Antenatal Screening
for Down Syndrome
and Other Conditions
Guidelines for health practitioners
Antenatal and newborn screening
The National Screening Unit (NSU) of the Ministry of Health is responsible for the
development, implementation and management of three antenatal and newborn
screening programmes:
> Universal Offer Antenatal HIV Screening Programme
> Newborn Metabolic Screening Programme
> Universal Newborn Hearing Screening and Early Intervention Programme.
The NSU is also responsible for the introduction of quality improvements to antenatal
screening for Down syndrome and other conditions.
Quality improvements to antenatal screening for Down syndrome and other conditions
have been introduced to bring this screening in New Zealand into line with international
best practice. While all pregnant women are advised about this screening, it is optional. It
is made available so that those women who wish to have this information about their baby
are able to find out during their pregnancy and plan accordingly.
These guidelines replace the
Guidelines for maternity providers offering antenatal
screening for Down syndrome and other conditions in New Zealand dated November 2009.
Acknowledgements
The National Screening Unit would like to thank the many individuals and groups who
contributed to the development of these guidelines.
National Screening Unit. 2012.
Antenatal Screening for Down Syndrome
and Other Conditions: Guidelines for health practitioners.
Wellington: Ministry of Health
Published in February 2013
by the Ministry of Health
PO Box 5013, Wellington 6145, New Zealand
ISBN 978-0-478-37338-7 (print)
ISBN 978-0-478-37341-7 (online)
HP 5409
This document is available on the National Screening Unit website:
www.nsu.govt.nz
link to page 2 link to page 2 link to page 5 link to page 7 link to page 8 link to page 8 link to page 8 link to page 10 link to page 10 link to page 11 link to page 11 link to page 11 link to page 11 link to page 13 link to page 15 link to page 16 link to page 22 link to page 23 link to page 23 link to page 24 link to page 24 link to page 27 link to page 33 link to page 37 link to page 39 link to page 44 link to page 47 link to page 47 link to page 48 link to page 48 link to page 49 link to page 53 link to page 61 link to page 62
 Contents
Antenatal and newborn screening
ii
Acknowledgements ii
Contents
Antenatal and newborn screening
ii
Acknowledgements ii
Key messages
v
1. Introduction
1
2. Background
2
2.1 Overview of antenatal screening for Down syndrome and other conditions
2
2.2 The screening options
2
2.3 Screening performance
4
2.4 Potential benefits and harms of antenatal screening for Down syndrome and other conditions
4
3. General requirements
5
3.1 Code of Health and Disability Services Consumers’ Rights
5
3.2 Health Information Privacy Code
5
3.3 Ensuring services meet the needs of women
5
4. The screening pathway
7
5. Documentation
9
6. Informed choice – consent or decline
10
6.1 Initial discussion
16
7. The screening tests
17
7.1 Timing of first trimester combined OR second trimester maternal screening tests
17
7.2 Ordering tests
18
7.3 Completing the screening request form
18
8. Receiving and communicating results
21
9. Diagnostic testing
27
10. Genetic services and other referrals
31
11. Nuchal Translucency (NT) scan
33
12. Screening laboratory processes
38
13. Data, information and monitoring
41
13.1 Data and information collection
41
13.2 Uses of data and information
42
13.3 Monitoring
42
Appendix 1: Resources and contacts
43
Appendix 2: Screened conditions
47
Appendix 3: Robinson equation
55
Glossary of terms
56
Antenatal screening for Down syndrome and other conditions: Guidelines for health practitioners
iii


 Key messages
Key messages
1. Antenatal screening for Down syndrome and other conditions provides a risk estimate
for Down syndrome (trisomy 21), trisomy 18 (Edwards syndrome), trisomy 13 (Patau
syndrome) and some other rare genetic disorders.
Page 2
2. Detection of fetal anomalies through this screening offers women information that may
help them prepare for the birth of their child: the option of delivery in a setting that has
access to specialist surgical or medical care; the possibility of considering termination;
or palliative care in the newborn period.
Page 2
3. Antenatal screening for Down syndrome and other conditions is optional for pregnant
women.
Page 10
4. The right to decline screening, decline tests or further investigations should be made
clear by the health professional and any such decision by the woman, including
withdrawal of consent, must be respected.
Page 10
5. Women who are less than 20 weeks pregnant must be advised about the availability of
antenatal screening for Down syndrome and other conditions.
Page 10
6. Up-to-date information about antenatal screening for Down syndrome and other
conditions must be provided to support the screening discussion, thus enabling women
to make an informed decision whether to accept or decline.
Page 10
7. Informed choice for this screening must include a discussion about the screened
conditions and the decisions that may need to be made as a result of participation in
this screening.
Page 10
8. No single test checks for everything. No screening test finds all cases of a condition.
Page 10
9. A thorough family history should be taken and where there is a family history of a
genetic condition, a referral for a discussion with a specialist obstetrician or genetic
services should be offered prior to screening.
Page 15
10. First trimester combined screening should be completed between 9 weeks and 13 weeks
6 days gestation.
The recommended timing for the blood test is 9 to 10 weeks and
for the Nuchal Translucency scan is at 12 weeks. Page 17
11. Second trimester maternal serum screening should be completed between 14 weeks and
20 weeks gestation.
The recommended timing for this test is 14 to 18 weeks. Page 17
12. A very high or very low level of the blood markers used in screening may indicate other
conditions such as pre-eclampsia or pre-term birth. Fetal anomalies such as a heart
condition or structural defect may be found on ultrasound.
Page 21
13. Screening for neural tube defects (NTD) can be reported after 15 weeks of pregnancy
using alpha fetoprotein (AFP) as the serum marker. It is noted that a better predictor of
NTD is the 18 to 20 week anatomy scan.
Page 21
14. The health professional requesting screening must fill in all sections of the screening
request form to ensure an accurate risk assessment.
Page 18
15. Clear documentation of the screening process must be kept in the clinical records
including the discussion, consent or decline of tests or referrals and results of
screening.
Page 9
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
v
List of abbreviations
AFP Alpha-fetoprotein
ASUM
Australasian Society for Ultrasound in Medicine
ßhCG
Beta-human chorionic gonadatrophin
BPD
Biparietal diameter
CRL
Crown–rump length
CVS
Chorionic villus sampling
DHB
District Health Board
EDD
Estimated date of delivery
FMF
Fetal Medicine Foundation
IVF
In vitro fertilisation
LMC
Lead maternity carer
LMP
Last menstrual period
MoM
Multiple of the median
NSU
National Screening Unit of the Ministry of Health
NTD
Neural tube defect
NT
Nuchal translucency
NZDSA
New Zealand Down Syndrome Association
PAPP-A
Pregnancy-associated plasma protein A
RANZCOG Royal Australian and New Zealand College of Obstetricians and Gynaecologists
RANZCR
Royal Australian and New Zealand College of Radiologists
uE
Unconjugated oestriol
3
vi Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
 1. Introduction
1. Introduction
These guidelines support health practitioners advising about the availability of services
for antenatal screening for Down syndrome and other conditions. They are intended for
all practitioners involved in aspects of antenatal screening for Down syndrome and other
conditions including:
> lead maternity carers (LMCs)
> midwives
> general practitioners
> nurses
> sonologists, sonographers, radiologists
> obstetricians, fetal medicine specialists
> screening laboratory staff.
Health practitioners advising women about maternity care have an obligation under the
Primary Maternity Services Notice 2007, issued pursuant to section 88 of the New Zealand
Public Health and Disability Act 2000, to advise women of screening services available that
are endorsed by the Ministry of Health, including antenatal screening for Down syndrome
and other conditions.
During the screening process, the health practitioner is responsible for:
(a) providing information and education about antenatal screening to pregnant women
(b) supporting women to make an informed decision
(c) offering referrals as agreed with the woman
(d) communicating screening results
(e) ensuring documentation of screening discussions and choices in the clinical notes
(f) ensuring compliance with the:
> Privacy Act 1993 and Health Information Privacy Code 1994
> New Zealand Public Health and Disability Act 2000
> Code of Health and Disability Services Consumers’ Rights 1996
> Health Act 1956
> Health Practitioners Competence Assurance Act 2003
> Public Records Act 2005
> Crimes Act 1961 (as amended).
It is strongly recommended that health practitioners complete the e-learning modules
at www.learnonline.health.nz which have been approved as professional development
by the Midwifery Council of New Zealand and the Royal Australasian College of General
Practitioners (RNZGP).
Other screening resources are available for health practitioners at www.nsu.govt.nz
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
1
 2. Background
2. Background
Antenatal screening for Down syndrome and other conditions has been available to
pregnant women in New Zealand since 1968. In October 2007, the government agreed to
implement quality improvements to antenatal screening for Down syndrome and other
conditions to ensure consistency with international best practice. The objective of the
quality improvements initiative is to ensure that the screening tests available for pregnant
women in New Zealand provide the best possible information, so that women can make an
informed decision about the way their pregnancy is managed.
2.1 Overview of antenatal screening for Down
syndrome and other conditions
Detection of fetal anomalies through this screening offers women information that
may help them prepare for the birth of their child: the option of delivery in a setting
that has access to specialist surgical or medical care; the possibility of considering
termination; or palliative care in the newborn period.
Antenatal screening for Down syndrome and other conditions is a way of assessing the
probability that a baby has Down syndrome or another genetic condition and offers women
information and choice in the care and management of their pregnancy and baby’s birth.
Antenatal screening for Down syndrome and other conditions has complex ethical
and social implications. In addition there are technical considerations which involve a
trade-off between the sensitivity (detection rate) and the specificity (false positive rate)
of the screening tests. The combination of ultrasound and maternal serum markers
increases detection rates (improves sensitivity) and/or reduces the number of women
considered to be at increased risk (improves specificity), compared with previous first
trimester screening practice.
These guidelines refer to the risk estimate calculations and reports. Health practitioners
are encouraged to use different methods for communicating individual risk results to
women and this may include words such as chance or likelihood. The use of risk in these
guidelines is synonymous with chance used in the consumer information.
2.2 The screening options
Antenatal screening for Down syndrome and other conditions provides a risk
estimate for Down syndrome (trisomy 21), trisomy 18 (Edwards syndrome),
trisomy 13 (Patau syndrome) and some other rare genetic disorders.
This screening divides women into two groups based on risk, either increased risk or low
risk. Table 1 outlines the screening options.
First trimester combined screening involves a nuchal translucency (NT) scan and
maternal serum testing. The risk is calculated by the screening laboratory from the NT
measurement, the serum marker levels and other factors including crown-rump length,
maternal age and weight. Women will receive one combined result from their health
practitioner, after they have had both the blood test and the NT scan. The incorporation of
serum results in the risk calculation significantly increases the sensitivity and specificity
of screening and provides a better risk assessment than NT scanning in isolation1.
1. Wald NJ, Rodeck C, Hackshaw AK, Walters J, Chitty L, Mackinson AM. 2003. First and second trimester
antenatal screening for Down’s syndrome: the results of the Serum, Urine and Ultrasound Screening Study
(SURUSS).
Health Technol Assess 7(11): 1-77.
2
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
Second trimester screening involves maternal serum testing only. The results of the serum
tests are incorporated with other parameters such as maternal age, weight and gestation to
provide a risk report.
The option of screening during the second trimester means screening can be offered to
women who:
> do not access maternity care early in their pregnancy
> do not have access to NT scanning for geographic, economic or other reasons
> have not completed first trimester combined screening
> prefer second trimester screening.
Table 1: The screening options available
First trimester
Second trimester
Recommendations
combined screening
OR maternal serum screening AND for practice
(9 – 13w and 6 days)
(14 – 20 weeks)
> Blood test that
> Blood test that
> The discontinuation of
measures two maternal
measures four maternal
the use of maternal age
serum markers (PAPP-A
serum markers (ßhCG,
and nuchal translucency
and ßhCG) combined
AFP, uE and inhibin A).
as screening tools in
3
with an ultrasound scan
> Available to women
isolation.
to determine NT and CRL
who present after the
measurements.
first trimester or who do
> Available to all women
not access first trimester
who present in the first
combined screening.
trimester.
> The blood test is fully
> The blood test is fully
funded.
funded.
> Women may be required
to make a co-payment
for the ultrasound scan.
(The Ministry of Health
funds the ultrasound
provider on a fee for
service basis for each
NT scan).
Provision of accurate, balanced information (both medical and non-medical).
Support for decisions made by women throughout pregnancy, including the decision as to
whether or not to participate in screening.
Support for women who want their family/whãnau to be actively involved.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
3
2.3 Screening performance
The screening test relies on accurate and full information being provided by the health
practitioner. The screening request form must include details of gestation, IVF, weight,
smoking status, ethnicity and relevant family history.
In New Zealand, the screening cut-off is 1:300. As an example, a woman with a risk result
of 1:250 will be increased risk and 1:350 will be low risk.
Based on international data, this screening finds approximately 85% of babies with Down
syndrome. Approximately 5% of women will receive an increased risk result.
2.4 Potential benefits and harms of antenatal
screening for Down syndrome and other
conditions
All pregnant women must be advised about the availability of antenatal screening
for Down syndrome and other conditions, including the risks, benefits and harms of
screening, so that they may make an informed decision to participate in screening or
not. Screening poses different ethical considerations from those that arise when a person
presents for medical care because they are unwell. Health practitioners have a special duty
of care when advising women of screening.
The potential benefits of antenatal screening for Down syndrome and other conditions
include:
> access to information that may provide more choice in the care and management of
the pregnancy and birth
> reassurance associated with low risk results for the screened conditions
> reassurance associated with no abnormalities found through scanning.
The potential harms of antenatal screening for Down syndrome and other conditions
include:
> anxiety and stress associated with the screening process
> women having a poor understanding of the screening process. This may include a lack of
understanding of risk estimates and what may or may not be detected
> anxiety and stress associated with an increased risk result which may be a false
positive result
> false reassurance when a low risk result is given when the baby does have a condition
ie, a false negative result
> a miscarriage resulting from diagnostic procedures following an increased risk result.
4
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
 3. General requirements
3.1 Code of Health and Disability Services
Consumers’ Rights
3. General requirements
3.1 Code of Health and Disability Services
Consumers’ Rights
The Code of Health and Disability Services Consumers’ Rights provides that New Zealand
health care consumers have a legal right to appropriate information to enable informed
consent. Information about the Code can be obtained from the Health and Disability
Commissioner’s website, www.hdc.org.nz
3.2 Health Information Privacy Code
The Health Information Privacy Code 1994 (HIPC) sets specific rules for agencies in
the health sector to ensure the protection of individual privacy. It addresses health
information collected, used, held and disclosed by health agencies.
For the health sector, the HIPC takes the place of the information privacy principles set out
in the Privacy Act 1993. The HIPC can be viewed at the Privacy Commissioner’s website,
www.privacy.org.nz
The 12 rules of the HIPC require agencies to be clear about the purpose for which they
collect information, and open about those purposes to the health consumers they collect
it from. Health information must be held securely to protect it against misuse, loss or
unauthorised disclosure.
Health consumers can access their health information (with some minor exceptions) and
seek its correction when it is wrong. Health information should only be used or disclosed
for the purposes for which it was collected, unless one of the exceptions in the HIPC
applies.
3.3 Ensuring services meet the needs of women
Health services should be tailored to meet the needs of the individuals receiving them.
This helps to ensure equity of access and outcomes. Health services should enable people
to take responsibility for managing their own health.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
5
Achieving Equitable Outcomes
Guidelines
Information
Health services should be attuned to
Health services should be tailored to meet the
the needs of individuals, families and
health needs of all New Zealanders, including
communities.
Mãori, Pacific peoples and Asian populations.
Health practitioners should recognise that
what works for different populations varies.
Health practitioners should familiarise
themselves with Whãnau Ora found at
www.health.govt.nz and the NZ Disability
Strategy found at www.odi.govt.nz
Health practitioners should offer additional
Appropriate information that allows for
support to women who have difficulty
informed consent includes using professional
understanding information because of
interpreter services, such as Language Line,
language difficulties, hearing impairment or
a DHB interpreter or a NZ Sign Language
intellectual disability.
interpreter where necessary. Using family
members or friends as interpreters is not
recommended practice.
Women who have an intellectual disability
may require extra support or the presence
of family/whãnau or other support people
(eg independent advocate, welfare guardian)
to understand the information and assist their
decision making.
Health practitioners should recognise other
Barriers to accessing aspects of antenatal care
barriers to access.
and screening may include lack of knowledge,
fear of health services, different cultural views
of health, the location and cost of ultrasound
services, the availability of transport, travel
time and child care.
6
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners

 4. The screening pathway
4. The screening pathway
Figure 1 details the screening pathway. It is the woman’s choice whether to accept
screening or not and she may also accept or decline any referral or test.
The points along the pathway where the woman needs to make an informed decision are:
(a) whether or not to be screened
(b) whether to accept an offer of referral to a specialist obstetrician or specialist medical
maternity service or Genetic Services to gather more information following an
increased risk or abnormal result
(c) whether to have diagnostic testing following a referral and discussion
(d) when deciding the next step after receiving the results of the diagnostic test.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
7
Figure 1: The screening pathway
Antenatal screening for Down syndrome and other conditions
Provision of information
Initial discussion
Offer of screening
about screening
First visit
End of screening
Screening declined
Screening accepted
process
Sc
reenin
g
First trimester combined
Second trimester combined
screening accepted
screening accepted
• Less than 13 Weeks 6 Days Pregnant
• 14–20 Weeks Pregnant
OR
• Blood test (2 maternal serum markers)
• Blood test (4 maternal serum markers)
• NT scan
Laboratory algorithm
generates risk report
Results to health
practitioner
Low risk result
Increased risk
received
result received
Offer of specialist referral
following increased risk result
Continue with
management
of pregnancy
Specialist referral
Specialist referral
Di
declined
accepted
agno
stic
Offer of diagnostic
testing
Offer of diagnostic
Offer of diagnostic
testing declined
testing accepted
No condition
Condition identified.
identified
Referral as appropriate
8
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
 5. Documentation
5. Documentation
Clear documentation of the screening process must be kept in the clinical records
including the discussion, consent or decline of tests or referrals and results of
screening.
Details of discussions and decisions must be documented by the health practitioner in
the clinical records. Signed consent for antenatal screening for Down syndrome and
other conditions is not required by the Code of Health and Disability Services Consumers’
Rights.
Clinical Records
Guidelines
Information
Health practitioners must document
Each stage of the screening process should be
discussions and decisions in the clinical
documented in the clinical records including:
notes.
> the content of discussions with the woman
> the use of interpreters or other services
> consent or decline for screening and
procedures or further testing
> details of results, follow up or referral
> discussions with the woman on results
received
> other support, resources or information
offered or provided.
Health practitioners who are referring
Referral information should include:
or handing over care to another health
> consent or decline for screening
practitioner must provide appropriate
> details of screening tests ordered
documentation.
> results of screening
> any follow-up from screening results
> any relevant family history
> referrals made to other services.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
9
 6. Informed choice –
consent or decline
Women who are less than 20 weeks pregnant must be advised about the availability
6. Informed choice –
consent or decline
Women who are less than 20 weeks pregnant must be advised about the availability
of antenatal screening for Down syndrome and other conditions.
Antenatal screening for Down syndrome and other conditions is optional for
pregnant women.
The right to decline screening, decline tests or further investigations should be made
clear by the health professional and any such decision by the woman, including
withdrawal of consent, must be respected.
Informed choice for this screening must include a discussion about the screened
conditions and the decisions that may need to be made as a result of participation
in this screening.
Up-to-date information about antenatal screening for Down syndrome and other
conditions must be provided to support the screening offer, thus enabling women
to make an informed decision whether to accept or decline.
No single test checks for everything. No screening test finds all cases of a condition.
Ensuring women make an informed decision about antenatal screening for Down
syndrome and other conditions is a legal requirement under the Code of Health and
Disability Services Consumers’ Rights that is central to best practice in maternity care.
Participation in antenatal screening for Down syndrome and other conditions is entirely
the woman’s choice. The woman also has the option to accept or decline further testing or
referrals within the screening pathway. For instance, a woman may decline first trimester
combined screening, but later change her mind and accept second trimester screening. All
choices that the woman makes must be respected and supported by health practitioners
providing her care.
10 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
Information to Women
Guidelines
Information
Health practitioners must advise women about
The discussion of screening must be made
the availability of antenatal screening for
with sufficient information, advice and time to
Down syndrome and other conditions which
enable women to make an informed decision.
is available to all pregnant women under 20
The discussion with women should be initiated
weeks gestation.
by the health practitioner as early as possible
in the pregnancy, to allow the opportunity to
ask questions, seek further information and
consider participation.
Women should be informed that only one
screening option will be publicly funded in
each pregnancy. Only one risk result will be
issued.
Women should be informed that screening
provides a risk estimate and not a definitive
result.
Some women may wish to discuss their
options with family/whãnau.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
11
Informed Consent or Decline
Guidelines
Information
Health practitioners must provide up-to-date,
Information should include the Ministry
balanced information about the screened
of Health consumer pamphlet
Antenatal
conditions.
screening for Down syndrome and other
conditions: optional screening – your choice,
Health practitioners must ensure women are
your decision.
aware this screening is optional.
Discussion about screening should include
Health practitioners must respect and support
that there may be unexpected findings. Refer
all screening choices the woman makes.
to Appendix 2 for more details.
Informed consent is a process that must occur
throughout the screening pathway.
Ensuring informed choice includes:
> provision of information about screening
> offering screening in a non-directive manner
> discussions about screening before and
during the screening process
> discussions about options following an
increased risk screening result
> giving sufficient time to consider options
> documenting discussions and consent or
decline to screening
> assuring the woman that whatever choice
she makes will be supported.
Communication
Guidelines
Information
Health practitioners must answer questions
Women should be given the opportunity to ask
women ask regarding screening.
questions about this screening and advised
where they can find further information.
Health practitioners may need to seek advice
from other sources to assist them to answer
questions from women for example from
screening laboratories, radiology practices,
obstetricians, paediatricians, Genetic Services
and/or maternal fetal medicine specialists.
12 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
Communication continued
Guidelines
Information
Health practitioners should give women time
Health practitioners should be cognisant of the
to reflect and consider decisions.
important implications for pregnant women
when screening is discussed.
Where there is a history of pregnancy problems
and/or genetic conditions in the family,
women may have given careful thought to how
they want to proceed with this pregnancy.
A woman’s decision whether or not to consent
to screening will depend on her personal
values and beliefs and the information
available to her.
Women will have a range of different views
that may change over time. Some women are
very clear what choices they may make if a
condition is confirmed and others are not.
This screening (and the implications of
screening) involves complex ethical issues
and women may want to explore these before
giving consent to begin screening or to
continue screening.
For some women, screening is an opportunity
to have information that enables them to
choose the care and management of their
pregnancy and birth. Screening and diagnostic
testing can inform the choice of location for the
birth, for instance a tertiary unit with specialist
care.
Women may wish to consider the choices
following an increased risk result. This may
include a discussion about:
> diagnostic testing including the risks
> what a positive diagnostic result may mean
for her.
If a woman does not wish to know further
information about the pregnancy then she may
choose not to have screening.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
13
Screened Conditions
Guidelines
Information
Health practitioners must discuss the
Conditions include:
conditions that may be indicated as a result
> risk estimates for trisomy conditions:
of participation in this screening.
> T21 (Down syndrome)
> T18 (Edwards syndrome)
> T13 (Patau syndrome)
> other rare genetic conditions for example:
> Smith-Lemli-Opitz
> Turner syndrome
> Triploidy
All the conditions above will require diagnostic
testing for confirmation.
Pregnancy conditions associated with poor
placentation including:
> stillbirth
> miscarriage
> growth restriction
> preterm birth
> pre-eclampsia.
The ultrasound scan may show structural
anomalies for instance:
> cardiac
> neural tube
> renal
> central nervous system.
The ultrasound scan may also suggest
a growth anomaly.
The conditions above require referral as
appropriate.
As with any medical test, there is a chance
that other conditions may be unexpectedly
identified and a recommendation for further
discussion with a specialist may be made.
Screening is not able to detect all conditions
that may be present.
The results will provide a risk estimate for T21,
T18 and T13 as well as incidental findings.
Further advice can be obtained from the
laboratory if required.
14 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
Screened Conditions continued
Guidelines
Information
Health practitioners must discuss with the
The 18 to 20 week anatomy scan is not
woman that the 18 to 20 week anatomy scan is
included in this screening, however, it may
another screening test.
identify potential markers for one of the
screened conditions.
A thorough family history should be taken and where there is a family history of a
genetic condition, a referral for a discussion with a specialist obstetrician or genetic
service should be offered prior to screening.
Family History
Guidelines
Information
Health practitioners must discuss and
If a woman has previously been pregnant with
document family history with the woman and
or has had a child with a genetic condition,
advise the laboratory of any relevant details.
or a family history of a genetic condition, they
may have a different risk status.
Appropriate family history questions (on both
sides of the family) may include:
> previous recurrent miscarriage
> previous pregnancy loss (still birth or
neonatal death)
> fetal or childhood abnormalities (for example
neural tube defects)
> developmental delay in other children
> any genetic conditions including childhood
diseases, cystic fibrosis, muscular dystrophy
or neurodegenerative conditions.
The practitioner may wish to consult with
Genetic Services prior to determining a
management plan.
It may be appropriate that the woman is
offered a referral to a specialist obstetrician or
specialist medical maternity service or Genetic
Services.
Health practitioners should exercise particular
sensitivity and be aware that women may have
already given careful thought to having or not
having screening or diagnostic testing.
A referral form for Genetic Services is available at www.nsu.govt.nz
Genetic Services
Phone Number
Northern and Midland Region
0800 476 123
Central and Southern Region
0508 364 436
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
15
6.1 Initial discussion
The discussion should include the following information.
(a) Screening information
> purpose of screening
> screening options available and what screening involves
> screened conditions
> detection of structural anomalies on the NT scan
> screening does not cover every condition
> incidental information may be found relating to the pregnancy or baby
> recommended timing for screening
> screening pathway and the decision points and options for screening
> screening provides a risk estimate only and is not diagnostic
> a further test would be required to determine whether a condition is present
> reliability of screening
> which tests may incur charges
> further information about the baby may be identified at the 18 to 20 week anatomy scan.
(b) Resources
> the consumer resource,
Antenatal screening for Down syndrome and other conditions:
Optional screening – your choice – your decision should be given at this time.
(c) Consent
> screening is optional and a woman may choose to participate or not participate in first
or second trimester screening and change her mind about this decision
> the woman may choose to participate in second trimester screening having declined
the offer of first trimester combined screening
> women who choose not to participate in screening will not have their maternity care
affected in any way
> if screening shows an increased risk result, diagnostic testing will be offered.
(d) Results
> how results are notified
> women will receive one risk result for first trimester combined screening combining
NT scan measurements and serum markers
> when screening results are available
> the screening will provide an increased or low risk result and may also indicate other
anomalies through ultrasound or serum markers
> for every 1000 women screened, about 50 will receive an increased risk result and 2
will be diagnosed with a baby with Down syndrome or another condition
> woman’s preference for receiving her results.
(e) Data and information collection and monitoring
> information and data is collected and securely stored
> information is used for monitoring and quality improvements of this screening
> that this screening is monitored at a national level including monitoring and
evaluating pregnancy and birth outcomes
> Monitoring reports or any public information will present summary information only
and will not be identifiable.
16 Antenatal screening for Down syndrome and other conditions: Guidelines for health practitioners
 7. The screening tests
7.1 Timing of first trimester combined OR
second trimester maternal screening tests
First trimester combined screening should be completed between 9 weeks and
7. The screening tests
7.1 Timing of first trimester combined OR
second trimester maternal screening tests
First trimester combined screening should be completed between 9 weeks and
13 weeks 6 days gestation. THE RECOMMENDED TIMING FOR THE BLOOD TEST IS
9 TO 10 WEEKS AND FOR THE NT SCAN AT 12 WEEKS.
Second trimester maternal serum screening should be completed between
14 weeks and 20 weeks gestation. THE RECOMMENDED TIMING FOR THIS TEST IS
14 TO 18 WEEKS.
Figure 2 shows when the different antenatal screening tests for Down syndrome and other
conditions may be undertaken.
Figure 2: Timing of first trimester combined screening and second trimester serum
screening
First trimester combined screening
Second trimester maternal serum screening
9 weeks to 13 weeks 6 days
14 weeks to 20 weeks
9W
10W
11W 12W
13W
6D 14W
15W
16W
17W
18W
19W
20W
Recommended
Recommended timing for
timing for
maternal serum markers
maternal
14 – 18 weeks
serum
markers
9 – 10 weeks
Recommended
timing for NT scan
12 weeks
Antenatal screening for Down syndrome and other conditions: Guidelines for health practitioners
17
7.2 Ordering tests
If a woman accepts screening, the health practitioner (midwife or doctor) will complete the
screening request form.
Eligibility criteria for publicly funded services can be found at www.moh.govt.nz
First Trimester Screening
Guidelines
Information
Health practitioners should inform women
For first trimester combined screening, health
where they can go for their blood test and NT
practitioners must ensure the woman knows
scan and the timing of each of these tests for
there are two components, blood test and
first trimester combined screening.
ultrasound scan, and she needs to have each
within certain timeframes.
Referrals for the NT ultrasound must be made
in accordance with Section 88 of the New
The woman is usually required to make a
Zealand Public Health and Disability Act 2000.
co-payment for the NT scan.
Second Trimester Screening
Guidelines
Information
Health practitioners should inform women
Second trimester serum screening is fully
where they can go for the blood test and
funded for eligible women.
the timing of the test for second trimester
screening.
7.3 Completing the screening request form
The health professional requesting screening must fill in all sections of the screening
request form to ensure an accurate risk assessment.
Screening Request Form
Guidelines
Information
The screening request form must be completed
All information requested on the laboratory
with all the requested information.
request form is needed by the laboratory to
ensure high quality testing. Screening results
may be inaccurate if the information on the
screening request form is not completed.
The current screening request form is a carbon copy, with the duplicate copy to be used for
NT scan requests. Figure 3 provides further explanation.
From time to time, the screening request form format may change, however, the
information required for accurate risk assessment will stay the same.
18 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners

Two laboratories perform antenatal screening for Down syndrome and other conditions.
LabPLUS (Auckland District Health Board) are responsible for screening women from
Taupo north. Canterbury Health Laboratories (Canterbury District Health Board) are
responsible for screening women south of Taupo.
Laboratory contact details for enquiries and screening request form orders:
Laboratory
Phone Number
LabPLUS
0800 LABPLUS (0800 522 7587)
Canterbury Health Laboratories
0800 THE LAB ( 0800 843 522)
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
19
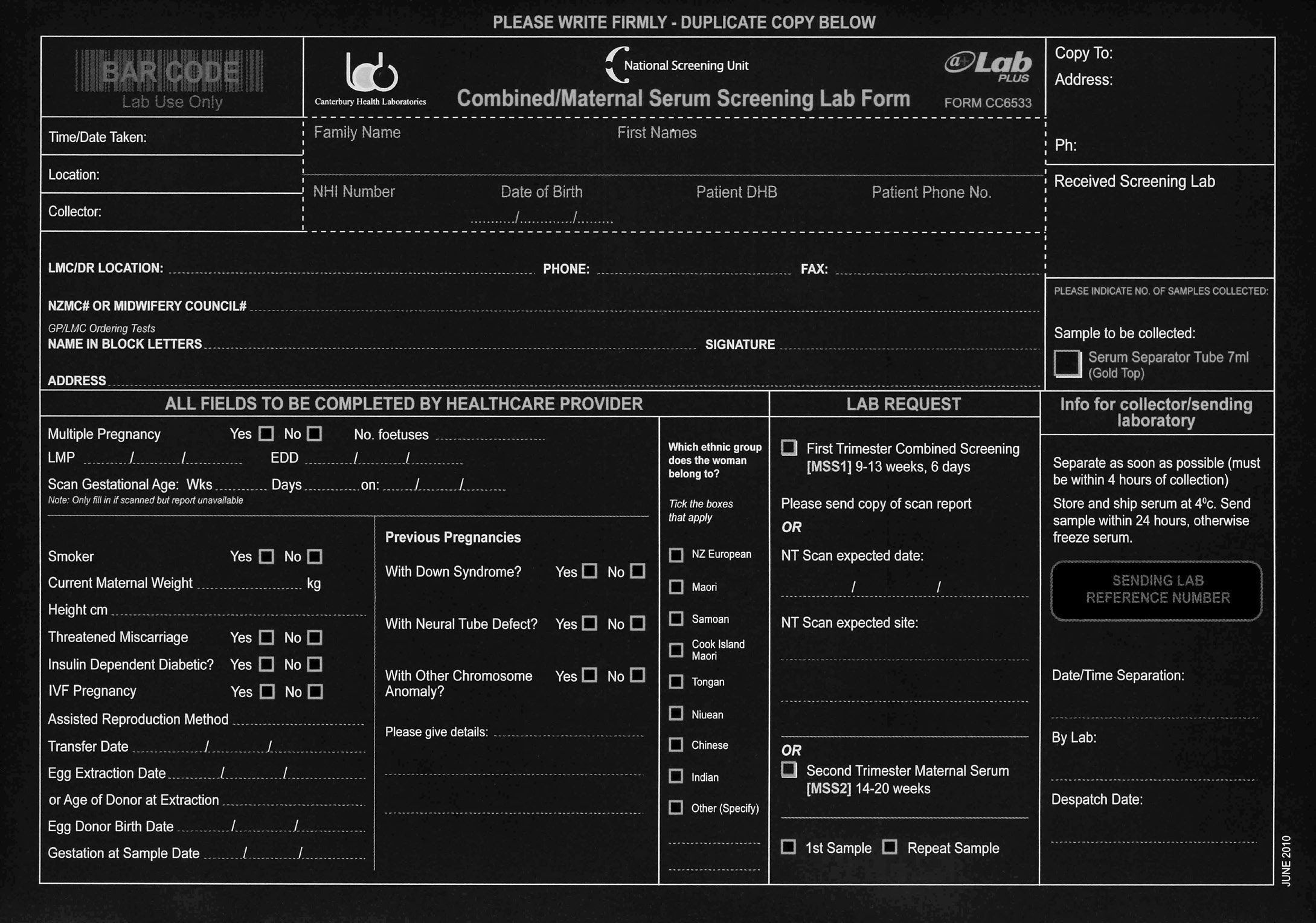 Figure 3: The screening request form
i
a
gg
h
b
f
c
d
e
a Multiple pregnancies
Figure 3: The screening request form
i
a
gg
h
b
f
c
d
e
a Multiple pregnancies: serum analyte levels come from the baby and placenta so will differ for multiple pregnancies.
b Smoking: affects placental function and serum analyte levels. The default if not provided is a non-smoker.
Weight: smaller women have higher serum analyte levels and larger women have lower serum analyte levels. This has a significant
c impact on the risk calculation.
d Diabetes: serum analyte levels differ for diabetic women.
Gestation and IVF: levels of serum analytes change through the pregnancy, so dating is important for accurate risk calculation.
e Essential information includes accurate gestation details including the method and age of the woman at the time of donation/
retrieval.
Previous pregnancy details: these are added into the risk calculation as they affect the chance of the current pregnancy. Add any
f relevant family history.
g Mother’s ethnicity: serum analyte levels vary with different ethnicities.
NT scan expected date and site: this relates to which practice the woman is most likely to go to for her NT scan.
h The laboratory will contact the radiology practice if they have not received an NT scan report by 13 weeks.
i Patient and health practitioner details: this section ensures the right patient is linked to the right result and sent to the right health
practitioner. Your phone number ensures you can be contacted to check details or provide results. Please provide alternative details if
you will be away.
20 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
 8. Receiving and
communicating results
A very high or very low level of the blood markers used in screening may indicate
8. Receiving and
communicating results
A very high or very low level of the blood markers used in screening may indicate
other conditions such as pre-eclampsia or pre-term birth. Fetal anomalies such as a
heart condition or structural defect may be found on ultrasound.
Screening for neural tube defects (NTD) can be reported after 15 weeks of pregnancy
using alpha fetoprotein (AFP) as the serum marker. It is noted that a better predictor
of NTD is the 18 to 20 week anatomy scan.
Blood samples are generally received by the screening laboratory two to three days after
collection. Screening results will be completed by the screening laboratory within three
business days after the receipt of the blood sample or scan information, whichever is
the later (if first trimester combined screening). Screening results include information
provided about the woman, details of the risks and recommendations.
The screening laboratory will send a report to the health practitioner if both parts of
screening (ie, NT scan and blood tests) have not been received by 13 weeks 6 days.
Receiving Screening Results
Guidelines
Information
The health practitioner is responsible for
It is useful to ascertain the woman’s
receiving screening results.
preference for receiving results at the time that
the screening offer is made.
The woman may wish to be accompanied by
family/whãnau or support person.
If the screening result is low risk the screening
laboratory will dispatch the result to the health
practitioner by mail or electronic means within
24 hours of the result being available.
If the screening result is increased risk the
screening laboratory will phone the health
practitioner within 24 hours of the result being
available. The result will also be dispatched to
the health practitioner by mail or electronically.
There are a number of situations where the
markers (both serum and the NT scan) may
indicate other conditions. Refer to Appendix 2
for further information.
If the screening result will indicate other
conditions, the screening laboratory will phone
the health practitioner within 24 hours of the
result being available.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
21
Preparing for Communicating Screening Results
Guidelines
Information
Health practitioners must communicate
Prior to communicating with the woman, the
results to women in an appropriate and timely
health practitioner should consider discussing
manner.
the result with the screening laboratory or
Genetic Services.
Communication to women needs to occur
through reliable methods such as face to face
or telephone, taking into account appropriate
timing (such as the need for timely referral or
follow up). Results or professional advice must
not be sent via a text message.
Consideration should be given to the timing of
giving results and whether access to timely support
services or further information is available (for
example on public holidays or Friday afternoons).
Health practitioners should be able to present
results in a clear and concise way to support
women in their decision-making. This includes
understanding statistical risk information.
It can be useful to communicate the risk result in
different ways to help women better understand
for example:
> ‘You have a 1 in 4 chance of…, or put another
way, you have a 25 percent chance of….’
> ‘You have a 1 in 20 chance of having a baby
with one of the conditions, this means there is
a 19 in 20 chance of having a baby without the
condition.’
Further information about the risk result can be
obtained from the screening laboratory.
The health practitioner should be prepared to
Discussion around the results may include:
discuss the results in detail and seek further
> the limitations of screening
information that supports them to inform
> that a low risk result means that the baby is
women what their screening results may mean.
unlikely to be born with one of the conditions
screened for, but it does not mean they will
definitely not be born with one of the conditions
(or another condition not indicated by screening)
> providing an opportunity for the woman
(and her family/whãnau) to ask questions
> providing information about other services,
including community support agencies the
woman (and her family/whãnau) can contact.
If a woman with a low risk result requests
diagnostic testing, a referral to a specialist
obstetrician may be made.
22 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
Communicating Increased Risk Results and Offering Referral
Guidelines
Information
Health practitioners must inform women
Consideration should be given to the timing
in a timely manner of all screening results
of giving results and whether access to timely
indicating an increased risk of Down syndrome
support services or further information is
or another condition.
available (for example, on public holidays or
Friday afternoons).
Anxiety following any increased risk result is
normal. Anxiety includes the stress and worry
experienced while waiting for decisions about
diagnostic testing, and the possibility of a
higher level of anxiety for the remainder of
the pregnancy.
If screening shows an increased risk of
a genetic condition, women may require
more information to enable them to make
an informed decision about the ongoing
management of their pregnancy; one which
they feel is best for themselves and their
families.
Sources of information and support are listed
in Appendix 1.
Document the discussion and management
plan in the clinical notes.
Provide the woman with a copy of the results if
requested.
Figures 4 and 5 provide an example of the screening reports produced by the laboratories.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
23
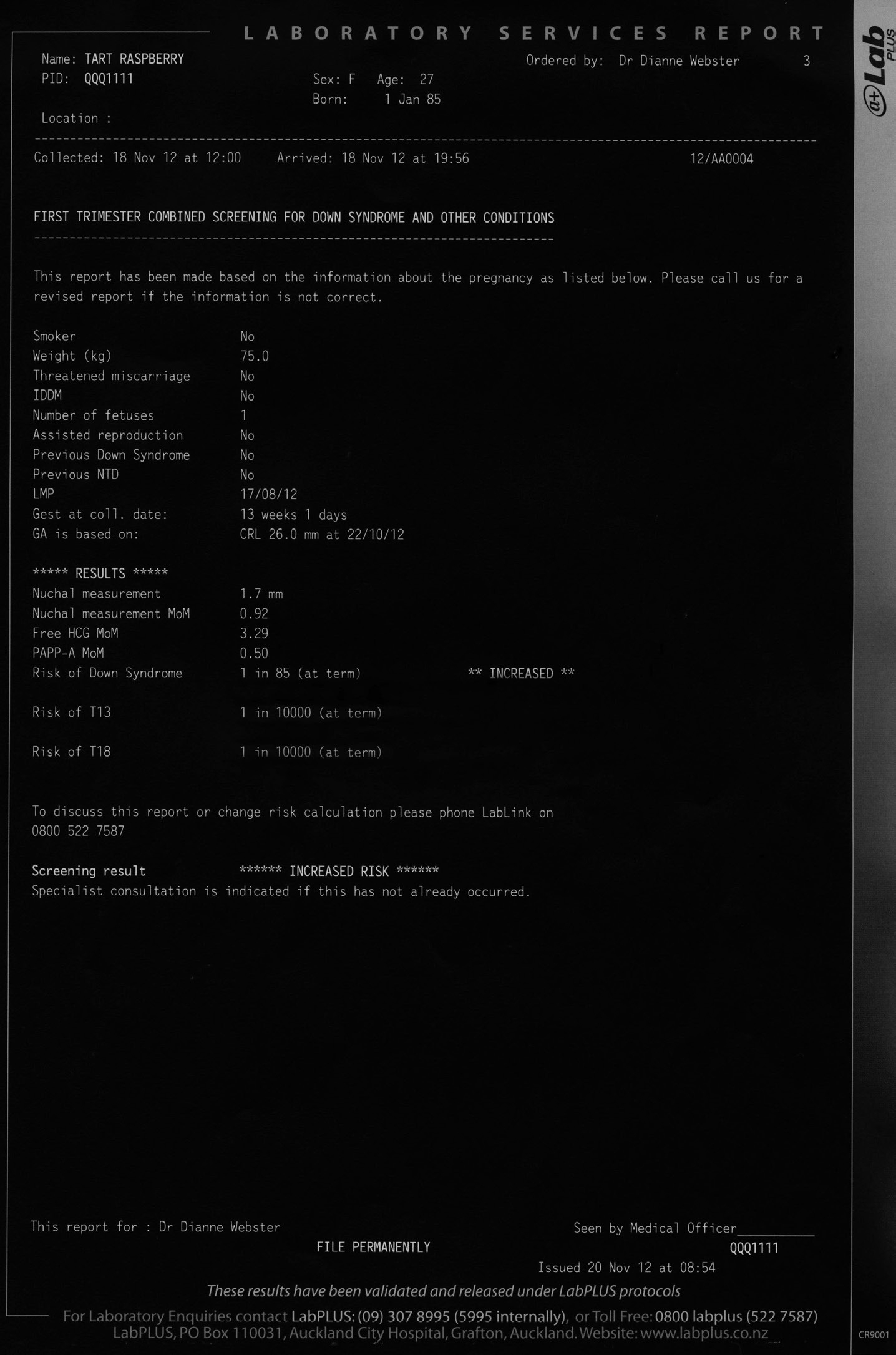 Figure 4: Example laboratory report: increased risk for Down syndrome
Figure 4: Example laboratory report: increased risk for Down syndrome
NHI and demographic
details of the patient.
Please check these
are correct.
Which trimester this
screening occurred in
The health practitioner
who ordered the test
This information is
(name on the request
based on what was
form), and who the
provided on the
result will be sent to.
request form. Please
check these are
correct.
The cut-off for
aneuploidy risk is
This is the results
1:300. This example
section. It details
report shows 1:85 which
the NT measurement
is an increased risk for
and MoMs for each
Down syndrome.
marker. It then
details the risk result
for the aneuploidies.
Note the ‘increased’
next to risk of Down
syndrome.
This is the summary
section detailing an
increased risk (relating
to the increased risk
for Down syndrome in
this example).
If any of the
woman’s details
are not correct or
the LMC has
any questions,
please contact
the laboratory
(LabPLUS or CHL).
24 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
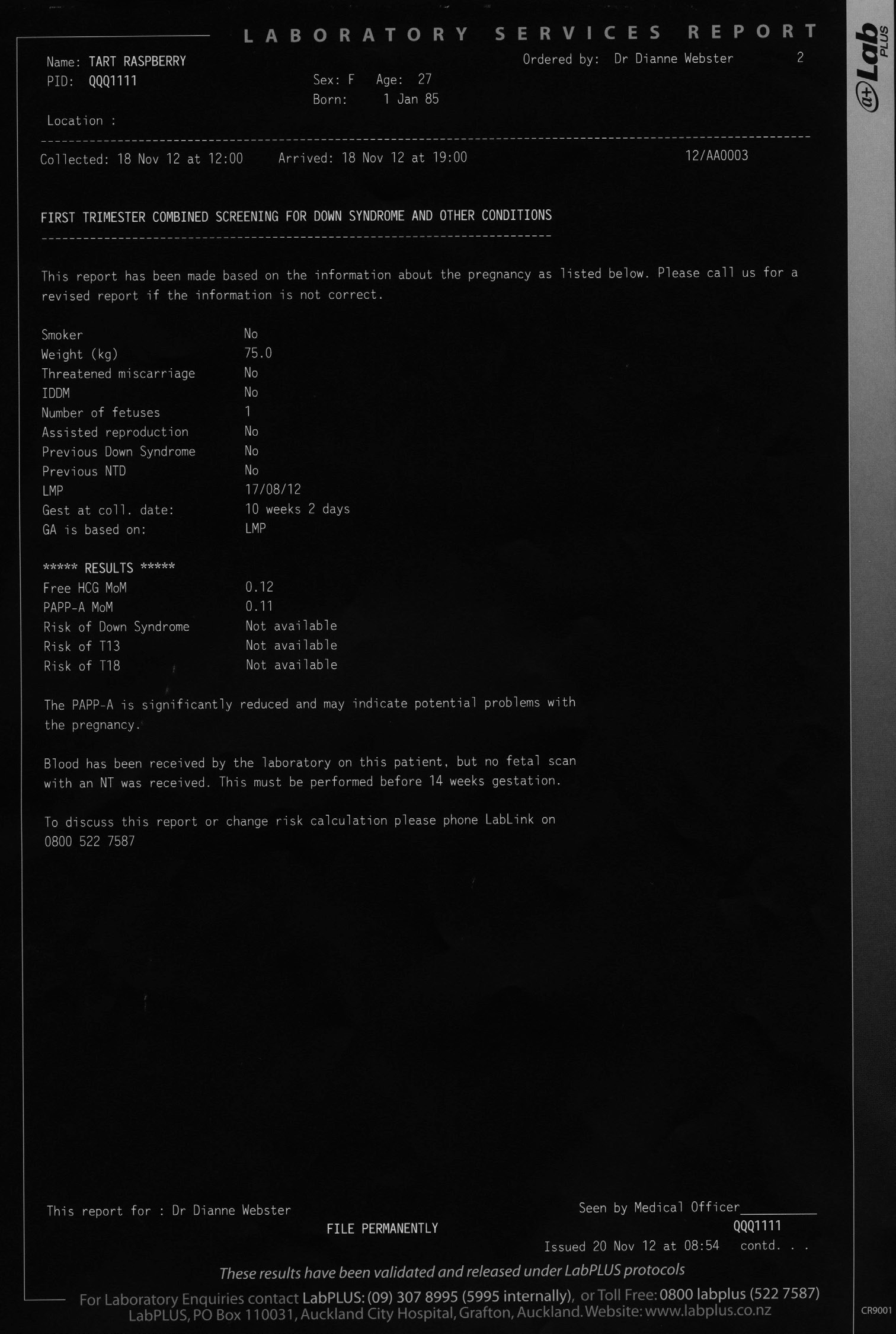 Figure 5: Example laboratory report: low PAPP-A (unusual analyte)
Figure 5: Example laboratory report: low PAPP-A (unusual analyte)
NHI and demographic
details of the patient.
Please check these
are correct.
Which trimester this
screening occurred in
The health practitioner
who ordered the test
(name on the request
This information is
form), and who the
based on what was
result will be sent to.
provided on the
request form. Please
check these are
correct.
This is the results
section. It details
the MoMs for
each marker.
In this example,
an NT has not yet
This is the summary
been received.
section showing the
The MoM for PAPP-A
very low PAPP-A result
is significantly
and that the NT scan
reduced. PAPP-A
has not been received
MoMs will be
by the laboratory.
reported as reduced
if they are less
than 0.2.
If any of the
woman’s details
are not correct or
the LMC has
any questions,
please contact
the laboratory
(LabPLUS or CHL).
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
25
Referral to Specialist
Guidelines
Information
Health practitioners must offer a timely referral
Following an increased risk result a woman
to all women with increased risk results or
may be undecided about her next steps. She
unusual analytes.
may require further information from other
sources about:
> what the increased risk result may mean and
how it may affect the on-going management
of the pregnancy and birth
> the difference between treatable conditions
(for instance heart defects) and non-treatable
conditions (for instance trisomy 13).
The referral should include details of:
> gestation
> screening results
> any issues identified which require further
discussion
> any relevant family history.
A referral to Genetic Services may provide the
opportunity to gather information to make
or confirm a diagnosis of a genetic disorder.
Other referrals may also be considered. These
include:
> a paediatrician
> a health social worker
> a counsellor.
The woman may wish to seek further
information from sources listed in Appendix 1.
The woman must be given time to reflect and
to consider her decision.
Health practitioners must make clear the
The provision of links to community
woman’s right to decline a referral following an
organisations to enable the gathering of more
increased risk result.
information and to access support may also be
helpful. These can be found in Appendix 1.
Health practitioners must respect and support
any decision made by the woman throughout
the screening process.
26 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
 9. Diagnostic testing
9. Diagnostic testing
Diagnostic testing includes a procedure to collect a sample of fetal cells either by
chorionic villus sampling (CVS) or amniocentesis. The sample collected is sent for
aneuploidy testing.
CVS can be performed from 11 to 14 weeks of pregnancy but is typically performed
between 10 and 13 weeks. CVS is only offered in a few centres. CVS results may take one
to three weeks.
Amniocentesis can be performed between 15 and 20 weeks. Amniocentesis results may
take one to three weeks.
A more detailed scan may be required following an abnormal finding on ultrasound or
from unusual analytes or positive NTD screen.
Diagnostic testing is publicly funded for women who have:
> an increased risk result
> an abnormal ultrasound scan (structural abnormalities)
> previously had a baby with a congenital anomaly
> maternal anxiety
> a family history of Down syndrome and/or other conditions, if recommended by Genetic
Services.
International best practice does not support direct referral to diagnostic testing based on
maternal age alone.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
27
Diagnostic Testing
Guidelines
Information
Health practitioners must provide information
Health practitioners should outline the
on diagnostic testing and inform the woman
following choices the woman has available:
that diagnostic testing is optional.
> whether or not to accept a referral and
diagnostic testing
> referral to another service for example a
paediatrician, Genetic Services, health social
worker or counsellor.
The health practitioner must explain:
> what information the diagnostic tests can
provide
> the risks associated with a diagnostic test
> the decisions that the woman may need
to consider
> the anxiety that may be experienced while
waiting for results and possibly for the
remainder of the pregnancy
> the support services that can be accessed.
Fetal cells can be analysed in a number
of ways.
There is an option of more rapid tests which
can provide a result in 24 to 48 hours. These
tests are accurate but do not test for as
many abnormalities as other testing. Further
information is available from the laboratories.
A charge may apply for these tests.
If diagnostic testing is undertaken, the sample
can be used for chromosome testing and
for other specific genetic tests that may be
indicated in the family history. These will need
to be specified on the diagnostic testing form
sent to the cytogenetics laboratory.
28 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
Diagnostic Testing continued
Guidelines
Information
Health practitioners must inform women of the
The risk of miscarriage after amniocentesis
risk of diagnostic testing procedures.
is about one miscarriage in every 100–200
women tested.
The risk of miscarriage after CVS is about one
miscarriage in every 50–100 women tested.
Other rare complications include:
> leaking of amniotic fluid from the vagina
> infection of the uterus or fetus
> some research has suggested that
development of arms, fingers, legs or toes
may be disrupted if CVS is performed before
nine weeks gestation: for this reason, a CVS
procedure is done after 10 weeks gestation.
> development of Rhesus factor
incompatibility. All women who have Rh-
negative blood group are given an injection
of anti-D to prevent this complication.
Specialist obstetricians who are performing
If diagnostic testing is undertaken, the sample
diagnostic testing must specify the genetic
can be used for chromosome testing and
tests required on the diagnostic testing form.
for other specific genetic tests that may be
This may include requests due to familial
indicated in family history. These will need to
conditions.
be specified on the diagnostic testing form
sent to the cytogenetic laboratory.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
29
Receipt of a Positive Result Following Diagnostic Testing
Guidelines
Information
The health practitioner must explain the
Health practitioners can seek further
meaning of any test results and provide
information from the cytogenetic laboratory
information about any diagnosis.
or other sources as required.
See Appendix 2 for more information on the
conditions.
Women may wish to have time to consider the
results and what they may mean for her and
her baby.
After receiving the results of the diagnostic
The following could be discussed:
test, health practitioners should support
> information about the condition
women to make an informed decision.
> options available which include:
Health practitioners must support the woman’s
> continuing with the pregnancy
decision.
> termination of the pregnancy.
If the woman chooses to continue with the
pregnancy, the options for antenatal care such
as specialist care and support, and postnatal
options should be discussed. If the baby
has a condition which has a very short life
expectancy, consideration should be given to
offering antenatal or postnatal palliative care
for the baby and counselling services to the
women (and her family).
Women may need to be provided with support,
which may include access to groups in
Appendix 1.
Health practitioners must provide women with
This may include referral to a:
opportunities to access additional information
> paediatrician
and support.
> health social worker
> Genetic Services
> counsellor.
The woman and/or her family/whãnau
may seek information from sources listed
in Appendix 1 to find out what living with
a specific condition may mean.
Written resources for example,
Living
With Down and web links are available
(see Appendix 1).
30 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
 10. Genetic services and
other referrals
Genetic Services
10. Genetic services and
other referrals
Genetic Services
Guidelines
Information
Health practitioners should advise women with
Staff from Genetic Services can provide
increased risk results about the availability of
information and support for families with,
Genetic Services.
or at risk of, a genetic disorder.
Referrals to Genetic Services should come
from the GP or LMC in the first instance. A copy
of the screening report should be included.
Initial discussions with the health practitioner
will be conducted with the cover (on call)
genetic associate.
If the health practitioner wishes a staff
member (genetic associate or clinical
geneticist) to subsequently talk to the woman,
this should be handled as a formal referral.
Please use the Genetic Services Referral
form available from the NSU website at
www.nsu.govt.nz/files/ANNB/Referral_form_
final120511.pdf
Genetic Services are physically located in
Auckland, Wellington, and Christchurch.
Telephone or in-person consultations will be
negotiated based on the woman’s location
and circumstances.
Any queries about the screening laboratory
analytical process and the result algorithm can
be referred back to the designated specialists
in LabPLUS and CHL.
Genetic Services
Phone Number
Northern and Midland Region
0800 476 123
Central and Southern Region
0508 364 436
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
31
 Other Referrals
Other Referrals
Guidelines
Information
Health practitioners must provide information
Health practitioners should find out about
about medical and non-medical services the
services in their area and how to access them.
woman may access to support her to make
Referrals may include:
decisions about the management of her
pregnancy.
> obstetrician
> specialist maternity services
> maternal fetal medicine specialist
> paediatrician
> general medical practitioner
> health social worker
> counsellor
> disability support services
> parent support groups.
Refer to Appendix 1 for resources and contacts.
32 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
 11. Nuchal Translucency
(NT) scan
11. Nuchal Translucency
(NT) scan
The NSU supports continual improvement in the quality of this screening initiative. This
includes working with the health sector to monitor and develop ultrasound screening
practices. Quality improvements will continue to evolve. This may result in changes in
delivery of service, monitoring and audit.
If the woman agrees to first trimester combined screening the ultrasound/radiology
provider would then complete the NT and CRL measurements and send the results to the
screening laboratory.
Referral for NT Scan
Guidelines
Information
Specialist medical maternity services,
This requires a written referral, stating the
including NT scans, may only be provided
clinical reason, either on the screening request
to women on written referral from another
form or radiology request form.
practitioner (midwife or doctor).
Risk Calculation
Guidelines
Information
The risk calculation will be performed by the
The two screening laboratories are LabPLUS at
screening laboratories.
Auckland District Health Board and Canterbury
Health Laboratories at Canterbury District
Health Board.
The screening laboratories use a single
database for risk calculation. This ensures
consistent risk calculation for all women across
New Zealand.
Discussions With Women
Guidelines
Information
Ultrasound/radiology providers
It is expected that practitioners may discuss the findings
may discuss the scan findings
of the NT scan with the woman, but will not calculate a risk
with the woman. However,
result.
ultrasound/radiology providers
In all but exceptional circumstances, the risk result will be
should not provide a risk
communicated to the woman by the referring practitioner.
assessment for Down syndrome
There may be very limited circumstances where the
and other conditions to the
radiology/ultrasound provider contacts the screening
woman based on NT alone (for
laboratory informing them of the NT and CRL measurements
example, 1:300 risk).
and requesting a risk assessment (if serum has already been
taken). This would generally be on the rare occasion where a
significant anomaly is found on the ultrasound scan.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
33
Reporting Requirements
Guidelines
Information
The following information from the NT scan
An NT scan is usually performed between
must be provided for this screening:
11 weeks 2 days and 13 weeks 6 days.
> National Health Index (NHI) number
For acceptance for first trimester combined
screening, at the time the NT scan is
> demographic information (DOB, name)
performed, the fetus must have a CRL between
> referrer’s name
45–84mm.
> date of NT scan
The CRL is used by the laboratory to determine
> the CRL measurement
gestational age from the Robinson equation
> the NT measurement
(see Appendix 3).
> multiple pregnancy (chorionicity and
Precise measurement of CRL and NT is
amnionicity)
essential in the interpretation and final risk
> other details that may inform the risk
assessment provided to the pregnant woman.
calculation
The combined screening test is highly
> significant abnormalities which may change
sensitive to errors in CRL measurement and
the management of the pregnancy
NT measurement.
> name of the practice
The name of the scanning practitioner in
> name of the radiologist
addition to the reporting radiologist or
> name of the practitioner performing the scan.
obstetrician on the report will provide audit
at an individual level.
Best practice report templates can be found
at www.nsu.govt.nz
Nasal Bone Assessment
Guidelines
Information
Nasal bone will be included in the risk
Nasal bone assessment is not currently
calculation if it is reported to the screening
required to provide a risk result for first
laboratory at the same time as the NT
trimester combined screening.
measurement.
When an NT measurement is provided to
the screening laboratory and a risk has
been issued, no further risk calculation will
be done if the nasal bone is assessed at a
subsequent scan.
Nasal bone is to be reported as:
If a result states that a nasal bone is
> not looked for
hypoplastic, this will not be included in the
risk calculation.
> present
> absent
> not able to be visualised for technical
reasons
34 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
CRL Out of Range for First Trimester Combined Screening
Guidelines
Information
If the CRL is greater than 84mm, the
For first trimester combined screening, the CRL
ultrasound/radiology provider is to inform the
should be between 45 – 84mm. Where the CRL
woman that the fetus is outside the range for
is greater than 84mm, the fetus is outside the
first trimester screening and an NT scan cannot
range for first trimester combined screening.
be completed. The ultrasound/radiology
provider will refer the woman back to her
health practitioner for other options including
second trimester maternal serum screening.
Specialist Referral Following Abnormal NT
Guidelines
Information
If an NT scan shows an obvious anomaly,
The referring health practitioner should offer
for instance structural/anatomical anomaly,
the woman referral to a specialist obstetrician.
the radiologist should:
(a) inform the referring health practitioner in
a timely manner;
(b) provide information to the woman at the
time of the scan.
NT Greater Than 3.5 mm
Guidelines
Information
If the NT scan shows a NT measurement greater
The referring health practitioner should offer
than or equal to 3.5mm, the ultrasound/
the woman referral to a specialist obstetrician,
radiology provider should communicate with
with the expectation she will be seen in a
the referring health practitioner to discuss the
timely manner.
scan results.
Completion of first trimester combined
screening is still recommended. This will assist
the specialist to develop a care pathway with a
full clinical picture.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
35
NT for Twins
Guidelines
Information
For twin pregnancies, an NT and CRL for each
The screening laboratory uses CRL to date
fetus must be measured at the same time to
the pregnancy and hence calculate the marker
ensure accurate risk assessment.
MoMs. Both NT measurements should be
made at the time of the CRL measurements.
If they are different in twins, the larger will
be used.
Any information that may assist risk calculation
for each fetus should be included in the report
to the screening laboratory.
If an NT measurement is only able to be
completed on one twin, a subsequent NT scan
must include NT and CRL for both fetuses
(if more than 2 days has elapsed).
Transmitting Scan Results to the Screening Laboratories
Guidelines
Information
Ultrasound/radiology providers will transmit
Ultrasound/radiology providers are to have a
copies of the report results in a timely
system in place to send the ultrasound report
manner direct to LabPLUS for Taupo north or
to the screening laboratory and to confirm the
Canterbury Health Laboratories (CHL) for south
report has been sent.
of Taupo.
Loss of One Twin
Guidelines
Information
For pregnancies where one twin has died,
If the NT scan identifies a sac showing fetal
a NT and CRL measurement is to be sent to
demise, it is possible that there could be a
the screening laboratory and will be used to
contribution to the maternal biochemical
calculate the risk assessment without serum
markers for many weeks. Therefore, serum
levels.
analytes are not used to calculate a risk
assessment. The screening laboratory will
provide a risk assessment based on NT without
biochemistry.
NT for Multiple Pregnancies – Triplets or Greater Multiples
Guidelines
Information
For pregnancies with three or more fetuses,
The screening laboratory software is not able
an NT alone can be used for risk assessment.
to provide a risk assessment for pregnancies
where there are triplets or greater multiples.
36 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
The NSU supports International Accreditation New Zealand (IANZ) radiology
accreditation. This occurs for the majority of practices around New Zealand and provides
assurance that the practice operates to established standards.
Individual Certification and Standards Requirements
Guidelines
Information
Practitioners must follow the requirements of
The NSU recommends radiology practices have
Section 88 of the New Zealand Public Health
IANZ accreditation. The NSU is developing
and Disability Act 2000.
initiatives to audit and monitor individual
operators.
Practitioners should follow the standards of
practice for diagnostic and interventional
In New Zealand, the quality of service
radiology (version 9.1) of the Royal Australian
requirements relates to appropriate education
and New Zealand College of Radiologists.
and training for the measurement of NT.
Appropriate certification is recognised through
Practitioners should follow the statements
FMF London and the Australian Nuchal
from the Royal Australian and New Zealand
Translucency – Ultrasound, Education and
College of Obstetricians and Gynaecologists.
Monitoring Program.
Practitioners should follow the requirements
Further policies and statements on fetal
of ASUM.
ultrasound can be found at:
www.ranzcog.edu.au
www.ranzcr.edu.au
www.asum.com.au
www.fetalmedicine.com
While ultrasound/radiology providers are no
longer required to provide the risk calculation
for women, the requirements of ultrasound
practitioners providing services remain
unchanged. This means ongoing participation
in certification and audit programmes
continues to be a requirement.
Nasal Bone Certification
Guidelines
Information
Practitioners assessing nasal bone must be
Nasal bone evaluation requires additional
certified for the assessment of nasal bone.
certification over and above that for NT
assessment. The certification is provided
by the FMF programme.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
37
 12. Screening laboratory
processes
Reporting Information to the Health Practitioner
12. Screening laboratory
processes
Reporting Information to the Health Practitioner
Guidelines
Information
The screening laboratory must provide a first
The screening laboratory report must include:
trimester combined screening or second
> screening result (‘increased risk’ or ‘low risk’)
trimester maternal serum screening result
> multiple of the median (MoM) of each
to the health practitioner who referred the
analyte
woman for screening, by electronic means
and/or hard copy reporting.
> NT measurement and MoM
> individual risk assessments for:
> trisomy 21 (Down syndrome)
> trisomy 18 (Edwards syndrome)
> trisomy 13 (Patau syndrome)
> neural tube defects (after 15 weeks).
The screening laboratory report may include
other information, for example that specialist
obstetric referral is recommended, that a rare
genetic disorder is indicated or that the marker
levels indicate other problems.
The screening cut-off is 1:300 for aneuploidies.
Provision of Specialist Laboratory Advice
Guidelines
Information
The screening laboratory must provide
The screening laboratory will phone all
specialist laboratory advice to the health
increased risk results and abnormal analyte
practitioner, when requested.
results and discuss these with the health
practitioner.
The screening laboratory must ensure
that health practitioners have screening
Health practitioners are welcome to contact
information required to inform women of their
the screening laboratory if required.
screening results.
38 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
Incomplete Screening
Guidelines
Information
The screening laboratory will provide a report
The screening laboratory will inform the
to the health practitioner when a blood sample
health practitioner if the NT scan has not been
for first trimester combined screening has
received.
been received, but no NT or CRL measurement.
The screening laboratory will advise the health
practitioner to contact the woman about the
need to have her scan performed before 13
weeks 6 days for a first trimester combined
screening risk assessment to be possible.
If the scan has not been performed by 13
weeks 6 days, the screening laboratory will:
> issue a report to the health practitioner that
provides the MoMs of the serum analytes only
> advise that first trimester combined
screening cannot be completed because
the scan data was not available
> recommend that the woman is offered
second trimester maternal serum screening.
The health practitioner should advise the
woman that first trimester combined screening
has not been completed and provide her with
information about second trimester maternal
serum screening.
The screening laboratory will advise the
The screening laboratory will accept a CRL of
health practitioner if first trimester combined
45–84 mm. If the result is above 84mm, the
screening cannot be completed because the
screening laboratory will advise the health
CRL is above 84mm.
practitioner that the woman is in the second
trimester.
If the blood has also been taken in the second
trimester, second trimester screening will be
performed.
If the blood has been taken in the first
trimester, the health practitioner will be
informed that first trimester combined
screening cannot be completed and provide
her with information about second trimester
maternity screening.
The screening laboratory will indicate on the
reports the dating used to calculate the risk.
Preference will be given to CRL or BPD over LMP.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
39
Further Serum Received
Guidelines
Information
The screening laboratory will advise the health
The screening laboratory will advise the health
practitioner if a serum sample has been
practitioner that a risk result has already been
received after a result has already been issued.
provided and a further result will not be issued
unless there are clinical indications. The
health practitioner must phone the laboratory
to discuss as required. Decisions regarding
recalculating risk assessments will be made on
a case by case basis.
Laboratory
Contact Details
Contact Details
LabPLUS
www.labplus.co.nz
Taupo and North (Northland,
Phone: 0800 LABPLUS (522 7587)
Waitemata, Counties Manukau,
Auckland, Waikato, Lakes and
Lead Clinical Scientist:
Bay of Plenty)
Dr Dianne Webster
[email address]
Canterbury Health
www.chl.co.nz
South of Taupo (Tairawhiti, Hawkes
Laboratories
Phone: 0800 THE LAB
Bay, Whanganui, Taranaki, Mid
(843 522 x 80484)
Central, Wairarapa, Capital & Coast,
Hutt Valley, Nelson Marlborough,
Chemical Pathologist:
West Coast, Canterbury, South
Dr Richard MacKay
Canterbury, Southern)
[email address]
40 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
 13. Data, information
and monitoring
13.1 Data and information collection
13. Data, information
and monitoring
13.1 Data and information collection
Antenatal screening for Down syndrome and other conditions collects, creates and retains
indefinitely the following data and information. Table 2 outlines what information is
collected.
Table 2: Data and information collected for antenatal screening for Down syndrome and
other conditions
Information About the Woman Sample Data
Health Practitioner Data
as Collected on the Request
Form
> name (in full)
> date and time of samples/
> name
> National Health Index (NHI)
scans
> midwifery/medical council
number
> collection and screening
number
> date of birth
laboratory assigned ID#
> radiology practice and
> gestation at time of
> screening results
practitioner
sampling
> diagnostic results and
> telephone numbers
> ethnicity
outcomes
> address
> weight
> information about what
has been reported and to
> information about the
whom including any clinical
pregnancy
information provided
> estimated date of delivery
> relevant family history
This data and information is held indefinitely by the screening laboratories on behalf of
the National Screening Unit.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
41
13.2 Uses of data and information
Only authorised personnel have access to the identifiable information and data for the
purposes of screening, quality assurance, monitoring and evaluation.
Data and information is collected and held securely to:
> interpret screening results
> make sure that results can be provided to health practitioners
> monitor and evaluate this screening including the results of diagnostic testing and
outcomes of pregnancies.
Data and information may also be used in research studies.
From time to time, there may be requests for screening data. This may include data requests
for research or other requests from individuals, committees, groups or organisations.
Any requests regarding this data must be forwarded to, and authorised by, the National
Screening Unit. The data access request form can be found at www.nsu.govt.nz
Data Requests
Guidelines
Information
All requests for screening data must be
To maintain consistency, all screening data
forwarded to, and authorised by, the National
requests will be managed by the National
Screening Unit.
Screening Unit. This includes data requests for
research, or from other individuals, committees,
groups or organisations.
13.3 Monitoring
Antenatal screening for Down syndrome and other conditions is overseen by the National
Screening Unit of the Ministry of Health. To maintain the quality of this screening, it is
closely monitored on a regular basis, with evaluation undertaken periodically. Monitoring
is dependent on the information collected as set out in Table 2 which includes the
numbers of screened women, practitioner information, results and outcomes (for instance
comparing screening results with diagnostic results or pregnancy outcomes).
The Ministry of Health publishes reports on this screening. These reports are summary
information only and do not contain identifiable data or information.
42 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
 Appendix 1:
Resources and contacts
Appendix 1:
Resources and contacts
Sources of further information and contact details for support services are listed here.
This list should be supplemented by the local or regional services within your own networks.
The National Screening Unit (NSU), of the Ministry of Health is responsible for oversight
of antenatal screening for Down syndrome and other conditions. The NSU produces
consumer and practitioner resources and audits and monitors this screening initiative.
The
consumer resource Antenatal screening for Down syndrome and other conditions:
optional screening – your choice, your decision can be downloaded in pdf form at www.nsu.
govt.nz Hard copies are available free of charge and can be ordered at www.healthed.govt.
nz or by contacting the Authorised Provider of Health Education Resources in your area.
A full list of who these are (by region) is at www.healthed.govt.nz/contact-us
These
practitioner guidelines can be downloaded from www.nsu.govt.nz Hard copies
are available from Wickliffe on (04) 496 2277, Ministry of Health Publications, c/- Wickliffe
Press, PO Box 932, Dunedin, or email [email address] Please quote Code: HP5409.
On-line education for health practitioners who provide services within the antenatal
and newborn screening programmes can be accessed at www.learnonline.health.nz
Consumer Questions and Answers and other support information can be found at
www.nsu.govt.nz
For questions or comments: [email address]
Mailing address: National Screening Unit
Private Bag 92522
Wellesley Street
Auckland
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
43
There are two Screening Laboratories. LabPLUS at Auckland District Health Board and
Canterbury Health Laboratories at Canterbury District Health Board.
Laboratory request forms can be ordered from the Screening Laboratories.
Laboratory
Contact Details
Contact Details
LabPLUS
www.labplus.co.nz
Taupo and North (Northland,
Phone: 0800 LABPLUS (522 7587)
Waitemata, Counties Manukau,
Auckland, Waikato, Lakes and
Lead Clinical Scientist:
Bay of Plenty)
Dr Dianne Webster
[email address]
Canterbury Health
www.chl.co.nz
South of Taupo (Tairawhiti, Hawkes
Laboratories
Phone: 0800 THE LAB
Bay, Whanganui, Taranaki, Mid
(843 522 x 80484)
Central, Wairarapa, Capital & Coast,
Hutt Valley, Nelson Marlborough,
Chemical Pathologist:
West Coast, Canterbury, South
Dr Richard MacKay
Canterbury, Southern)
[email address]
NZ Maternal Fetal Medicine Network www.nzmfm.health.nz
Genetic Services, New Zealand
Northern and Midland Region
Phone: 0800 476 123
Central and Southern Region
Phone: 0508 364 436
www.genetichealthservice.org.nz
Health and Disability Commissioner
www.hdc.org.nz/
Office of the Privacy Commissioner
www.privacy.org.nz
Ministry of Health
Primary Maternity Services Notice 2007
www.health.govt.nz
Other resources
New Zealand
Auckland District Health Board Management of Babies with Down syndrome
www.adhb.govt.nz/newborn/Guidelines/Anomalies/DownSyndrome.htm
ASUM www.asum.com.au
College of Midwives www.midwife.org.nz
44 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
CCS Disability Action
www.ccs.org.nz
Phone: 0800 227 200
IHC www.ihc.org.nz
Phone: (04) 472 2247
Kiwi Families Links to disability support articles
www.kiwifamilies.co.nz
Midwifery Council of New Zealand www.midwiferycouncil.health.nz
New Zealand Down Syndrome Association www.nzdsa.org.nz
Tel. 0800 693 724
Email: [email address]
New Zealand Federation of Disability Information Centres www.nzfdic.org.nz
New Zealand Organisation for Rare Disorders www.nzord.org.nz
Pacific Information Advocacy Support Services www.vakatautau.co.nz
Parent and Family Resource Centre www.parentandfamily.org.nz
Parent to Parent www.parent2parent.org.nz
People First www.peoplefirst.org.nz/Home/tabid/36/Default.aspx
Prenatal screening tests for trisomy 21 (Down syndrome), trisomy 18 (Edwards
syndrome) and neural tube defects www.ranzcog.edu.au/publications/statements/C-obs4.pdf
Royal Australian and New Zealand College of Obstetricians and Gynaecologists www.ranzcog.edu.au
Royal New Zealand College of General Practitioners www.rnzcgp.org.nz
Royal Australian and New Zealand College of Radiologists www.ranzcr.edu.au
Sands New Zealand www.sands.org.nz
Spina Bifida Association of New Zealand
What Everyone Keeps Asking www.weka.net.nz
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
45
Australia
Australian Centre for Genetics Education
Changes to Chromosomes – Number, Size and Structure Fact sheet
www.genetics.com.au/pdf/factsheets/fs06.pdf
Mosaicism – Complex Patterns of Inheritance Fact Sheet
www.genetics.edu.au/pdf/factsheets/fs13.pdf
Down syndrome Fact Sheet
www.genetics.com.au/pdf/factsheets/fs28.pdf
Trisomy 13 – Patau Syndrome
www.genetics.edu.au/factsheet/fs29
Trisomy 18 – Edwards Syndrome
www.genetics.edu.au/pdf/factsheets/fs30.pdf
Human Genetic Society of Australasia (HGSA) www.hgsa.com.au
United Kingdom
Antenatal Results and Choices (UK) www.arc-uk.org/
Down’s Syndrome Association (UK) A New Parent’s Guide
www.downs-syndrome.org.uk
Down syndrome online www.down-syndrome.org
Fetal Medicine Foundation, London www.fetalmedicine.com/FMF
The 11–13+6 Weeks Scan
www.studiolift.com/fetal/site/FMF-English.pdf
International Mosaic Down Syndrome Association Booklet for professionals
www.imdsa.org/Information/professional.htm
National Health Service (UK)
Antenatal Screening: Introduction
www.nhs.uk/conditions/Antenatal-screening/Pages/Introduction.aspx
Brief descriptions of other trisomies (13 Patau; 18 Edwards), monosomy (Turner) and also
Klinefelters, XXX, YY and features which might identify them antenatally
www.perinatal.nhs.uk/car/anomaly/chromosome/chromosome.htm
National Screening Committee (UK) Fetal Anomaly Screening Programme – Screening for Down’s Syndrome: UK NSC Policy
recommendations 2007–2010: Model of Best Practice
www.dh.gov.uk/en/Publicationsandstatistics/Publications/
PublicationsPolicyAndGuidance/ DH_084732
46 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
 Appendix 2:
Screened conditions
Appendix 2:
Screened conditions
The list of ‘other conditions’ cannot be exhaustive as it is unknown what the ‘condition’ for
a particular woman or her baby may be. This is the same for blood tests taken in any health
setting where unanticipated findings may be identified.
The following provides details of the aneuploidies and unusual analytes.
Trisomy 21
Trisomy 21, also known as Down syndrome is a genetic disorder caused by an extra
copy of chromosome 21 inside each of the body’s cells. The chromosomes are located
in the nucleus of each cell, and contain the genetic material that, in combination with
environmental influences, determines a person’s individual characteristics. In Down
syndrome, instead of a pair there are three copies of chromosome 21. The extra genetic
material from the extra chromosome results in the physical and intellectual attributes
which are the characteristics of Down syndrome.
The average life expectancy of people with Down syndrome has increased with improved
healthcare, better education, greater opportunities and a shift in societal attitudes during
the past 20 to 30 years. Studies indicate that average life expectancy in the UK was
estimated to be 9 years of age in 1929 and 12 years in 1949. Subsequent reports have shown
a marked increase in life expectancy that began in the 1950s. By the year 2000 the median
life expectancy for people with Down syndrome in Australia was 60 years2.
Recent research shows that parents appreciate information about the abilities and
potential of people with Down syndrome (eg participation in community sports, activities,
inclusion in mainstream education classes, employment, independent living, life
expectancy to 50–60s and having friends); as well as clinical details3. Balancing clinical
information (eg cause, recurrence risk for future pregnancies, physical features, associated
medical conditions, intellectual disability and developmental delay) with a better
understanding of the information parents consider most important, may enable health
practitioners to provide the information that satisfies the needs of families about Down
syndrome.
The New Zealand Down Syndrome Association note that:
‘People with Down syndrome are all unique individuals and vary
in their abilities and achievements. They do have features in
common, but they also closely resemble their parents and family.
Many characteristics are associated with Down syndrome, but any
one person will only have some of them. Thus each person is an
individual, with a unique appearance, personality and set of abilities.
The extent to which a child shows the physical characteristics of the
syndrome is no indication of his or her abilities and achievements’4.
2. Bittles AH, Glasson EJ. 2004. Clinical, social and ethical implications of changing life expectancy in Down
syndrome. Dev.Med.Ch.Neurol. 46(4): 282-6.
3. Sheets KB, Best RG, Brasington CK, Will MC. 2011. Balanced information about Down syndrome: What is
essential? Am J Med Genet Part A 155: 1246–1257.
4. www.nzdsa.org.nz (accessed 9 September 2009).
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
47
Similarly, the organisation Upside of Down report that:
‘Today people with Down syndrome live at home with their families
and are active participants in the educational, vocational, social
and recreational activities of the community. They are integrated
into the regular education system, and take part in sports, camping,
music, art programs and all the other activities of their communities.
In addition, they are socializing with people with and without
disabilities, and as adults are obtaining employment and living in
group homes and other independent housing arrangements’5.
People with Down syndrome experience varying degrees of delay in their learning and
development, and may have additional health needs. They will almost always learn to
walk, speak, read and write but commonly require support in using money, negotiating
public transport and building skills for appropriate social behaviour.
Some of the health issues associated with Down syndrome include:
> hearing loss in up to 50 percent of people with Down syndrome
> congenital heart disease in up to 50 percent
> thyroid disorders, most commonly hypothyroidism, in up to 40 percent
> gastrointestinal tract congenital malformations, such as duodenal atresia
and Hirschsprung’s disease
> cataracts and visual refractive errors
> childhood leukaemia in about 2 percent
> early onset Alzheimer’s disease.
Children with mosiac or partial forms of this trisomy are likely to be less severely affected.
Trisomy 18
Trisomy 18, also known as Edwards syndrome is a chromosomal condition caused by the
presence of all or part of an extra 18th chromosome.
The syndrome appears to affect females more frequently than males by a ratio of
approximately three or four to one. Large population surveys indicate that it occurs
in about one in 5,000 to 7,000 live births6. The incidence increases as the mother’s
age increases. The syndrome has a very low rate of survival, resulting from heart
abnormalities, kidney malformations, and other internal organ disorders.
About 50 percent of live born infants with trisomy 18 live to 2 months, and 5–10 percent
survive their first year of life. Major causes of death include apnea and heart abnormalities.
It is impossible to predict the exact prognosis of a child with Edwards syndrome during
pregnancy or post birth. The median lifespan is 5–15 days. A small percentage of babies
with the full Edwards syndrome who survive birth and early infancy may live to adulthood.
Children with mosaic or partial forms of this trisomy may have a different morbidity
and mortality statistics. In mosaic forms there are some cells in the body where the
chromosome number and structure is different from other cells.
5. www.upsideofdown.org/about_t21 (accessed 13 May 2012).
6. www.rarediseases.org/rare-disease-information/rare-diseases/byID/217/viewFullReport (accessed 13 May 2012).
48 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
Trisomy 13
Trisomy 13, also known as Patau syndrome, is a rare chromosomal condition, in which
there is an additional chromosome 13. The extra chromosome 13 disrupts the normal
course of development. It causes severe neurological, heart and kidney defects which
make it difficult for infants to survive. Newborns with trisomy 13 share common physical
characteristics including: extra fingers or toes (polydactyly), small head (microcephaly),
facial defects such as small eyes (microphthalmia), absent or malformed nose, cleft lip
and/or cleft palate.
Many infants have difficulty surviving the first few days or weeks due to severe
neurological problems or complex heart defects. Surgery may be necessary to repair heart
defects or cleft lip and cleft palate. Physical, occupational, and speech therapy will help
those individuals with trisomy 13 who live beyond the first few weeks/months.
Triploidy
Triploidy means that a baby has three copies of each chromosome in each cell rather
than two, making a total of 69 chromosomes rather than 46. The majority (more than 99
percent) of babies with triploidy will miscarry or be stillborn. Of those babies born alive,
most are likely to die in the hours or days following birth. A few babies with triploidy have
lived five months or longer, but this is rare and usually the babies who survive longer have
mosaic triploidy rather than full triploidy. Babies with triploidy usually have multiple
genetic problems and severe growth restriction.
Neural tube defects
Neural tube defects (NTDs) are birth defects of the brain and spinal cord. The two most
common neural tube defects are spina bifida and anencephaly. In spina bifida, the baby’s
spinal column does not close completely during the first month of pregnancy. There is
usually nerve damage that causes at least some paralysis of the legs. In anencephaly, much
of the brain does not develop. Babies with anencephaly are likely to be stillborn or will die
shortly after birth.
Adequate maternal intake of folate/folic acid (400 micrograms per day) commencing
antenatally and continued through the first trimester of pregnancy significantly reduces
the probability of NTD.
First trimester combined screening cannot estimate the risk for NTDs. Second trimester
screening performed after 15 weeks includes alpha fetoprotein (AFP) which may indicate
a risk of NTDs at this time. However, more severe forms may be detected at the nuchal
translucency ultrasound.
For NTDs, including spina bifida, the 18 to 20 week anatomy scan is the best available
screening tool. The use of AFP as a screening tool for NTDs is neither very sensitive nor
specific and is not considered best practice internationally and should not be ordered
specifically with the intention of screening for NTDs.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
49
Conditions identified by ultrasound
Ultrasound scans undertaken as part of this screening may detect some major fetal
structural anomalies, such as skeletal anomalies, brain and neural tube defects, congenital
heart defects, and abnormalities of the renal tract, gastrointestinal system and abdominal
wall. These will be mentioned in the ultrasound scan report.
An increased NT measurement is associated with trisomy 21, Turner syndrome and other
chromosomal defects as well as other fetal malformations and genetic conditions.
There are instances where babies have increased NT measurements but at diagnostic
testing have normal chromosomes. These babies may have an increased risk of a number
of abnormalities. Conditions associated with increased NT measurement include:
cardiac malformation, diaphragmatic hernia, omphalocoele, body stalk anomaly, skeletal
anomalies, Noonan syndrome, Smith-Lemli-Opitz syndrome and spinal muscular
dystrophy.
Unusual analytes
First trimester combined screening looks at two markers, pregnancy-associated plasma
protein A (PAPP-A) and Beta-Human Chorionic Gonadatrophin (ßhCG).
Second trimester maternal serum looks at four markers, Alpha-fetoprotein (AFP), Beta-
Human Chorionic Gonadatrophin (ßhCG), Unconjugated Oestriol (uE ) and Inhibin A.
3
The markers used in screening come from the fetus and the placenta. Very abnormal levels
may indicate a possibility of poor placentation or fetal growth restriction.
For example, if PAPP-A is reduced and/or inhibin-A and/or ßhCG is elevated it has
been shown that there is a possibility of conditions related to poor placentation such as
pre-eclampsia , preterm birth or intrauterine growth restriction.
All information identified through screening will be included in the risk report to the
health practitioner.
Table 3 indicates the analytes measured. It is noted that there may be combinations of
these markers that indicate increased pregnancy concerns, for instance low PAPP-A and
low ßhCG or high ßhCG and high AFP.
The correlation of low levels of one or two markers with adverse pregnancy outcomes
may not be strong, however very low level results can provide information which may be
combined with ongoing assessment to assist with pregnancy management.
50 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
Table 3: Analytes measured during first or second trimester serum testing
What is Measured
When is it
Where Does it
Other Information
Measured
Come From
Pregnancy
1st trimester
Produced by
Very low levels of PAPP-A in the
associated plasma
the baby and
mother’s blood can indicate poor
protein-A (PAPP-A)
placenta
placentation.
Beta human
1st and 2nd
Produced by the
High levels of ßhCG in the mother’s
chorionic
trimester
baby
blood can indicate problems with
gonadotrophin
the pregnancy (for instance fetal
(ßhCG)
growth restriction).
Unconjugated
2nd trimester
Produced by the
Very low levels of uE can indicate
3
oestriol (uE )
placenta
the biochemical disorders Smith
3
Lemli Optiz syndrome and steroid
sulphatase deficiency.
Alpha fetoprotein
2nd trimester
Produced by the
Very high levels of AFP in the
(AFP)
baby
absence of structural anomalies
can indicate problems with the
pregnancy (for instance fetal
growth restriction).
Inhibin A
2nd trimester
Produced by the
Very high levels of Inhibin-A can
placenta
indicate poor placentation.
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
51
Multiple of the median (MoM)
Serum marker levels used in antenatal screening change by gestational age. Therefore, for
accurate interpretation of the test results, a different reference range must be used for each
week of gestation, depending on when the test is drawn. To avoid the multiple reference
range problems and also to standardize test results a median value for test results in
normal pregnancies is determined for each week of gestation. The woman’s individual
analyte levels are compared with the median for that analyte at the appropriate gestational
age, and expressed as a multiple. This is the multiple of the median. The multiple of the
median is used as a standard reporting tool for antenatal screening.
Figure 6 shows that an analyte level of 5 may be increased or decreased depending on
the stage of pregnancy. At 10 weeks, the median value is 2.5, hence a level of 5 is 2 MoMs
(elevated) but at 14 weeks, the median value is 10 hence a level of 5 is 0.5 MoMs (decreased).
Figure 6: Serum marker levels by gestational age
10
MoM = 2
MoM = 1
5
MoM = 0.5
(iu/mL)
el
ev
2.5
er l
ark
Serum m
1.5
10
11
12
13
14
Gestation (weeks)
median serum marker level
tested serum marker level sample
MoM = Multiple of the median
52 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners

Table 4 show the analyte relationship with aneuploidy. These are not absolute. Most will
have these patterns but not all.
Table 4: First and second trimester analytes and the relationship with aneuploidy
First Trimester
PAPP-A
Free ßHCG
NT measurement
Trisomy 21
Trisomy 18
Trisomy 13
Second Trimester
Free ßHCG
uE
AFP
inhibin-A
3
Trisomy 21
Trisomy 18
Trisomy 13
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
53
Impact of accurate information
High quality screening results rely on complete and accurate information which informs
the risk calculation. This includes details of smoking status, ethnicity, weight, IVF, twins
and gestational age.
As an example, obesity dilutes the analytes measured, and IVF pregnancies have a higher
ßHCG. The risk calculation takes these factors into account when they are provided.
The table below provides some scenarios which affect the risk calculation and therefore
the risk result.
Table 5: Effect of different scenarios on pregnancy risk results
Scenario
Result 1
Change in
Result 2
Comment
Details
Change in
Gestational age
Ultrasound
Revised risk
The analytes
gestational age
calculated at
scan calculated
calculation
change over the
15.1
gestational age
pregnancy and
at 14.1
therefore the
risk calculation
changes
T21 risk result:
T21 risk result:
depending on the
1:220
1:910
gestational age.
Change from
Assumed
Ultrasound scan
Revised risk
The analytes are
singleton to
singleton
shows twins
calculation
divided when
twin pregnancy
pregnancy
there is more
than one fetus.
T21 risk result:
T21 risk result:
1:250
1:500
Non-smoker
Assumed
Health
Revised risk
Smoking affects
to smoker
non-smoker
practitioner
calculation
placental
informs the
function and
Screening
inhibin levels
Laboratory that
are higher in
T21 risk result:
the woman is a
T21 risk result:
women who
1:210
smoker
1:300
smoke.
Compounding
42 year old
Woman’s age
Revised risk
There is a
effect of many
woman using
incorrect –
calculation
compounding
changes
LMP dating at
found she is 32
effect when
18,2. No scan
years of age,
many of the
data, singleton
LMP was wrong
variables are
pregnancy
and it is actually
incorrect.
reported,
14,1. Twins,
no weight,
Smoker and
no smoking
weighs 45 kg
information
T21 risk result:
T21 risk result:
1:520
1:13,000
54 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
 Appendix 3:
Robinson Equation
Appendix 3:
Robinson Equation
The table below outlines the Robinson equation that is used by the screening laboratories
to measure gestational age. Ranges for NT acceptance are highlighted in the darker cells.
Table 6: The Robinson equation for measuring gestational age
CRL
GA
CRL
GA
in mm
weeks
days
in mm
weeks
days
5
7
1
54.5
12
0
10
7
5
56.5
12
1
15
8
2
58.5
12
2
20
8
6
60
12
3
25
9
2
62
12
4
28
9
4
64
12
5
30
9
5
66
12
6
35
10
0
68
13
0
35
10
2
70
13
1
40
10
5
72
13
2
41
10
6
74
13
3
42
10
6
76
13
4
43
11
0
79
13
5
45
11
0
81
13
6
45.5
11
1
82.6
14
0
46
11
2
83
14
0
48
11
3
84
14
0
49.5
11
4
85
14
1
51
11
5
86
not
available
53
11
6
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
55
 Glossary of terms
Glossary of terms
Alpha-fetoprotein (AFP) − a protein that is normally produced by the fetus. Maternal
serum AFP levels can be used as a biochemical marker in the detection of certain fetal
abnormalities including NTDs after 15 weeks of pregnancy.
Amniocentesis − a procedure involving the withdrawal of a small amount of amniotic
fluid by needle and syringe through the abdomen guided by ultrasound performed at the
same time. The tests performed on fetal cells found in the sample can detect a range of
chromosomal and genetic disorders.
Analyte − a substance that is undergoing analysis or being measured. Analytes measured
in antenatal screening include: pregnancy associated plasma protein-A, beta human
chorionic gonadotrophin, unconjugated oestriol, alpha fetoprotein and inhibin A.
Aneuploidy – is the condition of having less than or more than the normal diploid number
of chromosomes. For instance, Down syndrome has 47 (not 46) chromosomes with an
extra chromosome 21.
Beta-human chorionic gonadotropin (ßhCG) − a hormone produced during pregnancy
and present in maternal blood and urine. It is used as a biochemical marker for Down
syndrome and other conditions in first trimester combined and second trimester maternal
serum screening.
Biparietal Diameter (BPD) – the measurement of the distance between the fetal parietal
bones at their widest point. This is used for dating in the second trimester.
Chorionic villus sampling (CVS) – a procedure involving the withdrawal of a small
amount of placental tissue by needle and syringe through the abdomen guided by
ultrasound performed at the same time. Tests performed on the placental cells can detect
a range of chromosomal and genetic disorders.
Crown rump length (CRL) − the measurement from the fetal crown to the prominence
of the buttocks or breech. This is used for dating in the first trimester.
Chromosome − an organised structure of DNA and protein found in all living cells that
carries the genes determining heredity.
Cut-off point − The point that divides people into a group at lower risk or increased risk
for the condition being screened for. In New Zealand the cut-off point in screening for
Down syndrome and other conditions is 1:300 at term.
False negative result − when a woman receives a low risk screening result but the baby
does have the condition screened for.
False positive result − when a woman receives an increased risk screening result but the
baby does not have the condition screened for.
Inhibin A − a hormone secreted by the ovary that is used as a biochemical marker in
second trimester maternal serum screening for Down syndrome and other conditions.
Mosaic – the presence of two populations of cells with different genotypes in one patient,
where usually one of the two is affected by a genetic disorder.
56 Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
Multiple of the median (MoM) − a measure which compares the values of a biochemical
marker in an individual sample with the median value of that biochemical marker in other
women at the same gestation.
Neural tube defect (NTD) − a congenital anomaly involving the brain and spinal cord
caused by failure of the neural tube to close properly during embryonic development.
Open NTDs occur when the brain and/or spinal cord are exposed at birth through a defect
in the skull or vertebrae. Examples of open NTDs are spina bifida (myelomeningocele),
anencephaly, and encephalocele.
Nuchal translucency (NT) − sonographic appearance of the collection of fluid under the
skin at the back of the fetal neck. NT is a marker for chromosomal and other anomalies and
can be measured in the first trimester of pregnancy.
Pre-eclampsia − a condition that occurs in some women during the second half of
pregnancy, commonly associated with a rise in blood pressure and proteinuria.
Pregnancy-associated plasma protein A (PAPP-A) − a protein originating from the
placenta used as a biochemical marker in first trimester combined screening for Down
syndrome and other conditions.
Risk calculation algorithm − an explicit protocol (in this case computer based) that
combines a number of factors in determining overall risk of a particular outcome or
condition.
Screening − a way of identifying a group of people who are more likely than others to have
a particular condition. The screening process involves testing people for the presence
of the condition, and predicting the likelihood that they have the condition. Antenatal
screening for Down syndrome and other conditions predicts the likelihood of the
conditions being present in the fetus.
Sensitivity −the ability of screening to identify individuals with the condition screened
for. A test with high sensitivity will have few false negative results.
Specificity − the ability of screening to identify individuals who do not have the condition
screened for. A test with high specificity will have few false positive results.
Triploidy − an extremely rare chromosomal disorder in which a baby has three of every
chromosome making a total of sixty-nine rather than the normal forty-six chromosomes.
Trisomy − a group of chromosomal disorders in which there are three copies, instead of
the normal two, of a particular chromosome present in the cell nuclei. The most common
trisomies in newborns are trisomy 21 (Down syndrome), trisomy 18 (Edwards syndrome)
and trisomy 13 (Patau syndrome).
Unconjugated oestriol (uE ) −a hormone produced by the placenta and used as a
3
biochemical marker in second trimester maternal serum screening for Down syndrome
and other conditions.
Further terms can be found at www.nsu.govt.nz
Antenatal Screening for Down Syndrome and Other Conditions: Guidelines for health practitioners
57
Document Outline