link to page 2 link to page 2 link to page 2 link to page 2
Br J Sports Med: first published as 10.1136/bjsports-2019-100950 on 12 July 2019. Downloaded from
Infographics
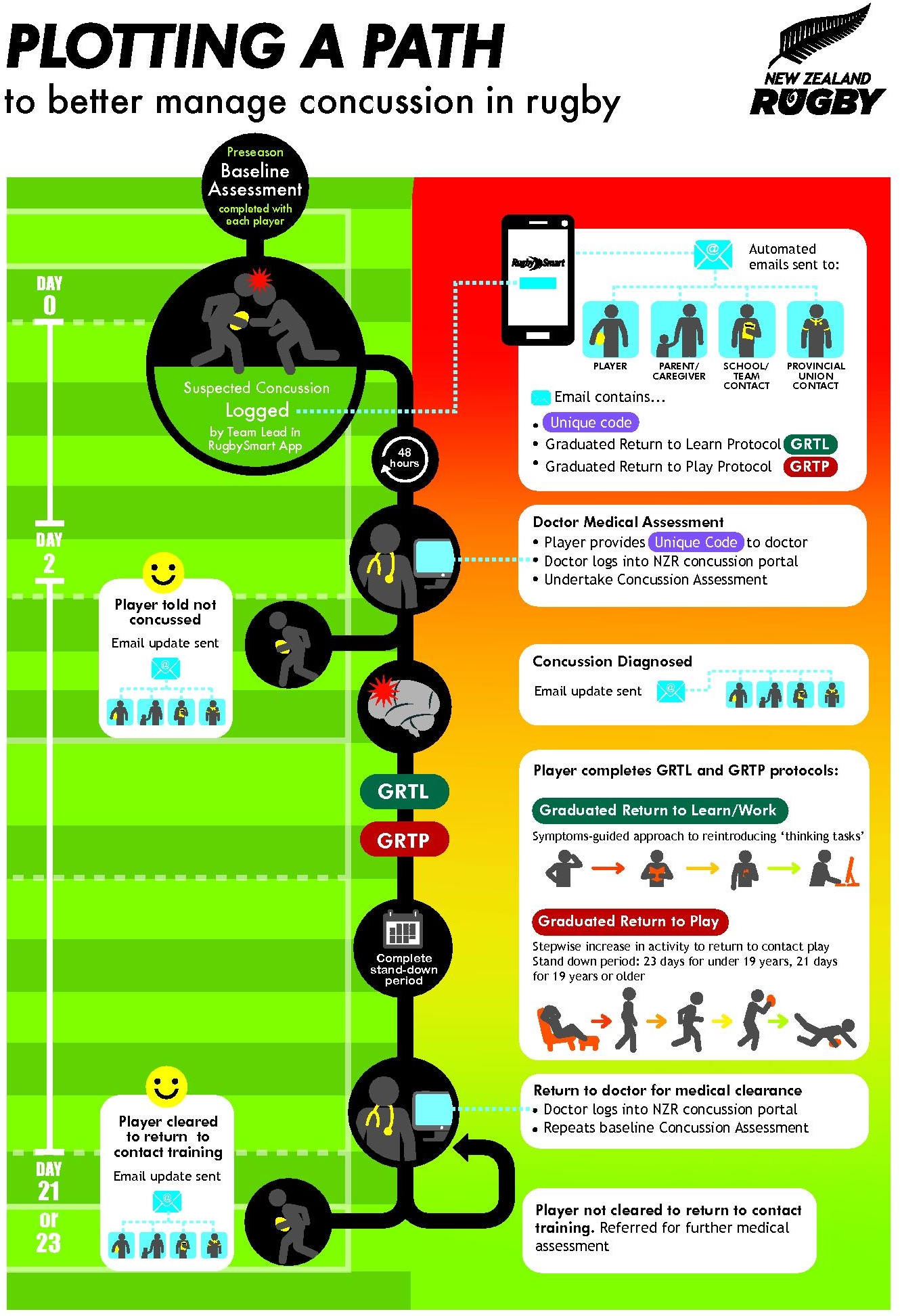
Infographic. New Zealand Rugby’s concussion
management pathway
Danielle Salmon, 1 Janelle Romanchuk,1 Ian Murphy,1 John Sullivan,
2 Simon Walters,3 Chris Whatman,3
Amanda Clacy,4 Sierra Keung,3 Klazina Van Der Vis5
Application (App) and a web-based
1982
Concussion Portal for medical practi-
tioners. The App allows the team lead (eg,
physiotherapist, manager and parent) to
complete the modified child SCAT5
ACT
baseline assessment during preseason
and then log suspected concussions in
the App as they occur during training
or match play. The Concussion Portal
allows medical practitioners to view
players’ baseline scores, provides guid-
ance for diagnosis and medical clearance,
and contains NZR regulations pertaining
to concussion recognition, management,
and graduated return to play (RTP) and
graduated return to learn guidelines.
The NZR CMP includes the following
steps: (1) initial player concussion base-
line testing performed using the App;
INFORMATION
(2) logging of a suspected concussion on
the App; (3) App generated automated
concussion email notifications that are
sent to the player, their parents/care-
givers, coaches, school/club and provin-
cial union; (4) the notifications sent to
the player and parents/caregivers contain
http://bjsm.bmj.com/
a unique identifier code that will enable
OFFICIAL the doctor to access that player’s baseline
concussion score through the Concus-
sion Portal; (5) clinical concussion diag-
nosis made by the medical doctor; (6)
email notifications sent out to identified
THE
stakeholders; (7) appropriate RTP and
on 7 August 2019 at University of Otago. Protected by copyright.
medical clearance and (8) notifications
that the player has been medically cleared
sent to identified stakeholders. The NZR
CMP has undergone extensive pilot
work and consultation with the wider
rugby community and is currently being
UNDER
trialled in several regions throughout NZ
prior to the planned national rollout. The
strength of the CMP is that it not only
facilitates concussion recognition, diag-
nosis and management but also involves
Concussions in rugby union (rugby) presents a challenge.
4 5 To address this a network of community rugby stake-
impact not only player welfare but challenge, New Zealand Rugby (NZR)
holders.5 The purpose of the CMP is to
parental and players’ decisions around as part of a National Concussion Initia-
close the loop between suspected concus-
participation, a concern for rugby tive (infographic 1) developed a concus-
sion recognition and RTP following
administrators around the world.
1 2 To sion management pathway (CMP) that medical clearance through the use of
RELEASED
ensure player welfare, World Rugby considers the various stakeholders technology to provide information to the
has developed concussion manage-
involved in the management of concus-
relevant stakeholders at the appropriate
ment recommendations (http://
player-
sion as well as ways to support improved time points to ensure player welfare.
welfare. worldrugby. org/ concussion)3; concussion management at the commu-
however, the practical application and nity level. The NZR CMP includes 1Health, Safety and Welfare, New Zealand Rugby Union,
enforcement of these recommendations a Concussion Management Phone Wellington, New Zealand
Salmon D, et al. Br J Sports Med Month 2019 Vol 0 No 0
1
Br J Sports Med: first published as 10.1136/bjsports-2019-100950 on 12 July 2019. Downloaded from
Infographics
2Centre for Health, Activity and Rehabilitation Research,
Funding The authors have not declared a specific
RefeRences
School of Physiotherapy, University of Otago, Dunedin,
grant for this research from any funding agency in the
1 Roberts SP, Trewartha G, England M, et al. Concussions
New Zealand
public, commercial or not-for-profit sectors.
and head injuries in English community rugby union
3Sports Performance Research Institute New Zealand,
Competing interests None declared.
match play.
Am J Sports Med 2017;45:480–7.
School of Sport and Recreation, Auckland University of
2 Murphy AM, Askew KL, Sumner KE. Parents’ intentions
Technology, Auckland, New Zealand
Patient consent for publication Not required.
4
to allow youth football participation: Perceived
Sunshine Coast Mind and Neuroscience – Thompson
Provenance and peer review Not commissioned;
concussion risk and the theory of planned behavior.
Institute, University of the Sunshine Coast, Birtinya,
externally peer reviewed.
Sport Exerc Perform Psychol 2017;6:230–42.
Queensland, Australia
5School of Medicine, University of Otago Medical
© Author(s) (or their employer(s)) 2019. No
3 Patricios JS, Ardern CL, Hislop MD, et al. Implementation
School, Dunedin, New Zealand
commercial re-use. See rights and permissions.
of The 2017 Berlin concussion in sport group consensus
Published by BMJ.
statement in contact and collision sports: a joint
Correspondence to Dr Danielle Salmon, New
position statement from 11 national and international 1982
Zealand Rugby Union, Wellington, New Zealand;
sports organisations.
Br J Sports Med 2018;52:635–41.
danielle. salmon@ otago. ac. nz
4 Register-Mihalik JK, Williams RM, Marshall SW, et al.
Contributors DS, JR and KVDV made substantial
To cite Salmon D, Romanchuk J, Murphy I, et al.
Demographic, parental, and personal factors and youth
contributions to the concept and design of the
Br J Sports Med Epub ahead of print: [please include
athletes’ concussion-related knowledge and beliefs.
J
ACT
infographic. All the authors were involved in revising
Day Month Year]. doi:10.1136/bjsports-2019-100950
Athl Train 2018;53:768–75.
and critical analysis of the infographic. DS, AC and JS
5 Clacy A, Goode N, Sharman R, et al. A systems approach
made substantial contributions to the initial draft of
Accepted 23 May 2019
to understanding the identification and treatment of
the supporting text. All the authors were involved in
Br J Sports Med 2019;
0:1–2.
sport-related concussion in community rugby union.
revising and critical analysis of the supporting text.
doi:10.1136/bjsports-2019-100950
Appl Ergon 2017;4:1–9.
INFORMATION
http://bjsm.bmj.com/
OFFICIAL
THE
on 7 August 2019 at University of Otago. Protected by copyright.
UNDER
RELEASED
2
Salmon D, et al. Br J Sports Med Month 2019 Vol 0 No 0
Original Research
Less Than Half of Patients Recover Within 2 Weeks
of Injury After a Sports-Related Mild Traumatic
Brain Injury: A 2-Year Prospective Study
Stephen Kara, MBChB, FRNZCGP, Dip Sports Med, MPhil (Hons),* Hannah Crosswell, BSc, MSc,*
1982
Katherine Forch, BHSc (Physiotherapy),* Alana Cavadino, BSc, MSc, PhD,† Josh McGeown, HBK, MSc,‡ and
03/23/2020
on
BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3ojN+4MJbriNzhpsNTPKy6B4ps2slyF0fYKzRAtBDkshm9jV7+pC/JQ==
by
https://journals.lww.com/cjsportsmed
from
Downloaded
Mark Fulcher, MBChB, FACSEP, MMedSci*
Downloaded
ACT
from
Abstract
https://journals.lww.com/cjsportsmed
Objective: To describe clinical recovery time and factors that might impact on recovery after a sports-related mild traumatic brain
injury (SR-mTBI; concussion). Design: Prospective cohort study (level IV evidence). Setting: New Zealand Sports Concussion Clinic.
Participants: Eight hundred twenty-two patients presenting within 14 days of a SR-mTBI/concussion over a 2-year period. Main
Outcome Measures: Clinical recovery measured as number of days after injury. Interventions Methods: Participants were
assessed and managed using a standardized protocol consisting of relative rest followed by controlled cognitive and physical loading. A
reassessment was performed 14 days after injury with initiation of an active rehabilitation program consisting of a subsymptom threshold
by
BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3ojN+4MJbriNzhpsNTPKy6B4ps2slyF0fYKzRAtBDkshm9jV7+pC/JQ==
exercise program 6 cervicovestibular rehabilitation (if required) for participants who remained symptomatic. Participants were then
assessed every 2 weeks until clinical recovery. Results: A total of 594 participants were eligible for analysis (mean age 20.2 6 8.7 years,
77% males) and were grouped into 3 age cohorts: children (#12 years), adolescents (13-18 years), and adults ($19 years). Forty-five
percent of participants showed clinical recovery within 14 days of injury, 77% by 4 weeks after injury, and 96% by 8 weeks after injury.
There was no significant difference in recovery time between age groups. Prolonged recovery was more common in females (P 5 0.001),
INFORMATION
participants with “concussion modifiers” (P 5 0.001), and with increased time between injury and the initial appointment (P 5 0.003).
Conclusions: This study challenges current perceptions that most people with a SR-mTBI (concussion) recover within 10 to 14 days
and that age is a determinant of recovery rate. Active rehabilitation results in high recovery rates after SR-mTBI.
Key Words: sports-related concussion, sports-related mTBI, recovery, rehabilitation
(Clin J Sport Med 2020;30:96–101)
INTRODUCTION
At the conclusion of each meeting, an international consensus
OFFICIAL
statement is produced and published. This document is an
Since 2001, the concussion in sport group (CISG) has met
important guide for clinicians and has been integrated into this
regularly to debate and define best practice relating to the
study.
assessment and management of sport-related concussion (SRC).1
Until recently, CISG statements have stressed the importance
THE
Submitted for publication May 31, 2019; accepted November 15, 2019.
of cognitive and physical rest until symptom resolution, widely
From the *Axis Sports Medicine Specialists, Auckland, New Zealand; †Section of
reported to occur in most people within 7 to 10 days.2–4 The
Epidemiology and Biostatistics, School of Population Health, University of Auckland,
most recent consensus statement reported the marked change in
Auckland, New Zealand; and ‡Sports Performance Research Institute New Zealand
direction that SRC management had taken in the intervening 4
(SPRINZ), Faculty of Health and Environmental Science, Auckland University of
years.5 It highlighted the limited evidence to support rest and
Technology, Auckland, New Zealand.
recommended that this was kept to a brief period of 24 to 48
The clinic was supported by funding from the Accident Compensation Corporation
(ACC), NZ. The content is solely the responsibility of the authors and does not
hours. After this period, patients are encouraged to become more
UNDER
on
03/23/2020
necessarily represent the official views of ACC, NZ.
active with potential treatment options including subsymptom
One of the authors (M. Fulcher) works for New Zealand Football and is a member of
threshold exercise (SSTE) programs, vestibular and cervical
the FIFA Medical Committee. The remaining authors report no conflicts of interest.
therapies, and targeted cognitive behavioral therapy approaches.
According to the definition given by the International Committee of Medical Journal Editors
Adoption of active management strategies for patients with
(ICMJE), the authors listed above qualify for authorship based on making one or more of the
a SRC has been internationally accepted,6,7 with trials confirm-
substantial contributions to the intellectual content of (1) conception and design (S. Kara
and M. Fulcher), (2) acquisition of data (S. Kara, H. Crosswell, and K. Forch), (3) analysis and
ing the safety of such interventions.8,9 A recent systematic
interpretation of data (S. Kara and A. Cavadino), (4) participated in drafting of the manuscript
review10 reporting on the approach to treatment and manage-
(S. Kara),and/or (5) critical revision of the manuscript for important intellectual content
ment of persistent postconcussive symptoms found only 25
(S. Kara; H. Crosswel , K. Forch, A. Cavadino, J. McGeown, and M. Fulcher).
studies for inclusion, highlighting the relatively limited data
Corresponding Author: Stephen Kara, Axis Sports Medicine Clinic, 71 Merton Rd,
available. This review included only 3 RCTs, whereas the
RELEASED
St. Johns, Auckland 1072, New Zealand
([email address]).
remainder were level IV evidence cross-sectional studies,
Supplemental digital content is available for this article. Direct URL citations appear
in the printed text and are provided in the HTML and PDF versions of this article on
historical cohorts, and case series ranging from 6 to 128 patients.
the journal’s Web site
(www.cjsportmed.com).
The consensus statements have widely reported that 80% to
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
90% of patients show symptom resolution over a short time
http://dx.doi.org/10.1097/JSM.0000000000000811
period of 7 to 10 days and that children and adolescents may
S. Kara et al. (2020)
Clin J Sport Med
Copyright © 2020 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
Volume 30·Number 2·March 2020
www.cjsportmed.com
require longer recovery periods.3,4 The evidence for both of these
Zealand. Participants attending the clinic were seen by a sports
assertions is limited to referencing an earlier consensus statement
medicine doctor, exercise physiologist, and a physiotherapist
that states simple concussions are the most common form of
with postgraduate vestibular therapy qualifications.
injury and resolve without complication within 7 to 10 days, with
no data or references given in support.2 Despite this lack of
evidence, these figures continue to be quoted even in recent
Patient and Public Involvement
guidelines.11,12 Estimated recovery times, especially for adults,
Patients and public were not involved in any way in our work.
remain vague even in the most recent consensus statement, which
states “it is reasonable to conclude that the large majority of
1982
injured athletes recover, from a clinical perspective, within the first
Definition
month after injury.” The reliance upon a clinical assessment, and
Sports-related mTBI is defined as a traumatic brain injury in
in particular a patient’s reported symptoms, as a measure of
line with the latest CISG consensus statements.5
recovery does have some limitations. For example, it is well
ACT
known that symptom report is not an effective proxy for
concussion diagnosis or treatment. Asymptomatic individuals can
Participants and Recruitment
have impairments, whereas those who have impairments may
Participants consisted of all people who presented between
report no symptoms.13 In the absence of a gold standard test for
January 2017 and December 2018 with a possible SR-mTBI.
SRC however, current diagnostic criteria rely heavily on these
Participants were either referred by general practitioners,
clinical findings. Given that there is increasing concern about the
physiotherapists, other allied health professionals, school
impact that SRC may have, we need to be clear about recovery
nurses, local and public hospital emergency clinics, team
times and the impact possible treatment options have on this.
coaches and sports clubs, or could self-refer. Exclusion criteria
Although the CISG have endorsed the label SRC, the Center
were people presenting after 14 days after injury and those
for Disease Control and Prevention has recently suggested that
with a non–SR-mTBI, the latter due to external public funding
SRC may be better termed as SR mild traumatic brain injury
restrictions. Analysis was limited to participants who achieved
(SR-mTBI)14 due to the belief that this better reflects the
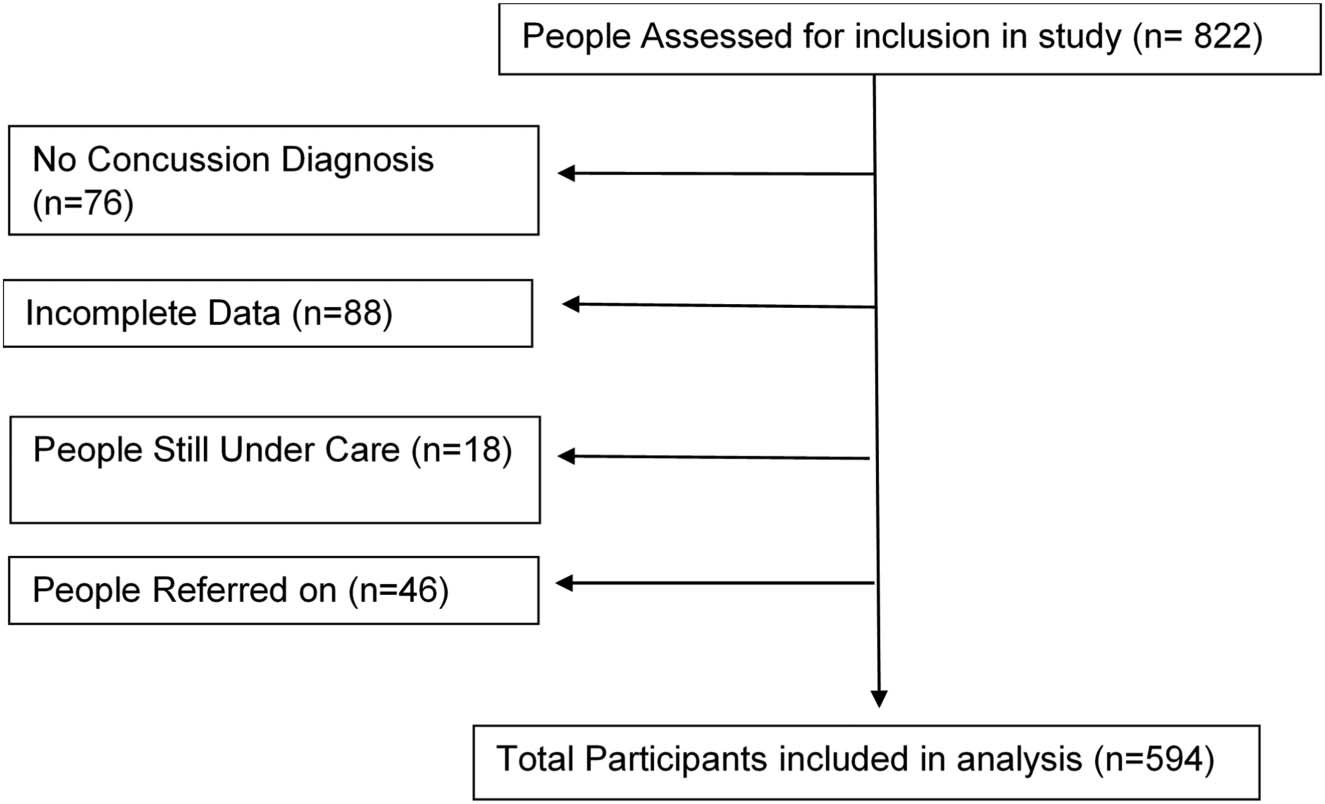
clinical recovery as defined below. Participants excluded from
potential impact of the condition. As a result, the term SR-
analysis (Figure 1) were those not diagnosed with a SR-mTBI
mTBI will be used in this article.
during their initial assessment, those who had incomplete
INFORMATION
This prospective cohort, from a single community-based
clinical data despite being clinically recovered, those who had
sports concussion clinic, will report outcomes on nearly 600
not yet completed 8 weeks of the model of care (and therefore
patients seen over a 2 year period, with the aim of quantifying
remained under care), or those referred on as requiring more
the length of clinical recovery and identifying factors that may
multidisciplinary care due to persistent symptoms 8 weeks
be associated with slower recovery. All patients followed
after injury (eg, occupational therapist, psychologist, and
a standardized assessment and an active rehabilitation
neuropsychologist). Ethical approval was obtained via the
protocol in line with current best practice methods.
Accident Compensation Corporation New Zealand Ethics
Committee. Informed consent and/or age appropriate assent
OFFICIAL
was obtained from each participant.
METHODS
Design and Setting
Assessment Protocol
A 2-year prospective observational cohort study (level of
Participants followed a standardized assessment and manage-
THE
evidence IV) was conducted in a dedicated fully funded
ment protocol in line with the latest CISG Statement.5 The
community–based sports concussion clinic in Auckland, New
initial consultation involved an injury history, previous
UNDER
RELEASED
Figure 1. Participant flow within the study.
97
Copyright © 2020 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
S. Kara et al. (2020)
Clin J Sport Med
SR-mTBI history, and an assessment of any “concussion
participant reached clinical recovery. As participants were
modifiers” (patient-reported preinjury history of migraine or
assessed once every 2 weeks, this figure permits accuracy for
mental health issues).5 An age-appropriate SCAT5 assessment
the time intervals measured against (within 2 weeks; 2-4
was performed. Physical examination to screen for more
weeks; 4-8 weeks; and $8 weeks).
serious pathology such as occult intracranial pathology and
cervical spine instability was performed. This involved
Statistical Analysis
a cranial nerve assessment (I-XII) and a targeted peripheral
neurological assessment of reflexes and motor and sensory
Participant characteristics were assessed for differences
function if dictated by patient presentation. A vestibular
according to age groups: children (#12 years), adolescents 1982
assessment via the vestibulo-oculomotor screening tool was
(13-18 years), and adults ($19 years). A Kruskal–Wallis test
conducted.15,16 The cervical spine was assessed using active
was used for continuous variables due to their skewed
range of movement with flexion, extension, and lateral
distributions, including days until initial appointment, num-
rotation. Additional tests assessed cervical alignment to assess
ber of previous concussions, days until asymptomatic, and
ACT
cervical joint position error, assessing the patient’s ability to
number of follow-up visits. A x2 test was used to assess
relocate their head to a neutral position with less than 5
potential differences in gender, sport type, and concussion
degrees of error, whereas the cervical flexion head rotation test
modifier by the age group. Length of recovery (measured by
assessed upper cervical movement.17,18 Palpation of the
time to clinical recovery; within 2, 2-4, 4-8, or $8 weeks) was
cervical spine for tenderness with trigger point reproduction
summarized overall and within each age group. Multiple
of headache symptoms completed the cervical spine assess-
linear regression was used to determine mutually adjusted
ment. Autonomic dysfunction was assessed using only supine
associations of participant characteristics with length of
and standing blood pressure measurements at 1 and 3
recovery, measured by the number of days to clinical recovery.
minutes. Follow-up consultations involved repeating the
A natural log transformation was used for the outcome due to
SCAT5 symptom evaluation and a review of previous
a skewed distribution, with the model including all factors that
abnormal physical findings.
showed an unadjusted association with the outcome. Because
the outcome is log-transformed, we calculated the average
percentage differences in the length of recovery for each
Management Protocol
variable in the model using the exponential of the regression
INFORMATION
After their initial consult, participants were given written and
coefficients.22 Statistical analyses were conducted using Stata
verbal advice consistent with the latest CISG statement.5 A 24-
version 15.1.
to 48-hour period of rest followed by controlled cognitive and
physical loading, guided by symptom exacerbation, was
prescribed to encourage activity, with emphasis on patient
RESULTS
education at this initial consult. Participants were re-assessed
All 822 participants presenting with a possible SR-mTBI
at day 14 after injury. At this stage, they were defined as being
during the study period from January 2017 to December
“clinically recovered” or “still symptomatic.” If a participant
2018 were assessed for inclusion in this study. A total of 594
OFFICIAL
was deemed to have clinically recovered, they commenced
(77% males) with age range 7 to 64 years (average age 20.2
a graduated return to a sport (GRTS) program with re-
years) were included in the analysis as presented in Table 1.
evaluation before return to full training.5 Those who were
Figure 1 shows that 28% of people presenting were not
“still symptomatic” underwent graded aerobic exercise testing
eligible for inclusion, with 39% (n 5 88) of these being
using the Buffalo Concussion Treadmill Test with subsequent
ineligible due to incomplete or missing information in
THE
development of a SSTE program.7,19 Adjunct cervical or
relevant data fields rather than loss to follow-up. Five
vestibular physiotherapy was prescribed if appropriate based
percent of participants were referred on as they did not
on relevant clinical signs either at this reassessment or at the
achieve clinical recovery under this model of care and were
initial consultation.20 Participants were assessed once every 2
assessed as requiring additional input. Those not included in
weeks until clinical recovery. At this point, they commenced
the analysis due to incomplete data (n 5 88) did not differ
the same GRTS protocol. This standardized model of care and
significantly from those eligible in terms of any of the
rehabilitation is outlined in Appendix 1 (see Supplemental
characteristics described in Table 1.
UNDER
Digital Content 1,
http://links.lww.com/JSM/A219).
The average number of days until the initial consultation
was 8.7 days after injury, whilst Rugby Union accounted for
54% of the all consultations. The #12 years age group had
Definition of Clinical Recovery
a significantly lower proportion of females (P 5 0.008) than
Participants were defined as achieving clinical recovery when
the older age groups. There was also an association between
both their SCAT5 symptom score and symptom severity score
age group and the number of previous concussions, with older
were ,5 for males and ,6 for females. This distinction is
participants having had more previous concussions (P 5
based on normative data for the general population.21
0.0001). There were no statistically significant differences by
Participants were also required to have resolution of any
the age group in terms of days until initial assessment, days
previous abnormal clinical examination findings and “nor-
until clinical recovery, number of follow-up visits, sport type,
RELEASED
mal” exercise tolerance. Normal exercise tolerance was
or presence of a concussion modifier (P . 0.05 for all
defined as being asymptomatic when exercising at 85% to
comparisons). Only 45% of participants across all age groups
90% of predicted heart rate if measured or return to the
had clinical recovery within 2 weeks after injury, increasing to
participants’ usual preinjury exercise levels. Length of re-
77% by 4 weeks, and 94% by 8 weeks (Table 2). All
covery was a reported measure by participant recall defined as
participants included in the analysis achieved clinical recovery
the number of days between injury and the time the
within the study period.
98
Copyright © 2020 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
Volume 30·Number 2·March 2020
www.cjsportmed.com
TABLE 1. Descriptive Summary of Eligible Participants by the Age Group
Age £12 years (n 5 45)
Age 13-18 years (n 5 290)
Age ‡19 years (n 5 259)
All (n 5 594)
Mean 6 SD
Mean 6 SD
Mean 6 SD
Mean 6 SD
Age (yr)
10.7 6 1.4
15.8 6 1.6
26.8 6 9.0
20.2 6 8.5
Days until initial assessment
8.4 6 4.5
8.2 6 4.9
9.2 6 7.1
8.7 6 6.0
No. of previous concussions
0.4 6 0.9
0.7 6 1.1
1.2 6 1.8
0.9 6 1.5
Days until asymptomatic
16.2 6 14.6
18.3 6 13.3
21.6 6 22.3
19.5 6 18.0
1982
No. of follow-up visits
1.7 6 1.1
1.9 6 1.2
1.8 6 1.5
1.9 6 1.3
N (%)
N (%)
N (%)
N (%)
Sex
Female
2 (4.4)
70 (24.1)
66 (25.5
138 (23.2)
ACT
Male
43 (95.6)
220 (75.9)
193 (74.5)
456 (76.8)
Sport
Rugby union
25 (55.6)
149 (51.4)
148 (57.1)
322 (54.2)
Rugby league
1 (2.2)
21 (7.2)
15 (5.8)
37 (6.2)
Football (soccer)
7 (15.6)
38 (13.1)
24 (9.3)
69 (11.6)
Field hockey
1 (2.2)
9 (3.1)
4 (1.5)
14 (2.4)
Netball
0 (0.0)
6 (2.1)
4 (1.5)
10 (1.7)
Other
11 (24.4)
67 (23.1)
64 (24.7)
142 (23.9)
Concussion modifier
Not present
44 (97.8)
246 (85.1)
219 (84.9)
509 (86.0)
Present
1 (2.2)
43 (14.9)
39 (15.1)
83 (14.0)
INFORMATION
In unadjusted analysis, there was no association between the
adults ($19 years, n 5 63, 50%). Vestibular rehabilitation
length of recovery and the number of previous concussions (P 5
alone or in combination with cervical rehabilitation was more
0.92) or age group (P 5 0.36). A multiple linear regression
likely in adults (44% of patients) than younger age groups.
model showed that females, those with injuries from sports
other than Rugby Union, those with a concussion modifier, and
OFFICIAL
those with more time between their injury and the initial
DISCUSSION
appointment had significantly longer recovery times (Table 3).
The current study shows that less than half of those presenting
On average, the number of days until clinical recovery was 43%
acutely with a SR-mTBI show clinical recovery within 14 days
(exp (0.36) 5 1.43, or a 43% increase) longer for females,
and therefore, at best, may be cleared to return to play at 21
THE
whereas those with modifiers had a 48% longer recovery time.
days following the accepted GRTS program. This rate of
For each additional day between injury and the initial
recovery is slower than described in previous CISG and other
appointment, there was an increase in the average recovery
position statements.3,4,11,12 It is only at 28 days postinjury
time; for a 7-day increase in time to the initial appointment, we
does this figure rise to be comparable with the recovery rates
could expect an approximate 15% increase in the number of
quoted in these publications. Those participants referred on
days until clinical recovery (exp(0.02 3 7) 5 1.15).
are not represented in this figure and if accounted for would
A total of 5% of participants received cervical rehabilita-
only strengthen our case by adding to the number who had not
UNDER
tion, 28% received vestibular rehabilitation, and 10%
recovered within certain time frames.
received combined cervicovestibular rehabilitation as part of
As previously stated, recovery rates of 80% to 90% within 7 to
their individualized management. A smaller proportion of
10 days appeared first in the third consensus statement on
children (#12 years) required cervicovestibular rehabilitation
concussion in sport4 referenced to the second consensus statement
(n 5 4, 17%) than adolescents (13-18 years, n 5 69, 42%) or
that has no supportive data.2 A review of references from this
TABLE 2. Recovery of all Patients by the Age Group, Measured as the Number of Weeks After Injury
Until Asymptomatic
No. of Days After injury Until Asymptomatic
RELEASED
Age Group
<2 wk
2-4 wk
4-8 wk
‡ 8 wk
#12 yrs
22 (48.9%)
16 (35.6%)
6 (13.3%)
1 (2.2%)
13-18 yrs
116 (40.0%)
117 (40.3%)
49 (16.9%)
8 (2.8%)
.18 yrs
130 (50.2%)
58 (22.4%)
46 (17.8%)
25 (9.6%)
All ages
268 (45.1%)
191 (32.2%)
101 (17.0%)
34 (5.7%)
99
Copyright © 2020 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
S. Kara et al. (2020)
Clin J Sport Med
TABLE 3. Multiple Linear Regression of Factors Associated With Length of Recovery, Measured by
the Number of Days After Injury to Asymptomatic Status
Variable
Category/Unit
Coefficient (95% CI)
P
Sex
Male
Reference
Female
0.36 (0.15 to 0.57)
0.001
Sport
Rugby union
Reference
Rugby league
0.16 (20.17 to 0.51)
0.339
1982
Football (soccer)
0.57 (0.30 to 0.83)
,0.001
Other*
0.64 (0.44 to 0.86)
,0.001
Modifiers
No
Reference
Yes
0.39 (0.15 to 0.62)
0.001
ACT
Time from injury to initial appointment
Days
0.02 (0.01 to 0.03)
0.003
* Including hockey, netball, bike sports, water sports, snow sports, lacrosse, and combat sports such as martial arts and boxing.
early consensus paper highlight only opinion pieces23 or small
Gender and “concussion modifiers” represent well-published
cohort studies within single sports discussing concussion grading
risk factors for recovery,5 and our results further support this. It is
and postinjury symptomatology.24,25 In fact, data within the
unclear why the Rugby Union seems to represent less risk of
second international conference on concussion in sport2 cites
prolonged recovery compared with other sports. This might
a rugby league study showing that 50% of players still
reflect a proactive system wide approach from within this sport,
demonstrated impaired neurocognitive performance on testing
with education, clear advice, and early management, resulting in
10 days after injury.24 A systematic review has estimated the
less overall morbidity.31 It is also possible that this is due to an
prevalence of prolonged recovery (defined as .14 days in adults
under-reporting of concussion symptoms and not true recovery
and .28 days in children) to be between 10% and 30%, after SR-
among those who play rugby.32 There are a number of other
INFORMATION
mTBI.10 Unfortunately, only 25 studies met the inclusion criteria.
factors that might influence recovery. We have found a positive
These studies generally had relatively small sample sizes, (n 5 6-
association between persistent symptoms and a higher initial
128, mean age 20.1 years, duration of symptoms 10-226 days),
symptom burden (SCAT5 symptom score/severity score) with
were of relatively poor quality, and had an inconsistent definition
this being the subject of another publication.33
of persistent symptoms. Outside sport, there are data supporting
This current study suggests that those who are seen more
a more prolonged recovery time after mTBI. A 2-year multicenter
quickly after a SR-mTBI may have a faster recovery. This is
retrospective electronic health record review analyzed the injury
consistent with existing data demonstrating that earlier
and treatment history of 1840 adolescent patients (10-17 years),26
assessment may reduce the severity of persistent symptoms
OFFICIAL
showing a similar duration of recovery as presented in the current
and enhance recovery.26,34 Many patients with a SR-mTBI do
study. In this study, 75% of patients were symptom-free or had
not appreciate the value of a medical assessment and do not
returned to preinjury symptom levels 4 weeks after injury. Only
present for an assessment until their symptoms fail to resolve.
16% had recovered within the first week, whereas 6.7%
Others return to sport before their injury has resolved and are at
remained symptomatic at 8 weeks. A large multicenter Canadian
an increased risk of a further SR-mTBI or other types of injury.35
THE
study also reported persistent symptoms at 4 weeks in 30% of
It is possible these attitudes and behaviors are partly driven by
patients.27 We believe that our data may reflect the natural
the perception that SR-mTBI is a self-limiting problem. The
recovery timeline for those with a SR-mTBI and that recovery
results of this study challenge this perception and illustrate
rates may be slower than previously reported. Given the
a need for more education for those involved in sport.
uncertainty around the original statements, and increasing data
suggesting that many people have a more prolonged recovery,
more conservative recommendations may need to be made in
STRENGTHS AND LIMITATIONS
UNDER
future consensus statements.
The main strength of this study is in the prospectively collected
The literature focuses on slower recovery times in younger
data from a large sample of participants with a SR-mTBI.
patients.3–5 Existing data compare adolescents with children28
Participants were assessed and managed using a standardized,
and high school athletes with collegiate athletes.29 Interpreting
best practice model of care. We acknowledge that SR-mTBI
these data is however difficult due to inconsistencies between
may be a different clinical entity to mTBI sustained outside
study designs.28 Age showed no significant association with
sport; hence, results may not be applicable to this group. The
recovery in our cohort, a finding consistent with another larger
lack of a gold standard test and the reliance on symptom
study.30 Our results suggest that the natural recovery timeline
reporting will continue to be a limitation for all clinical
for SR-mTBI is similar irrespective of age. It is possible that the
research in this area. Our definition of clinical recovery allows
current data may more accurately represent the true recovery
participants to have some symptoms reflecting the nonspecific
RELEASED
trajectory for SR-mTBI, given that all participants, regardless of
nature of symptom reporting. Mandatory use of the Buffalo
age or level of sport, followed a standardized treatment
Concussion Treadmill Test before the GRTS program may
protocol including early active rehabilitation and equal access
provide a more objective measure of physiological recovery,
to medical resources, with similar recovery times across groups.
but the logistical nature of this is difficult to achieve outside of
Given these findings, we would suggest a more conservative
the research setting. Another potential limitation relates to the
approach across all age groups and not just younger groups.
use of the SCAT5. This tool is a validated diagnostic support
100
Copyright © 2020 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
Volume 30·Number 2·March 2020
www.cjsportmed.com
tool designed for use on the sideline and was not designed for
11. Harmon KG, Clugston JR, Dec K, et al. American Medical Society for
specific clinical setting use,36 although use is widespread. The
Sports Medicine position statement on concussion in sport. Br J Sports
lack of baseline comparison neurocognitive scores is also
Med. 2019;53:213–225.
12. Elkington L, Manzanero S, Hughes D. Concussion in Sport
a potential limitation. Further limitations relate to the
Australia—Position Statement. ACT, Australia: Sports Australia; 2019.
discharge criteria used; although participants were followed
13. Asken BM, Snyder AR, Clugston JR, et al. Concussion-like symptom
up until their clearance to return to normal sporting activity, it
reporting in non-concussed collegiate athletes. Arch Clin Neuropsychol.
is not clear whether they did this successfully or not. This
2017;32:963–971.
14. Lumba-Brown A, Yeates KO, Sarmiento K. Centers for disease control
methodology was used for logistical reasons and has been
and prevention guideline on the diagnosis and management of mild
used in other papers.20 There is the potential for selection bias
traumatic brain injury among children. JAMA Pediatr. 2018;172:
1982
in this study. Patients were able to self-refer, which could
e182853.
indicate higher motivation to return to sport but equally
15. Mucha A, Collins M, Elbin R, et al. A brief vestibular/ocular motor
reflect patient fear or catastrophizing, both of which could
screening (VOMS) assessment to evaluate concussions. Am J Sports Med.
2010;42:2479–2486.
influence recovery duration. Finally, the overall number of
16. Moran RN, Covassin T, Elbin RJ, et al. Reliability and normative
ACT
participants younger than 12 years is very small and does not
reference values for the vestibular/ocular motor screening (VOMS) tool in
permit any meaningful analysis. We continue to collect
youth athletes. Am J Sports Med. 2018;46:1475–1480.
prospective data and now have a larger cohort of pediatric
17. Schafer A, Ludtke K, Breuel F, et al. Validity of eyeball estimation for
patients. In time, we are hoping to be able to publish some
range of motion during the cervical flexion rotation test compared to an
ultrasound-based movement analysis system. Physiother Theor Pract.
more meaningful data on this group in a separate paper. We
2018;34:622–628.
believe that this will be more useful.
18. Hall TM, Robinson KW, Fujinawa O, et al. Intertester reliability and
diagnostic validity of the cervical flexion-rotation test. J Manip Physiol
Ther. 2008;31:293–300.
CONCLUSIONS
19. Leddy J, Baker J, Kozlowski K, et al. Reliability of a graded exercise test for
assessing recovery from concussion. Clin J Sport Med. 2011;21:89–94.
Recovery from a SR-mTBI is slower than previous interna-
20. Schneider K, Meeuwisse W, Nettel-Aguirre A, et al. Cervicovestibular
tional consensus statements have indicated. Less than half of
rehabilitation in sport-related concussion: a randomised controlled trial.
all participants in this study recovered within 2 weeks after
Br J Sports Med. 2014;48:1294–1298.
injury, and it is only at 28 days after injury do recovery rates
21. Alla S, Sullivan S, McCrory P. Defining asymptomatic status following
sports concussion: fact or fallacy? Br J Sports Med. 2012;46:562–569.
match those quoted in these statements. This is irrespective of
INFORMATION
22. Barrera-G ´omez J, Basagaña X. Models with transformed variables.
age with adults, adolescents, and children showing similar
Epidemiology. 2015;26:e16–e17.
recovery rates within 2 weeks, by 4 weeks, and by 8 weeks
23. Cantu R. Concussion severity should not be determined until all
after injury with best practice clinical care delivered across all
postconcussion symptoms have abated. Lancet Neurol. 2004;3:437–438.
age groups. Delay to presentation leads to delay in recovery
24. Hinton-Bayre AD, Geffen G. Severity of sports-related concussion and
neuropsychological test performance. Neurology. 2002;59:1068–1070.
with the message of early access to care needing to be
25. McCrory PR, Ariens T, Berkovic SF. The nature and duration of acute
mandated within individual sports.
concussive symptoms in Australian football. Clin J Sport Med. 2000;10:
235–238.
26. Thomas DJ, Coxe K, Li H, et al. Length of recovery from sports-related
References
concussions in pediatric patients treated at concussion clinics. Clin J Sport
OFFICIAL
1. Aubry M, Cantu R, Dvorak J, et al. Summary and agreement statement of
Med. 2018;28:56–63.
the First International Conference on Concussion in Sport, Vienna, 2001.
27. Zemek R, Barrowman N, Freedman SB, et al. Clinical risk score for
Recommendations for the improvement of safety and health of athletes
persistent post-concussion symptoms among children with acute
who may suffer concussive injuries. Br J Sports Med. 2002;36:6–10.
concussion in the ED. JAMA. 2016;315:1014–1025.
2. McCrory P, Meeuwisse W, Johnston K. Summary and agreement
28. Davis GA, Anderson V, Babl FE, et al. What is the difference in concussion
THE
statement of the 2nd international conference on concussion in sport,
management in children as compared with adults? A systematic review. Br
Prague 2004. Br J Sports Med. 2005;39:196–204.
J Sports Med. 2017;51:949–957.
3. McCrory P. Consensus statement on concussion in sport—the 4th
29. Field M, Collins MW, Lovell MR, et al. Does age play a role in recovery
international conference on concussion in sport held in Zurich,
from sports-related concussion? A comparison of high school and
November 2012. Clin J Sport Med. 2013;23:89–117.
collegiate athletes. J Pediatr. 2003;142:546–553.
4. McCrory P, Meeuwisse W, Johnston K. Consensus statement on
30. Nelson L, Guskiewicz K, Barr W, et al. Age differences in recovery after
concussion in sport: the 3rd international conference on concussion in
sport related concussion: a comparison of high school and collegiate
sport held in Zurich, November 2008. Br J Sports Med. 2009;43:
athletes. J Athl Train. 2016;51:142–152.
UNDER
i76–i84.
31. Gianotti SM, Quarrie KL, Hume PA. Evaluation of RugbySmart: a rugby
5. McCrory P, Meeuwisse W, Dvorak J, et al. Consensus statement on
union community injury prevention programme. J Sci Med Sport. 2009;
concussion in sport—the 5th International conference on concussion in
12:371–375.
sport held in Berlin, October 2016. Br J Sports Med. 2018;51:838–847.
32. Kroshus E, Kubzansky LD, Goldman RE, et al. Norms, athletic identity, and
6. Grool AM, Aglipay M, Momoli F, et al. Association between early
concussion symptom under-reporting among male collegiate ice hockey
participation in physical activity following acute concussion and persistent
players: a prospective cohort study. Ann Behav Med. 2015;49:95–103.
postconcussive symptoms in children and adolescents. JAMA. 2016;316:
33. McGeown JP, Kara S, Fulcher M, et al. Predicting sport-related mTBI
2504–2514.
symptom resolution trajectory using initial clinical assessment findings:
7. Leddy J, Hinds A, Sirica D, et al. The role of controlled exercise in
a retrospective cohort study. Sports Med. 2019 [epub ahead of print].
concussion management. J Phys Med Rehabil. 2016;8:S91–S100.
34. Forrest RHJ, Henry JD, McGarry PJ, et al. Mild traumatic brain injury in
8. Leddy J, Hinds A, Miecznikowski J, et al. Safety and prognostic utility of
New Zealand: factors influencing post-concussion symptom recovery
provocative
exercise
testing
in
acutely
concussed
adolescents:
time in a specialised concussion service. J Prim Health Care. 2018;10:
a randomized trial. Clin J Sport Med. 2018;28:13–20.
159–166.
RELEASED
9. Chan C, Iverson GL, Purtzki J, et al. Safety of active rehabilitation for
35. Cross M, Kemp S, Smith A, et al. Professional Rugby Union players have
persistent
symptoms
after
pediatric
sport-related
concussion:
a 60% greater risk of time loss injury after concussion: a 2-season
a randomized controlled trial. Arch Phys Med Rehabil. 2018;99:242–249.
prospective study of clinical outcomes. Br J Sports Med. 2016;50:926–931.
10. Makdissi M, Schneider KJ, Feddermann-Demont N, et al. Approach to
36. Fuller G, Kemp S, Decq P. The international rugby board (IRB) pitch side
investigation and treatment of persistent symptoms following sport-related
concussion assessment trial: a pilot test accuracy study. Br J Sports Med.
concussion: a systematic review. Br J Sports Med. 2017;51:958–968.
2015;49:529–535.
101
Copyright © 2020 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
 BJSM Online First, published on April 26, 2017 as 10.1136/bjsports-2017-097506SCAT5
BJSM Online First, published on April 26, 2017 as 10.1136/bjsports-2017-097506SCAT5
To download a clean version of the SCAT tools please visit the journal online (http://dx.doi.org/10.1136/bjsports-2017-097506SCAT5)
Br J Sports Med: first published as 10.1136/bjsports-2017-097506SCAT5 on 26 April 2017. Downloaded from
SCAT5 SPORT CONCUSSION ASSESSMENT TOOL — 5TH EDITION
©
DEVELOPED BY THE CONCUSSION IN SPORT GROUP
FOR USE BY MEDICAL PROFESSIONALS ONLY
supported by
1982
Patient details
ACT
Name:
DOB:
Address:
ID number:
Examiner:
Date of Injury:
Time:
WHAT IS THE SCAT5?
Key pointsINFORMATION
The SCAT5 is a standardized tool for evaluating concussions
• Any athlete with suspected concussion should be REMOVED
designed for use by physicians and licensed healthcare
FROM PLAY, medically assessed and monitored for
professionals1. The SCAT5 cannot be performed correctly
deterioration. No athlete diagnosed with concussion
in less than 10 minutes.
should be returned to play on the day of injury.
If you are not a physician or licensed healthcare professional,
• If an athlete is suspected of having a concussion and
please use the Concussion Recognition Tool 5 (CRT5). The
medical personnel are not immediately available, the
SCAT5 is to be used for evaluating athletes aged 13 years
athlete should be referred to a medical facility for urgent
and older. For children aged 12 years or younger, please
assessment.
OFFICIAL
use the Child SCAT5.
• Athletes with suspected concussion should not drink
alcohol, use recreational drugs and should not drive a motor
Preseason SCAT5 baseline testing can be useful for
vehicle until cleared to do so by a medical professional.
http://bjsm.bmj.com/
interpreting post-injury test scores, but is not required for
THE
that purpose.Detailed instructions for use of the SCAT5 are
• Concussion signs and symptoms evolve over time and it
provided on page 7. Please read through these instructions
is important to consider repeat evaluation in the assess-
careful y before testing the athlete. Brief verbal instructions
ment of concussion.
for each test are given in italics. The only equipment required
• The diagnosis of a concussion is a clinical judgment,
for the tester is a watch or timer.
made by a medical professional. The SCAT5 should NOT
This tool may be freely copied in its current form for dis-
be used by itself to make, or exclude, the diagnosis of
on July 26, 2021 by guest. Protected by copyright.
tribution to individuals, teams, groups and organizations.
concussion. An athlete may have a concussion even if
UNDER
It should not be altered in any way, re-branded or sold for
their SCAT5 is “normal”.
commercial gain. Any revision, translation or reproduction
in a digital form requires specific approval by the Concus-
Remember:
sion in Sport Group.
• The basic principles of first aid (danger, response, airway,
breathing, circulation) should be fol owed.
Recognise and Remove
• Do not attempt to move the athlete (other than that required
A head impact by either a direct blow or indirect transmission
for airway management) unless trained to do so.
of force can be associated with a serious and potential y fatal
• Assessment for a spinal cord injury is a critical part of the
brain injury. If there are significant concerns, including any
initial on-field assessment.
of the red flags listed in Box 1, then activation of emergency
RELEASED
procedures and urgent transport to the nearest hospital
• Do not remove a helmet or any other equipment unless
should be arranged.
trained to do so safely.
© Concussion in Sport Group 2017
Davis GA, et al. Br J Sports Med
SCAT 2017;
5 © Co
0
nc:1–8.
ussi doi:10.1136/bjsports-2017-097506SCA
on in Sport Group 2017
T5
1
1
Copyright Article author (or their employer) 2017. Produced by BMJ Publishing Group Ltd under licence.
Br J Sports Med: first published as 10.1136/bjsports-2017-097506SCAT5 on 26 April 2017. Downloaded from
1
Name:
IMMEDIATE OR ON-FIELD ASSESSMENT
DOB:
Address:
The following elements should be assessed for all athletes who
are suspected of having a concussion prior to proceeding to the
ID number:
neurocognitive assessment and ideal y should be done on-field after
the first first aid / emergency care priorities are completed.
Examiner:
Date:
If any of the “Red Flags“ or observable signs are noted after a direct
or indirect blow to the head, the athlete should be immediately and
1982
safely removed from participation and evaluated by a physician or
licensed healthcare professional.
STEP 4: EXAMINATION
Consideration of transportation to a medical facility should be at
the discretion of the physician or licensed healthcare professional.
GLASGOW COMA SCALE (GCS)3
ACT
The GCS is important as a standard measure for all patients and can
be done serial y if necessary in the event of deterioration in conscious
Time of assessment
state. The Maddocks questions and cervical spine exam are critical
Date of assessment
steps of the immediate assessment; however, these do not need to
be done serial y.
Best eye response (E)
STEP 1: RED FLAGS
No eye opening
1
1
1
Eye opening in response to pain
2
2
2
Eye opening to speech
3
3
3
RED FLAGS:
Eyes opening spontaneously
4
4
4
• Neck pain or
• Seizure or convulsion
Best verbal response (V)
tenderness
• Loss of consciousness
No verbal response
1
1
1
• Double vision
• Deteriorating
Incomprehensible sounds
2
2
2
INFORMATION
• Weakness or tingling/
conscious state
Inappropriate words
3
3
3
burning in arms or legs
• Vomiting
Confused
4
4
4
• Severe or increasing
• Increasingly restless,
Oriented
5
5
5
headache
agitated or combative
Best motor response (M)
No motor response
1
1
1
STEP 2: OBSERVABLE SIGNS
Extension to pain
2
2
2
Abnormal flexion to pain
3
3
3
Witnessed
Observed on Video
OFFICIAL
Flexion / Withdrawal to pain
4
4
4
Lying motionless on the playing surface
Y
N
Localizes to pain
5
5
5
Balance / gait difficulties / motor incoordination: stumbling, slow /
Obeys commands
6
6
6
http://bjsm.bmj.com/
laboured movements
Y
N
Glasgow Coma score (E + V + M)
THE
Disorientation or confusion, or an inability to respond appropriately
to questions
Y
N
Blank or vacant look
Y
N
CERVICAL SPINE ASSESSMENT
Facial injury after head trauma
Y
N
Does the athlete report that their neck is pain free at rest?
Y
N
STEP 3: MEMORY ASSESSMENT
on July 26, 2021 by guest. Protected by copyright.
If there is NO neck pain at rest, does the athlete have a full
MADDOCKS QUESTIONS2
range of ACTIVE pain free movement?
Y
N
UNDER
“I am going to ask you a few questions, please listen carefully and
Is the limb strength and sensation normal?
Y
N
give your best effort. First, tell me what happened?”
Mark Y for correct answer / N for incorrect
What venue are we at today?
Y
N
Which half is it now?
Y
N
In a patient who is not lucid or fully
conscious, a cervical spine injury should
Who scored last in this match?
Y
N
be assumed until proven otherwise.
RELEASED
What team did you play last week / game?
Y
N
Did your team win the last game?
Y
N
Note: Appropriate sport-specific questions may be substituted.
© Concussion in Sport Group 2017
2
Davis GA, et al. Br J Sports Med
SCAT 2017;
5 © Co
0
nc:1–8.
ussi doi:10.1136/bjsports-2017-097506SCA
on in Sport Group 2017
T5
2
Br J Sports Med: first published as 10.1136/bjsports-2017-097506SCAT5 on 26 April 2017. Downloaded from
OFFICE OR OFF-FIELD ASSESSMENT
Name:
Please note that the neurocognitive assessment should be done in a
distraction-free environment with the athlete in a resting state.
DOB:
Address:
STEP 1: ATHLETE BACKGROUND
ID number:
Sport / team / school:
Examiner:
Date:
Date / time of injury:
Years of education completed:
1982
Age:
2
Gender: M / F / Other
STEP 2: SYMPTOM EVALUATION ACT
Dominant hand: left / neither / right
The athlete should be given the symptom form and asked to read this instruction
How many diagnosed concussions has the
paragraph out loud then complete the symptom scale. For the baseline assessment,
the athlete should rate his/her symptoms based on how he/she typically feels and for
athlete had in the past?:
the post injury assessment the athlete should rate their symptoms at this point in time.
When was the most recent concussion?:
Please Check:
Baseline
Post-Injury
How long was the recovery (time to being cleared to play)
Please hand the form to the athlete
from the most recent concussion?:
(days)
none
mild
moderate
severe
Has the athlete ever been:
Headache
0
1
2
3
4
5
6
“Pressure in head”
0
1
2
3
4
5
6
Hospitalized for a head injury?
Yes
No
Neck Pain
0
1
2
3
4
5
6
Nausea or vomiting
0
1
2
3
4
5
6
Diagnosed / treated for headache disorder or migraines?
Yes
No
Dizziness
0
1
2
3
4
5
6
INFORMATION
Blurred vision
0
1
2
3
4
5
6
Diagnosed with a learning disability / dyslexia?
Yes
No
Balance problems
0
1
2
3
4
5
6
Sensitivity to light
0
1
2
3
4
5
6
Diagnosed with ADD / ADHD?
Yes
No
Sensitivity to noise
0
1
2
3
4
5
6
Feeling slowed down
0
1
2
3
4
5
6
Diagnosed with depression, anxiety
or other psychiatric disorder?
Yes
No
Feeling like “in a fog“
0
1
2
3
4
5
6
“Don’t feel right”
0
1
2
3
4
5
6
Current medications? If yes, please list:
Difficulty concentrating
0
1
2
3
4
5
6
OFFICIAL
Difficulty remembering
0
1
2
3
4
5
6
Fatigue or low energy
0
1
2
3
4
5
6
http://bjsm.bmj.com/
Confusion
0
1
2
3
4
5
6
THE
Drowsiness
0
1
2
3
4
5
6
More emotional
0
1
2
3
4
5
6
Irritability
0
1
2
3
4
5
6
Sadness
0
1
2
3
4
5
6
Nervous or Anxious
0
1
2
3
4
5
6
Trouble fal ing asleep
on July 26, 2021 by guest. Protected by copyright.
(if applicable)
0
1
2
3
4
5
6
UNDER
Total number of symptoms:
of 22
Symptom severity score:
of 132
Do your symptoms get worse with physical activity?
Y N
Do your symptoms get worse with mental activity?
Y N
If 100% is feeling perfectly normal, what
percent of normal do you feel?
If not 100%, why?
RELEASED
Please hand form back to examiner
© Concussion in Sport Group 2017
Davis GA, et al. Br J Sports Med
SCAT 2017;
5 © Co
0
nc:1–8.
ussi doi:10.1136/bjsports-2017-097506SCA
on in Sport Group 2017
T5
3
3
Br J Sports Med: first published as 10.1136/bjsports-2017-097506SCAT5 on 26 April 2017. Downloaded from
3
Name:
STEP 3: COGNITIVE SCREENING
DOB:
Standardised Assessment of Concussion (SAC)4
Address:
ORIENTATION
ID number:
Examiner:
What month is it?
0
1
Date:
What is the date today?
0
1
1982
What is the day of the week?
0
1
CONCENTRATION
What year is it?
0
1
DIGITS BACKWARDS
What time is it right now? (within 1 hour)
0
1
ACT
Please circle the Digit list chosen (A, B, C, D, E, F). Administer at the
Orientation score
of 5
rate of one digit per second reading DOWN the selected column.
I am going to read a string of numbers and when I am done, you repeat them back to me
IMMEDIATE MEMORY
in reverse order of how I read them to you. For example, if I say 7-1-9, you would say 9-1-7.
The Immediate Memory component can be completed using the
traditional 5-word per trial list or optional y using 10-words per trial
Concentration Number Lists (circle one)
to minimise any ceiling effect. All 3 trials must be administered irre-
spective of the number correct on the first trial. Administer at the rate
List A
List B
List C
of one word per second.
4-9-3
5-2-6
1-4-2
Y
N
0
Please choose EITHER the 5 or 10 word list groups and circle the specific word list chosen
for this test.
6-2-9
4-1-5
6-5-8
Y
N
1
I am going to test your memory. I will read you a list of words and when I am done, repeat
back as many words as you can remember, in any order. For Trials 2 & 3: I am going to repeat
3-8-1-4
1-7-9-5
6-8-3-1
Y
N
0
the same list again. Repeat back as many words as you can remember in any order, even if
you said the word before.
INFORMATION
3-2-7-9
4-9-6-8
3-4-8-1
Y
N
1
Score (of 5)
6-2-9-7-1
4-8-5-2-7
4-9-1-5-3
Y
N
0
List
Alternate 5 word lists
1-5-2-8-6
6-1-8-4-3
6-8-2-5-1
Y
N
1
Trial 1 Trial 2 Trial 3
7-1-8-4-6-2
8-3-1-9-6-4
3-7-6-5-1-9
Y
N
0
A
Finger
Penny
Blanket
Lemon
Insect
5-3-9-1-4-8
7-2-4-8-5-6
9-2-6-5-1-4
Y
N
1
B
Candle
Paper
Sugar
Sandwich
Wagon
List D
List E
List F
C
Baby
Monkey
Perfume
Sunset
Iron
OFFICIAL
7-8-2
3-8-2
2-7-1
Y
N
0
D
Elbow
Apple
Carpet
Saddle
Bubble
9-2-6
5-1-8
4-7-9
Y
N
1
http://bjsm.bmj.com/
E
Jacket
Arrow
Pepper
Cotton
Movie
4-1-8-3
2-7-9-3
1-6-8-3
Y
N
0
THE
F
Dollar
Honey
Mirror
Saddle
Anchor
9-7-2-3
2-1-6-9
3-9-2-4
Y
N
1
Immediate Memory Score
of 15
1-7-9-2-6
4-1-8-6-9
2-4-7-5-8
Y
N
0
Time that last trial was completed
4-1-7-5-2
9-4-1-7-5
8-3-9-6-4
Y
N
1
2-6-4-8-1-7
6-9-7-3-8-2
5-8-6-2-4-9
Y
N
0
on July 26, 2021 by guest. Protected by copyright.
Score (of 10)
UNDER
List
Alternate 10 word lists
8-4-1-9-3-5
4-2-7-9-3-8
3-1-7-8-2-6
Y
N
1
Trial 1 Trial 2 Trial 3
Digits Score:
of 4
Finger
Penny
Blanket
Lemon
Insect
G
Candle
Paper
Sugar
Sandwich
Wagon
MONTHS IN REVERSE ORDER
Baby
Monkey
Perfume
Sunset
Iron
H
Now tell me the months of the year in reverse order. Start with the last month and go backward.
Elbow
Apple
Carpet
Saddle
Bubble
So you’ll say December, November. Go ahead.
Dec - Nov - Oct - Sept - Aug - Jul - Jun - May - Apr - Mar - Feb - Jan
0 1
Jacket
Arrow
Pepper
Cotton
Movie
I
Months Score
of 1
Dollar
Honey
Mirror
Saddle
Anchor
RELEASED
Concentration Total Score (Digits + Months)
of 5
Immediate Memory Score
of 30
Time that last trial was completed
© Concussion in Sport Group 2017
4
Davis GA, et al. Br J Sports Med
SCAT 2017;
5 © Co
0
nc:1–8.
ussi doi:10.1136/bjsports-2017-097506SCA
on in Sport Group 2017
T5
4
Br J Sports Med: first published as 10.1136/bjsports-2017-097506SCAT5 on 26 April 2017. Downloaded from
4
Name:
STEP 4: NEUROLOGICAL SCREEN
DOB:
See the instruction sheet (page 7) for details of
Address:
test administration and scoring of the tests.
ID number:
Can the patient read aloud (e.g. symptom check-
Examiner:
list) and fol ow instructions without difficulty?
Y
N
Does the patient have a full range of pain-
Date:
free PASSIVE cervical spine movement?
Y
N
Without moving their head or neck, can the patient look
1982
side-to-side and up-and-down without double vision?
Y
N
Can the patient perform the finger nose
coordination test normal y?
Y
N
5
Can the patient perform tandem gait normal y?
Y
N
STEP 5: DELAYED RECALL:
ACT
BALANCE EXAMINATION
The delayed recall should be performed after 5 minutes have
elapsed since the end of the Immediate Recal section. Score 1
Modified Balance Error Scoring System (mBESS) testing5
pt. for each correct response.
Which foot was tested
Left
Do you remember that list of words I read a few times earlier? Tell me as many words
(i.e. which is the non-dominant foot)
Right
from the list as you can remember in any order.
Testing surface (hard floor, field, etc.)
Time Started
Footwear (shoes, barefoot, braces, tape, etc.)
Condition
Errors
Please record each word correctly recal ed. Total score equals number of words recal ed.
Double leg stance
of 10
Single leg stance (non-dominant foot)
of 10
Tandem stance (non-dominant foot at the back)
of 10
Total Errors
of 30
Total number of words recalled accurately:
of 5
or
of 10
INFORMATION
6
STEP 6: DECISION
Date and time of injury:
Date & time of assessment:
If the athlete is known to you prior to their injury, are they different from their usual self?
OFFICIAL
Domain
Yes
No
Unsure
Not Applicable
Symptom
(If different, describe why in the clinical notes section)
number (of 22)
Concussion Diagnosed?
http://bjsm.bmj.com/
Symptom severity
Yes
No
Unsure
Not Applicable
score (of 132)
THE
If re-testing, has the athlete improved?
Orientation (of 5)
Yes
No
Unsure
Not Applicable
of 15
of 15
of 15
Immediate memory
I am a physician or licensed healthcare professional and I have personal y
of 30
of 30
of 30
administered or supervised the administration of this SCAT5.
Concentration (of 5)
Signature:
on July 26, 2021 by guest. Protected by copyright.
Neuro exam
Normal
Normal
Normal
Name:
Abnormal
Abnormal
Abnormal
UNDER
Title:
Balance errors (of 30)
Registration number (if applicable):
of 5
of 5
of 5
Delayed Recall
of 10
of 10
of 10
Date:
SCORING ON THE SCAT5 SHOULD NOT BE USED AS A STAND-ALONE
METHOD TO DIAGNOSE CONCUSSION, MEASURE RECOVERY OR
RELEASED
MAKE DECISIONS ABOUT AN ATHLETE’S READINESS TO RETURN TO
COMPETITION AFTER CONCUSSION.
© Concussion in Sport Group 2017
Davis GA, et al. Br J Sports Med
SCAT 2017;
5 © Co
0
nc:1–8.
ussi doi:10.1136/bjsports-2017-097506SCA
on in Sport Group 2017
T5
5
5
Br J Sports Med: first published as 10.1136/bjsports-2017-097506SCAT5 on 26 April 2017. Downloaded from
CLINICAL NOTES:
Name:
DOB:
Address:
ID number:
Examiner:
Date:
1982
ACT
INFORMATION
CONCUSSION INJURY ADVICE
(To be given to the person monitoring the concussed athlete)
Clinic phone number:
OFFICIAL
This patient has received an injury to the head. A careful medical
Patient’s name:
examination has been carried out and no sign of any serious
complications has been found. Recovery time is variable across
Date / time of injury:
individuals and the patient will need monitoring for a further pe-
http://bjsm.bmj.com/
riod by a responsible adult. Your treating physician wil provide
Date / time of medical review:
THE
guidance as to this timeframe.
If you notice any change in behaviour, vomiting, worsening head-
Healthcare Provider:
ache, double vision or excessive drowsiness, please telephone
your doctor or the nearest hospital emergency department
immediately.
on July 26, 2021 by guest. Protected by copyright.
Other important points:
UNDER
Initial rest: Limit physical activity to routine daily activities (avoid
exercise, training, sports) and limit activities such as school,
work, and screen time to a level that does not worsen symptoms.
1) Avoid alcohol
© Concussion in Sport Group 2017
2) Avoid prescription or non-prescription drugs
without medical supervision. Specifical y:
a) Avoid sleeping tablets
b) Do not use aspirin, anti-inflammatory medication
RELEASED
or stronger pain medications such as narcotics
3) Do not drive until cleared by a healthcare professional.
4) Return to play/sport requires clearance
by a healthcare professional.
Contact details or stamp
6
Davis GA, et al. Br J Sports Med
SCAT 2017;
5 © Co
0
nc:1–8.
ussi doi:10.1136/bjsports-2017-097506SCA
on in Sport Group 2017
T5
6
Br J Sports Med: first published as 10.1136/bjsports-2017-097506SCAT5 on 26 April 2017. Downloaded from
INSTRUCTIONS
Words in Italics throughout the SCAT5 are the instructions given to the athlete by the clinician
Symptom Scale
one error is recorded but the athlete should quickly return to the testing position, and
counting should resume once the athlete is set. Athletes that are unable to maintain
The time frame for symptoms should be based on the type of test being admin-
the testing procedure for a minimum of five seconds at the start are assigned the
istered. At baseline it is advantageous to assess how an athlete “typical y” feels
highest possible score, ten, for that testing condition.
whereas during the acute/post-acute stage it is best to ask how the athlete feels
at the time of testing.
OPTION: For further assessment, the same 3 stances can be performed on a surface
of medium density foam (e.g., approximately 50cm x 40cm x 6cm).
The symptom scale should be completed by the athlete, not by the examiner. In
situations where the symptom scale is being completed after exercise, it should
Balance testing – types of errors
be done in a resting state, general y by approximating his/her resting heart rate.
1982
1. Hands lifted off
3. Step, stumble, or fal
5. Lifting forefoot or heel
For total number of symptoms, maximum possible is 22 except immediately post
iliac crest
injury, if sleep item is omitted, which then creates a maximum of 21.
4. Moving hip into > 30
6. Remaining out of test
For Symptom severity score, add all scores in table, maximum possible is 22 x 6
2. Opening eyes
degrees abduction
position > 5 sec
= 132, except immediately post injury if sleep item is omitted, which then creates
ACT
a maximum of 21x6=126.
“I am now going to test your balance. Please take your shoes off (if applicable), roll up
your pant legs above ankle (if applicable), and remove any ankle taping (if applicable).
Immediate Memory
This test will consist of three twenty second tests with different stances.“
(a) Double leg stance:
The Immediate Memory component can be completed using the traditional 5-word
per trial list or, optionally, using 10-words per trial. The literature suggests that
“The first stance is standing with your feet together with your hands on your hips
the Immediate Memory has a notable ceiling effect when a 5-word list is used. In
and with your eyes closed. You should try to maintain stability in that position for 20
settings where this ceiling is prominent, the examiner may wish to make the task
seconds. I will be counting the number of times you move out of this position. I will
more difficult by incorporating two 5–word groups for a total of 10 words per trial.
start timing when you are set and have closed your eyes.“
In this case, the maximum score per trial is 10 with a total trial maximum of 30.
(b) Single leg stance:
Choose one of the word lists (either 5 or 10). Then perform 3 trials of immediate
memory using this list.
“If you were to kick a ball, which foot would you use? [This will be the dominant
foot]
Now stand on your non-dominant foot. The dominant leg should be held in
Complete all 3 trials regardless of score on previous trials.
approximately 30 degrees of hip flexion and 45 degrees of knee flexion. Again, you
should try to maintain stability for 20 seconds with your hands on your hips and your
“I am going to test your memory. I will read you a list of words and when I am done,
eyes closed. I will be counting the number of times you move out of this position. If
repeat back as many words as you can remember, in any order.” The words must be
you stumble out of this position, open your eyes and return to the start position and
read at a rate of one word per second.
continue balancing. I will start timing when you are set and have closed your eyes.“
Trials 2 & 3 MUST be completed regardless of score on trial 1 & 2.
(c) Tandem stance:
INFORMATION
Trials 2 & 3:
“Now stand heel-to-toe with your non-dominant foot in back. Your weight should be
“I am going to repeat the same list again. Repeat back as many words as you can
evenly distributed across both feet. Again, you should try to maintain stability for 20
remember in any order, even if you said the word before.“
seconds with your hands on your hips and your eyes closed. I will be counting the
number of times you move out of this position. If you stumble out of this position,
Score 1 pt. for each correct response. Total score equals sum across all 3 trials.
open your eyes and return to the start position and continue balancing. I will start
Do NOT inform the athlete that delayed recall will be tested.
timing when you are set and have closed your eyes.”
Concentration
Tandem Gait
Digits backward
Participants are instructed to stand with their feet together behind a starting line
(the test is best done with footwear removed). Then, they walk in a forward direction
Choose one column of digits from lists A, B, C, D, E or F and administer those digits
OFFICIAL
as quickly and as accurately as possible along a 38mm wide (sports tape), 3 metre
as fol ows:
line with an alternate foot heel-to-toe gait ensuring that they approximate their heel
and toe on each step. Once they cross the end of the 3m line, they turn 180 degrees
Say:
“I am going to read a string of numbers and when I am done, you repeat them
and return to the starting point using the same gait. Athletes fail the test if they
http://bjsm.bmj.com/
back to me in reverse order of how I read them to you. For example, if I say 7-1-9,
step off the line, have a separation between their heel and toe, or if they touch or
you would say 9-1-7.”
grab the examiner or an object.
THE
Begin with first 3 digit string.
Finger to Nose
If correct, circle “Y” for correct and go to next string length. If incorrect, circle “N” for
the first string length and read trial 2 in the same string length. One point possible
“I am going to test your coordination now. Please sit comfortably on the chair with
for each string length. Stop after incorrect on both trials (2 N’s) in a string length.
your eyes open and your arm (either right or left) outstretched (shoulder flexed to
The digits should be read at the rate of one per second.
90 degrees and elbow and fingers extended), pointing in front of you. When I give
a start signal, I would like you to perform five successive finger to nose repetitions
Months in reverse order
using your index finger to touch the tip of the nose, and then return to the starting
position, as quickly and as accurately as possible.”
on July 26, 2021 by guest. Protected by copyright.
“Now tell me the months of the year in reverse order. Start with the last month and
UNDER
go backward. So you’ll say December, November ... Go ahead”
References
1 pt. for entire sequence correct
1.
McCrory et al. Consensus Statement On Concussion In Sport – The 5th
Delayed Recall
International Conference On Concussion In Sport Held In Berlin, October 2016.
British Journal of Sports Medicine 2017 (available at www.bjsm.bmj.com)
The delayed recall should be performed after 5 minutes have elapsed since the end
2.
Maddocks, DL; Dicker, GD; Saling, MM. The assessment of orientation fol owing
of the Immediate Recall section.
concussion in athletes. Clinical Journal of Sport Medicine 1995; 5: 32-33
“Do you remember that list of words I read a few times earlier? Tell me as many words
from the list as you can remember in any order.“
3.
Jennett, B., Bond, M. Assessment of outcome after severe brain damage: a
practical scale. Lancet 1975; i: 480-484
Score 1 pt. for each correct response
4.
McCrea M. Standardized mental status testing of acute concussion. Clinical
Modified Balance Error Scoring System (mBESS)5 testing
Journal of Sport Medicine. 2001; 11: 176-181
RELEASED
This balance testing is based on a modified version of the Balance Error Scoring
5.
Guskiewicz KM. Assessment of postural stability following sport-related
System (BESS)5. A timing device is required for this testing.
concussion. Current Sports Medicine Reports. 2003; 2: 24-30
Each of 20-second trial/stance is scored by counting the number of errors. The
examiner will begin counting errors only after the athlete has assumed the proper
start position. The modified BESS is calculated by adding one error point for each
error during the three 20-second tests. The maximum number of errors for any
single condition is 10. If the athlete commits multiple errors simultaneously, only
© Concussion in Sport Group 2017
Davis GA, et al. Br J Sports Med
SCAT 2017;
5 © Co
0
nc:1–8.
ussi doi:10.1136/bjsports-2017-097506SCA
on in Sport Group 2017
T5
7
7
Br J Sports Med: first published as 10.1136/bjsports-2017-097506SCAT5 on 26 April 2017. Downloaded from
CONCUSSION INFORMATION
Any athlete suspected of having a concussion should be removed from
Graduated Return to School Strategy
play and seek medical evaluation.
Concussion may affect the ability to learn at school. The athlete may
Signs to watch for
need to miss a few days of school after a concussion. When going back
to school, some athletes may need to go back gradual y and may need to
Problems could arise over the first 24-48 hours. The athlete should not be
have some changes made to their schedule so that concussion symptoms
do not get worse. If a particular activity makes symptoms worse, then the
left alone and must go to a hospital at once if they experience:
athlete should stop that activity and rest until symptoms get better. To
• Worsening
• Repeated vomiting
• Weakness or
make sure that the athlete can get back to school without problems, it is
headache
numbness in
important that the healthcare provider, parents, caregivers and teachers 1982
• Unusual behaviour
arms or legs
talk to each other so that everyone knows what the plan is for the athlete
• Drowsiness or
or confusion
to go back to school.
inability to be
or irritable
• Unsteadiness
awakened
on their feet.
Note: If mental activity does not cause any symptoms, the athlete may
• Seizures (arms
be able to skip step 2 and return to school part-time before doing school
• Inability to
and legs jerk
• Slurred speech
activities at home first.
ACT
recognize people
uncontrol ably)
or places
Mental Activity
Activity at each step
Goal of
each step
Consult your physician or licensed healthcare professional after a sus-
pected concussion. Remember, it is better to be safe.
1. Daily activities
Typical activities that the athlete
Gradual
that do
does during the day as long as
return to
Rest & Rehabilitation
not give
they do not increase symptoms
typical
the athlete
(e.g. reading, texting, screen
activities.
After a concussion, the athlete should have physical rest and relative
symptoms
time). Start with 5-15 minutes at
cognitive rest for a few days to al ow their symptoms to improve. In most
a time and gradual y build up.
cases, after no more than a few days of rest, the athlete should gradual y
2. School
Homework, reading or other
Increase
increase their daily activity level as long as their symptoms do not worsen.
activities
cognitive activities outside of
tolerance
Once the athlete is able to complete their usual daily activities without
the classroom.
to cognitive
concussion-related symptoms, the second step of the return to play/sport
work.
progression can be started. The athlete should not return to play/sport
until their concussion-related symptoms have resolved and the athlete
3. Return to
Gradual introduction of school-
Increase
has successful y returned to full school/learning activities.
school
work. May need to start with
academic
part-time
a partial school day or with
activities.
INFORMATION
When returning to play/sport, the athlete should follow a stepwise,
increased breaks during the day.
medically managed exercise progression, with increasing amounts of
4. Return to
Gradual y progress school
Return to full
exercise. For example:
school
activities until a full day can be
academic
full-time
tolerated.
activities and
Graduated Return to Sport Strategy
catch up on
missed work.
Exercise step
Functional exercise
If the athlete continues to have symptoms with mental activity, some
at each step
Goal of each step
other accomodations that can help with return to school may include:
1. Symptom-
Daily activities that do
Gradual reintroduc-
limited activity
not provoke symptoms.
tion of work/school
• Starting school later, only
• Taking lots of breaks during
OFFICIAL
activities.
going for half days, or going
class, homework, tests
only to certain classes
2. Light aerobic
Walking or stationary
Increase heart rate.
• No more than one exam/day
exercise
cycling at slow to medium
• More time to finish
http://bjsm.bmj.com/
pace. No resistance
assignments/tests
• Shorter assignments
training.
THE
• Quiet room to finish
• Repetition/memory cues
3. Sport-specific
Running or skating dril s.
Add movement.
exercise
No head impact activities.
assignments/tests
• Use of a student helper/tutor
4. Non-contact
Harder training drills, e.g.,
Exercise, coor-
• Not going to noisy areas
training drills
passing dril s. May start
dination, and
like the cafeteria, assembly
• Reassurance from teachers
progressive resistance
increased thinking.
hal s, sporting events, music
that the child will be supported
training.
class, shop class, etc.
while getting better
on July 26, 2021 by guest. Protected by copyright.
5. Full contact
Following medical clear-
Restore confi-
UNDER
practice
ance, participate in normal
dence and assess
The athlete should not go back to sports until they are back to school/
training activities.
functional skills by
learning, without symptoms getting significantly worse and no longer
coaching staff.
needing any changes to their schedule.
6. Return to
Normal game play.
play/sport
In this example, it would be typical to have 24 hours (or longer) for each
step of the progression. If any symptoms worsen while exercising, the
athlete should go back to the previous step. Resistance training should
be added only in the later stages (Stage 3 or 4 at the earliest).
Written clearance should be provided by a healthcare professional before
return to play/sport as directed by local laws and regulations.
RELEASED
© Concussion in Sport Group 2017
8
Davis GA, et al. Br J Sports Med
SCAT 2017;
5 © Co
0
nc:1–8.
ussi doi:10.1136/bjsports-2017-097506SCA
on in Sport Group 2017
T5
8
 Brain Injury Screening Tool (BIST)
Brain Injury Screening Tool (BIST)
1982
A guide to traumatic brain injury assessment
ACT
The BIST was developed to be a brief tool
This tool should be used in addition to clinical
for use on initial presentation after injury to
judgment and other assessments such as
guide health care pathway decision making
the Vestibular/Oculomotor Motor Screening
and to monitor symptoms and recovery over
(VOMS), King-Devick or the Romberg’s test.
time. Its purpose is to help guide the clinical
Additional questioning to add to the clinical
assessment conversation by operationalising
picture is encouraged.
current international best practice guidelines.1
The first 9 questions in the BIST are designed
The BIST has been developed for health
to assist if there are clinical indicators that the
INFORMATION
professionals working across primary and
person is at high risk of complications or poor
secondary health care and for sports and other
recovery and requires hospital evaluation. The
contexts where traumatic brain injuries (TBI)
15-item symptom scale is designed to assist in
can occur.
identifying patients at moderate risk of poor
The BIST can facilitate clinical decision making
recovery who may benefit from early specialist
through identification of people who are at low,
treatment and low risk patients who are likely
medium or high risk of longer-term difficulties.
to recover well, supported within primary care.
OFFICIAL
Date of Injury:
Time of Injury:
Date of Consultation:
THE
Age1:
Gender/Sex:
UNDER
1. If over 65 years, socially isolated or living alone, consider referral to the Emergency Department
Female
Male
.
Ethnicty:
If your answer is OTHER please specify:
European
Maori
Pasifika
Asian
Middle Eastern
Other
1. Please tell me about what happened2 (Observe for high risk indicators such as suspicion of skull fracture, focal
neurological deficit, high speed, focal blunt trauma or fall from height (e.g. >5 stairs)
RELEASED
2. If high risk indicators present, consider referral to Emergency Department.
1
2. Did anyone with you at the time of the injury say anything else about what happened?
3. Have you been sick/vomited?3
1982
Yes
No
a. If yes, how many times
3. If >1 vomiting episode, consider referral to Emergency Department.
ACT
4. Were you knocked out (or did you lose consciousness)?4
Yes
No
Unknown
a. If yes, how long
hrs
mins
4. If loss of consciousness >brief, consider referral to Emergency Department.
5. Did you have a fit or seizure straight afterwards? E.g. go stiff or shake violently?5
Yes
No
Unknown
INFORMATION
5. If yes, consider referral to Emergency Department.
6. Are you feeling better, worse or about the same since the injury?6
Better
Worse
About the same
6. If symptoms have worsened, consider referral to Emergency Department.
OFFICIAL
7. Have you hit your head or had a concussion/brain injury before ?7
THE
Yes
No
a. If yes, how many times
b. when was the last injury?
7. If recent or unrecovered previous injury, consider referral to Emergency Department.
If recent injury but recovered the person may be moderate risk of poor recovery and early specialist input may be required.
Consider referral to concussion service.
UNDER
8. Are you currently taking any medications that thin the blood e.g. anti-
coagulants?Yes8
No
8. If yes, consider referral to emergency department.
9. Have you ever experienced any difficulties with your mental health?
RELEASED
Yes9
No
9. If yes, the person may be at moderate risk of poor recovery and early specialist input may be required. Consider referral to
concussion service.
2
Please ask the patient the following question.
Compared with before the accident, please rate how much you experience the following right now
(at this point in time);
Not
at
Mild
Moderate
Severe
all
(a little)
(quite bad)
(very bad)
1982
0
1
2
3
4
5
6
7
8
9
10
Headache (my head hurts)10
ACT
My neck hurts
Physical
I don’t like bright lights
I don’t like loud noises
Total physical score (out of 40)
I feel dizzy or like I could
be sick
If I close my eyes, I feel like
Vestibular- I am at sea
INFORMATION
ocular
I have trouble with my
eyesight (vision)
I feel clumsy
Total vestibular score (out of 40)
It takes me longer to think
OFFICIAL
I forget things
Cognitive I get confused easily THE
I have trouble concentrating
Total cognitive score (out of 40)
If more than 24 hours post-injury, please also rate these physical symptoms
UNDER
I get angry or irritated
easily
I feel restless
I feel tired during the day
I need to sleep a lot more or
find it hard to sleep at night
RELEASED
10. If severe headache, consider referral to Emergency Department.
3

Total symptom severity score within
Total symptom severity score
24 hours (out of 12011)
>24 hours (out of 16012)
Number of symptoms endorsed within
Number of symptoms endorsed
24 hours (out of 12)
>24 hours (out of 16)
What is the dominant symptom cluster?
(High proportion or most severe symptoms
reported (e.g. physical, vestibular or
cognitive?)
1982
11. If 50 or more consider referral to specialist concussion clinic, as this person is likely to be at moderate risk of poor recovery.
If <50 this person is at low risk, monitor and follow up in 7-10 days.
12. If 66 or more consider referral to specialist concussion clinic, as this person is likely to be at moderate risk of poor recovery.
If <66 this person is at low risk, monitor and follow up in 7-10 days. If minimal improvement in scores since previous visit, consider referral to concussion clinic.
ACT
Injuries to the brain can affect how a person feels, behaves, thinks and how able they are to do everyday tasks.
On a scale of 0 to 100, where 0 means that you do not feel the injury has had any impact on you at all and 100
means you feel that injury stops you from doing anything, how much do you feel your injury is impacting on you at
this point in time?
INFORMATION
0
10
20
30
40
50
60
70
80
90
100
OFFICIAL
THE
Acknowledgements
This tool has been developed by the ACC Concussion Clinical Expert Group: Alice Theadom, Natalie Hardaker, Penelope Day, Kris Fernando, Katherine Forch, Kevin
Henshall, Doug King, Mark Fulcher, Renata Gottgtroy, Sam Jewell, Stephen Kara, Patria Hume.
Reference
UNDER
Silverberg ND, et al on behalf of the American Congress of Rehabilitation Medicine Brain Injury Interdisciplinary Special Interest Group Mild TBI Task Force.
Management of Concussion and Mild Traumatic Brain Injury: A Synthesis of Practice Guidelines. Archives of Physical Medicine and Rehabilitation, 2020, 101; 382-393
© 2020 Auckland University of Technology. BIST (Brain Injury Screening Tool) is licensed under a
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
CC BY-ND: This license allows reusers to copy and distribute the material in any medium or format in unadapted form only,
and only so long as attribution is given to the creator. The license allows for commercial use.
RELEASED
4
link to page 23 link to page 23 link to page 23 link to page 23 link to page 23 link to page 23 link to page 23 link to page 22






















 http://bjsm.bmj.com/
Downloaded from
on April 26, 2017 - Published by group.bmj.com
BJSM Online First, published on April 26, 2017 as 10.1136/bjsports-2017-097492
Consensus statement
http://bjsm.bmj.com/
Downloaded from
on April 26, 2017 - Published by group.bmj.com
BJSM Online First, published on April 26, 2017 as 10.1136/bjsports-2017-097492
Consensus statement
The Child Sport Concussion Assessment Tool 5th
Edition (Child SCAT5)
Gavin A Davis,1,2 Laura Purcell,3 Kathryn J Schneider,4,5,6 Keith Owen Yeates,7
Gerard A Gioia,8,9 Vicki Anderson,1 Richard G Ellenbogen,10 Ruben J Echemendia,11
Michael Makdissi,2,12 Allen Sills,13 Grant L Iverson,14 Jiri Dvorak,15 Paul McCrory,2
Willem Meeuwisse,16 Jon Patricios,17,18 Christopher C Giza,19 Jeffrey S Kutcher20
1982
For numbered affiliations see
ABSTRACT
many younger children could not perform this
end of article.
This article presents the Child Sport Concussion
task with three-digit strings. Fourth, the Months
ACT
Assessment Tool 5th Edition (Child SCAT5). The
in Reverse Order was changed to Days of the Week
Correspondence to
Sport Concussion Assessment Tool was introduced
because many young children could not recite
Professor Gavin A Davis, Suite
53 - Neurosurgery, Cabrini
in 2004, following the 2nd International Conference
the months in order. Fifth, the Balance Exam-
Medical Centre, Malvern,
on Concussion in Sport in Prague, Czech Republic.
ination removed the single-leg stance because
Victoria, Australia; gavin. davis@
Following the 4th International Consensus Conference,
many younger children were unable to perform
me. com
held in Zurich, Switzerland, in 2012, the SCAT 3rd
this task. Finally, Return to School information
was provided for the child athlete. To date, very
Accepted 9 January 2017
edition (Child SCAT3) was developed for children aged
between 5 and12 years. Research to date was reviewed
few studies have been published using the Child
and synthesised for the 5th International Consensus
SCAT
3.5–8
Conference on Concussion in Sport in Berlin, Germany,
leading to the current revision of the test, the Child
SCAT5. This article describes the development of the
METHODS
Child SCAT5.
The 5th International Consensus Conference on
Concussion in Sport, held in Berlin, Germany, in
INFORMATION
2016, followed a consensus development process,
which incorporated systematic reviews to address
specific questions, and the results of the reviews
INTRODUCTION
were presented at the meeting in an open forum.
The Sport Concussion Assessment Tool (SCAT) Full methods of the 5th International Consensus
was introduced in 2004, following the 2nd Inter-
Conference on Concussion in Sport are published
national Conference on Concussion in Sport in
elsewhere.9 Poster abstracts, as well as audience
Prague, Czech Republic
.1 The aim was to ‘create questions and feedback, were included in the
a standardised tool that could be used for patient expert panel’s deliberations following the meeting
education as well as for physician assessment of
OFFICIAL in Berlin.
sports concussion’, by combining eight existing
A systematic review of the SCAT3 and Child
tools into one. However, the SCAT was not SCAT3 was performed
10 and the evidence was
age-specific and was not appropriate for younger synthesised to inform the expert panel convened
concussed children. The 3rd International Confer-
THE
to improve these tools. The panel unanimously
ence on Concussion in Sport, held in Zurich, agreed that a child-specific version of the SCAT
Switzerland, in 2008, introduced the SCAT2 and is required. A subgroup of the Berlin Expert Panel
recommended its use for athletes aged ≥10 years.
2 met on a separate day to develop a revised version
The 4th International Consensus Conference, held of the tool, the Child SCAT5.
The version number
in Zurich, Switzerland, in 2012, examined the
(5) was chosen to align the version number with the
evidence for the assessment of the child athlete and
consensus meeting number and, therefore, there is
determined that a child-specific tool was required.
UNDER
no Child SCAT4.
Thus, the Child SCAT3 was developed for chil-
dren aged between 5 and 12 yea
rs.3 Based on the
available evidence, the Child SCAT3 incorporated
RESULTS
several components that differed from the SCAT3. Based on the systematic reviews, conference discus-
►
http:// dx. doi. org/ bjsports-
First, the Maddocks questions were modified to sions and panel deliberations, we made several
2017- 097492childscat5
include questions more appropriate to children modifications to the Child SCAT3 to create the
engaged in both organised and playground sport. Child SCAT5. These modifications are set out in
Second, the Symptom Evaluation was changed
box 1. The format of the Child SCAT5 is consis-
from the adult version of the Post-Concussion tent with the SCAT5. The panel sought to minimise
Symptom Scale to the Health and Behavior Inven-
the changes to test elements that have demon-
RELEASED tory, which is a validated symptom list for both strated validity and are complemented by published
To cite: Davis GA, Purcell L,
child-reported and parent-reported symptoms.
4 normative data. We modified components that did
Schneider KJ, et al. Br J
Sports Med Published Online
Third, the Orientation assessment did not include not meet these criteria, as needed.
First: [please include Day
the time question because most young children
The Child SCAT5 is a tool for evaluating
Month Year]. doi:10.1136/
cannot answer this question. Fourth, the Digits injured children (aged 5–12 years) suspected
bjsports-2017-097492
Backwards introduced a two-digit string because of having suffered concussion and is designed
Davis GA, et al. Br J Sports Med 2017;
0:1–3. doi:10.1136/bjsports-2017-097492
1
Copyright Article author (or their employer) 2017. Produced by BMJ Publishing Group Ltd under licence.
link to page 23 link to page 23 link to page 23 link to page 23 link to page 23
http://bjsm.bmj.com/
Downloaded from
on April 26, 2017 - Published by group.bmj.com
Consensus statement
non-medically trained individuals for the identification and
Box 1 Modifications of the Child SCAT3 for the Child
immediate management of suspected concussion and is also
SCAT5.
published separately
.12
► The Potential Signs of Concussion Box was replaced with
a ‘Red Flags’ Box in the initial assessment to highlight the
DISCUSSION
potential of a structural brain injury that may require neuro-
The Child SCAT5 is consistent with the previous version—it
surgical intervention.
provides a standardised approach to the evaluation of suspected
► Declaration that the complete Child SCAT5 cannot be appro-
concussion that includes measures and methods valid for
priately completed in less than 10–15 min.
detecting sport-related concussion. The Child SCAT5 incorpo-
1982
► The modified Maddocks questions were removed because of
rates changes that address some of the limitations identified in
the questionable reliability and usefulness in young children.
the systematic
review10 and provides additional evaluative tools
► The Symptom Evaluation is recommended to be performed
(eg, RNS).
with the child in a resting state.
The diagnosis of concussion relies on a clinical synthesis of
► Neck pain was added to the list of child-reported and
complex, non-specific and, at times, contradictory information.
ACT
parent-reported symptoms.
Accordingly, only healthcare professionals trained in the assess-
► An overall rating of functioning (0-10) has been included for
ment and management of sport-related concussion should use
the Child Report and a rating (0-100) has been included for
the Child SCAT5. The Child SCAT5 is a tool to assist the quali-
the Parent Report.
fied health professional with the clinical diagnosis of concussion
► The Orientation questions were removed because of their
and is not designed to be used in isolation to make or exclude the
doubtful usefulness in young children.
diagnosis of concussion.
► The Immediate Memory word lists include two additional
The Child SCAT5 includes comprehensive instructions for
five-word lists and optional 10-word lists are provided for
the appropriate administration of the subscales that should
older children in whom a ceiling effect is identified with the
be carefully studied and practised prior to clinical use. Future
five-word lists. All six versions of the Standardised Assess-
research on the reliability and validity of the Child SCAT5 will
ment of Concussion word lists are now presented and they
inform further improvement of this tool. We note that there are
should be administered by choosing one at random for
insufficient data on the use of the Child SCAT in athletes with
baseline testing and then using them serially post-injury.
disabilities and across different cultures and language groups. We
INFORMATION
► The time at completion of the third trial of the word list is
recommended that a systematic approach be undertaken to trans-
recorded and the Delayed Recall is not to proceed <5 min
late and culturally adapt the Child SCAT5 into other languages.
from completion of the Immediate Recall.
The Concussion in Sport Group encourages research; there is a
► Digits Backwards has been modified to include two
need for a comprehensive set of norms in both sexes and across
additional digit lists and has been formatted to assist with
ages, language groups, sports and in people with disabilities.
administration of this test, in which a correct response from
The Child SCAT5 is available for free, unrestricted distribu-
one string length advances to the next string length, but
tion for use in childhood sport-related concussion, provided
an incorrect response requires a second trial at the same
that no modifications are made to the tool. The development of
string length. Administration of different digit lists should be
the tool is evidence-informed and we encourage its widespread
OFFICIAL
randomised at baseline and serially post injury.
distribution and use by medical professionals worldwide.
► The Balance Examination includes the single-leg stance for
Author affiliations
children aged 10–12 years.
1Murdoch Childrens Research Institute, Melbourne, Australia
► The Neck Examination and Coordination Examination have
2Florey Institute of Neuroscience and Mental Health, Austin Campus, Melbourne
THE
been removed and incorporated into a new section, the
Brain Centre, Heidelberg, Australia
3
Rapid Neurological Screen (RNS).
Department of Pediatrics, McMaster University, Hamilton, Ontario, Canada
4Sport Injury Prevention Research Centre, Faculty of Kinesiology, University of
► The RNS includes assessment of balance and gait, ocular
Calgary, Alberta, Canada
function, coordination and reading (assesses cognitive func-
5Alberta Children's Hospital Research Institute for Child & Maternal Health,
tion, cranial nerves [acuity, diplopia], dysphasia, dysarthria
Cumming School of Medicine, University of Calgary, Alberta, Canada
6
and response time). Younger children who cannot read are
Hotchkiss Brain Institute, University of Calgary, Alberta, Canada
7
asked to describe what they see in a photograph.
Department of Psychology, Alberta Children’s Research Institute, Hotchkiss Brain
UNDER
Institute, University of Calgary, Calgary, Canada
► The Return to School information has been modified to
8Division of Pediatric Neuropsychology, Children’s National Health System, George
inform the student that prolonged school absence is not
Washington University School of Medicine, Washington, DC, USA
9
recommended and that appropriate accommodations should
Department of Pediatrics and Psychiatry & Behavioral Sciences, George Washington
be made, in consultation with the medical team, teachers
University School of Medicine, Washington, DC, USA
10
and parents/caregivers. The Return to School section includes
Department of Neurological Surgery, University of Washington, Seattle,
Washington, USA
a stepwise table that allows for symptom-limited cognitive
11University Orthopaedic Center, Concussion Care Clinic, State College, PA, USA;
activity.
13
University of Missouri-Kansas City, Kansas City, Missouri, USA
12
► The Return to Sport information has been modified to inform
Olympic Park Sports Medicine Centre, Melbourne, Australia
13
the student that a symptom-limited activity programme
Vanderbilt University Medical Center, Nashville, Tennessee, USA
14Center for Health and Rehabilitation Research, Department of Physical Medicine
should be followed with healthcare professional guidance
.13
and Rehabilitation, Harvard Medical School, Charlestown, Massachusetts, USA
RELEASED
15Swiss Concussion Center, Schulthess Clinic Zurich, Switzerland
16Sport Injury Prevention Research Centre, Faculty of Kinesiolgy, University of
Calgary, Canada
for use by medical professionals. The SCAT5, for athletes
17Section Sports Medicine, Faculty of Health Sciences, University of Pretoria, Pretoria,
aged ≥13 years, is published separately
.11 A separate tool,
South Africa
the Concussion Recognition Tool 5, has been developed for
18Department of Emergency Medicine, Faculty of Health Sciences, University of the
Witwatersrand, Johannesburg, South Africa
2
Davis GA, et al. Br J Sports Med 2017;
0:1–3. doi:10.1136/bjsports-2017-097492
http://bjsm.bmj.com/
Downloaded from
on April 26, 2017 - Published by group.bmj.com
Consensus statement
19UCLA Steve Tisch BrainSPORT Program, Operation MEND TBI Program, Los Angeles,
research. Dr. McCrory is a cofounder and shareholder in two biomedical companies
USA
(involved in eHealth and Compression garment technologies) but does not hold any
20The Sports Neurology Clinic at the CORE Institute, Michigan, USA
individual shares in any company related to concussion or brain injury assessment or
technology. He did not receive any form of financial support directly related to this
Competing interests GAD is an honorary member of the Australian Football
manuscript. WM is Medical Director for the National Hockey League. JP is concussion
League Concussion Working Group and has attended meetings organised by
consultant to South African Rugby’s BokSmart injury prevention programme and
sporting organisations including the NFL (USA), National Rugby League (Australia)
a member of World Rugby’s Concussion Advisory Group; both organisations have
and FIFA (Switzerland); however, he has not received any payment, research funding
contributed honoraria towards conference expenses. GAG receives royalties as a
or other monies from these groups other than for travel costs. LP is an expert
test author from Psychological Assessment Resources, receives research funding
consultant to mdBriefcase in the development of an online concussion education
from the CDC and NIH, receives speaking Honoria for professional lectures, and is
module and has received speaking honoraria/travel expenses for presentations
on the pediatric mild TBI guidelines panel of the CDC. CCG receives grants/research
at scientific meetings. KJS has received speaking honoraria for presentations at
support from NIH, NCAA, DoD, Today’s and Tomorrow’s Children Fund, UCLA Brain 1982
scientific meetings. She is a physiotherapy consultant at Evidence Sport and Spinal
Injury Research Center, UCLA Faculty Grants Program, UCLA Steve Tisch BrainSPORT
Therapy in Calgary, Alberta, Canada, and for athletic teams. KOY has received grant
program, Avanir (research grant 2016-2017), NINDS Neural Analytics SBIR grant
funding from NIH and Canadian Institutes of Health Research and book royalties
(2016-2018)Consultant: NFL-Neurological Care Program, NHLPA, Neural Analytics
from Guilford Press and Cambridge University Press and has occasionally served
Inc (2015-16), is on the advisory panel of LoveYourBrain, MLS, NBA, NCAA, USSF,
as an expert witness in forensic cases; he is President-Elect of the International
performs medicolegal work 1-2 cases annually, and speaks on the Medical Education
ACT
Neuropsychological Society and a member of the Expert Panel on Acute Diagnosis
Speakers Network.JSK provides consulting to National Basketball Association,
and Management of Mild Traumatic Brain Injury among Children and Adolescents
National Football League Players' Association, National Hockey League Players'
convened by the Centers for Disease Control and Prevention. RGE is a volunteer
Association, ElMindA, Ltd. VA and JD have nothing to declare.
co-chairman of the NFL Head Neck and Spine Medical Committee. RJE is a
Provenance and peer review Commissioned; internally peer reviewed.
consultant to the NHL, Major League Soccer, US Soccer Federation and Princeton
University. He has received financial remuneration for these consulting relationships.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the
He has a clinical practice in sport neuropsychology and serves as an expert
article) 2017. All rights reserved. No commercial use is permitted unless otherwise
(neuropsychology, sport neuropsychology) in medico-legal cases involving traumatic
expressly granted.
brain injury. He at times has received honoraria and reimbursement of expenses
to attend professional meetings. MM is Consultant Sport and Exercise Medicine
REFERENCES
Physician at Olympic Park Sports Medicine Centre, Team Doctor—Hawthorn
1 McCrory P Johnston K, Meeuwisse W, et al. Summary and agreement statement of
football club (Australian Football League(AFL)). AFL research grant—funding for
the 2nd international conference on concussion in sport, Prague 2004.
Br J Sports
research program on concussion in AFL (collaboration between the AFL and the
Med 2005;39:i78–i86.
Florey Institute of Neuroscience & Mental Health). Shareholder—Olympic Park
2 McCrory P, Meeuwisse W, Johnston K, et al. Consensus statement on concussion
Sports Medicine Centre. IOC—travel and accommodation paid as part of Ad Hoc
in sport: the 3rd international conference on concussion in sport held in Zurich,
Committee to evaluate rule changes in boxing. FIFA—Travel and accommodation
November 2008.
Br J Sports Med 2009;43 (Suppl 1):i76–i84.
paid as part of International Concussion in Sport Group. AFL—support for travel
INFORMATION
3 McCrory P, Meeuwisse WH, Aubry M, et al. Consensus statement on concussion
to NFL concussion ‘think tank’ August 2014. CogState Pty Ltd—free access to
in sport: the 4th international conference on concussion in sport held in Zurich,
computerised neuropsychological testing program for research purposes. AFL Doctors
November 2012.
Br J Sports Med 2013;47:250–8.
Association—paid role as executive officer. Honorary member of the Australian
4 Ayr LK, Yeates KO, Taylor HG, et al. Dimensions of postconcussive symptoms in
Rugby Union Concussion Advisory Group; World Rugby Concussion working group;
children with mild traumatic brain injuries.
J Int Neuropsychol Soc 2009;15:19–30.
Concussion in AFL working group; AFL Concussion Scientific Committee and Member
5 Brooks A, McGuine T, Kebisek J, et al. Establishing the psychometric properties
and the International Olympic Committee ad hoc group to evaluate rule change in
of the child sport concussion assessment tool (Child SCAT3). Clin J Sport Med
boxing. AS is an unaffiliated neurotrauma consultant, the NFL . GLI acknowledges
2015;25:214.
philanthropic research support from the Mooney-Reed Charitable Foundation and
6 Glaviano NR, Benson S, Goodkin HP, et al. Baseline SCAT2 assessment of healthy
ImPACT Applications, Inc. He has a medical-legal consulting practice, including
youth student-athletes: Preliminary evidence for the use of the Child-SCAT3 in
expert testimony, in the area of neuropsychology and mild traumatic brain injury.
children younger than 13 years.
Clin J Sport Med 2015;25:373–9.
OFFICIAL
PMcC is a co-investigator, collaborator, or consultant on grants relating to mild
7 Jennings D, Sells P, Allison J, et al. Effects of a season of subconcussive contact
TBI funded by several governmental organizations. He is directly employed by the
on child- SCAT3 scores in 8-12 year-old male athletes. Int J Sports Phys Ther
National Health & Medical Research Council of Australia and is based at the Florey
2015;10:667.
Institute of Neuroscience and Mental Health. He is Co-Chair of the Australian Centre
8 Nelson LD, Loman MM, LaRoche AA, et al. Baseline performance and psychometric
for Research into Sports Injury and its Prevention (ACRISP), which is one of the
properties of the child sport concussion assessment tool 3 (Child-SCAT3) in 5- to
THE
International University Research Centres for Prevention of Injury and Protection
13-year-old Athletes.
Clin J Sport Med 2016:1.
of Athlete Health supported by the International Olympic Committee (IOC). He is
9 Meeuwisse W, Schneider K, Dvorak J, et al. The Berlin 2016 process: a summary of
co-chair of the International Concussion in Sport Group and is a member of the
methodology for the 5th international consensus conference on concussion in sport .
scientific advisory boards of the International Concussion & Head Injury Research
Br J Sports Med 2017 .
Foundation (London, UK) and the Sports Surgery Clinic (Dublin, Ireland). He has a
10 Echemendia RJ, Broglio SP, Davis GA, et al. What tests and measures should be
clinical and consulting practice in general and sports neurology. He receives book
added to the SCAT3 and related tests to improve their reliability, sensitivity and/or
royalties from McGraw-Hill and was employed in an editorial capacity by the British
specificity in sideline concussion diagnosis? A systematic Review Br J Sports Med
Medical Journal Publishing Group from 2001 to 2008. He has been reimbursed
2017.
by the government, professional scientific bodies, and sporting bodies for travel
11 Echemendia RJ, Meeuwisse W, McCrory P, et al. The Sport ConcussionAssessment
UNDER
costs related to presenting research on mild TBI and sport-related concussion at
Tool 5th Edition (SCAT5). British Journal of Sports Medicine 2017.
meetings, scientific conferences, and symposiums. He received consultancy fees in
12 Echemendia RJ, Meeuwisse W, McCrory P, et al. The Concussion RecognitionTool 5th
2010 from Axon Sports (US) for the development of educational material (which
Edition (CRT5). Br J Sports Med 2017.
was not renewed) and has received research funding since 2001 from CogState Inc.
13 Davis GA, Anderson V, Babl FE, et al. What is the difference in concussion
The Australian Football League funds research at the Florey Institute under a legal
management in children as compared to adults? A systematic review. Br J Sports
memorandum and Dr. McCrory does not receive any money from this industry funded
Med 2017.
RELEASED
Davis GA, et al. Br J Sports Med 2017;
0:1–3. doi:10.1136/bjsports-2017-097492
3
 http://bjsm.bmj.com/
Downloaded from
on April 26, 2017 - Published by group.bmj.com
The Child Sport Concussion Assessment
http://bjsm.bmj.com/
Downloaded from
on April 26, 2017 - Published by group.bmj.com
The Child Sport Concussion Assessment
Tool 5th Edition (Child SCAT5)
Gavin A Davis, Laura Purcell, Kathryn J Schneider, Keith Owen Yeates,
Gerard A Gioia, Vicki Anderson, Richard G Ellenbogen, Ruben J
Echemendia, Michael Makdissi, Allen Sills, Grant L Iverson, Jiri Dvorak,
Paul McCrory, Willem Meeuwisse, Jon Patricios, Christopher C Giza and
Jeffrey S Kutcher
published online April 26, 2017
Br J Sports Med
1982
Updated information and services can be found at:
http://bjsm.bmj.com/content/early/2017/04/26/bjsports-2017-097492
ACT
These include:
References
This article cites 7 articles, 2 of which you can access for free at:
http://bjsm.bmj.com/content/early/2017/04/26/bjsports-2017-097492
#BIBL
Email alerting
Receive free email alerts when new articles cite this article. Sign up in the
service
box at the top right corner of the online article.
INFORMATION
Notes
OFFICIAL
THE
UNDER
To request permissions go to:
http://group.bmj.com/group/rights-licensing/permissions
To order reprints go to:
http://journals.bmj.com/cgi/reprintform
RELEASED
To subscribe to BMJ go to:
http://group.bmj.com/subscribe/
Document Outline