People with mental distress and disorders
link to page 2 link to page 2 link to page 7 link to page 7 link to page 7 link to page 7 link to page 7 link to page 8 link to page 9 link to page 9 link to page 10 link to page 11 link to page 11 link to page 12 link to page 12 link to page 12 link to page 12 link to page 13 link to page 13 link to page 16 link to page 16 link to page 17 link to page 18 link to page 18 link to page 18 link to page 22 link to page 22 link to page 22 link to page 22 link to page 23 link to page 23 link to page 23 link to page 24 link to page 24 link to page 24 link to page 24 link to page 25 link to page 25 link to page 26 link to page 26
Table of Contents
Table of Contents
2
Policy statement and principles
7
What
7
Phase 1 changes - effective from 4 November 2024:
7
Phase Two went live as a national process on 16 June 2025:
7
Why
7
How
8
Overview
9
Introduction
9
Police contact with persons in mental distress
10
What this chapter covers
11
The new threshold - defining Police business
11
The use of TENR
12
Prevention First
12
Staff Safety persons of interest
12
Legal definition and Police involvement
12
Advising other agencies of offences
13
Recognising behaviours
13
Responding to people in mental distress
16
Verbal Communication
16
Non-Verbal Communication
17
Reducing environmental stress
18
Police wel being
18
Responding to suicide risk
18
Submit a report
22
Submit Self Harm/Suicidal Tendency safety alert
22
Risk factors for suicide
22
Groups at higher risk
22
Taking a suicidal person into custody
23
Supervising suicidal people in custody
23
Self-harm
23
Releasing the person-at-risk into the care of another
24
Releasing into the care of others
24
Information for the carer
24
Resolutions for mental health events
24
Co-Response Teams (CRTs) or sometimes cal ed Multi Agency Teams
25
Frequent cal ers/high-needs users
25
Adult intervention plans on NIA
26
Fear of Police
26
link to page 26 link to page 27 link to page 27 link to page 27 link to page 29 link to page 29 link to page 30 link to page 30 link to page 30 link to page 30 link to page 30 link to page 31 link to page 31 link to page 32 link to page 32 link to page 32 link to page 33 link to page 33 link to page 33 link to page 33 link to page 34 link to page 34 link to page 34 link to page 35 link to page 35 link to page 35 link to page 35 link to page 35 link to page 35 link to page 36 link to page 37 link to page 37 link to page 37 link to page 38 link to page 39 link to page 39 link to page 39 link to page 39 link to page 40
Bias
26
Mental Health categorisations and data quality
27
Mental health flags
27
Use of K1
27
Relevant legislation
29
Memorandum of Understanding
29
Mental Health (Compulsory Assessment and Treatment) Act 1992
30
Roles and responsibilities of clinicians
30
Directors of Area Mental Health Services (DAMHS)
30
Duly Authorised Officer (DAOs)
30
Mental Health Practitioner
30
Police’s role under the Mental Health (Compulsory Assessment and Treatment) Act 1992
31
Rights-based approach
31
Advance directives
32
People with a mental disorder (as defined by the Act)
32
Definition of mental disorder
32
‘Mental disorder’ does not include
33
Assessment and treatment procedure
33
Role of the DAO, responsible clinician and the court
33
Who to cal
33
Criminal behaviour
34
Duty to respect cultural identity
34
Duty to provide an interpreter
34
Compulsory assessment and treatment procedure
35
Application for an assessment
35
Compulsory Treatment Orders
35
Community Treatment Order
35
Inpatient Order
35
If the person commits an offence
35
Reducing and eliminating seclusion and restraint - Health guideline changes
36
Powers to assist Duly Authorised Officers
37
Authority
37
When a Police officer may assist
37
Warrant required
38
No documentation other than the warrant is required
39
Location for patient assessment
39
If a constable is not in uniform
39
Arrest provisions apply
39
Using force to enact a direction from DAO
40
link to page 40 link to page 42 link to page 42 link to page 42 link to page 43 link to page 43 link to page 43 link to page 43 link to page 44 link to page 44 link to page 44 link to page 45 link to page 45 link to page 45 link to page 46 link to page 46 link to page 47 link to page 47 link to page 48 link to page 48 link to page 48 link to page 48 link to page 50 link to page 50 link to page 50 link to page 50 link to page 51 link to page 51 link to page 53 link to page 53 link to page 55 link to page 55 link to page 55 link to page 56 link to page 56 link to page 56 link to page 57 link to page 57
Handcuffing
40
Procedures for assisting Duly Authorised Officers
42
If the DAO is not present
42
Limitations of Police powers and assistance (Section 38 and 40)
42
Check credentials
43
Check the certificate
43
Using force to transport the person (Section 122B)
43
Positional asphyxia risk factors
43
Responsibility for damage caused by force
44
Six-hour detention limit
44
Bil of Rights
44
Assisting a Mental Health Practitioner
45
Authority
45
When you can assist
45
If Police employee is not in uniform
46
Arrest provisions apply
46
Using force
47
Procedures
47
Transporting people
48
Returning a patient to hospital who is absent without leave (AWOL)
48
Police role
48
Two powers to retake
48
Voluntary patients
50
Definition of special patient
50
Definition of restricted patient
50
Offence to assist escape
50
Using force
51
If a patient is reported missing
51
Health-led media releases
53
When asked to return a patient
53
Mental y disordered person on private property
55
Authority
55
Power to enter premises
55
Power to prevent suicide
56
Retaking a patient
56
Cal ing a DAO or Mental Health Practitioner
56
Administrative offences under the MH (CAT) Act
57
Table of offences
57
link to page 60 link to page 61 link to page 61 link to page 61 link to page 61 link to page 62 link to page 62 link to page 63 link to page 63 link to page 65 link to page 65 link to page 65 link to page 65 link to page 65 link to page 66 link to page 67 link to page 67 link to page 68 link to page 68 link to page 68 link to page 68 link to page 69 link to page 70 link to page 70 link to page 70 link to page 71 link to page 71 link to page 71 link to page 71 link to page 71 link to page 72 link to page 73 link to page 73 link to page 73 link to page 73 link to page 74
People with an intel ectual disability
60
Suicidal indicators for people in custody
61
Responding to a suicide attempt or threat
61
Power to prevent suicide
61
Entering property to protect life and property
61
Action at the scene
62
Talking to the person
62
Informing others
63
Police responsibility
63
People affected by drugs or alcohol
65
Taking the person home
65
Detention
65
Child or young person
65
If the person has a mental disorder
65
Effect of drugs on mental disorder
66
Criminal procedures where mental y disordered person commits offence
67
Definition of ‘mental impairment’
67
Mental y disordered people who are suspected of having committed an offence,
or are the victim of an offence
68
Suspects
68
Offences punishable by imprisonment
68
Holding suspects in custody
68
Victims and witnesses
69
Fitness to stand trial
70
Definition of ‘unfit to stand trial’
70
If the defendant is not involved
70
Body samples
71
Appeals
71
Enquiry into detention options
71
Needs assessment
71
Detention in hospital or secure facility
71
Other treatment and care options
72
Insanity
73
Definition of insanity
73
Agreement on insanity
73
Judge or jury determining insanity
73
Convicted people
74
link to page 74 link to page 74 link to page 74 link to page 75 link to page 75 link to page 75 link to page 75 link to page 76 link to page 76
Detention options
74
Other options
74
Needs assessment
74
Assessing person in custody for mental impairment
75
Assessment report
75
Detention while report conducted
75
Needs assessment
75
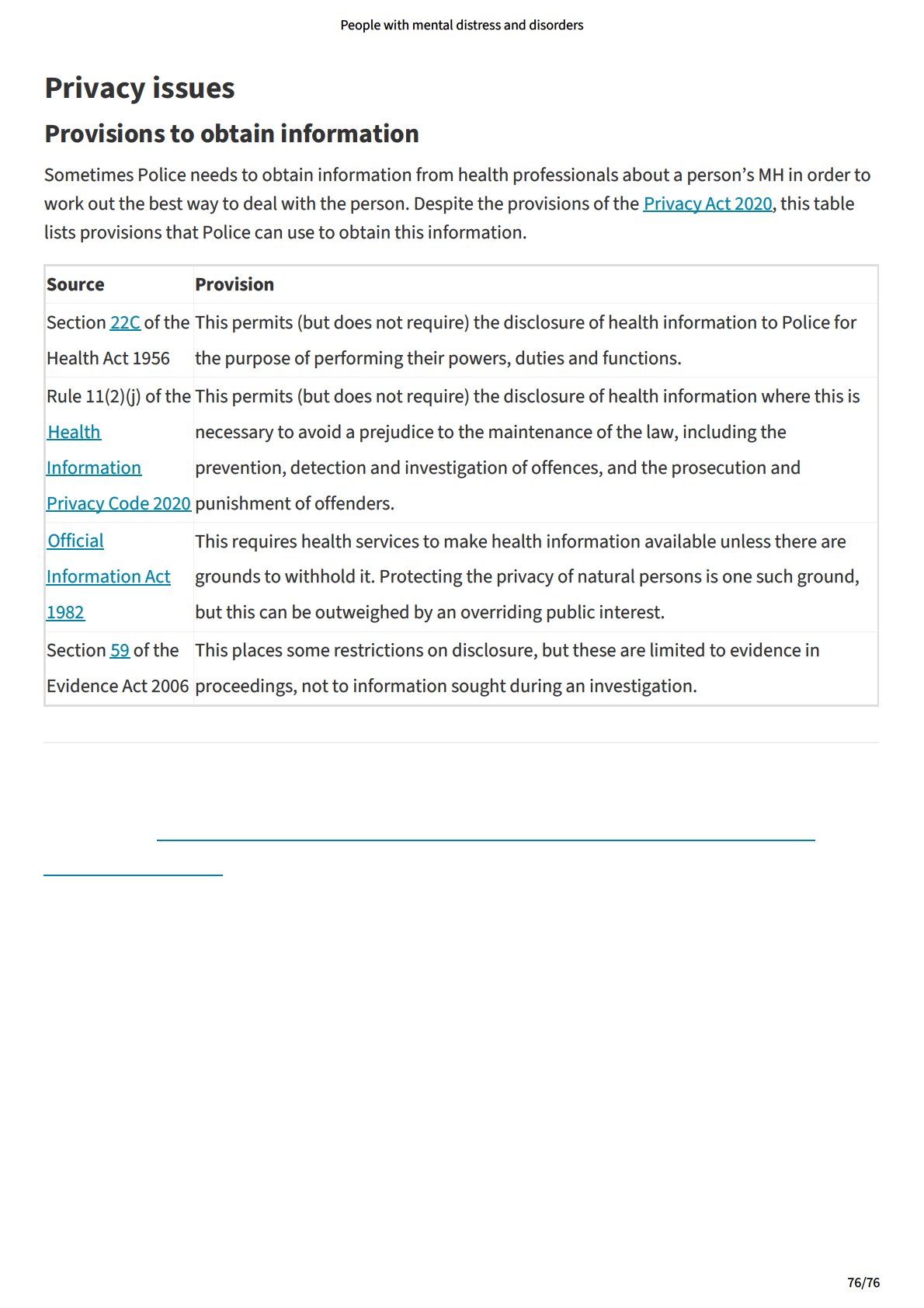
Privacy issues
76
Provisions to obtain information
76
link to page 2 link to page 2 link to page 2 link to page 2 link to page 2
People with mental distress and disorders
Policy statement and principles
What
Police is changing the way it responds to some mental health (MH) events. A four-phase change
programme wil :
- clarify Police’s roles and responsibilities
- ensure Police works within its statutory functions, and
- ensure people experiencing MH crises receive a health rather than a justice response wherever
possible (e.g., Police wil no longer attend low-risk MH events that are best responded to by other
agencies. Police wil continue to attend high-risk events per its standard operating procedures).
The Mental Health Response Change Programme (MHRCP) details the thresholds and criteria for Police's
involvement. The programme’s aim is to support Police’s focus on core policing functions, which means
Police wil only be involved where it identifies:
- an immediate serious risk to life or safety; or
- a criminal offence or activity that meets Police’s normal attendance threshold.
Further guidance and information about the MHRCP phases are provided in the MHRCP chapter of the
Police Manual. Each phase has a clearly set commencement date and wil be embargoed until that time.
More guidance and information wil be added to the MHRCP chapter as each phase comes into effect.
The People with mental distress and disorders chapter and the MHRCP chapter wil be merged once the
MHRCP is complete.
Phase 1 changes - effective from 4 November 2024:
- Voluntary handovers at ED
- Transportation requests from MH services
- Requests for Police attendance at Mental Health facilities
Phase Two went live as a national process on 16 June 2025:
- Handovers at Emergency Departments - Detained persons s109
- Handovers at Emergency Departments - Detained persons s41 and s110C
- Mental health Police custody rules changes
Why
MH distress is recognised as a significant driver of demand for Police. Research conducted in 2024 found
that 11% of al 111 cal s had a MH component and less than 5% of the MH events had an offence reported.
Although Police is available 24/7, it is not the best agency to provide support and care to people in
distress. There wil be times where Police is stil involved When handling those events, it is important to
remember that people who are experiencing mental distress and/or living with mental disorders are
particularly vulnerable. People with mental disorders are:
7/76
link to page 2
People with mental distress and disorders
- more likely to be discriminated against;
- more likely to be victims of crime; and
- experience poorer health outcomes.
Historical y, Police has been over-utilised during MH events to the extent that other agencies and the
community believe it is the norm and expect us to take the lead. Police’s involvement with MH matters
means people received a justice response for their health needs. Extensive feedback from lived
experience groups tel s us that Police involvement in MH matters is traumatising and detrimental to their
recovery.
How
The responsibility for providing services under the Mental Health (Compulsory Assessment and
Treatment) Act 1992 (MH (CAT) Act) rests primarily with the MH services. Police may assist in accordance
with the MH (CAT) Act and the MHRCP Manual Chapter sets new organisational rules that clarify its
involvement in MH matters.
Police recognises it has a specialist MH role. The threshold and criteria set by the MHRCP reflects this
specialist role and Police's need to focus on core policing functions. As such, Police wil only be involved
with MH events where Police identifies:
- an immediate serious risk to the life or safety of any person; or
- a criminal offence or activity that Police would normal y attend.
8/76
link to page 2 link to page 2
People with mental distress and disorders
Overview
Introduction
A health-led response is the preferred option for mental distress cal s for service and Police wil only be
involved where the threshold is met. The new MHRCP Manual Chapter has been developed to clarify the
parameters of Police’s role and support the graduated changes to its operational response. The Health
Partnerships Team at PNHQ works closely with Ministry of Health (Manatū Hauora) and Health New
Zealand (Te Whatu Ora) to ensure responses are health-led. In practice, this means Police wil attend only
where there is an immediate serious threat to life or safety.
Mental il ness is common and can severely impact people’s lives. The New Zealand Health Survey
2022/2023 found one in eight adults (11.9%) reported experiencing high or very high levels of
psychological distress. Research from the Mental Health Foundation NZ in 2022 found that nearly one in
four (23.6%) young people aged 15-24 years experienced high or very high levels of psychological
distress.
While mental distress is prevalent across communities, Police knows that its involvement is not the
answer. In 2024 a Marsden Fund-supported project entitled “Exploring the role of police in responding to
mental distress” was published. The report examined how a Prevention First approach is implemented
and experienced when Police officers respond to MH-related events. Consulting people with lived
experience of mental distress and Police staff resulted in an extensive analysis of different stakeholder
perspectives. Key findings of the report are:
- The significance of trauma: “Through the narratives shared by whānau/citizens, it became evident
that they attributed their experiences of mental distress to trauma. Trauma was described as the
result of multiple, severe, and sustained traumatic events, circumstances, or experiences that
occurred from childhood through to adulthood.”
- Humanistic approaches: “The study found that when frontline police of icers took a humanistic
approach, it resulted in a positive experience for many participants. Many of the of icers interviewed
described their approaches to mental health-related events as similar to the humanism participants
found helpful. Therefore, the study provides examples from both whānau/citizens and frontline police
of icers about what a humanistic response may look like and the consequences when it does not
happen.”
- New Zealand Police as default MH responders: “Content analysis of cal s to the Police Emergency
Communication Centres showed that frontline police of icers are being used as a primary and/or
default mental health and social support service. Many cal s, however, were assessed by the research
team as not necessarily requiring a police response and, instead, could have been supported through
a mental health or social service-led response.”
- Bias, racism and criminalisation: “there were examples of biased, racist, and discriminatory pre-
judgements (e.g., using the 1M code to label or describe a person in distress) of whānau/citizens,
which then shaped how frontline police of icers responded. A diverse police service was considered as
one way to reduce prejudgements.”
“Frontline police of icers expressed their concerns about the potential criminalisation and harm that
may arise from their use of cel s for detainment and their police powers in mental health-related
9/76
link to page 2
People with mental distress and disorders
events.”
The report also explored alternative ways of working and set out recommendations for Police.
Police contact with persons in mental distress
People with lived experience of mental distress may be referred to as Tāngata Whaiora - which means a
person seeking help. When officers interact with people in distress, their first contact should always be a
local MH team. Police must identify and understand what its role is in each event and seek advice and
guidance from MH teams. More information about Police’s MH roles and responsibilities can be found in
the MHRCP Manual Chapter.
People with a MH disorder have a significantly higher risk of becoming victims of violence than members
of the general population. As vulnerable members of the community, people experiencing mental
distress or disorders need to receive appropriate assessments, timely intervention and care, especial y if
they present a danger to themselves or others.
When interacting with people in mental distress, Police should:
- focus on mana enhancing interactions, ensuring the person's dignity and human rights are upheld
- liaise with other agencies, family/whānau/carers, and other social supports as they wil hold key
information and are often best placed to care for that person, including when the person may be
intoxicated
- utilise Prevention First - where appropriate, consider using Police discretion and alternative
resolutions when someone in mental distress is an offender. See Prevention First.
- ensure risk information is shared when passing a person into the care of a DAO. This includes
disclosing threats or words around suicidal intent or any other relevant risk.
Note: Recent coronial recommendations advise that al offences should stil be investigated, with
alternative resolutions offered where appropriate and relevant risk information around those offences
shared. See "Advising other agencies of offences"
It is also important to keep an open mind as to why people may be behaving differently. This could be
due to:
- physical condition (e.g., metabolic imbalance, diabetic hypoglycaemia, or infection);
- mental distress;
- intel ectual disability;
- brain injury or il ness;
- mental disorder.
10/76
link to page 2 link to page 2
People with mental distress and disorders
Police do not need to be concerned about a person’s unusual behaviour unless it involves an offence or
presents a serious danger, either to the person displaying the behaviour or others. The safety of the
person, Police officers, and personnel from other agencies and the community is paramount.
New thresholds for Police’s involvement with MH matters have been developed. These thresholds wil be
introduced in four phases that comprise Police’s Mental Health Response Change Programme.
Inform decision making by liaising with health services about planning and risk assessments. Using the
behaviour indicators may assist when you liaise with health services. Connecting with the local/District
Multiagency Teams and referring to NIA for Adult intervention plans may also be useful.
What this chapter covers
This chapter details:
- how to recognise behaviour indicators
- the legislation and procedures to fol ow when you deal with a person who is mental y disordered or
in distress. Procedures related to the MHRCP can be found MHRCP Manual Chapter
- the procedures to fol ow when a person in distress commits an offence.
For information, see the Intel ectual Disability (Compulsory Care and Rehabilitation) Act 2003.
Note: the terms mental distress and mental y disordered are used interchangeably throughout this
chapter. It should be noted that mental disorder has a legal definition a mental distress does not.
The new threshold - defining Police business
"Police wil always be involved where there is an offence (it would normal y attend) or an
immediate risk to life or safety."
A new risk threshold has been established to help identify what MH-related work belongs to Police. Only
matters that meet this threshold wil be considered a Police matter.
Police wil only attend MH events where it identifies:
- an immediate serious risk to life or safety of any person; or
- a criminal offence that Police would normal y attend as per its standard operating procedures.
Please refer to the MHRCP Manual Chapter for further information and guidance about Police's
thresholds and criteria for attending MH events.
11/76
link to page 2 link to page 2 link to page 2 link to page 2
People with mental distress and disorders
The use of TENR
The TENR operational threat assessment tool must be utilised to help staff assess the threat, exposure
and necessity to act, before, during and after incidents involving a person in mental distress or with a
mental disorder. TENR wil assist the decision whether Police needs to be involved. Where Police
involvement is required, use TENR to determine an appropriate Police response during and after the
incident). This wil help ensure that a person experiencing mental distress is dealt with lawful y and
safely, and that any response, including detention, is appropriate. Where appropriate, liaise with MH
agencies and organisations to inform the TENR. For more information see ‘Operational threat assessment
(TENR)’.
Prevention First
Police's Prevention First operating strategy requires that it considers the use of Police discretion and
alternative resolutions. When dealing with a person in mental distress, Prevention First means taking a
holistic approach to any offending and exploring opportunities to prevent re-offending. This may include
engaging with community health services. Where appropriate, attempt to resolve incidents involving
people in mental distress using a therapeutic response so that healthcare and treatment is provided to
the people who need it.
Staff Safety persons of interest
Tactical intel igence applies a proactive, prevention-focused approach to identify, analyse and prioritise
staff safety when dealing with persons of interest (SSPOIs) who likely pose a risk of physical harm to
People employees. Tactical Intel igence informs Police's risk assessments and operational planning,
including how it can best prioritise its resources to keep ourselves and the wider community safe. Police
wil always apply a tactical intel igence approach when delivering Our Business regardless of the person’s
MH status.
Legal definition and Police involvement
The MH (CAT) Act defines ‘Mental disorder’ as an abnormal state of mind (whether of a continuous or an
intermittent nature), characterised by delusions, or by disorders of mood or perception or volition or
cognition, of such a degree that it-
(a) poses a serious danger to the health or safety of that person or of others; or
(b) seriously diminishes the capacity of that person to take care of himself or herself.
Key words in the above definition are:
1. …poses a serious danger…, and
2. …seriously diminished capacity…to look after themselves.
Police are almost exclusively involved in the first part of the definition. The MH (CAT) Act defines the
police powers as being involved in the serious end of the spectrum, this includes when MH professionals
request Police assistance. For most requests under the MH (CAT) Act the MH Practitioner must form the
12/76
link to page 2 link to page 2
People with mental distress and disorders
view the person is mental y disordered. Accordingly, the role of Police is primarily to assist MH
professionals respond to people who present a serious danger (e.g., threat or risk) to themselves or
others.
Advising other agencies of offences
Offences should be investigated even if alternative resolutions are sought. When handing a person to
another agency for the purpose of a MH assessment, al relevant risk information pertaining to the offence
should be shared, including photos and notebook statements. Sharing relevant risk information wil help
the other agency’s decision making. For more information, refer to the ‘Prevention First strategy’.
Note: Police should only share photos of a person and their injuries if those images are needed to
support a MH assessment.
Recognising behaviours
When involved, it is important Police can describe the behaviours it is witnessing to help other agencies
understand the situation and provide support and care for the person in distress. At times, there may be
tension or disputes between agencies about behaviours of mental disorders and distress. This is common
when Police and other agencies respond to people with diagnosed personality disorders. The behaviours
that might seem alarming to us (like repeated threats of suicide) may be diagnosed as behavioural and
therefore not meet the criteria for MH services to support the person in need.
There is often disagreement between agencies when attention seeking behaviours are linked to suicidal
ideation. Police may assess this behaviour as life threatening, detain the person for assessment under the
MH (CAT) Act and transport them to ED, where a MH Practitioner determines the person does not meet the
criteria for further health treatment or support and releases the person back into the community.
To navigate some of these tensions, Police should use the behavioural descriptors listed below and
connect early with MH services for support on scene. Police should also consider previous behaviours
when deciding on the best response to people in distress. Research in 2024 (Crow’s Nest research) of 300
MH events found that 47% of cal s were from the individual and 65% of these described likely fictitious
offences. 25% were identified as frequent cal ers and 64% of frequent cal ers were likely to be clients of
MH services.
It is not the role of Police to diagnose MH conditions. However, identifying behaviour that might indicate
a person is in MH distress is helpful for creating a plan and when liaising with other agencies. Police
should be aware there may be other causes for behaviour, unrelated to MH distress, including:
- alcohol and drug use (including misuse of medications or interactions between them)
- physical disability or impairment
13/76
People with mental distress and disorders
- neurological impairment e.g. intel ectual disability, dementia, or acquired brain injuries, etc
- developmental disabilities e.g. autism spectrum disorder, foetal alcohol disorder, language/speech
disorders
- medical conditions e.g. diabetes, delirium, infection, dehydration (especial y in the elderly).
Behaviour
What this might look like
Imminent risk of
The person is threatening harm to themselves or others.
physical harm
Having suicidal thoughts does not necessarily equate to imminence, however it is a
risk factor that requires further assessment (see Suicide Risk section).
Delusions
The person is holding a belief that is false, yet the individual is convinced that it
is true. The person firmly believes in the delusion even when its demonstrably
false, such as believing:
- the TV is broadcasting messages just to them
- the CIA is spying on them
- they have been cloned.
Cultural and religious beliefs
Some persons may have a strongly held belief that is part of their cultural or religious
background. This is different from a delusion, which is a false belief. In these
situations, the person is convinced of its truth and there is no amount of evidence
that wil convince the person otherwise.
Hal ucinations
The person is perceiving things that are not real, such as:
- hearing voices that aren’t there
- seeing things that aren’t there
- feeling their skin crawl, without medical explanation.
Hal ucinations can occur in al senses, and include a perception of hearing, seeing,
touching, tasting and smel ing things that are not there.
Disordered
The person is exhibiting irregular speech patterns such as:
thought
- an inability to stay on subject
- rapid and/or pressured speech
- nonsensical speech
- speaking about topics that do not connect or do not have a point
- repetition or fixation on a particular point that signals an inability to
concentrate.
14/76
People with mental distress and disorders
Disturbance of:
The person is exhibiting behaviour, such as:
- orientation
- confusion
- memory
- paranoia
- perception.
- unrelenting irrational fear of particular persons, places or things
- fixation on particular things or topics
- being unsure of where they are.
Impulsivity or
A person is acting impulsively, without thought or consideration of
recklessness
consequences, and may appear to:
- rapidly change their mind
- be agitated
- demonstrate risky behaviours that may put the person in unsafe situations
(e.g., running through traffic without consideration for safety, reckless driving).
Unregulated or
The person is exhibiting unregulated or extreme emotions, such as:
extreme emotions
- an inability to calm themselves
- high levels of emotional distress
- volatility
- anger.
The person may also be exhibiting manic behaviours such as:
- elevated physiological arousal, elevated emotional arousal and frantic activity
level
- extreme emotional expression
- rapid changes in emotions
- a sense of invincibility or grandiosity.
Perception
The person may be saying things, such as:
of being a burden
- “The world would be better off without me”
isolation-
- “Nothing wil change or improve”
hopelessness.
- “No-one can understand or help”.
Hopelessness and helplessness are significant risk factors for suicide (see Suicide Risk
section).
While persons with MH issues are no more likely to be violent than anyone else, aggression and violence
may present when they:
15/76
link to page 2 link to page 2
People with mental distress and disorders
- have stopped using medication or are self-medicating with drugs/alcohol (or where the two are
interacting)
- act to protect themselves as a result of their delusions or hal ucinations.
Responding to people in mental distress
The MHRCP Manual Chapter includes more guidance and information on the Police response to MH
events. The MHRCP has four distinct phases that introduce Police's new MH framework in a graduated
way. It is important that Police's operational response is aligned with each scheduled phase of the
MHRCP.
When Police is involved in a MH event, the response should be person-centred, with a focus on respect
and empathy. Where appropriate, be responsive to the specific needs of the person’s social and cultural
context. Police should use calming and empathic verbal and non- verbal communication and reduce
environmental stress or triggers.
Verbal Communication
Communicating with people who are experiencing severe MH crises can be distressing and confusing for
the patient/person and chal enging for Police staff. The presence and impact of symptoms can create a
significant barrier to successful communication with the person. Communication with the person should
therefore be slow, clear, simple, and often repeated.
For the patient/person in distress, having Police respond to the event typical y aggravates their distress.
Police's simple and mere presence at the event can be traumatising for the patient/person. See the
Marsden Fund supported project “Exploring the role of police in responding to mental distress” for more
details.
16/76
link to page 2
People with mental distress and disorders
- Use neutral, non-biased language
- Ask short and simple
- Keep a slow and steady pace
questions, and al ow time
to respond
- Speak with a calm tone
- Use active listening e.g.
- Use appropriate volume - at times, you may need to raise your
paraphrase, mirror the
voice to be heard above environmental barriers. Should you
person’s words and avoid
need to do so, tel the person you need to raise your voice so
talking over the person
they can hear you, but you aren’t “yel ing” at them
- Repeat and rephrase
- Ask the person their name, and what name they would like to
messages
be cal ed
- At times, you may need to
- Emphasise the desire to help and keep them safe
repeat things often,
- Be genuine and truthful
particularly if the person is
- Avoid making promises that you cannot or do not intend to
experiencing symptoms of
keep
distress
- Acknowledge and respect how they are feeling - Don’t say “I
- Acknowledge the person’s
understand”, as it’s likely you cannot. Comments such as “It
experience, but do not
sounds like…”, “I can hear that…”, “It seems…” are more
argue about or reinforce
validating and supportive
delusions or hal ucinations
- Give short and simple
instructions, and avoid
jargon
- Seek permission to come
closer to the person before
approaching
- Meet them at the same
physical level, i.e. sit down,
kneel, etc.
- Consider the use of an
interpreter if there is a
language barrier.
If the person doesn’t engage, use the five AWOCA steps of tactical communication:
1Ask (make a direct request).
2Why (explain why you have made the request).
3Options (tel them what they can expect to gain or lose).
4Confirm (tel them what is required; make a confirming statement: “Is there anything I can reasonably
do or say to gain your cooperation?”).
5Action (use an appropriate tactical option based on TENR).
Non-Verbal Communication
17/76
link to page 2 link to page 2 link to page 2
People with mental distress and disorders
- Remain calm and be attentive.
- Be aware of facial expressions.
- Be aware of personal space. This may be influenced by
- Avoid touching the person.
factors such as culture.
- Avoid sudden movements.
- Be aware of body language e.g. adopt a non-
- Consider the appropriateness of
threatening stance. Standing side on rather than
eye contact. This may be influenced
directly face-to-face is less threatening.
by cultural factors
- Ensure that body language reflects what is being
communicated.
Reducing environmental stress
Being aware of potential environmental triggers may also assist Police in reducing stress for the person
experiencing mental distress. Environmental stimuli can often be overwhelming and overstimulating for
people already dealing with difficult symptoms. A highly stimulating environment can further aggravate
the situation and negatively impact communication. These techniques should be adapted within the
context of each incident.
- Disperse crowds.
- Provide space.
- Remove people or objects that upset the person.
- Reduce unnecessary distractions.
- Turn off sirens.
- Relocate the individual to a safe space.
- Lower radio volume.
Police wellbeing
Responding to any incident, in particular suicide, has the potential to impact the wel being of Police
employees. Dealing with people in distress and those with MH issues can be chal enging, frustrating, and
emotional y taxing. This can have a cumulative effect, and it may be particularly upsetting or triggering if
you, or someone close to you, have experienced MH concerns.
Police officers should be aware of their own and their col eagues’ wel being when attending such
incidents. Engage in self-care and, if necessary, use the range of support options available such as
Employee Assistance Programs, peer support, chaplains, or MH professionals. Officers should support
their col eagues by ‘checking in’ with those involved in incidents. They should assess how their
col eagues are coping and encourage them to seek assistance if needed. See Mental Health First Aid
training.
Responding to suicide risk
The fol owing guide may assist with communication and rapport if you are involved with a person
experiencing suicidal thoughts, attempting suicide or self-harming (also referred to as self-injury).
18/76
People with mental distress and disorders
Note - A previous non-fatal suicide attempt is the largest single factor indicating future suicide risk
and death by suicide. (Clinical Advisory Services Aotearoa)
A person can move from non-specific thoughts to action very quickly. While some plan for days or longer,
for others, ‘planning’ can occur in the space of moments or seconds. Moving from thoughts to action is
not necessarily linear or time-bound, and risk can fluctuate rapidly.
If the person has already taken action to attempt suicide by consuming large quantities of
medication, then the priority should be to seek immediate medical attention. A person will need to
be medically cleared before any MH assessment regardless of how much medication the person says
they have taken. These people should be transferred to ED or ambulance services as soon as
possible.
The following steps will assist Police to engage with a potentially suicidal person:
Establish
Ask the person what they are thinking and feeling.
rapport
- “How are you feeling?”
- “You seem distressed. Do you want to tel me about it?”
Tell the person you want to help. Give reassurance.
- “We want to get you some help.”
- “You are not in trouble.” (If this is the case)
Tell them your concerns about them, describing behaviours that have caused you to be
concerned about suicide.
- “We’re worried about your safety because…”
Encourage them to talk about their thoughts and feelings.
- “How are those thoughts making you feel?
Keep in mind it may be hard for those who are severely distressed to articulate how
they are thinking and feeling, as their thoughts and feelings may be overwhelming.
19/76
People with mental distress and disorders
Assess
Establish whether the person has thoughts of suicide. It is important to be clear and
suicidal
direct. Asking specific questions will not cause someone to act and is important to
obtain accurate information.
thoughts
and intent
- “Are you thinking about ending your life?”
- “Are you intending to end your life?”
Ask about their experiences with suicidal thinking. This will give you an idea of whether
they have made a previous attempt (strong risk factor), or how intense the thoughts
have been.
- “How long have you thought about suicide?”
- “Have you had thoughts like this before?”
- “What has changed today?”
Establish whether there is something contributing to their thoughts of suicide.
- “Is there something causing you pain that you want to stop?”
- "What’s brought you to this decision?”
Establish if they are experiencing a sense of isolation or hopelessness.
- “Look for statements such as “why bother”, “there’s no point”, “things wil never get
better”, “it wil always be like this”.
Be alert to the person using statements of last resort.
- “I want to die.”
- “Everyone would be better of without me.”
Do not ask if they are thinking of doing something “silly”.
Assess if a
Ask the person directly if they have made a suicide plan.
suicide
- “Do you have a plan for ending your life?”
plan is in
- “Have you thought about what you would use to end your life, or when?”
place
If it is established that the person has a plan, elicit details of the plan.
Be alert to the person “preparing” for a suicide attempt such as researching methods
online.
Where possible, remove potential means of suicide. Seek whānau support/inform
whānau friends/flatmates where needed to help with safety plans.
20/76
People with mental distress and disorders
Assess
Ascertain whether the person has access to means of suicide.
likelihood
- “Do you have access to what you would use to end your life?”
of action
- (i.e. have they stockpiled medication, bought rope)
- “Have you written any notes?”
- “Have you taken any steps in your plan?”
Establish whether they have taken action towards this plan, such as recently given
possessions away (including pets), prepared a will or prepared suicide notes.
Some persons may display a sense of calm or seem like their distress has been resolved.
Exhibiting a sense of calm does not mean a person is not at risk, it may mean that they
are comfortable with the decision to end their life.
Instil hope
Persons who attempt suicide may feel there is no hope for the future, and that others
would be better off without them.
The most important thing Police can do when a person is at risk of suicide is instil
hope but be careful about making promises.
- “There is help available and we want to make sure you get the support you need.”
- “It may not seem like it right now, but things can get better.”
Establish what helped the person in the past and use this information to reinforce that
they survived the previous experience, and therefore they can do so again.
- “What stopped you from going through with it before?”
- “What happened to turn things around?”
Connect the person and their family/whānau to professional health services at the
earliest opportunity and BEFORE you leave the incident. If suicide is likely, do not leave
them alone, for further information see releasing the person at risk into the care of
another.
Note: Police are encouraged to always be vigilant in these contexts as the greatest risk is at the start and
end of any intervention. Police staff should never place themselves at risk when engaging in an
intervention. Police staff should understand that some persons die by suicide despite Police and
other services taking appropriate actions and preventive measures.
21/76
link to page 2 link to page 2 link to page 2 link to page 2
People with mental distress and disorders
Submit a report
Officers should submit an incident report to their File Management Centre before the end of their shift,
outlining the facts and the action they have taken. They should make sure they have a NIA alert created to
identify the risk to al staff.
Submit Self Harm/Suicidal Tendency safety alert
If they are aware a person is experiencing suicidal thoughts, has a history of suicide attempts, or has
attempted suicide (whether in custody or not), they must enter a “Self-Harm/Suicidal Tendency” safety
alert into NIA.
If the person is in custody, the officer can create the flag from the Electronic Custody Module.
If the person is at large, the officer should cal their File Management Centre who wil load the alert for
them as part of the 1X occurrence. Where Districts do not have a 24/7 FMC and the matter is urgent,
officers should contact their local DCC.
Note: It is not uncommon for a person to have multiple "self-harm/suicidal tendency" safety alerts.
Please bring any examples to the attention of the multi-agency team or District MH Liaison officer who
may complete a safety alert "tidy up".
See: ‘People in Police detention’ in the Police Manual.
Risk factors for suicide
- Previous self-harm or suicide attempts
- MH history
- Involvement in the criminal justice system, particularly recent charges relating to family/whānau
harm or sexual assault (including sexual offending towards, around or involving children or young
people).
- Family/whānau or relationship problems
- Alcohol or drug abuse problems
- Disability or diagnoses of serious il ness
- Death or suicide of a family/whānau member or friend
- Financial problems
- Exposure to traumatic events
- Physical or sexual abuse
Groups at higher risk
- Māori people, in particular youth
22/76
link to page 2 link to page 2 link to page 2
People with mental distress and disorders
- Men are 3-4 times more likely to die by suicide than women
- LGBTQIA communities
- Current and former Police, emergency workers and military personnel
- Cultural y and linguistical y diverse communities
- People living in rural and remote communities
- Children and youth in care
Taking a suicidal person into custody
Suicidal persons should only be brought back to Police custody if they are violent, otherwise they should
be taken to ED.
Note: further operational guidance wil be provided here to coincide with Phase 2 of the MHRCP.
- Refer to the ‘Care and suicide prevention’ section in the ‘Arrest and detention’ chapter.
Supervising suicidal people in custody
- For information on supervising suicidal people who are in Police custody, see the ‘People in Police
custody’ chapter.
Self-harm
Just because a person is self-harming, does not mean there wil be a Police response. Police’s threshold
for attending much of this work wil change as part of the MHRCP. The bulk of the changes wil take effect
during Phase 4 (welfare checks), but smal er, gradual changes wil happen during earlier MHRCP phases.
To ensure Police handle self-harm matters consistently, employees should fol ow the guidance provided
for each phase. In practice, when Phase 4 takes effect, Police wil likely not attend many self-harm events
as most of these incidents wil not meet its attendance threshold. Should Police encounter persons who
are self-harming, they are not necessarily suicidal. Persons may self-harm for many reasons, for example:
- to manage painful feelings,
- to punish themselves,
- or to communicate with others.
These examples are referred to as Non-Suicidal Self Injury (NSSI).
Methods of self-harm could include:
- burning
- cutting
- scratching
23/76
link to page 2 link to page 2 link to page 2 link to page 2
People with mental distress and disorders
- ingestion of poison
- hitting your body on a hard surface
- re-opening existing wounds.
Police should be aware that people who self-harm are at risk of dying from their injuries, including
accidental y. They are also at higher risk of suicide. Health agencies must be contacted and should lead
the response to the person self-harming unless there is an immediate and serious risk to life and safety. It
should be noted that MH services might classify chronic NSSI behaviour as a tolerated risk. In that case
you cannot detain the person for their behaviour alone. Police should depart after communicating with
the person about any suicidal ideation/tendencies and providing advice.
Releasing the person-at-risk into the care of another
Releasing into the care of others
If MH services are involved, Police should speak with them before releasing the person into the care of
another. If there is a Multi-Agency Team in the district, Police can seek advice from them.
If the MH services decline involvement, but Police’s assessment is that a resolution or further support is
needed, then Police should consider taking the person to a carer.
Police must only release the person-at-risk into the care of another person (the carer) when they are sure
the carer is properly informed about how to deal with the person, is able to do so, and agrees to do so.
If the carer feels unable or they are unwil ing to care for the person, Police should take the person in
distress to a safe place, with al the information to contact relevant support lines (see below) and contact
MH services to advise of Police’s final action.
Information for the carer
There can be risk when transferring the care of people-at-risk.
The carer must agree to the transfer of care and Police should provide al relevant information about the
event.
The carer can get help from their family/whānau doctor, a community MH service, a Māori community
health service, or a phone counsel ing service such as LifeLine, Samaritans or Youthline, or the Mental
Health Foundation.
Police should give advice about removing risks from the home, for example (e.g., ropes, guns,
medications, and chemicals) and emphasise to the carer that a previous suicide attempt is a key risk
factor in further attempts.
Resolutions for mental health events
Police may pursue a number of possible outcomes in incidents involving a person experiencing MH
distress. Prevention First requires al staff to consider the use of Police discretion and alternative
24/76
link to page 2 link to page 2
People with mental distress and disorders
resolutions, where appropriate.
Possible options that Police may take include:
- leaving the person in the care of others (e.g., family/whānau and friends)
- referring the person to a MH service or another appropriate agency for fol ow up
- transferring responsibility for the care of the person to another appropriate agency present at the
incident, with no further Police involvement required (e.g., ambulance)
- transporting the person to a health facility for a MH assessment, as described by the MH (CAT) Act
- criminal justice response (e.g., arrest, report, summons, or caution/warning), where Police
considers the person has committed an offence.
Note - the preference when responding to people
in distress is to explore al other available options first and take a criminal justice response as a last
resort.
- undertaking no action.
See “Advising other agencies of offences”
Co-Response Teams (CRTs) or sometimes called Multi Agency Teams
Many Multi Agency Teams (MAT) offer expertise and advice to assist with MH-related cal s for service.
Working closely with Police’s partner organisations, MAT can share information and gain a better
understanding of normal risk patterns and chronic behaviour.
Access to health details and other relevant information can ensure Police link people into the most
appropriate agencies, creating timely access to the correct pathway (e.g. community MH teams, social
workers, Māori support services).
If the Police district has access to a MAT, then utilise this service at the earliest opportunity for every MH-
related event.
Frequent callers/high-needs users
People with chronic MH needs may become frequent cal ers. Police can sometimes tailor its response to
their cal s. Police are unlikely to be the only service they are frequently contacting, and working with its
partner agencies wil ensure a consistent approach is taken and the most appropriate services respond to
the cal s.
Police wil only be involved with frequent cal ers / high-needs users if the “immediate serious risk or
offence” threshold is met. Consider the person’s previous behaviours when deciding on the best response
to frequent cal ers. Research in 2024 of 300 MH events found that 47% of cal s were from the individual
and 65% included likely fictious offences. 25% were identified as a frequent cal er and 64% of frequent
cal ers were likely to be clients of MH services.
Identifying these people and working with them, their support networks and other agencies can result in
positive outcomes and reduced cal s for service. This can be achieved through District interagency
meetings. If the Police district has a MAT, the MAT should lead the process and create an adult
25/76
link to page 2 link to page 2 link to page 3
People with mental distress and disorders
intervention plan. Check the relevant District MOU/SLA for more details.
Adult intervention plans on NIA
Adult Intervention Plans (AIP) are created by Police and saved in NIA. They are a valuable resource, often
offering guidance from the individual’s MH team. General health information should not be retained as a
matter of course. However, there wil be times where the individuals’ MH information is relevant for
policing purposes. This may include information about chronic behaviour, normal risk patterns,
recommended strategies when interacting with the person such as topics to discuss or avoid, and
boundaries that might be useful. The AIP might also include alternative outcomes for people cal ing 111
or 105, including a community MH team or family/whānau being the first contact before a Police
response.
MH services cannot provide ful details of an individual’s management plan (unless permitted under the
Health Information Privacy Code). Nevertheless, MH services should inform Police as a matter of course
where their planned approach includes declining to admit a person to their services. Where permitted,
MH service should advise Police of other recommended actions to take if a person comes to Police's
attention again. This approach is often taken for people with diagnosed personality disorders and
requires a careful y designed behavioural plan. Odd behaviours that are commonly associated with
personality disorders may not warrant a ‘medical’ intervention. AIPs may therefore recommend a person
with a personality disorder is not taken or admitted to hospital even though they appear to be
experiencing a MH crisis. See ‘Privacy issues’.
If Police is considering creating an AIP, and there is a Multi Agency Team in the Police district, it is
preferred that they create the AIP as they wil have the most relevant and up-to-date information.
For more information and an example of an AIP, see NIA Enhancement 11.0 “Adult Intervention Portfolio”
Details for Youth Management Plans should be viewed under their youth profile within NIA. These details
are owned by the District Youth Aid staff.
Fear of Police
Many people experiencing MH distress have had negative experiences with Police or the MH system.
Police intervention may feel punitive and demeaning, therefore Police should prioritise the person’s
dignity and safety. Remember that merely having Police present at the event can be traumatic for people.
See the Marsden Fund supported project “Exploring the role of police in responding to mental distress”
for more details.
Bias
Police officers bring their own experience, attitudes, and biases with them to work. Police attitudes or
biases can have detrimental outcomes for people Police is interacting with. It is important Police
employee are aware of their own attitudes when interacting with people in mental distress, as these can
result in unfair treatment, discredit their lived experience, and create or reinforce stereotypes. Police
26/76
link to page 3 link to page 3 link to page 3
People with mental distress and disorders
employees must interact in mana enhancing ways especial y with those who have cal ed previously or
frequently. Keeping an open mind and being curious about situations can help reduce discrimination and
stigma for people experiencing mental distress. It is important to ensure there are no negative biases
created with the use of MH flags within NIA. Language is also important, and Police should not refer to
people as “1M” or “1X” or “frequent fliers”.
People with lived experience of mental distress may be referred to as Tāngata Whaiora - which means a
person seeking help.
See the Marsden Fund supported project “Exploring the role of police in responding to mental distress”
and “Understanding Policing Delivery” report for more details.
Mental Health categorisations and data quality
The correct classification of MH-related cal s for service al ows for improved analysis and understanding
of Police demand. Police should only attend MH cal s for service when there is an immediate serious
threat to life or personal safety. Accurate recording and data col ation is imperative, particularly the
classification of 1M, which is often used as a catch-al for cal s for service that have no obvious crime or
traffic involvement. Communications centres are Police’s business owner for the MH-related codes. The
relevant codes are defined in SOPs as:
- 1M - mental health; and
- 1X - threatens/attempts suicide.
Where a handover of a voluntary or detained person to an ED occurs, the handover form should be used.
Mental health flags
MH flags in NIA need to be accurate, helpful and should focus on risk. These flags can create or reinforce
bias among readers. Police should consider removing a flag if it is historic or no longer relevant /
accurate. If Police decide a NIA flag is needed, also consider the need for an adult intervention plan.
Further guidance is available in the Contributing Factors PowerPoint. MH is a contributing factor and
should be flagged if:
- the subject, victim or offender has MH issues, and this was a factor in the event
- misuse of medication has contributed to the event (this includes when a person stops taking their
medication, contrary to professional advice)
- the subject or victim is experiencing mental distress, and this is a contributing factor to the event.
Use of K1
With the implementation of the MHRCP, where it is determined that Police need to be involved, it is
important that it accurately col ects, col ates, and reports its MH data. Therefore, the use of K1 as a result
code for MH events is discouraged. Any persons taken to ED for a MH assessment, voluntarily or under
s109 MH(CAT) should be resulted as K6 and recorded. The result “Police attendance sufficient” (K1) in
27/76
People with mental distress and disorders
CARD should only be used if you do not wish to create a report in NIA and no Occurrence is required. See
National Recording Standard.
Note: Police should record and report al incidents and interactions with people in mental distress,
sharing these with local community MH teams. Reporting should be completed by phone where possible.
However, email reporting is appropriate if it takes a long time for the community MH team to answer and
you assess the matter is not urgent. Community MH Teams are often unaware when their clients are
contacting Police and sharing information al ows agencies to identify and appropriately manage patterns
of behaviour. This is important as seemingly trivial interactions may indicate a deviation from a person’s
baseline health (e.g., the person has become fixated on the colour of their socks, which could point to a
looming MH crisis).
28/76
link to page 3 link to page 3
People with mental distress and disorders
Relevant legislation
There are two principal Acts that govern Police’s interactions with people who present with mental
distress and disorders:
1. Mental Health (Compulsory Assessment and Treatment) Act 1992 (MH (CAT) Act). This applies
primarily to people with a diagnosed or apparent mental disorder where their mental condition
poses a threat to the health or safety of themselves or others, or seriously diminishes their capacity
to look after themselves, requiring professional MH intervention.
2. Criminal Procedure (Mental y Impaired Persons) Act 2003. This applies to people with an
intel ectual disability who are charged with, or convicted of, an offence. This Act gives the courts
appropriate options for their compulsory care and rehabilitation.
Note: 'Mental impairment' is not defined in legislation. High Court case law defines 'mental impairment'
as including a mental disorder or intel ectual disability, and also other mental or psychological disorders
such as degenerative neurological conditions, substance abuse or acquired brain injury, low intel igence
or impaired cognition (refer R v H [2014] NZHC 1423).
Click here for information on the Intel ectual Disability (Compulsory Care and Rehabilitation) Act 2003.
This covers people with an intel ectual disability who are charged with, or convicted of, an offence. This
Act gives the courts appropriate options for their compulsory care and rehabilitation.
For mental y impaired offenders - see ‘Criminal Procedures’
Memorandum of Understanding
As Schedule One of the MOU has been jointly withdrawn from, local Memoranda of Understanding (MOUs)
and Service Level Agreements (SLAs) that fal from this are no longer valid and wil be rewritten in the
months ahead.
Despite Schedule One being withdrawn from, there wil be a new MOU written between Police and The
Ministry of Health which wil replace al previous District Health Board MOUs. The new MOU wil
incorporate schedules with Health New Zealand (MH Services and Emergency Departments) and
Ambulance Services. These schedules wil clearly define each agency’s responsibilities and al ow for
appendices to incorporate operational policies and procedures that align with the changes to Police’s
response to MH events.
29/76
link to page 3 link to page 3 link to page 3 link to page 3 link to page 3
People with mental distress and disorders
Mental Health (Compulsory Assessment and Treatment) Act
1992
Police can act alone pursuant to three sections of the Mental Health (Compulsory Assessment and
Treatment) Act 1992 (the MH (CAT) Act),
Sections 109, 32 and 53. Al other Police activity under the MH
(CAT) Act occurs as a consequence of engagement with MH partners and where the threshold for Police
involvement is met.
Note: The MH (CAT) Act is under reform and significant changes are due in 2026. These reforms wil
prioritise a rights-based approach and eliminate or least reduce seclusion and restraint.
Roles and responsibilities of clinicians
Note: How Police respond to requests from MH Practitioners under the MH (CAT) Act wil not change until
Phase 3 of the MHRCP.
Directors of Area Mental Health Services (DAMHS)
DAMHS are highly qualified and experienced MH professionals appointed by the Director-General of
Health. DAMHS powers and responsibilities relate to administering the MH (CAT) Act in a specified area.
The DAMHS oversee the MH services and Duly Authorised Officers provide operational response within
each area.
Duly Authorised Officer (DAOs)
DAOs may cal for Police assistance under the MH (CAT) Act, sections 38, 40 & 41.
DAOs are health professionals designated and authorised by a DAMHS to perform certain functions and
use certain powers under the Act. DAOs respond to concerns about a person’s MH. They may arrange for
the assessment and treatment of people with MH problems.
Mental Health Practitioner
MH Practitioners may cal for Police assistance under the MH (CAT) Act, section 110.
Fol owing the Mental Health (Compulsory Assessment and Treatment) Amendment Act 2021, the term
‘mental health practitioner’ replaced ‘medical practitioner’ in certain sections of the MH (CAT) Act. Mental
Health Practitioner is defined in section 2 of the Act as:
30/76
link to page 3 link to page 3
People with mental distress and disorders
- a medical practitioner
- a nurse practitioner or
- a registered nurse practising in MH (which is also defined in section 2 of the Act)
If requested, a MH Practitioner may issue a certificate if they have reasonable ground to believe a person
is suffering a mental disorder.
DAOs and/or MH Practitioners may ask Police to assist them to:
- enter private property in order to establish if a MH assessment is required
- transport a person to a place of assessment or treatment
- detain a person at that place or another for assessment.
Assessment or treatment should take place in the most appropriate and least restrictive setting.
Sometimes assessment and/or treatment can take place in the person’s own home. A health facility
should be the first choice if the person is moved from their location. A Police station is the last resort and
should be used only if no other option is available.
Police’s role under the Mental Health (Compulsory Assessment and
Treatment) Act 1992
Note: How Police respond to requests from MH Practitioner’s under the MH (CAT) Act wil not change until
Phase 3 of the MHRCP.
Provision of services under the MH (CAT) Act rests with the MH services. Police provide assistance to MH
services in accordance with the Act. Remember that Police assistance with MH events is discretionary as
within the Act many sections say Police “may” provide assistance.
Rights-based approach
A rights-based approach to MH means Tāngata Whaiora (person seeking help) should be involved in
decisions that affect them, including decisions about their treatment and care.
New Zealand has signed the fol owing international conventions, which require a rights-based approach:
- Declaration on the Rights of Indigenous People (UNDRIP)
- United Nations Convention on the Rights of Persons with Disabilities
- United Nations Convention Against Torture and Other Cruel, Inhuman or Degrading Treatment or
Punishment (the Convention Against Torture)
- United Nations Convention on the Rights of the Child (UNCROC)
Compulsory treatment does not mean that Tāngata Whaiora lose their human rights. Rather, decisions
31/76
link to page 3 link to page 3 link to page 3
People with mental distress and disorders
about compulsory treatment require the clinician to balance an individual’s rights against the need for
coercive interventions permitted under the MH (CAT) Act.
Advance directives
Advance directives are documents or recorded statements that are developed when a person has
capacity to make decisions, and they outline the person’s preferences for situations if they need
treatment in the future. The Code of Health and Disability Services Consumers' Rights, (right 7 point 5),
provides that every health consumer may write an advance directive. Police and health services should
consider the instructions in an advance directive. (e.g., who looks after a person’s children when they are
unwel ).
People with a mental disorder (as defined by the Act)
The MH (CAT) Act provides for the assessment, treatment and care of people who have, or are suspected
of having, a mental disorder. The MH (CAT) Act also outlines the person’s rights.
The MH (CAT) Act details Police powers and duties when they may:
- assist health authorities;
- find a mental y disordered person wandering at large; or
- retake a patient who is absent without leave from a hospital.
Definition of mental disorder
‘Mental disorder’ is defined in the MH (CAT) Act to mean a person is in an abnormal state of mind
(continuous or intermittent) who may be delusional, or their mood or perception may be such that it
poses a serious danger to the health and safety of that person or others, or seriously diminishes the
capacity of such persons to look after themselves.
Key words in the above definition are:
- “…poses a serious danger…”, and
- “…seriously diminished capacity…to look after themselves.”
Therefore, a number of persons that Police likely come into contact with, and they perceive as mental y
disordered, do not meet the legislative definition of mental y disordered. E.g., a person acting erratical y
in a public place but otherwise functioning.
At times, a person with a personality disorder wil display behaviour or mood changes that fal within the
scope of the MH (CAT) Act. There are other times where their behaviour won’t meet that threshold, and
these instances can be frustrating for Police. Police should ensure it discusses the next steps with the MH
team as they may offer a solution when Police come into contact with such a person.
See Legal definition and Police involvement
32/76
link to page 3 link to page 3 link to page 3 link to page 3
People with mental distress and disorders
‘Mental disorder’ does not include
Section 4 of the MH (CAT) Act provides that the Act’s compulsory assessment and treatment procedures
may not be invoked simply because of a person’s:
- political, religious or cultural beliefs
- sexual preferences
- criminal or delinquent behaviour
- substance abuse - Substance Addiction (Compulsory Assessment and Treatment Act) 2017 (SACAT)
- intel ectual disability.
Assessment and treatment procedure
The Act sets out procedures for assessment and, if necessary, treatment of persons who are assessed to
have mental disorders. The procedure involves the MH service and the courts. Police may decide to
provide assistance when requested under the Act.
Role of the DAO, responsible clinician and the court
Anyone who believes that a person may be suffering from a mental disorder can ask a DAO for assistance
(section 8, 8A). The DAO is required to investigate and decide whether or not the person needs to have a
medical examination, and if so, whether this is required urgently.
The DAO must arrange for a MH Practitioner to examine the person. There may be several assessments
over a period of days and if the MH Practitioner believes there are reasonable grounds for believing the
person is suffering from a mental disorder they can be certified for compulsory assessment, and a
responsible clinician (usual y a psychiatrist or doctor) must carry out a further examination.
If found to be mental y disordered, the person can ultimately be compel ed, by order of the Court (either
through a community treatment order or inpatient order) to undergo treatment as long as that person’s
mental disorder continues (section 28 (1) of the MH (CAT) Act refers). See Compulsory assessment and
treatment procedure.
Who to call
When interacting with a person in distress, Police should contact its local MH team(s). Lists of appropriate
contacts are on Checkpoint, in the Communications Centres and in custody units of al Police stations.
Difficulties contacting the health authorities should be reported to a Police supervisor or District
Command Centre for liaison with local health authorities.
Consider registering the event in RIOD for fol ow-up by the District MH Lead.
If the cal has come to Police from another service and the officer does not believe it meets the new
threshold for attendance, they should fol ow the guidelines discussed in the MHRCP Manual Chapter and
discuss with their local DCC to determine if attendance is required.
33/76
link to page 3 link to page 3 link to page 3
People with mental distress and disorders
Criminal behaviour
It is common for Police to attend a MH-related event involving offending by a person who appears
mental y disordered. Police should deal with offenders who appear mental y disordered or distressed in
the same way as any other offender. Although there is a focus on Prevention First, al offences must be
recorded in accordance with the NRS and appropriately investigated. Where there are lawful grounds to
do so, al relevant recorded details and risk assessments should be shared with appropriate agencies.
These details may help inform any MH service response to that particular incident.
See “Advising other agencies of offences”
Duty to respect cultural identity
When exercising any power under the MH (CAT) Act, Police must have:
- proper recognition of the importance and significance to the person of the person’s ties with their
family/whānau, hapu, iwi and family/whānau group, and
- proper recognition of the contribution those ties make to the person’s wel -being, and
- proper respect for the person’s cultural and ethnic identity, language, and religious or ethical
beliefs.
See: Section 5 of the MH (CAT) Act.
Duty to provide an interpreter
If. . .
and. . .
and. . .
then. . .
Police is exercising
- the first or preferred
it is practicable to
Police must ensure that:
language of the person is a
any power under
language other than
provide the services
- the services of an
interpreter are
the MH (CAT) Act
English, or
of an interpreter,
provided for the
- the person is unable,
person, and
because of physical
disability, to understand
- as far as reasonably
English;
practicable, the
interpreter provided is
competent.
See: Section 6 of the MH (CAT) Act.
34/76
link to page 3 link to page 3 link to page 3 link to page 3 link to page 3 link to page 3
People with mental distress and disorders
Compulsory assessment and treatment procedure
If a person needs help for mental distress or disorder but doesn’t agree they need help, and hasn’t been
detained by Police under section 109, then Police can ask their local MH services to assess the person
under the Mental Health (Compulsory Assessment and Treatment) Act 1992 (MH (CAT) Act). If the
assessments indicate that the person needs compulsory treatment for the initial period of treatment, the
MH Service can apply to the Family Court for an order for compulsory treatment.
Application for an assessment
Any person can apply to have another person assessed (8A) under the MH (CAT) Act.
Note: Police is not routinely involved with assessment applications. Wherever possible, this should be left
to family/whānau and health professionals. Family/whānau should be advised to speak to their local MH
service before completing an 8A application. The local MH service can advise if an application is
warranted.
Compulsory Treatment Orders
A Compulsory Treatment Order is when a court orders that a person with a MH disorder must receive
treatment for up to 6 months. The person doesn’t necessarily need to stay in hospital for the treatment.
Community Treatment Order
The patient receives treatment in their own home or at some other place stated in the Order.
Inpatient Order
Under an Inpatient Order, a person must stay at the hospital stated in the Order to receive treatment.
Note: Treatment does not just include medication. It can also cover rehabilitation programmes,
education programmes, counsel ing and discussion groups. But these must be related to the mental
disorder.
If the person commits an offence
A compulsory treatment order ceases to have effect if the person is sentenced to detention in a prison.
(section 36 (2) (b)).
35/76
link to page 3
People with mental distress and disorders
A compulsory treatment order also ceases to have effect if the person is found unfit to stand trial, found
not guilty on the grounds of insanity, or convicted and ordered to be detained in a hospital or secure
facility or prison. The provisions of the Criminal Procedure (Mental y Impaired Persons) Act 2003 would
then apply.
Reducing and eliminating seclusion and restraint - Health guideline
changes
Manatū Hauora (Ministry of Health) have released guidelines for health staff focused on reducing and
eliminating seclusion and restraint under the MH (CAT) Act. There is a strong emphasis on person-centred
and cultural y appropriate approaches to safely reduce the use of seclusion and restraint within MH
facilities. This should see a reduction in the use of Police cel s for MH assessments, where there are no
immediate serious safety concerns. See “Rights based approach”
36/76
link to page 3 link to page 3 link to page 3
People with mental distress and disorders
Powers to assist Duly Authorised Officers
Note: How Police respond to requests from Duly Authorised Officers under the MH (CAT) Act wil not
change until Phase 3 of the MHRCP.
Authority
Police has legal powers under section 41 of the Mental Health (Compulsory Assessment and Treatment)
Act 1992 (MH (CAT) Act) to assist DAOs.
When a Police officer may assist
An officer may assist a DAO to do (or attempt to do) any of these three things.
37/76
link to page 3
People with mental distress and disorders
When a Police officer may assist a DAO
What you can do
If a person is believed to have a mental
If an officer is helping a DAO to have a medical
disorder and needs a medical examination
practitioner examine a person, they:
urgently, Police may help the DAO to effect
- may enter the premises where the person is, and
section 38(4)(b) of the MH (CAT) Act (e.g.
- must produce identification/evidence that they
are a Police constable if not in uniform
enable a medical practitioner to examine the
- may detain the person for up to six hours or the
person).
time it takes to complete the medical examination,
whichever is shorter.
Section 41(2) & (3) of the MH (CAT) Act refers.
If the person must go to the MH Practitioner for If an officer is helping a DAO to take a person to a MH
the examination but is unwil ing to go, an
Practitioner to be examined, they:
officer can help the DAO to take the person and
ensure that he or she is examined.
- may enter the premises where the person is, and
- must produce identification/evidence that they
Section 38(4)(d) of the MH (CAT) Act refers.
are a Police constable if not in uniform
- may take the person to the place of the medical
examination and detain the person there for up to
six hours or the time it takes to complete the
medical examination, whichever is shorter.
Section 41(2) & (4) of the MH (CAT) Act refers.
An officer can also help a DAO take al
If an officer is helping a DAO take or return a person to a
reasonable steps to take or return proposed
place of assessment or treatment, they:
patients and patients to places of assessment
or treatment if they are refusing to attend or
- may enter the premises where the person is, and
are absent without leave.
- must produce identification/evidence that they
are a Police constable if not in uniform
Section 40(2) of the MH (CAT) Act refers.
- may take the person to the place they are
required to attend and detain the person there for
up to six hours or the time it takes to conduct the
assessment, examination, review or treatment that
the person was refusing to attend for, whichever is
the shorter, or
- may take the patient back to the hospital.
Section 41(2), (5) & (6) of the MH (CAT) Act refers.
Warrant required
Under section 41(7) of the MH (CAT) Act, Police must not exercise its powers to enter without a warrant if
38/76
link to page 3 link to page 3 link to page 3 link to page 3
People with mental distress and disorders
it would be reasonably practicable to obtain one.
No documentation other than the warrant is required
Two warrants are required. First, a warrant to Take the patient or proposed patient, which needs to be
obtained by the Director of Area MH Services.
Second, a warrant
To Enter Premises, which a Constable needs to apply for and obtain. The Police
constable must sign the application and swear an affidavit. Section 113A of the MH (CAT) Act refers.
The warrant application wil need to be created by staff, and the Warrant itself needs to be in the form
prescribed by Manatū Hauora - the Ministry of Health.
See the Ministry of Health web site MH (CAT) Act forms | Ministry of Health NZ for the Section 113A
Warrant to enter, approved Warrant.
The two warrants wil be the only documentation required.
Location for patient assessment
The preferred action is to have a MH Practitioner assess the person in the person’s home. If this cannot be
done the DAO should take the person to another place, ideal y a health setting. As a final resort, where the
person is violent (e.g., in the assaultive range of the tactical options framework or higher) and only when
al other options are exhausted, should a police station be used as a place for assessment. Requests to
assess patients in Police cel s should be refused where there is no serious immediate risk to life or safety.
If MH services dispute Police’s decision, the officer should escalate the dispute to their DCC for guidance
and resolution.
For details on transporting people, see ‘Transporting people’.
Note: Further changes to the Location for patient assessment section wil take effect when Phase 2 of the
MHRCP commences.
If a constable is not in uniform
Under section 41(2)(b) of the MH (CAT) Act, if a Police constable is not in uniform when exercising their
powers to assist a DAO, they must produce to the occupier their identification card as evidence that they
are a Police constable.
Arrest provisions apply
Under Section 122A of the MH (CAT) Act, sections 30, 31 and 34 of the Crimes Act 1961 apply to Police’s
power to take and detain as if it were a power of arrest, with any necessary modifications. Specifical y:
39/76
link to page 3 link to page 4

link to page 4 link to page 4 link to page 4
link to page 4 link to page 4 link to page 4 link to page 4
People with mental distress and disorders
appropriateness of the actions requested and tel the health professional if they are proposing Police act
outside its powers or ability.
Check credentials
If a DAO asks for Police assistance, Police should check the credentials of the DAO.
Check the certificate
If a DAO asks Police to help them to take or return a patient to an assessment or treatment place (if the
patient is refusing to attend or is absent without leave), Police should ask to see a copy of the relevant
assessment certificate or compulsory treatment order, that directs the taking/returning of the patient.
Using force to transport the person (Section 122B)
Note: How Police responds to requests for transportation wil change when Phase 1 of the MHRCP
commences. Changes to MH services requests for Police assistance do not take effect until Phase 3 of the
MHRCP.
When a person must go to a MH Practitioner for an examination but is unwil ing to go, there are limited
provisions for Police to use force to transport the person. These provisions are set out in section 122B of
the MH (CAT) Act.
When a proposed patient or patient is refusing to attend an assessment or treatment place or is absent
without leave, Police can use force only if there is an emergency and only as is reasonably necessary in
the circumstances. A warrant may be needed under Section 113A.
If the person is being transported to attend for assessment and treatment under section 9, 11 or 13 of the
MH (CAT) Act, Police should ensure a health professional has issued a notice under the relevant section
and this has been explained to the patient. The notice should state the reason for the assessment
examination, the time and place of the assessment and the person who wil perform it. The person cannot
be moved without this notice and force cannot be used to enable transport without this.
Force should be reported in line with the “Reporting use of force/tactical options use” section in the Use
of Force manual chapter.
See: ‘Use of force’ chapter. For further information on transporting and restraining a person, see
‘Transporting people’ and ‘Restraining people’.
Positional asphyxia risk factors
Positional asphyxia arises when any person, due to their body position, is unable to breathe sufficiently to
43/76
link to page 4 link to page 4 link to page 4
People with mental distress and disorders
meet their body’s requirements.
See the ‘Positional asphyxia’ chapter.
Responsibility for damage caused by force
Police should not use force unless:
- the DAO has been informed and has accepted responsibility for the damage caused by force used
to gain entry and has asked Police to continue.
Six-hour detention limit
Police should not detain a person for longer than six hours. If they have not been seen by a medical
professional within this timeframe, they cannot be detained for any longer.
Note: there may be exceptions to the 6-hour limit, where the person is being held in custody after being
charged with an offence. A second common exception is when a person is seen within 6 hours, but the
assessment process takes longer than the initial 6-hour period.
Bill of Rights
If Police detains a person, Police must comply with the requirements of the New Zealand Bil of Rights Act
1990. See “rights-based approach section”.
44/76
link to page 4 link to page 4 link to page 4
People with mental distress and disorders
Assisting a Mental Health Practitioner
Note: How Police responds to requests from MH Practitioner’s under the MH (CAT) Act wil not change
until Phase 3 of the MHRCP.
Authority
Police’s powers to assist a MH Practitioner are contained in section 110C of the Mental Health
(Compulsory Assessment and Treatment) Act 1992 (MH (CAT) Act).
When you can assist
Police can help a MH Practitioner do any of these things.
45/76
link to page 4 link to page 4
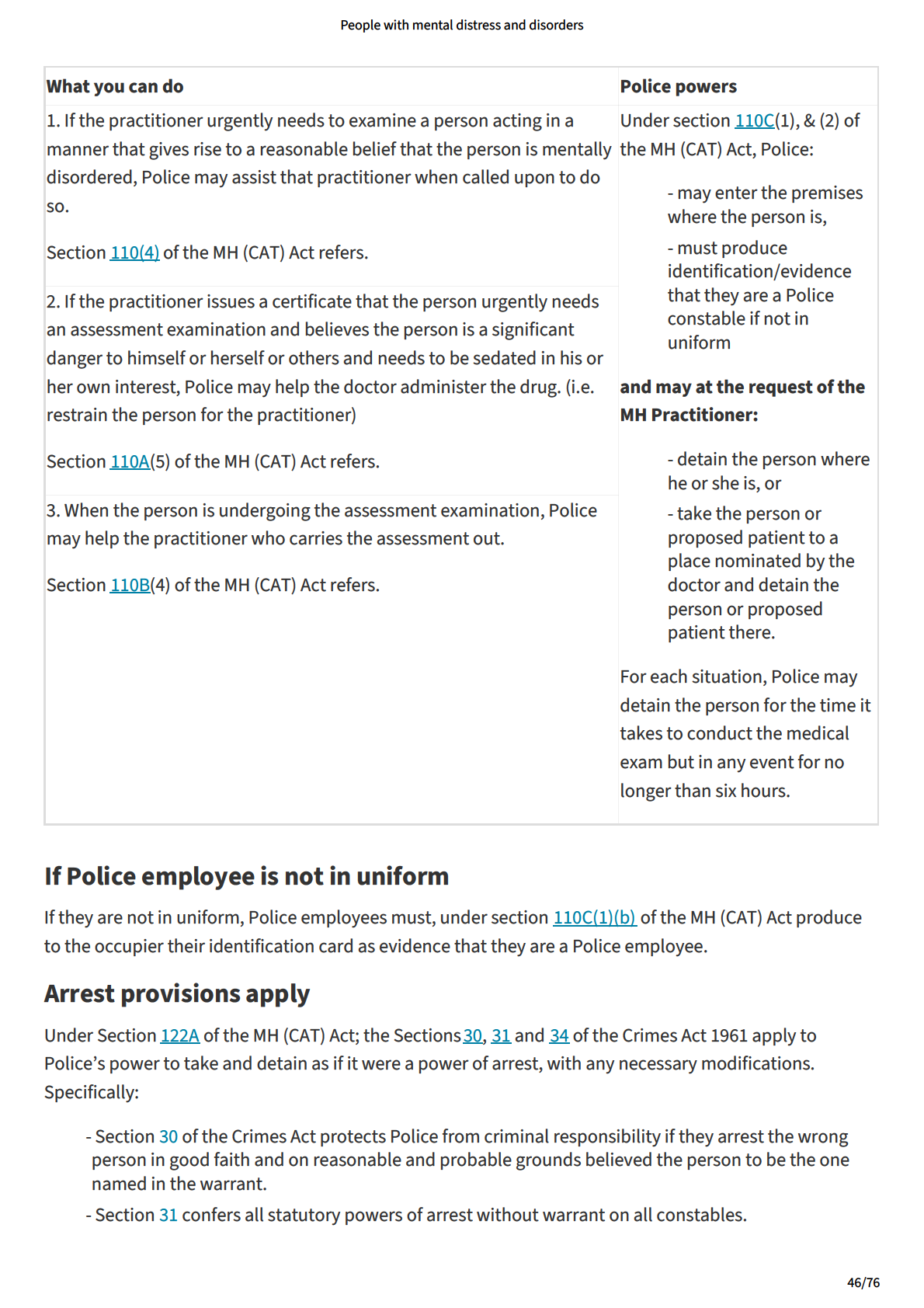
link to page 4 link to page 4
link to page 4 link to page 4 link to page 4 link to page 4
link to page 4 link to page 4 link to page 4 link to page 4
People with mental distress and disorders
Search and Surveil ance Act if there are reasonable grounds to suspect there is a risk to the life or safety
of any person that requires an emergency response. However, that power is limited to doing what is
necessary to avert the unfolding emergency, it does not al ow the re-taking of the person to the hospital.
Police can also consider if the person is a special or restricted patient, under Section 53-56 of the MH
(CAT) Act, they qualify as being unlawful y at large and therefore can be uplifted under section 7 of the
Search and Surveil ance Act, which enables entry without warrant to arrest a person unlawful y at large.
Voluntary patients
Note: This section
does not apply to patients who have voluntarily admitted themselves to a treatment
centre or hospital. See Mental y disordered person wandering at large’.
Definition of special patient
‘Special patient’ is defined in section 2 of the MH (CAT) Act and covers people who have been ordered to
be detained in hospital by the court because they are unfit to stand trial or have been acquitted on the
grounds of insanity, or who have been detained for assessment or, fol owing assessment, pending trial.
The term also includes people remanded to hospital after being convicted, acquitted, or found unfit to
stand trial while decisions are made on their future, as wel as convicted people who have been
sentenced to prison and detention in hospital.
Definition of restricted patient
Restricted patient means a patient who is declared to be a restricted patient by the Court under section
55 of the Act. The Court may make an order declaring the patient to be a restricted patient if it is satisfied
1. That the patient presents special difficulties because of the danger he or she poses to others; and
2. That, for that reason, it is appropriate that the order be made.
Offence to assist escape
Under section 122 of the Crimes Act 1962, Police must prove the identity of the suspect and that they:
- rescued any person ordered to be detained as a special patient while that person was being taken
to or from a hospital, secure facility or any other place;
or
- being a constable, officer of a prison, security officer or officer of or employee in any hospital or
secure facility,
- had in his or her custody any person lawful y detained as a special care recipient, and
50/76
link to page 4 link to page 4
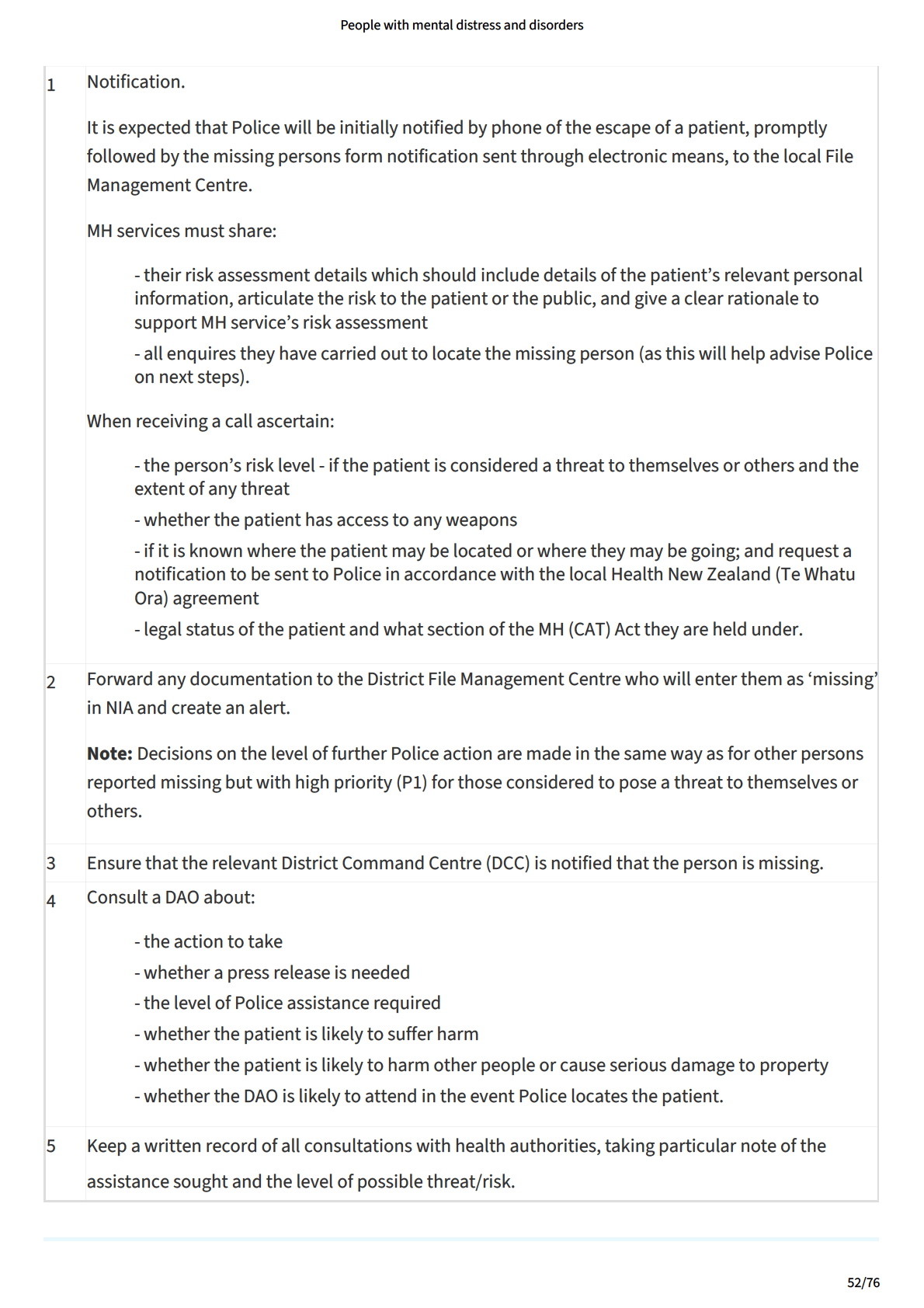
link to page 4 link to page 4
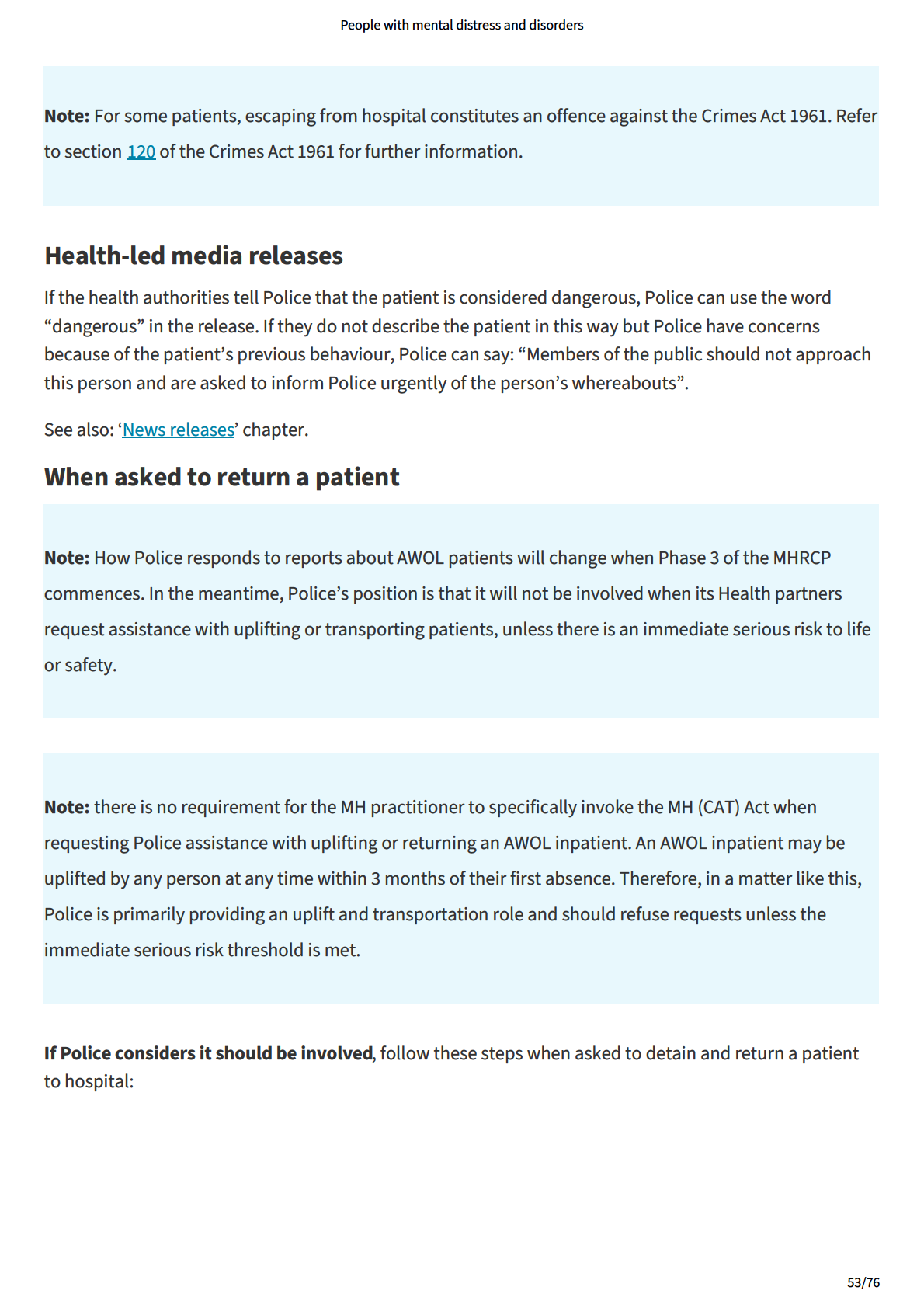
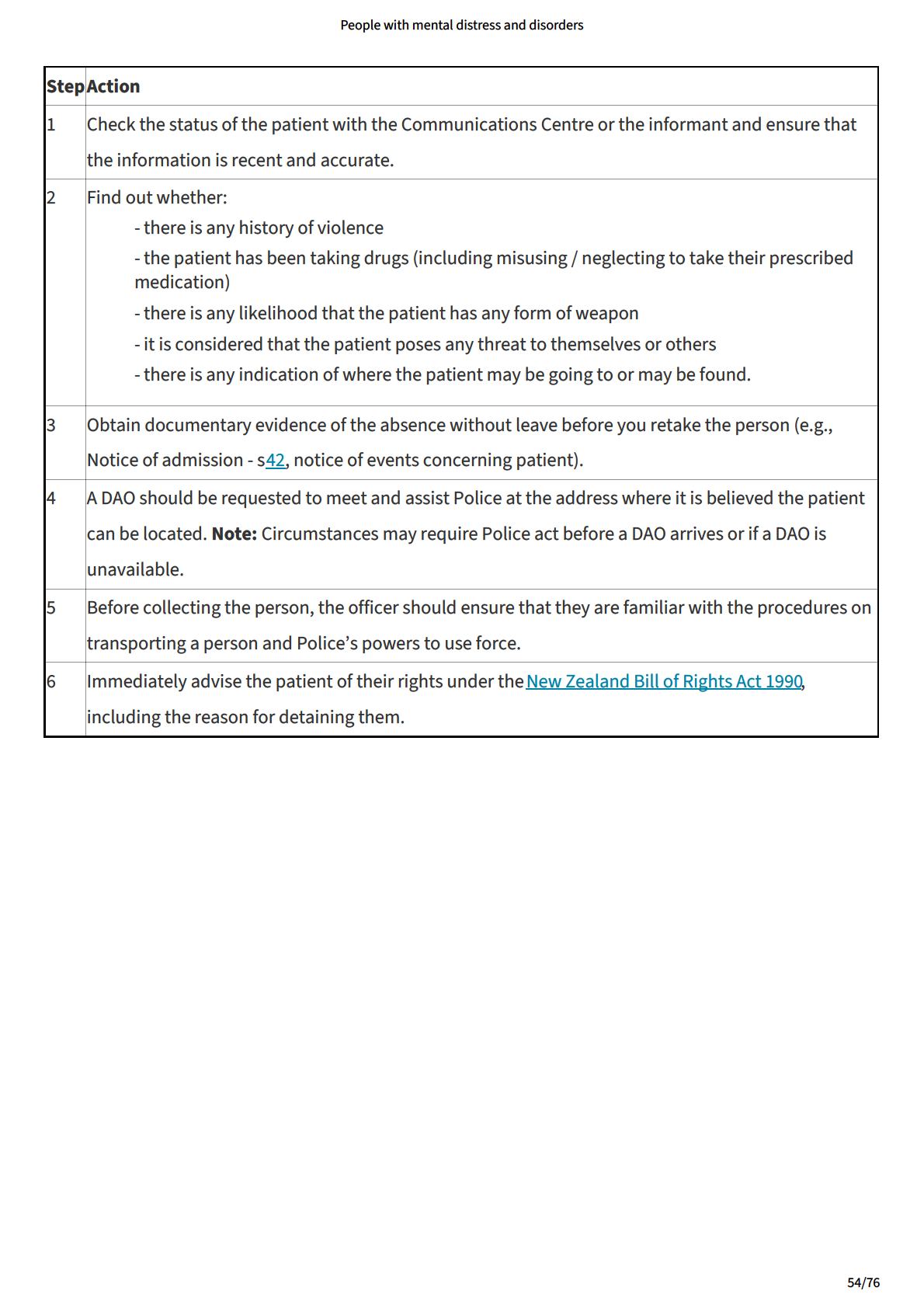
link to page 4 link to page 4 link to page 4
People with mental distress and disorders
Mentally disordered person on private property
Note: How Police respond to events involving mental y disordered persons on private property wil
change when Phase 3 of the MHRCP commences.
Authority
Police has no powers under the Mental Health Act with respect to mental y disordered persons private
property unless a DAO is present or directs us under the Act. The Mental Health (Compulsory Assessment
and Treatment) Act 1992 (MH (CAT) Act) al ows an officer to enter private property to retake a person who
has escaped in specific circumstances. Section 40 applies to a person who is subject to an inpatient order
and is absent without leave from a hospital. A DAO may seek Police assistance under section 41. A person
who has escaped and is subject to section 53 or a person who is absent without leave can be uplifted and
taken under sections 40 and 41.
When dealing with a person with a mental disorder on private property, use the operational threat
assessment tool (TENR), to assess the threat, exposure, the necessity to act now, later or not at al , and to
develop an appropriate response. If an offence is identified, consider the use of Police discretion and
alternative resolutions in appropriate circumstances, as required by the ‘Police operating strategy,
Prevention First’.
If action is required, and Police has no authority to enter the premises, an appropriate response may
involve seeking help from the DAO, the person’s doctor, family/whānau, friends or associates or using
other legislation to enter the premises. Officers should consider seeking consent of the occupier of the
premises to al ow Police entry.
Power to enter premises
Remember that Police officers, like any member of the public, have an implied licence to enter a property.
However, Police must immediately leave if requested to do so by a lawful occupier of the property, unless
it has a lawful justification to remain. Police can also enter a property if requested to do so by a lawful
occupier of that property.
However, if Police suspect a person has committed an offence that is punishable by imprisonment and
for which he or she can be arrested without a warrant, section 8 of the Search and Surveil ance Act 2012
al ows Police to enter private premises to search for and arrest that person without a warrant. Police can
only enter the premises if it reasonably believes the person wil leave to avoid arrest, and/or destroy,
conceal, alter or damage evidence, unless you arrest them immediately.
Section 7 Search and Surveil ance Act permits a constable to enter a place (including a private dwel ing)
or vehicle without a warrant to search for and arrest a person on reasonable grounds to suspect that the
55/76
link to page 4 link to page 4 link to page 4
People with mental distress and disorders
person is unlawful y at large and on reasonable grounds to believe the person is there.
Section 3 Search and Surveil ance Act defines a person unlawful y at large to include a special
patient/restricted patient who has escaped or failed to return from leave. So, Police can enter without a
warrant if the person is a restricted or special patient who has escaped or failed to return. This power
does not apply to a person subject to an inpatient order but who is not a restricted or special patient.
Section 14 of the Search and Surveil ance Act 2012 al ows Police to enter private property or a vehicle
without a warrant if it suspects there is a risk to life or safety that requires an emergency response. It also
al ows warrantless entry if Police has reasonable grounds to suspect that Police’s entry wil stop or
prevent an offence being committed that might injure someone, damage or cause serious loss of
property.
Final y, there are other particular circumstances in which Police can lawful y enter a property. For
example, under section 18 of the Search and Surveil ance Act 2012, Police can enter a private property if it
has reasonable grounds to suspect that a person is in possession of firearms but by reason of a mental
condition is incapable of having proper control of them.
Power to prevent suicide
Under section 41 of the Crimes Act 1961, Police can use such force as may be reasonably necessary to
prevent a suicide or the commission of any offence that would be likely to cause immediate and serious
injury to anyone, or serious damage or property, or to prevent an act that Police believes, on reasonable
grounds, would amount to suicide if committed. There is no power to justify ongoing detention under
section 41 unless, for example, there is a suspected overdose or laceration where the person wil need to
be transported to a medical facility.
Police can enter private property under an implied licence, for information on entering property to
protect life and property, see ‘Responding to a suicide attempt of threat’.
Retaking a patient
If the person is absent from hospital without leave, Police may be able to use its powers to retake the
person. See Returning a patient to hospital’.
Calling a DAO or Mental Health Practitioner
If none of the powers above are available to Police and action must be taken, Police should cal a MH
Practitioner or DAO to the scene.
For procedures on assisting a DAO or MH Practitioner, see ‘Procedures for assisting DAOs’ and ‘Assisting a
mental health practitioner’.
56/76
link to page 4 link to page 4
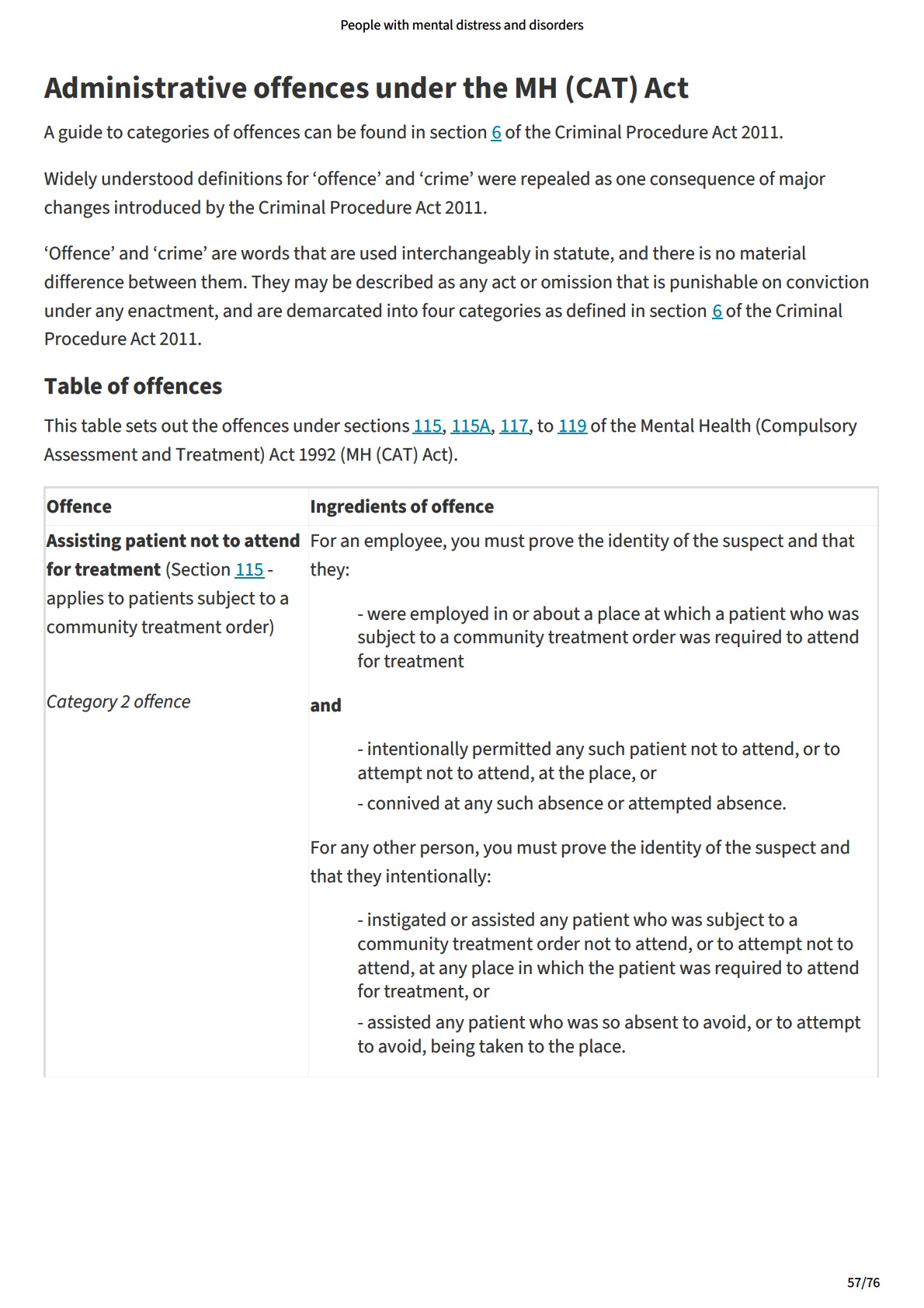
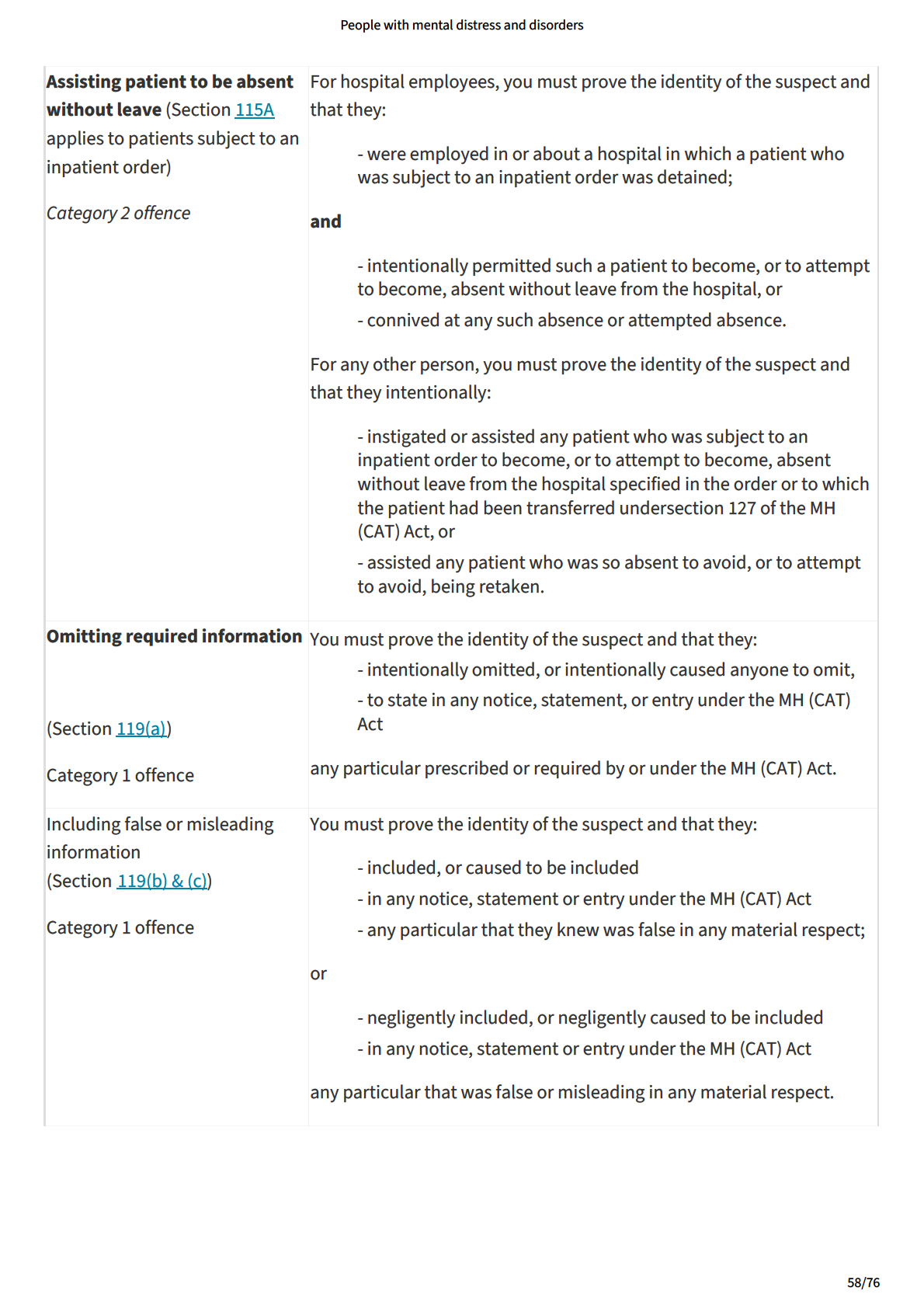
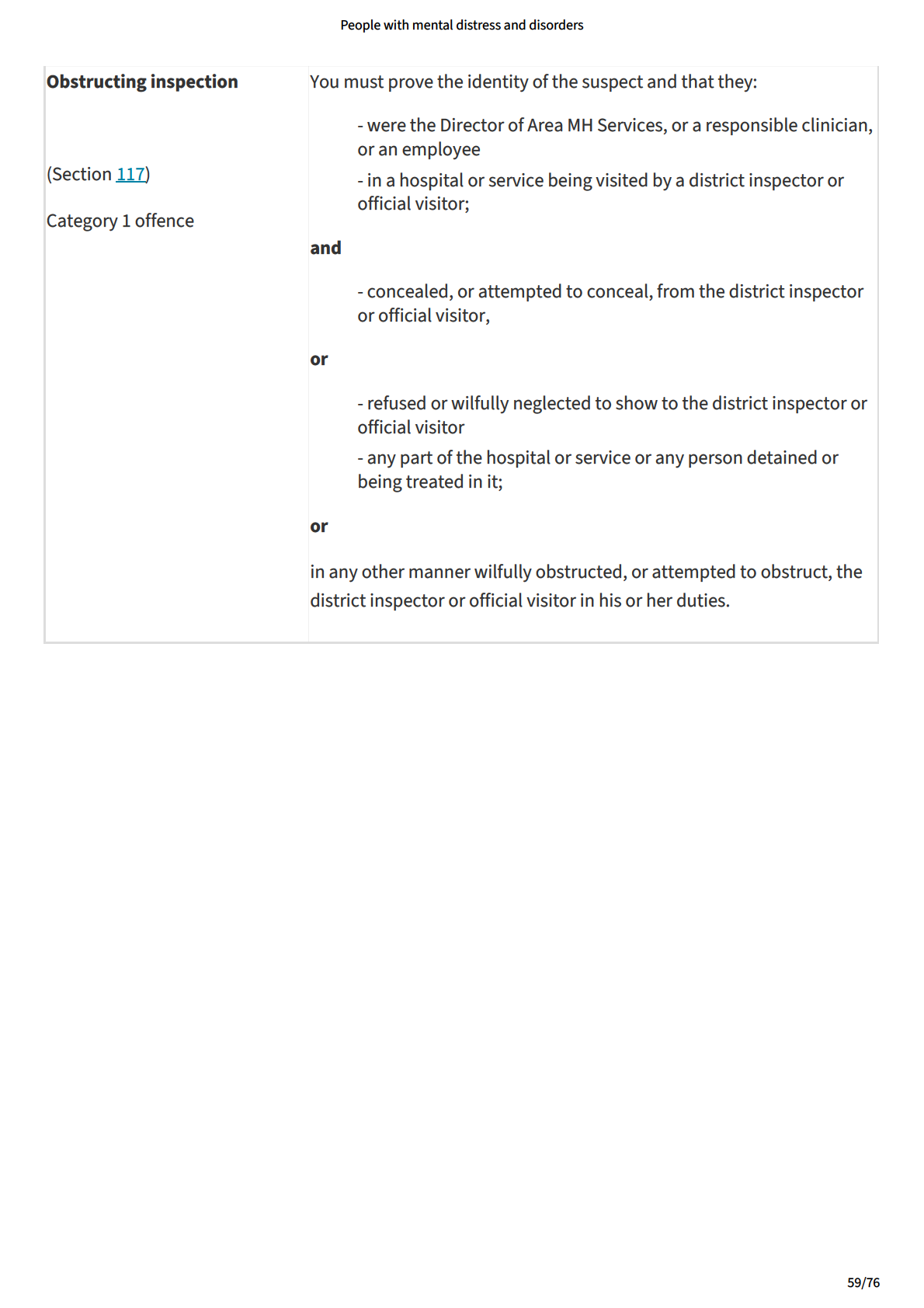
link to page 5
People with mental distress and disorders
People with an intellectual disability
This is now a separate manual chapter. See 'People with an intel ectual disability'.
60/76
link to page 5 link to page 5 link to page 5 link to page 5
link to page 5 link to page 5
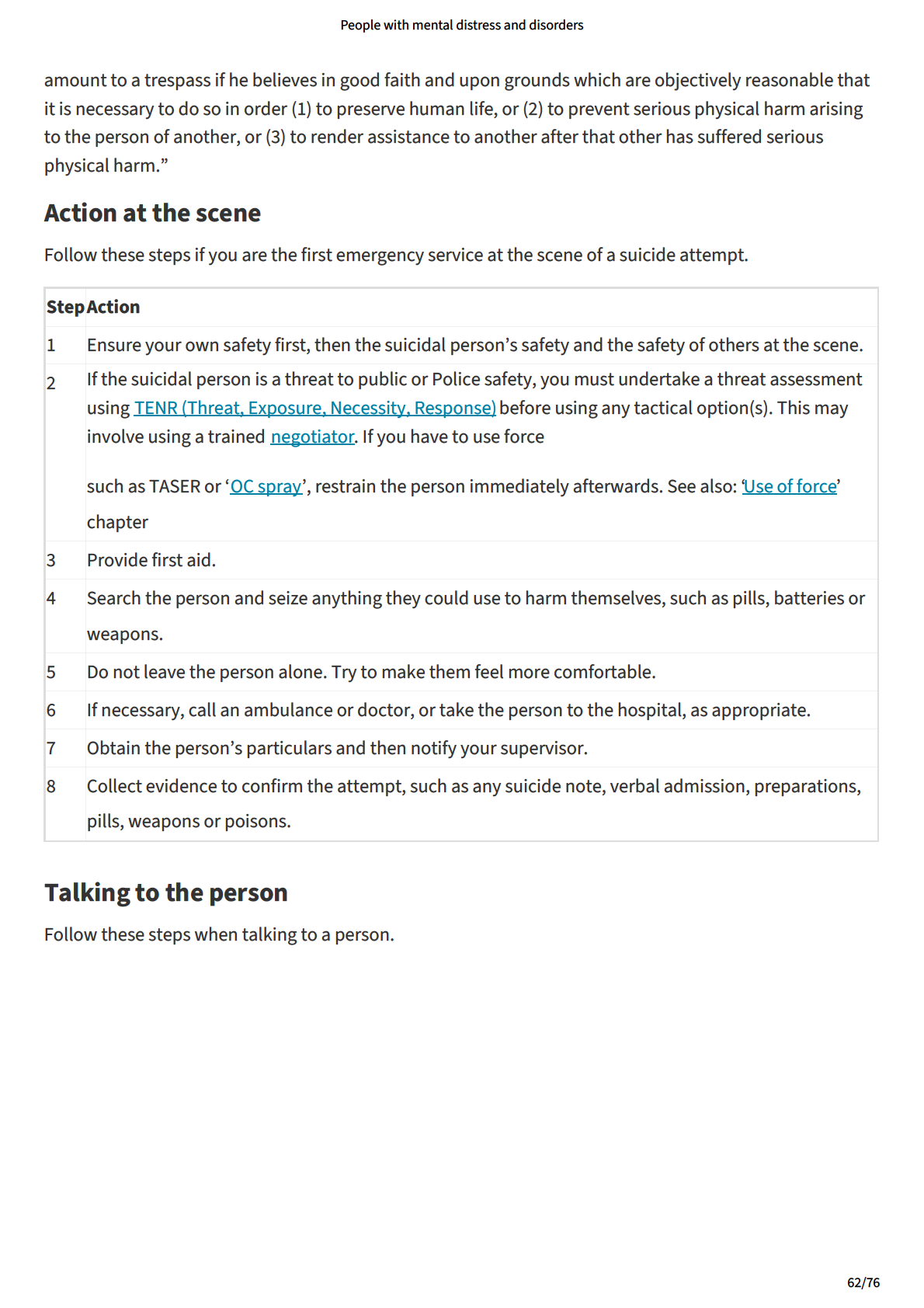
link to page 5 link to page 5
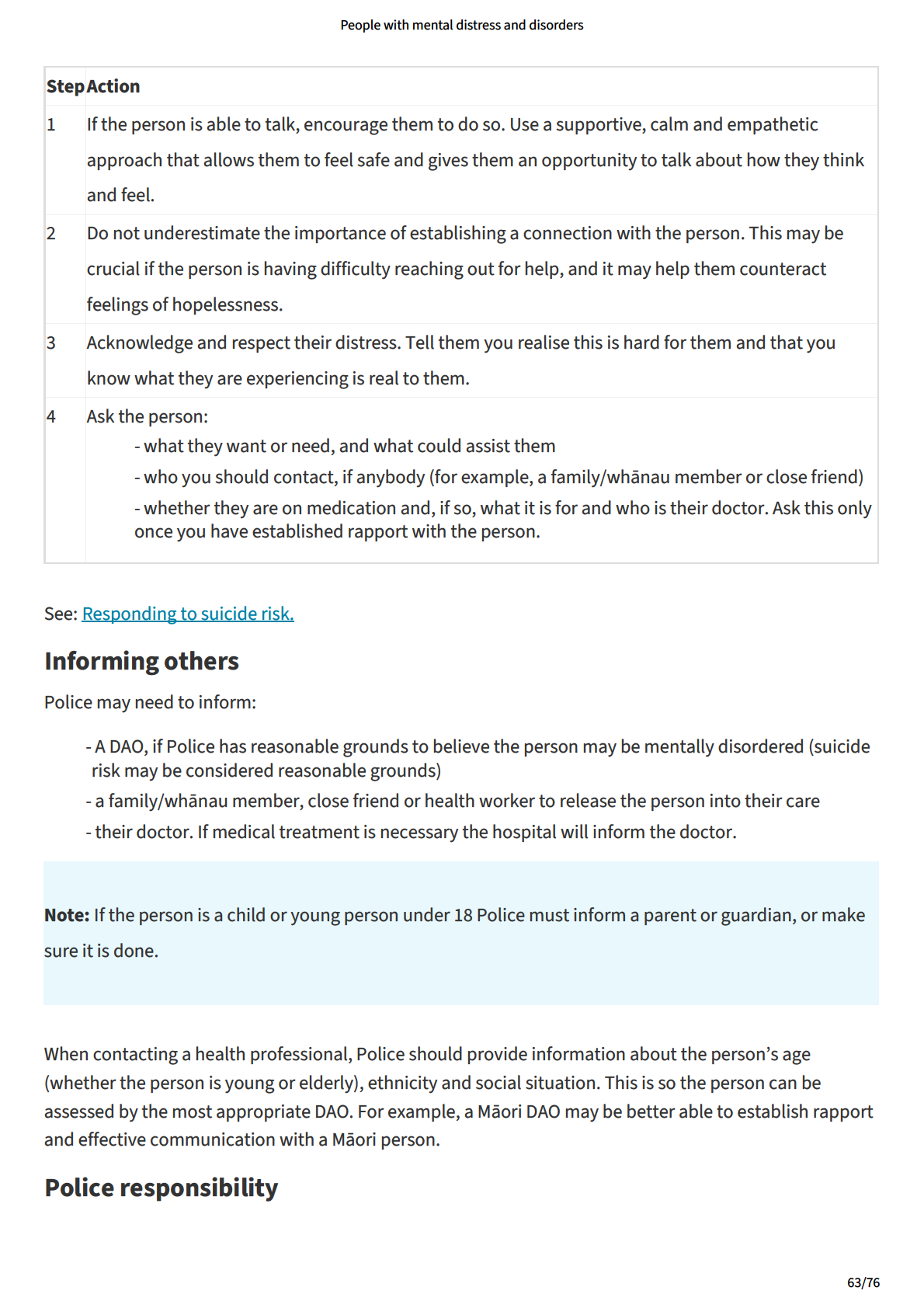
People with mental distress and disorders
When dealing with suspects, witnesses or victims, al Police employees must be alert to risk of suicide.
If Police has any serious concerns for the person’s safety, it must take steps to minimise the risk. This
could include informing a DAO or another suitable person as detailed above. Police may also be
authorised by a DAO to take the person into custody, or if they are in a public place, to detain them. See
‘Mental y disordered person wandering at large’ for information about Police powers to detain.
Police should detail any concerns it has about the person harming themselves and the action taken to
minimise those risks in a notebook. Officers should ensure they pass any concerns or related information
on to other Police staff or appropriate persons if necessary.
64/76
link to page 5 link to page 5 link to page 5 link to page 5 link to page 5
People with mental distress and disorders
People affected by drugs or alcohol
Alcohol and drugs can have a serious effect on a person with a mental disorder. There are provisions
under the Policing Act 2008 that provide Police with some powers to deal with these situations.
Taking the person home
If Police finds a person in a public place who seems to be affected by drugs or alcohol, it should consider:
- whether medical attention is required, and
- the possibility that the person is suffering from a medical condition, has a mental disorder or is
intel ectual y disabled.
If medical attention is not required, Police should take the person home. If Police cannot find out where
the person lives or it would not be practicable to take the person there or safe to leave the person there,
the person can be taken to a temporary shelter or detoxification centre, if one is available.
Detention
Only if these courses of action are not reasonably practicable should Police detain the person at the
station under section 36 of the Policing Act 2008.
Police can detain any person in a police station for up to 12 hours if that person is:
- in a public place, and
- intoxicated to such an extent that they are incapable of looking after themselves.
Child or young person
If Police find a child or young person affected by drugs and/or alcohol, it should consider the need for
immediate medical intervention and observation. What appears to be a mild intoxication can quickly
escalate to a serious situation requiring immediate medical intervention.
See Part 2 - Responding to youth offending and related issues
If Police has concerns for the young person regarding drugs or alcohol use, it should consider a referral to
local MH and addiction services.
If the person has a mental disorder
If Police thinks the person has a mental disorder, they should cal a DAO so that they can, if necessary,
arrange for an assessment examination under section 9 of the MH (CAT) Act.
Although intoxication complicates an assessment, it does not make an assessment of the person’s mental
state invalid. Therefore, there is no need to wait for the person to become sober and there should be no
delay in the DAO assessing the person. If the DAO is unwil ing to process the person until sober, Police
should remind them that position is inconsistent with the principles of the agreement between Police and
65/76
link to page 5
People with mental distress and disorders
Health and point out that a delay could mean that the person wil be released without assessment when
the six-hour period provided for assessment has elapsed. These instances should also be reported to the
District Command Centre. The use of a Police Medical Officer, although possible, is not encouraged as
they often do not have current training to complete crisis MH assessments.
Caution: Police cannot use other legislative provisions to hold a person beyond the six-hour mark for the
purpose of a MH assessment.
Effect of drugs on mental disorder
Sometimes alcohol and drugs can exacerbate symptoms of mental disorder. A combination of mental
disorder symptoms, misusing prescribed medication, and alcohol or drug abuse might increase the risk of
violence. Only some people with these three risk factors wil commit acts of violence. Most wil not.
The strongest risk factors for violence are not attributable to mental disorder or substance abuse. They
are:
- a past history of violence
- threatening to commit acts of violence in the future.
66/76
link to page 5 link to page 5
People with mental distress and disorders
Criminal procedures where mentally disordered person
commits offence
If a person with a mental impairment commits an offence punishable by imprisonment, they are dealt
with under the Criminal Procedure (Mental y Impaired Persons) Act 2003 (“the Criminal Procedure (MIP)
Act 2003” in this section).
Use the ‘operational threat assessment tool TENR’ to assess the threat, exposure, and necessity to act,
and decide whether dealing with the person under the Criminal Procedure (MIP) Act 2003 is an
appropriate response. Consider the use of Police discretion and alternative resolutions in appropriate
circumstances, as required by the ‘Police operating strategy, Prevention First’
When action is required, an appropriate response may involve seeking help from the DAO, the person’s
doctor, family/whānau, friends or associates.
The Criminal Procedure (MIP) Act 2003:
- addresses the legislative gap that was created with the enactment of the Mental Health
(Compulsory Assessment and Treatment) Act 1992 (MH (CAT) Act), which only included people with
an intel ectual disability if they also had a mental disorder
- provides for:
- determining whether a person is unfit to stand trial
- determining whether a person is not guilty on the grounds of insanity
- sentencing a person with a mental impairment who is convicted
- assessing a defendant for mental impairment
- contains procedures for assessing, detaining, treating and caring for such people.
Definition of ‘mental impairment’
‘Mental impairment’ is not defined in legislation. Recent case law has defined ‘mental impairment’ as
including a mental disorder or intel ectual disability, and also other mental or psychological disorders
such as degenerative neurological conditions, substance abuse or acquired brain injury, low intel igence
or impaired cognition (refer R v H [2014] NZHC1423).
67/76
link to page 5 link to page 5 link to page 5 link to page 5
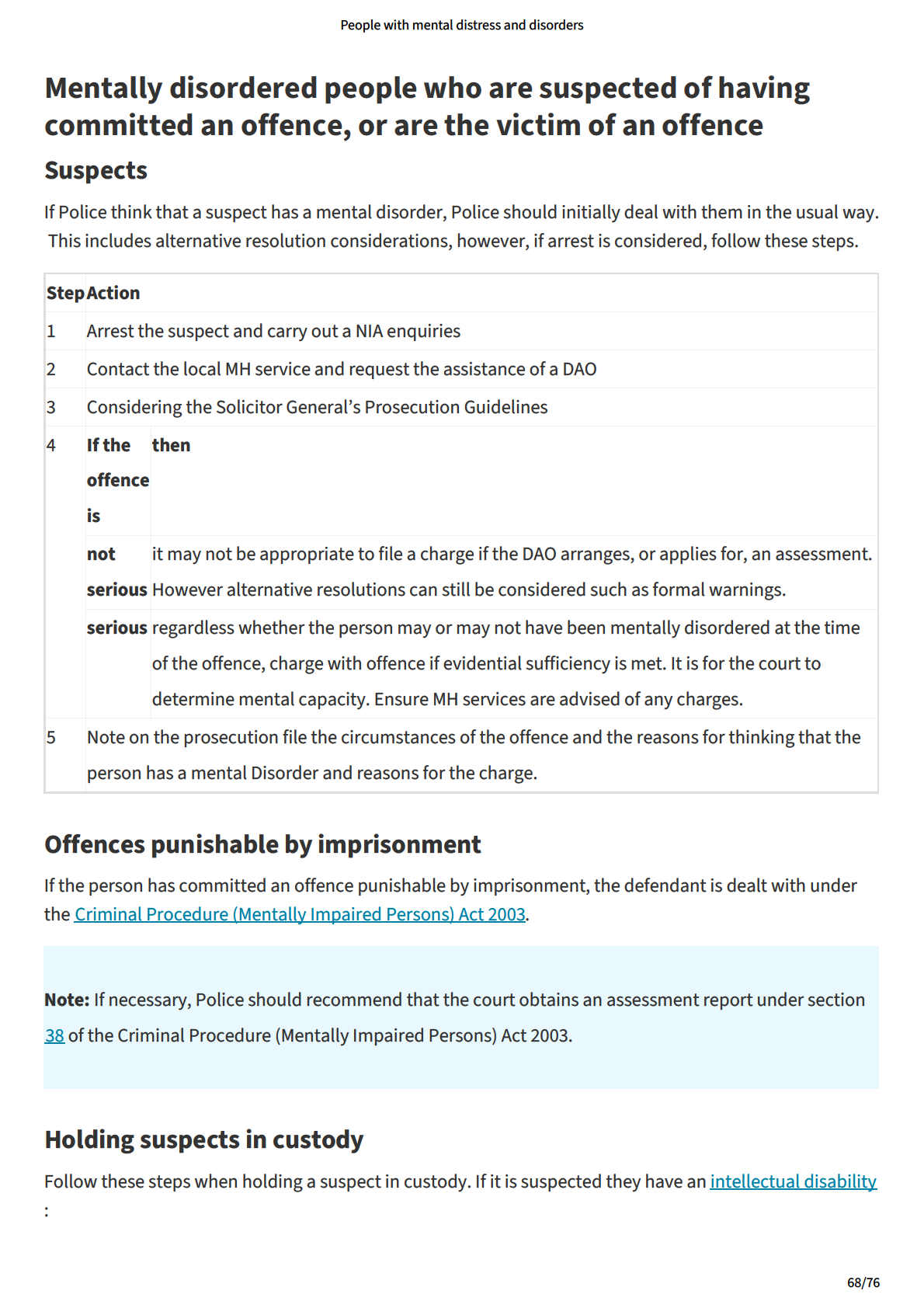
link to page 5
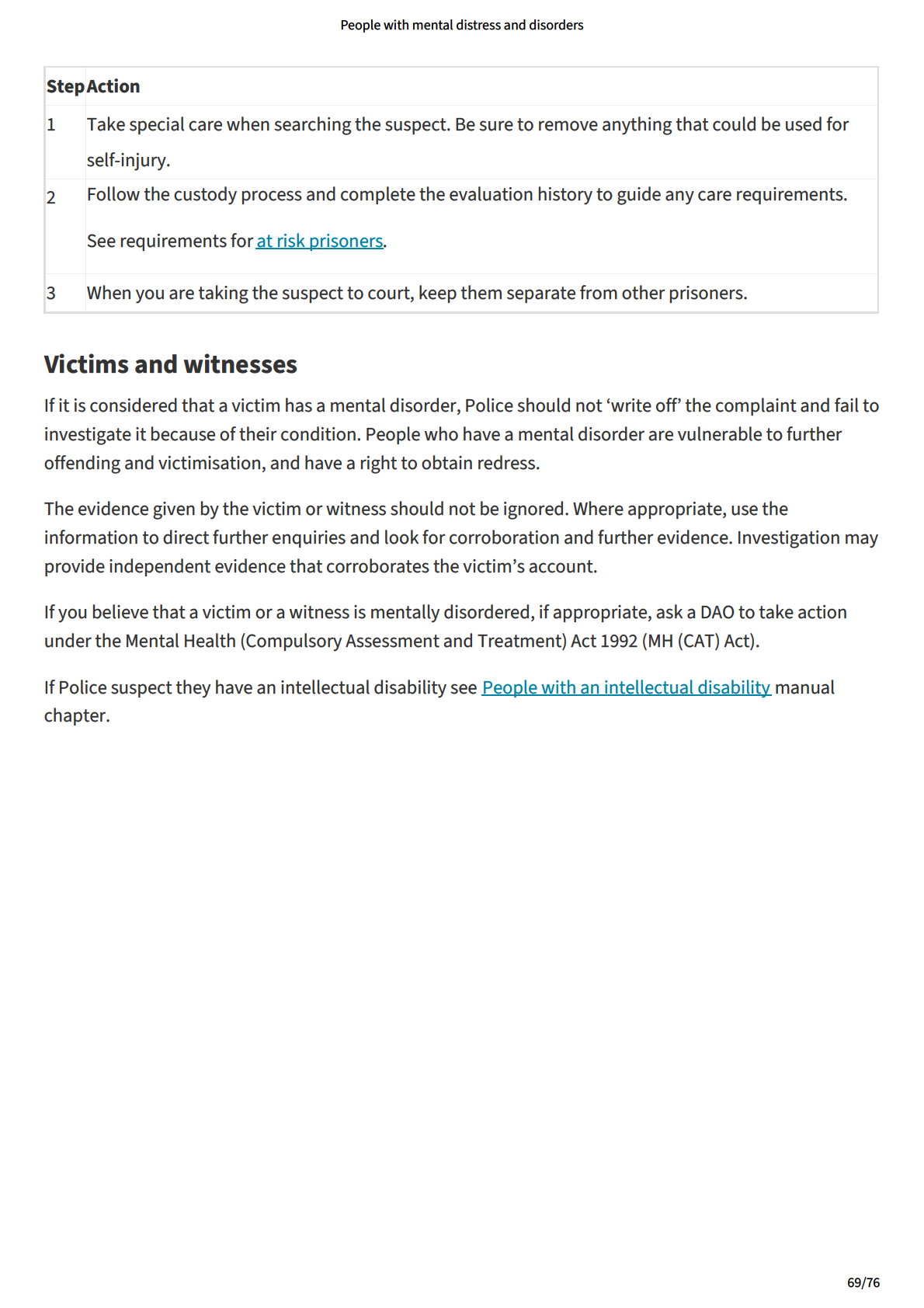
link to page 5 link to page 5 link to page 5
People with mental distress and disorders
Fitness to stand trial
At any stage after proceedings commence and until al the evidence is concluded, a court can find a
defendant unfit to stand trial. There are legal procedures for finding a person unfit to stand trial and the
process is covered in the Criminal Procedure (Mental y Impaired Persons) Act 2003.
Definition of ‘unfit to stand trial’
A person is unfit to stand trial if they are unable, due to mental impairment, to conduct a defence or to
instruct counsel to do so. The term also refers to a defendant who, due to mental impairment, is unable
to:
- plead
- adequately understand the nature or purpose or possible consequences of the proceedings
- communicate adequately with counsel for the purposes of conducting a defence.
Defendant’s involvement in the offence
If before trial the defendant is found unfit to stand trial, the court must decide whether the court is
satisfied, on the balance of probabilities, that the evidence against the defendant is sufficient to establish
that the defendant caused the act or omission that forms the basis of the offence with which the
defendant is charged (per s 10(2) of the Criminal Procedure (Mental y Impaired Persons) Procedure Act
2003).
See sections 11 and 12 of the Criminal Procedure (Mental y Impaired Persons) Procedure Act 2003 for
guidance concerning the inquiry as to the defendant’s involvement in an offence during a Judge-alone
trial (s11) and during a jury trial (s12).
If the defendant is not involved
In accordance with section 13 of the Criminal Procedure (Mental y Impaired Persons) Act, if the court is
not satisfied of the matter in section 9, it must discharge the person. This discharge does not amount to
an acquittal.
Determining fitness
If the court is satisfied that the defendant caused the act or omission that is the basis of the offence, it
must receive evidence from two health assessors about whether the person is mental y impaired. If it is
satisfied that this is the case, it must:
- give each party the opportunity to present evidence about whether the person is unfit to stand
trial, and
- find on that matter, on the balance of probabilities.
If the court finds the person is fit to stand trial, proceedings commence or continue in the usual way.
70/76
link to page 5 link to page 5 link to page 5 link to page 5 link to page 5
People with mental distress and disorders
Body samples
A person found unfit to stand trial is stil subject to the Criminal Investigations (Bodily Samples) Act 1995.
See the definition of ‘conviction’ under section 2, Interpretation and sections 4A(1) and 46(1) in that Act.
Conviction includes acquittal on account of insanity per s 2 Criminal Investigations (Bodily Samples) Act
1995.
Section 4A of the Criminal Investigations (Bodily Samples) Act 1995 defines a person detained under
sentence of imprisonment (fol owing conviction)
Section 46(1) applies to a person in custody who is subject to a compulsion order / databank compulsion
notice - including a person detained in a hospital under the MH(CAT)A.
A compulsion order may be granted when a person is in a MH facility, but a compulsion order may also be
refused due to incapacity see s 13(4).
Appeals
The defendant can appeal a finding that they caused the act or omission that forms the basis of the
offence or is unfit, or fit, to stand trial.
The prosecution can appeal on a question of law against a finding that the person caused the act or
omission that forms the basis of the offence, or is mental y impaired, or is unfit to stand trial.
Enquiry into detention options
If a person is found not guilty on reasons of insanity, or unfit to stand trial, the court must order enquiries
to be made to find the most suitable way of dealing with the person. For this purpose, the court must
remand the person to a hospital or secure facility or bail the person subject to them going to a place
approved by the court. In deciding whether to grant bail, the need to protect the public is the paramount
consideration.
Needs assessment
If the person has an intel ectual disability, they must, in the course of these enquiries, also undergo a
needs assessment under Part 3 of the Intel ectual Disability Act. See People with intel ectual disability.
Detention in hospital or secure facility
When the court has completed its enquiries, it must consider the circumstances of the case and the
evidence of one or more health assessors about whether it is necessary to detain the person in:
- a hospital as a special patient under the Mental Health (Compulsory Assessment and Treatment)
Act 1992 (MH (CAT) Act), or
- a secure facility as a special care recipient under the Intel ectual Disability Act.
71/76
link to page 5
People with mental distress and disorders
If it is satisfied that one of these orders is necessary in the interests of the public or anyone who may be
affected by the decision, it must record that order.
Other treatment and care options
If the court is satisfied that neither of the above orders is necessary, it must order that the person be:
- treated as a patient under the MH (CAT) Act (to make this order, the court must be satisfied that the
person has a mental disorder or intel ectual disability); or
- cared for as a care recipient under the Intel ectual Disability Act (to make this order, the court must
be satisfied that the person has an intel ectual disability); or
- subjected to no order, if the person is liable to a prison sentence; or
- immediately released.
72/76
link to page 5 link to page 5 link to page 5 link to page 5
People with mental distress and disorders
Insanity
At any stage before a judge-alone or jury trial, the issue of whether the defendant is insane at the time of
the offence can be raised. There are legal procedures for finding a person not guilty on the grounds of
insanity and the process is covered in the Criminal Procedure (Mental y Impaired Persons) Act 2003.
Definition of insanity
No person must be convicted of an offence by reason of an act done or omitted by them when labouring
under natural imbecility or disease of the mind to such an extent as to render them incapable:
- of understanding the nature and quality of the act or omission; or
- of knowing that the act or omission was moral y wrong, having regard to the commonly accepted
standards of right and wrong.
Insanity before or after the time when they did or omitted the act, and insane delusions, though only
partial, may be evidence that the offender was, at the time when they did or omitted the act, in such a
condition of mind as to render them irresponsible for the act or omission.
See: Section 23(2) & (3) of the Crimes Act 1961.
Agreement on insanity
If, before or at a hearing or trial, the:
- defendant indicates that they wil raise a defence of insanity, and
- prosecution agrees that the only reasonable verdict is not guilty on account of insanity, and
- Judge is satisfied, on the basis of expert evidence, that the defendant was insane within the
meaning of section 23 of the Crimes Act 1961 at the time of the offence,
the Judge must, under section 20 (2) of the Criminal Procedure (Mental y Impaired Persons) Act, find the
defendant not guilty on account of insanity.
Judge or jury determining insanity
If there is no agreement, the case goes to trial and the Judge or jury wil determine whether the defendant
is not guilty on the grounds of insanity.
If it appears from the evidence that the defendant may have been insane at the time of the offence, the
Judge may ask the jury to find whether the defendant was insane even if the defendant has not raised this
possibility themselves.
73/76
link to page 5 link to page 6 link to page 6 link to page 6
People with mental distress and disorders
Convicted people
Detention options
If the person with a mental impairment is convicted, the court may sentence the person to a term of
imprisonment and also order that they be detained in:
- a hospital as a special patient under the Mental Health (Compulsory Assessment and Treatment)
Act 1992 (MH (CAT) Act) (if the person has a mental disorder), or
- a secure facility as a special care recipient under the Intel ectual Disability Act (if the person has an
intel ectual disability) See People with intel ectual disability
if it is satisfied that the order is necessary in the interests of the person or for the safety of the public or
any person or class of person and if the person is not, at the time of the conviction, already subject to a
sentence of imprisonment. Section 34(1)(a), (2)-(5) of the Criminal Procedure (Mental y Impaired Persons)
Act refers.
Other options
Alternatively, instead of passing sentence, the court may, in accordance with section 34(1)(b), (3)-(5) of
the Criminal Procedure (Mental y Impaired Persons) Act, order that the person be:
- treated as a patient under the MH (CAT) Act (if the person has a mental disorder), or
- cared for as a care recipient under the Intel ectual Disability Act (if the person has an intel ectual
disability).
Needs assessment
If the person has an intel ectual disability, a needs assessment is carried out to determine the kind of care
required, identify the services able to provide it, and prepare a care and rehabilitation plan. See People
with intel ectual disability.
74/76
link to page 6 link to page 6 link to page 6 link to page 6
People with mental distress and disorders
Assessing person in custody for mental impairment
At any stage during proceedings, the court can ask for a report on the defendant’s mental state.
Assessment report
If there is reason to believe that a person in custody has a mental impairment, the court can order a
health assessor to prepare an assessment report on the person. It can do this at any stage of the
proceedings, on its own initiative or on application by the prosecution or defence. The report is intended
to help the court determine:
- whether the person is fit to stand trial
- whether the person is insane within the meaning of section 23 of the Crimes Act 1961
- the type and length of sentence that might be imposed
- the nature of a requirement the court might impose as part of a sentence or order.
Note: In relation to children and young people, a similar provision exists in relation to the Youth Court in
section 333 of the Oranga Tamariki Act 1989.
Detention while report conducted
While the report is being prepared, the person may be detained in a prison, hospital or secure facility, as
the court thinks fit, for a period not exceeding 14 days. If the person is bailed, the court may require the
person to go to a place approved by it for the assessment.
Needs assessment
If the report finds that the defendant has an intel ectual disability, a needs assessment is carried out
under section 15 of the Intel ectual Disability Act. The purpose of the assessment is to determine the kind
of care required, identify the services able to provide it, and prepare a care and rehabilitation plan. See
'People with intel ectual disability'.
75/76
link to page 6 link to page 6