

GOV-025316 Appendix 1
Assess and Arrange Neuropsychological Assessment v28.0
Outputs
8.0
Create and send referral documents
9.0
Receive and review Assessment Report
7.0
Create purchase order
6.0
Confirm availability of provider
4.0
Request assessment referral
5.0
Review task
3.0
Contact client or family to discuss assessment
2.0
Determine need for assessment
riggers & Inputs
T
1.0
Receive assessment request
Assistant
Administrator
Assistant
Assessor
Cover
Recovery
Recovery Coordinator
Recovery Partner
Recovery
Recovery
Recovery Coordinator
Recovery Partner
ACC > Claims Management > Manage Claims > Manage Treatment Interventions / Supports > Assess and Arrange Neuropsychological Assessment
Uncontrolled Copy Only : Version 28.0 : Last Edited Monday, 9 January 2023 10:33 AM : Printed Thursday, 1 June 2023 7:19 AM
Page 1 of 6

GOV-025316 Appendix 1
Assess and Arrange Neuropsychological Assessment v28.0
NOTE What do you need to consider when the
Summary
entitlement request is received and deemed
cover exists?
Objective
Refer to the Deemed Cover and Entitlements
To assess and arrange Neuropsychological assessment re-
Policy for considerations to determine client
quests to support a client’s covered injury.
entitlement eligibility while in deemed cover
period.
These requests are managed directly by Recovery Team Mem-
Deemed Cover and Entitlements Policy
bers.
NOTE What if further guidance is needed to deter-
mine if an assessment is needed?
Refer to Seek Internal Guidance.
PROCESS Seek Internal Guidance
Background
b Approve or decline the request. Refer to NG Principles
The neuropsychological assessment service aims to:
Decision Making.
• confirm the existence of traumatic brain injury (TBI) and deter-
NG Principles Decision Making
mine how the client is affected by the TBI
• confirm whether the client’s symptoms have been caused by
the injury or if there may be other possible causes
3.0 Contact client or family to discuss assessment
• provide recommendations for intervention, if appropriate.
Cover Assessor, Recovery Assistant, Recovery Coor-
dinator, Recovery Partner
Assessments look at the client’s cognitive, behavioural, emo-
a Contact the client to discuss the need for a Neuropsy-
tional, social and vocational functioning.
chological Assessment.
b Confirm you are speaking with the right person by asking
Owner
[Out of Scope]
ACC's identity check questions. If this is not the client,
ensure the requestor has an Authority to Act on file.
Expert
Identity Check Policy
Procedure
NOTE What if the client requests the Recovery
Team Member to discuss the treatment re-
1.0 Receive assessment request
quest with another person?
Cover Assessor, Recovery Assistant, Recovery Coor-
Go to Obtain Authority to Act (ATA).
dinator, Recovery Partner
PROCESS Obtain Authority to Act (ATA)
a Assess the request for a Neuropsychological Assess-
ment, refer to Neuropsychological Assessment Overview
c Explain the purpose of the assessment, and what their
Service Page for more information on the assessment.
rights and responsibilities are.
Neuropsychological Assessment Overview Service
Client Legislative Rights and Responsibilities Policy
Page
NOTE What if the client has a preferred provider?
Neuropsychological assessment overview
If the client has a preference, load the provider
https://go.promapp.com/accnz/Process/8ce3affe-069f-4f1b-9ebe-414fd618a897?force=False
and their vendor as a participant. Ensure the
vendor and provider are contracted for this ser-
NOTE What if the request involves a change or
vice by using the Geographic Location search.
update in the client's diagnosis or covered
This enables Recovery Administration to validate
injury?
the email and then email the purchase order di-
Refer to the process below.
rectly from Eos if required.
PROCESS Assess Cover for an Additional
• The Recovery Team Member must ensure all
Injury or Change in Diagnosis
known participants are loaded on the file and
then removed when no longer relevant. For infor-
mation on how to manage participants, refer to
2.0 Determine need for assessment
Manage Participants (Eos Online Help).
Cover Assessor, Recovery Assistant, Recovery Coor-
Manage Participants (Eos Online Help)
dinator, Recovery Partner
Client choice of providers Policy
a Confirm the client's eligibility for the assessment.
d Check the client has provided consent to collect and
NOTE What is the eligibility criteria for a Neuropsy-
share information.
chological assessment?
A client is eligible for a neuropsychological
View Client Consent
assessment when they’ve suffered a covered
NOTE What if the client has not provided consent?
personal physical injury for which they have
Go to Obtain Client Authority to Collect Infor-
entitlement. See the AC Act 2001, Section 67 for
mation.
more information.
PROCESS Obtain Client Authority to Col-
AC Act 2001, Section 67
lect Information
https://legislation.govt.nz/act/public/2001/0049/latest/DLM100999.html?search=ad_act__accident+compensation_2001__67_25_ac%40bn%40rn%40dn%40apub%40aloc%40apri%40apro%40aimp%40bgov%40bloc%40bpri%40bmem%40rpub%40rimp_ac%40ainf%40anif%40bcur%40rinf%40rnif_a_aw_se_&p=1
e In Salesforce, record the details of the discussion with
the client as a contact.
ACC > Claims Management > Manage Claims > Manage Treatment Interventions / Supports > Assess and Arrange Neuropsychological Assessment
Uncontrolled Copy Only : Version 28.0 : Last Edited Monday, 9 January 2023 10:33 AM : Printed Thursday, 1 June 2023 7:19 AM
Page 2 of 6
GOV-025316 Appendix 1
NOTE What do you have to do to document your
NOTE What if you find information that needs to be
decision?
redacted?
Refer to Issue Recovery Decision process.
Send an email to Recovery Administration
PROCESS Issue Recovery Decision
([email address]) and include the
document to be redacted plus your redaction
NOTE What if the request is declined?
instructions, before adding the document to the
Generate the SPD999 decision letter and create
document group.
an NGCM - Send Letter task.
NGCM - Redact information from PDF documents
f Add the Neuropsychological Assessment action as an
c
agreed intervention to the Recovery Plan.
Add the documents to the group.
NOTE How do you update the Recovery Plan?
NOTE What if there are documents from other
claims that are relevant to the assessment?
Go to Create or Update Recovery Plan.
When a request for a referral is required and the
PROCESS Create or Update Recovery
supporting documents are on another claim, it is
Plan
important to transfer the documents to the rele-
g Contact the client's GP or relevant specialist (if neces-
vant claim. This will ensure the right documents
sary) to request relevant medical information needed to
support the recovery decisions for each claim.
assess the assessment request, refer to the process
To transfer documents from one claim to anoth-
below.
er:
• Create a bulk print of all documents on the
NOTE How do you request medical records?
other relevant claim and complete mandatory
Refer to Request Clinical Records.
fields and description
PROCESS Request Clinical Records
• Open PDF document from email link
• File the PDF away to the relevant claim
• Repeat these steps if there is relevant docu-
4.0 Request assessment referral
ments on multiple relevant claims
Cover Assessor, Recovery Assistant, Recovery Coor-
dinator, Recovery Partner
The PDF should also be renamed something
short but relevant, and identify which claim
a In Eos, create a referral-specific document group and
number the information came from, so it is in-
name it 'Neuropsychological Assessment'. Refer to the
cluded/printed in further referrals or copy files eg.
system steps below for further guidance.
Medical records and reports from claim:
Manage document groups
100XXXXXXXX
NOTE What documents need to be included?
Do not create a bulk print on one claim and then
• A recent medical certificate
move it to another claim, renaming it and using it
• ACC6300 or ACC6300D Authority to Collect
in a referral for advice as it will not appear in any
medical and other Records. NOTE: If verbal con-
file copy subsequently used.
sent was provided note this is in the task eform
for Recovery Admin
Manage document groups
• Any clinical advisor comments
d At Recovery Plan level, select Add Activity and select
• Relevant clinical notes
NGCM - Manage Referral task.
• Any relevant reports, ie medical, psychological,
counselling reports
Creating Manage Referral Tasks - System Steps
NOTE What information do you need to include in
Refer to the Neuropsychological assessment
the task/e-form?
referral page below for more information
Refer to the ‘Manage Referral Task Templates
PROCESS Neuropsychological Assess-
document’
ment Referrals Service Page
Manage Referral Task Templates
NOTE What if you don't have the information to
complete the referral?
NOTE What are the NP104 Standard questions to be
included?
Request the information needed.
a. Provide a summary of injury and medical his-
PROCESS Request Clinical Records
tory as well as all other personal history of relev-
b Perform privacy checks on documents.
ance
b. Fully assess cognitive and psychological/
Privacy Check Before Disclosing Information Policy
affective functioning, incorporating named meas-
NOTE What do you need to check?
ures of performance and symptom validity
Check documents:
c. Provide a detailed, balanced clinical opinion
• are relevant to the referral
on causation of any cognitive or psychological
• do not contain any third party information
symptoms/difficulties identified, including discus-
• do not contain any other information that needs
sion of injury versus non-injury factors
to be withheld.
d. Provide your opinion on whether or not there
is/are any residual cognitive or other difficulty/ies
For details on what checks you need to complete
related to the index event and the functional
before sending documents out, refer to NG SUP-
impact/s of those difficulties
PORTING INFORMATION Inbound and Out-
e. Provide your recommendations for any addi-
bound Document Checks.
tional assessment/s required
f. Provide your recommendations for ongoing
NG SUPPORTING INFORMATION Inbound and
input required and the appropriate avenues for
Outbound Document Checks
accessing this
ACC > Claims Management > Manage Claims > Manage Treatment Interventions / Supports > Assess and Arrange Neuropsychological Assessment
Uncontrolled Copy Only : Version 28.0 : Last Edited Monday, 9 January 2023 10:33 AM : Printed Thursday, 1 June 2023 7:19 AM
Page 3 of 6
GOV-025316 Appendix 1
NOTE How do you refer a task to Recovery
Administration?
5.0 Review task
Refer to Referring Tasks to Recovery Adminis-
Recovery Administrator
tration - Principles for further information and
a Following the task assignment in Salesforce, navigate to
guidance.
Eos and select 'Do Task' from your task queue.
Contracted Suppliers by Geographic Area of Cov-
b Review the tasks to ensure it has the required infor-
erage
mation to complete the referral form
Service Contracts and Contracted Providers - MFP
NOTE What if you don't have all the information you
spreadsheet
need
Referring Tasks to Recovery Administration - Prin-
If required information is missing from the task,
ciples
or you need guidance on working within the
NOTE What do you do if Mental Injury Claim Infor-
Administration Team, refer to the link below
mation needs to be sent with a referral from a
NG PRINCIPLES Working in the Administration
Physical Injury Claim?
Team
In Eos, manually transfer the Referral Task gen-
erated to the Recovery Administration depart-
ment with the Sensitive Claims Administrator
6.0 Confirm availability of provider
Role.
Recovery Administrator
If Complex Mental Injury reports need to be sent
with the referral and there is an open claim, the
a Identify and select the vendor as specified in the task.
Recovery Partner can be contacted directly to ar-
NOTE What if no vendor is specified in the task?
range this. If there is not an open claim, you will
Refer to Client Admin - Finding Providers System
need to send a task through to the Partnered
Steps
Recovery queue for allocation to a Recovery
Partner who can help.
Client Admin - Finding Providers System Steps
NOTE What if your client has a Care indicator?
Contracted Suppliers by Geographic Area of Cov-
You need to clearly outline this in the e-form.
erage
b Add the vendor as a participant on the claim.
Refer to the ‘Disclosure of care indicator infor-
mation to third parties’ policy below for more
Add a participant
information on how information is disclosed.
Disclosure of Care Indicator Information to Third Par-
7.0 Create purchase order
ties Policy
Recovery Administrator
NOTE What if the request is urgent and needs to be
a In Eos, generate a purchase order for the specified refer-
completed that day?
ral. Refer to the document below to confirm what infor-
• Call Recovery Administration
mation is needed for the purchase order.
• Give the Recovery Administrator who answers
the call the claim number
Creating purchase orders using general + QE
• The Recovery Administrator will open the claim
Purchase Order - Handy Hints on how to create and
in Eos and find the task on the claim
edit POs
• Transfer the task into the Recovery Admin-
istrator's name. This will move it to their personal
Purchase Order Details - Neuropsychological
Eos queue and stop it from being reallocated by
Assessment.docx
Salesforce.
NOTE What if a vendor has not been specified?
NOTE What if the request is required in the future?
If no vendor has been specified, select an appro-
If the request is required in the future, set a re-
priate contracted vendor for the referral type and
minder task for the future date when the service
client's geographic area.
will be required. When the reminder task comes
Manage Participants (Eos Online Help)
up send a task to Recovery Administration to
continue with the process. Consider the contract
b Approve the purchase order.
timeframes and SLAs as specified in the service
NOTE What if the purchase order requires a higher
page
delegation?
NOTE What are the SLAs?
Save the purchase order. Create and send a Re-
The referral tasks route to the Recovery Adminis-
quest Authorisation task to a Recovery Leader
tration team with an SLA of 24 hours.
for a purchase order approval.
NOTE What if you need to seek vendor availability?
Refer to the link below.
Within the task, note if applicable:
• Availability for telehealth or preference for face
Request Authorisation for a Purchase Order -
sessions, or openness to both
System Steps
• How far can the client travel
• Provider gender preference
• Additional provider skills, specialties or expe-
8.0 Create and send referral documents
riences? (EDMR/CBT, paediatrics, experience
Recovery Administrator
with prisoners)
a Create the referral for a Neuropsychological assessment
Advise in task if you require Admin to advise of
documents: ACC110 referral to the Vendor and the
positive Vendor responses, prior to sending
NPS01 Referral to the client.
referral to next best available Vendor.
ACC > Claims Management > Manage Claims > Manage Treatment Interventions / Supports > Assess and Arrange Neuropsychological Assessment
Uncontrolled Copy Only : Version 28.0 : Last Edited Monday, 9 January 2023 10:33 AM : Printed Thursday, 1 June 2023 7:19 AM
Page 4 of 6
GOV-025316 Appendix 1
b Populate the ACC110 with information noted on the refer-
j In Salesforce, close the assigned referral task.
ral task and include the NP104 standard questions.
Ensure you have checked that all the relevant information
within the task has been captured.
9.0 Receive and review Assessment Report
Admin Template - ACC110 Neuropsychological
Recovery Assistant, Recovery Coordinator, Recovery
Assessment Referral - vendor
Partner
Admin Template - NPS01 Neuropsychological
a Review the Neuropsychological Assessment report
assessment - Client
(NP104).
c Complete the document (to convert the document into a
NOTE What should you be checking in the report?
non-editable pdf).
Check the following:
• All sections of the report are completed
d Link the referral document to the document group already
• Injury, client and Provider details are correct
created.
• Diagnoses (if relevant) are clearly stated
e Perform privacy checks using Inbound and Outbound
• An explanation for the development of the
Document Checks.
symptoms and the causal link to the injury event
• There are clear, logical and practical treatment
NG SUPPORTING INFORMATION Inbound and
recommendations
Outbound Document Checks
NOTE What if the client fails to attend and/or partic-
NOTE What if the document group contains an old
ipate in the Neuropsychological Assess-
e-form?
ment?
Convert the e-form to PDF so it can be emailed
If the client fails to attend or take part in the
by Eos.
assessment, you should find out why.
In some cases you may need to decline or stop
Refer to the System Steps link below for further
entitlements/supports.
information and guidance on how to convert an
PROCESS Manage Non-Compliance
e-form to PDF.
Convert an Internal Referral e-form to a PDF docu-
b Determine the next steps based on the recommendations
ment.
in the report.
NOTE What if the referral contains sensitive per-
NOTE When should you seek internal clinical guid-
sonal information?
ance?
If the referral contains unnecessary sensitive
If the following criteria are met, consider fol-
personal information, refer to NG PRINCIPLES
lowing the assessor's advice without seeking
Working in the Administration Team, for infor-
internal clinical comment:
mation and guidance on redactions, password
1. The client has cover for a moderate or severe
protecting documents and sending passwords to
traumatic brain injury (TBI), and
providers.
2. The neuropsychological assessor is not
recommending any additional covered injury, and
NG PRINCIPLES Working in the Administration
3. You do not have any concerns regarding the
Team
report's conclusions or recommendations.
Sending docs to providers.docx
If the following criteria are met, consider seeking
f Create an email to the provider using the Requests and
internal clinical advice from a Psychology Ad-
referrals template, attach the referral and document
visor via the hotline:
group and select the most appropriate email address
1. You are unsure regarding aspects of the
(commonly listed under General Purchasing).
conclusions or recommendations of the
NGCM - FINAL Emailing from Eos using a Template
neuropsychological assessment report, or
- System Steps
2. The neuropsychological assessor has raised
concerns regarding risk, issues or client vulne-
g Send the referral to the provider.
rability.
NOTE What if the provider requires the documents
to be sent via courier?
If the following criteria are met, consider seeking
internal clinical advice from a Psychology Ad-
Go to Prepare and Send Client Information by
visor via written guidance:
Courier process.
1. The client has a suspected or covered mild
PROCESS Prepare and Send Client Infor-
traumatic brain injury (concussion) sustained
mation by Courier
more than six months ago, and
h Check the client's preferred communication channel
2.The neuropsychological assessor has con-
(SMS, email, etc), and if the client has a safe contact (if
cluded that the client has injury-related cognitive
this has not been included in the referral task).
impairment, or
3. The neuropsychological assessor has sug-
NOTE How do I confirm if the client has a safe con-
gested that the client may be entitled to cover for
tact?
an additional condition (e.g. a mental injury).
Refer to the process below
View a safe contact (Eos Online Help)
Go to the Seek Internal Guidance process, if
clinical guidance is required.
i Send the NPS01 Neuropsychological Assessment refer-
PROCESS Seek Internal Guidance
ral letter to the client.
NOTE How do you send a notification to a client?
Refer to the system steps below.
Create a Notification - System Steps
ACC > Claims Management > Manage Claims > Manage Treatment Interventions / Supports > Assess and Arrange Neuropsychological Assessment
Uncontrolled Copy Only : Version 28.0 : Last Edited Monday, 9 January 2023 10:33 AM : Printed Thursday, 1 June 2023 7:19 AM
Page 5 of 6
GOV-025316 Appendix 1
NOTE What if you're considering suspending
entitlement(s)?
In cases of Complex Mental Injury/Traumatic
Brain Injury consider obtaining Psychology Ad-
visor and/or Medical Advisor guidance before
suspending entitlements. Refer to the ‘Seek
Internal Guidance’ process for details on how to
do this.
PROCESS Seek Internal Guidance
ACC > Claims Management > Manage Claims > Manage Treatment Interventions / Supports > Assess and Arrange Neuropsychological Assessment
Uncontrolled Copy Only : Version 28.0 : Last Edited Monday, 9 January 2023 10:33 AM : Printed Thursday, 1 June 2023 7:19 AM
Page 6 of 6

GOV-025316 Appendix 1
Neuropsychological Assessment Overview Service
Page v11.0
Summary
3.0 Service details
Neuropsychological assessments
Objective
https://go.promapp.com/accnz/Process/d50e5fb0-3457-4545-8cda-bc708e4ea6e1
The neuropsychological assessment service aims to:
Neuropsychological assessment referrals
https://go.promapp.com/accnz/Process/c276e516-2c20-41ff-8c6f-a6037163e6f7
• confirm the existence of traumatic brain injury (TBI) and deter-
mine how the client is affected by the TBI
• confirm whether the client’s symptoms have been caused by
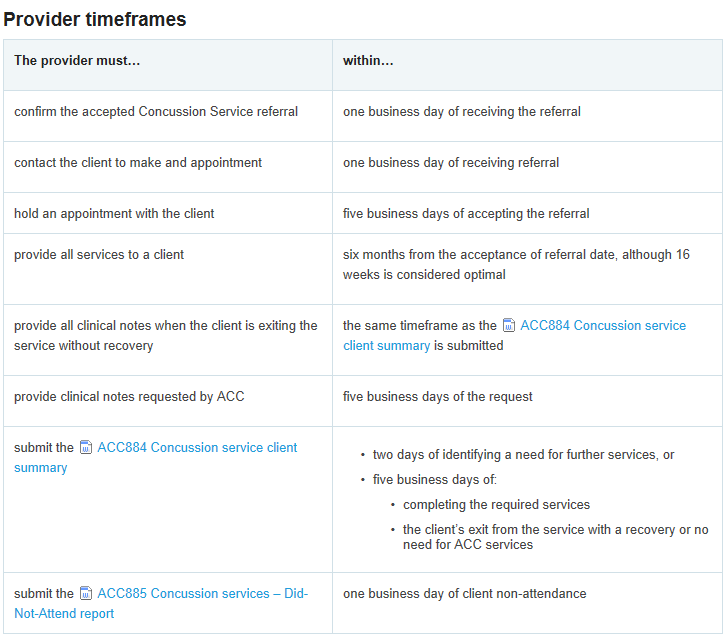
4.0 Timeframes
the injury or if there may be other possible causes
a The service provider must meet the timeframes shown
below. If they can’t meet any of the required timeframes
• provide recommendations for intervention, if appropriate.
they should advise the claims management staff member
within the same timeframe.
Assessments look at the client’s cognitive, behavioural and
emotional, and social and vocational functioning.
- The Supplier contacts the Client to arrange an appoint-
ment for an assessment within 5 Business Days of re-
[Out of Scope]
ceiving the referral
Owner
- The Service Provider initiates the Assessment within 15
Expert
Business Days of the Client being contacted
- Once the Assessment is initiated, the Service Provider
completes the Assessment within 15 Business Days
Procedure
- The Service Provider completes the Client Feedback
1.0 Who is this service for?
Session within 10 Business Days of completing the
assessment
a A client is eligible for a neuropsychological assessment
- The Neuropsychological Assessment Report is sent to
when they’ve suffered a covered personal injury for which
ACC within 15 Business Days of completing the Assess-
they have entitlement. See the AC Act 2001, Section 67
ment
for more information.
AC Act 2001, Section 67
https://www.westlaw.co.nz/maf/wlnz/app/authentication/signon?startChunk=1&redirect=%2Fmaf%2Fwlnz%2Fapp%2Fdocument%3Fsrc%3Drl%26docguid%3DI7f252f423b3e11e18eefa443f89988a0%26hitguid%3DI17001bd4e03011e08eefa443f89988a0%26snippets%3Dtrue%26startChunk%3D1%26endChunk%3D1%26isTocNav%3Dtrue%26tocDs%3DAUNZ_NZ_LEGCOMM_TOC%26extLink%3Dfalse&tocDs=AUNZ_NZ_LEGCOMM_TOC&hitguid=I17001bd4e03011e08eefa443f89988a0&src=rl&snippets=true&extLink=false&endChunk=1&isTocNav=true&docguid=I7f252f423b3e11e18eefa443f89988a0#anchor_I17001bd4e03011e08eefa443f89988a0
2.0 Qualifications
a The neuropsychological report must be signed by a
trained and ACC-contracted neuropsychology provider.
b Trainees
Trainee neuropsychologists may do a neuropsychological
assessment and report. Their supervising neuropsy-
chologist must be a named provider and ensure the trai-
nee meets the criteria in the contract.
If a neuropsychological provider doesn’t have the expe-
rience to be a named provider they can do the assess-
ment as long as they meet the following criteria:
• they’re a registered psychologist in NZ with a clinical
scope of practice
• they hold a current Annual Practising Certificate with the
NZ Psychologists Board
• they’re a current member of at least one of the fol-
lowing:
- NZPS Institute of Clinical Psychology
- NZ College of Clinical Psychologists
- an international Neuropsychological Society acceptable
to ACC
• they have successfully completed a university based
postgraduate course in clinical neuropsychology.
ACC > Claims Management > Manage Claims > Service Pages > Primary Care > Mental Health > Neuropsychological assessment > Neuropsychological Assessment Overview
Service Page
Uncontrolled Copy Only : Version 11.0 : Last Edited Wednesday, 20 July 2022 3:59 PM : Printed Thursday, 1 June 2023 7:20 AM
Page 1 of 1

GOV-025316 Appendix 1
Neuropsychological Assessment Referrals Service
Page v15.0
Summary
Neuropsychological Assessment Overview Service
Page
Objective
b Additional Considerations in Assessments of Children/
Guidelines for Making Neuropsychological Assessment Refer-
Adolescents:
rals (NP104)
Case owners can refer for neuropsychological assess-
Owner
[Out of Scope]
ment when clients (or parents/guardians) are concerned
about cognitive, behavioural and/or emotional difficulties
Expert
that are impacting on recovery and/or return to school
and/or where the provider has recommended the assess-
Procedure
ment.
1.0 About referrals
The neuropsychological assessment with children/
a
adolescents aims to:
• There needs to be a clear and valid reason for referring
for a neuropsychological assessment as these assess-
a) Confirm the existence of traumatic brain injury (TBI)
ments are time consuming for clients and relatively costly
and determine how the client is affected by the TBI.
for ACC.
b) Clarify the possible role of brain injury related cognitive
difficulties in presenting behavioural and/or emotional
• Where case owners have established that a neuropsy-
concerns.
chological assessment is necessary and appropriate for a
c) Provide a re-assessment to track recovery/ cognitive
client with cover for traumatic brain injury, there is no
development
need to refer for Psychology Advisor (PA) comment prior
d) Provide recommendations for intervention (or any
to making the referral. Standard questions/requests are
changes in the existing rehabilitation plans), if appro-
suggested below, under 'Making the referral' (4.0). In
priate.
practice, most experienced neuropsychological asses-
sors are familiar with the areas that need to be assessed.
• If cover for traumatic brain injury has not yet been
2.0 Choosing a provider
established, and a neuropsychological assessment has
a Approved neuropsychological assessment providers can
been recommended as part of the cover investigations,
be found on the list linked below.
psychology advice should be sought via the PA Hotline in
the first instance.
Contracted Suppliers by Geographic Area of Cov-
erage
• For clients who have sustained moderate to severe
traumatic brain injuries, referral for a neuropsychological
assessment would usually occur no sooner than six
3.0 Service location
months’ post-injury. The aim is to identify those longer-
a Assessment venues are specified in the individual pro-
term enduring cognitive, behavioural and emotional diffi-
vider’s contract. Alternative venues may be used with the
culties which need targeting in rehabilitation. However,
prior approval of the case owner.
there may be times when an assessment may occur ear-
lier than six months’ post-injury, such as when a client
• If the case owner asks the provider to assess a client in
has made a rapid recovery and wants to return to
a different location from the provider’s usual place of
employment.
practice, the provider may invoice ACC for travel time,
kilometres travelled, and the cost of room hire, as set out
• While there is no need to involve a Psychology Advisor
in the contract in Part A, Clause 4
when considering a first neuropsychological assessment,
Psychology Advisors should be consulted via the Hotline
• You must direct clients to the nearest approved provider
when case owners are considering a neuropsychological
location. If a client needs to travel to the appointment,
re-assessment, to ensure that the timing is appropriate.
see Non-emergency transport for guidelines on reim-
bursing for travel.
• If a referral is made directly to the service provider, ie
not by the case owner, the provider must get the case
owner’s approval owner before starting any part of the
assessment.
• We do not pay a provider if they don’t have prior ap-
proval.
• All referrals must be in writing.
• The assessment must be arranged and carried out
within expected timeframes. Refer to Neuropsychological
Assessment Overview Service Page (1.0 Who is this ser-
vice for? and 4.0 Timeframes).
Neuropsychological Assessment Overview Service
Page
Psychology Advisors (PAs) Team Space
ACC > Claims Management > Manage Claims > Service Pages > Primary Care > Mental Health > Neuropsychological assessment > Neuropsychological Assessment Referrals
Service Page
Uncontrolled Copy Only : Version 15.0 : Last Edited Wednesday, 20 July 2022 3:59 PM : Printed Thursday, 1 June 2023 7:20 AM
Page 1 of 3
GOV-025316 Appendix 1
NOTE When can Telehealth be used to provide ser-
4.0 Making the referral
vices?
a The case owner sends the referral document (ACC110)
Services can be delivered by Telehealth, where
to the contracted service provider, along with all relevant
clinically appropriate. Telehealth Services must:
information, such as GP notes, hospital records including:
- have client or authorised representative con-
ambulance records, hospital admission report/s, any daily
sent (recorded in the clinical notes), and with the
hospital progress notes (usually hand-written records)
option of an in-person meeting if the client pre-
when available, hospital discharge report/s, imaging (CTI
fers
MRI scan) findings, rehabilitation progress reports,
- be preceded by an initial risk assessment to
Concussion Clinic notes, counselling, psychological and
ensure client safety
psychiatric assessment and intervention/treatment re-
- meet the same required standards of care pro-
ports, vocational and other medical reports. Relevant pre-
vided through an in-person consultation
injury GP/mental health notes for a period of 2 years pre-
- have clinical records that meet ACC and
dating the head injury up to present should be accessed
professional body requirements
and included with the neuropsychology assessment
- meet the requirements outlined in the stan-
referral.
dards/guidelines of the New Zealand Psychol-
ogist's Board
Note: GP notes should include mental health concerns
- If there is a difference between the regulatory
(e.g. symptoms of low mood, depression, anxiety,
body statements and what is stated in this con-
trauma, stress, and other non-specific symptoms such as
tract, then the contract conditions take prece-
headache, fatigue), head injuries/brain injuries, persis-
dence
tent/chronic pain and unexplained medical symptoms.
- have both the client receiving the Telehealth
Internal clinical guidance transcripts related to the head
service, and the provider delivering the Tele-
injury should also be sent, along with a summary of other
health service, physically present in New Zeal-
head/brain injury/concussion, mental injury, and sensitive
and at the time the service is provided.
claims and relevant records for those claims. It is impor-
tant to obtain client consent to share the sensitive claim
The 'Alias Code' for Telehealth Services is
information.
NP104T
• Provide the reason for referral so that the provider
knows exactly why the referral is being made. If there are
complexities present, please outline what these are. It is
important that the assessor has a comprehensive under-
standing of the client and any risks/complexities which
are present. Risks include risk of harm to the client or
other people (such as providers), such as aggressive
behaviour. Complexities might include multiple head
injury claims associated with persisting impairment, the
presence of mental injury, or claims with a history of
external reviews.
• There is one purchase order code – NP104. The max-
imum of 16 hours should be entered in the purchase
order as the neuropsychologist only bills for the number
of hours actually used.
• Please see below suggested questions and areas of
focus for neuropsychological assessments for both adults
and young people. It is important to look carefully at the
areas of focus to determine whether they are relevant for
the client in question and to establish whether any further
information is required from the assessor.
•All neuropsychological assessment reports need to be
reviewed by the Psychology Advisors.
NOTE What if you need to request medical or clin-
ical records
Go to Request Clinical Records process
PROCESS Request Clinical Records
ACC110 Neuropsychological assessment referral –
vendor
b Send NPS01 to the client to advise that the provider will
be in contact.
NPS01 Neuropsychological assessment request -
claimant letter
ACC > Claims Management > Manage Claims > Service Pages > Primary Care > Mental Health > Neuropsychological assessment > Neuropsychological Assessment Referrals
Service Page
Uncontrolled Copy Only : Version 15.0 : Last Edited Wednesday, 20 July 2022 3:59 PM : Printed Thursday, 1 June 2023 7:20 AM
Page 2 of 3
GOV-025316 Appendix 1
c Areas of Focus to include in Neuropsychological Refer-
rals:
Case owners can request that providers carry out a
neuropsychological assessment incorporating the fol-
lowing requests:
a) Provide a summary of injury and medical history as
well as all other personal history of relevance
b) Fully assess cognitive and psychological/affective
functioning, incorporating named measures of perfor-
mance and symptom validity
c) Provide a detailed, balanced clinical opinion on cau-
sation of any cognitive or psychological symptoms/
difficulties identified, including discussion of injury versus
non-injury factors
d) Opinion on whether or not there is/are any residual
cognitive or other difficulty/ies related to the index event
and the functional impact/s of those difficulties
e) Provide your recommendations for any additional
assessment/s required
f) Provide your recommendations for ongoing input re-
quired and the appropriate avenues for accessing this
PROCESS
Assess and Arrange Neuropsy-
chological Assessment
ACC > Claims Management > Manage Claims > Service Pages > Primary Care > Mental Health > Neuropsychological assessment > Neuropsychological Assessment Referrals
Service Page
Uncontrolled Copy Only : Version 15.0 : Last Edited Wednesday, 20 July 2022 3:59 PM : Printed Thursday, 1 June 2023 7:20 AM
Page 3 of 3

GOV-025316 Appendix 1
Concussion Service Assessments Service Page v20.0
b
Summary
Where clients are assessed as needing more services
that are available under the concussion services, a refer-
ral to Training for Independence - Traumatic Brain Injury
Objective
(TI-TBI) should be made as early as possible. In this situ-
The Concussion Service is flexible service and can be adapted
ation, please keep the following in mind:
to client needs.
• Clients who have been identified as having more com-
The provider will assess and triage the client to determine their
plex needs should be discharged from the Concussion
rehabilitation needs. In consultation with the client, the provider
Service and referred to other services such as: Clinical
and ACC will agree on the appropriate services for the client’s
Services, Neuropsychology contract, Training for
rehabilitation.
Independence (TBI) or other appropriate services. Pro-
viders will notify ACC of this decision via the ACC884
[Out of Scope]
Client Summary Form.
Owner
Expert
• Providers should only recommend that a client stay in
the Concussion Service if they feel they can achieve an
outcome within the maximum funding limit. If during the
Procedure
assessment phase the providers feel that the clients
1.0 Case Reviews
needs are too complex to be able to achieve an outcome
within this service they should be discharging client out of
a All clients who are referred to the Concussion Service
the Concussion Service at that time and no further treat-
must receive the following services:
ment and rehabilitation should be undertaken or invoiced
• Education about Concussion
for under the Concussion Service.
• A case review by a medical specialist
• A case review by a clinical neuropsychologist.
• Where a recommendation has been made for a client to
exit the concussion service and be referred for a Training
The case reviews allow the medical specialist and the
for Independence program, no further treatment should
neuropsychologist to conduct a preliminary review of the
be invoiced for under the Concussion Contract. The only
client’s clinical history, any risks that may hinder the
exception to this is if the client still requires a Neuropsy-
client’s recovery, and to determine whether they need to
chological Screen. In this instance, the Concussion sup-
see the client face to face. (The case reviews may be
plier can keep the client’s file open until the screen has
conducted soley on the referral documentation provided)
been completed then invoice for the Neuropsychological
and a decision could be made to:
Screen (TBI23) accordingly.
• confirm diagnosis and recommend further assessment
and treatment within the concussion service
• decline the client
3.0 Clinical History
• recommend the client be referred to other services
• other recommendations which the provider will discuss
a The service item ‘Education and assessment’ (TBI21 or
with the case owner.
TBI31) requires the provider to gather both clinical and
the psycho-social background of the client. It is important
that the provider collects all information about the client
2.0 Assessment of therapy needs
that may be relevant to their rehabilitation and recovery,
including:
a The client’s needs should be assessed throughout the
rehabilitation. Clinical assessments are completed by
• GP clinical notes, specifically about prior brain injuries
professionals working in their scope of practice and
and other health issues such as depression, mental ill-
within the interdisciplinary team.
ness etc up to five years previous
• any clinical notes from Te Whatu Ora District hospitals
(previously DHBs) acute services such as emergency
department, wards etc
• work or education information, to help assess the cog-
nitive demands on the client throughout the recovery
• family composition and responsibilities, to help assess
any stressors that may hinder recover and where ACC
may need to provide supports
• social background, to identify any underlying social
issues that may hinder recovery
ACC > Claims Management > Manage Claims > Service Pages > Specialist Care and Rehabilitation > Specialist Rehabilitation and Disability Services > Concussion Service >
Concussion Service Assessments Service Page
Uncontrolled Copy Only : Version 20.0 : Last Edited Friday, 29 July 2022 4:26 PM : Printed Thursday, 1 June 2023 7:18 AM
Page 1 of 3

GOV-025316 Appendix 1
4.0 Requesting Clinical notes from GPs and DHBs
7.0 Rehabilitation planning
a The provider can pay and reclaim from ACC costs asso-
a The supplier’s interdisciplinary team will develop a
ciated with the obtaining of the clinical notes using COPY.
rehabilitation plan that describes client’s goals (ex-
The maximum is $30.
pressed as SMART goals) and the therapy required to
meet those goals.
When a Concussion Service provider:
ACC and the provider will finalise and agree service
• is a DHB and they obtain up to 5 years of GP client
composition and timeliness. The plan may be adapted as
notes and are billed by the GP they can be reimbursed by
new information comes to hand.
ACC billing COPY
• is a DHB and they review up to 5 years of DHB notes
they can cannot bill ACC as they have not incurred a
cost, unless a copy of those notes are requested by ACC
8.0 Risks to Recovery
as which point ACC will pay the normal changes.
a The risk to recovery assessment is described in the
• is not a DHB and they obtain up to 5 years of GP client
Concussion Service Operational Guidelines. It is a
notes and are billed by the GP they can be reimbursed by
communication tool used by suppliers to indicate to ACC
ACC billing COPY obtains client notes but is not billed the
any barriers or hindrances the client may be facing in
provider cannot seek reimbursement.
their rehabilitation and recovery.
• obtains client notes but is not billed the provider cannot
The matrix describes the client’s risks in four main cate-
seek reimbursement.
gories:
• physical
• psychological
• social
5.0 Assessment
• work (including study and activities requiring an in-
creased cognitive function).
a The supplier will submit the ACC884 Concussion service
client summary form when all the assessments are com-
The matrix rates those risks based on their potential
pleted and will make recommendations on the way for-
impact on the client’s recovery:
ward. Prior to this the case owner can expect to be kept
updated on the client’s progress where appropriate via
• 1 – No/Low Risks
email and phone.
• 2 – Low-Medium
b
• 3 – Medium
When the Assessment, Education and Triage stage has
• 4 – Medium/High
been completed and if the Supplier requests further ser-
• 5 - High.
vices via the ACC884 - The purchase order will need to
be updated. See table below
The risk to recovery assessment is an important part of
the triage process and can help to determine whether the
client’s rehabilitation and service needs can be met within
the funding limit of the Concussion Service.
Refer to the Concussion Service Operational Guidelines
on the TBI Contracted Providers page for full detail on the
risk assessment.
9.0 Triage
a The Concussion service has a strong triage focus and a
full interdisciplinary team using all available information
will determine the suitability of the service for the client.
b If the client:
• has recovered and no longer requires treatment, or
• has needs greater than what the Concussion Service
can provide
Treatment and Rehabilitation (services as appro-
priate to meet the injury related needs of the
the provider will recommend the client exits from the ser-
client).PNG
vice
6.0 Completion Report
a The provider will keep in contact with the case owner
c If the client has needs that can be met within the scope of
throughout the rehabilitation programme by phone or
the Concussion Service, either by itself or alongside
email. They will notify ACC formally using the ACC884
other services, the provider will recommend the client
Concussion service client summary form when the
continues with the service and suggest appropriate ser-
client’s rehabilitation is complete. This may include
vices
recommendations for further services.
ACC > Claims Management > Manage Claims > Service Pages > Specialist Care and Rehabilitation > Specialist Rehabilitation and Disability Services > Concussion Service >
Concussion Service Assessments Service Page
Uncontrolled Copy Only : Version 20.0 : Last Edited Friday, 29 July 2022 4:26 PM : Printed Thursday, 1 June 2023 7:18 AM
Page 2 of 3
GOV-025316 Appendix 1
10.0 Triage and Planning Report
a The key worker will keep in contact with the case owner
throughout the rehabilitation programme by phone or
email. They will notify ACC formally using the ACC884
Concussion Service Client Summary form when the
triage recommendation and rehabilitation plan has been
finalised by the interdisciplinary team.
ACC884 Concussion service client summary
ACC > Claims Management > Manage Claims > Service Pages > Specialist Care and Rehabilitation > Specialist Rehabilitation and Disability Services > Concussion Service >
Concussion Service Assessments Service Page
Uncontrolled Copy Only : Version 20.0 : Last Edited Friday, 29 July 2022 4:26 PM : Printed Thursday, 1 June 2023 7:18 AM
Page 3 of 3

GOV-025316 Appendix 1
Concussion Services Service Page v36.0
c
Summary
The IDT is co-ordinated by a key worker to ensure that
the service is flexible to meet the individual needs of the
client.
Objective
• The concussion service is capped at $3,551.98 (GST
The Concussion Service is a clinical assessment and rehabil-
exclusive).
itation service for clients with a mild to moderate traumatic brain
• The maximum timeframe for treatment within the
injury (TBI). The service is delivered by an interdisciplinary team
Concussion Service is 6 months. Ideally clients should be
of professionals specialised in the diagnosis and rehabilitation
complete treatment and rehabilitation within 16 weeks of
of TBI. The service aims to prevent long-term consequences,
referral.
such as persisting concussion symptoms, by identifying clients
• Clients who have more complex needs should be re-
at risk and delivering effective assessments, education, triage
ferred to other services such as: the clinical services con-
and rehabilitation.
tract, neuropsychology contract, Training for Indepen-
dence (TBI) or other appropriate services.
[Out of Scope]
Owner
• Providers should only recommend that a client stay in
Expert
the Concussion Service if they feel they can achieve an
outcome within the maximum funding limit. If during the
assessment phase the providers feel that the clients
Procedure
needs are too complex to be able to achieve an outcome
1.0 Who is this service for?
within this service they should be discharging client out of
the Concussion Service at that time and no further treat-
a Clients who have been diagnosed with a mild to mod-
ment and rehabilitation should be undertaken or invoiced
erate traumatic brain injury, or are suspected of having a
for under the Concussion Service.
brain injury that needs investigation. The Concussion
Service deals with:
• Where a recommendation has been made for a client to
exit the concussion service and be referred for a Training
• mild to moderate traumatic brain injury (TBI)
for Independence program, no further treatment should
• persisting concussion symptoms (PCS).
be invoiced for under the Concussion contract. The only
exception to this is if the client still requires a Neuropsy-
chological Screen. In this instance, the Concussion sup-
2.0 Key features
plier can keep the client’s file open until the screen has
been completed then invoice for the Neuropsychological
a The purpose of the Concussion Service is to:
Screen (TBI23) accordingly.
• Confirm a diagnosis of concussion or rule out diagnosis
of concussion
d Services are delivered up to a maximum spend of
• Support the Client’s recovery and prompt return to
$3,551.98 (GST exclusive).
every-day life including work or school
e Clients who require more services than are available
• Reduce the incidence of further brain injury, and long
under the Concussion Service are referred to other ser-
term consequences, such as persisting concussion
vices as recommended by the Supplier on the ACC884.
symptoms by providing clients with education and effec-
tive interventions
The Concussion Service is delivered by an interdis-
ciplinary team (IDT). The core IDT is made up of a:
• Medical Specialist
• Neuropsychologist
• Occupational Therapist
• Physiotherapist
b The IDT may also include a:
• Nurse
• GP
• Speech Language Therapist
• Psychologist
• Social Worker
• Optometrist
ACC > Claims Management > Manage Claims > Service Pages > Specialist Care and Rehabilitation > Specialist Rehabilitation and Disability Services > Concussion Service >
Concussion Services Service Page
Uncontrolled Copy Only : Version 36.0 : Last Edited Monday, January 23, 2023 1:03 PM : Printed Thursday, 1 June 2023 7:18 AM
Page 1 of 4
GOV-025316 Appendix 1
3.0 Eligibility for Concussion Services
c The referral should be completed using the ACC883
a
Concussion Service Referral form:
To be referred to the Concussion Service, the Client must
• GP’s and UCCs can send the ACC883 to either ACC or
meet all the following criteria:
directly to the Concussion Supplier.
• Have sustained a TBI (or suspected TBI) within the pre-
Te Whatu Ora (Health NZ) District Hospitals can continue
vious 12 months
to use the ACC883 but it is preferred that they use the
• Have an accepted ACC claim, and
ACC7988.
• Be diagnosed with or be suspected of having a mild
• If sent to ACC – the Recovery Team Member will ap-
TBI, moderate TBI or persisting concussion symptoms
prove the service if appropriate and forward the referral
document to a Concussion Supplier.
AND Have at least one of the following on-going signs
and symptoms:
Te Whatu Ora (Health NZ) District Hospitals can send the
• Mood changes
ACC7988 directly to the Concussion Supplier. ACC will
• Memory problems
be cc’d in to this referral for our records.
• Fatigue
If a provider is unable to accept a referral, they will notify
• Difficulty concentrating
ACC, and ACC is to select and refer to another provider
• Loss of balance
using the current process.
• Headaches
• Visual disturbances
• ACC led referrals can be sent straight to the Concus-
• Nausea
sion Supplier. Recovery Team Members will need to gen-
• Muscular aches
erate the ACC883 in EOS and fill it in with as much claim
• Dizziness
details as possible. The ACC883 will then need to be in-
cluded as part of the relevant document group prior to the
AND have at least one of the additional risk factors such
referral task being sent to Recovery Admin to process.
as:
• The inability to work or attend school for more than one
week
ACC883 Concussion service referral
• Second or subsequent MTBI within 6 months
d For continuity of service, clients should be referred to the
• Post traumatic amnesia lasting more than 12 hours
Supplier named in the referral information unless there is
• A requirement to operate machinery or drive at work
a reason to refer the client to a different Supplier, such
• A pre-existing psychiatric disorder or substance abuse
as:
problem
• a clinical reason the client should be referred elsewhere
• A high functioning job such as engineer, medical practi-
• to avoid clients having to undertake unnecessary travel
tioner or lawyer
• the client chooses a particular supplier
• Currently attending secondary or tertiary education
• there is another reason that ACC makes in the best
b A client is ‘likely’ to have received a TBI if the mechanism
interests of the client
of injury indicates that the head and brain has been
e Referrals for children and adolescents into the Concus-
moving and then stopped rapidly, eg as a result of a
sion Services are made on an ACC7412 which is equiv-
motor vehicle crash, sports injury or fall from a bike and
alent to the ACC883 adult referral form. Prior to sending
hitting the ground hard
a referral for children and adolescents, a phone call
c If the accident occurred more than 12 months ago, the
should be made to the Supplier to check that the Supplier
concussion service should be declined, and other ser-
has expertise to provide services to a Child or Adoles-
vices should be considered.
cent.
f Referrals cannot be sent from other clinical professionals
(such as a physiotherapist in the community). They may,
4.0 Referrals into the Concussion Service
however, refer a Client to a registered Medical Practi-
a The referrer must only refer Clients who meet the eligi-
tioner for a medical assessment, after which the Client
bility criteria. The Supplier should decline any referral that
may be referred to the Concussion service.
does not meet these criteria.
g Clients cannot self-refer into this service.
b Referrals can come from the following:
• Te Whatu Ora (Health NZ) hospitals – via a Medical
Practitioner or an Allied Health professional acting on
5.0 Assessment and Triage of Client
behalf of a Medical Professional
a The assessment component of this service covers inves-
• General Practitioner (GP) or Accident and Medical (A &
tigation of the presenting symptoms, diagnosis and treat-
M)
ment as follows:
• ACC – via a Recovery Team Member
• education about mild to moderate traumatic brain injury
• Note: No prior approval is required for the Assessment
to the client
and Triage stage (until 30 June 2023).
• identify and assess the client’s risks to recovery
• all clients undergo a case review by a Medical Spe-
cialist and Neuropsychologist to assess the need for full
assessments (this is a file review of all relevant clinical
notes)
• investigation of the clinical and psycho-social back-
ground of the client
• confirmation of the diagnosis where unconfirmed
• assessment of the client’s therapy needs
• development of a rehabilitation plan
• development of the client summary report
• referral to other services if needed
.
ACC > Claims Management > Manage Claims > Service Pages > Specialist Care and Rehabilitation > Specialist Rehabilitation and Disability Services > Concussion Service >
Concussion Services Service Page
Uncontrolled Copy Only : Version 36.0 : Last Edited Monday, January 23, 2023 1:03 PM : Printed Thursday, 1 June 2023 7:18 AM
Page 2 of 4
GOV-025316 Appendix 1
b Phone triage: If a Service Provider after a phone call to
9.0 Provision of Concussion Services to Children
the client determines the client doesn't need to enter the
a
concussion service, the supplier can charge the TBI05
Children and young people can recover from Concussion
code (no prior approval required).
and many children can be managed with treatment and
education and support to self-manage their symptoms.
However, some children who present with multiple ortho-
paedic injuries (eg from playing sport) or repeated head
6.0 Updating the client's diagnosis
injuries should be escalated to a full Neuropsychological
a When we don’t have a confirmed diagnosis the case
assessment – without any delay in referral process
owner must ask the provider to confirm the diagnosis
NOTE Definition of Children
during a medical assessment.
Children are defined here as 0-16 years, or still
at school. The provider will also take the client's
The provider is responsible for ensuring there is a con-
developmental stage into account - eg some 16
firmed diagnosis before therapy services are provided.
year olds may be independent and can be
b For example, Section 2 of the ACC883 asks the referrer:
treated in the same way as an adult. Other
What is the suspected or confirmed injury diagnosis? If
clients may be developmentally delayed and
the referrer writes their suspected diagnosis then the
remain at school longer.
Concussion Supplier will undertake an assessment of the
b Where a Clinical Neuropsychological assessment is
client to determine whether the Client has a diagnosis of
undertaken, consideration should be given to whether
Concussion.
additional time is needed as five hours may not be ade-
c At times, a GP might list an additional diagnosis of
quate when assessing children and young people.
Concussion onto a Medical Certificate stating that a client
c Where indicated by the Provider, children may require a
is not fit for work due to a concussion and there is no
longer period of time in the concussion service to allow
diagnosis listed on the ACC45. In addition, a Concussion
the provider to monitor and support the child or young
Supplier might also list an additional diagnosis of
person during the school term.
Concussion on a report to ACC where concussion has
not previously been listed on the ACC45.
d Before making the referral, always contact the Supplier
d
first to check they have the specialist skills in their team
In these instances, where a subsequent diagnosis of
to provide services to children.
Concussion has been made:
1) Check that that the diagnosis has been made by a
e You can also search for Concussion Service Providers
Medical Practitioner as only a Medical Specialist or GP
and whether they provide child and youth services using
can make a diagnosis of Concussion. This is because
the link below
only a Medical Professional (GP etc) can rule out (or con-
Concussion Service Providers
firm) the presence of any other medical conditions which
may be contributing to the Client’s symptoms.
https://www.acc.co.nz/for-providers/treatment-recovery/referring-to-rehabilitation/concussion-service-providers/
2) Request lodgement notes or clinical notes
3) Seek Clinical Advice
e
10.0 Timeframes
Follow the process for updating a client's diagnosis
a The service and stages must be completed within the ex-
Updating a Client's diagnosis process
pected timeframes.
https://go.promapp.com/accnz/Process/Minimode/Permalink/C5dzKYRy4qR26S0w7lTtea
f When we don’t have a confirmed diagnosis the case
owner must ask the provider to confirm the diagnosis
during a medical assessment.
The provider is responsible for ensuring there is a con-
firmed diagnosis before therapy services are provided.
7.0 Reimbursement of costs when requesting a
copy of client clinical notes
a Where a Provider provides up to 5 years of clinical notes
they can be reimbursed $1 per page up to a max of $30
by sending an invoice to ACC using the code COPY. A
purchase order is not required. ACC can provide a pur-
chase order if costs exceed $30.
Timeframes - Provider.PNG
8.0 Treatment and Rehabilitation
a Where the Client requires therapy following the assess-
ment stage, the Treatment and Rehabilitation should
cover:
• Providing advice on managing concussion symptoms
• Therapy to help the client manage emotional and
psychological issues
• Medical treatment for symptoms which may require
medication
Timeframes - Acc.PNG
• Notifying ACC of the outcome.
ACC > Claims Management > Manage Claims > Service Pages > Specialist Care and Rehabilitation > Specialist Rehabilitation and Disability Services > Concussion Service >
Concussion Services Service Page
Uncontrolled Copy Only : Version 36.0 : Last Edited Monday, January 23, 2023 1:03 PM : Printed Thursday, 1 June 2023 7:18 AM
Page 3 of 4
GOV-025316 Appendix 1
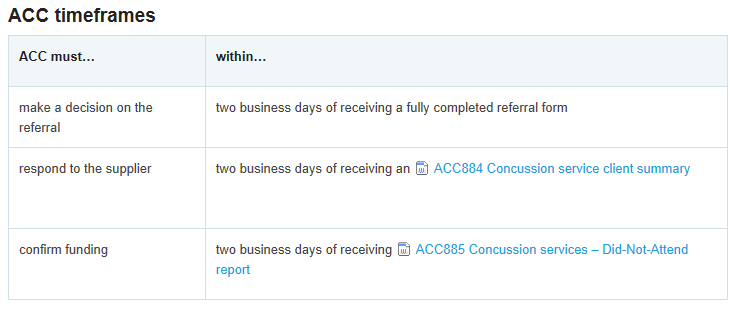
b If you are not able to make a decision to accept or de-
c Referrer responsibilities:
cline a claim within two days of receipt of the referral, you
1) Only refer clients who need and will benefit from the
must seek advice either from a case manager mentor,
Concussion Service. The client should have signs and
team manager, seek clinical advice, or go back to the
symptoms of mild to moderate TBI or persisting concus-
referrer and seek further information or clarification.
sion symptoms (PCS).
2) Complete and submit an ACC883 Concussion service
PROCESS
Concussion Service Assessments
referral form for approval. Please note: a Medical Practi-
Service Page
tioner or DHB may refer a client using other formats eg a
referral letter. This is acceptable if the information pro-
vided is similar standard to the information which would
be provided on an ACC883
11.0 Service details
d Client responsibilities
Concussion Service client non-attendance
https://go.promapp.com/accnz/Process/Minimode/Permalink/DDEFsER0Sno9EMtINEdcs7
The client is responsible for:
Concussion Service therapy
https://go.promapp.com/accnz/Process/1e3cd255-a3fb-415b-9f26-cf504fda7afe
• attending scheduled appointments or reorganising them
when unable to attend
Concussion Service assessments
• participating in the rehabilitation process
https://go.promapp.com/accnz/Process/17cb7c4c-fd72-404c-8198-db7ca325f534
• discussing any problems that may impact their recovery
with their case manager and provider.
Concussion service initial purchase order
https://go.promapp.com/accnz/Process/a722a895-ca69-4265-a5e9-d9c25188afea
ACC885 Concussion service - did not attend
ACC884 Concussion service client summary
12.0 Exclusions
a • Transport of the client to and from the clinic or place of
service
14.0 Measuring outcomes
• Provider travel to or from their residence to their place
a We consider the service successful when:
of business or the clinic
• Services provided under other entitlements such as:
• the client has returned to the usual activities of eve-
- inpatient services for traumatic brain injury (TBI)
ryday life and no longer needs any support from ACC for
- elective surgical treatment arising out of any assess-
their brain injury
ment
• services are provided in the shortest timeframe and at
- social rehabilitation assessments
the lowest cost, while still being clinically appropriate
- vocational rehabilitation services, where there is an
• clients are satisfied with the services provided.
identified need for long-term support
- long-term clinical psychological therapy
- comprehensive neuropsychological or neuropsychiatric
assessment and treatments
- radiological and other clinical investigations, eg: compu-
terised tomography (CT), magnetic resonance imaging
15.0 Completing the service
(MRI), electro-encephalogram (EEG), sleep studies.
a A client has completed the service when:
• they’ve returned to work and/or everyday life and no
longer need support from ACC for their brain injury
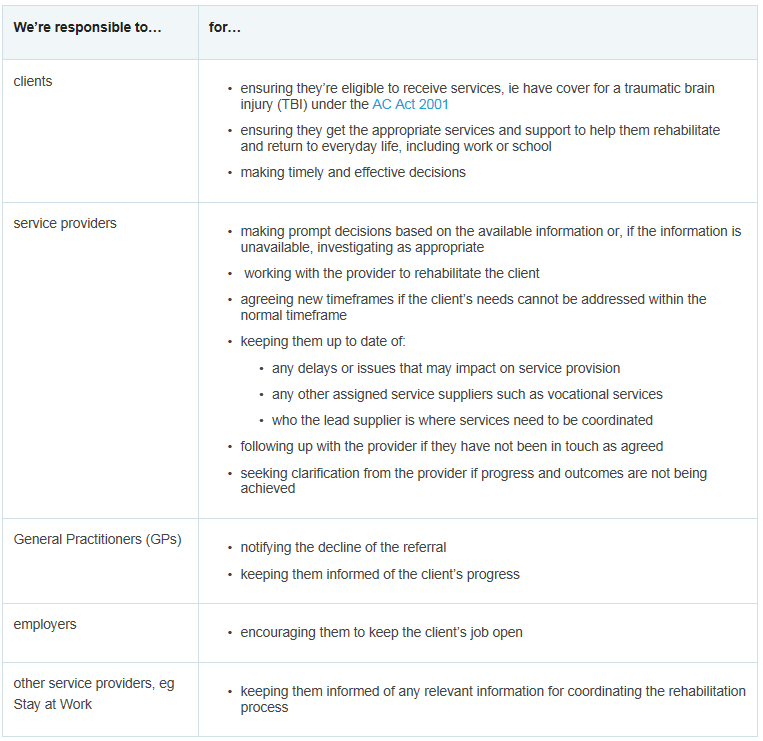
13.0 Responsibilities
• they’ve withdrawn from the service
• we’ve withdrawn the service from the client
a ACC responsibilities
• the maximum funding limit is reached
• they’ve received all approved services and no further
services have been approved
• Six months from the date of referral has passed.
ACC responsibilities.PNG
b Provider responsibilities
Provider responsibilities.docx
ACC > Claims Management > Manage Claims > Service Pages > Specialist Care and Rehabilitation > Specialist Rehabilitation and Disability Services > Concussion Service >
Concussion Services Service Page
Uncontrolled Copy Only : Version 36.0 : Last Edited Monday, January 23, 2023 1:03 PM : Printed Thursday, 1 June 2023 7:18 AM
Page 4 of 4

GOV-025316 Appendix 1
Training For Independence Services Service Page v25.0
Summary
1.2 What services are delivered under the TI con-
tract?
Objective
a Each of these services include flexible and tailored pro-
The Training for Independence (TI) and Training for Indepen-
grammes to meet the individual’s identified needs and
dence Advisory Service (TIAS) programmes provide education,
achieve specific outcomes in the required timeframes.
support, training, and rehabilitation to clients in the most appro-
b Types of services delivered under this contract:
priate setting for the client, eg their own home, community,
• education of the client and their family/whānau/carers
school, workplace, or remotely via telehealth where clinically
about the impact of the injury
appropriate.
• training and coaching, eg: energy conservation and how
to manage fatigue, behaviour, health, budgeting and hy-
The services are outcome focused and allow for providers to
giene.
tailor services to a client’s needs. The services aim to:
• developing social and communication skills, and estab-
•restore the client’s independence and ability to participate in
lishing social confidence
their wider community as much as possible
• identifying and managing any injury-related risks and
•reduce the client’s need for ongoing rehabilitation and support
teaching how to manage these risks safely, eg a person
services.
living alone may have rugs or electrical cords on the floor
• engaging the client with community-based activities and
Training and coaching can also be provided to the client’s family
teaching them skills to be able to access these activities
and carers where appropriate to assist the client with their
safely, appropriately and independently
rehabilitation goals.
• rebuilding a client’s confidence by increasing indepen-
dence with daily tasks, such as self cares, mobility,
[Out of Scope]
Owner
household management, childcare and transport
• promoting healthy choices about lifestyle, which may in-
Expert
clude education around drugs and alcohol, exercise and
nutrition.
Procedure
1.0 Who are these services for?
1.3 Training for Independence contracts (service
a The Training for Independence (TI) service is available to
schedules)
clients with a covered injury, such as a fractured hip, se-
a The five Training for Independence services each have a
rious brain injury, spinal injury, burns or mental injury who
separate service schedule (or contract) for each service.
require training and coaching to increase their level of
The Operational Guidelines covers all the TI services.
independence and who meet the eligibility criteria.
b TI - Adults with Traumatic Brain Injuries service schedule
Training for Independence - adults with traumatic
1.1 Eligibility criteria
brain injuries service schedule
a To access TI or Advisory programmes a client must:
NOTE Adults with TBI who are discharged from a
• have an accepted claim for cover
TBIRR facility
• have an assessed need for a TI service. The client’s
Please note: The TI-Adults with Traumatic Brain
needs may have been identified by:
Injuries contract enables TBIRR Suppliers to
• a social rehabilitation assessment or reassessment
refer to a TI-TBI provider without the need for ob-
• a medical report, eg an acute hospital admission dis-
taining ACC approval.
charge report, the ACC705 Referral for Support Services
c
on Discharge, the ACC706 - Early Notification of Com-
TI - Children and Young People service schedule
plex Case or General Practitioner’s report
Training for Independence - Children and Young
• a recommendation from another relevant assessment/
People Service schedule
service, eg Neuropsychological Assessment, Concussion
d
Service, Psychiatric Services, clinical psychologist report
TI - Adults with Sensitive Claims service schedule
etc.
Training for Independence - adults with Sensitive
• Recovery Team Members
Claims
• meet any additional eligibility criteria under each TI or
e
TIAS programme.
TI - Advisory Services service schedule
b If there is doubt about the need for TI, consider obtaining
Training for Independence Advisory Services - Ser-
a Social Rehabilitation Assessment to confirm.
vice Schedule
f TI - Adults with other injuries service schedule https://
See TI or TIAS programme selection for further eligibility
www.acc.co.nz/assets/contracts/tis-og.pdf
criteria and what to do if the client is not eligible for TI or
TIAS.
Training for Independence - Adults with other injuries
service schedule
TI or TIAS Programme Selection Service Page
c Referral into Training for Independence service
1.4 Training for Independence Operational Guide-
ACC2134 Training for independence referral
lines
ACC705 Referral for Support Services on Discharge
Training for Independence - Operational Guidelines
ACC706 - Early Notification of Complex Case
ACC > Claims Management > Manage Claims > Service Pages > Community and Independence > Community Rehabilitation Services > Training for Independence > Training
For Independence Services Service Page
Uncontrolled Copy Only : Version 25.0 : Last Edited Thursday, 27 October 2022 2:27 PM : Printed Thursday, 1 June 2023 7:19 AM
Page 1 of 2
GOV-025316 Appendix 1
2.0 Key Features
4.0 Related pages
a The two categories of Training for Independence services
Vocational Rehabilitation Services Overview (VOC)
are:
Service Page
• Training for Independence (TI) services. These services
Integrated Home and Community Support (IHCS)
meet client needs that include:
service
I. TI for children and young people
II. TI for adults with a traumatic brain injury
About the Managed Rehabilitation Equipment Ser-
III. TI for adults with sensitive claims
vices Service Page
IV. TI for adults with other injuries.
Concussion Service Assessments Service Page
Social Rehabilitation Assessment Service Page
Advisory Services which has two services types:
• Advisory Services Short Term programmes. This service
Neuropsychological Assessment Overview Service
is for clients who have needs that can be met in eight
Page
weeks and a maximum of six hours. It is to assist clients
Clinical Psychiatric Services Service Page
who have an injury but may require coaching and training
to restore their normal pre-injury level of confidence and
Other Social Rehabilitation
independence, eg an elderly client who has a fracture
neck of femur and has needs that can be met in six
weeks
• Advisory Services Long Term . These are for clients who
need support over an extended period of time. This ser-
vice can be used to maintain the client’s function or skills
and prevent secondary injury.
b Timeframe
Rehabilitation goals should be able to be achieved within
either three months (non-serious injury clients) or six
months (long term/serious injury clients).
c Gym memberships/Pool passes
We do not usually fund gym memberships as they are
considered the personal responsibility of a client. How-
ever, we may fund gym memberships alongside an ap-
proved TI or TIAS programme if the gym membership is:
• targeted to achieving a specific rehabilitation goal (eg
work conditioning which will result in a return to work, or
use of an injured limb which will result in a return to usual
daily activities)
• limited to a specific timeframe, with clear goals which
are reported on by the Provider
If approved, gym memberships/pool passes must be
funded outside of the TI contracts.
d Clients progress should be monitored throughout the TI
service to determine if the client is achieving their agreed
rehabilitation goals. If there is doubt about the need for
TI, consider obtaining a Social Rehabilitation Assessment
or referring the client to another more appropriate ser-
vice.
See TI or TIAS programme selection for further eligibility
criteria and what to do if the client is not eligible for TI or
TIAS.
3.0 Complementary and alternative services
a Depending on the client’s identified needs, it may be
more appropriate to provide other option(s) in addition to,
or instead of, TI or TIAS, eg:
• Integrated Home and Community Support services or
Living my Life
• Vocational Rehabilitation
• Equipment, housing, vehicle modifications
It’s important to consider the timing of any other services
in relation to any TI or TIAS programme provided, so that
the services provided are co-ordinated.
ACC > Claims Management > Manage Claims > Service Pages > Community and Independence > Community Rehabilitation Services > Training for Independence > Training
For Independence Services Service Page
Uncontrolled Copy Only : Version 25.0 : Last Edited Thursday, 27 October 2022 2:27 PM : Printed Thursday, 1 June 2023 7:19 AM
Page 2 of 2
Document Outline