From:
Sarah Fitt
Sent:
Friday, 4 March 2022 8:45 AM
To:
Lisa Williams; Andrew Oliver
Cc:
Adrienne Martin; Caroline De Luca; Peter Alsop; Allanah Andrews; Jane Wright
Subject:
RE: 2022-03-02 Memo to proceed: Influenza vaccine widened access consultation
(A1573477)
All fine with me and agree with the plan
Ngā mihi,
Sarah
Sarah Fitt | Chief Executive
___________________________________________________________________
PHARMAC | Te Pātaka Whaioranga | PO Box 10-254 | Level 9, 40 Mercer Street, Wellington
9 (2) (b) (ii)
-----Original Message-----
From: Lisa Williams <[email address]>
Sent: Friday, 4 March 2022 8:38 AM
To: Andrew Oliver <[email address]>
Cc: Adrienne Martin <[email address]>; Caroline De Luca <[email address]>;
Sarah Fitt <[email address]>; Peter Alsop <[email address]>; Allanah Andrews
<[email address]>; Jane Wright <[email address]>
Subject: 2022-03-02 Memo to proceed: Influenza vaccine widened access consultation (A1573477)
Hi Andrew, thanks for the comprehensive memo.
I'm happy to endorse going ahead with consultation on this proposal (subject to any comment from SF), however
I'm not comfortable with the timing.
Rachel M from the MOH called me last night to say that the draft briefing to Vaccine ministers was going in the DG's
overnight reading bag and it would go across to Ministers to go in their weekend bags. Rach was going to confirm to
me today the planned timing for any meeting of Ministers to discuss the briefing, but she thought it would likely be
discussed on Monday at some stage.
On that basis, I would prefer that we send a 'no surprises' to Minister Little today about our intention to issue a
truncated consultation early next week (and make mention of the briefing that we are aware Ministers will be
receiving today). Then we issue our consultation on Monday or Tuesday next week. I am comfortable, that given
the urgency caused by Covid and the impending start of the flu vaccination programme that our consultation period
is less than 10 days.
Lisa
Lisa Williams has sent you a link to "2022-03-02 Memo to proceed: Influenza vaccine widened access consultation"
(A1573477) from Objective.
Open in Navigator
1
Double click on the attachment
Open in Supported Application
url:objective://id:[email address]:8643
Open in Your Browser
Latest: https://objective.pharmac.govt.nz:8643/id:A1573477/document/versions/latest
Published:
https://objective.pharmac.govt.nz:8643/id:A1573477/document/versions/published
2
From:
Allanah Andrews
Sent:
Friday, 4 March 2022 3:09 PM
To:
Senior Leadership Team; Engagement & Implementation Managers
Cc:
Stephen Tat; Adrienne Martin; Caroline De Luca; Jane Wright; Andrew Oliver
Subject:
FW: No surprises update - public consultation for influenza vaccination
FYI
From: Allanah Andrews
Sent: Friday, 4 March 2022 3:05 pm
To: Haley Ataera <[email address]>; Adelia Hallett <[email address]>
Cc: Carol Morris <[email address]>; Lisa Williams <[email address]>;
[email address]
Subject: No surprises update - public consultation for influenza vaccination
Kia ora Haley
This is a no surprises update for the Minister relating to Pharmac’s intention to publicly consult on widening the
access criteria for funded influenza vaccinations in 2022. Consultation is planned for early in the week beginning 7
March 2022.
Pharmac intends to consult on a proposal to widen access to the influenza vaccine for Māori and Pacific peoples
from 55 to 64 years for the 2022 season. Continued funding for future seasons will be considered as a separate
funding decision.
The consultation period will likely be shorter than our normal practice. Given the urgency caused by the current
COVID-19 situation and impending start to the influenza vaccination season we consider this to be reasonable.
A decision on whether to expand access will be made in time for the commencement of the influenza vaccination
season, 1 April 2022.
Pharmac has been working closely with the Ministry of Health on the 2022 influenza vaccination programme and are
aware the Minister is likely to receive advice on the approach to the 2022 programme today (Friday 4 March).
We intend to put out a media release, to accompany the consultation, with a link to our website for more
information. Pharmac’s director of operations Lisa Williams will be Pharmac’s spokesperson and available for
interviews.
Please let me know if you would like any further information.
Ngā mihi / Warm Regards,
Allanah Andrews (she/her) | Manager, Policy and Government Services
Te Pātaka Whaioranga | Pharmac
PO Box 10-254, Wellington 6140 | Level 9, 40 Mercer Street, Wellington 6011
9 (2) (b) (ii)
| www.pharmac.govt.nz
1
 MINUTE OF THE DIRECTOR OF OPERATIONS DECISION UNDER
DELEGATED AUTHORITY
JUNE 2022
MINUTE OF THE DIRECTOR OF OPERATIONS DECISION UNDER
DELEGATED AUTHORITY
JUNE 2022
The Director of Operations, exercising the authority delegated by the Chief Executive under
the Financial Delegations Policy has made the following decision to:
resolve to amend the eligibility criteria for Influenza vaccine inj 60 mcg in 0.5 ml
syringe (quadrivalent vaccine) (Afluria Quad) in Section I of the Pharmaceutical
Schedule from 1 July 2022 (additions in bold):
A. INFLUENZA VACCINE – people 3 years and over
is available each year for patients aged 3 years and over who meet the following criteria, as
set by Pharmac:
a. all people 65 years of age and over; or
b. people 55 to 64 years of age (inclusive) who are Māori or any Pacific ethnicity; or
c. people under 65 years of age who:
i.
have any of the following cardiovascular diseases:
a. ischaemic heart disease, or
b. congestive heart failure, or
c. rheumatic heart disease, or
d. congenital heart disease, or
e. cerebrovascular disease; or
ii.
have either of the following chronic respiratory diseases:
a. asthma, if on a regular preventative therapy, or
b. other chronic respiratory disease with impaired lung function; or
iii.
have diabetes; or
iv.
have chronic renal disease; or
v.
have any cancer, excluding basal and squamous skin cancers if not invasive;
or
vi.
have any of the following other conditions:
a. autoimmune disease, or
b. immune suppression or immune deficiency, or
c. HIV, or
d. transplant recipients, or
e. neuromuscular and CNS diseases/disorders, or
f.
haemoglobinopathies, or
g. are children on long term aspirin, or
h. have a cochlear implant, or
i.
errors of metabolism at risk of major metabolic decompensation, or
j.
pre and post splenectomy, or
k. down syndrome, or
vii.
are pregnant; or
d. children 3 and 4 years of age (inclusive) who have been hospitalised for respiratory
illness or have a history of significant respiratory illness; or
e. people under 65 years of age who:
i) have any of the following serious mental health conditions:
a. schizophrenia; or
b. major depressive disorder; or
c. bipolar disorder; or
d. schizoaffective disorder; or
ii) are currently accessing secondary or tertiary mental health and addiction
services; or
A1597908 - qA60567

f.
children 3 to 12 years of age (inclusive), from 1 July 2022 to 31 December 2022;
Unless meeting the criteria set out above, the following conditions are excluded from funding:
a
asthma not requiring regular preventative therapy,
b
hypertension and/or dyslipidaemia without evidence of end-organ disease.
B. Contractors will be entitled to claim payment for the supply of influenza vaccine to patients
eligible under the above criteria pursuant to their contract with Heath NZ for subsidised
immunisation, and they may only do so in respect of the influenza vaccine listed in the
Pharmaceutical Schedule.
C. Contractors may only claim for patient populations within the criteria that are covered by their
contract, which may be a sub-set of the population described in paragraph A above.
resolve to amend the restriction criteria for Influenza vaccine inj 60 mcg in 0.5 ml
syringe (quadrivalent vaccine) (Afluria Quad) in Part II of Section H of the
Pharmaceutical Schedule from 1 July 2022 (new criteria shown only):
Restricted
Initiation – Serious mental health conditions or addiction
Any of the following:
1. schizophrenia; or
2. major depressive disorder; or
3. bipolar disorder; or
4. schizoaffective disorder; or
5. person is currently accessing secondary or tertiary mental health and addiction
services.
Initiation – children from 3 to 12 years of age (inclusive)
Children 3 to 12 years of age (inclusive) from 1 July 2022 to 31 December 2022.
resolve that no consultation on this proposal is required.
note that we recently consulted on a proposal to fund influenza vaccine for Māori and
Pacific peoples from 55 to 64 years of age in March 2022 and received consultation
feedback supporting funding for school aged children and people with serious mental
health conditions.
note that the widened access for children 3 to 12 years age is only for the 2022
influenza season, while widened access for serious mental health or addiction is for
2022 and future seasons.
A1597908 - qA60567
 MEMORANDUM FOR CONSIDERATION BY DIRECTOR OF OPERATIONS
MEMORANDUM FOR CONSIDERATION BY DIRECTOR OF OPERATIONS
UNDER DELEGATED AUTHORITY
To:
Director of Operations
From:
Manager Pharmaceutical Funding
Date:
21 June 2022
__________________________________________________________________________
Influenza vaccine widened access for children 3-12 years of age and people
with serious mental health conditions or addiction
Recommendations
It is recommended that having regard to the decision-making framework set out in
PHARMAC's Operating Policies and Procedures you exercise your delegated authority and:
resolve to amend the eligibility criteria for Influenza vaccine inj 60 mcg in 0.5 ml
syringe (quadrivalent vaccine) (Afluria Quad) in Section I of the Pharmaceutical
Schedule from 1 July 2022 (additions in bold):
A.
INFLUENZA VACCINE – people 3 years and over
is available each year for patients aged 3 years and over who meet the following criteria, as
set by Pharmac:
a. all people 65 years of age and over; or
b. people 55 to 64 years of age (inclusive) who are Māori or any Pacific ethnicity; or
c. people under 65 years of age who:
i.
have any of the following cardiovascular diseases:
a. ischaemic heart disease, or
b. congestive heart failure, or
c. rheumatic heart disease, or
d. congenital heart disease, or
e. cerebrovascular disease; or
ii.
have either of the following chronic respiratory diseases:
a. asthma, if on a regular preventative therapy, or
b. other chronic respiratory disease with impaired lung function; or
iii.
have diabetes; or
iv.
have chronic renal disease; or
v.
have any cancer, excluding basal and squamous skin cancers if not invasive;
or
vi.
have any of the following other conditions:
a. autoimmune disease, or
b. immune suppression or immune deficiency, or
c. HIV, or
d. transplant recipients, or
e. neuromuscular and CNS diseases/disorders, or
f.
haemoglobinopathies, or
g. are children on long term aspirin, or
h. have a cochlear implant, or
i.
errors of metabolism at risk of major metabolic decompensation, or
A1596684 – T22-1368
j.
pre and post splenectomy, or
k. down syndrome, or
vii.
are pregnant; or
d. children 3 and 4 years of age (inclusive) who have been hospitalised for respiratory
illness or have a history of significant respiratory illness; or
e. people under 65 years of age who:
i) have any of the following serious mental health conditions:
a. schizophrenia; or
b. major depressive disorder; or
c. bipolar disorder; or
d. schizoaffective disorder; or
ii) are currently accessing secondary or tertiary mental health and addiction
services; or
f.
children 3 to 12 years of age (inclusive), from 1 July 2022 to 31 December 2022;
Unless meeting the criteria set out above, the following conditions are excluded from funding:
a
asthma not requiring regular preventative therapy,
b
hypertension and/or dyslipidaemia without evidence of end-organ disease.
B. Contractors will be entitled to claim payment for the supply of influenza vaccine to patients
eligible under the above criteria pursuant to their contract with Heath NZ for subsidised
immunisation, and they may only do so in respect of the influenza vaccine listed in the
Pharmaceutical Schedule.
C. Contractors may only claim for patient populations within the criteria that are covered by their
contract, which may be a sub-set of the population described in paragraph A above.
resolve to amend the restriction criteria for Influenza vaccine inj 60 mcg in 0.5 ml
syringe (quadrivalent vaccine) (Afluria Quad) in Part II of Section H of the
Pharmaceutical Schedule from 1 July 2022 (new criteria shown only):
Restricted
Initiation – Serious mental health conditions or addiction
Any of the following:
1. schizophrenia; or
2. major depressive disorder; or
3. bipolar disorder; or
4. schizoaffective disorder; or
5. person is currently accessing secondary or tertiary mental health and addiction
services.
Initiation – children from 3 to 12 years of age (inclusive)
Children 3 to 12 years of age (inclusive) from 1 July 2022 to 31 December 2022.
resolve that no consultation on this proposal is required.
note that we recently consulted on a proposal to fund influenza vaccine for Māori and
Pacific peoples from 55 to 64 years of age in March 2022 and received consultation
feedback supporting funding for school aged children and people with serious mental
health conditions.
note that the widened access for children 3 to 12 years age is only for the 2022
influenza season, while widened access for serious mental health or addiction is for
2022 and future seasons.
A1596684 – T22-1368
2
SUMMARY OF PHARMACEUTICAL – INFLUENZA VACCINE – CHILDREN 3-12 YEARS OF AGE
Brand name
Afluria Quad
Chemical name
Influenza vaccine
Therapeutic Group
Vaccines
Presentation
Inj 60 mcg in 0.5 ml
syringe
Supplier
Sanofi Pasteur
Pharmaceutical type
Restriction change
MoH Restriction
Prescription medicine
Application date
March 2022
Market data
YE 30
YE 30
YE 30
YE 30
YE 30
June
June
June
June
June
2023
2024
2025
2026
2027
Number of patients
650,510
Number of Māori / Pacific peoples
272,590
9 (2) (b) (ii)
Community
Subsidy (gross)
Pharmaceutical
Expenditure
Net cost of
community
pharmaceuticals
Net present
value (NPV)
TOTAL –
Net cost to CPB
Combined
Pharmaceutical
Net present
Budget
value
Other DHB
Distribution
$0
$0
$0
$0
$0
costs
costs
Other costs to
$7,670,000
$0
$0
$0
$0
DHBs
Net other costs
$7,670,000
$0
$0
$0
$0
to DHBs
Net present
$7,670,000
value (NPV)
9 (2) (b) (ii)
TOTAL
Total cost to
DHBs
Net present
value (NPV)
Notes:
1.
Number of patients = number of new patients in each financial year.
2.
Subsidy (gross) = forecast of all spending at the current subsidy.
3.
Net cost of community pharmaceuticals = forecast of change in total spending on pharmaceuticals listed in the
Schedule compared with status quo. Costs would be recovered from the COVID-19 Response and Recovery
Fund (CRRF).9 (2) (b) (ii)
4.
Other costs to DHBs = Cost of the Immunisation Benefit paid to vaccinators by MoH (Health NZ) for
administering vaccines less savings from reduced hospitalisations and outpatient admissions.
5.
Total cost to DHBs = net cost to the Schedule plus net cost to DHBs.
6.
All costs are expressed ex-manufacturer, ex-GST.
7.
NPV is calculated over 5 years using an annual discount rate of 8%.
8.
Calculations are in A1596684.
A1596684 – T22-1368
3
SUMMARY OF PHARMACEUTICAL – INFLUENZA VACCINE – SERIOUS MENTAL HEALTH OR ADDICTION
Brand name
Afluria Quad
Chemical name
Influenza vaccine
Therapeutic Group
Vaccines
Presentation
Inj 60 mcg in 0.5 ml
syringe
Supplier
Sanofi Pasteur
Pharmaceutical type
Restriction change
MoH Restriction
Prescription medicine
Application date
March 2022
Market data
YE 30
YE 30
YE 30
YE 30
YE 30
June
June
June
June
June
2023
2024
2025
2026
2027
Number of patients
174,000
177,000
180,000
182,000
185,000
Number of Māori / Pacific peoples
19 281
20 888
22 495
24 101
25 708
9 (2) (b) (ii)
Community
Subsidy (gross)
Pharmaceutical
Expenditure
Net cost of
community
pharmaceuticals
Net present
value (NPV)
TOTAL –
Net cost to CPB
Combined
Pharmaceutical
Net present
Budget
value
Other DHB
Distribution
$0
$0
$0
$0
$0
costs
costs
Other costs to
$880,000
$970,000
$1,050,000
$1,150,000
$1,240,000
DHBs
Net other costs
$880,000
$970,000
$1,050,000
$1,150,000
$1,240,000
to DHBs
Net present
$4,500,000
value (NPV)
9 (2) (b) (ii)
TOTAL
Total cost to
DHBs
Net present
value (NPV)
Notes:
1.
Number of patients = number of new patients in each financial year.
2.
Subsidy (gross) = forecast of all spending at the current subsidy.
3.
Net cost of community pharmaceuticals = forecast of change in total spending on pharmaceuticals listed in the
Schedule compared with status quo. 9 (2) (b) (ii)
9 (2) (b)
4.
Other costs to DHBs = Cost of the Immunisation Benefit paid to vaccinators by MoH (Health NZ) for
(ii)
administering vaccines less savings from reduced hospitalisations and outpatient admissions.
5.
Total cost to DHBs = net cost to the Schedule plus net cost to DHBs.
6.
All costs are expressed ex-manufacturer, ex-GST.
7.
NPV is calculated over 5 years using an annual discount rate of 8%.
8.
Calculations are in A1596684.
A1596684 – T22-1368
4
Why proposal should be considered by the Director of Operations under Delegated
Authority
The proposal involves a Schedule change that has an estimated Financial Impact (NPV) of
less than $10,000,000 and:
will not result in the Pharmaceutical budget or its future funding path being exceeded;
is not inconsistent with previous Board decisions; and
is not considered contentious by Pharmac staff.
Background and Analysis
Background
Border restrictions and other COVID-19 related public health measures have
resulted in very little influenza virus circulating in the community for the last two
years. Our clinical advisors have told us that the lack of community exposure to the
influenza virus is likely to have reduced the natural level immunity in the New
Zealand population. We are aware that the opening of New Zealand’s international
border is likely to increase the risk of severe illness from influenza for people at
high risk.
We widened access to influenza vaccine for the 2022 season (beginning 1 April
2022)
for Māori and Pacific peoples from the earlier age of 55 to 64 years,
recognising that Māori and Pacific populations have a younger age distribution than
other population groups and a high incidence of comorbidities.
The Ministry has been engaging with us to scope possible options for further
widened access to flu vaccine for the 2022 season, in the context of current uptake
figures indicating likely surplus stock the end of the 2022 season, and recent
widening of access by several states in Australia due to the heightened risk.
Pharmac worked with the contracted vaccine supplier to ensure that two million
doses would be available for the 2022 season, to allow for high uptake due to the
heightened risk of severe illness from influenza, and to reduce hospitalisations
during a period when the sector is under strain managing COVID-19 cases. As of
16 June 2022, 1.4 million doses of vaccine have been distributed, approximately
the same as the same time in 2021. Staff note that the distribution rate has slowed
considerably in early June and forecast that the final distribution total is likely to be
1.5 to 1.6 million doses. This would result in unused stock of 400,000 to 500,000
doses.
To ensure the availability of two million doses, 9 (2) (b) (ii)
9 (2) (b) (ii)
9 (2) (b) (ii)
9 (2) (b) (ii)
9 (2) (b) (ii)
At current
usage rates, staff estimate the likely cost of unsold stock at the end of the season
would be 9 (2) (b) (ii)
to the COVID-19 Response and Recovery Fund (CRRF).
Proposal
This proposal is to widen access to influenza vaccine from 1 July 2022 for two
A1596684 – T22-1368
5
groups:
o Children 3-12 years of age (inclusive), only for the 2022 influenza season;
and
o People with serious mental health conditions or addiction, for the 2022 and
future influenza seasons.
Children 3-12 years of age (inclusive)
If approved, this widened access is expected to reduce the impact of influenza not
only on the children themselves, but on the whole population, particularly older
high-risk populations during the COVID-19 pandemic (with consequent pressure on
the health system through epidemic influenza with ICU and hospital admissions,
affecting COVID-19 hospital care). This would be by reducing the transmission of
influenza
in 3 to 12 year olds (who have a high incidence of influenza infection),
and thus reducing wider community transmission. The Afluria Quad influenza
vaccine is approved by Medsafe for people aged 3 years and over.
Widened access for children aged 3-12 years would only be available for the 2022
influenza season, and continued funding for future seasons would be assessed as
a separate proposal.
We did not receive clinical advice directly supporting the age range from 3-12
years, but it is a combination of two of the recommended age groups (all school
aged children and children under 5 years), and is in line with the quantity of vaccine
that is expected to be surplus at the end of the season with the current distribution
pattern. Staff note that Afluria Quad is approved by Medsafe for use in children
from 3 years of age, so the proposal includes children from 3 years as well as
primary school-aged children. Staff note that there is insufficient stock of Afluria
Quad Junior to widen access to children under 3 years.
Staff note that our clinical advisors considered that changes requiring a targeted
recall programme to reach the right people would be challenging for vaccination
providers to implement. We have raised this with the Ministry who are responsible
for the implementation of immunisation programmes. The Ministry remains
supportive of the proposal and has advised that pharmacists can now administer
influenza vaccine to children from 3 years of age and will be a key provider for
supporting the proposed widened access.
This proposal addresses health needs related to reduced population immunity,
secondary to public health measures taken to reduce community transmission of
COVID-19 which have reduced population immunity to influenza and other
respiratory disease. Therefore staff consider the costs would be recovered from the
COVID-19 Response and Recovery Fund (CRRF), and it would be appropriate to
progress this proposal, despite it not being ranked on the OFI.
People with serious mental health conditions or addiction
This proposal is currently ranked at 9 (2) on the Options for Investment list. A
(b)
smaller sub-group of this proposal is currently ranked at 9 (2) on the Options for
Investment list. We note that at this time it is estimated that there are sufficient
(b) (ii)
funds in the Combined Pharmaceutical Budget for FYR 2022/23 to progress this
proposal 9 (2) (b) (ii)
9 (2) (b) (ii)
As this proposal has been ranked on the OFI and we consider it good value for
money, it would be funded from the CPB for the 2022/23 FY and future years.
A1596684 – T22-1368
6
Agreement (if applicable)
There is an existing agreement with Seqirus for the supply of influenza vaccine,
dated 9 May 2019. The agreement resulted from a Request for Proposals (RFP)
dated 20 November 2018. No changes to this contract are included as part of this
proposal.
Health Need
Influenza can be a serious illness that is sometimes fatal. Infection with the
influenza virus may need treatment in hospital for people of any age, but
particularly for people who are elderly or have an ongoing medical condition.
Influenza can worsen existing medical conditions such as asthma or diabetes.
Influenza infection rates are highest in children. For example, in the SHIVERS
(Southern Hemisphere Influenza and Vaccine Effectiveness Research and
Surveillance) study (covering Auckland/Counties Manukau DHBs 2012-13) 26% of
influenza infections reported were in children under 5 years of age, and 31% were
in school aged children 5-
19 years (Huang et al. Influenza Other Respir Viruses.
2015; 9:179-90).
Influenza vaccine is currently funded for all people 65 years of age and older as
well as other high-risk groups, however, vaccination rates are much lower for Māori
and Pacific peoples compared to the wider non-Māori, non-Pacific population.
Māori and Pacific peoples have a younger age distribution than other population
groups and a high incidence of comorbidities. The relative risk of hospitalisation for
influenza infection (and its complications) is higher for Māori and Pacific peoples
than the wider population, across all age groups.
The significant health need of people with serious mental health conditions or
addiction have been noted, in the context of influenza immunisation, by both the
Immunisation Subcommittee
(August 2021) and PTAC (February 2022). Māori
experience higher rates of mental illness, higher rates of suicide and greater
prevalence of addictions than the wider population (Mental Health and Addiction
Inquiry 2018).
These funding applications
align with the following Government health priorities:
o Child wellbeing: To improve child wellbeing and support children to have a
healthy start in life, noting the impact of influenza in children
o Prevention: To improve wellbeing by preventing health conditions, which
includes immunisation against infectious diseases.
o Health equity: To better population outcomes, noting the disproportionate
representation of influenza infection in Māori, Pacific peoples, and those
living in high socioeconomic deprivation.
o Infectious disease is also listed as a priority condition, which includes
immunisation to prevent infectious diseases.
o Mental health and respiratory or listed among Pharmac’s Māori health areas
of focus.
Health Benefit
Influenza vaccine is funded each year for a range of people, including those 65
years and older, in pregnancy, and for people with medical conditions such as
A1596684 – T22-1368
7
heart disease, respiratory conditions, diabetes, renal disease, and autoimmune
diseases. It is also funded for Māori and Pacific peoples from 55 years of age. Over
1.4 million people are usually vaccinated annually (funded and privately
purchased).
The Afluria Quad and Afluria Quad Junior are the only funded influenza vaccines
for the 2022 season and this proposal relates to only the Afluria Quad vaccine. It is
a quadrivalent vaccine, protecting against four strains of influenza virus. For the
2022 season, the strains included are: A/Victoria, A/Darwin, B/Austria and
B/Phuket.
The Immunisation Subcommittee (May 2018) has commented that vaccination of
primary school age children contributes to herd immunity, protecting high risk
individuals who may respond less well to vaccines.
Both the Immunisation
Subcommittee (August 2021) and PTAC (February 2022)
have considered that although there is not strong empirical evidence for health
benefit from influenza vaccine in people with serious mental health conditions or
addiction, there is good biological and psychosocial plausibility for benefit.
Immunisation Advisory Committee View
Children 3-12 years of age (inclusive)
In March 2022, members of the Immunisation Advisory Committee provided clinical
advice by email about options for widened access to influenza vaccine. Members
considered that there is likely to be low immunity to influenza in the community due
to border restrictions and other public health measures to manage COVID-19. With
the opening of international borders we are aware that this is likely to increase the
risk of severe illness from influenza for people at high risk.
Members considered that open access for the highest risk age groups, such as
children under 5 years of age and people over 55 years of age would be their
preferred approach. Members highlighted that there are also other high needs
groups that were not included in the options under discussion, such as people with
serious mental health or addiction issues. Members also noted that funding for a
range of additional groups would be desirable, such as: all children under 5 years
of age, school aged children, all people from 55-64 years of age, Māori and Pacific
peoples aged 50-64 years, and Community Services Card holders.
Members considered that COVID-19 has had a major impact on the workload of
General Practitioners, pharmacists and other organisations that are involved in
providing vaccination services. Members considered that this proposed change
would be challenging for vaccination providers to implement a targeted recall
programme to reach the right people.
Full details of the advice provided is available fro
m fA312477.
The Immunisation Advisory Committee provided further clinical advice at its May
2022 meeting. The Committee noted that most members’ preferred option for
widened access was open access for all ages, or some priority groups such as
school aged children, or those from 6 months to 5 years of age.
The draft record of this advice is available from A1585874.
A1596684 – T22-1368
8
People with serious mental health conditions or addiction
The Immunisation
Subcommittee (August 2021) recommended influenza vaccine
for people with serious mental health conditions or addiction be listed with a
medium priority (within the context of vaccines and immunisation). Such listing was
recommended subject to eligibility criteria, in effect to include:
1. people with a serious mental health condition (schizophrenia, major depressive
disorder, bipolar disorder, or schizoaffective disorder); and
2. people currently accessing secondary and tertiary mental health and addiction
service.
Both the Immunisation
Subcommittee, in August 2021, and later PTAC (February
2022) noted the significant health need of people with serious mental health
conditions or addiction, and considered that although there was not strong
empirical evidence for health benefit [from influenza vaccine] in this group, there
was good biological and psychosocial plausibility for benefit.
PTAC noted and agreed with the Subcommittee’s recommendation that influenza
vaccine for people with serious mental health conditions or addiction be listed with
a medium priority.
Advisor Conflicts of Interest
All declared conflicts of interest for any clinical advisors who contributed to the above
advice, and actions taken to manage the conflicts, are recorded in the relevant minutes.
Consequences for the health system
The Ministry’s National Immunisation Programme team (NIP) has advised that it is
supportive of the proposed widened access for both children 3-12 and for people
with serious mental health conditions or addiction, and can support an
implementation date of 1 July 2022. The NIP provided the following details of how it
intends to support the implementation of widened access, which address the
Immunisation Advisory Committee concerns about implementing targeted
immunisation programmes late in the influenza season:
o The National Immunisation Programme (NIP) supports Pharmac further
extending the influenza eligibility criteria for the 2022 season. The NIP will
work with the sector including pharmacy, who are instrumental in the
delivery of the 2022 influenza programme, to communicate
the eligibility change. With the recent amendments to the Medicine
Regulations 1984, pharmacists can now vaccinate people aged 3+
years and will be a key provider for vaccinating people who meet the
expanded criteria. The NIP will also engage with the Mental Health and
Addiction directorate to provide support and ensure eligible people can
access the funded influenza vaccine.
o NIP has advised that it is urgently seeking approval of funding for the
Immunisation Benefit costs associated with widened access.
Suitability
Influenza vaccine (Afluria Quad) has been approved by Medsafe for the prevention
of influenza caused by Influenza Virus, Types A and B contained in the vaccine. It
is approved for use in people 3 years of age and older.
A1596684 – T22-1368
9
Each 0.5 ml dose of the vaccine is supplied in a prefilled syringe with needle
included.
Costs and Savings
Children 3-12 years of age (for 2022 only)
This proposal would not result in any additional expenditure to the CPB or
CRRF as the stock that would be used for the widened access 9 (2) (b) (ii)
9 (2) (b) (ii)
rom the CRRF.
The proposal to fund this group would benefit up to 650,000 children, although
staff estimate that uptake would be unlikely to exceed 55% as it is late in the
influenza season and parents would need to take the children to their GP or
local pharmacy for vaccination.
The financial impact assumes 55% uptake of the proposed group. While this
uptake is likely higher than might be achieved, it is difficult to estimate
accurately as it is dependent on the implementation plans put in place by the
Ministry of Health. The Ministry has advised us that it intends to leverage
mechanisms established to target populations for COVID-19 vaccinations, so
staff do not consider it unreasonable to assume a greater uptake (ie 55%) than
might otherwise be achieved.
This proposal would incur costs to the Ministry of Health (Health NZ from 1 July
2021) of $8,300,000 for the Immunisation Benefit paid to vaccinators for
administering influenza vaccine. The would be offset by savings of $630,000
from reduced hospitalisations and outpatient admissions. The total net impact
to DHBs (soon to be Health NZ), would therefore be $7,600,000. The Ministry is
supportive of the widened access and has advised it is seeking approval of
funding to support widened access.
There are no costs or savings to the person or their whānau as part of this
proposal.
People with serious mental health conditions or addiction
The proposal to fund this group would benefit up to 174,000 people in the first
year, and up to 185,000 people in year five. There would be a cost to the CPB
in the 2022/23 FYR of 9 (2) (b) (ii)
with a 5-year NPV (8%) of 9 (2) (b) (ii)
This proposal would incur costs to the Ministry of Health (Health NZ from 1 July
2021) of $1,200,000 for the Immunisation Benefit paid to vaccinators for
administering influenza vaccine in the first year, rising to $1,700,000 in year
five. This would be offset by savings of $330,000 in year 1, from reduced
hospitalisations and outpatient admissions, rising to $480,000 in year five. The
total net impact to DHBs (soon to be Health NZ), would therefore be
$4,500,000 5yr NPV (8%). The Ministry is strongly supportive of the widened
access and has advised it is seeking approval of funding to support widened
access.
A1596684 – T22-1368
10
Comments from Interested Parties
Section 49(a) of the New Zealand Public Health and Disability Act 2000 (the Act) requires
Pharmac to consult, when it considers appropriate to do so.
Pharmac staff consider consultation on the recommendations contained in this paper is not
necessary as we recently received consultation feedback supporting the funding of school
aged children and people with serious mental health conditions when we consulted on the
proposal to fund influenza vaccine for Māori and Pacific peoples from 55 to 64 years of age
in March 2022. Staff note that the proposal for children from 3-12 years of age is to only fund
for the remainder of the 2022 influenza season. Any future proposal for the ongoing funding
of this group would be subject to public consultation. The decision paper with the March 2022
consultation response summary is available at A1576521.
Legal advisors’ view
Legal advice has not been sought on this proposal because Pharmac staff do not consider it
to be contentious or to raise any issues of legal concern.
Implementation
Section 49(b) requires Pharmac to take measures to inform the public, groups and
individuals of Pharmac’s decisions concerning the pharmaceutical schedule. Accordingly, if
the Director of Operations adopts the recommendations contained in this paper Pharmac
staff will notify all suppliers, and implement the listing of these products via the usual
Schedule processes. The Ministry of Health (Health New Zealand from 1 July 2022) is
responsible for implementation for vaccines. It has advised that it is supportive of the
widened access and activities it intends to use to support the widened access are outlined
above in the ‘Consequences for the health system’ section.
A1596684 – T22-1368
11
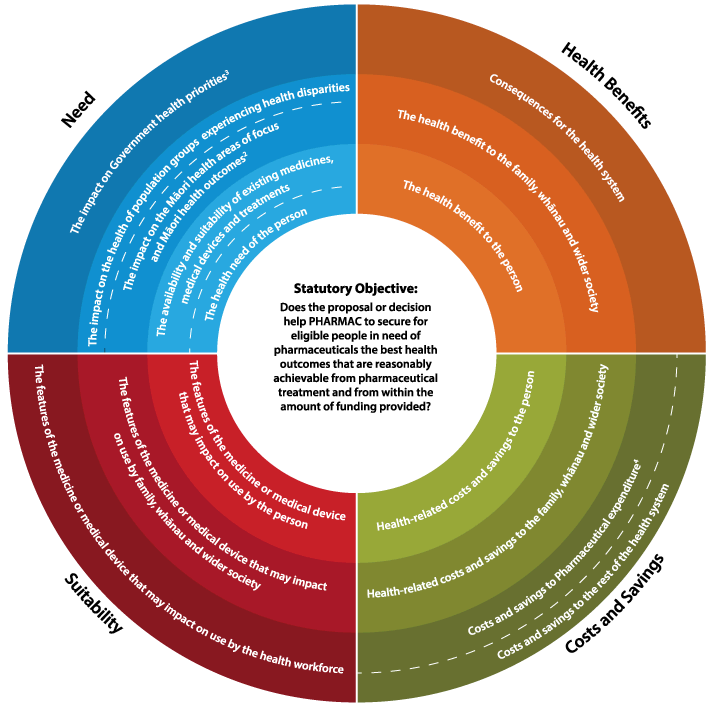 Factors for Consideration
Factors for Consideration
This paper sets out PHARMAC staff’s assessment of the proposal using the Factors for
Consideration in the Operating Policies and Procedures. Some Factors may be more or less
relevant (or may not be relevant at all) depending on the type and nature of the decision
being made and, therefore, judgement is always required. The Decision Maker is not bound
to accept PHARMAC staff’s assessment of the proposal under the Factors for Consideration
and may attribute different significance to each of the Factors from that attributed by
PHARMAC staff.
Footnotes
1 The person receiving the medicine or medical device must be an eligible person, as set out in the
Health and Disability Services Eligibility Direction 2011 under Section 32 of the New Zealand Public
Health and Disability Services Act 2000.
2 The current Māori health
areas of focus are set out in PHARMAC’s Te Whaioranga Strategy.
3 Government health priorities are currently communicated to PHARMAC by the Minister of Health’s
Letter of Expectations.
4 Pharmaceutical expenditure includes the impact on the Combined Pharmaceutical Budget (CPB) and
/ or DHB hospital budgets (as appropriate).
5 Please note PHARMAC’s Factors for Consideration schematic currently does not explicitly refer to
the health needs of family, whānau and wider society, but this Factor should be considered alongside
those depicted in the schematic.
A1596684 – T22-1368
12
PHARMACEUTICAL SCHEDULE APPLICATION
To:
Immunisation Advisory Committee
From:
Funding Application Advisor
Date:
May 2022
Influenza vaccine widened access options [P- 001779]
QUESTIONS TO IMMUNISATION ADVISORY COMMITTEE
Note to Committee members: These questions have been identified by Pharmac staff as
being particularly relevant to the application. Please feel free to provide additional
information as appropriate.
Need
1.
Considering the currently available vaccines for influenza, is there an unmet health
need? If so, why?
1.1. What is the strength and quality of evidence for these needs?
2.
Does influenza disproportionally affect:
Māori?
Pacific people?
Other groups already experiencing health disparities relative to the wider New
Zealand population (eg NZ Dep 9-10 deprivation, refugees/asylum seekers)?
2.1. What is the strength and quality of evidence for populations disproportionally
affected by influenza?
Health benefit
3.
Do high dose quadrivalent influenza vaccines (hdQIV), adjuvanted quadrivalent
influenza vaccines (aQIV) or live attenuated influenza vaccines (LAIV) provide any
additional health benefit or create any additional risks compared with other funded
treatment options? If so, what benefits or risks are different from alternative vaccines?
4.
Does reduction of community spread through widened access to any of the following
groups provide any additional health benefit of create any additional risks compared
with currently funded treatments?
universal vaccination of the whole population
universal vaccination of school-aged children
direct and indirect protection within households
5.
What is the strength and quality of evidence, including its relevance to NZ, for health
benefits that may be gained from influenza vaccine for the reduction of community
spread by vaccination of each of these groups?
6.
Does individual protection of any of the following groups provide additional health
benefit of create any additional risks compared with currently funded treatments?
1
A1582930
universal vaccination of children under 5 years of age
Māori and Pacific peoples from an earlier age than 65 years
7.
What is the strength and quality of evidence, including its relevance to NZ, for health
benefits that may be gained from influenza vaccine for individual protection by
vaccination of children under five years of age or Māori and Pacific peoples from an
earlier age than 65 years?
8.
Which patient population would benefit most from each of the following types of
influenza vaccines?
QIV
aQIV
hdQIV
LAIV
9.
Which direct or indirect protection strategies does the Committee consider would be
most effective in the New Zealand setting? Please describe the patient population that
would benefit from each preferred strategy.
10.
What is the strength and quality of evidence, including its relevance to NZ, for health
benefits that may be gained from influenza vaccine for the preferred direct or indirect
protection strategies?
Suitability
11.
Are there any non-clinical features of the different influenza vaccines that may impact
on use, either by the patient, by family, or by healthcare workers, that have not been
considered in this paper?
12.
Are there any features of QIV that may impact on its use in school-age children?
12.1.
Are there any age groups where an intranasal vaccine (such as LAIV) would be
preferred over an injectable vaccine (such as QIV).
General
13.
Is there any data or information missing from the application, in particular clinical trial
data and commentary?
Recommendations
14.
Which of the following influenza vaccine types should be considered for a future listing
in the Pharmaceutical Schedule (subject to product availability) and be included in the
next commercial process for influenza vaccine in addition to QIV?
aQIV
hdQIV
LAIV
15.
Should widened access to include any of the following groups be listed in the
Pharmaceutical Schedule?
Universal vaccination of the whole population
2
A1582930
Universal vaccination of school-aged children (please specify age ranges)
Universal vaccination of all children younger than 5 years of age
Māori and Pacific peoples from an earlier age than 65 years (please specify age
ranges)
Healthcare workers
Family or whānau of high-risk groups
Any other groups not described above
16.
If widened access is recommended, what priority rating would you give to each patient
group within the context of vaccines and immunisation? [low / medium / high / only if
cost-neutral]?
17.
Does the Committee have any further comments or recommendations additional to the
application?
3
A1582930
PURPOSE OF THIS PAPER
The purpose of this paper is to stimulate discussion about possible influenza vaccination
strategies and seek advice from the Committee regarding alternative approaches to
seasonal influenza vaccination. It introduces a Pharmac initiated application to widen access
criteria for influenza vaccine.
This paper summarises the evidence for vaccinating the following groups:
Universal vaccination of the whole population
Universal vaccination of school aged children
Universal vaccination of children younger than 5 years of age
Māori and Pacific peoples from an earlier age than 65 years
Healthcare workers
Family or whānau of high-risk groups
DISCUSSION
BACKGROUND
Previous consideration of influenza vaccine
The Pharmaceutical Schedule currently lists two influenza
vaccines (Afluria Quad Junior and
Afluria Quad), each with specific funding criteria, which is further discussed below under
The
availability and suitability of existing medicines, medical devices and treatments.
Previously considered applications for the funding of influenza vaccines in different
population groups and the recommendations made are shown in Table 1:
Table 1: Funding recommendations for influenza vaccines
Population
Recommendation
Status
Inactivated influenza vaccine
Influenza in patients with serious
Immunisation Subcommittee Oct 2019: Decline
Options compared
mental health conditions and
Immunisation Subcommittee Aug 2021: Medium
addiction
Ring protection for high-risk
Immunisation Subcommittee May 2018: Decline
Options compared
group, Māori people from an
earlier age than 65 years, Pacific
people from an earlier age than 65
years
Adjuvanted quadrivalent influenza vaccine
Influenza vaccination for people
PTAC Aug 2020: Decline
Options compared
aged 65 years and over
Immunisation Subcommittee Sep 2020: Cost
Neutral
Adjuvanted trivalent influenza vaccine
Influenza vaccination for people
Immunisation Subcommittee Sep 2018: Decline
Declined
aged 65 years and over
PTAC Feb 2019: Decline
Additional advice sought from the Committee about widened access options
4
A1582930
Pharmac staff sought email clinical advice from the members of
the Immunisation Advisory
Committee in late February 2022. Advice was sought on a number of options for widened
access that had been discussed with the Ministry of Health for widened access during the
2022 influenza season:
Māori and Pacific peoples aged 55 to 64 years
Children aged six months to five years
Eligible people and their whānau who live in the same dwelling (also known as
“whānau approach” or “ring protection”)
Most members’ preferred option was open access (“universal coverage”) of all ages, or
some priority groups such as school age children or those from six months to five years of
age.
While open access was a preferred option, most members were supportive of widened
access for Māori and Pacific peoples from an earlier age. It was also suggested by members
that Pharmac consider extending this down to 50 years age as this is when immune
response starts to wane due to ageing.
Members noted that currently Māori and Pacific rates for influenza vaccination are much
lower in those aged 65 years and over, compared to non-Māori, non-Pacific peoples.
Members also noted that Māori and Pacific peoples are at increased risk from seasonal
influenza. Māori and Pacific populations have a younger age distribution than other
population groups and high incidence of comorbidities. Widening access from an earlier age
would increase coverage in Māori and Pacific Peoples as a greater proportion of the
population would be able access funded vaccination.
The eligibility criteria for influenza vaccine were widened from 1 April 2022 to include Māori
and Pacific people who are 55-64 years of age, for the duration of the 2022 calendar year.
This widened access was intended to reduce the impact of influenza to at-risk populations
during the COVID-19 pandemic. Many Māori and Pacific people in this age range may
already have been eligible for funded influenza vaccine if they had comorbidities, however,
additional criteria including age and ethnicity was considered to reduce health system
barriers to accessing funded influenza vaccine, as these eligible people would not have to
have already accessed health services to receive a diagnosis of a qualifying condition. Other
options for widened access considered by Committee members in February 2022 were also
evaluated, but this option was progressed taking into account the planned vaccine supply,
particularly in relation to constrained paediatric vaccine supply.
Commercial strategy and future funding applications
The last influenza vaccine RFP in 2018 resulted in the award of sole supply to Seqirus for
Afluria Quad / Afluria Quad Junior.
At its May 2018 meeting, the Committee recommended
that hdTIV, aTIV and LAIV be included in the RFP that was issued at the end of 2018. In
recent years there have been advances in vaccine technology and there are now a number
of different vaccine technologies that may have advantages or disadvantages compared to
standard inactivated influenza vaccine (IIV) in different patient subgroups. The newer
technologies include high dose vaccines (hdQIV), adjuvanted vaccines (aQIV) and live
attenuated influenza vaccines (LAIV). As Pharmac plans for the next RFP later in 2022, we
seek the Committee’s advice on which types of influenza vaccines could be included in the
RFP. If suppliers of preferred types of vaccines do not yet have Medsafe approval in NZ,
5
A1582930

they will need to submit their Medsafe application and make a funding application to
Pharmac. Such applications would most likely be considered by the Committee and PTAC at
a meeting in early 2023, once RFP bids have been received and analysed.
The Subcommittee should consider whether it is appropriate to continue the current model
where there is one subsidised vaccine brand for all people, which allows for sole supply
commercial arrangements, or if it would be preferred to fund different vaccines for different
patient groups, taking into account the added implementation complexities.
The following table summarises the availability of other vaccines that Pharmac is aware of.
Some of the vaccine types discussed at this meeting are not yet available in New Zealand,
so suppliers will need to submit registration applications for these vaccines if they intend to
participate in the influenza RFP to be issued in late 2022.
Table 2: Availability of influenza vaccines
Vaccine
Brand
Supplier
Medsafe Registration
Funding application
Cell based QIV
Flucelvax Seqirus
Approved
Expected July 2022
Quad
Adjuvanted QIV
Fluad
Seqirus
Approved
Updated application to be
Quad
considered at this meeting
High Dose QIV
Fluzone
Sanofi
Not yet submitted
Expected July 2022
LAIV
FluMist
AstraZeneca
Not yet submitted
Unknown
Need
Description of the disease
Influenza is a common viral infection that attacks the lungs, nose and throat and is spread
through the air from people coughing or sneezing. It characteristically begins with the onset
of fever, malaise, muscle aches, and headache, followed by the development of a cough,
congestion, and a sore throat.
People suffering from influenza usually recover within one to four weeks, but there is a risk
that some will develop complications, such as secondary infections, inflammation of the
heart, brain, or muscle, and sometimes organ failure. Population groups most at risk of
complications from influenza include very young children, pregnant women, and the elderly.
Overall mortality rates with seasonal influenza in New Zealand are estimated around 13.5
per 100,000 population, but with wide variation according to gender, ethnicity and
socioeconomic status and ranging up to 214 per 100,000 in the very elderly (Khieu et al. J
infect. 2017;75:225-33).
The strains that most commonly affect humans are Type A, Type B and Type C.
6
A1582930
 Epidemiology
Epidemiology
The influenza season in NZ usually occurs from May to August. The Southern Hemisphere
Influenza Vaccine Effectiveness Research Study (SHIVERS) started in 2012 and collected
data on influenza vaccines and hospitalisations associated with severe acute respiratory
illness (SARI) and general practice presentations for influenza-like illness (ILI) in the
Auckland and Counties Manukau District Health Boards.
During the 2015 influenza season the SHIVERS study collected serology samples to
measure the immune response to influenza infection. The serosurvey provided data on mild
influenza that did not require GP consultation and information about the level of symptomatic
and asymptomatic infection within the community.
The preliminary serological data suggested that around a quarter of the population would
have been infected with influenza, and of these, 80% of children and adults with influenza
did not have symptoms of influenza when infected. Of those with symptomatic infections,
77% did not seek medical attention.
During the 2020 and 2021 influenza seasons, ESR had reported that there had been very
little, if any, influenza circulating, due to COVID-19 pandemic public health measures such
as closed borders and mask wearing. For this reason, this section focuses on the 2019
season, albeit also a season with lower than usual influenza circulation.
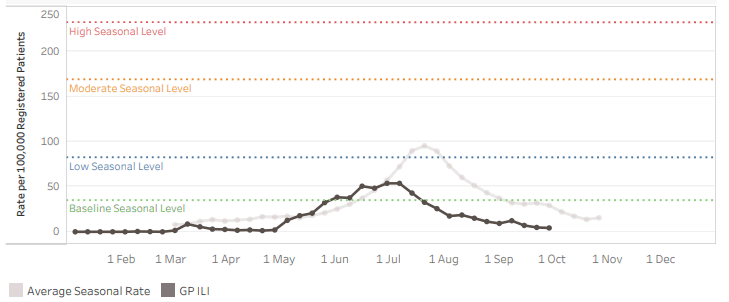
Rates of weekly GP visits for ILI (influenza like illness) were lower than previous years in
2019 and did not exceed 60 cases per 100,000 people in any given week (Figure 1).
Figure 1: Weekly general practice ILI rates to 29 September 2019
Note: The black line denotes the 2019 rates of ILI. Grey line denotes historical rates for previous years.
Source: ESR 2019 Influenza Surveillance intelligence dashboard
Hospitalisations
The highest proportion of influenza infections resulting in hospitalisation and death is seen in
adults aged over 65 years, who have decreased immune function due to their age and may
have other conditions (including diabetes, heart disease, and respiratory conditions), which
increase the risk of complications from influenza.
7
A1582930
Khieu et al. Vaccine 2015;33:4087-92 (Appendix 1) used negative binomial regression
models with weekly counts of hospitalisations and isolates of influenza A, B and respiratory
syncytial virus for the period 1994-2008. The modelled hospitalisation rates per 100,000 are
Table 3 below. Research by Khieu et al. highlights the highest disease burden in those
under 65 years of age from influenza hospitalisation is in the <1 year, 1 to 4 year, 20 to 34
year and 50- to 64-year-old age groups. Noting the relative risk of hospitalisation for Māori
(1.38) and Pacific peoples (1.43) across all age groups, the hospitalisation rate in each of
these age groups is likely to be amplified for Māori and Pacific relative to non-Māori.
Table 3: Hospitalisation rates attributable to influenza (1994-2008), per 100,000
Description
Rate per
100,000
Hospitalisations attributable to influenza (1994-2008) – all ages, all causes*
62.4
Hospitalisations attributable to influenza (1994-2008) – <1 years, all causes*
244.5
Hospitalisations attributable to influenza (1994-2008) – 1-4 years, all causes*
161.1
Hospitalisations attributable to influenza (1994-2008) – 5-19 years, all causes*
15.8
Hospitalisations attributable to influenza (1994-2008) – 20-34 years, all causes*
52.3
Hospitalisations attributable to influenza (1994-2008) – 35-49 years, all causes*
15.7
Hospitalisations attributable to influenza (1994-2008) – 50-64 years, all causes*
53.2
Hospitalisations attributable to influenza (1994-2008) – 65-79 years, all causes*
149.9
Hospitalisations attributable to influenza (1994-2008) – >80 years, all causes*
327.8
Hospitalisations attributable to influenza (1994-2008) – Māori population all ages, all causes*
80.0 (RR vs
non-Māori
1.38)
Hospitalisations attributable to influenza (1994-2008) – Pacific population all ages, all causes*
83.3 (RR vs
non-Māori
1.43)
Hospitalisations attributable to influenza (1994-2008) – European/other population all ages, all causes*
58.1
*Causes included in the analysis: pneumonia and influenza, respiratory illness, circulatory illness, all medical illness, all
causes
Weekly ESR surveillance data for 2019 shows that hospitalisations from influenza confirmed
SARI were mostly caused by influenza A virus strains and did not exceed 40 cases per
100,000 in any given week (Figure 2).
8
A1582930
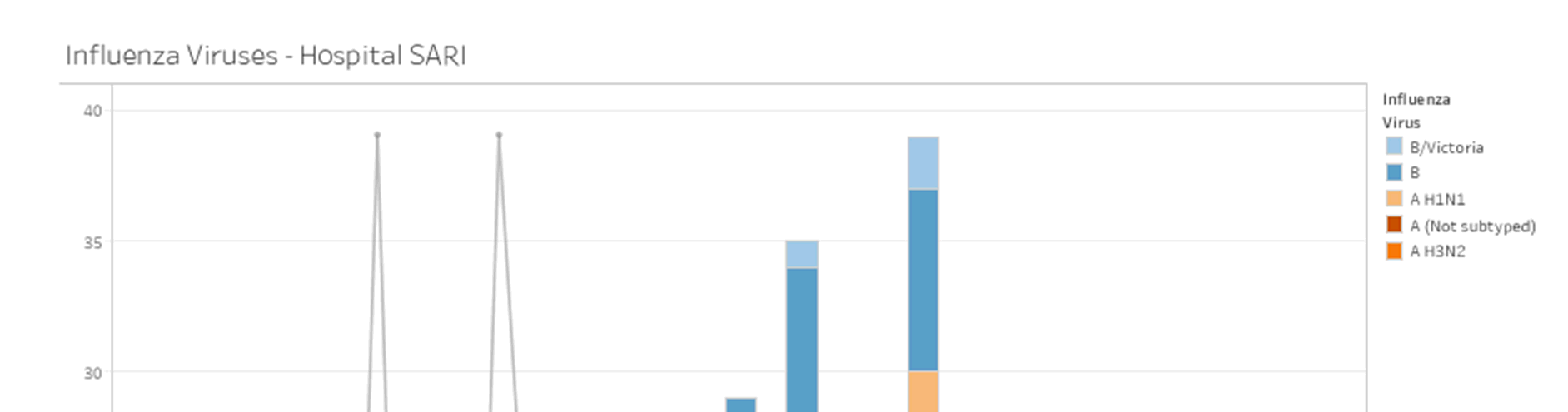
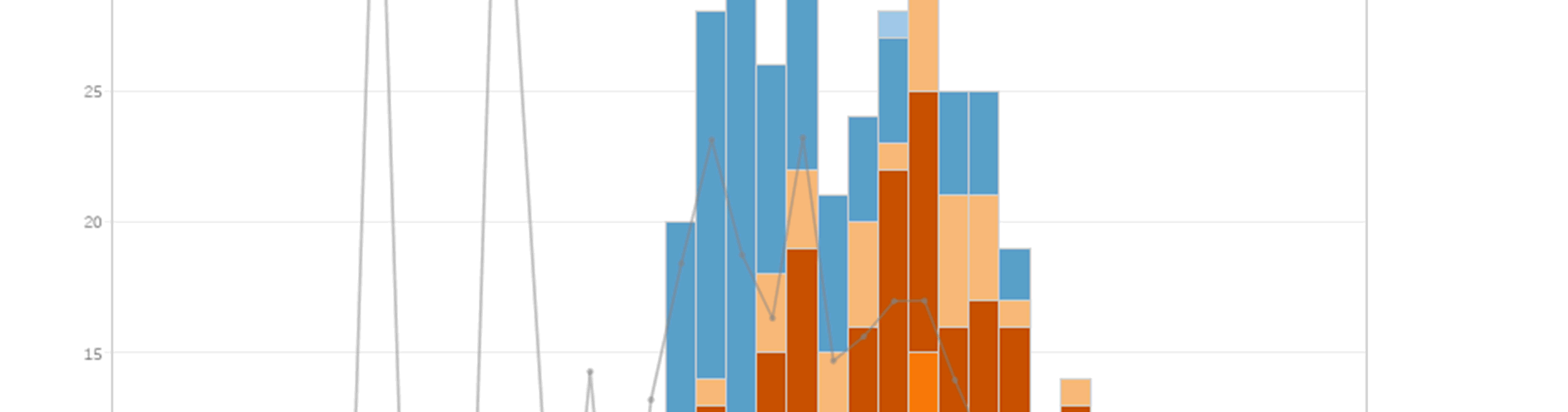
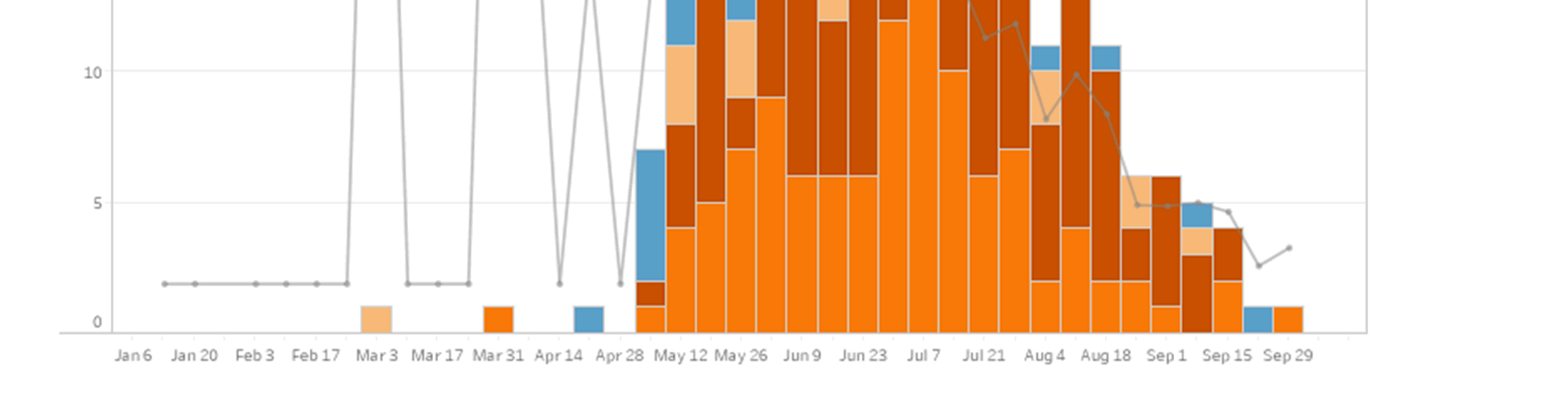 Figure 2:
Figure 2: 2019 rates of hospitalisation due to SARI, by influenza strain, per 100,000
Note: The grey line denotes the percentage of tested samples for that week which were influenza positive.
Source: ESR 2019 Influenza Surveillance intelligence dashboard
Mortality
Khieu et al. J Infect 2017;75:225-33 (Appendix 1) modelled seasonal influenza mortality in
New Zealand, estimating the average mortality rate and identifying differences in risk by age,
sex, ethnicity and socioeconomic position. Data was drawn from the New Zealand mortality
dataset for the period 1994 to 2008. Mortality rates per 100,000 are shown in the Table 4
below:
9
A1582930
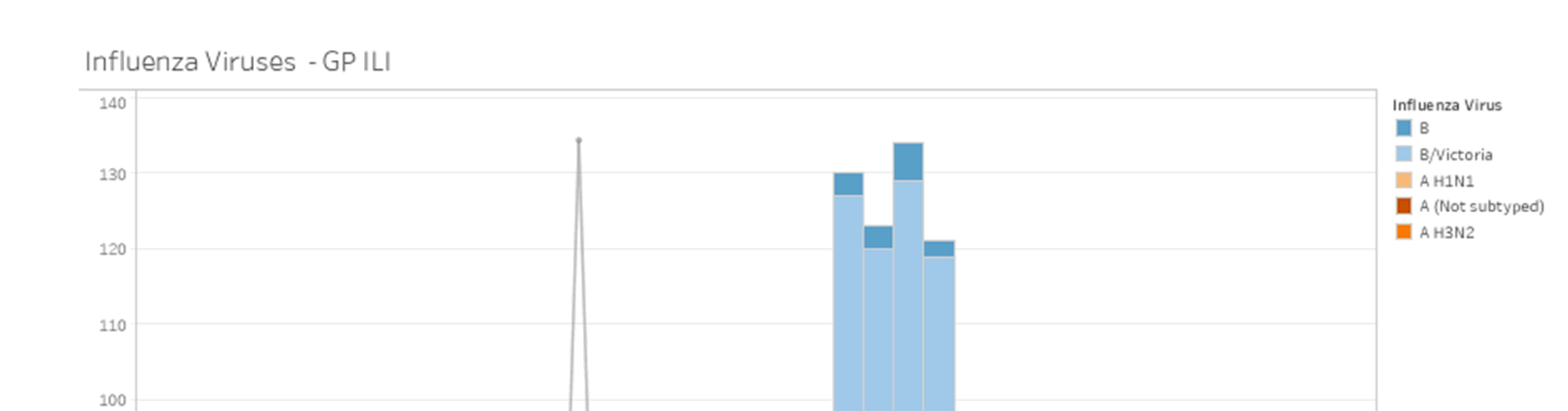
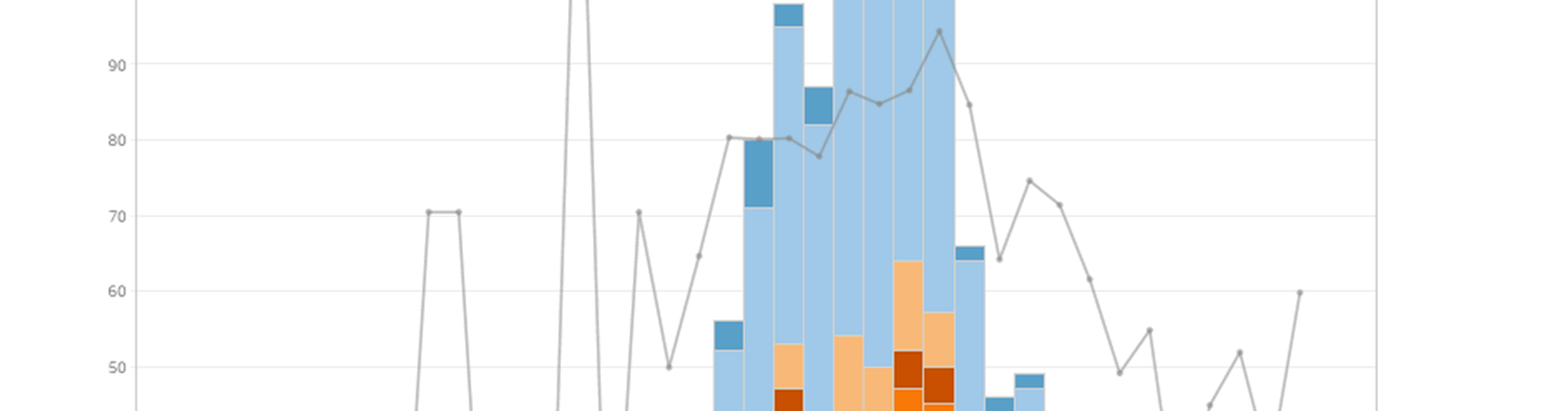
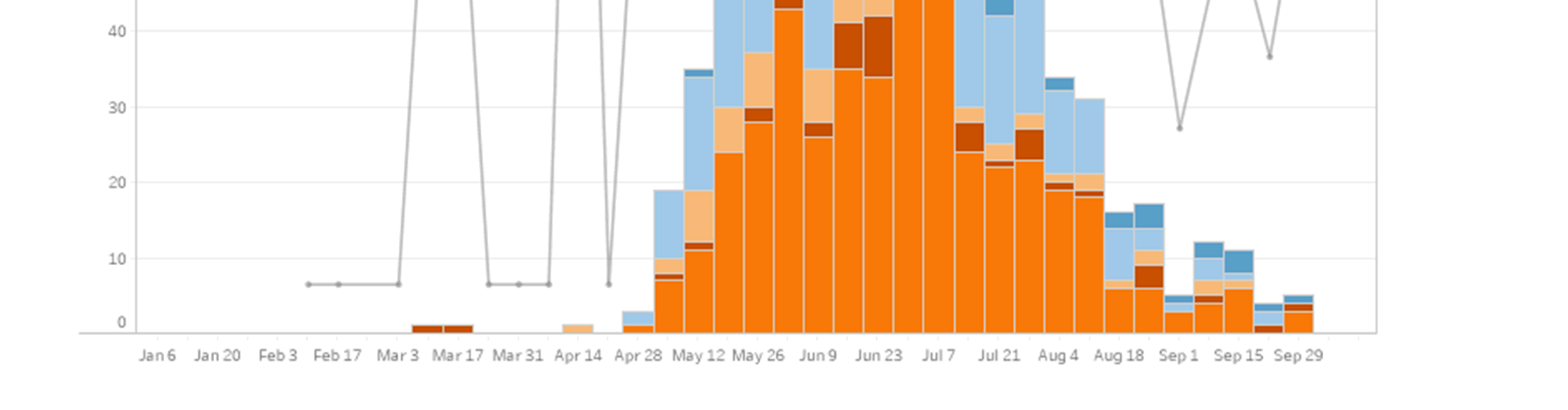 Table 4:
Table 4: Estimated rate of influenza-associated deaths (1994 to 2008) per 100,000
Description
Value
Estimated rate of influenza-associated deaths per 100,000 people (95% CI), all causes
13.5 (13.4, 13.6)
Estimated rate of influenza-associated deaths per 100,000 people, 20-64 years old (95%
2.5
CI), all causes
Estimated rate of influenza-associated deaths per 100,000 people, 65+ years old (95% CI), 90.3
all causes
Estimated rate of influenza-associated deaths per 100,000 people, 65-79 years old (95%
49.7
CI), all causes
Estimated rate of influenza-associated deaths per 100,000 people, 80+ years old (95% CI), 214
all causes
Estimated proportion of total deaths caused by influenza (%), all causes
1.8%
General practice community sentinel surveillance
According to ESR Influenza Surveillance data, 2019 GP visits for influenza confirmed ILI
were predominantly caused by influenza B virus strains, mainly B/Victoria (Figure 3).
Figure 3: 2019 rates of GP visits due to ILI, by influenza strain, per 100,000
Note: the grey line denotes the percentage of tested samples for that week which were influenza positive.
Source: ESR 2019 Influenza Surveillance intelligence dashboard
10
A1582930
Influenza immunisation coverage
Influenza vaccination claims data show that the coverage rate for adults aged 65 years and
over was 65% in 2019. The coverage for pregnant women is 30% and for children aged 0-4
years was 3%.
Influenza vaccination claims data for 2021 show that the overall coverage rate for adults
aged 65 years and over was 63.8%. Coverage data for people over 65 years of age overall
and by ethnicity, provided by the Ministry of Health (MoH) Immunisation Team is provided in
Table 5 below (both funded and unfunded). 2020 data is not presented due to the influence
of the public health measures from the COVID-19 pandemic response, which affected this
data.
Table 5: Influenza vaccination coverage uptake for adults aged over 65 years, by ethnicity, for the
2019 and 2021 influenza season
Group
Coverage
2019 influenza season
Adults aged 65 and over (excludes unfunded)
66%
Māori people aged 65 and over
57%
Pacific people aged 65 and over
70%
2021 influenza season
Adults aged 65 and over (excludes unfunded)
63.8%
Māori people aged 65 and over
50%
Pacific people aged 65 and over
62.4%
Source: MoH Immunisation Team
The health need of the person
Influenza is a viral infection that is associated with high morbidity and mortality due to the
effects and complications of acute respiratory illness in young children, the elderly, pregnant
women and those with a range of underlying medical conditions. However, healthy children
and adults can also be at risk of serious illness following influenza infection.
The availability and suitability of existing medicines, medical devices and treatments
The funded influenza vaccine for 2022 for the adult population is AFLURIA QUAD (Seqirus),
a non-adjuvanted QIV. The vaccine offers protection against strains A/Victoria/2570/2019
(H1N1) pdm09-like virus, A/Darwin/9/2021 (H3N2)-like virus, B/Austria/1359417/2021-like
virus, B/Phuket/3073/2013-like virus.
11
A1582930

 The health need of family, whānau, and wider society
The health need of family, whānau, and wider society
Pharmac acknowledges that there may be a health need for other people as a result for
caring for patients with influenza. The impact on whānau primarily comes from the risk of
transmission to those living with and caring for patients with influenza.
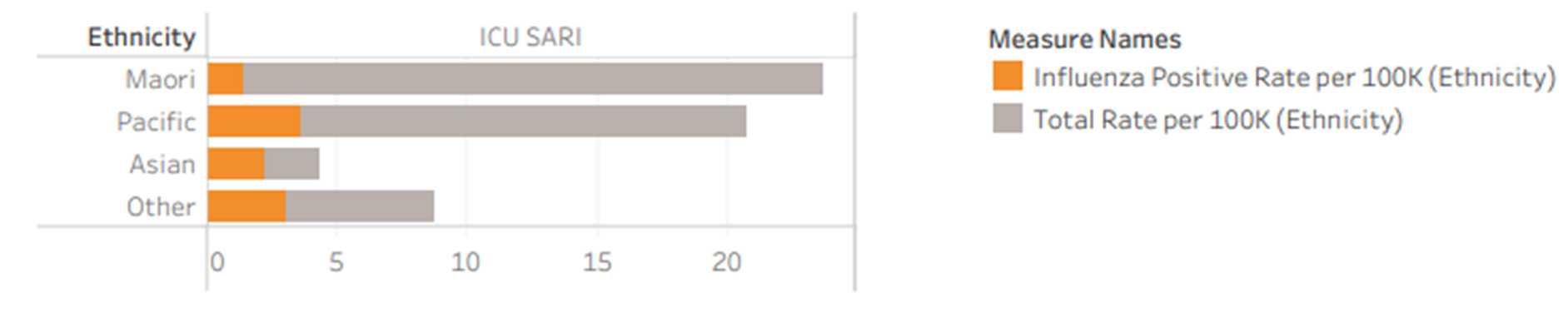
The impact on the Māori health areas of focus and Māori health outcomes
Influenza disproportionately affects Māori health outcomes, which may be in part due to
lower rates of immunisation in the Māori population. Māori and Pacific peoples are more
likely to be hospitalised from SARI compared with non-Māori and non-Pacific populations
(Figure 4) and are also more likely to have to be treated in ICU due to SARI, though Māori
rates of ICU admission from confirmed influenza are lower than for non-Māori (Figure 5).
Figure 4: Cumulative rate of hospitalisations due to SARI, by ethnicity, per 100,000
Source: ESR 2019 Influenza Surveillance intelligence dashboard.
Figure 5: Cumulative rate of ICU admissions due to SARI, by ethnicity, per 100,000
Source: ESR 2019 Influenza Surveillance intelligence dashboard.
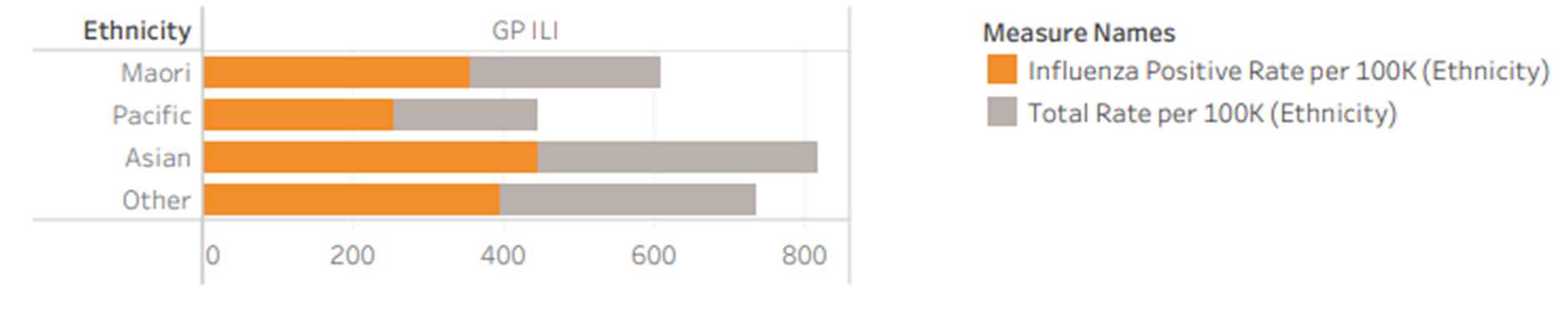
In addition, Māori and Pacific people are less likely to visit a GP than Asian, non-Māori and
non-Pacific people with ILI symptoms (Figure 6) which may contribute to the increased
severity of complications from influenza seen in the Māori and Pacific population.
Figure 6: Cumulative rate of GP visits for ILI, by ethnicity, per 100,000
Source: ESR 2019 Influenza Surveillance intelligence dashboard
Khieu et al (2015) estimated that influenza hospitalisation rates were 58.1 per 100,000 for
the European population compared with 80.0 and 83.0 per 100,000 for Māori and Pacific
people
, respectively (Khieu et al. Vaccine 2015;33:4087-92). In 2017, the same authors
reported that when standardising for age, the mortality rate attributable to influenza in the
12
A1582930
Māori population was statistically significantly higher than Other/European populations with
21.1 per 100,000 compared with 4.5 per 100,000 for European/Other. The Pacific population
also experienced a statistically significantly higher rate of influenza attributable mortality
compared with European/Other with a rate of 6.8 per 100,000
(Khieu et al. 2017).
Currently Māori aged 65 years and over are less likely to receive their annual vaccination.
Coverage measured through claims data submitted to the Ministry of Health suggests that
only 50.0% of this group were able to access vaccination in 2021; uptake in this age group
for the overall population was 63.8%. By contrast, Pacific people aged 65 years and over are
more likely to receive their annual vaccination; claims data submitted to the Ministry of
Health suggests that 62.4% of this group were vaccinated in 2021.
The impact on the health outcomes of population groups experiencing health
disparities
Baker et al. conducted a national epidemiological study of hospital admissions for infectious
and non-infectious diseases in New Zealand from 1989 to 2008 to investigate trends in
incidence across various socioeconomic and ethnic landscapes. They found that those living
in the most deprived areas (NZDep 9&10) have a higher rate of infectious disease related
hospitalisations than the least deprived areas (NZDep 1&2) (Baker et al. Lancet.
2012;379(9821):1112-9)
Khieu et al. reported the influenza-attributable death rate per 100,000 was higher for more
deprived areas (NZDep 9&10) compared with least deprived areas (RR 1.8, 95% CI 1.3-2.4)
(Khieu et al. 2017).
The impact on Government health priorities
This funding application aligns with the following Government health priorities:
Child wellbeing: To improve child wellbeing and support children to have a healthy
start in life, noting the impact of influenza in children
Prevention: To improve wellbeing by preventing health conditions, which includes
immunisation against infectious diseases.
Health equity: To better population outcomes, noting the disproportionate
representation of influenza infection in Māori, Pacific peoples, and those living in high
socioeconomic deprivation.
Infectious disease is also listed as a priority condition, which includes immunisation to
prevent infectious diseases.
13
A1582930
 Health Benefit
The health benefits to the person, family, whānau and wider society
Evidence Summary
Health Benefit
The health benefits to the person, family, whānau and wider society
Evidence Summary
The Immunisation Advisory Centre (IMAC) has provided a brief review of the evidence to
provide insight into potential further immunisation strategies that could be implemented to
reduce the spread of influenza and reduce the impact of severe influenza in New Zealand.
The full text version of the references in this section are available in Appendix 1, and the
review (
Role of vaccination in influenza control strategies, IMAC 2022) is provided in
Appendix 2.
The IMAC 2022 review proposes a range of vaccination strategies that address the
reduction community spread or the protection of high-risk individuals. The approaches are
outlined in Table 6 below:
Table 6: IMAC 2022 proposed vaccination strategies
Individual protection
Broadening eligible risk groups
Protection of high-risk
Age groups for Māori and Pacific peoples
individuals (direct
protection)
Consideration of additional groups funded in other
jurisdictions
Ring-fencing high-risk groups to reinforce protection
Full universal vaccination
Reduction of community
Universal vaccination of school aged children
spread (indirect protection)
Direct and indirect protection within households
Direct protection
Vaccination of children
The Ministry of Health recommends vaccination of children from six months of age, but
influenza vaccine is only funded from this age for people with underlying health conditions
and children under five years of age who have been hospitalised for respiratory illness or
have a history of significant respiratory illness. Th
e full eligibility criteria are available on the
Pharmac website.
Immunisation coverage
A study from the US (Bleser et al. PLoS ONE 2020;15(6): e0234466) examined data from
the 2011 National Immunization Survey and reported that although children six months and
older are recommended to receive annual influenza vaccination, uptake was substantially
lower than other schedule vaccines. The study reported that about 71% of children aged 6-
23 months were up to date on routinely recommended vaccines but only 33% had the
14
A1582930
recommended influenza vaccine by their second birthday and 44% had hidden vulnerability
to influenza.
Improving vaccine uptake through universal childhood vaccination
A study in Australia (De Oliveira Bernardo et al. Hum Vaccin Immunother. 2020;16(3):630-5)
reported that overall influenza vaccination coverage in general practice for children aged
under 5 years increased by more than five times from 2015 (3.9%) to 2018 (19.6%). Prior to
universal funding, children under five years of age in the wealthiest areas were most likely to
receive the influenza vaccine. After the vaccine was funded, all children in these wealthier
areas (irrespective of their individual household socioeconomic levels) benefited more than
those in less advantaged areas. This was because although the vaccine was accessible to
all children (under five years), there was a greater increase in coverage from 2017-2018 in
the wealthier areas than the disadvantaged areas.
Reduction in influenza in children following vaccination with IIV or LAIV
A 2018 systematic review reported that vaccination of healthy children with inactivated
influenza vaccines (IIV) reduced influenza infection from 30% to 11% (risk ratio 0.36, 95% CI
0.25-0.48; n=1,628) and may reduce influenza-like illness (ILI) (from 28% to 20%; risk ratio
0.72, 0.65-0.79; n=19,044) in children aged between two and 16 years. Based on this, five
children would need to be vaccinated with inactivated vaccine to prevent one case of
confirmed influenza and 12 vaccinated to prevent one cases of ILI. The confidence of
evidence for live attenuated influenza vaccine (LAIV) was less certain but demonstrated
protection against influenza (from 18% to 4%; risk ratio 0.2, 0.11-0.41; n=7,718) and a
reduction in ILI in children (from 17% to 12%; risk ratio 0.69; 0.6-0.8, n=124,606). Seven
children would need to be vaccinated with LAIV to prevent one case of influenza and 20
children vaccinated to prevent one case of ILI in children. (Jefferson et al. Cochrane
Database Syst Rev. 2018;(2):CD004879)
Vaccination in pregnancy to protect infants
A meta-
analysis (Jarvis et al. Vaccine. 2020;38(7):1601-13) that pooled two randomised
controlled trials reported that maternal influenza vaccination was associated with a 34%
(95% CI 15% to 50%) overall reduction in laboratory confirmed influenza, but not ILI in
infants up to six months of age. Two studies that were excluded from the meta-analysis for
the outcome of laboratory confirmed influenza due to different controls, reported vaccine
efficacy of over 70% against influenza in maternally vaccinated infants.
Vaccination of other high-risk groups: Māori and Pacific peoples
In 2013 the Ministry of Health reported that Māori people aged five to 34 years were almost
twice as likely than non-Māori to be hospitalised for asthma than non-Māori people (risk ratio
[RR] 1.96, 95% CI 1.87 to 2.07) and 25% more likely to be diagnosed with chronic
respiratory disease at age 15-45 years (RR 1.27, 95% CI 1.06 to 1.52). Mortality rate due to
COPD was almost three times that of non-Māori from the age of 35 years in 2010-12. In
2012-14, life expectancy from birth was around seven years lower for Māori than non-Māori
(Ministry of Health; Health status indicators; updated 02 August 2018).
In 2010, more than half of the Māori population were aged under 25 years, and Māori had a
higher prevalence of acute and chronic respiratory tract infections than non-Māori. The
factors contributing to this increased risk appear to be environmental (overcrowding, poor
housing, socioeconomic status, smoke exposure, nutrition), and reduced access to health
15
A1582930
promotion programmes, such as immunisation programmes, and health care, rather than
underlying genetic or medical disorders
(Byrnes et al. J Paediatr Child Health.
2010;46(9):521-6).
A study investigating emergency department (ED) presentation of infants age <1 year for
acute respiratory infection (ARI) at Kidz First Childrens’ Hospital in South Auckland (as part
of the SHIVERS project) reported that the influenza hospitalisations incidence ratio per 1,000
infants was 6.2 (95% CI 3.4 to 9.0) for Māori, 6.1 (95% CI 3.5 to 8.8) for Pacific, 0.5 (95% CI
-0.01 to 1.0) for Asian, and 0.7 (95% CI 0.1 to
1.3) for European/Other (Prasad et al. Pediatr
Infect Dis J. 2020;39:e176-85), in effect rates nine times higher in Māori and Pacific children
compared with European/Other children.
Vaccination of other high-risk groups: Elderly
A review of literature concluded that, overall, standard influenza vaccination can attenuate
the course of disease in those with breakthrough infection compared with those who are
unvaccinated among community-dwelling adults ≥65 years with laboratory-confirmed
influenza. A meta-analysis reported the odds of influenza-associated ICU admission was
reduced by 26% (pooled odds ratio [OR] 0.74, 95% CI 0.58 to 0.93) by vaccination. The risk
of death in adults hospitalised with influenza was reduced by 31% (OR 0.69, 95% CI 0.52
to0.82) compared with unvaccinated patients. Vaccination was not significantly associated
with a reduction in pneumonia among adults hospitalised with influenza (OR 0.92, 95% CI
0.82 to 1.04) nor risk of hospitalisation with influenza illness seeking outpatient care (OR
0.60, 95% CI 0.28 to 1.28)
(Ferdinands et al. Vaccine. 2021;39:3678-95).
Indirect protection - community (herd) immunity
Vaccination of children
A systematic review investigating vaccination of children aged six months to 17 years
against influenza reported that indirect protection was conferred in some but not all settings.
Across 20 out of 30 studies, the point-estimate indirect protection effectiveness (IPE) ranged
from 4% to 66%. When looking at randomised controlled trials, an IPE of 60% (95% CI 41%
to 72%) was shown against laboratory-confirmed influenza in members of closely connected
communities when school-aged children were vaccinated, and IPE of 22% (95% CI 1% to
38%) against acute respiratory tract infection/ILI in household members of vaccinated
preschool-aged children. Indirect protection against influenza mortality of the elderly was
also seen by vaccinating school children who play a key role in transmission. Despite this,
the review concluded that most effective way to prevent influenza at an individual level was
through annual vaccination
(Yin et al. Clin Infect Dis. 2017;65:719-28).
A study based in Japan observed the role of mass vaccination in schoolchildren in providing
protection to the elderly and young children. During a mass vaccination campaign of school
children (aged 6-15 years) from the mid-1970s to late 1980s, adjusted mortality reduced by
36% (17-51%) in Japanese seniors, which corresponded to 1,000 (400-1,800) deaths
averted by annual vaccination of children. This was compared with the US, in which
influenza-related mortality remained unchanged despite vaccination of the elderly
population. Younger children were also reported to be indirectly protected against influenza
complications during the period of mass schoolchild vaccination
(Sugaya. Expert Rev
Vaccines. 2014;13:1536-70).
16
A1582930
A Dutch epidemiologic study modelled infections and argued that vaccinating young children
would likely lead to an age shift in infection dynamics, which would result in limited indirect
impact on the elderly from vaccinating children (Backer et al. Epidemics. 2019;26:95-103).
Using a dynamic transmission model, it predicted a smaller impact and more variability in the
infection attack rate. Reasons were firstly that while modelled influenza infections in young
children were reduced, after years of vaccination they increased in young adults with limited
natural immunity, which could drive an epidemic. Secondly, after a mild influenza season,
the modelled proportion of susceptible individuals increased to result in a peak of cases the
following year. The authors observed that targeting the group that plays the largest role in
transmission potential requires a secure vaccine supply.
A school-based influenza vaccination programme in Autumn 2005 using LAIV were
associated with directly reduced school absenteeism in elementary schools (children aged 5
to 11 years) during an influenza outbreak in Carroll County, Maryland US. With a 44%
vaccination coverage, school absenteeism was observed to decline from 1.8% in the 2001-
05 seasons to 0.6% in the 2005/6 season. An indirect effect was also seen in high schools
(children aged 14 to 18 years) (0.3% from 1.8%); a similar trend was seen in middle schools
(children aged 10 to
14 years) (Davis et al. Paediatrics. 2008;122(1):e260-e65).
A study in Israel reported that when influenza vaccine was administered in a school setting,
a reduction in ILI was observed among the those vaccinated (by 60.5%) and their household
members (by 27.5%). (Roseman et al. Isr J Health Policy Res. 2021;10:38). The
retrospective cohort study across nine schools in Tel Aviv compared self-reported ILI within
children and their households for those who were vaccinated at school in the second grade
(age ~8 years) with those in the third grade (~age 9 years) who were not vaccinated a part of
the school-based vaccination. In the second-grade cohort, 133/168 (79.2%) had been
vaccinated. In this cohort, unvaccinated children had a higher rate of reported ILI than those
who had been vaccinated (19.5% vs 7.7%, rate reduction of 60.5%,
P<0.001); the
unvaccinated children had a greater number of doctors’ visits and missed school days
(35.7% vs 14.9% and 42.9% vs 25.6%, respectively); and the rate of ILI among household
members was also higher for unvaccinated children (35.4% vs 25.0%; rate reduction 27.3%;
p = 0.03). When the second-grade cohort (52.8% vaccinated) were compared with the third-
grade cohort not vaccinated as part of the programme (12.7% vaccinated), those who had
been vaccinated had a 44.6% rate reduction of ILI and their household had a 22.9% rate
reduction in ILI.
Ring protection
Close contacts of high-risk individuals (family members or carers)
A study in the UK reported that higher rates of vaccination rates within NHS trusts were
associated with reduced sickness absence, reporting that a 10% increase in influenza
vaccination rate would be associated with a 10% fall in sickness absence. (Pereira et al. Clin
Med (Lond). 2017;17:484-9).
An Italian study reported that around 20% of healthcare workers were infected with influenza
each year, resulting in nosocomial outbreaks and staff shortages, and that influenza vaccine
coverage remained low. Over the study period, influenza vaccine coverage decreased
significantly from 13.2% to 3.1% (
P<0.001), and an associated increase in frequency of
nosocomial ILI in hospitalised patients from 0.11% to 0.57% (
P<0.001) was observed
(adjusted OR of 0.97; 95% CI 0.94 to 0.99)
(Amodio et al. J Hosp Infect. 2014;86:182-7).
17
A1582930
International recommendations
International Recommendations
Table 7: International recommendations regarding the funding of influenza vaccine in different populations
Country
QIV
LAIV
Adjuvanted or high dose
Age group
Comments
Age group
Age group
Comments
Australia
All aged 6 months to 5 years
Funded
Not available
2022
season
All ATSI people aged from 6
Funded
≥60 years
HD QIV
months
≥65 years
aQIV
All aged ≥65 years
Funded
≥65 years
aQIV
Ages 5 to <65 years
Funded for:
Certain medical
conditions
In pregnancy
Canada
All aged 6 months to 23
months
Children ages 2 to 17 years
Unless LAIV is not
Children aged 2 to 17 years
with immunocompromise or
contraindicated
severe asthma
18 to 64 years
18 to 59 years
≥65 years
HD QIV, aQIV, or QIVc
Pregnant
HCW
QIV not LAIV
Ireland
From 6 months
24 months to <18 years
≥65 years
aQIV
UK
All infants aged 6 months to
QIVe funded
All children aged ≥2 years
All adults aged ≥65 years
aQIV
<2 years
All aged ≥2 years
QIVc, if LAIV contraindicated
QIVr or QIVc
At risk adults 18 to 64 years
QIVc or QIVr (or QIVe, if
other options unavailable)
All adults aged 50 to 64
years
Abbreviations: ATSI, Aboriginal Torres Strait Islander peoples; LAIV, live attenuated influenza vaccine; QIV, Quadrivalent inactivated influenza vaccine; QIVc, cell-based;
QIVe, egg-based; QIVr, recombinant.
18
A1582930

 Consequences for the health system
Consequences for the health system
If the funding criteria for the influenza vaccine were to be widened, this would be expected to
reduce the number of and complications of influenza infection, thereby reducing the pressure
on and costs to the healthcare system.
Suitability
The features of the medicine or medical device that impact on use
Standard dose inactivated influenza vaccines are an injectable presentation. These are
suitable to be given to most individuals, including young children, the elderly, pregnant
women, and immunocompromised people.
Adjuvanted and high dose inactivated influenza vaccines are injectable presentations. Both
are indicated for people 65 years of age or older. Adjuvanted vaccine is associated with
injection site reactions. An adjuvanted influenza vaccine funding application is to be
reviewed as a separate agenda item at this meeting. It is anticipated that a funding
application for high dose inactivated influenza vaccine will be reviewed the upcoming
September 2022 Committee meeting.
Live attenuated influenza vaccines (LAIV) are nasal spray presentations. They are indicated
for children and adolescents from two years of age and adults up to 49 years of age. There
is insufficient data around the use of LAIV in adults aged 50-64 years of age.
The intranasal presentation is more acceptable to parents / caregivers, possibly leading to
increased uptake of vaccination in children compared to injectable vaccines. However, the
introduction of a school or pre-school-based programme would have significant resource
implications for DHBs to implement each year, and significant financial implications for the
Ministry of Health funding vaccination claims.
Since live virus is administered intranasally, there is the possibility of spreading virus through
viral shedding. Shedding is inversely correlated with age, with the youngest children most
likely to shed virus over the longest time.
LAIV are contraindicated for immunosuppressed individuals.
LAIV are not Medsafe approved for use in New Zealand and Pharmac has not received any
funding applications to date.
Costs and Savings
Costs and savings to pharmaceutical expenditure
No cost analysis has been undertaken at this time, as this paper discusses possible strategic
options for widening access to influenza vaccine in New Zealand, rather than listing any
A1582930
19
particular vaccine. Once clinical advice is obtained on the most appropriate options for
widening access, cost analysis can be undertaken on those options.
The annual gross subsidy on influenza vaccine is approximately 9 (2) million for 730,000
(b) (ii)
doses.
A1582930
20
APPENDICES
Appendix 1:
Key evidence
Amodio et al. 2014
Backer et al. 2019
Bleser et al. 2020
Byrnes et al. 2010
Davis et al. 2008
De Oliveira Bernado et al. 2020
Ferdinands et al. 2021
Jarvis et al. 2020
Jefferson et al. 2018
Khieu et al. 2015
Khieu et al. 2017
Pereira et al. 2017
Prasad et al. 2020
Roseman et al. 2021
Sugaya. 2014
Yin et al. 2017
Appendix 2:
Role of vaccination in influenza control strategies, IMAC 2022
A1582930
21
THE FACTORS FOR CONSIDERATION
Factors are presented here in the order they appear in the paper, without implying any
ranking or relative importance.
NEED
The health need of the person
The availability and suitability of existing medicines, medical devices and treatments
The health need of family, whānau, and wider society
The impact on the Māori health areas of focus and Māori health outcomes
The impact on the health outcomes of population groups experiencing health disparities
The impact on Government health priorities
HEALTH BENEFITS
The health benefit to the person
The health benefit to family, whānau and wider society
Consequences for the health system
SUITABILITY
The features of the medicine or medical device that impact on use by the person
The features of the medicine or medical device that impact on use by family, whānau
and wider society
The features of the medicine or medical device that impact on use by the health
workforce
COSTS AND SAVINGS
Health-related costs and savings to the person
Health-related costs and savings to the family, whānau and wider society
Costs and savings to pharmaceutical expenditure
Costs and savings to the rest of the health system
A1582930
22
Document Outline