

Document 1
COVID-19 Home Monitoring Program: Timed Position Changes Instructions
Timed Position Changes: You can use the monitor to check your oxygen saturations 15 minutes
after each position change to ensure oxygen saturation has not decreased.
-
Please try to not spend a lot of time lying flat on your back. Lying on your stomach and
1982
in different positions will help your body to get air into all areas of your lungs
-
It is recommended to change your position every 30 minutes to 2 hours rotating as
Act
below. Please note sitting up is better than lying on your back.
-
Continue to monitor oxygen saturations at 8AM and 1PM.
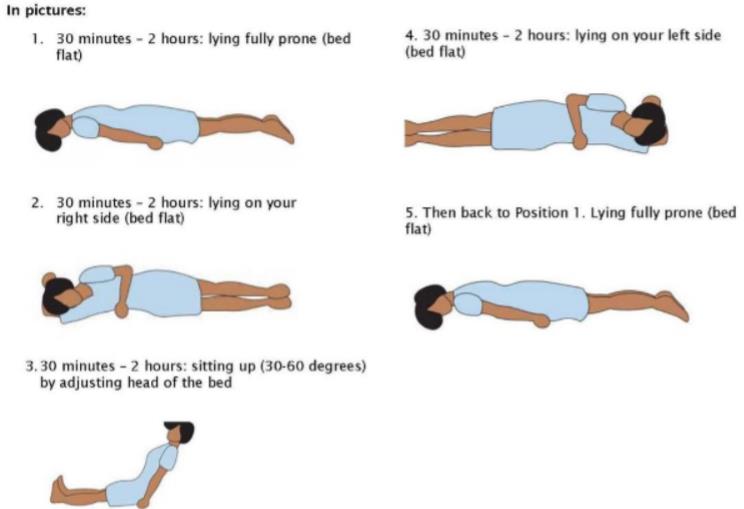
1. 30 minutes to 2 hours lying fully prone (bed flat)
2. 30 minutes to 2 hours lying on right side (bed flat)
3. 30 minutes to 2 hours sitting up (30-60 degrees) by adjusting head of the bed
4. 30 minutes to 2 hours lying on left side (bed flat)
5. 30 minutes to 2 hours lying prone again Information
6. Continue to repeat the cycle…
Official
the
under
Released
*Adopted from Sources: ICS Guidance for Prone Positioning of the Conscious COVID Patien
t 2020. https://emcrit.org/wp-
content/uploads/2020/04/2020-04-12- Guidance-for-conscious-proning.pdf https://www.embeds.co.uk/wp-
content/uploads/2020/04/Self-Proning-Positioning-leaflet.pdf
Document 2
Timeline of COVID-19 Symptoms:
Early symptoms of COVID-19 vary widely. It can start with a tickle in your throat, a cough, fever, headache
and feeling a bit ‘chesty’.
Day 5-10 of COVID-19 are often the most worrisome time for respiratory (lung) complications, particularly
for older patients and those with underlying conditions like high blood pressure, obesity or diabetes.
Days 1 – 3
•
Sometimes it begins with a bout of diarrhoea
•
Some people just feel tired and lose their sense of taste and smell
•
Many people have several symptoms but no fever
•
Some patients with gastrointestinal symptoms go on to develop respiratory symptoms,
Days 4 – 6
1982
•
Some patients never develop more than mild symptoms, or none at all
•
Others begin to feel terrible, with an ever-present fever, aches, chills, cough and an inability to get
Act
comfortable
•
Some younger patients with mild disease may develop rashes, including itchy red patches, swelling
or blistering on the toes or fingers, similar to frostbite
Days 7 – 8
•
For patients with mild illness, the worst is over after a week.
•
Patients who have felt terrible may get worse. And some patients might start to feel better briefly
then take a turn for the worse
Information
•
Patients with home oxygen monitors should monitor their oxygen levels at least 3 times per day
and check in with a doctor if they start to feel more unwell.
•
Monitoring should continue for the second week of illness. Patients may feel better sleeping on
their stomachs or sides
Day 8 – 12
Official
•
Monitor for worsening symptoms including increasing shortness of breath, worsening cough
the
•
If you have a home oxygen monitor continue to use it at least 3 times per day.
Days 13 – 14
•
Patients who had mild illness should be well recovered
under
•
Patients who had worse symptoms, but maintained normal oxygen levels, should feel mostly
recovered after two weeks, although many patients report lingering fatigue
•
Doctors advise a slow return to activity, even if you had mild or moderate illness
•
Patients with severe symptoms and those who needed additional treatment because of low oxygen
levels, may still feel unwell and fatigued and take far longer to recover .
* Information sourced from
: https://www.nytimes.com/2020/04/30/well/live/coronavirus-days-5-through-
Released
10.html
Adapted from United against Covid-19 (covid19.govt.nz) and Sydney Local Health District RPA Virtual
Hospital. Adapted from hfam.ca pathways with permission from Dee Mangin (McMaster University,
University of Otago)
Shared goals of care plan
Family Name:
Document 3
Given
Name:
Gender:
AFFIX PATIENT LABEL HERE
Date of Birth:
NHI#:
Discuss the goal of care for this admission with the person, family, whānau or other (as appropriate).
Outline which treatments are more likely to cause benefit than harm during this admission.
Select the agreed goal of care and document your discussion.
A The goal of care is
curative or
restorative.
Treatment aims to prolong life.
Attempt CPR: it is clinically recommended and in accordance with the person’s known wishes.
Also for referral for ICU level care, 777 calls and all appropriate life sustaining treatments.
Additional comments:
Attempt CPR
1982
B The goal of care is
curative or
restorative.
Act
Treatment aims to prolong life and enhance its quality.
Do not attempt CPR: this is likely to cause more harm than benefit or is not desired by the person.
Referral for ICU level care is appropriate Yes No
777 calls are appropriate.
Additional comments (e.g. non-invasive ventilation, dialysis):
Information
C The goal of care is primarily
improving quality of life.
Treatment aims to control symptoms, enhance wellbeing and should be easily tolerated.
Official
Do not attempt CPR: this is likely to cause more harm than benefit.
Referral for ICU level care is unlikely to be appropriate.
the
777 calls are appropriate Yes No
Additional comments (e.g. antibiotics, IV fluids, NG feeding):
under
Do not attempt CPR
D The goal of care is
comfort whilst dying.
Treatment aims to alleviate suffering in the last hours or days of life and allow a natural death.
SHARED GOALS OF CARE PLAN—TEST FORM
Consider end of life guidelines such as Te Ara Whakapiri.
Released
Do not attempt CPR, refer for ICU level of care or make 777 calls.
Additional comments (e.g. pain management, fluids):
This plan has been discussed with the person. If not, record reason overleaf.
Name: Date: / /
Time:
Designation: Signature:
SMO informed, name:
This plan is not valid unless signed and dated. Clinically review the person if there are concerns or a change
in their condition. Any change to the goal of care requires a new plan and the earlier plan crossed out.
Include a copy of this plan with discharge information.
Side 1 of 2
HQSC test SGOC form v16 March 2020
Shared goals of care plan
Family Name:
Document 3
Given
Name:
Gender:
Use this side first to guide the conversation
AFFIX PATIENT LABEL HERE
and record key points.
Date of Birth:
NHI#:
Consider the person’s capacity, their privacy, support people, cultural needs and medical trajectory.
Do they have an:
• Advance Care Plan and/or Advance Health Directive?
Yes No
Unknown
• Enduring Power of Attorney (EPoA) or legally appointed guardian?
Yes No
Unknown
If yes, circle either EPoA or legal guardian and record their full name:
Prepare Seek agreement with the person to have the conversation, with the people they want present.
Full name(s), relationship(s) and role(s) of those present:
1982
Act
Ask about their understanding of their current condition and what may lie ahead.
Ask how much information they would want to know.
Share your understanding of their current condition and what may lie ahead.
Explore their values and what is important — their priorities, hopes, worries, what helps in tough times
and what they would be willing to go through for more time: Information
Discuss
Official
the
Summarise and check for shared understanding.
under
Explain your recommendation in plain language.
Reach a decision and document the goal of care overleaf.
Additional comments:
Released
Further information in clinical record.
If conversation not held with person, record reason below:
Recommend and close
Document follow-up plan in the clinical record.
Side 2 of 2
HQSC test SGOC form v16 March 2020
Document Outline