
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
Recommendations
Hon Chris Hipkins, Minister for Education;
It is recommended that you:
1.
discuss options regarding the School of Rural Medicine initiative with officials;
2.
forward this briefing to the Minister of Health and the Minister of Finance (please circle);
YES
NO;
3.
confirm whether you and the Ministers of Health and Finance support continuing, deferring or
stopping the tender process to establish a School of Rural Medicine (please circle).
CONTINUE
DEFER
STOP
Tim Fowler
Chief Executive
Tertiary Education Commission
21 November 2017
Hon Chris Hipkins
Minister for Education,
__ __ / __ __ / __ __
REPORT NUMBER: B/17/00840
| 3
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
Purpose
1. This briefing provides background information on the previous Cabinet’s decision to establish
a School of Rural Medicine, and outlines the next steps in the process as requested in the
Cabinet decision (refer CAB-17-MIN-0464).
2. We are also seeking confirmation of whether you and your fellow Ministers are supportive of
continuing with this initiative at this time. We recommend sharing this briefing with your
fellow Ministers followed by discussion to determine what your next steps will be. A covering
letter to provide with the briefing is provided in Appendix 1.
Executive summary
3. In August 2017, Cabinet agreed in principle to the establishment of a School of Rural
Medicine though a competitive tender. This paper reports back following that decision,
setting out the background to the decision and options for progression.
4. The School of Rural Medicine responds to a shortage of doctors in rural areas. Although
Health Workforce NZ (HWNZ) data indicates that New Zealand’s health needs will continue
to be met through domestic graduates and International Medical Graduates (IMGs) through to
2026, Officials agree there is a maldistribution issue within the medical workforce with rural
areas having poorer access to doctors than urban areas.
5. This issue was initially raised by the University of Waikato and Waikato DHB in their joint
proposal to establish a third School of Medicine based in Hamilton. This Graduate Medical
School would focus on recruiting students who are more likely to choose a rural career (those
coming from rural backgrounds, and/or with an early interest in pursuing a rural career) and
provide an enhanced clinical training experience through regional clinical training centres
were students would complete rotations and placements.
6. This School would be innovative in that it would enrol 60 graduate students each year into a
four-year graduate training programme, but would be expensive to set up.
7. In response to this, the existing medical Schools at the Universities of Auckland and Otago
developed a counter proposal – a national School of Rural Health. This expands on existing
initiatives to provide students with an enhanced rural training experience, which would
encourage them to choose a rural career.
8. There would be no increase in the number of medical students, but other health professions
such as physiotherapy, nursing, and pharmacy would be incorporated. This would support
integrated learning between professions, supporting the development of alternative care
models, as well as help address shortages in these professions.
9. The two existing proposals both have some merit in that they are likely to increase
recruitment into rural careers and make some contribution to regional development, but there
are a number of issues including that it is not clear how successful the proposals would be, or
how they would address retention of the rural workforce.
10. Establishing a School of Rural Medicine through a tender process would allow these diverse
proposals to be considered against common criteria, together with other ideas from other
interested parties. This would allow a solution to rural health problems to be selected that is
creative, innovative and provides the best solution to the problem.
11. We recommend discussing the proposal with your Ministerial colleagues before determining
whether to pursue the initiative, and the priority you would give it. If the initiative is pursued,
we suggest a two-stage competitive process comprising submission of expressions of
interest, followed by full proposals from entrants of interest.
REPORT NUMBER: B/17/00840
| 4
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
Medical training in New Zealand
Medical training is delivered by the Universities of Auckland and Otago
12. The Universities of Auckland and Otago both offer six-year medical programmes primarily
focussed on enrolling school-leavers. At both universities, prospective medical students
enrol in a Bachelor’s qualification in their first year, along with students seeking admission to
other aligned programmes such as pharmacy, dentistry and physiotherapy.
13. The first-year of study acts as a ‘weeding-out’ process to ensure students progressing to the
medical programme are academically equipped. Following this, successful students continue
for a further five years to complete their medical qualification, which includes several clinical
placements. The final year of study is the Medical Intern year in which students complete a
preparation year of clinical attachments – learning the skills to become a house surgeon.
14. There is a graduate entry pathway at both universities where those who already have an
undergraduate degree start at the second year. About 30 percent of students commencing
the second year of the current medical training programmes enter as graduates from another
degree programme.
15. In 2016, Auckland delivered over $46.5 million (approximately 1,200 equivalent full-time
Students - EFTS) and Otago delivered over $54 million (approximately 1,400 EFTS) Student
Achievement Component Level 3 and above (SAC 3+) funded provision in years 2-6 of the
Bachelor of Medicine and Bachelor of Surgery (MB ChB) qualification. Additional information
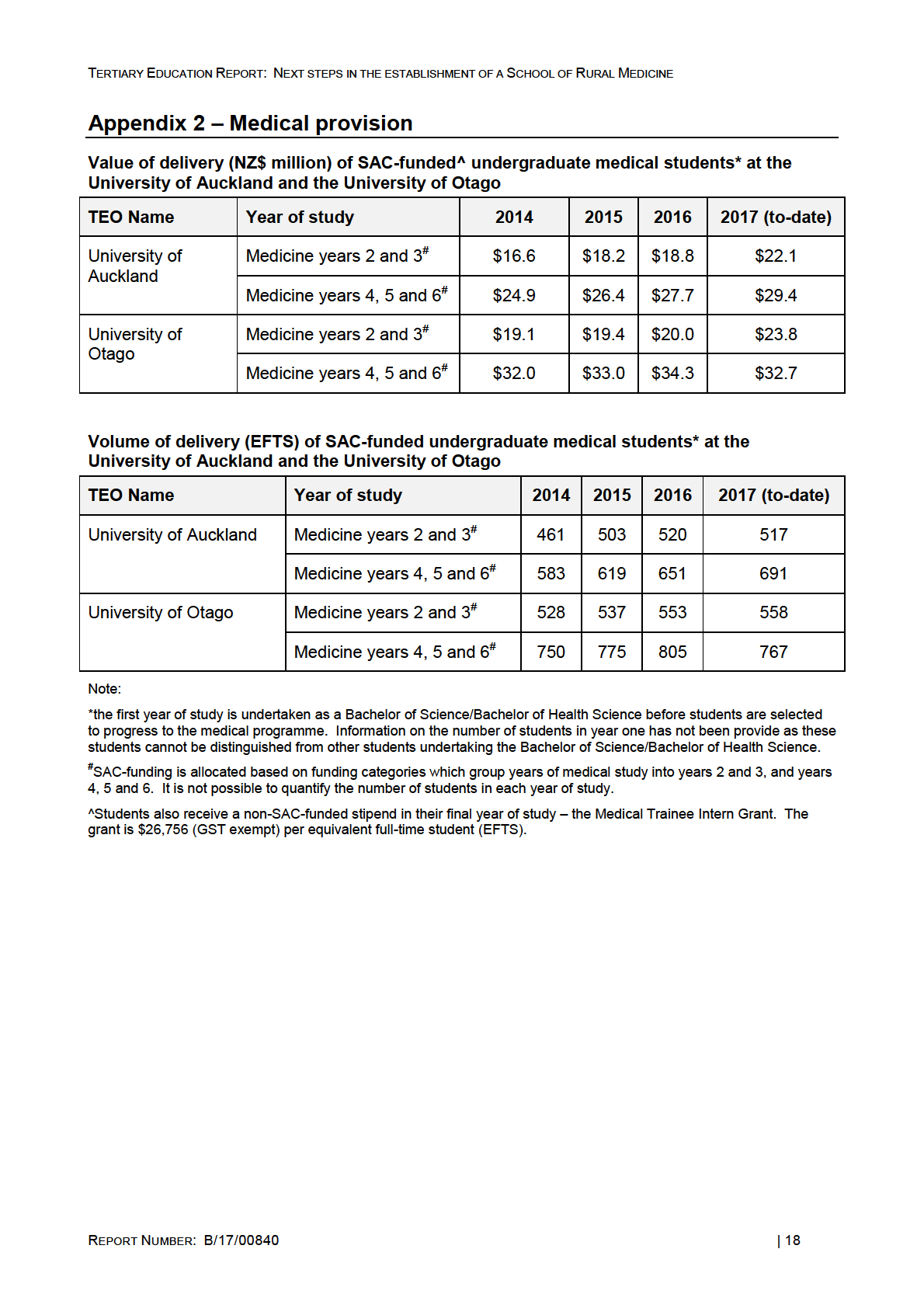
about the number of students and SAC funding is provided in Appendix 2.
Medical provision is capped
16. Medical provision is considered high-cost and the amount of delivery is therefore capped on
the first-year EFTS intake. The cap currently sits at 539 SAC 3+ funded EFTS. The
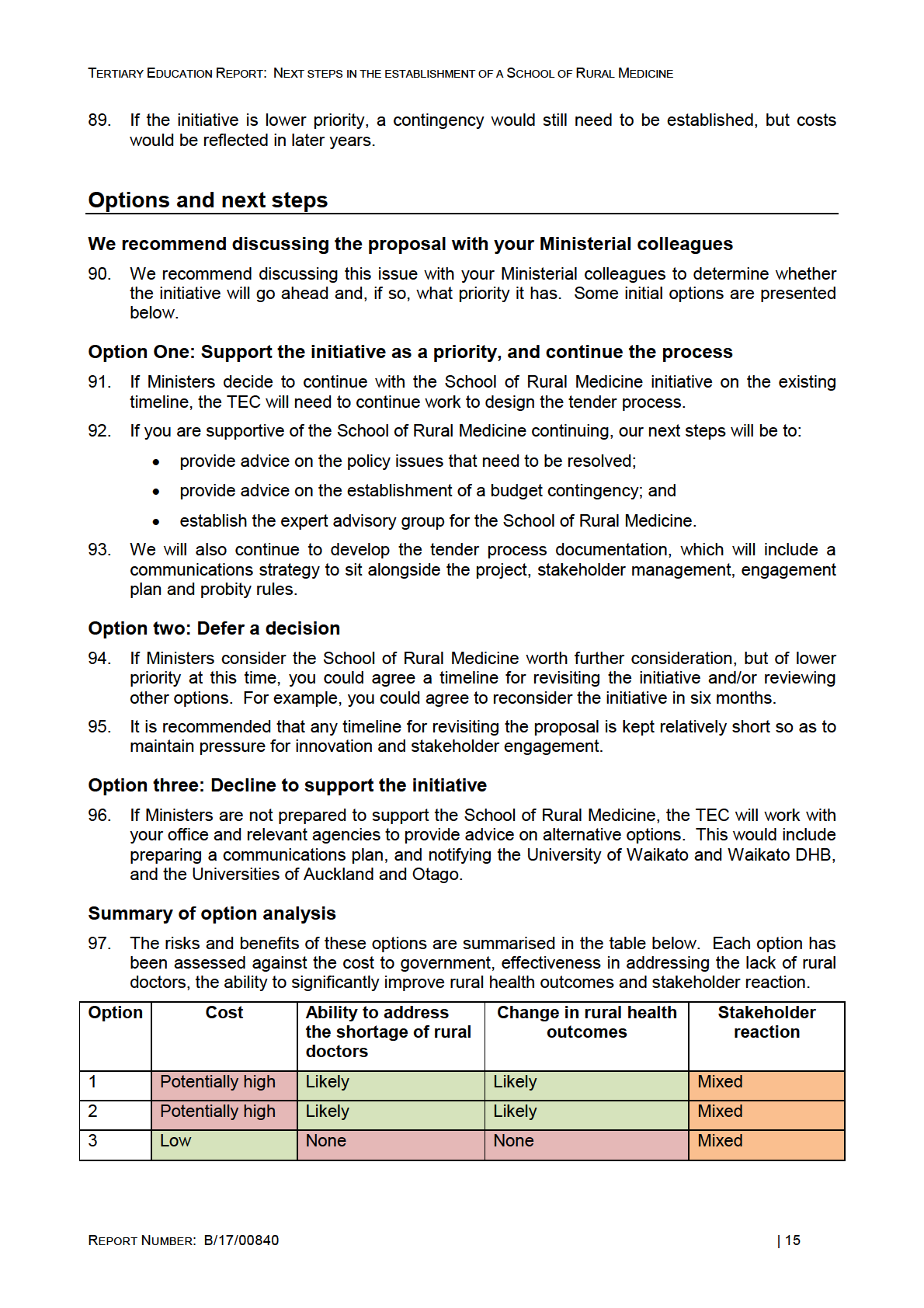
Universities of Auckland and Otago work together to agree the distribution of the cap.
Applications far exceed the number of places.
17. The cap has been raised from 365 SAC 3+ funded first-year EFTS in 2009, to its current level
of 539 SAC 3+ funded first-year EFTS. A table illustrating the total cap and how it has been
split between the Universities is provided below. It is proposed to further increase the cap to
565 EFTS.
Medical EFTS cap over time
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
First year EFTS cap
155
155
191
191
219
219
233
257
257
257
(Auckland)
First year EFTS cap
210
210
234
254
266
266
272
282
282
282
(Otago)
Total Cap
365
365
425
445
485
485
505
539
539
539
There is further training following medical school
18. Following graduation, students first undergo two years of prevocational medical training -
postgraduate year 1 (PGY1) and postgraduate year 2 (PGY2). During this period, graduate
doctors (known as interns) complete clinical attachments to gain further skills and experience.
REPORT NUMBER: B/17/00840
| 5
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
19. Following successful completion of the PGY1 and PGY2 training, doctors who wish to
specialise must undertake vocational training, usually through the relevant professional body.
This allows them to gain specialist skills and those successfully completing these courses
can then practice as specialists.
20. For General Practitioners, vocational training is a three year programme undertaken through
the Royal New Zealand College of General Practitioners. In 2015/16, there were 183
placements in GP year one training programmes and 241 applicants.
Cabinet decisions
Cabinet agreed in principle to the establishment of a School of Rural Medicine
21. On 21 August 2017, Cabinet agreed in principle to the establishment of a School of Rural
Medicine (CAB-17-MIN-0464 refers). Cabinet:
•
noted the Government has been considering two proposals to address the shortages
of doctors in rural areas in New Zealand, put forward by the University of Waikato and
the Waikato DHB, and the Universities of Auckland and Otago;
•
noted the Government has been considering advice from agencies on the issue and
potential solutions to address the shortages of doctors in rural areas, including running
a competitive process to establish a new medical school;
•
agreed in principle to the establishment of a School of Rural Medicine;
•
noted that funding would be required for the establishment of the School and its
operating costs; and
•
invited the Tertiary Education Commission (TEC) in consultation with other agencies
as appropriate, to develop a detailed plan for the competitive tender process, with a
view to reporting back to the Minister for Tertiary Education Skills and Employment in
October 2017 on their next steps.
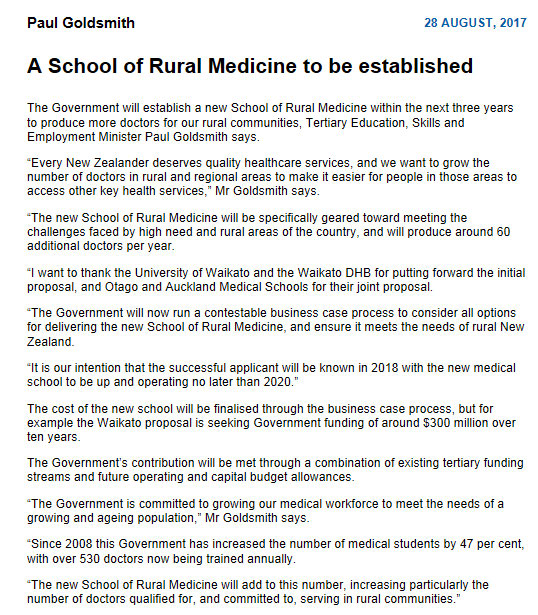
22. This report back responds to the Cabinet minute. The previous Minister’s press release
relating to the decision is provided in Appendix 3 for your information, stating the
Government’s intention for the school “to be up and operating no later than 2020”.
The School of Rural Medicine initiative responds to proposals to address rural
health issues
23. Nationally, there is a shortage of doctors in rural areas. Although the current and projected
number of New Zealand medial graduates together with International Medical Graduates
(IMGs) is enough to keep pace with population growth, there is a maldistribution of the
workforce arising from the recruitment and retention of doctors in rural areas.
24. Lack of access to primary care has the potential to impact significantly on the health of New
Zealand’s rural population. Studies from the USA indicate that primary care supply has been
associated with improved health outcomes including for all-cause mortality, cancer, heart
disease, stroke and infant mortality, low birth weight, life expectancy and that self-rated
health is also improved.
25. Over the last 12 months, two proposals have been presented to Government, both aimed at
increasing rural healthcare provision. These proposals are discussed further below.
Both
proposals aim to improve recruitment of the rural health workforce, but both proposals differ
significantly in both scope and cost.
26. Given the differences between the existing proposals it was determined that a competitive
tender process would best allow these proposals to be compared. The process could
generate a wider range of options from a wider range of providers, which could generate a
more innovative and cost-effective solution to be developed.
REPORT NUMBER: B/17/00840
| 6
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
The problem…
There are fewer medical practitioners in most rural areas
27. Nationally, urban areas have on average greater access to general doctors than rural areas.
The latest data we have (below and Appendix 4) is from 2014, but we understand it is soon to
be updated by HWNZ.
28. The 2014 data from HWNZ illustrates that whilst mostly urban DHBs such as Capital and
Coast have high numbers of general doctors (87 per 100,000 population), rural DHBs such
as West Coast and Taranaki have fewer general doctors (61 and 60 per 100,000 population
respectively). Full data is provided in Appendix 4, but it is noted that HWNZ has recently
received data from 2016, which will be presented to the Minister of Health shortly.
29. The inequalities in the distribution of doctors also extends to other health professions as
illustrated below:
30. The underlying reasons for the maldistribution are complex. Factors which contribute to
difficulties in recruiting and retaining health professionals in rural locations include:
• a general lack of support, including cover for training or holidays due to overall shortage
of health professionals and lack of rural staff
• perceptions of long hours and reduced down-time (particularly relevant for doctors,
nurses and midwives who are often ‘on-call’ outside of working hours)
• practices are often located in remote areas with few facilities and few opportunities for
partners and children
• geographic distance between patients (this particularly applies to midwives and other
professions that undertake home visits) or practices (relevant to professions that
undertake clinics at differing locations)
• lower intensity than urban practices, which leads to lower salaries for those remunerated
on a per patient or per hour basis.
REPORT NUMBER: B/17/00840
| 7

TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
31. In addition the age profile of the current rural medical workforce means a significant number
of existing doctors will retire in the near future. A diagram setting out the issues faced by the
rural medical workforce is provided below:
International Medical Graduates (IMGs) fill the gaps
32. To mitigate the geographic and specialty maldistribution of the medical workforce, New
Zealand imports approximately 1,100 IMGs per year1. In 2016, IMGs made up around 35
percent of the registrar workforce.
33. In 2017, IMGs made up 43 percent of the senior medical officer (SMO) workforce2. HWNZ
estimates that 51 percent of IMG SMOs have a New Zealand or Australasian vocational
qualification. This means while they may have done their basic medical training overseas,
they did their specialty training in New Zealand or Australia. In the case of general practice,
rural hospital medicine, and urgent care, approximately 75 percent of the IMGs practising
under these specialties only have a qualification from the respective New Zealand medical
college.
34. Most of these IMGs only remain in New Zealand for a short period of time and of each cohort,
only around 30 percent are retained in the medium term.3
35. The high turnover of IMGs affects continuity of care, which is particularly important in general
practice. One way of addressing this is to improve retention of IMGs to ensure their skills
remain in the New Zealand health system.
36. Whilst IMGs bring diversity, which contributes to innovation, as well as addressing workforce
pressures, they often have little understanding of the social and cultural context in which they
practice, which can have significant impacts on some patients. This is more important in
some specialties than others.
1 Three distinct groups of IMGs come to New Zealand. Firstly, junior doctors on short term (one to two years) contracts having a working overseas holiday,
who help fil a short term service need. This level of service need is reducing with the rise in the number of domestic graduates. Secondly a group of IMGs
come to obtain specialist training in New Zealand’s high quality training programmes and many of these are retained in New Zealand when they obtain
employment as a specialist. Thirdly there are IMGs who obtained their undergraduate and specialist training overseas, or are working in New Zealand as
locum generalists.
2 Based on the number of practising SMOs as at May 2017 according to Medical Council of New Zealand data
3 Medical Council of New Zealand. (2016).
The New Zealand medical workforce in 2013 and 2014.
REPORT NUMBER: B/17/00840
| 8
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
37. Importing medical graduates reduces the number of medical students that need to be
educated in New Zealand. This means there are fewer opportunities available to New
Zealanders to study medicine at an undergraduate level in New Zealand. However, importing
SMOs assists with the ability to provide high quality specialist training programmes.
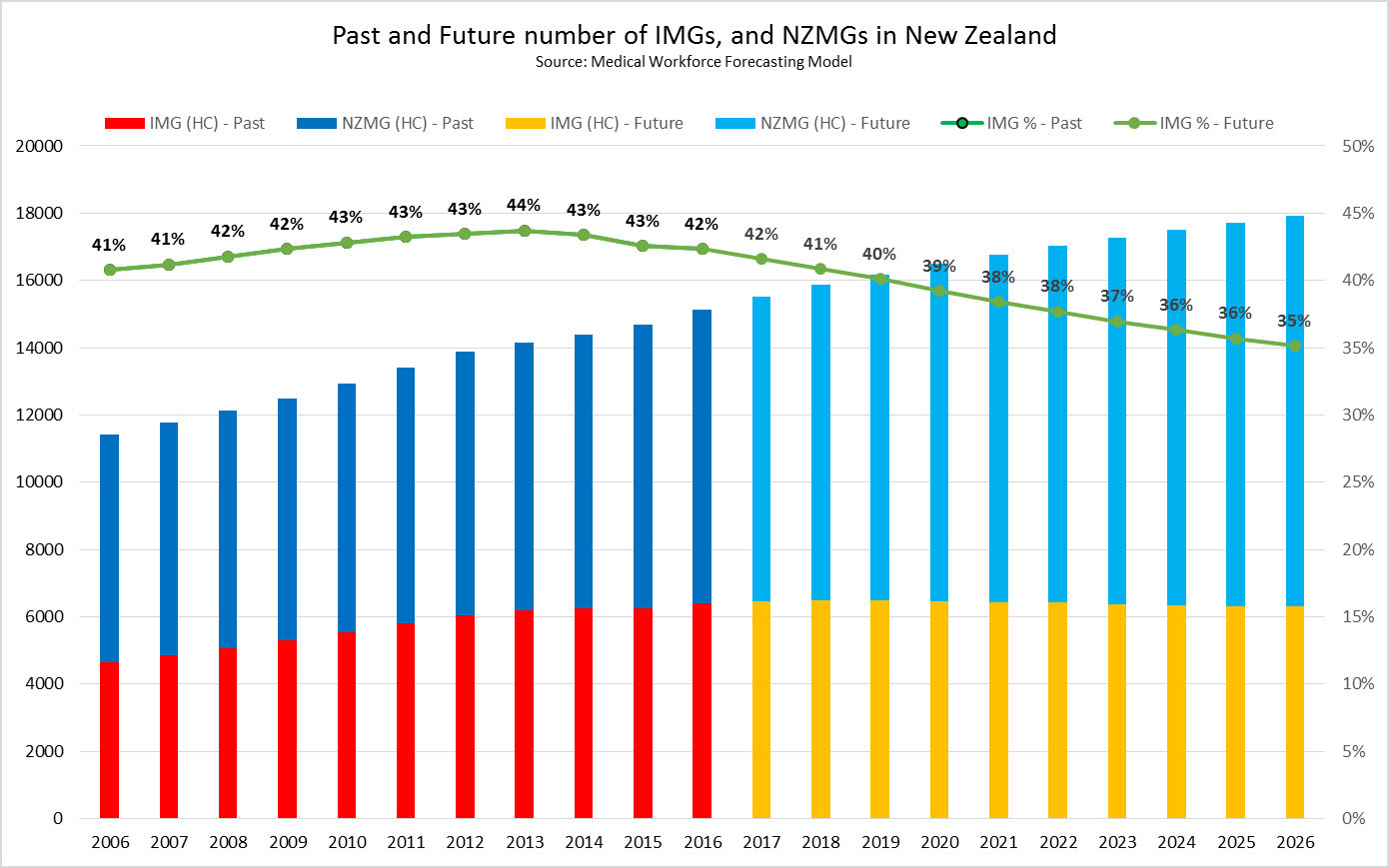
38. The chart below shows the past, current and forecast future number of IMGs and New
Zealand medical graduates in the health workforce. Between 2006 and 2013, the number of
IMGs employed in New Zealand rose, but reliance on IMGs from 2018 onwards is forecast to
level off or slightly reduce with increased numbers of New Zealand medical graduates
meeting New Zealand health needs.
There are two recent proposals to address problems in the rural medical
workforce, but both have positives and negatives
39. Proposals have been received from the University of Waikato and Waikato DHB, and the
Universities of Auckland and Otago. Background information about the Universities involved
in each proposal is provided in Appendix 5.
40. The University of Waikato and Waikato DHB proposal was submitted as an Indicative
Business Case in accordance with the Treasury’s Better Business Case process. The
proposal from the Universities of Auckland and Otago is a presentation accompanied by a
discussion paper and has not yet been developed into a business case.
41. Officials have provided advice to Ministers on both proposals, including the steps required to
produce a business case that contains enough information on which a decision can be made
by Ministers. This information has also been provided to the Universities and Waikato DHB
as comments.
42. The two proposals are briefly summarised below, with additional information provided in
Appendix 6. A comparison between the proposals is provided in Appendix 7.
REPORT NUMBER: B/17/00840
| 9
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
A graduate-entry medical school is proposed by the University of Waikato and
Waikato District Health Board (the Waikato proposal)
43. In late 2016, the University of Waikato and Waikato DHB submitted a joint proposal to
establish a new graduate-entry medical school. The new medical school would be based in
Hamilton and 12-15 regional clinical training facilities would be established over a ten-year
period to deliver enhanced clinical training in a rural setting.
44. This proposal is estimated to require government capital expenditure of $111.7 million with an
operating subsidy over its establishment phase of around $100 million.
45. Once fully established, operational funding of approximately $75 million per year would be
needed. It is noted that the business case does not include the additional funding needed for
vocational training of graduates. The total amount of HWNZ funding for vocational training
years would depend on the graduate’s choice of vocational training, but is likely to be at least
$9 million per annum4.
46. The school would provide a four-year graduate-entry medical programme for 60 students per
annum beginning in year five of the establishment period. This is a model of training used
commonly overseas and is one year shorter than the current graduate entry pathways at the
Universities of Auckland and Otago.
47. Student selection would be based around practices shown to be effective in recruiting
students who will later choose a rural career.5,6,7,8 It will also provide an enhanced rural
training experience, which has also been shown to be important in encouraging graduates to
work in rural areas.
The Waikato proposal has put pressure on current medical schools to innovate
48. One significant advantage of the Waikato proposal is that it encouraged the existing medical
schools to think about how they could change their current practice to address rural health
needs.
49. The Universities of Otago and Auckland have both invested time and effort in developing a
counter-proposal, which whilst based on international best practice, is something that both
Universities could have developed much sooner.
The Universities of Auckland and Otago propose establishing a dedicated School of
Rural Health (the Auckland/Otago proposal)
50. This proposal builds on the expertise that the Universities of Auckland and Otago have
established through their existing medical training programmes. It is based on the existing
Rural and Regional Admission Schemes, which use rural ‘hubs’ to train medical students.
The proposal would establish additional hubs nationwide, which would be based in rural
hospitals and linked to local communities.
51. The proposal does not ask for an increase in the medical EFTS cap so there will be no new
doctors.
4 It is noted that the vocational funding is the minimum amount required and is based on al students pursuing general practice careers. If students
pursue other specialties, costs wil be higher.
5 Playford DE., Evans, SF., Atkinson, DN., et al. 2014. Impact of the Rural Clinical School of Western Australia on work location of medical graduates. Medical
Journal Australia 200: 104-107
6 Poole, P., Stoner, T., Verstappen, A., and Bagg, W. (2016). Medical Students: Where have they come from and where are they going? NZ Medical Journal,
129.
7 Shelker, W., Zaharic, T., Sijnja, B., & Glue, P. (2014). Influence of rural background and rural medical training on postgraduate medical training and location
in New Zealand.
NZ Medical Journal, 127, 12-16
8 Matthews, C., Bagg, W., Yielder, J., Mogol, V., and Poole, P (2015). Does Pūkawakawaka (the regional-rural programme at the University of Auckland)
influence workforce choice? NZ Medical Journal, 128, 35-43.
REPORT NUMBER: B/17/00840
| 10
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
52. The proposal does incorporate vocational medical training. This allows for medical training to
be vertically integrated with more advanced medical students contributing to teaching and
learning experiences of newer students, and supporting other professions.
53. Although the proposal includes several options for scaling the proposal, their preferred option
is to develop ten hubs over a five-year period to provide education across multiple health
disciplines including medicine, nursing, midwifery, pharmacy and physiotherapy. The hubs
would accommodate full-year rural immersion and short-term rural clinical placements for
both undergraduate and postgraduate vocational students.
54. The hubs would address retention of the existing rural workforce by providing a focal point for
networking, professional development and general support. In addition, students involved in
the hub would provide support to established rural practices and help reduce pressure on the
existing workforce.
55. Their preferred option seeks additional operational funding of up to approximately $13.8
million per annum from the Crown. No capital funding has been sought. Officials believe
these costings to be underestimated.
Both proposals have merit
56. In addition to using student recruitment practices that are likely to encourage more medical
graduates to seek a rural career, each proposal has the potential to deliver several other
benefits.
57. Each has some capacity to incorporate other professions. This is stronger for the
Auckland/Otago proposal where integrated learning between professions is a key feature.
This facilitates closer interdisciplinary working relationships and post graduate learning
opportunities, and the introduction of alternative models of care that would support existing
rural general practices.
58. Both proposals could contribute to regional development goals. The Waikato proposal
specifically identifies the key economic benefits that the medical school would bring to the
region, including increased GDP, increased direct and indirect employment, skills and training
opportunities, and increased innovation. The Auckland/Otago proposal would spread the 10
hubs and spokes in rural areas throughout New Zealand.
59. The proposals may also contribute to Crown-Māori economic growth partnership goals
including growing the future Māori workforce, and strengthening the transition from education
to work for Māori.
60. Additionally, each proposal indicates that it would incorporate a research component. The
outputs from this research would bring benefits to DHBs, primary care providers, community
groups and local iwi, as well as tertiary education providers. There is also significant
opportunity for the research to contribute to the wider aims of government, including the
Health Research Strategy.
61. Finally, it is noted that the Waikato proposal would provide a less costly option for graduate
medical training as it is one year shorter than the current graduate entry programmes offered
by the Universities of Auckland and Otago. Compared to the Waikato proposal, the graduate
pathway at the Universities of Auckland and Otago involves an additional year of study at a
cost of approximately $15,000 to the student (currently) and $43,000 to Government (per
EFTS). However, the cost of undertaking a degree followed by medical training is likely to be
higher than direct entry into a medical training programme.
REPORT NUMBER: B/17/00840
| 11
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
But there are issues and risks associated with each of them
62. The chief concern with both proposals is that although they are based on established
strategies, it is not clear how many medical graduates would enter rural practice or, how long
they would be retained in the rural health workforce. They will both need to have other
programmes and support measures built around them to support doctors practicing in rural
and remote areas.
63. The Waikato proposal is costly. There is also potential for the costs of both proposals to
increase if any of the other funding streams are unable to deliver.
64. An important concern with the Waikato proposal is Waikato DHB's ability to focus on this
work when it has a number of issues to deal with, including its financial performance,
updating core IT systems, leadership, relationships with Midland Health Network and
performance on the ‘Shorter Stays in Emergency Department’ Health Target.
65. Any increase in numbers of medical students may affect the availability of clinical
placements. It is noted that Waikato DHB has already informed the Auckland Medical School
that if the Waikato proposal is successful, it will look to reduce the number of University of
Auckland students undertaking clinical placements in its hospitals. The Universities of
Auckland and Otago already report difficulties in securing enough clinical placements for their
students. One of the issues behind this appears to be funding, and the demands on already
busy practitioners resulting from having students in their practice. However, the Waikato
proposal intends to tackle this by broadening the range of clinical placements.
66. There may also be system capacity issues associated with training additional doctors, who
will need mentoring and supervision when they enter the workforce.
The tender process can be designed to ensure that the best solution to
the problem is chosen
Diverse proposals from a range of providers should be encouraged to allow the
best, most cost-effective proposal to be identified
67. If the initiative goes ahead, the School of Rural Medicine must provide the best available
solution to the rural medical problem, addressing recruitment, distribution and retention of the
rural health workforce. Recruiting students who are more likely to choose a rural career does
not guarantee that they will choose or remain in a rural location. Therefore, the School of
Rural Medicine could support recommendations made by the WHO to implement initiatives
which would encourage retention of the existing rural medical workforce.
68. The tender process should encourage innovation and creativity in addressing rural health
inequalities, as well as allow diverse proposals to be considered against a common set of
goals and criteria.
69. It is important that the tender process we establish is able to accommodate both options that
are already proposed. It is noted that other Universities have expressed interest in the
School of Rural Medicine and may develop proposals that will address rural health issues in
other new and innovative ways.
70. In addition, the School of Rural Medicine could be used to promote different models of care in
rural practice outlined earlier, such as increased use of technology to address health needs,
greater use of nurse practitioners etc.
REPORT NUMBER: B/17/00840
| 12
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
A two-stage tender process will allow other parties to indicate their interest
71. If you support continuing the initiative, we suggest a two-stage process. The first stage is to
seek expressions of interest (EOIs), which will be reviewed prior to inviting a more detailed
proposal to be submitted in the second stage of the process. This will both allow other
entrants to get up to speed without requiring significant costly work, and ensure unsuitable
proposals are rejected before parties commit too much time, effort and money in developing
detailed proposals.
72. Proposals would be considered in terms of their ability to address both recruitment and
retention of the rural medical workforce, and provide a pipeline for rural medical provision.
The cost-effectiveness of the proposals will also be considered.
73. The TEC has previously run competitive tender processes to select ICT Graduate Schools,
Centres of Research Excellence, Entrepreneurial Universities and other initiatives. The
documentation and standard process requirements can be adapted for the School of Rural
Medicine process.
74. As both existing proposals have received advice from agencies, we will need to ensure that
this does not constitute an unfair advantage to these proposals over other novel proposals.
Therefore ensuring probity requirements are met will be an important consideration.
Establishment of an expert advisory group to assist in the process
75. As significant levels of funding may be required, Cabinet will need to make the final funding
decision. It is suggested that this is based on advice from officials and an independent expert
advisory group as this will bring credibility to the final decision and reinforce that the decision
is made on merit.
76. The independent expert advisory committee would review the EOIs and provide advice on
detailed proposals. This advice would then be considered by the Minister(s), then Cabinet,
which would decide which final option to support.
77. Care would be needed to ensure the advisory group is perceived as truly expert and
independent. It is recommended that members are sought who have skills and experience
with rural health, medical training, and procurement. It would also be useful to appoint some
members who have international expertise in addressing rural health issues, since they would
bring different knowledge and perspective.
78. It would also be important to effectively manage conflicts of interest. A large number of
expert advisors have been involved in the development of the existing proposals. In addition,
given New Zealand medical professionals will likely have attended the Universities of
Auckland or Otago, the perception of loyalties to these institutions must be carefully
managed.
REPORT NUMBER: B/17/00840
| 13

TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
Proposed timelines
Under current timelines the successful applicant would be known by 2018, and the
School of Rural Medicine would be up and operating no later than 2020
79. The following timeline is proposed:
80. To meet the timeline previously announced, a public call for EOIs would be made in February
2018, closing end of March. Successful entrants would be invited to submit full in-depth
proposals in June 2018.
81. It is anticipated that advice to Cabinet would be provided to enable a final decision to be
made by late September/early October 2018. A period of establishment would then occur
and the new School of Rural Medicine could commence operations in 2020.
There are some policy issues that need to be addressed
82. The above timeline calls for preparation and planning to be completed by early 2018. This
includes resolving some policy issues and Budget contingency establishment.
83. The most pressing policy issue is whether the School of Rural Medicine will deliver additional
doctors as noted in the press release (Appendix 3), or not. If so, consideration will need to be
given to whether the existing model of allowing students to choose places and specialities will
be followed, or whether a different model can be implemented to funnel a greater proportion
of graduates into rural general practice.
84. It should also be considered whether the School of Rural Medicine should provide training
and support to other professions as well as medicine.
85. As noted, there are also opportunities to design the initiative to encourage proposals to
support recommendations made by the WHO to support implementation of additional
strategies to mitigate rural health workforce issues.
86. If you support continuing with this initiative, we will provide a policy decision paper to you to
consider these issues.
A Budget contingency would need to be established
87. If you wish to continue with the initiative, agencies, particularly Treasury, can provide advice
on how to place this within the Budget process and the part of the Government’s fiscal plan
this should sit under.
88. If the initiative is to be funded and is a Government priority, a contingency would have to be
established in Budget 2018 that would facilitate the tender process, with full cost implications
to be reflected in Budget 2019 and beyond.
REPORT NUMBER: B/17/00840
| 14
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
Consultation
98. The TEC has prepared this briefing. The Treasury and the Ministries of Health and
Education have been consulted.
Ministry of Health comment
99. The Ministry of Health’s view is that rural health workforce shortages are not due to a lack of
medical graduates, but rather a maldistribution of the workforce arising from the recruitment
and retention of health practitioners, including doctors, in rural areas.
100. The Ministry supports increasing access to rural health services through initiatives that
promote interdisciplinary ways of working and enabling health practitioners to work to the full
extent of their skills and abilities. Other health professionals, including primary care nurses,
midwives, pharmacists, dentists, and physiotherapists, also have a role in providing rural
health services. As such, the Ministry support an interdisciplinary school rather than a
medical school.
101. The Ministry supports introducing packages of initiatives to improve retention and distribution
of the rural health workforce, including international health practitioners.
102. The level of funding that is required from Vote Health would need to be further clarified.
REPORT NUMBER: B/17/00840
| 16
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
Appendix 1 – Cover note for other Ministers
Hon Grant Robertson
Minister of Finance
PARLIAMENT BUILDINGS
Hon David Clark
Minister of Health
PARLIAMENT BUILDINGS
Dear Grant and David,
Establishment of a School of Rural Medicine
I attach a briefing from the Tertiary Education Commission regarding the previous Government’s
proposal to establish a School of Rural Medicine. This briefing takes account of the events that led
to the decision and sets out some options for our next steps. Comment from the Treasury, the
Ministry of Health and Ministry of Education is also incorporated.
I look forward to discussing the options for progressing the consideration of this proposal, and the
broader issues of the rural health workforce with you.
Yours sincerely
Chris Hipkins
Minister of Education
REPORT NUMBER: B/17/00840
| 17
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
Appendix 3 – Press release
REPORT NUMBER: B/17/00840
| 19
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
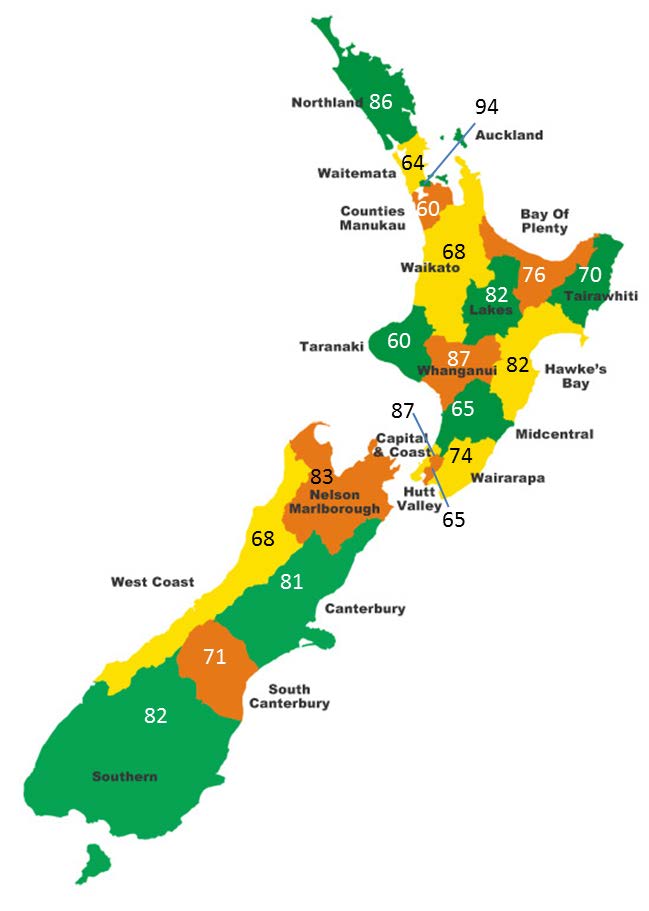
Appendix 4 – Distribution of GPs
General practitioner FTE per 100,000 population (data from 2014)
Note:
The data presented is for 2014. We understand additional data from 2016 will soon be available.
The data indicates clustering around the main training centres (Auckland, Christchurch and Dunedin). When split into
regions, the distribution of GPs in the Southern DHB is 85 GPs per 100,000 in Otago and 78 GPs per 100,000 in
Southland.
It is noted that health inequalities for rural populations are likely to be greater than they appear because of problems with
data collection and the use of inappropriate geographic classification systems. This is particularly troublesome for Māori
health as Māori are more likely to live rurally than other groups. Given issues with data collection in main centres (caused
by GPs practicing across DHBs, or living in one and working in the other) it is better to view Capital and Coast and Hutt
Valley as a combined entity with 80 FTE per 100,000 population and Waitemata, Auckland and Counties Manukau as a
combined entity with 70 FTE per 100,000 population.
REPORT NUMBER: B/17/00840
| 20
TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
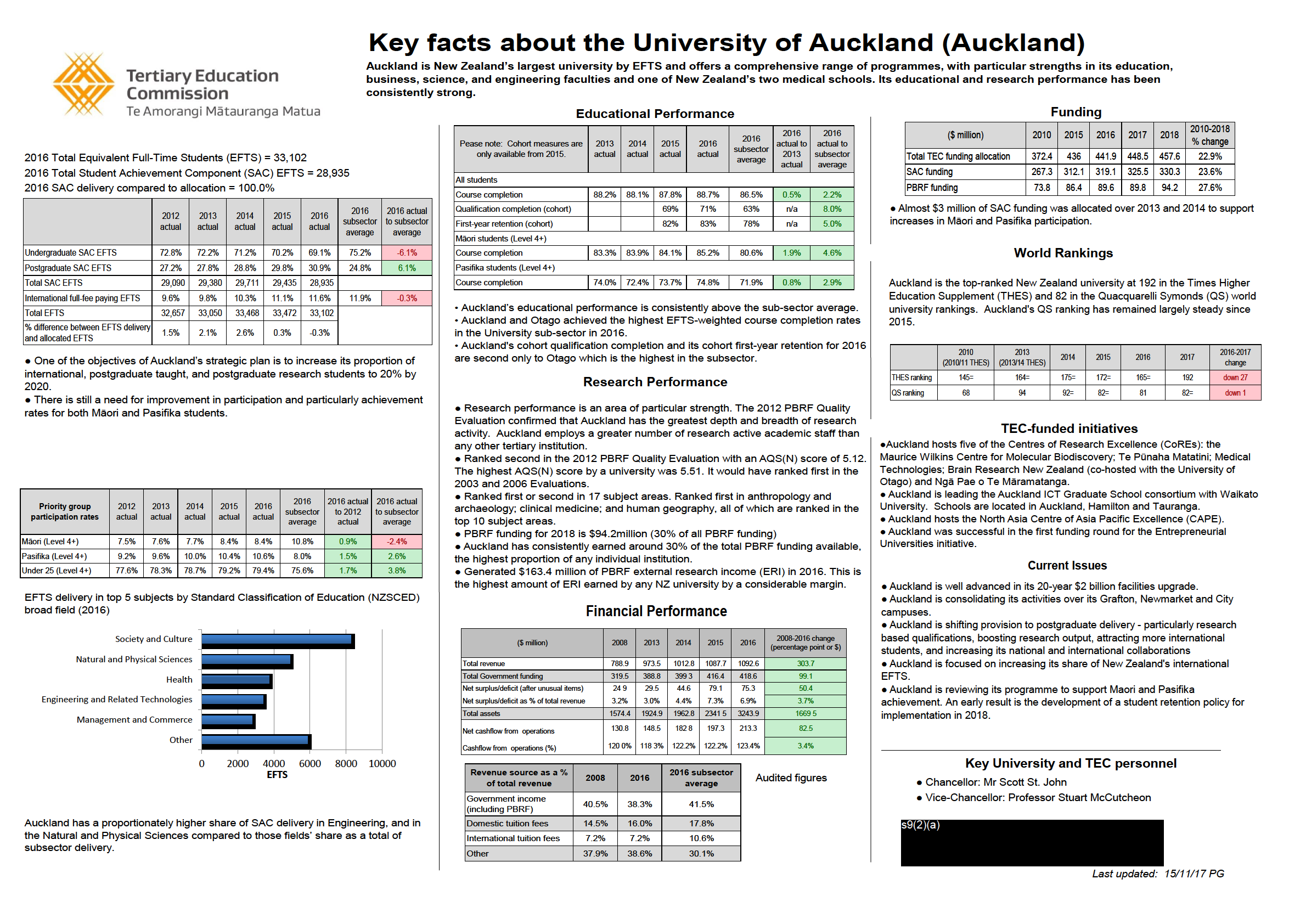
Appendix 5 – Key facts about the Universities of Auckland, Otago and
Waikato
See attached A3s.
REPORT NUMBER: B/17/00840
| 21


 Appendix 6 – Summaries of each proposal
Appendix 6 – Summaries of each proposal

TERTIARY EDUCATION REPORT: NEXT STEPS IN THE ESTABLISHMENT OF A SCHOOL OF RURAL MEDICINE
REPORT NUMBER: B/17/00840
| 23
