
Sent by:
To: <MentalHealth&[email address]>,
Released generalmanager@mhaps.
cc:
org.nz
bcc:
12/01/2017 11:21 a.m.
Subject: Nga Hau E Wha Contract
Ngā mihi mahana ki a koe,
Hoping this finds you well and refreshed after the Christmas / New Year break.
under the Official Information Act 1982
Please find attached the 6 monthly documentation for Nga Hau E Wha comprising the narrative and
financial reports.
With all best wishes,
Nāku, nā
Sue
Sue Ricketts
General Manager
MHAPS – Mental Health Advocacy and Peer Support
826 Colombo Street, Christchurch, 8013
P.O. Box 33332, Barrington, Christchurch 8244
Phone: 365 9479
s 9(2)(a)
www.mhaps.org.nz


2016 July to December report NHEW.xlsx June - Dec 2016 MOH Report. Final VGJ.docx
Released
under the Official Information Act 1982


Released
HALF YEARLY FINANCIAL REPORT
under the Official Information Act 1982
REPORTING DATE:
11th January 2017
PERIOD DATE:
1st July 2016 - 31st December 2016
EXPENDITURE ITEM
BUDGET (12 month) ACTUAL (6 month)
Travel (airfares, taxis, shuttles)
$ 18,
800.00 $ 6,
971.89
Accommodation
$ 4,
800.00 $ 2,
332.94
Venue hire, catering and other meeting costs
$ 6,
400.00 $ 942.
95
Administration allocation
$ 3,
880.00 $ 1,
068.58
Meeting fees
$ 6,
120.00 $ 3,
490.00
Overheads (MHAPS' fee)
$ 8,
000.00 $ 4,
000.00
TOTAL $ 48,
000.00 $ 18,
806.36
Please note $1364.35 are for airfares for the February meeting. The taxi charges can be very
late coming through as it is dependant on when the taxi company puts there claim through.
Released
Agreement 570458 / 344777/00 – Ngā Hau e Whā Report to Ministry of Health
under the Official Information Act 1982
\
Ngā Hau e Whā
June to December 2016
Report to Ministry of Health
1
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Table of Contents
Page number
1. Meetings held during reporting period ................................................................................................. 3
2. Membership Updates January 2016 – June 2016 .................................................................................. 4
under the Official Information Act 1982
3. Ngā Hau e Whā Strategic Plan 2016-2020 .............................................................................................. 4
4. Compliance ........................................................................................................................................... 5
5. Terms of Reference ................................................................................................................................ 5
6. Overview of national issues or chal enges in the Mental Health and Addiction sector .......................... 8
7. Overview of areas of best practice in the Mental Health and Addictions sector ................................. 17
8. Changes or developments that have come out of Rising to the Chal enge .......................................... 19
9. Impact of Ngā Hau e Whā ..................................................................................................................... 21
Regional Reports
10. Tui Taurua-Peihopa - Northland .......................................................................................................... 23
11. Guy Baker - Midland ............................................................................................................................ 27
12. Jak Wild - Central North ...................................................................................................................... 31
13. Kieran Moorhead - Northern – Auckland............................................................................................. 41
14. Victoria Roberts - Central South .......................................................................................................... 51
15. Julie Witla and Grant Cooper - Southern ............................................................................................. 64
2
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Agreement 570458 / 344777/00 – Ngā Hau e Whā Report to Ministry of Health
2.2
Meetings Held During Reporting Period
Present
Victoria Roberts (Central)
Julie Whitla (Vice Chair)
(Chair)
(Southern)
under the Official Information Act 1982
Tui Taurua (Northern)
Kieran Moorhead (Northern) By
phone
Grant Cooper (Southern)
Guy Baker (Midland)
Jak Wild (Central)
Vacancy Midland)
Present
Victoria Roberts (Central)
Julie Whitla (Southern) (Vice
(Chair)
Chair)
Guy Baker (Midland)
Grant Cooper (Southern)
Kieran Moorhead(Northern)
Tui Taurua (Northern)
Jak Wild (Central)
Vacancy (Midland)
In the six months from June 2016 Ngā Hau e Whā has hosted the following guests:
Dr John Crawshaw - Director of Mental Health – Ministry of Health
Emma Tonks Fund Administrator – Ministry of Health
Kevin Allan – Mental Health Commissioner
Grant O’Brien - Health and Disability Commission
Rod Bartling – Group Manager Mental Health Improvement
Suzy Stevens – Partnership Works
See the embedded minutes for the January/May 2016 meetings for more information in regard to
these visits.
Currently we have the following people waiting to attend our meeting:
Dr John Crawshaw - Director of Mental Health - Ministry of Health
Caro Swanson - Te Pou
Kevin Allan Mental Health Commissioner
Emma Tonks -Ministry of Health
Ngā Hau e Whā is now receiving regular requests by organisations and individuals to attend
meetings. This is due to
Ngā Hau e Whā becoming more widely known and the quality of work
improving.
3
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Membership Updates
January 2016 – June 2016
The Central Region has had one vacancy for about 3 years and this was recently filled by Jak
Wild who has extensive networks throughout the north of the Central Region.
under the Official Information Act 1982
The Waikato region has one vacancy which we are hoping will be filled by the Midland
Regional Network.
All other positions are currently filled.
Ngā Hau e Whā has had stable representation now in the majority of positions for the past two
years. Some members of Ngā Hau e Whā are in paid employment and their work is often done
with the support and at the discretion of their employers. It is to their credit those members are
still able to do the work and produce the reports that they do. Some members are not in paid
employment and there has arisen for these members some difficulties with accessing the means
and the resources needed to complete the tasks associated with being a member of the group.
1.7
Ngā Hau e Whā Strategic Plan 2016-2020
Victoria Roberts
In October Ngā Hau e Whā undertook a complete revamp of our Strategic Plan. This was the first
rewrite of the Plan since the first one was completed in 2013. During that time the Ngā Hau e Whā
Strategic Plan document had been updated with appropriate language as per the strategic plan
goals. A Strategic Planning meeting was planned for November 2015. This was to update the
Strategic Plan as per the schedule. Because of uncertainty regarding the funding for Ngā Hau e
Whā this was delayed and the Strategic Plan has been rolled over to late 2016.
In October 2016 Ngā Hau e Whā contracted with Suzy Stevens of Partnership Works Ltd to revise
the plan to include the variations which we have added to our portfolio. We are continuing to
work with Suzy to the goal of having our new Strategic Plan by early January.
4
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
4.
Compliance
People
No. Objective
Indicator
1.
Increase and
NHEW is working collaboratively with individuals who are receiving
strengthen local,
services and other groups local y, regional y and national y
regional and
Ngā Hau e Whā continues to work collaboratively with many
national
individuals, groups and organisations.
relationships
The National DHB Family and Whānau Advisors Mental Health and
under the Official Information Act 1982
Addictions are continuing to liaise through network meetings and
email. The two groups will be working together to ensure a family
and whānau perspective is included in
Ngā Hau e Whā work. They
have contributed their up to date statements to this report
Ngā Hau e Whā continues to share with the networks any useful
information in regard to issues that affect people with lived
experience and the group is pleased to be of assistance to our
peers and colleagues. Our distribution list continues to function
well.
Requests continue to come in from organisations who would like
to have time at
Ngā Hau e Whā meetings.
The email network continues to grow and
Ngā Hau e Whā is
always looking to increase the contacts which include individuals
using services, as well as advisory groups, peer groups, and
service providers with a specific focus on peer led services. People
have been approaching Ngā Hau e Whā to be included in this
network.
2.
Be a recognised
There is an increase in the level and quality of feedback on issues for
and respected
people receiving mental health services.
conduit for the
Current members have large networks that contribute to the
people’s voice
information that is reported to the Ministry. The quantity and
quality of feedback continues to improve.
Individuals and groups with lived experience approach
Ngā Hau e
Whā with items that they would like the Ministry to know about.
Ngā Hau e Whā continually works on increasing its profile.
Commissioning Framework for MH & Addictions.
Ngā Hau e Whā
represented on the steering group by the Chair
NZ Health Strategy was commented on by individuals from
Ngā Hau
e Whā
Mental Health and Addiction Workforce Action Plan was to be
reviewed and feedback was provided by 20 January 2016. The chair
has been working with the Sector Leaders Group on the Plan.
Ngā Hau e Whā was part of the Fit For the Future and submitted
ideas for evidence based interventions
Ngā Hau e Whā collated the ideas of service users at 2 forums for
the Disability Strategy rewrite.
National Organisations request attendance at
Ngā Hau e Whā
5
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
No. Objective
Indicator
meetings, to use the
Ngā Hau e Whā network and to provide
consultancy.
Three members of
Ngā Hau e Whā were part of the
Draft Suicide
Mortality Review (SuMRC) Feasibility Study Report which has been
reported back this year by the Health Quality Safety Commission.
3.
Champion the use Newly written documents contain appropriate language.
of appropriate
Ngā Hau e Whā endeavours to use appropriate language in all
under the Official Information Act 1982
language in all
minutes, letters, reports and other documents it produces. The
major documents.
wording in the
Ngā Hau e Whā Strategic Plan and Terms of
Reference has been revised so labelling language isn’t used and all
language is appropriate.
The contract document between MOH, MHAPS and
Ngā Hau e Whā
is still to be reviewed to ensure appropriate language.
Ngā Hau e Whā continues to advocate for appropriate use of
language in any feedback on documentation that it provides.
4.
Initiate projects
There is an increase in leadership and initiatives.
and promote
Ngā Hau e Whā led the recruitment for the New Zealand Police
leadership forums.
National Mental Health Project. We continue to follow and receive
reports
Ngā Hau e Whā was well involved in The Fit for the Future run by
the Ministry.
Ngā Hau e Whā has also been working within the Mental Health
and Addiction Workforce Planning producing written feedback and
workshop attendance.
Ngā Hau e Whā attended forums and gave significant feedback to
the Draft Disability Strategy
Ngā Hau e Whā has plans to become an Incorporated Society with
the aim of achieving Disabled Persons Organisation status with the
United Nations Convention on the Rights of People with Disabilities
(UNCRPD).
Performance
No. Objective
Indicator
1.
Fulfill contractual The Ministry of Health demonstrates that it values Ngā Hau e Whā,
obligations to the and funding is increased.
Ministry of Health
Ngā Hau e Whā continues to build its capabilities to ensure that the
and be in a strong
Ministry of Health has access to a strong lived experience
position to
perspective, whether that comes from within the group or is
negotiate for the
sourced from the network.
future.
The Ministry of Health has requested consumer input from
Ngā
Hau e Whā members during this reporting period.
6
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
No. Objective
Indicator
2.
Connect with the
Ngā Hau e Whā has increased the mechanisms for providing and
grass-roots and
receiving information.
collate issues and Due to
Ngā Hau e Whā, now nearly having almost full membership
common themes.
an increase in information is expected.
Regular forums are being held to gauge the priorities and the mood
of the consumer movement
Most meetings and forums are attended by an
Ngā Hau e Whā,
member in each region.
under the Official Information Act 1982
3.
Be a useful and
Reports and submissions are timely and well-received.
valued
Informed and comprehensive reports by members in regard to
commentator on
their region are received quarterly.
mental health and Ministry of Health reports are delivered on time.
addiction service
Ngā Hau e Whā provides feedback to a number of organisations.
issues.
4.
Have strong and
Ngā Hau e Whā is well-known in each of the four regions and
effective
representatives are well-supported.
representation in
One vacancy remains at present.in Midland
NHEW from the
Midland Region is supported by He Tipuana Nga Kakano (Midland
four regions.
Region Consumer Network).
Northern Region is supported by Changing Minds.
Southern is supported by Incite and Awareness.
Central is supported by Kites Trust and the Oasis Network
Positive feedback from members of the network has been received.
5.
Improve
Ngā Hau e Whā produces a regular bulletin, has a website and
communication
Facebook page.
processes.
A new website has gone live.
www.nhew.org.nz – see later in this
report
The new website has been further developed to improve our online
presence.
It includes various ways for people to make comment and to
connect with their local representatives and networks. People are
already contacting us via the new website.
The email network is continually expanding and the website will
help drive this expansion further.
A Facebook page will continue to be worked on though at present
the capacity and capability for this is limited.
Business cards have been developed and are being used by
members
7
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Strategies
No. Objective
Indicator
1.
Become familiar
Ngā Hau e Whā has undertaken some market research and applied
with service user
the findings.
demographics in
Still to complete
our regions and
identify where we under the Official Information Act 1982
need
to in-crease
our visibility.
2.
Maintain the
Business processes are working wel . A financial report is provided
budget and
regularly.
administrative
Mental Health Advocacy and peer Support (MHAPS) forward an
support to ensure
updated expenditure report for each
Ngā Hau e Whā meeting.
our business
All administrative tasks including organisation of travel,
processes are
accommodation, venue, refreshments, are provided.
efficient.
Ngā Hau e Whā would like to acknowledge Shelley Englebretson for
her admin support.
3.
Review our
Strategic objectives are addressed and plans in place for the next
strategic plan and strategic plan (2016 - 2020)
objectives
The Strategic Plan for 2016-2020 was revised in November 2016.
regularly.
The final draft of the Plan should be ready for distribution by mid-
January 2017.
Terms of Reference
The
Ngā Hau e Whā Terms of Reference is in the process of being updated to coincide with our
new Strategic Plan and will be available for distribution early in the new year.
Service Specification Deliverables
1.7
Overview of National Issues or Challenges in the Mental Health and Addiction Sector
National issues: Discussions with Ngā Hau e Whā members and their networks have identified
that aside from the perennial issues such as housing, employment and mental health service
providers as serious concerns for service users there is also a vast array of single issue areas which
service users’ battle with on a daily basis. So we have chosen to focus on these in this report.
8
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
1.
Mental Health Services:
Grant Cooper – Otago
Attitudes: There is still so much variation in staff attitudes and values within mental health from
face to face workers to managers, planners and funders. Mental Health services would generally
agree that the service user is at the centre of all the work they do yet actions speak louder than
words. For example the peer workforce is still only 2% of the mental health workforce (source:
under the Official Information Act 1982
Adult Mental Health and Addiction Workforce 2014 Survey of Vote Health funded services). If the
service user was truly at the centre of all the work, would not their experiences be more valued
not only as paid peer workers but more paid advisors for example in co-design of services.
Note writing: Another example is the lack of collaborative note writing. Mary O’Hagan the former
Mental Health Commissioner in an interview with Radio New Zealand in June 2016 commented
about acute inpatient units that have “ Staff who spend more time in the office than talking to the
patient.” She also talked about “solutions that are driven by reason and compassion rather than
by fear and risk management.”
Language and values: The values and attitudes expressed in mental health strategic plans, policy
documents and mental health training seem to be watered down at the coal face running of
services. Some of these issues are around funding however feedback from service users is still
strong as to the variability of attitude of staff towards service users with some positive practices
and those contrary to recovery.
Emergencies: Issues still arise with the wait time at Emergency Psychiatric Services. Staffing levels
seem to be a significant issue.
A number of people would like to have more crisis options available to them. One idea that has
had success in London is a crisis café which people could go along to instead of going to the
Emergency Department of the hospital for a coffee and a chat during the night. Over a 6 month
period admissions to A&E went down 33%. See the story at:
https://www.theguardian.com/society/2015/dec/01/mental-health-problems-late-night-cafe-not-
a-and-e
A number of people who access mental health services would like a similar service here in Dunedin
for after-hours support.
Access to talking therapies is an ongoing issue with waiting times of concern.
Medications: A number of people are concerned about the level of medication and the length of
time they are on it. Feedback includes feeling “numbed” and not been able to feel the emotions
he once did as well as memory issues for example not being able to remember the chords on his
guitar.
9
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Complaints: Issue for some people of the cost of challenging the mental health system for
example getting a lawyer as well as the length of time complaints can be worked through.
Feedback from peers is that the Raise Hope Mental Health Strategic Plan rollout has been dragging
on for a long time.
CTO’s: There is still a concern over the high number of people under the Mental Health Act. This
concern is expressed nationally as well. Of particular concern is the numbers of Maori on CTO’s
especially in the north of the country.
under the Official Information Act 1982
Sharon Gutsel – Consumer Advisor – PACT Southland
Peer support:
Lack of peer support and peer advocacy services in Invercargill and Southland.
No training opportunities in Peer Support.
Carron Cossens – Waitaki:
Supporting people bereaved by suicide: Issue exists around finding support for people
traumatised by attempts to rescue another person: doesn’t really fall under ACC descriptors as far
as I can identify. This is particularly important when the rescue is unsuccessful- flashbacks,
recriminations etc. Risk of PTSD if not dealt with in early stages
An ongoing concern is support for children impacted by a suicide death. Child services in Dunedin
will only respond if a mental health issue is apparent and my argument is that careful
management post incident following the death will prevent mental health issues from developing
later in life.
Health education: Issue that more and more health pamphlets are now no longer in print- people
are referred to websites for material. Government initiative that I think is short-sighted
Staffing: A developing concern for us is service provision for Palmerston South. Currently Brief
Intervention service is only provided out of Dunedin. We don’t think this is adequate, and have
asked for the service to be resumed based in Palmerston.
Julie Whitla - Christchurch
Counselling: A person with complex issues has been told that they cannot access the free Brief
Intervention Counselling more than once a year by their GP.
There has been a noticeable increase of people accessing the drop in at MHAPS which is open at
the weekend due to housing difficulties.
Outcomes identified by people with mental health and addiction needs are:
• Homelessness with debts for storage to HNZ for new WINZ issued washing machines and
fridges.
• Families living in cramped conditions with inadequate number of bedrooms in huge
complexes with limited outdoor space for their children.
10
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
• Complexes are busy and for some people the stress of the noise, people coming and going
has not been suitable for people with mental health issues.
• “
I cal ed the police because after weeks of abuse, intimidation such as him putting security
cameras pointed on my property I”
•
“ The police said I can’t get a protection order as I live at a HNZ home and I feel my housing
manager is out of her depth with facilitating a solution”
• Physical health needs were not considered in my application “
Although I have a flat from
CCC, My flat is damp and I have to wipe condensation off the windows every day, I am
under the Official Information Act 1982
awaiting a lung transplant and have been hospitalised five times in the last two years and
still there is no word from the city council”
•
My HNZ flat is nice but I have low vision eyesight problems and the stairs are not safe. My
housing manager said they have done everything they can to make them safe but wil not
fill in the stairs or transfer me to a suitable unit.
The WINZ Linwood office in Christchurch no longer has paper applications for benefits and you
have to ask the manger for an application. The expectation is to complete applications on line. It
causes delays in people receiving benefit entitlement in a timely manner. People who have
identified with mental health issues who were placed in HNZ or city council housing during the
earthquakes have been seeking housing transfers or have been evicted due to not fit for purpose
housing.
(Please see the article – Internet as Disability/Health Issue)
Housing:
• At the moment there is no single person accommodation available in Christchurch.
• There are a number of people in the acute wards who could leave if there was a place to
go.
• Purapura Whetu is now partnering with Comcare for family housing.
• People who have identified with mental health issues who were placed in HNZ or city
council housing during the earthquakes have been seeking housing transfers or have been
evicted due to not fit for purpose housing.
Awareness Consumer Group - Canterbury
Formatted: Font color: Auto
• People have raised concern at Awareness about Lifeline losing their funding as it is an
established name in the community where as many consumers do not know anything
about the new tele health providers.
• Suicide rate in Canterbury is still high and there has been little change in the numbers. It is
of concern to the network as so many initiatives and focus of the whole region has been on
mental health since the earthquake including substantial Health Promotion campaigns on
well-being.
• One person fed back that they were not given any choice about where to meet at Specialist
Mental Health Services except in an old de-commissioned seclusion room and were made
to feel blamed when they didn’t want to meet there.
11
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
2.
Whanau/ Family
Corinda Taylor Otago
“As a family we were excluded from the care of our loved one right from the start when our
family member was placed under the mental health act. In 1999 Parliament made an amendment
to the Mental Health Act that required clinicians to consult family/whānau at particular junctures
of a person’s compulsory assessment and treatment under the Mental Health Act. However this
under the Official Information Act 1982
requirement is rarely observed and families are regularly excluded from the care process. We
know our loved ones best and can provide valuable information that can aid the clinical evaluation
processes.
The privacy act also prevents clinicians from sharing valuable lifesaving information such as the
person being suicidal. If families are expected to care for their loved ones in the community then
they need to be well informed and well supported by the system since we are not trained mental
health workers.
Lack of collaboration with family, lack of transparency and collaborative note writing with the
person under their care can seriously hinder the care of the person.
Families struggle when their loved ones become mentally unwell and when they visit their loved
one in the hospital setting it becomes a frightening experience. Mental health clinicians do not
communicate well with the families who are in shock when it is their first experience with mental
health and services. There is no support for families and there is no information on where to seek
help.
The first time we became aware of Otago Mental Health Support Trust was well after our son’s
suicide. This service could have provided us with much needed support and this could have saved
our son’s life. If the Southern DHB mental health services do not want to support the families then
they need to at least provide information as to where families can seek support.
We wish to see an independent family support person AND an independent consumer support
person available on the mental health wards specifically dealing with this issue. This person MUST
be independent from the Southern DHB.
Navigating the mental health system is complicated which most people find hard. An attitudinal
change can go a long way.
Services need to understand that not all families are bad and that we are not the enemy. Work
with us to help the person to avert tragedies and let it become a life full of hope.”
I am not aware of any new initiatives or developments in our region since all family involvements
and feedback are discouraged by Southern DHB services. The last time I was invited to participate
12
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
in a survey from the Early Intervention for Psychosis services in 2012 I was told that the survey
results were ignored as they had a poor return of only 20% of participants. 20% of people
bothered to respond and their feedback which included my own was valuable information that
was discarded. Perhaps the truth in those surveys can bring about much needed change.
DHB Family and Whanau Advisors:
Co-Chair Leigh Murray under the Official Information Act 1982
DHB Family Whānau Advisors continue to provide guidance on working with families and whānau
to mental health and addiction workforce via Handover nursing newsletter & Te Pou website.
Latest article is ‘Moving from Individuation of risk to a shared safety agenda’ written by DFWA co-
chair Leigh Murray.
http://www.tepou.co.nz/news/moving-from-individualisation-of-risk-to-a-
shared-safety-agenda/810
• Family Whānau Advisors are looking forward to their annual national meeting Nov 3-4 in
Christchurch. This is a great opportunity to feed into & be updated about key projects as
well as share best practice ideas ‘kanohi te kanohi’. There is a full agenda with all 4
workforce centres, MH Foundation, MoH & HDC Mental Health Commissioner taking up
slots. Unfortunately some of our key family advisors won’t be there due to travel
restrictions currently in place for some DHBs. We are hoping to link them in via video
conference.
• DFWA recognises there is probably not a widespread understanding/appreciation of the
systemic advocacy family whanau advisor role across NZ. This may be a contributing factor
to family advisor vacancies that are of several years duration in a few DHBs. We appreciate
that this might also be the case for some consumer advisor positions. Currently there are
22 family advisors in post which equates to 17.87 FTEs nationally.
• We also note that the importance of family, whānau perspective and participation is
increasingly mentioned in MH & addictions though this does not always seem to translate
into tangible ways of ensuring that the whanau voice is present or included.
• To end on a positive note DHB Family Whānau Advisors contributed significantly to the
successful TheMHS pre-conference family & whānau forum held in Auckland on August
23rd with 65 attendees. At the start of the day we demonstrated our commitment to the
theme of ‘Building Authentic Relationships’ with our own whānau by presenting the
consumer forum delegates with the gift of a peace lily, a fun fruit face & chocolate with
good wishes for an inspirational, fun and learning day.
3. Internet Access as a Disability / Health Issue
Victoria Roberts - Chair
This issue has previously been raised in earlier reports but with the current rewrite of the
Disability Strategy it is useful to revisit the matter. There is a need for robust discussion and sound
policy formulation around internet access as a health issue.
13
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
link to page 99 link to page 99
Released
There is also a need for the current working group whose brief is to align the Mental Health Act
with the UNCRPD to take note of this. Other Government departments need to be engaged to
ensure that this is progressed (e.g. MSD; ODI)
Internet access is widely available in New Zealand. In 2013 according to Statistics NZ 4 out of 5
homes in NZ have access to the internet
i and two thirds of rural households had a broadband
connection.
ii This survey showed that for two thirds of those households not connected to the
under the Official Information Act 1982
Internet, concern over cost was the reason for them not being connected.
Some of the poorest people in New Zealand are long term beneficiaries and especially those who
are unable to supplement their benefits by working such as those on Supported Living Payments
(formerly Invalids Benefits) and Job seeker support – with medical deferment (formerly Sickness
Benefit). Many of these are people with lived experience of mental illness and/or addiction. The
Ministry of Social Development who administer Work and Income (WINZ) do not keep statistics on
the numbers of people receiving these benefits who have diagnosed mental illnesses.
Currently, there hundreds of people receiving Disability Allowances in Aotearoa NZ. Beneficiary
advocates know that of these a very small number will have persuaded WINZ to pay them an
allowance to cover the cost of Internet even if a large number will have a telephone covered as an
‘essential’ need.
Day-to-day living: The internet has many practical applications and it is widely used for
entertainment purposes; reading; games; accessing music, videos and movies. As well connecting
with friends’ online, chatting, skyping, social networking are all new ways of social interactions
that have become the norm and that now hold across all age groups and most socio economic
demographics.
For many people with lived experience not having the ability and the right to use this modern day
facility because of having inadequate income is unfair and debilitating. When public spaces are too
overwhelming and scary due to noise lights and stimulation and online peer support is your only
option, then that is when public policy should champion the right to an adequate income to
enable that to happen. Some situations are such that people are confined to their homes and the
internet becomes their link to the outside world.
14
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
E-therapy: Modern medics too are using the internet to provide mental health supports like
recent e-therapy tools such as the Sparx e-therapy for young people which was launched 28th April
2014 – a CBT technique in a youth friendly game to teach young people how cope with negative
thoughts and to think more positively. There are other mental health tools available on the
Internet – John Kirwan’s Depression.org.nz; Through Blue; and any number of positive thinking
websites. Even the ability to distract is invaluable for someone who is alone and vulnerable. But as
under the Official Information Act 1982
detailed above without sufficient resources these sites and such diversions are not be available to
all those who could benefit from them.
Employment: The internet has become the first port of call for most job seekers. Job listings, job
alerts, employer alerts, are all posted on the internet. So for many people with lived experiences
of mental distress, who are seeking employment, many of whom are either unemployed or
underemployed, access to the internet is of vital importance. Also there is an increase in the
availability of “from home” and online job vacancies. Working from home via the internet may be
the only option for some job seekers. Work can be shown to be therapeutic in and of itself.
It has already been demonstrated by others that to be in the workforce or to be looking for work
is also to be experiencing discrimination if one has lived experience. Therefore to have an added
hurdle of not having instant and easy access to the internet decreases the odds of the much
sought employability.
Disability costs: The Internet is also a vital connection to anyone with restricted mobility including
those who experience mental distress that makes it difficult to leave their home. However it is not
included by the
Ministry of Social Development when assessing Disability Allowance costs. It is so
rarely, as to be almost never included as an allowable cost of disability even though as shown
quite clearly above it can quite reasonably be demonstrated to be so. The Ministry of Health may
be able to offer guidance in this regard.
International obligations: The UNCRPD underscores the need for disabled persons to be able to
communicate freely, and access things they need and having internet in the home undoubtedly
facilitates this. The
Ministry of Social Development appears to be deliberately obstructing
applications for the inclusion of internet as part of disability costs. WINZ facetiously make the
claim that “most households have internet access and therefore it is not a cost that is due to a
15
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
persons’ disability. However it is not true that most of the households which have people with
disabilities that require internet access actually have it.
Article 9 Accessibility
1. To enable persons with disabilities to live independently and participate fully in all aspects of
life,
States Parties shal take appropriate measures to ensure to persons with disabilities access,
on an equal basis with others, to the physical environment, to transportation,
to information and
under the Official Information Act 1982
communications, including information and communications technologies and systems, and to
other facilities and services open or provided to the public, both in urban and in rural areas.
These measures, which shall include the identification and elimination of obstacles and barriers
to accessibility, shall apply to, inter alia:
(b) Information, communications and other services, including electronic services and
emergency services.
2. States Parties shall also take appropriate measures:
(g)
To promote access for persons with disabilities to new information and communications
technologies and systems, including the Internet;
We at Ngā Hau e Whā
respectfully suggest that the Ministry of Health might assist the Ministry of
Social Development to understand its obligations and responsibilities to people living with
distress
and addictions or the after effects of these to enable them to counter stigma and discrimination
that many of us experience at the hands of other people and regrettably at the hands of other
government departments as well. Enshrining obligations into the newly rewritten Disability
Strategy will be a good way of signalling to everyone a decent way to go.
1. Household Use of Information and Communication Technology: April 2012
16
Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
1.8
Overview of areas of best practice in the Mental Health and Addictions sector
Corinda Taylor Otago
I would have liked to put something in this section since I am a very positive person and like to find
positives in services but unfortunately cannot find one positive at this stage. I do hope that
feedback will in time be able to improve this.
Projected best practice in future would be:
under the Official Information Act 1982
• Inform family of what is happening every step of the way so that we can best support our
loved ones
• Inform family if loved one is suicidal and the risk factors
• Consult with family to get a full clinical history
• Collaborative note writing
• Keep the service transparent to keep people honest
• Phone calls to be well recorded with parental or family concerns
• Record keeping to be electronic as current handwritten notes can be tampered with after a
serious adverse event since there would be no evidence of it
• Inform family/whanau of
all the other agencies in their district so that they can make their
own decisions as to where to seek additional support
• Provide real time feedback from people and their families/whanau so that services can
know immediately where their failures are it and can be addressed/rectified immediately
Kia Noho Rangatira Ai Tatou:
Jak Wild Central Region North
• Kia Noho Rangatira Ai Tātou is a unique education programme that puts the human rights
of disabled people and the UNCRPD into a New Zealand cultural context. This two day
workshop has an applied focus which will help ensure that disabled people’s human rights
are upheld. The Disabled Persons Assembly and Te Pou o te Whakaaro Nui have worked
together to develop this programme which examines human rights and the United Nations
Convention on the Rights of Persons with Disabilities (Disability convention). Workshops
are being held throughout New Zealand with attendees of the most recent workshop in
Napier, Hawkes Bay giving positive evaluation feedback
From Julie Whitla - Christchurch:
•
Acute Wards
Occupancy (midnight census) of the adult acute inpatient service has remained at 93% for
a second consecutive month. There were 17 sleepovers required in July 2016.
Canterbury are exceeding Ministry of Health targets with respect to wait times for adult
services. The targets are 80% of people seen within 21 days and 95% within 56 days.
97.4% of people referred to the Adult Community Service were seen within 21 days, and
100% seen within 56 days for July 2016. The percentages are 92.9% and 98.8%
17
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
respectively when other adult services i.e. Specialty, Rehabilitation and Forensic are
included.
Seclusion
• The CDHB focus on reduction of seclusion in Te Awakura (acute inpatient service)
continues. Two consumers experienced seclusion during July 2016 for a total of 6.75
hours. There is strong and effective nursing leadership and staff dedication and
commitment to maintain the focus of reduction.
• There was discussion around the steeply dropping seclusion rate – this has decreased from
under the Official Information Act 1982
800 hours in April 2012 to 1 hour in the last month commendations to the CDHB for doing
this. Awareness (Canterbury Consumer action Group on Mental Health and Addiction) are
to be thanked for helping instigate this focus on seclusion reduction and elimination.
Debbie Selwood mentioned the DHB is talking much more about seclusion elimination
now, rather than just reduction. There is much more of a focus on upskilling staff to be
able to provide talking therapies, not just assessment. Mental health staff are also being
supported to upskill around supporting people with alcohol or drug problems as well as
mental illness.
• In June there was only
one hour of seclusion recorded in the acute wards. Though rates
are going up in other parts of the country, likely as a back lash from some bad media and
incidents, the efforts of staff in Canterbury have been excellent. There is anxiety among
staff over changes in policy and the increase in assaults on staff. Some feel they are at risk
but are still de-escalating patients.
From Sharon Gutsell – Consumer Advisor PACT Southland
• Working on a new referral protocol for people to receive community support services
without the need for a needs assessment, removing this barrier to people receiving
support services.
Lisa Perniskie, Peer Support, Mirror HQ, Ōtepoti
• Within my team I have been working on how to collaborate and spent time recently on
developing a process for our internal referrals to my role.
• With our taiohi it works well to have a mihi whakatau process with myself, taiohi and the
clinician to clarify for them what support I can offer and what the clinician will be working
with. The taiohi is given the opportunity to discuss what they would like support with.
• It is very isolating for me being in Dunedin as there are very few peer support workers
here. I have had a lot of support from OHMST and would like to thank Grant for his
ongoing support of my role.
• I would like to participate more in best practise within the southern area and find out
more about what is happening in our area- Te Wai Pounamu.
•
18
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Changes or developments that have come out of Rising to the Chal enge
Rising to the Challenge
Kieran Moorhead - Auckland
Rising to the Challenge
Health outcome: Reduce morbidity and mortality for people with mental il ness
under the Official Information Act 1982
What are we aiming for in2016/17? (Our measures)
Key measures
• At least 95% of child and youth clients discharged from community mental health and
addiction services will have a transition (discharge) plan
• 80% of 0-19 year olds referred for non-urgent mental health or addiction services are seen
within three weeks and 95% within 8 weeks.
Other measures
• Access targets for mental health and addiction services: 3.1% (4.4% for Māori) for 0- to 19-
year-olds, 3.4% (7.6% for Māori) for 20-to 64-year-olds, and 2.1% for those aged 65+ years
• 95% of older adult service users meeting the criteria will have a current relapse prevention
plan.
How will we achieve this?
• Providers will be reliably and consistently collecting social outcome indicators by June 2017.
Actively using our current resources more effectively
• Continue roll-out of a new model of community acute response in Rodney and West
Auckland, following the successful North Shore pilot, by June 2017
• Participate in regional plan activity – High and Complex needs, Eating Disorders, Substance
Addiction (Compulsory Assessment and Treatment) Bill, Māori workforce development plan,
framework for suicide prevention training, review of child and youth services, offender
health, and forensics (youth and adult) - ongoing
• Mental Health and Addictions NGO sustainability - with the Mental Health and Addictions
sector, implement the agreed work plan and complete 2016/17 objectives by June 2017
• Utilising a co-design process, develop a Shifting Services plan across DHB Provider Arm and
NGO services to deliver the right care, in the right place, at the right time, by the right people.
Plan to be completed by June 2017
• Continue to work collaboratively with Police to identify and implement initiatives that will
improve the experience of people with mental distress who come to Police attention.
Ongoing.
• Actively participate in the development of the Commissioning Framework and develop an
implementation plan once the final Framework is published by June 2017.
• Maintain regular meetings and communication with key stakeholders from the Ranui Social
Sector Trial to develop, agree and implement a transition plan. June 2017
Integration between primary and specialist services
• Plan and implement integration of General Practice and NGO support services based on the
19
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Rising to the Challenge
model(s) developed within the Tamaki Mental Health and Well-being Initiative, prioritising
Whānau House and Totara Health, by June 2017
• Further develop primary mental health integration with Totara Health based on the
evaluation (evaluation due March 2016) by June 2017
• Improve the interface between the Community Alcohol and Drug Service and primary care –
ongoing
• Design access for primary care clinicians to advice, information and screening from provider
under the Official Information Act 1982
arm clinicians by June 2017
Resilience and recovery
• Develop an Equally Well action plan for the Waitemata and Auckland DHBs to improve the
physical health of service users. The initial stages of this plan will include the ability to record
physical health status and development of baseline data, to be completed by June 2017
• Evaluate clinical processes around assessment and treatment of Māori under community
treatment orders by June 2017
• Monitor and analyse section 29 Mental Health Act treatment orders for Māori. Ongoing
• Run focus groups with non-Māori clinical staff to better understand perceived differences in
assessment and treatment of Māori under CTOs (Section 29), identify gaps in current service
delivery to Māori and recommend steps for improvement by June 2017
• Ensure reliable collection of seclusion and restraint use data for Māori, and analyse the data
to understand differential rates of use for Māori by June 2017
• Māori and Pacific service users have the highest physical health comorbidities. Ensure
routine metabolic screening for secondary service users, with priority focus on Māori and
Pacific clients by June 2017
• Deliver 2016/17 actions of the Auckland and Waitemata DHBs’ Suicide Prevention and
Postvention Action Plan (2015-2017). The plan and the actions will be guided by the Advisory
Working Group and Inter-Agency Advisory Group, and will prioritise at-risk populations (e.g.
youth/rural/Māori). Activities in 2016/17 will include developing community resources,
wellbeing and resiliency; training community members and health providers to identify and
support at risk individuals; and develop pathways between primary and secondary care
providers – to be completed by June 2017
• Implement the priority actions identified from Everyone’s Business: a mental health and
employment strategy for the Auckland and Waitemata DHB regions by June 2017
• Support Parents Healthy Children (COPMIA) – all services to develop action plans, and
establish routine data collection and service champions by June 2017.
Delivering increased access
• Implement the 2016/17 actions of the Waitemata Stakeholder Network Service development
Plan (2015-2020). Actions to be completed by June 2017 include increasing access to Child
and Youth services in Rodney, delivering the first Incredible Years course in Chinese and
Korean languages, and utilising service user feedback in Older Adult service planning and
evaluation
• Continue development of shared care between secondary and primary services for aging
population between Services for Older Adults and primary care. Ongoing.
• Increase access to alcohol and drug services through improved relationships with education,
justice, health and child protection services by June 2017
20
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Impact of Ngā Hau e Whā
Formatted: Font color: Red
Formatted: Font: Bold, Underline, Font color: Red
Victoria Roberts – Central Region NorthChair
Formatted: Font color: Red
The Information Provided by Ngā Hau e Whā to the Ministry of Health
Ngā Hau e Whā work supports the Ministry of Health (MOH) to respond to the issues people
receiving mental health and addiction services face in a timely manner. This information is
directly from people using services and includes NGO’s and their clients and so cannot be
under the Official Information Act 1982
sourced from the reporting District Health Boards. Because it is sourced from people with lived
experience it is invaluable.
MOH is able to use the information provided by
Ngā Hau e Whā to inform policy, procedure
and new developments.
Ngā Hau e Whā gives the ministry an insight into what matters to the
people who are affected by the decisions made at ministry level.
Ngā Hau e Whā reports are distributed throughout the ministry and sent to the Director of
Mental Health’s office.
The integrity of
Ngā Hau e Whā’s work means that the group is a ready resource for gaining
the viewpoint of people with lived experience for example: the external reference group for
‘Rising to the Challenge’ and for ministry interview panels. Also quarterly reports keep the
ministry in touch with what is happening in service user’s daily lives.
The MOH sees worth in the work that
Ngā Hau e Whā is doing. Especially the networking of
groups such as
Ngā Hau e Whā with SF, Platform and other service user interest groups.
Many opinions and standpoints, give the Ministry a more rounded picture of what is
happening for people with lived experience in the sector.
E-Network
The
Ngā Hau e Whā E-network continues to grow. Requests are now coming in for
Ngā Hau e Whā to send out information through the network on behalf of others. Members are utilising their
business cards as a means of growing the network.
Ngā Hau e Whā has no way of knowing how far
and wide the E-network reaches. Work will continue on increasing the network and sharing
information.
Website
Ngā Hau e Whā Website June 2016 <www.nhew.org.nz>
The new Ngā Hau e Whā website is completed and has gone ‘live’, replacing the old website
hosted by Midland Health. Ngā Hau e Whā sees this as a bold step that indicates the importance
that independence and autonomy brings to our work.
We see the website as key to helping to build, educate and connect the sector networks, both
locally and nationally.
21
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
The website is based on the previous design, but has much greater capability for modifications and
further development, with Ngā Hau e Whā 3 representatives forming a sub-group as
administrators and developers of the site, including the person who was contracted to re-host, re-
design and build the new site.
The website is designed in a way that it’s content, functioning, and design is ‘open’, flexible and
simple for administrators to manage, allowing the site to remain in the hands of the Ngā Hau e
Whā representatives into the future, rather than having limited funds go to professional
under the Official Information Act 1982
developers and a third-party host. Previously the website was overseen by third-party developer,
Black Sheep who were contracted by Midland Health.
Further work is being undertaken so that the website will manage the entire Ngā Hau e Whā
networking capability, such as the distribution list, feedback and comment, and promotion of our
stakeholders and network communications, and most importantly a blog and links to Facebook
and Twitter.
It is expected this new arrangement for our website and online and social media presence will
bring about a considerable cost benefit to Ngā Hau e Whā. This saving will be presented in the
next report, once we are better informed as to the previous specific costs associated with Midland
Health hosting the website.
It is expected this new arrangement for our website and online and social media presence will
bring about a considerable cost benefit to Ngā Hau e Whā. This saving will be presented in the
next report, once we are better informed as to the previous specific costs associated with Midland
Health hosting the website.
Jak Wild Website Design.
Bulletin
Ngā Hau e Whā has intentions to produce a regular bulletin of highlight items from the minutes
and regional reports which are of specific use to those in our networks. The intention was to send
out to e-networks and place on the website. Unfortunately our human resource does not have the
capacity to do this work currently. Minutes from
Ngā Hau e Whā meetings will continue to be
posted on the webpage and sent out via the network.
22
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health

Released
Regional Reports
under the Official Information Act 1982
Member: Tui Taurua-Peihopa
Region: Northland
Meeting: 7/8 September 2016 3/4 November 2016
1. Issues/chal enges identified by people in your region
Hui to discuss the Mental Health and Addiction Framework
• 40 attendees including the Northland Ngā Hau e Whā representative.
• Lots of discussion around choice, partnership, and communications
Prescribing of medication
• Issue around prescribing in the region. There is only one psychiatrist who is able to
prescribe medication and an alternative provider is not available to tangata whaiora and
this causes problems when a person s requires daily prescribing.
• If a person does not want to use a particular pharmacy or they can’t, then it is about an
hour to Kaikohe.
Not all tangata whaiora have GP’s and are reliant on the psychiatrist to prescribe. Without a nurse
or other clinician people have too little choice.
Security at WINZ
• Up to 4 security guards are being stationed at each of the WINZ offices which claimants
report they find intimidating with a feeling of being judged and watched. A report from
one Maori security guard is that he “felt he was being used against his own people
Maori Consumer advisor
• Reports from clinicians that there is a need for a Maori consumer advisor in the region.
Issues also raised around the need to have face to face contact rather than over the phone
which raises challenges due to the remoteness of the Northland region
23
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Communications
• A report of a letter from the Kaikohe Community Mental Health team to a service user was
sent out without the name of the psychiatrist the person that the person was due to be
seen by. The person had an hour drive to attend the appointment but the psychiatrist was
sick but no one had attended to informing the service user not to attend.
• Lack of communicating appointments e.g. Appointment contacts; little or no advancement
acknowledgement appointments
under the Official Information Act 1982
• One psychiatrist for Far North; changing of psychiatrists up to every six months.
• Lack of choices when requiring a change of psychiatrist.
• Mental Health persons being bullied on the streets.
• Children and poverty; young children seeking funds through using criminal tactics as have no
food at home; parents are using money for their alcohol and drug needs.
We need to develop a Peer Support Service using Maori Models of Practice.
2. Best Practice according to people in your region
Intra-muscular prescribing
• Reports of inconsistency between clinicians around aspects of holistic health at Kaikohe
health center. A new clinician gave an excellent assessment and education around all
aspects of holistic health which had not ever happened with previous clinicians
• We need to develop a Peer Support Service using Maori Models of Practice.
3. New Initiatives /Developments in your region
Te Haurahi te Pounamu – Maori pathways
• This is the name of the newly formed national Maori network
• Northland Ngā Hau e Whā representative attending a hui in Nelson to support Iwi to
reconnect with each other.
Kia Noho Rangatira Ai Tatou:
• Kia Noho Rangatira Ai Tātou is a unique education programme that puts the human rights
of disabled people and the UNCRPD into a New Zealand cultural context. This two day
• workshop has an applied focus which will help ensure that disabled people’s human rights
are upheld.
• The Disabled Persons Assembly and Te Pou o te Whakaaro Nui have worked together to
develop this programme which examines human rights and the United Nations Convention
on the Rights of Persons with Disabilities (Disability convention).
• Workshops are being held throughout New Zealand. Workshops in the Northland region so
far have included one for Disability Support Services in Whangarei last month, with another
24
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
planned for Disabled persons later this month. Attendees have reported very favourable on
last month’s workshop.
• Human Rights Workshop October 2016 Whangarei by Te Pou Auckland:
Attended this workshop with my team of Maori. Very good workshop provided by Jak Wild; Hee
Barnett and Vicki Terrell.
An evaluation of the workshop was provided to Te Pou by my team.
We evaluated the Te Tiriti o Waitangi presentation.
under the Official Information Act 1982
We were clear that as members of Nga Puhi we were not happy with the presentation thus far.
From this evaluation, we had a phone conference with Frances Anderson, Bill Hamilton and
Kaumatua Peter Mason.
We had an in-depth discussion which would be included they coming back to us when completed
their process.
Staff Recruitment
A belief of a Tangata Whaiora Maori Workforce: re Ngā Hau e Whā and Te Rau Matatini
One psychiatrist for Kaikohe; lack of choices
Distribution List
Over next three months will develop a distribution list for Northland. I will make contact with
people who may be interested in being on this distribution list.
Rural Community
Work on proposed ‘Framework to improve Mental Health and Addictions Outcomes in Rural NZ.’
The Kaikohe rural group met in September and they have run a workshop that 500 or so people
responded to. A draft proposal has been completed and a second meeting on the 16th November
to discuss this draft.
Northland Issues pending -
1. Prisoners and Mental Health: Nga Wha Prison
2. Veterans and Post Traumatic Stress Disorder, Depression, Suicide, Physical Health due to Agent
Orange (Wai Claims)
3. Mental Health Act and the Marae
4. Suicide Prevention Action Plan
5. Seclusion Numbers
6. Respite
Relationship Building Expectations
25
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
o Te Rau Matatini
o Te Huarahi o te Pounamu (Maori National Tangata Whaiora Roopu)
o Te Pou
o Rural NZ
o Maori Networks
o Nelson Consumer Networks
under the Official Information Act 1982
o Maori Networks
o United Convention Human Rights
o NGO Governance Group, Northland
Tui Taurua-Peihopa
Mobile: s 9(2)(a)
s 9(2)(a)
26
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health

Released
under the Official Information Act 1982
Representative Name: Guy Baker
Region:
Midland
Meeting Date:
8-9 September 2016
1. Issues or Chal enges in the sector as identified by people receiving services in your region
TAIRAWHITI – Guy Baker
Consumer Advisory Group (made up of service users, meeting held second Monday of every
month)
• Still a lot of discrimination being experienced by those under the Mental Health Act.
Gisborne District Council Councillors reported in the Gisborne Herald their desire to rid
beggars, whom they termed as mental health sufferers, from the streets of Gisborne. This
was followed by a covert survey by Heart of Gisborne (Business Collective) asking retailers
if “beggars” were sitting outside their premises or if they were aware that “beggars” were
outside other premises, if they supported this and if so why? Some Councillors were of the
opinion that they should be prosecuted through the courts.
Feedback gleaned from support workers, peer support worker, whanau ora workers, and others
providing services in the Tairawhiti region:
• Suicides continue to be prevalent. Although hard statistics have yet to be confirmed by the
Coroner’s office for recent periods the numbers that services have been involved in
suggest that rates continue to climb. An 8-day period in August saw four completed
suicides alone where services attended post vention incidents.
• Housing respite services being placed under increasing pressure as there are not enough
beds to cope.
• Lack of emergency and social housing continue to be a struggle for all workers alike.
27
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
TARANAKI UPDATE- Nic Magrath
• The Taranaki Consumer Advisory Groups still struggle to encourage people to attend.
• Ombudsman Report highlighted the appalling state of the environment in Te Puna Waiora.
This has been on the risk list of Taranaki District Health Board for a number of years and
the inpatient unit awaits much needed refurbishment.
EASTERN BAY OF PLENTY – Arana Pearson
under the Official Information Act 1982
• Workloads are peaking with varied and challenging circumstances.
• Lack of supportive accommodation adding to continuing social issues that impact mental
health needs. Wait lists are long.
• Several male clients have been victims of violence and robbery.
• Transport remains a problem in the area as many do not have driver’s licenses, no vehicle
or access to public transport despite efforts to alleviate.
LAKES – Susan Freeman
• Difficulties for consumers to access emergency housing. Life wise hold the contract
however referrals are only accepted through two providers.
• Very limited free counselling available in Rotorua. Salvation Army are no longer offering
free counselling services.
• Emergency food grants are increasingly becoming difficult to obtain through MSD and are
often declined. Only recourse is through Salvation Army who are still willing to provide
food parcels.
• Taupo Consumer Group is difficult to get up and running.
2. Best Practice according people in your region.
TAIRAWHITI – Guy Baker
• Feedback Informed Treatment data is providing valuable indicators however progress is
developing in this area with the knowledge that wider use and increased data will only
enhance current services
• Consumer Engagement Strategy has been completed and wider consultation workshops
are to be held this month.
• Peer debriefs for those currently being placed in seclusion continue to support initiatives
for ending seclusion.
• Consumer Advisory Group (CAG) continues to be very active despite the wintery months.
This monthly meeting of consumers has had a number of different guest speakers including
Psychiatric Ward Manager, Health & Disability, Budget Advice and even a previous
Consumer who related benefits they have had after successfully completing a smoke
cessation programmes following 14 months of continuing to be smoke free etc.
28
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
• A submission to the Minister of Justice, Amy Adams, is currently being prepared to
advocate for marae based mental health hearings.
•
TARANAKI – Nic Magrath
• Real Time Feedback is now available through Alcohol & Drug, Adult Community
outpatients, across the three acute services and with community teams. A review of this is
under the Official Information Act 1982
yet to be conducted.
• Telemedicine (consultations via video conference) through the South Taranaki MH Service
have been found acceptable but staff are disappointed that it hasn’t yet equated to more
appointment slots as promised.
EASTERN BAY OF PLENTY – Arana Pearson
• Peer support and advocacy groups meet weekly and provide on-going programme delivery
to participants.
• Support of local dentists to access urgent dental care has been outstanding and tangata
whaiora have been able to obtain urgent appointments.
• Good collaboration with WINZ staff have been particularly helpful.
LAKES – Susan Freeman
• Focus Groups are underway for YouthNav, a new addition to WebHealth.
• Monthly Consumers Groups continue to be held.
• VIP (Consumer) Group, Rotorua, trial run a consumer led facilitation and participation
workshop.
3. New initiatives / developments in your region.
TAIRAWHITI – Guy Baker
• A collaborative Post Vention Suicide Group has been formed bringing together an array of
services (Police, Victims Support, Hauora Tairawhiti Mental Health & AOD, NGO Mental
Health & AOD providers etc.)
• Developments occurring as Hauora Tairawhiti works towards “ending seclusion”. Funding
has recently been granted to refurbish a current seclusion room into a low sensitive
environment. Training for staff is also being planned.
• Revelations of occurring themes continuing to be identified in SAC1 incidents have
prompted further investigations into the effectiveness of initiatives to address the gaps
and the recommendations and whether these have actually been fully incorporated.
• Dr. Di Rangihuna (ICAMHS Psychiatrist) and her Whanau Ora Pakeke husband Mark Kopua
continue to develop their Mahi-a-Atua programme, that delivers a holistic approach to
instill “purakau” (Maori Atua stories) to enhance a consumers well-being, by training of
mataora (practitioners) to facilitate workshops on this practice.
29
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
TARANAKI – Nic Magrath
• Suicide Prevention and Postvention Coordinator has been appointed to this new role that
is being supported by Tui Ora
• Recovery Action Plan (RAP) has now been rolled out but faces challenges in its
implementation.
EASTERN BAY OF PLENTY – Arana Pearson
under the Official Information Act 1982
• Partnership between the Peer Group and Centre 401 (consumer run service) has developed
confidence, participation and enthusiasm for continued peer run experiences and events.
• An opportunity to work with mental health clients from Opotiki in partnership with CMH
Whakatane is being welcomed.
LAKES – Susan Freeman
• Representation has been gained on Lakes DHB MH&AS Clinical Governance (via Consumer/
Whanau Representative) and on the SPHC working party at Lakes DHB.
• Linkage to commence a peer led LGBTI group
4. Addiction
TAIRAWHITI – Guy Baker
• AOD Review of Hauora Tairawhiti has commenced with an initial stocktake of services and
meetings with a myriad of stakeholders including services, managers, stakeholder
organisations, consumers and whanau. This review and final reporting will conclude in
December 2016.
TARANAKI – Nic Magrath
• An OST programme survey coinciding with an external audit was completed. A work plan
has been developed to address the recommendations given.
5. Family and Whānau
TAIRAWHITI – Guy Baker
• A Family and Whanau Consult Group has been established to ensure family and whanau
are provided with an opportunity to have input into local, regional and national mental
health and addiction service provision and that their views contribute to the ongoing
development and quality.
LAKES – Susan Freeman
• With Linkages new service development input from consumer and family is a priority.
30
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health

Released
under the Official Information Act 1982
Representative: Jak Wild
Region: Central North
Meeting date: 8/9 September 2016 3 /4 November 2016
Introduction:
This is the writers’ first report after recent selection for the Central (North) representative role.
The role had been vacant for some time with contact details not readily available for the previous
representative, resulting in their not being a handover of the role. Therefore, communications
with stakeholders and networks will take some time to build up, hence the limited information in
this report, with reporting relying mainly on information from local media and online networks
Networking
Contact and communications with the Central Region (North) stakeholders and networks has been
slowly progressing, with new persons identified to include in our local distribution list.
Face to face meetings with numerous services has resulted in communications with relevant
persons for ongoing liaison including: Whatever it Takes Team Leader, Emerge Aotearoa Consumer
Advisors and GM, Salvation Army Consumer Advisor and Lieutenant Colonel, Dalcom Health Care
GM and Consumer Advisors, Supporting Families National Coordinator and Manager, Te Hauora
Runago O Wairarapa Consumer Advisor, Wharenikau Consumer Advisor.
Although there has been only small number of reports from stakeholders for this quarters report,
the expectation is there will be increased information for the next report based on the new
contacts made over the last two months
1. Issues/chal enges identified by people in your region
1. Mental health services:
Opposition parties, trade unions and special interest groups have been highlighting many issues of
concerns nationally in Mental Health service delivery over the last 6 months. Local Media has
culminated reporting on calls for a public inquiry with special mention of waiting lists for youth in
the region. Up to June 2016 Whanganui DHB had 35.6% of young people waiting more than three
31
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
weeks to access mental health services. Hawkes Bay DHB reportedly reduced their waitlists for
youth of 3 weeks or more from 32.6% to 13.9%. The national target is 20%.
2. Crisis services
Ward 21, Mid Central DHB’s Palmerston North inpatient unit continues to raise concerns in the
media including a recently released Ombudsman report under the Crimes of Torture as well as a
recent report by the Counties Manukau, chief medical officer, Dr. Gloria Johnson. Reporting to
MidCentral DHB's quality and excellence advisory committee Dr. Johnson noted that the ward
under the Official Information Act 1982
design was "
very unsuitable… the intensive care unit still looks and feels intimidating and
imprisoning, rather than therapeutic". The 2015 Ombudsman Crimes of Torture report noted
“incomplete seclusion and restraint records and ….call bel s in seclusion rooms that did not
register….and a ward design not conducive to providing safe effective mental health care”. The
parents of a woman who suffered a self-inflicted death at the ward have appealed for the
MidCentral District Health Board to get on with a rebuild.
Star 1, Mid Central DHB’s 15-bed elder care ward including mental health service users also had a
concerning 2015 Ombudsman’s Crimes of Torture report noting
“Service Users were being
subjected to prolonged and excessive use of mechanical restraints, specifically having a device
called a ‘T-Belt’ used on them for up to four hours at a time”.
The recently released 2013 Ombudsman Crimes of Torture report into Whanganui’s inpatient unit
Stanford House, noted night safety orders still being used (e.g.; service users being locked in their
rooms at night, effectively being an unrecorded seclusion event). It is currently not known
whether night safety orders are continuing at Stanford House.
3. Housing
Local media has continued to highlight the problems of homeless ness particularly in Palmerston
North. A recent inquiry into homelessness led by the Labour, Green and Maori parties reported on
research that found each person living on the street in New Zealand cost the Government around
$65,000 a year. Getting them off the streets and into secure housing could cost as little as
$15,000.
The Salvation Army reported New Zealand's housing crisis is having a devastating impact on the
most vulnerable families and individuals. With housing and living costs now at an all-time high,
one in 100 Kiwis are classed as homeless because they are living in unsafe or unsuitable locations.
An overnight event in October in Palmerston North titled “14 Hours Homeless” had a good turn
out with people joining hundreds of other Kiwis around the country who slept out in a car, on a
couch or on cardboard to raise funds to help New Zealand’s homeless population.
4. Legal Chal enge
Local peers have attended the past months high court hearing in Wellington brought by human
32
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
rights lawyer Dr. Tony Ellis. The case involved three men with intellectual disability and mental
health issues (two also have autism). Dr. Ellis said the treatment of all three had caused them to
become institutionalized describing their treatment as ‘warehousing’.
Allegations include arbitrary detention, solitary confinement (seclusion), restraint and injury, over-
medication and a denial of access to family, friends, advocates and lawyers, and a denial of access
to possessions. These incidents are alleged to have happened over many years while the three
men were in forensic health facilities, where two still remain. They were all committed as special
under the Official Information Act 1982
patients after coming before the courts more than 10 years ago. They are suing the Government
for more than $800,000 for the years they have allegedly experienced ill-treatment. The men did
not appear in person with video interviews shown to the court instead.
Dr. Ellis reported that the case is significant because
‘the rights of the intel ectually disabled are
rarely, if ever, litigated .. this case becomes important because of that’. The court has heard from
DHB clinicians, Ministry of Health staff and others who work in the field. The abusive treatment, if
proved, would contravene the NZ Bill of Rights Act and the UN Convention on the Rights of
Persons with Disabilities including Article 14, liberty and security of disabled people.
Link to Herald article containing Ombudsman’s Reporting on Torture in NZ
http://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=11676336
Mental health services:
Media
Mental health continues to be a major focus in the local media since our last Ngā Hau e Whā
report. Concerns raised, focus on service access and availability, staffing levels, the increased
suicide rates, availability of and misuse of methamphetamine, seclusion and restraint (especially in
schools and dementia units), homicide in the context of mental health distress, and policing issues
(including mechanical restraints such as Spit hoods and the increased crisis calls to regional police
forces)
Many of these media stories increase debate in our communities and concerns that can at times
fuel additional stigma and discrimination. Service users have commented on the lack of positive
discrimination initiatives such as the Like Minds media campaigns in years gone by.
Places of detention
The Ombudsman has recently released their 2015/16 Annual Report which is available on their
website. Pages 40 and 45 - 49 of the report has the specific detail related to Health and Disability
places of detention but there is also other relevant comment to people who have lived experience
of a psychosocial disability elsewhere in the report.
33
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
A summary of the concerns specific to mental health facilities are as follows;
- Some adult inpatient units being “unfit for purpose”
- Older persons being arbitrarily detained
- Prolonged and excessive use of mechanical restraints
- Complaints policies not being readily available
under the Official Information Act 1982
- Incomplete and missing seclusion records
- Seclusion rooms used as long-term bedrooms
- Lack of restraint training for staff
- A service user found still in seclusion after being seriously assaulted despite requiring surgery 10
days prior
- 'Informal service' users being "environmentally detained" in locked wards and then being
concerned they would be committed if they wanted to leave
- Service users not being able to access the minimum entitlement to daily fresh air
- Night Safety procedures continuing
WINZ Beneficiaries
Around the country the Ministry of Social Development has introduced a type of app for
smartphones and computers (requiring very little data cost) called “My MSD”. It is a user friendly
app and provides a lot of information individuals need about checking payment details, declaring
income, changing bank accounts, managing appointments, reporting job search, re-applying for
job-seeker support, change of address, updating contact details.
Social Services “One Stop Shop” in a rural location has reported a number of their clients don’t live
in cellphone range and don’t own a computer or afford data for their phone. They noted these
clients are always out of credit for phone calls and texts. Even establishing a “RealMe” login is
challenging for many, which is a requirement for pre setting up the MyMSD login. It is reported
that many Social Service providers have despaired at setting up the Government’s RealMe
identifier. It can be quite a stressful experience, particularly for the elderly and those who already
experience stress in their lives.
2. Crisis services
Spithoods
Statistics released by police under the Official Information Act show Spit hoods were used 316
times between August 2014 and July 2016. In just over a quarter of those times, the hoods were
34
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
used on people who were 18 years old or younger. Concerns have been raised in the media about
the impact especially on vulnerable adults such as persons with mental health issues which it
could be particularly distressing for.
New Zealand Police acknowledge Spit hoods are “an intrusive mechanical device” with Amnesty
International UK warning the hoods “could restrict breathing and create disorientation, and could
be dangerous”.
Mid Central DHB inpatient services
under the Official Information Act 1982
STAR 1 (Elderhealth) the 15 bed ward that provides services for the treatment, assessment and
rehabilitation of older people (over 65), including those with mental health issues is again
reported on by the Ombudsman, this time in their annual report. Mention is highlighted of
evidence that some service users are being arbitrarily detained without documentation, and some
service users were being subjected to prolonged and excessive use of mechanical restraints.
Mid Central’s Ward 21 is a 24 bed ward with dedicated wings for both men and women. The High
Needs Unit (HNU) is a secure, 6 bed unit for clients under the Mental Health Act experiencing
more traumatic symptoms of mental illness. Crimes of Torture Inspectors found that the ward
design, in particular the HNU, was not conducive with providing safe and effective mental health
care. Also the DHB’s complaints policy, and information on access to the District Inspectors, was
not readily available in the ward. The seclusion and restraint registers were incomplete and some
seclusion records were missing.
Visits to STAR 1 and Ward 21 in December 2015 resulted in 19 recommendations by the Crimes of
Torture Inspectors across both facilities.
2. Best Practice according to people in your region
Fielding Integrated Health Centre
MidCentral DHB has opened its latest integrated family health center in Fielding. The new center is
a multi-million dollar facility that houses many of the health services a person needs including
mental health and all other general practices, as well as radiology and a pharmacy.
Integrated family health centers (IFHC) are a goal across the MidCentral region so as to provide
central health hubs for communities which are more than just health centers. They will bring
services closer to home, allow for more specialist services, and work to strengthen communities.
IFHCs around the district include Te Waiora in Foxton and now Feilding, with a further IFHC
nearing completion in Palmerston North. Once the Palmerston North facility is completed, around
60 percent of the MidCentral regions population will be covered by an IFHC.”
Kites Trust
• Kites are continuing to undertake 3DHB funded action research looking at peer advocacy
work. The work will continue until the end of December 2016 and is proceeding very well.
35
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
• Kites Trust have successfully received new contracts, including additional contracts for
their Buddies Peer support service which will now extend to Hutt Valley DHB’s inpatient
unit, in addition to the pre-existing contract with CCDHB, a new Youth Advocacy Project -
Peer Tree, and a successful collaboration with Te Korowai Whariki with the Intentional
Peer Support contract.
Whirlwind
under the Official Information Act 1982
• Whirlwind men’s mental health support networks are popping up around the region. They
have a website
(www.whirlwindstories.com) and facebook page. A monthly male-only
dinner get together is held at Hightide Café, Paraparaumu Beach.
3. New Initiatives /Developments in your region
Kia Noho Rangatira Ai Tatou:
• Kia Noho Rangatira Ai Tātou is a unique education programme that puts the human rights
of disabled people and the UNCRPD into a New Zealand cultural context. This two day
workshop has an applied focus which will help ensure that disabled people’s human rights
are upheld. The Disabled Persons Assembly and Te Pou o te Whakaaro Nui have worked
together to develop this programme which examines human rights and the United Nations
Convention on the Rights of Persons with Disabilities (Disability convention). Workshops
are being held throughout New Zealand with attendees of the most recent workshop in
Napier, Hawkes Bay giving positive evaluation feedback
Mental health Awareness week:
• The region is gearing up for this year’s Mental Health Awareness week from 10th to 16th
October with this year’s theme being on connecting with nature. Previous years has seen
many events organized in the region with this year expecting to be no exception.
Campaign to review the mental health system:
• Over the next 3 months in the lead up to Mental Health Awareness Week in October,
campaign group Action Stations is inviting New Zealanders to share their experiences of
the public mental health system. Their aim is to promote public pressure to initiate a
review of the mental health system.
Titled ‘The People’s Review of the Mental Health System” it is designed to allow anyone
involved with mental health in New Zealand – from mental health professionals to those
with either personal or family experience of the system – to tell their story via a purpose-
built website
, publicmentalhealthreview.nz.
36
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Review of the Disability Strategy
• Ngā Hau e Whā representatives attended Disability Strategy review meetings. Based on
group discussions at the Wellington and Manawatu region Hui’s a report was drafted on
behalf of Ngā Hau e Whā and submitted as part of the consultation specific to psychosocial
disability.
Peer Tree
•
under the Official Information Act 1982
Kites Trust is developing a Youth Peer Support Programme for young people who
experience mental distress. This project has been made possible through funding by the
Todd Foundation.
The program is for young people (18-24 years old) who are experiencing mental distress.
The groups will be facilitated by young people with lived experience of recovery, trained in
the
Intentional Peer Support model.
Buddies
• Kites agreed to extend its Buddies service to the Hutt Valley DHB in-patient service Te
Whare Ahuru. The new Buddies service will be based on the current CCDHB Buddies
service at Te Whare O Matairangi. Volunteers are being recruited and a coordinator has
been employed.
New Hawkes Bay mental health unit
• Hawke's Bay’s new mental health unit was officially opened earlier in the year and has just
won an accolade for its design. The new $22 million unit, Ngā Rau Rākau, is on the grounds
of the Hawke's Bay Hospital. It is a 23-bed unit made up of 16 inpatient beds and seven
sub-acute beds. However, the Improvements to the mental health unit were reported in
the media to have “blown out the MidCentral District Health Board's budget with the DHB
forecasting a deficit expected to be $2.7m”
Rural Mental Health
• New rural health national initiatives continue to generate local interest especially in the
Wairarapa. This includes new initiatives such as
Farmstrong who have a series of North
Island Woolshed music events in October and November. Also DairyNZ introduced the
GoodYarn initiative in February and has run more than 30 workshops nationally including
in our own region, helping more than 600 farmers and rural professionals. The East Coast
rural Support Trust have created a resource
“Feeing Down on the Farm”
3. New Initiatives /Developments in your region
Kia Noho Rangatira Ai Tā
tou:
The Kia Noho Rangatira Ai Tātou education programme that puts the human rights of disabled
people and the UNCRPD into a New Zealand cultural context continues to be held around the
37
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
county. This two day workshop has an applied focus which will help ensure that disabled people’s
human rights are upheld.
The Disabled Persons Assembly and Te Pou o te Whakaaro Nui have worked together to develop
this programme which examines human rights and the United Nations Convention on the Rights of
Persons with Disabilities.
Workshops in the Central region so far have included one for Disability Support Services and one
for Disabled Persons in Whanganui, one for Disabled Support Services in Hawkes Bay, with another
under the Official Information Act 1982
due in Wellington the end of November. Attendees have reported very favourably on the
workshops to date.
Mental Health Awareness week (MHAW):
The region held many events and initiatives in celebration of Octobers Mental Health Awareness
week. The theme was connecting with nature with initiatives including:
• Mental Health services at Mash Trust having a series of special events on including bush
walks and arts projects linked to nature.
• ‘State Highway 48’ was a musical that toured the North Island throughout Oct as part of
MHAW. Good turnouts were seen for the Central Region shows including shows in Napier,
Palmerston North and Whanganui. The musical tracked the life and times of an everyday
family and their friends as they navigate the road of middle age with a reminder about
what’s important; the dangers of not facing up to depression and a celebration of the
everyday.
• The New Zealand Association of Counsellors had a series of public lectures in Hawkes Bay
as part of MHAW including topics such as Reducing stress with Beachcombers Q&A’s,
Causes and Tools for Managing Anxiety, and Holistic Wellbeing
• Other events included Palmerston North’s ‘Gentle Stroll around the Esplanade’ followed
by morning tea, Whanganui Regional Health’s team Shared Picnic Kai, and various bake
and cake events in Manawatu, a week-long series of talks in Whanganui by various service
user and services, and a series of guided walks throughout Manawatu.
• Unfortunately there was no reports of any events being held in the Wairarapa region
•
Review of the Disability Strategy
Embedded with this report is the submission that the Ngā Hau e Whā Central Regions
representatives drafted for the Disability Strategy review. The submissions was based on
group discussions at the Wellington and Manawatu regions hui’s, with the focus on the
consultation that was specific to psychosocial disability.
•
Tahatū Rangi Symposium
Both Central Representatives attended the Te Pou / Platform Tahatū Rangi Symposium on
behalf of Ngā Hau e Whā. The two day symposium was an opportunity for sector leaders
38
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
and their allies to come together to collectively re-imagine the mental health and
addiction system. New liaisons were forged as well as meeting up with numerous people
we have worked closely with in the past. The outcomes from the two days were captured
creatively in this poster presentation. (Note the Lived Experience section on the photo
that NHEW reps ensured was highlighted throughout the two days!)
•
Ombudsman ‘Experts with Experience’
The Ombudsman Office was successful with an application for funding from the UN’s
under the Official Information Act 1982
Optional Protocol - Crimes against Torture. The funding is for training and monitoring skills
to a group of people who have personal experience of using or caring for someone who
uses mental health services in New Zealand. Termed
‘Experts by Experience’ they
will
assist the Ombudsman Crimes Against Torture Inspectors to undertake visits to places of
detention.
The writer was successfully selected for the initiative and will report back on progress with
the project in next month’s report.
•
Wel ington Regions Suicide Prevention and Postvention Leadership Group
This new wider Wellington region initiative aims to reduce suicide and minimize the
impact of suicide across Wairarapa, Hutt Valley and Capital Coast DHBs populations. Both
Central Region representatives are applying to join the group on behalf of Ngā Hau e Whā.
4. Addictions
New Wairarapa Gambling service
• The Salvation Army has been contracted to provide a new problem gambling services in the
Wairarapa -- including counselling support for those struggling with a gambling addiction,
as well as family members, partners and others affected by someone else's gambling.
• Public Health services are also delivered, aiming to reduce the harm that gambling can
cause, help agencies to develop policies around gambling and raise awareness of problem
gambling in the community.
• Counselling for problem gamblers in Wairarapa was previously offered by Wairarapa
Addiction Services and then Care NZ, until the Salvation Army picked up the contract
recently. Since then, the service has seen new clients, including family members, who
range from professionals to beneficiaries.
5. Whanau/family services
New links with Family Whanau Services
• New links were forged at recent Hui’s with staff from both Manawatu and Whanganui
‘Supporting Families in Mental Illness’ organisations.
39
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
• Manawatu Supporting Families report they are finding that people that are experiencing
depression and anxiety are finding it hard to access GP’s because of the cost. Therefore
they become more unwell and the challenge is getting people assessed at Community
Mental Health as they are asked to see their GP for a referral. It becomes a never ending
circle and people are running up debits at GP practices. Because of this people are
presenting more acutely unwell at services.
under the Official Information Act 1982
6. Maori services
Advice will be sought around making links to Iwi, and Maori networks and stakeholders so
progress will be noted in the next report
• Both Central Representatives are due to visit a local Maori respite crisis service (Te Waka
Whaiora). The new liaison will help us continue to extend Nga Hau e Whā’s regional
communications and liaison with other Maori services throughout the Central Region
• The Emerge Aotearoa Consumer Advisor is helping us engage and liaise with his own pacific
networks
• The Kia Noho Rangatira Ai Tatou education programme that is being presented around the
country for disabled people (including persons with psychosocial disability) and Disabled
Support Services (not including psychosocial support services) is partly presented by either
a regional or National Kaumatua. The programme has a strong focus on presenting Te Tiriti
o Waitangi from a human rights perspective.
40
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health

Released
under the Official Information Act 1982
Member: Kieran Moorhead
Region: Northern - Auckland
Meeting date: 8/9 September 2016 3/4 November 2016
1. Issues/chal enges identified by people in your region
CHAMP – Counties Manukau Peer Potential Project – Cassandra Laskey
Counties Manukau Mental Health and Addictions Partnership (CHAMP) commissioned the Peer
Potential Strategic Action Plan (2016 – 2021) to develop the mental health and addiction peer
support workforce funded by Counties Manukau Health in both the DHB and NGOs.
There is a growing international trend towards a peer workforce in mental health and addictions,
therefore it is timely to discuss and analyse the peer workforce in NZ:
Counties Manukau (CMDHB) has the largest funded peer workforce in NZ – 69.0 FTE.
CMDHB has three fully peer-led services, the rest of the peer workforce operate in Multi-
Disciplinary Teams.
Over 130 people participate in Peer Employment Training (PET) in CMH but only 12% of the people
go on to employment as peer support workers. This could be because of the lack of growth of peer
support roles in CMH over the past few years.
Recommendations:
o Reconfigure the PET course into three levels – personal recovery, informal peer support
with open entry and formal peer support with limited places for people who want to work
in peer support.
o Clarify the respective roles of the two PET providers.
o Encourage the development of more peer support positions.
Next part of the Peer Potential Project 2016/2017:
41
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
o A fully established Peer Support Governance Group to drive and monitor the
implementation of the Action Plan.
o Complete evaluation of peer support in the CMH district.
o Redesigned peer support workforce development opportunities with a clear pathway
for progression for peer support workers.
o Redesigned and accessible training for colleagues on peer support and recovery.
2. New Initiatives /Developments in your region
under the Official Information Act 1982
Feedback from Waitemata DHB CAMHS:
Respect –
4.5 / 5
“The majority of you feel that you are respected by people here”
Communication –
4.5 / 5
“Most of you feel that staff work as a team and support each other to ensure you get the best
care”
Support –
4.5 / 5
“We’re glad most of you feel safe here. If you’ve been here a little while and still feel unsure about
stuff, talk to your keyworker or write the consumer advisor a letter”
Appointments –
3.2 / 5
“This is one we are pretty worried about. We’ve implemented CHOICE teams to get through
appointments quicker as our demand increases!”
Plan Reviewed –
4.5 / 5
“Treatment goals should be reviewed consistently – even if it’s just to say ‘Yep all good’.”
Decision Making
– 5 / 5
“Clinicians ask you what you want for yourself”
“We’re committed to this, so we are happy to see this result”
Recommend –
4.3 / 5
“Most of you would recommend us to friends/family”
Family/Whanau –
4.5 / 5
“The majority feel their family is encouraged and informed”
Culture –
4.5 / 5
42
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
“You feel that we acknowledge your cultural needs”
“Many NZ Europeans did not answer this question – please do!”
Rodney working party is scoping out some locations for a permanent building in Whangaparoa –
we’re also looking for a few rooms in Warkworth and Wellsford.
New Clinicians – Our Choice Team in the North will be filled by some clinicians from Youth Health
Hub, and an experienced Eating Disorders Clinician will be joining the Liaison Team in September.
under the Official Information Act 1982
CMDHB Health – Mental Health and Addictions Integration update:
Progressing the implementation plan An implementation plan for the roll-out of the integration agenda was presented to a meeting of
CM Health’s Exec Leadership Team on 8th November. The plan put forward an approach for
enabling integration through proposed changes across specialist mental health provision,
specialist addiction provision and NGO provision. The plan recognised the excellent contribution
that each component part has to make in delivering an enhanced experience for people using our
services, and to the gains in their overall health outcomes and health equity. ELT endorsed the
plan to be progressed to a meeting of the Community and Primary Health Advisory Committee
(CPHAC) on 21st December and the February 2017 meeting of the CM Health Board. Subject to the
outcome of those discussions, we commit to update the sector with clear next steps and
timescales after the February meeting of the Board. Recognising the significance of this agenda,
the timescales for progressing implementation will ensure that sector partners receive maximum
notice of any proposed changes.
Franklin Integrated Care Locality Team (ICLT)
The Franklin Integrated Care Locality Team (ICLT) was formally established within the Franklin
Locality on Monday 21st November. The first members of the team are providing the initial
presence and will be joined by colleagues, including our NGO and specialist addiction partners.
The initial team includes two nurses and an OT with combined experience across child and youth,
adult, and older adult mental health. The team is enhanced with dedicated psychiatrist time, and
support from a CAMHS nurse practitioner and an adult mental health clinical nurse specialist. The
team has a base at Pukekohe Hospital alongside other DHB community healthcare teams and will
be working with those teams in a multi-disciplinary team model. This approach will enhance our
capability in relation to a ‘whole of health’ approach to people’s wellbeing. In the coming days and
weeks, the team will be engaging with primary care, offering a range of ways to work together
through consult liaison, shared care, care planning, assessment and advice. The work of the ICLT
will be in addition to the existing referral pathways.
We are excited about the progression of this initiative and see it as the first step towards an
integrated model of care across all of Counties Manukau. The team will be working with an
improvement advisor from Ko Awatea to assess the impact and benefits through PDSA cycles,
43
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
learning and developing as we go. This initial step is the first of many moving forward and we are
excited about enhancing the team with NGO and specialist addiction capability.
Integrated Mental Health and Addictions Leadership Group
The Integrated Mental Health and Addiction Leadership Group was established in April 2015 to
help guide and inform progress towards an integrated model of care. Members were selected for
their experience and expertise across mental health and addictions and the broader health and
care system. The membership provided perspectives from Māori, Pacific, primary care, NGO,
under the Official Information Act 1982
specialist mental health, specialist addictions, and locality community services. The group met
earlier this month and gave their reflections and contributions on the implementation plan due to
be presented to ELT and the next steps for the programme.
Subject to feedback from CPHAC in December and the Board in February 2017, the work
programme will move into a defined implementation phase. With the expectation that this phase
will involve a procurement process to deliver locality services, it was recognised that clear
consideration needed to be given to any conflicts of interest moving forward and how best to
provide the necessary sector-wide leadership within that context. Members agreed that it would
be appropriate to disband the group, with no further meetings under the current membership.
The group has been an invaluable resource in progressing the agenda, providing insight and
challenge. Moving forward, we will look at what leadership is required to support the
implementation at both a governance and operational level.
CMDHB Inpatient Unit Tiaho Mai re-design update: The architect leading the re-design of
Middlemore Hospitals Tiaho Mai acute mental health unit provided an update. Construction has
already begun on the grounds of Middlemore, and the foundations and walls are being laid
currently. The design of the unit utilised a co-design process with people who use the inpatient
services, as well as overseas experts from Australia. The new Tiaho Mai will have 76 individual
rooms each with its own bathroom, separated into two areas, High dependency and Low
dependency. Feedback from CHAMP NGO network was to be wary of language used as high
dependency and low dependency might not be appropriate, there was also a room labelled
‘Judge’s Room’ which CHAMP asked to be changed as that is not language we wish to use
anymore. There are 5 grass and concrete courtyards inside the unit and each room has a view into
one of these courtyards which was based on feedback from people currently using inpatient
services. There are no labelled seclusion rooms but there is an area which has been labelled ‘low
stimulus’ and it has its own room, bathroom, and lounge area which can be kept separate from
the rest of the unit. It was mentioned that this area may not be for people deemed ‘too at risk’ but
could be for say mothers who have children or families to stay together in.
Housing First Initiatives: There is new Housing First Initiatives beginning across Auckland, which
are working with CORT social housing provider to get vulnerable people into housing, and not
44
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
using the requirement of being in accommodation a barrier for receiving support. One initiative
discussed is a mental health initiative that houses four women who have historically been
categorized by the mental health system as ‘dysfunctional’ or ‘uncooperative’. The aim is to have
the women in safe, reliable housing where there is no expectation for them to leave any time
soon, and for mental health services to provide support for the women when and how they want
it. There is also a desire for the women to provide informal peer support for each other as might
occur in a flatting situation.
under the Official Information Act 1982
Consumer/Mental Health Promotion Event: A group of ADHB providers including Changing Minds
are planning an event for 2017 that aims to bring public awareness about mental health and
provide ways of seeking information and support. The group are currently speaking to the
organisers of Pasifika Festival, a large public event held in Western Springs annually, and they are
keen to partner and have a large public mental health attraction at Pasifika. The attraction will be
experiential, for all ages/families/whanau, and there will be information, resources and support
available.
Formatted: Font: 8 pt
Collaborative research:
Optimising treatment outcomes for depression in primary care (OptiMA3-NZ)
Formatted: Heading 2, Justified
Formatted: Font: (Default) Calibri, 11 pt, Bold
Formatted: Normal, Left
Formatted: Heading 2, Justified
Richard Tranter is a consultant psychiatrist at Nelson Marlborough DHB with honorary
appointments at NMIT and the University of Otago. His research in the UK was focused on
improving outcomes for depression in primary care settings. He has experience of being a principal
investigator on large clinical trials and has developed successful primary care networks for
recruiting to clinical trials.
Formatted: Font: 8 pt
Dr. Jacquie Kidd Nga Puhi,
is a Senior Lecturer at the School of Nursing, University of Auckland.
She has experience in qualitative research with Māori communities, and has led two significant
kaupapa Maori projects focusing on palliative care and prostate cancer respectively, with a strong
focus on health literacy. Jacquie will be involved with study design, data analysis, dissemination
and stakeholder partnerships for the Māori arm of the project and for the nurse led aspect of the
intervention.
Varsha Parag is the lead biostatistician at the National Institute for Health Innovation at the
University of Auckland with 16 years’ experience in epidemiological studies and clinical
trials. Varsha will provide statistical oversight of the trial in relation to study design, and conduct
the data analyses.
45
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Aim
• To evaluate the clinical effectiveness and economic benefits of a nurse led intervention,
assisted by an online system, Psynary, to optimise existing treatments for depression in
primary care.
under the Official Information Act 1982
Primary hypothesis
•
For new presentations of depression to GP practices utilising the “blended” Psynary assisted
nurse practitioner health care pathway there wil be a significant increase in patients achieving
complete remission from their depressive symptoms after three months of treatment
compared to GP practices fol owing their usual care pathways.
Exploratory aims
• Acceptability and accessibility of the online system to patients and practice nurses will be
explored using semi-structured interviews and framework analysis. There will be particular
focus on the impact of the “blended” nurse led health pathway on accessibility to
interventions for Māori health consumers.
Centres and Participants
• A consortium of five schools of nursing will act as the research hubs for conducting the clinical
trial. Each hub will recruit and coordinate three - six GP practices. Practice nurses will be the
lead points of contact with the research team.
• All patients presenting to the trial GP practices with a suspected diagnosis of depression over a
12-month recruitment period will be invited to participate in the study.
• Patients who verbally agree to take part will be registered on to the Psynary system by the
practice nurse. When patients log on to Psynary for the first time they will be presented with
information about OptiMA3-NZ, available in English or Te Reo Māori.
• Patients will then complete the online consent form. Only if they consent to all the items will
they be able to proceed with the Psynary baseline assessment (detailed below).
• The initial part of that assessment involves a diagnostic algorithm for ICD-10 mood and anxiety
disorders. Only those patients meeting criteria for a moderate or severe depressive episode
will be included in the intervention or Treatment As Usual arms of the trial.
46
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
• Practice nurses will keep records linking patient identification, including NHI number, to the
anonymous Psynary username. These records will be stored at the GP practice and will not be
shared with the research team. These records will be used by the GP practice to identify
patients as part of their routine clinical use of Psynary, and for adverse event reporting to the
research team
Interventions
under the Official Information Act 1982
Description of the online support system: Psynary
• Psynary is an anonymous web-based system that assists non-specialist clinicians and
patients in the assessment of mood and anxiety disorders, treatment planning, monitoring
and optimisation.
• Patients are registered on to the system by their clinical team and are allocated an
anonymous username (a colour and a number) and a temporary password.
• Patients are then able to complete a detailed baseline assessment in their own time, in a
setting of their choice.
Psynary does not collect any personal identifiable information, such as names, date of birth or
addresses. The baseline assessment covers the following domains:
• Demographic information
• ICD-10 mood and anxiety diagnoses
• Past psychiatric and medical history
• Family history
• Current and past psychiatric medications, including dosages, duration, compliance and side
effects
• Psychological interventions
• Depression symptom severity
• Anxiety symptom, avoidance and impairment severity
• Pregnancy, breast feeding and contraceptive status
• Alcohol and drug usage
• Cognitive functioning
• Patient identified goals for recovery
• Patient treatment preferences
4. Addictions
Counties Manukau Health - AOD Collaborative:
Peer Group Project:
47
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
We know that when we broadly target teenagers and young adults, we don’t tend to reach and
engage the young people who need support the most. This project used Rescue’s Peer Crowd
Discovery methodology, which has been successfully implemented in the USA and other countries,
to segment the New Zealand teenage and young adult population into specific “peer crowds” with
similar interests, attitudes, lifestyles, and behaviours.
This was used to explore the relationship between these peer crowds, alcohol, and other risk
factors. These findings will make it easier to engage diverse teen and young adult populations, and
under the Official Information Act 1982
break down barriers by making peer influence easier to understand and to be incorporated in
interventions. We focused on the multifaceted Counties-Manukau area, and tested whether these
findings were generalizable to another New Zealand region.
“We’ve got an international expert in behaviour change marketing, Jeff Jordan (President and
Executive Creative Director | Rescue | The Behaviour Change Agency), coming to New Zealand,
and we’d love for you to join us as he presents. The most exciting part is that a group of health and
social support organisations have been working with him and his company to get information on
New Zealand teenagers and young adults. He will be sharing what we have learnt about our youth,
with alcohol as the main risk factor, and it will be a great opportunity for you to reflect on how this
can inform your work!”
LookUp Auckland DHB Youth Event – Wellbeing and AOD:
Official number of attendees: 230 – 110 young people – 14 schools
Auckland DHBs Youth event co-created by young people and delivered by a collaboration of young
people and DHB + NGO organisations.
1. Balance and Connect
o Youth line interactive workshop to create support trees.
o Pocket pick-me up (box art) designed with Toi Ora that reflects on your life and identity.
2. Know Better, Do Better
o Auckland Sexual Health Service workshop on consent, including the viral video on the ‘tea’
analogy and scenarios.
o St John’s Cadets teaching some basic first aid skills for situations involving alcohol and
other drugs.
3. Brave Conversations
o Odyssey House have giant traffic lights on the floor and a bunch of scenarios – what would
you do if your mate was in trouble with alcohol or other drugs?
o Altered High is also running an activity that reflects on the tough stuff that can happen
when alcohol and other drugs are involved.
48
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
4. Making a Difference
o Come and participate in a community action workshop with CAYAD about how to make a
difference to an alcohol or other drug problem.
o Hear a panel of young people speak about their involvement leading youth health
programs – including young people from St John’s Cadets, Mental Health Foundation’s
POD, Affinity Youth Advisor Group, Peer Sexuality Support People, Rainbow Youth, and
under the Official Information Act 1982
School Health Councils.
ADHB Providers DHB/NGO:
Substance Abuse Compulsory Treatment Bil : Cate Wallace from the shared Funding and
Planning team at WDHB/ADHB provided an update on the new Substance Abuse
Compulsory Treatment legislation that has recently had its third reading at parliament,
with the bill set to become law next year (2017). Cate said that the legislation applies to
people who are at the extreme end of substance abuse for example people experiencing
Korsakoff Syndrome from alcohol misuse. Cate and the rest of the funding team are in
conversations with the Ministry of Health about how many people the legislation may
apply to, which was originally around 200 but this estimate has increased to 500 people.
The funders are also negotiating funding for the people who will require services under the
new legislation, which the Ministry of Health initially costed at $500,000, but Cate
estimates they will probably be looking at closer to $1 million.
TheMHS Conference August 2016
Keynotes:
- Arthur Evans from Philadelphia spoke about public health approach to mental health and
wellbeing and showed off some emotive and visually impressive murals that have been done
across Philadelphia to highlight some of the health and social problems and encourage people to
work together to be a part of the solutions to these problems.
- Robin Youngson an anesthatologist emphasised the power of being compassionate, taking the
time to listen to people that you encounter in your work life, clinical or non-clinical and the
resounding impact that your compassion has on others and the evidence-base that supports this.
- Joe Macdonald spoke on the final day, about people as not just discrete entities to be catalogued
by a system and treated, but as people who live in a context with a story, and motivations and
struggles, and how our systems do not cater to this variation.
TheMHS Conference - Coercive Community Treatment:
• Discussion on the readiness to end coercive community treatment practices.
49
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
• Clinicians argue that CTOs enable people to reliably access treatment in their community.
• Some questions were raised asking why we can’t have reliable and effective services
without CTOs.
• In the context of reviewing NZ’s mental health legislation, someone who works for the
under the Official Information Act 1982
Ministry of Health commented that there is the fear that we are currently living in a more
socially conservative time and any changes to our legislation could result in more coercive
practices.
Whanau and Family
Waitemata Stakeholders Network:
Supporting Parents Healthy Children: To mandate MHS & Addiction services to work in a family
focused way to help parents achieve the best for their children.
• Risks related to parental mental health and addiction issues, e.g. poor outcomes, increased
risk of MH and/or addiction issues, children taking on care giving responsibilities for their
parent.
• There is growing international evidence for effective interventions to improve short and
long term outcomes for children.
• What is needed:
o Data on the number of children in NZ affected
o Services to routinely identify children of parents
o Adult services to recognise and respond to people as parents and develop
family/whanau focused practices
• Where are we up to:
o Supporting Parents Healthy Children Leadership Group underway since 2013
o Review and dissemination of resources, auditing, development of an
implementation of guidelines across the services, building relationships, reviewing
policy, developing pathways (DHB/NGO)
o COPMIA full days training, 3 x in 2016
• Data – regional group undertaking work to identify and agree the data collection
regionally.
• Next steps – seek further representation by Adult Clinicians and managers, agree and
progress actions in implementation plan, socialise and train.
50
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health

Released
under the Official Information Act 1982
Member: Victoria Roberts
Region: Central South
Meeting date: 8/9 September 2016 3 /4 November 2016
Issues/chal enges identified by people in your region
1. Mental health services:
Oasis Network
Te Whare Ahuru HVDHB
o Staff in mental health wards need to be trained to be non-aggressive
o Long term services users do not get a fair go.
o In the inpatient unit there are no discharge plans; informed consent does not happen at all;
no wellness plans
o Service users need more advocacies around their rights.
o Most agencies will only pick up new clients if they are suicidal or threatening harm to
themselves.
o Person reported that while they were in TWA (Te Whare Ahuru – inpatient ward) they
were refused permission to call a lawyer.
o There are no services funded especially for the elderly: this makes it hard for them to get
to Oasis; maybe there is a need for an elderly peer support group?
o The staff bullies the patients and treat them like children. (Tell them to go to bed at 8pm.)
o The staff are heavy handed and frequently threaten the people in the ward with the lock
up if they object to what is being demanded from them. (Not obeying staff directions)
o “The staff throw their weight around” it is a hierarchical system and people using the ward
are well below the staff.
o It is a power and control issue with ward staff.
o There is some worry about the soon to begin frozen meals they will be made in
Christchurch and Auckland and sent frozen to TWA. They have concerns about people’s
health and want the current great meals to continue.
o There is no counselling available at Te Whare Ahuru (TWA)
51
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
2. Communication:
Oasis Network
A well-known Hutt Valley DHB (HVDHB) service user went missing recently and the people at Oasis
said they would have welcomed immediate input from clinical services.
o Clinical services should reach out to service user groups who are at the forefront of
under the Official Information Act 1982
supporting service users especially at times of emergency.
o Clinicians should have realised that there would be a lot of strain and grief within peer
services.
o They could have designed some information/education about how people in Oasis might
be feeling; what to notice about people who are grieving;
o They should also realise that people who use mental health services often have lots of
other past unresolved grief; even having a diagnosis of chronic illness can cause grief.
o People would like to hear from speakers: mental health services in the community; the
DHB could be invited to talk about hospital services and functions.
3. Crisis services
Oasis
o CATT takes too long to respond – if they respond at all.
o They seem to be overworked and underfunded
o They have heard that CATT has been restructured by don’t know how.
o People don’t know when to ring Te Haika (crisis line) or who they will get and would like
some education from them.
o There is a need for a crisis service for mothers and babies.
o Respite services in the Hutt are operated by PACT and EmergeAotearoa
o There is no instant access/emergency housing in the Hutt.
Mental Health Services
Crisis Service CATT
o Aggressive clinicians; interactions create large misunderstandings
o If you ring up CATT you are always put on hold and you are sometimes just cut off after
waiting for a while.
o It’s hard to get CATT to see you when you need help.
Knowing my rights
o “I need to know my rights around the Mental Health Act. Who can put me under the Act?”
o “If I go to the Wellington and Hutt Valley Community Law center can I request a man (or a
woman) to talk to?”
52
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Consumer Leadership Development Fund
o This is needed for all consumers especially those who are unemployed.
o It would be a training fund that people could apply to, to be upskilled.
o It should be administered by peer workers from several different services in the region.
Medication issues
o Why can’t people who have been stable on clozapine for years be monitored by their GP?
It could also be overseen by a trained nurse or nurse practitioner.
under the Official Information Act 1982
o The same issue with Opioid Substitution Treatment - why can they not transfer to a GP?
o Some people have been on anxiety medications for many years and they are now being
taken off these cold turkey. People have major changes made to their medication and do
not receive adequate notice, advice or support. This is dangerous practise and sadly it is
the consumers and their loved ones who face the consequences.
o There needs to some professionals who can assist people to gently taper off medication
o Given that there are many side effects (physical) of psychotropic medications many people
are keen to reduce the use of these medications – a professional to assist would be
valuable. People trying to reduce these medications are often seen as non-compliant and
punished.
The medical model which says that there is a chemical imbalance is losing ground. It says
medication will be needed forever in spite of the knowledge that the medications used are causing
brain damage. A biosocial model that privileges the developing complex neuroplasticity knowledge
is preferred. Our brains can and do, heal.
4. Housing
Oasis
o Clinical staff have a far too high tolerance for homelessness
o Homelessness can be linked to wellness because people who are even slightly unwell can
make bad choices.
o Some mental health funding should be ring-fenced for housing.
5. Civil defence
Oasis
o Many service users are just not financial enough to put aside emergency supplies for 2-3
days. It takes time, money and space which many people do not have,
o Medication supplies for 2-3 days – what do other people do?
o Civil defence helplines should be tied into peer support lines and numbers
53
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
6. Service user fund
Oasis
• There should be a dedicated fund (government funding required) for peers to apply to.
• This could fund: first aid training; governance; civil defence and others as well.
Linkage
Rex Delaney
under the Official Information Act 1982
• Dairy owners have been letting people accrue debts and then demand to take their cards
off them. In one case the debt was up to $1,000 and the person had to go to a loan agent
to repay the dairy and get his card back.
• Some dairies are selling people single cigarettes (around $1 each). This is totally illegal. If
anyone hears about this practice please let the community constable know.
• The Mental Health Foundation has met with the Wellington City Council (WCC) and there is
to be a project focused on isolated men in the community
PATHS Wellington
• This service was provided by Cap Coast DHB and MSD to assist people on sickness and
invalids benefits into work. The funding has been cut and the service closed down.
Feedback from Oasis Network’s Regional Consumer Forum 8 November 2016
o Given that there are many side effects (physical) of psychotropic medications many people
are keen to reduce the use of these medications – a professional to assist would be
valuable. People trying to reduce these medications are often seen as non-compliant and
punished.
o The medical model which says that there is a chemical imbalance is losing ground. It says
medication will be needed forever in spite of the knowledge that the medications used are
causing brain damage. A biosocial model that privileges the developing complex
neuroplasticity knowledge is preferred. Our brains can and do, heal.
Community Mental Health Team (CMHT):
Requests to change clinicians
o There have been several requests for people to have a change of doctor and/or nurse or
social worker. These came from people who have not made these requests before. These
requests are routinely declined.
54
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
o There is no reply to these offers
Homelessness
o There is a very high tolerance within mental health services of homelessness. It is known
that people who are delusional or suffering from PTSD find it hard to maintain a home.
o It is common for people being released from prison to end up being homeless and living
under a bridge. Rimutaka Prison is quite near. On release people only get $360 – Steps to
Freedom.
under the Official Information Act 1982
Local PHO
o Has reduced funding of 15% This means many community services have had to be cut e.g.
Women’s Centre groups
o But it appears that funding to Youth groups may have increased
People under the Act
If you are not under the MH Act you do not have access to District Inspectors even if you are in the
ward. And we all know there are ways for people to be kept in the ward without using the Mental
Health Act (like threatening to use it). There is not legislative or paid ability for a DI to see people
not under the Act.
Housing New Zealand
o HNZ is evicting people for drug use and with P there can even be just a low reading. This
may not even be the fault of the tenant being evicted.
o There appears to be a policy by HNZ not to upgrade their houses if people have been in
them a long time. No repairs or renovations are being done and some people have shabby
wall paper and paintwork.
Men’s Support
There is a need for men who have been given six- day no contact orders by police to be given
some place to stay. Many are broke, have nowhere to stay and often go home with their partners
consent because she feels sorry for them. Then the cycle of violence restarts.
All specific anger management programs have stopped running. There is a need for these for men
and women.
Best Practice according to people in your region
Oasis Network
o A question was asked: When you first make contact with Ambulance, Police or CATT do
they routinely ask if you affected by drugs, alcohol or gambling? The group agreed that
they did.
55
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
o A nurse from Ward 27 (Wellington Hospital) told a person that the first thing she asks for
when a new person is admitted is whether or not they have an Advance Directive.
o Warmline is excellent and Samaritans are a good support. A suggestion was made for a list
of all available support services.
o Oasis is a great community support. People are not sure why there is no money for food at
Oasis because the DHB always has plenty of money for food at their events and meetings.
Vincents Art Workshop under the Official Information Act 1982
o Vincents is open to the whole community in the spirit of inclusion. Different to Pablo’s is
that they are more like an art school.
o Vincents is now involved in Peer Advocacy work and has a contract along with Te Ara
Korowai, Newtown Union Health and Kites. The work is going well and there has been a 6-
month extension from CCDHB to 31 December 2106.
Suzy spoke about the peer advocacy work and how the numbers of people seeking it is
steadily increasing.
Linkage
Rex Delany
• The Mental Health Foundation has met with the Wellington City Council (WCC) and there is
to be a project focused on isolated men in the community.
Hutt Valley
o “I find that people are more accepting of me than they were. Retailers and people like
that”
o “I was not sleeping and needed some help. I was asked if I wanted to go to respite or go
into the ward. I said respite of course and it was the best thing ever. It had curtains and I
got some much needed sleep. I was there for five days for assessment. After that I was
okay to go home.”
Kaibosh – a food rescue group has been giving Oasis Network (as well as other groups) some food.
Buddies Peer Support has now started in the Hutt Valley. They are based at MIX.
Housing New Zealand (HNZ) now has a regular forum with Oasis Network. This supports HNZ to
support their tenants with mental health or addiction issues.
There are now men’s and women’s support group running at Oasis every week. These are
excellent.
56
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Amigos Wellington
The Joy of Improvisation.
Discover your creative potential and enjoy improvising scenes and stories in a safe, positive group
environment.
o Explore roles under the Official Information Act 1982
o Create dramas
o Learn about performing
o Gain more understanding about human life together
These classes will resume again on
Wednesday 12th October 2016 and run weekly until 14th
December 2016 only. Sessions run
2pm to
4pm. Once again, our wonderful tutor will be Ali Little.
Venue is Newtown Hall in Daniell Street Newtown, and is wheelchair-accessible.
People found these sessions fun and non-intimidating. Free to people who are, or have been
mental health consumers.
Oasis Network Program – an excellent format.
Advocacy group: Tuesdays 1–2:30
o These groups cover self-advocacy and systemic advocacy. We discuss our rights and
responsibility to honour other people’s rights. In October we learn about what our Annual
General Meeting is for and how to make informed voting decisions.
o Tuesday 4th - Guest speaker:” Vicki - Salvation Army, Oasis. Gambling
o Tuesday 11th - AGM: What do our board members need to know?
o Tuesday 18th - AGM: Checking out the candidates
o Tuesday 25th - AGM: Understanding the voting process
AGM: Thursday the 27th October from 5:30. Please let staff know if you need a ride home.
Healing Voices movie: Wednesday 19th October at 12: 45pm at Pathways. There are only a few
tickets so book with Sue.
Recovery Art Journaling: Wednesdays 1– 3.00
o Recovery journaling continues this month.
o We will continue trying new techniques and recording thoughts and feelings in creative
ways. Please book in as this is very popular.
o Wednesday 5th — Creative self-care
o Wednesday 12th— Stop sabotaging self-care
o Wednesday 19th
- 8 artsy self-care projects
o Wednesday 26th—Easing anxiety
57
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Kai time on Fridays
o Would you like to eat a hot meal on Fridays at Oasis?
o Add your name to the whiteboard near the kitchen on Friday morning.
o When we have three volunteers’ we will start cooking.
o NB: Volunteers may do a Food Handling course in the future.
Members meetings every 2nd Friday 1- 2:30
o Friday 7th October 1-2
under the Official Information Act 1982
o Friday 21st October 1-2
o We encourage members to attend your members’ meetings.
Men’s group
Runs Thursdays from 1– 2:30
Mental Health Awareness week:
o
Friday 14th 11– 3
o River walk : leaving Oasis at 11
o Lunch at Oasis: 12 –1
o Mindful river stone art 1-3
Recovery group: Fridays 10:30-12
o Friday 7th
o Friday 14th - Mental Health Awareness week: walk and lunch
o Friday 21st - Work focus – who can help me find work?
o Friday 28th - Work focus – who can help me find work?
Study Buddies: Wednesdays 10 - 12
o We are really excited to see so many members are studying.
o If you want to find out about courses or are studying you are welcome. Sue is here to
support your study or help you apply for courses.
“It does not matter where you go and what you study,
what matters most is what you share with yourself and the world.”
Santosh Kalwar
Women’s group -Thursdays 10 -12
Life style and substance addictions
We have great caring and sharing and learning happening in Women’s group. During each group
we touch on a topic women have chosen. We also integrate relaxation and sensory techniques
into each session.
58
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
During October we will be discussing addictions and or misuse of substances etc.
o Thursday 6th October— Problematic substance use: Rosemary Casey HALT Services
o Thursday 13th October—Components of Addiction: Rosemary Casey HALT Services
o Thursday 20th October 2016—Who can help:
o Thursday 27th October 2016—The quit cycle: Lisa Phillips, Salvation Army, Bridge.
o
Women’s group peer mentors and volunteers
under the Official Information Act 1982
o Thanks again to our three wonderful volunteers for your contributions to the Women’s
Group. We all appreciate your help and support.
New Initiatives in your region
Buddies Are Coming To Lower Hutt!
o For a number of years now, people have been asking for Buddies to come to Lower Hutt
and as we have been successful in securing a contract with HVDHB, we are now able to
extend our service to the Hutt.
o We will be providing peer support at the inpatient unit Te Whare Ahuru, and are delighted
some of the current and past Buddies living in the Hutt Valley will be joining us there. We
are also looking for new Buddies for Lower Hutt, so if you are keen to volunteer or know
someone who is, let us know as soon as you can!
o For those who meet our volunteer requirements, training will be held late November in
Lower Hutt. We have already interviewed a few people and are looking for some more—
that could be you! We are looking for peers who are far enough along in their own
recovery and are willing to give some of their time for a visit each week or once a fortnight.
We are really looking forward to getting to know the team at TWA and plan to start with 2
visits each week and increase these as we increase our volunteer team capacity.
o We already sprang into action with the set up phase from 1 September, and this has
included the training and induction of the new coordinator (read more about Candice on
the next page). She is amazing and has already hit the ground running and finished the
Buddies Induction training this week.
o For Wellington, we were also be busy recruiting and training new Buddies for Te Whare o
Matairangi (TWOM), who will be ready to start ward visits soon—they are an awesome
bunch of people and we look forward to them being a par
59
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Training and Development Opportunities for Buddies
o Buddies give so freely of their time and energy and it takes great courage to share their
personal stories. They are the face of our service and we acknowledge the importance of
the work they do. It is only natural that we want to support them to be the best they can
be.
o New Buddies all go through 4 days of intensive training, spread out over 2 weeks and we
under the Official Information Act 1982
cover a wide range of topics including recovery concepts, communication, listening and
feedback, diversity and stereotypes, as well as discrimination and stigma. We also cover
the operational side of the service, what it is like to be a Buddy, stress and self-care.
Confidentiality and professionalism are also on the training agenda.
o To support Buddies with their ongoing development, training is provided once a month as
part of their team meeting. This generally covers topics the Buddies are interested, in as
well as networking and visits from other local service providers.
o In addition to the main support we provide for Buddies like pastoral care and supervision,
we have been exploring how we can add value to the Buddies by offering a wider range of
training and development opportunities. This is optional for those who wish to develop
their skills further in different areas relating to Peer Support, as well as building on work
skills for those who want to return to the paid workforce.
o New Buddies volunteer alongside experienced ones for up to 6 months to ensure they are
confident in providing peer support on the ward and “know the ropes” of how we do
things. At this point they are then “Graduated” and are able to visit the ward with other
new Buddies. Regardless of being new or experienced, our Buddies always visit in pairs and
keep each other in line of sight.
o One of our new initiatives has been a 3 part introduction to mentoring training for the
experienced Buddies who want to take on a mentoring role for new Buddies. This
programme is still being reviewed and further developed and builds on the induction
training the Buddies receive. It is optional for Buddies to attend as they do not have to take
on a formal mentoring role for new Buddies, however we would like the training to be
beneficial for all Buddies and build on their skills and knowledge.
o For new Buddies, being able to volunteer alongside a more experienced Buddy is a valuable
experience for both, so we look forward to how this evolves over the coming months, and
will be inviting the current Buddies who would like to be involved, to collaborate and
contribute to the revision and further development of the training.
60
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
o We have other ideas too and are keen to hear what other training and development
opportunities Buddies would like. We have talked about how being a Buddy has been a
pathway to employment for some and this is an area we are also keen to support for those
who wish to pursue it.
BUDDIES I Peer Support Service I Level 6, Education House I 178 Willis Street I WELLINGTON
(04) 384 3303 I [email address] I www.kites.org.nz
under the Official Information Act 1982
New Initiatives /Developments in your region
Oasis
• Kuranui Marae has started a kaupapa Maori group called Bereaved by Suicide that is based
on the training delivered by Skylight Trust
• Hutt Valley Day Service is now operated by Pathways after the closure of the HVDHB day
hospital. It is a very limited budget and not many resources; it is only a short term service.
CATT
• Crisis Assessment and Treatment team in Wellington (CATT) is undergoing a restructure. In
the future it will be Crisis Resolution Service – CRS.
• The CATT restructure plan is for it to be more proactive and less reactive. Less assessment.
Staff will aim to see people where they are rather than expecting them to get to a clinical
center. Staff will be closer to places like Police station, ED, more GP practices. The service
will be available in the CCDHB and Hutt Valley DHB areas. It may be up and running by 1st
November 2016, providing some of the issues holding it up are resolved.
Homeless Women’s Shelter
• There is a new service in Wellington
• It is for women alone (no children)
• There has been a Homeless Men’s shelter in Wellington for many years and this new
service is long overdue.
• There is to be a fundraiser and awareness-raising event. It’s the 14 hours homeless
campaign. People will be sleeping in cars, boxes, on couches in Wellington on the 7th of
October
Mosaic
• Mosaic, is a new support group for male survivors of sexual abuse. There are also Men’s
Sheds.
• There are issues with the Porirua Council around not supporting initiatives in their city.
61
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
• There is currently a need for more anger management services.
Col aborating with DPA
Central reps have begun a new relationship with DPA which is centered in Wellington. Attached is
the Disability Strategy submission that was submitted by DPA. We will be spending time regularly
as this relationship matures.
Addictions
under the Official Information Act 1982
Oasis Network
• There is no Peer addiction support or recovery group in the Hutt.
• AOD services in Hutt include: Welltrust, Care NZ
• Problem is knowing what exists, how to access it and being able to afford it (e.g. transport)
• Alcohol is a depressant and the use of illegal drugs is not helpful but the group would like
more wellness information and information about harm reduction.
• Also education regarding the interaction between medications and street drugs.
• Before people can get into rehab they have to have been abstinent for 2 weeks. It was
stated that if you could be abstinent for two weeks on your own then why would you need
rehab? This requirement also makes it impossible for many people to access rehab that
otherwise would.
• Detox is mainly done in people’s homes or in police cells. Home detox is okay but hospital
would be the best.
• The Smoke free work is creating stigma and discrimination for smokers. Mental health
services “should not back smoke free. They should back wellness and some people need to
smoke to be well.”
Whanau/family services
DHB Family and Whanau Advisors:
Co-Chair Leigh Murray
DHB Family Whānau Advisors continue to provide guidance on working with families and whānau
to mental health and addiction workforce via Handover nursing newsletter & Te Pou website.
Latest article is ‘Moving from Individuation of risk to a shared safety agenda’ written by DFWA co-
chair Leigh Murray.
http://www.tepou.co.nz/news/moving-from-individualisation-of-risk-to-a-
shared-safety-agenda/810
• Family Whānau Advisors are looking forward to their annual national meeting Nov 3-4 in
Formatted: Line spacing: Multiple 1.15 li
Christchurch. This is a great opportunity to feed into & be updated about key projects as
well as share best practice ideas ‘kanohi te kanohi’. There is a full agenda with all 4
62
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
workforce centres, MH Foundation, MoH & HDC Mental Health Commissioner taking up
slots. Unfortunately some of our key family advisors won’t be there due to travel
restrictions currently in place for some DHBs. We are hoping to link them in via video
conference.
• DFWA recognises there is probably not a widespread understanding/appreciation of the
systemic advocacy family whanau advisor role across NZ. This may be a contributing factor
to family advisor vacancies that are of several years duration in a few DHBs. We appreciate
that this might also be the case for some consumer advisor positions. Currently there are
under the Official Information Act 1982
22 family advisors in post which equates to 17.87 FTEs nationally.
• We also note that the importance of family, whānau perspective and participation is
increasingly mentioned in MH & addictions though this does not always seem to translate
into tangible ways of ensuring that the whanau voice is present or included.
• To end on a positive note DHB Family Whānau Advisors contributed significantly to the
successful TheMHS pre-conference family & whānau forum held in Auckland on August
23rd with 65 attendees. At the start of the day we demonstrated our commitment to the
theme of ‘Building Authentic Relationships’ with our own whānau by presenting the
consumer forum delegates with the gift of a peace lily, a fun fruit face & chocolate with
good wishes for an inspirational, fun and learning day.
Atareira Family Whanau Services Wellington
• Atareira provides a multidisciplinary team: whanau/family workers; counselling
• Atareira has a COPMIA worker and support group.
• Atareira was formerly SF in this region.
• Oasis Network is going to offer a family / whanau workshop in December. We hear very
good feedback about Atareira family/whanau workers.
Child Youth and Family Reports are that they discriminate early with people with experience of mental distress. This
means they assume because of the people’s history that they are not able to give birth and parent
their children so the babies are being taken off people who just need good ongoing support. Then
the parents are not given any support or education once their children have been taken from
them
Maori services
More Maori than ever are visiting and returning to Oasis Network which they are really happy to
see.
Wellington Community Law just launched ‘
Ngā Rerenga o Te Tiriti, a new resource for community
organisations changing and engaging with the Treaty of Waitangi. Highly recommended.
63
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Kuranui Marae (Hutt Val ey) has started a kaupapa Maori group called Bereaved by Suicide that is
based on the training delivered by Skylight Trust but focuses on tikanga.
Te Paepae Arahi
•
Te Paepae Arahi in the Upper Hutt is a kaupapa Maori service that supports a multidisciplinary
Formatted: Font: (Default) +Body (Calibri)
practice.
Formatted: Normal, Space After: 0 pt, Line spacing: single,
•
No bullets or numbering
They have a social worker, counsellor, a regular visiting GP and operate a peer support
under the Official Information Act 1982
64
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health

Released
under the Official Information Act 1982
Members: Julie Witla and Grant Cooper
Region: Southern
Meeting: 7/8 September 2016 3 /4 November 2016
1. Issues/chal enges identified by people in your region
Carron Cossens – Waitaki:
Issue exists around finding support for people traumatised by attempts to rescue another person:
doesn’t really fall under ACC descriptors as far as I can identify. This is particularly important when
the rescue is unsuccessful- flashbacks, recriminations etc. Risk of Post-Traumatic Stress Disorder
(PTSD) if not dealt with in early stages
Issue that more and more health pamphlets are now no longer in print- people are referred to
websites for material. Government initiative that I think is short-sighted
Lisa Perniskie, Peer Support, Mirror HQ, Ōtepoti
Kia ora Koutou
For those of you who do not know me
Ko wai au
Ko Hereweka te maunga
Ko Rees te awa
Ko Kotimana te iwi
Ko Airihi te hapu
Ko Perniskie rātau, ko Gray, ko Bartlett, ko Munro nga ingoa ōu tipuna
Ko Felix te pāpā, ko Isla te whaea
Ko David toku hoa rangatira
65
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Ko Hollie taku tamahine
Ko Sam raua ko Jasper aku tama
No Ōtepoti au.
Kei te Kaiawhina taku mahi
No reira,
under the Official Information Act 1982
Nga mihi mahana ki a koutou
Tēna koutou, Tēna koutou, Tēna koutou katōa
I work with taiohi (youth) with co-existing issues.
Our age group is from 12-22 years.
We offer a multi-disciplinary team including a whanau therapist, myself, a psychiatrist and all
clinicians are CEP trained. One of the issues the young people I work with is finding suitable
housing at an affordable house. I do a lot of advocacy with our youth so they are not taken
advantage by landlords and property managers.
Adequate resourcing for youth as our service now has a waiting list.
Addressing stigma relating to young people with addiction issues
Grant Cooper –Otago
Issues still arise with the wait time at Emergency Psychiatric Services. Staffing levels seem to be a
significant issue.
Access to talking therapies is an ongoing issue with waiting times of concern.
A number of people are concerned about the level of medication and the length of time they are
on it. Feedback includes feeling “numbed” and not been able to feel the emotions he once did as
well as memory issues for example not being able to remember the chords on his guitar.
Issue for some people of the cost of challenging the mental health system for example getting a
lawyer as well as the length of time complaints can be worked through.
Feedback from peers is that the Raise Hope Mental Health Strategic Plan rollout has been dragging
on for a long time.
Brief Intervention Counsel ing
A person with complex issues has been told that they cannot access the free Brief Intervention
Counselling more than once a year by their GP.
66
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Housing in the community
People who have identified with mental health issues who were placed in Housing New Zealand
(HNZ) or city council housing during the earthquakes have been seeking housing transfers or have
been evicted due to not fit for purpose housing.
There has been a noticeable increase of people accessing the drop in at MHAPS which is open at
the weekend due to housing difficulties.
under the Official Information Act 1982
Outcomes identified by people with mental health and addiction needs are:
• Homelessness with debts for storage to HNZ for new WINZ issued washing machines and
fridges.
• Families living in cramped conditions with inadequate number of bedrooms in huge
complexes with limited outdoor space for their children.
• Complexes are busy and for some people the stress of the noise, people coming and going
has not been suitable for people with mental health issues.
• “
I called the police because after weeks of abuse, intimidation such as him putting security
cameras pointed on my property I”
•
“ The police said I can’t get a protection order as I live at a HNZ home and I feel my housing
manager is out of her depth with facilitating a solution”
• Physical health needs were not considered in my application “
Although I have a flat from
CCC, My flat is damp and I have to wipe condensation off the windows every day, I am
awaiting a lung transplant and have been hospitalised five times in the last two years and
still there is no word from the city council”
•
My HNZ flat is nice but I have low vision eyesight problems and the stairs are not safe. My
housing manager said they have done everything they can to make them safe but wil not
fill in the stairs or transfer me to a suitable unit.
Work and Income expectations of on-line applications
The WINZ Linwood office in Christchurch no longer has paper applications for benefits and you
have to ask the manger for an application. The expectation is to complete applications on line. It
causes delays in people receiving benefit entitlement in a timely manner.
The advocates in Christchurch have found there are still many people with addiction/mental
health issues who do not have email addresses, internet and internet devices, data on their mobile
phones.
• Still a concern over the high number of people under the Mental Health Act. A concern that
is expressed nationally as well
67
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Carron Cossens – Co-ordinator – Peer Support Group Oamaru
• A developing concern for us is service provision for Palmerston South. Currently Brief
Intervention service is only provided out of Dunedin. We don’t think this is adequate, and
have asked for the service to be resumed based in Palmerston.
• An ongoing concern is support for children impacted by a suicide death. Child services in
Dunedin will only respond if a mental health issue is apparent and my argument is that
careful management post incident following the death will prevent mental health issues
from developing later in life.
under the Official Information Act 1982
• We continue to need a peer support worker based in Oamaru/Waitaki
Sharon Gutsel – Consumer Advisor – PACT Southland
• Lack of peer support and peer advocacy services in Invercargill and Southland.
No training opportunities in Peer Support.
Housing for people with mental health issue
Julie Whitla - Christchurch
At the moment there is no single person accommodation available in Christchurch. There are a
number of people in the acute wards who could leave if there was a place to go.
Purapura Whetu is now partnering with Comcare for family housing.
Acute Wards
• Occupancy (midnight census) of the adult acute inpatient service has remained at 93% for a
second consecutive month. There were 17 sleepovers required in July 2016.
• We are exceeding Ministry of Health targets with respect to wait times for adult services. The
targets are 80% of people seen within 21 days and 95% within 56 days. 97.4% of people referred
to the Adult Community Service were seen within 21 days, and 100% seen within 56 days for July
2016. The percentages are 92.9% and 98.8% respectively when other adult services i.e. Specialty,
Rehabilitation and Forensic are included.
Best Practice according people in your region.
Lisa Perniskie, Peer Support, Mirror HQ, Ōtepoti
Within my team I have been working on how to collaborate and spent time recently on developing
a process for our internal referrals to my role.
With our taiohi it works well to have a mihi whakatau process with myself, taiohi and the clinician
to clarify for them what support I can offer and what the clinician will be working with. The taiohi
is given the opportunity to discuss what they would like support with.
68
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
It is very isolating for me being in Dunedin as there are very few peer support workers here. I have
had a lot of support from Otago Mental Health Support Trust (OHMST) and would like to thank
Grant for his ongoing support of my role.
I would like to participate more in best practise within the southern area and find out more about
what is happening in our area- Te Wai Pounamu.
Julie Whitla - Christchurch
Canterbury District Health Board Specialist Mental Health Services September 2016 (SMHS)
under the Official Information Act 1982
Occupancy of the adult acute inpatient service decreased from 95% in August 2016 to 91% in
September 2016. There were 32 sleepovers required in September 2016, of which 29 were for
patients waiting to be formally admitted to the Seager Inpatient Rehabilitation Unit of (a recovery
based programme to enable people with mental health issues to live in the community), or Tipuna
units (24 hour care and support in a home-like environment with the aim of assisting people who
have ongoing mental health issues to work towards finding a suitable place to live in the
community).
STAFF RECRUITMENT
The CDHB are also experiencing challenges recruiting Specialist Medical Officers into mental
health. There are a number of vacancies and locums across Specialist mental Health services.
Recruitment into Crisis Resolution is currently challenging putting additional pressure on an
already busy team.
CRISIS RESOLUTION SERVICE
Demand for Crisis Resolution remains steady. There was a slight decrease from 219 new crisis case
starts in August 2016 to 196 in September 2016. New crisis case starts require an assessment
within a day of referral.
SECLUSION
A total of 126.8hours.
69
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
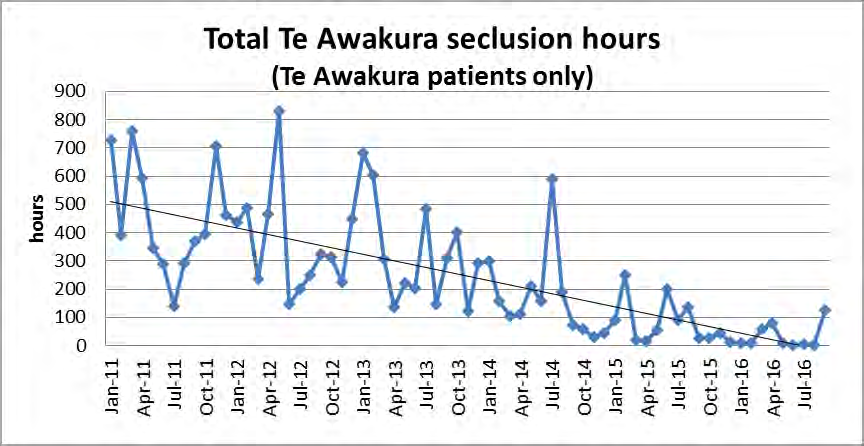
Released
under the Official Information Act 1982
Acute Inpatient House Emergency Solution Labour Weekend
Over labour weekend there were
more people needing beds than were available at Hillmorton
Hospital at the inpatients unit.
A respite house was made available by Stepping Stones Trust and
6-8 people were cared for in the community instead of the hospital with a Registered nurse. The
people were close to discharge or were on day leave were moved to the house, with support of a
RN. The initiative was a step down approach back to the community in a more homely
environment. Another respite provider Pathways took the people who were getting respite.
Acute Inpatient House Emergency Solution Labour Weekend
Over labour weekend there were
more people needing beds than were available at Hillmorton
Hospital at the inpatients unit.
A respite house was made available by Stepping Stones Trust and
6-8 people were cared for in the community instead of the hospital with a Registered nurse. The
people were close to discharge or were on day leave were moved to the house, with support of a
RN. The initiative was a step down approach back to the community in a more homely
environment. Another respite provider Pathways took the people who were getting respite.
Brief Intervention Counsel ing
A person with complex issues has been told that they cannot access the free Brief Intervention
Counselling more than once a year by their GP.
Housing in the community
People who have identified with mental health issues who were placed in HNZ or city council
housing during the earthquakes have been seeking housing transfers or have been evicted due to
not fit for purpose housing.
70
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
There has been a noticeable increase of people accessing the drop in at MHAPS which is open at
the weekend due to housing difficulties.
Outcomes identified by people with mental health and addiction needs are:
• Homelessness with debts for storage to HNZ for new WINZ issued washing machines and
fridges.
• Families living in cramped conditions with inadequate number of bedrooms in huge
complexes with limited outdoor space for their children.
under the Official Information Act 1982
• Complexes are busy and for some people the stress of the noise, people coming and going
has not been suitable for people with mental health issues.
• “
I called the police because after weeks of abuse, intimidation such as him putting security
cameras pointed on my property I”
•
“ The police said I can’t get a protection order as I live at a HNZ home and I feel my housing
manager is out of her depth with facilitating a solution”
• Physical health needs were not considered in my application “
Although I have a flat from
CCC, My flat is damp and I have to wipe condensation off the windows every day, I am
awaiting a lung transplant and have been hospitalised five times in the last two years and
still there is no word from the city council”
•
My HNZ flat is nice but I have low vision eyesight problems and the stairs are not safe. My
housing manager said they have done everything they can to make them safe but wil not
fill in the stairs or transfer me to a suitable unit.
Work and Income expectations of on line applications
The WINZ Linwood office in Christchurch no longer has paper applications for benefits and you
have to ask the manger for an application. The expectation is to complete applications on line. It
causes delays in people receiving benefit entitlement in a timely manner.
The advocates in Christchurch have found there are still many people with addiction/mental
health issues do not have email addresses, internet and internet devices, data on their mobile
phones.
2. Best Practice according to people in your region
From Sharon Gutsell – Consumer Advisor PACT Southland
• Working on a new referral protocol for people to receive community support services
without the need for a needs assessment, removing this barrier to people receiving
support services.
• Consumer Advisor has been appointed for Pact Southland, whose responsibilities include
individual and systemic advocacy, and peer support.
71
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
• Extending “Giving Tuesday” (community art event held at Southland Museum and Art
Gallery for Mental Health Awareness Week); to a full day programme building on the
success of last year’s event.
•
Carron Cossens – Waitaki:
• The Men’s Wolfpack support group are setting up headquarters as a drop in centre in
Oamaru. They are currently doing renovations.
under the Official Information Act 1982
• Youth line Otago is now established in the Waitaki.
Acute Wards in Christchurch:
• Occupancy (midnight census) of the adult acute inpatient service has remained at 93% for a
second consecutive month. There were 17 sleepovers required in July 2016.
• We are exceeding Ministry of Health targets with respect to wait times for adult services. The
targets are 80% of people seen within 21 days and 95% within 56 days. 97.4% of people referred
to the Adult Community Service were seen within 21 days, and 100% seen within 56 days for July
2016. The percentages are 92.9% and 98.8% respectively when other adult services i.e. Specialty,
Rehabilitation and Forensic are included.
From Grant Cooper –Otago
• Raise Hope SDHB Strategic Plan is still in development. A lot of behind the scenes work is
going on and hopefully some concrete proposals will be able to be released for wider
release.
From Carron Cossens – Co-ordinator – Peer Support Group Oamaru
• The Wolfpack (Men’s mental health peer support group) are looking at finding premises so
they can meet with those needing support every evening. Funding is an issue with this of
course. They are now a charitable trust.
• The Men’s Wolfpack support group are setting up headquarters as a drop in centre in
Oamaru. They are currently doing renovations.
• Youth line Otago is now established in the Waitaki.
• Artsenta 9mental health art group) are re-establishing in Oamaru on a monthly basis for
ten people at a time. I hope to have secured funding for room rental through the Waitaki
District Council but won’t know for a while.
72
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Seclusion
Julie Witla Christchurch
Our focus on reduction of seclusion in Te Awakura (acute inpatient service) continues. Two
consumers experienced seclusion during July 2016 for a total of 6.75 hours. There is strong and
effective nursing leadership and staff dedication and commitment to maintain the focus of
reduction.
under the Official Information Act 1982
There was discussion around the steeply dropping seclusion rate – this has decreased from 800
hours in April 2012 to 1 hour in the last month commendations to the CDHB for doing this.
Awareness was thanked for helping instigate this focus on seclusion reduction and elimination. It
was mentioned the DHB is talking much more about seclusion elimination now, rather than just
reduction. There is much more of a focus on upskilling staff to be able to provide talking therapies,
not just assessment.
Mental health staff are also being supported to upskill around supporting people with alcohol or
drug problems as well as mental illness. In June there was only
one hour of seclusion recorded in
the acute wards. Though rates are going up in other parts of the country, likely as a back lash from
some bad media and incidents, the efforts of staff in Canterbury have been excellent. There is
anxiety among staff over changes in policy and the increase in assaults on staff. Some feel they are
at risk but are still de-escalating patients. (This may be what is reflected in unpleasant anonymous
comments that follow media articles.)
Individualised Funding TRENDS
Discussion about viability of increasing number of IFA requests (from a cost perspective), which
must be balanced with right of individuals to live in the community (in so far as possible).
Agreed that Planning and Funding team will draft a discussion/analysis paper covering the issues,
options etc and circulate for further consideration.
Stigma and Discrimination
A recent literature review prepared by CDHB, Commmunity and Public Health –
Impacting stigma-
related inequalities among those who have been diagnosed with a mental il ness , particualrly from
within maori, pacific and CALD populations.
The main research question was:
what policies, interventions or programmes work to reduce
stigma/self-stigma amongst those who have been diagnosed with a mental il ness? The
importance being that self-stigma can negatively impact on health i.e. barrier to seeking
treatment, poorer health outcomes expected and the “why try” effect contributes to ongoing
diability/social withdrawal.
73
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Key findings included:
there are 3 types of stigma: stuctural, public and self;
mental illness stigma varies accross cultures – stigma does
not operate in a similar way for
everyone;
in the study period maori and pacific people had a higher prevalence of disorder/serious
disorder but were less likley to seek treatment;
reasons for not seeking treatment included racism and stigma;
there are 3 types of racism: institutionalised; interpersonal and internalised; and there are
under the Official Information Act 1982
parallels with the 3 types of stigma;
maori, pacific and people from asian communities were more likely to access culturally
specific health initiatives;
culturally appropriate health frameworks can reduce inequality;
reducing stigma needs a “whole of system” approach;
reducing stigma should be focused for different population groups, reflecting diversity of
needs;
reducing stigma needs to be tackled from a policy level;
psychological first aid may help in reducing stigma;
cultural responsiveness should be improved by incorporating cultural competency training
at a structural level;
self-stigma programmes should be delivered by relevant providers e.g. kaupapa maori
providers for maori populations;
KPI’s for programmes should be orientated at achieveing equity; and
evaluation should be built in to programmes.
The aim of the report/findings is to support/inform mental health providers to reduce self-stigma
in priority populations, to inform initiatives and policies etc.
Lisa Perniskie, Peer Support, Mirror HQ, Ōtepoti
I have been in discussion with Sue Paton from DAPAANZ and some peer support workers from
Auckland and Christchurch. DAPAANZ is the membership association representing the professional
interests of practitioners working in addiction treatment.
There are some new categories being discussed for the Peer Support role with the DAPAANZ
organisation
Grant Cooper Otago
Mental Health Awareness Week initiatives in Dunedin with a number of events. The largest was a
picnic in the Octagon in Dunedin with over 200 people with more than 15 community and mental
health providers with interactive displays and activities including yoga, tai chi and mindfulness
Julie Whitla - Christchurch:
Acute Wards
74
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
• Occupancy (midnight census) of the adult acute inpatient service has remained at 93% for a
second consecutive month. There were 17 sleepovers required in July 2016.
• Canterbury are exceeding Ministry of Health targets with respect to wait times for adult services.
The targets are 80% of people seen within 21 days and 95% within 56 days. 97.4% of people
referred to the Adult Community Service were seen within 21 days, and 100% seen within 56 days
for July 2016. The percentages are 92.9% and 98.8% respectively when other adult services i.e.
Specialty, Rehabilitation and Forensic are included.
Seclusion
under the Official Information Act 1982
The CDHB focus on reduction of seclusion in Te Awakura (acute inpatient service) continues. Two
consumers experienced seclusion during July 2016 for a total of 6.75 hours. There is strong and
effective nursing leadership and staff dedication and commitment to maintain the focus of
reduction.
There was discussion around the steeply dropping seclusion rate – this has decreased from 800
hours in April 2012 to 1 hour in the last month commendations to the CDHB for doing this.
Awareness (Canterbury Consumer action Group on Mental Health and Addiction) are to be
thanked for helping instigate this focus on seclusion reduction and elimination. Debbie Selwood
mentioned the DHB is talking much more about seclusion elimination now, rather than just
reduction. There is much more of a focus on upskilling staff to be able to provide talking therapies,
not just assessment. Mental health staff are also being supported to upskill around supporting
people with alcohol or drug problems as well as mental illness. In June there was only
one hour of
seclusion recorded in the acute wards. Though rates are going up in other parts of the country,
likely as a back lash from some bad media and incidents, the efforts of staff in Canterbury have
been excellent. There is anxiety among staff over changes in policy and the increase in assaults on
staff. Some feel they are at risk but are still de-escalating patients.
From Sharon Gutsell – Consumer Advisor PACT Southland
Working on a new referral protocol for people to receive community support services without the
need for a needs assessment, removing this barrier to people receiving support services.
Lisa Perniskie, Peer Support, Mirror HQ, Ōtepoti
Within my team I have been working on how to collaborate and spent time recently on developing
a process for our internal referrals to my role.
With our taiohi it works well to have a mihi whakatau process with myself, taiohi and the clinician
to clarify for them what support I can offer and what the clinician will be working with. The taiohi
is given the opportunity to discuss what they would like support with.
It is very isolating for myself being in Dunedin as there are very few peer support workers here. I
have had a lot of support from OHMST and would like to thank Grant for his ongoing support of
my role.
75
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
I would like to participate more in best practise within the southern area and find out more about
what is happening in our area- Te Wai Pounamu.
3. New Initiatives /Developments in your region
Psychosocial Committee
Julie Whitla Christchurch
under the Official Information Act 1982
There was an update on the work of the Psychosocial Committee, led by CDHB for 9 months now
(previously CERA):
The committee meets monthly and meetings continue to be well attended
The committee are responsible for the shared programme of action (
SPOA)
SPOA is comprised approx. 90 services working together to achieve the shared goal of recovery in
Canterbury.
Two thirds of the services are engaged and committed to working together. A review of SPOA is
underway and will be completed by 2017. The intention is that future iterations of SPOA will be
split between services for recovery (past) and reactive services (future).
The committee are working with MBIE (and other relevenat agencies) around what services are
still required for the 6500 households with outstanding EQC claims. Emphasised that there are
other vulnerable people that may require ongoing assistance e.g. households who have cash
settled and are managing complex/stressful rebuilds by themself and/or managing re-repairs due
to defective EQC works. Both of the latter groups are still under stress capable of affecting
wellbeing/mental health.
It was noted that as well as a wind down of some services that the funding environement is
changing: Red Cross funded social workers in schools funding has ended; it’s unclear what the
$1million allocation to CCC (from additional mh funding) will be used for; and likewise MSD
residual funding (approx $800K). It is hoped that the CCC and MSD funding will be targeted at high
need groups e.g. people with disabilities; people with outstanding EQC claims and people with
health conditions.
A recent evaluation of All Right? found that:
75% of people were aware of All Right? (compared to 49% awareness of
Push Play the
most visible/expensive public health campaign)
83% said it was valuable
71% had a greater awareness of taking care of self
75% had a greater awareness of taking care of others
74% had done something different as a result of the campaign
76
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
On the whole, the signs are that population wellbeing measures are rising. The WHO – 5 score has
risen from 15.4 (in 2013) to 16.2 (2016). At the next meeting Lucy will provide an update on the
latest reuslts from the Canterbury wellbeing survey, which will have been published by then.
PRIMARY HEALTH
Work is commencing with the primary mental health providers to consider where the
opportunities are to increase responsiveness to the community and provide more support for
General Practice to manage people with complex issues.
under the Official Information Act 1982
Meetings are being held with groups of providers to illustrate how their routine reporting can be
collated to provide useful data for system planning. This is generating useful discussions about the
development of KPIs that reflect local priorities and add context to national reporting.
Primary Mental Health Discussion Paper
Background
Primary Mental Health Services (PMH) are a highly valued and an essential part of the Canterbury
mental health system. The clinical work force is highly skilled in delivering services to those with
mild to moderate mental health and AOD conditions. PMH Services are provided by the,
Christchurch, Rural Canterbury and Pegasus PHO’s.
Current Primary Mental Health Service
Role
Brief Description
Resource
Brief
Intervention BIC offer up to 5 counselling sessions for people
23.16 FTE
Counselling/Co-ordination
with mild to moderate mental health and AOD
(BIC)
issues referred from their General Practice.
In addition to the 3 main PHO providers St John
of God Waipuna have 1.75 FTE specifically for
youth BIC in Primary Mental Health
General Practice Liaison
GPL are to provide clinical interventions and
5.2 FTE
supports for those with enduring mental illness
but no longer require specialist services or
those who have a more serious episode of
mental illness but it is deemed appropriate to
manage their needs within Primary Care
Intensive General Practice While these new roles will increase the capacity
8 FTE
Liaison (IGPL)
in PMH of the standard GPL role, it is expected
that this role will include a range of different
Being recruited at the time
77
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
of writing this paper
interventions such as group work, family work,
support for those post a suicide and strengthen
the integration with Specialist services
Senior Clinical
Provides clinical supervision to staff and clinical
2 FTE
expertise required to deliver services that meet
best practise requirements
Extended Consultations
Allows for double the time for the General
5919
under the Official Information Act 1982
Practitioner to spend with an individual who is
sessions
presenting with a mental health /AOD issue
per annum
Brief Summary of Current Model of Service Delivery
Each of the PMH teams receive referrals from the PHOs affiliated General Practices with the
exception of 5 Practices who transferred from Rural PHO to Pegasus in July 2014, for those
Practices RCPHO continue to provide the PMH services.
Each PMH team has a Senior Mental Health Clinician to triage the referrals and allocate
appointments based on urgency and availability of staff. Prior to the allocation of the additional 8
FTE IGPL roles, eighty percent of the FTE’s in PMH are BIC workers, who deliver up to 5 sessions of
brief intervention counselling sessions to patients. Brief Intervention Counselling is provided to
youth and adults
GPL provide support and education to General Practice Teams and also work with mental health
consumers who require episodic and on-going monitoring and support for those with more severe
and enduring mental illness. In RCPHO and CHPHO the GPL role is delivered by a clinician
employed specifically for the GPL role. In Pegasus PHO the GPL role is part of the BIC role, rather
than a separate FTE.
IGPL is a new role which is envisaged to expand the GPL role to include family and group work,
more capacity to work with those with enduring mental illness and to include working with youth.
The role is specified and is not to be used to expand BIC capacity.
The General Practice is the ‘health home’ for the mental health consumer and as such when
discharged from the PMH service, the General Practice team receives a summary of the
engagement with the service. While there is some variation for individual circumstances and
between PMH teams, consumers are given information on other services available for on-going
support or when assessment with Specialist services is required this will occur via the General
Practice.
Service Performance
Data is taken from the quarterly reporting from the 3 PHOs.
78
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Total referrals for Brief Intervention Counselling (BIC) combined for 3 PMH services are on average
between 750 and 900 referrals per month.
BIC services worked with 1,000 12-19 year olds in 2014/15 and 7,505 adults aged between 20 and
64 years.
This reduced in 2015/16 to 444 12 – 19 year olds in 2015/16 and 5,509 adults aged between 20
and 64 years.
under the Official Information Act 1982
There is no information provided for the 2,000 per annum plus referrals not seen in BIC services.
Average number of BIC sessions per individual is 3 sessions. This is unchanged despite reports
from PMH teams that this has increased with the number of people needing interventions for
their complex needs.
There is no discharge information as providers refer back to the General Practice and there is
inconsistent reporting on the numbers referred onto Specialist Mental Health.
While no clear conclusions can be drawn, the data in Table 1 and 2 has been obtained by cross
checking SMHS and Primary Care reporting for 2015/16.
Table 1:
2015/16
Count of SMHS NHI also seen by Prim ary M H Teams
Count of NHI By
Age
2015/16
Group
Grand
Ethnicity
0-19
20-64
65+
Total
Maori
37
144
2
183
Other
226
897
97
1220
Pacific
1
17
1
19
Grand Total
264
1058
100
1422
79
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Table 2:
% of SMHS NHI also seen by Primary Mental Health
Teams
Grand
Ethnicity
0-19
20-64
65+
Total
Maori
4.51%
9.07%
3.28%
7.41%
under the Official Information Act 1982
Other
7.55%
11.65%
4.21%
9.39%
Pacific
1.04%
7.76%
3.85%
5.57%
Grand Total
6.75%
11.13%
4.18%
8.99%
There is i
nconsisten
t reporting for the GPL role therefore it is not reported here.
Extended Consults
Yr 2014/15
5,834
Yr 2015/16
4,947
Where some of the opportunities might lie?
• PMH services provide services to those who have mild to moderate mental health
conditions. While these people make up the majority of people seen, in reality PMH
services work with people who are experiencing psychosocial distress through to those
with severe and enduring mental illness. Are we seeing the right people? Are services
configured in a way that meets peoples’ needs? Are there barriers for people getting the
services they need in a primary care setting?
• New ways of working adopted in the NGO sector and SMHS, such as the youth
collaborative provided by 3 NGO’s for those with mild to moderate mental health
conditions and centralised referral points, needs to be considered for their applicability to
PMH.
• Could the Service model be adapted so that there was direct flow of information from PMH
to NGO and SMHS e.g. does the referral pathway and discharge processes lead to an
integrated system? How could IT systems support this?
• Over the last 5 years an increasing number of Mental Health NGO services have accepted
referrals from General Practice. The majority of these services are non-clinical and they rely
on the General Practice for their clinical support when working with a consumer referred
from General Practice. How could PMH increase their involvement with mutual consumers
in the NGO sector?
80
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
• How can PMH, work together to provide packages of care, group work, etc. in collaboration
with and for other parts of the system.
• The additional 8 IGPL FTE from MOH, BIC 3 FTE from Red Cross and MSD and Community
Connector are all time limited agreements from between 12 -36 months. Without this
resource services across the mental health sector are at capacity. Looking to 3 years ahead,
are we making the best use of the resources we have?
• Are there opportunities to move work to other parts of the health and social service
system e.g. telephone consults, e-therapies, MSD services. Who decides?
under the Official Information Act 1982
• There is variation across the 3 PMH services, what needs to happen to provide equitable
services? Why aren’t more Maori accessing BIC services?
• PMH undertake Alcohol Brief Intervention Counselling, are we doing enough in Primary
Care for people with alcohol and other drug issues
Consumer Thoughts
Will the Intensive GPS be free?
Will there be adequate choice of Intensive GPS?
Seeing people in their homes is a great idea.
Crisis Service Resolution Service
Demand for the Crisis Resolution remains steady. In July 2016, there were 185 crises new case
starts. This was a slight decrease from the 215 new case starts in June. Crisis new case starts
require an assessment within a day of referral. In July 2016, 28 initial assessments occurred in the
consumer’s home.
Consumer Thoughts Below is a Consumer Satisfaction Report of Crisis Resolution services as the
Crisis has undergone a shift in model of care and its good practice to look at what people who are
using the service think of it.
Satisfaction with Crisis Resolution: Consumer, family and referrer perspectives
Project Information Sheet
Satisfaction with Crisis Resolution: Consumer, family and referrer perspectives
Name and address of service/department/organisation
Name: Clinical Research Unit, Specialist Mental Health Service, Canterbury District
Health Board
81
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Address: Terrace House, 4 Oxford Terrace, Christchurch 8011
Contact person
Name
Job Title
Email
under the Official Information Act 1982
Frances Carter
Clinical Psychologist/
[email address]
Scientific Officer
Address:
Terrace House, 4 Oxford Terrace, Christchurch 8011
Telephone:
03 3720400 extension 86440
Please tick the category you think best fits your project
Improved quality, safety and experience of care
Improved health and equity for all populations
Best value for public health system resources
(Please note Assessors make the final decision)
Full list of project investigators
Frances Carter (Clinical Psychologist (Scientific Officer, Senior Clinical Lecturer); Joan Taylor
(Clinical Liaison, Nurse Consultant); Steve Duffy (Consultant Psychiatrist); Robert Green
(Consultant Psychologist), Teresa Quigley (Consumer Advisor); John Beveridge (Nurse Consultant-
Informatics); and Maddie Weston (Interviewer).
ABSTRACT
Overview
In 2014, the ways that help was provided to people with urgent mental health needs in Canterbury
was changed. Prior to the present study, only anecdotal evidence existed about how people who
use the new Crisis Resolution services, experience them. Almost by definition, having an urgent
mental health need is a highly stressful time for consumers, family and potentially referrers. We
wanted to understand the perspectives of all of these key stakeholders.
Aim
82
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
The broad aim of the study was to evaluate the service satisfaction of consumers, their families
and referrers, for consecutive people discharged from Crisis Resolution over a five week period.
Goals and objectives
Specifically, the study sought to do the following:
• Evaluate
global satisfaction with Crisis Resolution;
• Evaluate satisfaction with
specific aspects of care that the service was striving to achieve
under the Official Information Act 1982
(e.g., ease of access, efficiency and effectiveness);
• Compare service satisfaction amongst different
demographic groups for consumers;
• Assess how participants think that the service could be
improved, and which aspects of the
service were especially
helpful or good.
The ultimate goal of the study was to improve Crisis Resolution for all key stakeholders.
Results
75 consecutive, eligible and consenting consumers, 22 family and 16 referrers completed
structured interviews. High levels of satisfaction were found amongst consumers, family and
referrers with Crisis Resolution for global satisfaction and most specific aspects of care. If
consumers were dissatisfied with care, they were more likely to be 25-34 years of age. Staff
manner and having effective treatment of sufficient duration were the most important issues
discussed by participants on open questions. A diverse range of specific suggestions were made by
participants.
Conclusions
High levels of satisfaction were found with Crisis Resolution. Staff manner and having effective
treatment of sufficient duration were the most important issues for participants.
INTRODUCTION AND BACKGROUND
What is the health care context in which this project occurred?
In 2014, the ways that help was provided to people with urgent mental health needs in Canterbury
was changed. The new model of care involved a Crisis Resolution function being built into the
existing four geographical mental health teams. The aim of the new model of care was to provide
care that was easy to access, efficiently delivered and highly integrated. For example, because
consumers were now dealing with the same team for different needs, it was hoped that meeting
new staff and undergoing unnecessary assessments would be minimised, and the transition
between outpatient and inpatient care would be improved. An emphasis was also placed on
trying to see consumers where they wanted to be seen, such as in their own home, where
feasible. Prior to the present project, only anecdotal evidence existed about how the people who
use Crisis Resolution, experience it.
83
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Why was it important to understand how people receiving help from Crisis Resolution,
experienced this? Who was it important to ask?
Almost by definition, needing help from Crisis Resolution is a highly stressful time for consumers
and their families. These situations may also be difficult for referrers, such as General
Practitioners, who are trying to organise urgent and appropriate help for people in crisis. Mental
health guidelines and commentaries note the importance of consumers having the best possible
experience of care [1], recognise that carers are vital partners in the provision of care [2], and
under the Official Information Act 1982
advise that Crisis Resolution services need to work closely with other care providers [3].
Surprisingly, no previous study has systematically evaluated the service satisfaction of all key
stakeholders (consumer, family and referrer) for the same case, when somebody has an urgent
mental health problem.
PLANNING
Aims
The broad aim of the study was to evaluate the service satisfaction of consumers, their families
and referrers, for consecutive people discharged from Crisis Resolution over a five week period.
Specifically, the study sought to do the following:
• Evaluate
global satisfaction with Crisis Resolution;
• Evaluate satisfaction with
specific aspects of care that the service was striving to achieve
(e.g., ease of access, efficiency and effectiveness);
• Compare service satisfaction amongst different
demographic groups for consumers;
• Assess how participants think that the service could be
improved, and which aspects of the
service were especially
helpful or good.
The ultimate goal of the study was to improve Crisis Resolution for all key stakeholders who use
the service.
Links to planning principles and service priorities
The project was consistent with the Canterbury DHB (CDHB) ideals for “our way of working” [4] as
follows:
• Understand and respond to the needs of populations;
• Make decisions based on where services are best provided, including “what is best for the
patient?” and
• Use information to plan and drive service improvement.
•
The project linked with the following SMHS priorities [5]:
• Crisis Resolution development;
• Collaborative care;
84
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
• Family safety and wellbeing, communicating with (listening to) family and supporting
family;
• Technical support with service improvement (evaluation); and
• NGO integration with SMHS (i.e., seeking General Practitioner’s views).
Team process
Originally a broad range of people expressed the view that it would be desirable to evaluate Crisis
under the Official Information Act 1982
Resolution, such as clinical staff, Consumer and Family Advisors and service management (SMHS).
Following an initial ‘expression of interest’ meeting involving around twenty people, a smaller
working group was formed consisting of people with the key skills, knowledge and experience
needed to undertake an evaluation (e.g., research skills, knowledge on the original goals of Crisis
Resolution, clinical expertise, data base expertise, and consumer advisory expertise). This working
group then critically examined which evaluation questions were important and which were
feasible to examine. We then agreed on roles and responsibilities for the project, identified key
tasks (e.g., obtaining funding, gaining ethical approval, employing and training the interviewer and
developing a recruitment plan) and established a timeline for completing these tasks.
Collaboration
This project was collaboration between SMHS and the University of Otago, Christchurch (UOC).
The latter provided funding via the Summer Studentship programme for an interviewer to be
employed for three months, support and advice regarding (research) data bases, statistical advice
and paid for the telephone calls that were made by the interviewer.
Sensitive issues identified in the planning phase
Privacy issues
We became aware that privacy concerns had the potential to jeopardise the project. In particular,
concern was expressed by the Research Committee (SMHS) about us contacting consumers to ask
them if they would like to participate in a service satisfaction survey. We spent a considerable
amount of time talking with the Complaints Officer at Hillmorton Hospital and the Office of the
Privacy Commissioner about how privacy issues could be managed. This input enabled us to come
up with a research design that the Research Committee (SMHS) and the University of Otago
Human Ethics Committee were satisfied with, and that was still valuable from a research
perspective. Specifically, we developed a study protocol that ensured that consumers had “no
surprises” about the study, and that they had multiple opportunities to indicate that they did not
wish to be contacted about the study. In addition, we recommended to management (SMHS) that
an addition be made to the Initial Treatment Information Form for all consumers, explaining the
integral nature of quality improvement in health care and clarifying that consumers may be
contacted for these purposes. This suggestion was accepted and implemented.
85
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Vulnerability
By definition, people with a “mental illness” are “vulnerable” according to the National Ethics
Committee Guidelines. Therefore, there is (appropriately) an even greater expectation on
researchers that the study question under investigation is important, and that the study is
carefully designed and implemented to ensure that no harm is done to anybody through
participation in the study. This consideration influenced our planning of the study in numerous
ways. For example, we only included consumers who had been recently
discharged from Crisis
under the Official Information Act 1982
Resolution (i.e., judged by their clinician to be well enough to be discharged). We also set up
systems so that we identified anybody who might have been put at risk or made worse through
participation in the study (e.g., people who may be put at risk of family violence if letters or phone
calls from the CDHB were intercepted, or people with delusions about being spied upon). The
Clinical Liaison (Joan Taylor) personally screened consumer notes and liaised with clinical staff
around this issue.
Avoiding unwanted communication following loss
Sadly, it seems likely that consumers who have recently had an urgent mental health problem (and
needed to use Crisis Resolution), are at increased risk of suicide. We were mindful of this, and
were keen to ensure that we did not inadvertently add to the distress of families in this situation
by sending letters to consumers who had deceased or phoning their homes. Therefore, we
enlisted the help of staff within SMHS who manage information of this nature, and set up a system
for them to inform the Clinical Liaison of situations where consumers who had used Crisis
Resolution were deceased.
Consultations
Conducting structured interviews
Professor John Horwood from the Christchurch Child Development Study (UOC) provided expert
advice on how to form questions for use in structured interviews. He recommended asking
participants to provide words as opposed to numbers, to keep the response options to a
minimum, and to use plain and simple language wherever possible (e.g., good/bad/ok).
Maori
We consulted with the CDHB Maori consultation committee regarding the project, and liaised with
Henare Te Karu (Pukenga Atawhai at Hillmorton Hospital) about how to ensure that the interview
process was accessible to Maori.
Crisis Resolution staff
We met with staff and outlined the purpose of the study, sought their ideas and addressed their
concerns. This was done on three occasions to ensure that staff from all geographical teams on a
range of shifts had the opportunity to participate.
86
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Training
The interviewer received comprehensive training on a range of issues including how to manage
potentially difficult scenarios with participants, and relevant protocols were developed.
Ethical approval
The study was approved by the University of Otago Human Ethics Committee.
IMPLEMENTATION (METHOD)
under the Official Information Act 1982
Participants
Consumers
Consecutive individuals discharged from Crisis Resolution (from any of the four geographical SMHS
teams) over a five week period (last week of October 2015 until the end of November 2015). For
participation in the study, consumers were required to meet the following criteria.
Inclusion criteria Individuals had been newly discharged from Crisis Resolution. Specifically, they
needed to meet the following criteria:
• Had face to face contact with Crisis Resolution within the previous six weeks;
• Discharged from being a Crisis Resolution ‘case’ within the past seven days. Individuals
were suitable for participation. Specifically, they needed to meet the following criteria:
• 18-65 years of age;
• Contact information available for participant (address and phone);
• Currently residing in New Zealand;
• Able to adequately participate in the structured telephone interview (e.g., sufficient
English language, adequate intelligence)
• Able to provide informed consent (e.g., not too unwell);
• Consent provided for participation in the study.
Exclusion criteria
Consumers needed to not meet any of the following criteria:
• Consumer refused contact with SMHS;
• Consumer opted out of being contacted about participation in the study;
• Participation in the study deemed to be potentially distressing, unhelpful or harmful to the
consumer as judged by either their treating clinician and/or the Clinical Liaison.
Family
‘Family’ was broadly defined to include any people who had been involved in the consumer’s
recent care with Crisis Resolution in a non-professional capacity (e.g., partner, friend, Pastor,
87
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
link to page 91
Released
neighbour who facilitated the consumer’s involvement with Crisis Resolution, or supported them
while they were under the care of Crisis Resolution).
Referrer
‘Referrer’ was broadly defined to include any people who had been involved in the consumer’s
recent care with Crisis Resolution in a professional capacity (e.g., General Practitioner, Psychiatrist
or Counsellor who facilitated the consumer’s involvement with Crisis Resolution, or worked
alongside them while they were under the care of Crisis Resolution).
under the Official Information Act 1982
Measures
Brief structured interviews were conducted via telephone with participants. Questions were
designed to assess global satisfaction with care and satisfaction with specific aspects of care, and
involved nine forced choice questions and two open ended questions. The specific questions that
were asked are outlined in the results section of this report (together with responses), for
economy of space. Consumers and family were asked all eleven questions. Referrers were asked
the first four questions, plus an additional question addressing communication (How would you
rate the communication that you received from Crisis Resolution about this patient?
good/ok/bad/don’t know). Consumers were also asked brief demographic questions assessing age
category (18-24, 25-34, 35-44, 45-64 years), ethnicity and gender.
RESULTS
Who participated?
Figure 1 summarises recruitment for the study. Of the 123 consumers who met inclusion and
exclusion criteria, 75 participated (response rate = 61%). This rate compares favourably with other
similar studies that have recruited consumers who have recently had an urgent mental health
problem [3]. Briefly, consumers were roughly evenly split by gender (51% female), were most
likely to be aged 18-24 years, and most commonly identified as being New Zealand European
(81%), followed by Maori (14%), Samoan, Indian and other (each ≤ 1%). The demographic
characteristics of the consumers interviewed were broadly consistent with those of people who
use CR. This means that the findings from this study can be generalised to people who typically
use Crisis Resolution.
What did participants say?
Forced choice questions
1
1 To ease interpretation, only summarised responses are presented. ‘Satisfied’ includes response
categories such as ‘good’ and ‘ok.’ Response categories such as ‘not applicable’ or ‘unsure’ were
excluded.
88
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Would you recommend the Crisis Resolution Service to family and friends if they
needed similar care or treatment?
Consumer = 92% satisfied, Family = 86% satisfied, Referrer = 93% satisfied.
How would you rate the care you received from the Crisis Resolution Service?
Consumer = 96% satisfied, Family = 91% satisfied, Referrer = 91% satisfied.
How easy was it for you to access the Crisis Resolution Service (e.g., find out how to
under the Official Information Act 1982
contact them, get someone on the phone and make an appointment)?
Consumer = 86% satisfied, Family = 88% satisfied, Referrer = 91% satisfied.
Were you seen and helped quickly enough by the Crisis Resolution Service? Consumer
= 88% satisfied, Family = 77% satisfied, Referrer = 93% satisfied.
Were you given a choice about where you were seen (at least some of the time)?
Consumer = 65% satisfied, Family = 57% satisfied
Were you asked if you wanted family involved in your care? (e.g., maybe to attend
appointments with you, or for staff to talk to them)?
Consumer = 84% satisfied, Family = 79% satisfied.
How straightforward was it for you to meet with staff, tel your story and develop a
plan?
Consumer = 86% satisfied, Family = 83% satisfied.
Were your needs met by the Crisis Resolution Service (either by them, or did they
suggest somebody else who could help)?
Consumer = 81% satisfied, Family = 81% satisfied.
How respected did you feel by staff at the Crisis Resolution Service?
Consumer = 93% satisfied, Family = 91% satisfied.
How would you rate the communication that you received from the Crisis
Resolution Service about XX?
Referrer = 81% satisfied.
89
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Who was more likely to feel dissatisfied?
If consumers felt dissatisfied with care on global measures, they were significantly more likely to
be aged 25-34 years.
Open questions
Participants were more likely to offer comments on what they thought was especially helpful or
good about the care (approximately 3/4 commented), than about how the service could be
under the Official Information Act 1982
improved (approximately 1/2 commented). The same themes were identified for both the
positive and negative questions, as follows: staff issues, access to the service, where consumers
were seen, the interventions provided or facilitated, involvement of family,
communication/liaison/record issues and transport.
Overall, participants were most likely to comment on the manner of staff and the treatment that
had been received. For staff manner, it was important to participants that staff were: warm,
interested, empathetic, respectful, not rushed or dismissive, that they listened well, treated
people as individuals, and were positive and reassuring. For treatment, it was important to
participants that they received effective treatment of sufficient duration.
A diverse range of specific suggestions were made about how the service could be improved,
including the following:
• Better publicity about the existence of the service and how to contact them;
• The 111 service suggest use of Crisis Resolution as an option, rather than necessarily using
the Police;
• Access to the service at a “non-crisis level;”
• Somewhere private to sit and be looked after if experiencing an anxiety attack in the
waiting room;
• Better options for managing intoxicated people needing crisis care;
• Improved security for staff; and
• Not being discharged “too soon.”
In terms of what was especially good or helpful about the service, many people made general
comments about how grateful they were that the service existed, how appreciative they were of
having someone to talk to and listen to them (or their family member) at a difficult time. Specific
aspects of care that people commented favourably about included the following:
• Being seen quickly;
• Having the option of being seen at home;
• Being given a “minder” while in hospital;
• Receiving “good respite care;” and
• Receiving “good follow-up.
90
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
EMBED, SUSTAIN & FUTURE DIRECTIONS
The findings have been presented in person and in writing to both the front line Crisis Resolution
staff and to clinical leadership teams on several occasions. Open discussions have occurred with
these groups about what can be learned from the results, and what the implications may be for
service delivery. The present research is also informing a working party looking at improving Crisis
Resolution services. A complimentary piece of work has been conducted by Dr Charlie Whan
(SMHS) on
staff perspectives, and is also contributing to the working party. By taking all
under the Official Information Act 1982
perspectives into account, meaningful improvement will occur within Crisis Resolution services
and changes will be more likely to be consistently implemented and maintained.
Of concern, the present project identified that 19% of referrers were not satisfied with the
communication that they received from Crisis Resolution. Work is currently underway looking at
how SMHS and General Practitioners can work together better, including improving
communication. It is not clear why consumers who were aged 25-34 years may have been more
dissatisfied with the care they received (global ratings). This finding highlights the importance of
collecting demographic data in the future, so that it can be seen if this finding is replicated. In the
event of this, further in depth investigation would be warranted.
A manuscript detailing this study is presently under consideration with a peer reviewed journal
(BMC Psychiatry). If successful, publication would mean that this project contributed to the
international literature on this topic, as well as helping to improve local services.
Finally, one of the key, ongoing benefits of the project has been the addition that has been made
to the Initial Treatment Information Form (SMHS) as a consequence of our consultations with the
Office of the Privacy Commission, as follows:
I understand that…
•
CDHB aims to continually improve the quality of care that it provides. Therefore I may be
contacted and asked about the quality of care that I have received. I understand that I
have a right to decline to participate, and that this wil not adversely affect the care that I
receive in the present or in the future, nor wil it adversely affect the quality of the care I
receive.
This addition will help clarify for future consumers how their contact information may be used and
what they might expect when receiving care from SMHS. Importantly, it will also mean that future
Quality initiatives within SMHS should be more straightforward to undertake, and be more clearly
consistent with expectations around the management of information collected in a health context.
CONCLUSIONS
High levels of satisfaction were found with Crisis Resolution. Staff manner and having effective
treatment of sufficient duration were the most important issues for participants.
91
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
REFERENCES
1.
NICE. Service user experience in adult mental health: improving the experience of care for
peole using adult NHS mental health services. 2011. nice.org.uk/guidance/cg136. London.
2.
Worthington A, Rooney P. The Triangle of Care. London: National Mental Health
Development Unit, 2010
3.
Lloyd-Evans B, Johnson F. Crisis resolution teams: how are they performing? Ment Health
under the Official Information Act 1982
Today 2014;18-19.
4.
Canterbury District Health Board. "We need the whole system to be working for the whole
system to work". 2012.
5.
Specialist Mental Health Service. Specialist Mental Health Service Priorities 2016.
New initiatives / developments in your region.
Home care Health lines and Spark Home care health line have a new app that they have
developed for mobiles and devices; they are currently in talks with Spark about making the pp free
for people to access when they have no data!! Come on Spark help our people.
Child, Adolescent and Family Changes:
Reducing wait times has been a key focus for CAF services. The number of case starts for
September 2016 was 239 compared to 293 in August.
The service has undergone significant growth over the past 15 years, which accelerated after the
quakes. In recent years, it has become apparent that the individual components of the service that
developed, somewhat independently of each other, need to be drawn closer together to ensure
smooth clinical and administrative processes and efficient utilisation of resources. The first stage
of implementing the Direction of Change got under way in September, which has involved co-
locating staff that are part of the integrated community teams into
North (Hillmorton) and
South (Princess Margaret Hospital campus). The idea being the services will be closer to the communities
and the people that are using them.
The School Based Mental Health Team
The Team continues to engage with a large number of schools across Canterbury and at end
September 2016 were working with 112 schools. The ongoing focus is to help schools to identify
the mental health support needed for their population and to meet these needs through
workshops, pastoral care meetings, learning and development activities for staff, and liaison and
engagement with other agencies. Families in the community have found the educational
presentations that were provided in the evenings at local schools or community halls such as to be
very helpful after the earthquakes. Presentations were on anxiety and children, E- Devices Safety
etc.
92
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Awareness Mental Health Consumer Network October
Awareness celebrated mental health awareness week by having a picnic in the Christchurch
Botanic gardens. A cake donated by the Mental Health Foundation plus a carrot cake provided by
Awareness was a great starting point for conversations around mental health.
Please check out the Facebook page.
People have raised concern at Awareness about lifeline losing their funding as it is an established
under the Official Information Act 1982
name in the community where as many consumers do not know anything about the new tele
health providers.
Suicide rate in Canterbury is still high and there has been little change in the numbers. It is of
concern to the network as so many initiatives and focus of the whole region has been on mental
health since the earthquake including substantial Health Promotion campaigns on well-being.
Minutes attached to Southern Regional Report
Minutes of the Awareness: Monthly Meeting
Monday the 8th August 2016, 12.30pm-2.00pm
SPEAKER Debbie Selwood: SERVICE MANAGER
Debbie Selwood presented on the new model of care in Specialist Mental Health Services (SMHS)
has been implementing and the impact it is having on the services. Debbie summed up the major
issues that people were experiencing in the system about three years ago. These included: lack of
flexibility, multiple assessments meaning people needed to tell their story over and over, delays in
non-urgent assessment leading to some people waiting eight weeks, delays in transitioning people
into other services that would be helpful, overcrowding in the acute inpatient units, an inpatient
service with a high number of locked beds, and high seclusion rates.
After consultation with people who have used services and families, the services made a plan to
increase consumer choice, reduce wait times, prevent the use of seclusion, and increase
community teams’ face to face time with people. The new model has reduced waiting times for
initial assessments, home visits increased, community case manager’s caseloads decreased to be
able to work more with people, increased capacity to support an extra 600-700 people following
the earthquakes and dramatically reduced seclusion.
ISSUES One person fed back that they were not given any choice about where to meet at
Specialist Mental Health Services except in an old de-commissioned seclusion room and were
made to feel blamed when they didn’t want to meet there.
93
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
Mental Health Awareness Week: Naturally Happy
At the last meeting we talked about holding a Mad Hatters Ball to celebrate mental health
awareness week. Since then the exec has thought about the logistics of this and are considering
smaller events or activities. This could be a poetry night if we bring this forward for October, a
music event, a film screening, or even doing some positive chalking around the city. The theme of
the week this year is “naturally happy” which may also help inform what we do.
Fundraising
under the Official Information Act 1982
A friend of Awareness started the first Depressed Cake pop-up Shop. It is happening at "First
Thursdays" market at The Colombo Shopping Complex.
It is about reducing the stigma of depression and mental illness, and all the proceeds are going to
MHAPS. They have cakes and cake shops from all over Canterbury (as far down as Ashburton)
contributing to the fundraising. All cakes were grey on the outside, and had rainbows in the inside!
The Chair of Awareness meets with the General Manager of Specialist Mental health service, Toni
Gutschlag bi-monthly for the membership to directly ask pertinent questions and for Toni to
update them on
1/ How do you ensure transgender people are represented accurately and that their need get
meet? For example, when a Trans person fills out a form can they put their gender down
accurately and then have their choice of pronouns used? One consumer noted “As a Trans person
I find it hard to accurately fill out forms in a way that represent my gender because there is
normally only a female and male box. Neither describes my gender. When I tried to change my
prefix to Mx it got change but when I went there again it got change back to Ms. I feel this does
not meet my need of my gender being recognized.” Another example Trans people have
experienced is a practitioner needing to lie for them to get access to trans health care such as
Hormone Replacement therapy.
This hasn’t been fully worked out yet so the question is timely. This would be a good issue to take
to the Consumer Council as it is a concern across al health. In a recent form she noted that they
offered Male, Female and Agender as options. Darryn did mention this at the Consumer Council
meeting and they wil look at it as wel . Toni wil fol ow up with Wayne at Planning and Funding.
Toni Gutschlag acknowledged that there needs to be more engagement with the transgender
community. Has Ngā Hau e Whā been discussing this? Have Pacifica leaders? Toni will raise this
with the Ministry of Health to see how other DHBs are handling it. As far as she is aware there are
no guidelines available yet. Her expectation of services is that someone’s personal needs wil be
met with sensitivity. If this doesn’t happen, please note the concerns to the CDHB and use and
advocate or the Human Rights Commission for support.
94
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
2/ Collaborative note writing – where is this at in services? This is a huge thing for members of the
network, especially people who struggle with having their experiences reworked or reframed
The CDHB doesn’t have a policy at this point. Anyone can ask to see their notes and can correcting
or amending them is encouraged. Again, you can seek advocacy support if needed.
3/ Are there any opportunities for patients in the inpatient units to meet all together to provide
feedback on how the units are administered? There are some inconsistencies members have
noticed between the different units.
Yes, there is likely to be but Wendy Lowerson and Steve Duffy
under the Official Information Act 1982
would know how to also, those going in to do peer support could pass information or concerns on.
4/ A member of the network has recently had difficulties with her family accessing support
through specialist mental health services. Her family member has been denied further support
from SMHS on each occasion after a number of referrals. When the family see staff at crisis
resolution, or talk to SPOE staff the focus has been on the Awareness member’s previous mental ill
health, and their family member, who is seeking help has only had their depression and anxiety
explained by SMHS staff as being in relation to the Awareness member’s prior mental ill health
experience, or “family relationship issues” and then been referred back to their GP. 5/How does
the mental health system work when a family or couple have multiple people who have mental
illness? What should the process be for staff to provide support in this situation? What should be
happening to prevent one family member’s previous diagnosis becoming the lens through which
all other family members’ struggles are perceived?
This is a concern. Toni would want every referral to be considered on its own merits. She
encourages taking an advocate. Perhaps a second opinion would help. The staff have training
available for family support and being aware of individual needs.
Making a complaint can help. Each first goes to the Quality Manager, then to the Leadership team
(as do all serious incident reports) where they are assessed for any clinical changes needed. Then
they go to Toni for any final support required. Complaints can be made anonymously if needed.
5/ There have been disparities in what members of the network have been offered in terms of
support following a contact with Crisis Resolution, for example, one member was contacted every
day for a week following being in touch with CR where staff checked how they were doing.
Another member was told the only options would be a medication change or inpatient stay and if
they didn’t want an inpatient stay then their GP could just as easily oversee medication change so
further SMHS or CR support would not be needed. Why does this discrepancy occur? Should
consumers be given the full range of options for support and be able to choose what feels best for
them?
These issues can be taken to Joan Taylor as she is developing clinical pathways right now. It may
help people to know that they are short of Doctors right now and there has been a lot of staff
change. Thankfully the request for services has levelled off and isn’t still increasing. It has stabilised
at a very high level though.
95
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Released
6/ Some comments from presumably mental health staff (not necessarily from CDHB) have been
posted on a Stuff article and show incredibly negative views. Does the CDHB require staff to not
comment publicly in this kind of way? It’s hard knowing that health professionals can talk about
consumers like this on a public forum. (Examples were given)
Yes, the CDHB has a policy that staff may not make public comments, can’t say they work in a
particular part and are not meant to criticise their employer or breach the privacy of patients or
col eagues. Especially on facebook or any other social media. No one can control anonymous
comments though. We don’t have the same support from a Mental Health Commission as we used
under the Official Information Act 1982
to. The Mental Health Foundation should be able to offer some leadership here. We also have the
right to write to Fairfax Media to express our concern re lack of balance or moderation.
7/ Do you have plans yet for Mental Health Awareness Week? Would you like to work with
Awareness to put on an event?
Yes, a broad project could be good though cost has to be a concern. We could talk to Cathy King
who runs projects and conferences for the CDHB. Toni would support a project if there were
enough people to help. The 150th Commemoration Family Picnic went wel but it also required a
great deal of time and co-ordination.
8/ We read in the paper that Hillmorton will go Smoke Free again. What is the plan this time?
They have been moving toward reducing and eliminating smoking since the last temporary
cancel ation .They have a group who is establishing a good time frame and good systems, and
further cessation supports.
Toni’s (Gutschlag) Items
At a previous meeting Toni said she would talk to the Christchurch co-ordinator of Child, Youth and
Family. She wanted us to know that she was on leave then they were on leave but she is stil
fol owing this up within the next 2 months.
The changes at CYF wil be important to the CDHB. In about 2 years’ time a percentage of the
CDHB’s Child/Youth funding wil be given to CYF (or their equivalent organisation) to give out to
providers. There is grave concern that the providers won’t understand clinical needs and the
governance required to support clinical programmes. As it is there isn’t enough funding to cover
services requested?
One advantage for Mental Health in Christchurch is that there has been such good work done
with keeping older persons healthy in their home that the hospitalisation rate has reduced. The
funding freed up has come to mental health.
96
Ngā Hau e Whā Ngā Hau e Whā Ngā Hau e Whā June to December 2016 Report to the Ministry of Health
Document Outline
- 1_Redacted
- 1A
- 1B
- Ngā Hau e Whā Website June 2016 <www.nhew.org.nz>
- The website is based on the previous design, but has much greater capability for modifications and further development, with Ngā Hau e Whā 3 representatives forming a sub-group as administrators and developers of the site, including the person who was...
- The website is designed in a way that it’s content, functioning, and design is ‘open’, flexible and simple for administrators to manage, allowing the site to remain in the hands of the Ngā Hau e Whā representatives into the future, rather than having ...
- Further work is being undertaken so that the website will manage the entire Ngā Hau e Whā networking capability, such as the distribution list, feedback and comment, and promotion of our stakeholders and network communications, and most importantly a ...
- It is expected this new arrangement for our website and online and social media presence will bring about a considerable cost benefit to Ngā Hau e Whā. This saving will be presented in the next report, once we are better informed as to the previous sp...
- It is expected this new arrangement for our website and online and social media presence will bring about a considerable cost benefit to Ngā Hau e Whā. This saving will be presented in the next report, once we are better informed as to the previous sp...
- Jak Wild Website Design.
- CRISIS RESOLUTION SERVICE