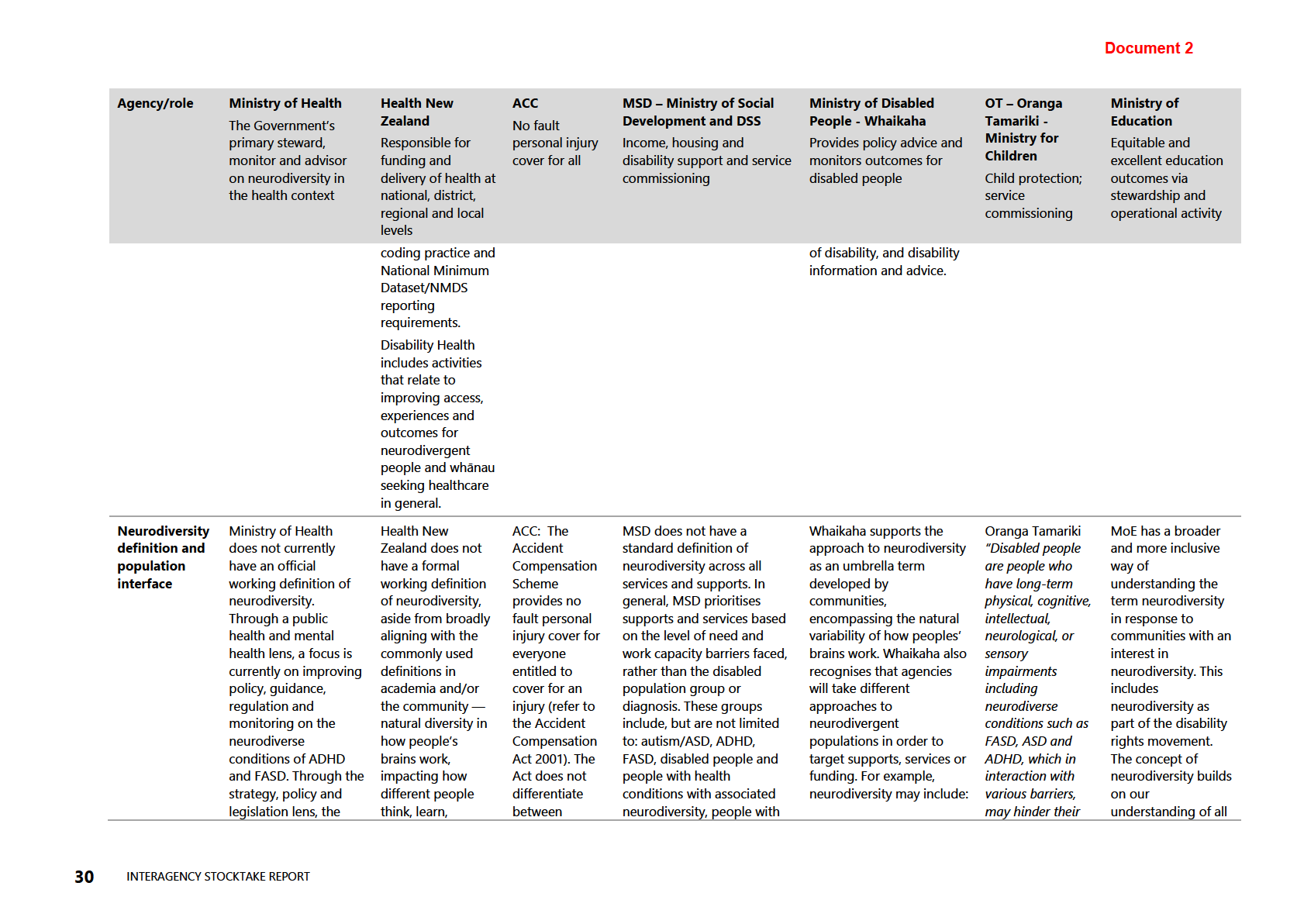
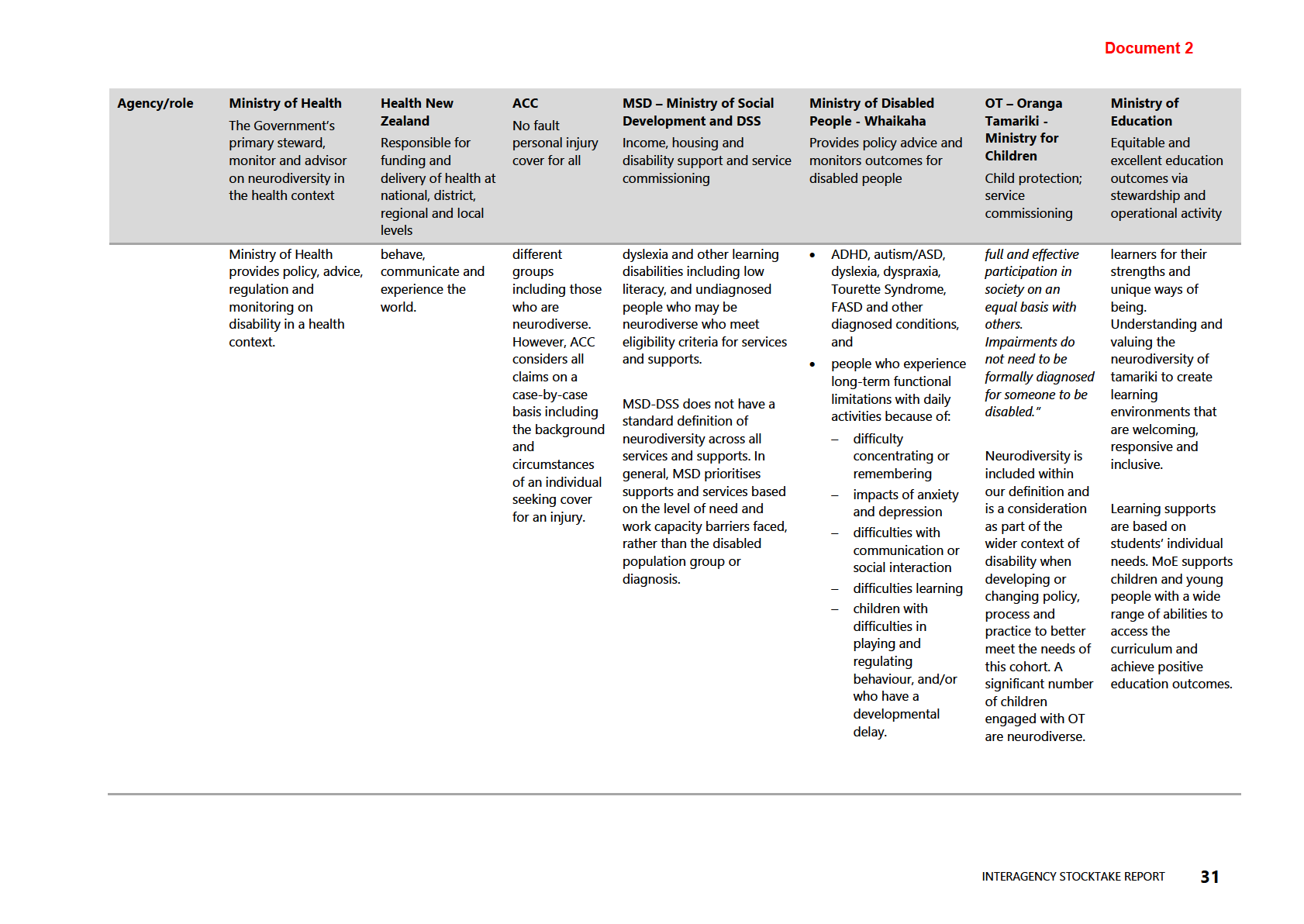
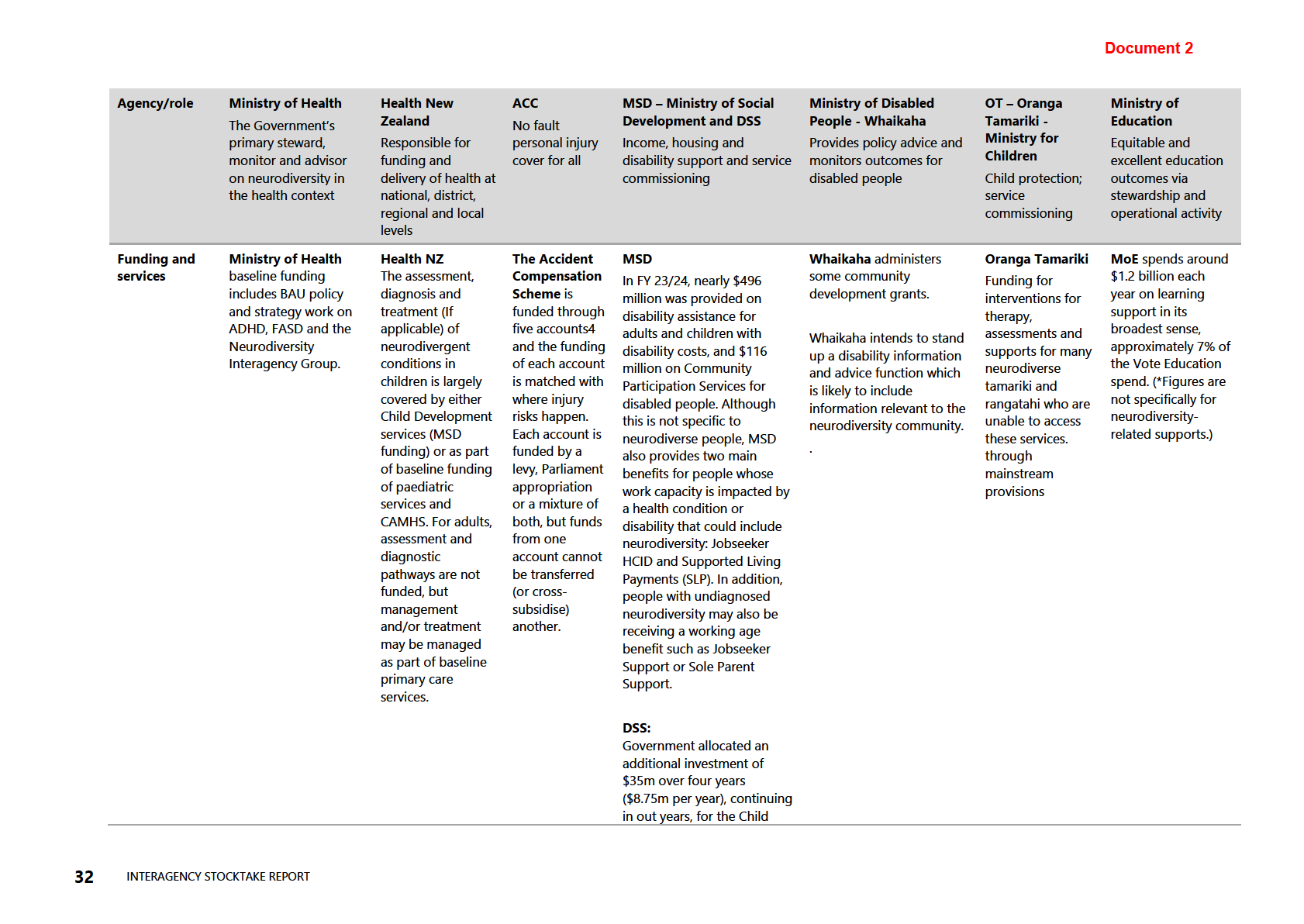
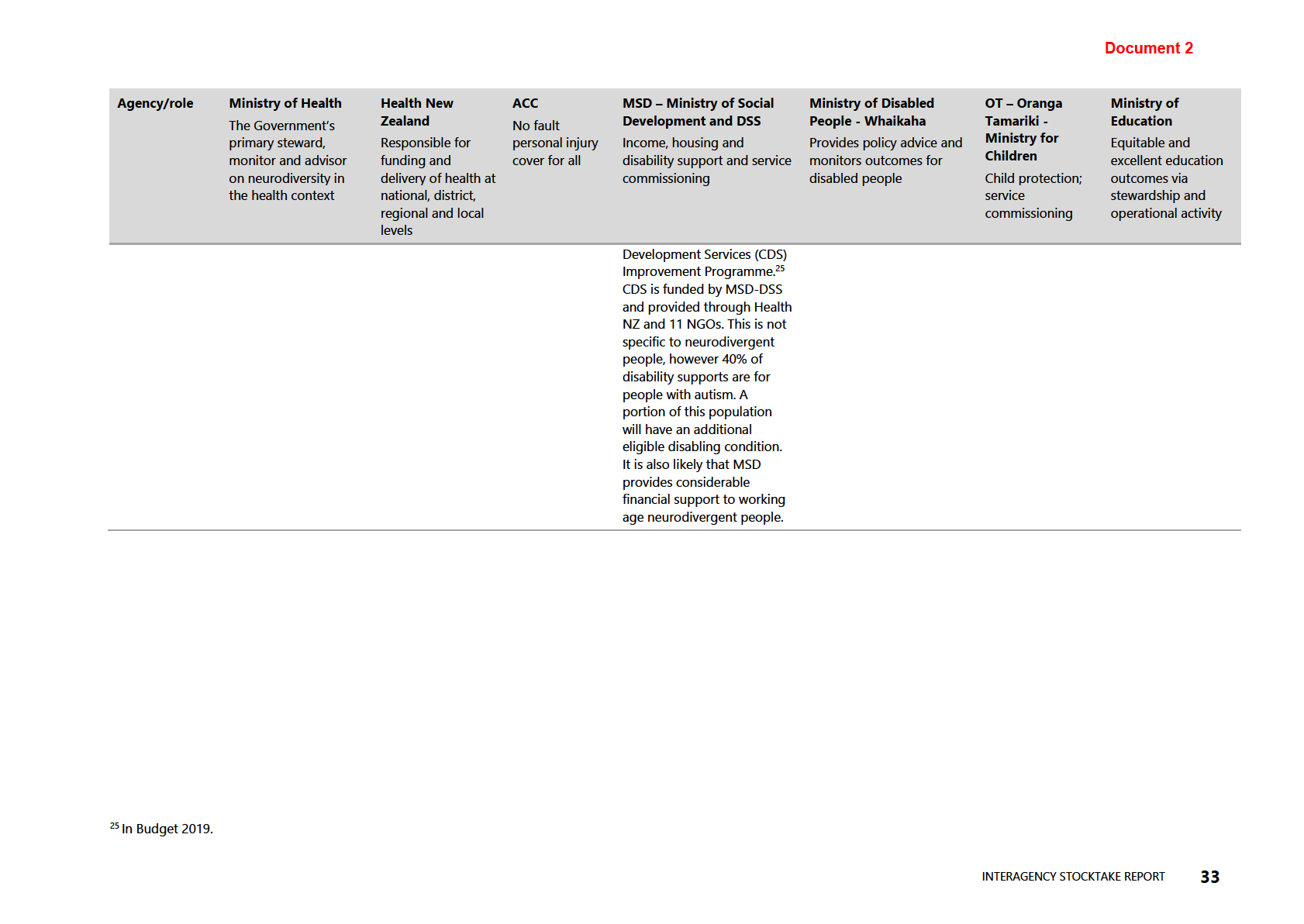
The Ministry completed an Interagency Stocktake report on how government agencies design
and deliver supports and services with neurodiversity in mind. Please see Document 2, noting
the context for the following statements:
• “
40% of disability supports in New Zealand are for people with autism” on pages 4 and
33. This does not represent all of government or Ministry of Social Development (MSD)
funded disability supports.
• “
Ministry of Social Development and Whaikaha hold data on specific clinical diagnosis,
much of this on autism.” on page 19. This refers specifically to MSD-Disability Support
Services (MSD-DSS) and Whaikaha. It does not refer to MSD as a whole.
• “
Co-lead with Ministry of Education on the Transition from School Services and
Employment Services in Schools (ESiS)” on pages 25 and 29. MSD co-leads with the
Ministry of Education on the transition service
Employment Services in Schools (ESiS).
This is a separate programme to the
Transition from School Service.
Page 2 of 5
4. ADHD Collaborative Network
a. Have any agencies considered providing funding or secretariat support to reinstate the
ADHD Collaborative Network, given that coordination became unsustainable for ADHD NZ
in 2023 due to lack of resourcing?
b. Are there any current plans to establish or fund an alternative ADHD-specific
coordination mechanism?
The Ministry and Health New Zealand have previously considered a proposal received from
ADHD NZ to fund a programme director, research director, part time project coordinator and
secretariat support. The Ministry is not aware of any current plans to fund an ADHD-specific
coordination mechanism. If you require further information on funding, please contact Health
New Zealand vi
a [email address].
5. Monitoring and Accountability
a. Please provide any progress reports, briefings, updates, or minutes tracking
implementation of the six actions agreed at the 2024 Parliamentary Hui.
b. Please identify the mechanisms or governance structures in place to monitor delivery
across agencies.
The Ministry provided Ministers with advice on the progress and next steps for the actions
agreed at the 2024 Parliamentary hui and noted that the range of actions means that there are
many responsible agencies requiring a coordinated cross-government approach. The Health-led
actions include increasing access to stimulant medications, working with the Clinical Reference
group to develop guidelines, and progressing an updated prevalence study have now either
been completed or have made significant progress. Document 6 outlines this in more detail. As
of February 2026, the action to develop clinical guidelines for ADHD has been completed and is
publicly available. Please refer to Document 5 for this information. The action to increase
access to stimulant medications has achieved the key milestone of enabling GPs and nurse
practitioners to prescribe stimulant medications from 1 February 2026. Further information
relating to this can be found in a press release issued on 1 February by the Hon Matt Doocey,
Minister for Mental Health which is available at:
www.beehive.govt.nz/release/faster-access-
adhd-support-coming. Further work is now underway to provide appropriate training and
guidance for GPs and nurse practitioners who wish to undertake ADHD assessments and
treatment. The action to progress a prevalence study is progressing. Please refer to the
response to question 2a above for more information relating to this.
The Ministry is not aware of any ongoing monitoring of actions agreed at the 2024
Parliamentary hui. The Ministry continues to provide stewardship for the health sector on the
changes to assessing and treating ADHD, and ongoing advice to the Government on ADHD
related activities as required.
6. Next ADHD Parliamentary Hui
a. Please confirm whether a further ADHD Parliamentary Hui is scheduled.
b. If so, please provide the planned or proposed date, the hosting agency, the invited
organisations, and any agenda or draft-agenda documents.
The Ministry is not aware of a further ADHD Parliamentary hui being scheduled. The previous
Parliamentary hui in 2024 was organised and facilitated by ADHD NZ and may be better placed
to respond to any plans for future events. Their contact details are available here:
www.adhd.org.nz/about/contact.
If you wish to discuss any aspect of your request with us, including this decision, please feel
free to contact the OIA Services Team on:
[email address].
Page 3 of 5
Under section 28(3) of the Act, you have the right to ask the Ombudsman to review any
decisions made under this request. The Ombudsman may be contacted by email at:
[email address] or by calling 0800 802 602.
Please note that this response, with your personal details removed, may be published on the
Ministry website at:
www.health.govt.nz/about-ministry/information-releases/responses-official-
information-act-requests.
Nāku noa, nā
Steve Barnes
Associate Deputy Director-General
Strategy and Policy | Te Pou Rautaki
Page 4 of 5
Appendix 1: List of documents for release
#
Date
Document details
Decision on release
1
30 April 2025
Briefing for information:
An initial Some information is withheld
stocktake on neurodiversity work under section 9(2)(a) of the Act,
across government
to protect the privacy of natural
(H2025062730)
per
sons.
2
Interagency stocktake report:
how Some information is withheld
government agencies design and under section 9(2)(f)(iv) of the
deliver supports and services
Act, to maintain the
with neurodiversity in mind
constitutional conventions that
protect the confidentiality of
advice tendered by Ministers
and officials.
3
19 July 2025
Briefing:
Progressing a Child and Some information is withheld
Youth Mental Health and
under section 9(2)(a) of the Act.
Addiction Prevalence Survey
(H2024042404)
4
2 September 2025 Appendix 3 in Cabinet paper:
This document has been
Updated suicide prevention action proactively released on the
plan consultation document
Ministry’s website at:
(SOU‑
24‑
MIN‑
0104)
www.health.govt.nz/system/file
s/2024-
10/Cabinet%20material%20-
%20Updated%20Suicide%20Pr
evention%20Action%20Plan%2
0Release%20of%20Consultatio
n%20Document%20CAB-24-
MIN-0518%20CAB-24-MIN-
0327%20BLACK%20BOX.pdf.
Therefore, section 18(d) of the
Act applies.
5
September 2025
New Zealand Clinical Principles This document has been
Framework for At ention Deficit proactively released on the
Hyperactivity Disorder
Ministry’s website at:
www.health.govt.nz/system/file
s/2025-10/new-zealand-clinical-
principles-framework-for-
attention-deficit-hyperactivity-
disorder-v2.pdf. Therefore,
section 18(d) of the Act applies.
6
18 September 2024 Aide-Mémoire:
ADHD Actions,
This document has been
Dependencies and Milestones
released in relation to an earlier
(H2024050133)
OIA request, which is already
available on the Ministry’s
website at:
www.health.govt.nz/system/file
s/2024-12/H2024055559-
response.pdf. Therefore,
section 18(d) of the Act applies.
Page 5 of 5
 Document 1
Briefing for information
An initial stocktake on neurodiversity work across government
Date due to MO:
Document 1
Briefing for information
An initial stocktake on neurodiversity work across government
Date due to MO: 30 April 2025
Action required by:
N/A
Security level:
IN CONFIDENCE
Reference:
H2025062730
To:
Hon Matt Doocey, Associate Minister of Health
Consulted:
Health New Zealand: ☐
ACT 1982
Proactive release: This
title is proposed by the Ministry of Health for proactive release: ☐
Contact for telephone discussion
Name
Position
Telephone
INFORMATION
Steve Barnes
Acting Deputy-Director General, Strategy,
s 9(2)(a)
Policy and Legislation
Caleb Johnstone
Acting Group Manager, Primary Care,
s 9(2)(a)
Family and Community Health Policy,
Strategy, Policy and Legislation
Minister’s office to complete:
☐ Noted
☐ Seen
☐ Needs change
☐ Withdrawn
☐ See Minister’s Notes
☐ Overtaken by events
Comment:
RELEASED UNDER THE OFFICIAL

IN CONFIDENCE
Document 1
Briefing for information
An initial stocktake on neurodiversity across Government
Security level:
IN CONFIDENCE
Date:
30 April 2025
To:
Hon Matt Doocey, Associate Minister of Health
Recommendations
1982
We recommend you:
a)
Note the attached
Neurodiversity Stocktake Report provides a current
Noted
ACT
baseline of Government agencies responses to neurodiversity including
challenges and gaps and work underway
b)
Agree for the Ministry of Health to socialise the report with Senior Officials
Yes/No
across agencies.
c)
Agree to the Ministry of Health progressing further policy work to understand
Yes/No
specific opportunities within your Associate Health portfolio.
INFORMATION
OFFICIAL
Caleb Johnstone
Hon Matt Doocey
Acting Group Manager
THE
Primary Care, Family and Community Health
Associate Minister of Health Policy,
Strategy, Policy, and Legislation
Date:
UNDER
Date: 29/04/2025
RELEASED
Briefing: H2025062730
IN CONFIDENCE
1
IN CONFIDENCE
Document 1
An initial stocktake on neurodiversity
across Government
Background
1.
In 2023, the Minister of Health listed neurodiversity as one of the Associate Health
portfolio responsibilities delegated to you. You then received advice from officials
providing a high-level overview of neurodiversity in the Government space
1982
(H2024036865 refers).
2.
Following the Young Neurodiversity Champions Hui at Parliament in July 2024 you also
asked the Ministry of Health to lead inter-agency coordination on neurodiversity w
ACT ith
the initial task being to undertake a stocktake to understand the current baseline of
neurodiversity activity within and across Government agencies to inform opportunities in
this area. This stocktake report has now been completed and is attached as
Appendix 1.
The Inter-Agency Neurodiversity Group
3.
The Inter-Agency Neurodiversity Group (IAG) was comprised of officials from Whaikaha,
Ministry of Health, Health New Zealand, Ministry of Education, Ministry of Social
INFORMATION
Development, Disability Support Services (which transferred from Whaikaha to MSD in
2024), Ministry for Children, and the Accident Compensation Corporation (which joined
the IAG in January 2025).
The Inter Agency Stocktake
OFFICIAL
4. The stocktake provides an initial assessment of activity underway across government
agencies. As noted, there is limited cross agency overlap in definition, data and service
THE
provision. From an initial assessment some of this variation could be well reasoned and we
would need to understand whether there would be benefit to neurodivergent people in
enabling greater alignment.
5. However, the stocktake has usefully identified an initial set of key themes that could be
UNDER
better understood through further work on policy or research and evidence. These include:
a. Government agencies define and respond to people with neurodiversity in different
ways according to their roles and responsibilities.
b. There are issues with assessments, services and supports, including long wait times
for initial assessments; service gaps; workforce pressures; and funding constraints.
RELEASED
c. There are barriers to identifying neurodiverse people in Government data systems to
better understand their needs and monitor outcomes.
d. There is growing awareness across Government agencies of the need to design and
deliver all aspects of their business with neurodiversity in mind.
Briefing: H2025062730
IN CONFIDENCE
2
IN CONFIDENCE
Document 1
6. To support an improved understanding of opportunities related to neurodiversity the
Ministry could undertake further policy work to identify specific opportunities in your
associate health portfolio. Subject to wider Ministerial agreement this could be expanded
across other portfolios.
7. As noted in the report participation from some agencies was limited due to their capacity in
needing to service other Government or Ministerial priorities. The Ministry could look to
engage with senior officials within these agencies to determine how further work could be
progressed.
Next steps
8.
With your agreement the Ministry of Health will:
1982
a. socialise this report at senior level across agencies.
b. progress further policy work to understand specific opportunities in your associate
ACT
health portfolio.
9.
Ministry of Health officials will update you via a weekly report item in July 2025.
10.
Officials are available to meet with you to discuss the stocktake. We can provide
additional information and advice at your request.
ENDS.
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Briefing: H2025062730
IN CONFIDENCE
3
Document 2
1982
ACT
Interagency Stocktake
report: how
government agencies
design and deliver
INFORMATION
supports and services
with neurodiversity in
OFFICIAL
mind
THE
UNDER
Ministry of Health
Strategy Policy and Legislation
Family, Communi
RELEASED ty and Primary Health Policy
Health of Disabled People Policy Team
2025
Document 2
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 2
Contents
Purpose
1
Context of neurodiversity – definitions, experiences and outcomes
1
About the stocktake
6
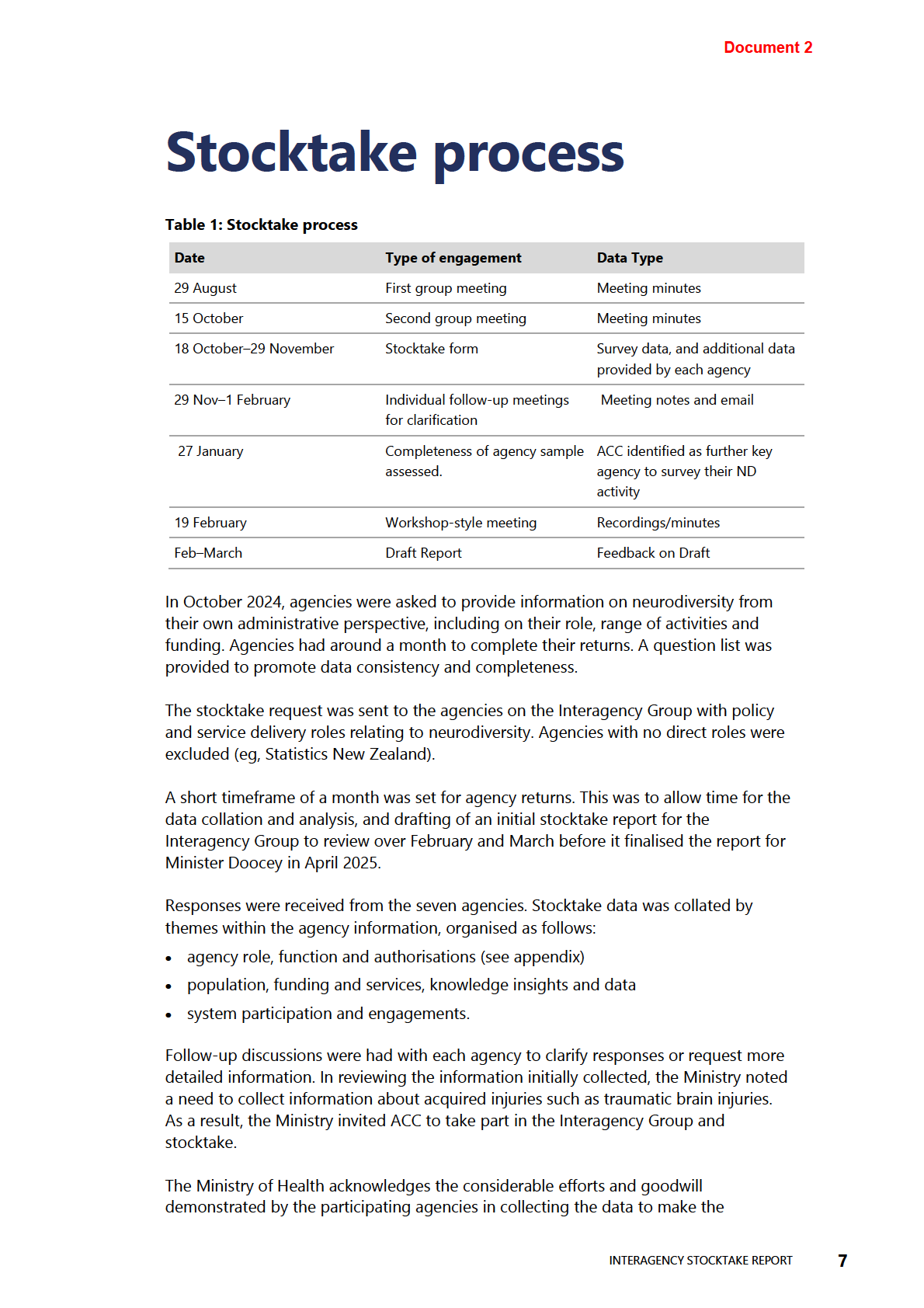
Stocktake process
7 1982
Limitations
9
ACT
Key themes
10
Roles and functions of agencies
11
Challenges and gaps
16
Work underway
21
INFORMATION
Opportunities and next steps
26
Appendix 1
27
OFFICIAL
List of Figures
THE
Figure 1: Some common neurodiversity types and associated attributes
3
List of Tables
UNDER
Table 1: Stocktake process
7
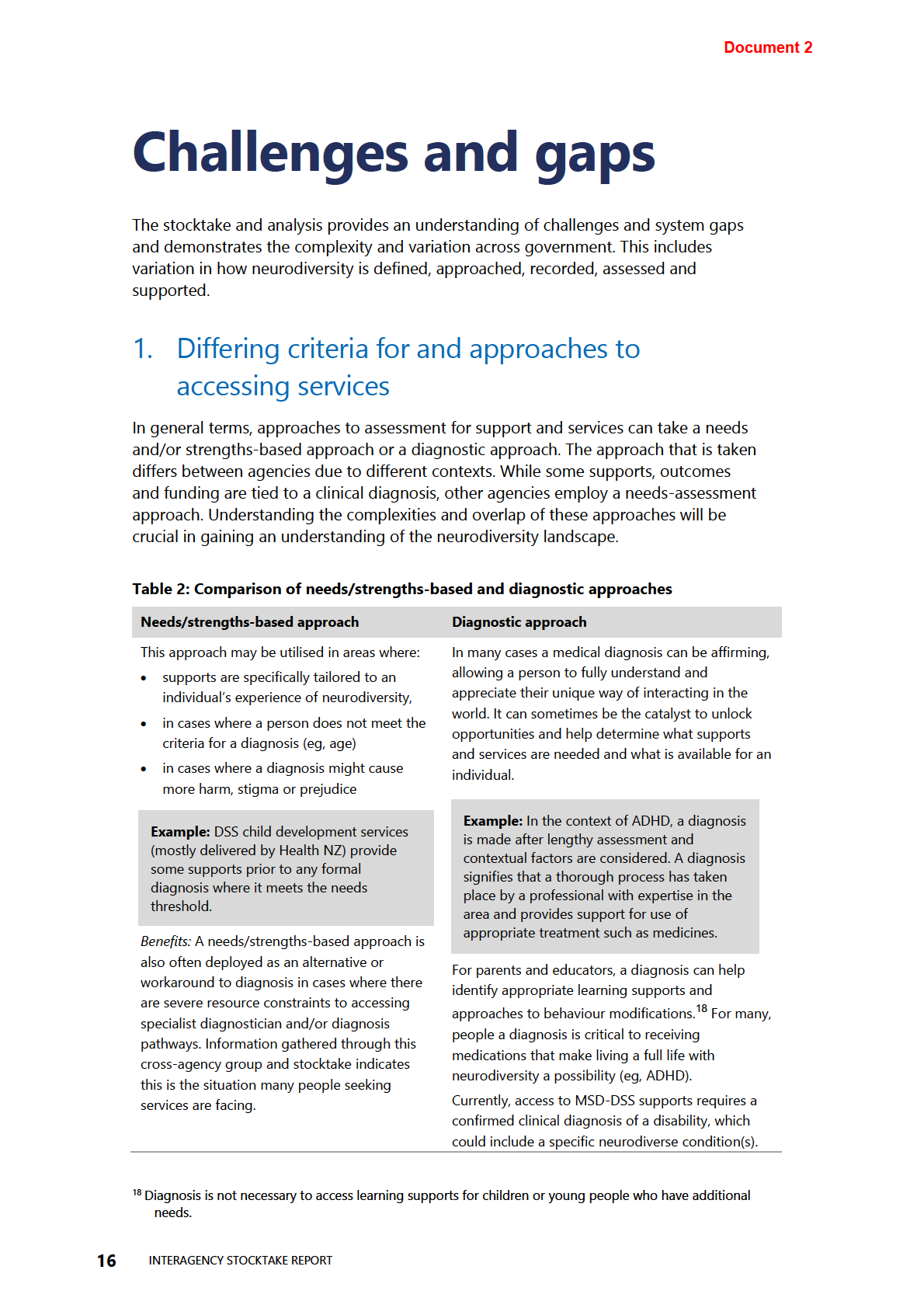
Table 2: Comparison of needs/strengths-based and diagnostic approaches
16
Table 3: Work underway addressing challenges and gaps
22
Table 4: Work underway, cross-sector actions by agency
24
Table 5: Neur
RELEASED odiversity Responsibilities (by Ministerial portfolio and government
agency, as at April 2025)
27
Table 6: Neurodiversity: working definitions by agency and role
29
INTERAGENCY STOCKTAKE REPORT
iii
Document 2
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 2
Purpose
This stocktake report provides a current baseline of neurodiversity activity within and
across government agencies. The stocktake aims to support:
• better understanding of government’s neurodiversity activity
• interagency coordination on neurodiversity
• information and advice to government on its neurodiversity work programme.
1982
The stocktake shows that while there is a wide range of work across government
agencies (see Tables 1 and 3), there could be better coordination amongst agencies to
ACT
align neurodiversity work programmes. Better coordination between work programmes
could result in greater efficiencies and better outcomes for people who are
neurodiverse.
In order to make better sense of the neurodiversity landscape, the Interagency group
also participated in discussions on the multiple definitions of neurodiversity and aimed
to understand the experiences and needs of neurodiverse people and their
communities, including within Aotearoa. Developing a shared understanding of
INFORMATION
neurodivergent experiences and concepts built an important foundation from which
the interagency group could then understand each agency’s work in this area.
Context of neurodiver
OFFICIAL sity –
definitions, experiences and
THE
outcomes
Neurodiversity is a term often used to refer to the natural variability in how peoples’
UNDER
brains engage in learning, perceive information, organise, communicate and relate with
others. It encompasses people from al walks of life, is commonly intersectional in
nature, and not limited to individuals of specific age, gender or ethnicity.
Neurodivergent and
neurodivergence
Since the term neurodiverse was first coined in the
are somewhat recent and emerging
late 1990s, different approaches have emerged to
concepts. Rather than a clinical
RELEASED
understand neurological differences, including as a
diagnosis, these terms are used as
natural variation in human cognitive functioning,
an umbrella term to describe a
medical condition or disability. Both
neurodivergent
person who has neurological
and
neurodiversity are terms based on a human
variances as compared to a
rights approach to disability, and not unlike the
neurotypical person, a person whose
term
ethnic diversity. They aim to acknowledge that
neurological development and
differences, chal enges and uniqueness in human
functioning aligns with the majority
neurology are natural variations.
of people.
INTERAGENCY STOCKTAKE REPORT
1
Document 2
Conceptually, there are overlapping concepts of neurodiversity and disability, which is
defined in the convention on the Rights of Persons with Disabilities (UNCRPD) as
resulting from the interaction between persons with impairments and the attitudinal
and environmental barriers that hinder their full and effective participation in society
on an equal basis with others. In line with the UNRCPD, the New Zealand Disability
Strategy is inclusive of all disabled people, including people with neurodevelopmental
conditions. Some people consider neurodivergence disabling, identifying themselves
as part of the disability community, whilst others do not. Neurodivergence is often
invisible, making its identification or diagnosis harder. A lack of awareness about this
kind of diversity can result in misunderstanding people’s unique requirements.1
There is no clinical assessment or diagnosis for neurodivergence/neurodiversity,
1982
instead these terms are used informal y and loosely as umbrella terms to describe the
shared experiences of people with a range of conditions, experiences, and diagnoses.
ACT
Today, it is accepted that neurodivergent conditions include a range of specific
presentations including:
• neurodevelopmental2 conditions such as autism spectrum disorder (ASD), attention
deficit hyperactivity disorder (ADHD), fetal alcohol spectrum disorder (FASD),
dyspraxia/DCD and learning disabilities including dyslexia or dyscalculia
• acquired3 neurodiverse mental health conditions (such as PTSD, anxiety and
depression), traumatic brain injury (TBI), dementia, Alzheimer’s and neurological
effects resulting from stroke
INFORMATION
• neurologic variations that are not clearly diagnosable including children who have
not yet reached the age where a clinical diagnosis is possible or where diagnosis is
indeterminate, unwanted or considered unwarranted.
There is variation in definitions of neurodivergence and/or neurodiversity, with some
OFFICIAL
including epilepsy and acquired neurodiverse mental health conditions, and others not.
In addition, this report recognises that:
THE
• people can, and often do have more than one neurodiverse condition or other
disability
• neurodivergent people are more likely than neurotypical people to also experience
acquired neurodiverse ment
UNDER al health condition(s) such as obsessive-compulsive
disorder (OCD), anxiety or depression4, 5
• mental health conditions can be exacerbated by a person not knowing they are
neurodivergent and/or not having access to the type of supports6 they require
RELEASED
1 See
https://www2.deloitte.com/us/en/insights/topics/talent/neurodiversity-in-the-workplace.html.
2 Those conditions that arise as the brain is developing.
3 Changes in a person’s brain functioning following an injury, disease or health condition.
4 French, B., et al. 2024. “The impacts associated with having ADHD: an umbrella review.” Frontiers in
Psychiatry 15.DOI.
https://www.frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2024.1343314
5 Zhang, S., et al. 2020. “Neuropsychiatric issues after stroke: Clinical significance and therapeutic
implications.” World J Psychiatry 10(6): 125–138.DOI.
6 This experience can be exacerbated in the context of additional health or disability needs and it is often
the complexity of managing both that results in higher levels of support need.
2
INTERAGENCY STOCKTAKE REPORT
 Document 2
Document 2
• people with disabilities who are neurodivergent can have difficulties accessing
mental health support due to their symptoms being attributed solely to
neurodiversity
• many adults learn of their neurodiversity after first seeking help for a mental health
concern.
1982
ACT
INFORMATION
OFFICIAL
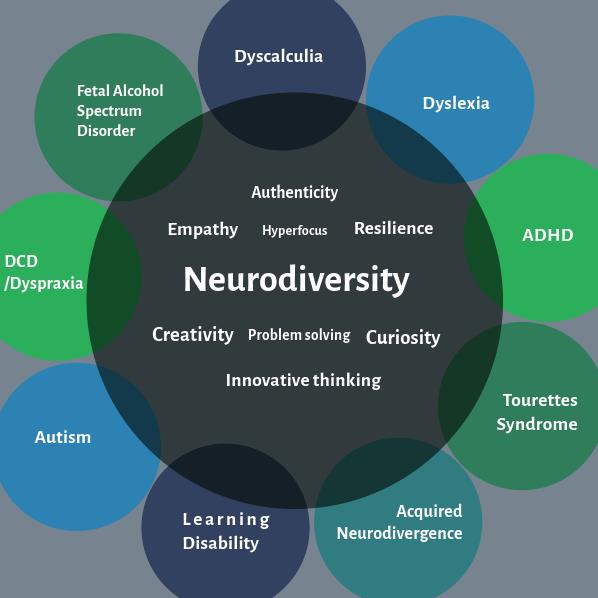
Figure 1: Some common neurodiversity types and associated attributes
THE
Neurodivergent people have diverse experiences and may find that their
neurodivergence impacts them differently in different contexts or at specific stages in
their life course such as entering early childhood education, leaving school or starting a
new job. Many people wil live full and active lives while others wil be disabled by a
neurodiverse condition, re
UNDER quiring high levels of assistance and medical intervention.
For example, an autistic person may be non-speaking and have difficulty expressing
need, require a carer or support worker in daily life and a dedicated learning
environment. Another autistic person may be able to communicate well verbally but
might find deciphering social cues difficult or find change difficult. Both may benefit
from support, but the required levels and type of support vary greatly and are
individual and unique to each person and stage of life.
RELEASED
Neurodivergent people sometimes describe the positive attributes of their condition as
allowing periods of extended concentration, high levels of empathy, curiosity, creativity
and strategic problem solving. In Aotearoa, mirroring the wider disability movement,
there is an emerging human-rights, strengths-based, mana-enhancing lens on
neurodiversity.7
7
https://gazette.education.govt.nz/articles/takiwatanga-in-your-own-time-and-space
INTERAGENCY STOCKTAKE REPORT
3
Document 2
For the Neurodivergent population, outcomes vary greatly. From global data, we know
that on the whole, Neurodivergent people experience worse health, disability,
education8 and justice outcomes than neurotypical individuals.9 For example, people
with FASD have a life expectancy of 34 years, with 44% of deaths from external causes
including suicide and accidents.10 Research by Deloitte showed the total social and
economic costs of ADHD in Australia in 2019 were estimated to be $20.42 billion, or
$25,071 per person (this figure includes education, justice, productivity costs and loss
of wellbeing costs).11 Outcomes reach across many aspects of society, therefore calling
for a cross-government approach looking for opportunities for targeted policy
interventions.
1982
Neurodiversity in Aotearoa
Figures and data that encompass the entire neurodiversity umbrella are not available,
ACT
however there are pockets of information that help us begin to understand the
landscape within New Zealand.
ASD and ADHD rates are trending higher. Reasons for this are multifactorial and likely
include better awareness and earlier diagnosis.
Studies indicate that children and young people from more deprived families are
between 1.5–4 times more likely to have ADHD than children and young people from
INFORMATION
less deprived families.12 In one New Zealand study, 2.8% of Māori and 1.6% of non-
Māori were screened as showing ADHD concerns.13
• Research also indicates the prevalence of FASD to be between 1.1% and 3.9% of the
general population and 1.7% and 6.3% for Māori, however, diagnostic barriers make
this difficult to ascertain.14
OFFICIAL
• New Zealand Statistics Survey data shows that 2% of New Zealanders aged five
years and over have been diagnosed with autism and that 3% of people aged five
years and over have been diagnosed
THE with ADHD.15
• 40% of disability supports in New Zealand are for people with autism
UNDER
8
https://gazette.education.govt.nz/articles/takiwatanga-in-your-own-time-and-space/ 9 French, B., et al. 2024. "The impacts associated with having ADHD: an umbrella review." Frontiers in
Psychiatry 15.DOI.
https://www.frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2024.1343314.
10 Thanh, N., & Jonsson, E. 2016. Life Expectancy of People with Fetal Alcohol Syndrome
https://pubmed.ncbi.nlm.nih.gov/26962962/
11 The social and economic cost of ADHD in Australia. 2019. Deloitte:
https://www.deloitte.com/au/en/services/economics/perspectives/social-economic-costs-
RELEASED
adhd-Australia.html
12 Sayal, K., Prasad, V., Daley, D., Ford, T., & Coghill, D. 2018. ADHD in children and young people:
prevalence, care pathways, and service provision. The Lancet Psychiatry, 5(2), 175–186.
https://doi.org/10.1016/S2215- 0366(17)30167-0
13 Cargo, T., Stevenson, K., Bowden, N., Milne, B., Hetrick, S., & D'Souza, S. 2022. Medication dispensing
among Māori and non-Māori screened for preschool ADHD. The New Zealand medical
journal, 135(1565), 95–103.
https://doi.org/10.26635/6965.5862
14 Foetal alcohol spectrum disorder in Aotearoa, New Zealand: Estimates of prevalence and indications of
inequity. Romeo 2023. Drug and Alcohol Review – Wiley Online Library.
15
https://www.whaikaha.govt.nz/news/news/17-percent-of-new-zealanders-are-disabled#scroll-to-4
4
INTERAGENCY STOCKTAKE REPORT
Document 2
• 2023/24 New Zealand Health Survey data shows that ADHD and Autism Spectrum
Disorder are relatively common conditions among children and young people (0–15
years). 12
There has been previous work, both within agencies and at an inter-agency level, which
intersects with parts of the neurodivergent population or elements of the neurodiverse
experience.16. This historic context may provide valuable insights to support the
Government’s provision of support for the neurodivergent population. However, as this
report is focused on current and planned work, historic work was deemed out of scope.
Although data on neurodivergent learners is not currently available, a high proportion
of disabled learners wil be neurodivergent, therefore the statistics below are included
1982
to provide an understanding of how neurodivergent students might experience the
education system in New Zealand.
ACT
• Disabled learners are between 1.5 and 3 times more likely to be stood down,
suspended, move schools frequently and they are more likely to end up in statutory
care.
• Disabled learners experience higher rates of bullying and physical restraints than
their non-disabled peers.
• Disabled learners are half as likely to attain NCEA Level 3 and more than twice as
likely to attain no qualification at school.
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
16
https://www.whaikaha.govt.nz/about-us/programmes-strategies-and-studies/guidelines/nz-
autism-guideline
INTERAGENCY STOCKTAKE REPORT
5
Document 2
About the stocktake
There has been recent and growing interest in and focus on neurodiversity within
government. This has included the Minister of Health listing neurodiversity as one of
the Associate Health portfolio responsibilities in 2023, and the Associate Health
Minister speaking at a Young Neurodiversity Champions Hui at Parliament on Friday 19
July 2024
. The neurodiverse sector has noted that government agencies’ siloed
responses to neurodiversity can create barriers and has called for government
approaches and activities on neurodiversity to be more joined up. The sector has also
1982
called for a greater focus on early identification, intervention and support for
neurodiverse people.
ACT
The Associate Minister of Health requested the Ministry of Health establish and
coordinate a new interagency group on neurodiversity consisting of key government
agencies with responsibilities for neurodiversity.
As this is a new group and initiative, the initial key task of the interagency group was to
do a stocktake to build a shared understand of the landscape of existing government-
funded responsibilities and activity on neurodiversity. Findings would identify and
inform further scoping and prioritisation of strategic, whole-of-government actions on
INFORMATION
neurodiversity.
OFFICIAL
THE
UNDER
RELEASED
6
INTERAGENCY STOCKTAKE REPORT
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 2
stocktake possible, especially given the short timeframes. That said, the ability of
agencies to provide information varied based on their systems and available
administrative data, as well as their capacity to dedicate resources to participating in
the stocktake. Some administrative data therefore differed in terms of coverage,
completeness, consistency and granularity. For example, agencies generally do not
have an agreed definition of neurodiversity to guide their work. This variability is
expected as neurodiversity is a new ministerial portfolio and a relatively new and
emerging concept in the New Zealand government sector.
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
8
INTERAGENCY STOCKTAKE REPORT
Document 2
Limitations
The stocktake was limited in its ability to assess the full extent to which neurodiversity
activity cuts across different government systems, including health, education, disability,
injury, children’s care and justice.
Neurodiversity is a relatively recent concept, and, for the purposes of this report, this
umbrella term can encompass a number of clinically defined conditions and, for some
agencies, anyone who self-identifies as neurodiverse and/or neurodivergent. The way
1982
in which neurodiversity is understood and defined varies. Given the variation in how
the term neurodiversity is understood and defined, and that there are different ways of
ACT
defining needs and col ecting data, there wil be limitations to getting a clear picture of
the range of complexities that people face, and when considering the scope of
government services that exist and/or are needed.
Combined with aspects of diagnostic reluctance, access issues, differing definitions of
need and differing data col ection methods, we begin to see a picture of the
complexities faced when seeking to understand the landscape of neurodiversity as a
whole across government.
INFORMATION
Some agencies within the group have not been able to fully participate in the stocktake
exercise due to internal resourcing constraints and pressures from change processes.
In compiling insights on neurodiversity across government, it is evident that there are
data limitations. This is not only due to a dearth of New Zealand neurodiversity and
OFFICIAL
overall disability data, but also to complicating factors which include the definition and
scoping for neurodiversity.
THE
Therefore, this stocktake summarises the information we had access to but may not
reflect the full scope of unmet needs or work underway to meet these needs.
UNDER
RELEASED
INTERAGENCY STOCKTAKE REPORT
9
Document 2
Key themes
Through discussion, stocktake activities and report co-development a number of key
themes emerged:
• Government agencies define and respond to people with neurodiversity in different
ways according to their roles and responsibilities.
• There are issues with assessments, services and supports, including long wait times
for initial assessments; service gaps; workforce pressures and funding constraints.
1982
• There are barriers to identifying neurodiverse people in government data systems
to better understand their needs and monitor outcomes.
ACT
• There is growing awareness across government agencies of the need to design and
deliver all aspects of their business with neurodiversity in mind.
• There is some appetite for a coordinated cross-agency programme of government
action on neurodiversity.
This section presents the stocktake findings of current approaches to neurodiversity
across seven key agencies. It provides an initial analysis of similarities and differences in
government agencies’ responses to neurodiversity, including how neurodivergent
INFORMATION
people are identified, assessed and supported, and the corresponding data and
information available. Fol owing this, the report discusses emerging challenges and
gaps and looks at an overview of actions in progress that are addressing some of
these.
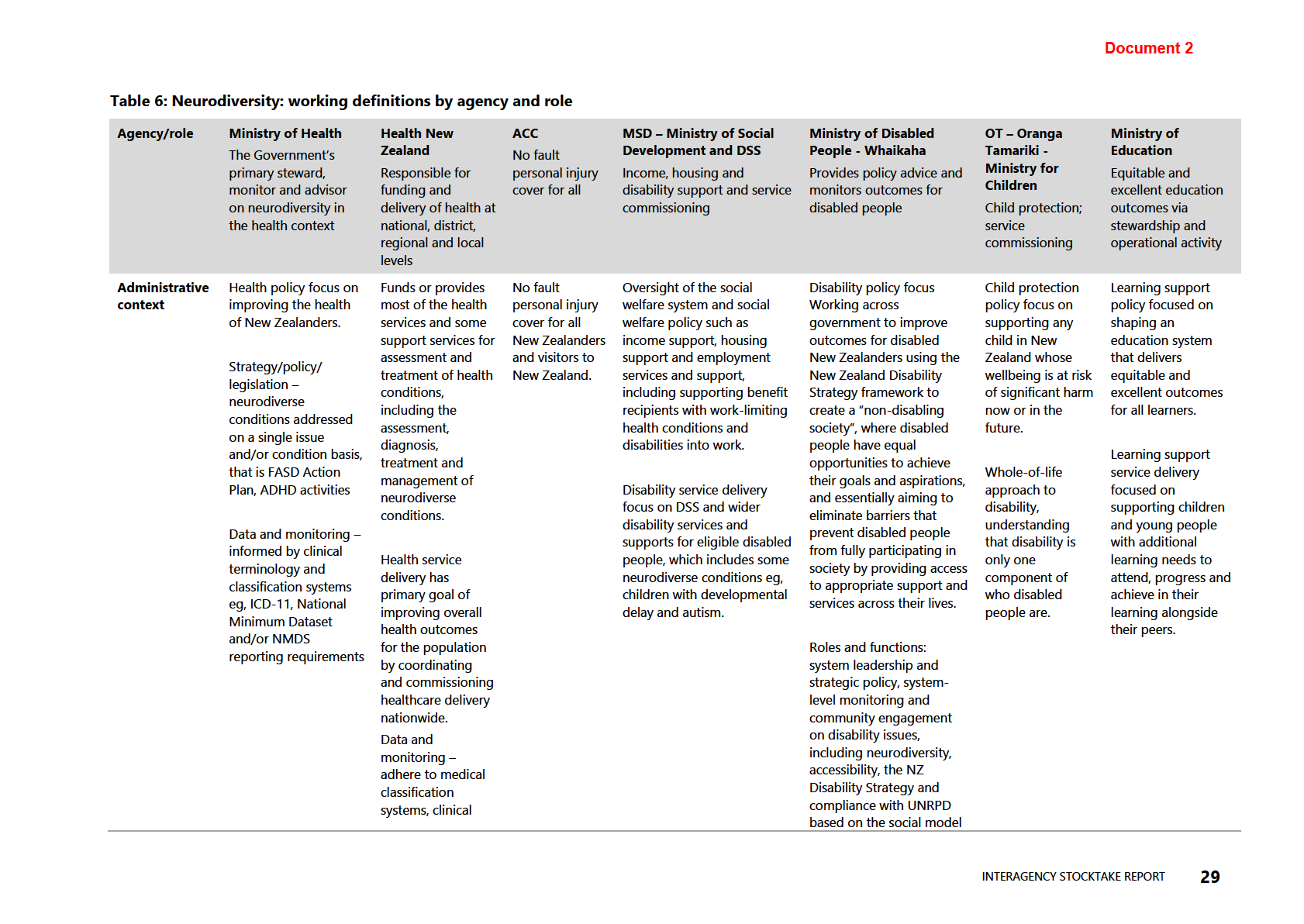
The stocktake asked agencies about their roles and responsibilities on neurodiversity.
OFFICIAL
In summary, the responses confirmed agencies have different roles and responsibilities
on neurodiversity which have led to different definitions and understandings of
THE
neurodiversity within their agency mandates, thus resulting in different approaches,
responses and service delivery. The information in Table 5 (see appendix) demonstrates
the variations in working definitions for neurodiversity, how each agency interfaces
with aspects of neurodiversity and neurodivergent people, and what, if any, funding
and services are allocated.
UNDER
RELEASED
10
INTERAGENCY STOCKTAKE REPORT
Document 2
Roles and functions of
agencies
Government agencies who are involved in this stocktake were identified as being
critical to gaining an understanding of the neurodiversity landscape. When considering
each agency’s role and function, it is important to note that people may access services
1982
from one or more agency at the same time, and needs can vary across a person’s life
course (see example below). In addition, many agencies not only work across
government, but they contract with community and NGO providers to deliver supports.
ACT
This level of detail was outside the scope of this stocktake.
Understanding of the varied philosophical underpinnings help us to conceptualise the
approaches to neurodiversity that have been taken when shaping strategies and
policies. Although across government there are varied working definitions of
neurodiversity, this is not necessarily a barrier, nor is it required to move forward with
some actionable steps.
INFORMATION
Example: A neurodivergent individual may receive day-to-day personal and
mental health support from their GP in the health system, have received support
through the benefit system in their lifetime while they could not work due to
mental health and neurodivergence impacts, and, as a child, may have had
learning support in the education system such as a teacher aide. This individual
OFFICIAL
may have been supported by ACC when they were younger due to a childhood
accident (eg, a TBI), and, as an adult, may have explored and privately funded a
THE
diagnostic process (eg, autism spectrum disorder).
Whaikaha
UNDER
The Ministry for Disabled people provides:
Approach to neurodiversity
• interagency policy advice and information
Whaikaha approaches
about disability.
neurodiversity by considering both
• advises the Minister for Disability.
people who self-identify as
RELEASED
•
neurodiverse and those who have
monitors the size, characteristics and
outcomes of disability population groups
been diagnosed with a
including the neurodiverse population; and
neurodivergent condition.
• holds and attends disability sector
engagements, meetings and community engagement including with groups that
have neurodiverse memberships.
INTERAGENCY STOCKTAKE REPORT
11
Document 2
Ministry of Health – Manatū Hauora
The health sector has a central role in the Government’s response to those with
neurodiverse conditions. The Ministry of Health is the Government’s primary steward
and advisor on neurodiversity in the health context. We monitor the overall
performance of Health New Zealand in meeting the health needs of disabled people
including FASD and possible FASD, and ADHD.
Work programmes and
Approach to neurodiversity
initiatives related to
neurodiversity are delivered
The Ministry of Health, as Crown monitor, has
1982
through the Health of Disabled
historically seen neurodiversity as an umbrella
People Policy Team, the
term in which a col ection of clinically diagnosed
Mental Health and Addiction
conditions fall. The majority of our resources and
ACT
Programme, the Public Health
work are currently in relation to ADHD and FASD
Agency and Med Safe.
through a public health and mental health lens,
with a focus on advice, regulation and monitoring.
Relevant work the Ministry of
In our stewardship function, however, we
Health leads focuses on ADHD,
recognise the wide variability of neurodivergent
FASD and leading a cross-
people and the intersectionality between disability
agency group to coordinate
and mental health and wellbeing.
the Government’s
INFORMATION
neurodiversity work programmes.
Health New Zealand (Health NZ) | Te Whatu Ora
Health NZ funds most of the health services and some support services for
OFFICIAL
neurodiversity in the health context. It leads the day-to-day management and running
of the health system across Aotearoa, with functions delivered at local, district, regional
and national levels. Health NZ is responsible for improving services and outcomes
THE
across the health system including upholding Te Tiriti o Waitangi.
Disabled people are recognised as a priority
Approach to neurodiversity
population in the Interim NZ Health Plan - Te
UNDER
Pae Tata, which includes actions to improve
Health New Zealand includes
access, inclusion and equity for disabled
neurodivergence within its
people in the delivery of healthcare services.
broader definition of disability and
recognises the intersectionality of
The Disability Health function is responsible
this group with other disability
for providing strategic advice and alignment
groups and priority populations.
on applying disability equity across all business
RELEASED
units, services and workstreams, and leads the planning, development and
implementation of disability actions, initiatives and workstreams. It engages,
col aborates and provides advice on disability in health.
Work underway across Health New Zealand - Te Whatu Ora can broadly be
categorised into two areas of focus:
• pathways and activities that relate directly to the assessment, diagnosis, treatment
and management of neurodivergent conditions.
12
INTERAGENCY STOCKTAKE REPORT
Document 2
• pathways and activities that relate to improving access, experiences and outcomes
for neurodivergent people and whānau seeking healthcare, in general.
Ministry of Education Te Tāhuhu o te Mātauranga
(MoE)
MoE is responsible for shaping an education system that delivers equitable and
excellent outcomes through two distinct roles:
• stewardship-focused – on policy and performance of the education system and
1982
• operations-focused – on delivery of services and supports nationally, regional y and
locally, delivered though Te Mahau, a business unit within the Ministry.
ACT
Te Mahau supports,
advises, leads, funds and
Approach to neurodiversity
regulates schools and
The Ministry of Education takes an inclusive approach
early learning services.
to neurodiversity: “Students learn best when they have
The largest operational
a strong sense of belonging and feel valued and
function of Te Mahau is to
supported. Awareness that students vary in their
provide learning support
strengths and needs helps teachers create welcoming,
for children with
responsive and inclusive environments that nurture
disabilities, learning
students’ learning, identities, languages and cultures.
INFORMATION
difficulties, and physical
Because students engage with learning, process
or mental health issues.
information and demonstrate knowledge in diverse
ways, teachers design experiences that al ow students
Learning Support is part
to participate in a range of ways. Inclusive frameworks
of everyday teaching and
like Te Tūāpapa o He Pikorua, integrate flexible
OFFICIAL
learning. MoE provides
supports into day-to-day teaching and learning. They
learning supports and
enable teachers to create environments that
services a Learning
acknowledge and address the needs and strengths of
THE
Support Service (LSS)
all students. Explicitly teaching essential knowledge and
from birth to 21 years of
skills and addressing barriers to learning provides
age. Services are
equitable access to language and literacy learning.”
delivered by a range of
UNDER
practitioners including early intervention teachers, speech language therapists,
psychologists, Advisors on Deaf Children, and kaitakawaenga.
RELEASED
INTERAGENCY STOCKTAKE REPORT
13
Document 2
Ministry of Social Development (MSD)
MSD performs a mix of advisory,
service delivery, regulatory,
Approach to neurodiversity
purchasing, funding and
MSD provides a range of supports and services to
commissioning roles. It is
neurodiverse populations, including income
responsible for the oversight of
support, employment and training services, and
New Zealand’s social welfare
housing. Neurodiverse people are likely to engage
system. Key functions include:
across all MSD services and supports depending on
•
their individual needs and work capacity barriers,
policy and investment advice
1982
and meeting specific eligibility criteria such as
• income support
income, relationship status, age, residency and
• employment services and
work capacity. Generally, though not exclusively,
ACT
support
tailored supports and services for neurodiverse
• housing support
people are related to MSD’s mandate to support
disabled people and people with health conditions.
• communities and partnership
MSD also provides support for people whose work
• agreements to commission,
capacity is impacted by a health condition or
fund and contract social
disability, which may include neurodiversity.
service providers.
INFORMATION
Disability Support Services (business unit within
Ministry of Social Development)
In December 2024, responsibility for administration of disability support service
funding transferred from the Ministry of Disabled People – Whaikaha to the Ministry of
OFFICIAL
Social Development. Disability Support Services (DSS) is now a branded business unit
within the Ministry of Social Development. As the transfer of DSS from Whaikaha to
MSD happened so recently, this report
THE wil examine DSS separately from MSD, to
reflect the different approaches and
actions taken by each.
Approach to neurodiversity
DSS provides a range of supports and services
DSS is responsible for providing
UNDER
to neurodiverse populations, where they meet
essential support to around 50,000
DSS eligibility criteria. Generally, people are
disabled people and their whānau, as
eligible for disability support funded by DSS if
well as equipment and modification
they have a long-term intellectual, physical or
services for approximately 100,000
sensory disability, including autism, that arises
New Zealanders.
before they turn 65 and which lasts longer
than six months and requires ongoing
RELEASED
Examples of supports include:
support to live independently. Disabled
• help around the home and with
people with neurodivergent conditions other
personal care
than autism may be eligible for DSS if they
•
also have an eligible condition. Young people
respite for carers
with autism are a significant cohort of the DSS
• equipment and aids
population. DSS has played a central role in
• child development services
the development of the autism guidelines.
including assessments, therapies
and assistance navigating supports across agencies
14
INTERAGENCY STOCKTAKE REPORT
Document 2
• behavioural supports
• residential care17
• autism-specific supports including parent education, behavioural support services,
development services and support-coordination.
Oranga Tamariki Ministry for Children (OT)
OT is the statutory child protection agency
which includes children in care, youth justice and
Approach to neurodiversity
adoption. It holds statutory powers for all child
Neurodiversity is included within
1982
and youth through the Oranga Tamariki Act. OT
Oranga Tamariki’s definition of
also commissions services for children and
disability and is a consideration
whānau. Although there are no specific functions
as part of the wider context of
ACT
related to neurodiversity, most of the work
disability when developing or
within OT that involves neurodiversity is across
changing policy, process and
disability as a larger cohort. A significant number
practice to better meet the
of tamariki and whānau who engage with OT are
needs of this cohort.
neurodiverse.
Accident Compensation Corporation (ACC)
INFORMATION
ACC undertakes a mix of purchasing, funding
and commissioning functions to provide injury
Approach to neurodiversity
cover and rehabilitation services for its clients, as
The Accident Compensation Act
well as injury prevention initiatives. There are a
2001 (the Act) does not
range of services available to clients depending
differentiate between different
OFFICIAL
on their specific injury-related needs.
groups including those who are
neurodiverse. However, ACC
The Accident Compensation Act 2001 (the Act)
considers all claims on a case-
THE
provides the legal framework for no fault
by-case basis including the
personal injury cover to all New Zealanders (and
background and circumstances
visitors to New Zealand). There are no specific
of an individual seeking cover for
powers under the Act that relate to
an injury.
UNDER
neurodiversity as all New Zealanders (and
visitors to New Zealand) who are entitled to cover under the Act wil receive it.
RELEASED
17 People who also have autism may receive residential care when needed to meet their other disability
related needs.
INTERAGENCY STOCKTAKE REPORT
15
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
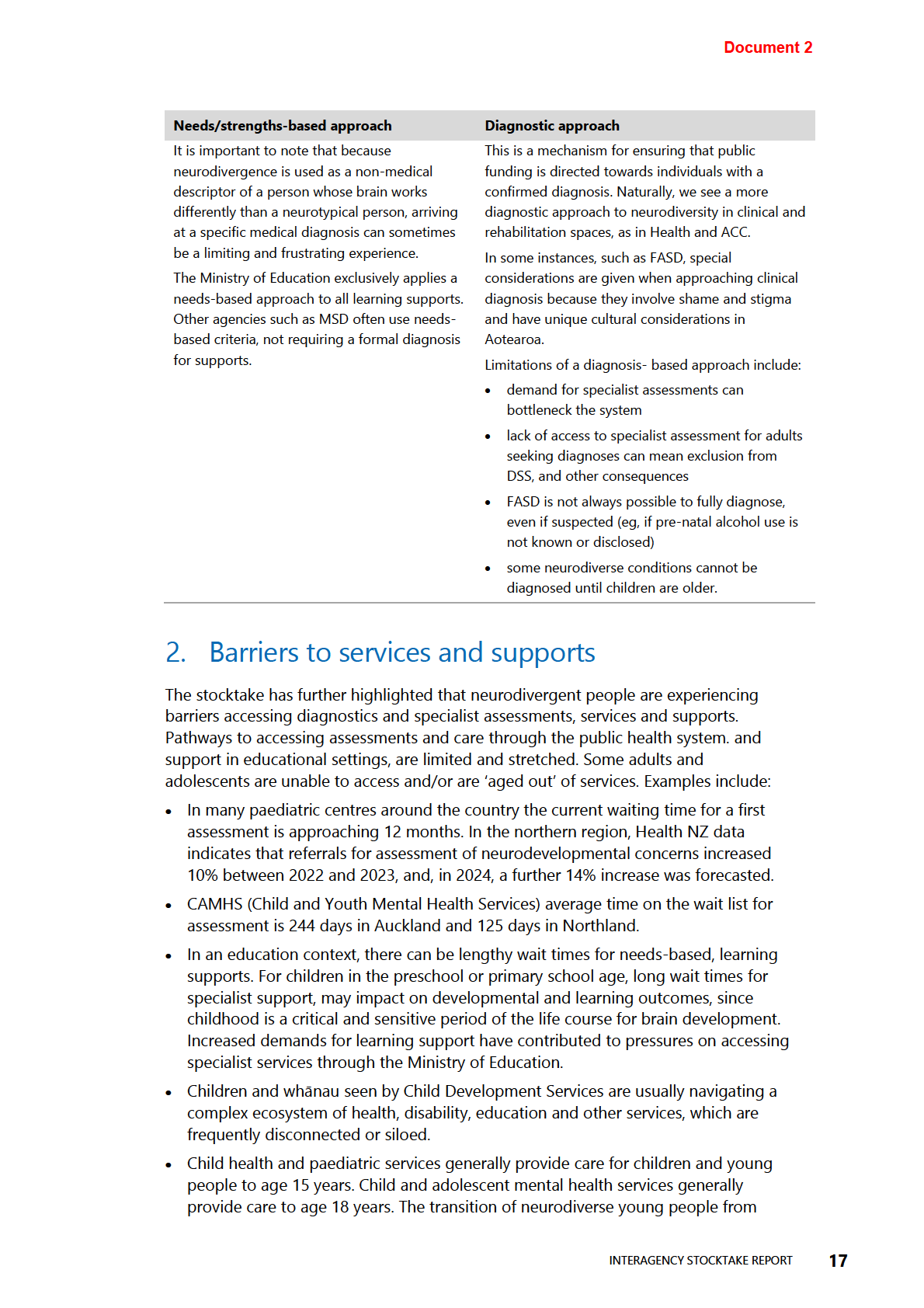
Document 2
child health to adult health services can be stressful for the young person and their
families, and gaps in care can arise due to differing acceptance criteria between
child health and adult health services. This can lead to neurodiverse young people
not having access to psychiatric or clinical specialist care in certain circumstances.19
• Adults with a diagnosis of autism are being declined access to adult mental health
and addiction services despite many having co-occurring mental health conditions.
• For adults seeking diagnoses for autism spectrum or ADHD, there are extremely
limited pathways for assessment within the public health system. Cost and access to
private specialists are known issues, with greatest impact facing populations with
the fewest resources.
1982
• There are also limited pathways to psychiatric and/or clinical specialist care for
adults who have transitioned out of child health services, even for individuals who
are prescribed psychotropic and stimulant medications and/or have co-occurring
ACT
mental health conditions. These individuals may be managed by primary care
providers without easy access to psychiatric or clinical specialist input.
• Presently, there is no publicly funded Health NZ pathway for adults seeking a
diagnosis of autism or for adults with an existing autism diagnosis seeking clinical
care and psychiatric oversight for psychotropic and stimulant medications. Cost and
access to private specialists are known issues, with greatest impact facing
populations with fewest resources.
• Difficulties accessing diagnostic assessments mean that prevalence data can
INFORMATION
underestimate the reported numbers of neurodiverse people who would benefit
from additional supports or services.
3. Pressure on services and pathways
OFFICIAL
Agencies are reporting both increased volume and increased complexity of caseloads
as they pertain to neurodiversity. As recognition of neurodiversity increases, a greater
number of people are seeking diagnos
THE is and support. The barriers for those seeking
assessment, and therefore supports, are further constrained by system and workforce
pressures in both the health and education sectors. Agencies also report variability in
accessibility to supports due to location and workforce expertise spread un-equally
across regions.
UNDER
Examples of this include:
• funding and resource constraints not meeting current requirements, while levels of
need increasing and predicted to increase
• variability in access to services based on location, particularly rural
RELEASED
• funding constraints on programmes
• specialist workforce shortages
• skills development needs.
19
https://bmjopen.bmj.com/content/bmjopen/12/11/e065138.full.pdf
18
INTERAGENCY STOCKTAKE REPORT
Document 2
4. Gaps in data
It is generally accepted that there is a need for better disability data in New Zealand.
There are projects underway across government to address this gap and explore the
wider issues of design, col ection and ownership.
In terms of neurodiversity data, there is wide agreement that there is not enough. This
requires inferences and extrapolations to be made from both wider disability data and
more limited, and condition-specific data sets.
Examples of this include:
1982
• Ministry of Health col ects survey data on neurodiversity prevalence. However, for
the time period up to and including 2023, this data only captures children and only
considers two of the clinically diagnosed conditions (ADHD and ASD) which fall
ACT
under the wider neurodiversity umbrella.
• Ministry of Education holds data on learning supports accessed, however these data
sets give service-based insights, rather than condition-based.
• Ministry of Social Development and Whaikaha hold data on specific clinical
diagnosis, much of this on autism.
• Oranga Tamariki hold some data on disabled children in its care, but not on specific
types of disability or on neurodiversity as a whole.
INFORMATION
• Health New Zealand Paediatric Medicine and Child and Adolescent Mental Health
Services (CAMHS) col ect specific data for neurodevelopmental presentations in
children and young people in some districts, however these data col ection practices
vary by district, making it difficult to build a picture of national demand.
• ACC hold data on TBI supports, but do not col ect data on neurodivergent
OFFICIAL
customers or in relation to their experiences with the ACC system.
• There are opportunities to better utilise available data within the IDI to paint a
THE
picture of disability needs and access of government services over time. The IDI
represents an opportunity for better disability data insights.
• Analyses using the IDI contain limitations, including that the population group with
neurodiverse needs must be inferred since it is not consistently captured in
UNDER
diagnostic data (or diagnostic data is simply not recorded) and data is based upon
individual’s interactions with government services.
• Absence of data means that neurodivergent Pacific individuals are either
misdiagnosed, underdiagnosed or left unsupported entirely. This not only impacts
individual and whānau (family) wellbeing but also has long-term consequences for
education, employment, mental health and overall quality of life. 20, 21, 22
RELEASED
20 Nafatali, R. 2023.
E lē Ma’i, o le Malosi!” (He’s not Sick, He’s Strong!): Pacific Parents’ Journey of Raising
Autistic Children in Aotearoa, Massey University. Auckland, New Zealand.
21 Rangiwai. 2024. Flighty like the pīwakawaka!: personal reflections on mid-life ADHD diagnosis and the
beginnings of a framework for conceptualising the condition from a Māori perspective.
AlterNative: An
International Journal of Indigenous Peoples,
20(3), 360–369.
https://doi.org/10.1177/11771801241250058
22 Roy, R., Greaves, L. M., Peiris-John, R., Clark, T., Fenaughty, J., Sutcliffe, K., Barnett, D., Hawthorne, V., Tiatia-
Seath, J., & Fleming, T. 2021.
Negotiating Multiple Identities: Intersecting Identities among Māori, Pacific,
INTERAGENCY STOCKTAKE REPORT
19
Document 2
In addition, it is important to note that the neurodiverse population may always be
underrepresented in the data because of limitations around existing data, including but
not limited to:
• system delays (and denials of service)
• financial constraints
• cultural stigma and systemic racism
• reluctance to attend assessments and screenings.
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Rainbow and Disabled Young People (Youth2000 Series), The Youth19 Research Group, The University of
Auckland and Victoria University of Wellington, New Zealand.
20
INTERAGENCY STOCKTAKE REPORT
Document 2
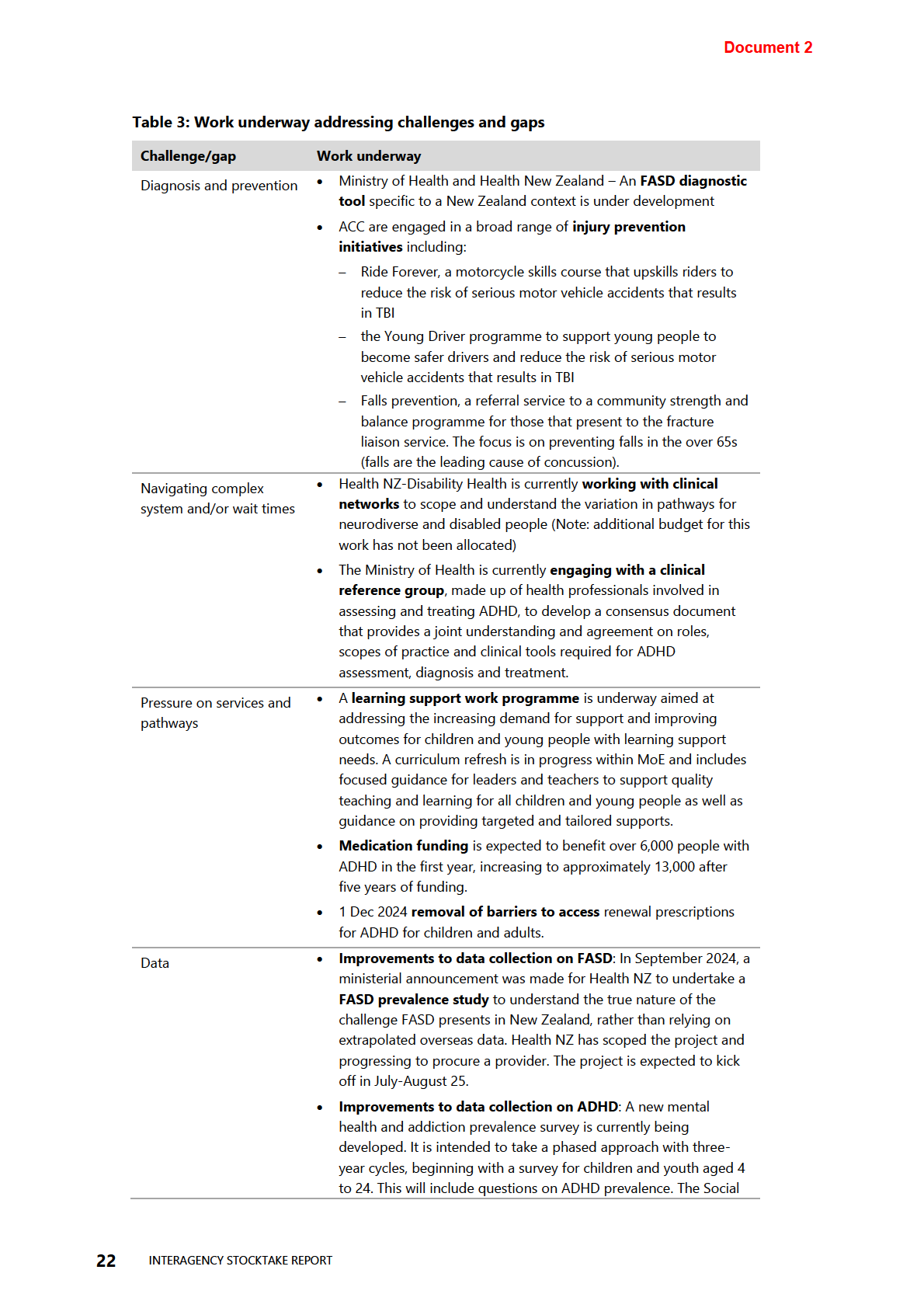
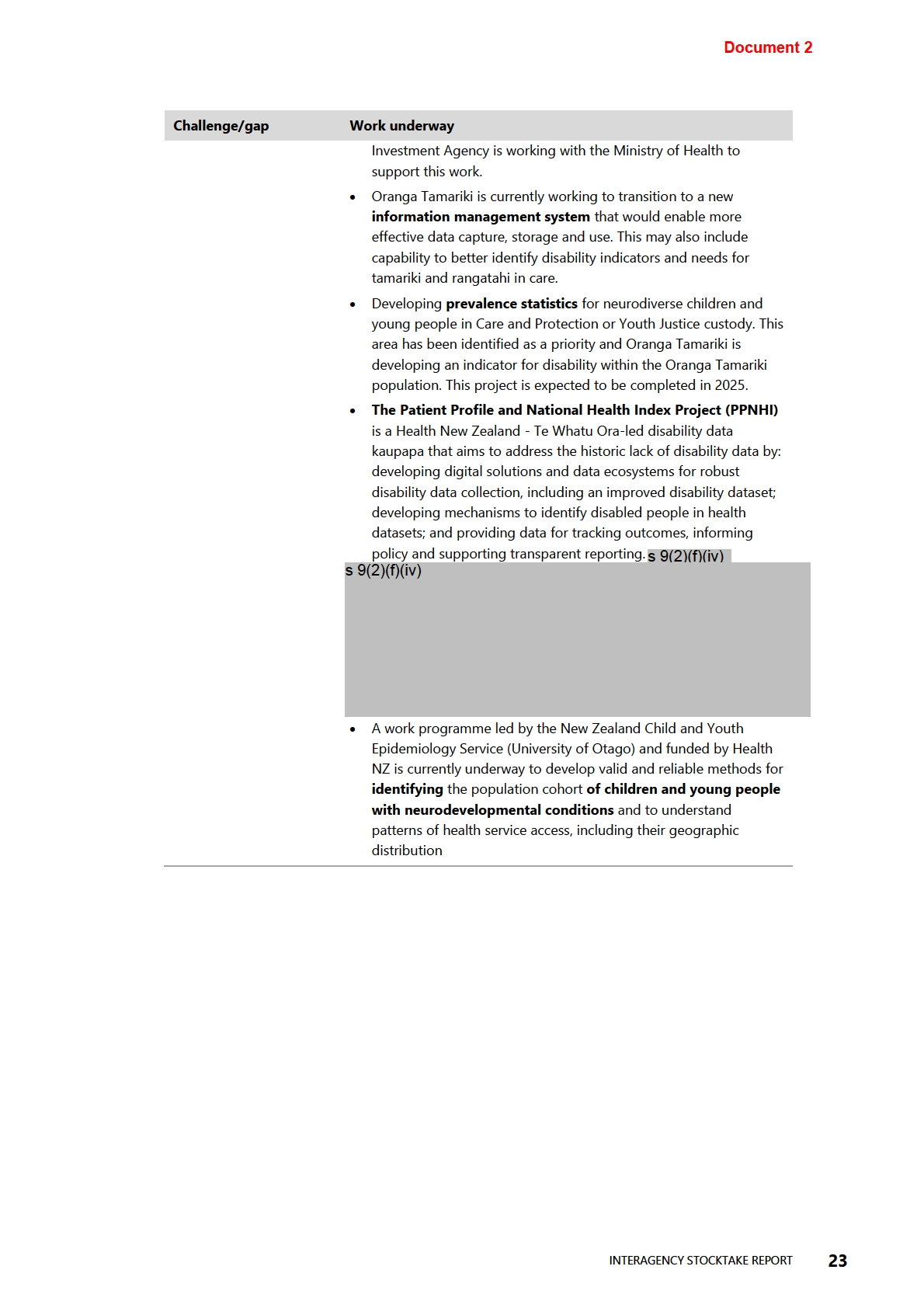
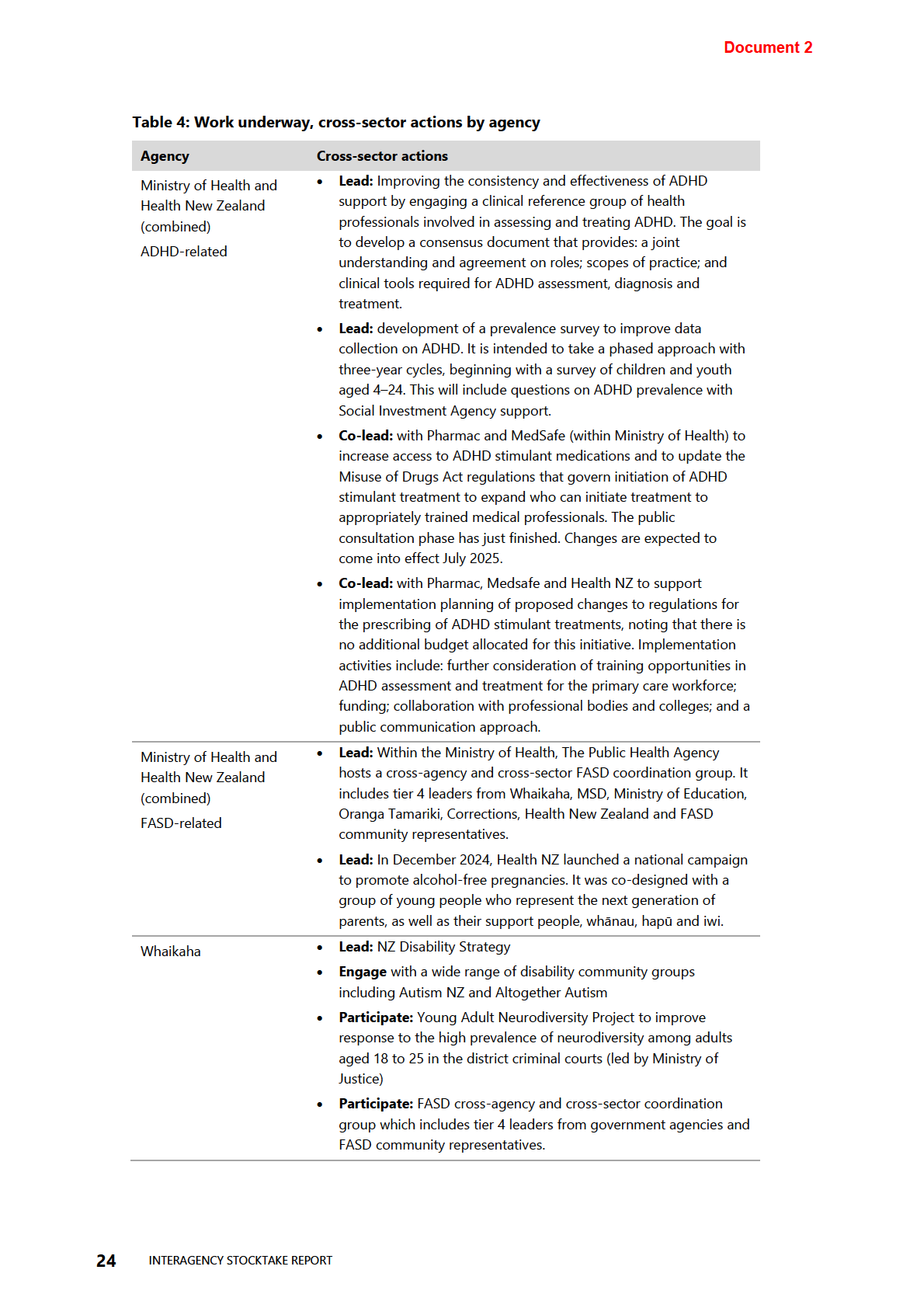
Work underway
The stocktake also captured work that is underway to address some of these known
challenges and service gaps, including:
• activities, resources and support for some specific Neurodiverse conditions (ASD,
ADHD, FASD, etc)
• expanding the scope of government supports that has resulted in supports for more
Neurodiverse people (eg, DSS adding ASD)
1982
• increasingly recognising and identifying Neurodiverse conditions within its
responses to disabled people
ACT
• Prevention programmes for preventable Neurodiverse conditions
A large proportion of work is based on data and highlights a shared understanding of
historical disability (including neurodiversity) data constraints.
Analysis of the stocktake has also provided evidence of many cross-agency efforts
underway in the neurodiversity space, purposes of which vary from improving health
and social outcomes, understanding and responding to need, and addressing systemic
barriers. The level of impact also varies from high-level all of government stra
INFORMATION tegy
through to operational/service delivery level.
Table 3 and Table 4 below provide more detail.
OFFICIAL
THE
UNDER
RELEASED
INTERAGENCY STOCKTAKE REPORT
21
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 2
Opportunities and next
steps
This cross-agency stocktake has provided an initial snapshot of how the Government is
responding to neurodiversity. The engagement and information offered by
government agencies, and the extent of agencies’ responses, is an indication of the
1982
Government’s commitment to people with neurodiversity.
The stocktake has surfaced and established different agency responses to
ACT
neurodiversity, including different definitions, services and supports. These reflect
agencies’ individual responsibilities and accountabilities to various neurodiverse
populations. This cross-agency view has enabled the identification of some common
themes and work areas across multiple agencies’ neurodiversity work programmes.
Common themes across agencies include:
• Government agencies define and respond to people with neurodiversity in different
ways according to their roles and responsibilities.
•
INFORMATION
There are issues with assessments, services and supports, including long wait times
for initial assessments; service gaps; workforce pressures and funding constraints.
• There are barriers to identifying neurodiverse people in government data systems
to better understand their needs and monitor outcomes
• There is growing awareness across government agencies of the need to design and
deliver all aspects of their business with neurodiversity in mind.
OFFICIAL
• There is some appetite for a coordinated cross-agency programme of government
action on neurodiversity.
THE
The next steps are to explore these themes further to understand where cross-agency
col aborations can be beneficial in the short, medium and long term. Understanding
more from neurodivergent people about the effectiveness of existing services and
UNDER
engaging other agencies such as Corrections, Justice, Statistics, and the Social
Investment Agency, provides an opportunity to explore how health and wider
government targets could provide direction and prioritising of actions. Analysis of
historical work could provide further insights to support these next steps.
RELEASED
26
INTERAGENCY STOCKTAKE REPORT
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 Document 3
Briefing
Progressing a Child and Youth Mental Health and Addiction Prevalence
Document 3
Briefing
Progressing a Child and Youth Mental Health and Addiction Prevalence
Survey
Date due to MO: 19 July 2024
Action required by:
9 August 2024
Security level:
IN CONFIDENCE
Health Report number: H2024042404
1982
To:
Hon Matt Doocey, Minister for Mental Health
ACT
Consulted:
Health New Zealand: ☒
Contact for telephone discussion
INFORMATION
Name
Position
Telephone
Dean Rutherford
Deputy Director-General, Evidence,
s 9(2)(a)
Research and Innovation
Robyn Shearer
Deputy Director-General, Clin
OFFICIAL ical,
s 9(2)(a)
Community and Mental Health
THE
Minister’s office to complete:
UNDER
☐ Approved
☐ Decline
☐ Noted
☐ Needs change
☐ Seen
☐ Overtaken by events
☐ See Minister’s Notes
☐ Withdrawn
Comment:
RELEASED
Document 3
Progressing a Child and Youth Mental
Health and Addiction Prevalence Survey
Security level:
IN CONFIDENCE
Date:
19 July 2024
To:
Hon Matt Doocey, Minister for Mental Health
1982
Purpose of report
1.
This briefing responds to your request for advice on options for progressing a mental
ACT
health and addiction prevalence survey with an initial focus on children and young
people.
2.
It follows discussion at your meeting with Ministry of Health Officials on 20 May 2024.
Recommendations
We recommend you:
INFORMATION
a)
Note work to test potential mental health and addiction survey tools with
Yes/No
children and young people aged 2–19 years is underway
b)
Note the Ministry of Health is collaborating with the Ministry of Social
Yes/No
Development to deliver timely and improved data related to mental health
and substance use and service use via the Youth Health and Wellbeing Survey
OFFICIAL
2025
c)
Note the Ministry of Health has committed to providing approximately $300k
Yes/No
THE
of additional, one-off baseline funding to support delivery of new and
improved mental health and substance use data via the Youth Health and
Wellbeing Survey 2025
d)
Note that the Ministry recomm
UNDER ends delivering a mental health and addiction
Yes/No
prevalence survey in three phases over a three-year period, beginning with a
survey for children and youth aged 4–24 years
e)
Note this approach will require funding of approximately $6m over three
Yes/No
years, or approximately $2m per annum, and that providing funding on an
ongoing basis will allow information needs to be met sustainably with a clear
pathway to full population prevalence data
RELEASED
f)
Note that the Ministry of Health and Health New Zealand will seek your final
Yes/No
decisions about use of uncommitted Budget 2019 and Budget 2022 mental
health and addiction funding for a package of initiatives, including a child and
youth prevalence survey, through a separate briefing by the end of July 2024
Briefing: H2024042404
1

 Document 3
Document 3
g)
Agree to meet with Ministry of Health Officials to discuss the recommended
Yes/No
approach to a mental health and addiction prevalence survey
Dean Rutherford
Hon Matt Doocey
Deputy Director-General
Minister for Mental Health
Evidence, Research and Innovation
1982
Date: 18 July 2024
Date:
ACT
Robyn Shearer
Deputy Director-General
Clinical, Community and Mental Health
Date: 18 July 2024
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Briefing: H2024042404
2
Document 3
Progressing a Child and Youth Mental
Health and Addiction Prevalence Survey
Background
1.
In early 2024, the Ministry of Health | Manatū Hauora (the Ministry) commenced work to
identify the tools and infrastructure that will be required to support future mental health
and addiction prevalence studies in New Zealand [Weekly Reports of 7 March, 17 April
and 10 July 2024 refer]. Ministry Officials have met with you to discuss this work, the
need for a national mental health and addiction prevalence survey and a potential
1982
pathway towards this, as set out in May 2024 [H2024039734 refers].
2.
At your meeting with Ministry Officials on 20 May 2024, you requested further advice on
ACT
options for a mental health and addiction prevalence survey, initially focussed on
children and young people. This briefing responds to that request.
3.
Ministry Officials are available to meet with you to discuss this briefing and can provide
additional material if this is required.
Context
4.
In his report,
Meeting the mental health needs of young New Zealanders, the Auditor-
INFORMATION
General emphasises that agencies require detailed information on the nature, extent and
distribution of young people’s mental health needs in order to support well-informed
decisions. The Auditor-General recommends that the Ministry prioritises work to
understand the prevalence of mental health conditions in the population.
5.
A survey on mental health and addiction prevalence in New Zealand (Te Rau Hinengaro)
OFFICIAL
was last conducted in 2003/04, and this did not include children. Decisions related to
resource allocation and mental health and addiction service design are currently being
THE
made without detailed understanding of prevalence, and the relationship between
existing service use and service need.
6.
At a time where services are under pressure and high rates of distress are reported by
young people, New Zealand does not have data to understand mental health and
UNDER
substance use related conditions among our children and young people. Prevalence data
for adults (previously collected through Te Rau Hinengaro in 2003/04) is outdated and
unlikely to accurately represent the realities of today.
7.
In the absence of a mental health and addiction prevalence survey, we cannot determine
the range, proportion, or distribution of specific diagnosable conditions, and critically,
what services are required to respond to existing or unmet need, with certainty that it
RELEASED
matches population needs.
Briefing: H2024042404
3
Document 3
Work is underway to prepare for a mental health and addiction prevalence
survey and fill immediate and ongoing information gaps
Testing of potential survey tools has commenced
8.
The Ministry has contracted Ipsos Limited to deliver testing of potential mental health
and addiction survey tools with children and young people aged 2–19 years in New
Zealand.
9.
This work is being delivered through one-off time-limited funding of $680k from the
Ministry’s baseline, and will be delivered across three stages:
a.
stage 1 (to be completed in July 2024) – with support of subject matter experts,
1982
identify mental health and substance use survey tools for testing
b.
stage 2 (by end of September 2024) – cognitive testing of tools identified in stage
ACT
1 with children and young people, from Māori, Pacific and Asian ethnic groups in
their homes
c.
stage 3 (by end of December 2024) – a small pilot survey to test delivery of tools
in a survey format. This is not intended to deliver data, rather inform how future
surveys could be conducted – e.g., interview format and materials, interviewer
training and engagement methodology.
10.
From this work, the Ministry aims to understand the effectiveness of internationally
validated mental health and substance use survey tools in a New Zealand conte
INFORMATION xt –
particularly how the meaning and acceptability of these tools may vary between ethnic
groups.
11.
The knowledge gained will inform what survey tools, including questionnaire sets, could
be delivered in a New Zealand child and young people mental health and addiction
prevalence survey.
OFFICIAL
12.
Work with Ipsos Limited is expected to run through to the end of 2024, and a final
report, with recommendations, is du
THE e with the Ministry in the first quarter of 2025.
We are also progressing quick wins through the Youth Health and Wellbeing Survey 2025
13.
The Ministry is collaborating with the Ministry of Social Development (MSD) to explore
how the Youth Health and W
UNDER ellbeing Survey 2025 (YHWS) could support the timely
delivery of improved data related to substance use, mental health conditions, and access
and barriers to mental health services.
14.
The Ministry and MSD have collaborated to include baseline mental health questions,
validated in the United Kingdom’s National Health Services Mental Health of Children
and Young People Survey, into the YHWS.
RELEASED
15.
Inclusion of these questions will provide new insights for New Zealand faster than a full
prevalence survey. Results from these questions are expected to highlight changes in the
proportion of young people experiencing mental distress/probable mental health
conditions over time, and whether the needs of those with conditions are being met by
services for those aged 13–19 years. It is also expected some new data will be available
for conditions that are not currently captured, including neurodevelopmental conditions
and disordered eating.
Briefing: H2024042404
4
Document 3
16.
The YHWS will not provide data on the prevalence of specific mental health conditions,
or data for those younger than 12 years. It also will not provide data for the young adult
cohort (those aged 18–24 years) who are considered a critical group in relation to
developmental stage and associated heightened risk of emergence of serious mental
health conditions and of death by suicide.
17.
However, inclusion of additional questions in the YHWS is a low cost and effective way
to deliver better data while work to design and deliver a prevalence survey commences.
18.
The Ministry has committed to providing additional, one-off baseline funding to expand
the size and representativeness of the YHWS 2025.
19.
This will enable increased data quality to understand differences in mental wellbeing
across New Zealand’s youth population, informing the design of a mental health and
1982
addiction prevalence survey.
20.
The YHWS 2025 is currently in its implementation phase, with findings reports expected
ACT
to be available in late 2025.
We still need a mental health and addiction prevalence survey
21.
The health system has reached a point where updated mental health and addiction
prevalence data is critical. A mental health and addiction prevalence survey will expand
our evidence beyond what’s currently available or possible through the YHWS 2025 (or
its future iterations) and New Zealand Health Survey. It will also respond to the Auditor
General’s recommendations.
INFORMATION
22.
A prevalence survey is the only way to fill longstanding information gaps, including:
a.
diagnosable and condition specific information – for example, distinguishing
between normal experience of symptoms of anxiety (worry) and depression
(sadness) and the experience of mental health conditions that require specialist
OFFICIAL
treatment, and distinguishing between anxiety conditions such as post-traumatic
stress disorder and obsessive-compulsive disorders which may require different
service responses
THE
b.
unmet need – capture population experience and treatment need beyond existing
service delivery or interactions with the system.
23.
Filling the above longstanding information gaps will support more effective decisions
UNDER
and planning, including:
a.
needs-based allocation of resource – funding based on what conditions exist,
what services are used or needed and the distribution of these
b.
design targeted prevention, treatment, and care options – for those in need or
at risk, delivering interventions at the point that most makes sense and where the
RELEASED
outcomes will be greatest, including early intervention and prevention approaches
(which may be cross-sector or cross-portfolio)
c.
anticipating future need – planning for workforce requirements and the settings
required to support this – e.g., education and training pathways to meet gaps in
services and review of migration settings
d.
evaluation of the effectiveness of current and future services – investment in
what’s needed and what works, and disinvestment in what doesn’t
Briefing: H2024042404
5
Document 3
e.
long-term and cross-sector analysis – over time, support the ability to explore the
relationship between mental health and addiction with other components of health
(e.g., nutrition), and analysis of the influence of social and economic determinants of
health.
Delivering a mental health and addiction prevalence survey, starting with
children and young people
24.
Since meeting with you on 20 May 2024, the Ministry has worked with Health New
Zealand | Te Whatu Ora (Health New Zealand) to define the information need more
clearly – scrutinising what information is needed in order to develop options for how a
mental health and addiction prevalence survey may be delivered.
1982
25.
This, alongside collaboration with MSD on the YHWS 2025, has allowed the Ministry to
scale options for how a prevalence survey could be delivered, starting with children and
ACT
youth, with a pathway towards understanding full population prevalence over time.
Process for delivering a mental health and addiction prevalence survey
26.
Work to deliver a mental health and addiction prevalence survey would be conducted in
three phases over a three-year period. Appendix 1 illustrates these phases and
associated milestones, alongside work already underway.
Development and detailed design phase (September 2024 – December 2025)
INFORMATION
27.
The development and detailed design phase is comprehensive, particularly when there is
limited, outdated, or no available survey methodology to build on. Consistent with the
development and design practices and timeframes of other government surveys and
international practice, this phase includes:
OFFICIAL
a. selection or development of questions and sample design that will permit
production of high quality and relevant statistics, including for sub-population
groups, building on the initial
THE tools testing underway and the YHWS 2025
b. testing of survey delivery approaches to ensure content is structured coherently,
easily allows participation for all populations groups, and minimises respondent
burden
UNDER
c. given the sensitive subject matter, progressing through appropriate safeguards,
such as the Health and Disability Ethics Council, to ensure the survey is ethically
sound and does not cause harm to respondents
d. ensuring the right workforce, collateral, and systems are available to support data
collection and delivery the survey – e.g., clinically trained or specialist expertise,
RELEASED
pathways to care and services for respondents should they be needed.
28.
The Ministry will leverage opportunities for efficiencies as they present, and take steps to
minimise delays or disruption where possible. However, some timeframes are outside of
the Ministry’s control. For example, engagement with the Health and Disability Ethics
Council is expected to be substantial and intensive, particularly for surveying children
aged 4–12 years and their families.
Briefing: H2024042404
6
Document 3
Implementation phase (January 2026 – December 2026)
29.
The implementation phase involves taking the survey into the field and collecting data
from individuals. It is routinely the most costly phase with key costs covering:
a. the recruitment or procurement and training of collection workforce and associated
personnel costs – e.g., management and health and safety requirements
b. ensuring IT support and technical subject matter expertise is available to support
interviewers deliver the survey effectively and efficiently.
30.
Throughout the development and detailed design phase, options for how data collection
could be executed may be identified e.g., school-based or home-based collection.
1982
However, consistent with the delivery of other government surveys that collect
information from individuals (including the New Zealand Health Survey, General Social
ACT
Survey, and Household Income and Living Survey) the Ministry anticipates a mental
health and addiction prevalence survey would be collected over a 12-month period.
Analysis and reporting phase (January 2027 – June 2027)
31.
Through the analysis and reporting phase the Ministry will seek to utilise internal
expertise and existing systems (including the Health Surveys Team) where possible and
seek specialist epidemiological and mental health and addiction expertise where
INFORMATION
appropriate.
32.
This phase includes:
a. processing of the data collected and organising data into a format for analysis
b. analysis, interpretation of data and preparation of proposed outputs – isolating key
OFFICIAL
results and metrics, mock-ups of statistics and products and validating that these
respond to information needs
THE
c. application of quality, confidentiality, and privacy controls – peer review of outputs
(including by subject matter experts) to ensure accurate and safe articulation and
presentation of results and safeguarding the privacy of survey participants.
UNDER
Recommended approach to a mental health and addiction prevalence survey
33.
The Ministry has explored different models for delivering a mental health and addiction
prevalence survey, and options for scaling and phasing of these – e.g., cohort by cohort
collection and scaling of content or sample size. Options were assessed based on
delivery confidence, cost, timeframes, and ability to meet the defined information need.
Appendix 2 prese
RELEASED nts the options considered and a high-level assessment of these.
34.
The Ministry’s recommended approach is to implement a three-yearly mental health and
addiction prevalence survey – starting with children and young people over the period
of 2024/25–2026/27.
35.
This approach is feasible, cost effective, and prioritises meeting information needs for
the highest priority population cohort first. Reconducting a survey at regular intervals
safeguards the ongoing production and availability of data and allows creation of a
Briefing: H2024042404
7
Document 3
long-term timeseries. There are options in relation to the frequency with which a child
and youth prevalence survey could be conducted, discussed further below.
36.
The Ministry’s recommended approach will require funding of approximately $6m over
three years, or approximately $2m per annum, ongoing.
37.
Milestones associated with process and timeframes above, alongside work currently
underway, are set out below, with further information outlined in Appendix 1:
a.
December 2024 – completion of work with Ipsos Limited on testing potential
mental health and addiction survey tools
b.
March 2025 – final report from testing of potential mental health and addiction
survey tools delivered, with recommendations for survey design
1982
c.
Late 2025 – findings from the YHWS 2025 available with information related to
probable mental health conditions and service responsiveness for those aged 13
ACT –19
years, and new data on neurodevelopmental disorders and disordered eating
d.
December 2025 – completion of development and detailed design of a child and
youth prevalence survey
e.
January 2026 – commencement of field work and data collection
f.
December 2026 – completion of data collection and commencement of analysis
INFORMATION
g.
Mid-late 2027 – publication of survey results and repots on prevalence of mental
health and substance use conditions in children and youth.
Funding for a child and youth mental health and addiction prevalence survey
38.
Ministry and Health New Zealand Officials recently provided you with advice on
OFFICIAL
initiatives that could be funded utilising uncommitted Budget 2019 and Budget 2022
mental health and addiction funding [H2024044383 and HNZ00051267 refer]. At a
discussion with Ministry Officials on 1 July 2024, you indicated an interest in progressing
THE
with a shortlist of priority initiatives, including a mental health prevalence survey.
39.
Your Office has requested further advice on potential investment packages and scaling
and phasing options. This further advice will seek your final decisions about use of
uncommitted funding for a p
UNDER ackage of initiatives, including a child and youth prevalence
survey, through a separate briefing by the end of July 2024. It will reflect the advice set
out in this briefing and the estimated costs of a child and youth prevalence survey.
40.
As previously indicated, the Ministry considers that progressing with a mental health and
addiction prevalence survey would be a substantively new policy initiative and would
trigger the threshold for ensuring Cabinet awareness. The Ministry will support you with
RELEASED
this process pending your decisions about preferred investment packages.
Pathway to understanding full population prevalence
41.
As indicated earlier (see paragraph 35), there are options related to the frequency of
conducting a mental health and addiction prevalence survey as well as the cohorts of
focus for each survey. Decisions related to this should seek to balance the preference to
Briefing: H2024042404
8
Document 3
sustainably meet information needs, with cost implications and allowing sufficient time
between surveys to register changes within and across the population.
42.
While undertaking a child and youth-focused prevalence survey every three years would
ensure robust and continuous data, it may be too frequent to add significant value for
decision making. However, assuming a three-yearly survey cycle is supported, there is an
opportunity to build towards understanding full population prevalence over six years –
with the first three-year period focused on children and youth (those aged 4–24 years)
as recommended, and the second three-year period focused on the adult population
(those aged 25 years and above).
43.
With ongoing funding, the Ministry recommends alternating the cohort of focus each
time the survey is conducted years to maintain an understanding of full population
1982
prevalence. This provides a clear, feasible and sustainable pathway to mental health and
addiction prevalence data across the whole population and maintaining this over time.
ACT
44.
This does not require your decision at this stage, but Officials are available to discuss this
with you in more detail.
Equity
45.
A mental health and addiction prevalence survey will improve understanding of
inequities in needs, service provision, population behaviours and experiences, as well as
factors that may contribute to these.
INFORMATION
46.
This, in turn, supports evidence informed investment for services that address inequities,
and monitoring of the impact services have on mental health outcomes, and whether
this impact is equitably distributed.
47.
An ongoing, iterative prevalence survey can respond to dynamic population needs, for
example, enhancing culturally responsive mental heal
OFFICIAL th care options to enable more
equitable service use.
THE
Next steps
48.
The Ministry is available to discuss this briefing you with you and respond to any
feedback or questions you have.
UNDER
49.
The Ministry and Health New Zealand will present advice by the end of July and seek
your final decisions regarding use of uncommitted funding, including investment in a
child and youth mental health and addiction prevalence survey.
50.
Following this advice and your decisions, the Ministry will progress work to support to
give effect to your decisions.
51.
The Ministry will continue to update you via the Weekly Report on its work with Ipsos
RELEASED
Limited on testing of potential survey tools.
ENDS.
Briefing: H2024042404
9
Document 3
Minister’s Notes
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Briefing: H2024042404
10
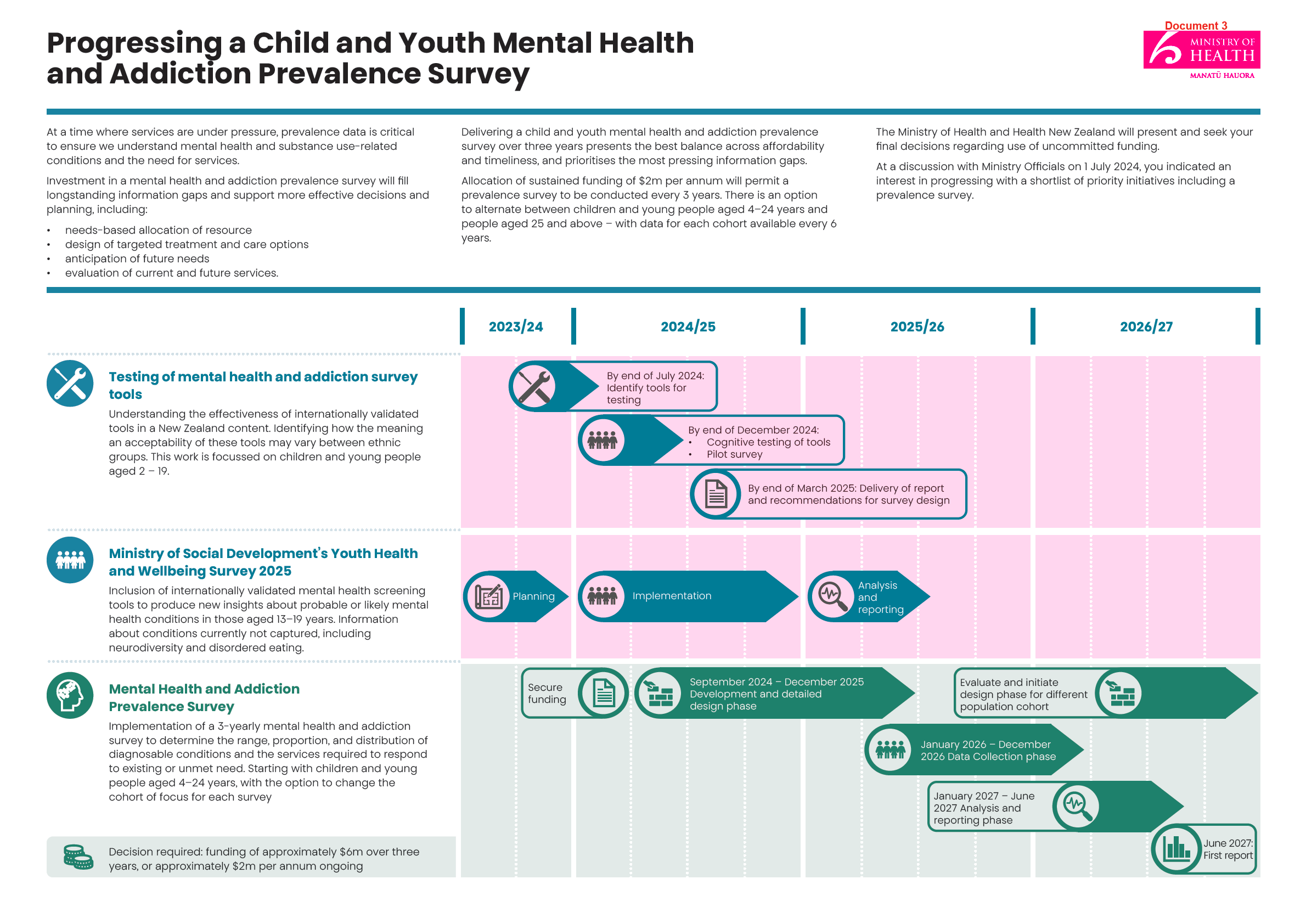 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
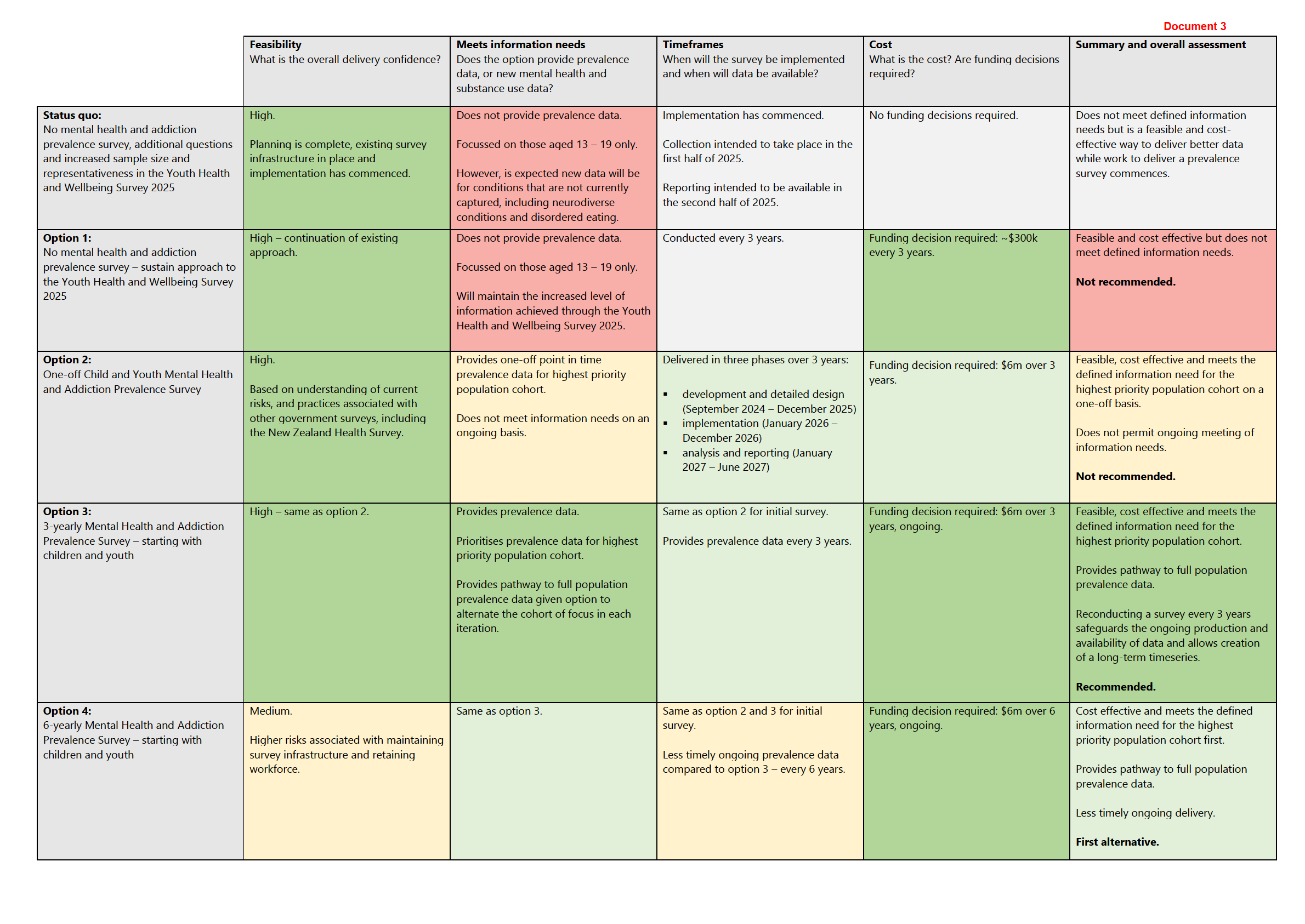 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED