Draft National Air Ambulance Strategy
c/- ACC Healthwise
PO Box 242
Wellington
1 December 2004
Please find attached the
Draft National Air Ambulance Strategy.
This document outlines a proposed model for the
provision of air ambulance services in New Zealand over the next 5-10 years.
In seeking to ensure New Zealanders receive world class emergency medical care, the strategy
acknowledges evolving technology and professionalisation of emergency transport services, and
looks to ensure that these enable improvements in patient outcomes.
Air ambulance services are used for a range of activities in New Zealand. To be effective, the air ambulance network
needs to be integrated with, and complement, both road based ambulance services and the emergency care functions,
inter-hospital transfers and other services of District Health Boards.
The draft strategy is very much a strawman. We welcome your consideration and discussion. We have highlighted a
number of areas that need significant further refinement. These areas are complex and need feedback from providers,
clinicians, users and funders.
We invite you to consider the strategy and respond in the format provided. Following feedback on the draft strategy,
the strategy will be finalised in 2005.
Electronic copies of this document and a Feedback Booklet can be found on the ACC website http://www.acc.co.nz/ or
email
@acc.co.nz.
On behalf of the Steering Committee for the National Air Ambulance Strategy, I invite you to consider the issues raised
by the discussion document and provide us with feedback
before 25 February 2005 as to your views regarding air
ambulance services in New Zealand.
Dr David Rankin
General Manager
ACC Healthwise
Draft National Air Ambulance Strategy
Air Ambulance Services in
New Zealand:
A Discussion Document
DRAFT FOR CONSULTATION
29 November 2004
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Page intentionally left blank
2
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Draft National Air Ambulance Strategy
Foreword
This draft Strategy provides direction for the future development of air ambulance sector
so that it can play a central role within the evolving health system. There is increasing
evidence available about the specific contribution air ambulance services can make to
improving health outcomes.
This Strategy has not been developed in isolation; it follows on from the New Zealand
Health Strategy, New Zealand Primary Health Care Strategy, Roadside to Bedside and
the Cull Report – all of which have guided the development of the Draft National Air
Ambulance Strategy.
Trends in pre-hospital care are changing, technology is evolving and the air ambulance
service has come of age – providing (often fully dedicated) professional high quality, timely
clinical care supported by up to date equipment. It is in recognition of this increasing
sophistication in the sector that the aim of the strategy is ‘for the air ambulance network to
provide cost effective pre-hospital care and inter-hospital transfer services complementary
to the road ambulance system ensuring people get the right care, at the right time, in the
right place from the right person’.
This release of this document for consultation is one of the key steps in the process of
developing a National Strategy. The draft document contains more questions than
answers and consequently will generate significant and robust debate within the sector.
Following consultation, it is anticipated that the sector will continue to work with
stakeholders to refine the Strategy ensuring it continues to provide the quality of air
ambulance services that the public has come to expect.
The configuration described within this Strategy is one of a range of options that could
achieve the above aim. Alternatively, existing air ambulance services are well proven,
having served New Zealanders admirably for 20 years, competently providing local
solutions to meet local needs. The challenge therefore is to identify an outcome that
achieves a balance between the aim of this Strategy and the status quo whilst not loosing
sight of the quality of service currently being provided.
The detail of the Strategy implementation will evolve over the next few years and may
not be fully realised for five to ten years. Further changes may need to be made as
more detail comes to light. However, ACC contracts are already in place until
October 2006 ensuring current services will be maintained for some time. During this
transition there will be opportunities for future work to review and validate some of the
core assumptions made in the draft Strategy (e.g. max volumes per HEMS helicopter per
year and per day, cost benefit of national coordination, ability to fly from each HEMS base
to all points of their flying radius 24/7).
The Strategy considers a new vision for air ambulance services; it does not contain details
of implementation, which will involve evolutionary change to protect the gains already
made. Involvement and collaboration with the air ambulance sector will be a key feature of
the implementation process in the coming years. This is crucial to ensure that all issues
and options are considered in developing the new arrangements.
3
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Although this Strategy principally describes a single model, and the air ambulance sector
has expressed reservations in regard to the practicality of providing it, it is anticipated that
through this consultation process a range of alternate models or variations to the one
described will be developed. Readers of this draft Strategy should not draw conclusions if
their existing service is not specifically referred to within the draft. The proposed
deployment configuration and diagrams are a discussion option only and it is anticipated
that feedback from the sector and stakeholders will develop these further and ensure any
real or perceived geographic gaps are served appropriately.
It is essential to the process that all parties carefully consider the content of this
consultation document and provide detailed comment that ensures their particular
expertise or interest in pre-hospital care is tabled for consideration. It is important that the
final strategy reflects the best available air ambulance strategy for New Zealand.
4
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Draft National Air Ambulance Strategy
Draft for Consultation
This is a draft strategy for the Air Ambulance services in New Zealand. It is the
culmination of more than 12 months of discussion with stakeholders about the role and
nature of air ambulances in New Zealand.
Following feedback this draft strategy, a final strategy will be prepared in the New Year.
FEEDBACK ON THIS DRAFT STRATEGY
Title:
Draft National Air Ambulance Strategy
Provide feedback to:
From: (Your Name, Address, Telephone)
Project Manager
National Air Ambulance Strategy
C/- ACC Healthwise
PO Box 242
Wellington
Or by email to
@acc.co.nz
Closing date for
Date of your
comment
comments
25 February 2005
Comment is preferred in electronic format using Microsoft Word, following the layout below.
Note that
this is available as a separate Feedback Booklet for comments to be submitted electronically.
GENERAL COMMENT
Type your general comments in the box. The comment box will automatically expand to accommodate
comments of any length.
5
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
SPECIFIC COMMENT
Insert the section heading and page. Insert the page; paragraph and line number as appropriate. Use
a new row for each comment.
The rows will automatically expand to accommodate comments of any length. Remove unused rows,
or insert additional rows as required. To insert extra rows at the end of the table, go to the last cell and
press the TAB key.
Section and Page
Comment
Please detail supporting facts and/or rationale exactly
6
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Draft National Air Ambulance Strategy
Draft for Consultation
Executive Summary
The Accident Compensation Corporation (ACC), Ministry of Health and Ambulance New
Zealand through the vehicle of their Memorandum of Understanding together with the Air
Rescue/Air Ambulance Division of the Aviation Industry Association have sponsored the
development of this National Air Ambulance Strategy (NAAS) to ensure an effective and
efficient network of air ambulances (both rotary and fixed wing) serving patient needs in
New Zealand.
This document is the draft National Air Ambulance Strategy and has been made available
for public consultation. The process of development has employed consultation at each
step of the way – over the project scope, the assessment of current services, consultation
feedback and key elements of the strategy.
To be effective, the air network needs to be integrated with, and complement, both road
based ambulance services and the emergency care functions, inter-hospital transfers and
other services of District Health Boards. Air ambulance services are used for a range of
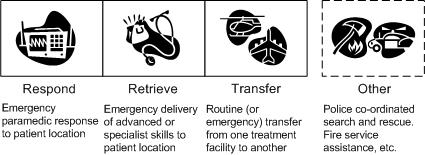
activities in New Zealand, as illustrated in the Figure 1.
Figure 1 – Range of Activities for Air Ambulance Services
Consistent with established local and international practice, an effective emergency care
system that integrates pre-hospital management, hospital treatment and rehabilitation
services will optimise patient outcomes. The National Air Ambulance Strategy endeavours
to ensure the pre-hospital component of an effective emergency care system will provide a
quality rapid retrieval/primary emergency response ambulance service for New Zealand as
well as an effective network to meet the needs for urgent and non-urgent inter-hospital
transfers.
The strategy proposes a comprehensive network of air ambulances servicing both
emergency response and inter-hospital transfer air ambulance needs:
7
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
n An enhanced standard of Helicopter Emergency Medical Services (particularly in
respect to clinical crewing by advanced paramedics and closer integration with major
DHB emergency departments and ICU retrieval teams)
n The preservation of local community rescue helicopters in areas more peripheral to
the likely HEMS coverage (i.e. greater than 45 minutes flying time)
n National coordination of inter-hospital transfers by air supported by a network of
intensive care air ambulances and associated DHB clinical retrieval teams.
The strategy advances a more consistent and equitable standard with greater coordination
of services for all of New Zealand, whilst retaining good local services. It has focused on
the nature and quality of emergency pre-hospital clinical service delivery, differentiating it
from community need for rescue capability (an established part of local search and rescue
service capability). Some areas where rescue resources are not configured as effectively
or efficiently for health purposes, while not precluded, have not been explicitly endorsed by
the strategy.
The strategy balances clinical advice from leading specialists, clinical colleges and
international literature with the strong desire by communities for the preservation of local
services.
Recommendations of the strategy, including integration with the new Ambulance
Communications Centres, improving national coordination through a flight desk, greater
organisation of DHB retrieval services and more streamlined Crown funding processes,
will ensure air ambulance services are well integrated with the other pre-hospital
emergency medical services and the hospital-based components of the emergency
management system to obtain optimal patient outcomes.
8
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Draft National Air Ambulance Strategy
Table of Contents
Executive Summary ....................................................................................................7
Introduction ................................................................................................................12
Background................................................................................................................14
An Evolving Health Sector ....................................................................................................................14
Why we need a strategy for Air Ambulance services..........................................................................17
What work is in progress to address these issues? ............................................................................18
Overview – A Proposed National Network of Air Ambulances...........................19
Aim .........................................................................................................................................................19
Principles................................................................................................................................................19
Key Themes ..........................................................................................................................................20
Defining Air Ambulances Services .........................................................................22
Emergency Air Ambulance Services....................................................................................................22
Inter-hospital transfer by Air Ambulance ..............................................................................................29
Linkages with Key Sector Initiatives .....................................................................................................33
Geographical Deployment of Air Ambulance Services .......................................................................34
Recommendations ................................................................................................................................36
Coordinating Air Ambulance Operations...............................................................37
Emergency Air Ambulance Services....................................................................................................37
IHT Air Ambulance Services.................................................................................................................38
Recommendations ................................................................................................................................41
Funding and Contracting of Air Ambulance Services .........................................42
Funding ..................................................................................................................................................42
Recommendations ................................................................................................................................42
Appendix 1 – People and Organisations Consulted ............................................44
Appendix 2: Progress on Air Ambulance Issues Identified by Cull...................47
Current Air Ambulance Issues..............................................................................................................48
Appendix 3: Aircraft Type and Standards..............................................................50
9
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Appendix 4: Decision Trees for Delivery, Retrieval and Transfer ......................51
A Continuum of Decisions ....................................................................................................................51
Decision Tree 1 – Delivery....................................................................................................................52
Decision Tree 2 – Retrieval from Scene ..............................................................................................53
Decision Tree 3 – Transfer (Inter-hospital) ..........................................................................................54
References..................................................................................................................55
10
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Glossary of Key Terms
ACC
Accident Compensation Corporation
AIA
Aviation Industry Association
CAA
Civil Aviation Authority
Casevac
Missions for the retrieval of acute accident victims in the pre-
hospital emergency situation
CFIT
Controlled Flight Into Terrain
DHB
District Health Board
ECCT
Emergency Care Coordinating Team
EMS
Emergency Medical Service
HEMS
Helicopter Emergency Medical Services
IFR
Instrument Flight Rules – operation of an aircraft by instruments
when visibility is below minimum visual levels
IHT
Inter-hospital Transfers – the transfer of seriously ill patients
between hospitals
Medivac
Acute medical evacuations in the pre-hospital emergency situation
MSA
Minimum Safe Altitude
NAAS
National Air Ambulance Strategy
PHO
Primary Health Organisation – as defined by the New Zealand
Primary Care Strategy (Ministry of Health)
SAR
Search and Rescue – Missions initiated by the Police or by CAA
via the National Rescue Coordinators Centre, for search and
rescue of people either on land or at sea
VFR
Visual Flight Rules – operation of an aircraft in normal visual
conditions
11
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Draft National Air Ambulance Strategy
Development of the Draft Strategy
Introduction
The Accident Compensation Corporation (ACC), Ministry of Health and Ambulance New
Zealand through the vehicle of their Memorandum of Understanding together with the Air
Rescue/Air Ambulance Division of the Aviation Industry Association have sponsored the
development of this National Air Ambulance Strategy (NAAS) to ensure an effective and
efficient network of air ambulances (both rotary and fixed wing) serving patient needs in
New Zealand.
To be effective, the air network needs to be integrated with, and complement, both road
based ambulance services and the emergency care functions, inter-hospital transfers and
other services of District Health Boards.
This document is the draft National Air Ambulance Strategy and has been made available
for public consultation.
It needs to be read in conjunction with the Current State Assessment Discussion
Document released in August 2004 that presented a summary of air ambulance services
in New Zealand, and the subsequent summary of the consultation feedback. Both of
these documents are available by request from ACC.
The earlier published Current State Assessment focuses on air ambulance services, and
reviews current environmental issues, including:
n The Health Sector
n The Ambulance Service
n Air Ambulance Services
n Air Ambulance Volumes and Costs
n International Research.
It also takes particular note of the following recent developments and initiatives, including:
n Roadside to Bedside
n Ambulance Communications Project
n National Framework for Delivery, Retrieval and Transfer Protocols
n Standards (AIA, Ambulance Service Sector)
n Sustainable Funding Review for Ambulance Services.
It invited discussion on a wide range of issues, for example:
n The rapid growth of air ambulance services over the past decade
n The sizeable role air ambulances have supporting District Health Boards transferring
patients from one hospital to another
n The high number of air ambulances operating in New Zealand (relative to other
jurisdictions when we compare geographical area and/or population)
12
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
n The low average utilization of air ambulances operating in New Zealand and the
consequent high average hourly costs
n The variety of funding sources, particularly of individual communities, sponsorship and
the Crown through the Ministry of Health, District Health Boards, and ACC.
As the feedback document graphically illustrated, there exists a wide range of opinion as
to how air ambulance services should be configured in New Zealand.
This strategy has endeavoured to build on these first two documents, based on many
input sources:
n 100+ members of Emergency Care Coordinating Teams
n DHBs, primary care, emergency services, health care workers
n 5 centres: Auckland, Hamilton, Wellington, Christchurch and Dunedin
n Through meetings and workshops, members of key stakeholder organisations:
n Ambulance New Zealand
n Aviation Industry Association
n Air Rescue NZ (previously NZSARTS)
n 65 Written responses to the Current State Assessment Discussion Document
n Prior documentation and knowledge
n International literature
n NZ Health Strategy, Roadside to Bedside, Hospital Plan
The strategy recognises the:
n Substantial and historical contribution of communities to existing service network
n Unique geographical challenges of NZ
n Dedication of existing operators who have developed network into what it is today
n Increasingly positive relationship between air operators and Ambulance NZ
n Increasing focus by DHBs on ensuring effective supply of clinical staff for the retrieval
and repatriation of patients by air ambulance.
We invite you to consider this strategy for the provision of air ambulance services in New
Zealand over the next 5-10 years.
13
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Draft National Air Ambulance Strategy
An integrated national network of air ambulances
Background
An Evolving Health Sector
Within the last five years the provision and focus of medical care has changed
considerably with a move towards:
n Increasing specialisation and sub-specialisation in many areas of medical practice –
changing the nature of services and locality
n Centralisation of acute care, with resuscitation/stabilisation and transportation of
patients from smaller centres and definitive care being undertaken at larger hospitals
n Integration of primary and secondary care within the rural health sector with general
practitioners becoming more involved in health centres and accident services
n Proportionally fewer hospitals and hospital beds generally as result of increasing
population base
n Increased travel distances between secondary and tertiary care providers
n Increasing public expectations of healthcare delivery
n Increased emphasis on preventative and educational health
n Greater use of primary care and PHOs
n Increased emphasis on quality, safety, and outcomes
n Greater awareness and willingness to contribute personally to improve access.
Continuum of Care
The aim of Roadside to Bedside1 is to ensure an acute management system consisting of
a number of complementary components that together should provide a patient-focused,
seamless service and the best possible outcome for people who need to access
emergency services. For this to occur:
It is essential that people get the right care, at the right time, in the right place from the right person.
It describes a system of five regional networks, incorporating all hospitals and providers
involved in trauma and emergency work within a defined geographic region. At the ‘hub’ of
each network will be one of New Zealand’s five tertiary centres (Auckland, Waikato,
Wellington, Christchurch and Dunedin). The ‘spokes’ will extend out through secondary
hospitals and sub-acute units to health centres and all rural health professionals. Providers
will work together to ensure that patients get to the nearest place capable of providing
definitive care as quickly and safely as is reasonably practicable. Networks will also need
to work together at a national level.
The proposed HEMS network will provide a surer way to implement the regional care
networks as envisaged by Roadside to Bedside particularly as:
14
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
n Co-located with DHB-based retrieval teams and emergency doctor (referred to by
Waikato DHB as an “A-Zero response”) arrangements, greater expertise can be
delivered to the side of the patient more quickly than can now
n Advanced paramedics rostered to HEMS will be more practiced at providing care
routinely in an air ambulance and will have greater knowledge of the actual and
potential safety and clinical threats to patients than can paramedics who are called on
to occasionally staff local helicopters
n Operating regionally, with close liaison with the regional tertiary centre, HEMS will be
better placed to safely deliver patients to hospitals that can provide definitive care
improving outcomes and reducing patient inconvenience
n Approximately 90% of New Zealanders will be able to be access advanced clinical
skills within the 60 minute golden hour.
Population Health
With the establishment of District Health Boards (DHBs), the emphasis shifted from
funding for individual services to funding for a district’s needs. More attention was focused
on providing resources for an equitable level of services across the country. The way
funding is calculated changed to reflect this new emphasis, ensuring that funds were
divided evenly across the country (e.g. Population-Based Funding Formula).
As a result of how services are funded, DHBs have a need to understand the burden of
disease on local populations and to develop a greater range of preventative services. In
the past, regional services had a ‘sickness’ focus, but are now moving towards both a
‘wellness’ and ‘sickness’ focus.
DHBs have agreed that the DHB of domicile of the patient will pay retrieval and
repatriation by air ambulance. Key considerations include:
n The substantial cost and clinical commitment (e.g. training, supervision, etc.) of
staffing retrieval teams has led to concern at the potential for too many to be
established causing duplication, low utilisation and wastage.
n The need to be informed by a more robust data set than is currently available. DHBs
are collecting data now during the 2004/05 year which will usefully inform the
development of a business case for a national network of clinical retrieval teams and
air ambulances required to support IHT service needs.
n The need for agreed clinical standards, dispatch protocols and operational processes
to ensure seamless and safe collaboration by DHBs, particularly retrieval teams
n The compliance costs to the health and aviation sector if the current funding model of
23 Crown funders continues, with operators requiring contracts with multiple funding
agencies.
Local Decision-Making
Up to 11 board members sit on each DHB board. Seven members are elected every three
years at the time of local body elections. In addition to the elected members, up to 4
members can be appointed by the Minister of Health, in consultation with his or her
colleagues. The selection process for board member appointments identifies people with
capabilities and skills that contribute to the effective functioning of the board.
15
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
The strategy proposes an affordable, quality national air ambulance network of HEMS and
Fixed Wing Intensive Care air ambulances that will service the needs of patients
throughout New Zealand. However, the strategy recognises the right of local communities
to establish and fund the health services they perceive they require – either through
community donations, local sponsorship or DHB funding.
Need for National Frameworks for Co-ordination
The 21 DHBs throughout New Zealand are responsible to the Minister of Health for the
health of the population. However, in a devolved environment challenges arises on how to
best optimise the use of scarce skills and resources to achieve national health objectives.
The need to federate governance arrangements and planning for services such as air
ambulance will help understand interfaces between district requirements and the national
view (e.g. back-filling of air ambulance flights, inter-district support/backup).
The Ambulance Communications Project2 and the National Framework for Ambulance
Delivery, Retrieval and Transfer3 have highlighted the need for greater national co-
ordination for air ambulance services.
It is important that these services integrate with the broader emergency management
framework and systems for coordinating services to optimise patient need, resource
utilisation and simplify data collection. DHBs are encouraged to ensure that this occurs,
specifically:
n Rescue helicopters, for air ambulance services, and HEMS may only be dispatched
through ambulance communications centres for all missions including IHTs
n National Flight Desk is able to provide a complete information service as to IHT
current and planned IHT operations, that quality data is collected in one place and that
services are coordinated in such a way that urgent calls for assistance can be
responded to with the nearest and most appropriate resource.
Small Rural Hospitals and Transport
Changes in health care delivery have increasingly challenged the availability of some
medical specialities at smaller hospitals. Difficulties to retain staff with specialist skills by
small rural hospitals have increased the need to transport patients quickly and safely to
major hospitals for treatment and rehabilitation.
The lack of specialist skills available in rural areas have also increased the demand for
quicker transport of specialist hospital and paramedical staff to emergencies and the
retrieval of patients to specialist medical facilities.
This strategy proposes greater use of regional tertiary based retrieval services – either
HEMS or Intensive Care Fixed Wing services – in order to deliver more advanced skills to
patients earlier than is otherwise available. In most instances this is through retrieval and
back-up to local services at the scene or point of stabilisation (e.g. GP/rural health centre).
16
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Why we need a strategy for Air Ambulance services
Consistent with established local and international practice, an effective emergency care
system that integrates pre-hospital management, hospital treatment and rehabilitation
services will optimise patient outcomes.
The pre-hospital component of an effective emergency care system needs to provide a
rapid retrieval/primary emergency response ambulance service. That service is provided
primarily by road ambulance and emergency air ambulance helicopters. Fixed wing
aircraft and emergency helicopters are also used for urgent and non-urgent inter-hospital
transfers. Air ambulance services, therefore, need to be well integrated with the other pre-
hospital emergency medical services and the hospital-based components of the
emergency management system to obtain optimal patient outcomes.
The last review of air ambulance services in New Zealand was in 1996. This was a
scoping report for ACC and the combined Regional Health Authorities as to the
establishment of a national air ambulance network. Specifically, it sought to give
operational effect to the Royal Australasian College of Surgeons (RACS) Trauma Care
Guidelines as the affect the provision of emergency air ambulance services.
Since that time, there has been considerable progress in many areas including:
n Standards – new Ambulance Service Sector Standards have been promulgated.
n Service Specifications – common service specifications between the Ministry of
Health and ACC have been implemented.
n Implementation of nationally consistent emergency dispatch protocols
n Development of a protocols framework for the delivery, retrieval and transfer of
patients in New Zealand providing a foundation upon which local protocols for the
transport of patients can be built in conjunction with regional Emergency Care Co-
ordinating Teams established to implement the vision of
Roadside to Bedside.
n Communication Centres – agreement by ACC and the Ministry of Health to a
business case for the rationalisation of the current eight centres to three, based in
Auckland, Wellington and Christchurch, and the implementation of standard modern
technologies to improve quality and service.
These and other developments in the sector have meant that much has been done to
progress many of the issues identified in the 1996 report. However, some of the issues
identified in 1996 persist and there is concern within the sector that supports the need to
look now at how we can improve the current air ambulance services network in New
Zealand. Current issues include:
n Independent contracting approaches by Crown agencies – the 21 DHBs, Ministry of
Health and ACC – has led to fragmentation, duplication and inefficiency including
coverage, funding models and standards
n Concern at poor coordination of flights between regions, or within a region when
things are busy
n Lack of information on activity, patients serviced, quality or cost
n Concern expressed from within the ambulance sector regarding:
n Representation of sector interests by industry bodies
n Part-time pilots with planes competing with dedicated operators
n Concern over conflict of interests
n Inappropriate use of helicopters for long distance travel
n Variable clinical retrieval team staffing practices by DHB
17
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
n Development of regional or district solutions that have promoted greater supply which
appears to have had the effect of:
n lowering quality (e.g. labour cost of pilots, part time operators)
n constraining the investment capability of operators to upgrade machines and
equipment
n creating duplication in frontline and back up aircraft
without necessarily improved quality local communities should expect, or the lower
costs as would naturally occur in a contestable market.
What work is in progress to address these issues?
It is worthwhile to recognise that promising efforts to address many of these issues are
underway:
n DHBs are working collectively to improve cost and activity data
n New communications infrastructure and state of the art communication systems,
funded by ACC and the Ministry of Health are being implemented by Ambulance New
Zealand
n DHBs are clarifying the provision of clinical retrieval teams
n DHBs, with ACC, are developing services specifications for IHTs with minimum quality
levels, response times, etc.
n Ministry of Health is unbundling the Central Region IHT road ambulance funding and
transferring it to the population based funding approach as it is elsewhere in New
Zealand
n Both AIA and Ambulance New Zealand are working to improve trust of their members
in their respective governance arrangements, member representation and
organisational relationships with key stakeholders.
18
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Overview – A Proposed National Network of Air Ambulances
The purpose of this strategy is to outline how New Zealanders can be assured of an
effective and efficient network of air ambulances services to patients in need of pre-
hospital care and transportation to and between health facilities.
The strategy has focused on the three issues that are most important to improving the
patient-focus, effectiveness and efficiency of air ambulance services in New Zealand. For
each of the three issues it makes a number of recommendations and proposes a high
level implementation plan. The three key issues are:
1. Ensuring clarity in the role and definition of Air Ambulance Services in New Zealand
2. Ensuring effective operational coordination of air ambulance operations
3. Improving the air ambulance funding model and contracting process.
Each of these issues is addressed in the chapters that follow.
Aim
The air ambulance network should provide cost effective pre-hospital care and inter-hospital transfer
services complementary to the road ambulance system ensuring that people get the right care, at the
right time, in the right place from the right person.
Principles
Principles that should drive the funding and provision of air ambulance services are:
n Quality emphasis – compliance with standards for patient care and safe transport
n Community participation and choice
n Collegiality and service
n Maintenance of standards through Membership of Ambulance New Zealand (ensures
service quality) and accreditation by AIA (ensures aviation quality)
n Transparent governance, funding and tendering
n Coordination and utilisation
n Efficient and affordable.
19
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Key Themes
More specialist clinical skills to patients, earlier
For the vast majority of patients, earlier access to more specialist skills leads to better
outcomes. Air ambulances have a key role in delivering these skills to patients so that
care can be delivered pre-hospital.
Current demand levels, the need to maintain competency and good practice skills, the
need for dedicated clinical resources from hospitals and the cost of providing more
specialist skills means these need to be distributed through New Zealand and available
primarily as a first response, or back-up to local emergency resources.
Some services of New Zealand already provide the service level proposed by this strategy
for emergency responses by HEMS. The majority of services however, who undertake on
average one mission every three days, are challenged to maintain the competency and
familiarity of clinical skill that a HEMS would provide. This strategy proposes that as a
consistent high quality standard for all of New Zealand.
Faster is not always better
The balance of clinical opinion canvassed during the development of the strategy is that it
is better to wait slightly longer for better quality clinical care than to save up to half an hour
through faster access to care that is not as practiced, as familiar or of the same clinical
standard.
The proximity of provincial centres to regional tertiary centres in New Zealand enables us
to cost effectively support provinces with higher quality services by air. Few provincial
centres are more than 80nm (or 40 minutes flying time) from a regional tertiary hospital
e.g. Queenstown – Dunedin, Invercargill – Dunedin, Wanganui – Wellington, Nelson –
Wellington, Whakatane – Hamilton. New Plymouth – Hamilton is approximately 90nm.
For this to be effective, we will however need to ensure effective support systems are in
place, including robust dispatch criteria and best practice mobilisation times.
Where there are longer distances to tertiary centres and good support from local DHBs,
additional HEMS are proposed by the strategy to complement the proposed HEMS
coverage from tertiary centres (i.e. Whangarei for the Far North and Hastings for East
Coast of the North Island).
On average existing HEMS services respond to 1 mission per day. Using them more than
we currently do is more efficient, more affordable as a nation, and the new standard
proposed by this strategy will provide a better quality of service.
Preservation of urgent local rescue capability
New Zealand geography, our active outdoor lifestyle and our growing tourism industry
means that there will always be a need for local communities to support search and
rescue. Inhospitable terrain, changeable weather patterns and challenging terrain for
rescue pilots means that the unpredictable and occasional call for urgent rescue needs
local rescue helicopters and their pilots with local knowledge to rapidly respond when
called.
20
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
As is the case now, local communities and sponsors contribute substantially to preserve
the capability of these services. This strategy recognises the strong local support for these
services and the important urgent service they provide. These services are particularly
important when:
n Patients require urgent extrication from inhospitable terrain and local pilot skills or
helicopter equipment are appropriate to the needs of the mission
n Patients require transport for critical life-saving skills of the nearest health facility.
It is important that in an integrated system, advanced clinical skills support local rescue
efforts through timely back-up and retrieval.
21
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Defining Air Ambulances Services
There are two key services provided by air ambulances in New Zealand. The first is the
provision of emergency response to the need for pre-hospital care and transportation to a
health facility. This requires the delivery of specialist clinical skills to the patient at the
scene, and the transportation of the patient to an appropriate health facility. In most
instances the local district hospital will be able to provide the patient with definitive care.
Occasionally, a local medical or health centre may be all that is required. On other
occasions, the patient requires the specialist care from a regional tertiary hospital for their
definitive treatment.
The second service is the transfer by air of patients from one health facility to another.
This requires specialist clinical skills to accompany the patient during the transfer. This is
usually in order for more specialised care to be provided to the patient than is otherwise
available locally. Most occasions this means a transfer to one of the five regional tertiary
hospitals – Auckland (including Auckland City, Starship and Middlemore), Hamilton,
Wellington, Christchurch and Dunedin. Clinical staff may be provided by the hospital
sending the patient, or a specialist team from the receiving hospital will retrieve and
accompany the patient back to the receiving hospital.
Emergency Air Ambulance Services
The strategy proposes a network of emergency helicopters that will continue to provide
coverage to all significant populated areas of New Zealand by using existing rescue
helicopters (e.g. Palmerston North, New Plymouth, Greymouth) complemented by an
enhanced network of high-quality and dedicated Helicopter Emergency Medical Services
(HEMS).
The strategy proposes a HEMS network that will provide services to New Zealanders:
n Primarily retrieving patients to the nearest definitive care provider – either the nearest
regional tertiary centre, or local health services where suitable
n Covering approximately 90% of the population, within a radius of major centres and
major incidence of road trauma
n Staffed by flight-trained advanced paramedics, rostered to the HEMS but rotating
through road ambulance duties ensuring well-rounded and practiced skill sets
n Supported by regional hospital services:
n specialist emergency doctors from who are available to respond when required
n dedicated retrieval teams of aero-medical trained doctors and flight nurses
providing support to fixed and rotary wing retrievals
n Providing support to remote health centres and provincial hospitals triaging and
stabilising patients
n Enabling urgent intensive-care inter-hospital transfers, complementing fixed wing and
road ambulance transfers
n Delivering advanced clinical skills in support to local rescue efforts where patients
have been extricated from inhospitable terrain.
The HEMS network will be supported by existing local rescue helicopters whose role will
be predominantly rescue-related, providing urgent local response when patients require
22
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
rescue from inhospitable locations while supporting specialist clinical skills are brought to
the patient.
This network will, as now, provide a range of services to their local communities of which a
part is supporting emergency ambulance services. In some centres, the ‘rescue
helicopter’ may be a roster of local operators as they are now in Queenstown. Rescue
helicopters would not ordinarily transport patients for more than 30 minutes (i.e. HEMS
should already be en-route with specialist clinical skills to uplift the patient for transport to a
definitive care provider).
Emergency Response - Dispatch Criteria
The key to safely transporting any patient is getting the appropriate skills that the patient’s
condition requires to the patient, or the patient to them, within the clinically required time.
The National Framework for Ambulance Delivery, Retrieval and Transfer4 (NFADRT)
proposed a decision tree for assigning skills and the mode of transport to patients
according to need. A Clinical Reference Group advising the strategy believes that these
schema, based on time and skills, are appropriate to base the dispatch of all modes of
aeromedical transport upon. To develop a system equitable for all New Zealanders, this
strategy needs to focus on patient needs, regardless of location, rather than existing
regional protocols.
Getting patients with life threatening trauma to stabilising care, with appropriate escort,
within an hour remains an excepted principle by the Clinical Reference Group. An
Australian study5 appeared to show significant patient survival benefit to having skilled
physician participation in HEMS, and a prospective randomised controlled trial is
underway in Sydney to test this hypothesis. A recent report on HEMS in the United
Kingdom6 identified that HEMS might save 2-3 lives/100 cases of serious blunt trauma but
the difficulty is appropriately assigning aeromedical transport to patients. The decision
assisting program “ProQA” is in use in New Zealand and with consensus adjustment for
New Zealand conditions the Clinical Reference Group believes it should be able to
implement the principles of the NFADRT for the majority of primary air ambulance tasks.
There is also an important issue of equity of ‘access’ to emergency care services, and
HEMS enables a similar level of care to be provided for all patients in the population
wherever they live.
The appropriate allocation of skill to aeromedical patients can be assisted further by
having clinical expertise available to the Ambulance Dispatcher, Various strategies are
used around the world. The London Helicopter Emergency Service has a paramedic
reviewing ambulance calls for potentially serious trauma cases and who further questions
the caller for more detailed information which has substantially reduced the number of
inappropriate HEMS responses7. The French have a physician on 24 hour immediate
contact to provide clinical expertise to the Ambulance Despatch centre to help with the
decision to allocate clinical expertise or aeromedical resource to a case8. The Clinical
Reference Group believes that there is a need to provide aeromedical transport expertise
to the ambulance dispatch centres, augmented by medical expertise on call. These
systems are in use by all the International Medical Assistance organisations and this
model should be able to be used within New Zealand.
Data collection and audit in the ambulance service needs to be improved, and begins with
robust collection at point of dispatch and job oversight. Mortality, while easily measured,
does not provide the only measure of the effectiveness of an ambulance (air or road)
23
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
service. The sector should focus on initiatives that will assist in the measurement of
morbidity and functional independence. While substantially harder to obtain, these
measures provide better information on effectiveness of intervention.
Once implemented, ACP will provide a robust data set and audit methodology that should
be used by ECCTs to review the appropriateness of protocols and the effectiveness with
which they are being adhered to by Ambulance Communications Centres.
Improving and Standardising Clinical Crewing
This strategy proposes an enhanced level of professional staffing for HEMS in line with
emerging clinical evidence from overseas. While internationally there are substantial
differences in the crewing profile of air ambulance services, the use of volunteers is
extremely limited with the emphasis on full-time professional staffing.
Operational crews proposed by this strategy are:
n Standard - 1 pilot, 1 crewman, 1 flight trained advanced paramedic; with a second
paramedic on call as required
n A0 (“A Zero”) - 1 pilot, 1 aero-medical trained doctor, 1 flight trained advanced
paramedic.
An A Zero response does require the support of the base hospital and appears to be
operating at varying degrees throughout New Zealand now. For example, the current
Otago HEMS responds to approximately 40% of missions with medical staff from Dunedin
Hospital onboard. This strategy proposes that HEMS services in New Zealand formalises
and standardise this arrangement to ensure New Zealanders can access superior pre-
hospital care within a reasonable timeframe.
The A0 response is in line with many European crewing models and can be found through
Switzerland; France, Germany, Norway and Italy. While New Zealand would struggle to
afford this as a standard crewing model, the Waikato Hospital experience is that a doctor
on call for A0 responses from the emergency department works very well when required.
Advanced paramedics should be rostered to the HEMS on a 24x7 basis. They should
rotate through regular road ambulance duties ensuring their clinical and patient
management skills are maintained and well rounded. They should also be specially flight
trained to a similar level as is found in medical training for doctors and flight nurse training
for nurses. This will provide in particular provincial and rural New Zealand with greater
confidence in the safety and quality of care they will receive relative to that usually
available to them today.
Operational Area - Urban and Rural Areas
The usefulness of helicopters in remote or rural areas where they can reduce response
times and time to definitive care is widely recognised. Evidence suggests that they can
improve outcomes in time dependent emergencies such as serious trauma and coronary
emergencies. Of course, improved response times could also be achieved by a sufficient
increase in ground ambulance resources, and it may seem therefore that the HEMS
question is just one of cost-effectiveness. However, when the time to definitive hospital
care is also considered, there is no realistic possibility of increasing hospital-based
24
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
emergency care resources to meet the needs of all emergency patients, and
consequently, the effectiveness of HEMS in remote rural areas is clear.
Importantly, the strategy endorses the primary ability of HEMS to deliver expert and
experienced emergency care to the scene, rather than just their ability to improve
response and transfer times. The ability to transport advanced paramedic skills, familiar
and practiced in providing care in air ambulances, is a significant enhancement to the
original concept of the ‘golden hour’ where patients twenty years ago required transport to
hospital for what are today basic life-saving skills available in the pre-hospital environment.
Bringing a doctor to the patient is in many situations advantageous. The model of
emergency department or intensive care doctors responding to particular and well triaged
incidents like that developed by Waikato and Dunedin Hospital are recommended by this
strategy. The advantages are that a single doctor can extend the skills of the advanced
paramedic’s emergency pre-hospital care and that the service is able to more confidently
deliver patients to the most appropriate source of
definitive hospital care, not just the
closest.
Operational Area - Geographical and Population Size
The HEMS coverage proposed by this strategy ensures coverage of over 90% of the New
Zealand population within a 45-60 minute flight time. With better integration with road and
search and rescue operations envisaged through the new ambulance communications
centres, this will provide superior quality of pre-hospital emergency care.
Operational imperatives that the strategy proposes are required to ensure improved
services include:
n Continued refinement in on-scene triage for HEMS back-up based on the clinical
expertise providing on scene triage (e.g. PRIME doctor, advanced paramedic) and
taking into account clinical risks according to best practice protocols (i.e. ProQA being
implemented through Ambulance Communications Project)
n More frequent use of standby to minimise mobilisation times
n More frequent precautionary back-up dispatch (provided there are contracting
arrangements to support this).
HEMS use within a 40-50 kilometre radius of urban areas is not envisaged by this strategy
in the normal course of operations. Exceptions may include an incident where there are
multiple casualties and/or traffic congestion will jeopardise timely service by road
ambulances.
Improving rotary wing air ambulance services
Rotary-wing air ambulances, in contrast to fixed-wing, perform a wide variety of roles.
Over the past decade, the proportion of air ambulance related work has diminished as the
number of helicopters has increased relative to the available air ambulance work. Roles
today incorporate casevac, medivac, inter-hospital transfers and other work such as
search and rescue.
The strategy calls for a stronger emphasis on quality – in terms of patient care and of safe
transport. Quite apart from being substantially more expensive that alternative
25
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
transportation, helicopter travel is inherently risky and should only be used when it is
probable that clinical risks to a patient are outweighed by risks (and relative discomfort)
associated with rotary wing travel.
There are two categories of rotary wing services proposed that are designed to balance
the needs for local DHB flexibility and cost effectiveness with ECCT regional care
coordination, utilisation and quality.
There are a number of components to improving rotary wing air ambulance services:
n Configuring a service network that balances higher quality and skilled response with
the needs for urgent rescue and extrication from inhospitable locations.
n Funding of HEMS should recognise the emergency preparedness (service capacity)
that is required for 24x7 operations.
n Ministry of Health and ACC agreement of common service specifications, quality
measures and process measures to ensure transparent commercial practices
n Collection of quality data measures should to occur as part of routine processes, not
as an additional compliance based data collection
n Ensuring the integrity and quality of the system means that only industry accredited
quality providers who are members of Ambulance New Zealand should provide
Rotary Wing Air Ambulance Services.
Categories of Rotary Wing Service
Two categories of rotary wing services are envisaged, balancing local community
imperatives for urgent response for the extrication of patients from inaccessible locations
and the need to ensure rapid access to superior quality HEMS services (includes aircraft,
utilisation, skills, access to medical crewing, etc).
HEMS Air Ambulances could be based in seven centres, based largely on population and
a 45-60 minute range from base. They will provide primary response to the need for
advanced skills at the scene of an emergency, and will need to work more closely with
ambulance communications centres to better anticipate their needs through better use of
standby and earlier dispatch, cancelling en route if not required. They will also provide
back up to locally based Rescue Helicopters.
Characteristics of Helicopter Emergency Medical Services (HEMS) include:
n Rostered, on-site Advanced Paramedic with air ambulance training, rotated through
road duties for maintenance of rounded clinical skill set
n Ready access/on call emergency specialist (emergency medicine, trauma surgeon,
intensivist) sourced from tertiary DHBs (similar to Waikato’s A0 response) with aero-
medical training
n Experienced pilots
n Purpose built aircraft and facilities
n Fully dedicated, 24x7
n ‘Float’ within broad ECCT regions, delivering patients to appropriate hospital relative to
the scene
n ‘Home’ tertiary DHB for clinical staff training, credentialing and competency
n Capacity funding for emergency response capability matched by reduced fee-for-
service.
26
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Consistent with overseas performance, time from call to HEMS Unit to take-off service
levels should be revised to 5 minutes during the day and 20 minutes at night.
On occasion, HEMS may as is the case now, provide urgent services to Police and the
Rescue Coordination Centre. However, these should in future be requested through the
ambulance communications centre so as to take into account regional emergency
resource demands.
Due to the special service needs of intensive care HEMS, it is proposed that these be
encouraged to be located in:
n Whangarei
n Auckland
n Hamilton or Tauranga
n Hastings
n Wellington
n Christchurch
n Dunedin.
Consideration will also be given to the location of additional rescue helicopter coverage for
the Central Plateau. This could be located in Palmerston North. We seek further
discussion on how to best achieve appropriate coverage in this area and the central North
Island.
Suitable aircraft considered to be a good fit to HEMS service needs in New Zealand would
have the following characteristics:
n Good access to patients
n Capable of 2 stretchers if needed.
n Agile
n High wind start up/shut down
n Operates well in high wind
n Two pilot capable
n Twin engine
n Isolated patient compartment from pilots
n Common in New Zealand
n Good space for reasonable size crew.
While the strategy does not preclude the use of aircraft that are superior in size or
performance for HEMS use, this is a factor for local community and DHB consideration
and should not be reflected in HEMS contracts.
Rescue helicopters, like other search and rescue resources, should continue to be based
close to the district they serve. They will provide speedier extrication of patients when a
HEMS is not immediately available, or there are specialist pilot skills required given the
terrain (e.g. mountain rescue from the Southern Alps).
In most cases where they are within 30 minutes of a definitive care facility, they will
transport the patient. In other cases, they will transport the patient to a safe location where
the patient can be stabilised, and care transferred to a HEMS for transfer to a more distant
definitive care facility (as is the case where patients are often taken from a mountain for
stabilisation in Queenstown, and immediately transferred to Dunedin). They should not
ordinarily be used for lengthy patient transport.
27
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Characteristics of local rescue helicopters include:
n Provide for local community identification and sponsorship
n Integrate with national communications for coordination, backup, safety
n Use of local operators with experienced pilots
n May or may not be dedicated depending on local demand
n Preferably purpose built aircraft and facilities
n Back-up capability for HEMS.
Rescue helicopters will need local arrangements with road ambulance services for on-call
flight trained paramedics.
Given their special circumstances, the strategy and industry recognise that rescue
helicopters should be considered as essential in the following areas to ensure complete
emergency network coverage:
n New Plymouth for urgent mountain and off-shore rescues (approximately
90nm/45mins flying time from Hamilton HEMS)
n Gisborne – for urgent access north to East Cape (approximately 80nm/40mins flying
time from Hastings HEMS)
n Greymouth – for urgent support to West Coast, including mountain rescue and
transport to Greymouth for stabilisation (back up from Christchurch HEMS or
Christchurch or Wellington fixed wing air ambulance)
n Queenstown (approximately 80nm/40mins flying time from Dunedin HEMS)
n Invercargill (approximately 80nm/40mins flying time from Dunedin HEMS)
Rescue helicopters in other areas will be dependant on community ability to support such
a service. Community based rescue helicopters will be engaged as part of the emergency
response network on a fee for service basis at a predetermined contract rate as they are
now.
The two categories of rotary wing services are contrasted in the following table.
28
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Rescue Helicopter
HEMS
Service
Joint MOH/ACC
Joint MOH/ACC
Specification
Member Ambulance NZ
Member Ambulance NZ
Standards
Accredited AIA
Accredited AIA
Clinical skill
Rescue Crewman;
Advanced Paramedic, air trained full time;
set
Minimum Paramedic, as required
Specialist Doctor, air trained on call
Clinical
Local arrangements – Road Ambulance
Local arrangements
resources
(advanced paramedics) and DHB (doctors)
Workload
District
Regional
Dedicated
As required
Yes – 24/7
Exclusive dispatch for air ambulance missions
(including IHT), and aircraft tracking by
Exclusive dispatch for all missions (including
Ambulance Communications. Others e.g.
Flight desk
SAR, IHTs, etc.), and aircraft tracking by
SAR may contact operator directly but
Ambulance Communications
operator must first notify Ambulance
Communications
Timely rescue and extrication of patients from
Delivery of advanced skills to patient/scene,
inhospitable locations and delivery to
Focus
facilitating delivery to definitive care within
advanced skills (HEMS, road ambulance or
ECCT region according to protocol
local hospital)
Contracting
Local arrangements
Nationally coordinated
Funding
Mix of emergency capability (national) and fee
Local arrangements
model
for service
Sponsorship
Local / Regional
National
opportunity
Twin engine
Winch/strop
Winch/strop
Aircraft
Experienced, senior pilots
Prefer experienced pilots
Specification
VFR
IFR capable
Night vision goggles
Night vision goggles
20 minutes day
5 minutes day
Mobilisation
30 minutes night
20 minutes night
Inter-hospital transfer by Air Ambulance
Inter-hospital transfers (IHTs) will be provided by a network of dedicated intensive care
fixed and rotary wing air ambulances:
n Primarily retrieving and repatriating patients from tertiary centres
n Primarily fixed wing, particularly where rotary wing transfers approach or exceed 90
minutes flying time
n Based from DHB hospitals providing dedicated retrieval team capability:
n dedicated retrieval teams of aero-medical trained doctors and flight nurses
providing support to fixed and rotary wing retrievals
n specialist emergency doctors from who are available to respond when required.
29
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
A second tier of fixed wing air ambulances will provide back up to intensive care services,
co-ordinated by the national flight desk when required.
The draft strategy proposes a minimum number of intensive care fixed and rotary wing air
ambulances until such time as the current process by DHBs to better quantify and define
IHT air ambulance service needs is completed. The intensive care services proposed
here will provide for most neonate, paediatric and some adult inter-DHB IHT needs. It is
acknowledged however that the vast majority of current services are provided by the
second tier proposed in this strategy. The strategy proposes that a collective agreement
(/business case) is developed by DHBs late in calendar 2005 based on the activity data
currently being collected on air ambulance IHTs to determine a final configuration of
intensive care and second tier services that will best meet the needs of DHBs for fixed and
rotary wing IHT services.
Of note is the significant variability amongst DHBs as to the choice of mode for routine
IHTs for trips of 100-200km. Some routinely use road ambulances with 2-3 ambulances
travelling inter-city daily, others rotary wing and others fixed wing air ambulances. More
than anything else, this appears largely due to historical practice but clearly has significant
cost implications for some DHBs. A commitment by DHBs to a robust collection of data –
covering road and air IHTs – will be critical to inform any useful review of activity and
agreement as to appropriate levels of quality and cost.
Categories of Fixed Wing Air Ambulances
Fixed-wing air ambulances, with very few exceptions, provide services that are exclusively
inter-hospital transfers (IHTs). These range from quality intensive care air ambulances
requiring a pressurised aircraft, sophisticated equipment and a specialist clinical retrieval
team, through to cost efficient air transfers for stable ambulatory patients.
There are two categories of fixed wing services proposed that are designed to balance the
needs for local DHB flexibility and cost effectiveness with national coordination, utilisation
and quality.
There are a number of components to improving fixed wing air ambulance services:
n Configuring a service network that reflects the range of DHB need – from a need for
quality intensive care air ambulance capability through to cost efficient air transfers for
stable ambulatory patients
n Funding of air ambulance IHTs is by the DHB of domicile. However, improved IHT
coordination requires clearer IHT coordinator roles in DHBs particularly improved out
of hour arrangements to avoid unnecessary delays and confusion regarding clinical
escort requirements and choice of providers
n DHBs and ACC agreement of common service specifications, quality measures and
process measures to ensure transparent commercial practices
n Roster costs are substantial for clinical retrieval teams; therefore the fewer, more
coordinated services, that meet patient clinical needs, are sensible. These need
capability to operate nationally (‘float’) according to need, but will need the appropriate
clinical support environment for supervision, training and peer review that a ‘home’
DHB should provide
n Collection of quality data measures should to occur as part of routine processes, not
as an additional compliance based data collection
30
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
n Ensuring the integrity and quality of the system means that DHBs should use only
industry accredited quality providers who are members of Ambulance New Zealand
n Improved coordination for air ambulance IHTs through a single, specialist flight desk
that will:
n provide a one-call service to locate the nearest and most appropriate air
ambulance
n coordinate logistics (crews, equipment and road ambulance pick up/delivery)
n support of the dialogue between clinical teams at the sending and receiving
hospitals
n provide robust data on activity, service and quality
n lead to improved utilisation of air ambulances
n support better safety and quality.
n Avoiding competing or duplicate communication and coordination for inter-DHB travel
services, while providing local flexibility for intra-DHB IHTs.
Two categories of Fixed Wing Air Ambulances are proposed, balancing local DHB
imperatives for operational flexibility and cost effectiveness and improved national
coordination and support.
Intensive Care Fixed Wing Air Ambulances (“tier one”) should be based in the larger
tertiary centres, which have the infrastructure and staffing to support clinical retrieval
teams. They should operate seamlessly throughout New Zealand, supporting urgent and
scheduled transfer of patients who particularly require intensive care services while in
transit. Intensive Care Fixed Wing Air Ambulances will provide a primary ‘backbone’
service for IHTs located in:
n Auckland
n Wellington
n Christchurch.
An Intensive Care Fixed Wing Air Ambulance network includes:
n Clinical retrieval team staffing based from tertiary DHBs
n Experienced pilots
n Purpose built aircraft and facilities
n Fully dedicated, 24x7
n Ability to ‘float’ nationally, requiring agreed clinical crewing standards by DHBs
n ‘Home’ tertiary DHB for clinical staff training, credentialing and competency
n Capacity funding for emergency (IHT) response capability matched by reduced fee-
for-service.
Stretcher Care Fixed Wing Air Ambulances (“tier two”) should be based in areas of need
as determined by DHBs (such as Hastings by arrangement with Hawkes Bay DHB). They
should be integrated with a national flight desk and be available in support of the Intensive
Care Fixed Wing Air Ambulances as well as providing services to their local DHB(s).
DHBs have expressed concern that the number of retrieval teams is managed to avoid
duplication and excessive cost to the public of New Zealand. This issue should also be
addressed by the DHB collective agreement (/business case) as recommended by this
strategy.
Characteristics of Stretcher Care Fixed Wing Air Ambulances include
:
n Maximise operational flexibility for DHBs
31
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
n Provide for local community identification and sponsorship
n Integrate with national communications for coordination, backup, safety
n Use of local operators with experienced pilots
n May or may not be dedicated depending on local demand
n Preferably purpose built aircraft and facilities.
The two categories of fixed wing air ambulances are contrasted in the following table.
Stretcher
Intensive Care
Service
Joint DHBs/ACC
Joint DHBs/ACC
Specification
Member Ambulance NZ
Member Ambulance NZ
Standards
Accredited AIA
Accredited AIA
Clinical skill
Usually flight nurse, occasional doctor or
Usually doctor, flight nurse and advanced
set
paramedic
paramedic
Clinical
Local DHB arrangements
Tertiary based Retrieval Team
resources
Mainly intra-DHB services and some
Workload
Usually inter-DHB
inter-DHB services
Dedicated
As required
Yes - on demand
Book/dispatch by hospital calling flight desk
Book/dispatch by hospital calling flight desk
Flight desk
Aircraft tracking
Aircraft tracking
Cost-effective and timely support to local
Cost-effective and timely national support.
DHB.
Flight desk manages operations optimising
Focus
Flight desk manages operations optimising
utilisation and inter-district needs, balances
utilisation and inter-district needs, balances
urgent work and back loading
urgent work and back loading
Contracting
Local arrangements
Nationally coordinated
Funding
Mix of emergency capability (national) and fee
Local arrangements
model
for service
Sponsorship
Local / Regional
National
opportunity
Twin engine
Twin engine
Aircraft
Optional - pressurised
Pressurised
Specification
Experienced, senior pilots
Experienced, senior pilots
IFR, de-icing
IFR, de-icing, turbo-prop
IHTs by Rotary Wing Air Ambulance
Two centres for reasons of time, geography, workload and support of the local DHB suit
rotary wing air ambulances as their primary mode of IHT:
n Whangarei (by arrangement with Northland DHB for Kaitaia-Whangarei and
Whangarei-Auckland)
n Hamilton (by arrangement with Midland DHBs).
Helicopters for this role, while largely identical in quality to those proposed for emergency
HEMS network, are additional and complement the seven proposed for the emergency
HEMS backbone service.
32
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Note that it is not proposed that the Dunedin regional tertiary service, for reasons of
workload, requires additional fixed or rotary wing aircraft. With Invercargill and
Queenstown barely 80nm or 35 minutes by helicopter from Dunedin, there is sufficient
capacity in their existing HEMS service with support as required from the Christchurch
based fixed wing intensive care air ambulance.
Linkages with Key Sector Initiatives
Roadside to Bedside: A 24 hour clinically integrated acute management system
Roadside to Bedside should continue to be endorsed by ACC, Ministry of Health and
DHBs as the preferred model for a clinically integrated acute management system for New
Zealand.
Ambulance Communications Centre
This project is vital to the effective operation and coordination of air ambulance services. It
is required to effectively coordinate HEMS and Rescue Helicopter operations and will
provide the infrastructure required for a national flight desk.
National Framework for Delivery, Retrieval and Transfer Protocols
The National Framework for Delivery, Retrieval and Transfer Protocols should continue to
be adopted by DHBs. While there continue to be some debate as to potential costs
associated with their implementation, feedback from consultation suggests they are
increasingly being used as a basis for clarifying, standardising and agreeing local practice
– which appears to have been the purpose of the framework. ECCTs should continue to
provide the forum for localising protocols consistent with the framework.
Ambulance Service Sector Standard
Ambulance Service Sector Standard should be endorsed by ACC, Ministry of Health and
DHBs as a minimum foundation as they related to air ambulance services and continue to
evolve under sector stewardship.
Aviation Industry Association of NZ Air Rescue/Air Ambulance Standards
AIA Air Rescue/Air Ambulance Standards should be endorsed by ACC, Ministry of Health
and DHBs as a minimum foundation as they related to air ambulance services and
continue to evolve under sector stewardship.
33
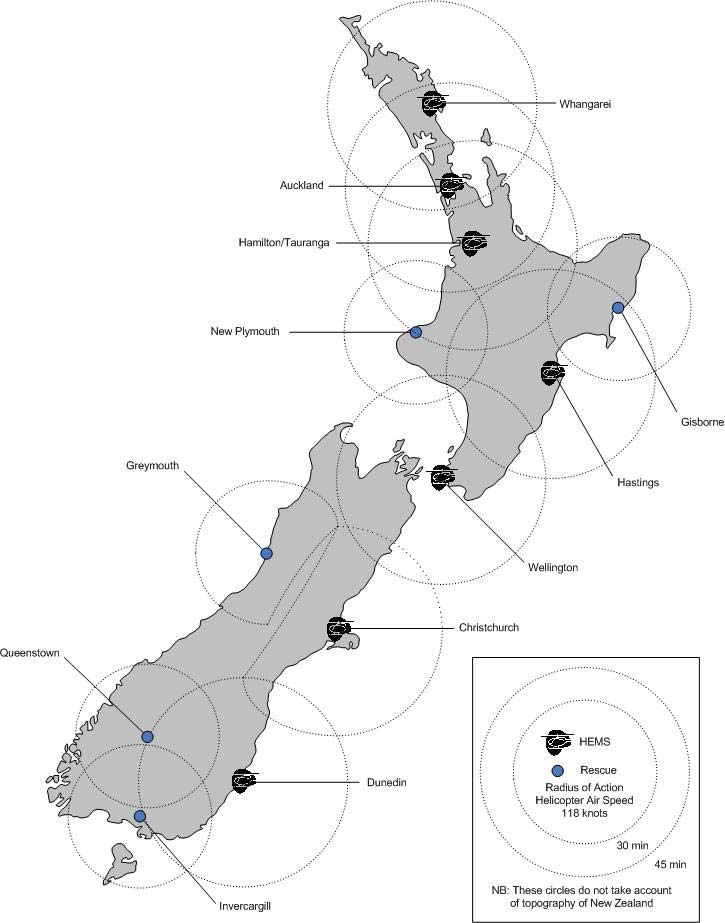
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Geographical Deployment of Air Ambulance Services
Figure 2 – Possible Deployment of HEMS Air Ambulances
We seek further feedback and comment around the ranges of HEMS in the North Island,
particularly in relation to providing a safe reliable emergency air ambulance service within
the geographic, topographic and climatic conditions experienced in this central North
Island
34
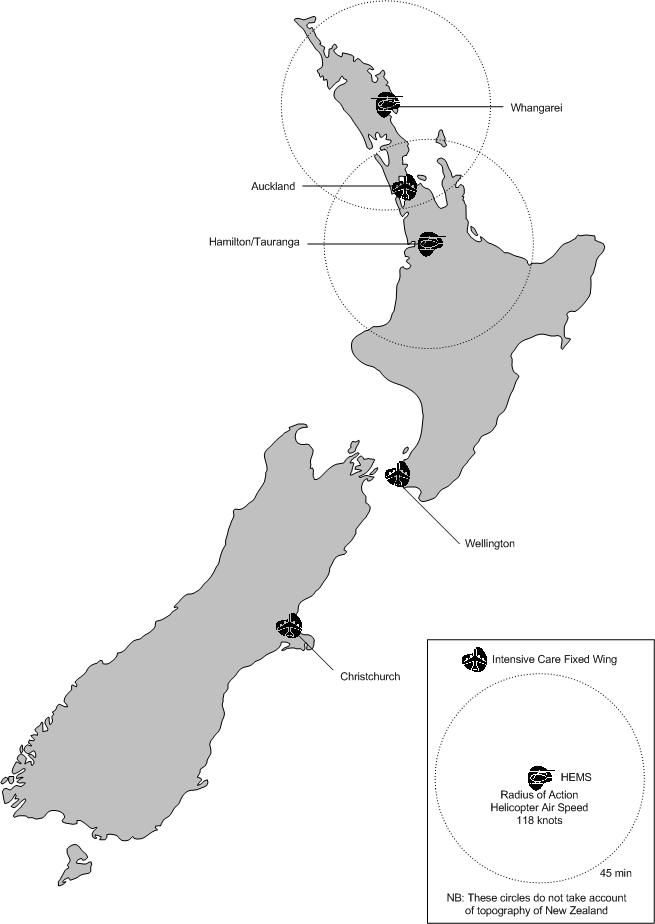
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Figure 2 – Suggested Deployment of IHT Fixed and Rotary Wing Intensive Care Air
Ambulances
35
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Recommendations
1. That the two tier rotary and fixed wing service models are endorsed by DHBs, Ministry
of Health and ACC as the basis of a national air ambulance network.
2. That air ambulance service specifications are revised in line with this strategy by
DHBs, Ministry of Health and ACC.
3. That contracting frameworks of DHBs, Ministry of Health and ACC for air ambulance
services are revised in line with this strategy.
4. That Roadside to Bedside is endorsed by ACC, Ministry of Health and DHBs as the
preferred model for a clinically integrated acute management system for New
Zealand.
5. That ACC, Ambulance New Zealand and relevant DHBs continue to implement ACP
as soon as is practicable, ensuring the systems and infrastructure capability to provide
a national flight desk and standard, robust data on road and air IHTs and patient
domicile.
6. That ACC, Ministry of Health and DHBs continue to work towards implementation of
Ambulance Service Sector Standards as they relate to air ambulance services.
7. That the National Framework for Delivery, Retrieval and Transfer Protocols is adopted
by DHBs under the guidance of ECCTs.
8. That ACC, Ministry of Health and DHBs continue to work towards implementation of
AIA Air Rescue/Air Ambulance Standards.
9. That relevant Medical Colleges, Flight Nurse Association (part of New Zealand Nurses
Organisation) and Ambulance New Zealand establish and implement standardised
flight training requirements for doctors, nurses and advanced paramedics respectively.
36
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Coordinating Air Ambulance Operations
The need for improved coordination of air ambulance services was the most common
issue raised in consultation during the development of this strategy. This section outlines
key recommendations for improving the coordination of air ambulance services in New
Zealand. It is addressed in two parts: emergency services and IHTs.
Emergency Air Ambulance Services
This draft strategy proposes that emergency activation is principally via ambulance
communications centre(s).
As the predominant role of rotary wing air ambulance is emergency work, their integration
with the communications infrastructure that responds road ambulance services is critical.
The decision to activate the helicopter is made by the ambulance dispatcher in response
to the information received by the caller. Primary dispatch would be according to
protocols, with secondary responses being the most common form of dispatch following a
request from an ambulance crew or doctor on scene. Requests, through ambulance
communications centres, can also be made from other emergency services (e.g. mountain
rescue, coastguard) and, in some remote areas, by GPs.
Sound dispatch protocols, while substantively in place, continue to require refinement
while at the same time substantial improvements need to be made in the information on
activity, services, quality and patients that is available for audit and service planning and
analysis.
Coordination for rotary wing air ambulance services through ambulance control rooms will:
n provide a one-call service to locate the nearest and most appropriate emergency
response of skills to the scene
n coordinate logistics with other services (hospitals, police, fire, road ambulance, first
responders, PRIME or other primary care providers)
n support of the dialogue between at-scene clinical teams and potential receiving
hospitals (for stabilisation or definitive care)
n enable dual dispatch where a HEMS delivers more advanced clinical skills to patients
earlier
n provide robust data on activity, service and quality, casemix etc. through state of the
art CAD (Computer Aided Dispatch) systems
n lead to improved utilisation of air ambulances
n support better safety and quality.
37
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
IHT Air Ambulance Services
The effective coordination of IHTs within New Zealand, given our size, resource
constraints, and increasing specialisation of hospital services, requires national
management of inter-hospital transfers by air ambulance.
Key elements of an improved and more coordinated national approach to IHTs include:
n Effective regional coordination by Clinical Transport Coordinators located in each
tertiary centre, supported by local DHB Transport Coordinators (often a duty nurse in
ICU) as per the National Protocols Framework. These coordinators will ensure
effective clinical assessment of patients requiring transfer, articulate the clinically time
urgency agreed between referring and accepting specialist doctors, clinical skills
required during the transfer, clinical capacity at the receiving hospital (including bed
availability), and any required clinical equipment. They also confirm necessary last
minute arrangements such patient condition prior to instigating the transfer.
n The establishment of a single, specialist flight desk that will provide logistical support
to Transport Coordinators, managing aircraft and retrieval team movements and/or a
one-call service to locate the nearest and most appropriate air ambulance, coordinate
logistics (crews, equipment and road ambulance pick up/delivery) and importantly
support the dialogue between clinical teams at the sending and receiving hospitals
n Specialist Clinical advisor for the flight desk to be established as a 24x7 roster of
areomedical trained on-duty Intensive Care Specialists (nominally the Director of the
ICU or their delegate) rotating through the five tertiary centres (and other ICUs with
suitably trained specialists by agreement). Standard procedures will require
development, ensuring clinical oversight over the coordination and scheduling of
intensive care transfers by the national flight desk.
Current issues that require consideration include:
n a desire expressed by DHBs to be able to accurately and cost effectively monitoring
all IHTs, regardless of mode
n a lack of robust and standard data collected on IHT activity and the need for a
systems approach to improve available data (preferably as a by-product of the
process and not as a compliance activity)
n the limited ability within current system to optimise national IHT air ambulance
resources
n existing variations in coordination at regional tertiary level (notably the effective
regional coordination by transfer/flight coordinators at Wellington and Canterbury
hospitals)
n the cumulative costs of retrieval team staffing across many DHBs
n parochial attitudes within regions that constrain national economies of scale relative to
international experience.
Key to improving IHTs by air ambulances will be the data set currently being collected by
DHBs through a collective initiative of DHBNZ. In late 2005, DHBs will be in a position to
develop a collective agreement as to the national need, resource implications, and
configuration of clinical retrieval crewing and air ambulance deployment required for
servicing IHTs.
38
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
National Flight Desk
A National Flight Desk will provide benefits of better staff and aircraft utilisation, improved
service integration and less compliance for data collection. This strategy recognises
existing co-ordination roles in DHBs, particularly those with dedicated transfer teams and
the need to encourage DHBs without a nominated transport coordinator role.
The Flight Desk will support DHB staff and transfer/flight coordinators regarding
aircraft/equipment/staff logistics, particularly when busy and routine options unavailable. It
will provide a knowledge base – one point, one call of capacity and resource now and
scheduled over that day. The role is focused on transfer logistics only: DHB to DHB
dialogue and clinical co-ordination occurs alongside.
Benefits include the ability to better leverage capacity between regions – where fleet/crews
are, and where they are going, while preserving existing regional dispatch practices
(particularly the linking with beds and clinical staff) while establishing a national information
base.
Obtaining economies of scale requires a national flight desk to provide national
coordination of:
n Aircraft movement and mission coordination
n Confirming final clinical capacity/arrangements (e.g. bed availability) with hospital
coordinators
n Dispatch
n Management of appropriate clinical tier/urgency/triage/prioritisation, e.g.
n Back loading
n Diversion
n Competing jobs
n Coordination of resources required end to end (road ambulance to airport, aircraft and
retrieval staff, road ambulance to destination hospital)
n Clinical stewardship, oversight and advice from on-call senior specialist ICU doctors.
There are several considerations that suggest the national flight desk should be
established in the Auckland ambulance communications centre:
n Experience of working with an earlier flight desk model that operated in the Auckland
region until the end of 2003
n The necessary systems infrastructure substantively exists now, without having to wait
an estimated 18-24 months for ACP implementation to be complete in Wellington or
Christchurch.
National Framework for Ambulance Delivery, Retrieval and Transfer
This draft strategy, in recommending enhanced regional tertiary network coordination with
logistical support from a national flight desk, builds on the National Framework for
Ambulance Delivery, Retrieval and Transfer.
The framework was published in April 2003 under the auspices of the memorandum of
understanding between Ambulance New Zealand, ACC and the Ministry of Health by the
39
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Ambulance Protocol Working Group, representing the ambulance sector and key
professional bodies, in consultation with the wider health and disability sector.
It is a protocols framework for the delivery, retrieval and transfer of patients in New
Zealand and was designed to provide a national foundation upon which local protocols for
the delivery, retrieval and transfer of patients can be built in conjunction with regional
Emergency Care Co-ordinating Teams established to implement the vision of Roadside to
Bedside.
Relevant to IHTs by air ambulance, the following exert details an expectation as to the
roles that DHBs are encouraged to consider so as to develop an integrated and
coordinated approach to IHTs.
1.3 Arranging Emergency Inter-hospital Transfers
4.
That in obtaining agreement to transfer a patient from one hospital to another, the on-site doctor responsible at the
sending site is responsible for communicating to the responsible
specialist at the receiving site.
5.
That a referring hospital should ideally only require
one call to obtain specialist advice from a receiving hospital as
to treatment and need for transfer of the patient.
6. That
the
receiving specialist clinician should be responsible for alerting all other relevant specialist services and
for determining the urgency of a transfer.
7.
That an Emergency Inter-Hospital Transfer should be able to be initiated via a
single call by either the sending or
receiving hospital.
1.4 Co-ordination of Emergency Inter-hospital Transfers
8. That
the
DHB base hospital is the default inter-hospital transfer destination within a DHB: Where a patient needs
definitive Specialist Skills not available within a DHB base hospital, regional protocols for inter-DHB transfers for
patients to definitive Specialist Skills are to be endorsed by regional ECCTs.
9. That
retrieval and transfer team resources be based around the main tertiary referral services identified in
Roadside to Bedside (Auckland, Waikato, Wellington, Christchurch and Dunedin) and that the Ministry of Health
and ACC consider the funding arrangements for such teams. These teams should predominantly be
supernumerary retrieval-trained staff, who would better support the safer retrieval and transfer of patients to and
from tertiary centres. The composition and funding of these teams should take account of the role, expertise and
funding of qualified ambulance officers, nursing and medical staff.
10. That
Clinical Transport Co-ordinator role be established the in the main tertiary referral services identified in
Roadside to Bedside. This role would be responsible for implementing the Clinical Transfer Plan agreed between
referring and receiving clinicians in conjunction with the Transport Co-ordinator function (see next paragraph). The
Clinical Plan includes urgency required, transfer team skil s and equipment requirements. The Clinical Transport
Co-ordinator would also (as required) support and co-ordinate intra-regional transfers within their regional
Roadside to Bedside region.i
11. That
Transport Co-ordinator function be established in regions identified in
Roadside to Bedside. This function
would work with the Clinical Transport Co-ordinator and would establish the Transport Plan which co-ordinates
logistics between the referring and receiving hospitals, road and air providers. The Transport Plan would
incorporate scheduling of transfer resources (level and type of care, equipment and mode). The Transport Co-
ordinator would be responsible for communicating arrangements in the Transport Plan to referring and receiving
hospitals, dispatching the necessary resources and for filing the plan with the RCC (for monitoring and data capture
purposes).
1.5 Organisation of ALL Inter-hospital Transfers
12.
That funders consider establishing a function that provides a single source of information related to the retrieval and
transfer of patients by air throughout on-shore New Zealand. This information may be used to improve the co-
ordination, effectiveness and efficiency of inter-hospital transfer. Such a co-ordination service may take into
account all air movements and aircraft locations and would co-ordinate staffing, choice of air modes (rotary wing,
fi
d i
)
d
i
t
40
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Figure 1: Exert from National Framework for Ambulance Delivery, Retrieval and Transfer, April 2003
Decision trees that were developed appear in appendix 4 and are useful in articulating the
clinical coordination between referring and receiving hospitals and the point at which a
flight desk supports operational logistics of a transfer.
Recommendations
10. Ambulance Communications Centres continue to dispatch air ambulance missions:
a. exclusive dispatch of HEMS
b. dispatch of Rescue Helicopters (i.e. also able to be dispatched by other
emergency services as required after notification to Ambulance
Communications Centre)
11. ACC and relevant DHBs to consider the establishment of a National Flight Desk as
soon as practicable, building on the existing capability of the Auckland Ambulance
Communications Centre conjunction with ACP
12. That Auckland Ambulance Communications Centre and DHBs establish knowledge
management systems to support the coordination of IHTs and functioning of the Flight
Desk as described in this strategy
13. DHBs establish retrieval teams in at least the five tertiary centres and limit the
establishment of additional retrieval teams until the completion of a DHB IHT Air
Ambulance Collective Agreement (refer Funding and Contracting Recommendations)
14. Regional Tertiary DHBs establish clinical transport coordinators and transport
coordinator functions, and regional DHBs.
41
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Funding and Contracting of Air Ambulance Services
Ambulance Operators and Air Ambulance Operators have concerns about the present
methods of funding. A number of DHBs have a capped funding arrangement with
emergency ambulance providers which includes a budgeted amount for air ambulance
work. Some air ambulance operators believe that this funding arrangement at times
governs whether the air ambulance will be used or not.
Air ambulance operators have large amounts of capital and fixed costs committed to
ensure their services are available when required. The operators have suggested that
uncertainty of work and income makes it difficult for them to plan their business operations.
Funding
A range of funding models were considered and consulted on. In light of the current
multiple funding approaches, the high cumulative compliance costs for DHBs and
operators and the mix of incentives (both promoting and discouraging air ambulance use),
reviewing the funding model for Crown funds is a key part of moving the air ambulance
sector forward into the future.
Moving to a philosophy of HEMS and intensive care fixed wing air ambulances requires
consideration of funding model implications on the part of DHBs, Ministry of Health and
ACC.
Any change to a funding model, particularly involving 23 Crown agencies (21 DHBs,
Ministry of Health and ACC), is not without challenge e.g. the need for a clear process and
collective agreement to support a combined DHB approach to improving IHT air
ambulance services. There are also costs – both time and effort – required to transition to
an improved funding model.
The draft strategy recommends a mixed model for the future funding of air ambulance
services that provides a consistent pricing framework for national Crown funding: ACC,
Ministry of Health and DHBs. A first priority should be to address the recommended
mixed capacity and fee for service funding recommendations for first tier services (i.e.
HEMS and intensive care fixed wing air ambulances).
This will provide the flexibility to enhance current services in a cost effective manner and
reduce compliance costs for the sector (which in light of the relative proportion of funding
from the Crown, is particularly onerous).
Recommendations
Revision of the funding model for air ambulances should provide an improved set of
incentives for quality, effectiveness, probity and efficiency. The timelines of current
contracts and the lead time in establishing collaborative funding arrangements means that
transition to a new funding model will take a number of years.
42
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Funding recommendations include:
15. That DHBs continue the collection of 12 months of baseline information on IHT node-
node volumes and retrieval team activity to June 2005 to improve understanding of
activity, costs and casemix.
16. That a national price list is developed for air ambulance services including transfer and
retrieval teams.
17. That HEMS are funded on a mixed capacity and fee for service basis, providing for
lower missions costs (on a fee for service arrangement).
18. That national intensive care fixed wing air ambulances are funded on a mixed
capacity and fee for service basis, providing for lower missions costs (on a fee for
service arrangement).
19. That DHBs develop an IHT Air Ambulance collective agreement by the end of 2005
encompassing:
a. National supply agreement for DHB clinical retrieval teams
b. National deployment of fixed and rotary wing aircraft for IHTs
c. National flight desk operating costs.
43
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Draft National Air Ambulance Strategy
Appendices
Appendix 1 – People and Organisations Consulted
There are a substantial number of people who contributed to the development of the
strategy for which the project team and sponsors are grateful. Gratitude is expressed to all
of the many contributors through consultation and workshops; in particular the individuals
and organisations identified below.
New Zealand – People and Organisations Consulted
Civil Aviation Authority
Philips Search and Rescue Trust
Manager of Rotary Wing – General Aviation
Secretary
Police – SAR
Life Flight
National SAR Co-ordinator
General Manager
Order of St John
Taranaki Rescue Helicopter Trust
Director of Ambulance Operations (Northern
Manager
Region)
Northland Health
Auckland Rescue Helicopter Trust
- Chief Executive
Manager of Surgery and Critical Care
– Medical Advisor / NAAS Clinical
Reference Group
Ambulance New Zealand
Hawkes Bay Helicopter Rescue Trust
- Chief Executive
– Previous Chief Executive
Chief Executive
Aviation Industry Association and
Garden City Helicopters Ltd
Air Rescue New Zealand
General Manager
Canterbury DHB
Northland Emergency Services Trust
Canterbury ECCT Chair / NAAS Clinical
Chairman
Reference Group
Waikato DHB
The Square Trust Rescue Helicopter
Midland Trauma Systems Co-ordinator (Regional
Operations Assistant/Flight Nurse
Trauma Service)
44
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Otago DHB
Helicopters Otago Ltd
Otago ECCT Chair / NAAS Clinical Reference
Group
Starship Hospital (Auckland DHB)
Hawkes Bay DHB
Paediatrician /
NAAS Clinical Reference Group
Intensivist / NAAS Clinical Reference Group
Capital Coast DHB
Waikato DHB
Intensivist
/ Clinical Reference Group
Midland ECCT Chair
Garden City Helicopters Ltd
RNZAF
Chief Pilot
Chief of Air Staff
Contributors of Written Feedback to Current State Assessment
Providers
Local Government
• Air Hawkes Bay Ltd
• Far North District Council
• Air
Wanganui
• Hastings District Council
• Auckland Rescue Helicopter Trust
• Hawkes Bay District Council
• Eastland Helicopter Rescue Trust
• Hawkes Bay Regional Council
• Fixed wing air ambulance pilot
• Invercargill City Council – Civil Defence
• Garden City Helicopters Ltd
Emergency Management
• Hawkes Bay Helicopter Rescue Trust
• Napier City Council
• Helipro
• Nelson City Council
• Lakes District Air Rescue Trust
• New Plymouth District Mayor
• Northland Emergency Services Trust
• South Taranaki District Mayor
• Peet
Aviation
Ltd
• Stratford District Deputy Mayor
• Philips Search and Rescue Trust
• Taranaki Regional Council
• Order of St John
• Wairoa District Council
• Taranaki Rescue Helicopter Trust
• Wanganui District Mayor
• The Life Flight Trust
• Wanganui Air Ambulance Trust
District Health Boards
Clinicians
• Auckland
DHB
• Anaesthetic Department – Northland Base
• Canterbury
DHB
Hospital
• Capital and Coast DHB
• CDHB provider arm of air ambulance services
• Good
Health
Wanganui
• Central Region Emergency Care
• Hawkes
Bay
DHB
Coordinating Team
• Lakes
DHB
• Flight
Nurse
• MidCentral
DHB
• Intensive Care Specialist – Auckland City
• Southland
DHB
Hospital
• Tairawhiti
DHB
• Intensive Care Unit – Northland Health
• Taranaki
DHB
• Intensive Care Unit – Tauranga Hospital
• Waikato
DHB
• Joint Faculty of Intensive Care Medicine
(JFICM)
45
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
• Midland Region Emergency Care
Industry
Coordinating Team
• Air Rescue New Zealand
• Midland Regional Trauma Director
• Aviation Industry Association
• Neonatal Service – Christchurch Women’s
• New
Plymouth
Police
Hospital
• Rescue Coordination Centre New Zealand • New Zealand Committee of Australian and
(RCCNZ) – Manager
New Zealand College of Anaesthetists
• Rescue Coordination Centre New Zealand
(ANZCA)
(RCCNZ) – Training Manager
• Otago/Southland Region Emergency Care
• SAR - Police
Coordinating Team
• Royal Australasian College of Surgeons
• Royal Australian and New Zealand College of
Obstetricians and Gynaecologists
• Royal New Zealand College of General
Practitioners
International – People and Organisations Consulted
Aeromedical Services – NSW Health
Metropolitan Ambulance Service – Air
Ambulance Victoria
Manager
Operations Manager
Scottish Ambulance Service
European HEMS and Air Rescue Committee
Head of Ambulance and Emergency Services
Chairman
Ambulance Service – ACT
London Ambulance Service
– Chief Executive
Manager of Operations and Executive Support
- HEMS Co-ordinator
Queensland Emergency Medical Services
Executive Officer
46
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Appendix 2: Progress on Air Ambulance Issues Identified by Cull9
The following is a summary of the key issues identified during research, consultations and
observations of the industry and any progress made to resolve issues:
Issue Identified by Cull
Progress
Lack of adequate, or variations between, dispatch
Remains contentious, however, in reality Cull
protocols
protocols substantially implemented. The
Lack of protocols or guidelines in some
Ambulance Communications Project and the
ambulance regions resulting, in some cases, in
Protocols Framework for Retrieval, Delivery and
delays or inappropriate use of ambulance
Transfer provide a basis to continue to refine.
helicopters and ambulances
ProQA addresses variations in dispatch protocols.
A need to improve training of ambulance control
Currently in Auckland, being adopted nationally
room staff in the complexities of emergency
via Ambulance Communications Project. ACP will
ambulance related telephone triage
enhance transparency and audit capability
Shortage of road ambulance resources, both
Additional analysis required to inform this issue,
vehicles and staff, in smaller remote areas and in
particularly well populated areas of New Zealand
large metropolitan areas where single crewed
that do not have access to advanced paramedic
ambulances can still attend emergencies
skills locally.
Training (qualifications) and experience of road
This remains an issue in some regions – refer
ambulance staff, particularly volunteers
above issue.
Lack of inter-control room liaison (in some
The Ambulance Communications Project will
regions), which results in poor co-ordination and
address this issue through newer technologies
use of resources, and possible delays to incidents
and ability for 3 proposed new Ambulance Control
occurring near regional boarders
Rooms to act as a ‘virtual’ single Control Room
Lack of national and regional co-ordination of non-
emergency air ambulance flights (in some
This remains an issue. The National Flight Desk
regions), resulting in higher costs per trip and less
proposed in this strategy should resolve.
than optimal use of resources
The Protocols Framework for Retrieval, Delivery
Lack of protocols or guidelines (in some regions),
and Transfer provides framework for ECCTs to
to ensure patients are transported to the most
develop regional protocols. However, remains an
appropriate medical facility for the patient’s injury
issue in some regions and is a key issue for
or illness
ECCTs to address.
PRIME (Primary Response in Medical
Emergency) aims to ensure high quality access to
Lack of protocols or guidelines (in some regions),
medical emergency treatment. The scheme funds
to ensure the services of rural doctors are utilised
general practitioners and practice nurses to attend
when necessary
emergencies and has the support of ACC, the
HFA, the New Zealand Rural GP Network, and
the Order of St John.
Lack of emergency ambulance service contracts
Ministry of Health and ACC have developed
(in some regions) with clear service delivery
standard service specifications and intend to have
standards and monitoring and auditing
a joint funding manager
requirements
47
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Current Air Ambulance Issues
The following is a summary of the key issues identified during research, consultations and
observations of the industry and any progress made to resolve issues:
Current Issue
Progress
Over capacity exists within the air ambulance
This still remains an issue. The HEMS network
service resulting in low utilisation of aircraft.
proposed in this strategy, with support from local
rescue capability, will address this issue. DHB
collective agreement on IHTs also proposed in this
strategy should address fixed wing aircraft.
In some regions, resources are used inefficiently
The proposed HEMS network provides greater
and are poorly co-ordinated
consistency in quality and access.
Variance with call out procedures in some
The National Flight Desk proposed in this strategy
ambulance areas, and a reluctance to use air
should resolve.
ambulances in some parts of New Zealand
Transportation of patients, at times, to
This remains an issue in two main areas:
inappropriate care facilities
1. Not all DHBs have yet to implement National
Delivery, Retrieval and Transfer Protocols
Framework in conjunction with their ECCT
2. Lack of clarity in role for immediate extrication
by “rescue” helicopters with subsequent
clinical support from “air ambulance”
helicopter. The proposed HEMS network
provides greater consistency in quality and
access.
Lack of accessible, valid and reliable information
ACP will enhance transparency and audit
on which to base decisions
capability. Contracting frameworks to address
integrity and transparency of air ambulance
services.
Lack of conclusive research, both nationally and
The proposed HEMS network provides greater
internationally, on patient outcomes and cost
consistency in quality and access, combined in
benefit of air ambulance use
appropriate areas with local rescue capability.
Lack of common service standards
Membership of AIA and Ambulance New Zealand
should be mandatory for all services funded by
DHBs, as is the case for Ministry of Health and
ACC now.
Lack of appropriate helicopter access to some
Hospitals where a lack of suitable landing pads
major hospitals
result in undue patient delays and additional road
ambulance use include:
- Akaroa
- Ashburton
- Christchurch
- Greymouth
- Hutt
Valley
- New
Plymouth
- Palmerston
North
- Tauranga
- Timaru
and
48
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Current Issue
Progress
- Waitakere.
Fragmentation of purchasing (e.g. DHB payments
Funding approach proposed in this strategy
to ambulance operators for emergency medical
should address.
cases and inter-hospital fee for services, ACC fee
for service for accident cases as required by
current regulations
Lack of a review system to audit nationally the use
ACP will enhance transparency and audit
of air ambulance services
capability. Contracting frameworks to address
integrity and transparency of air ambulance
services.
Tensions between operators of helicopter
ACP will enhance transparency and audit
services, especially in rural areas
capability.
Varying skill mix of attendant services for different
The proposed HEMS network provides greater
levels of mission training and credentialing
consistency in staff training, competency and
workload.
Significant increase in use of air ambulances in
DHB collective agreement on IHTs proposed by
recent years, which has lead to concerns about
this strategy should address.
costs
Lack of integration at many levels concerning:
The National Flight Desk, funding approach
n Fixed wing and helicopters
proposed in this strategy should contribute to
n Funding
improvements as will ACP.
n Emergency services/inter-hospital services
n Links between air ambulance services and
hospital based emergency departments and
intensive care
Lack of formally defined relationships between
Continued efforts to improve stakeholder
road and air ambulance operators
engagement – by AIA and Ambulance NZ will
improve.
Impact of changes in current air ambulance
The proposed HEMS network provides greater
infrastructure for patient outcomes (e.g.
consistency in quality and access, combined in
equipment, cost for providers)
appropriate areas with local rescue capability.
Infection control issues in terms of movement of
DHB collective agreement on IHTs proposed by
patients between service facilities
this strategy should address.
49
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Appendix 3: Aircraft Type and Standards
AIA, together with CAA involvement, have put together standards for various categories of
air ambulance10. AIA also have auditing procedures to ensure that aircraft registered in
particular categories meet the Standards. However, currently operators are not
contractually bound to adhere to AIA categories (except for ACC contracts that require AIA
accreditation to any one of the following categories). Accreditation to AIA categories is
mandatory for all members of the Air Ambulance/Air Rescue Division of AIA, but not for
operators who do not belong to AIA.
AIA is currently reviewing these categories with a view to simplifying and improving the
framework. Existing categories are:
Category A – Intensive Care Air Ambulance (IFR)
An ‘Intensive Care Air Ambulance’ shall be used to transport patients who may require
continuous attachment to a ventilator, other means of life support and/or physiological
monitoring throughout the flight.
Category B – Rapid Response Air Ambulance (VFR)
A ‘Rapid Response Air Ambulance’ shall be used to transport patients needing intensive
care and continuous treatment and/or monitoring prior to initial hospitalisation, and usually
needing emplanement at or near the site of an accident soon after its occurrence.
Category C – Stretcher Care Air Ambulance
A ‘Stretcher Care Air Ambulance’ shall be used to transport patients needing to be
transferred on a stretcher and needing some medical attention, but not intensive care
during flight. Some monitoring might be required. The patient would usually be transferring
from one hospital to another.
Category D – Seated Care Air Ambulance
A ‘Seated Care Air Ambulance’ shall be used to transport patients who are semi-mobile,
perhaps convalescent (or a walking casualty) and who may need to be
embarked/disembarked using a wheelchair or other forms of assistance. There is little
need for on-going care, but a risk of some form of incapacitation during flight could arise.
Seated care patients include post-operative stable patients transferring between hospitals.
Category E – Independent Patient Air Transport (VFR/IFR)
An ‘Independent Patient Air Transport’ aircraft may be used to transport patients who do
not require an air ambulance or attendant. No wheelchair is needed during
embarkation/disembarkation.
Category F – Search and Rescue Aircraft
A ‘Search and Rescue’ aircraft may be fixed wing or rotary wing suitably equipped with
navigation, communications and rescue capabilities and may include any category of air
ambulance.
50
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Appendix 4: Decision Trees for Delivery, Retrieval and Transfer
The following material has been copied from the National Framework for Delivery Retrieval and Transfer Protocols.
A Continuum of Decisions
Key decisions in the emergency response and transportation of patients with illness or injury are shown in the
following figure. In particular, it shows the alignment of Dispatch Protocols (encompassing the priority and type of
an emergency response) with the three protocol components documented here.
Note that in the following figure:
n ALS means Advanced Life Support, BLS means Basic Life Support and are defined in national
Ambulance Standards
n RCC means the Regional Communications Centres, envisaged by the Ambulance
Communications Project
n SSP means a Specialist Skill Provider, ASP means an Advanced Skill Provider and are defined in
[the National Framework for Delivery Retrieval and Transfer Protocols] document.
Nature
u of f
Delivery
e
Ret
e rieva
r
l
ieva
Transfer
r
Cal Priority
Res
Re pon
o se
s
Deci
c sion
o
Decisi
ecis on
Decision
eci
NEW ZEALAND AMB
A
UL
U AN
A C E
EP
R OT
O OC
O O LS
L
DELI
L VE
V R Y PR
P O TO
T CO
C L - P ATIE
I NT D ES
E TI NAT
N
IO
I N
D oe
o s
e
s t
h
t e
e p
at
a iten
e t
n n
e
n ed
e
d
Spec
e i
c a
i l
a i
l s
i t
Re fe
f r
e to
t
D1
Sk
S i
k ll
l
Yes
l
Ye
l
int
in e
t r
e ve
v nti
n o n to
n e
to na
n bl
b e r
e et
e rire val
va
RE
R TR
T IEVAL
I
N EW
W ZE
Z AL
A AN
A D A
M
A B UL
U AN
A CE
C P
R OT
O OC
O OL
O S
N EW
W ZE
Z AL
A AN
A D AM
A B UL
U AN
A CE
C PR OT
O OC
O OL
O S
fr o m th
m e
th ir
r cur
cu r en
e t
n loca
o
tion
o ?
TRE
TR E
PAT
PA IEN
I
T
EN RE
R TRI
R E
I V AL
A F
R
F OM
O S
C
S EN
E E P
RO
R TOC
O O
C L
TR ANSFER PR OT
O OC
O OL
O - IN
I TER
E -H
- O SP
S IT
I A L
N o
Do
D e
o s
e t
h
t e
h
e p
at
a it en
e t
n
t n
ee
e d
e
D2
TIM
I E CR IT
I IC
I AL
1
Yes
Ye
Do
D e
o s
e
s th
t e
h
e p
at
a ite nt
n
t n
ee
e d
e
TIME
d
TIM
d
TI
Ref
Re e
f r
e to
Ad
A v
d an
a ce
c d Ski
k l
i l
l l
int
in e
t r ve
v nt
n ito n
n NO
N T
t
T
N o
R 1
T1
Is
I
s th
t i
h s
s h
o
h sp
s ita
t l
a d
e
d fifn ed
e
d a
s
a p
r
p o vid
v in g
No
av
a a
v i
a lab
a l
b e
e a
t
t t
he
h
e S
C EN
E E?
1
E?
E
CR
C I
R T
I IC
I AL
A Spec
e i
c alis
a t
lis Sk ill
Se
S t
DELI
L VE
V R Y
th is se
s
r
se vic
v e?
N o
e
o
int
n er
e ve
v n
e t
n ito n?
n
TR
T EE
E
Do
D e
o s
s a
n
a
n a
gr
g ee
e d
e
RE
R GI
G ON
O AL
A
Re
R fe
f r
e
r a
g
a re
r e
e d
D3
PRO
R TO
T CO
C L
L
al
a r ea
e d
a y
y d
i
d r e ct
c
t t
h
t e
Yes
he
Ye
he
REGI
G O
I N
O AL
Yes
Ye
Yes
Ye
di
d s po
p s
o i
s tit on
o
n o
f
o
f y
o
y u
o r p
a
p t
a it en
e t
n ?
PR
P OT
O OC
O OL
O
C ON
O S
N UL
U T WI
T W TH
I
SPE
P CI
C A
I LI
A S
LI T
CO
C NS
N UL
U T W IT
I H SPEC
H
IA
I L
A IST
I
Do n
Do o
n t T
t ra
r nsf
n e
sf r
N o
Cons
C
u
ons l
u t w
t
i
w t
i h
D oe
o s
e
s t
he
h
e p
at
a iten
e t
t n
ee
e d
e
d
TI
TM
I E
D4
CR
C ITIC AL
A Sp
S ec
e ial
ia is
i t
s Skill
Yes
Ye
D EF
E IN
I IT
I I
T VE
2
kill
k
int
in e
t r
e ve
v nt
n ito n?
CAR E
n?
n
R 2
Wi
W l l re
r tr
t ie
r va
v l ta
l t ke
k m
o
m r
o e
e t
ha
h n
a
n t
h
t e
Sp
S ec
e ialis
ia t
h
list
lis
N o
T2
No
N o
TIM
I E CRI
E
TIC
I AL
A
Is
I
s th
t e
h t
e r
t an
a sf
s e
f r
e AC CEPT
C
ED?
ED
timefr
e am
a e?
e
N EAR
E
EST
AR
Do
D e
o s
e t
h
t e
h
e p
at
a it en
e t
n
t n
ee
e d
e
TIM
I E
M SEN SI
S TI
TV
I E
Yes
Ye
3
D5
E
D5
SPEC
SP
I
EC AL
A I
L ST
Ad
A va
v nc
n ed
e S
ki
k l
i l
l
pr
p ov
o i
v de
d r?
r
Yes
( e.
e g
. . jo
.
int
in r
t elo
e c
lo at
a it on
o ,
n I
, V
I p ain
a r
in eli
e ef
e )
Ye
f)
f
SK
S IL
I L
Hot/
L
Yes
/
Ye
N o
Do
D e
o s
e t
h
t e
h
e p
at
a it en
e t
n
t n
ee
e d
e
d
Spec
e i
c a
i l
a is
i t
s
PRO
PR V
O ID
I ER
Cal
Ca l
ER
l
N o
R 3
R ou
o t
u itne
n T
r
T an
a s
n f
s e
f r
Cons
C
u
ons l
u t w
t
i
w t
i h
3
h
No
Nat
Na io
i na
n l
Do
D e
o s
e t
h
t e
h
e p
at
a it en
e t
n
t n
ee
e d
e
Sk
S ill Set
e
in te
t r
e ve
v n
e t
n ito n
n f
or
o
T3
O R,
R
, i f
f ne
n e
e d
Is thi
th s T
s IM
I
E C
E RI
R TI
T CA
C L?
D6
L
D6
TIM
I E
M SEN SI
S TI
TV
I E
D EF
E IN
I IT
I I
T VE
4
E
Tran
a s
n fe
f r
( de
d t
e e
t r mi
mn e
e e
sc
s o
c r
o t
t ty
t p
y e
p
Spe
p c
e ialis
ia t
lis Sk
S ill
pr
p ov
o i
v de
d r?
CAR E
ex
e t
x r
t ac
a t
c ion
o ?
Ad
A va
v n
a c
n e
c d S
d k
S ills,
ills
r?
r
Cold
Sp
S ec
e ialis
ia t
d
lis
3
4
Sk ill Set
in ter ventio n f or
O R, if nee d
extr act ion ?
Ad vance d Sk ills
- se
s e
e b
e
b l
e o w)
De
D s
e k
w
sk
s
Yes
N EAR
E
EST
Yes
AR
Yes
Yes
4
Ye
ADVAN
AD
C
VAN ED
E
Cal
Ca l
l
Do
D e
o s
e r
e
r tr
t ir e va
v l a
n
a d
d S
pe
p c
e i
c al
a is t
t S
ki
k ll
SK
S IL
I L
IM
I MEDI ATE
LL
L
N o
R 4
Set
e
t i nt
n er
e ve
v n
e titon
o
n h
a ve
v th
t e
h
e
pot ent
e i
nt a
i l
T4
Nat
Na io
i na
n l
al
a
PRO
PR V
O ID
I ER
Ca
C n
a
n t
he
h
e p
a
p titen
e t
t w
ai
a t
t f
o
f r
o t
r
t an
a s
n f
s e
f r
e
No
Tran
a sf
s er
e :
ER
r
t o im
i prov
pr
e out
e
c
out ome
?
tea
te m
m
OR
O
R
re
r tr
t ie
r va
v l t
a e
l t a m?
m
Any a
y v
a a
v il
i a
l b
a le
Tran
a s
n fe
f r
l
r
es
e c
s o
c rt
De
D s
e k
s
Yes
Ye
Yes
Ye
Cal
Ca l
l
R 5
N o
EM
E ERG
R ENCY
o
Is
I
s t
h
t e
h r
e e
e a
r
et
e r
t ie va
v l t
e
t am
a a
va
v i
a lab
a le?
e
Do
D
o we
w h
e a
h ve
v s
e kills
k
an
a d
n
d s
t
s a
t ff
f
f to
t
o s
en
e d
No
nd
n
Nat
Na io
i na
n l
T5
R ET
E RI
R EV
E AL
A
N EAR
E
EST
AR
wi
w t h
h p
a
p t
a ien
e t
?
Tran
a s
n fe
f r
1
2
( de
d t
e e
t r mi
mn e
e e
sc
s o
c r
o t
t ty
t p
y e
p
ADVAN
AD
C
VAN ED
E
De
D s
e k
s
- se
s e
e b
e
b l
e o w)
w
Yes
Ye
SK
S IL
I L
L
Yes
Ye
PRO
PR V
O ID
I ER
Cal
Ca l
l
Ca
C n
a re
r tri
tr e va l tea
te m g et to
e
p
t to ati
a en
e t
n
N o
EM
E ERG
R ENCY
2
o
R 6
T6
Nat
Na io
i na
n l
T6
sce ne
n w
e it
wi
w hi
h n e
x
e t
x r
t a ct
c iton
o
n titme?
ALS /
AL
BLS
e
As
A se mb
m l
b e T
e
ra
r nsf
n er
e te
a
te m
Tr
T an
a s
n fe
f r
m
e
m
Tran
a s
n fe
f r
( de
d t
e e
t r mi
mn e
e e
sc
s o
c r
o t
t ty
t p
y e
p
De
D s
e k
s
- se
s e
e b
e
b l
e o w)
LS
L
w
Yes
Ye
RE
R TR
T IEVE T
I
O
EVE T
SPEC
SP
I
EC AL
A I
L ST
SK
S IL
I L
L
PRO
PR V
O ID
I ER
( De
D f
e init
in i
it ve
v C ar
a e
r )
What priority
What type
Where to
Does the patient Does the patient
of response?
(mode and skill)
deliver the
need skill
need transfer to
of response?
patient to
delivered to
specialist skills
skills, within
them (retrieval)?
(inter-hospital
needed time?
transfer)?
ROLES
Regional
Regional
Provider with
Provider with
Provider with
Communications
Communications Patient
Patient
Patient
Centre
Centre
Assisted by RCC
Assisted by RCC & Assisted by SSP &
SSP
Transport
PROCESS AND DECISION SUPPORT
co-ordinator
ProQA assists to
National Ambulance
Delivery protocol
Retrieval protocol
Transfer protocol
assign one of 132
Standards support
assists determine
assists determine
assists determine the
determinants of cal
assignment of ALS
that based on
whether a patient’s
need and form of
priority
(e.g. paramedic or GP)
patient need for
need for specialist
transfer from one
or BLS (ambulance
skills within
skil s require their
treatment setting to a
officer or first
timeframe, patient is transport to the
SSP
responder)
delivered to nearest
patient’s location
ASP or SSP
Figure 2 - Continuum of Decisions in an Emergency Response
Three decision trees were developed to provide a simple, timely and practical process to assist the decision-
makers. The decision trees are relatively generic in nature and consequently should have wide application.
Equally they are not overly prescriptive and allow the decision-maker some flexibility. They are as follows:
n Decision Tree 1 – Delivery
n Decision Tree 2 – Retrieval from Scene
n Decision Tree 3 – Transfer (Inter-hospital).
51
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Decision Tree 1 – Delivery
NEW ZEALAND AMBULANCE PROTOCOLS
DELIVERY PROTOCOL - PATIENT DESTINATION
Does the patient need
Specialist
Refer to
Yes
Skill intervention to enable retrieval
RETRIEVAL
D1
from their current location?
TREE
No
Does the patient need
TIME CRITICAL Advanced Skill
Yes
D2
1
intervention NOT available at the
SCENE?
No
Does an agreed
Refer agreed
REGIONAL PROTOCOL
Yes
REGIONAL
D3 already direct the disposition of your
PROTOCOL
patient?
No
CONSULT WITH SPECIALIST
Does the patient need
Yes
TIME CRITICAL Specialist Skill
D4
2
intervention?
No
Does the patient need
Yes
TIME SENSITIVE Advanced Skills?
D5
3
(e.g. joint relocation, IV pain relief)
No
Does the patient need
TIME SENSITIVE Specialist Skills?
D6
4
3
4
NEAREST ADVANCED
DEFINITIVE SPECIALIST
Time Sensitive
SKILL PROVIDER
SKILL PROVIDER
(not Time Critical)
1
2
FASTEST ACCESS TO
ADVANCED SKILL
DEFINITIVE SPECIALIST
Time Critical
PROVIDER
SKILL PROVIDER
(via skill to scene or
patient to skill)
Advanced Skills
Specialist Skills
52
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Decision Tree 2 – Retrieval from Scene
NEW ZEALAND AMBULANCE PROTOCOLS
PATIENT RETRIEVAL FROM SCENE PROTOCOL
Does the patient need
No
TIME CRITICAL Specialist Skill
R1
for
EXTRICATION or
TRANSFER FROM SCENE?
Yes
CONSULT WITH SPECIALIST
Does retrieval and Specialist Skill
Refer to
No
Set intervention have the
DELIVERY
R2
potential to improve outcome?
TREE
Yes
D2
No
Is there a retrieval team available?
R3
Yes
Can retrieval team get to patient
No
scene within an
R4
APPROPRIATE TIMEFRAME?
Yes
RETRIEVE TO
SPECIALIST
SKILL
PROVIDER
(Definitive Care)
53
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
Decision Tree 3 – Transfer (Inter-hospital)
NEW ZEALAND AMBULANCE PROTOCOLS
TRANSFER PROTOCOL - INTER-HOSPITAL
Is the referring hospital defined as
Yes
T1
providing this service?
No
CONSULT WITH SPECIALIST
Do not Transfer
No
Is the transfer ACCEPTED?
T2
Yes
No
Is this TIME CRITICAL?
Routine Transfer
T3
Yes
IMMEDIATE
Can the patient wait for transfer
No
Transfer:
T4
er
team
OR retrieval team?
Best available
escort
Yes
e Transf
at
g
Do we have skills and staff to send
No
EMERGE
ERG N
E C
N Y
T5
with patient ?
Insti
RE
R TR
T I
R EVAL
EVA
Yes
EMERGE
ERG N
E C
N Y
Transfer
e
54
DRAFT FOR CONSULTATION
DRAFT NATIONAL AIR AMBULANCE STRATEGY
References
1 Ministry of Health. (1999). Roadside to bedside: Developing a 24 hour clinically integrated acute management
system for New Zealand. Wellington.
2 Ambulance Communications Project. Ambulance New Zealand. February 2004.
3 National Framework for Ambulance Delivery, Retrieval and Transfer. The Ambulance Protocols Working Group.
March 2003.
4 The Ambulance Protocols Working Group. National Framework for Ambulance Delivery Retrieval and Transfer.
Published April 2003 by Ambulance New Zealand, the Ministry of Health and ACC under their Memorandum of
Understanding. Section 6.
5 Garner A, Rashford S, Lee A, Bartolacci R. Addition of physicians to paramedic helicopter services decreases
blunt trauma mortality. Aust. N.Z.J.Surgery 1999; 69: 697-701.
6 J. Nicholl, J. Turner, K. Stevens et al. A review of the costs and benefits of Helicopter Emergency Ambulance
Services in England and Wales. Final report to the Department of Health. 3 July 2003. p 70.
7 Coats T, Newton A. Call selection for the Helicopter Emergency Medical Service: Implications for ambulance
control. J. R. Soc Med 1994; 87: 208-210.
8 Nikkanen H, Pouges C, Jacobs L. Emergency medicine in France. Annals of Emergency Medicine 1998;
31:1 116-120.
9 A National Air Ambulance Network for New Zealand: A Scoping Report for the ACC and Combined RHA’s, ACC
1996.
10 The Aviation Industry Association of NZ Air Rescue/Air Ambulance Standards Manual. Aviation Industry
Association of NZ (Inc). Version 8, July 2003.
55