link to page 1 link to page 3 link to page 3 link to page 3 link to page 4 link to page 4 link to page 4 link to page 5 link to page 5 link to page 5 link to page 5 link to page 5 link to page 5 link to page 6 link to page 6 link to page 6 link to page 7 link to page 7 link to page 8 link to page 8 link to page 10 link to page 10

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
Bladder Care Post Gynaecology and Urogynaecology Surgery
Unique Identifier
PP2844/RBP/033 - v03.00
Document Type
Clinical Guideline
Risk of non-compliance
may result in significant harm to the patient/DHB
Function
Clinical Practice, Patient Care
User Group(s)
Auckland DHB only
Organisation(s)
Auckland District Health Board
Directorate(s)
Women’s Health
Department(s)
Gynaecology
Used for which patients? All postoperative gynaecology patients
Used by which staff?
All clinicians in gynaecology
Excluded
Keywords
n/a
Author
Obstetrician and Gynaecologist
Authorisation
Owner
Service Clinical Director - Secondary Gynaecology Services
Delegate / Issuer
Team Leader - Urogynaecology Services
Edited by
Document Control
First issued
April 2014
This version issued
30 October 2021 - updated
Review frequency
3 yearly
Contents
1. Purpose of guideline ..................................................................................................................... 3
2. Guideline management principles and goals ............................................................................... 3
3. Risk factors .................................................................................................................................... 3
4. Catheter-associated urinary tract infection ................................................................................. 4
5. Postoperative assessment on admission to the ward .................................................................. 4
6. Subsequent assessment during the first four hours postoperatively or after removal of IDC .... 4
6.1
Assessment ............................................................................................................................ 5
6.2
Supportive measures ............................................................................................................. 5
7. In and out catheterisation for trial of voiding .............................................................................. 5
7.1
Purpose .................................................................................................................................. 5
7.2
Goal........................................................................................................................................ 5
7.3
Documentation ...................................................................................................................... 5
7.4
Actions ................................................................................................................................... 6
8. Urinary retention .......................................................................................................................... 6
9. Trial removal of catheter (TROC) following reinsertion of catheter ............................................ 6
10. Bladder care following a urogynaecology procedure ................................................................... 7
10.1 Post-void residual measuring ................................................................................................ 7
10.2 Backfill voiding technique ..................................................................................................... 8
11. Bladder care following Radical hysterectomy .............................................................................. 8
12. Suprapubic catheter (SPC) management ................................................................................... 10
12.1 Contradictions ..................................................................................................................... 10
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 1 of 14
link to page 1 link to page 10 link to page 10 link to page 10 link to page 10 link to page 10 link to page 11 link to page 11 link to page 11 link to page 11 link to page 12 link to page 12 link to page 12 link to page 13 link to page 13 link to page 13 link to page 13 link to page 14 link to page 14

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
12.2 Precaution ........................................................................................................................... 10
12.3 Complications ...................................................................................................................... 10
12.4 Types of Suprapubic catheter (SPC) .................................................................................... 10
12.5 Insertion of Suprapubic catheter (SPC) ............................................................................... 10
12.6 Equipment required ............................................................................................................ 10
12.7 Procedure ............................................................................................................................ 11
12.8 SPC dressing of insertion site .............................................................................................. 11
12.9 Removal of SPC for an inpatient.......................................................................................... 11
12.10 Equipment ........................................................................................................................... 11
12.11 Discharging a patient with a Suprapubic catheter (SPC)..................................................... 12
12.12 Follow-up ............................................................................................................................. 12
12.13 Recognising infection .......................................................................................................... 12
12.14 Residual urine measurement .............................................................................................. 13
13. Self-catheterisation..................................................................................................................... 13
14. Supporting evidence ................................................................................................................... 13
15. Associated documents ................................................................................................................ 13
16. Disclaimer ................................................................................................................................... 14
17. Corrections and amendments .................................................................................................... 14
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 2 of 14
link to page 1

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
1. Purpose of guideline
The purpose of this guideline is to facilitate safe and effective bladder care following gynaecology
or urogynaecology surgery within Auckland District Health Board (Auckland DHB).
Bladder care management includes:
Prevention of urinary retention and its long-term consequences
Catheter placement and removal
Management of postoperative urinary retention with use of intermittent catheterisation and
use of bladder scanners.
2. Guideline management principles and goals
Vigilant surveillance of bladder function and early intervention where problems exist will prevent
permanent bladder damage and long-term voiding problems (Rizvi, 2005).
Aims of care:
To assess bladder function
To detect any deviations from normal
To carry out timely preventative measures to avoid complications of urinary dysfunction
following surgery.
3. Risk factors
While a patient in the immediate postoperative period has the potential to experience urinary
problems, several factors may increase the risk:
Age – postoperative urinary retention can affect up to 20% of individuals but the incidence
increases in a patient over the age of 50
Anaesthetics
Radical hysterectomy (Wertheim surgery)
Bladder incontinence procedures
Communication issues (e.g. English second language)
Comorbidities (neurologic diseases, diabetes, chronic urinary tract infections (UTIs), cystocele,
rectocele)
Constipation
Epidural analgesia, particularly with local anaesthetic
Length of surgery
Medication (antispasmodics, antidepressants, antihistamines, antipsychotic including Lithium)
Opiates or narcotics
Over-distension of the bladder
Pain
Reduced mobility
Pelvic organ prolapse.
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 3 of 14
link to page 1

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
4. Catheter-associated urinary tract infection
Catheter-associated urinary tract infection (CAUTI) comprises 30-40% of all hospital-acquired
infections, and 70-80% of these infections are related with the use of indwelling urinary catheters
(Bagshaw and Laupland 2006).
Duration of urinary catheterisation is the predominant risk factor for CAUTI. Hence, preventive
measures directed at limiting placement, along with early removal of urinary catheters, have the
greatest impact on decreasing CAUTI rates (Chenoweth et al. 2014).
Our nursing and medical team are encouraged to limit insertion of catheters, and the aim is to
remove the catheter as soon as clinically safe.
5. Postoperative assessment on admission to the ward
The initial bladder assessment should include:
A review of surgical and anaesthetic method used
Pain relief used
Bladder palpation
Check to see if the patient has voided in Post Anaesthesia Care Unit (PACU)
Indwelling catheter (IDC) in situ – check that is draining and positioned lower than patient’s
bladder.
An initial assessment should provide information on:
The presence of any urinary problems
Risk factors that may contribute to urinary problems.
6. Subsequent assessment during the first four hours postoperatively or after
removal of IDC
Careful monitoring of intake and output is imperative to assess fluid balance concerns.
Note:
The onset and progression of urinary retention may be gradual and asymptomatic.
It can take eight hours for the bladder to regain sensation following epidural or spinal
analgesia.
The adult urinary bladder has capacity of 400-600 mL. In a normally functioning adult bladder, the
first urge to void is felt at 150 mL and the sense of fullness is achieved at 300 mL by the activation
of the bladder wall receptors.
When the bladder contains an excess of 500 mL in a non-obese patient, a large bulge can be seen
in the suprapubic area.
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 4 of 14
link to page 1 link to page 5

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
6.1 Assessment
Establish by questioning void or no void
If yes to void, ask the patient if she is experiencing any discomfort or difficulty when voiding.
(Did it feel like a normal void?)
Check the frequency with which urine is passed
Ask volume and quality of flow with each void
Examine the patient’s abdomen for swelling of the lower abdomen
Palpate the patient’s bladder
Assess if the patient is receiving adequate pain relief (this is a common cause for retention)
Manage constipation (this is a common cause for retention).
6.2 Supportive measures
If no void occurs at four hours post-surgery or removal of IDC, use non-invasive measures such as
ambulation, privacy, shower, hands under cold running water, warm flannel over bladder, or if
necessary, appropriate analgesia to enhance the likelihood of micturition. Ensure adequate
amount of fluid intake and commence Fluid Balance Record.
If the patient is still unable to void, then verify bladder volume using a bladder scanner. If volume
is 400 -500 mL or more, intervention is necessary:
In and out catheter is advised initially.
7. In and out catheterisation for trial of voiding
7.1 Purpose
To retain and restore bladder capacity after surgery or removal of catheter
To prevent over-distension of bladder (if the bladder becomes over-distended, it is more likely
that the patient will fail trial removal of catheter (TROC).
To prevent reflux or hydronephrosis leading to kidney damage.
7.2 Goal
To maintain total bladder volume (void plus residual) less than 500 mL
To keep the patient informed of all the actions and goal at all times.
7.3 Documentation
Use form CR5797: Trial Removal of Catheter
Document accurately times of voids, residuals and volumes
Document exact times of in and out catheterisation or IDC insertion.
Monitor a further two hours (i.e. until six hours postoperatively or removal of IDC, or sooner if
discomfort):
○ If void volume is good (approximately 200 mL or more) continue with non-invasive
measures (in
Section 6.2) and encourage two to three hourly voiding.
○ If no void or voids minimal amounts, verify bladder volume using a bladder scanner.
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 5 of 14
link to page 1 link to page 5 link to page 5

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
○ If volumes up to 400 mL offer supportive measures and encourage drinking up to 200 mL
per hour.
○ If volume is 400-500 mL, then intervention is necessary.
When bladder volume exceeds a critical limit of 500 mL, actions to empty the bladder should
be initiated, and in and out catheterisation is required.
A patient may have no symptoms despite high post-void residuals, identified by:
○ Ability to void
○ But no urge to void
○ No obvious symptoms of retention.
7.4 Actions
Commence on two-hourly timed voiding, and double voiding
Ensure adequate fluid intake
Start the Fluid Balance Record
Obtain urine sample for dipstick analysis and send mid stream urine (MSU) as required.
Assess for constipation and prescribe laxatives as necessary.
8. Urinary retention
Alert the Gynaecology team. Diagnosed by symptoms and bladder scanner:
○ In and out catheter initially (see
Section 7).
If unable to pass urine after further four to six hours and supportive measures have been
exhausted (see
Section 6.2): ○ Residual urinary volume 400-700 mL with inability to void will require IDC for 24 hours
○ Residual urinary volume > 700 mL with inability to void will require IDC for 48 hours.
Catheterisation rests the over distended bladder allowing it to gain its elastic recoil. It is
advisable to remove urinary catheters early in the day, to allow time for careful and regular
post-catheterisation bladder assessment.
After a failed trial of removal of catheter consider discussion with the Urogynaecology team
for further management and consideration of suprapubic catheter (SPC), and refer to the ward
physiotherapist.
Exclude constipation as a reason for urinary retention
9. Trial removal of catheter (TROC) following reinsertion of catheter
Reassure the patient.
Encourage two to three hourly voiding and document voids, until normal voiding patterns are
established.
Document all findings on form CR5797: Trial Removal of Catheter and document actions in the
patient’s clinical record.
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 6 of 14
link to page 1 link to page 5

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
Persistent urinary retention will require long-term resting of the bladder and management by
the Gynaecology team in conjunction with Urogynaecology.
If TROC failed twice, then consider IDC for duration of one week. Discuss with operating
surgeon if IDC or SPC is more appropriate.
Post-void residual results:
< 50 mL normal at most ages
< 150 mL normal for elderly
50-199 mL use clinical judgement to determine impact on each individual patient
> 200 mL inadequate voiding, refer back to supportive measures (see
Section 6.2) 500 mL requires an in and out catheter.
10. Bladder care following a urogynaecology procedure
Anti-incontinence surgical procedures are effective for the treatment of urethral hypermobility
and bladder descent, eliminating urinary leakage associated with stress urinary incontinence.
Preoperative and postoperative nursing care is critical for identification of potential risks,
preparation for surgery and interventions to prevent or diminish possible complications.
Although nonsurgical intervention is recommended as a first-line therapy, a patient may require
surgery for successful elimination of leakage such as:
Tension-free vaginal tape (TVT)
Anterior and posterior repair of vagina (colporrhaphy)
Burch colposuspension
Sacrospinous fixation
Fascial sling.
Monitoring of bladder function in postoperative period is paramount and nursing role is crucial.
The guideline on bladder care for urogynaecology patients should be read in conjunction with
sections 5-9 above. Most rules about bladder care for a urogynaecology patient apply as for
general gynaecology, with some vital exceptions.
It is important to remember that the urogynaecology patient might not feel urge to void due to
swelling related to the surgical procedure.
There are two techniques used to ensure adequate voiding is achieved after a urogynaecological
procedure. The surgeon will stipulate which technique they wish to be followed in their operating
note. If not stipulated the default technique will be the post-void residual measuring:
10.1 Post-void residual measuring
Refer to the above sections for immediate assessment on admission to the ward, removal IDC
and in and out catheterisation for trial of voiding (see sections 5-7).
Recommendation is for post-void residuals (unless otherwise specified by a surgeon):
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 7 of 14
link to page 1

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
○ Residual <150 mL – normal. Aim for three consecutive residuals of <150 mL and the patient
can be discharged home.
○ Residual 150-350 mL – continue monitoring and apply supportive measures (see above) as
necessary.
○ If ongoing residuals of >350 mL – continue into early evening, place IDC overnight to allow
the patient a good rest.
○ Repeat TROC next morning. Allow four hours to assess residuals, as above. If residuals
remain high, then operating surgeon is to be contacted and an IDC or SPC to be placed, and
followed up in one week’s time. A patient can be discharged, with written information on
catheter care.
○ DO NOT TROC A PATIENT MORE THAN TWICE.
Referral to a district nurse with recommendation to remove IDC in one week. If TROC fails,
district nurse to phone directly to the operating surgeon for further instructions.
SPC – to be removed once residuals are <150 mL on three consecutive voids.
It is recommended for a patient following urogynaecology surgery to receive regular laxatives
starting on the night of the surgery.
○ Lactulose 20 mL once a day and a Psyllium husk preparation 2tsp BD prescribed as regular
medication – lactulose should be stopped once bowel opened or if bloating occurs.
○ If a patient has history of constipation, Macrogol laxatives or similar three times a day to
be added.
○ It is useful to advise a urogynaecology patient to consume kiwifruit, Kiwi Crush, or
substitute for a duration of one week prior to surgery, to enhance bowel function in
preparation for surgery. This advice is given in preadmission clinic by a preadmission nurse.
10.2 Backfill voiding technique
Prior to removing the indwelling catheter postoperatively, backfill the bladder with 300 mL of
saline, then remove the catheter.
If a vaginal pack has been in place, ensure that this is also removed.
Ask the patient to void immediately after the backfill.
Measure the voided volume. If >150 mL then no further intervention is required.
If the void is <150 mL or the patient feels she has not completely emptied her bladder, have
her void again (double void).
If the total void volume is still <150 mL then run the bladder scanner to confirm residual
volume. If > 150 mL repeat voiding trials until residual <150 mL.
If unable to void after three trials replace IDC. Aim to re-TROC next day using post-void
residual measuring technique.
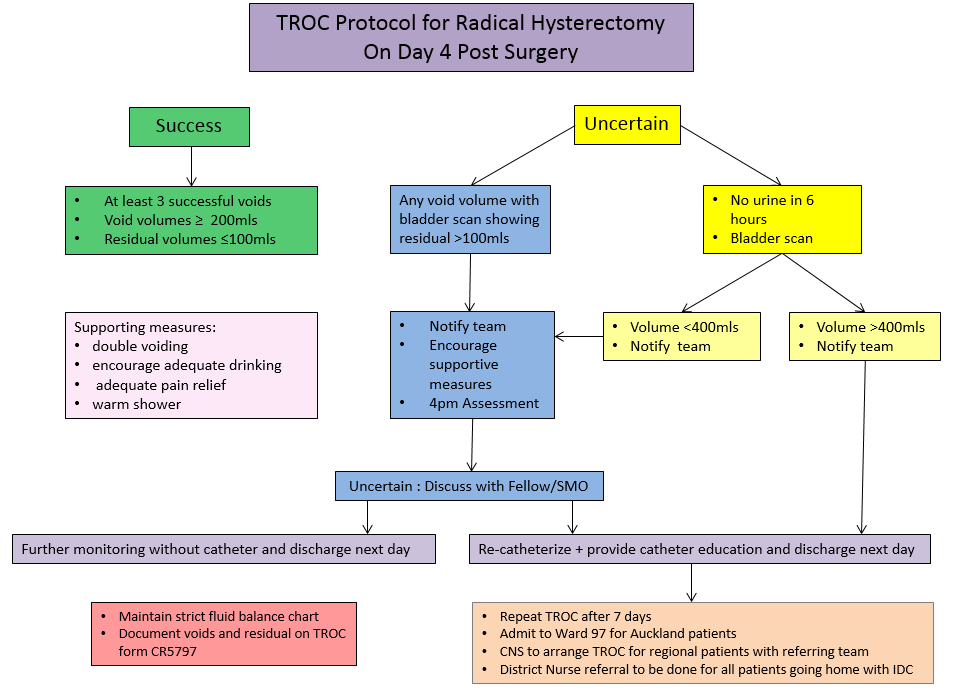
11. Bladder care following Radical hysterectomy
Bladder care following Radical hysterectomy varies slightly from that of Urogynaecology due to
the differences in the operations performed, amount of swelling that occurs around the nerves
due to the dissection involved, and the age of the patients. The main difference in protocol is that
the catheter stays in until day four. The following flow chart below explains the steps that should
be taken with this group of patients.
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 8 of 14
link to page 1


 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 9 of 14
link to page 1

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
12. Suprapubic catheter (SPC) management
Suprapubic catheterisation may be required postoperatively following surgery to the genitourinary
system.
The nurse is responsible for the patient’s education, dressings and discharge planning,
documentation on DD3089: Suprapubic Catheter Clamp and Void, and ensuring that SPC care is
performed safely.
12.1 Contradictions
Known bladder tumour
Empty or indefinable bladder.
12.2 Precaution
Lower abdominal wound or scarring.
12.3 Complications
Accidental trauma on SPC piercing the peritoneum or bowel
Urinary tract infection
Haemorrhage
Swelling, infection, encrustation or granulation at the insertion site.
12.4 Types of Suprapubic catheter (SPC)
In the Gynaecology service, a 12-14 g Foley catheter or a SPC with fixation plate such as Cystofix is
used.
12.5 Insertion of Suprapubic catheter (SPC)
Suprapubic catheterisation is an aseptic procedure carried out by a doctor. A nurse may be
required to assemble equipment, assist with the procedure and dress the site. The nurse should
also ensure the patient’s comfort and education. The patient should have full bladder prior to the
insertion of a SPC.
Ways to achieve this in elective procedures include:
Spigot the urethral catheter if already in situ and encourage oral fluids (where not
contraindicated).
Instil normal saline into the bladder via urethral catheter until the bladder is full. Spigot
urethral catheter.
Encourage oral fluids or administer prescribed intravenous fluids to fill bladder. Instruct the
patient not to pass urine.
12.6 Equipment required
Catheterisation pack
Extra gauge swabs x 2
Povidone- iodine2 large sterile guards
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 10 of 14
link to page 1

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
Needle 22 g x 2
10 mL syringe x 1
20 mL syringe x 1
Xylocaine 2% Scalpel blade and needle holder
Razor
Disposable incontinence sheets
Sterile gloves (2 pairs)
Catheter 12-14 g Foley, 2-way
Introducer (e.g. Cook Peel-Away) set must be 4 g higher in size (i.e. 16-18 g)
Urinary drainage bag
Sterile water for balloon (10 mL)
Opsite visible drain dressing or Hypafix
Secutape (NG small).
12.7 Procedure
Inform the patient of the procedure. Ensure the patient has a full bladder.
Assemble equipment and trolley.
Position the patient supine.
Assist with procedure as necessary.
Secure catheter and tubing to the patient. Dress insertion site with Opsite visible dressing or
Hypafix.
Document date, type and size of catheter inserted in the patient’s clinical record.
Secure the tubing laterally to the abdomen with Secutape.
12.8 SPC dressing of insertion site
Monitor for infection, bleeding or discharge on insertion, then as required.
12.9 Removal of SPC for an inpatient
Prior to the removal, it is a usual practice to spigot the SPC to ensure the patient is able to void
urethrally with acceptable residual urine volume. Recommended <150 mL residual urine. When
suprapubic drainage of the bladder is no longer required, the catheter can be removed by nursing
staff members.
12.10 Equipment
Small dressing pack
Sterile gloves
Sodium chloride 0.9%
Gauze squares
Combine dressing
Transparent dressing (e.g. Tegaderm)
20 mL syringe
Suture cutter (if suture present).
Note:
Ensure the patient’s bladder is empty prior to the SPC removal.
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 11 of 14
link to page 1 link to page 13 link to page 13

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
If the catheter has been spigoted for assessment of voiding, unspigot it to drain the residual
urine.
Persistent leakage from the insertion site may require frequent dressing changes or the
application of a urostomy bag for one to two days or until leakage settles down.
12.11 Discharging a patient with a Suprapubic catheter (SPC)
Key points:
Explain and educate SPC management and care to the patient and caregiver. Ensure that they
are aware that:
○ The SPC should be reinserted promptly if it falls out. Urgent medical attention should be
sought.
○ If the SPC blocks they should contact their district nurse or hospital.
Provide the patient with leaflet ‘Managing your Suprapubic Catheter at Home’ (see
Associated
documents)
Refer the patient to the District Nursing service.
Provide initial supplies such as leg bag and night bag.
Instruct the patient on how to connect leg bag to night bag for overnight drainage.
A District Nurse is able to manage suprapubic catheters and remove them once three voids or
residuals are <150 mL.
Send Referral Adult Community Services CR2144 form with clear instruction and a contact number
at the hospital for further support or queries.
12.12 Follow-up
Arrange outpatient appointment as advised by the team.
12.13 Recognising infection
A patient should seek help promptly from her General Practitioner (GP) if she has any of the
following signs or symptoms as they may indicate a urinary tract infection:
Fever, shivering, chills
Blood in the urine
Urine has an offensive odour
Urine is cloudy
Pain or aching in the back
Pain over the bladder
Offensive discharge, redness or pain from insertion site.
Note: Bacteriuria is only treated when the patient is symptomatic of a urinary tract infection or
compromised.
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 12 of 14
link to page 1

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
12.14 Residual urine measurement
Following some urological and gynaecological procedures, the patient may be discharged with a
SPC that is spigoted whilst a normal voiding pattern is re-established. The residual urine should be
measured immediately after voiding by releasing the spigot at regular intervals (e.g. BD, TDS or
QID), draining the catheter into a plastic container and then recording the volume. There is no
need to attach a catheter bag.
When voiding pattern and control returns to normal and the residual urine is minimal (as
determined by the medical team according to the patient’s history), it is likely that the doctor will
request the removal of the SPC.
13. Self-catheterisation
For patients with persistent retention a self-catheterisation to be considered as an option.
Use the Auckland DHB Urology Department guideline Urinary Drainage – Intermittent
Catheterisation on Hippo: Pages 9-13 are relevant for FEMALE intermittent self-catheterisation.
14. Supporting evidence
Baldini, G., Bagry, H., Apirikian, A., & Carli, F. (2009). Postoperative urinary retention:
Anaesthetic and periopreative considerations.
Anesthesiology, 11(5), 1139-1157.
Johnson, V. Y. (2002). Bladder neck suspension nursing care: preop, postop, and beyond.
Perspectives in Nursing Strategies, 8, 53-57.
Pavlin, D. J., Pavlin, E. G., Gunn, H. C., Taraday, J. K., & Koerschgen, M. E. (1999). Voiding in
patients managed with or without ultrasound monitoring of bladder volume after outpatient
surgery.
Anaesthesia Analgesia, 89, 90-97.
Rizvi, R. M., Khan, Z. S., & Khan, Z. (2005). Diagnosis and management of postpartum urinary
retention.
International Journal of Gynecology and Obstetrics, 91, 71-72.
Striker, K. & Steiner, W. (1991). Postoperative urinary retention.
Anaesthetist, 40(5), 287-290.
Wynd, C.A., Wallace, M., & Smith, K.M. (1996). Factors influencing postoperative urinary
retention following orthopaedic surgical procedures.
Orthopaedic nursing, 15(43), 43-50.
Foster Sr, R. T., Borawski, K. M., South, M. M., Weidner, A. C., Webster, G. D., & Amundsen, C.
L. (2007). A randomized, controlled trial evaluating 2 techniques of postoperative bladder
testing after transvaginal surgery.
American journal of obstetrics and gynecology, 197(6), 627-
e1.
Bagshaw, S. M., & Laupland, K. B. (2006). Epidemiology of intensive care unit-acquired urinary
tract infections.
Current opinion in infectious diseases, 19(1), 67-71.
Chenoweth, C. E., Gould, C. V., & Saint, S. (2014). Diagnosis, management, and prevention of
catheter-associated urinary tract infections.
Infectious Disease Clinics, 28(1), 105-119.
15. Associated documents
Bladder Care Postpartum and Management of Urinary Retention
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 13 of 14
link to page 1

 If printed, this document is only valid for the day of printing.
If printed, this document is only valid for the day of printing.
Infection Prevention and Control
Latex Safety
Urinary Drainage Suprapubic Catheter Management
Urinary Drainage Intermittent Catheterisation
Clinical forms
CR0023: Trial of Removal of Catheter (TROC) Referral Form
CR2144: Referral Adult Community Services
CR5797: Trial Removal of Catheter
DD3089: Suprapubic Catheter Clamp & Void
CR0452: Fluid Balance Record
Patient information
•
Managing Your Suprapubic Catheter at Home
16. Disclaimer
No guideline can cover all variations required for specific circumstances. It is the responsibility of
the health care practitioners using this Auckland DHB guideline to adapt it for safe use within their
own institution, recognise the need for specialist help, and call for it without delay, when an
individual patient falls outside of the boundaries of this guideline.
17. Corrections and amendments
The next scheduled review of this document is as per the document classification table (page 1).
However, if the reader notices any errors or believes that the document should be reviewed
before the scheduled date, they should contact the owner o
r Document Control without delay.
Back to Contents
Bladder-Care-Post-Gynaecology-and-Urogynaecology-Surgery_2021-10-30
Page 14 of 14