
133 Molesworth Street
PO Box 5013
Wellington 6140
New Zealand
T+64 4 496 2000
12 December 2023
Al Johnson
By email: [FYI request #24663 email]
Ref:
H2023032995
Tēnā koe Mr Johnson
Partial response to your request for official information
Thank you for your request under the Official Information Act 1982 (the Act) to Manatū Hauora
(the Ministry of Health) on 14 November 2023 for information regarding COVID-19. You
requested:
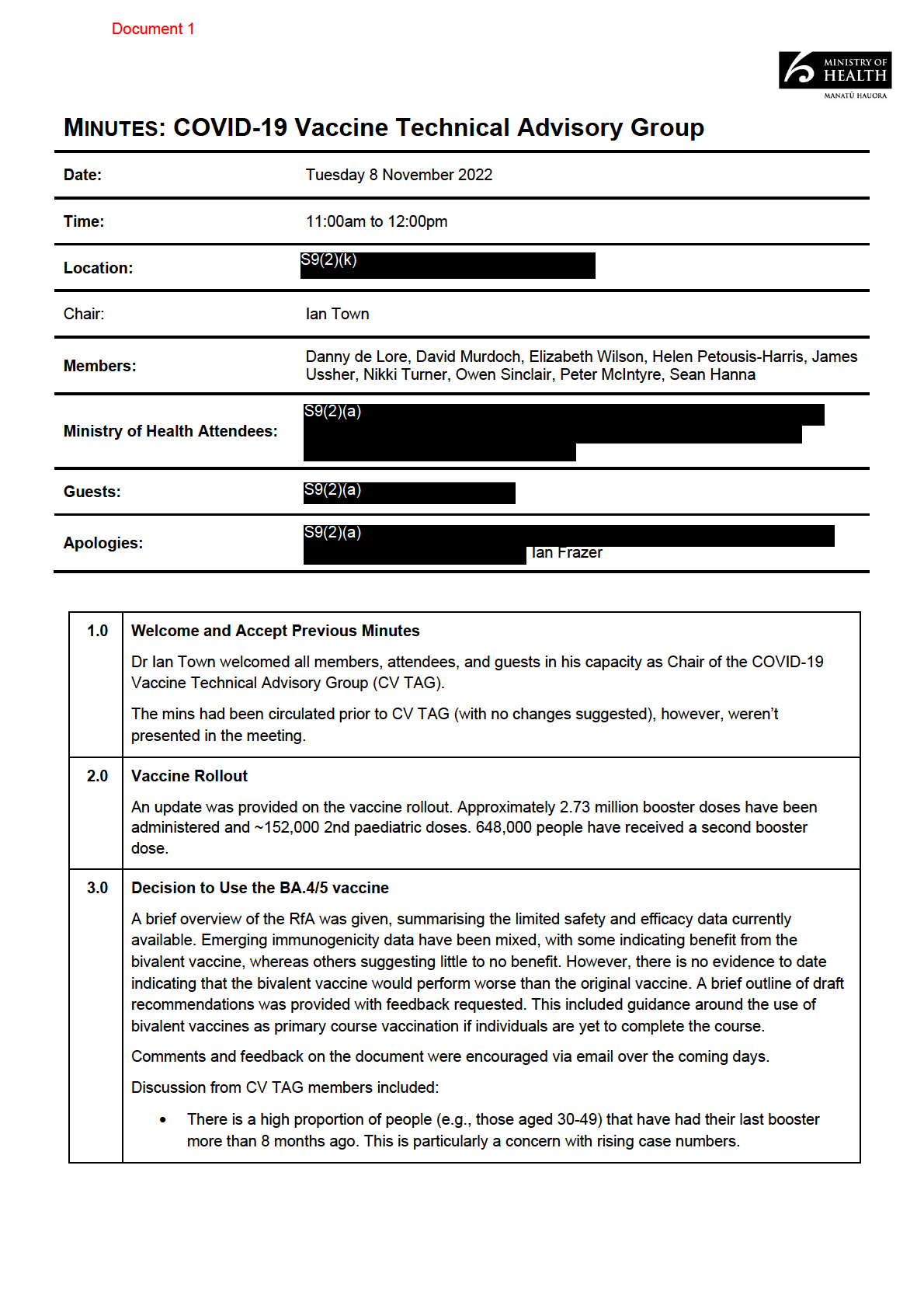
The meetings held and associated minutes from the COVID-19 Vaccine Technical
Advisory Group after the 11th of October 2022 meeting to the dissolution of this advisory
group on the 25th of March 2023.
The meetings held and associated minutes and any briefings or memos (or documents of
a similar nature) produced by the Covid Technical Advisory Group after the 10th of
February 2023 meeting.
The COVID-19 Vaccine Technical Advisory Group met three times within the specified time
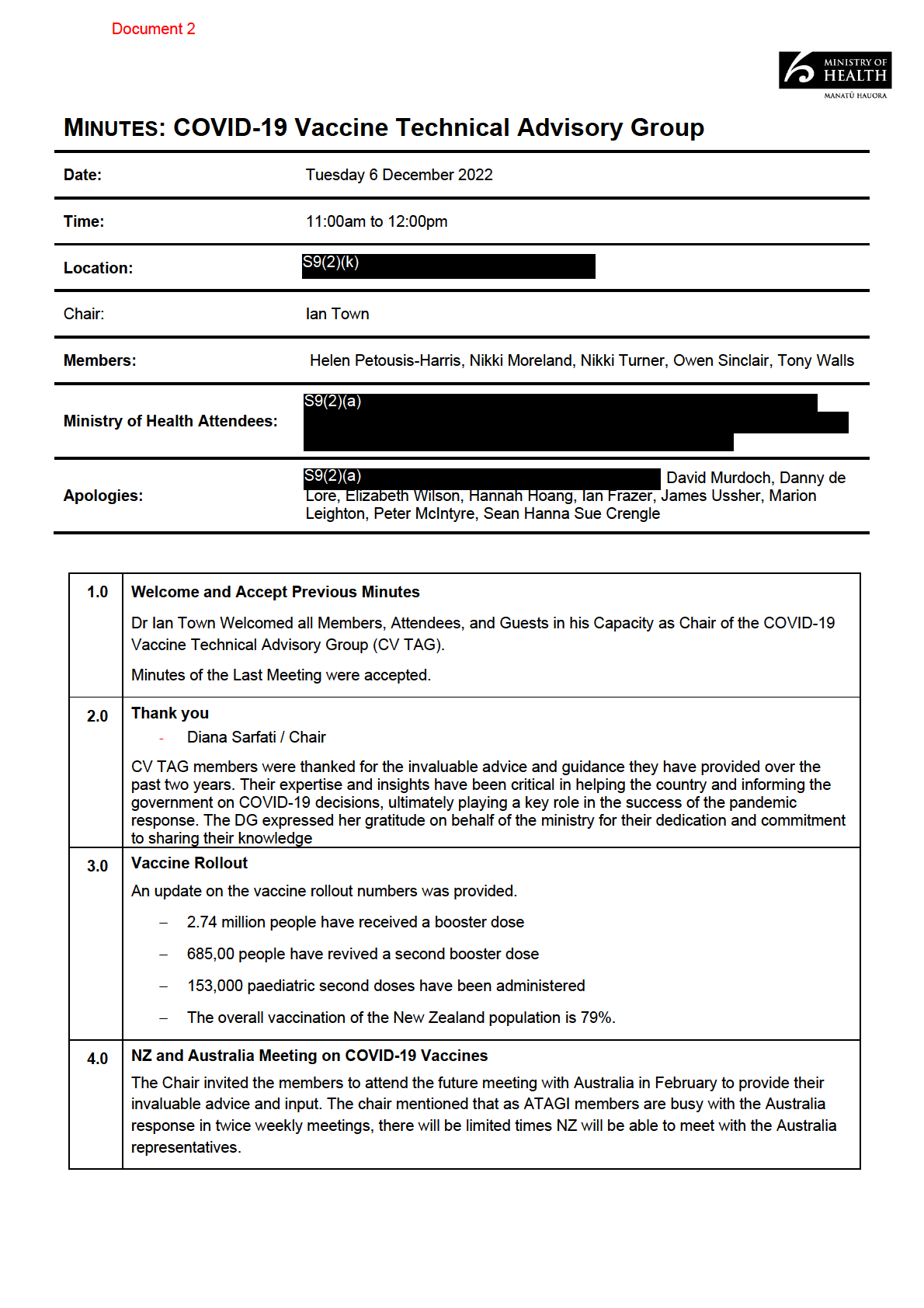
period, on 8 November 2022, 6 December 2022 and 2 February 2023. The minutes for these
meetings are attached (refer to documents 1-3).
The COVID-19 Technical Advisory Group met twice within the specified time period, on 10
March 2023 and 19 May 2023. The minutes for these meetings are attached (please refer to
documents 4 and 5).
Al documents are itemised in Appendix 1 and copies of the documents are enclosed. Where
information is withheld, this is outlined in the Appendix and noted in the document itself. Where
information is withheld under section 9 of the Act, I have considered the countervailing public
interest in release in making this decision and consider that it does not outweigh the need to
withhold at this time.
Any documentation or discussion as to who or what wil review or make recommendations
on Covid vaccines since the dissolution of the COVID-19 Vaccine Technical Advisory
Group in March 2023. This could be memos or briefings or documents of a similar nature.
The meetings held and associated minutes and any briefings or memos (or documents of
a similar nature) produced by the Long COVID Expert Advisory Group since its formation
in May 2022.
Manatū Hauora has decided to extend the period of time available to respond to this part of your
request under section 15A of the Act, as consultations are necessary to make a decision are
such that a proper response this part of your request cannot reasonably be made within the
original time limit. You can expect copies of the remaining documents on or before 22
December 2023.
You may also be interested to know that Manatū Hauora has made a range of information
related to long COVID publicly available. This includes resources for health providers to support
and manage long COVID symptoms and research that informs the ongoing response to long
COVID in Aotearoa New Zealand. This information is available at the following links:
•
www.health.govt.nz/our-work/diseases-and-conditions/covid-19-novel-coronavirus/covid-
19-response-planning/long-covid-programme
•
covid19.health.nz/advice/i-have-covid-19/long-covid
•
www.health.govt.nz/our-work/diseases-and-conditions/covid-19-novel-coronavirus/covid-
19-response-planning/covid-19-science-news#long-covid
I trust this information fulfils your request. If you wish to discuss any aspect of your request with
us, including this decision, please feel free to contact the OIA Services Team on:
[email address].
Under section 28(3) of the Act, you have the right to ask the Ombudsman to review any
decisions made under this request. The Ombudsman may be contacted by email at:
[email address] or by calling 0800 802 602.
Please note that this response, with your personal details removed, may be published on the
Manatū Hauora website at:
www.health.govt.nz/about-ministry/information-releases/responses-
official-information-act-requests.
Nāku noa, nā
Louise Karageorge
Group Manager, Intelligence, Surveil ance and Knowledge
Public Health Agency | Te Pou Hauora Tūmatanui
Page 2 of 4
Appendix 1: List of documents for release
#
Date
Document details
Decision on release
1
8 November 2022 Minutes: COVID-19 Vaccine
Some information withheld
Technical Advisory Group
under the following sections of
the Act:
• 9(2)(a) – to protect the
privacy of natural
persons.
• 9(2)(ba)(i) – to protect
information that is
subject to an obligation
of confidence and
making it available
would likely prejudice
the supply of similar
information, or
information from the
same source and;
• 9(2)(k) - to prevent the
disclosure or use of
official information for
improper gain or
advantage.
2
6 December 2022
Some information withheld
under the following sections of
the Act:
• 9(2)(a) and;
• 9(2)(k)
3
2 February 2023
Some information withheld
under the following sections of
the Act:
• 9(2)(a);
• 9(2)(k);
• 9(2)(b)(ii) – where its
release would likely
unreasonably prejudice
the commercial
position of the person
who supplied the
information and;
• 9(2)(g)(i) – to maintain
the effective conduct of
public affairs through
the free and frank
expression of opinions
by or between or to
Ministers and officers
Page 3 of 4
#
Date
Document details
Decision on release
and employees of any
public service agency.
4
10 March 2023
Minutes: COVID-19 Technical
Some information withheld
Advisory Group
under sections of the Act:
• 9(2)(a) and;
• 9(2)(k) of the Act.
5
19 May 2023
Page 4 of 4
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 1
•
Consideration is needed about the timing of additional boosters, such as in Autumn, to coincide
with flu season. A vaccine in Autumn would also al ow time to acquire an updated vaccine.
•
Data available on bivalent vaccines remains limited.
•
S9(2)(ba)(i)
4.0 Interval Duration for Next COVID-19 Dose/Booster
This is discussed in item 3.0
5.0 Moderna/Novavax as a Heterologous Booster
An overview of the use of heterologous boosters was given, this included using Novavax as this is
already in the country and approved. Moderna was also mentioned as a possibility but not an option at
this current time.
The consensus from the Committee was to not over complicate guidelines. If people want an alternative
vaccine to Pfizer, or if they have had a reaction to the previous Pfizer dose, then they can choose t
1982o
have Novavax instead as their next dose.
ACT
6.0 CV TAG Transition
This item was not discussed as there wil be an additional TAG meeting on the 8th of December
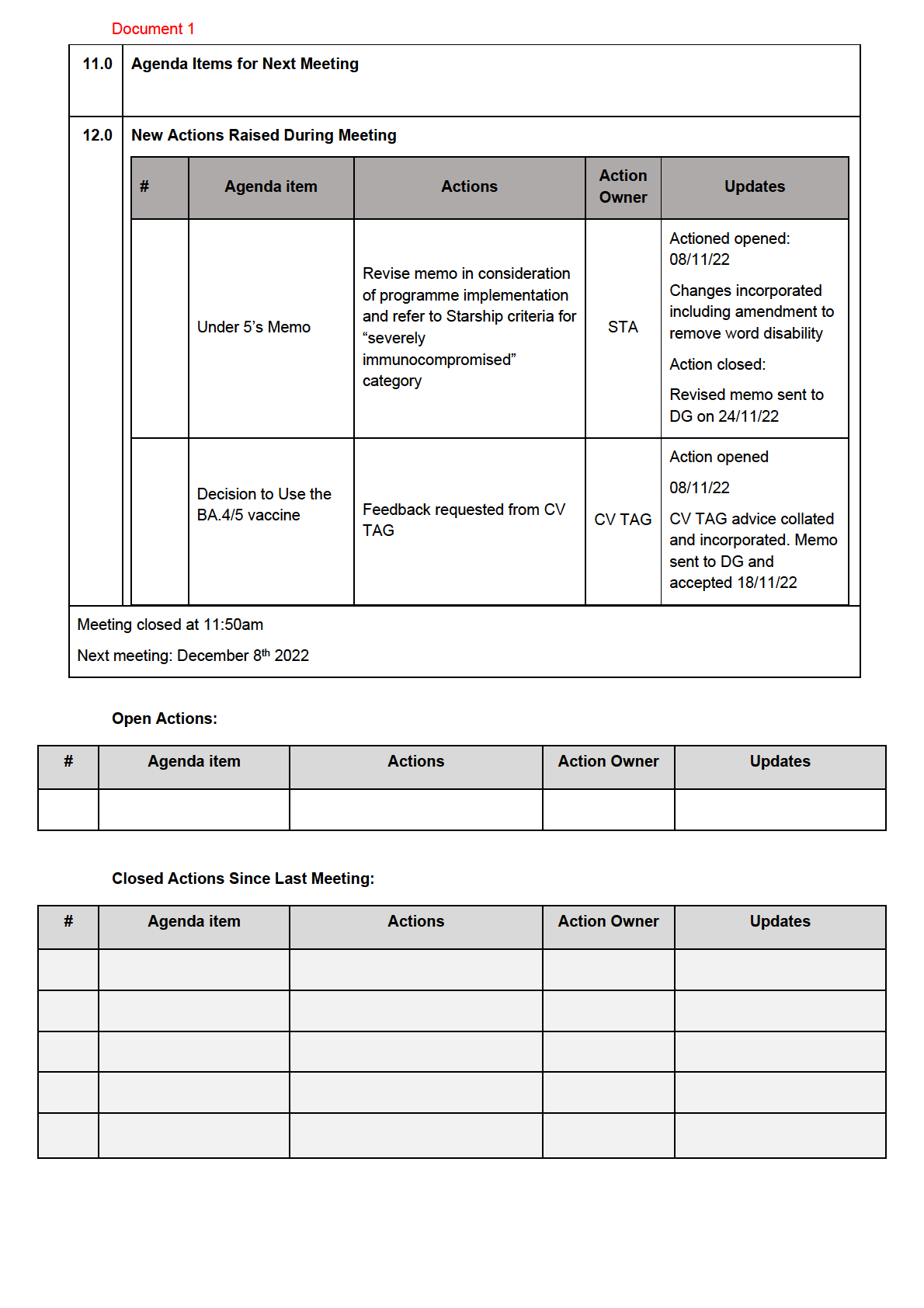
7.0 Under 5’s Memo
The final memo was noted and distributed for to members to view. The memo summarises CV TAG’s
advice to not routinely recommend vaccination in under 5’s and the data supporting this decision.
Discussion from CV TAG members included:
INFORMATION
•
The wording “not recommended” can have varied and incorrect interpretations and suggested
that “not needed” OR “not required” be used as alternatives.
•
Suggestion that while ATAGI list is adequate, the Starship document may be more prudent, as
this matched up to the New Zealand context more effectively.
•
Request for specificity around ICU admissions for
OFFICIAL under 5’s, however noting that the data is
limited and may not be possible.
•
The dosing interval requires further clarification once Medsafe has approved this vaccine and the
THE
stock has arrived in the country in the new year.
•
There was discussion around clarification on who could access the vaccine and where it can be
accessed. As there is a limited number of children that wil be eligible there needs to be a clear
line on who is responsible and what guidelines should be followed. It was suggested that the
UNDER
best place for this would be at hospitals.
Action: Revise memo in consideration of programme implementation and refer to Starship criteria for
“severely immunocompromised” category.
8.0 Second boosters for Māori and Pacific Peoples aged 40-49
A brief overview of th
RELEASED is memo was given by the Chair. Thanks was given for mahi, and expertise
provided to produce this advice. This memo has been sent to the Director General.
9.0 Next Steps/Decisions Pending
10.0 Any Other Business
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 2
The ATAGI members and Australian representatives have provided invaluable advice on their rollout of
the COVID-19 bivalent vaccine. This included a brief summary of data col ected and early findings from
the bivalent rollout. This is to be shared amongst CV TAG members only.
The meeting covered
-
The similarities between NZ and Australia with vaccines uptake, inequities and high infection
rates were highlighted
-
The focus on increasing uptake in specific populations groups e.g., based on age and
indigenous population groups
-
Simplifying a 2023 strategy such as an annual booster as well as refining the criteria.
-
Currently ATAGI do not recommend 5th doses based on current data on hybrid immunity, with
potential for duration of protection against severe disease/death lasting beyond a year
-
The role of T-cells in the immune response and the subsequent protection against several
disease from COVID-19 is not well understood.
-
The value of bivalent boosters in the changing environment of COVID-19 variant. Noting that
current data shows marginal benefits. There is a need to avoid varirent chasing and focus
1982on
preventing severe disease.
-
The roll of vaccination in prevention of long-covid and the value of next generations of vaccines,
ACT
such as the Novavax Nanoflu (Covid-19+Flu) and mucosal vaccines.
-
The need to share more information to benefit both sides such as ATAGIs rollout and the
serosurveys
There was discussion on the bivalent vaccine and the input ATAGI members had provided further
validated CV TAG’s thinking on this matter. It was also mentioned that the ancestral strain vaccine stil
has significant value.
A member inquired about their expanded eligibility criteria and the uptake of vaccines since introduced.
INFORMATION
5.0 Dosage Intervals RFA
An evidence brief is being drafted on dosing Intervals, which require CV TAG input.
Advice requested include:
OFFICIAL
-
What is the recommended minimum interval between the last dose received and an additional
dose (excluding exceptional circumstances)?
THE
-
What is the recommended minimum interval between a covid-19 infection and an additional
dose?
-
Wil these intervals vary by population group?
Key considerations here wil be hy
UNDER brid immunity and its duration of protection.
The Ministry’s current strategy is focused on preventing severe disease outcomes rather than
transmission however, there may be some utility in a vaccination drive to reduce some transmission.
The coverage can be grouped into 3 populations
-
High-Risk: From poor outcomes, Elderly and immunocompromised
RELEASED
-
Moderate-Risk: Of poor outcomes from COVID-19 and low risk of poor vaccination outcomes,
these would be the 30-50 year olds.
-
Low-Risk: Of poor outcomes, this would include under 30s, but would also have a low risk of
vaccine adverse outcomes.
A member noted that the current general recommendation of a minimum of 6 months is an ample length
of time, but there needs to be al owance for more flexibility. Flexibility is already seen in the immunisation
schedule, where there is already a large amount of flexibility on when you can give a vaccine dose. The
NACI wording is a good example, allowing for both shortening to 3 months and lowering the 8-week
interval to 3 months in context of immunological risk.
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 3
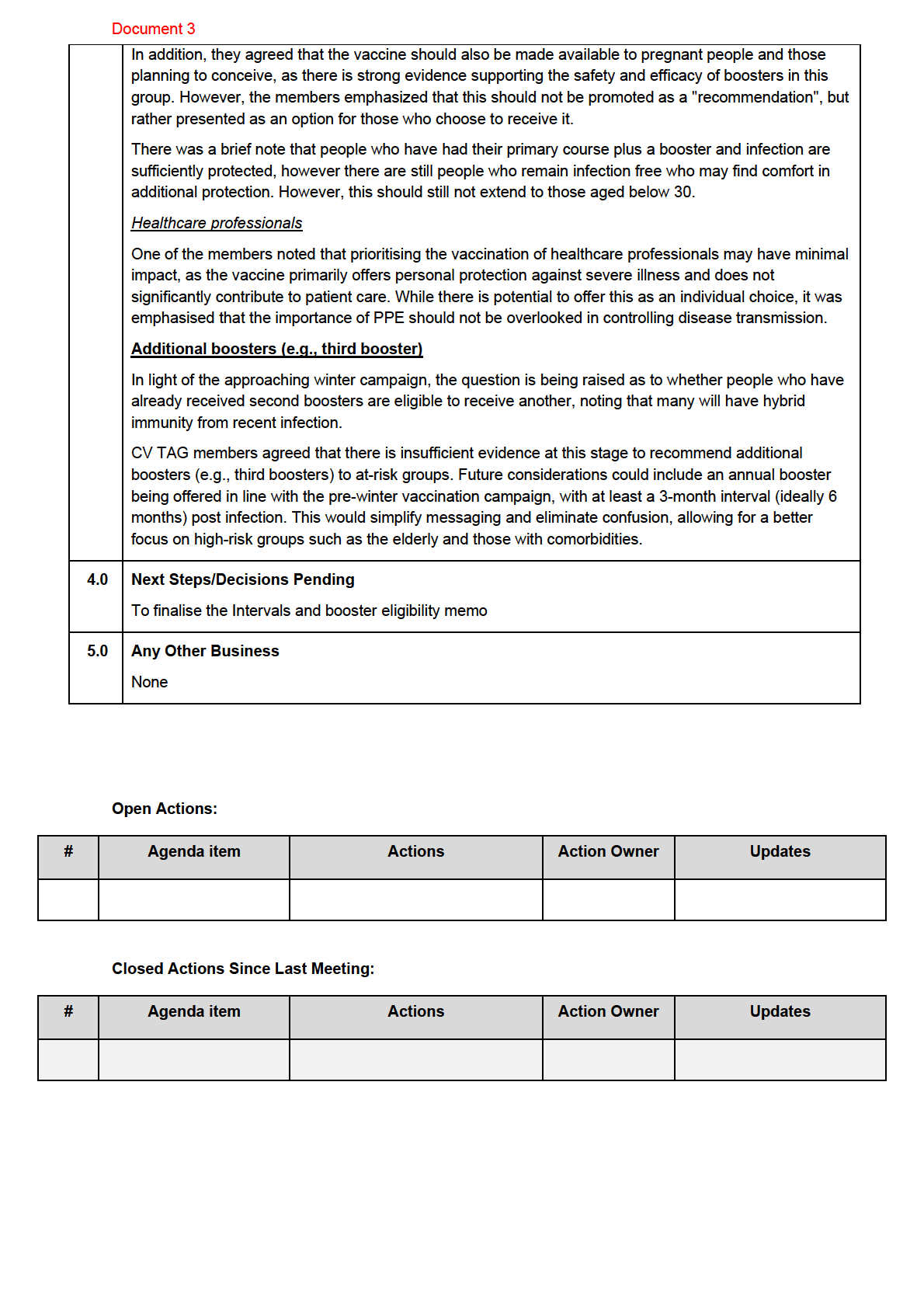
more information and data becomes available. Additionally, it was noted that in the field of medicine,
treatments are often changed for marginal improvements, and this is a common practice.
Members remarked that the new bivalent vaccine does not require dilution, thus minimising waste,
making it easier to store and administer.
Considerations for programme implementation
CV TAG discussed the potential for a targeted campaign with the new and improved bivalent vaccine to
increase uptake and readiness among Māori and Pacific Peoples who are yet to get a booster shot.
Members agreed that it is potential y unethical and problematic to offer a split booster campaign (i.e.
S9(2)(b)(ii), S9(2)(ba)(i)
This
could initially be targeted for those who have not yet received a booster, which include a large proportion
of Māori and Pacific Peoples. Then, once eligibility is broadened, the bivalent booster can continue to be
offered to the wider population.
1982
Although the monovalent vaccine is set to be phased out, it can stil be useful for the smal proportion of
individuals who have not yet received a primary course. S9(2)(ba)(i)
ACT
To avoid confusion, it will be crucial to communicate clearly that the BA.4/5 bivalent vaccines, contain
both the original Wuhan strain and the new BA.4/5 strain. Many people may mistake it for a completely
new vaccine if this information is not provided clearly.
3.0 Vaccination Intervals and Expanding Booster Eligibility
INFORMATION
Update on booster eligibility and intervals
A summary of the draft advice on intervals between boosters, and expanding eligibility was presented,
drawing on previous input from CV TAG. The summary noted that some individuals may require an
additional vaccine dose due to waning immunity and risk of severe disease. However, the appropriate
OFFICIAL
interval for an additional dose has not yet been determined, and input from CV TAG was requested.
Safety concerns regarding myocarditis in younger people were also conveyed. Additionally, there was a
THE
need for clarity on expanding 2nd booster eligibility, particularly among those aged 30-49 and pregnant
people.
Expanding vaccine eligibility cr
UNDER iteria (for 2nd boosters)
Aligning at-risk criteria with the flu vaccine eligibility criteria
During the meeting, members suggested aligning the high-risk COVID-19 vaccination criteria (i.e., those
“recommended” to receive the vaccine) with the eligibility criteria for the flu vaccine, except for children.
Expanding to al individuals aged 30+, and pregnant people
RELEASED
CV TAG members agreed that second boosters should be available to individuals aged 30 years and
over, while noting the limited data available on the efficacy of boosters for those aged 30-49. They also
discussed a recent safety study that found a relatively high incidence of pericarditis in those under 18
years old, but reassuring data for most other age groups, with no increased risk of myocarditis or
pericarditis in those aged 30 years and above.
The members acknowledged that younger males face a certain level of risk, but they also highlighted
that there is a rigorous and transparent process in place to inform them of the potential risks when they
present at the clinic.
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 4
MINUTES: COVID-19 Technical Advisory Group
Date:
Friday 10 March 2023
Time:
10.30 am – 12:00 pm
Location:
S9(2)(k)
Chair:
Nicholas Jones
Bryan Betty, Michael Baker, Michelle Balm, Nigel French, Nigel Raymond, Sal y
Members:
1982
Roberts, Virginia Hope
ACT
S9(2)(a)
Ministry of Health Attendees:
Guests:
S9(2)(a)
Apologies:
Anja Werno, Col in Tukuitonga, Erasmus Smit, Matire Harwood, Nikki Turner,
Shanika Perera
INFORMATION
1.0 Welcome and accept previous minutes
Minutes of the last meeting (10 February 2023) were approved subject to the following
amendments (in
italics) on item
5.0 Policy choices for the ongoing management of
COVID-19
OFFICIAL
Intro:
The management wil shift from an all-of-government response to increasingly considering
THE
COVID-19 alongside other health issues. This coincides with the decision to
no longer have
a separate ministerial portfolio for COVID-19.
5.0 Policy choices for the ongoing management of COVID-19
UNDER
Feedback from the members:
•
The role of antivirals should be considered careful y when planning making access
to antivirals as broad as possible. General y, vaccines are more effective than
antivirals and the focus should remain on vaccines. A large UK study among
25,000 people of moderate risk shows that
Molnupiravir did not alter hospitalisation
number, however, they shortened the period of viral shedding and reduced some
RELEASED
symptoms.
2.0 Trends and Insights
A member from the Intel & Analytics team reported a slight increase in COVID-19 case rates, however,
hospitalisation rates have remained steady.
Feedback from the members:
Document 4
• Based on clinical and wastewater whole-genome-sequencing (WGS) the proportion
of sublineage XBB.1.5 (‘Kraken’) continues to increase and is expected to overtake
BA.2.75 to become the dominant variant next week.
3.0 COVID-19 cases and hospitalisation rates in areas affected by cyclone Gabrielle
Reported COVID-19 cases in cyclone-affected areas seem to have dropped, however, this could be a
result of limited data from affected areas, including Tairawhiti and Hawke’s Bay, making it hard to
calculate the effects of the cyclone. For example, the decrease in numbers might be a result of restricted
access to infrastructure and lack of wastewater testing in the aftermath of the cyclone, rather than a
decrease in infections. Additionally, available numbers are too smal to have statistical power.
4.0 PHRA update
The review of three current orders wil be on the agenda at the next Public Health Risk Assessment
(PHRA) meeting on 16 March 2023.
1982
4.1 Mask wearing in health care settings
ACT
A member of the Manatū Hauora Policy team commented on the public health policies and strategies
which wil be up for review in the upcoming PHRA meeting. In relation to masks, staff in hospitals and
residential aged care facilities have reported fatigue, with staff in pharmacies reporting difficulties in
being able to distinguish between a patient and a visitor. However, the aim of the order is the need to
protect at risk populations and mask use is easier to enforce with a mandate in place.
Feedback from members:
•
Mask use is an issue for GPs who cannot differentiate between patients and visitors. The
INFORMATION
College of General Practitioners recommends mask use in waiting areas (especially considering
winter will likely bring an expected increase in influenza and other viral diseases). However, this
recommendation does not apply to one-on-one interactions in the examination room.
•
Healthcare workers in residential aged care facilities would like to have their own direction rather
than a one size fits al approach.
OFFICIAL
•
A member from the Ministry’s Infection Prevention and Control (IPC) team reported that the IPC
Sub-TAG will seek input regarding mask use from the COVID-19 Clinical Outbreak Group.
•
The size of groups who support the order and those who do not is unknown, however, it might
THE
be likely that those in favour of keeping the order are less vocal.
•
One member noted that the overview table of ‘Recommendations for minimum PPE
requirements based on risk assessment’ on the last page of the printed version of the updated
Mask wearing in health care settings Feb- May 2023 require further clarification.
UNDER
•
There have been difficulties receiving updated advice from COVID-19 TAG, since the transfer of
operational and IPC groups to Te Whatu Ora. The dissemination process and who is leading it
seem to be unclear.
•
Universal mask use is difficult to enforce, however, the ability to introduce mass masking as a
prevention tool should be taken into consideration
RELEASED
4.2 Isolation Policy team is currently awaiting modelling data.
Feedback from members included:
•
If order were to become a guidance, a question was raised on whether people isolating would
stil be eligible to receive leave support. Financial support can be crucial for people to isolate.
•
What impact would isolation guidance have on absenteeism? Would it change the current trend
of sick people staying at home?
Document 4
• Reported high levels of isolation compliance (75% in February) do not account for people who
do not report and are therefore hard to measure. This raises the question of how big the gap
might be.
• The results of a recently published metanalysis on virus shedding in relation to Omicron supports
shorter isolation periods. However, the review does not report on considerable variation in
shedding times observed between individuals.
• Asymptomatic people might have a similar infectious period. Infection can only be detected by
testing and by that point asymptomatic people might already be 2-3 days into their course.
• The review of the isolation period wil be a trade-off between simplicity and proportionality
• A comparison between hospitalisation rates in NZ given isolation order and rates in Australia
with no isolation order should be considered.
4.3 Point of Care Testing (POCT) The POCT order was primarily developed in context of a developing private market for rapid antigen
tests (RAT). Subsequently, the government purchased large amounts of RATs. The Chair invited
members to provide feedback on the implications of dropping the order.
1982
Feedback from members includes:
ACT
• The testing team should link in to the POCT advisory group
• Once the order disappears a mechanism should be put in place for continued regulation and
support of devices in stock for post market monitoring.
• Other tests, such as pregnancy tests, do not fall under the order and many bulk purchases are
managed through Pharmac
• The future Therapeutics Goods Bil and subsequent recommendations wil be of importance for
invitro devices
• POCT should be used in a sensible way in the future
INFORMATION
• Pharmacy guild and pharmaceutical society can be consulted with on mask use within
pharmacies (Bil y Al en as the pharmacy manager at Te Whatu Ora)
ACTION:
• As part of the inquiry into the “Future of TAG”, examine the role of COVID-19 TAG or future
OFFICIAL
infectious diseases TAG within Manatū Hauora, in making recommendations regarding mask
use. What role does this/ future TAG have in terms of reviewing, consulting, endorsing, or
signing off on guidelines?
THE
5.0 COVID-19 Strategic Framework
The COVID-19 Strategic Framework (FW), replacing the current Variants of Concern FW, will be
presented to Cabinet in early Apri
UNDER l. This high-level FW will inform the areas of activity in the more
detailed plan.
Feedback from members included:
• A member asked for the reasoning to put vaccination under preparation and not under
management. A member from the Manatū Hauora Policy team pointed out that the terms used in
the draft FW are not identical to IPC terminology (e.g., prepare ≠ prevent, manage ≠ respond)
RELEASED
• The FW is broad and can be applied to other threats which is consistent with transitioning the
COVID-19 response in line with other infectious diseases.
• A member underlined the importance of knowledge and surveil ance across al stages.
6.0 Hospitalisation admission rates per 100,000 of population by ethnicity and age
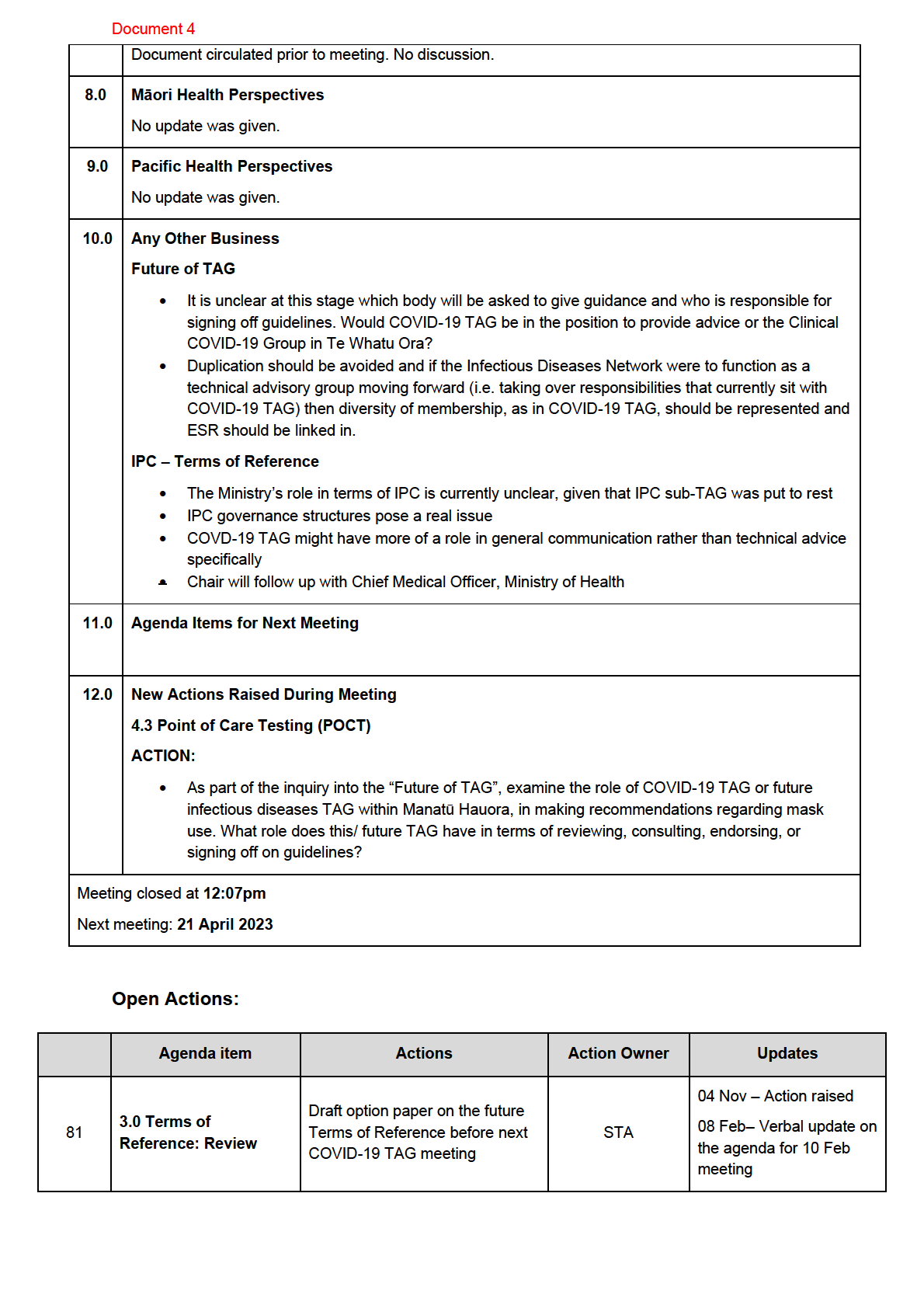
Document circulated prior to meeting. No discussion.
7.0 Delay between admission and diagnosis of COVID-19
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 4
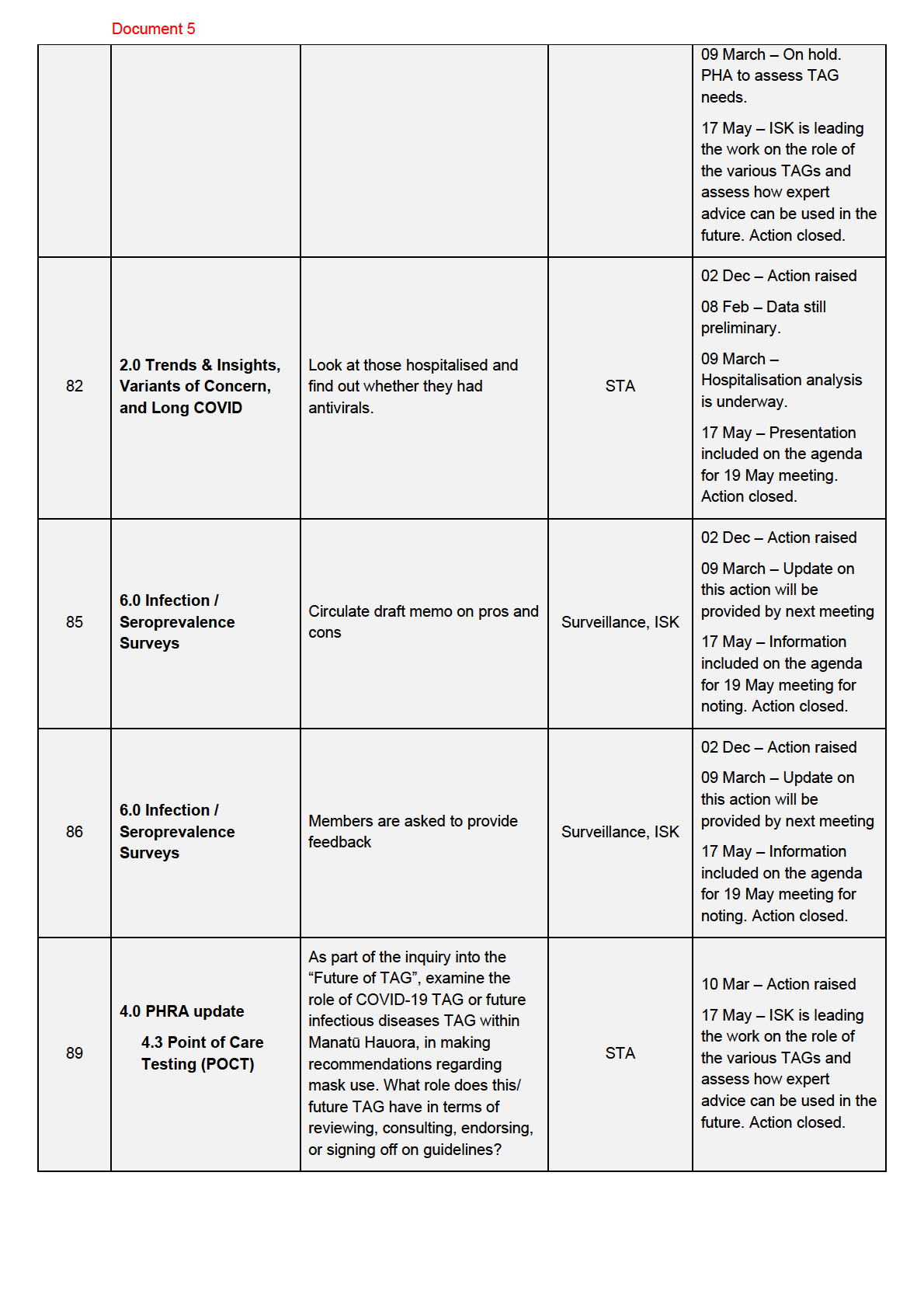
09 March – On hold. PHA
to assess TAG needs.
02 Dec – Action raised
2.0 Trends & Insights,
08 Feb – Data still
Look at those hospitalised and
preliminary.
82
Variants of Concern,
find out whether they had
STA
and Long COVID
antivirals.
09 March –
Hospitalisation analysis is
underway.
02 Dec – Action raised
6.0 Infection /
Circulate draft memo on pros and
85
Seroprevalence
Surveil ance, ISK 09 March – Update on
cons
Surveys
this action wil be
provided by next meeting
1982
02 Dec – Action raised
6.0 Infection /
Members are asked to provide
ACT
86
Seroprevalence
Surveil ance, ISK 09 March – Update on
feedback
Surveys
this action wil be
provided by next meeting
As part of the inquiry into the
“Future of TAG”, examine the
role of COVID-19 TAG or future
4.0 PHRA update
infectious diseases TAG within
Manatū Hauora, in making
INFORMATION
89
4.3 Point of Care
Testing (POCT)
STA
10 Mar – Action raised
recommendations regarding
mask use. What role does this/
future TAG have in terms of
reviewing, consulting, endorsing,
or signing off on guidelines?
OFFICIAL
THE
UNDER
RELEASED

Document 5
MINUTES: COVID-19 Technical Advisory Group
Date:
Friday 19 May 2023
Time:
10.30 am – 12:00 pm
Location:
S9(2)(k)
Chair:
Nicholas Jones
Bryan Betty, Collin Tukuitonga, Erasmus Smit, Michael Baker, Michelle Bal
1982 m,
Members:
Nigel French, Nigel Raymond, Nikki Turner, Sal y Roberts, Shanika Perera,
Virginia Hope
ACT
S9(2)(a)
Ministry of Health Attendees:
Guests:
S9(2)(a)
Apologies:
Anja Werno, S9(2)(a)
, Matire Harwood, Michael Baker
INFORMATION
1.0 Welcome and accept previous minutes
Minutes of the last meeting (10 March 2023) were approved.
Feedback included:
OFFICIAL
•
An assessment of requirements for future expert and technical advice is currently underway by
Public Health Agency (PHA). This review wil consider which government entity (e.g., Te Whatu
THE
Ora or PHA) should be leading convention of certain TAGs, such as IPC Sub-TAG. A member
requested that this process consider representation and inclusion of expertise from general
practice and community sectors.
2.0 The effect of COVID-19 oral anti
UNDER virals on hospitalisation and mortality in Aotearoa
New Zealand
A Manatū Hauora representative presented on the preliminary analysis of oral antivirals and
their effect on hospitalisation and mortality in Aotearoa New Zealand.
Feedback from the members included:
RELEASED
•
Very few cases of hospitalisations appear to be the result of adverse reaction to antiviral
treatment and therefore unlikely to have an impact on the findings.
•
It is also noteworthy that real world studies can be majorly impacted by biases and confounding.
•
The way antivirals are used makes it difficult to control behaviours and risks associated with
hospitalisation. Caution needs to be exerted against interpreting early analysis as strong
evidence between antiviral usage and reducing risk of hospitalisation.
•
The risk of death and harm appears to be concentrated in older people. The target groups have
shifted to older age groups and those with comorbidities of concern.
Document 5
•
Members noted that the prescription of Paxlovid can almost be seen as a marker that a GP
views the individual as having high risk of severe disease if untreated
•
Severity measures may be more useful and less biased than hospitalisation rates.
•
The presenter indicated that when stratified by various factors, there was initial evidence of
potential effect modification, for example by age for Molnupiravir, and by age-residential care
status (data not presented). Preliminary analyses have not shown substantial confounding by
vaccination status.
•
A case control study may be of use in the future as a different methodology if resources were
available.
3.0 PHRA – update and discussion
A representative from the Science and Technical Advisory team provided an update of the national
COVID-19 situation.
1982
Masking
The representative presented a range of evidence on the benefits of masking and highlighted the utility
to protect against a range of viral infectious diseases in the upcoming winter months. The mas
ACT k mandate
in healthcare settings was then reviewed by the COVID-19 TAG members.
Feedback from the members:
•
With the start of winter, it does not seem to be the right time to remove the mask wearing
mandate of visitors in health care settings.
•
A strong central recommendation is most likely required as the most pragmatic and workable
approach. However, residential care facilities believe they can manage outbreaks and develop
INFORMATION
their own policies for IPC guidance rather than using the COVID-19 specific mandate.
•
Masking can be a polarising issue and staff don’t want to have to be responsible to enforce this.
Additionally, appropriate risk assessments prior to patient interaction can be chal enging for
some healthcare workers.
OFFICIAL
•
The winter communication campaigns needs to be highlight to visitors that masks need to
remain on throughout all areas of the hospital including at patient's bed sides. For health care
worker the message should focus on mask use in health care facilities due to increasing winter
THE
rates of viral respiratory il nesses.
•
A mask-wearing fatigue can be noted among patients, visitors and staff and the distinction of
visitors and patients can be challenging in environments such as pharmacies, residential aged
care facilities and general
UNDER practices.
•
Mask use requirements of visitors in health care setting should be aligned to seasonal
epidemics. In general practices, policy requires the use of masks for patients and visitors;
however, in a 1:1 setting a more pragmatic approach can be noted and mask usage appears to
be dependent on the patient's concern.
•
A shift away from focus on an individual disease towards viral disease management would be
RELEASED
welcomed.
•
While masking as means of protection against influenza and RSV was neglected pre-COVID-19
pandemic, al three pathogens and their seasonality need to be considered
•
The way hospitals operate should be reviewed and needs to include measures beyond mask
wearing such as increasing ventilation and improving hand hygiene.
Self-isolation: test-to-return
Document 5
The representative informed the members that test-to-return (TTR) has been proposed as an alternative
to required isolation lengths. Evidence suggests that most cases of Omicron are infectious for up to five
days following symptom onset and international y self-isolation requirements vary. The members were
asked to review TTR, which has been used since March 2022. A TTR pathway would likely reduce the
isolation period by two days but may also increase number of people in community who are infectious
which going into winter can increase transmission and hospitalisation
Feedback from the members:
•
The NZ model ing is produced from an aggregated distribution of infectiousness and does not
account for individuals who are less infectious by day five. Evidence shows that infectiousness
by day five is a range which can vary even between household contacts
•
The impact of prior COVID-19 exposure or vaccination is probably quite smal on the period of
infectiousness in subsequent il nesses
1982
•
Current data shows that the current seven-day-system is stil exposing vulnerable groups who
later become cases or require hospitalisation.
ACT
•
The current isolation period solely focuses on COVID-19, however, public health measures
should focus on a broader context, such as including influenza and RSV.
•
The message of “if you are sick stay at home” has only risen during the COVID-19
pandemic, with previously prevalent cultural expectations of people returning to
work while stil unwell. On the other hand, many staff take up to ten days of sick
leave which highlights to need to encourage people to return to work wearing a
mask if well.
INFORMATION
•
Isolation is a social issue and mandates do not have any effect on people who don’t want to
isolate as they won't test. Having a shorter isolation of five day might encourage people to
isolate for the shorter period.
•
A transition is required and the removal of requirement for self-isolation likely is
needed but now is not the right time due to a lack of protection for vulnerable group
OFFICIAL
4.0 Pathways for removal of mandates
THE
A member from the Policy team asked the COVID-19 TAG members what types of policies/ strategies
wil need to be in place to support both COVID and general infectious disease response when these self-
isolation restrictions are removed. The public attitude towards COVID-19 is changing and pathways
towards the removal of restrictions are being explored
UNDER
Feedback from the members included:
•
The primary need should be better protection for vulnerable groups and that both public health
system responses and polices should have a wider focus to include other viral respiratory
diseases
•
Areas to focus on would include improving mask usage and increasing ventilation in health care
RELEASED
settings and to then investigate changes
•
Many members stated that the start of winter is not the right time for a transition
•
Evidence from other countries following the removal of mandates could be used to shape the
New Zealand transition. This needs to be communicated to the public clearly.
5.0 Māori Health Perspectives
•
No update was given.
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED