

133 Molesworth Street
PO Box 5013
Wellington 6140
31 March 2025
New Zealand
T+64 4 496 2000
Wellingtonian
By email: [FYI request #30168 email]
Ref:
H2025061874
Tēnā koe Wellingtonian
Response to your request for official information
Thank you for your request under the Official Information Act 1982 (the Act) to the Ministry of
Health – Manatū Hauora (the Ministry) on 21 February 2025. Responses to your questions are
outlined below:
1. Any involvement of Dr. Avataeao Junior Ulu in the development, review, or
implementation of policies concerning LGBTQ+ communities within the Ministry of
Health.
Dr Ulu has not been involved in any internal Ministry of Health policies concerning LGBTQ+
communities.
2. Any instances in which Dr. Avataeao Junior Ulu has advised against policies or
initiatives related to LGBTQ+ health and well-being.
The Ministry is not aware of any instances of this occurring.
3. Any briefing documents that include Dr. Avataeao Junior Ulu’s name and contain terms
such as "queer," "LGBTQ+," "gay," "HIV," or any other language indicating relevance to
queer communities.
No briefing documents have been identified as being within scope of your request. However, 2
memos and 1 report you may be interested in are itemised at Appendix 1.
4. Any policy initiatives aimed at supporting the queer community that did not proceed to
formal policy status and involved Dr. Avataeao Junior Ulu in any capacity.
The Ministry is not aware of any instances of this occurring.
5. Any advice or briefing documents authored by Dr. Avataeao Junior Ulu that include
terms such as "queer," "LGBTQ+," "gay," "HIV," or other indicators of relevance to queer
communities.
The Ministry has no information within scope of this part of your request. Therefore, this is
refused under section 18(g)(i) of the Act, as the information requested is not held by the Ministry
and there are no grounds for believing it is held by another agency subject to the Act.
 6. Any measures or safeguards in place within the Ministry of Health to ensure that policy
development for the Rainbow Community is free from homophobia or heteronormative
bias.
6. Any measures or safeguards in place within the Ministry of Health to ensure that policy
development for the Rainbow Community is free from homophobia or heteronormative
bias.
Al Ministry employees are required to adhere to the Public Service Standards of Integrity and
Conduct, and the Ministry Code of Conduct. The Standard of Integrity and Conduct is available
publicly online here: www.publicservice.govt.nz/assets/DirectoryFile/Code-Standards-of-
Integrity-and-Conduct.pdf.
No Ministry policy is developed in isolation without peer review, to ensure policies are free from
any unconscious biases.
7. Any actions taken by the Ministry of Health upon learning of Dr. Avataeao Junior Ulu’s
involvement with homophobic complainants in the case against Wellington City Council
regarding the rainbow crossing on Cuba Street.
The Ministry does not publicly disclose information about individual employment matters. It is
important that staff know that their personal employment information, is held correctly and wil
not be disclosed. I am therefore unable to provide information in response to your request
where your questions relate to Dr Ulu’s employment matters, in accordance with section 9(2)(a)
of the Act.
I appreciate the public interest in this matter and can assure you that there are no ongoing
issues relating to Dr Ulu’s conflicts of interest. In can advise that Dr Ulu took part in the court
action in a private capacity and informed the Ministry about his involvement on Tuesday 18
February 2025 when he became aware that his name had been published and linked him to the
court action. He took action to withdraw from the court action to counter the potential for his
actions being misinterpreted. He also acknowledged the need to declare and manage the
perceived conflict of interest. I can confirm that Dr Ulu has not been involved in any policies
relating to LGBTQ+ communities.
I trust this information fulfils your request. If you wish to discuss any aspect of your request with
us, including this decision, please feel free to contact the OIA Services Team on:
[email address].
Under section 28(3) of the Act, you have the right to ask the Ombudsman to review any
decisions made under this request. The Ombudsman may be contacted by email at:
[email address] or by calling 0800 802 602.
Please note that this response, with your personal details removed, may be published on the
Ministry website at:
www.health.govt.nz/about-ministry/information-releases/responses-official-
information-act-requests.
Nāku noa, nā
Dr Andrew Old
Deputy Director-General
Public Health Agency | Te Pou Hauora Tūmatanui
Page 2 of 3
Appendix 1: List of documents for release
#
Date
Document details
Decision on release
1
2024
Pacific Peoples report
Refused under section 18(d) of
the Act as this wil soon be
made publicly available.
2
6 March 2023
Pacific Wellbeing Chief
Released in full.
Executives' Monthly Meeting
3
25 May 2023
The Soalaupule Eco-system
Released in full.
Framework
Page 3 of 3
 ELT Memorandum
ELT Memorandum
The Soalaupule Ecosystem Framework
To:
Executive Leadership Team
1982
From:
Dr Andrew Old, DDG Public Health Agency - Te Pou Hauora Tūmatanui
Date:
Thursday, 25 May 2023
ACT
For your:
Information to note
Classification:
UNCLASSIFIED
Purpose
1.
This memo provides you with information on the Soalaupule Ecosystem Framew
INFORMATION ork
(Soalaupule) and other indigenous Pacific knowledge frameworks relevant to the development
of Te Mana Ola: Pacific Health Strategy (Te Mana Ola).
Recommendations
OFFICIAL
2.
We recommend that ELT:
a.
Note the slide deck titled ‘Soalaupule Eco-System Framework’ attached at Appendix A.
THE
b.
Note that Soalaupule was further explored as part of the development of Te Mana Ola.
Context
UNDER
3.
Pacific peoples in Aotearoa represent a multitude of Pacific island nations, and while Pacific
peoples share common worldviews and values, we recognise the diversity of each nation
through their own cultural identity.
4.
To achieve Te Mana Ola’s vision of pae ora (healthy futures) for Pacific peoples in Aotearoa, it
is important to understand that Pacific health is broad and holistic. It incorporates physical,
RELEASED
mental, and spiritual wellbeing that is steeped in community, and acknowledges the
environment in which Pacific peoples live.
5.
Te Mana Ola acknowledges the importance of embracing indigenous Pacific knowledge
frameworks, particularly Soaluapule. Frameworks like Soalaupule are necessary because they
recognise the diversity of Pacific peoples. Furthermore, they draw from the expertise,
knowledge, and worldviews of Pacific peoples to help strengthen the health system’s
responsiveness to improving Pacific health and wellbeing outcomes.
UNCLASSIFIED
 Indigenous Pacific knowledge frameworks
Indigenous Pacific knowledge frameworks
The Soalaupule Ecosystem Framework
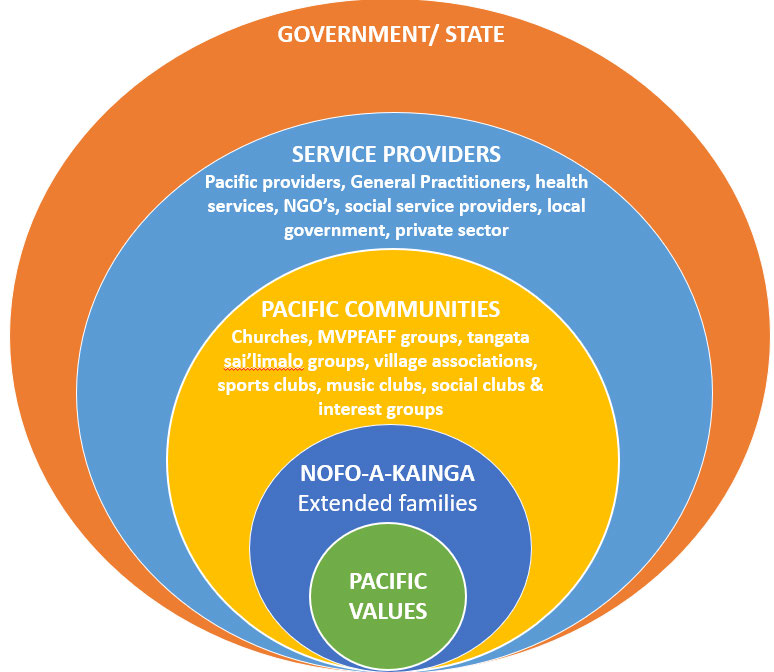
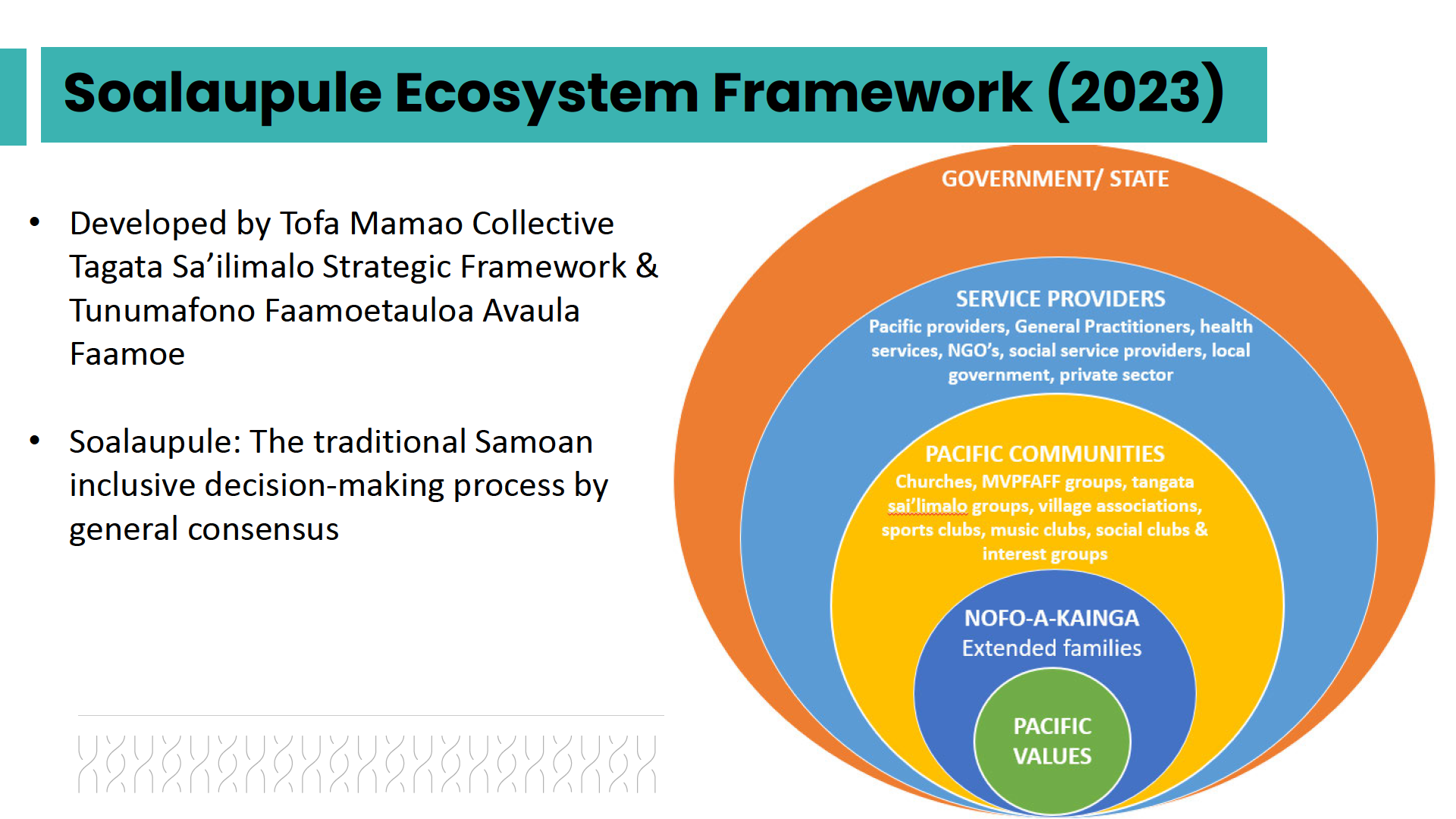
6.
Soalaupule (Figure 1) acknowledges the importance of col ectivism and natural supports within
Pacific communities. It recognises that when decisions are made, everyone who needs to be
consulted is consulted, and the final decision is based on consensus.1
7.
At the core of Soalaupule are the Pacific values of family, collectivism, consensus, reciprocity,
respect, spirituality, love, and culture; these values permeate throughout the eco-system.
Soalaupule highlights the importance of considering Pacific values in policy, commissioning,
and service design decisions for Pacific peoples.
1982
8.
‘Nofo-a-kainga' acknowledges the strong extended families who reside within communities.
These extended families col ectively make up Pacific Communities with its various groups and
ACT
clubs that operate within Pacific worldviews.
9.
Service Providers, represented by health, social services, and local governments, serve the
diverse Pacific communities and their ethnic-specific needs.
Figure 1. Soalaupule Ecosystem Framework
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1 Soalaupule was developed by Tunumafono Fa’amoetauloa Avaula Fa’amoe who sits on Manatū Hauora’s Pacific Health Strategy
Advisory Group. The Advisory Group provided advice and guidance on the development of Te Mana Ola, including the process of
community and health sector engagement.
2
10. Soalaupule exists in and of itself and is a mechanism by which the Government/State can work
alongside Pacific peoples to achieve equitable health outcomes. Col ectively, each circle of
Soalaupule is interlinked and cannot operate in isolation.
11. The nation-wide rapid response and significant increase in testing and vaccination results, as
wel as care provided in the community by Pacific peoples during the COVID-19 pandemic, can
be attributed to Soalaupule. There is an opportunity to explore how Manatū Hauora and the
wider health system can apply Soalaupule to strengthen how we respond to the health and
wellbeing needs of Pacific peoples.
12. A key component of Te Mana Ola’s development involved Pacific community and health sector
engagement. Over 40 fono throughout the country was held to ensure that Manatū Hauora
1982
captured the diverse voices of Pacific communities in Aotearoa. These diverse voices
considered regional (rural/urban) differences, ethnic-specific input, and population groups
such as women, tagata sa’ilimalo (people with disabilities, their families and carers), youth and
ACT
the Pacific rainbow+/LGBTQIA+/MVPFAFF+ community.2
13. The Pacific Health team’s extensive engagement approach reinforces Soalaupule and adds to
the richness of existing Pacific health data. The approach is consistent with the requirement
under Section 3F of the Health Act 1956 for the Public Health Agency to consult to ensure that
the views of the public involved in public health services are considered in the formulation of
advice to the Director-General of Health. It is also consistent with the Public Service
Commission’s Long-term Insights Briefing which articulates how public participation is central
to building and maintaining trust in government and to working through compl
INFORMATION ex issues.
Pacific models of health and wellbeing
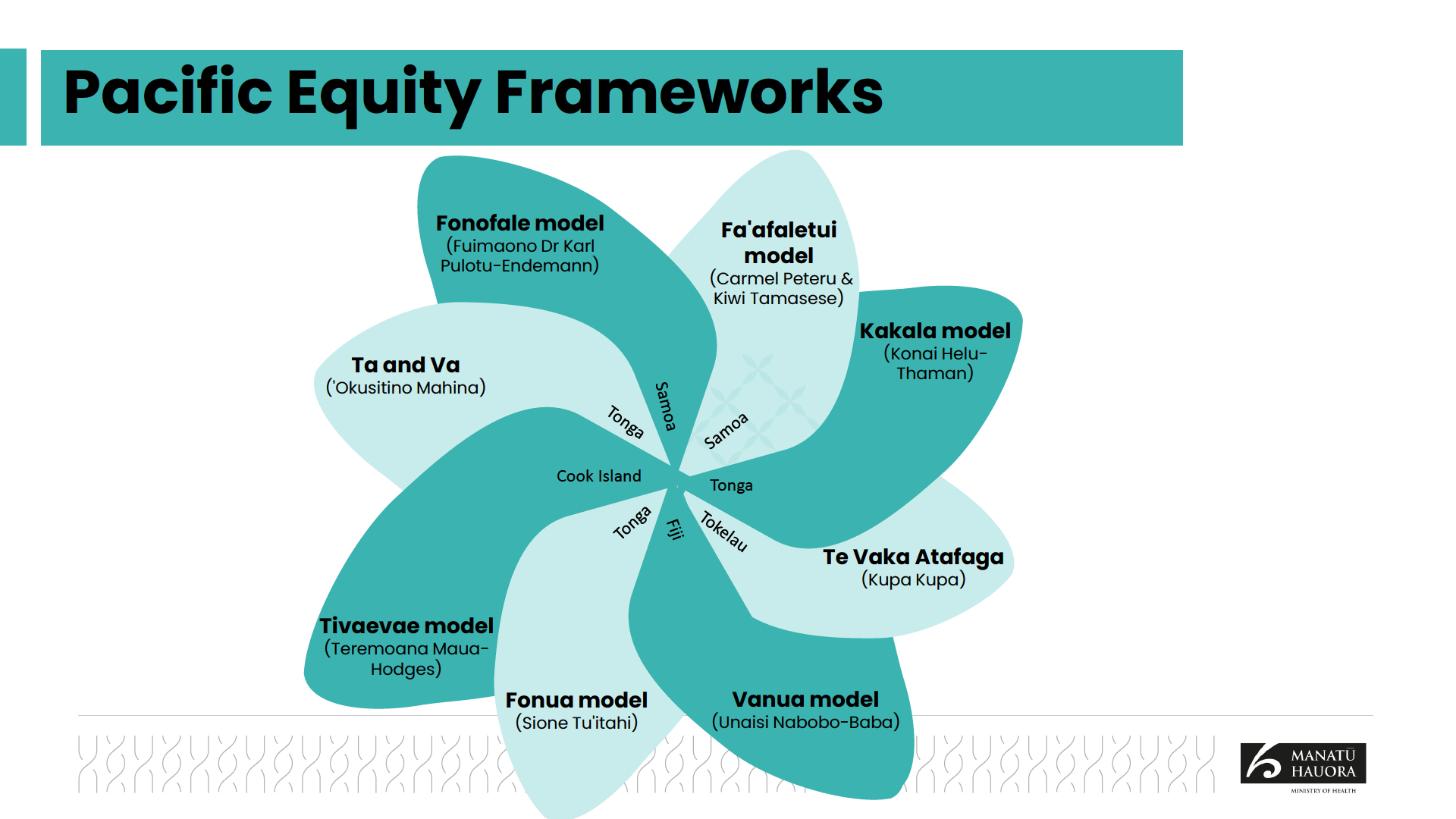
14. Te Mana Ola’s vision and development is also positioned within existing indigenous Pacific
knowledge frameworks, including Pacific health and wellbeing models such as the Fonofale
model and the Kakala framework. Despite these model
OFFICIAL s being developed more than 20 years
ago, they stil hold relevance for Pacific peoples today.
THE
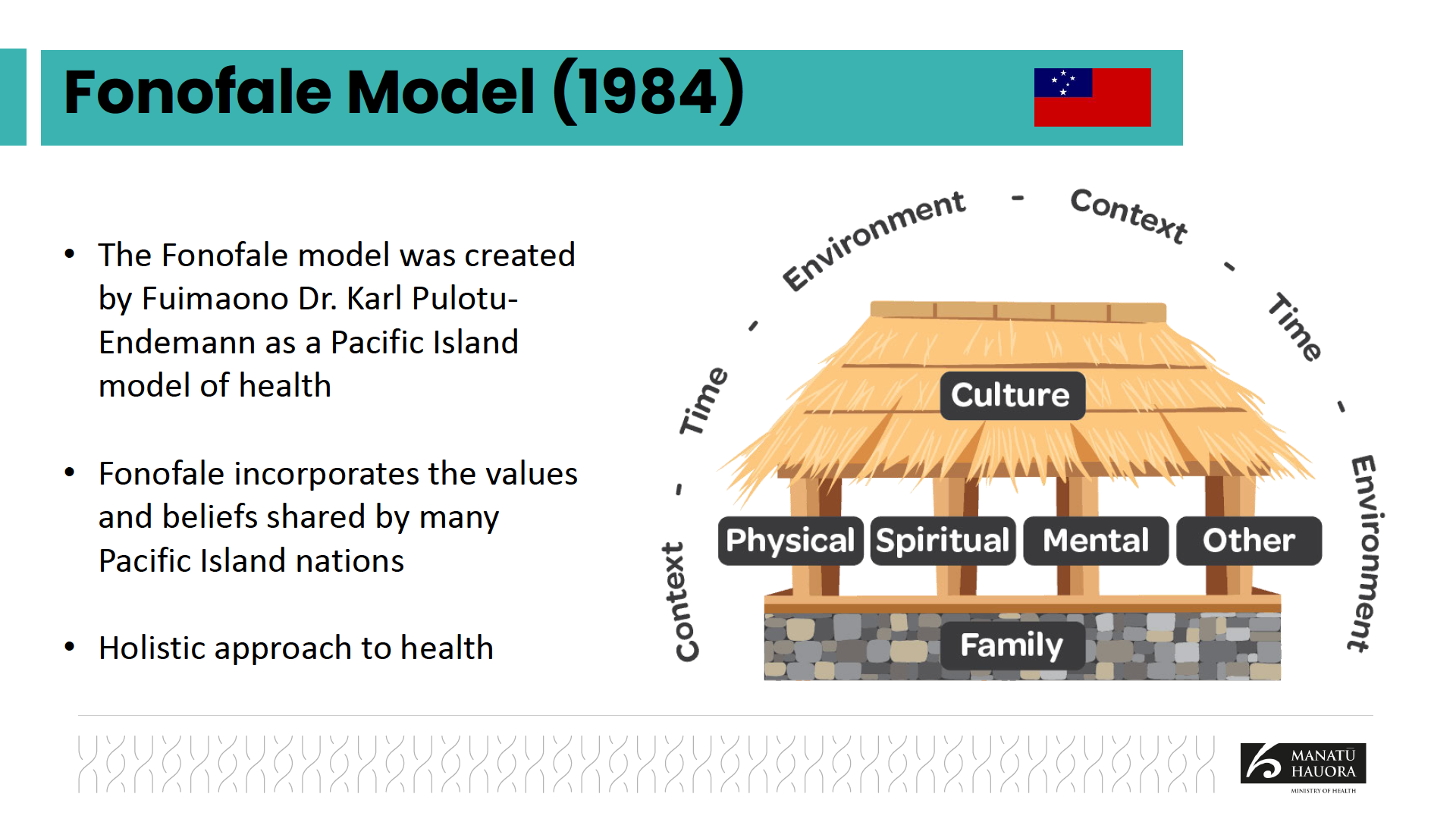
15. The Fonofale model is a pan-Pacific Model of health created for the New Zealand context.3 The
model incorporates values and beliefs that are shared across other Pacific groups, including
the Cook Islands, Niue, Fiji, Tokelau and Tonga. The model incorporates the metaphor of a
Samoan fale (house) with the foundation or floor, posts and roof encapsulated in a circle to
promote the philosophy of ho
UNDER lism and continuity. The elements of the Fonofale model are
outlined below.
a. The foundation represents the central role of family, including extended family and those
linked from partnerships or agreements.
b. The roof represents culture, including beliefs and value system that provide protection and
shelter for life. This element can be traditional beliefs tied to a specific Pacific identity but
RELEASED
can also focus more on European identity and values.
c. The 4 Pou that support these structures are spiritual, physical, mental and ‘other’ aspects of
wellbeing, including sexuality, socioeconomic status and gender.
2 Mahu (Hawai'i & Tahiti), Vaka sa lewa lewa (Fiji), Palopa (PNG), Fa'afafine (Samoa), Akava'ine, (Rarotonga), Fakaleiti
(Tonga), Fakafifine (Niue).
3 Developed in 2001 by Samoan-born academic Fuimaono Karl Pulotu-Endemann.
3
d. The Fale is surrounded by the environment, time and context. Environment focuses on the
physical setting. Time and context refer to respectively, a point in time that impacts Pacific
people and the surrounding socioeconomic, political, legal, or personal context.
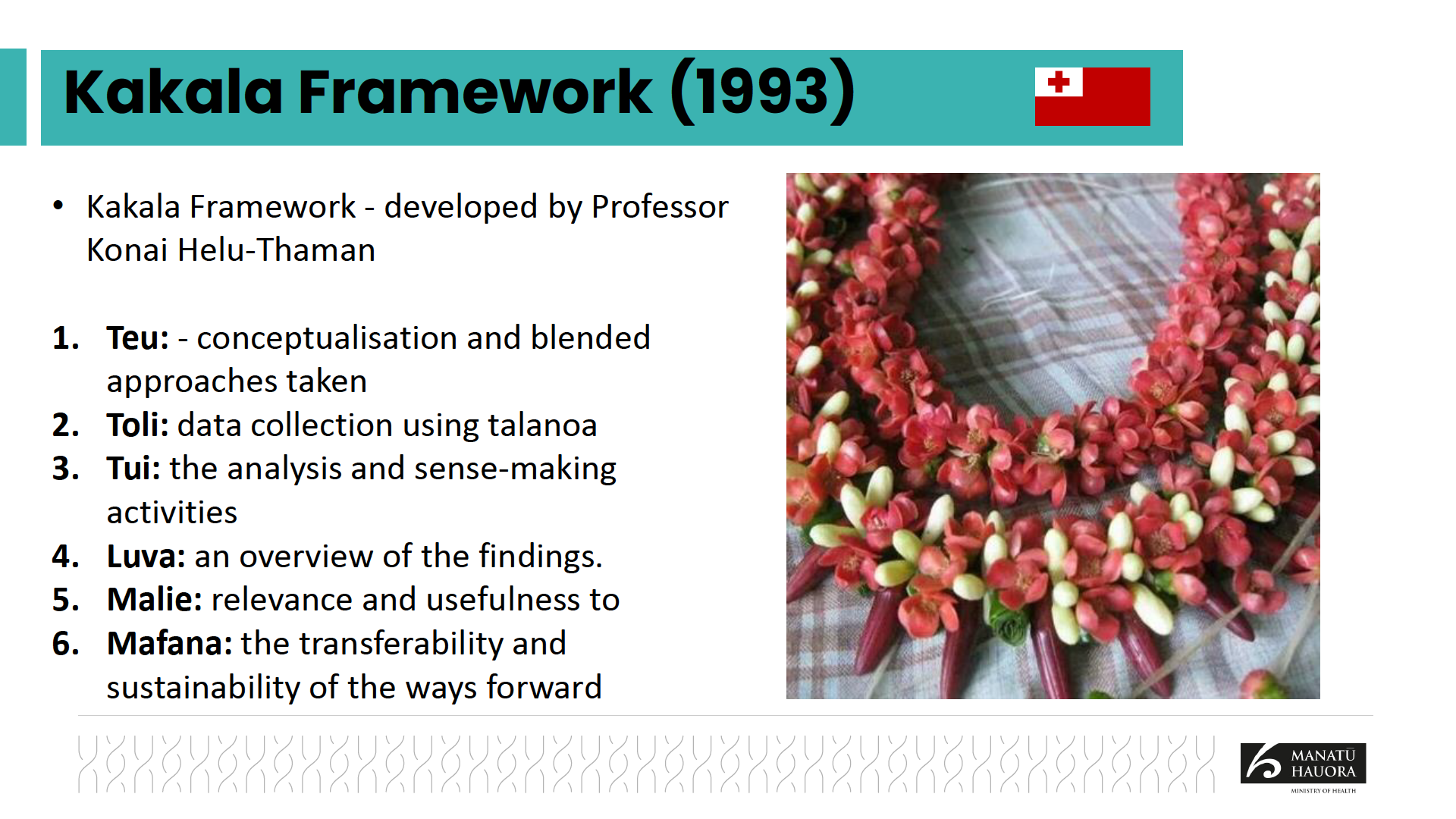
16. The Kakala framework is a Tongan model that represents a garland made of flowers and leaves
to be worn on special occasions or presented to a special guest as a sign of ofa (love) and
faka’apa’apa (respect).4 The framework aims to ensure that Pacific approaches, values and
perspectives are interwoven into al aspects of research. It also demonstrates collaboration,
sharing of resources and the passing of skil s to the next generation. The 6 components of the
Kakala framework are outlined below.
a. Teu: This the first phase of the making of a kakala and also the first step of the kakala
research framework process. It encompasses the thinking, identifying information to be
1982
gathered, the planning and design of the next steps to fol ow.
b. Toli: This phase is about gathering the flowers to make the kakala. The toli phase invo
ACT lves
the col ecting of the data. If the previous teu step has considered who is best to col ect the
data, the best sources of this data, and how best to col ect the data, then it will naturally
lead to the collection of the best data to inform decisions to support Pacific wellbeing.
c. Tui: This phase is about creating the kakala. It involves bringing together what has been
col ected, applying cultural y nuanced methods and lens to tell the story of Pacific peoples.
d. Luva: This phase is about gifting the completed kakala. This is the handing over of the
kakala with sincerity, humility and honour to the wearer, acknowledging the ha
INFORMATION rd work and
sacrifice taken to create the garland. It honours those who have given their voice and
knowledge to help the research.
e. Mālie: This phase signifies the evaluative process of ensuring that the consultation was
worthwhile. Some considerations during this evaluative process include whether the
OFFICIAL
communities it was designed to help would benefit from it, whether the process made
sense, and whether it served the needs of the communities.
THE
f. Māfana: This phase describes a continual process of reflection on the work. It is a place
where everyone involved is giving heartful expressions as a result of the work as it is being
woven. It too needs to be present at every stage to ensure the best kakala is being woven
together. UNDER
17. Essential y, Pacific health models describe how the health of Pacific peoples is determined by
the balance of different dimensions including spiritual, cultural as well as environmental
factors on health. They encompass the cultural, values and belief of health to Pacific peoples
and recognises Pacific-specific knowledge to inform what works for Pacific peoples.
Next steps
RELEASED
18. The Pacific Health team can provide further information about this topic at your request.
4 Developed in 1993 by Professor Konai Helu Thaman.
4
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 Engagements
Engagements
1982
ACT
•
Health Act, Section 3F, Public Health Agency to consult in order to
ensure that the views of the public, persons involved in the provision
of personal health services and public health services, and other
persons are able to be considered in the formulation of the Public
Health Agency’s advice to the Director-General
INFORMATION
• Public Service Commission – Long-term Insights Briefing
OFFICIAL
•
THE
Community and professional bodies (development of Te Mana Ola)
UNDER
• Coordination with interagency groups to avoid ‘engagement fatigue’
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 Role of Data
Role of Data
1982
•
ACT
Regular, up-to-date info on health outcomes, access, experience & quality of
health care
• Recognition of the diversity of Pacific peoples (ethnic-specific data where
possible)
INFORMATION
• Data that is focused on the strengths of Pacific people & communities that
can be built on
OFFICIAL
• More info on the experiences of specific groups (e.g. LGBTQIA+/
THE
MVPFAFF+**, tagata sa’ilimalo, people with mental health needs, rural
communities, Māori + Pacific).
UNDER
•
**Mahu (Hawai'i & Tahiti), Vaka sa lewa lewa (Fiji), Palopa (PNG), Fa'afafine (Samoa), Akava'ine, (Rarotonga),
Fakaleiti (Tonga), Fakafifine (Niue).
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED