

IR-01-24-37415
28 November 2024
Rodney Parsons
[FYI request #28868 email]
Tēnā koe Rodney
Request for information
Thank you for your Official Information Act 1982 (OIA) request of 22 October 2024. You
asked for information regarding the changes to Police’s mental health response.
My response to each part of your request can be found below.
1.
Please outline the steps that have been taken the public health risk related to the
imminent police withdrawal from providing mental health responses.
Police is not withdrawing from providing mental health responses, Police is changing the
way they respond to mental health incidents. Safety is a priority for Police and thus,
Police wil always attend incidents where there is an immediate risk to life or safety,
including where there are requests from the health sector for assistance. There are four
phases of the Mental Health Change Programme, with the first phase that commenced on
4 November 2024.
This first phase streamlines the process of Police handing over people in mental distress
who have voluntarily agreed to a Mental Health assessment to Emergency Departments.
It also seeks to reduce the unnecessary presence of police officers at Mental Health
facilities and in the transporting of mental health patients, by requiring Mental Health
Services to provide increased risk assessment and planning.
This part of your request is therefore refused under section 18(e) of the OIA as the
information requested does not exist.
2.
Provide any health internal or external advice provided to police on this matter,
including any estimates made on anticipated loss of life related directly to this policy
recommendation, and financial or reputational risk assessment undertaken by police
on this.
3.
Outline the proportion of budget that is being witheld from police, corresponding to
this service reduction and any discussions occurred about transferring this budget to
FENZ, Ambulance and Mental Health services.
Police wil continue to respond to mental health events that have an immediate risk to life,
therefore, Police has not sought internal or external advice regarding the potential loss of
life with the implementation of the Mental Health Change Programme.
An overall risk assessment for the programme was completed and has been attached to
this letter for your convenience.
No budget or funding is specifically al ocated for Police to respond to mental health
activities, this is a function that forms part of police’s general duties. Therefore, no


financial assessments have been undertaken by Police. As no such information exists
this part of your request is refused under section 18(e) of the OIA.
Please note that as part of its commitment to openness and transparency, Police
proactively releases some information and documents that may be of interest to the
public. An anonymised version of this response may be publicly released on the New
Zealand Police website.
You have the right to seek an investigation and review by the Ombudsman of this
decision. Information about how to make a complaint is available at
www.ombudsman.parliament.nz or freephone 0800 802 602.
Nāku noa, nā
Kirsten Evans
Acting Director: Māori and Community Prevention Partnerships
New Zealand Police

 Executive Leadership Team
Governance Paper
Title
Executive Leadership Team
Governance Paper
Title
Police response to mental health – change programme
Paper Reference
ELT/24/107
Meeting date
10 June 2024
Sponsor
Pieri Munro, Deputy Chief Executive, Iwi and Community
Presenter/s
Inspector Matt Morris – Manager Health Partnerships Team
Author/s
Inspector Matt Morris – Manager Health Partnerships Team
Consultation
DL_Governance Consultation Subject Matter Experts Districts
External Other (specify)
Distribution
Executive Members Publish on Ten One Other (specify)
Purpose
1.
To update the ELT on the change programme to support the Police response to Mental
Health cal s for service, and to seek approval for the scope and timeline for this work.
Recommendation
It is recommended that the Executive Leadership Team:
(i)
Note that Police continue to work with Health New Zealand (Health NZ) on the five-year
plan directed by Cabinet to transition to a multi-agency led response to 111 Mental Health
demand. Due to pressures on partner agencies, this work is unlikely to provide scalable
solutions in the short-term.
(ii)
Note the change programme outlined in this paper is independent of the five-year plan,
however some initiatives in the five-year plan wil support the changes contained within the
Police plan, like faster ED handovers and support for ECC’s.
(iii)
Note the following key elements of the change programme:
(iv)
moving to 1-hour handovers of all mental health emergency department events by
October 2024 (a slight postponement from September 2024)
(v)
moving to 15-minute handovers if all mental health emergency department events
by April 2025
(vi)
a new threshold definition for Police attendance at mental health events -
Police will
be only involved where there is an offence or a real and immediate risk to life or
safety.
(vii)
Approve the proposed programme of change as attached in Appendix One
(viii)
Direct the Manager Health Partnerships to prepare a briefing to the Minister of Police and
partner agencies on the key elements of the change programme.
_________________________________
Pieri Munro
Deputy Chief Executive – Iwi and Community
30 May 2024
 Executive Leadership Team
Police response to Mental Health – Change
Programme
Executive Leadership Team
Police response to Mental Health – Change
Programme
Background
2.
This paper outlines the programme of work to progress internal operational changes to the
police response to Mental Health (MH) demand. It follows previous updates to both
Strategic Tasking & Coordination Governance Group (23 May 2023) and ELT [ELT/24/023].
3.
ELT previously endorsed in principle a change to Police’s response to MH demand that
enables Police to step-back and redirect resources to deliver core policing services.
4.
The programme outlined in this paper is independent of the 5-year Cabinet paper, though
some of the proposals in that paper (e.g., removing Police from Emergency Departments
faster, and support for ECC’s) if implemented, will support the changes listed here.
5.
These internal changes move police closer to alignment with Health NZ: Te Whatu Ora
Strategies such as Kia Manawanui (Pathway to mental wellbeing) by reducing the pipeline
into the hospital care system, focusing on human rights and reducing “restrictive practices.”
6.
Discussions have been had, and continue with, Family Harm and ECC leads, and their own
upcoming changes have been worked through to ensure alignment.
7.
Appendix one provides a visual representation of the changes including key milestones and
dates for implementation.
8.
This internal change wil be titled:
• Programme of change: Police Mental Health Response.
Reducing a justice response to
a health need
Response to earlier ELT feedback [ELT/24/03]
9.
Following the earlier briefing [ELT/24/03] ELT requested the following:
• Clarity of purpose: the aim is to reduce police time spent on an incident, not to reduce
our response.
• An assurance that there would be a mechanism to measure any shift from this change
in process.
• An assurance this work is aligned with FH and P2 triage work.
Aim is to reduce police time spent on an incident, not to reduce our response
10. The ELT discussion focussed mainly on emergency department handovers. Further clarity is
requested for the following reasons.
11. A MH change programme must have both
reduced response and reduced time as they are
closely interlinked in almost all the demand areas.
12. MH matters are complex, and police wil often have numerous interactions with a person, only
tighter rules around response wil resolve the problems we are facing with MH demand.
 Executive Leadership Team
Executive Leadership Team
13. Below is a common example (and there are many versions of this) which illustrates the
interplay between
response and
time which our staff have to frequently navigate:
• Frontline staff take a male in distress to ED then leave to continue other duties.
• The male runs off from ED, police are called to go locate him by ED staff.
• Police locate him and return him to ED, and he is then admitted to a MH ward.
• Later that day he runs off from the ward and is reported as a missing person, a report is
taken and reviewed by the DCC. Police do not prioritise this.
• Police are later called by MH services who ask they go uplift the male from an address.
Police do not agree to this.
• MH services call back and direct police under Sec 41 of the MH Act. Police comply and
uplift the male and return him to the ward.
• One week later he is released home. After being at home he starts posting suicidal
thoughts on social media, Police are asked to carry out a welfare check.
• As he is a “released patient” Police are directed to take him to ED for medical triaging
(he cannot be taken direct to a ward).
• And the process starts repeats.
An assurance that there wil be a mechanism to measure any shift from this change in process.
14. MH data collection is very poor. s.9(2)(f)(iv) OIA
In regard to ED handovers, police have no way of measuring
this change without ICT prioritisation of a new handover form that police can access online.
An assurance this work is aligned with FH and P2 triage work.
15. The Health Partnerships Team has been and continues to work closely with both ECC’s and
FH. The work is aligned.
Mental Health response change programme – key elements
Statement of intent for the change programme
16.
“Reducing a justice response to a health need.” is the proposed statement of intent for the
change programme. This aligns well with research advising that police are over policing MH
and that most persons in distress do not want police at their events unless absolutely
necessary.
17. Police anticipate this statement of intent should be well received by partner agencies.
Timeframes for Police attendance / handover to Emergency Departments
18. The programme of work and its delivery time frame can be amended but at this stage has been
set to align with future ECC planned changes and Commissioners priorities.
19. Initial analysis indicates that there are minimal costs for police in implementing this programme.
s.9(2)(f)(iv) OIA
 Executive Leadership Team
Executive Leadership Team
20. This programme aligns with the Commissioners prior direction of:
• Moving to 1-hour handovers of all MH ED handovers in October 2024 – we bumped this
back one month from Sept 2024.
• Moving to 15 min handovers of all MH ED handovers in April 2025.
21. The overall programme of change has several change points which have been traversed in
previous briefings. For familiarisation, these are:
• ED handovers: Better reporting and data capture. Faster police exit times.
• MH Transportations: Increasing threshold for compliance with MH requests.
• Assistance to MH wards: Tightening of rules around attending MH wards.
• MH Custody rules: Tightening of rules around custody MH assessments.
• MH requests for assistance: Increasing threshold for compliance.
• Missing/AWOL MH persons: Increasing threshold of taking reports and responding only
when new rules have been met.
• Welfare checks: Increasing threshold of response to these (from public and other
agencies).
s.6(c) OIA
 Executive Leadership Team
Timeline
Executive Leadership Team
Timeline
27. It should be noted that all UK counties are progressing similar changes, and Australia appears
to be actively progressing similar changes (WA has pushed ahead).
28. In the UK similar changes implemented in Humberside (UK) and some other counties were
staggered over a two-year period.
29. The rollout wil progress as detailed in Appendix one and wil enable the following:
• Early changes are modest in nature, no significant impact for police and partners to
progress.
• Early changes will help support the more substantive changes planned at later stages.
• It aligns with ELT expectations relating to ED handovers.
• It keeps the most complex change at the end – welfare checks. This allows time to
consider earlier changes and incorporate learnings into this proposal.
Alignment with strategic priorities
30. This change programme aligns to the ELT’s current priority under ‘Focus on Core Policing’ by
supporting the Family Harm and Mental Health non-emergency response implementation plan.
Policy and Government
31. Once this programme is confirmed police wil commence consultation with partner agencies
on how they wil be able to support these proposed changes. It is recognised that some of
these changes wil have a likely impacts on them. As noted in the recommendations, Health
New Zealand should be formally advised of the proposed changes.
Media and Communications
32. Police will need to keep partner agencies well informed of the proposed changes. To support
this, an internal and external communications plan has been progressed with the assistance
of Strategic Communications. This plan wil be finalised once ELT direction on the change
programme is confirmed.
Concluding Comments and Next Steps
33. The primary consideration for any next steps is engagement. To this end, it is recommended
that Police brief the Minister of Police and Health NZ on both the intent and key elements of
the change programme.
34. This would be followed by further engagement with Health New Zealand and other partner
agencies by the Health Partnerships team (within Iwi and Community) to ensure the plan is
well understood and to identify areas where partners may need our support.
APPENDICES
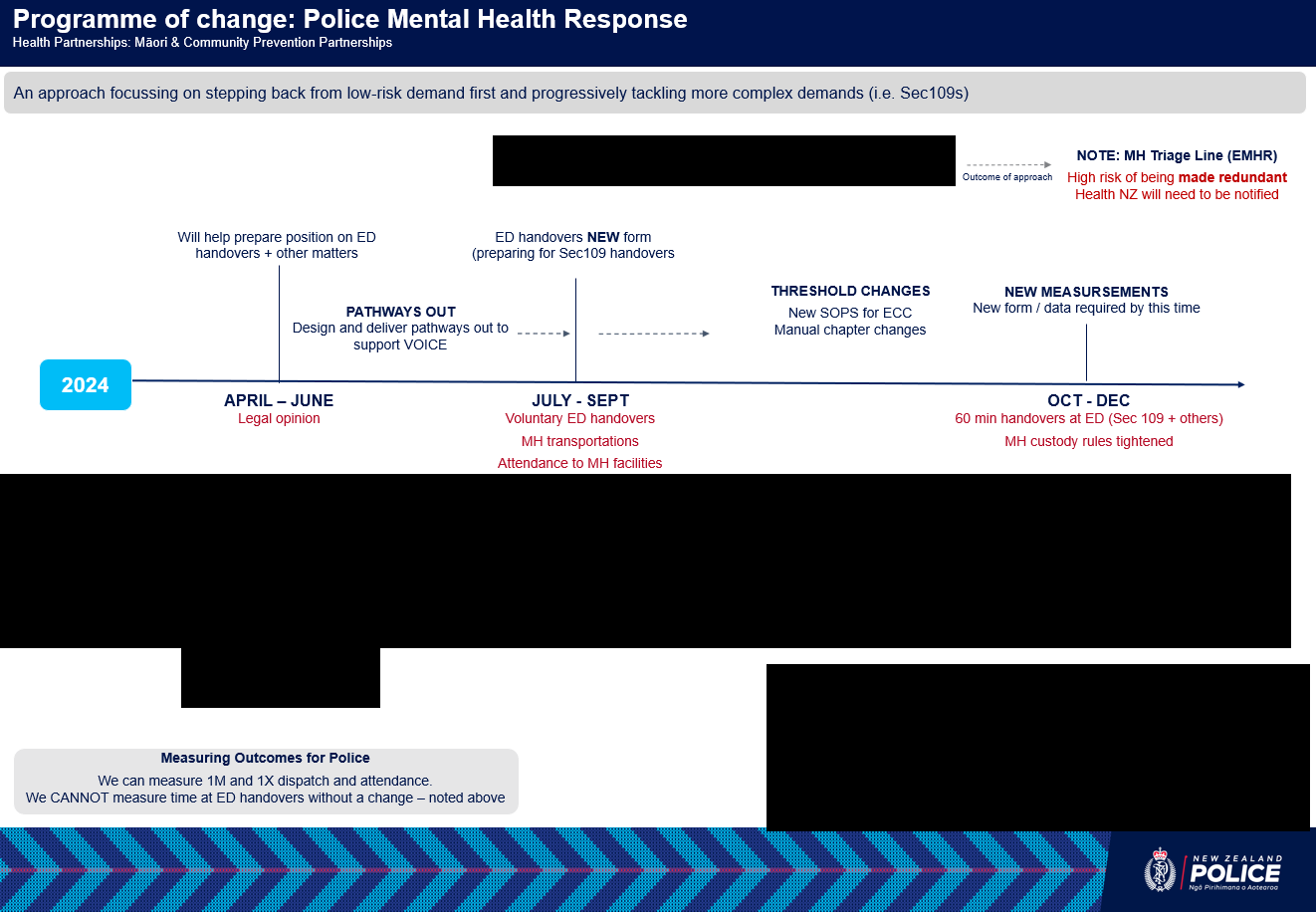
A. Programme of change – timeline and key milestones

 Executive Leadership Team
Appendix A: Programme of change – timeline and key milestones
Executive Leadership Team
Appendix A: Programme of change – timeline and key milestones
s.9(2)(f)(iv) OIA
s.9(2)(f)(iv) OIA
s.6(c) OIA