link to page 2 link to page 4 link to page 7 link to page 9 link to page 10 link to page 12 link to page 16 link to page 17 link to page 20 link to page 23 link to page 26 link to page 26 link to page 27 link to page 29 link to page 31 link to page 31 link to page 31 link to page 33

Productivity Report
January 2024
Contents
Summary ....................................................................................................................................................... 2
Report findings .............................................................................................................................................. 4
Future productivity measurement and reporting ......................................................................................... 7
1.
Overarching productivity measurement ............................................................................................... 9
Overview of the analysis included in this report ................................................................................ 10
1.1 Case-weighted hospital discharges per FTE .................................................................................. 12
1.2 FTE growth over time .................................................................................................................... 16
1.3 Changes in complexity of patient needs over time ...................................................................... 17
1.4 National and regional Case-weight changes over time ................................................................ 20
2.
International Comparisons ................................................................................................................. 23
3.
Additional efficiency measures ........................................................................................................... 26
Percentage Long Stay (>7 Days) – medical and surgical episodes of care .......................................... 26
3. Plan for developing productivity measurement and reporting .............................................................. 27
Appendix A: Limitations of Data and Refinement of Measures ................................................................. 29
Appendix B: Methodology .......................................................................................................................... 31
Case-weights per FTE .......................................................................................................................... 31
Long stays (>7 days) – medical and surgical episodes of care ............................................................ 31
Appendix C – Additional figures .................................................................................................................. 33
1
Summary
This preliminary report represents a baseline and continuing commitment to the development of robust
measurement, understanding and improvement of health system productivity as part of the evolving
wider system performance and reporting framework.
The report outlines the trends and some drivers of productivity in the former District Health Boards and
Te Whatu Ora since the financial year 2015/2016, through exploration of an overarching (labour)
productivity measure: Case weighted hospital discharges per full time equivalent employee (CWD / FTE).
The focus is on clinical and support FTE, with case-weights per total FTE reported in the appendices. All
case-weights that were discharged from a public hospital and funded with a purchaser code of publicly
funded are included in this analysis – including ACC events. Case-weights per Clinical and Support FTE
trended down between 2015/16 and 2022/23 with the most notable drop occurring during 2019/20 –
2021/22. However, there has been a longer-term decrease in productivity which has been observed
globally, primarily due to increasing costs of inputs.
Healthcare in New Zealand faces intricate challenges stemming from geographical variations, changing
demographics, and diverse disease trajectories. Particularly in remote regions, healthcare access and
equity present unique complexities. Our productivity measures must evolve considering these
complexities, including changing illness patterns, demographic shifts, and social determinants like
socioeconomic status. A truly effective healthcare system must embed these factors into its approach to
improve wider wellbeing in our nation. It is not within the scope of the analysis within this preliminary
report to adjust for these factors – this will occur as our measurement and understanding of their
contribution to productivity evolves.
Finally, it is critical to acknowledge that productivity measurement is about identifying how policy,
processes and systems can best support the health workforce to do the right things, for the right patients,
at the right times, and in the right settings. Productivity measurement helps to identify where people are
spending time doing work due to inefficiencies elsewhere in the system – this is wasteful and is
undoubtably frustrating. Additionally, the productive delivery of health care requires the inputs of many
individuals, teams, departments and organisations. Measuring productivity helps with identifying how
these inputs could be better coordinated. For these reasons, the focus of our productivity measurement
and reporting work programme is on major patient pathways within the system – taking a patient and
system view to support addressing the fundamental drivers of productivity.
Limitations
While CWDs capture a component of employed sector activity, there are many other areas of activity that
the employed workforce contributes to each year e.g., more than 700,000 non-admitted Emergency
Department (ED) attendances, more than 2 million medical & surgical outpatient attendances, and many
community based services such as district nursing and community mental health. Future productivity
reporting will move towards capturing this activity to enable greater insights into this component of
system performance.
Additionally, there are limitations to the use of CWD / FTE metric including but not limited to:
2
• it does not fully capture complexity of patient needs and impact on workload, and how they may
change over time
• alone it does not enable understanding of:
o the quality and safety of health care (including acceptability and appropriateness of care)1
o the cost-effectiveness of care
• it does not provide clarity on the respective drivers of any changes in productivity (e.g.
contribution of capital, regulation etc)
• the creation of Te Whatu Ora is enabling the greater standardisation of business rules, clinical
coding, FTE definitions, and reporting. This means that as we improve our financial and activity
systems and reporting there will likely be shifts in the metric.
More information detailing inclusions and exclusions as to what data is captured for the case-weights and
FTE used in this analysis can be found under Appendix B: Methodology.
1 As noted in the independent baseline review of hospital & specialist services “It is widely recognised that
technical efficiency measures can understate productivity where there is investment into improving the quality of
care (better outcomes per output). The Centre for Health Economics in York has published research (Arabadzhyan
et al., 2021) on a quality-adjusted productivity index for the period for the English NHS for 2004-2018-19. This
approach quality-adjusts outputs for changes in in-hospital survival rates after heart attack and stroke, patient-
reported outcomes, life expectancy and the timeliness of care waiting times.” Refer p. 147. Note waiting time for
patients can consist of several parts, such as waiting for a first specialist appointment, waiting for diagnostic
procedure or test, waiting for procedure. This total time waiting is the patients experience with cost to society of
unproductive workforce.
3
 Report findings
Report findings
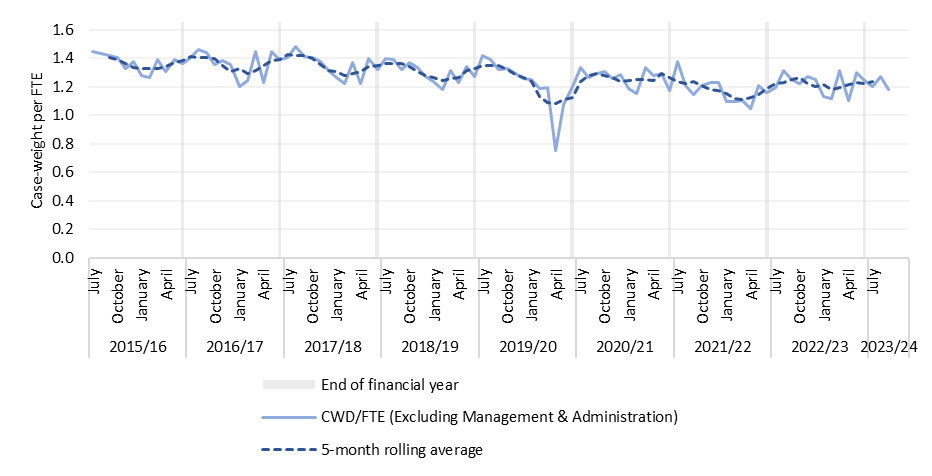
Case-weights per Clinical and Support FTE trended down between 2015/16 and 2022/23, from an average
of 1.37 in 2015/16 to an average of 1.23 in 2022/23 (1.5% decrease per annum). While the most notable
drop occurred during 2019/20 – 2021/22, there has been a longer-term decrease in productivity. This
trend has been observed in comparable health systems, including the countries across the EU and the
NHS. Decreased productivity has primarily been due to increasing costs of inputs, such as increased
expenditure for labour and for goods and services.
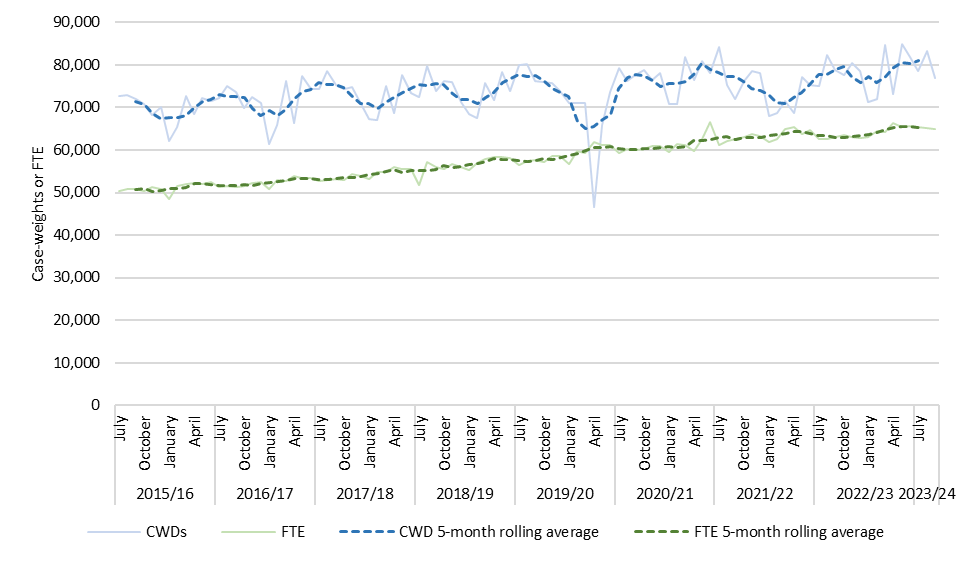
Figure 1: Case-weights per Clinical* and Support FTE, Nationally, July 2015 – September 2023
Source: NMDS, Finance, EY Analysis
*Clinical Personnel includes Medical Personnel, Nursing Personnel, and Allied Health Personnel
A 5-month rolling average has been applied to all graphs either nationally or regionally to smooth the variation in monthly data and help
illustrate the seasonality of productivity, which tends to be lowest over December to February, and highest over July to September.
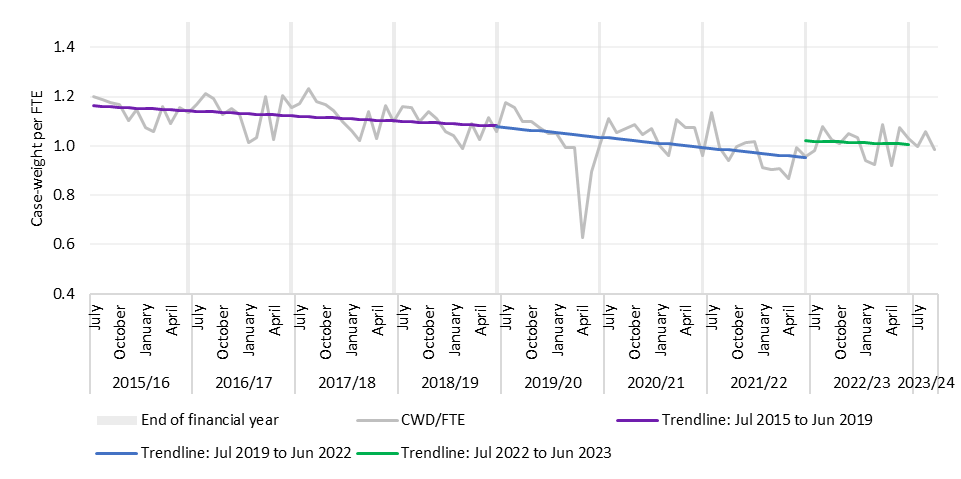
To better understand the trends in case-weights per Clinical and Support FTE, the time series has been
broken into three distinct periods with a least square regression slope calculated to see the relative
change over period:
• Pre-Covid 19 pandemic (July 2015 through to June 2019)
• During Covid 19 pandemic (July 2019 through to June 2022)
• Post-Covid 19 pandemic (July 2022 through to June 2023)
This shows there was a 1.8% drop per annum in case-weights per Clinical and Support FTE over the ‘Pre-
Covid’ period, followed by a steeper drop during the ‘Covid-19’ period, and a continuation of the trend
with a 2.6% drop in case-weights per FTE in the ‘Post-Covid’ period.
4
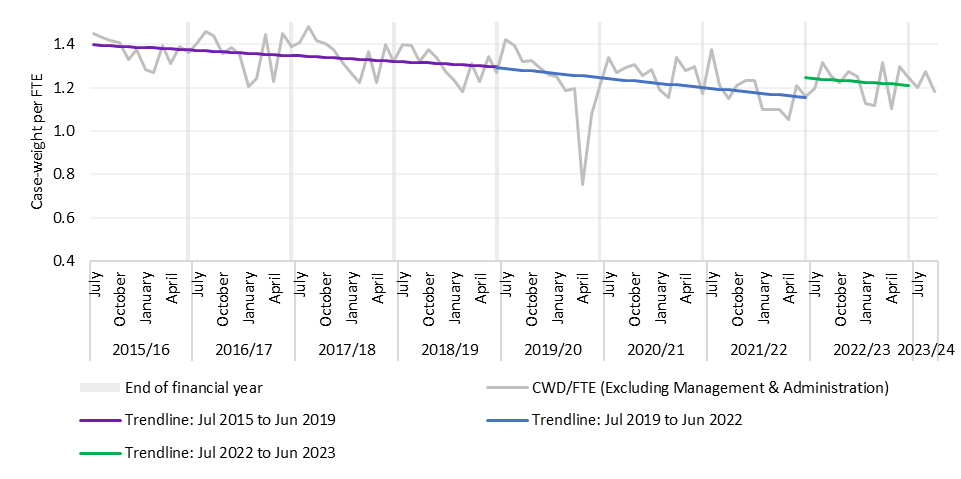 Figure 2: Case-weights per Clinical* and Support FTE, Nationally, July 2015 – September 2023
Figure 2: Case-weights per Clinical* and Support FTE, Nationally, July 2015 – September 2023
Source: NMDS, Finance, EY Analysis
*Clinical Personnel includes Medical Personnel, Nursing Personnel, and Allied Health Personnel
The main driver of these trends has been the much faster growth in labour input (FTEs) than output
growth (case-weights), which has occurred across all three-periods. Between 2015/16 to September 2023,
Clinical and Support FTE grew faster than case-weights, driving case-weights per Clinical and Support FTE
down. From June 2016 to June 2023, Clinical and Support FTE grew 25.3% while from 2015/16 to 2022/23,
case-weights grew 12.1%.
5
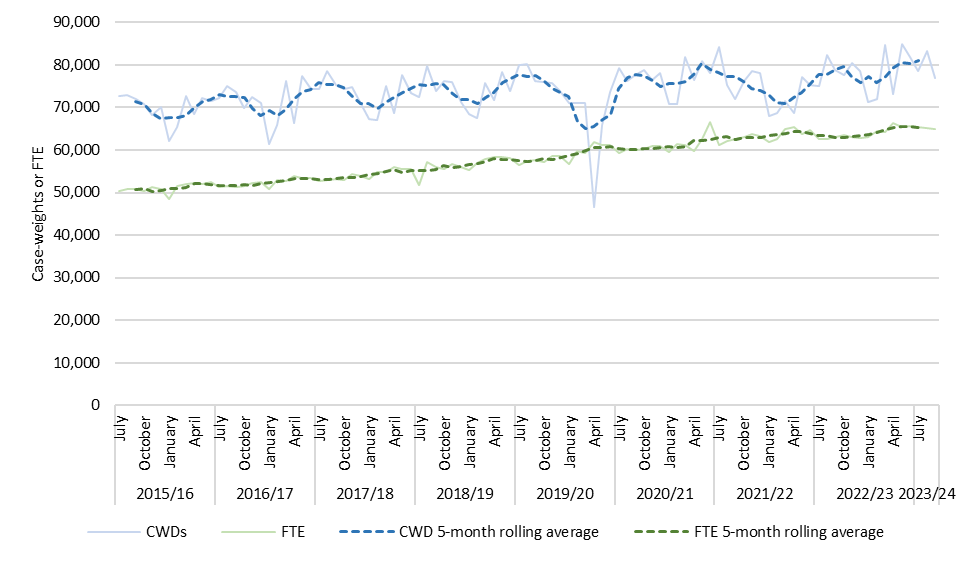 Figure 3: Case-weights and Clinical* and Support FTE, Nationally, July 2015 – September 2023
*Clinical Personnel includes Medical Personnel, Nursing Personnel, and Allied Health Personnel
Figure 3: Case-weights and Clinical* and Support FTE, Nationally, July 2015 – September 2023
*Clinical Personnel includes Medical Personnel, Nursing Personnel, and Allied Health Personnel
Employment Agreements and Staffing Conditions
There have been notable shifts in employment models throughout this time: the implementation of safe
staffing for nursing from 20162, the changes in safe rostering changes for registered medical officers
(Junior Doctors) from 2019 and the increase in senior medical officer non-clinical time. These employment
model changes through collective employment agreements terms and conditions are intended to improve
safety and workforce well-being – with expected benefits for patient care and workforce recruitment and
retention.
These employment model changes have generally increased the quantity of labour inputs per output
delivered, contributing to decreasing CWDs per Clinical and Support FTE. In addition, continued challenges
with more frequent bargaining, cost creep relating to additional payments in addition to recruitment
issues, and higher rates of sick leave have contributed to decreasing labour productivity.
2 With Ministerial direction to expedite implementation in 2018/19.
6
Future productivity measurement and reporting
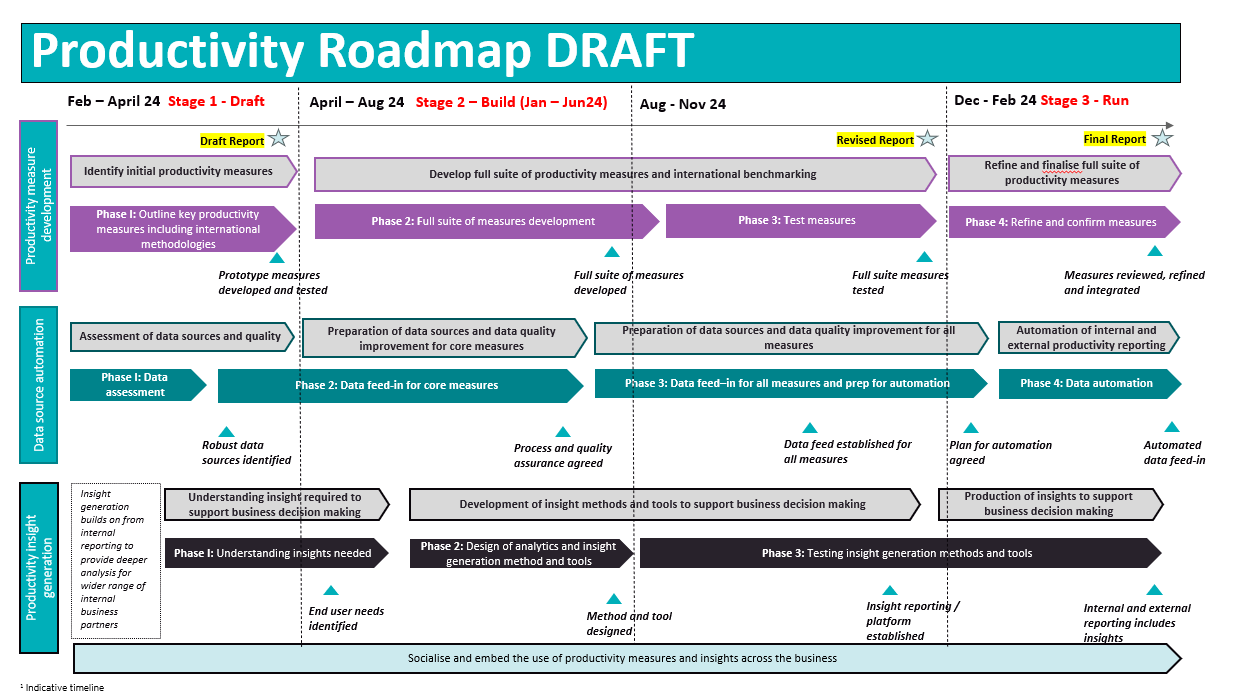
Productivity measurement and reporting will continue to be developed. Along with two overarching
productivity measures, a modular suite of productivity, efficiency and performance measures will be
developed for major patient journeys within the health system, to have insight into optimising efficiency
of processes and systems to support the delivery of healthcare. This is anticipated to be a twelve month
programme of work with ongoing development and refinement into the future, as the high level roadmap
overleaf shows.
There are three components to developing productivity measurement and reporting:
1. Develop measures that help understand trends in productivity and relevant drivers
2. Consolidation and automation of data sources including data quality assessment and control
3. Productivity insight generation to increase the use of productivity reporting to support business
decision making.
7
8
1. Overarching productivity measurement
The Te Whatu Ora Productivity Working Group have agreed to an approach to productivity measurement
and reporting with a 12-month roadmap. This initial productivity report includes the following:
-
A high level productivity measure, case-weighted hospital discharges (Case-weights) per Full-Time
Employee (FTE) that reports on productivity trends for the whole organisation, focused on Clinical
and Support FTE
-
Approach and roadmap for developing productivity measures and regular robust reporting.
Overview of overarching organisational productivity measure development and reporting
This report provides a preliminary view of health system productivity using one overarching measure of
organisational productivity Case-weights per FTE. We intend to continually refine this measure alongside
a new measure in development: a New Zealand Weighted Activity Unit per FTE to include outpatient and
community-based service delivery weighted for relative costs as available – giving greater breadth of
productivity measurement within the organisation.
The current health system is expansive and multifaceted, particularly within hospital and specialist
services. This presents significant challenges, including the present data capture system which does not
allow us to suitably assign FTEs to specific tasks and activities performed. The breadth and complexity of
the purchase unit range presents additional hurdles due to its large scale; this further compounds the
error of Case-weight alone being an incomplete unit for the capture of total output.
Addressing these issues will be a priority moving forward. Upgrading our data-gathering mechanisms,
refining our systems, and developing more precise tools for tracking FTE allocation will be essential steps.
It's critical to improve the accuracy and reliability of our data to ensure a more effective and efficient
hospital system that genuinely reflects activity and output.
Case-weights per FTE was selected for this first report, because the measure can be reasonably calculated
and analysed within the currently available data sources. It is a measure that has been used historically
and is known and understood by stakeholders and can be simply explained. This measure will be further
modified in future reporting for improvements in data and breadth of inclusion. All case-weights that were
discharged from a public hospital and funded with a purchaser code that is publicly funded are included
in this analysis – including ACC events. More information detailing inclusions and exclusions as to what
data is captured for the case-weights and FTE used in this analysis can be found under Appendix B:
Methodology
For future iterations of productivity reporting, we aim to develop a measure similar to Australia’s NWAU
(National Weighted Activity Unit). This measure provides a standardised way to price public hospital
services based on the number and complexity of patients treated. The NWAU considers activity across a
range of services delivered at public hospitals, including inpatient services, outpatient services, and
emergency department activity. All activity is weighted for complexity, with one NWAU corresponding to
an ‘average’ public hospital service, and provides an indicator for hospital efficiency, as well as a means
of comparing hospitals or regions. As the maturity of New Zealand productivity measurement improves,
the aim would be to consider international benchmarks of productivity in similar health systems.
9
In addition, we recognise the importance of measuring and understanding population changes including;
population demographics, changing disease trajectories, particularly for chronic conditions, and the
impact of socioeconomic factors on health and illness. We are also seeking ways to include the
geographical distribution of services and its influence on productivity as we further develop measurement
and understanding of productivity. We recommend that further refinement of productivity measures
include the development of a complete set of measures will account for changes in the quality of care and
case complexity over time.
Overview of the analysis included in this report
Note that inpatient data used for the analysis below has missing data for the districts of Tairāwhiti and
West Coast for the months of July 2023 through to September 2023. On average, Tairāwhiti and West
Coast account for 0.9% and 0.4% of total annual case-weights, respectively, so the exclusion of the data
is unlikely to materially impact on findings.
The following analysis has been calculated using an FTE as full time equivalent employee (40 hours per
week) and is calculated as the total number of hours employed per week (to a maximum of 40 hours per
week), divided by 40. There have been two notable step changes in Management and Administrative FTE
since 2015/2016. One related to the management of the COVID-19 pandemic and the other occurred
when District Health Board management personnel, shared service agencies and some Ministry of Health
teams joined Te Whatu Ora on 1st July 2022 due to health system reform. Productivity has been measured
through changes in case-weighted hospital discharges compared to FTE and the analysis for this report
considered both measures: case-weights per all FTE and case-weights per Clinical and Support FTE
(excluding management and administrative FTE). In addition to the notable jumps in Management and
Administrative FTE, there have also been increasing FTE for Nursing Personnel and Medical Personnel over
2015/16 – 2022/23. Through Care Capacity Demand Management (CCDM) and various SMO and nursing
agreements, this has included changes to improve working conditions and working hours for staff. While
these changes are important for improving the work environment for staff and patient care, in the context
of productivity, these changes mean that at least initially case-weights per FTE decrease as FTEs grow at
a faster rate than case-weights have increased, other things being equal.
As most of the results mirrored each other the decision was made to focus on case-weights per Clinical
and Support FTE with Management/Administration personnel excluded in this report. Appendix C has
additional figures reporting on productivity measures for case-weights per all FTE.
10
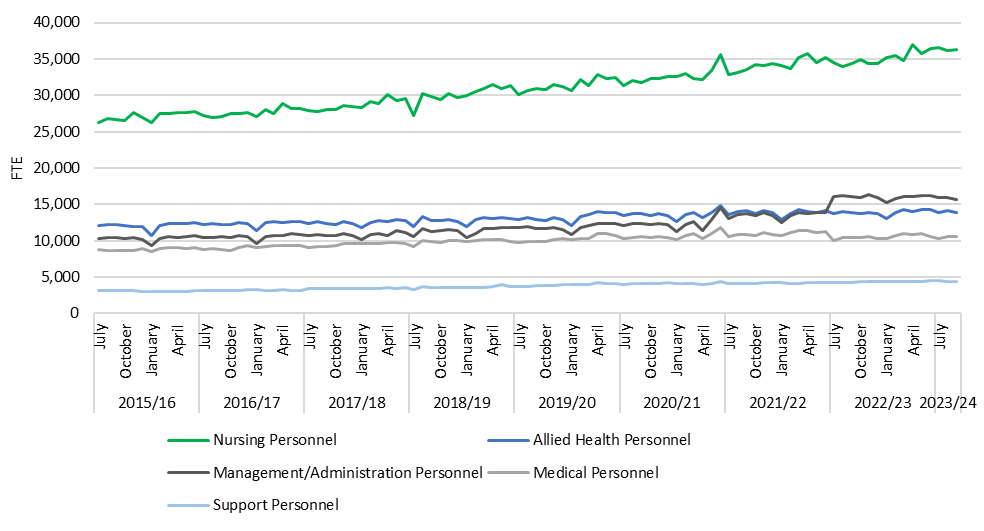 Figure 4: National monthly FTE count by professional group, July 2015 – September 2023
Figure 4: National monthly FTE count by professional group, July 2015 – September 2023
Source: Finance, EY Analysis
The figure above includes national FTE count by FTE type (Medical, Nursing, Allied Health,
Management/Administration, and Support Personnel). Over the period, Nursing Personnel increased the
most in actual terms, however Management/Administration Personnel increased the most in percent
terms (39.7% for Nursing Personnel and 53.7% for Management/Administration Personnel between July
2015 and July 2023), likely due to the two notable jumps seen in July 2021 and July 2022. The 2021 jump
likely came from managing the Covid-19 pandemic, and the step-up in 2022 likely came from the health
system reform, which included many personnel across the motu from shared service agencies, and
transfers from the Ministry of Health, becoming part of Te Whatu Ora as Management and Administrative
Personnel.
11
1.1 Case-weighted hospital discharges per FTE
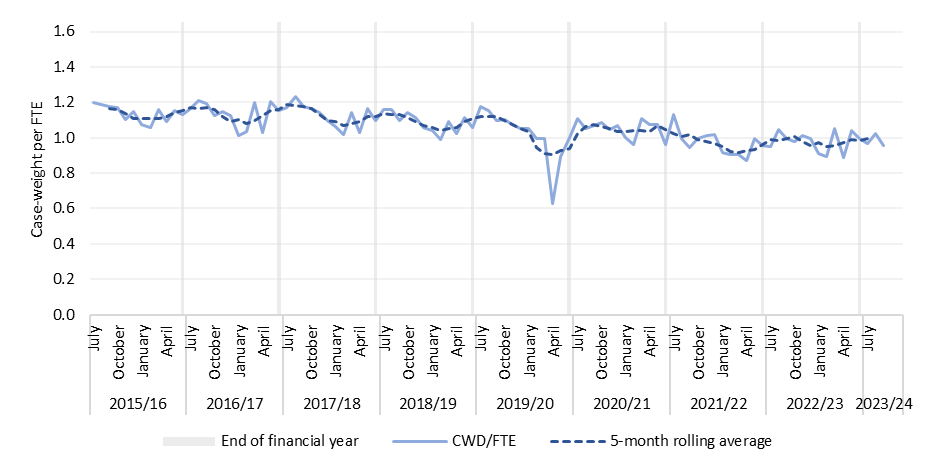
From 2015/16 to September 2023, nationally case-weights per FTE have fluctuated between 0.7 and 1.4
and have on average dropped over the period. From 2015/16 to September 2023, nationally case-weights
per FTE (excluding Management and Administration Personnel) have trended downwards from 1.45 case-
weights per FTE in July 2015 to 1.20 in July 2023.
In addition to the overall decrease in case-weights per FTE over the period, there is also an annual seasonal
trend; case-weights per FTE tends to be lowest over December through February, and peak over July to
September, which will reflect the impact of the holiday period and seasonal illnesses (FTE numbers do not
have as notable seasonality).
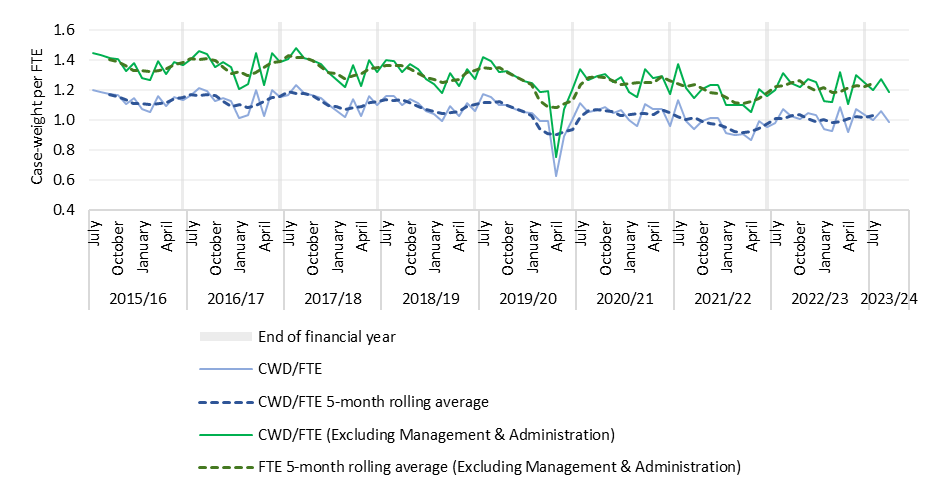
Figure 5: Case-weights per Clinical* and Support FTE vs Total FTE, Nationally, July 2015 – September
2023
Source: NMDS, Finance, EY Analysis
*Clinical Personnel includes Medical Personnel, Nursing Personnel, and Allied Health Personnel. Note that Y-axis has been truncated to 0.4 Case-
weight/FTE to illustrate the relationship clearer.
Case-weight discharges has been measured against two sets of FTE in Figure 5: ‘Clinical and Support FTE’
including Nursing, Medical, Allied Health and Support Personnel, and Total FTE, which includes all ‘Clinical
and Support FTE’ as well as Management and Administration personnel. The data shows that the
percentage decline in Case-weight per FTE from 2015/16 to 2022/23 was -10.3% (1.37 down to 1.23) for
Clinical and Support FTE versus -11.0% (1.14 down to 1.01) for Total FTE.
12
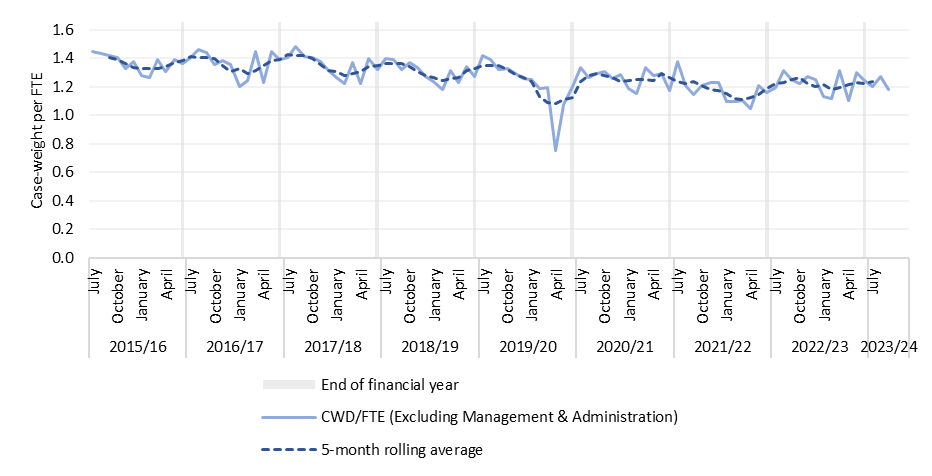 Figure 1: Case-weights per Clinical* and Support FTE, Nationally, July 2015 – September 2023
Figure 1: Case-weights per Clinical* and Support FTE, Nationally, July 2015 – September 2023
Source: NMDS, Finance, EY Analysis
*Clinical Personnel includes Medical Personnel, Nursing Personnel, and Allied Health Personnel
The slope of trend in Figure 2 on the following page has been separated into three time periods to better
understand the trend in case-weights per Clinical and Support FTE before, during and after the Covid-19
pandemic. Allowing for seasonal changes, the periods all start in July and end in June which does not fully
correspond to with the periods of lock-down related to the Covid-19 pandemic. The slopes for each
segment of trendline are shown in Figure 2 and Table A below: all three periods have a negative slope,
with the most recent time period (July 2022 – June 2023) having a more negative slope, indicating a faster
rate of decline than the ‘Pre Covid’ period – which suggests that productivity measured by case-weights
per Clinical and Support FTE continues to decrease at a rate faster than the immediate years pre-
pandemic.
13
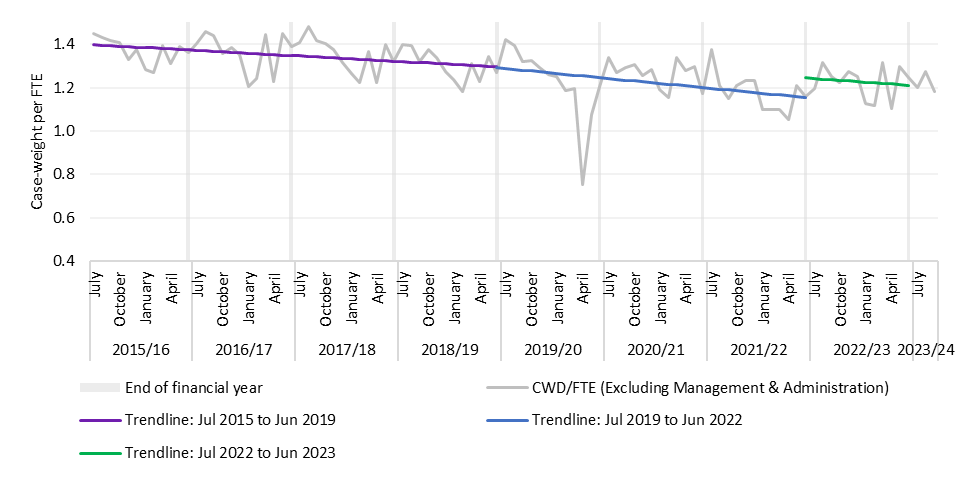
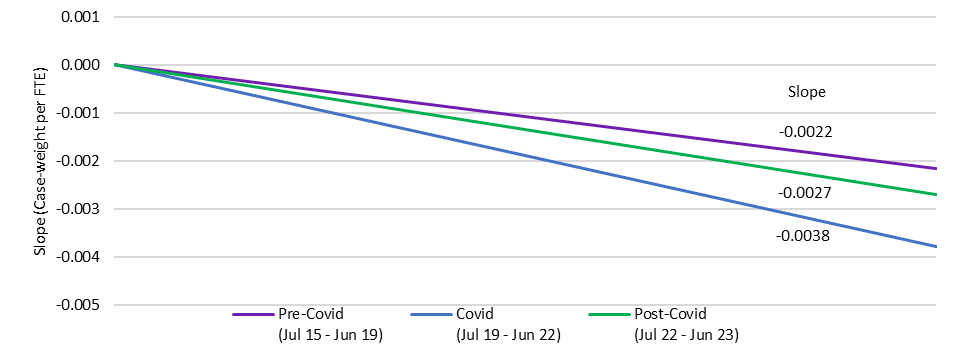 Figure 2: Case-weights per Clinical* and Support FTE, Nationally, July 2015 – September 2023
Figure 2: Case-weights per Clinical* and Support FTE, Nationally, July 2015 – September 2023
Source: NMDS, Finance, EY Analysis
Note: case-weight data is unavailable for July 2023 – September 2023 for Tairāwhiti and West Coast District. This will not have an impact on the
trendlines as the trendlines only go to June 2023. Axis has been truncated to start at 0.4 Case-weight/FTE
Figure 6: Slope of Case-weights per Clinical* and Support FTE, Nationally, Three Periods over July 2015
– June 2023
Source: NMDS, Finance, EY Analysis
14
Table A: Slope of Case-weights per Clinical* and Support FTE, Nationally, Three Periods over July 2015
– June 2023
Source: NMDS, Finance, EY Analysis
Slope (Case-weight per
Average percent change per
Period
Clinical* and Support
annum
FTE)
Pre-Covid, July 2015 – Jun 2019
-0.0022
-1.8%
Covid, Jul 2019 – Jun 2022
-0.0038
-3.5%
Post-Covid, Jul 2022 – Jun 2023
-0.0027
-2.6%
Note that due to seasonal changes, the periods all start in July and end in June. This means the periods may not fully align with impacts due to
Covid-19.
The main driver of these trends is the much faster growth in labour input (FTEs) than output growth (case-
weights), which has occurred across all three-periods. Over 2015/16 to September 2023, Clinical and
Support FTE grew faster than case-weights, driving case-weights per Clinical and Support FTE down. From
June 2016 to June 2023, Clinical and Support FTE grew 25.3% while from 2015/16 to 2022/23, case-
weights grew 12.1%.
Over the 2022/23 financial year there is a 1.5% increase in Clinical and Support FTE vs 0.8% increase in
all FTE, indicating that post Covid increases are mainly clinical. This is influencing the post-covid
productivity 'drop’ as although there is the same number of case-weights delivered for case-weights per
Clinical FTE compared to case-weights per all FTE (see Appendix C) - Clinical and Support FTE are the
fastest growing personnel categories for that year.
15
1.2 FTE growth over time
Clinical and Support FTE nationally have increased from 52,475 FTE at the end of 2015/16 to 65,079 by
September 2023, an increase of 24.0%. Over the same time, the sum of case-weights (annually from July
- June) has increased from 838,923 in 2015/16 to 940,720 for the 2022/23 financial year, an increase of
12.1%. In other words, Clinical and Support FTE (inputs) have increased at roughly twice the rate of case-
weights (outputs) so even though the rate of decrease in case-weights per FTE has improved since the
Covid-19 pandemic, labour productivity using this measure continues to decrease – which likely reflects a
combination of capital constraints (physical infrastructure, information technology) and other factors
(policy, regulation, collective agreements, culture and staff engagement / wellbeing).
Figure 3: Case-weights and Clinical* and Support FTE, Nationally, July 2015 – September 2023
*Clinical Personnel includes Medical Personnel, Nursing Personnel, and Allied Health Personnel
16
1.3 Changes in complexity of patient needs over time
The relative complexity of patient need can impact on workload and the scope and mix of resources
required. If complexity of patient need is increasing then it is more likely that additional workforce
resources will be delivered to deliver quality and safe health care.
Figures 7-10 help with understanding how complexity of patient needs have been changing in terms of
multi-morbidity, based on coded clinical characteristics for acute and arranged events for medical,
surgical and some maternity services. The measures provide an indication of disease burden and multi-
morbidity – they do not indicate severity of disease or acuity.
• Figure 7 shows trends in average length of stay (ALOS) and the average case-weight per
discharge over the period 2010 to 2022. For much of the period, ALOS was reducing,
reflecting ongoing efficiency improvements, but started to increase from 2017 through
to 2022. The average case-weight per discharge declined initially before increasing from
2014, and steeply from 2018. These trends indicate increasing workload and complexity
of care.
• Figures 8 and 9 compare the average case-weight per discharge to two measures of
multi-morbidity based on diagnosis coding and one-year mortality risk. Each measure
suggests generally continuing, modest growth in complexity of care needs in terms of
multi-morbidity.
Figure 7: ALOS and average case-weights
Figure 8: Change in M3 score and case-weights
per discharge, 2010 – 2022
per discharge from 2010, 2010 – 2022
Source: SI&I Analysis
Source: SI&I Analysis
17
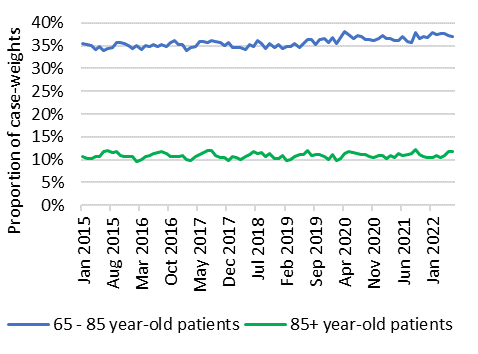
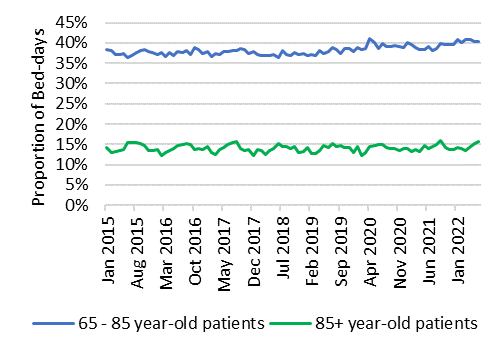

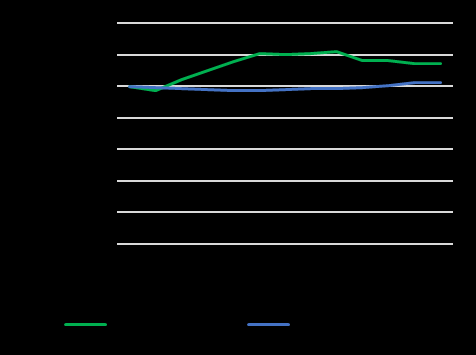 Figure 9: Change in Charlson score and case-
Figure 10: Change in M3 score and Charlson score
weights per discharge from 2010, 2010 – 2022
from 2010, 2010 – 2022
Figure 9: Change in Charlson score and case-
Figure 10: Change in M3 score and Charlson score
weights per discharge from 2010, 2010 – 2022
from 2010, 2010 – 2022
Source: SI&I Analysis
Source: SI&I Analysis
The figures below look at the proportion of acute and arranged medical and surgical case-weights and
bed-days for patients 65 years-old or older. Overall, the proportion of case-weights for patients which
are 65+ has increased from 45.9% to 48.1% from 2015/16 to 2022/23, and the proportion of bed-days
for patients which are 65+ has increased from 51.6% to 52.4% from 2015/16 to 2022/23. By ethnicity,
Māori patients who are 65+ had the biggest growth (in actual terms) in proportion of activity, from 3.6%
to 4.5% and 4.0% to 5.0% over 2015/16 to 2022/23 for case-weights and bed-days, respectively. Asian
patients who are 65+ had the biggest growth in percent terms for case-weights (36.5%) and bed-days
(37.7%) over 2015/16 – 2022/23, while Other patients had a notably lower growth in percent terms than
Māori, Pacific, and Asian patients for case-weights (0.9%) and bed-days (1.4%).
Figure 11: Proportion of case-weights for
Figure 12: Proportion of bed-days for patients 65+,
patients 65+, January 2015 – June 2022
January 2015 – June 2022
Source: NMDS, EY Analysis
Source: NMDS, EY Analysis
18
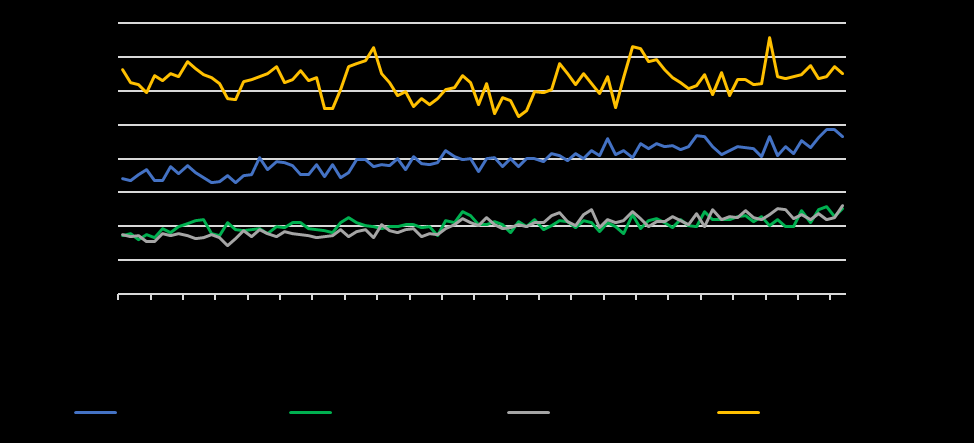
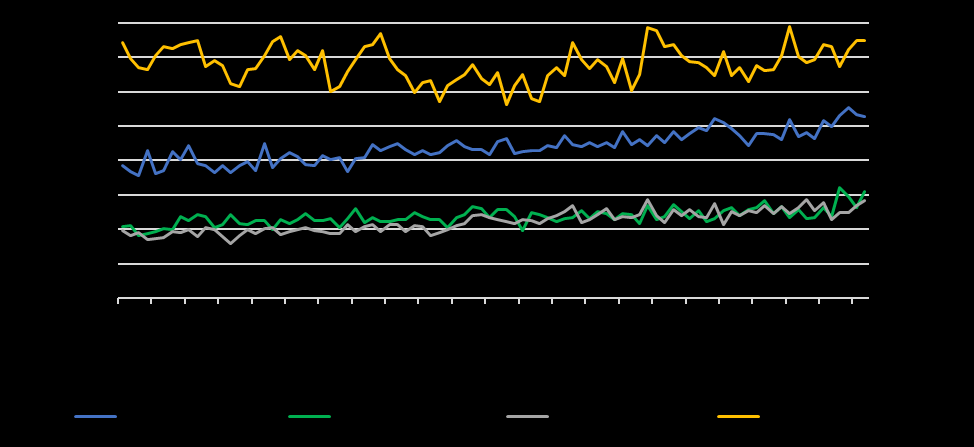 Figure 13: Proportion of case-weights for 65+ patients, by ethnicity, January 2015 – June 2022
Figure 13: Proportion of case-weights for 65+ patients, by ethnicity, January 2015 – June 2022
Source: NMDS, EY Analysis
Figure 14: Proportion of bed-days for 65+ patients, by ethnicity, January 2015 – June 2022
Source: NMDS, EY Analysis
19
1.4 National and regional Case-weight changes over time
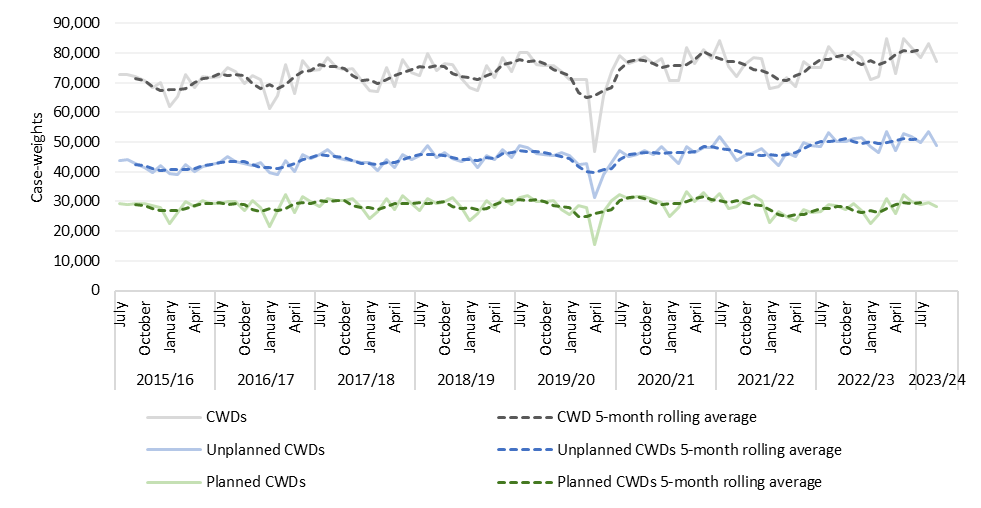
Figure 15: Planned and unplanned case-weights, Nationally, July 2015 – September 2023
Source: NMDS, EY Analysis
Note: case-weight data is unavailable for July 2023 – September 2023 for Tairāwhiti and West Coast District.
Figure 15 depicts the relationship of planned to unplanned cases for case-weight discharges across all
regions. Most notable is the relevant percentage increase of unplanned cases increasing from 59.5% in
2015/16 to 64.3% of total Case-weight discharges in 2022/23. This trend needs to be considered in the
context of the indications of increasing complexity of patient needs as discussed above, and the impact
this is likely to be having on resourcing.
20
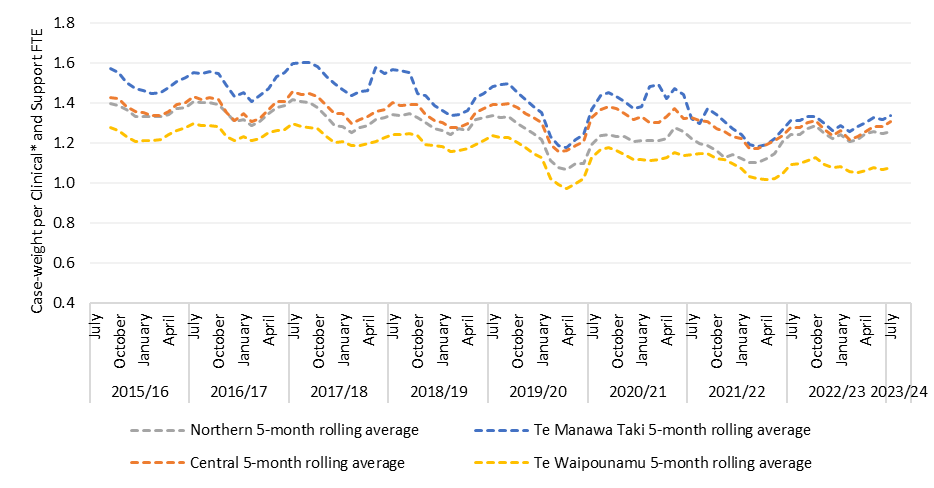 Figure 16: 5-month rolling average Case-weights per Clinical* and Support FTE, by region, July 2015 –
Figure 16: 5-month rolling average Case-weights per Clinical* and Support FTE, by region, July 2015 –
September 2023
Source: NMDS, Finance, EY Analysis
*Clinical Personnel includes Medical Personnel, Nursing Personnel, and Allied Health Personnel. Axis has been truncated to start at 0.4 Case-
weight/FTE
Note that FTE which sit outside of the four regions are excluded from the figure above
The figure above includes a regional view of the 5-month rolling average of case-weights per Clinical and
Support FTE. Across regions, there are seasonal peaks of activity at the start of each new financial year.
The largest decrease in case-weights per FTE occurred in the Te Manawa Taki region – see Table B.
Table B: Change in case-weights per Clinical* and Support FTE by region – 2015/16 and 2022/23
Source: NMDS, Finance, EY Analysis
Region
2015/16 average
2022/23 average
Change
Northern
1.37
1.25
-0.12
Te Manawa Taki
1.51
1.31
-0.20
Central
1.38
1.27
-0.11
Te Waipounamu
1.25
1.09
-0.16
Importantly, over the period July 2015 to September 2023, there has been a shift towards an increasing
number of unplanned hospitalisation case-weights, with more unplanned case-weighted hospital
discharges than planned each month. In 2015/16, 40.5% of case-weights were for planned care, while in
2022/23, 35.7% of case-weights were for planned care. The proportion of case-weights which were
planned is shown by month are shown in Figure 17 below.
21
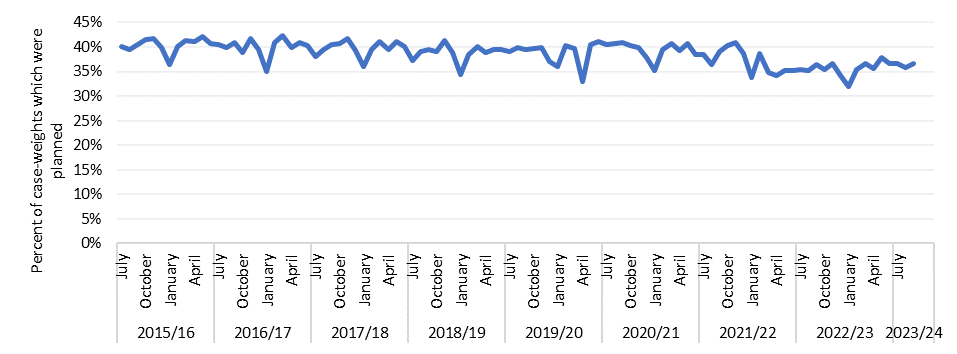
Figure 17: Percent of case-weights which were planned, Nationally, July 2015 – September 2023
Source: NMDS, EY Analysis
Note: case-weight data is unavailable for July 2023 – September 2023 for Tairāwhiti and West Coast District.
22
2. International Comparisons
Productivity measures tend to vary between health care systems. While there are standardised measures
for productivity commonly used to compare productivity between countries, such as the Malmquist
productivity index (MPI) and data envelopment analysis (DEA), many healthcare systems require a more
tailored means of measuring productivity. As such, most countries employ their own method of assessing
productivity or instead track other metrics such as quality or efficiency in its place.
While the Covid-19 pandemic has played a significant role in the global decline in healthcare productivity,
for many countries this decline was evident in the years leading up to the pandemic. For instance, a 2022
study found that a trend of declining or stagnating productivity across many European Union member
countries between 2013-2019 (Lacko, et al, 2022).
Case studies of how international health systems similar to New Zealand assess productivity or similar
measure) are outlined below.
UK (ONS)
The Office for National Statistics (ONS) measures productivity of the UK’s National Health Service (NHS)
by comparing the growth in the total quantity of healthcare output provided (adjusted for quality where
possible) with the growth in the total quantity of inputs. As a result, the productivity estimates do not
measure value for money or the wider performance of public healthcare services.
The ONS determines the quantity of healthcare outputs using the follow data from the National accounts:
• Cost-weighted aggregates of procedures performed (by Health Resource Groups/HRGs)
• Primary care consultations
• Primary care prescriptions of government-funded drugs
These measures are quality adjusted to reflect whether desired outcomes are achieved, or whether user
needs were met. The three main adjustments are as follows:
• HRG adjustment – Assesses the increase in quality adjusted life years (QALYs) for patients derived
from the procedures performed for HRGs, accounting for age and wait times.
• Care management quality adjustment – Assesses the management of chronic disease by GPs for
patients diagnosed with hypertension, coronary heart disease, strokes and chronic kidney disease by
measuring the proportion of patients within the desired clinical target range.
• Patient experience - the average ratings of care given by patients across five key domains in each area
of the NHS, including a growth factor adjustment made to the appropriate activity. Ratings are
measured based on surveys from the Care Quality Commission targeting five key domains across
different areas of the NHS.
These quality adjustments are applied to all applicable data in the ONS, resulting in some areas and
measures requiring two adjustments, in which case the two adjustment factors are multiplied together.
The ONS displays the outputs of productivity measurement as an index, showing the change over time of
the amount of quality-adjusted output provided for each unit of input with FYE 1996 serves as the index
23
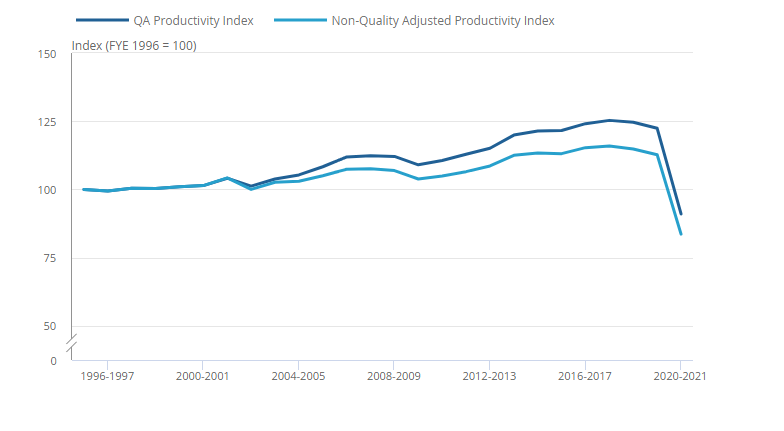
start-point, equal to 100 percentage points. The most recently released productivity indices for healthcare
in England are outlined in Figure 18 below.
Figure 18: Public service healthcare quality and quality productivity indices for England for financial
years ending 1996 to 2021 (Source: Office for National Statistics (ONS), released 29 March 2023, ONS
website, Public service productivity, healthcare, England: financial year ending 2021).
The most resent productivity index shows that NHS productivity decreased dramatically over covid.
However, productivity began to decrease in FY 2018/19 following slower-than-usual growth in FY
2017/18. The slowing growth in productivity was primarily due to increasing input growth, primarily driven
by increased expenditure for labour and for goods and services. Factors which were key contributors to
the faster growth of inputs in FY 2018/19 were:
• an increase in agency staff inputs caused by negative inflation in agency staff costs given by the new
agency staff deflator
• increased growth in non-NHS inputs relative to FYE 2018
• relatively rapid growth in goods and services inputs in general practice
Australia (AIHW):
The Australian Institute for Health and Wellness (AIHW) tracks the efficiency of the Australian healthcare
system rather than productivity. Efficiency is measured by the Australian Institute for Health and Wellness
(AIHW) which looks to ensure that the right care is delivered at minimum cost. Efficiency is measured by:
• The average cost per weighted separation (a casemix adjusted average cost). It uses the national cost
weights to weight separations at the Diagnosis Related Group (DRG) level. If the weighted average is
lower than the simple average, the activity had a higher proportion of complex DRGs.
• Net growth in health workforce.
Australian hospitals are reported to have achieved an 0.5% annual growth rate in labour productivity over
the 10-year period to 2018-19 but overall productivity is 0.1% per year over the decade due to increased
capital investment and costs. (Australian Bureau of Statistics, 2021). The Independent Pricing Authority
for hospitals and aged care published more recent benchmark data over the four year period to 2020-21
24
showing a 16.8% rise in costs, and 6% rise in case-weighted output, resulting in a 10.3% rise in cost per
case-weighted output. The Australian Government Productivity Commission is currently drafting a
productivity report of the healthcare system which will be released in April of 2024.
Ireland (HSE):
The Irish Health Service Executive (HSE) manage performance by focusing on quality of care, which assess
performance across 7 key areas:
• Safety – measure rates on hospital-derived infections and staff absences
• Efficacy – readmission rates following discharge from emergency care
• Timely – proportion of patients waiting more than a given time for select procedures or services
• Person-centred – proportion of referrals seen within a 13-week timeframe and proportion of >75yr
olds seen and discharged/admitted from ED with 6 hrs.
• Efficiency – ambulance wait times and transfer wait times
• Equity – the proportion of completed assessments of need within a 3-month period out of all
assessment of need
• Wellbeing – proportion of babies with a completed health & development check-up within first 12
months of life
The HSE publishes a quarterly report on these seven areas available to the public, providing transparency
on the performance of the healthcare system in these areas.
While these measures assess the performance of the healthcare system, the HSE currently lacks a method
of measuring the productivity for expenditure. However, recent increases in expenditure in the Irish
healthcare systems have resulted in the need to develop a productivity measure providing an estimate of
health-related social expenditure.
25
 3. Additional efficiency measures
3. Additional efficiency measures
In addition to case-weights per FTE, additional efficiency measures to be developed to understand
productivity in the short-term include:
• Long stays (>7 day length of stay) – medical & surgical events
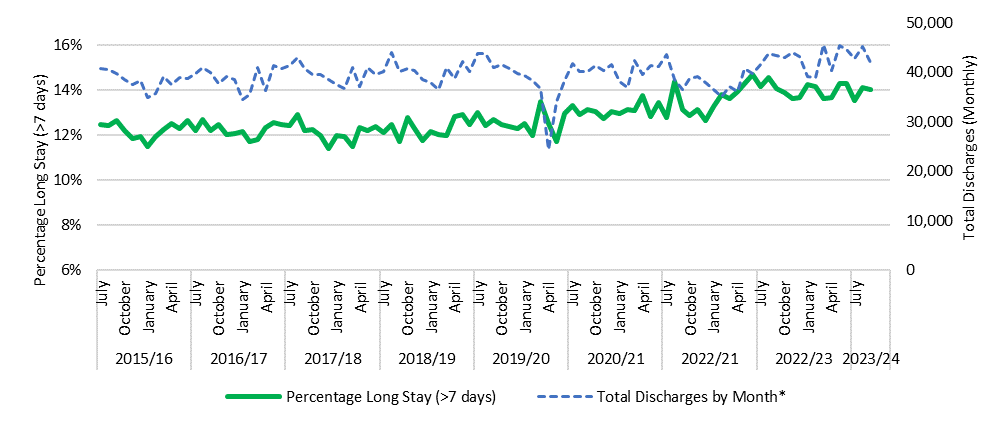
Percentage Long Stay (>7 Days) – medical and surgical episodes of care
The methodology for long stays is under development, however a draft view of long stays has been
provided below (see Appendix B: Methodology for the methodology). This view of long stays looks at
events which have a length of stay longer than 7 days and has been limited to medical and surgical events.
The proportion of events which are longer than 7 days has increased over 2015/16 – 2022/23, from 12.2%
to 14.0%. Note that similar to ALOS, the annual percent of long stays remained steady (between 12.1%
and 12.3%) from 2015/16 to 2018/19 and increased over 2018/19 – 2022/23. This adds further support
to the hypothesis that growing ALOS driven by people staying longer than the bounds of the primary
period driving ‘case-weight’ values will contribute to some of the decrease in productivity observed in the
case-weight to FTE measure.
Figure 19: Percentage Long stays (> 7 days), Nationally, July 2022 – September 2023
Source: NMDS, EY Analysis
*Total Discharges exclude day stays
Note: Data is unavailable for July 2023 – September 2023 for Tairāwhiti and West Coast District.
26
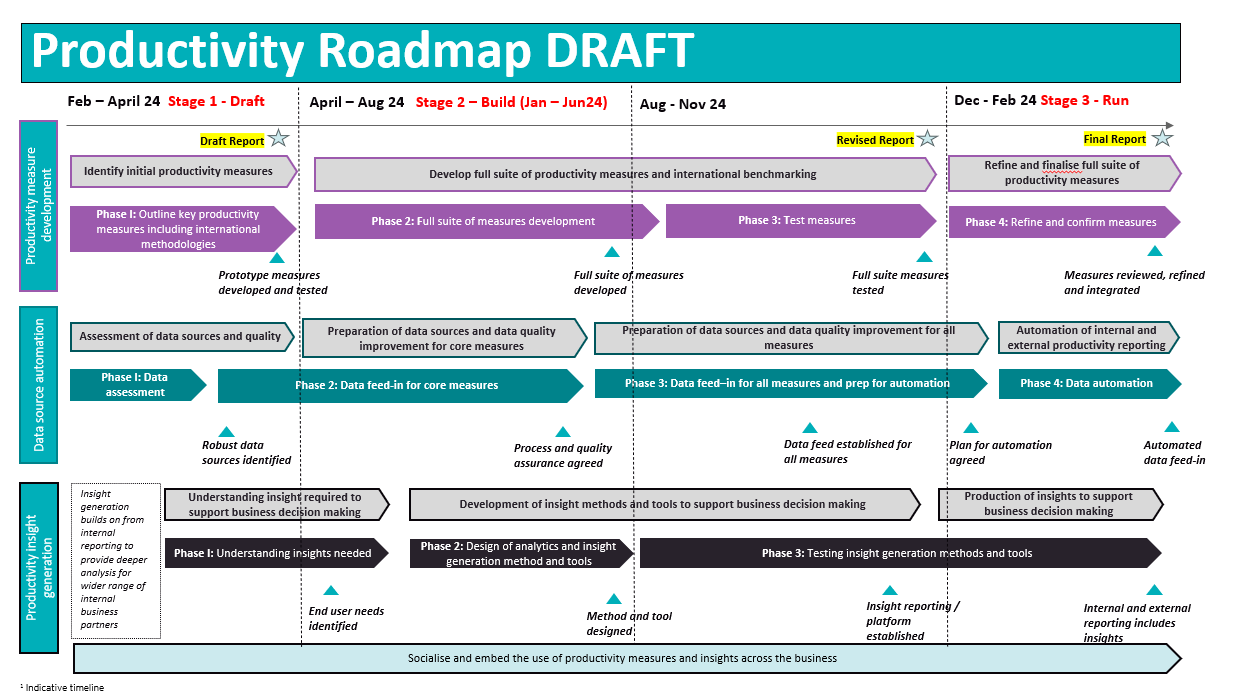 3. Plan for developing productivity measurement and reporting
3. Plan for developing productivity measurement and reporting
There is work underway to refine existing productivity measures and develop suits of productivity
measures, supported by performance and quality measures to be able to understand not just productivity
trends but also drivers and influencer on productivity within service delivery settings. This is anticipated
to be a twelve month programme of work, as the high level roadmap below shows.
There are three components to developing productivity measurement and reporting:
1. Development of productivity measures and the efficiency and performance measures that help
understand drivers of productivity
2. Inclusion of additional measures of productivity, including analysis of a more sophisticated
measure of average length of stay (ALOS) adjusted for several influential factors including the
complexity of patient activity and seriousness of disease / injury
3. Consolidation and automation of data sources including data quality assessment and control
4. Productivity insight generation to increase the use of productivity reporting to support business
decision making
Development of productivity measurement and reporting – first twelve months
Development of productivity measures is planned to centre around a patient journey approach. This
includes focusing on ensuring that there are productivity measures throughout the patient journey, from
diagnostic tests to discharging the patient from the hospital following surgery.
27
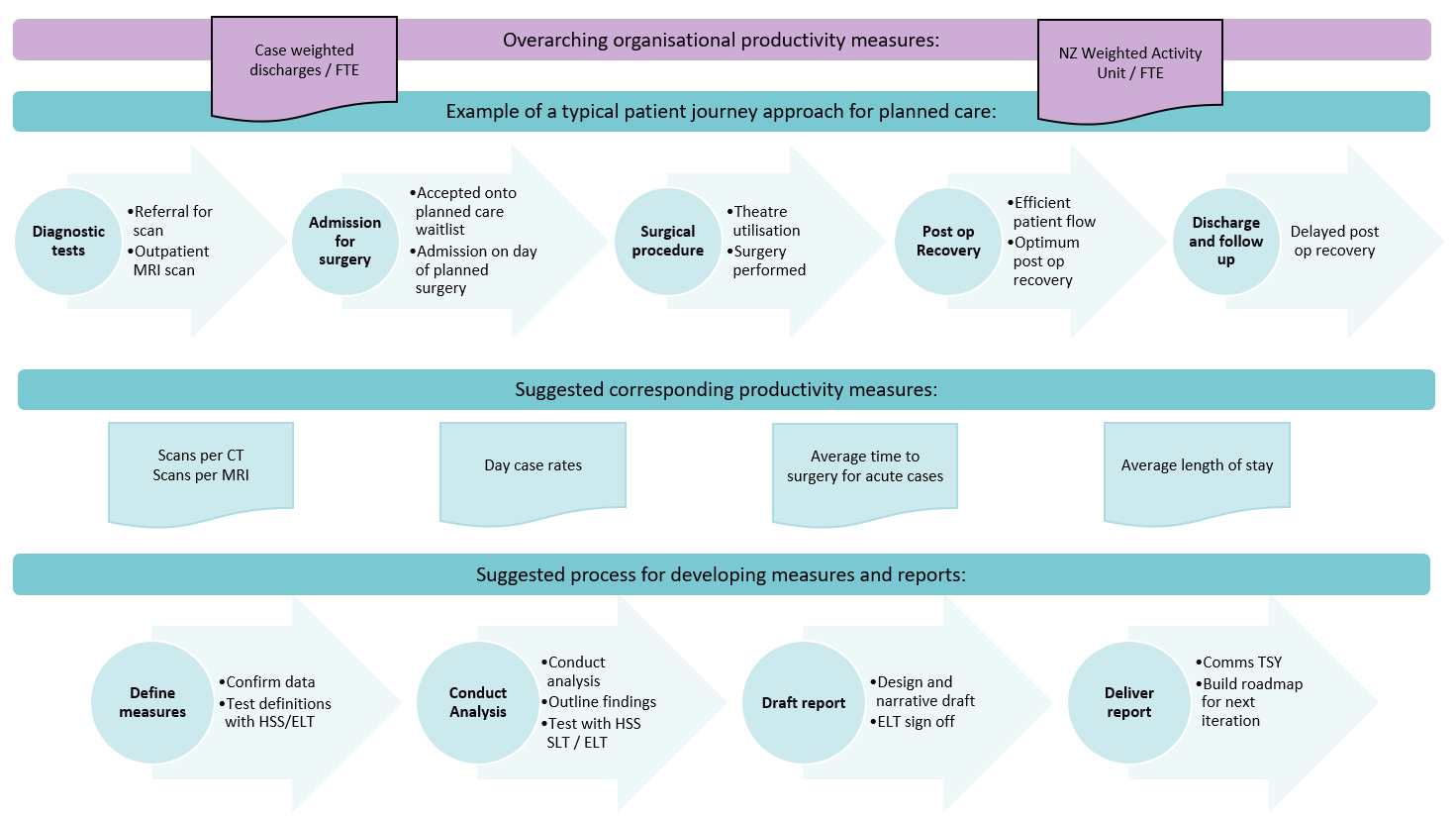 Patient journey approach to productivity reporting
Patient journey approach to productivity reporting
28
 Appendix A: Limitations of Data and Refinement of Measures
Appendix A: Limitations of Data and Refinement of Measures
Recorded discharges and case-weights: Tairāwhiti and West Coast Districts
Data used in this analysis are currently missing inpatient data for the districts of Tairāwhiti and West Coast
for the months of July 2023 through to September 2023. Case-weights per FTE productivity will be
minimally impacted by this as Tairāwhiti and West Coast contributed 0.9% and 0.4% of monthly case-
weights on average over July 2021 and June 2023, accounting for roughly 1% of case-weights nationally.
In addition, trendline analyses only looked at the period of July 2015 to June 2023, so are unaffected by
these missing data.
FTE data
FTE data for the Bay of Plenty district shows a sharp decline in FTE volume for the month of July 2018
followed by a spike in August, while Waikato district had a decline in April 2021 and a large spike in FTE
count for the month of June 2021. A review of the data to determine if FTE has been incorrectly recorded
for these months would further improve the case-weight per FTE measure over this period.
To address the anomaly in FTE data, more robust data capture could be explored, consisting of stronger
quality control measures on FTE data. Additionally, the scale of the FTE measure is at 75,000 staff
nationwide. The variation in FTE quantities between facilities and then variation in services provided
means that although a reliable measure for change in productivity over time, there are challenges
mapping FTE to specific purchase units and activity as the scope of services outlined below suggests.
29
Adjustment for historical case-weight data
The current analysis is performed using case-weights from the year relevant to the event recorded. A
modified calculation of case-weights has been performed for one district to explore discrepancies over
time, using case-weights which have all been mapped to case-weighting for 2023/24. This case-weight
calculation showed that activity growth may be overreported by a factor of approximately 2.0%,
suggesting that the change in productivity (in terms of case-weight per FTE) may be more of a decrease
than this analysis reports.
• A solution to the variation in case-weight over time would be the implementation of an adjusted case-
weight in the case-weight per FTE measure to account for the discrepancies in case-weight over time.
• For the incorporation of Outpatient data or non-case mix events, a system based on price similar to
Australia's National Weighted Activity Unit could address the absence of case-weight.
30
Appendix B: Methodology
Case-weights per FTE
The methodology for case-weights per FTE is under development. The current methodology for this
measure is described in the table below, noting that there is potential for future development of the
measure, including to limit the measure to medical and surgical events and estimated medical and surgical
FTE, and considering a case-weight equivalent for outpatient events.
Metric:
Case-weights per FTE
Numerator
Sum of case-weights
Denominator
Sum of FTE
Data source
Numerator: NMDS
Denominator: Finance
Analysis/Exclusions
Numerator:
• Exclude events which didn’t occur in a public hospital (events must
have an agency code in: '1011', '1021', '1022', '1023', '2031', '2042',
'2047', '2051', '2071', '3061', '3081', '3082', '3091', '3092', '3093',
'3101', '4111', '4121', '4123', '4160', and must have a Facility which
is NOT ‘0314’ or greater than ‘6000’)
• Exclude non-publicly funded events (events must have a purchaser
code of 13, 20, 34, 35)
• Exclude events where the purchase unit is equal to ‘EXCLU’
Comments/Rationale
This metric provides a view of how much the workload has been
increasing or decreasing for FTE in terms of complexity
Long stays (>7 days) – medical and surgical episodes of care
Metric:
Long stays (>7 days) – medical and surgical episodes of care
Numerator
Percentage of Discharges with length of stay greater than 7 days
Denominator
Sum of Discharges (excluding same day patients)
Data source
NMDS
Analysis/
Numerator & Denominator:
Exclusions
• Exclude same day events (events with event start date = event end date)
• Exclude events which didn’t occur in a public hospital (events must have
an agency code in: '1011', '1021', '1022', '1023', '2031', '2042', '2047',
'2051', '2071', '3061', '3081', '3082', '3091', '3092', '3093', '3101', '4111',
31
'4121', '4123', '4160', and must have a Facility which is NOT ‘0314’ or
greater than ‘6000’)
• Exclude non-publicly funded events (events must have a purchaser code
of 13, 20, 34, 35)
• Exclude non-medical/surgical events (events must have a health
specialty code starting with ‘M’ or ‘S’)
• Exclude national transplant service events (events with a DRG code in
'A01Z','A03Z','A05Z','E03Z', 'F23Z','H09Z’)
Comments/
This metric has been set up as a percentage, i.e. the proportion of events
Rationale
which are greater than 7 days.
32
Appendix C – Additional figures
Figure 20: Case-weights per FTE, Nationally, July 2015 – September 2023
Source: NMDS, Finance, EY Analysis
Note: case-weight data is unavailable for July 2023 – September 2023 for Tairāwhiti and West Coast District.
Figure 21: Case-weights per FTE, Nationally, July 2015 – September 2023
Source: NMDS, Finance, EY Analysis
Note: case-weight data is unavailable for July 2023 – September 2023 for Tairāwhiti and West Coast District. This will not have an impact on the
trendlines as the trendlines only go to June 2023. Axis has been truncated to start at 0.4 Case-weight/FTE.
33
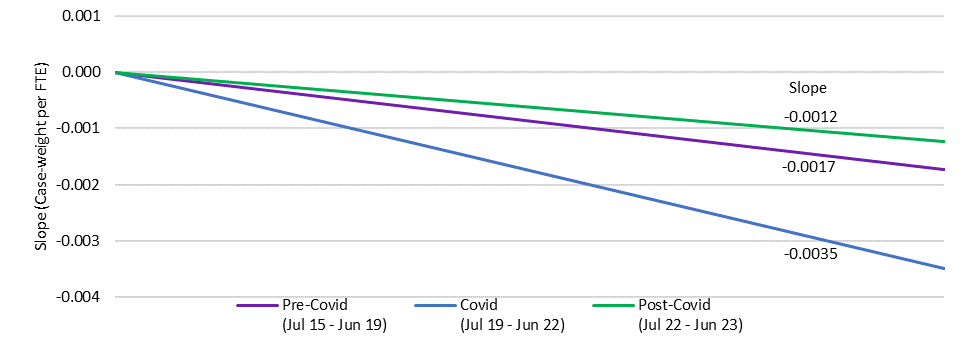 Figure 22: Slope of Case-weights per FTE, Nationally, Three Periods over July 2015 – June 2023
Figure 22: Slope of Case-weights per FTE, Nationally, Three Periods over July 2015 – June 2023
Source: NMDS, Finance, EY Analysis
The slope of trend for Figure 22: Slope of Case-weights per FTE, Nationally
has been calculated to
illustrate rate of change of decline in Case-weight per FTE from July 2015 to June 2023.
Table C: Slope of Case-weights per FTE, Nationally, Three Periods over July 2015 – June 2023
Source: NMDS, Finance, EY Analysis
Slope (Case-weight per
Average percent change per
Period
FTE)
annum
Pre-Covid, July 2015 – Jun 2019
-0.0017
-1.8%
Covid, Jul 2019 – Jun 2022
-0.0035
-3.9%
Post-Covid, Jul 2022 – Jun 2023
-0.0012
-1.5%
Note that due to seasonal changes, the periods all start in July and end in June. This means the periods may not fully align with impacts due to
Covid-19.
34
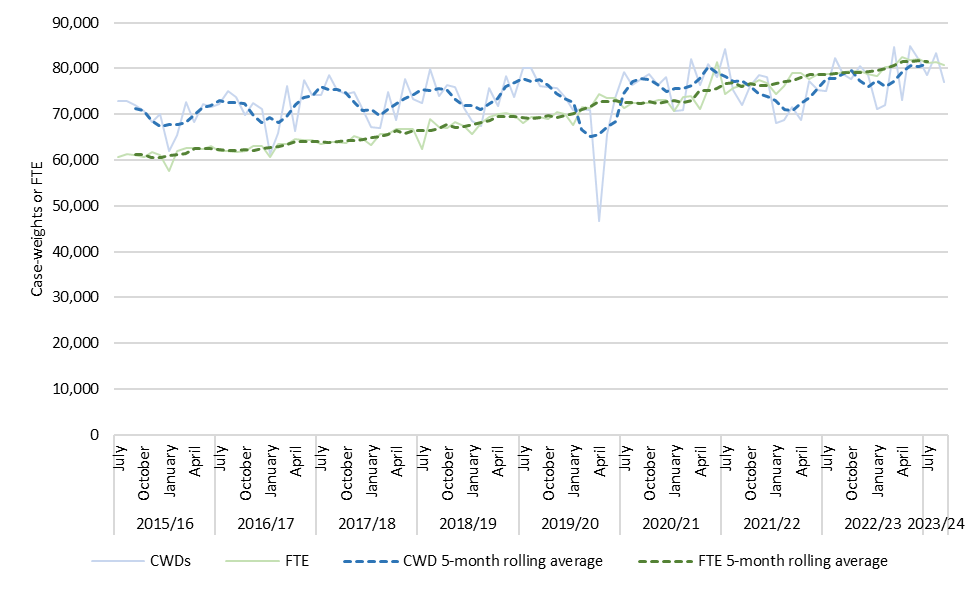 Figure 23: Case-weights and FTE, Nationally, July 2015 – September 2023
Figure 23: Case-weights and FTE, Nationally, July 2015 – September 2023
Source: NMDS, Finance, EY Analysis
Note: case-weight data is unavailable for July 2023 – September 2023 for Tairāwhiti and West Coast District.
FTE nationally has increased from 63,148 FTE at the end of 2015/16 to 80,789 by September 2023, an
increase of 27.9%. Over the same time, the sum of case-weights (annually from July - June) has increased
from 838,923 in 2015/16 to 940,720 for the 2022/23 financial year, an increase of 12.1%. In other words,
Total FTE (inputs) have increased at nearly 2.5 times the rate of case-weights (outputs) so even though
the rate of decrease in case-weights per FTE has slowed following the Covid-19 pandemic, labour
productivity using this measure continues to decrease – which likely reflects a combination of capital
constraints (physical infrastructure, information technology) and other factors (policy, regulation,
culture).
35
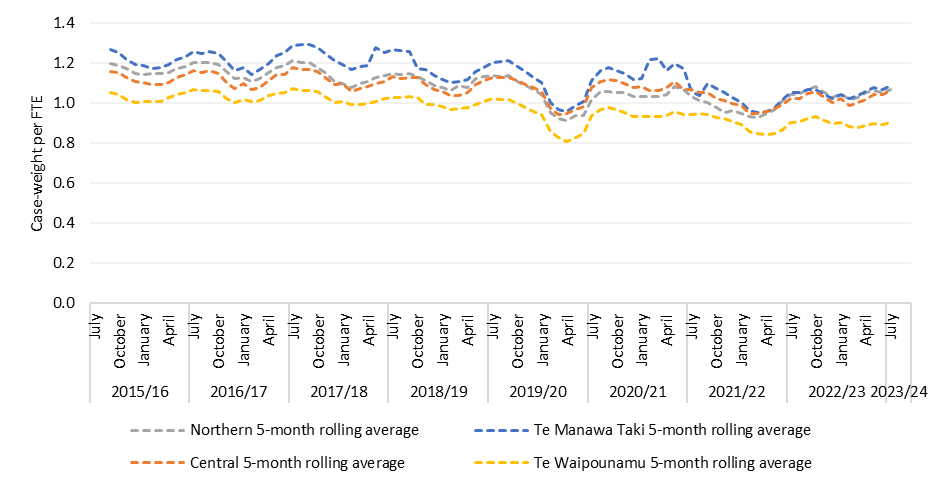 Figure 24: 5-month rolling average Case-weights per FTE, by region, July 2015 – September 2023
Figure 24: 5-month rolling average Case-weights per FTE, by region, July 2015 – September 2023
Source: NMDS, Finance, EY Analysis
Note: case-weight data is unavailable for July 2023 – September 2023 for Tairāwhiti and West Coast District.
Table D: Change in case-weights per FTE by region – 2015/16 and 2022/23
Source: NMDS, Finance, EY Analysis
Region
2015/16 average
2022/23 average
Change
Northern
1.17
1.05
-0.12
Te Manawa Taki
1.22
1.05
-0.17
Central
1.12
1.02
-0.10
Te Waipounamu
1.03
0.90
-0.13
36