CONTENTS
1
Foreward ............................................................................................................................................................ 4
2
Scoping Review Findings .................................................................................................................................... 5
3
Introduction ....................................................................................................................................................... 6
4
Our Landscape is Changing – The Why? ............................................................................................................. 7
4.1
Are we Confident we are on Track to Meet the Needs of Health Graduates and Aotearoa in 2030? ....... 7
4.2
Implications for the FMHS ........................................................................................................................... 9
4.3
Equity ........................................................................................................................................................... 9
4.4
Workforce Equity ................................................................ ...................................................................... 10
4.5
Gender Identity and Equity ........................................................................................................................ 11
4.6
Sustainability with a Focus on the Impact of Climate Change on Human Health ..................................... 11
5
Health Professional Education - Medicine ....................................................................................................... 13
6
Health Professional Education – Nursing, Optometry and Pharmacy .............................................................. 16
6.1
Optometry Education ................................................................................................ ............................... 17
6.2
Pharmacy Education .................................................................................................................................. 18
6.3
Nursing Education ...................................................................................................................................... 20
7
Work to Date and Options Considered ............................................................................................................ 22
7.1
The Scoping Study ...................................................................................................................................... 22
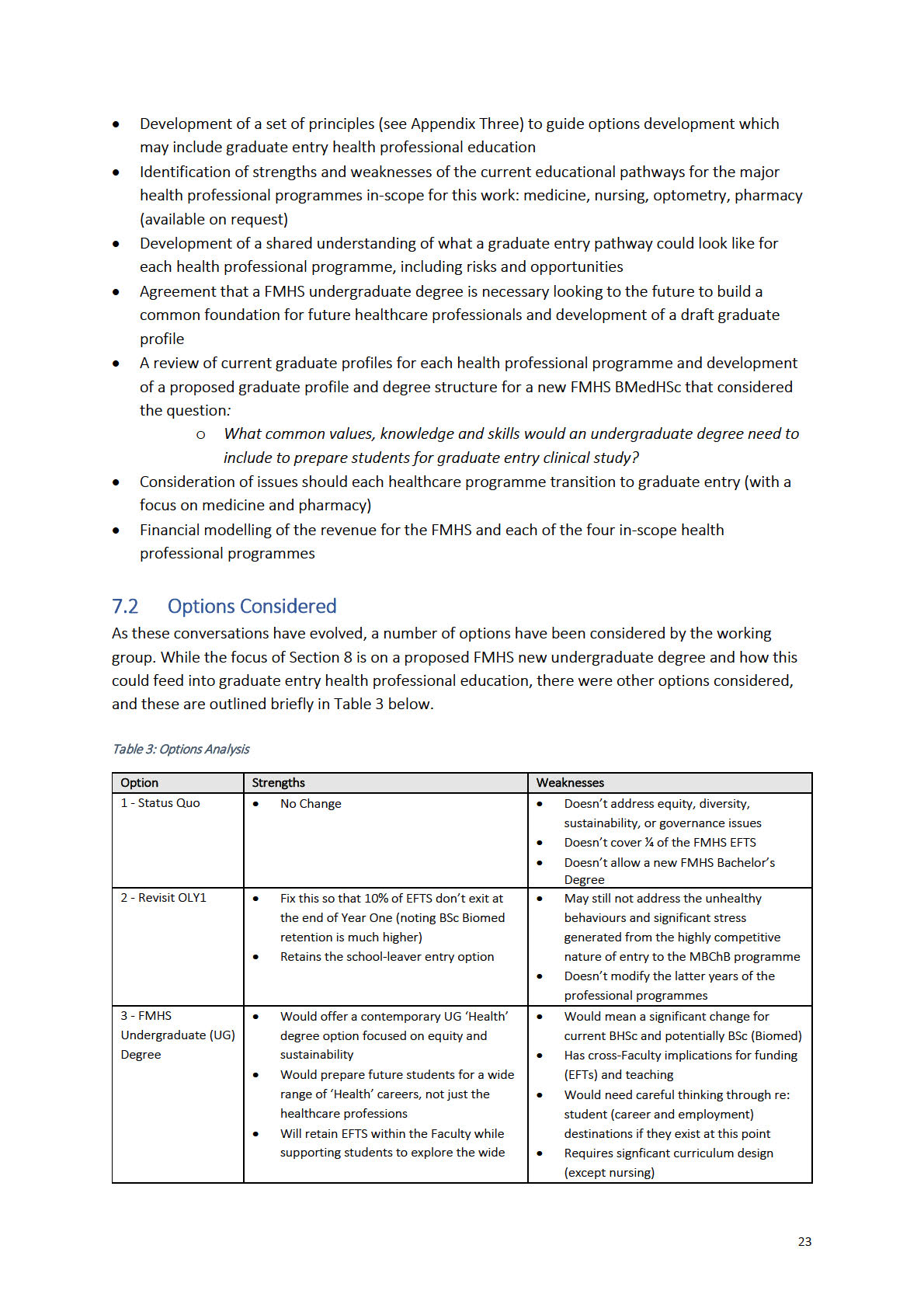
7.2
Options Considered ................................................................................................................................ .. 23
7.3
Pedagogy ................................................................................................ ................................................... 25
8
A Proposed Way Forward ................................................................................................................................. 26
8.1
An FMHS Undergraduate Degree .............................................................................................................. 26
8.2
Selection ................................................................................................................................ .................... 29
8.3
Pre-Requisites for Graduate Entry Health Professional Programmes ...................................................... 30
8.4
Māori and Pasifika Student Feedback ................................ ...................................................................... 32
8.5
Potential models for Optometry and Pharmacy ....................................................................................... 32
8.6
Threats and Opportunities Analysis ................................................................................................ .......... 33
8.7
Financial Modelling .................................................................................................................................... 36
8.8
Transition Considerations ................................ ......................................................................................... 40
Appendix One ............................................................................................................................................................ 44
Optometry - Employment ................................................................................................................................ ... 44
Appendix Two ........................................................................................................................................................... 45
Pharmacy - Current education and training pathway leading to initial registration .......................................... 45
Appendix Three ......................................................................................................................................................... 46
Proposed Guiding Principles for Future Healthcare Professional Education ...................................................... 46
Appendix Four ........................................................................................................................................................... 48
1
Healthcare Programme Graduate Entry Pre-Requisites ................................ ..................................................... 48
Appendix Five ............................................................................................................................................................ 53
Working Group Membership ................................ .............................................................................................. 53
Appendix Six .............................................................................................................................................................. 54
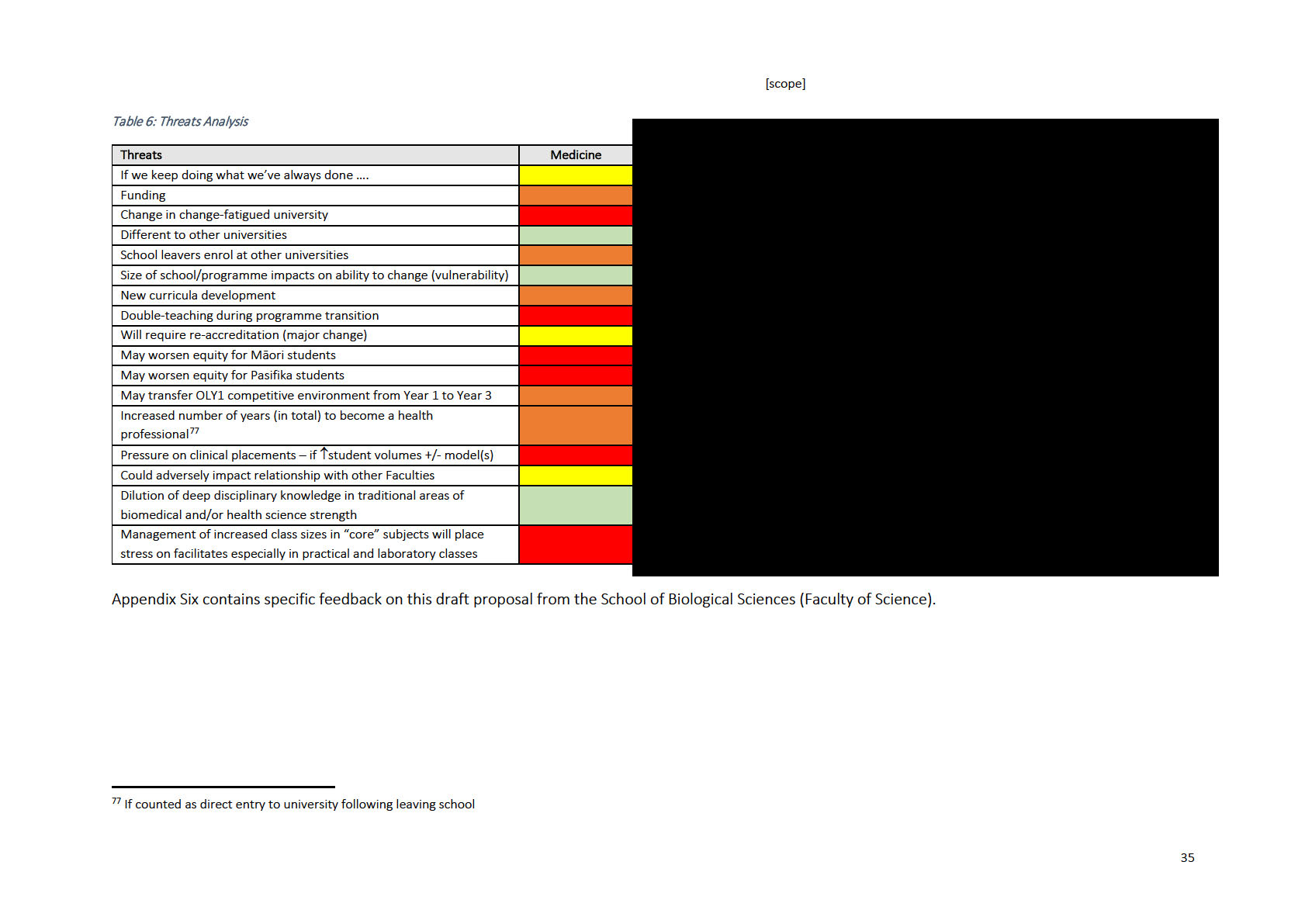
School of Biological Sciences Feedback on Draft Report..................................................................................... 54
FIGURES
Figure 1: The Future University of Auckland Degree ................................................................................................. 8
Figure 2: Transformational Curriculum ...................................................................................................................... 8
Figure 3: Number of Deaths Avoided 2040 under the SPS and the HPS per 100,000 Population, Relative to the
CPS ................................................................................................ ........................................................................... 12
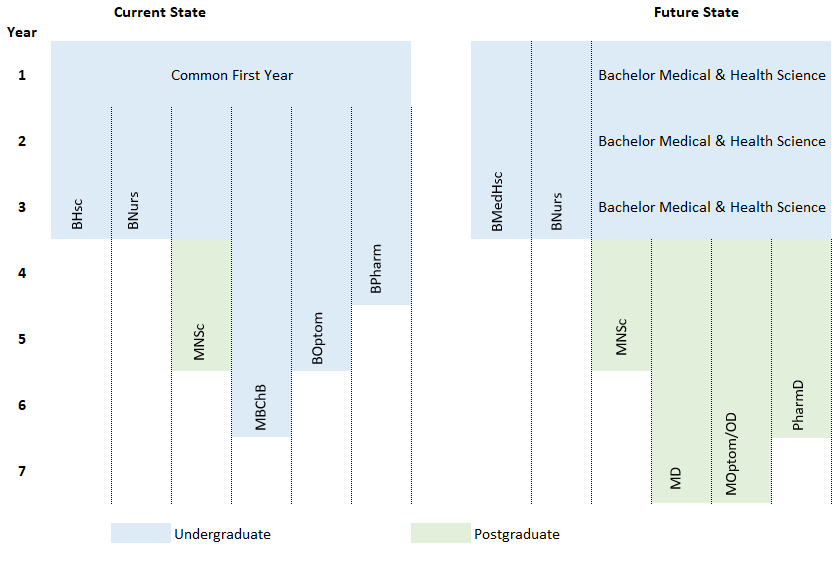
Figure 4: Current and Proposed Future State of Programmes ................................................................ ............... 26
Figure 5: Proposed New Bachelor Medical & Health Science (BMedHSc) Degree .................................................. 26
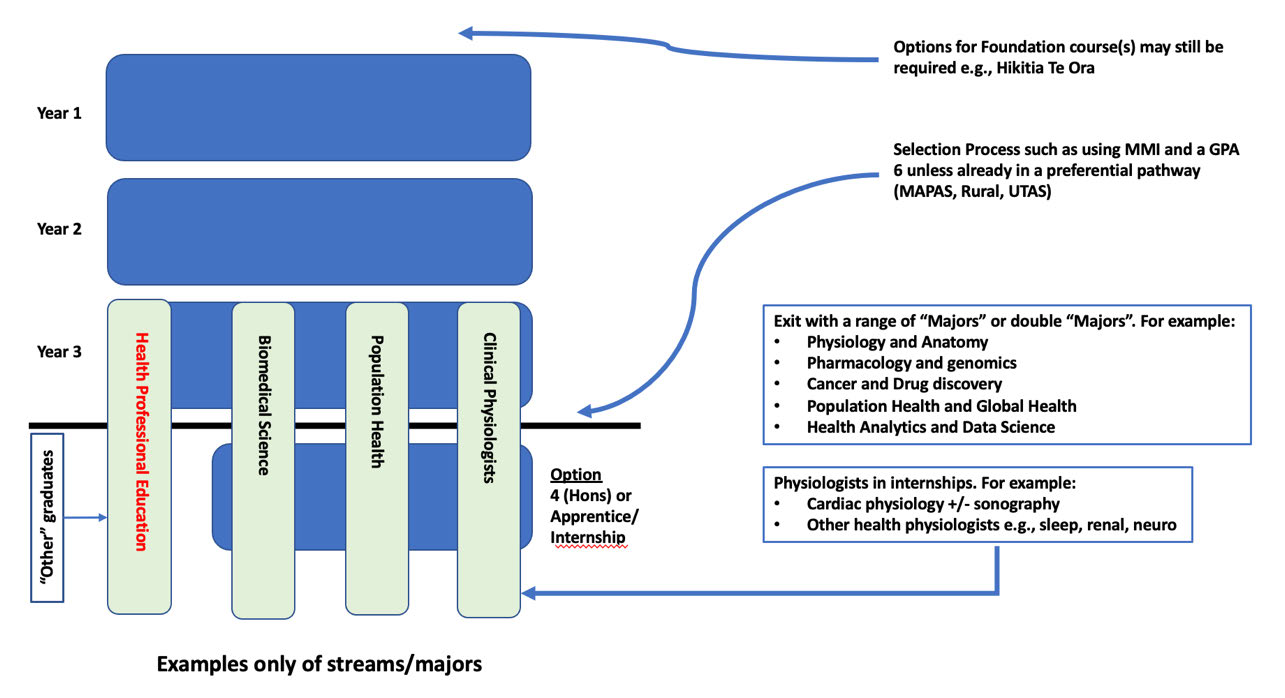
Figure 6: Proposed ‘Health Professional Stream’ Graduate Entry Pathway Options .............................................. 27
Figure 7: Proposed Graduate Entry Pathways for Optometry and Pharmacy ......................................................... 33
Figure 8: Variance to the Current Revenue Base ..................................................................................................... 37
Figure 9: Outcome of OLY1 Students 2018 – 2020 .................................................................................................. 37
Figure 10: Transition Modelling Showing the ‘Gap Year’ for Medicine ................................................................... 40
Figure 11: Medicine Only ‘Reduced Intake’ Model .................................................................................................. 41
TABLES
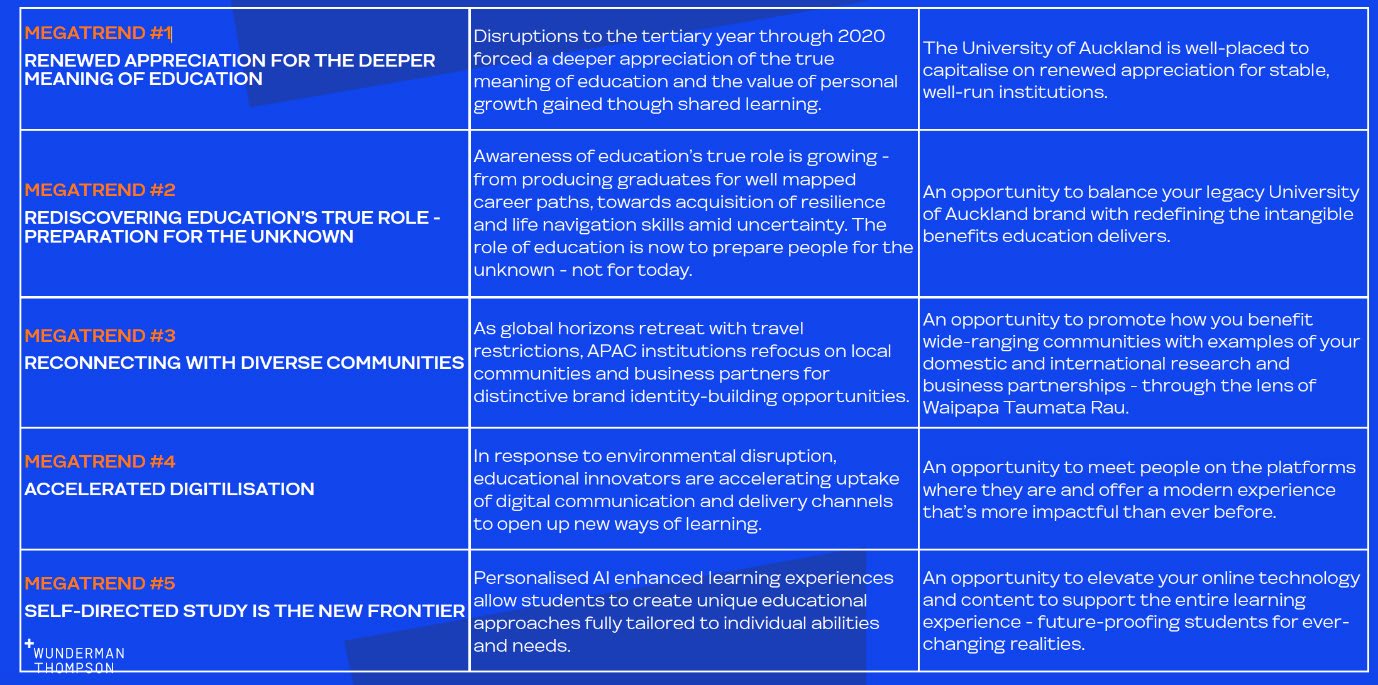
Table 1: Megatrends in Education ............................................................................................................................. 7
Table 2: Aotearoa New Zealand Nursing Programme Graduate Entry Academic Pre-requisites ........................... 20
Table 3: Options Analysis .......................................................................................................................................... 23
Table 4: Bachelor Medical & Health Sciences - Draft Graduate Profile ................................................................... 28
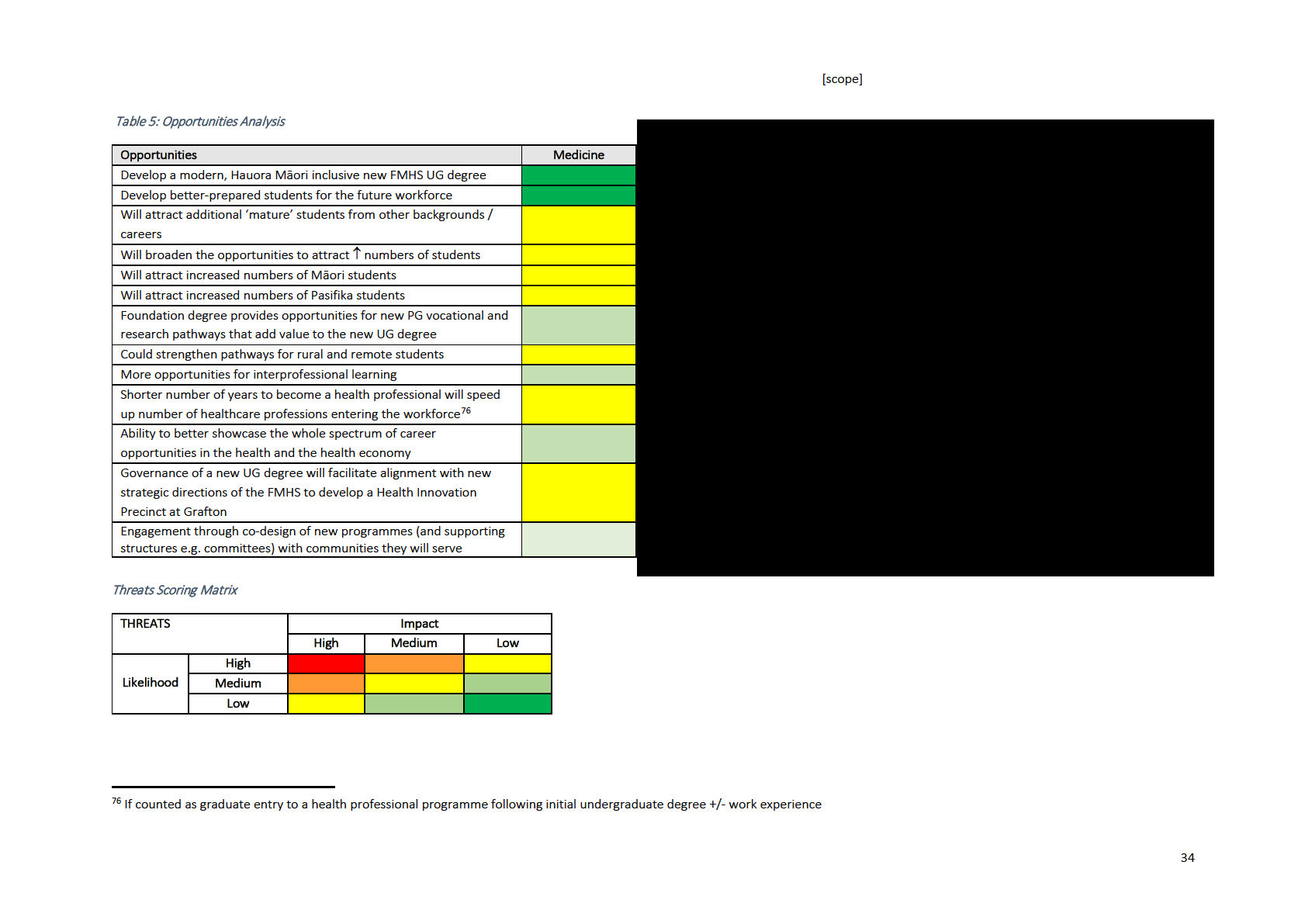
Table 5: Opportunities Analysis ................................ ............................................................................................... 34
Table 6: Threats Analysis .......................................................................................................................................... 35
Table 7: G8 University Medicine Programme Pre-requisites ................................................................................... 48
Table 8: G8 University Pharmacy Programme Pre-requisites .................................................................................. 49
Table 9: G8 University Optometry Programme Pre-requisites ................................................................ ............... 50
Table 10: G8 University Nursing Programme Pre-requisites ................................................................................... 51
Table 11: Relevant AHPRA Regulated Al ied Health Professions Accredited Programmes ..................................... 52
Table 12: Number of students enrolled in BSc Biomedical Science ........................................................................ 56
BOXES
Box 1: Cultural Safety in Aotearoa ........................................................................................................................... 10
Box 2: Analysis of the current MBCHB Year Two cohort of 264 domestic students (2021) .................................... 31
Box 3: Prescribed Qualifications for Aotearoa Nursing Graduates .......................................................................... 42
2
LIST OF ABBREVIATIONS USED
AHPRA
Australian Health Practitioners Regulation
MD
Medical Doctor
Agency
AI
Artificial Intelligence
MMI
Multiple mini interviews
ATAR
Australian Tertiary Admissions Rank
MNSci
Master Nursing Science
AUT
Auckland University of Technology
MPharm
Master of Pharmacy
BMedHSc
Bachelor Medical & Health Sciences
MPJE
Multi-State Pharmacy Jurisprudence Exam
Bnurs
Bachelor of Nursing
NAPLEX
North American Pharmacist Licensing Exam
BHSc
Bachelor of Health Sciences
OBA
Optometry Board of Australia
BOptom
Bachelor of Optometry
OCANZ
Optometry Council of Australia and New
Zealand
CAPEX
Capital Expenditure
OD
Doctor Optometry
CertHealthSci Certificate in Health Science
ODOB
Optometrists and Dispensing Opticians Board
CCAPP
Canadian Council for Accreditation of
OLY1
Overlapping Year One
Pharmacy Programs
DHB
District Health Board
PG
Postgraduate
DPT
Doctor Physiotherapy
PharmD
Doctor of Pharmacy
FMHS
Faculty of Medical & Health Sciences
RRAS
Regional and Rural Admission Scheme
FoS
Faculty of Science
SAC
Student Achievement Component
GAMSAT
Gradaute Medical School Admissions Test
SBS
School of Biological Sciences
GMC
General Medical Council
SES
Socioeconomic Status
GPA
Grade Point Average
TEC
Tertiary Education Commission
GPhC
General Pharmaceutical Council
UCAT
University Clinical Aptitude Test
Hons
Honours
UG
Undergraduate
HPE
Healthcare professional education
UK
United Kingdom
ITP
Institutes of Technology & Polytechnics
UoA
University of Auckland
ITP
Intern Training Program
UN
United Nations
MAPAS
Māori and Pasifika Admissions Scheme
USA
United States of America
MBBS
Bachelor of Medicine, Bachelor of Surgery
UTAS
Undergraduate Targeted Admissions Scheme
MCNZ
Medical Council of New Zealand
3
1
Foreward
The health workforce, with an estimated 80,000 employees is our country’s single largest employer.
Unsurprisingly, Health (capital H encapsulating all health disciplines) attracts many students to Waipapa
Taumata Rau each year, with a career in medicine the major drawcard. The requirements for an effective Health
practitioner across the many disciplines have evolved, and it is time to consider whether our education
pathways in Health are fit-for-purpose and meet the new ambitions of the university strategic plan
Taumata
teitei. One of the chal enges of
Taumata teitei is how best to accommodate new concepts and learning now
deemed to be essential in a competent work-ready Health graduate. Our Health curriculum has remains
constrained by a degree structure and student pathways that have changed little since their establishment 25
years ago. Since that time, Schools of Pharmacy, Nursing and Optometry have been established, and new
programmes in areas such as medical imaging, nutrition and dietetics and physiotherapy have been established.
In medicine, we have moved towards graduate entry into medicine (48% in 2021) and a significant expansion of
our Māori and Pacific student cohorts.
Our faculty’s mission is to produce competent Health graduates for tomorrow, ensuring that they are
knowledgeable, skilled, and ethical and are deeply cognisant of and sensitive to the complex natural and
societal chal enges of tomorrow’s world. Vastly different tools and alternative approaches require new
competencies that are not part of our current curriculum. Climate change, sustainable practices, Hauora and
matauranga Māori, equity, advanced technologies, digital science, artificial intelligence and complex systems
analysis, understanding data governance and sovereignty, changing scopes of practice and inter and
transdisciplinary activities are areas we acknowledge are significant, but to which we are chal enged to apply to
our existing curricula.
A school student coming to Waipapa Taumata Rau considering a career in Health, is immediately confronted
with a difficult choice of two parallel non-intersecting degrees; the BSc Biomed or the BHSc, which contribute to
the common overlapping year 1 (OLY1) but then go in quite separate directions. Little has changed in OLY1 since
its inception and students regularly report that this is a difficult and confusing first year at university. A recent
medical graduate told me “… that was the worst year of my life!”. This is not an uncommon sentiment.
After 25 years, it is time to consider alternative approaches that provide a more nurturing student experience
with clearer pathways to Health specialties and innovative learning strategies that foresee new challenges.
Many universities have already made a transition to a generalist undergraduate learning feeding into a range of
specialised post-graduate professional training programmes. Almost al Australian universities (led by the
landmark Melbourne model) now offer a 3- or 4-year postgraduate MD following a general undergraduate
degree.
In 2021, I asked Professor Warwick Bagg, Deputy Dean to chair a faculty working group to consider the pros and
cons of moving to postgraduate professional Health degrees and the subsequent development of a revised
undergraduate degree that incorporates more of what we believe all Health students need to learn. This
document is the work of many, but I especially thank Warwick and Janice Muel er of Waipiata Consulting for the
intensive work required in conducting research, consulting with Australian col eagues, col ating the findings and
compiling this concise report. I hope that this document will be read in the spirit it is intended and forms the
foundation for a wider consultation process around the Health curriculum for Waipapa Taumata Rau.
Prof John Fraser
Dean, FMHS
4
2
Scoping Review Findings
In summary, this scoping review has concluded that:
• There is significant FMHS desire to update the health curriculum to prepare graduates for 2030
and beyond
• Consequently, the FMHS will need to engage in the development of a new transdisciplinary
undergraduate health degree, considering the outcomes of the UoA curriculum transformation
project and that this degree replaces the BHSc
• The FMHS develops detailed plans for graduate entry health professional programmes and other
postgraduate offerings within the broad scope of health to determine the size, shape, and
composition of the suite of opportunities
• That the unique and flexible educational offerings developed offset any potential loss of school-
leaving students choosing an alternative university
• The FMHS engages with Māori and Pasifika whānau and communities to ensure that changes are
beneficial, and any lengthening of learning is offset by educational and employment benefits
• That detailed engagement occurs with the University, and subsequently the Ministry of Health
and TEC to align health education and workforce strategy and ensure adequate funding
• Wider community and stakeholder engagement needs to occur to assist in the development of
the transdisciplinary health degree
• Detailed work is undertaken to minimise selection competition for capped programmes e.g.,
medicine
•
•
[s 9(2)(k)]
5
3
Introduction
Healthcare professional education (HPE) has developed significantly since the early 1900’s when the
health professions were largely unregulated, few hospitals existed and only in 1910 was the first
effective therapeutic agent made available1. In 1910, Flexner proposed the first major shake-up in
medical education, emphasising the importance of the science underpinning medical practice2. In
2021, almost every aspect of healthcare is different to what it was in 1910. Traditional y, healthcare
education centred on the individual mastery of biomedical knowledge, in much simpler settings and
in teams that don’t reflect the current complexity, nor working reality of healthcare delivery today3.
Multidisciplinary teamwork in complex and uncertain healthcare settings are the norm today.
Therefore, modern HPE emphasises the importance of working in teams, lifelong learning, critical
thinking and a knowledge of models beyond the biomedical causes of illness.
No discussion on HPE in Aotearoa can be undertaken without first acknowledging that there is
significant inequity at every level of society for Māori and Pasifika people as a consequence of racism
and colonisation. Inequity impacts adversely on health and social wellbeing culminating in younger
onset of complex chronic disease and reduced life expectancy. These inequities must be put to right
and the Faculty of Medical & Health Sciences (FMHS) is committed to contributing to solutions
through affirmative HPE selection policies, anti-racism education, and considering education policies
through an equity lens. Many of the features of modern HPE are already present in the FMHS
professional programmes, which are fully accredited by the relevant regulatory authorities and
graduates of the faculty are held in high esteem. Nevertheless, the FMHS needs to consider if the HPE
models currently in use will continue to serve Aotearoa well in the future.
The core role of health professionals is to provide timely and appropriate patient centred care. How
health professionals deliver their role, and in what contexts, continues to evolve over time. Health
professionals in Aotearoa stand at a juxtaposition. On the one hand inequity for Māori has continued
to increase and may be further exacerbated by current and future global challenges, the most
pressing of which is climate change. The delivery of health services is inequitable, with poorer people
and rural populations being most affected. On the other hand, rapid advances in medical treatments
and devices, the use of data science and artificial intel igence, advances in genetics and a myriad of
other developments, all present opportunities, but require cost effective implementation plans.
Interprofessional healthcare learning, collaborative practice and Māori clinical and cultural
competence / safety for practitioners are increasingly important to enhancing patient safety and
improving equity.
In sum, there are ongoing chal enges and opportunities for healthcare delivery, and future-proofing
healthcare professional learning and assessment, considering both context and content. Inevitably
there are financial considerations of any change, but also there is also a ‘cost’ of maintaining the
status quo. Therefore, it is timely to consider if the HPE models as currently configured at the FMHS
are fit for future purpose.
1 Moseley GB. The U.S. Health Care Non-system, 1908-2008. The Virtual mentor 2008 May 1,;10(5):324-331.
2 Flexner A. Medical education in the United States and Canada. New York: Carnegie Foundation for the Advancement of Teaching; 1910.
3 Shelton PG, Corral I, Kyle B. Advancements in Undergraduate Medical Education: Meeting the Challenges of an Evolving World of
Education, Healthcare, and Technology. Psychiatric quarterly 2017 Jun;88(2):225-234.
6
4
Our Landscape is Changing – The Why?
4.1 Are we Confident we are on Track to Meet the Needs of Health Graduates
and Aotearoa in 2030?
Are there unique reasons for the FMHS to change to graduate health (professional) education? To
begin to answer this question the FMHS needs to consider changes in the worldwide delivery of
education and the implications of Taumata Teitei. In a worldwide context, Wunderman and
Thompson have identified the following ‘megatrends’ in education and the implications for the
University of Auckland.
Table 1: Megatrends in Education
Taumata Teitei – Vision 2030 & Strategic Plan 20254 provides a new context for the University over
the coming five to 10 years. Importantly it stresses focus and impact in four priority areas:
• Leading transition to sustainable and abundant ecosystems
• Improving health and wellbeing for all
• Advancing just, cultured, and engaged communities
• Innovating contemporary, secure knowledge systems
The education priorities of Taumata Teitei are identified as:
• Accessible, equitable lifelong higher education opportunities
• Student-centric learning, co-curricular and extra-curricular cultures
• Education that is research informed, transdisciplinary, relevant and with impact for the world
• Graduates who make the world better tomorrow then it is today
Taking these priorities into consideration the future University of Auckland degree is schematically
represented in Figure 1 below.
4 Available from https://cdn.auckland.ac.nz/assets/auckland/about-us/the-university/official-publications/strategic-plan/2021-
2030/taumata-teitei-vision-2030-and-strategic-plan-2025.pdf [Accessed 14 September 2021]
7
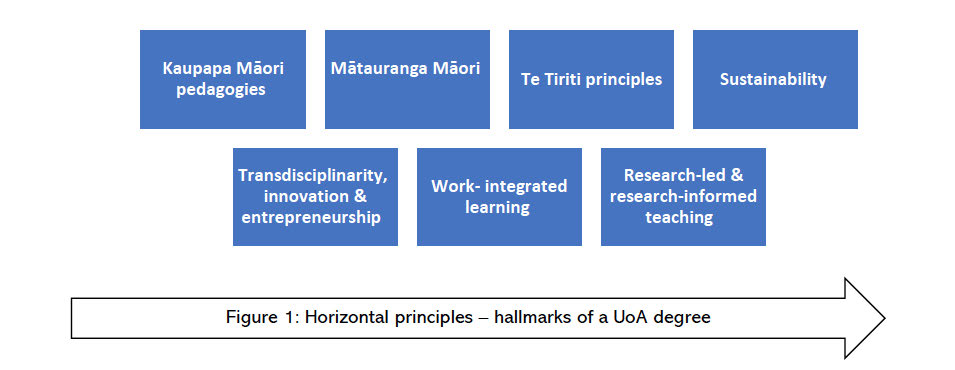
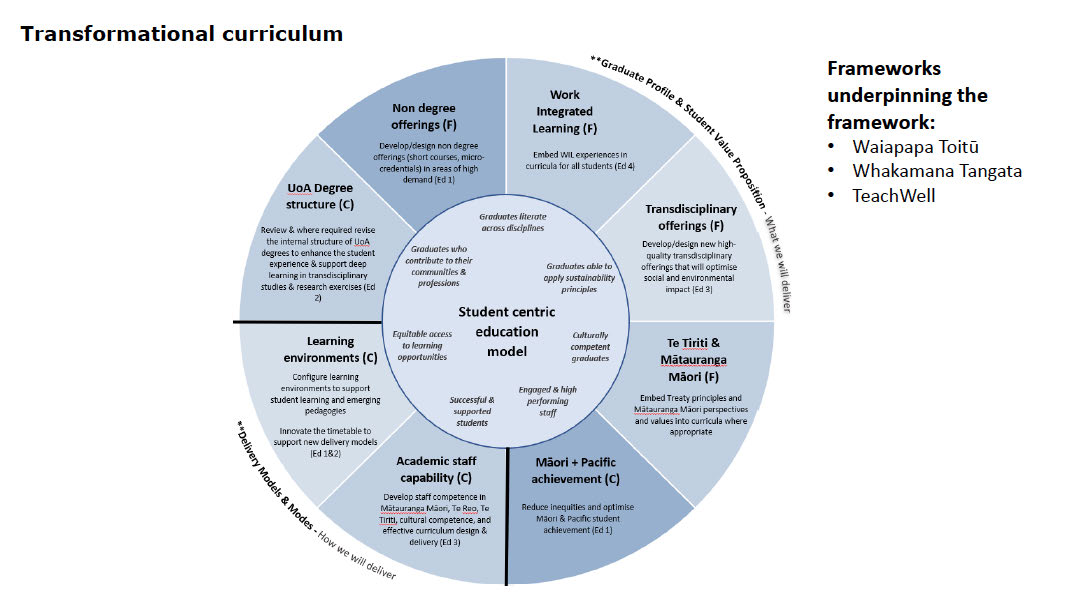
Figure 1: The Future University of Auckland Degree
The University wide curriculum transformation work is framework is schematically represented by
Figure 2 below.
Figure 2: Transformational Curriculum
Health System Reforms
Major reforms in the health system in Aotearoa also need to inform the delivery of future health care
education. The announcement of the establishment of the Māori Health Authority by mid 2022
signals the Government’s intention to improve health outcomes for Māori. While much of the detail
of the health reforms has yet to be made public, this generational change invites us to reflect on how
the FMHS delivers education. In summary, there are global changes in education, the university is
undergoing curriculum transformation and the health sector is undergoing major reform.
8
4.2 Implications for the FMHS
This working group was specifical y asked to consider a change to graduate health professional
education. Graduate health professional education is not a new concept. There have been several
reasons articulated in the literature as to why graduate health professional education may be a
preferred model and these are explored in detail in subsequent sections of this document. While
many laudable reasons that have been put forward as potential benefits of graduate health
professional education,
there is no overall compelling evidence-based reason in the literature to
change to graduate health professional education.
There are several reasons for the mixed evidence. Most of the evidence relates to medicine and in
this context entry to medical programmes is highly competitive, meaning that high achieving students
will general y succeed no matter what the educational model. Medical education has undergone a
number of revisions over time, but is still a largely apprentice-based education, irrespective of the
model of education. The apprenticeship model, to varying degrees, also exists for other health
professional education. Given the largely apprenticeship-based education model it may be difficult to
demonstrate clear benefits of undergraduate over graduate education. When longer term outcomes
are evaluated, graduate entry programmes generally graduate older students, who are more
indebted, have more complex lives but don’t generally take up different specialities to their
undergraduate counterparts.
To shape the graduates of the future will be dependent on the type of students selected, the nature
of the educational environment and ethos of the institution. Perhaps the clearest example of this in
Australasia is James Cook University. The deliberate selection policy, ethos, curriculum and
placements polices increase the likelihood that graduates wil work in regional and remote Australia
as generalists serving their community.
The FMHS ‘why’ considers Equity and Sustainability as the foundational concepts for re-design.
4.3 Equity
There are multiple components to equity that need to be addressed. The most pressing of these is
ongoing inequity for indigenous Māori. This has been recognised by the Government and the
establishment of the Māori Health Authority by mid 2022 signals the Government’s intention to
improve health outcomes for Māori. In addition, He Puapua, released under the Official Information
Act, clearly articulates the changes that need to occur by 2040 in societal political norms to ensure
Aotearoa’s constitution is rooted in te Titiriti and the UN declaration on the Rights of Indigenous
Peoples5. Wil FMHS graduates be wel equipped to work within the reality of the Māori Health
Authority and the rangtiratanga-centric approach advocated for in He Puapua?
Pasifika people also suffer significant inequity on every measure, in particular in related to health
outcomes. While much of the inequitable health outcomes for Māori and Pasifika may be due to
causes beyond that are considered the traditional roles of health professionals, we argue that a
bigger picture of HEALTH needs to be considered. Thus the concept of Health, with a ‘capital H’,
needs to be considered in re-imagining of FMHS education. Education is centred on Mataūranga
5 Charters C, Kingdon-Bebb K, Olsen T, Ormsby W, Owen E, Pryor J, et al. He Puapua. 2019 November.
9
Māori, embodies all of human health including health policy which decolonises health education and
is antiracist. ‘Capital H’ health education includes health professional education that is research led
and evidence based and produces culturally safe practitioners. Recognition that the ‘capital H’ health
education incorporates emerging technologies delivered by a wide range of professionals including
biomedical scientists, advanced physiologists, genomic experts and others who understand that at the
heart of healthcare delivery is equity. We argue that these outcomes can be best achieved by a broad
undergraduate ‘capital H’ education, prior to entry to health professional education and other ‘capital
H’ health disciplines.
4.4 Workforce Equity
There continues to be significant underrepresentation of Māori and Pasifika people in every part of
the health workforce. The FMHS has invested significantly over several decades to improve access
and entry of Māori and Pasifika to and graduation from health professional degrees. This has been
especial y successful for medicine, but less successful for other aspects of ‘capital H’ health education.
While the reasons for the mixed success are multifactorial, one factor is the difficulty for prospective
students to grasp the ful range of ‘capital H’ health professions available to peruse as a career. This is
a challenge faced by all prospective students and is an argument for graduate entry after a broad
‘capital H’ degree to be given the opportunity to see the multiplicity of pathways that are open to
them to participate in the heath workforce.
There is also a duty for the FMHS to ensure that students are educated in culturally safe practices.
This has also been recognised in legislation at an individual practitioner level, with the 2019
amendments to the Health Practitioners Competence Assurance Act (2003) now requiring al
authorities to
‘set standards of … cultural competence (including competencies that wil enable
effective and respectful interaction with Māori) …’ (Section 118(i)). Box 1 below shows a
contemporary definition of cultural safety.
Box 1: Cultural Safety in Aotearoa
Cultural safety requires healthcare professionals and their associated healthcare organisations to examine
themselves and the potential impact of their own culture on clinical interactions and healthcare service delivery.
This requires individual healthcare professionals and healthcare organisations to acknowledge and address their
own biases, attitudes, assumptions, stereotypes, prejudices, structures, and characteristics that may affect the
quality of care provided.
In doing so, cultural safety encompasses a critical consciousness where healthcare professionals and healthcare
organisations engage in ongoing self-reflection and self-awareness and hold themselves accountable for
providing culturally safe care, as defined by the patient and their communities, and as measured through
progress towards achieving health equity.
Cultural safety requires healthcare professionals and their associated healthcare organisations to influence
healthcare to reduce bias and achieve equity within the workforce and working environment.
Source: Curtis E, Jones R, Tipene-Leach D, Walker C, Loring B, Paine S-J, Reid P (2019). Why cultural safety rather than
cultural competency is required to achieve health equity: a literature review and recommended definition.
Int. J. For Equity
in Health, 18:174. https://dx.doi.org/10.1186/s12939-019-1082-3
10
4.5 Gender Identity and Equity
Over time there has been an increase in women who participate in health professions and the
majority of the professional health workforce positions are held by women. However, participation is
not equal and in many professions there is a dearth of women particularly in senior positions. Thus
there continues to be a gender inequality in the health workforce. Sadly, there continue to be sexist
and discriminatory behaviours based on gender identity within the health workforce. ‘Capital H’
education will seek to address the importance of gender equity.
4.6 Sustainability with a Focus on the Impact of Climate Change on Human
Health
The recently published sixth assessment report of the Intergovernmental Panel on Climate Change
has reported that ‘Human-induced climate change is already affecting many weather and climate
extremes in every region across the globe’6. We need to prepare the future ‘capital H’ health
workforce for the reality of health impacts of human-induced climate change. Indigenous equity and
land rights are inextricably linked to sustainability. Thus we see the lenses of Equity and Sustainability
as foundational partners for ‘capital H’ health education. This is not just a unique concept in in
Aotearoa, but around the world, as described by key United Nations (UN) people.
‘Climate change is happening now and to al of us. No country or community is immune’, said UN
Secretary-General António Guterres. ‘And, as is always the case, the poor and vulnerable are the
first to suffer and the worst hit’. .. ‘Climate justice insists on a shift from a discourse on
greenhouse gases and melting ice caps into a civil rights movement with the people and
communities most vulnerable to climate impacts at its heart’.
Mary Robinson - President of Ireland. https://www.un.org/sustainabledevelopment/blog/2019/05/climate-justice/
In Aotearoa (and worldwide) the concepts of indigenous equity, land rights and sustainability are
embodied in the concept of Kaitiakitanga:
• Indigenous peoples play a crucial role in the conservation of the environment
• They make up around 5% of the global population and occupy, own, or manage an estimated 20%
to 25% of the Earth’s land surface
• This land area holds 80% of the planet’s biodiversity and intersects with about 40% of all
terrestrial protected areas and ecologically intact landscapes
In Aotearoa there are indigenous organisations that are leading substantiality. They are described as
‘
Rangatahi led. Rangatahi driven. We are indigenous youth from the Pacific and Aotearoa working for
climate action and indigenous sovereignty’7. One of the domains of quality used in the Royal College
of Physicians definition of quality includes sustainability:
Sustainability should be viewed as a characteristic of healthcare which must run through and
moderates other domains. Healthcare should be considered not only in terms of what can be
delivered to an individual today, but also to the population in general and the patients of the
future8.
6 Available from https://www.ipcc.ch/report/ar6/wg1/downloads/report/IPCC AR6 WGI SPM.pdf
7 Available from https://tearawhatu.org [Accessed 14 September 2021]
8 Available from https://www.rcpjournals.org/content/clinmedicine/10/6/537 [Accessed 14 September 2021]
11
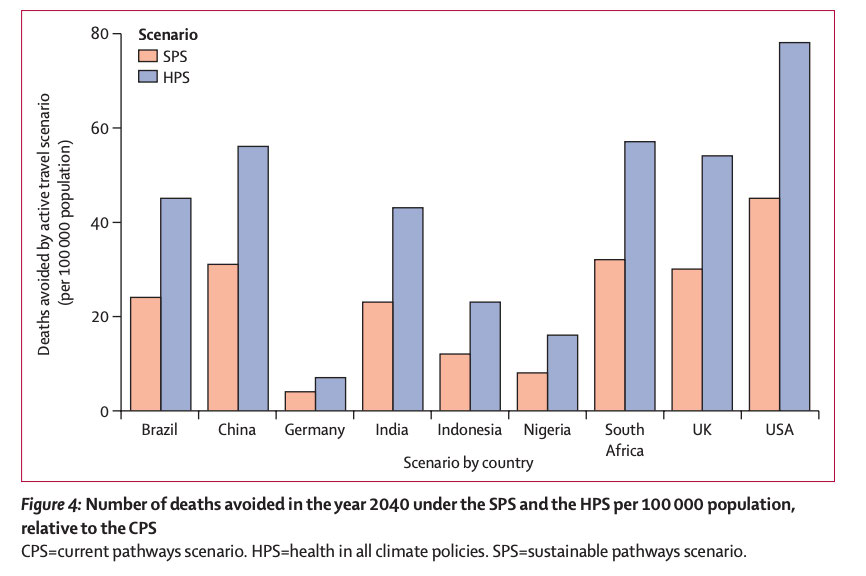
Moreover, when placing health as a key focus of the national y determined contributions to meet the
goals of the Paris Agreement there is an opportunity to improve health co-benefits. This is il ustrated
in the transport scenario shown below9.
Figure 3: Number of Deaths Avoided 2040 under the SPS and the HPS per 100,000 Population, Relative to the CPS
It is abundantly clear that the FMHS must prepare graduates for a world that is going to be impacted
by climate change. It is an opportunity to focus on sustainable health care delivery and solutions.
Other considerations for redesigning ‘capital H’ healthcare education include:
• Opportunities for greenfield development to include wide range of topics and redesign
• Wide range of health opportunities and to modernise the curriculum
• International partnership opportunities
In summary, there are compelling reasons to consider an overhaul and redesign of FMHS health
education.
9 Available from https://www.thelancet.com/journals/lanplh/article/PIIS2542-5196(20)30249-7/ful text [Accessed 14 September 2021]
12
5
Health Professional Education - Medicine
In North America, MD degrees after a four year pre-med college degree have been the norm in the
USA for many decades. In 1997 the United Kingdom (UK) Medical Workforce Standing Advisory
Committee recommended that clinical courses with graduate entry should be developed10. The
rationale was to al ow the faster production of doctors (a once-off effect), broaden the field from
which doctors are recruited, to make more efficient use of existing educational capacity, and increase
flexibility to respond to changing demand11. Nearly half of the UK’s 33 medical schools now offer
graduate medical programmes, with 18 out of 20 of the highest ranked medical schools in the world
being graduate entry12.
There is some evidence that graduate entry students perform better on GAMSAT and UCAT, are more
likely to graduate with honours degrees or first-class degrees, and favour deep over superficial
learning, but findings are inconsistent13 14. Moreover, much of the apparent advantages of graduate
entry may be attributed to older age, rather than a prior degree15. Because the General Medical
Council (GMC) mandates a minimum 5,500 hours of training to study medicine, graduate courses
have a longer academic year and are more compressed than undergraduate courses, creating
pressure on students16 17. Despite the added pressure, some authors have found that graduate entry
students have better coping skil s and are not more stressed than undergraduates18 19. In contrast,
others have found that nearly half of graduate students have significantly higher anxiety scores, in the
distressed range, than their undergraduate counterparts20. Debt levels tend to be higher for graduate
entry students and consequently these students take more time to pay off their debt21.
The dominant driver of the transition to graduate education in Australia was the University of
Melbourne22. The philosophy of the so called ‘Melbourne model’ is for undergraduates to develop
broader skil s through a small number of general three-year degrees, while shifting to graduate entry
professional training23. This was a significant, university-wide transformation, that resulted in 96
undergraduate degrees being replaced by six degrees24. To make the financial case, the university
successfully lobbied for publicly subsided graduate professional courses, the cap on the national
student loan scheme to be lifted and an amendment to the Youth Allowance policy25. During the 13-
10 Carter YH, Peile E. Graduate entry medicine: high aspirations at birth. Clinical Medicine 2007 April;7(2):143-147.
11 Ibid
12 Olivarius-McAllister J, Yapp N, Jacquemot A, Robinson A. Graduate entry medicine: the right way forward? Postgraduate medical journal
2021 Apr;97(1146):207-208.
13 Ibid
14 Sandover S, Jonas-Dwyer D, Marr T. Graduate entry and undergraduate medical students’ study approaches, stress levels and ways of
coping: a five year longitudinal study. BMC medical education 2015 Jan 24; 15(1): 5.
15 Wilkinson TJ, Wel s JE, Bushnel JA. Are differences between graduates and undergraduates in a medical course due to age or prior
degree? Medical education 2004 Nov; 38(11): 1141-1146.
16 Carter YH, Peile E. Graduate entry medicine: high aspirations at birth. Clinical Medicine 2007 April; 7(2): 143-147.
17 Olivarius-McAl ister J, Yapp N, Jacquemot A, Robinson A. Graduate entry medicine: the right way forward? Postgraduate medical journal
2021 Apr; 97(1146): 207-208.
18 Ibid
19 Sandover S, Jonas-Dwyer D, Marr T. Graduate entry and undergraduate medical students’ study approaches, stress levels and ways of
coping: a five year longitudinal study. BMC medical education 2015 Jan 24; 15(1): 5.
20 Casey D, Thomas S, Hocking DR, Kemp-Casey A. Graduate-entry medical students: older and wiser but not less distressed. Australasian
Psychiatry 2016; 21(1): 88-92.
21 Olivarius-McAllister J, Yapp N, Jacquemot A, Robinson A. Graduate entry medicine: the right way forward? Postgraduate medical journal
2021 Apr; 97(1146): 207-208.
22 James R, McPhee P. Case study: The whole-of-institution curriculum renewal undertaken by the University of Melbourne, 2005–2011.
Strategic Curriculum Change in Universities: Routledge; 2012. p. 157-172.
23 Ibid
24 Bolton R. Melbourne University vice chancellor Glyn Davis on funds, freedom and his future. Financial Review 2018 24 August.
25 Ibid
13
year tenure of the Vice-chancel or, spanning the introduction of the model, annual funding increased
from $1.1 bil ion to $2.56 bil ion26.
The University of Melbourne educational objectives are set out in aspirational statements aiming to
deliver the ‘
Melbourne Experience’27:
• distinctive undergraduate courses that offer pathways into professional graduate programs, but
which also stand alone as strong degrees;
• a sound discipline-based education, including an introduction to research as a foundation for
research higher degrees;
• closer alignment of course structures with desired graduate attribute outcomes;
• ‘deep generalist’ graduates with the generic and interdisciplinary skills suitable for both
postgraduate programs and diverse and changing workplaces;
• a stronger likelihood of well-rounded and motivated graduate students at both Master’s and PhD
level;
• more informed student choice about careers and graduate education;
• a stronger shared experience, engagement and sense of university community;
• enhanced opportunities for external experiences such as community work or international study;
• strengthened international recognition of degrees;
• broader access for students, especial y those from disadvantaged backgrounds;
• greater opportunity for students (and staff) to experience interdisciplinary teaching and research
collaborations across the University;
• an improved classroom experience, including smal er classes for courses which move to graduate
entry.
To address selection to vocational programmes an admission policy was put in place for very high
achieving school students to be offered a guaranteed place in one of the university’s graduate
schools28. An unanticipated outcome of the change was a modest improvement in the enrolments of
students from lower SES backgrounds29. The university is increasingly attractive to international
students, who made up 44% of the student body in 2019 (pre-Covid)30.
While there has been much debate about the success or otherwise of the change at the University of
Melbourne, the university is ranked 31 in the world (THE) and 18 (WUR) for medicine and is financially
viable. The Melbourne model change has been cited as the major reason that most Australian
universities are now offering MD degrees. The move to graduate education occurred at the same
time as the introduction of problem based learning, and necessitated a review of selection policies31.
26 Ibid
27 Ibid
28 Ibid
29 Ibid
30 University of Melbourne 2019 Annual Report. University of Melbourne 2020 March 31:1-196.
31 Elliott SL, Epstein J. Selecting the future doctors: the role of graduate medical programmes. Internal Medicine Journal 2005;35:174-177.
14
Other reasons cited in Australia for introducing graduate entry medical programmes included:
• largely supported by students32;
• broaden diversity so that not just school leavers with high maths and science achievers enter
medicine33;
• address social inequity caused by an imbalanced school system34 ;
• higher motivation of graduates and a more informed career choice35 ;
• students with increased maturity, breadth of education, diversity of background, and the capacity
for self-directed learning and communication skills36 ;
• evidence from the USA that older graduates were more likely to work in underserved areas37.
What is less obvious from the literature, but clear from speaking to colleagues in Australia, is that
while most medical programmes have shifted to MD degrees, many have retained undergraduate
entry. In effect, some Australian universities took their existing 5/6 year MBBS programmes and
converted them into a ‘pre-med’ degree and an MD. At these universities there is no graduate entry,
other than through the specified ‘pre-med’ degree. The reasons for changing to MD degrees are
diverse: so called ‘market forces, the opportunity to modify the curriculum and assessment in a
medical programme, to attract international students, enhanced funding and international name
recognition of the MD degree.
The ability to attract international students is a major financial advantage for a number of universities
in Australia, especially when there are overseas campuses. Not all Australian universities are
necessarily trying to attract overseas students, preferring to focus on graduating doctors selected
from their local catchment area and intending to return to work in the same area.
A significant difference between Australia and Aotearoa is the competition between medical schools.
Consequently, medical schools have developed medical programmes with a point of difference. These
include:
• Undergraduate entry as their ‘competitive’ advantage
• The type of doctor they wish to graduate e.g., clinician researchers
• Graduating doctors in the shortest time possible (4.75 and 5 years) to be ‘work ready’ and
completing a professional project rather than a research project (typical y thought to be
necessary for an MD)
• Different campuses, including overseas campuses, with different lengths of programmes al owing
for distinct learning experiences e.g., rural pathways
32 Ibid
33 Sefton AJ. Australian medical education in a time of change: a view from the University of Sydney. Medical education 1995 May; 29(3):
181-186.
34 Miflin B, Harris P, Donald K, Bore P, Parker M, Groves M, et al. Graduate entry to medical studies: thoughts from 'down under'. Medical
teacher 2003 Mar; 25(2): 109-111.
35 El iott SL, Epstein J. Selecting the future doctors: the role of graduate medical programmes . Internal Medicine Journal 2005; 35: 174-177.
36 Finucane, Terry Nicholas, David Prideaux, Paul. The new medical curriculum at Flinders University, South Australia: from concept to
reality. Medical teacher 2001; 23(1): 76-79.
37 Carter YH, Peile E. Graduate entry medicine: high aspirations at birth. Clinical Medicine 2007 April; 7(2): 143-147.
15
[scope]
16
[scope]
17
[scope]
18
[scope]
19
[scope]
20
[scope]
21
7
Work to Date and Options Considered
7.1 The Scoping Study
To consider graduate health professional education, the FMHS undertook a scoping study. The
working group were tasked with considering the medical programme and the role of the health
professional in 2030 and beyond. They also considered the potential implementation of an MD
degree for medicine; and whether other health professional programmes wished to consider
postgraduate entry (or alternative educational strategies) to ensure fit for purpose health
professionals.
Terms of Reference
1. Develop a model of the attitudes, knowledge and skills required of a health professional
graduating in Aotearoa in 2030
2. Study the strengths and weakness of the current MBChB programme
3. Propose a rationale for why a change to an MD degree may be appropriate based on published
evidence
4. Learn from overseas jurisdictions that have implemented MD degrees
5. Design entry pathways to an MD degree
6. Model the financial implications of a change to an MD degree
7. Propose a timeline for implementation of an MD, including regulatory approvals
8. Consider graduate entry for other FMHS health professional programmes
9. Consider alternative educational strategies to enhance health professional education in the FMHS
To summarise, this work has specifically considered the question
: ‘would graduate entry educational
model for the professions of medicine, nursing, optometry and pharmacy enable the health professional
of the future to be better prepared?’
Methodology
A working group was established (refer Appendix Five), with the membership growing and evolving
during the course of the work as interested stakeholders requested to participate. Given the initial
scoping nature of this work, the majority of participants have been from the FMHS. This has resulted
in rich and varied conversations which have been key to the work described in this report.
The group met face to face monthly from March to August 2021, the via zoom in September 2021,
with the final report due to FMHS in October 2021. In addition to monthly working group meetings, a
student meeting with FMHS student stakeholder representatives, a stakeholder meeting with Māori
and Pasifika student FMHS representatives and an FMHS Faculty Forum session have all been held,
with themes from this feedback included within in the report.
Work To Date
This work completed has included:
• Review of the literature regarding health professional graduate entry programmes for the four in-
scope professions
• Engagement with stakeholders across a range of medical schools at Australian universities to gain
feedback regarding their graduate entry journeys
22
range of health career options that are
available to them
4 - FMHS
•
As above plus ...
•
As above plus ...
Undergraduate (UG) •
Provides time and course options to
•
Would require suitable bridging course(s)
Degree AND health
prepare students for ‘Health’ and health
/ programme for potential healthcare
professional
professional carreers
students who did not take the FMHS UG
graduate entry
•
Green field approach to reshape
degree
education in professional degrees and
•
The (potentially) longer study time in
clinical placement models
years (for all programmes) could be a
•
International partnership arrangements
significant disadvantage for all students,
could be explored
especially Māori and Pasifika students
•
Streaming e.g.,
•
Tāmaki Makaurau is expensive to live and
o Rural
study
o Research (e.g., MD/PhD
•
School-leaver students who want a
programme), and/or
‘shorter time’ to achieve their
o Te Reo Māori stream for
qualification will choose other universities
indigenous speakers
•
[scope]
•
May be some trade-offs for Medicine with
a 5 year professional programme reduced
to 4 years
If the curriculum and structure of any such future health UG degree is considered at another time, the
working group’s view of the major advantages of the proposed new degree are associated with
governance of the proposed degree, and include:
1. Being FMHS-led allows the Faculty to determine entry criteria, student numbers, promotion to
schools, and the marketing of the degree in terms of showing the full spectrum of career
opportunities in health and the wider health related economy
2. FMHS governance allows the Faculty to determine the graduate profile, the curriculum direction,
assessment, administration, and communication associated with a single broad health degree, in
consultation with other Faculties
3. It allows FMHS to have a more comprehensive and ongoing approach to support Māori and
Pasifika students in al domains covered by the degree rather than just the students in
professional programmes
4. Strategical y it underpins FMHS strategic goals out to 2030 to become a health innovation campus
that is part of a wider health innovation precinct to produce graduates who can contribute to the
health and wealth of Aotearoa
5. It gives FMHS the mana that has been earned as the major provider of health professional
education and health research in Aotearoa
Outstanding areas of common concern/uncertainty currently include:
• Are graduate entry health programmes suitable for al four programmes within scope of this
work, or only some?
• What would this do for equity? We must not lose (and need to continue to build on) equity gains
for Māori and Pasifika, particularly for the non-medicine professions
24
• Do the families and whānau of Māori and Pasifika students (and potential students themselves)
understand and support this change, including the risks of increased student debt and longer
total training time (in years)?
• Do employers want a longer/shorter pathway to train these specific healthcare professions?
• How would selection processes work for a graduate entry health professional programme
(assuming current affirmative pathways remain)?
• Could OLY1 be retained and improved if a health professional programme did not move to a
graduate entry pathway?
• How do we continue to strengthen interprofessional learning?
• How wil competitor universities respond (or not) if (these selected) health professional
programmes move to a graduate entry model?
• Financial implications of any proposed change
• Relationship with other Faculties
7.3 Pedagogy
Taumata Teitei has reinforced the importance of innovative pedagogy, while building on existing
expertise. The pandemic has also driven us to engage in new ways of learning, using online
and blended methodologies. While the detail of the pedagogy is still be decided, and may vary
according to the discipline, the core tenants wil include:
• Teaching wil be framed in Te Tiriti accountabilities
• Kaupapa Māori pedagogies and matāuranga Māori will be employed to ground student learning in
the context of Aotearoa
• Research led teaching that is grounded in scientific evidence and transdisciplinary in nature
• Col aborative and enquiry-based learning pedagogies along with work-integrated learning, are
core for health professional work readiness
• Student choice and a wide range of learning experiences and pathways will be available
Delivery of learning
• A mixture of small group, hybrid, and experiential methodologies, supplemented by online
material will be used to deliver a high-quality learning experience
• Where practicable, small groups and small cohorts wil be used to maximise col aborative learning
and a nurturing learning environment
• Simulated and clinical skills learning experiences will ground contextualise student learning and
prepare health professional students for learning in clinical environments
25
8
A Proposed Way Forward
8.1 An FMHS Undergraduate Degree
Figure 4 below shows the current and proposed future state with the inclusion of the new BMedHSc
degree.
Figure 4: Current and Proposed Future State of Programmes
Figure 5 below shows the schematic of a proposed FMHS new undergraduate degree that would act
as a feeder to graduate entry healthcare prorammes.
Figure 5: Proposed New Bachelor Medical & Health Science (BMedHSc) Degree
26
There is a tension between clinical discipline-specific knowledge and skills (i.e., medicine, nursing,
pharmacy, optometry, etc.) and shared and/or interprofessional knowledge and skills. If a three-year,
interprofessional undergraduate degree is of value to the professions, then it must have covered
essential skil s and knowledge. Therefore, that should be a legitimate rationale for reducing the
number of subsequent years required for discipline-specific learning (rather than grafting of the same
number as currently). Discipline-specific years in all programmes will also need radical revision if the
three-year undergraduate programme precedes them. The three-year BMedHSc programme will also
need sufficient content to prepare students who do not choose a health professional career pathway
for careers in Health (and health science).
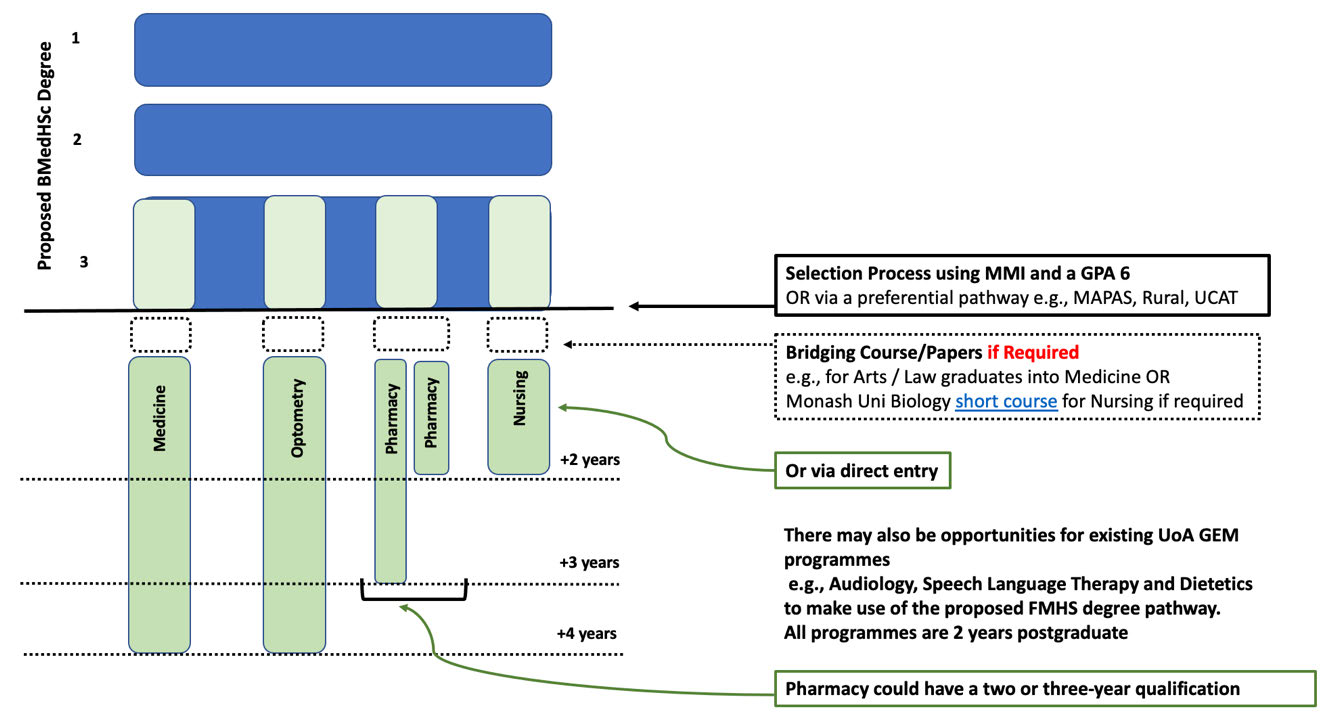
Figure 6 below shows more detail of the proposed health professional stream as a graduate entry
option for the four health programmes currently under consideration.
Figure 6: Proposed ‘Health Professional Stream’ Graduate Entry Pathway Options
A proposed draft graduate profile for the new degree has been developed (refer Table 4 below),
taking into consideration current work around the curriculum transformation project.
27

Table 4: Bachelor Medical & Health Sciences - Draft Graduate Profile
•
Demonstrate a commitment to practice in accordance with Te Tiriti o Waitangi in the context of
i
improving Indigenous health and upholding Indigenous rights by appropriately engaging with
Māori individuals, whānau and communities
āor
•
Apply the knowledge of historic, demographic, socioeconomic, and policy influences on health
ra)
status to explain how ethnic inequalities in health are created and maintained and how they may
Te A
be reduced and eliminated.
a M om • Critique the influence of one’s own culture and that of the health system on patient and
(fr
population health outcomes to continually reflect on one’s practice and actively participate in self
audit in respect of the Te Tiriti
auor
•
Identify and address professional development needs as a basis for life-long learning about Māori
H
health
•
Draw on a broad scientific body of knowledge encompassing biological, behavioural, and social
sciences to explain the normal structure, function and development of the human body and mind
at all stages of life, the factors that may disturb these and the interactions between body and mind
ces
•
Explain how social, political, economic, environmental, and cultural determinants: (1) influence
morbidity and mortality that affect the health and wel being of whole populations; and (2) could
potentially prevent diseases, disability, and injury
cien
•
Apply the scientific body of knowledge appropriately to address sustainability and sustainable
practices, explaining the causes and consequences of climate change, adaptation, and mitigation
lin)
C
strategies pertinent to Aotearoa and the South Pacific
lth/ S
•
Demonstrate an understanding of the role of data science, machine learning, artificial intelligence,
BSc +
and advanced technologies in the context of human health and wel being
ea c + • Demonstrate the ability to communicate about risk in an environment of uncertainty through
HS
reasoned arguments and interpretations constructed by locating and evaluating information, and
s / H B
analysing qualitative and quantitative data about health
•
Apply disciplinary theory, analysis, research, and creative skills in seeking solutions to complex
(from
health problems and inequities
tion
•
Form and evaluate research strategies, including developing research questions, and discern and
assess possible methods for answering them, demonstrating independent critical thought
ula
•
Take a systems-based approach to designing responses to chal enges in health, health systems and
society
Pop
•
Appraise national and global dimensions of intellectual, political, environmental, and economic
activities affecting health
•
Use, manage, present, and communicate information effectively using clear English and/or Te Reo
Māori in a range of media and formats
•
Demonstrate understanding of self in relation to others, reflecting on one’s own and others’ world
viewpoints and principles of cultural safety
kills
•
Build and enable respectful and sustainable collaborative relationships to improve health within
S
diverse communities
•
Recognise the responsibilities associated with autonomous academic inquiry and engage in
scholarship respectful y and constructively
onal and
ation
•
Identify the ethical dimensions of contexts, actions and policies and draw upon ethical theory to
formulate and justify principled responses
fessi
unic
•
Navigate personal, academic, and professional challenges with integrity, taking responsibility for
m
academic and professional decisions, conduct
Pro
•
Use appropriate teaching and learning strategies to educate themselves, peers, other professionals
Com
working in health and the community
•
Lead and be advocates of health in a diverse community, including accepting social and civic
responsibilities
28
8.2 Selection
There has been robust debate regarding a selection process for any graduate entry programme, with
the major concern being that it is not good enough to merely shift the ‘pressure point’ from the
current OLY1 process to (potentially) the end of a three-year degree, without other factors also
changing. It is widely acknowledged that the competitive nature of the current OLY1 selection process
does not promote the types of attitudes and behaviours needed from our future healthcare
professionals, and is significantly detrimental to students’ health and well-being. This must change.
The most competitive programme entry currently is medicine. Options for selection that have been
debated have included:
• School leaver entry (confirmation of medical school place, subject to meeting required academic
and professional practice requirements) on entry to a proposed new FMHS undergraduate degree
• A weighted ballot for entry to the medical programme (like the Netherlands model)
• Graduate entry pathways
• Graduate entry pathways with/without a bridging programme
• A range of GPA scores
It is currently proposed that:
• The current preferential entry pathways for MAPAS students, students from regional and rural
backgrounds and those via the undergraduate targeted admissions scheme (UTAS) remain
unchanged,
• Other criteria include a minimum GPA of 667 and
• An interview process inclusive of an MMI.
Māori and Pasifika Student Selection
It has been chal enging to find any commentary regarding the ability (or otherwise) of graduate entry
programmes to address the lack of ethnic diversity in healthcare programmes, particularly for
indigenous populations where there are increased health disparities compared to the dominant
colonial culture(s).
A study of over 500 undergraduate and graduate entry physical therapy graduates in the USA in the
early 1990s concluded that the undergraduate programmes appeared to attract a greater percentage
of ‘minority’ individuals (14.9% versus 5.8%, respectively)68. A single-site study in the UK also found
that ethnic minority (non-white) applicants formed a smal er proportion of applicants for the
graduate entry compared to the undergraduate programme (31.7% versus 39.8% respectively)69. A
large multicohort study looking at applicants to UK medical schools from 2006 – 2014 found that
‘the
odds of getting an offer to study medicine were lower if the applicant was male, graduate, from black
and minority ethnic background and from lower socioeconomic groups’70.
67 Note that this proposed GPA score is higher than the GPA required for the MNurs Sci programme (refer Table 2 above).
68 Warren SC, Pierson FM. Comparison of characteristics of entry-level bachelor’s and master’s degree students in physical therapy. Physical
Therapy (1994). 74:4
69 James D, Ferguson E, Powis D, Symonds S, Yates J (2008). undergraduate and graduate entry to medicine: widening academic and socio-
demographic access.
Medical Education. 28: 294 – 300.
https://dx.doi/org/10.1111/j.1365-2923.2008.03006.x
70 Kumwenda B, Cleland J, Greatix R, MacKenzie RK, Prescott G (2018). Are efforts to attract graduate applicants to UK medical schools
effective in increasing the participation of underrepresented socioeconomic groups? A national cohort study.
BMJ Open. 8:e018946.
https://dx.doi.org/10.1136/bmjopen-2017-018946
29
What is known from UoA published research regarding health professional study (non-graduate
entry) for BHSc, BNurs and BPharm is that:
Ethnic disparities in academic outcomes show patterns of privilege and should be alarming to
tertiary institutions. If institutions are serious about achieving equitable outcomes for Māori and
Pacific students, major institutional changes are necessary that ensure the unique needs of
Māori and Pacific students are met (Wikaire et al, 2016) 71.
Of ongoing and significant concern to the non-medical programmes is their lack of students from
Māori and Pasifika backgrounds, as those students who are successful via the OLY1 process will
almost invariably go into medicine. For example, the optometry school offers 150 places to fill 60, but
the top ranked students invariably go to medicine and attracting Māori and Pasifika students is almost
impossible. A key principle of this work (refer Appendix Three also) is shown below:
‘Any change to education must enhance the participation and ultimately graduation of Māori and
Pasifika people in health professional education. This means that any consideration of proposed
change has an equity lens applied as a first principle. To avoid doubt, no change to the delivery of
healthcare professional education should create further barriers for Māori and Pasifika people’
Feedback from one Australian stakeholder at a medical school commented
‘graduate entry healthcare
programmes are about contesting status, rather than aligning to community needs’. We need to be
cognisant of this perspective when engaging with and considering feedback from Māori and Pasifika
communities and stakeholders.
This means that the wider work must continue and expand to support Māori and Pasifika tamariki to
be successful in science subjects at high school, including exposure as early as possible to the wide
range of health careers available at the UoA. The Hikitia Te Ora - CertHealthSci may also remain
important to ensure students have good foundation skil s before commencing tertiary programmes,
as wel as ongoing MAPAS pastoral and academic support. Additionally, ongoing work to address the
lack of diversity in the teaching staff and student body, and addressing implicit and explicit
institutional racism is both necessary and essential if these programmes are going to attract, retain,
and successfully graduate Māori and Pasifika students72 73.
8.3 Pre-Requisites for Graduate Entry Health Professional Programmes
Potential bridging courses / papers (pre-requisites) for each health professional programme are still
to be determined, and could be different depending on where (and when) the student’s
undergraduate degree was completed. Appendix Four contains details of current pre-requisites for
the G8 universities for each in-scope health programme. Australia has the ATAR74, which provides a
71 Wikaire E, Curtis E, Cormack D, Jiang Y, McMillan L, Loto R, Reid P. Patterns of privilege: A total cohort analysis
of admission and academic outcomes for Māori, Pacific and non-Māori non-Pacific health professional students. BMC Education (2016).
16:262 https://dx.doi/org/10.1186/s12909-016-0782-2
72 Reid P, Cormack D, Paine S-J. Colonial histories, racism and health – the experience of Māori and indigenous peoples. Public Health (2019).
172; 119 – 124
73 Morrison N, Machado M, Blackburn C. Student perspectives on barriers to performance for black and minority ethnic graduate-entry
medical students: a qualitative study in a West Midlands medical school. BMJ Open (2019). 9:e032493
74 The ATAR is the primary mechanism used nationally in Australia for tertiary admissions and indicates a student’s position relative to other
students. It is the standard measure of a student’s overal academic achievement in relation to other students where these students have
studied different subject combinations. ATARS are expressed as a number on a 2000-point scale from 99.95 down to 0.00 in steps of 0.05.
30
standardised comparable rank between students, and al programmes set a minimum ATAR for
admission.
The G8 graduate entry medical programmes al require students to complete an undergraduate
degree, and some also specify subjects (UQ, UWA, Uni Melbourne and Uni Sydney). University of
Sydney is the only university that offers an online foundational knowledge course is available to all
students on enrolment to ensure assumed knowledge in anatomy, physiology, molecular and cell
biology is met, and 20% of their MD students come from non-biomedical science educational
backgrounds.
Given that there are only two medical schools in Aotearoa and 48% of the UoA 2021 intake (year two
of the MBChB) are graduates, flexibility for student options to enter the programme will need to be
considered to maintain the diversity of student backgrounds and experience that is beneficial for our
future doctors.
Box 2: Analysis of the current MBCHB Year Two cohort of 264 domestic students (2021)
•
45% of all students have come through a UoA pathway
•
48% of the class (127 students) are graduate entry
•
The majority education provider for previous qualifications for the graduate entry cohort was UoA (68
students), followed by Otago University (44 students)
•
Most graduate entry students came from a science background (50%), fol owed by ‘other’ (24%),
health sciences (14%) and biomedical science (11%)
•
Within the ‘other’ cohort were 15 students with previous healthcare qualifications: pharmacy (5),
nursing (4), physiotherapy (3), oral health (2) and podiatry (1)
•
45% of the class came through OLY1
•
18 students completed the Cert in Health Science
[scope]
31
8.4 Māori and Pasifika Student Feedback
Fifteen 3rd, 4th and 5th year Māori and Pasifika medical students participated in a zoom meeting
specifically to discuss and share their feedback on this proposal75. Overall, the students liked the
concept of diversity of graduates entering health careers and felt this was a positive move.
We bring our families with us and it plays a big role in what we do, how long we do it for, and what
ends up being given back to our families and communities. Seven years is an extra year, and Māori
and Pasifika students are more likely to be in poorer areas of education, from low decile schools -
then that would make it eight years. Time, money, living in Auckland. What would you do to help
Māori and Pasifika students? (Student participant)
Student feedback centred on their concerns regarding the increased length of study required to
register as a health professional, but there were other themes and these are summarised below:
• Increased length of the medical programme (3 + 4 years), and added another year if the CertHSc
needs to be completed
• Burnout for students - related to additional length of time studying and associated stresses
• Living and training in Auckland (e.g., cost of living, housing), with concerns about any potential
increase in the cost of training (with additional years)
• Is the vision of what you are trying to achieve worth lengthening of training?
• Could students study a different UG degree (or this degree via distance learning) closer to home,
then enter the pathways for health professions at UoA?
• The main barrier for Māori and Pasifika students is getting to university in the first place. High
school preparation for Māori and Pasifika students (many of whome come from low decile
schools) is inadequate, which is why the CertHSc is currently important
• High school students do not receive good knowledge about the range of health careers available
and this impacts their choices (coupled with whānau/family pressure) as medicine is seen as a
good (prestigious) career where you can earn good money
• Some people would still want to do an UG pathway for a health career as it’s shorter e.g., nursing
• Māori and Pasifika students need support and a safe space to achieve academically. Would you
increase programmes and funding to MAPAS to enable Māori and Pasifika students to reach their
potential?
• In terms of selection criteria, some students felt an interview would be good to include, as well as
the MMI. There was also Feedback that aptitude tests are another barrier for Māori and Pasifika
students (compared to Australian indigenous student medical school selection processes)
[scope]
32
[s 9(2)(k)]
36
37
[s 9(2)(k)]
39
8.8 Transition Considerations
How the cohorts of students wil move through the years of study have also been modelled, looking at
when the current structure ends and when the new one begins. The two programmes with significant
transition considerations are medicine and pharmacy, and these are discussed in more detail below.
A key operational constraint is related to the medical programme clinical placements, currently
limited to 900 placements. Modelling has been conducted to account for this constraint in years 4-6
of the current MBChB programme and years 2-4 of the proposed MD programme.
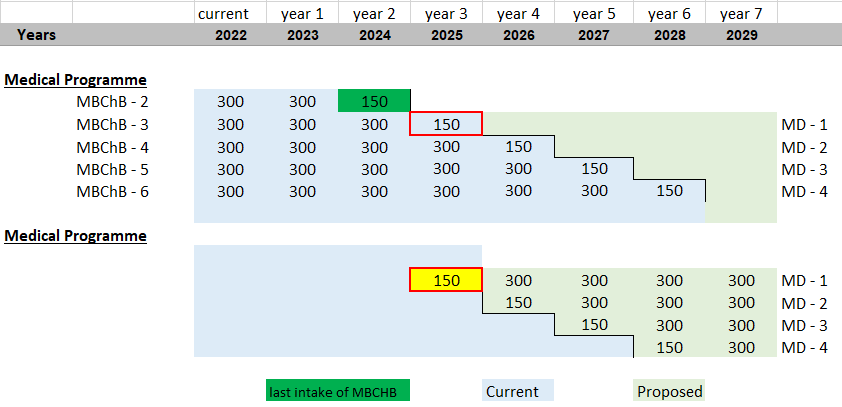
Figure 10 below shows the transition modelling for all programmes and includes a ‘Gap Year’ for
medicine. In this model, there is a year of ‘no intake’ of medical students into either of the medical
programmes. In this example, Figure 10 shows no students in MBCHB 2 or MD 1 in 2025. This al ows a
continuous supply of graduates each year, without exceeding (clinical placement) capacity. There will
be a transition year in 2023 at the undergraduate level al owing a cohort of students to proceed into
the second year of the BMedHSc if they do not gain entry into the first year of the MBChB programme
for 2024. A gap year approach would result in a revenue drop in Year 3 as a year of TEC SAC funding is
lost, with no new students entering the medical programme in 2025.
Figure 10: Transition Model ing Showing the ‘Gap Year’ for Medicine
current
year 1
year 2
year 3
year 4
year 5
year 6
year 7
Years
2022
2023
2024
2025
2026
2027
2028
2029
UG Entry OLY1
x
x
x
x
x
x
x
x
BMHS 1
x
x
x
x
x
x
BMHS 2
x
x
x
x
x
BMHS 3
Medical Programme
MBChB - 2
300
300
300
gap
MBChB - 3
300
300
300
300
300
300
300
300
MD - 1
MBChB - 4
300
300
300
300
300
300
300
300
MD - 2
MBChB - 5
300
300
300
300
300
300
300
300
MD - 3
MBChB - 6
300
300
300
300
300
300
300
300
MD - 4
[scope]
transition
Current
Proposed
Note:
2022 OLY1 - entry to Medical/Pharmacy/Optometry
2023 OLY1 - entry to BMHS 2/Medical/Pharmacy/Optometry
2024 OLY1 - entry to BMHS 2/Pharmacy/Optometry
40
Alternative Model for Medicine
An alternative ‘Reduced Intake Model’ was also explored (Figure 11 below), which would al ow both
the MBCHB and MD programme to run concurrently by halving each of the intake to maintain a class
size of 300. This would mitigate the pressure on clinical placement years and enable the Faculty to
iron out of any wrinkles in the new degree during early implementation.
Figure 11 demonstrates the last intake of MBCHB in 2024 and the first intake of MD in 2025. This
model has two elements of double-teaching which will require further investigative work:
i.
At the undergraduate level when there will be students yet to complete their qualification
under OLY1 while students are beginning BMedHSc; and
ii.
When MBCHB Y3 is taught at the same time as MD 1, which makes this model more
challenging to adopt
Figure 11: Medicine Only ‘Reduced Intake’ Model
There are additional issues for medicine that will also require consideration:
• International opportunities to ‘twin’ with an offshore university to deliver MD 1 and MD 2 in New
Zealand, where the student returns home for their clinical placement to complete their MD. This
would enable FMHS to exceed the intake of international students into medicine (currently
between 20-25 students a year)
• The number of graduate entry places into the proposed MD would further enlarge the revenue
loss position as they won’t need to do two extra years of undergraduate degree
• Depending on the transition model selected, the implications of any peak in medical graduates
would need to be discussed with Health NZ
• What proportion of the EFTS will come to FMHS for students doing BMedHSc 1,2,3 who don’t go
on to a health professional programme, and how that wil be distributed across the FMHS
schools?
• If there is a very careful y crafted BMedHSc 1,2,3 is another 4 years of MD required? Could it be
done in three years?
41
• The cost of the MD has not yet been examined. Consideration needs to be given to any
incremental increase in teaching costs, transition time, staffing, additional capex investment
[scope]
42
Capacity
Further understanding of existing capacity of staffing and physical assets will be required for all
programmes, and how the transition may impact on operational constraints. These factors include
the need to balance being operationally achievable and financially acceptable, while delivering on
required demand for quality graduates during the transition phase.
Other Transition Issues
Other transition matters that wil require further consideration include:
• Cost of course development requirements is unknown at this stage however there will be a
degree of building on current course material
• The transferability of content covered in OLY1 to BMedHSc
• Duplicated teaching costs during transition – details yet to be worked through
• Current CAPEX capacity and any additional CAPEX that may be required
• Response (or otherwise) by the University of Otago (medicine and pharmacy)
43
[scope]
44
[scope]
45
Appendix Three
Proposed Guiding Principles for Future Healthcare Professional Education
(Last updated 18 September 2021)
1. Education and training in all the Health disciplines remains fundamentally a science-based
curriculum that espouses the principles of the scientific method and quantitative evidence-based
evaluation and decision making. There is nevertheless a need to expand the curriculum to ensure
future Health graduates have a wider appreciation of local and global factors that determine the
health of society.
2. The UoA FMHS aims to be the leading health professional education provider in Aotearoa,
graduating health professionals who are employable in a wide range of settings and able to
pursue a wide variety of careers
3. Any change to education must enhance the participation and ultimately graduation of Māori and
Pasifika people in health professional education. This means that any consideration of proposed
change has an equity lens applied as a first principle. To avoid doubt, no change to the delivery of
healthcare professional education should create further barriers for Māori and Pasifika people
4. All education provided by the FMHS must affirm, and actively prevent the erasure of, people with
LGBTQI/Takatāpui+82 identities. Moreover, any changes to education must reflect that our faculty
is committed to instilling in our graduates a robust knowledge of LGBTQI/Takatāpui+ identities
and an understanding of health disparities and barriers affecting these communities
5. Learning and practicing cultural safety is the central to future health professional education
6. Future healthcare professional education needs to prepare students for the greatest health
challenges they may face. These include but are not limited to:
a. Climate crises and the implications in the South Pacific
b. The ongoing effects on health of inequity, racism, and colonisation
c. Ageing population with more complex health and social needs
d. Changes in technology and how to leverage those changes to improve health
e. Rapid changes in knowledge (e.g., genetics, AI, data science) and how to manage new
information into existing practice, that can be applied to individual patients
f. Managing complexity, uncertainty, and limited resources with the patient at the
centre of care
g. Understanding determinants of chronic disease, and effectively tackling the
prevention and management of such diseases
82 The LGBTQITakatāpui+ community includes people who identify as Takatāpui (‘Intimate partner of the same sex’), lesbian, gay, bisexual,
queer, intersex, transsexual, transgender, whakawahine, tangata ira tāne, māhū (Tahiti and Hawaii), vakasalewalewa (Fiji), palopa (Papua
New Guinea), fa’afafine (Samoa, American Samoa and Tokelau), akava’ine (Cook Islands), fakaleiti or leiti (the Kingdom of Tonga), or
fakafifine (Niue). https://www.auckland.ac.nz/en/on-campus/student-support/personal-support/lgbti-students/support-lgbti-students.html
[Accessed 14 September 2021]
46
7. Learning and working in multi professional teams wil be built into the future healthcare
professional education. This means creating opportunities for future healthcare professional
students to learn together in an environment that is mana enhancing for al students
8. Structures and systems wil need to be in place to ensure that student wel being is ensured and
well catered for
9. Pathways will be created to allow students to choose different learning opportunities e.g.,
research pathways, longitudinal rural placements
10. There will be early opportunities for students to be exposed to the clinical environment. The
purpose of this early clinical exposure is to enable students to understand the broad range of
careers available to them as future healthcare professionals
11. Selection strategies must actively consider ways of minimising competition, recognising that their
will inevitably be some competition, unless a (weighted) bal ot system is adopted
12. The FMHS has autonomy over the structure and content of health professional education and
collaborates with faculties that deliver health professional education. This will enable flexibility,
adaptability of teaching and learning
13. Where possible, interprofessional teaching and learning will occur to ensure effective and
efficient use of resource across the faculty
14. Allow for students to exit degrees/programmes early with options to obtain a valuable
qualification
47
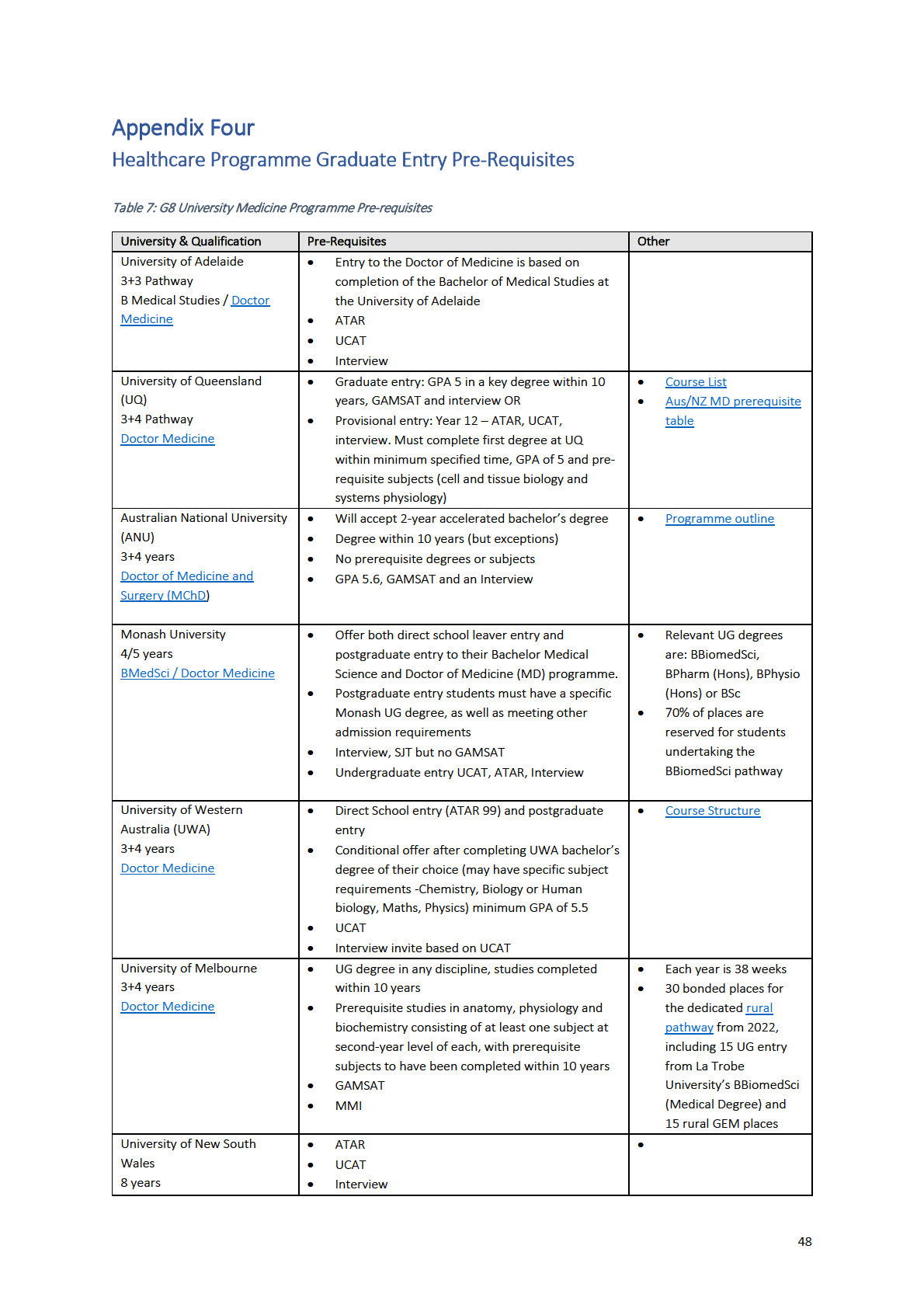
B Med / MD / Arts
•
NO GRADUATE entry (except as below)
•
UNSW Medicine’s Lateral Entry Scheme is a
graduate-entry stream into the BMed/MD, only
for domestic UNSW Bachelor of Medical Science
(BMedSci) students
•
BMedSci students apply second year of study. If
application is successful, required to complete the
BMedSci then undertake a Science Honours year
before entry MD
University of Sydney
•
This double degree medicine pathway combines
•
20% of Sydney's MD
3+4 Pathway
the MD with an undergraduate degree in arts or
students come from
Doctor Medicine
science. Arts students need to complete all
non-biomedical science
requirements for the Bachelor of Arts, including
educational
the designated foundational knowledge units for
backgrounds
medicine offered by the Faculty of Science within
three years.
•
An online foundational knowledge course is
available to all students on enrolment to ensure
assumed knowledge in anatomy, physiology,
molecular and cell biology is met
•
GAMSAT
[scope]
49
[scope]
50
[scope]
51
[scope]
52
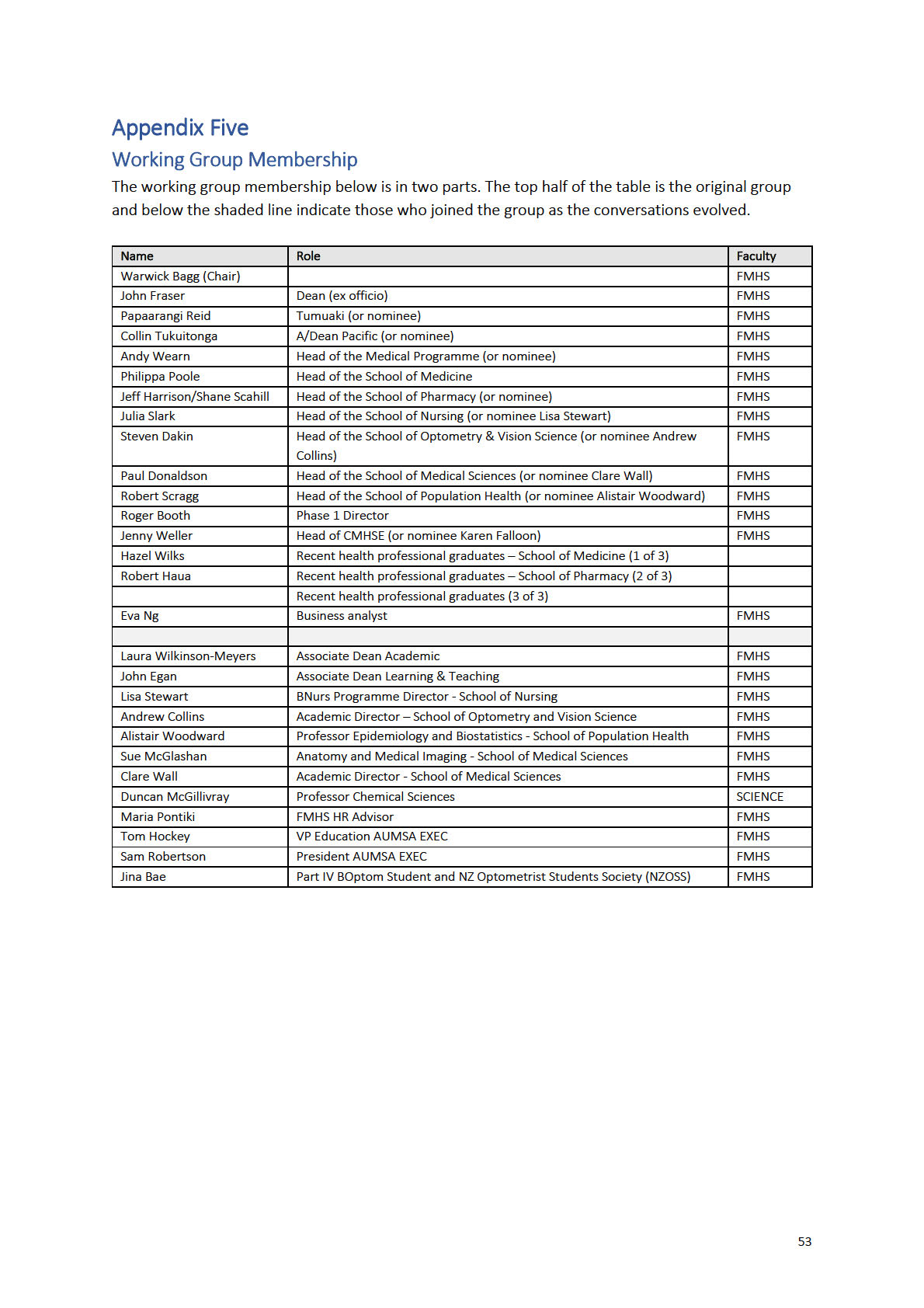
Appendix Six
School of Biological Sciences Feedback on Draft Report
We thank FHMS for sharing their Future of Healthcare Professional Education draft working group
report with us. Here is our feedback around some key questions that we see as important, specifically
regarding the Biomedical Science Programmes.
Key Questions
1. Does one undergraduate program provide sufficient capacity to incorporate the depth and
breadth required for both the Biomedical and Health Sciences?
In the proposed UG degree program there is justifiably considerable emphasis on the population
health issues currently facing NZ and the world. We are concerned that there would not be sufficient
capacity to incorporate the diverse field of Biomedical Science into this same program. Biomedical
Science studies the biological processes that underpin human function, health, and disease, and the
treatment of disease, and is hence a diverse multidisciplinary field. This is reflected by the nine
discipline focused pathways in the recently restructured UoA BSc in Biomedical Science* and
furthermore by the multiple discipline-based majors offered by other academic institutions in their
Biomedical Science and Medical Science programs i.e. Universities of Sydney, Melbourne, New South
Wales, Otago (NZ) & Oxford (UK).
To provide the depth and breadth required for these Biomedical Science pathways/majors the UoA
together with the aforementioned academic institutions allocate a large proportion of these
programs for the delivery of core or elective Biomedical Science courses. For example, UoA BSc
Biomedical Science students take 6 stage II and 5 stage III Biomedical Science courses, the course
combinations for which are prescribed for each pathway. Overall, the UoA BSc Biomedical Science
includes 11 stage II and 26 stage III courses, further reflecting the diversity of this field.
To remain internationally competitive, we therefore need to continue to offer multiple discipline
based Biomedical Science pathways/majors and dedicate enough of the program to these
pathways/majors ensuring our students graduate with a qualification comparable to their
international counterparts.
Another important point to highlight about the Biomedical/Medical Science programs provided by the
Universities of Sydney, Melbourne, New South Wales, Otago (NZ) & Oxford (UK), is that they all
include substantial amounts of cell & molecular biology, chemistry, biochemistry and genetics in their
1st year, some also extend this into years 2 to run in parallel & compliment major. This highlights the
importance of providing students with a sound understanding of the basic biological and chemical
process in the human body to support their transition into the more specialised pathways/majors in
Biomedical Science. The current UoA BSc Biomedical Science also includes a large amount of this
material at stage I to underpin the subsequent specialised studies in the pathways.
54
* Restructured UoA BSc Biomedical Science pathways
SMS (FMHS) BSc Biomed Sci designed pathways:
Anatomical Imaging Science
Cancer Biology and Therapeutics
Cardiovascular Biology
Infection & Immunity
Neuroscience
Nutrition & Metabolism
Reproduction and Development
SBS (FoS) BSc Biomed Sci designed pathways:
Cellular and Molecular Biomedicine
Genetics
NB: all the above pathways also include a Quantitative Biology course (BIOSCI 220)
2. Wil there be a pathway to ensure that students graduating from UG Biomedical studies can
seamlessly transition into PG Biomedical Science studies?
Many of the career paths that Biomedical Science leads to (e.g. medical researcher, clinical trial
administrator/scientist, pharmaceutical scientist, science writer/communicator, policy advisor), also
require students to have taken PG Biomedical Science programs (this trend is evident internationally);
therefore students graduating from this program need to have sufficient background in Biomedical
Science and basic laboratory skills to embark on PG Biomedical Science studies.
SMS (FMHS) has designed a very successful suite of PG Biomedical Science programs
(PGDipBiomedSci, MBiomedSci and BBiomedSciHons), which many of our BSc Biomedical Science
students transition into, furthermore some of our students go to Otago or overseas for their PG
Biomed studies. We need to ensure that we adequately equip our UG Biomedical Science students so
they can transition into these PG Biomedical Science programs. Given what has been discussed above,
can a combined Health and Biomedical Science degree prepare students for PG Biomedical studies, as
their Biomedical Science knowledge and skills may not be comparable with their NZ or international
counterparts?
3. Does FMHS have the staff, resource and building capacity to run a combined Biomedical and
Health Science Programme?
Table 13 below shows the increase in stage I enrolments in the BSc Biomedical Science program, and
further shows retention in years 2 and 3 has also increased. Collectively these factors have led to
elevated numbers in this program and financial benefits for the UoA. If we were to switch to a
combined Health and Biomed program, would we be able to maintain this level of student capacity? If
so, how would this work? For example, teaching distributed between FMHS and FoS to accommodate
similar student numbers so the UoA doesn’t suffer what could be substantial financial losses?
Alternatively, if Biomedical Science and Health Science continued to be delivered separately, but both
incorporated some common courses over the 3 years that were deemed to be essential by FMHS
professional programs, could both be feeder programs for PG entry into the professional programs?
55

Each program could then make changes in response to the curriculum transformation, address
curriculum scaffolding issues caused by OLY1 and incorporate & scaffold in key courses deemed
necessary for professional program entry. This would help retain student capacity (and maybe
minimise financial losses) and the professional programs could recruit graduates from these two
programs using the GPA and interview criteria detailed in the FMHS proposal.
N.B. if we change to entirely PG professional program entry, we will inevitably see changes in UG
student numbers across stages I, II & III. But by ensuring capacity is available we would be better
placed to deal with these changing student numbers and navigate our way through the transition
period (when new and old programs are delivered simultaneously).
Table 12: Number of students enrol ed in BSc Biomedical Science
Note: Figures in grey calculated previously, using different parameters compared to 2020 and 2021
4. You describe a new graduate profile and education mega-trends but don’t specifically comment
on the pedagogies you will be using to teach into the new programme. What wil these be?
This also relates to the capacity question, and if the programme will be EFTS driven or limited in
places. There is a lot of information in the review on medical educational programmes, but not on the
quality of teaching within them or the breadth of pedagogies used. How will you align Taumata
Teitei’s desire for student-centered, inclusive teaching into what may still be large classes with a
competitive cohort in the UG programme? How are you planning on changing traditional didactic
teaching pedagogies and assessment practice to be in line with the scholarship of teaching and
learning research into best practices in higher education? How will you upskill your academic staff to
be able to teach these new courses, specifical y in the Mātauranga Māori space with so few Maori
academic staff members? How will you manage these large-scale changes in teaching within current
staff workloads?
5. We are pleased to see that adverse impacts on other Faculties has been included in your Threats
Analysis
We would like to continue working in good faith with FHMS in order to provide the best education
possible for students that span our faculties, and ask to be included in working groups where possible.
There is considerable expertise in the School of Biological Sciences in the areas of computational
biology, microbiology, microbial ecology, conservation and climate change. Al areas of importance in
population health and the future medical workforce described in your review document. We can
contribute with research-led teaching into these transdisciplinary curriculum areas and would like to
be involved with curriculum building in these areas.
56