

133 Molesworth Street
PO Box 5013
Wellington 6140
New Zealand
T+64 4 496 2000
4 February 2026
Elspeth Baker-Vevers
By email: [FYI request #33049 email]
Ref:
H2025076277
Tēnā koe Elspeth
Response to your request for official information Thank you for your request under the Official Information Act 1982 (the Act) to the Ministry of
Health – Manatū Hauora (the Ministry) on 28 November 2025 for information regarding attention
deficit hyperactivity disorder (ADHD) policy, governance, data, and rights oversight.
The Ministry notes that you have made multiple requests on the same topic (H2025076364,
H2025076972, H2025076445, and H2025076281 refer), which has resulted in some overlap
in subject matter across the documents identified. To avoid unnecessary repetition or
reproduction of the same material, these are instead referenced in the appropriate releases as
referenced in Appendix 1.
Please find a response to each part of your request below:
1. Leadership / Ownership
Any documents identifying which team, unit, or role holds responsibility for ADHD policy,
inter-agency coordination, governance, or oversight.
2. Policies / Frameworks
Any national policies, guidelines, briefings or advice specifically addressing ADHD, or
service-delivery guidance since 2015 that address ADHD diagnosis, treatment, service
delivery, or cross-agency coordination.
This section refers to national health policies and Ministry-held service-delivery guidance,
and does not seek the New Zealand Clinical Principles Framework for ADHD, which is
covered in a separate request.
The Ministry of Health is not responsible for providing clinical guidelines. The Health
Practitioners Competence Assurance Act 2003 requires al health practitioners to be registered
with a professional health workforce body. These health workforce bodies regulate health
professionals, providing oversight to ensure they work within their scope of practice including
providing clinical guidelines.
For example, the Royal Australian and New Zealand College of Psychiatrists have endorsed the
Australian Evidence-Based Clinical Practice Guideline for ADHD and have their own guidelines
for adult ADHD.
Therefore, these parts of your request are refused under section 18(g)(i) of the Act, as the
information requested is not held by the Ministry and there are no grounds for believing it is held
by another agency subject to the Act.
3. Data & Monitoring
Any documentation describing how ADHD is identified, coded, monitored, or reported in
national health datasets (for example ICD, ATC, SNOMED, or pharmacy indicators), and
any outcome or performance measures used since 2015.
If ADHD is grouped under another category, please specify which category and provide
the associated coding guidance or definitions.
On 13 January 2026, this part of your request was transferred to Health New Zealand – Te
Whatu Ora in accordance with section 14(b)(ii) of the Act. You can expect a response from them
in due course. They can be contacted via email at:
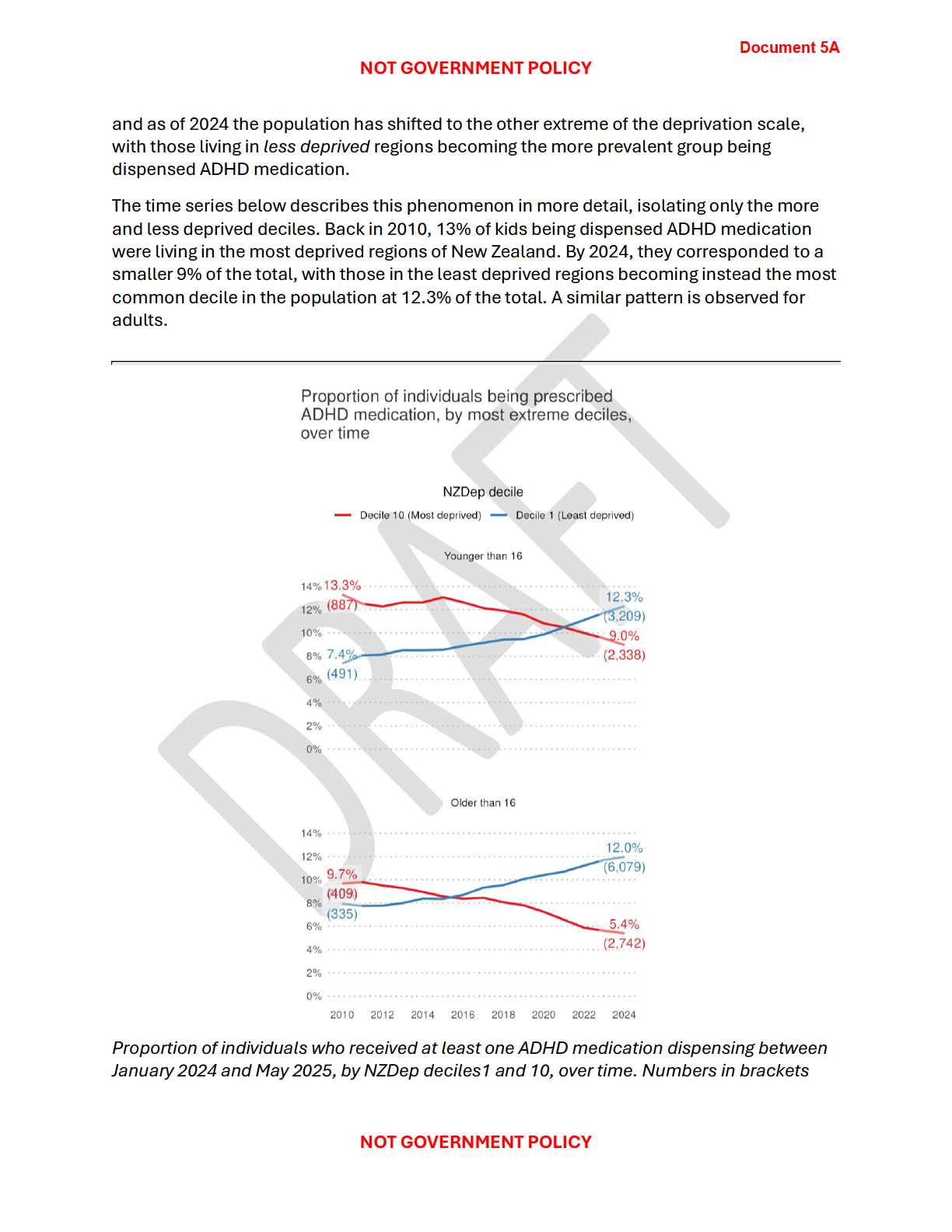
[email address]. The New Zealand Health Survey has reported an estimate, since 2011/12, of the proportion of
children (5-14 years) who have been diagnosed with ADHD. The estimate, and relevant
definition, is publicly available on the New Zealand Health Data Explorer here:
minhealthnz.shinyapps.io/nz-health-survey-2024-25-annual-data-explorer.
4. IDI Evidence and Follow-Up
In light of growing evidence (including the 2025 University of Otago study) that ADHD
cohorts can be identified in the IDI and that neurodivergent youth face significantly higher
premature mortality, please provide:
a. Any documents, advice, or correspondence (2018–present) discussing Manatū
Hauora’s response to, use of, or planned engagement with ADHD related research
using the IDI;
Three pieces of advice were provided to the Minister for Mental Health, Hon Matt Doocey,
regarding how the Integrated Data Infrastructure (IDI) could be used to understand the
effectiveness of changes to diagnosis and prescribing practices (please refer to documents 2
and 4). There are emails exchanged between the Ministry, Pharmac, and the Social Investment
Agency regarding this work (please refer to documents 1 and 3).
Some initial scoping analysis to test use of datasets for understanding the effectiveness of the
changes has been completed. Work to determine next steps and further IDI work is ongoing,
and no formal decisions have been made.
These only cover work from 2024-2025, but please note that this is the only ADHD specific
research that has been undertaken by the Ministry using the IDI.
b. Any records of Ministry led or Ministry commissioned analyses of ADHD using the IDI
or linked administrative datasets; and
As noted above, three pieces of advice were provided to the Minister for Mental Health
regarding how the IDI could be used to understand the effectiveness of changes to diagnosis
and prescribing practices. Some initial scoping analysis to test use of datasets for
understanding the effectiveness of the changes has been completed.
Work to determine next steps and further IDI work is ongoing, and no formal decisions have
been made.
Page 2 of 6
c. Any plans, proposals, or discussions regarding the development of ongoing ADHD
population level monitoring or outcomes reporting using the IDI or equivalent data
systems.
Work to determine an approach to monitoring and evaluating the regulatory change is ongoing,
with no formal decisions yet made. Initial discussions about key components of a monitoring
approach were held in late 2025, but no decisions have been made to date. As such, this part of
your request is refused under section 18(g)(i) of the Act.
5. Equity / Risk
Any analysis, reports, or targeted briefings addressing inequities, suicide risk, self-harm
risk, health loss, or comorbidity for people with ADHD, and any actions taken or proposed
in response.
Initial scoping analysis has included investigating discrepancies between genders, ethnicity and
deprivation. Understanding the distribution and equity implications of the changes wil be
considered in developing a monitoring or evaluation approach. This part of your request is
refused under section 18(g)(i) of the Act.
If any Māori data governance or Māori equity considerations were applied when deciding
whether to collect, categorise, or monitor ADHD-related information, please provide the
relevant documents.
This part of your request is refused under section 18(g)(i) of the Act as the information
requested is not held by the Ministry and there are no grounds for believing it is held by another
agency subject to the Act.
Rainbow+/Takatāpui populations: Please include any analysis or data relating to ADHD
outcomes, or confirm if such data are not collected.
If no such analysis exists, please confirm this.
No specific analysis relating for ADHD has been completed for rainbow and/or Takatāpui
populations to date. The data required to conduct this analysis is limited, and there are quality
considerations with its use – e.g., inconsistent collection of sex and gender across the system
and limited collection of other aspects such as sexual identity. Therefore, this part of your
request is refused under section 18(g)(i) of the Act.
6. Rights / Compliance
Any assessments or advice since 2015 considering obligations relevant to ADHD under:
the New Zealand Public Health and Disability Act
the UN Convention on the Rights of Persons with Disabilities (UNCRPD)
accessibility and non-discrimination requirements (including Human Rights Act 1993 and
NZBORA s19).
7. Oversight Position
Please confirm whether Manatū Hauora currently holds policy or service-delivery
oversight for ADHD, or whether this function is formally assigned elsewhere.
If no agency holds this role, please confirm this.
If information is not held
If your agency does not hold some or all of the information requested, that absence also
helps clarify how ADHD is currently tracked and managed across the system. Please
Page 3 of 6
 confirm if the information is not held, and include any existing documents or
confirm if the information is not held, and include any existing documents or
correspondence that record a decision not to collect or monitor ADHD-related information.
Please also specify how related matters are categorised (e.g., under neurodiversity,
mental health, disability, or other categories)
These parts of your request are refused under section 18(g)(i) of the Act.
Overal , the Ministry has identified 9 documents within scope of your entire request. All
documents and decisions regarding release are itemised in Appendix 1 with copies enclosed.
Where information is withheld under section 9 of the Act, I have considered the countervailing
public interest in release in making this decision and consider that it does not outweigh the need
to withhold at this time.
If you wish to discuss any aspect of your request with us, including this decision, please feel
free to contact the OIA Services Team on:
[email address]. Under section 28(3) of the Act, you have the right to ask the Ombudsman to review any
decisions made under this request. The Ombudsman may be contacted by email at:
[email address] or by cal ing 0800 802 602.
Please note that this response, with your personal details removed, may be published on the
Ministry website at:
www.health.govt.nz/about-ministry/information-releases/responses-official-
information-act-requests. Nāku noa, nā
Andy Bartle
Acting Group Manager, Data Analytics and Surveys Strategy and Policy | Te Pou Rautaki
Page 4 of 6
Appendix 1: List of documents for release
#
Date
Document details
Decision on release
1
9 – 30 September
Email correspondence:
the
Some information is withheld
2024
Ministry sending a draft briefing
under section 9(2)(k) of the
(H2024050136) for review to SIA Act, to prevent the disclosure
and Pharmac
or use of official information
for improper gain or
advantage.
2
10 October 2024
Briefing for information:
Some information is withheld
Understanding impacts of
under section 9(2)(a) of the
proposed changes to diagnosing Act to protect the privacy of
and prescribing practices for
natural persons.
ADHD (H2024050136)
3
7 – 11 March 2025 Email correspondence:
Feedback Some information is withheld
from Social Investment Agency to under the fol owing sections of
the Ministry regarding briefing
the Act:
(H2025062661)
• section 9(2)(a) of the
Act; and,
• section 9(2)(g)(i) to
maintain the effective
conduct of public
affairs through the free
and frank expression
of opinions by or
between or to Ministers
and officers and
employees of any
public service agency.
4
12 March 2025
Briefing for information:
Further
Some information is withheld
analysis to understand the
under section 9(2)(a) of the
impacts of changes to ADHD
Act.
diagnosing
and prescribing practices
(H2025062661)
5
3 – 13 July 2025
Email correspondence: Internal
Released in full.
MoH communication
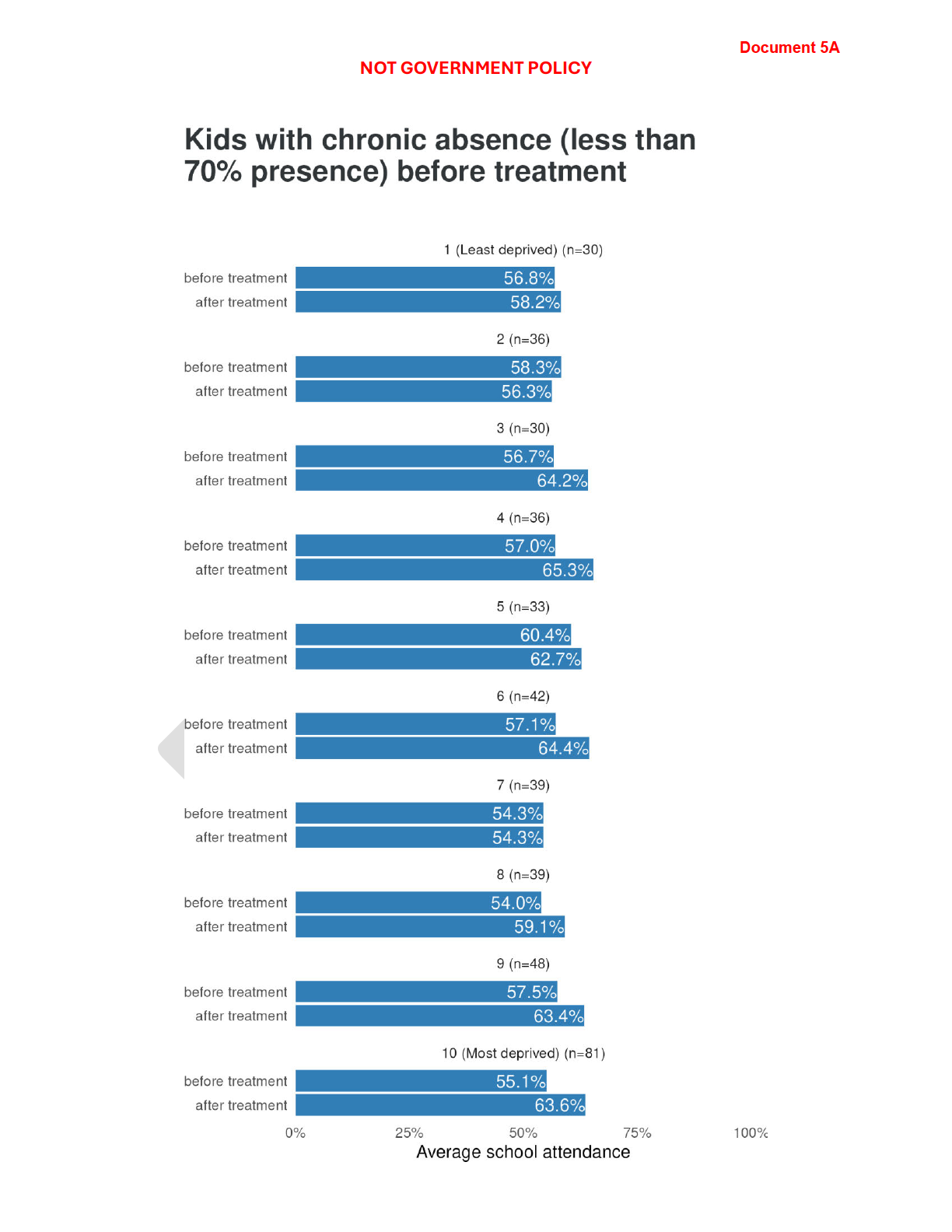
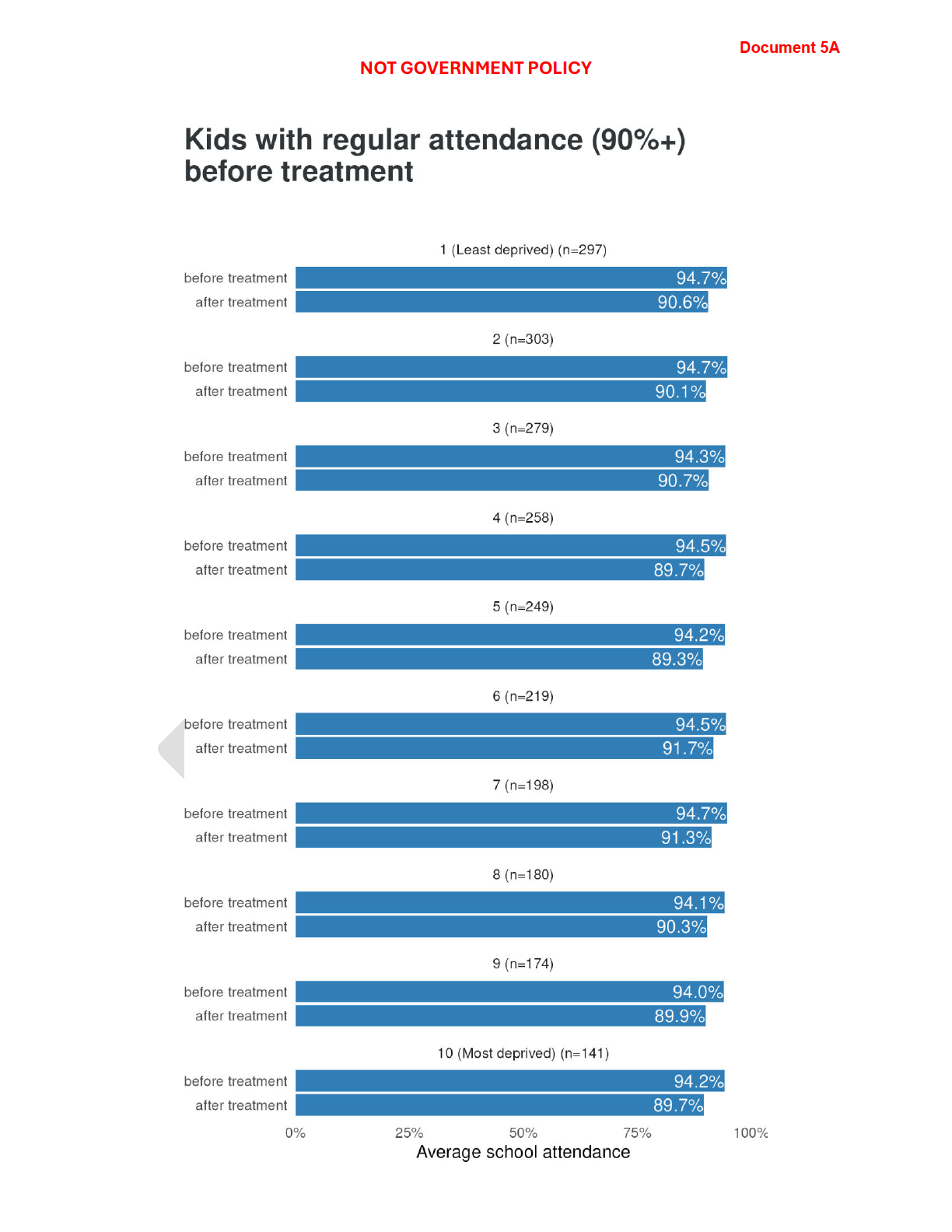
5A
Attachment: ADHD medication
dispensing: the impact of
changes and the characteristics
of the population being
dispensed drugs
6
14 – 18 August
Email correspondence: Between Some information is withheld
2025
the MoH and Pharmac
under section 9(2)(k) of the
Act.
7
20 – 21 August
Email correspondence: Internal
Some information is withheld
2025
MoH communication
under section 9(2)(a) of the
Act.
Page 5 of 6
#
Date
Document details
Decision on release
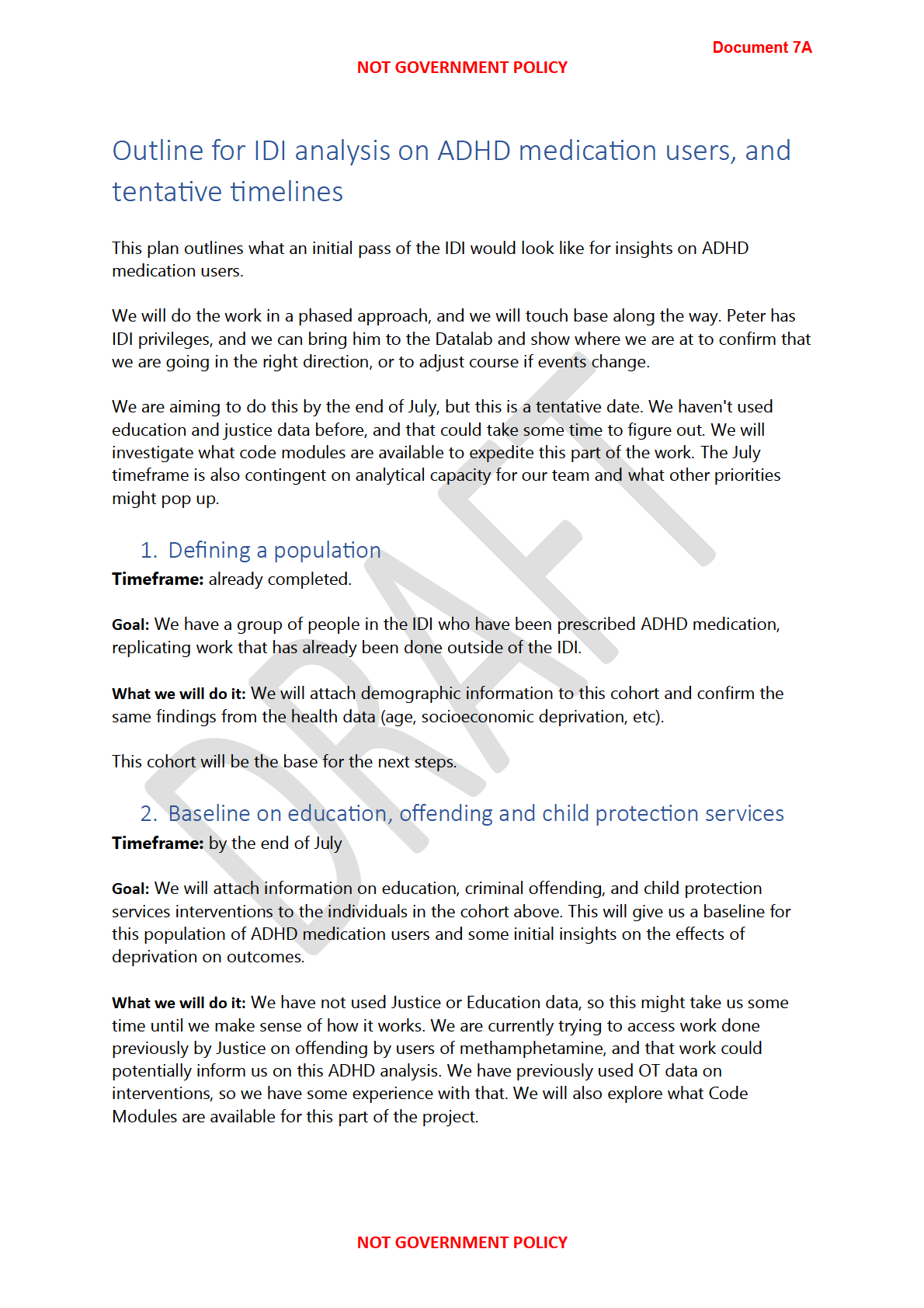
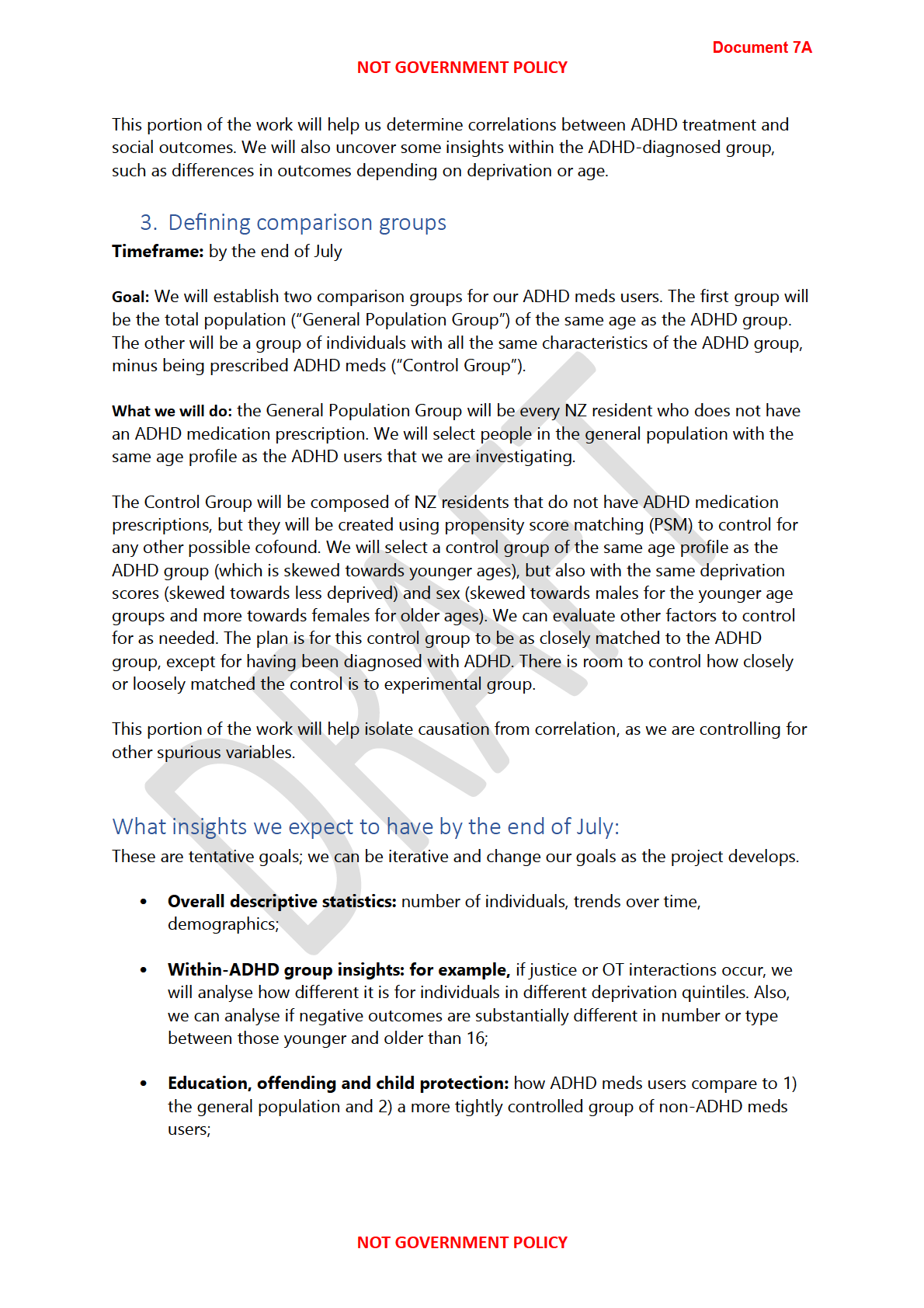
7A
Attachment: Outline for IDI
Released in full.
analysis on ADHD medication
users, and tentative timelines
Page 6 of 6
Document 1
From:
Grace Spraggs
Sent:
Monday, 30 September 2024 7:43 pm
To:
Luke Scullion; Rebecca Hollingsworth; Andrew Webber
Cc:
Peter Dolan
Subject:
RE: ADHD next steps
Attachments:
ADHD evaluation.docx
Please refer to document 2 for the final version.
Kia ora koutou,
Thank you for your me today, I appreciated being able to chat through the briefing and work through the points of
1982
challenge.
Apprecia ng you hadn’t seen an earlier version, I’ve worked on a revised version that I hope responds to the points
ACT
Andrew raised this a ernoon – being clearer about the evalua ve ques ons we could answer/aspects we can
measure, with some suppor ng informa on about there being a wider context we could look at over me.
Will leave you to work through it and provide input and comments. Happy to schedule me to chat through any
unanswered ques ons and work in your input.
Hope tomorrow isn’t as crazy for you all
Grace
INFORMATION
From: Grace Spraggs
Sent: Tuesday, September 24, 2024 4:26 PM
To: Rebecca Hollingsworth <[email address]>; Andrew Webber <[email address]>;
Luke Scullion <[email address]>; Oliver Whitehead <[email address]>; David Hughes
OFFICIAL
<[email address]>
Cc: Peter Dolan <[email address]>; Kieran Moorhead <[email address]>; Tim
Jelleyman <[email address]>
THE
Subject: RE: ADHD next steps
Kia ora koutou,
Firstly, I’m sorry I haven’t been in touch sin
UNDER ce our mee ng with a progress or direc on update! Hopefully this email
will provide answers to the ques ons I’ve le unanswered!
I have been working away on the briefing and will get a first dra through to you all for review by Friday which will
enable discussion about the detail rather than overall pitch and narra ve. Un l then, I’ve included a rough sketch of
what I’m working to pull together. Let me know if there are any red flags or gut reac ons!
SIA – could you please let me
RELEASED know what your sign-out expecta ons are? Dean Rutherford will be signing it out from
this end, but the DG will review.
Happy to schedule me to get together as a group early next week to discuss.
Context:
There’s been mee ngs and discussions on implemen ng the ac ons taken from the parliamentary hui on
ADHD.
Insights provided by SIA indicate dispari es in outcomes.
1
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 1
-----Original Appointment-----
From: Rebecca Hollingsworth <[email address]>
Sent: Monday, September 9, 2024 2:22 PM
To: Rebecca Hollingsworth; Aphra Green; Andrew Webber; Luke Scullion; Kieran Moorhead; Oliver Whitehead;
David Hughes
Subject: ADHD next steps
When: Tuesday, 10 September 2024 3:30 pm-4:00 pm (UTC+12:00) Auckland, Wellington.
Where: SIA_MTG_L03_Tieke_Rm
Kia ora,
We’re a bit tight on time here at SIA, but I’m hoping this time works to regroup on ADHD
next steps – particularly where SIA has been asked to jointly participate in briefings.
1982
Rebecca
________________________________________________________________________________
ACT
s 9(2)(k)
INFORMATION
OFFICIAL
THE
UNDER
This email and any attachments may contain information that is confidential and/or subject to legal privilege. If you
are not the intended recipient, any use, dissemination, or duplication of this email and attachments is prohibited. If
you have received this email in error please notify the author immediately and erase all copies of the email and
attachments. The Social Investment Agency accepts no responsibility for changes made to this message or
attachments after transmission from the Agency. The Social Investment Agency accepts no responsibility for any
improper or unauthorised use, dissemination, or duplication of the message or attachments. Any views expressed in
RELEASED
this email may be those of the individual sender and may not necessarily reflect the views of the Social Investment
Agency.
3
 Document 2
Briefing for information
Understanding impacts of proposed changes to diagnosing and
Document 2
Briefing for information
Understanding impacts of proposed changes to diagnosing and
prescribing practices for ADHD
Date due to MO: 10 October 2024
Action required by:
N/A
Security level:
IN CONFIDENCE
Reference:
H2024050136
1982
To:
Hon Matt Doocey, Minister for Mental Health, Associate Minister of Health
Copy to:
Hon Nicola Willis, Minister for Social Investment
ACT
Hon David Seymour, Associate Minister of Health
Consulted:
Health New Zealand: ☐
Proactive release: This
title is proposed by the Ministry of Health for proactive release: ☐
INFORMATION
Contact for telephone discussion
Name
Position
Telephone
Dean Rutherford
Deputy Director-General, Evide
OFFICIAL nce
s 9(2)(a)
Research and Innovation, Ministry of
Health
THE
Peter Dolan
Group Manager, Data Analytics and
s 9(2)(a)
Surveys
UNDER
Minister’s office to complete:
☐ Approved
☐ Decline
☐ Overtaken by events
☐ Needs change
☐
RELEASED
Seen
☐ See Minister’s Notes
☐ Withdrawn
Comment:
 Document 2
Briefing for decision
Understanding impacts of proposed changes to diagnosing and
Document 2
Briefing for decision
Understanding impacts of proposed changes to diagnosing and
prescribing practices for ADHD
Security level:
IN CONFIDENCE
Date:
10 October 2024
To:
Hon Matt Doocey, Minister for Mental Health and Associate Minister of
Health
1982
Copy:
Hon Nicola Willis, Minister for Social Investment
Hon David Seymour, Associate Minister of Health
ACT
Purpose of report
1.
This briefing responds to your request for advice that outlines approaches for
understanding the impacts of proposed changes to diagnosis and prescribing practices
for Attention Deficit Hyperactivity Disorder (ADHD).
2.
This briefing was developed by the Ministry of Health, with input from the Social
Investment Agency. Pharmac was consulted.
INFORMATION
3.
Given this briefing was jointly commissioned by your Office and the Office of the
Minister for Social Investment, it has been copied to Hon Nicola Willis. As this briefing
discusses proposals consulted on by Pharmac, it has been copied to Hon David Seymour
as Associate Minister of Health.
OFFICIAL
Recommendations
THE
We recommend you:
a)
Note that we have identified options for how the impacts of proposed
Yes/No
changes to ADHD diagnosing and prescribing practices could be evaluated
UNDER
Dean Rutherford
RELEASED
Hon Matt Doocey
Deputy Director-General – Evidence
Minister for Mental Health, Associate
Research and Analytics
Minister of Health
Ministry of Health
Date:
Date: 11 October 2024
Briefing: H2024050136
IN CONFIDENCE
1
Document 2
Understanding impacts of changes to
prescribing practices for ADHD
Context and background
1.
At the Attention Deficit Hyperactivity Disorder (ADHD) parliamentary hui on 2 May 2024,
stakeholders developed and agreed six actions focussed on addressing barriers and
improving support across the ADHD care continuum.
2.
On 26 August 2024, officials from Health New Zealand, the Ministry of Health (the
1982
Ministry) and Pharmac met with you (in your respective capacities as Minister for Social
Investment, and Associate Minister of Health) to discuss progress on these actions. The
Ministry of Health, Pharmac and Health New Zealand recently provided an update on
ACT
progress towards cross-agency ADHD actions, including work to improve data collection
[H2024050133 refers].
3.
Pharmac has recently completed public consultation (12 – 26 September 2024) on a
proposal to fund lisdexamfetamine for management of ADHD. If approved by the
Pharmac Board (or delegate), lisdexamfetamine will be available to eligible consumers in
early December 2024.
4.
Pharmac has also recently completed consultation (12 September – 3 October 2024) on
INFORMATION
a proposal to remove the renewal criteria for stimulant treatments for people with
ADHD. If approved by the Pharmac Board (or delegate), the renewal criteria would be
removed from stimulant treatments in early December 2024.
5.
In December 2024, Pharmac and Medsafe will work together to publicly consult on a
proposal to change both the regulatory and funding settings for who can initiate
OFFICIAL
prescribing funded and unfunded stimulant medication for ADHD.
6.
Considering these proposed changes, and following discussion with officials on 26
THE
August 2024, your Offices commissioned advice from the Ministry and the Social
Investment Agency (SIA) on how impacts of changes to prescribing and diagnosing
practices could be measured.
Understanding the impacts
UNDER of the proposed changes
7.
The proposed changes to prescribing and diagnosing practices aim to improve services
and care for those with ADHD through:
a. increasing supply of ADHD medication
b. improving ongoing access to funded stimulant treatment, ongoing and long-term
RELEASED
care
c. allowing a wider range of health professionals to diagnose ADHD and initiate
stimulant treatment.
Briefing: H2024050136
IN CONFIDENCE
2
Document 2
8.
To understand the impact of these changes, we would evaluate:
a. changes in prescribing and dispending patterns in order to understand the extent to
which medication accessibility has changed for whom pharmaceutical treatment is
preferred – both initial access and access to long-term care
i. specific aspects of change that could be investigated include overall
prescription and dispensing volumes, continuity of prescription and dispensing
for individuals, variation across regions or population groups
b. changes in diagnosis rates and diagnosis patterns in order to understand the extent
to which access to diagnosis has improved
i. specific aspects of change that could be investigated include the practitioner
types (e.g., psychiatrist, general practitioner, nurse practitioner), changes in
1982
initial special authority requests (indicating diagnosis where pharmaceutical
treatment is preferred/appropriate)
ACT
c. how changes in diagnosis and prescribing practices influence social outcomes for
those with ADHD
i. using the Integrated Data Infrastructure (IDI), these outcomes can be observed
across cohorts, across domains, and through time. Key outcomes of interest
include school attendance, student achievement, employment stability, and
labour force participation
ii. analysis using the IDI will support evaluation of outcomes of those who have
INFORMATION
ADHD compared to those who don’t and inform further policy and investment
decisions based on changes in outcomes (whether positive or negative)
Some evaluation will be straightforward, but there are some important limitations to be
aware of
OFFICIAL
9.
It may be challenging to determine from the kinds of analysis described above whether
changes in outcomes are the result of the proposed changes, other supports (e.g.,
THE
tailored, or bespoke learning supports) or contributing factors (e.g., environmental, or
wider health supports).
10.
The datasets currently available to support analysis are administrative datasets. As
administrative datasets are designed to record health service user interactions with the
UNDER
health system, they will provide an effective avenue for evaluating the impacts of the
proposed changes on those who receive a diagnosis or are receiving pharmaceutical
treatment.
11.
However, administrative datasets do not allow us to understand unmet need or
accurately define the population with the greatest potential to benefit. This does not
prevent analysis from being undertaken, but it does set the parameters for which
RELEASED
analysis can be interpreted or used.
12.
There is likely to be some lag time between implementation of the changes and impact
on social outcomes being observed through analysis. This is because of the time needed
for changes to be:
a. embedded in clinical settings and practice, and for the corresponding uptake to
occur
Briefing: H2024050136
IN CONFIDENCE
3
Document 2
b. represented in data collections and for these to be available in the IDI to support
analysis.
Recent data investment will support further analysis in the future
13.
The recently announced mental health and addiction prevalence survey will measure the
range, proportion, and distribution of mental health conditions among children and
young people, including neurodevelopmental conditions such as ADHD.
14.
Supplementing existing administrative datasets with data from this survey will allow
analysis to stretch beyond snapshots of service delivery and interactions with the system.
The survey will permit understanding of the underlying prevalence of ADHD among
children and young people in New Zealand (i.e., the size of the problem among that
1982
population cohort) and identify unmet need.
15.
The survey will increase visibility of the population with the greatest potential to benefit
ACT
from changes to prescribing and diagnosing practices, where barriers may exist within
the system, and how this differs across the country and population groups.
Equity
16.
Our administrative datasets provide an effective and efficient avenue for understanding
interactions with the health system – particularly who is accessing which services.
17.
Access to ADHD diagnoses and corresponding treatments and care may be unevenly
INFORMATION
distributed across New Zealand’s population. Analysis that utilises administrative data
will not completely account for groups of the population who experience barriers to
accessing health care. The proposed analysis therefore is unlikely to be representative of
the population with the potential to benefit from interventions. In some cases, analysis
will only represent those who have access to prescriptions (i.e., have an ADHD
diagnosis).
OFFICIAL
Next steps
THE
18.
Further advice on the scope, resource requirements and timeframes can be provided on
request. Where appropriate and required, this advice will seek decisions related to
priorities and trade-offs.
UNDER
19.
The Ministry of Health is establishing an ADHD programme oversight group to support
ongoing coordination of cross-government activity in relation to ADHD actions. This
could include oversight further activities to evaluate impacts of changes through the use
of ADHD data.
ENDS.
RELEASED
Briefing: H2024050136
IN CONFIDENCE
4
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 3
attachments after transmission from the Agency. The Social Investment Agency accepts no responsibility for any
improper or unauthorised use, dissemination, or duplication of the message or attachments. Any views expressed in
this email may be those of the individual sender and may not necessarily reflect the views of the Social Investment
Agency.
****************************************************************************
Statement of confidentiality: This e-mail message and any accompanying
attachments may contain information that is IN-CONFIDENCE and subject to
legal privilege.
If you are not the intended recipient, do not read, use, disseminate,
distribute or copy this message or attachments.
If you have received this message in error, please notify the sender
immediately and delete this message.
****************************************************************************
1982
This email and any attachments may contain information that is confidential and/or subject to legal privilege. If you
ACT
are not the intended recipient, any use, dissemination, or duplication of this email and attachments is prohibited. If
you have received this email in error please notify the author immediately and erase all copies of the email and
attachments. The Social Investment Agency accepts no responsibility for changes made to this message or
attachments after transmission from the Agency. The Social Investment Agency accepts no responsibility for any
improper or unauthorised use, dissemination, or duplication of the message or attachments. Any views expressed in
this email may be those of the individual sender and may not necessarily reflect the views of the Social Investment
Agency.
****************************************************************************
INFORMATION
Statement of confidentiality: This e-mail message and any accompanying
attachments may contain information that is IN-CONFIDENCE and subject to
legal privilege.
If you are not the intended recipient, do not read, use, disseminate,
distribute or copy this message or attachments.
OFFICIAL
If you have received this message in error, please notify the sender
immediately and delete this message.
****************************************************************************
THE
This email and any attachments may contain information that is confidential and/or subject to legal privilege. If you
are not the intended recipient, any use, dissemination, or duplication of this email and attachments is prohibited. If
you have received this email in error please notify the author immediately and erase all copies of the email and
UNDER
attachments. The Social Investment Agency accepts no responsibility for changes made to this message or
attachments after transmission from the Agency. The Social Investment Agency accepts no responsibility for any
improper or unauthorised use, dissemination, or duplication of the message or attachments. Any views expressed in
this email may be those of the individual sender and may not necessarily reflect the views of the Social Investment
Agency.
RELEASED
5
 Document 4
Briefing for information
Further analysis to understand the impacts of changes to ADHD diagnosing
Document 4
Briefing for information
Further analysis to understand the impacts of changes to ADHD diagnosing
and prescribing practices
Date due to MO: 12 March 2025
Action required by:
N/A
Security level:
IN CONFIDENCE
Reference:
H2025062661
1982
To:
Hon Matt Doocey, Associate Minister of Health
Copy to:
Hon Nicola Willis, Minister for Social Investment
ACT
Hon David Seymour, Associate Minister of Health
Consulted:
Health New Zealand: ☐
Proactive release: This
title is proposed by the Ministry of Health for proactive release: ☒
INFORMATION
Contact for telephone discussion
Name
Position
Telephone
Dean Rutherford
Deputy Director-General, Evidence
s 9(2)(a)
OFFICIAL
Research and Innovation
Peter Dolan
Group Manager, Data Analytics and
THE
s 9(2)(a)
Surveys
UNDER
Minister’s office to complete:
☐ Noted
☐ Seen
☐ Needs change
☐ Withdrawn
☐ See Minister’s Notes
RELEASED
☐ Overtaken by events
Comment:
 Document 4
Briefing for information
Further analysis to understand the impacts of changes to ADHD diagnosing
Document 4
Briefing for information
Further analysis to understand the impacts of changes to ADHD diagnosing
and prescribing practices
Security level:
IN CONFIDENCE
Date:
12 March 2025
To:
Hon Matt Doocey, Associate Minister for Health
Purpose of report
1982
1.
This briefing provides you with information on analysis the Ministry of Health (the
Ministry) will carry out to understand the impacts of changes to prescribing and
ACT
diagnosing practices for Attention Deficit Hyperactivity Disorder (ADHD). This briefing
expands on advice provided to you in November 2024 [H2024050136 and H2024054483
refers].
2.
The Social Investment Agency and Pharmac have contributed to this briefing. Given this,
it is recommended you share this briefing with Hon Nicola Willis, Minister for Social
Investment and Hon David Seymour, Associate Minister of Health.
INFORMATION
Recommendations
We recommend you:
a)
Note the Ministry of Health will carry out analysis to understand the impacts
Yes/No
of changes to diagnosis and prescribing practices for Attention Deficit
OFFICIAL
Hyperactivity Disorder
b)
Note that this analysis will include:
Yes/No
THE
a. evaluating whether, and to what extent, the aims of the changes have
been successful
b. investigating the impacts the changes have on social outcomes
UNDER
c)
Note that analysis focussed on the impact on social outcomes will include
Yes/No
education, employment and health outcomes
d)
Note the Social Investment Agency and Pharmac have contributed to this
Yes/No
briefing
RELEASED
Dean Rutherford
Hon Matt Doocey
Deputy Director-General
Associate Minister of Health
Evidence, Research and Innovation
Date:
Date: 12 March 2025
Briefing: H2025062661
IN-CONFIDENCE
1
Document 4
Further analysis to understand the impacts
of changes to ADHD diagnosing and
prescribing practices
Background
3.
In late 2024 Pharmac and Medsafe approved proposals to fund lisdexamfetamine for the
management of ADHD and remove the special authority renewal criteria for stimulant
treatments for those with ADHD.
1982
4.
In October 2024, the Ministry of Health (the Ministry), in consultation with the Social
Investment Agency and Pharmac, provided advice on initial approaches for how the
ACT
impacts of these changes could be measured [H2024050136 refers]. Following receipt of
this advice, and discussion with Ministry Officials, you sought further advice on options
for analysis that the Ministry could carry out [H2024054438 refers].
5.
Since this advice was provided, the Ministry has worked with the Social Investment
Agency to scope further analysis that is focused on understanding impacts the changes
have on social outcomes.
INFORMATION
Analysis to be carried out by the Ministry of Health
Evaluating the success of the changes
6.
The changes approved by Pharmac and MedSafe aim to improve services and care for
those with ADHD by:
OFFICIAL
a. ensuring adequate supply of ADHD medication
b. improving ongoing access to funded stimulant treatment, and long-term care
THE
c. allowing a wider range of health professionals to initiate stimulant treatment.
7.
The Ministry will carry out analysis focused on evaluating whether, and to what extent,
the aims of the changes (outlined in paragraph 6) have been successful. Specifically, this
UNDER
analysis will support understanding of:
a. increases in ADHD diagnoses and overall uptake of lisdexamfetamine for eligible
users
b. which health practitioners are diagnosing ADHD and initiating pharmaceutical
treatment for eligible users
RELEASED
c. any instances where eligible users are not taking up pharmaceutical treatment, or
where eligible users are opting for lisdexamfetamine over other available
medications
d. where access to long term and ongoing pharmaceutical treatment and care has
improved
e. the attributes of the population who receive pharmaceutical treatment for ADHD.
This includes demographic information and socioeconomic attributes such as
Briefing: H2025062661
IN-CONFIDENCE
2
Document 4
household income, deprivation, housing, and education. This will provide contextual
information that supports interpretation of the analysis and monitoring of changes
and observation of trends through time.
Analysis to identify changes in social outcomes
8.
Since the advice provided to you in November 2024, the Ministry has worked with the
Social Investment Agency to scope further analysis that is focused on identifying
changes in social outcomes.
9.
Using the Integrated Data Infrastructure, the Ministry of Health will work to identify
differences or patterns in outcomes (whether positive or negative) across cohorts and
domains through time. This analysis could be used to inform future policy and
1982
investment decision. Specifically, the Ministry will look to identify:
a. changes in education outcomes:
ACT
i. through analysis that investigates the relationship with ADHD and school
attendance, stand downs or suspension, tenure, qualification attainment,
higher education pathways/uptake
ii. comparing outcomes before and after diagnosis and/or pharmaceutical
treatment
iii. comparing outcomes between defined cohorts.
b. changes in employment outcomes:
INFORMATION
i. through analysis that investigates the relationship between ADHD and income
earnings, receipt of benefits or other incomes supports, labour force
participation and employment stability
ii. investigating employment outcomes of parents of children diagnosed with
ADHD
OFFICIAL
iii. comparing outcomes before and after diagnosis and/or pharmaceutical
treatment
THE
iv. comparing outcomes between defined cohorts.
c. changes in health outcomes:
i.
UNDER
through analysis that investigates the relationship between ADHD and other
mental health conditions, potential risk-taking behaviours, and physical health
ii. comparing outcomes before and after diagnosis and/or pharmaceutical
treatment
iii. comparing outcomes between defined cohorts.
d.
RELEASED
changes in the overall life satisfaction of those with ADHD.
10.
Based on results of the analysis above, the Ministry may also extend its analysis to
secondary changes in social outcomes. For example, the Ministry could look at whether
improvements in education and employment outcomes mean fewer contacts with the
justice sector for people with ADHD.
Briefing: H2025062661
IN-CONFIDENCE
3
Document 4
11.
There is likely to be some lag time before changes in outcomes are observed, and this
will influence the overall timeframes associated the Ministry’s analysis. This lag time is
outside of the control of the Ministry and is due to the time needed for changes to be:
a. embedded in clinical settings and practice, and for the corresponding uptake by
health service users to occur
b. represented in data collections and for these to be available in the IDI to support
analysis.
Further analysis will be permitted by the Child and Youth Mental Health and Addiction
Prevalence Study
12.
The recently announced Child and Youth Mental Health and Addiction Study will
1982
measure the range, proportion, and distribution of mental health conditions among
children and young people, including neurodevelopmental conditions such as ADHD.
ACT
13.
Data from this survey will allow further analysis, specifically increasing visibility of those
with potentially undiagnosed ADHD and where barriers may exist within the system (eg,
why diagnosis has not been achieved) and how this differs across the country and
population groups.
Connection with Pharmac’s work programme
Monitoring use of ADHD medicines
INFORMATION
14.
Pharmac will monitor use of relevant ADHD medicines in line with its statutory objective
to achieve the best health outcomes for New Zealanders within its fixed budget. This will
be reviewed by Pharmac’s Mental Health Advisory Committee.
15.
Pharmac also has a workstream planned on responsible use of funded medicines. This
work would look at any differences in access rates by
OFFICIAL demography and may inform
targeted access equity initiatives. There is scope to have an ADHD focus as part of this
work.
THE
Ongoing supply issues
16.
There are ongoing significant global supply issues affecting methylphenidate.
Methylphenidate is a funded stimulant medicine used to treat ADHD. Pharmac funds
UNDER
multiple treatment options for people with ADHD, including methylphenidate,
lisdexamfetamine, and dexamfetamine. Funding a range of stimulant medicines gives
prescribers more options for treating people with ADHD when there are supply issues.
17.
The supply issues are currently affecting the availability of the Concerta, Rubifen and
Teva brands of methylphenidate globally. This may mean
that some people with ADHD
will not have ac
RELEASED cess to the medicine they normally use – particularly if they are not
eligible for lisdexamfetamine. Pharmac is working closely with suppliers to manage
supply and has asked clinicians to prioritise methylphenidate for people who need it
most (children and adolescents) and consider other treatment options for adults.
18.
Pharmac is considering how the supply issues may affect the implementation of the
approved changes. Widening access to ADHD medications could exacerbate the
ongoing supply issue with methylphenidate. The Ministry and Pharmac will work
together to understand how supply shortages will impact planned analysis.
Briefing: H2025062661
IN-CONFIDENCE
4
Document 4
Next steps
19.
Officials from the Ministry are available to discuss this advice with you at your request.
20.
The Ministry will commence work on the analysis presented, collaborating with the
Social Investment Agency and Pharmac as appropriate. The first output will be
establishing baselines (how things are now), against which any changes that result from
new diagnosis and prescribing practices will be compared.
21.
The Ministry will update you on the progress of its analysis through the Weekly Report
and can meet with you to discuss progress at your request.
22.
Pharmac will continue to provide separate updates to ministers on its progress in
managing the current supply issues.
1982
ENDS.
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Briefing: H2025062661
IN-CONFIDENCE
5
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 6
Confiden ality no ce: This email may be confiden al or legally privileged. If you have received it by mistake, please tell the
sender immediately by reply, remove this email and the reply from your system, and don’t act on it in any other way.
-----Original Appointment-----
From: Claudia Rees <[email address]>
Sent: Thursday, August 14, 2025 3:13 PM
To: Claudia Rees; Robyn Harris; Jason Arnold-Ext; Grace Spraggs; Carlos Barroso Silva
Subject: Pharmac / MoH - ADHD regulatory changes - analytics and evaluation
When: Monday, 18 August 2025 3:00 pm-3:30 pm (UTC+12:00) Auckland, Wel ington.
Where: Microsoft Teams Meeting
Kia ora koutou
1982
Popping time in to discuss the Ministry’s planned approach to analytics and evaluation for the ADHD
ACT
regulatory changes, and how Pharmac may be able to support.
Ngā mihi
Claudia
________________________________________________________________________________
s 9(2)(k)
INFORMATION
OFFICIAL
THE
UNDER
______
RELEASED
2
Document 7
From:
Grace Spraggs
Sent:
Thursday, 21 August 2025 2:40 pm
To:
Jin Russell; Debra Begg; Billy Allan; Anna Skinner; Peter Abernethy; Chris James;
Kieran Moorhead; Suzanne Townsend; Carlos Barroso Silva
Cc:
Joe Bourne; Michael Woodside; Lauren Hancock; Victoria Manning; Michael Haynes;
Alastair Shum; Ben Clayton
Subject:
RE: ADHD diagnosis and treatment discussion: Work Programme Document
Kia ora koutou,
For visibility and to ensure we’re all keeping connected on this, I had a meeting with Pharmac earlier in the wee
1982k to
connect on the analytical work Data Analytics and Surveys is leading. This was largely to ensure we’re not
duplicating effort, and to explore possible areas of collaboration.
ACT
I’ve provided them with information on what we were commissioned to do for Minister Doocey and shared the
analysis that @Carlos Barroso Silva has done to date. Consistent with the discussion we had, I emphasised that the
work we’re doing isn’t a formal monitoring or evaluation piece, but indicated we’d be happy to explore shaping it
into that with them if required, or support them to develop a monitoring/evaluation/outcomes framework.
We’re also going to explore whether it’s possible to get access to Pharmac’s special authority data which will help us
understand any shifts following the regulatory changes in February.
INFORMATION
Happy to chat if anyone has any questions.
Thanks,
G
OFFICIAL
From: Jin Russell <[email address]>
Sent: Wednesday, August 20, 2025 1:47 PM
THE
To: Debra Begg <[email address]>; Billy Allan <[email address]>; Anna Skinner
<[email address]>; Peter Abernethy <[email address]>; Chris James
<[email address]>; Kieran Moorhead <[email address]>; Suzanne Townsend
<[email address]>; Grace Spraggs <[email address]>
Cc: Joe Bourne <[email address]>; Michael Woodside <[email address]>; Lauren
UNDER
Hancock <[email address]>; Victoria Manning <[email address]>; Michael Haynes
<[email address]>; Alastair Shum <[email address]>; Ben Clayton
<[email address]>
Subject: RE: ADHD diagnosis and treatment discussion: Work Programme Document
Thanks Debra, I’ve made some tracked changes to be clearer re. implementation of ADHD regulatory changes in lead
up to Feb 2026. Hopefully it is c
RELEASED learer now that the Ministry’s role will be to convene stakeholders who are involved
in implementation, not to implement per se.
Ngā mihi
Jin
From: Debra Begg <[email address]>
Sent: Wednesday, August 20, 2025 11:05 AM
To: Jin Russell <[email address]>; Billy Allan <[email address]>; Anna Skinner
<[email address]>; Peter Abernethy <[email address]>; Chris James
<[email address]>; Kieran Moorhead <[email address]>; Suzanne Townsend
1
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED