

Final report
Aviation inquiry AO-2019-003
Diamond DA42 aeroplane, ZK-EAP
Controlled flight into terrain
Kaimanawa Range, near Taupō
23 March 2019
November 2021
About the Transport Accident Investigation Commission
The Transport Accident Investigation Commission (Commission) is a standing commission of
inquiry and an independent Crown entity responsible for inquiring into maritime, aviation
and rail accidents and incidents for New Zealand, and co-ordinating and co-operating with
other accident investigation organisations overseas.
The principal purpose of its inquiries is to determine the circumstances and causes of
occurrences with a view to avoiding similar occurrences in the future. It is not the
Commission’s purpose to ascribe blame to any person or agency or to pursue (or to assist an
agency to pursue) criminal, civil or regulatory action against a person or agency. However,
the Commission will not refrain from fully reporting on the circumstances and factors
contributing to an accident because fault or liability may be inferred from the findings.
Final Report AO-2019-003
| Page i
Notes about Commission reports
Commissioners
Chief Commissioner
Jane Meares
Deputy Chief Commissioner
Stephen Davies Howard
Commissioner
Richard Marchant
Commissioner
Paula Rose, QSO
Key Commission personnel
Chief Executive
Martin Sawyers
Chief Investigator of Accidents
Harald Hendel
Investigator in Charge
Ian McClelland
General Counsel
Cathryn Bridge
Citations and referencing
This report does not cite information derived from interviews during the Commission’s
inquiry into the occurrence. Documents normally accessible to industry participants only and
not discoverable under the Official Information Act 1982 are referenced as footnotes only.
Publicly available documents referred to during the Commission’s inquiry are cited.
Photographs, diagrams, pictures
The Commission has provided, and owns, the photographs, diagrams and pictures in this
report unless otherwise specified.
Verbal probability expressions
Where possible, the Commission uses standardised terminology in its reports. This is for the
benefit of investigation participants, readers of its reports and recipients of its
recommendations. One example of this standardisation is in the terminology used to
describe the degree of probability (or likelihood) that an event happened or a condition
existed in support of a hypothesis.
This terminology, set out in the table below, has been adopted by the Commission and is
based on the Intergovernmental Panel on Climate Change and Australian Transport Safety
Bureau models. The Commission chose these models due their simplicity, usability and
international use. The Commission considers the suitability of these models as being
reflective of the Commission’s functions, which include the making of findings and
recommendations based on a wide range of evidence received, whether or not that evidence
would be admissible in a court of law.
Final Report AO-2019-003
| Page ii
Terminology
Likelihood
Equivalent terms
Virtual y certain
> 99% probability of occurrence
Almost certain
Very likely
> 90% probability
Highly likely, very probable
Likely
> 66% probability
Probable
About as likely as not
33% to 66% probability
More or less likely
Unlikely
< 33% probability
Improbable
Very unlikely
< 10% probability
Highly unlikely
Exceptional y unlikely
< 1% probability
Final Report AO-2019-003
| Page iii
 Figure 1: Diamond DA42, ZK-EAP
(Credit: Rodney Maas)
Figure 1: Diamond DA42, ZK-EAP
(Credit: Rodney Maas)
Final Report AO-2019-003
| Page iv
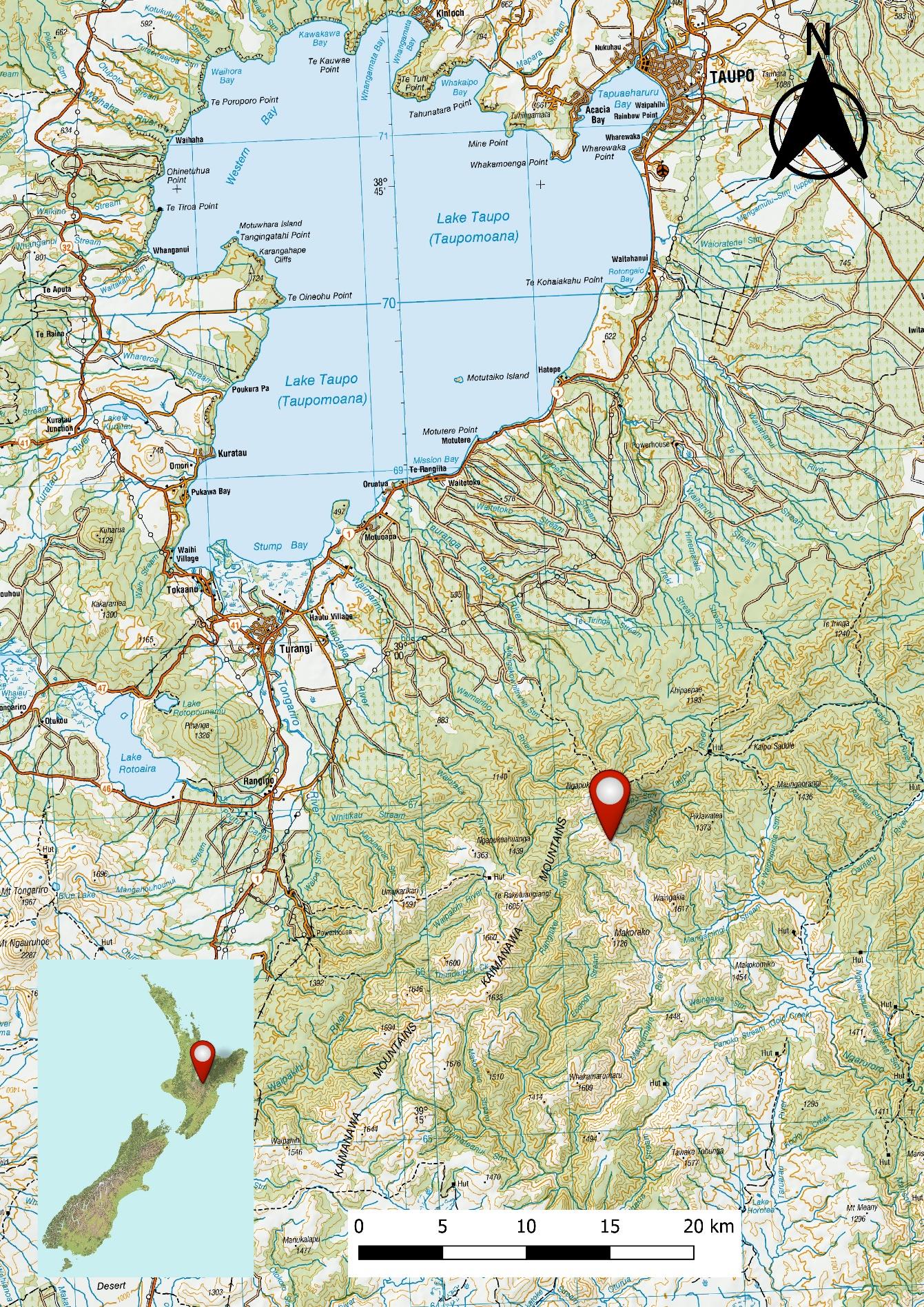 Figure 2: Location of accident reproduced on LINZ Topo250 map
Figure 2: Location of accident reproduced on LINZ Topo250 map
Final Report AO-2019-003
| Page v
link to page 10 link to page 10 link to page 10 link to page 10 link to page 11 link to page 12 link to page 12 link to page 14 link to page 14 link to page 15 link to page 16 link to page 17 link to page 19 link to page 21 link to page 21 link to page 22 link to page 22 link to page 23 link to page 24 link to page 26 link to page 26 link to page 26 link to page 26 link to page 28 link to page 28 link to page 28 link to page 29 link to page 29 link to page 31 link to page 36 link to page 36 link to page 37 link to page 38
Contents
1
Executive summary .............................................................................................................. 1
What happened ........................................................................................................................................................ 1
Why it happened...................................................................................................................................................... 1
What we can learn ................................................................................................................................................... 1
Who may benefit...................................................................................................................................................... 2
2
Factual information.............................................................................................................. 3
Narrative ....................................................................................................................................................................... 3
Background................................................................................................................................................................. 5
Safety pilot................................................................................................................................................................... 5
The flight ...................................................................................................................................................................... 6
Personnel information ........................................................................................................................................... 7
Aircraft information ................................................................................................................................................ 8
Meteorological information .............................................................................................................................10
Recorded data .........................................................................................................................................................12
Site and wreckage information .......................................................................................................................12
Medical and pathological information........................................................................................................13
Survival aspects.......................................................................................................................................................13
Organisational information...............................................................................................................................14
Other relevant information ...............................................................................................................................15
3
Analysis.............................................................................................................................. 17
Introduction ..............................................................................................................................................................17
Flight authorisation and flight planning.....................................................................................................17
Authorisation ............................................................................................................................................................17
Flight planning.........................................................................................................................................................19
Diversion from planned track and descent through the sector minimum safe altitude ...19
The diversion ............................................................................................................................................................19
Direct routing ...........................................................................................................................................................20
Minimum safe altitudes ......................................................................................................................................20
Minimum safe altitude warning ......................................................................................................................22
Safety pilot ................................................................................................................................................................27
Emergency locator transmitter........................................................................................................................27
4
Findings ............................................................................................................................. 28
5
Safety issues and remedial action ...................................................................................... 29
Final Report AO-2019-003
| Page vi
link to page 38 link to page 38 link to page 39 link to page 39 link to page 39 link to page 40 link to page 41 link to page 42 link to page 43 link to page 43 link to page 44 link to page 45
General ........................................................................................................................................................................29
Robustness of flight-authorisation procedures......................................................................................29
6
Recommendations ............................................................................................................. 30
General ........................................................................................................................................................................30
New recommendations.......................................................................................................................................30
7
Key lessons ........................................................................................................................ 31
8
Data summary.................................................................................................................... 32
9
Conduct of the inquiry ....................................................................................................... 33
10 Report information ............................................................................................................ 34
Abbreviations ...........................................................................................................................................................34
Glossary.......................................................................................................................................................................35
Appendix 1 Timeline .............................................................................................................. 36
Final Report AO-2019-003
| Page vi
link to page 5 link to page 6 link to page 13 link to page 13 link to page 34 link to page 34 link to page 34 link to page 35 link to page 35
Figures
Figure 1: Diamond DA42, ZK-EAP (Credit: Rodney Maas) .......................................................................... iv
Figure 2: Location of accident reproduced on LINZ Topo250 map ..........................................................v
Figure 3: Flight planned route (Not to be used for navigation) (Credit: Aeropath [Civil
Aviation Authority])........................................................................................................................................................... 4
Figure 4: The Diamond DA42 aeroplane G1000 instrument panel........................................................... 9
Figure 5: The G1000 multifunctional display moving map, showing a graphical presentation
of the terrain-conflict-proximity function (not representative of the flightpath of the accident
aircraft) .................................................................................................................................................................................... 9
Figure 6: GRAFOR before the accident .................................................................................................................10
Figure 7: GRAFOR after the accident .....................................................................................................................11
Figure 8: Accident site ...................................................................................................................................................12
Figure 9: Taupo RWY 35 RNAV Aeronautical Information Publication Approach Plate scaled,
georeferenced and superimposed on LINZ Topo250 map, with surveillance data showing
deviation and track direct to reporting point MASKU ..................................................................................25
Figure 10: Relationship between flight profile and MSA/terminal arrival altitude .........................26
Figure 11: Flight profile from top of descent to ground impact..............................................................26
Final Report AO-2019-003
| Page vi i
1 Executive summary
What happened
1.1. On 23 March 2019, a four-seat Diamond DA42 aeroplane was being flown from
Palmerston North to Taupō as part of a navigation flight originating from Ardmore.
Thirty minutes into the flight, while at 9,000 feet (2,745 metres) above sea level, the
aeroplane was turned away from the planned track and the pilot made a ‘top of
descent’ radio call to the flight information service. The aeroplane commenced a
descent at that time.
1.2. At 2213, about eight minutes after the descent had commenced, the aeroplane struck
terrain at about 4,500 feet (1,371 metres) and about 38 kilometres south of Taupō
Aerodrome. The pilot and safety pilot were fatally injured.
Why it happened
1.3. The Transport Accident Investigation Commission (Commission)
found that the pilot
descended the aeroplane below the specified minimum safe altitude for the area in
which the aeroplane was being flown, and a controlled flight into terrain occurred.
1.4. The Commission
found that the pilot operated the aeroplane outside the parameters
required for ‘direct routing’ navigation in uncontrol ed airspace, when attempting to
connect with an instrument approach from the en-route phase of the flight.
1.5. The Commission
found no evidence that any malfunction of or unserviceability with
the aeroplane, or any medical issue, contributed to the accident.
1.6. The Commission
found that the aeroplane was equipped with a terrain proximity
awareness capability but that it was very likely not used by the pilot.
1.7. The Commission
found that weaknesses in the flight-authorisation procedures
permitted pilots to conduct flights without the applicable authorisation, and therefore
supervision, of senior instructors. This is what occurred in this case.
1.8. The Commission
found that the pilot was licensed and rated to conduct flights in
accordance with instrument flight rules and at night. However, both the pilot and the
safety pilot had little experience in navigating at night under instrument flight rules.
They were therefore subject to an increased level of supervision by the operator until
they gained more experience.
What we can learn
1.9. The key lessons identified from the inquiry into this occurrence are:
• pilots, especially instructor pilots, should be fully aware of the parameters
prescribed by the Civil Aviation Rules, including for navigating away from pre-
planned and instrument flight rules- approved flight routes
• where possible, pilots should use and be proficient in the full capabilities of the
flight instrumentation systems available to them. In this case, thorough training in
Final Report AO-2019-003
| PAGE 1
the use of onboard ground-proximity conflict and warning systems, including the
dimming of instrument and cockpit lights at night, would have enhanced
situational awareness
• flight training schools should ensure that their procedures for flight authorisation
and supervision are sufficiently robust to ensure that pilots can only conduct
training flights after obtaining appropriate authorisation and supervision.
Who may benefit
1.10. Pilots, instructor pilots and flight training schools may all benefit from the findings in
this report.
Final Report AO-2019-003
| PAGE 2
2 Factual information
Narrative
2.1. On 23 March 2019 at 19401, a four-seat Diamond DA42 aeroplane, registration ZK-EAP
(the aeroplane), owned and operated by Ardmore Flying School (the operator),
departed Ardmore Aerodrome on an instrument flight rules (IFR)2 night navigation
consolidation flight. On board were a pilot and a safety pilot. The planned route was
from Ardmore to Palmerston North, returning via Taupō. The flight south to
Palmerston North was uneventful.
2.2. While on the ground at Palmerston North Aerodrome, the pilot talked to Ōhakea
Control and obtained an air traffic control clearance for the next leg to Taupō.3 The
aeroplane was “cleared Taupō via [reporting points4] APITI, RUAHI, TURUA, TAIKI at
9,000 feet [2,745 metres (m)]” above sea level5 (see Figure 3).6 At 2135 the aeroplane
departed Palmerston North. Once clear of Palmerston North Aerodrome the pilot
called Ōhakea Control and advised climbing past 2,300 feet (700 m) for 9,000 feet. The
Ōhakea controller acknowledged the call and advised that the aeroplane had been
identified.
2.3. At 2152 the Ōhakea controller passed on the latest weather information for Taupō. This
was given as a surface wind of 030° magnetic at 8 knots (15 kilometres per hour
[km/h]), 17 kilometres (km) visibility and overcast cloud at 4,500 feet (1,371 m). This
was acknowledged by the pilot. Shortly afterwards, the Ōhakea control er instructed
the pilot to change radio frequency to Christchurch Information as the aeroplane was
leaving control ed airspace7 and flying into uncontrol ed class G airspace.8
2.4. At 2203, after several attempts, the pilot established radio communication with
Christchurch Information. The Christchurch flight information officer (FIO)9 advised that
the aeroplane was in uncontrol ed airspace and that there was no reported traffic at
9,000 feet to Taupō. The FIO also passed on the local Manawatū altimeter pressure
setting10 and requested the pilot call when they were commencing their descent. The
pilot acknowledged the request.
1 Times are in New Zealand daylight time (co-ordinated universal time + 13 hours) and expressed in the 24-hour
format.
2 Flight by reference to instruments. The alternative is flight by visual reference, termed visual flight rules.
3 The Palmerston North air traffic control tower was off watch.
4 Sometimes termed waypoints. Reporting points can be compulsory or non-compulsory.
5 Al altitudes are in reference to above mean sea level.
6 Approval is required for aircraft to operate in controlled airspace and is subject to the direction of the
responsible controller.
7 In uncontrolled airspace around New Zealand, flight following is typical y provided by Christchurch Information,
operating on a range of frequencies. Pilots are responsible for maintaining their own separation from terrain
and other aeroplanes.
8 Airspace international y and in New Zealand can be either controlled or uncontrolled, and is further divided into
various classes. Uncontrolled airspace is termed class G airspace.
9 Airways New Zealand provides a flight information service through a flight information officer, who offers
limited assistance for pilots operating in uncontrolled airspace. The pilots remain responsible for terrain-conflict
avoidance and separation from other aircraft.
10 When the local pressure or QNH is set on an altimeter, it provides altitude above mean sea level.
Final Report AO-2019-003
| PAGE 3
Taupō
TAIKI
accident
site
TARUA
minimum safe
altitudes
RUAHI
APITI
Palmerston
North
Figure 3: Flight planned route
(Not to be used for navigation)
(Credit: Aeropath [Civil Aviation Authority])
Final Report AO-2019-003
| PAGE 4
2.5. At 2205 the aeroplane was recorded on radar turning left as it passed TARUA. At the
same time the pilot reported ‘top of descent’11 and the aeroplane was recorded as
starting to descend from 9,000 feet. The FIO replied, advising that there was no
reported traffic for the descent to Taupō, and asked, “Which runway lights would you
like?”.12 At 2207, after two further calls by the FIO, the pilot responded and was given
the local area altimeter pressure setting.
2.6. At 2209 the pilot requested the lighting for runway 3513 and confirmed that they would
be conducting the “RNAV [area navigation] 35 approach” followed by the “missed
approach14 onwards [to] Ardmore” (see Figure 9). The latest Taupō altimeter pressure
setting was passed during this time. The pilot and the FIO confirmed the routing to
Ardmore and when the air traffic control clearance for the next leg could be given. The
last transmission by the pilot concluded at 2212:48.
2.7. The wreckage of the aeroplane was located at about 1030 the following day. Both
occupants had died in the accident.
Background
2.8. The pilot, a Category B instructor with the operator, was working towards gaining a
multi-engine instrument instructor endorsement. This was in accordance with the
operator’s IFR instructor training programme approved under Civil Aviation Authority
(CAA) exemption 15/EXE/20. The purpose of the flight was for the pilot to gain
experience as the ‘pilot in command’ in a range of areas, including with multi-engine
aeroplanes and flying cross-country under IFR and at night. This formed part of the
operator’s CAA-approved instructor training programme, for the purpose of qualifying
the pilot as a multi-engine IFR instructor.
Safety pilot
2.9. The safety pilot was also a Category B instructor and was accompanying the pilot in
accordance with the operator’s procedures for IFR training flights. Civil Aviation Rules
Part 61 – Pilot Licences and Ratings, and Part 91 – General Operating and Flight Rules,
both referred to the role of a safety pilot. A safety pilot was to have adequate visibility
outside the aircraft, a current pilot’s licence and both aircraft type and instrument
ratings. For simulated instrument flight15, a safety pilot had to be able to take control
of the aircraft. The safety pilot on the accident flight met the criteria to perform the
function.
2.10. The operator’s standard operating procedures directed that “pilots will not be
approved for single-pilot IFR, without a safety pilot, unless authorised by the HoT
[head of training].” The procedures then described the role of the safety pilot as:
The safety pilot is essential y a passenger on the flight and as such is legal y unable to
11 When an aircraft transitions from the cruise phase of flight and starts to descend for the approach.
12 The aerodrome approach and runway lighting were remotely controlled by the FIO.
13 Runways are identified by their magnetic alignment, rounded to the nearest 10 ° increment. Runway 35 is
therefore aligned about 350° magnetic.
14 The phase of an instrument approach when an aircraft overshoots from the approach and climbs back to a safe
altitude.
15 Flight in simulated instrument meteorological conditions, with a pilot typical y flying with a hood or cover over
their head to prevent their looking outside the aeroplane.
Final Report AO-2019-003
| PAGE 5
touch the controls, or the radios. Once an instructor on board begins to give instruction they
also become Pilot in Command so there is a fine line that needs to be navigated to ensure the
students are getting the maximum out of the flight without making any errors relating to safety
(note: failing to fol ow correct procedures also compromises safety).
2.11. The procedures then listed the duties required of the safety pilot in relation to the “sort
of errors that may require intervention from the safety pilot or not”. These included:
• write all clearances, and communicate errors with readbacks, understanding, or
responsiveness
• point out to the pilot flying any altitude/speed/tracking deviations more than
100 [feet]/5 knots/half scale deflection respectively
• confirm with flying pilot their intentions if there is a likelihood of serious
infringement of airspace/aircraft limits/IFR procedural limits
• keep a good lookout, listening watch, and high level of situational awareness,
and identify to the pilot flying the position of any conflicting traffic
• communicate/discuss any issue at any time that may directly compromise the
safe conduct of the flight – i.e. a decision to fly into bad weather etc.
2.12. Any safety-critical intervention by the safety pilot had to be followed up with an
incident report on completion of the flight.
The flight
2.13. The pilot booked the flight at 1132 the day before the accident, using the ‘staff rental’16
facility built into the operator’s electronic booking system. A timeline of significant
events is at Appendix 1.
2.14. The operator was required by the CAA to ensure that IFR flights undertaken by
Category B instructors were authorised by training management (typical y the IFR team
leader or a Category A instructor). On the day of the accident, a Saturday, one of the
operator’s Category A instructors was present but left work that evening after
completing a navigation training flight. Because of other continued flying activities, the
operator’s operations or duty desk remained staffed by a senior Category B instructor
as required by the operator’s procedures.
2.15. The pilot and safety pilot arrived at the operator’s offices after the Category A
instructor had left. The pilot then accessed the authorisation system and was recorded
as self-authorising the flight at 1754. The operator’s flight booking form showed the
pilot nominated a ‘due back’ time of 0030 the next day.
2.16. The pilot also submitted an IFR flight plan to Air Traffic Services (ATS) for all three of
the flight sectors from Ardmore to Palmerston North and return. The flight plan
included a proposed take-off time from Ardmore of 1930 for the flight to Palmerston
North. The return flight to Ardmore was to be via Taupō and was planned for a take-off
from Palmerston North at 2140 and an arrival at Taupō 45 minutes later. The planned
route from Palmerston North to Taupō was via reporting points APITI, RUAHI, TARUA
and TAIKI at an altitude of 9,000 feet. This would result in the aeroplane approaching
16 One of the options available for booking a flight.
Final Report AO-2019-003
| PAGE 6
Taupō Aerodrome from an easterly direction. The return time at Ardmore was planned
to be 2330.17
2.17. At about 1900 the duty instructor18 noticed that the pilot and safety pilot were
preparing for their flight. The duty instructor, familiar with the latest weather reports
and aware of occasional showers in the area, thought the forecast “didn’t look the
best” for the planned flight. This was brought to the attention of the pilot. The pilot
reportedly checked the weather information again and said to the duty instructor that
they were happy with it. The duty instructor, as a Category B instructor, was able to
supervise Category C instructors and students only and was therefore not able to
authorise the pilot’s flight in accordance with the operator’s procedures.
2.18. Airways New Zealand surveillance data recorded the aeroplane taking off from
Ardmore at 1940 and landing at Palmerston North at 2127. The aeroplane then took
off from Palmerston North at 2135 for the return flight to Ardmore via Taupō. The
landing and take-off at Palmerston North were on runway 25.
2.19. The surveillance data showed that at 2205, while in the cruise at 9,000 feet on a north-
easterly flightpath at TARUA, the aeroplane turned onto a north-westerly flightpath.
This change in flightpath was coincident with the pilot making a radio call to the FIO
stating “top of descent”.
2.20. The data showed that shortly after the radio call the aeroplane started to descend
steadily at 500 feet (152 m) per minute, and after six minutes the rate of descent
increased to 750 feet (228 m) per minute.
2.21. Between 2207 and 2212, the FIO and the pilot discussed the type of instrument
approach to be flown, the runway lighting and the onwards clearance to Ardmore after
the planned missed approach. There were no further routine or emergency radio
transmissions heard from the aeroplane. (See paragraphs 2.44 to 2.46 for a further
discussion on post-accident events.)
Personnel information
2.22. Both the pilot and the safety pilot held aeroplane commercial pilot licences, Category B
flight instructor ratings, multi-engine instrument ratings and current medical
certificates, and were employed by the operator as flight instructors. The pilot
commenced flying training in September 2011 and obtained the Category B instructor
rating on 31 May 2018. The safety pilot commenced flying training in June 2009 and
obtained the Category B instructor rating on 15 February 2019.
2.23. The pilots had logged the following flight hours:
Pilot
Safety pilot
Total flight time
822.9 hours
832.0 hours
Total time pilot in command 603.3 hours
459.0 hours
17 This was earlier than the booking time return of 0030, which al owed for potential delays along the way.
18 The job title used the term ‘operations assistant’.
Final Report AO-2019-003
| PAGE 7
Total time instructing
395.4 hours
290.6 hours
Total night flying
46.7 hours
27.6 hours
Total night pilot in command 36.1 hours
19.1 hours
Total multi-engine flying
76.6 hours
68.3 hours
Total multi-pilot in command 15.6 hours
3.4 hours
Total instrument time
141.1 hours
108.9 hours
Total instrument flight time:
• Actual
13.9 hours
17.0 hours
• Simulated
44.7 hours
38.0 hours
• Ground
82.5 hours
57.0 hours
At the commencement of the flight the pilot had completed 8.8 hours of the required
25 hours of IFR cross-country flying.
2.24. The most recent medical certificate issued to the pilot by the CAA was dated 10
January 2019. The certificate precluded the pilot from carrying passengers on “single
pilot air operations”. This related to commercial flights and was therefore not
applicable to the pilot flying with students, non-fare-paying passengers or the safety
pilot. The certificate therefore was valid at the time of the accident.
Aircraft information
2.25. The aeroplane was a Diamond Aircraft Industries DA42 Twin Star, serial number 42.258,
manufactured in Austria in 2007. The aeroplane was powered by twin inline four-
cylinder, turbocharged Centurion 2.0 TAE 125-02-99 diesel engines, manufactured by
Thielert Aircraft Engines. The engines were fitted with three-blade constant speed
propellers.
2.26. The aeroplane had first been operated in Australia with the registration VH-DTS. It had
then been imported to New Zealand in August 2018 and registered as ZK-EAP.
2.27. The aeroplane was mainly constructed of carbon-composite material and each engine
was controlled by a full authority digital engine control (FADEC) system.
2.28. The aeroplane was equipped with a Garmin G1000 integrated flight instrument system
and a three-axis GFC 700 digital autopilot. The G1000 system in the accident aircraft
comprised two electronic display units. The display unit on the left was typically used
as the primary flight display. The display unit on the right was typical y used as a
multifunctional display (MFD) (see Figure 4). The MFD could be used to programme
flight plan data and display engine parameters and navigation information, including a
moving map and terrain-conflict-proximity information. The functions could be moved
between the two display units.
2.29. Terrain-conflict-proximity information was displayed graphically on the moving map.
Colour-coded areas of the map corresponded to the altitude of the aeroplane
determined by the global positioning system (GPS) with respect to the terrain elevation
stored in the digital database loaded into the G1000 system.
Final Report AO-2019-003
| PAGE 8

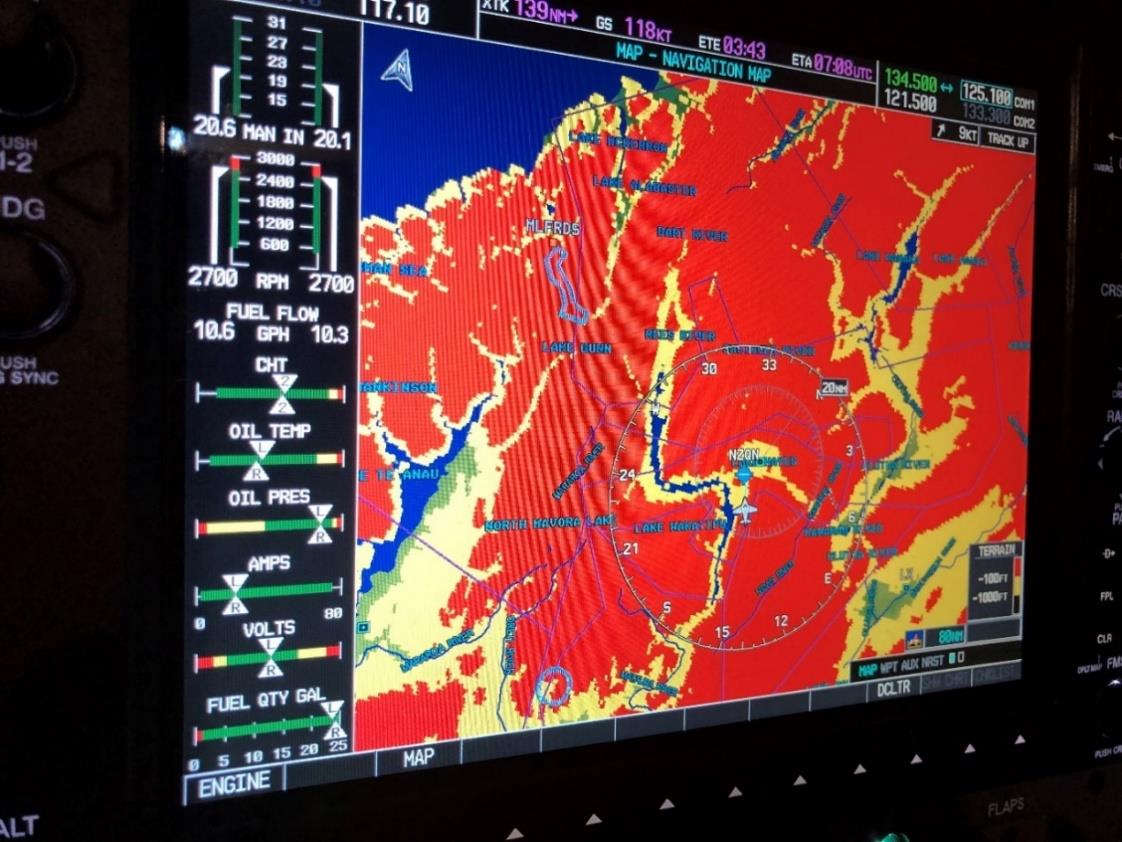
2.30. Yellow on the map signified that the terrain elevation was within 1,000 feet (304 m) of
the aeroplane’s GPS altitude. Red signified that the terrain elevation was within 100
feet (30 m) of the aeroplane’s GPS altitude (see Figure 5). The terrain conflict proximity
functionality could be selected on and off by the pilot. In night or low-light flight the
displays could be dimmed to reduce the glare generated by the display units.
Figure 4: The Diamond DA42 aeroplane G1000 instrument panel
2.31. The G1000 system manufacturer offered an optional augmentation to the terrain-
conflict-proximity functionality. The augmentation consisted of a secure digital card19
that unlocked the Class-B Terrain Avoidance and Warning System.20 The operator had
not purchased this augmentation for its DA42 aeroplane fleet.
Figure 4:
Figure 5: The G1000 multifunctional display moving map, showing a
graphical presentation of the terrain-conflict-proximity function (not
representative of the flightpath of the accident aircraft)
19 Secure Digital, official y abbreviated to SD, is
a proprietary non-volatile memory card format developed by
the
SD Association for use in portable devices.
20 A system that provides flight crew with sufficient information and alerting to detect a potential y hazardous-
terrain situation, so the flight crew may take effective action to prevent a collision with terrain.
Final Report AO-2019-003
| PAGE 9
 Meteorological information
Meteorological information
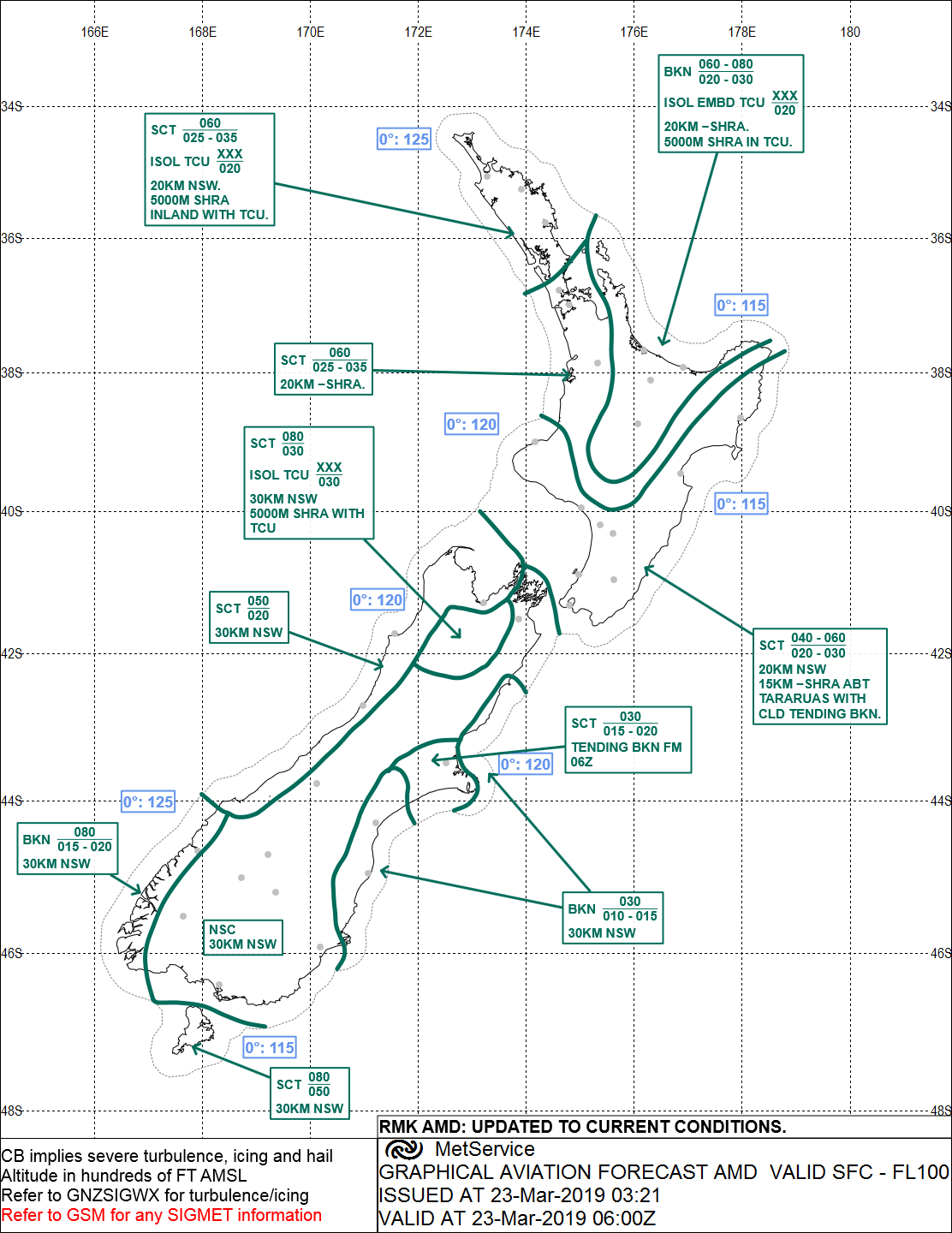
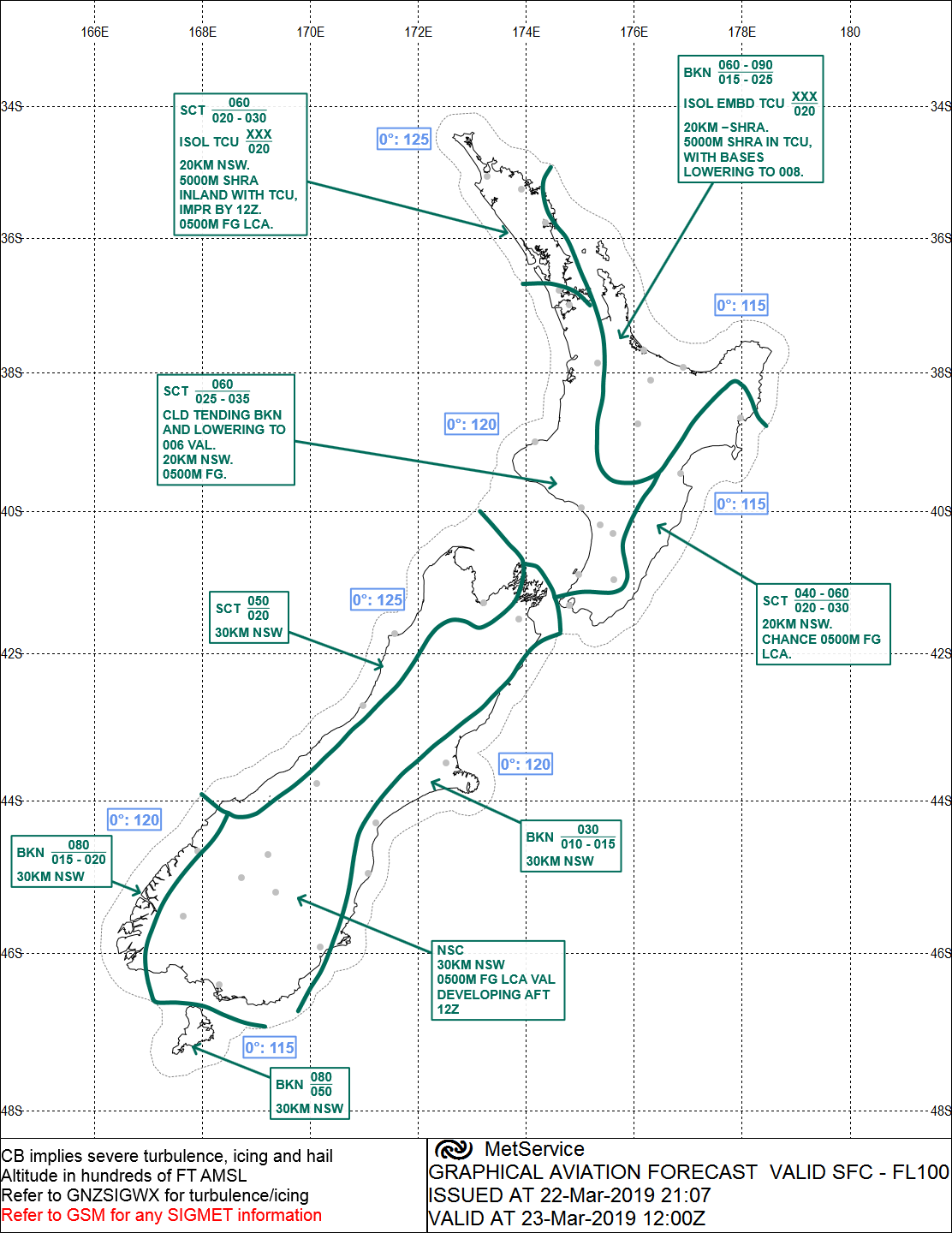
2.32. The graphical aviation forecast (GRAFOR) valid for approximately three hours prior to
the time of the accident (see Figure 6) specified for the Bay of Plenty and Taupō area
broken cloud21 between 2,000-3,000 feet (609-914 m) and 6,000-8,000 feet (1,828-
2,438 m), isolated embedded towering cumulonimbus above 2,000 feet, 20 km visibility
with showers and rain and 5 km visibility with showers and rain in towering
cumulonimbus cloud.
Figure 6: GRAFOR before the accident
21 Cloud is measured in eighths or oktas. Broken cloud is 5-7 oktas.
Final Report AO-2019-003
| PAGE 10
The GRAFOR valid for approximately three hours after the time of the accident (see Figure 7)
detailed broken cloud between 1,500-2,500 feet (457-762 m) and 6,000-9,000 feet (1,828-
2,745 m), isolated embedded towering cumulonimbus above 2,000 feet (609 m), visibility 20
km with showers and rain and 5 km visibility with showers and rain in towering
cumulonimbus cloud, with cloud bases lowering to 800 feet (243 m).
Figure 7: GRAFOR after the accident
Final Report AO-2019-003
| PAGE 11

2.33. A rescue helicopter pilot from Taupō Aerodrome who attempted to search for the
aeroplane at about midnight, said they had had to return to base as the conditions
about the Kaimanawa Range had deteriorated and were not suitable for flying in visual
meteorological conditions.22
2.34. The cloud conditions in the Taupō region and around the Kaimanawa Range were
forecast to worsen throughout the evening.
Recorded data
2.35. The Transport Accident Investigation Commission (Commission) obtained ATS
secondary surveillance radar data.23 This data showed positional information such as
latitude, longitude and altitude for the aeroplane during the accident flight. The data
included the descent path of the aeroplane, with the final radar plot closely matching
the actual location of the accident.
Site and wreckage information
2.36. The accident scene was situated at 4,500 feet (1,371 m) on sloping ground in the
Kaimanawa Range, approximately 38 km south of Taupō Aerodrome (see Figure 2).
2.37. The aeroplane had first hit the ground with the left wing tip. The left wing had
separated as a result. With the terrain sloping away, the remainder of the aeroplane
had continued in the general direction of the original flightpath for a further
approximately 250 m before striking the northern face of a gulley. The initial ground
scar made by the left wing tip and the location of the wreckage showed that the
aeroplane had been in about a straight and level attitude when the ground strike
occurred (see Figure 8).
Figure 8: Accident site
22 Flight under visual flight rules requires pilots to remain clear of cloud and in sight of ground or water.
23 Primary radar transmits a radar pulse and is reliant on the detection of sufficient reflected energy. Secondary
radar uses an aircraft’s transponder, which responds to a pulse from a ground-based antenna by transmitting a
return signal. The return signal may include aircraft identification (transponder code) and altitude information.
Final Report AO-2019-003
| PAGE 12
2.38. The blades on the left and right propellers had shattered, and shards of wood had
been dispersed widely throughout the first 100 m of the accident scene. The main
portion of the aeroplane comprising the fuselage, right wing and right engine
indicated the end of the wreckage trail. The right engine had separated structurally
from the wing but remained attached to the wing by electrical cables. The left engine
was found embedded in the ground nearby. There was no evidence of a fire having
occurred.
2.39. The aeroplane was examined at the accident scene and all flight-critical and major
components were accounted for. The aeroplane was then removed and taken to the
Commission’s facility, where a more detailed examination was conducted.
2.40. The digital engine control units were removed from the aeroplane and sent to
Bundesstelle für Flugunfal untersuchung (the German Federal Bureau of Aircraft
Accident Investigation) (BFU)24 for analysis of the recorded data. It was determined
from the analysis of the data that the engines had been operating normally throughout
the flight.
2.41. There was no evidence found of any technical abnormality with the aeroplane or its
engines that could have contributed to the accident.
Medical and pathological information
2.42. Post-mortem examinations of the pilot and safety pilot identified nothing that might
have been considered contributory to the accident. Toxicology results for both pilots
were negative for any performance-impairing substances. Low levels of a medication
were found in the pilot, but these were considered by a specialist aviation medical
practitioner to be of such low value that they would not have impaired pilot’s
performance.
Survival aspects
2.43. Following the scheduled missed-approach time when the pilot was expected to call
Christchurch Information to obtain the onwards clearance to Ardmore, the FIO called
the aeroplane repeatedly. The FIO received no response so the aeroplane was declared
overdue. The Rescue Coordination Centre New Zealand was informed and at 2245
initiated search action. Inclement weather prevented rescuers accessing the search area
during the remainder of the night. A helicopter crew involved in the search eventual y
located the wreckage of the aeroplane at about 1030 the next day.
2.44. The aeroplane was fitted with a 406-megahertz emergency locator transmitter (ELT),
which did not emit an emergency locating signal as intended. Searchers were therefore
reliant on available radar data and visual search techniques.
2.45. The Commission has investigated previous accidents where ELTs failed to operate as
designed. Following an accident in 2011 the Commission made two recommendations
to the CAA on the matter.25 The issue was also added to the Commission’s Watchlist,
24 The BFU is the state organisation responsible for the investigation of accidents and serious incidents within
Germany. Germany was the state of manufacture for the aeroplane and engines.
25 Inquiry 11-003: Inflight break-up ZK-HMU, Robinson R22, near Mount Aspiring, 27 April 2011.
Final Report AO-2019-003
| PAGE 13
under the title ‘Technologies to track and to locate’, and included rail and maritime
transport as well as air.
Organisational information
2.46. The operator of the aeroplane was a flight training school certificated under Civil
Aviation Rules Part 141 – Aviation Training Organisations Certification. At the time of
the accident the operator offered training for qualifications ranging from ab-initio
private pilot to Category C commercial multi-engine IFR instructor.26 At the time of the
accident there were approximately 35 instructors and 150 students at the school.
2.47. The operator employed Category C instructors on a salaried full-time basis, while also
providing developmental flight training for them through the operator’s internal
instructor training programme.
2.48. The instructors were mentored through their training to Category B qualifications, after
which they had more responsibilities in their roles and associated rises in salaries. The
intent of this arrangement was to encourage instructors to remain with the operator
until they ultimately left to further their careers with airlines.
26 See
www.aviation.govt.nz/assets/rules/consolidations/Part_061_Consolidation.pdf for information.
Final Report AO-2019-003
| PAGE 14
2.49. The pilot of the accident aeroplane, as part of the bonding agreement for salaried
instructors, had been permitted ‘free gratis’ use of the operator’s aeroplanes for
training purposes. The cost of the flying was held against a bond.
2.50. Civil Aviation Rules 61.307(c) – Currency Requirements states that the holder of a
Category A, B, C or D flight instructor rating must not give IFR cross-country navigation
instruction unless the flight instructor holds a current instrument rating. The instructor
must also have completed a minimum of 50 hours as ‘pilot in command’ on IFR cross-
country operations that has been certified by a flight examiner in the instructor’s
logbook.
2.51. The CAA had granted the operator an exemption (15/EXE/20) from Civil Aviation Rules
61.307(c) for the training of instructors. This allowed a trainee instructor to conduct
their accumulation of flight hours and IFR training under supervision with less than the
minimum 50 hours as ‘pilot in command’ of a cross-country flight under IFR.
2.52. The exemption allowed a reduced-hour programme for an upgrade to a multi-engine/
instrument instructor qualification, which involved a trainee instructor completing 25
hours’ instrument time/cross-country instead of the 50 hours. The reduced-hour
programme called for seven hours of flight-simulator time and three hours of single-
engine time, then 15 hours of instructor consolidation flight time. This was the purpose
of the accident flight.
2.53. The operator’s exposition stated that instructors seeking to take advantage of this
programme had to agree to the initial 25 hours being strictly supervised by the HoT,
the IFR Team Leader or a senior instrument-rated instructor approved by the HoT.
Before undertaking a flight under the programme, instructors were required to obtain
authorisation from a training management instructor. The pilot on the accident flight
did not conform with this requirement before departing Ardmore.
Other relevant information
2.54. The pilot, by deviating from the planned route at TARUA and flying directly towards
MASKU, was flying an unevaluated route, termed direct routing.27 The following Civil
Aviation Rules Part 19.217 – Transition Rules prescribes the standard for IFR flight on
unevaluated routes:
CAR 19.217: Flight on unevaluated routes
a)
Subject to paragraph (b), a pilot-in-command of an aircraft operating within
the New Zealand flight information region under IFR using GPS equipment as
a primary means navigation system is permitted random flight routing if
operating—
1)
within the area of a circle 20 nm radius centred on 43O36’S
170O 09’E (Mount Cook), at or above flight level 160; or
2)
in any other airspace, at or above flight level 150.
b)
A pilot-in-command of an aircraft is only permitted random flight routing
within control ed airspace if authorised by ATC [air traffic control]
.
27 When an aircraft is flown along a route that has not been charted and has not been evaluated Sometimes
referred to as ‘random routing’. AIP New Zealand, ENR 1.6-19, effective 6 February 2014.
Final Report AO-2019-003
| PAGE 15
c)
A pilot-in-command of an aircraft operating under IFR using GPS equipment
as a primary means navigation system is permitted random flight routing
below flight level 150 if—
1)
authorised by ATC; and
2)
ATC continuously radar monitor the flight for adequate terrain
clearance.
2.55. The following relevant excerpts from the Aeronautical Information Publication New
Zealand outlines the authorisation for clearance to descend on an instrument approach
provided for by a flight plan filed with ATS:
AIP [Aeronautical Information Publication] ENR 1.5: 4.4 Minimum Initial
Approach Altitude
4.4.1 A clearance for an IFR aircraft to carry out an instrument approach:
a)
except where otherwise instructed, authorises the aircraft to descend to
the minimum procedure commencement altitude in accordance with:
i.
STAR[standard instrument arrival];
ii.
RNAV arrival;
iii.
Route MSAs [minimum safe altitudes] including distance
steps;
iv.
25 NM MSA sector altitude chart;
v.
TAA [terminal arrival altitude]28;
vi.
VORSEC [VOR/DME Minimum Sector Altitude] chart; and
b)
may include level restrictions applicable prior to approach
commencement; and
c)
may include level restrictions associated with circuit integration.
4.4.2 Except when under radar control, or in accordance with a specific arrival
procedure promulgated in AD 2, the minimum initial approach altitude
issued to an aircraft that is to carry out an instrument approach must be
the higher of:
a)
the minimum procedure commencement altitude shown on the
instrument approach chart; or
b)
the MSA for the route sector.
The MSA for the route sector will be determined using one of the following
procedures. Where more than one option is available the procedure
that offers the lowest MSA will be used.
i.
the MSA for the ATS route including enroute descent
(Distance) steps;
ii.
the MSA after VORSEC chart steps;
iii.
the altitude quoted in the 25 NM MNM Sector Altitude
diagram;
iv.
for GNSS [global navigation system satel ite] approved
aircraft the altitude quoted in the Terminal Arrival Altitude
diagram.
28 A terminal arrival altitude provides a transition from an en-route structure to an RNAV approach procedure.
Final Report AO-2019-003
| PAGE 16
3 Analysis
Introduction
3.1. The flight was a pre-planned IFR navigation exercise for the pilot to build flying hours
towards a multi-engine instrument instructor qualification. Both the pilot and the
safety pilot were appropriately qualified to conduct such a flight. The flight proceeded
normally until the aeroplane deviated from the planned and evaluated route at TARUA
directly towards MASKU. A descent from the cruise altitude of 9,000 feet (2,745 m) was
commenced at this time. The aeroplane consequently descended below the minimum
safe altitude (MSA)29 of 7,800 feet (2,377 m) for that sector. The aeroplane struck the
terrain at about 4,500 feet (1,371 m) in about a straight and level attitude, and both
pilots died in the accident.
3.2. The investigation found no evidence of any medical or mechanical issues that may
have contributed to the accident. The investigation found no evidence that either pilot
was likely fatigued during the flight. The nature of the accident therefore has the
characteristics of a ‘controlled flight into terrain’ accident. A control ed flight into
terrain can be described as when “an airworthy aircraft under the complete control of
the pilot is inadvertently flown into terrain, water, or an obstacle. The pilots are
generally unaware of the danger until it is too late” (sources: ICAO [the International
Civil Aviation Organization] and SKYbrary30).
3.3. The following sections analyse the circumstances surrounding the event to identify
those factors that increased the likelihood of the event occurring or increased the
severity of its outcome. It also examines any safety issues that have the potential to
adversely affect future operations.
Flight authorisation and flight planning
Authorisation
3.4. The operator’s reduced-hour instructor training programme syllabus specified that IFR
cross-country flights had to be authorised by a training management instructor. The
intent of this requirement was to provide an added level of supervision for pilots who
were newly qualified and gaining experience in this type of flying.
3.5. The operator’s computerised flight-booking system was designed to ensure that the
syllabus for the course-based flights was completed in the correct order and that the
appropriate authorisations were completed. The computerised system was not
configured to limit personnel authorising their own flights electronical y if the flight
bookings were being made as ‘refreshers or rentals’. These bookings were made using
the booking computer programme ‘tab’ to select the ‘refresher or rental’ booking
page.
29 The minimum safe altitude (MSA) is the lowest altitude which may be used which wil provide a minimum
clearance of 1,000 feet (304 m) above al objects located in the area contained within a sector of a circle of 46
km (25 nautical miles) radius centred on a radio aid to navigation (ICAO).
30 SKYbrary is a repository of aviation safety information created by ICAO, the European Organisation for the
Safety of Air Navigation and the Flight Safety Foundation.
Final Report AO-2019-003
| PAGE 17
3.6. The accident flight was planned for a weekend evening. The operator had minimal
senior personnel available at this time. This was reported to be normal for that time of
day and week. The flying schedule component of the operator’s computerised flight-
authorisation system showed that the pilot authorised the flight at 1754 on the day of
the accident as a ‘refresher or rental’.
3.7. The pilot was well respected by fellow staff and known to be knowledgeable and
conscientious. The pilot was
very likely31 aware of the authorisation requirements,
their having previously fol owed the correct process. Why the pilot elected to self-
authorise the flight could not be determined. In the absence of the Category A
instructor who had left earlier, the pilot could have phoned another senior instructor to
approve the flight. Telephone records showed that this did not occur.
3.8. A review of the operator’s flight-authorisation records found no previous incidence of
unapproved flight self-authorisation by the pilot or any other instructor.
3.9. The role of the duty instructor or operations assistant was to ensure the smooth-
running of the flying schedule for the day. It was not to authorise flights, which was the
role of a student’s allocated instructor. The duty instructor on duty on the day of the
accident was being proactive in ensuring the pilot was aware of the current and
forecast weather conditions. As
3.10. junior B-category instructor, and therefore less familiar with IFR navigation
requirements, the duty instructor considered the pilot knew best.
3.11. The operator advised that the Palmerston North to Taupō route flown by the pilot was
not one of the approved routes typical y used for single-pilot IFR training. This was
because of the high MSA for the route, which a light twin-engine aeroplane such as the
DA42 aeroplane would struggle to maintain should an engine malfunction occur. Any
flight to Taupō would normal y have approached from the north or west where there
were lower MSAs available.
3.12. Following the accident the operator advised that had a senior instructor examined the
proposed flight plan and weather information as part of the authorisation process, the
flight would most likely not have been authorised. Following the accident, the
operator’s standard operating procedures were amended to state that the chief flying
instructor’s approval was required for any single-pilot IFR navigation flights other than
those routes specifical y listed in the procedures. (Note the Commission would also
expect that, before authorising such a flight, an authorising person would review how a
pilot intended to transition from the intended route to an instrument approach. See
the section below on ‘Diversion from planned track and descent through the sector
minimum safe altitude’.)
3.13. Further, the operator amended the list of tasks for duty instructors to include, among
other things, ensuring that no flight (including simulator flight) takes place without the
correct authorisation, and informing the operator’s chief flying instructor should any
student or instructor fail to follow procedures.
31 ‘Very likely’ suggests a >90% probability. Refer to the verbal probability expressions on page i i.
Final Report AO-2019-003
| PAGE 18
Flight planning
3.14. A pre-planned pilot’s flight log was found at the accident scene. This listed the planned
track reporting points from Palmerston North to Taupō. The entries are depicted in the
following table:
From
To
Route
Track
MSA
Altitude
Airspeed
Groundspeed
(magnetic) (feet)
(feet)
(knots)
(knots)
PM
APITI
H364
SID
4,300
9,000
120
120
APITI
RUHAHI
”
003
7,100
“
“
“
RUHAHI
TARUA
“
“
7,000
“
“
“
TARUA
TAIKI
”
004
7,800
“
“
“
TAIKI
NZAP
H211
298
6,500
“
“
“
3.15. The flight log showed that the pilot had reviewed and validated each of the legs along
the planned route, including the relevant MSAs. The flight log made no reference to
the deviation from the planned track at TARUA. Therefore, it would appear that the
pilot did not undertake any form of route check or validation of the revised route from
TARUA, or at the very least did not record it.
Diversion from planned track and descent through the sector
minimum safe altitude
The diversion
3.16. At 2205, while near TARUA, 46 nautical miles (85 km) south of Taupō, flying at a
groundspeed of 165 knots (305 km/h) at 9,000 feet, on a track of 003° magnetic, the
pilot advised the FIO that the aeroplane was at ‘top of descent’. The ATS surveillance
data showed that the aeroplane then turned left some 35° and started to descend. The
rate of descent soon stabilised at 500 feet per minute.
3.17. The turn was considered to be deliberate given the accuracy of the navigation up to
TARUA, the large change in heading and the sustained new direction. However, despite
ensuing radio communication between the pilot and the FIO, the pilot made no
reference to the manoeuvre or to amending the flight plan with ATS.
3.18. The reason for the change in flightpath could not be fully established; however, it was
very likely influenced by the weather, both current and forecast. The weather report
passed by the Ōhakea controller at 2152 was the first confirmation of the actual
weather conditions at Taupō since the aeroplane had left Ardmore. Up until this time
the pilot would not have been sure of which runway was in use at Taupō – runway 35
or runway 17.
3.19. The wind at Palmerston North during the approach to land there was reported as 150°
magnetic at less than 5 knots (9 km/h). The pilot subsequently landed and took off
using runway 25. Both the wind and runway 25 at Palmerston North were closer
aligned to using runway 17 at Taupō. With this new information, the pilot would have
been able to determine the preferred instrument approach to fly.
Final Report AO-2019-003
| PAGE 19
3.20. The pilot’s intention was confirmed when the pilot advised the FIO of the runway lights
that should be turned on and that they intended to complete the RNAV 35 instrument
approach and missed approach procedures. The new track from TARUA would take the
aeroplane directly towards reporting point MASKU, which was one of three initial
approach fixes that led to the RNAV 35 instrument approach (see Figure 9). The other
two initial approach fixes, EMSAR and AKABA, catered for aircraft joining from a more
northerly or western approach direction.
3.21. The new routing from TARUA to MASKU also provided several advantages over the
original route via TAIKI. Firstly, it was better orientated for the RNAV 35 approach.
Secondly, it did not require the pilot to fly overhead Taupō and then head south before
turning back to intercept the inbound track from reporting point AP506. And thirdly,
because it was a shorter route, it offered a not-insignificant timing saving. The forecast
deterioration in weather conditions during the late evening would also have had an
influence.
Direct routing
3.22. The change in route from TARUA took the aeroplane away from an evaluated and
charted route. The aeroplane was now flying along a direct and unevaluated track in
uncontrolled airspace below flight-level 150 or 15,000 feet. This did not meet the
requirements of Civil Aviation Rules relating to IFR flight in uncontrol ed airspace (see
2.56).
3.23. To change the flight plan loaded in the aeroplane’s flight-navigation system while en
route, the pilot would have had to update the route and activate it manual y. This
would have required a purposeful action from the pilot. Having updated the flight plan,
the pilot should then have updated the flight log with the revised reporting points, and
validated the integrity and safety of the new plan prior to activation. Once the plan was
activated, the pilot could then have manual y followed the new plan or used the
autopilot function.
3.24. The accuracy with which the aeroplane followed the route, including the altitude, from
Palmerston North to TARUA and then turning directly overhead TARUA, made it
likely that the aeroplane was being flown using the autopilot. In this situation, it would be
expected that a pilot activating a revised flight plan would complete a validation of the
new plan and update the flight log, and then monitor the aeroplane’s performance
once the autopilot system was engaged into the appropriate mode. The validation of
the revised flight plan would include safety checks, including whether the revised
profile would complied with airspace restrictions, such as the MSA.
3.25. To comply with Civil Aviation Rules, the pilot needed to continue flying the aeroplane
along an evaluated route until it was within the 25-nautical-mile (46 km) terminal
arrival altitude of an initial approach fix, then adhere to the relevant sector MSA until
established on the instrument approach. Direct routing is only permitted in controlled
airspace subject to obtaining clearance from air traffic control.
Minimum safe altitudes
3.26. The MSA for the sector between TARUA and MASKU, specified in the Aeronautical
Information Publication chart for the RWY 35 RNAV approach at Taupō Aerodrome,
was 7,800 feet (2,377 m). After MASKU this lowered to 4,500 feet (1,371 m) until the
Final Report AO-2019-003
| PAGE 20
initial fix AP506. This was the commencement point for the instrument approach. The
surveillance data showed that at 2208, five minutes prior to the accident, the aeroplane
descended below 7,800 feet. This was some 20 nautical miles (37 km) short of MASKU
(see Figures 10 and 11).
3.27. The rate of descent during the early part was steady at 500 feet (152 m) per minute.
This would indicate that positive control of the aeroplane was being maintained.
During the descent the pilot was engaged in regular radio communication with the
FIO. There was no declaration of an emergency or a state of urgency.32 The radio cal s
were what would have been expected in the circumstances – a planned descent for an
instrument approach in uncontrol ed airspace.
3.28. At 2211, while at an altitude of 6,550 feet (1,996 m) and a groundspeed of 160 knots
(296 km/h), the rate of descent increased to 750 feet (228 m) per minute and the
groundspeed began to decrease slightly. This rate of descent continued for a further
approximately two minutes until the aeroplane was approaching the terrain at about
150 knots (278 km/h). The increase in rate of descent was
likely related to the pilot
attempting to be at 4,500 feet and starting to configure33 the aeroplane by MASKU.
The aeroplane struck the terrain at 4,500 feet in about a level attitude.
3.29. The aeroplane descending below 7,800 feet, the sector MSA, indicates that an effective
validation of the new route was not performed by either pilot. Had this been done, it
should have revealed the likelihood of a conflict with the MSA and possibly a terrain
conflict. It is therefore
very likely that the pilots were focused on the commencement
of the instrument approach and not what was immediately in front of and below them.
3.30. If the MFD had been appropriately configured, and according to the G1000 reference
guide for the DA42 aeroplane, it should have been depicting yellow terrain in proximity
to the aeroplane for approximately one minute prior to the impact, and red terrain
forward of the aircraft for approximately 20 seconds (Figure 5). The red terrain
corresponded to the ridgeline with which the aeroplane collided.
3.31. The two alerts should have provided sufficient time for the pilots to initiate an
immediate climb back to above the MSA. That this did not occur indicates four
possibilities: the terrain proximity function was not selected; it was selected but the
displays were dimmed to the extent that any alert was not clearly visible; the pilots did
not react to the alerts; or there was an electronic display malfunction. It was considered
exceptionally unlikely that either pilot would have ignored an altitude alert or that
there was an electronic display malfunction for the following reasons:
• both pilots had learned to fly and subsequently instructed on single-engine
aeroplanes equipped with G1000s, and therefore should have been familiar
with the electronic displays and their functions
• the terrain proximity display was large, imposing and directly in front of the
pilots
32 A condition concerning the safety of an aircraft or other vehicle, or of some person on board or within sight,
but that does not require immediate assistance. Urgency messages should be preceded by the word ‘PAN’
repeated three times.
33 Slowing an aeroplane to lower flaps and landing gear.
Final Report AO-2019-003
| PAGE 21
• there was no previously reported problem with the electronic displays fitted to
the aeroplane, including during the flight immediately preceding this one
• a malfunction, including a partial malfunction, that relates to the display of
navigation data on an MFD should be quickly detected by a pilot, especial y
when it is providing critical information
• should an MFD fail, the navigation information could still be displayed on the
second electronic display
• should a double electronic display failure occur, the aeroplane was fitted with
backup primary flight instruments34 that would have guided a pilot to climb to
above the MSA
• the last radio transmission from the aeroplane was less than one minute before
the collision, and this suggested nothing was wrong.
3.32. It is therefore
very likely that the terrain proximity was either not selected or, to assist
with the pilots’ night vision, the display had been dimmed too far. The pilot and safety
pilot subsequently focused on the task of descending at the required rate to achieve
the promulgated terminal arrival altitude of 4,500 feet, prior to reaching MASKU. This
would have assisted in a successful capture35 of the instrument approach for runway
35.
3.33. When considering the forecast weather conditions and the weather reports from the
searching helicopter pilots, it was
very likely that the aeroplane was descending in
cloud from 6,000 feet (1,828 m) to the point of collision with the terrain. The pilots
therefore would have not been able to visually assess the proximity of the aeroplane to
the terrain. The darkness further compounded the situation.
3.34. Other than the graphical presentation of terrain proximity on the MFD, the aeroplane
was not equipped with an impending-terrain-collision warning, nor was it required to
be.
Minimum safe altitude warning
3.35. As ZK-EAP descended below the 7,800-foot MSA for that sector, it was being recorded
on radar. A radar display was available at the FIO’s workstation. However, while an FIO
may refer to the display, an aircraft cannot be controlled in class G airspace because of
the rules relating to this classification of airspace. Further, radar coverage in class G
airspace is not always reliable and is often non-existent. Importantly, FIOs are not
trained radar control ers, and air traffic surveil ance procedures do not require FIOs to
continuously monitor individual aircraft in uncontrol ed airspace using radar. For this
and other reasons described below, several of the functions available at some of the
radar controllers’ workstations are not available or are disabled for an FIO. These
include minimum safe altitude warnings (MSAWs), short-term conflict alerts and
airspace intrusion warnings.
3.36. A MSAW is a ground-based safety net designed to detect an aircraft descending too
low, increasing the risk of a controlled flight into terrain (CFIT) accident. MSAW was
34 Attitude indicator, altimeter, airspeed indicator and compass.
35 The term ‘successful capture’ is used to describe commencing an instrument approach procedure in a stable,
controlled and correct manner.
Final Report AO-2019-003
| PAGE 22
designed specifical y to protect an aircraft when it descended below the minimum safe
altitude for an area while fol owing an approved instrument approach procedure to a
controlled aerodrome.
3.37. A MSAW is restricted to controlled airspace, where an air traffic controller trained in
the use of MSAW can react appropriately. The automated system generates an alert on
the controller’s radar display in sufficient time to enable the controller to issue an
instruction or warning to a pilot of an aircraft under their control. To ensure a MSAW is
credible, the system requires reliable radar coverage, the transmission of aircraft
altitude information and an accurate survey of the local terrain. The pilot and controller
must also be on the same radio frequency.
3.38. In New Zealand, MSAWs are only enabled for the instrument approaches (control
zones and areas) at nine aerodromes where aircraft are under control of and radar
monitored by air traffic controllers (for example, at Auckland, Wellington and
Christchurch airports).36 MSAWs are not available at other aerodromes where air traffic
control is present (for example, at Napier, Nelson and Dunedin airports). It is also not
available in uncontrolled class G airspace, including Taupō and the area where the
accident occurred.
3.39. An FIO, as part of the Area Flight Information Service for Airways New Zealand, works
within the airways transportation system section. This section includes the national
briefing office, the NOTAM37 office and air traffic services supervision. These facilities
are individually staffed during a normal working day and provide services such as
aircraft flight plan processing, pre-flight planning information, aviation safety notices,
weather information, departure and arrival coordination at busy aerodromes38 and
alerting services. Up to five staff are required during a normal day. At night this
reduces to one person responsible for all the functions. Radio communications for an
FIO are therefore the primary, and in some cases the only, means of supporting a pilot
tuned in to their frequency.
Other relevant CFIT accidents
3.40. On 2 February 2005, Piper PA34 Seneca ZK-FMW was on an instrument approach to
Taupō when it struck Mt Tauhara, 8 km north-east of the aerodrome. The Commission
report described the accident as a CFIT accident and recommended to the CAA that
onboard terrain awareness warning systems be fitted as standard equipment for Civil
Aviation Rules Part 135 – Air Operations – Helicopters and Small Aeroplanes
operators.39 The recommendation followed a similar recommendation made as a result
of the Commission’s investigation into another CFIT accident two months earlier.40
3.41. Both of these earlier accidents occurred in class G uncontrolled airspace. The two
recommendations recognised that the responsibility for terrain awareness in
36 Refer Aeronautical Information Publication New Zealand (AIP) En-route 1.6 Radar Service and Procedures,
paragraph 5.12.15, effective 5 February 2015.
37 NOTAMS, or Notices to Airmen, are safety notices that may affect the conduct of a flight. Examples include
runway work and obstructions at an aerodrome, activation of danger or restricted areas and military exercises.
38 Defined as CAM or Collaborative Arrival Management.
39 Aviation Occurrence Report 05-003 Piper PA34-200T Seneca I , ZK-FMW, controlled flight into terrain, 8 km
north-east of Taupō Aerodrome, 2 February 2005.
40 Report 04-007 Piper PA34-200T Seneca I ZK-JAN, controlled flight into terrain, Mt Taranaki/Egmont, 30
November 2004.
Final Report AO-2019-003
| PAGE 23
uncontrolled class G airspace remained with the pilot. The use of terrain awareness
warning system equipment, like that instal ed in ZK-EAP and if used as intended,
should have prevented these accidents.
Final Report AO-2019-003
| PAGE 24
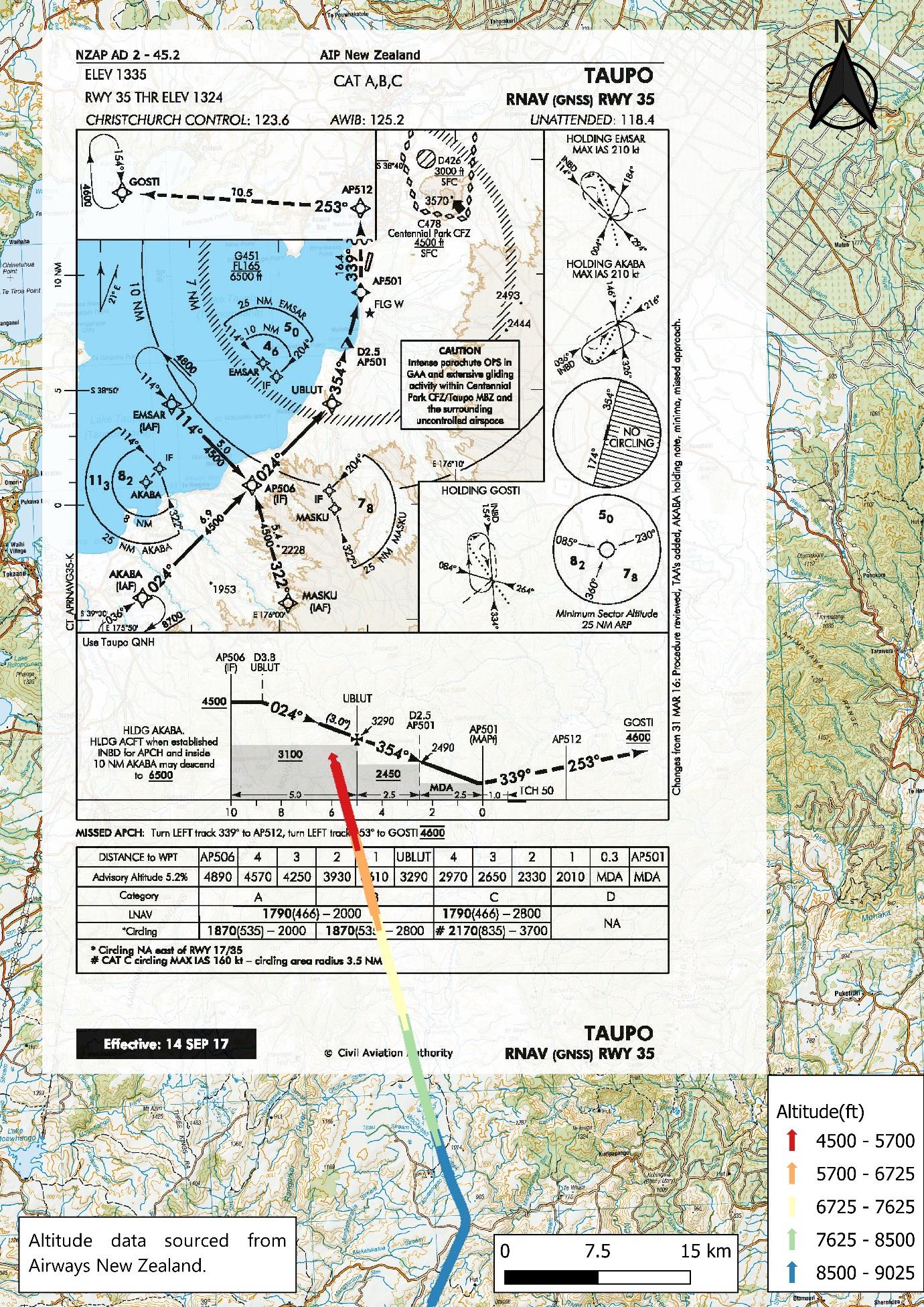
MASKU
flight track
point of
deviation from
planned track
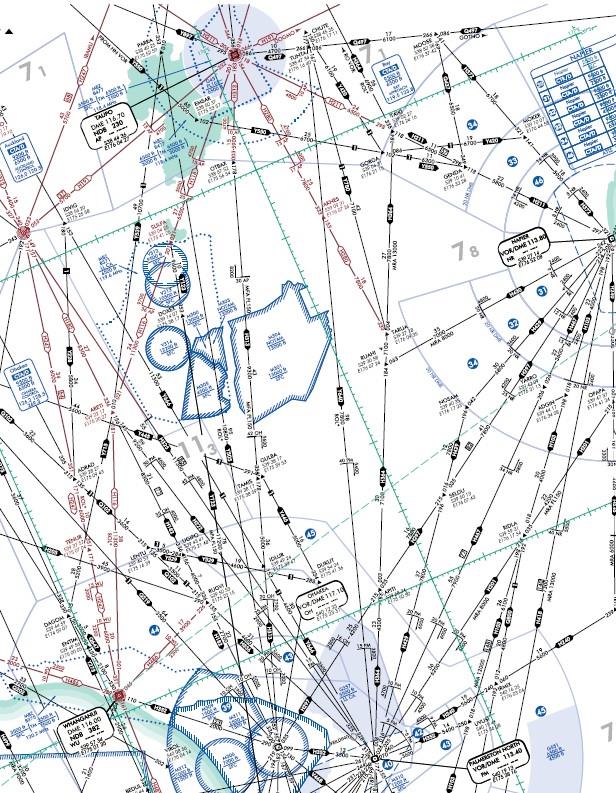
Figure 9: Taupo RWY 35 RNAV Aeronautical Information Publication Approach Plate scaled,
georeferenced and superimposed on LINZ Topo250 map, with surveillance data showing
deviation and track direct to reporting point MASKU
Final Report AO-2019-003
| PAGE 25
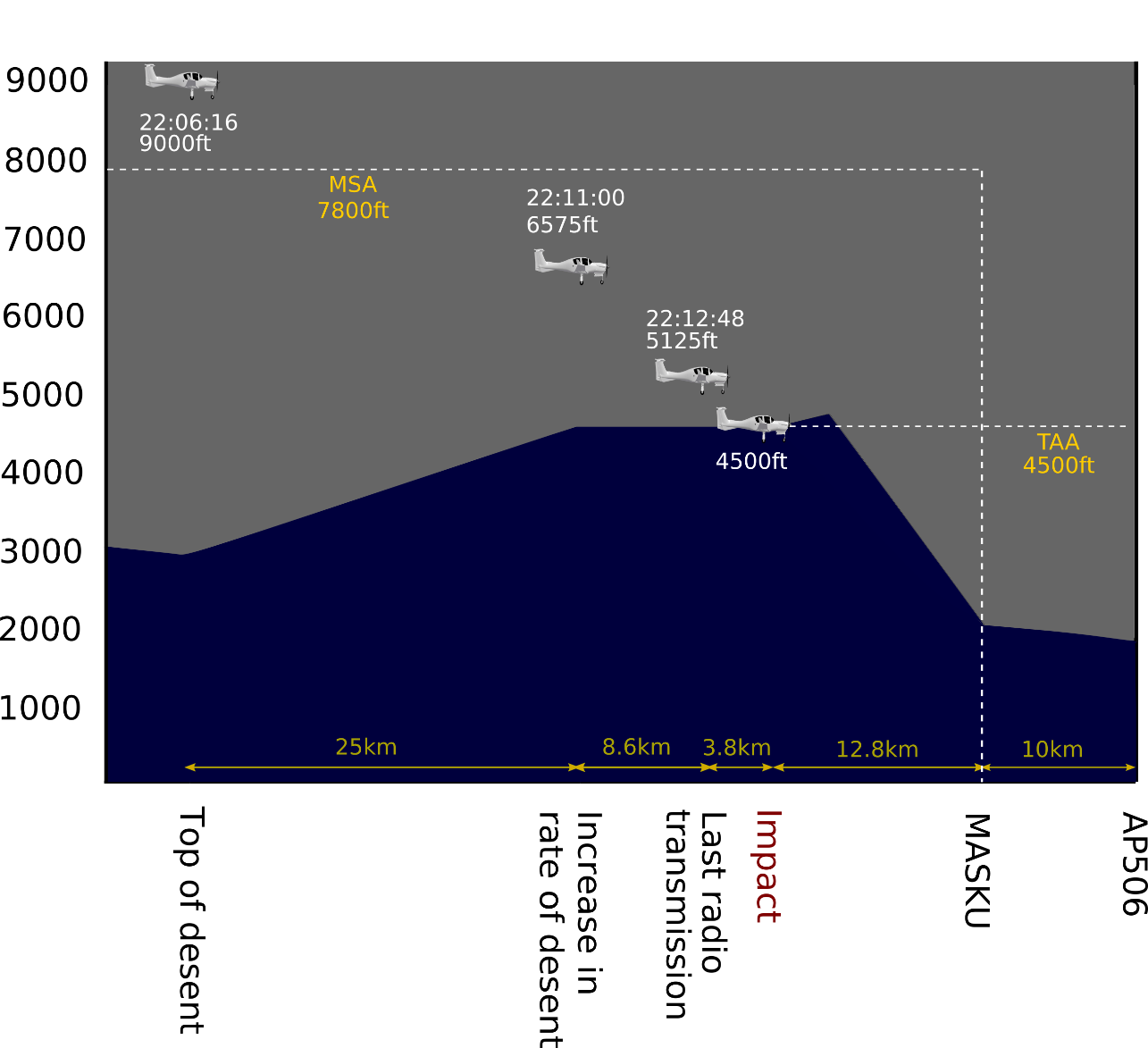
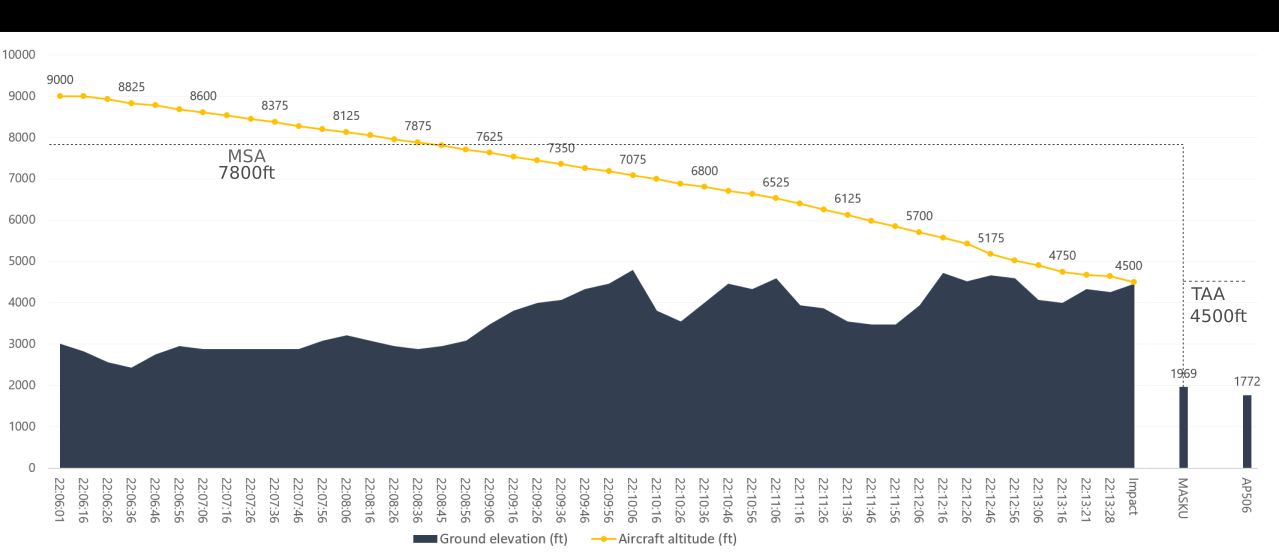 Figure 10: Relationship between flight profile and MSA/terminal arrival altitude
Figure 11: Flight profile from top of descent to ground impact
Figure 10: Relationship between flight profile and MSA/terminal arrival altitude
Figure 11: Flight profile from top of descent to ground impact
Final Report AO-2019-003
| PAGE 26
Safety pilot
3.42. The aeroplane was not equipped with a cockpit voice recorder, and therefore the
actions of the safety pilot could not be confirmed. The responsibilities of a safety pilot
were clearly defined in the operator’s procedures. Had a flight-safety-critical situation
developed it would have been expected that the safety pilot would inform the pilot
and ensure an appropriate response was made.
3.43. The pilot made numerous radio calls after turning at TARUA and after descending
below the 7,800-foot MSA. There was no indication of any concern being raised by
either pilot during these calls. The aeroplane was equipped with a second set of flight
controls, including a second radio-transmit button. This would have allowed the safety
pilot to make a radio call had they wished to do so.
Emergency locator transmitter
3.44. The Commission has investigated previous accidents where ELTs failed to operate as
designed. Following an accident in 2011 the Commission made two recommendations
to the CAA on the matter.41 The issue was also added to the Commissions Watchlist,
under the title ‘Technologies to track and to locate’, and included rail and maritime
transport as well as air.
3.45. On 27 November 2019 the CAA issued advisory circular AC43-11 with the objective of
“encourage[ing] the use of flight tracking devices and provide[ing] guidance on how to
install ‘non-aeronautical’ electronic equipment safely for the purposes of tracking flight
movements”. On 26 March 2021 the CAA advised that tests had been conducted on
the use of a secondary antenna to help ensure geo-orbiting satel ites could receive
emergency signals. However, this had been found to be “suboptimal” as the signal had
become degraded. In the meantime, the CAA “continues to monitor ongoing ICAO
work on Emergency Locator Transmitters and supports improvements wherever
possible”.
41 Inquiry 11-003: Inflight break-up ZK-HMU, Robinson R22, near Mount Aspiring, 27 April 2011.
Final Report AO-2019-003
| PAGE 27
4 Findings
4.1. The aeroplane was descended below the specified minimum safe altitude for the area
in which the aeroplane was being flown, and a controlled flight into terrain occurred.
4.2. The aeroplane was being flown outside the parameters required for direct navigation,
having deviated from the planned track onto an unevaluated route when attempting to
connect with a runway approach.
4.3. ATS was not advised of any changes to the filed and cleared flight plan.
4.4. The change in route was not properly validated by the pilots.
4.5. It was very likely that the aeroplane’s terrain proximity awareness system was either
excessively dimmed or not selected, so the terrain ahead was not displayed during the
descent.
4.6. There was no evidence that any malfunction or unserviceability of the aeroplane
contributed to the accident.
4.7. The pilot and safety pilot were appropriately licensed and qualified for the flight, but
had little experience in night instrument-flight-rules navigation.
4.8. The pilot’s experience and training status required appropriate supervision that should
have been provided by the operator’s flight-authorisation procedures.
4.9. The pilot did not follow the operator’s authorisation procedures.
4.10. The operator’s flight-authorisation procedures were not sufficiently robust to prevent
students and qualified pilots conducting flights without the requisite authorisation
from supervising instructors.
4.11. The added defence of having a safety pilot on board did not prevent the accident.
4.12. The emergency locator transmitter did not function as designed.
Final Report AO-2019-003
| PAGE 28
5 Safety issues and remedial action
General
5.1. Safety issues are an output from the Commission’s analysis. They typically describe a
system problem that has the potential to adversely affect future operations on a wide
scale.
5.2. Safety issues may be addressed by safety actions taken by a participant, otherwise the
Commission may issue a recommendation to address the issue.
Robustness of flight-authorisation procedures
5.3. The operator’s flight-authorisation processes and procedures for IFR flights were not
sufficiently robust to ensure that pilots under training conducted flights with
appropriate flight authorisation and supervision (including separate authorisation
where needed). The operator advised that had the pilot followed the authorisation
procedures as intended, it is likely that the authorising officer would have checked and
challenged the route to be flown and, as likely as not, the flight would not have been
approved as planned.
5.4. The operator has completed an extensive review of its processes and procedures
relating to the management, approval and supervision of training flights, and has
provided evidence to the Commission of the actions taken to eliminate the weaknesses
that were identified in the associated systems. The Commission believes that these
actions are satisfactory in addressing the respective issues.
5.5. The operator has taken the following safety action to address this issue:
• The operator has amended its flight-authorisation processes and procedures.
5.6. In the Commission’s view, this safety action has addressed the safety issue. Therefore,
the Commission has not made a recommendation.
Final Report AO-2019-003
| PAGE 29
6
Recommendations
General 6.1. The Commission issues recommendations to address safety issues found in its
investigations. Recommendations may be addressed to organisations or people and
can relate to safety issues found within an organisation or within the wider transport
system that have the potential to contribute to future transport accidents and
incidents.
6.2. In the interests of transport safety, it is important that recommendations are
implemented without delay to help prevent similar accidents or incidents occurring in
the future.
New recommendations 6.3. No new recommendations were issued.
Final Report AO-2019-003
| PAGE 30
7 Key lessons
7.1. Pilots, especially instructor pilots, should be fully aware of the parameters prescribed
by Civil Aviation Rules, including for navigating away from pre-planned and IFR-
approved flight routes.
7.2. Where possible, pilots should use and be proficient in the full capabilities of the flight
instrumentation systems available to them. In this case, thorough training in the use of
onboard ground-proximity conflict and warning systems, including the dimming of
instrument and cockpit lights at night, would have enhanced situational awareness.
7.3. Pilots should be aware of the consequences of, and the required validation steps
(including altitude distance cross-checks) when making en-route changes to flight
plans, in combination with onboard navigation systems.
7.4. Flight training schools should ensure that their procedures for flight authorisation and
supervision are sufficiently robust to ensure that students can only conduct training
flights after obtaining the appropriate authorisation and supervision.
Final Report AO-2019-003
| PAGE 31
8 Data summary
Aircraft particulars
Aircraft registration:
ZK-EAP
Type and serial number:
Diamond DA42; SN 42.258
Number and type of engines:
two Thielert Centurion 2.0 TAE 125-02-99 diesel
engines
Year of manufacture:
2007
Operator:
Ardmore Flying School
Type of flight:
IFR cross-country training
Persons on board:
two
Crew particulars
Pilot in command
Safety pilot
Pilot’s licence:
commercial pilot
commercial pilot
licence (aeroplane)
licence (aeroplane)
Pilot’s age:
27
29
Pilot’s total flying
823 flight hours
832 flight hours
experience:
(17 on type)
(10 on type)
Date and time
23 March 2019, 2213
Location
Kaimanawa Range, about 38 km south of Taupō
latitude:
39° 6.0´ south
longitude: 176° 2.7´ east
Persons on
two
board
Injuries
two fatal
Damage
aeroplane destroyed
Final Report AO-2019-003
| PAGE 32
9 Conduct of the inquiry
9.1. On 24 March 2019 the Rescue Coordination Centre New Zealand notified the
Commission of the occurrence. The Commission subsequently opened an inquiry
under section 13(1) of the
Transport Accident Investigation Commission Act 1990 and
appointed an investigator in charge.
9.2. On 25 March 2019 Commission investigators travelled to Taupō. They received
briefings from New Zealand Police before continuing to the accident scene to conduct
the site investigation. At the same time a Commission investigator travelled to
Auckland and interviewed the operator’s senior staff and the aeroplane occupants’ next
of kin.
9.3. In accordance with Annex 13 to the Convention on International Civil Aviation, the
Commission notified the state of manufacture of the aircraft and engines, the BFU. On
28 March 2019 the BFU appointed an accredited representative for France and
appointed Technify Motors as its technical adviser.
9.4. On 4 April 2019 the wreckage of the aeroplane was removed from the accident scene
and relocated to the Commission’s secure facility in the Wellington region.
9.5. On 10 May 2019 the two engine-control units from the aeroplane’s FADEC system
were sent to the BFU, where the data was downloaded and analysed.
9.6. On 7 June 2019 the Commission received a copy of the operator’s internal
investigation report.
9.7. On 27 January 2021 the operator provided the Commission with evidence of how it
had addressed the recommendations contained in its internal investigation report.
9.8. Between 26 March and 6 April 2021, the CAA provided an update on activities relating
to the recommendations referred to in paragraphs 3.36 and 3.37, ELT reliability data
following fatal accidents since 2011 and other safety initiatives.
9.9. On 28 April 2021 the Commission approved a draft report for circulation to five
interested persons for their comment. The Commission received three responses, while
the remaining two advised that they had no comments to make. As a result of the
responses, further enquiries were made of Airways New Zealand, the CAA and Air
Services Australia. Changes have been incorporated in this final report as a result.
9.10. On 22 September 2021, the Commission approved the final report for publication.
Final Report AO-2019-003
| PAGE 33
10 Report information
Abbreviations
ATS
Air Traffic Services
BFU
Bundesstelle für Flugunfal untersuchung (the German Federal Bureau
of Aircraft Accident Investigation)
CAA
Civil Aviation Authority (of New Zealand)
CFIT
controlled flight into terrain
ELT
emergency locator transmitter
FADEC
full authority digital engine control
FIO
flight information officer
GPS
global positioning system
GRAFOR
graphical aviation forecast
HoT
head of training
ICAO
International Civil Aviation Organization
IFR
instrument flight rules
km
kilometre(s)
km/h
kilometre(s) per hour
m
metre(s)
MFD
multifunctional display
MSA
minimum safe altitude
RNAV
area navigation
Final Report AO-2019-003
| PAGE 34
Glossary
direct routing
when an aircraft is flown along a route that has not been charted and
has not been evaluated. Sometimes referred to as ‘random routing’
flight information Airways New Zealand provides a flight information service through a
officer
flight information officer, who offers limited assistance for pilots
operating in uncontrol ed airspace. The pilots remain responsible for
terrain-conflict avoidance and separation from other aircraft
instrument flight flight by reference to instruments. The alternative is flight by visual
rules
reference, termed visual flight rules
minimum safe
the lowest altitude which may be used which will provide a minimum
altitude
clearance of 1,000 feet (300 m) above all objects located in the area
contained within a sector of a circle of 46 km (25 nautical miles) radius
centred on a radio aid to navigation (ICAO)
missed approach the phase of an instrument approach when an aircraft overshoots
from the approach and climbs back to a safe altitude
reporting point
sometimes termed waypoints. Reporting points can be compulsory or
non-compulsory
terminal arrival
a terminal arrival altitude provides a transition from an en-route
altitude
structure to an approach procedure
top of descent
when an aircraft transitions from the cruise phase of flight and starts
to descend for the approach
uncontrolled class under ICAO Annex 11 and New Zealand Civil Aviation Rules Part 71 –
G airspace
Designation and Classification of Airspace, airspace is divided into
seven classifications: classes A to G. Class G is uncontrol ed airspace.
Classes B, E and F are not available in New Zealand
Final Report AO-2019-003
| PAGE 35
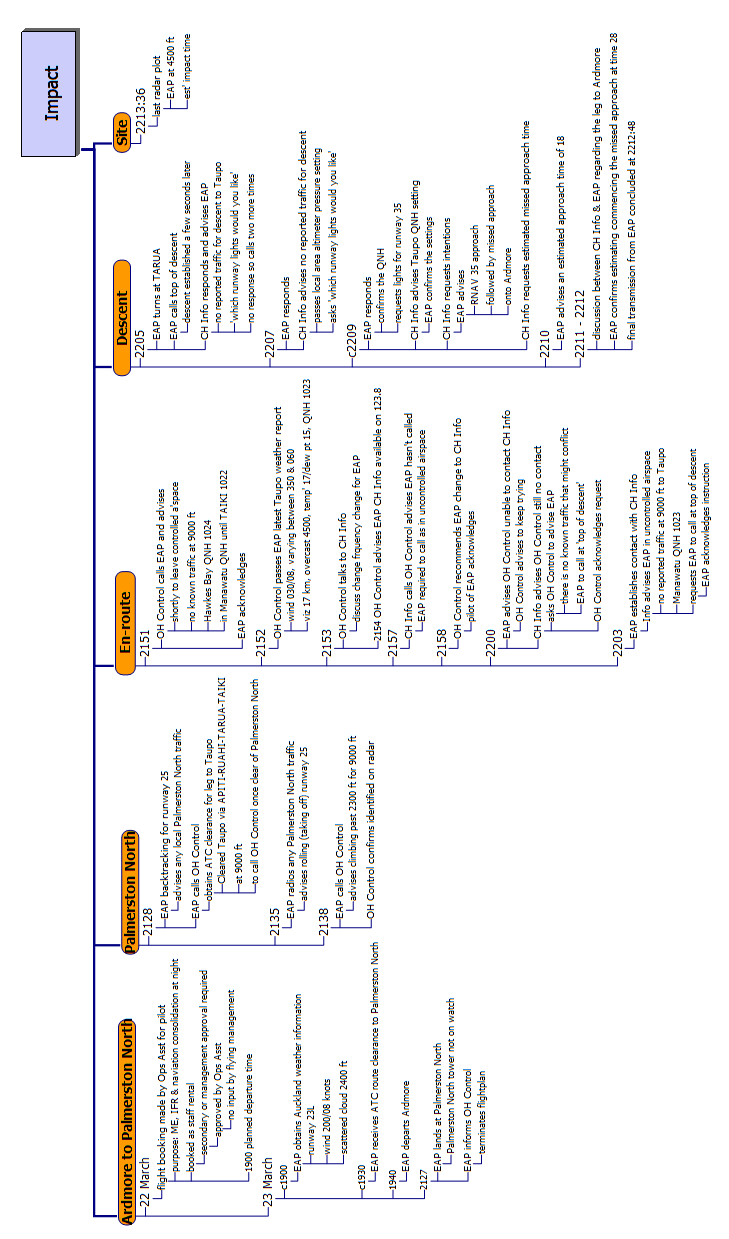
Appendix 1 Timeline
Final Report AO-2019-003
| PAGE 36




TAIC Kōwhaiwhai - Māori scroll designs
TAIC commissioned its kōwhaiwhai, Māori scroll designs, from artist Sandy Rodgers (Ngati Raukawa,
Tuwharetoa, MacDougal). Sandy began from thinking of the Commission as a vehicle or vessel for seeking
knowledge to understand transport accident tragedies and how to prevent them. A ‘waka whai mārama (i te
ara haumaru) is ‘a vessel/vehicle in pursuit of understanding’. Waka is metaphor for the Commission. Mārama
(from ‘te ao mārama’ – the world of light) is for the separation of Rangitāne (Sky Father) and Papatūānuku
(Earth Mother) by their son Tāne Māhuta (god of man, forests and everything dwelling within), which brought
light and thus awareness to the world. ‘Te ara’ is ‘the path’ and ‘haumaru’ is ‘safe or risk free’.
Corporate: Te Ara Haumaru - The safe and risk free path
The eye motif looks to the future, watching the path for obstructions. The encased double koru is the mother
and child, symbolising protection, safety and guidance. The triple koru represents the three kete of
knowledge that Tāne Māhuta collected from the highest of the heavens to pass their wisdom to humanity.
The continual wave is the perpetual line of influence. The succession of humps represent the individual
inquiries.
Sandy acknowledges Tāne Māhuta in the creation of this Kōwhaiwhai.
Aviation: ng
ā hau e wh
ā - the four winds
To Sandy, ‘Ngā hau e whā’ (the four winds), commonly used in Te Reo Māori to refer to people coming
together from across Aotearoa, was also redolent of the aviation environment. The design represents the sky,
cloud, and wind. There is a manu (bird) form representing the aircraft that move through Aotearoa’s ‘long
white cloud’. The letter ‘A’ is present, standing for aviation.
Sandy acknowledges Ranginui (Sky father) and Tāwhirimātea (God of wind) in the creation of this
Kōwhaiwhai.
Marine: ara wai - waterways
The sections of waves flowing across the design represent the many different ‘ara wai’ (waterways) that ships
sail across. The ‘V’ shape is a ship’s prow and its wake. The letter ‘M’ is present, standing for ‘Marine’.
Sandy acknowledges Tangaroa (God of the sea) in the creation of this Kōwhaiwhai.
Rail: rerewhenua - flowing across the land
The design represents the fluid movement of trains across Aotearoa. ‘Rere’ is to flow or fly. ‘Whenua’ is the
land. The koru forms represent the earth, land and flora that trains pass over and through. The letter ‘R’ is
present, standing for ‘Rail’.
Sandy acknowledges Papatūānuku (Earth Mother) and Tāne Mahuta (God of man and forests and everything
that dwells within) in the creation of this Kōwhaiwhai.

Recent Aviation Occurrence Reports published by
the Transport Accident Investigation Commission
(most recent at top of list)
AO-2019-003
Diamond DA42 aeroplane, Impact with terrain, 22 nautical miles south-southeast of
Taupō, Kaimanawa Ranges, 23 March 2019
AO-2018-005
MD Helicopters 600N, ZK-ILD, Engine control malfunction and forced landing,
Ngamatea Station, 14 June 2018
AO-2018-001
Tandem parachute UPT Micro Sigma, registration 31Z, Double malfunction,
Queenstown, 10 January 2018
AO-2017-009 and Commission resolution to close aviation inquiries Boeing 787, near Auckland, New
AO-2017-010
Zealand, 5 and 6 December 2017
AO-2019-001
Airbus Helicopters AS350, ZK-HEX, Forced landing, Wakefield, Nelson, 17 February
2019
AO-2017-004
MBB BK117 A-3 helicopter, ZK-IED, Loss of control, Porirua Harbour, 2 May 2017
AO-2017-002
Robinson Helicopter Company R22, ZK-IHA, Impact with terrain, near Reefton, 27
March 2017
AO-2017-003
ATR72, ZK-MCY, Landing gear failure, Nelson, 9 April 2017
AO-2015-003
Robinson R44, Main rotor blade failure, Waikaia, Southland, 23 January 2015
AO-2015-007
Airbus Helicopters AS350BA, ZK-HKU, Col ision with terrain, Fox Glacier, 21
November 2015
AO-2017-007
Airbus A320 VH-VGY, Descent below clearance limit, Christchurch, 6 August 2017
AO-2016-007
Col ision with terrain, Robinson R44, ZK-HTH, Glenbervie Forest, Northland, 31
October 2016
Interim Report
MDHI (Hughes) 369D, registration ZK-HOJ, Wanaka, 18 October 2018
AO-2018-009
Interim Report
Robinson R44, ZK-HTB, Stevensons Arm, Lake Wanaka, 21 July 2018
AO-2018-006
Price $ 17.00
ISSN 1179-9080 (Print)
ISSN 1179-9099 (Online)
Document Outline