18 August 2022
 Aotearoa New Zealand’s Strategic Framework for COVID-19
ACT 1982
Variants of Concern
Aotearoa New Zealand’s Strategic Framework for COVID-19
ACT 1982
Variants of Concern
Effective June 8 2022
Previous versions
INFORMATION
Initial draft version
6 May 2022
Initial draft updated for engagement
11 May 2022
Engagement on the plan
Strategic COVID-19 Public Health Advisory Group 18 May 2022
COVID-19 Technical Advisory Group
20 May 2022
COVID-19 Independent Continuous Review,
24 May 20222
Improvement and Advice Group
RELEASED UNDER THE OFFICIAL
 Contents
Contents Aotearoa New Zealand’s Strategic Framework for COVID-19 Variants of Concern ...................................... 1
I.
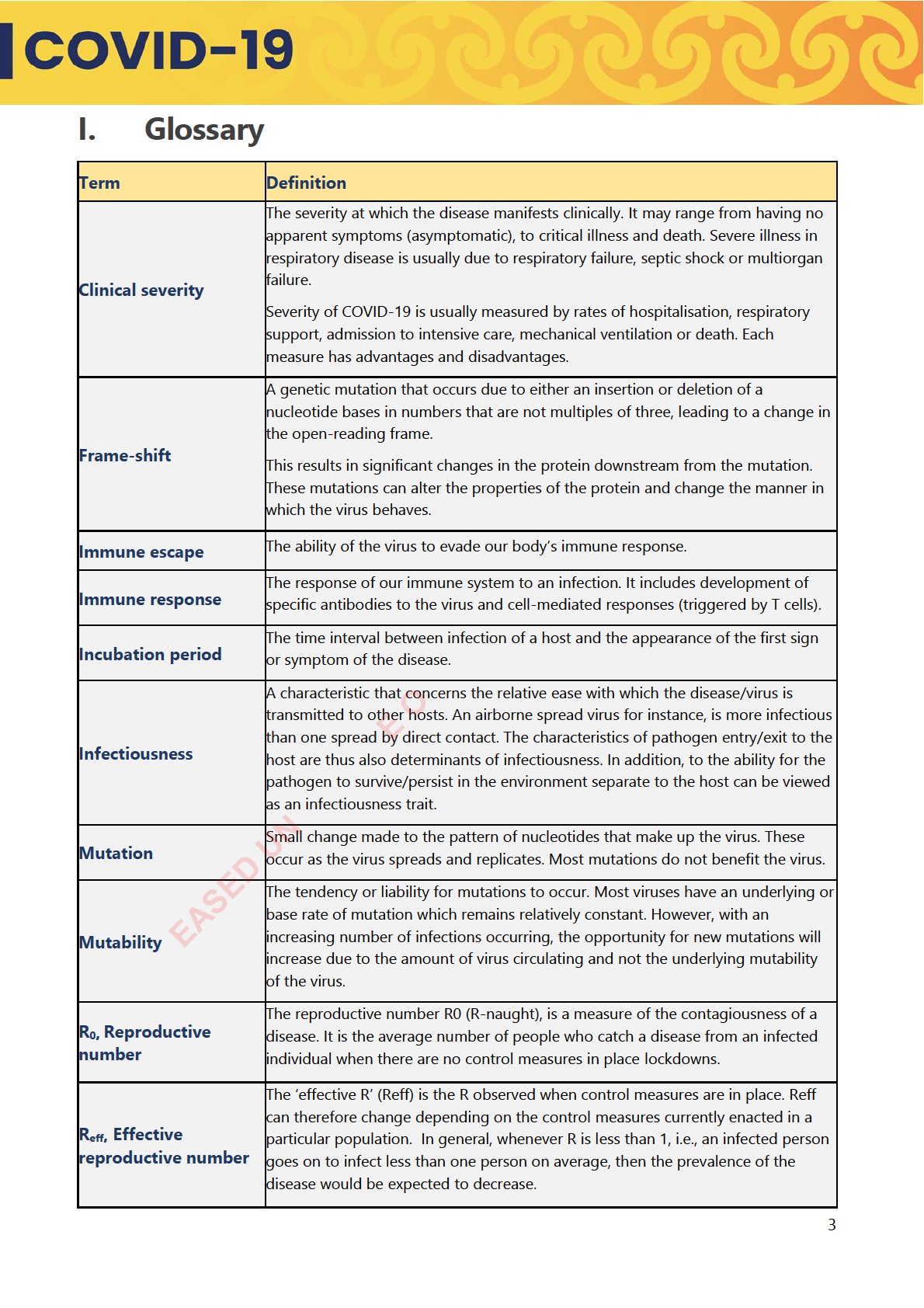
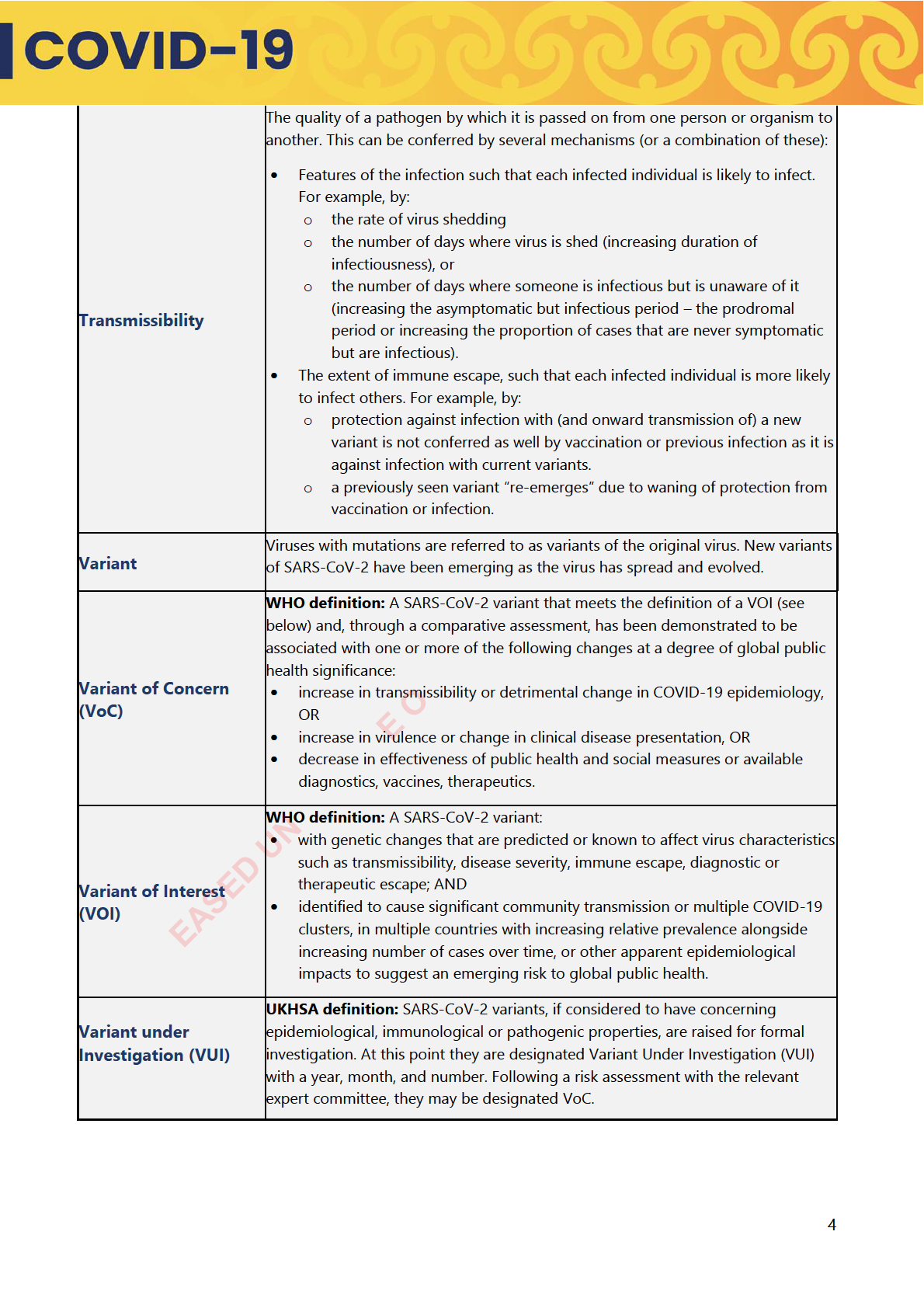
Glossary ........................................................................................................................................................................... 3
II. Executive summary ................................................................................................................................................... 5
III. Purpose ........................................................................................................................................................................... 7
IV. Context ............................................................................................................................................................................ 8
What we know about Variants of Concern ......................................................................................................... 8
The situation has changed from March 2020 .................................................................................................... 9
V. The COVID-19 Strategic Approach ........................................................................................................... .. . 11
VI. Scenarios to inform the Strategic Framework for new Variants of Concern ............... . ......... 13
Disease characteristics and contextual factors ............................................................................ ... ............... 13
Co-circulating variants: the balance between transmissibility and immune escape .. . .................. 15
VII. The response decision-making process ......................................................................... .............................. 16
ACT 1982
The role of the Public Health Risk Assessment ....................................................... .... .................................. 16
Connection to the Al -of-Government Response ........................................... .. ........................................... 16
Preparedness wil need to factor in the absence of detailed information ........................................... 16
VIII. Responses to each of the scenarios ................................................... ... ........................................................ 18
Strategic approach to new Variants of Concern .......................... .... ........................................................... 18
Determining the best approach ..................................................... .. .................................................................. 18
Targeted approaches for particular areas and communities ..................................................................... 20
INFORMATION
Trade-offs ............................................................................... .... .............................................................................. 20
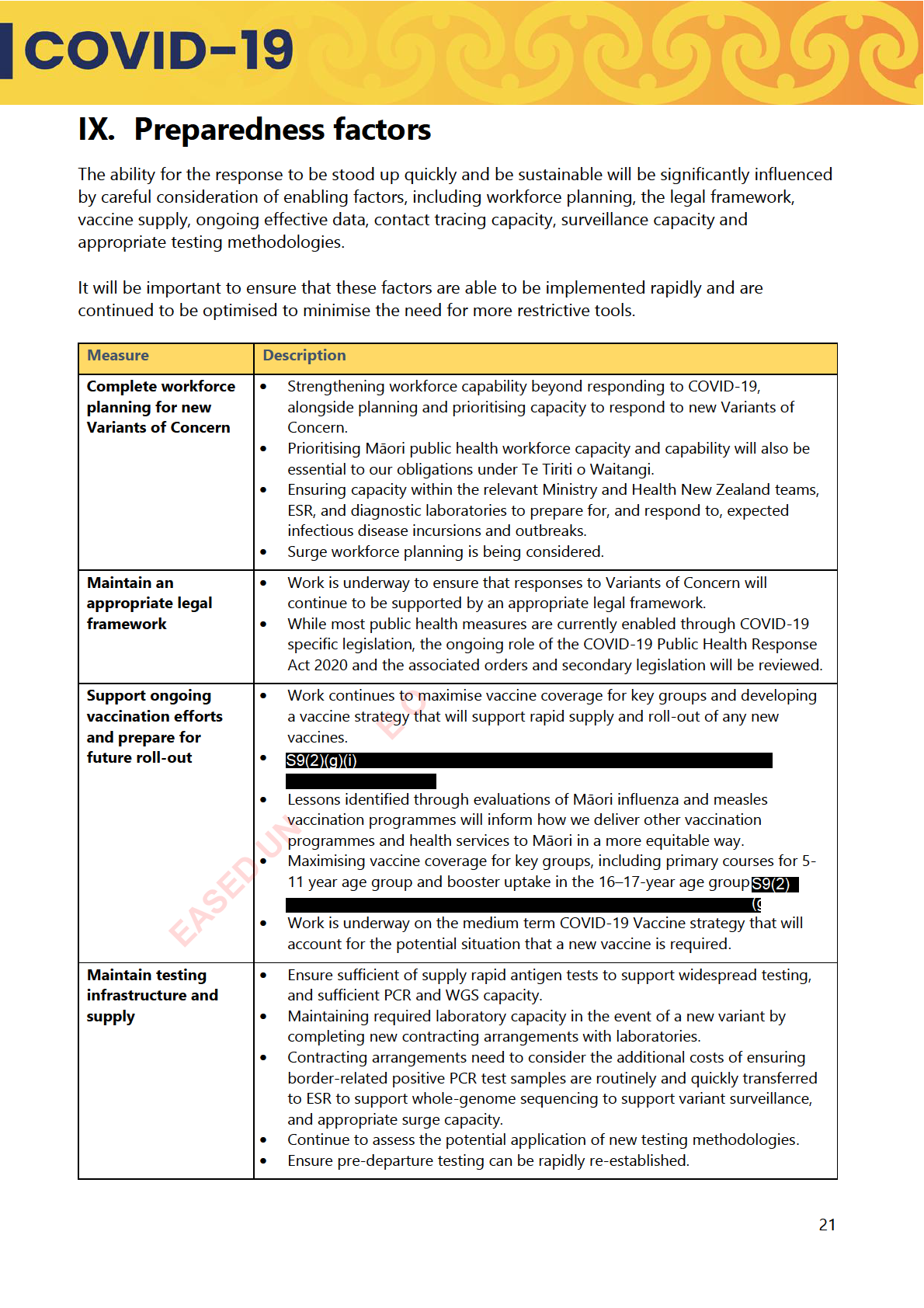
IX. Preparedness factors ................................................ ............................................................................................. 21
All-of-Government measures for consideration. ........................................................................................... 23
X. Te Tiriti o Waitangi and Equity commitments .......................................................................................... 25
Te Tiriti o Waitangi .................................. ................................................................................................................. 25
Working with Māori on design and delivery of services ............................................................................. 25
Equity 26
Devolving power and resources to communities .......................................................................................... 26
XI. Global Responses to Variants of Concern ................................................................................................... 27
Global surveil ance efforts ....................................................................................................................................... 27
International approaches to strategic planning ............................................................................................. 27
International scenario planning ............................................................................................................................ 28
Supporting Pacific states - the Pacific Health Corridors work programmes ....................................... 28
XII. Next steps .................................................................................................................................................................... 29
XIII. Appendices .................................................................................................................................................................. 30
Appendix 1: Evidence base for new variants, including information on co-circulating variants . 30
RELEASED UNDER THE OFFICIAL
Appendix 2: Modelling on Variants of Concern ............................................................................................. 36
Appendix 3: Process for Identifying New Variants of Concern ................................................................. 39
Appendix 4: Proposed response to scenarios ................................................................................................. 40
References ............................................................................................................................................................................. 41
2
 II. Executive summary
II. Executive summary
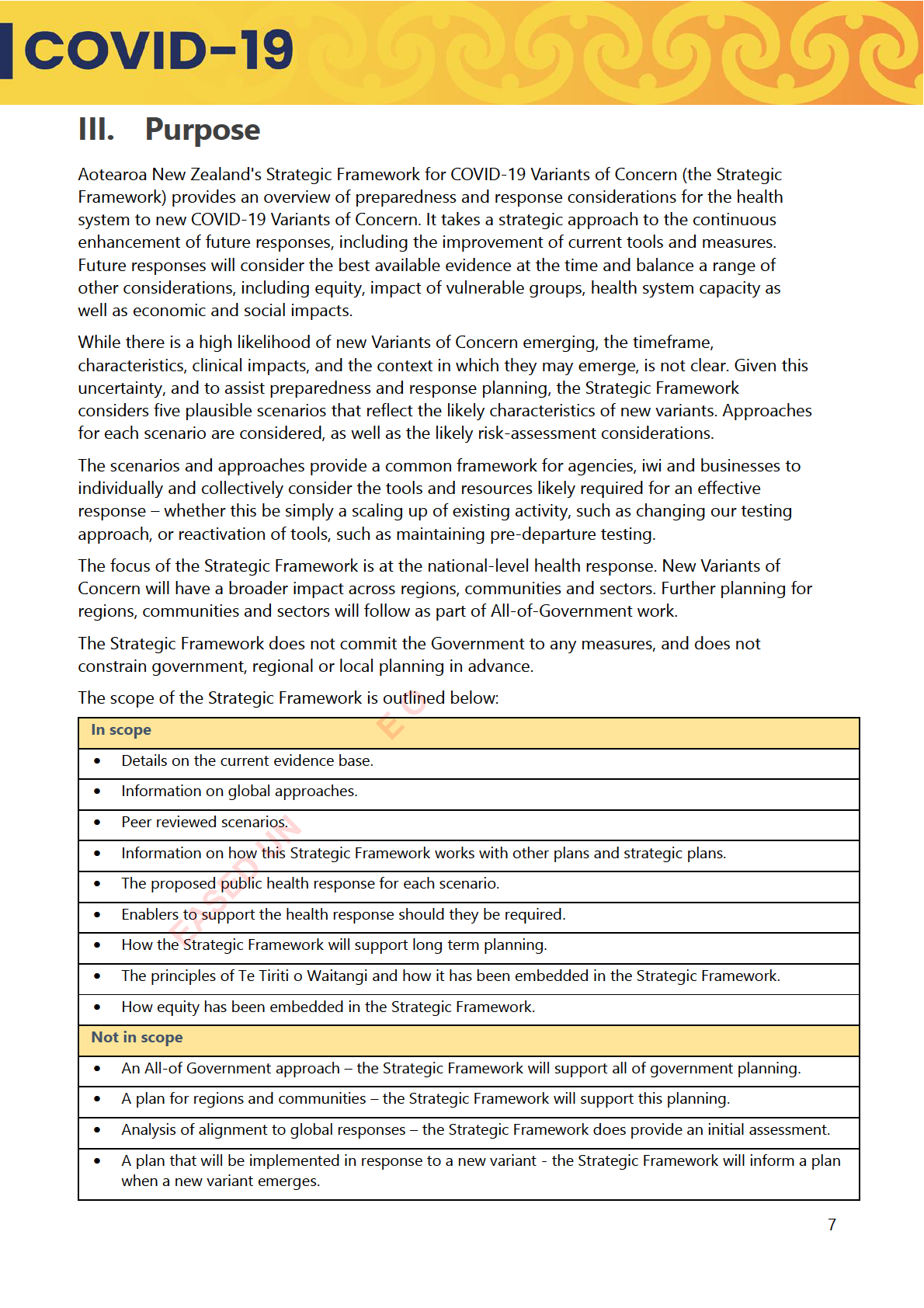
Aotearoa New Zealand’s Strategic Framework for COVID-19 Variants of Concern (the Strategic
Framework) considers likely and potential scenarios to inform planning considerations and ensure
that we are prepared to respond as required. While these scenarios are based on evidence and
have been subject to review, it is important to note they are hypothetical.
The scenarios prepared as part of the Strategic Framework range from low transmissibility and
low immune-evasion, essentially where the virus has enough transmissibility to create a high case
load, but current effective immunity is protection enough. Other scenarios include a high
transmissibility and high immune-evasion, where without significant intervention the pressure on
the healthcare system would be immense and the number of COVID-19 related deaths would be
likely to increase, particularly among the elderly. We have also accounted for the possible
scenario of multiple co-circulating variants, however based on current evidence this is somewhat
less likely.
In planning for future variants, we have the advantage of having systems and an evidence
informed range of responses in place that can be applied to the scenario at hand. Currently, it is
likely that responses to most potential variants are focussed on minimisation and protection. This
means that the focus would be on:
• continuing the focus on minimising impacts with widespread transmission to reduce the
effects on the population, particularly vulnerable communities,
• avoiding additional burdens on the healthcare system that could be caused by Influenza
Like Illnesses; and
• long-term planning for recovery and ensuring the system can respond to Variants of
Concern.
Our access to global insights and monitoring provides some lead time and indicators on Variants
of Concern to inform preliminary health risk assessments. As an island nation we do have the
E O
advantage of increasing border surveillance, which can be enacted quickly when we are alerted to
any serious new Variant(s) of Concern. By increasing surveillance at the border, we should be able
to slow the spread of any new variants and buy time to stand up a response if it is required and
consider options that support or increase our understanding of a new Variant.
In the plan we have identified our key response measures, as a combination of baseline measures
and extra measures that would be used with more severe Variants of Concern. The baseline
measures include:
• ongoing border and community surveillance
EASED UN
• RAT based testing except for PCR where required for diagnostic or surveillance purposes,
isolation requirements for current cases
• infection prevention controls including mask use
• vaccination and therapeutics
• border measures, including pre-departure testing and post-arrival testing
• the ongoing use of Care in the Community networks.
Further reserve measures that can be called on for more severe Variants of Concern, noting the
measures will be very context specific:
• Increased use of testing through targeted interventions
• Contact tracing
5

• Capacity limits
• stronger border measures, including self-isolation for arrivals, MIQ or border closures, and
• Regional and national lock-downs.
By completing this preparedness process now, we have the advantage of being able to identify
what future responses may look like and work on preparedness measures to strengthen our
response. This will not only make it easier to activate the response more rapidly, but also make
the responses more effective. An example of this is the development of potential seroprevalence
surveys which will provide information on the level of immunity in the community and inform
measures that may be required as part of a response.
We know that in using these measures there will be trade-offs that will need to be made between
the health impacts and impacts on social and economic wellbeing. Work is currently underway to
develop a detailed understanding of the impacts of these measures and will be used to inform
future decision making.
E O
EASED UN
6

population. Note, that the immunity to infection and immunity to severe
disease may vary for different variants.
Speed of
A new successful variant that arises from incremental changes to the
transmission
dominant variant is likely to be more transmissible than the existing
predominant variant. A “frame shift” variant may be able to spread by not
having to compete with dominant variants due to substantial immune
evasion and changes to the mode of infection (to date all variants have
entered cel s through the ACE receptor in the nose or throat).
A new variant may spread so quickly and be so transmissible that there is no
option of buying time, by keeping it out, as it may already be in New
Zealand. As we have seen with Omicron, the speed at which a new variant
can replace old variants can be very swift. Omicron is estimated to have
infected approximately 50% of the US population in about 10 weeks.
On the other hand, a new variant may spread relatively slowly, on its way to
becoming the dominant variant. For example, BA.4 and .5 have an
approximately 10-20% transmission advantage over BA.2, which means that
one or both are destined to become the dominant variant (all else being
equal) but it may be a relatively slow burn, over a period of a few months.
The situation has changed from March 2020
Since the initial outbreak in New Zealand in March 2020 much has changed and much has been
learned about the virus and how best to respond to the pandemic. Time has allowed us to learn
from the experience of other countries, as well as reflect on our own, and to consider the vast
amount of scientific knowledge about the nature of the virus and how best to protect the health
and wellbeing of our communities.
Nationally and internationally, there is better surveillance than in 2020
E O
Global surveillance means that we will most likely receive early warning (within days of a sample
being analysed) of a new threat before it is detected in New Zealand. This could include an
understanding of the potential level of immune escape of the new variant as there is a better
knowledge of which mutations are associated with this. Within weeks there may be early evidence
of immune escape and changes in transmissibility. What will not be immediately known however,
is the severity of a new variant as it takes 1-2 months for the data to be gathered and analysed.
It is possible that a new variant may already be circulating within the community by the time we
are alerted of its emergence internationally. In this situation, rapid identification to inform a
EASED UN
strong health response can still be effective (as those tactics were in March 2020), particularly if
the new variant has a modest transmission advantage over the prevalent variant.
Some level of protection will already exist
The immunity (infection or vaccine related) that New Zealanders have built over the last two years
will likely provide some continued level of protection against severe disease, as the mRNA
vaccines did for Omicron. However, vulnerabilities due to waning immunity, unvaccinated and
immunocompromised individuals should be considered, as there will be a significant proportion
of the population who remain highly vulnerable to severe disease.
9
 SARS-CoV-2 vaccines may be developed at greater speed
SARS-CoV-2 vaccines may be developed at greater speed
The first COVID-19 vaccines were developed in just 11 months. As mRNA technology evolves
further, new vaccines can be developed within an even shorter timeframe – potentially within a
few months to respond to new variants. However, global demand and manufacturing constraints
may mean that it could take several months before there is sufficient supply for distribution. It will
also remain important that the regulatory assessment is robust and Ministerial approvals
processes are thorough.
As with the current situation with the influenza vaccine, some prediction based on best evidence
and modelling is involved, but there is no guarantee of a good match between the vaccine in
development and the actual variant that occurs during the season.
It is unknown at this point whether new COVID-19 vaccines will be updated annually, similar to
the seasonal Influenza vaccine, or less frequently. As noted, the new variant may be sufficiently
similar that a new vaccine is not required. Rather, a further dose of existing vaccines may be
protective.
Higher transmissibility may mean fewer public health measures are effective
The degree of infectiousness of a new variant may be so great that some public health and social
measures (PHSM) may not be effective.
During Delta, PHSMs including Managed Isolation and Quarantine (MIQ) bought time to reach
high levels of population immunity through vaccination programmes (above 90% percent). MIQ
and other border measures were effective in stopping the introduction of the Delta variant into
the community for an extended time from May to August 2021.
The most effective way of protecting communities at greater risk is to strengthen layers of
protection to reduce the levels of community transmission. Once Omicron became the dominant
variant, effective vaccines were available but substantial protection against severe disease was
only provided by three doses. The 7-day MIQ requirements and other border restrictions were
E O
still in place at the time slowed the introduction of Omicron into the community and bought us
time until a sufficient proportion of the population (particularly older people) could receive three
doses.
Erosion of social licence
To date, the success of our response to the COVID-19 pandemic has relied on an outstanding
level of community support, adherence to the public health measures and participation in
vaccination programmes. Understandably, as the pandemic has extended for over two years,
some parts of the community have become less willing to cooperate with some public health
EASED UN
measures. As such, there may be fewer public health levers available, and/or the interventions
that are still available may be less effective.
Effective and engaging messaging is likely to be required to gain broad population support if
restrictive public health measures were to be introduced once again.
Throughout the pandemic, research has monitored and assessed community attitudes. There will
be an ongoing need for such research to ensure public health messaging remains effective and to
act as a barometer of social licence.
10

 V. The COVID-19 Strategic Approach
V. The COVID-19 Strategic Approach
As the COVID-19 pandemic moves into its third year, Aotearoa New Zealand’s health response
has continually evolved as both the virus and our ability to manage it has changed. From our
initial elimination strategy we have shifted to one of minimisation and protection. We have
continued to refine our response from the earlier Alert Level settings to the current COVID-19
Protection Framework.
As we look to shift to an environment where COVID-19 is endemic in Aotearoa New Zealand and
globally, the potential for new Variants of Concern needs to be carefully considered as part of any
future planning as changes are made in the post-peak Omicron environment, and to inform
planning.
As we work to create a system that is resilient to new Variants of Concern, we need to carefully
consider the role of preparedness measures to support an effective response. We are working to
optimise the effectiveness of relevant measures and to minimise the need for more restrictive
measures where possible.
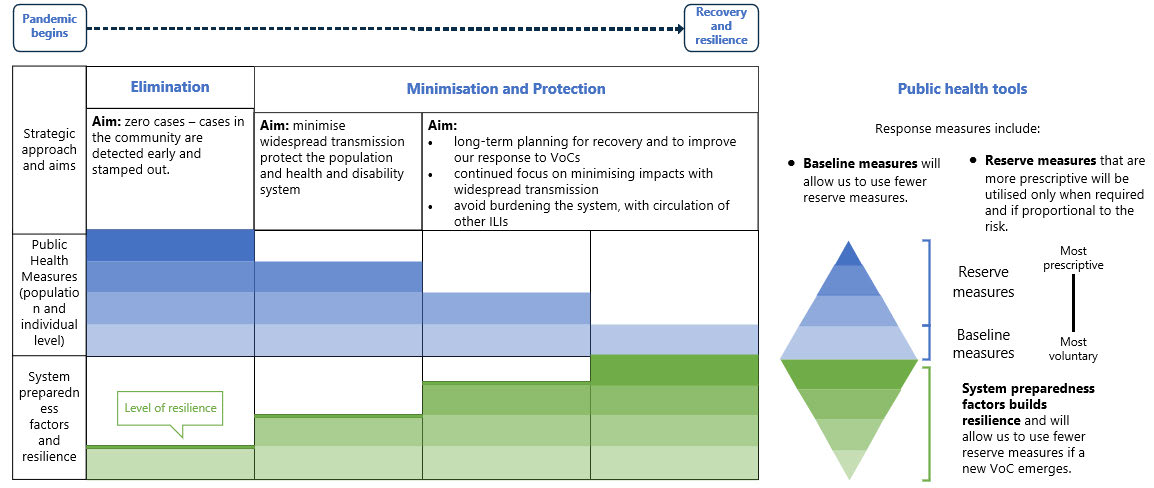
This is highlighted in Figure 1 below which shows how the use of measures has progressed
throughout our response to the pandemic, to the current state where in the minimisation and
protection phase we are looking to use baseline measures where possible, although there are
reserve measures that can be used if required. The green parts of the diagram show the enhanced
system resilience through preparedness, that support more effective baseline measures- for
example, improved through testing and surveillance technology.
Figure 1. The role of the public health response and preparedness factors
E O
EASED UN
As such, the Strategic Framework sits within a wider strategic context which includes:
• the development of a strategy for the COVID-19 health response over the medium to long-
term, focused on recovery and building resilience. It will provide strategic guidance for the
health system and wider All-of-Government COVID-19 response and will inform the operating
context in which we respond to new variants.
• revising the current surveillance and testing strategies to reflect the updated and more
nuanced responses to different variant scenarios.
11

• informing the development of the Health Border Strategy and the interim and enduring
arrangements for the health presence at the border.
• ensuring that responding to new Variants of Concern is supported in consideration of the
future legal framework.
• advice and recommendations from World Health Organization (WHO), and other peak bodies
and the potential impact of amendments to the International Health Regulations 2005 and
proposals for a pandemic treaty.
• development of a COVID-19 vaccine strategy that will consider measures to maintain vaccine
effectiveness and support agility to enable vaccines to respond new Variants of Concern as
and when required.
The Ministry of Health continues to work with Department of Prime Minister and Cabinet (DPMC),
Ministry of Business Innovation and Employment (MBIE), Ministry of Education, Ministry of
Primary Industries, the New Zealand Customs Service and the Ministry of Foreign Affairs and
Trade to progress broader planning for the All-of-Government response.
The scenario planning will also be available to inform broader strategic planning, with potential
uses including the ongoing consideration of national quarantine capability and Treasury’s work on
resilience planning.
E O
EASED UN
12
 VI. Scenarios to inform the Strategic Framework
for new Variants of Concern
VI. Scenarios to inform the Strategic Framework
for new Variants of Concern
Five hypothetical COVID-19 variant scenarios have been developed to inform the Strategic
Framework. Each scenario considers clinical severity, immune evasion, transmissibility, disease
burden, and the availability of effective vaccines and antiviral therapeutics. The scenarios are:
• Scenario 1: High clinical severity, high immune escape
• Scenario 2: Low clinical severity, high immune escape
• Scenario 3: High clinical severity, low immune escape
• Scenario 4: Low clinical severity, low immune escape
• Scenario 5: Multiple co-circulating variants with different levels of severity and different levels
of cross-protection.
All scenarios are compared to the Omicron BA2 variant which is the dominant variant in
New Zealand at this time.
While there are clear uncertainties ahead, there are a number of expected assumptions based on
science. A first assumption is that COVID-19 will continue to evolve with new Variants of Concern.
Secondly it is assumed that in all scenarios the new variant has transmission advantage (increased
Ro)) and is able to out-compete Omicron BA2 (the current dominant in New Zealand).
We have also assumed that in all scenarios there is a degree of prior immunity from previous
vaccination or infection. As such, the disease severity as discussed below refers to the severity
observed in a population with an existing degree of prior immunity, rather than the ‘intrinsic’
E O
severity associated with infection of an individual with no prior protection. For example, Omicron
typically causes mild disease in vaccinated or previously infected populations but can be severe in
unvaccinated individuals.
Disease characteristics and contextual factors
There are a range of factors that will need to be considered that could apply to all scenarios –
which in turn which will impact on the response approach. For example, evidence that the variant
results in a longer infectious period or is resulting in chronic infections may lead to more severe
impacts. These factors are outlined in the below:
EASED UN
13
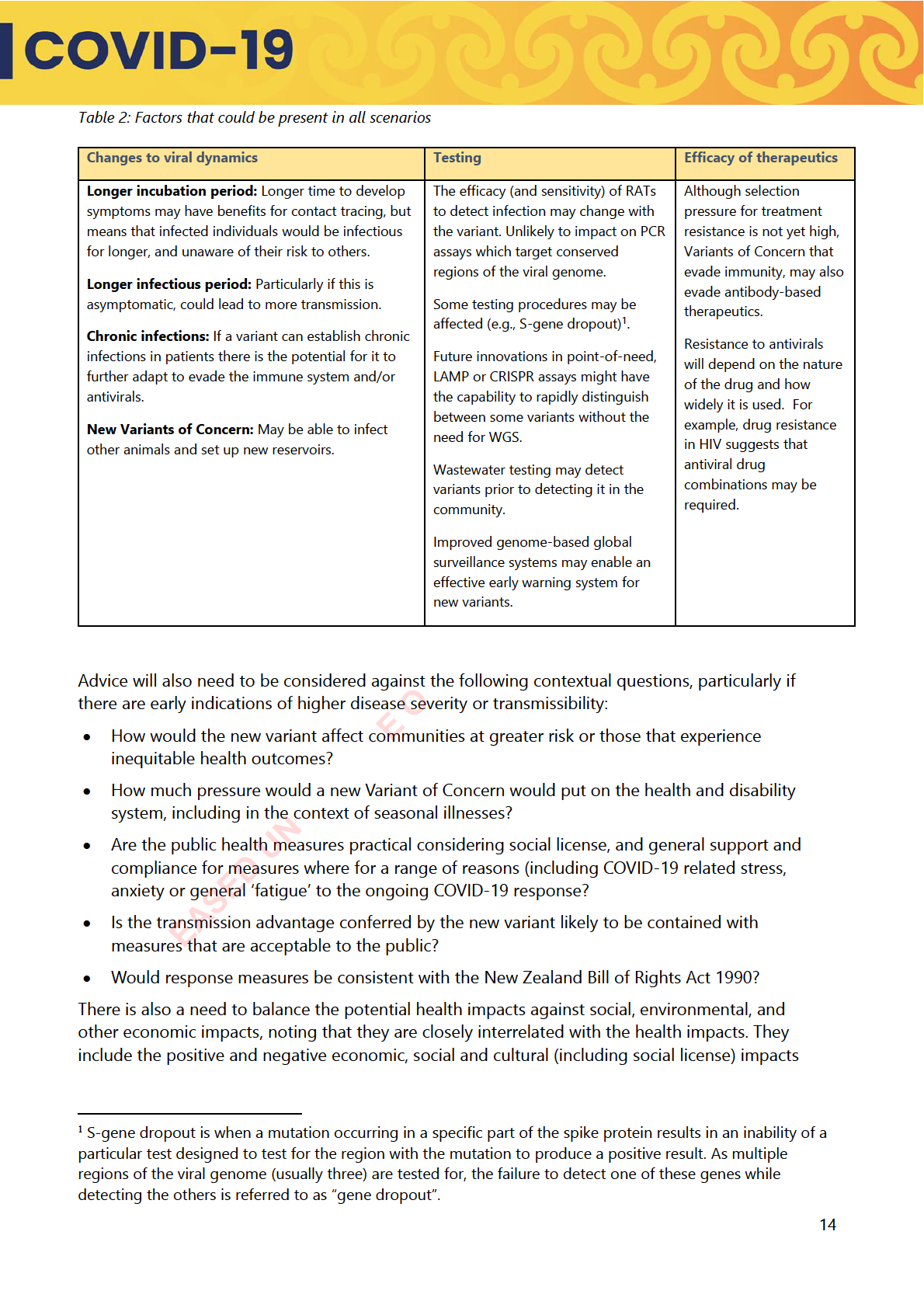

of the response, and the distributional impact of measures. Some of these impacts are currently
directly addressed by the government through economic and social supports.
Co-circulating variants: the balance between transmissibility and immune
escape
The potential for more than one circulating and co-existing variant is also considered, however
given the limited evidence for this we have not planned for this or included it in modelling.
Co-circulating variants is when two or more variants have substantial immune escape from each
other (e.g., immunity associated with infection with variant one does not provide protection from
variant two, and vice versa) the more the two variants have distinct ecological niches and so are
able to co-exist without being in direct competition.
The emergence of Omicron and other highly transmissible sub-variants has largely replaced
previous lineages. It is not known if multiple variants with different severity, transmissibility and
immune escape will be re-established, or if the pandemic will be dominated by a single highly
transmissible variant2. Appendix 1 contains further detail on this.
E O
EASED UN
Although Delta does still circulate globally in very low numbers, and the implications of that are still unclear
15
 VII. The response decision-making process
VII. The response decision-making process
Throughout the COVID-19 pandemic we have continued to refine the decision-making process,
and this has been enhanced by an improved evidence base.
To provide clarity of the response process, key decisions and the information we draw on, we
have outlined the process in Appendix 3. This includes the stages of decision-making and the
relevant information sources at each stage. It is important to note that this process focuses on the
current role of the Ministry of Health, and once established on 1 July 2022, will change to include
Health New Zealand and the Māori Health Authority.
The role of the Public Health Risk Assessment
Should a new Variant of Concern emerge, a Public Health Risk Assessment (PHRA) will remain an
integral part of assessing the situation and providing considered public health advice at key decision
points for Ministers. As outlined above, any response will vary depending on the contextual
characteristics and the nature of the new Variant of Concern.
Connection to the All-of-Government Response
There is a process for an All-of-Government response as required where a response is critical, or
decisions are required within 24 hours. The National Response Leadership Team3 would take the
lead in providing advice and enacting a response through agreement from COVID-19 Ministers with
Powers to Act. Ongoing responses would be supported by governance from the wider National
Response Group.
Preparedness will need to factor in the absence of detailed information
A systematic approach will be taken to the assessment of the potential impact of the new
variant(s) to determine which scenario is most li
E O kely. The Strategic Framework will include a
process for rapid information gathering and management in the period before the scenario
becomes clear. For each new variant, it will take time for researchers, data scientists, virologists,
public health specialists and epidemiologists to determine the features and epidemiological
characteristics of the virus, and therefore the threat that the new variant poses.
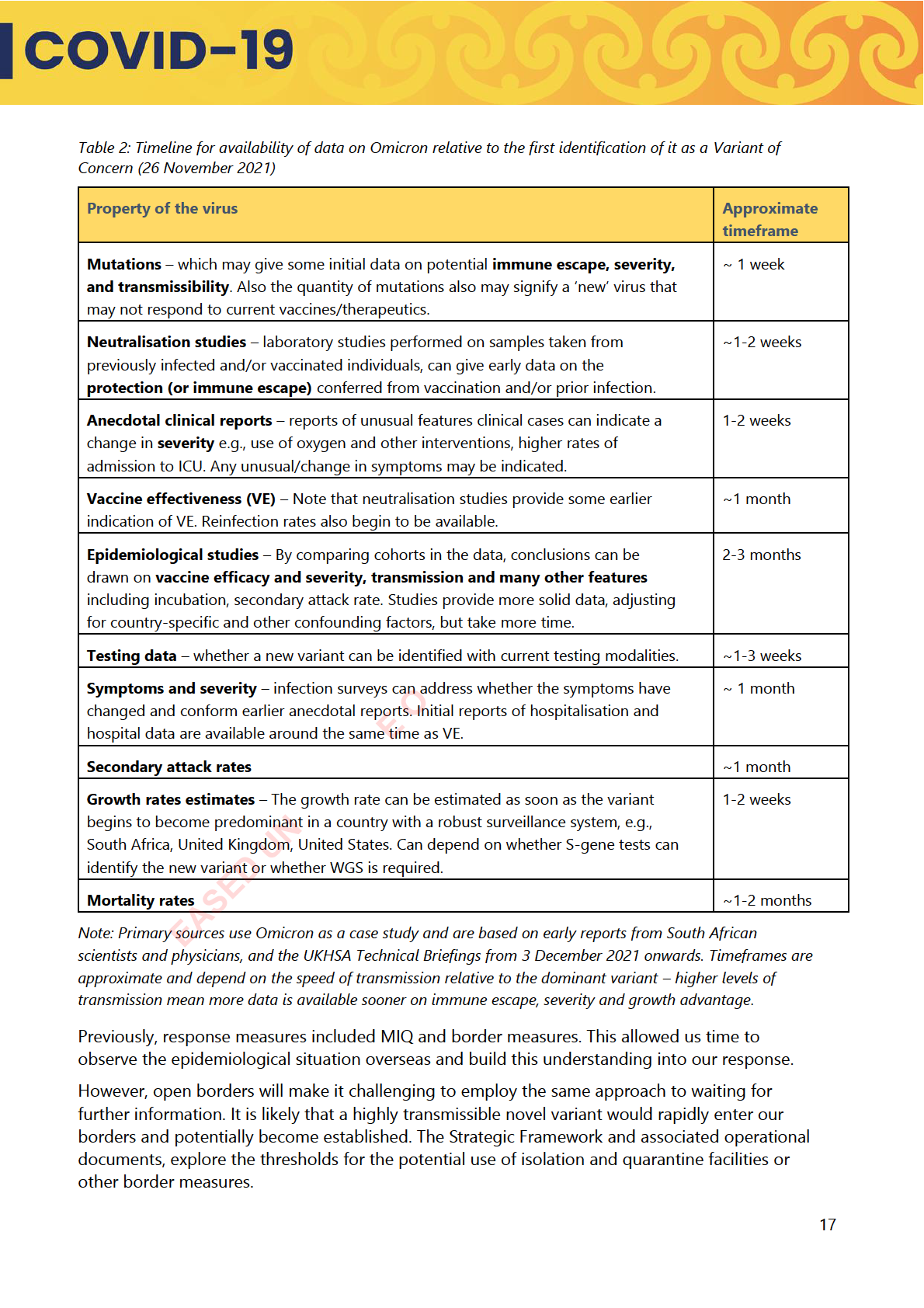
As an indication of timeframes, in the two-four weeks following initial detection of the Omicron
variant offshore, anecdotal findings and early data gave indications on the transmissibility,
immune evasion and severity characteristics of the Omicron variants. However, strong
epidemiolog cal and clinical data to support these findings only emerged in the one-two months
EASED UN
following detection.
The NRLT consists of the Chief Executives or delegates of the Ministries of Health; Education; Business,
Innovation and Employment; Social Development; Foreign Affairs and Trade; Transport; Justice; Housing and
Urban Development; and Department of the Prime Minister and Cabinet; Treasury; Public Service Commission;
Police; Customs and Te Arawhiti.
16
 VIII.
Responses to each of the scenarios
Strategic approach to new Variants of Concern
VIII.
Responses to each of the scenarios
Strategic approach to new Variants of Concern
Planning for new Variants of Concern needs to occur at several levels, from global and national level
responses to local and community-based responses. The intention is that this initial Strategic
Framework is focussed on the national health response. Further local and community-based
responses will then be developed and informed by this.
The overall objectives in response to COVID-19 Variants of Concern remain focussed on reducing
and controlling the incidence of COVID-19 infections and to prevent, diagnose and treat COVID-19
to reduce mortality, morbidity, and long-term impact. It will also need to be aligned with a strategic
context where we are increasingly going to be focussing on resilience and recovery, and a context in
which there will be greater reliance on voluntary and non-prescriptive measures.
Any effective response will also need to consider how we support equity of outcomes and uphold Te
Tiriti o Waitangi as part of an effective health response. This will mean tailoring responses and
leveraging relationships with communities.
A response will also need to be cognisant of the broader impacts on social and economic wellbeing.
It will also need to recognise that we are working as part of the All-of-Government response to
identify and mitigate negative impacts of any public health measures so these can be factored into
planning and decision making.
Determining the best approach
If a new Variant of Concern emerged that could lead to significant health, social and economic
impacts, and it was feasible to keep the variant out of the country to buy time to develop a more
effective response through domestic measures, the adoption of an elimination approach may be
considered. However, the threshold for this is likely to be particularly high.
E O
We note that an elimination approach is less likely to be used. This is due to the increased levels
of population immunity that is likely to limit the severity of disease and the reduced social license
for more stringent public health measures, including MIQ. It is also likely to be complicated by the
likelihood of high transmissibility levels which makes eliminating any new variants particularly
challenging. No country has successfully eliminated Omicron, which has a higher R value than
preceding variants
Based on recent experience we know that the right combination of public health measures can
minimise the spread and health and disability system impact of pandemics. This this may be
EASED UN
preferrable over an elimination approach.
An elimination approach is only likely to be proposed in a situation that contained a range of the
following factors:
• if there were indications of very high clinical severity and likely high fatality rates (based on
early evidence from overseas).
• transmissibility levels that could be managed with strong border measures, including MIQ.
• there are high levels of immune escape and current immunity is unlikely to be effective.
• there were clear benefits that could be realised in the time that an elimination approach
could be sustained.
18

• where the health and disability system are already under pressure, or a new Variant of
Concern is likely to place the health and disability system under extreme pressure.
• where at-risk communities are likely to be severely affected.
The use of ‘prepare’, ‘contain’ and ‘manage’
We have developed the Strategic Framework to include three response stages:
• Prepare: System is alerted to new Variant of Concern - system readies to pivot and if needed
to move to contain.
• Contain: First community case - system pivots to reduce transmission.
• Manage: Widespread community transmission - system pivots to preserving critical
infrastructure and protecting communities at greater risk and priority populations.
Surveillance supports all stages. This involves the ongoing international and national monitoring of
Variants of Concern to inform Public Health Risk Assessments and response decisions. Surveillance
will also inform the effectiveness of any measures we have in place domestically.
The three response stages reflect the different context that we are operating in from March 2020
and in December 2021 when the COVID-19 Protection Framework was introduced. In our new
context where the R value of the virus is likely to be higher, the likelihood of elimination and
‘stamping it out’ is much less viable. Additionally, the levels of immunity from COVID-19 vaccination
or prior infection in the population is now higher and we have greater understanding of the of the
effectiveness of domestic public health measures in reducing transmission.
Public health measures considered
Across key public health aspects of the response, certain measures will change through each phase
of the response:
Government and community-led responses:
E O
• Surveillance
• Vaccination and therapeutics
• Testing
• Border measures
• Case investigation and contact tracing
• Infection prevention and controls,
•
including requirements for ongoing
Isolation and quarantine
mask use.
• Care in the community and broader
health response.
Individual-led responses:
EASED UN
• Mask use
• Social distancing
• Isolation and appropriate use of sick
leave
Decisions around the appropriate measures reflect likely contextual factors, including the impact of a
Variant of Concern on health outcomes, and broader socio-economic outcomes. Decisions have also
considered the expected pressure on the health and disability system.
Some measures, most notably mask use, have a wider value in preventing the spread of other
respiratory illnesses as well as COVID-19. This additional value will be considered in future decisions,
and as part of system preparedness we will need to consider how we can bolster ongoing mask use
in some settings or circumstances.
19

The COVID-19 Protection Framework has a potential role in providing clear public health settings to
support the response to different variants. The use of this tool is contextual and will need to be
considered as part of planning any potential public health response.
This process set out above will still occur when functions from the Ministry of Health transfers to
interim Health New Zealand. The Ministry (including the iPHA) and iHNZ have worked together to
ensure that the functions will transfer in a way that maintains a strong response and mitigates any
risk to the continuity of the response.
Appendix 4 presents the responses to each of the scenarios, across each of the phases from
prepare, contain and manage.
Targeted approaches for particular areas and communities
We know particular communities and areas are at greater risk from new Variants of Concern, and
this needs to be included in our planning processes. There is a concentration of risk in particular
communities around South Auckland (and the broader Auckland region to an extent) due to the
combination of proximity to the border and the number of communities at greater risk that live in
the area. In other communities, e.g. parts of the Eastern Bay of Plenty, there are communities with
high concentrations of social deprivation, high co-morbidities and limited access to health care
which require their own targeted approaches. This should be a factor that informs prioritisation of
targeted preparedness and response activities.
To this end we will be increasing using All-of-Government responses to provide integrated
responses, including working with the Ministry of Social Development, Ministry of Housing and
Urban Development, the health entities, iwi partners and Care in the Community networks to
provide localised responses that are tailored to their needs.
Trade-offs
Economic, social and health outcomes are inextri
E O cably linked as the pandemic has demonstrated.
Decisions on what measures to employ need to consider likely benefits, risks and trade-offs. Where
possible, data should be gathered to measure these impacts across a range of outcomes.
We should be particularly mindful of the value that preparedness activities and our baseline
measures present: for example, the more people we can get vaccinated and boosted, and provide
with access to antivirals the less we should need to respond to protect the health system during
peaks. Furthermore, the safer we can make being in the community through the use of face masks
and public health communication to support good health behaviours, the more people can continue
to participate in the economy.
EASED UN
Some public health and social measures such as contact tracing, quarantine (particularly when the
criteria for who must quarantine includes close contacts) and isolation, provision of economic and
social supports to enhance compliance with public health measures, border closures, and lockdowns
are resource-intensive. Response measures are generally more costly than our baseline measures
and preparedness activity.
Further work is underway as part of the All-of-Government response to better understand the
detailed impacts.
20
 Prepare
Prepare
• Engaging with the public will be key in the success of responses to any future
communication
outbreaks or incursions.
plans, including
• Targeted campaigns can assist the Ministry in fulfilling its Te Tiriti o Waitangi
targeted
and equity obligations.
communication for
• Strong communications campaigns are needed to boost vaccination.
communities
• Learning from the past e.g. a key lesson from the 2019 measles response was
to bring the population onside to respond in an agile way.
Improve data
• Continue to improve our disease and vaccination data collection, wastewater
collection, reporting
surveillance sequencing and analysis capabilities to immediately identify and
and analysis
detect new and emerging variants.
• Continue improvements to COVID-19 disease and vaccination data collection,
wastewater surveillance, and virus sequencing capacity so we are better
prepared to respond rapidly to emerging threats.
• Identify appropriate indicators to inform continuous monitoring and
improvement.
Leverage contact
• In the early stages Public Health Unit-led contact tracing with national source
tracing
tracking and case management may be deployed to provide New Zealand with
some local and regional areas for targeted focus. In a high clinically vulnerable
and high immune escape setting the value of contact tracing after the first and
second identified case and contacts will need to be clear.
Surge Response Plan • S9(2)(g)(i)
Maintain surveillance • Surveillance testing will be used to identify when we have a new variant. We
capacity
must ensure that we have sufficient capacity to undertake the surveillance
required.
E O
• The Surveillance Strategy provides information on the detailed response,
including the relative importance of respective surveillance measures.
• Ongoing work to enhance the surveillance system to identify new cases and
Variants of Concern at our border and in our communities.
• Working with the Institute of Environmental Science and Research (ESR) to
increase Whole Genome Sequencing capacity. Wastewater surveillance is also
important for understanding community cases, and we continue to enhance
this including work with ESR on enabling surveillance to distinguish between
variants.
• Enhan
EASED UN ce understanding of levels of immunity in the population to understand
potential risk and inform responses. Consideration is being given to how to
identify both natural immunity levels and vaccine-based immunity levels.
Laboratory device
• A stocktake across the laboratory and hospital settings is being undertaken. It
review and
will help inform regions with variability to scale and target testing modalities
Innovation
and enable the right testing modality to the right presentation of contact or
framework
potential case.
• The Ministry, DPMC, and MBIE are establishing a Testing Innovation
Framework across laboratory groups, networks and science and research
institutes. It will inform the regulatory assessment processes and undertake
horizon scanning for the latest in innovation and technologies to support our
ongoing response to COVID-19 and other infectious disease.
22
 Contact tracing
Contact tracing
•
Recognise that the value of contact tracing will be limited in the absence of
restrictive policy settings at the border and in community.
•
In the short-term, it is likely that we could not scale contact tracing to the
levels we have had previously, primarily because we could be contending with
more than one variant at a time over the course of the coming months.
•
In the early stages of each phase across the responses, Public Health Units led
contact tracing with national source tracking and case management will
provide New Zealand with some local and regional areas for targeted focus.
The value of contact tracing after the first and second identified case and
contacts will need to be clear.
Leveraging our
•
Developing a series of plans in coordination with suppliers and the health care
COVID-19 Variant
system for delivery of updated vaccines, tests, and treatments.
responses and play
•
These plans and processes suggest that vaccines, PPE, and tests can be
book
deployed in days and weeks rather than months using the vaccine supply chain
and logistics to sites, community testing centre and pop-ups, and the PPE
portal.
Leverage a proven
•
S9(2)(g)(i)
COVID-19 surge
Response Plan
Regulatory review of • S9(2)(g)(i)
variant-specific
versions of vaccines
and treatments
Critical medical items •
The Ministry currently maintains a national stockpile of at-home tests, PPE and
supply
critical medical supplies for use in surge events.
•
Pharmac is responsible
E O for securing antiviral medications and are part of the
all-of-government COVID-19 Vaccine Strategy.
•
Continue to assess the utility of therapeutics.
•
S9(2)(g)(i)
•
The Government will be ready to deploy supplies to the health and disability
sector alongside clinically vulnerable and priority populations ensure adequate
supply in times of surges, COVID-19 outbreaks, or new variants.
All-of-Government measures for consideration
EASED UN
S9(2)(g)(i)
23

S9(2)(g)(i)
E O
EASED UN
24
 X. Te Tiriti o Waitangi and Equity commitments
X. Te Tiriti o Waitangi and Equity commitments
Consistent with the principles underpinning the long-term COVID-19 Strategy, this Strategic
Framework is underpinned by Te Tiriti o Waitangi obligations and support equity of outcomes.
Te Tiriti o Waitangi
Embedding the principles of Te Tiriti o Waitangi into our work is a key part of being responsive to,
and providing a response for, Māori.
Meeting our obligations under Te Tiriti is necessary if we are to realise the overall aims of He
Korowai Oranga - our Māori Health Strategy and to achieve outcomes for the health and
disability system as a whole. This includes a desire to see all New Zealanders living longer,
healthier, and more independent lives. These Tiriti obligations underpin Whakamaua: Māori
Health Action Plan 2020 - 2025 which sets the Government’s direction for Māori health
advancement over this time.
The principles of Te Tiriti o Waitangi provide the framework for how we will meet our obligations
under Te Tiriti in our day-to-day work. These are:
• Tino rangatiratanga
• Options
• Equity
• Partnership
• Active protection
The COVID-19 pandemic has seen Māori experience worse outcomes, compared to other
ethnicities, which means Māori are at greater risk of worse outcomes should a new Variant of
Concern emerge. It is therefore critical that the needs of Māori, and the commitments made in Te
Tiriti o Waitangi, are integral to the health and disability response to COVID-19.
Changes to our COVID-19 response measures therefore need to continue to support iwi, hapū,
E O
whānau, and hapori Māori to make decisions for themselves, regardless of legal settings, e.g.
within the COVID-19 Protection Framework and relevant COVID-19 orders.
Working with Māori on design and delivery of services
The Crown’s obligations to Māori under Te Tiriti o Waitangi require active protection of tāonga,
and a commitment to partnership that includes good faith engagement and knowledge of the
views of iwi and Māori communities. In the context of the COVID-19 response, this involves
considering what will support a national response that is co-ordinated, orderly, and
proportionate, considering the
EASED UN Crown’s obligation to actively protect Māori health, interests and
rangatiratanga.
Māori vaccination and booster rates remain lower than the rest of the population largely due to a
slower rollout of the initial vaccination campaign to Māori communities. While in the week to 3
May 2022 1,900 Māori received a vaccination dose, trending up for the third consecutive week,
first dose vaccinations for tamariki Māori aged between 5 and 11 are under 1,000 for the seventh
consecutive week. This has been exacerbated by the high numbers of Māori recently infected with
COVID-19 and the three-month interval between becoming a case and receiving a booster dose.
Locally-led responses continue to be relied upon particularly in Māori communities where local
Māori providers and providers contracted by Whānau Ora commissioning agencies are mobilising
to respond to the demands of their communities.
25

Across many of the measures in the Variants of Concern Strategic Framework, there are effective
examples of equity-centred approaches informed by Te Tiriti o Waitangi. A testing action plan
focused on advancing equitable access for Māori, Pacific, and disabled people has been
developed and is currently being implemented. The COVID-19 Care in the Community framework
has created opportunities for community-led responses, including working with iwi.
As part of the COVID-19 Māori Health Protection Plan, work is underway to build community
resilience and increase vaccination uptake. These measures will be beneficial and support the
principle of active protection in the event of a new variant.
Māori providers are becoming increasingly more concerned about the wider health and
socioeconomic impacts of the pandemic on whānau, and in ‘catching up’ on health services (such
as flu immunisations, childhood MMR, screening services) that have been deferred.
Ensuring Māori whānau have comprehensive and immediate supports through the Omicron
outbreak will contribute to their resilience so they can leverage recovery opportunities, and these
impacts and opportunities will need to be considered as part of wider planning.
Equity
In Aotearoa New Zealand, people have differences in health that are not only avoidable but unfair
and unjust. Equity recognises that people with different levels of advantage require different
approaches and resources to obtain equitable health outcomes.
To support this, and as per our minimisation and protection approach, the priority is to slow down
transmission of the virus and protect our communities at greater risk. These communities include
Māori, Pacific peoples, disabled people, rural and isolated populations, communities that
experience barriers to engaging with the health and disability system. We also know that certain
geographical factors that disadvantage particular groups, including proximity to the border for
South Auckland communities.
E O
There are also a range of underlying risk factors that may negatively impact equitable outcomes.
These risk factors are intersectional and compound the effects of other risk factors on individuals
and communities. Risk factors include vaccine status, age, sex/gender, ethnicity, pregnancy, co-
morbidities, disability, mental health and addictions, material deprivation and poverty,
occupation, household characteristics, high risk settings, inadequate access to health care.
An equitable approach to public health and outbreak management includes not only a focus on
communities at greater risk. It also requires understanding the barriers faced by these
communities, enabling public health participation, and promoting health and wellbeing.
Community engagement strengthens relationship and build health literacy for the long term.
EASED UN
We will continue to learn from All-of-Government engagement with community leaders and
technical experts to ensure that responses are tailored to the needs of communities, and
proactively enables community-led responses.
Devolving power and resources to communities
Local communities have played an important communications role by supporting ongoing
messaging to support various efforts of the COVID-19 response, such as supporting safe isolation
and helping to increase vaccination uptake. We will continue to work through the networks
established as part of caring for our communities and other local responses to support active
partnership.
26
 XI. Global Responses to Variants of Concern
XI. Global Responses to Variants of Concern
Understanding the broader global context is an important principle that underpins our COVID-19
response. While recognising that New Zealand has its own unique situation and national COVID-
19 response, it is important that we remain attuned to global developments, and that we meet our
international obligations and contribute to the global response effort.
Global surveillance efforts
Global surveillance efforts will be vital to the early identification and response to new variants,
and as a member of the World Health Organization, we are committed to strengthening these
efforts, including working towards increased information sharing between members.
The International Health Regulations (2005) (IHR), administered by the WHO, sets out the
international legal framework for preventing and controlling the spread of disease and other
ACT 1982
public health hazards between countries. Under the framework, member States are required to
notify the WHO of any events which may constitute a public health emergency of international
concern, as well as any health response measures implemented. This includes the notification of
new Variants of Interest and Variants of Concern.
Our response will also be informed by other global surveillance efforts including:
• the Centre for Disease Control and Prevention’s (CDC) system for monitoring all variants and
classifying those requiring more attention and plans to continue this surveillanc
INFORMATION e effort as the
pandemic continues.
• the European Centre for Disease Prevention and Control (ECDC) variants dashboard, which is
updated weekly providing an overview of new variants in EU/EEA member states.
The WHO has also reiterated that surveillance activities require coordination between the human
and animal health sectors and more global attention on the detection of animal infections and
possible reservoirs among domestic and wild animals. We expect that this will become worse with
the effects of climate change.
International approaches to strategic planning
We have considered global approaches to our strategic planning, including the WHO’s
Strategic
Preparedness, Readiness and Response Plan to End the COVID-19 Emergency in 2022 (the WHO’s
Plan). The WHO s Plan outlines a global strategic response to COVID-19 based on scenarios that
include new Variants of Concern, and a proposed roadmap to inform national and local planning.
The report is built on six pillars, which have informed our thinking:
• Enabled and empowered communities
RELEASED UNDER THE OFFICIAL
• Enhance surveillance, laboratory, and public health intelligence capacity
• Supported and protected public health and medical workforce
• Resilient health systems
• Emergency medical supply systems
• Research and innovation.
27

We are in regular contact with similar jurisdictions to inform our planning and to share our own
lessons. We regularly meet with Chief Medical Officers from Australia, Canada, the United
Kingdom (UK), and the United States, and are in regular contact with Singapore health officials.
We have also received information on other countries’ Variants of Concern planning, including
South Africa and the Republic of Korea. These relationships are particularly valuable as those
jurisdictions are currently developing their own approaches to potential new variants
International scenario planning
Global approaches were considered in the development of our scenarios and proposed
responses. Our scenarios broadly align with the UK’s Scientific Advisory Group for Emergencies
(SAGE) scenarios regarding the emergence of new variants, and the WHO’s Plan.
Both plans predict that:
ACT 1982
• milder variants will have lower severity and that vaccines will remain effective
• worst-case scenarios will have high severity of disease and significant immune escape.
For comparison, the worst-case scenarios proposed by SAGE and the WHO are as follows:
UK’s
Reasonable worst-case: global incidence, incomplete vaccination and animal
SAGE
reservoirs lead to repeated emergence of variants with some displaying
significant immune escape. Severe disease, mortality and long-term
INFORMATION impacts
following infection are seen. Updated vaccines and annual, widespread rollouts
are necessary. Protections will need to be enforced especially when new variants
outpace vaccine updates.
WHO
Worst-case: Future variants are highly transmissible and able to evade vaccines
and immunity requiring vaccine alteration and broader boosting.
In addition to the high-level alignment, our scenarios have considered the potential for chronic
disease, the need for ongoing vaccinations, and potential for animal reservoirs to spread disease.
Supporting Pacific states - the Pacific Health Corridors work programmes
Consistent with information sharing and support provided as part of the Pacific Health Corridors
work programme, we will share the scenarios and information on the planning process and
responses with Tokelau, Cook Islands, Niue, Samoa, Tonga and Tuvalu.
RELEASED UNDER THE OFFICIAL
28
 XII. Next steps
XII. Next steps
This Strategic Framework is focussed on the preparedness and response measures in place to
respond to the emergence of new Variants of Concern, with a particular focus on national level
responses. Further detailed consideration of regional, local and community health responses is
required with Health New Zealand, the Public Health Agency and Māori Health Authority.
A government wide planning process is underway to support detailed operational planning of
response measures, informed by the information in this Strategic Framework.
The Strategic Framework is a living document that will continue to evolve based on regular scanning
of emerging research and evidence, and experiences in other jurisdictions. The Ministry produces a
bi-weekly monitoring document on Variants of Concern that will inform ongoing consideration of
the Framework, and the potential need for responses.
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
29
 XIII.
Appendices
Appendix 1: Evidence base for new variants, including information on co-
XIII.
Appendices
Appendix 1: Evidence base for new variants, including information on co-
circulating variants
SARS-CoV-2 has been characterised by the emergence of new Variants of Concern, with “successful
” new variants rapidly becoming dominant strains worldwide. To date the Alpha, Delta and
Omicron variants have sequentially emerged and dominated. The rapidity of the emergence and
dominance of new variants is demonstrated by the replacement of Delta by BA.1 within about one
month in New Zealand, and the subsequent replacement of BA.1 by BA.2 within a similar period.
[ESR analysis] These variants have had a transmission advantage over previous variants. This pattern
of enhanced transmission advantage with each new dominant variant is likely to continue, because
ACT 1982
increased transmissibility confers a substantial evolutionary advantage.[1]
New Omicron variants and subvariants are being reported frequently, with at least three Omicron
subvariants, BA.4, BA.5 and BA.2.12.1, increasing in prevalence in many parts of the world including
New Zealand.
Therefore, the identification of new Variants of Concern arriving in New Zealand will depend on
three main variables: the prevalence of the Variants of Concern in the arrivals to New Zealand (which
reflects prevalence overseas); the detection rate of cases arriving into New Zealand and the efficacy
INFORMATION
of the WGS surveillance of arrivals.
SARS-CoV-2, as with many viruses, has an intrinsic ability to mutate frequently. This, coupled with
extensive global transmission, means SARS-CoV-2 has a large mutational potential, and therefore it
is difficult to predict the emergence of future novel Variants of Concern.[2] The ability of SARS-CoV-
2 to jump into other mammalian hosts further complicates predictions.
SARS-CoV-2 is a virus that is constantly undergoing mutation, which may or may not have a
significant functional impact on the phenotype or ‘characteristics’ of the virus. A new variant is one
that has marked phenotypic differences that impact on disease characteristics, primarily its intrinsic
transmissibility, ability to evade immunity or disease characteristics such as severity. Concerning
SARS-CoV-2 variants can be classified in several ways:
Variant of Interest (VOI): WHO defines a VOI as a SARS-CoV-2 variant with genetic changes that are
predicted or known to affect virus characteristics such as intrinsic transmissibility, disease severity,
immune escape, or may adversely impact diagnostics or treatments; and is identified to cause
significant community transmission or multiple COVID-19 clusters, in multiple countries with
increasing relative prevalence alongside increasing number of cases over time, or other apparent
epidemiological impacts to suggest an emerging risk to global public health.[3]
RELEASED UNDER THE OFFICIAL
Variant of Concern (VOC): WHO defines a VOC as a SARS-CoV-2 variant that meets the definition of
a VOI and, through a comparative assessment, has been demonstrated to be associated with one or
more of the following changes at a degree of global public health significance:
•
Increase in transmission advantage or detrimental change in COVID-19 epidemiology; or
•
Increase in virulence or change in clinical disease presentation; or
•
Decrease in effectiveness of public health and social measures or available diagnostics,
vaccines, treatments.
30

Variant of High Consequence (VOHC): The U.S. CDC defines a VOHC as a variant that has clear
evidence that prevention measures or medical countermeasures have significantly reduced
effectiveness relative to previously circulating variants.[4] This could include failure to be detected by
diagnostic tests, a significant reduction in vaccine effectiveness, reduced susceptibility to treatments
or more severe clinical disease. Currently, no SARS-CoV-2 variants are designated as VOHC.
It is also possible for variants of SARS-CoV-2 to undergo recombination, where two different variants
infect the same host at the same time, exchange genetic material, and form a new ‘combined’
variant. For example, the XE subvariant of Omicron is a recombinant of BA.1 and BA.2. The likelihood
of recombination events is increased when more than one variant is prevalent and there is extensive
ongoing transmission.
Many Omicron mutations associated with the spike protein were unexpected and had not previously
been seen in any previously circulating variants. Concerning, even though Omicron is thought to
have branched off from the other variants in mid-2020, it went undetected by global surveillance
ACT 1982
systems until November 2021. The two most likely competing theories that explain how it was able
to mutate extensively and go undetected for an extended period are:
•
the variant evolved in an animal reservoir and then made the jump back into humans, or
•
the variant evolved over a period of time within one or more immunocompromised
individuals who were unable to clear the virus.
In addition, there are a range of other factors that can make the surveillance more challenging, e.g.,
INFORMATION
the lower morbidity associated with Omicron makes the initial identification of the disease more
difficult.
The probability of emergence of a new, concerning variant is difficult to estimate. There is some
evidence that the likelihood of coronaviruses jumping the species barrier is increasing, given two
new emergent coronaviruses in the last 20 years (including SARS in 2003 and MERS in 2012) in
addition to SARS-CoV-2, against a backdrop of only four other endemic coronaviruses in total, and
as human activity is increasingly encroaching on wildlife areas.[5] In a recent presentation to the
FDA’s Vaccines and Related Biological Products Advisory Committee, Dr Trevor Bedford estimated
that an ‘Omicron-like’ event (i.e., substantial mutations associated with the spike protein) may
occur every 1.5 to 10 years, with a probability of approximately 30% for one occurring in the next 12
months, based on the current speed of genetic change.[6] This probability will decrease and gain
more precision as the observed time between ‘Omicron-like’ events increases. More likely
(approximately 70%) was continued evolution within BA.2.
It is unknown why certain variants become predominant at different times, however we can infer
from some general principles. Any ‘successful’ new variant will likely employ a variety of
characteristics to spread in human and/or animal populations. These characteristics are outlined
RELEASED UNDER THE OFFICIAL
below.
Transmission advantage: Any ‘successful’ new variant would need to be more transmissible
than the predominant variant, such as Omicron, which is already extremely well adapted. Enhanced
transmissibility could be achieved either through increased:
Intrinsic transmissibility: Intrinsic features of the virus (e.g., higher viral load, greater
environmental stability, easier aerosolisation, increased infectivity of cells in the upper airways, and
ACE-receptor access/binding) may allow it to be transmitted more rapidly.[7] Transmission by
asymptomatic cases has been a key feature of SARS-CoV-2, that has enabled extensive
transmission.[1] The protection provided by vaccines against onward transmission tends to wane
31

quickly, however vaccines designed for the original strain of SARS-CoV-2 have continued to be
remarkably effective, particularly against severe disease.
Immune escape: Increased immune evasion relative to the current effective immunity within the
population (i.e., has many more ‘susceptible’ individuals available for it to infect) will also enhance
transmission. In the current post-vaccination/post-infection era, even with waning of protection, it is
likely that for a variant to be successful it will need access to a large pool of susceptible individuals
from those with some, or no, prior immunity.[8]
Severity: A new Variant of Concern could be more or less severe than previous variants: disease
severity does not necessarily create a selection advantage or disadvantage.[9, 10] For example if a
virus kills a host quickly then the virus has less opportunity to transmit to others. Similarly if the
disease is symptomatic and the symptoms develop soon after infection, causing the individual to
stay home or go to the hospital, then less transmission in the community will tend to occur.
However, the severity of disease caused in the host days or weeks after infection is less relevant to
ACT 1982
successful onward transmission of the SARS-CoV-2 compared to some other pathogens. This is
because SARS-CoV-2 is able to be transmitted for several days following infection without causing
severe disease, or even symptoms, in many or most people. Transmission from asymptomatic and
pre-symptomatic individuals has been a key feature of the success of SARS-CoV-2. It is unclear if a
new variant will be more or less severe, but greater intrinsic severity is certainly a possibility.[11]
Severity would be selected ’for’ if it also increases transmission, or it could be simply incidental to
the transmission advantage. For example:
INFORMATION
• Lower severity means that people who are infectious but remain asymptomatic or mildly
symptomatic continue to socialise and infect more people than if disease were more severe
and they stayed at home.
• A variant which results in more severe disease may also be associated with higher viral
shedding (causally or incidentally) and therefore be more transmissible, as appears to have
been the case with Delta.
• A variant associated with a higher likelihood of chronic infections (especially in
immunocompromised patients) may generate further subvariants with unknown
characteristics.
Caution should be used when describing some forms of COVID-19 as ’mild’, for several reasons. If a
variant is highly transmissible but relatively mild in a vaccinated individual, as we saw with Omicron,
the overall disease burden on the healthcare system and the community can still be huge. Secondly,
the disease may not be mild for many parts of our community, such as the elderly, Māori and Pacific
Peoples, the immunocompromised, those with underlying risk factors and comorbidities, and those
not up to date with their vaccinations; the disease associated with a variant may only be mild for
those who are otherwise healthy with prior immunity (from vaccination or prior infection), i.e., the
‘intrinsic’ severity may not be mild. Finally, the disease burden
RELEASED UNDER THE OFFICIAL of long COVID is still unknown, and
preliminary data indicates that long COVID can follow a mild or a severe acute phase of the disease.
Nonetheless, in the long run, the most likely scenario is that the existing ‘layers of immunity’ from
prior infection and vaccination will blunt the severity of disease caused by new variants. For example,
even though Omicron was substantially different to Delta, with respect to mutations in the spike
protein, population immunity conferred by vaccines and/or prior infection was effective in protecting
against severe disease, albeit that a third dose was essential to deliver the bulk of that protection.
With regard to the responses triggered by particular scenarios, there is a raft of public health
measures and surveillance that apply generally.[12] For example: continued surveillance of COVID-19
32

and new variants; accessible and timely treatments and ‘up to date’ vaccinations, particularly for
communities at greater risk; ventilation improvements; sufficient sick leave in order to enable
reduction in spread. Many of these measures are ‘pandemic preparedness’ measures that are
either already in place or would have to be put in place in advance, such as treatments, vaccinations,
ventilation and sick leave entitlements. If possible, other measures should be ready to be ‘stood
up’ quickly when needed. However, if the new variant is substantially better at transmitting than the
existing prevalent variant, then the speed of transmission may mean that some measures are unable
to be implemented in time.
However, endemicity – in the sense of the pattern of spread of COVID-19 becoming more ‘
predictable’ with potential seasonal variation – is not guaranteed in the short or medium te m.[13] It
is prudent to Document for less optimistic scenarios, as they still remain a possibility.[1]
Out of the scope of this document, but nonetheless a major long-term planning consideration, is the
burden of long COVID. Research on long COVID is still emerging – although some case definitions
ACT 1982
have been proposed, the wider research community has not yet settled on the general description
for the case definition of the syndrome, which is a necessary precursor to conducting most clinical
research.[14] Nonetheless, given high transmissibility, if even a small percentage of individuals suffer
disease burden in the long-term, then long COVID will shift to be a larger focus for the response to
COVID-19. Other long-term planning considerations such as public health infrastructure and
decision-making will also need to be considered.[15]
INFORMATION
Co-circulating variants: the balance between transmissibility and immune escape
The potential for more than one circulating and co existing variant is also considered, however
we given the limited evidence for this we have not planned for this or included it in modelling.
Co-circulating variants is when two or more variants have substantial immune escape from each
other (e.g., immunity associated with infection with variant one does not provide protection from
variant two, and vice versa) the more the two variants have distinct ecological niches and so are
able to co-exist without being in direct competition.
[5] This situation was common at the beginning of the pandemic with gradual replacement of the
original SARS-CoV-2 variant with Beta in Africa, Gamma in South America, Alpha in Europe and
Delta in India. The emergence of Omicron and other highly transmissible sub-variants has largely
replaced previous lineages. It is not known if multiple variants with different severity,
transmissibility and immune escape will be re-established, or if the pandemic will be dominated
by a single highly transmissible variant4.
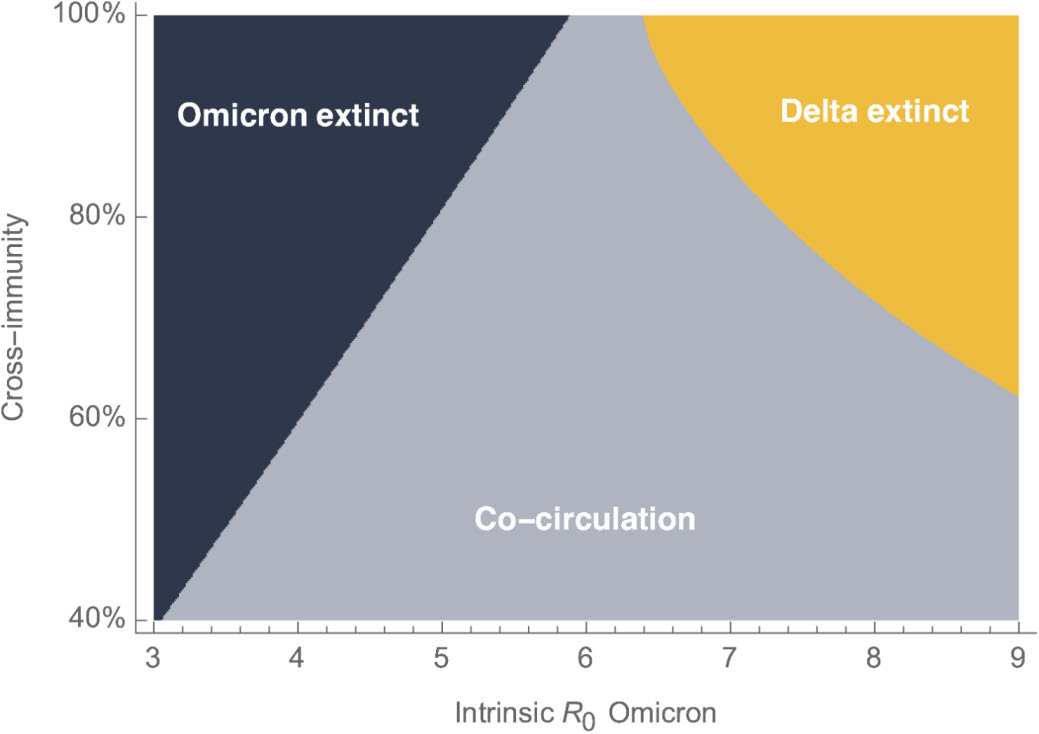
Figure 2 shows the relative balance between transmissibility (R0) and immune escape that is
needed for co-circulation to occur, i.e., if two variants have a similar R0and/or infection with one
does not provide protection from the other, then the two variants have the potential to co-
RELEASED UNDER THE OFFICIAL
circulate. In the case of Figure 2, calculations were performed to help determine if Delta and
Omicron may co-circulate. We now know that Omicron has a higher R0 than Delta, and that
Although Delta does still circulate globally in very low numbers, and the implications of that are still unclear
33

Omicron and Delta did not provide much cross-protection from each other for unvaccinated
individuals, but there was substantial cross protection when the individual was vaccinated.[3, 6]
Figure 2. Relative balance between transmissibility (R0) and immune escape needed for co-circulation to
occur
ACT 1982
INFORMATION
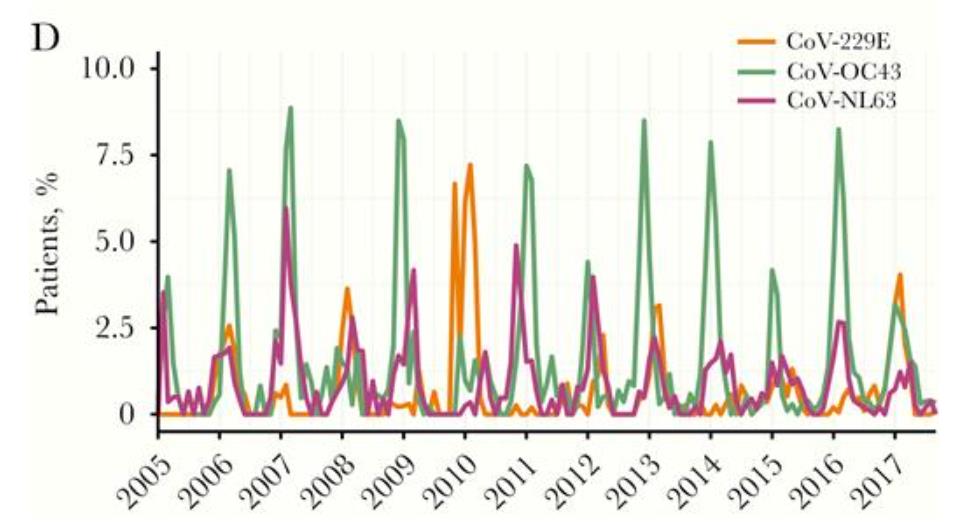
Co-circulation does occur between the other endemic coronaviruses that are associated with
influenza. However, some coronaviruses have a similar peak each season whereas others appear
to alternate as to how high the peak of infection is each year. This implies that some
coronaviruses potentially confer some cross-protection with each other, and others do not. Figure
3 below illustrates how this has been observed in Scotland in recent years.
Co-circulating variants may or may not be a final state for SARS-CoV-2, and even if it is, the
timing of when this will happen is unknown. It could be happening now, with BA4, BA5, and
BA2.12.1. BA.4 and BA5 are increasing at the same time in United Kingdom and other countries,
for example, or it may take a long time to settle into this pattern. Currently, there is evidence that
BA4 and BA5 now have evolved to be better at reinfecting than BA.2, and that this is part of an
overall trend of greater immune escape (from Delta to Omicron, and now between the successive
successful sub- ineages of Omicron).
It is not yet known how SARS-CoV-2 will behave seasonally, and the extent of any cross-
protection from future circulating coronaviruses.
RELEASED UNDER THE OFFICIAL
It is possible to get two or more co-circulating variants of SARS-CoV-2, we may have more
frequent COVID-19 waves each year, less so if there is some cross protection. Currently, even
Figure Error! Main Document Only. The combination of R0 and cross-immunity from two variants that might be needed in order for
two variants to co-circulate (labelled as Omicron and Delta). These two variants had the potential to co-circulate (grey region20) if the
cross-immunity was low or if Omicron’
s R0 was similar to Delta’
s (R0=6). If cross-immunity from Delta was high and Omicron’
s
R0 was relatively low compared to Delta’
s, then Omicron would become extinct (dark blue); conversely, if cross-immunity was high
and Omicron’s R0 was high, then Delta was predicted to become extinct (yellow). This analysis was performed prior to Omicron
becoming dominant. Link to figure: https://twitter.com/trvrb/status/1470420216232374281
34

without co-circulation. We are likely to see 3-4 pandemic waves a year for the short to medium
term, due to evolution within Omicron and waning of protection, albeit ‘mild’ disease due to
vaccines and prior immunity. Either way, this would still be a substantial increase in the overall
burden of disease, even though the severity is lower compared to the start of the pandemic
Figure 1 Monthly prevalence of seasonal coronaviruses (sCoVs) detected among patients with respiratory illness virologically
tested in NHS Greater Glasgow and Clyde, Scotland, United Kingdom, between January 2005 and September 2017. A, CoV-
229E. B, CoV-OC43. C, CoV-NL63. D, Comparing all sCoV types.
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
35

 Appendix 2: Modelling on Variants of Concern
Appendix 2: Modelling on Variants of Concern
We have conducted modelling based on the scenarios and differing levels of clinical severity and
immune escape to provide an indication of the range of potential health impacts. The modelling
is included in Appendix 2. The key points from the modelling are:
• variants with a high degree of immune escape or high virulence are the most concerning
ones; a variant with both would place very high loads on the hospital system.
• variants that reach the older population would place extremely high demands on hospital
and treatment capacity, and in some cases, very high mortality.
• the least severe hypothetical variants that respond to current vaccines would have effects
similar to the recent Omicron wave.
These are based on a purely hypothetical start date of 1 July.
ACT 1982
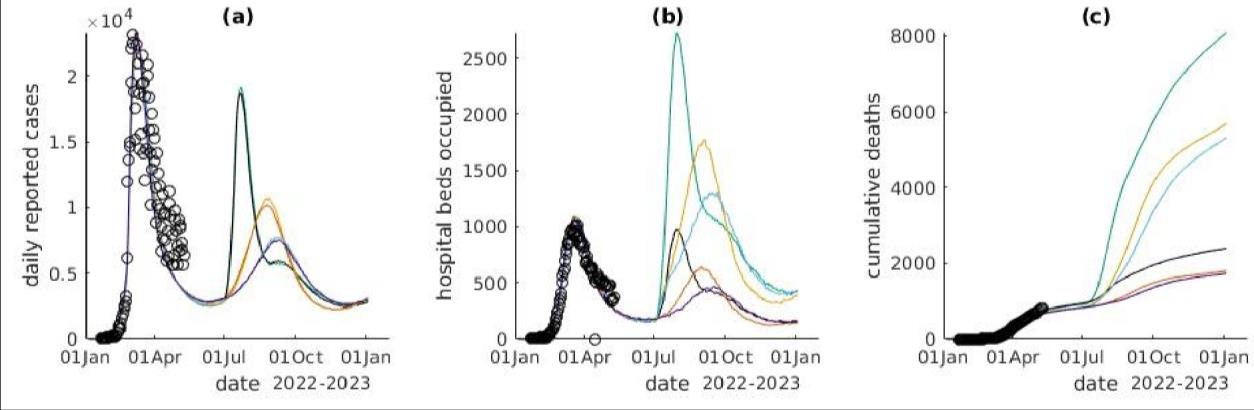
Figure 3: Cases (a), hospital occupancy (b), and deaths (c) by variant scenario
INFORMATION
In these scenarios, the population response is enough to keep cases below the March 2022 peak.
However if we assume no or a muted change in PHSMs or voluntary behaviour change the
numbers of cases, hospitalisations and deaths would be much higher.
RELEASED UNDER THE OFFICIAL
The pattern for hospitalisations is different: most scenarios with would see hospital occupancy
above March 2022 Omicron levels. The reason is the higher virulence in most scenarios, and that
the older population (who have higher case-hospitalisation and case-fatality rates) have the least
36

prior immunity. Additionally, they may be eligible for antivirals which may reduce their
hospitalisation rate (assuming antivirals are effective against a new variant.
After the initial peak, each scenario has a pattern of rebound and/or second wave. The timing of
these would be uncertain; they are due to the population relaxing social controls, and then to
waning immunity.
We noted that in some of the scenarios, hospital capacity is clearly exceeded; however the model
does not include any excess mortality or additional response if this were to happen.
The hospital workload in a normal winter is about the same as in the recent COVID-19 peak.
DHB’s winter planning work indicates that over 1,000 beds are needed for respiratory conditions
in peak winter months, 400 more than summer levels. An RSV outbreak could need another 900
beds over one month. This demand would be at the same time as any beds needed for COVID-19
patients.
ACT 1982
Assumptions that underpin the modelling
Each scenario assumes that the new Variant of Concern reaches New Zealand on July 2022. A variant
that arrives later could have less effect if more people experience prior infection before the
introduction of a new variant; but could also have larger effects if population immunity has waned
significantly. Current evidence is that immunity wanes noticeably over a period of several months.
The scenarios have been based on the effects of the Delta and Omicron variants. In general, Delta
INFORMATION
has been used as the model for a variant with greater severity than Omicron, while transmission and
immune escape are relative to Omicron.
We also note that the fifth planning scenario is for SARS-CoV-2 co-circulating with other
infectious diseases is not considered in these modelling scenarios.
The model is based on a number of hypothetical assumptions. Firstly it assumes that the population
would respond to news of a severe variant by reducing social mixing and increasing social distancing
even before any official change in the Community Protection Framework. This response likely
represents a mixture of public health interventions, such as the “Red” setting, and spontaneous
behaviour change in response to perceived risk. Examples include using masks, working from home,
and adopting the levels of precautionary behaviour seen in February 2022. Whether the response is
as effective as during February 2022 in flattening the curve is uncertain.
Table 3: Model settings for variant scenarios
Parameter
Variant 1
Variant 2
Variant 3
Variant 4
Variant 5
Intrinsic transmissibility
Omicron
Omicron
O
RELEASED UNDER THE OFFICIAL micron
Omicron
Omicron
(R0)
Severity of new variant
Probability of
Delta
Omicron
Delta
Omicron
Delta
hospitalisation
Probability of death
Delta
Omicron
Delta
Omicron
Delta
37
 Vaccine effectiveness against new variant
Vaccine effectiveness against new variant
Infection
60% relative
60% relative
Omicron
Omicron
Omicron
to Omicron*
to Omicron*
Severe disease
90% relative
90% relative
Omicron
Omicron
Omicron
to Omicron*
to Omicron*
Mortality
90% relative
90% relative
Omicron
Omicron
Omicron
to Omicron*
to Omicron*
Cross immunity to new variant from prior
infection with Omicron
Infection
50%**
50%**
80%***
80%***
Omicron
ACT 1982
Severe disease
94%**
94%**
100%***
100%***
Omicron
Mortality
94%**
94%**
100%***
100%***
Omicron
* Multipliers of the VE (vaccine effectiveness) parameters used for Omicron
** Immunity wanes rapidly
*** with faster reduction in immunity
INFORMATION
RELEASED UNDER THE OFFICIAL
38

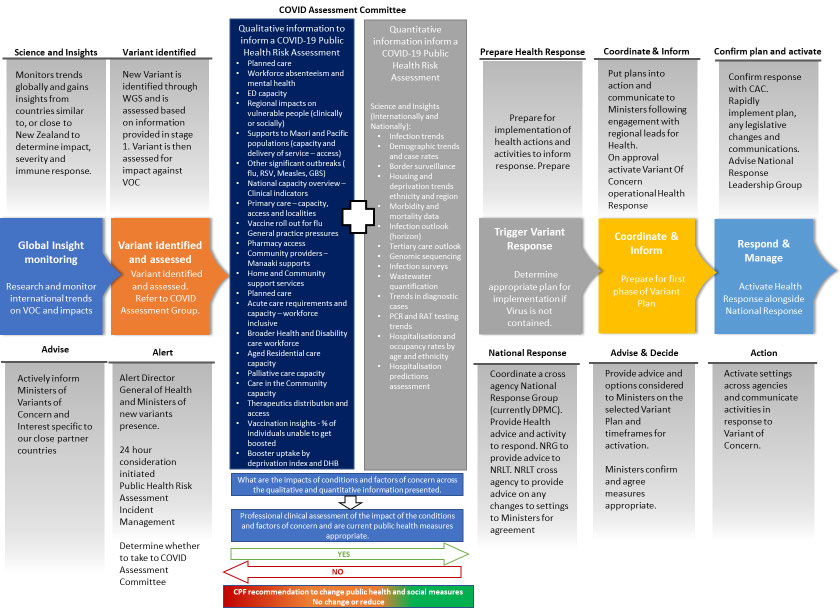 Appendix 3: Process for Identifying New Variants of Concern
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Appendix 3: Process for Identifying New Variants of Concern
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
39
 Appendix 4: Proposed response to scenarios
Appendix 4: Proposed response to scenarios
Note: This appendix did not eventuate. As such, there is no further information.
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
40
 References
References
1.
Farrar, J. Two years of the covid-19 pandemic. 2022 22 March 2022; Available from:
https://www.economist.com/podcasts/2022/03/22/two-years-of-the-covid-19-pandemic.
2.
Maher, M.C., et al., Predicting the mutational drivers of future SARS-CoV-2 Variants of Concern.
Sci Transl Med, 2022. 14(633): p. eabk3445.
3.
WHO. Tracking SARS-CoV-2 variants. Tracking SARS-CoV-2 variants 2022 12 April 2022 [cited
2022 22 April 2022]; Available from: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/.
4.
CDC, U. SARS-CoV-2 Variant Classifications and Definitions. Variant Surveil ance 2021 01
December 2021 [cited 2022 22 April 2022]; Available from: https://www.cdc.gov/coronavirus/2019-
ncov/variants/variant-classifications.html.
ACT 1982
5.
Metcalf, C.J.E. The Evolutionary ecology of coronaviruses (Mar 10). CCDD ID Epi Spring Seminar
Series 2022 [Youtube] 2022 14 March 2022 [cited 2022 15 April 2022]; Available from:
https://ccdd.hsph.harvard.edu/id-epi-series-2022/.
6.
Bedford, T. Continuing SARS-CoV-2 evolution under population immune pressure. Vaccines and
Related Biological Products Advisory Committee April 6, 2022 2022 06 April 2022 [cited 2022 15 April
2022]; Available from: https://www.fda.gov/media/157471/download.
7.
Bhattacharyya, R.P. and W.P. Hanage, Challenges in Inferring Intrinsic Severity of the SARS-CoV-2
INFORMATION
Omicron Variant. N Engl J Med, 2022. 386(7): p. e14.
8.
Fauci, A., In conversation with Dr Anthony Fauci, in Preparing for the worst, hoping for the best, E.
Carr, Editor. 2022, The Economist: https://www.economist.com/films/2022/03/24/in-conversation-with-
dr-anthony-fauci.
9.
Katzourakis, A., COVID-19: endemic doesn't mean harmless. Nature, 2022. 601(7894): p. 485.
10.
Markov, P.V., A. Katzourakis, and N.I. Stilianakis, Antigenic evolution wil lead to new SARS-CoV-2
variants with unpredictable severity. Nat Rev Microbiol, 2022. 20(5): p. 251-252.
11.
Andersen, K., In the Bubb e with Andy Slavitt, in The Country That Decided the Pandemic Is Over
(with Kristian Andersen), A. Slavitt, Editor. 2022: https://omny.fm/shows/in-the-bubble/the-country-that-
decided-the-pandemic-is-over-with.
12.
Hanage, W. From ‘herd immunity’ to today, Covid minimisers are still sabotaging our
pandemic progress Guardian 2022 29 March 2022 [cited 2022 15 April 2022]; Media article]. Available
from: https://www.theguardian.com/commentisfree/2022/mar/29/herd-immunity-covid-minimisers-
sabotaging-pandemic-progress.
13.
Callaway, E., Beyond Omicron: what's next for COVID's viral evolution. Nature, 2021. 600(7888): p.
204-207.
RELEASED UNDER THE OFFICIAL
14.
World Health Organisation. A clinical case definition of post COVID-19 condition by a Delphi
consensus, 6 October 2021. 2021 06 October 2021 [cited 2022 15 April 2022]; Available from:
https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-
Clinical_case_definition-2021.1.
15.
Baker M, W.N. New Zealand’s Covid strategy was one of the world’s most successful – what
can we learn from it? Comment is free 2022 05 April 2022 [cited 2022 21 April 2022]; Available from:
https://www.theguardian.com/world/commentisfree/2022/apr/05/new-zealands-covid-strategy-was-one-
of-the-worlds-most-successful-what-can-it-learn-from-it.
41