



 N A L P Y C N E G R
A (
E M
M
E
P
D
LA
N
N
A
Z
T
)
N
N
E
EW ZEALAND AMBULANCE MAJOR INCID
N A L P Y C N E G R
A (
E M
M
E
P
D
LA
N
N
A
Z
T
)
N
N
E
EW ZEALAND AMBULANCE MAJOR INCID
New Zealand Ambulance Major Incident
and Emergency Plan (AMPLANZ)
1982
Act
The Plan
September 2016
Information
Official
the
under
Released
Acknowledgements
Ambulance New Zealand would like to acknowledge and warmly thank the following organisations for their
support and contributions towards the completion of the 2011 version and also this review of AMPLANZ:
Members of Ambulance New Zealand especially St John, Wellington Free Ambulance and the Northern
Emergency Services Trust for releasing the members of the AMPLANZ review work group:
Tim Chiswell, St John
Warren Cornor, Wellington Free Ambulance
Kelvin Perriman, St John
Bruce MacDonald, St John
Peter Turnbull, NEST
Andrew Keenan, Wellington Free Ambulance
Ambulance NZ Standards and Accreditation Committee
1982
New Zealand Fire Service
Ambulance Victoria, Specialist Emergency Response Department
NZ Ministry of Health, Emergency Management Team and especially Murray Mills as a member of the
Act
Review work group
UK Department of Health, Emergency Preparedness Division
Thank you to Paul O’Connell (St John Learning Media) for the design of this document.
Thank you also to Catherine Preston, David Wethey, Glenn Cockburn, Matt Ohs, Oz Golan, The Lifeflight Trust
and Hawke’s Bay Today for the use of their photographs in this document
Foreword
Information
New Zealand has for a number of years had a national ambulance major incident and emergency plan
– AMPLANZ. This has ensured that there is a common understanding between ambulance services,
communications and control centres and our emergency management partners as to how an ambulance will
respond in a time of crisis.
Official
This document is the reviewed plan based largely on the 2011 plan, the changes in the sector and its
experience relating to major incident management. There have also been changes to the New Zealand
Coordinated Incident Management System (CIMS) as well as a new National Health Emergency Plan (NHEP).
the
Developments in CIMS or the NHEP are reflected here.
Thankfully, unlike before the previous extensive rewrite of AMPLANZ in 2011, New Zealand has not had
significant local or regional emergencies like the Pike River tragedy and the Canterbury Earthquakes. That
said, we have seen improvements to our management and an increased awareness of our plans and
procedures through reviews of incident management and ongoing local and national exercises. Examples
under
where significant development has occurred is in the formalisation of Ambulance’s National Crisis
Coordination Centre run by St John and improvements in the sector’s business continuity management.
AMPLANZ continues to provide the sector with the appropriate guidance for each service to development its
own detailed major incident and emergency plan.
Finally there continues to be development of our national understanding of the risks we face and the need
to ensure that our plans, organisations, people and communities are resilient. AMPLANZ covers all aspects
of our management in a major incident and enables ambulance services to coordinate effectively with
Released
partner agencies.
David Waters
CEO
Ambulance New Zealand
AMPLANZ Part 1:
Introduction to AMPLANZ and Emergency Management for the
Ambulance Sector
For all staff of New Zealand Ambulance Services
1982
September 2016
Act
Content
Part 1: Introduction to AMPLANZ and Emergency Management of
the Ambulance Sector
Information
1.0 Introduction
4
1.1 What is AMPLANZ?
4
1.2 The Aim of AMPLANZ
4
1.3 Mandate of AMPLANZ
4
1.4 Format of AMPLANZ
4
1.5 The Ambulance Sector
5
Official
2.0 Frameworks and Concepts of Emergency Management
6
2.1 Legislation and National Emergency Management Plans
6
2.2 The 5 ‘Rs’
6
the
2.3 CIMS (New Zealand Coordinated Incident
Management System)
7
2.4 Concept of Ambulance Emergency Management
7
2.4.1 The Responsibilities of Ambulance Services in a
Major Incident
7
under
2.4.2 A structured and consistent approach
8
2.4.3 Whole of Organisation and Sector
8
Part 2: Consistent Operations at the Scene
Part 3: Ambulance Service Approach
Part 4: National Crisis Coordination Centre
Appendices
Released
1.0 Introduction
AMPLANZ is mandated to provide:
“….all Ambulance Services with the nationally
1.1 What is AMPLANZ?
standardised framework to command, control and co-
ordinate ambulance resources locally, regionally and
AMPLANZ is a detailed operational framework for
nationally, for the greatest good of the greatest number
the New Zealand ambulance sector to provide clear
of casualties during major incidents”.
guidance for all Ambulance Services in all parts of the
emergency management cycle. It provides standard
1.4 Format of AMPLANZ
terminology, structures, and roles. It also provides tools
to assist an Ambulance Service in its readiness and
The format of AMPLANZ is one document made up of
reduction, response and recovery, for example, task
four parts as noted below.
cards, planning templates, debriefing templates etc.
Specific Ambulance Service Major Incident and
AMPLANZ – The Plan
1982
Emergency Plans must be developed Ambulance
Services based on this framework.
Part 1
Part 2
Part 3
Part 4
AMPLANZ cannot be arbitrarily changed. There is a
Introduction
Consistent
Ambulance
National
Act
to AMPLANZ
Operations
Service
Crisis
review process through the Ambulance New Zealand
and Emergency
at the
Approach
Coordination
Standards and Accreditation Committee outlined as
Management for
Scene
Centre
part of AMPLANZ.
the Ambulance
Sector
In line with health sector and the emergency
management sectors as a whole, there are a large
number of specialist terms and abbreviations. To
Part 1: Introduction to AMPLANZ and Emergency
assist the reader, there is a Glossary of Terms and
Management for the Ambulance Sector: This part
Abbreviations in Appendix 1.
summarises what AMPLANZ is, the sector, and key
ambulance and emergency management concepts.
Information
1.2 The Aim of AMPLANZ
Part 2: Consistent Operations at the Scene: This
The aim of AMPLANZ is to:
Part focuses on the activities to be undertaken by
responding crews, the duty management and those
Ensure the effective and consistent management of
operational officers directly involved at the scene in
major incidents at local, service and national levels
coordination with other responding agencies.
for the benefit of patients
Official
Part 3: Ambulance Service Approach: This Part focuses
Minimise the impact of a major incident or multiple
on the activities to be undertaken by Ambulance
major incidents on normal operations
Service Management in all parts of the emergency
the
Adopt and encourage a whole-sector approach to
management cycle. It is designed to guide ambulance
major incident management
managers who are required to support the response
at the scene, as well as play a role in preparing for or
Adopt and encourage a whole-of-organisation
recovering from a major incident.
approach within services to major incident
management.
Part 4: National Crisis Coordination Centre: This
under
Part provides a framework for the development and
1.3 Mandate of AMPLANZ
management of National Crisis Coordination Centre to
ensure that the ambulance sector is able to respond to
AMPLANZ applies to all Ambulance Services1 in
a significant regional or national emergency.
New Zealand and it is noted in Section 3.2.7 of
the Ambulance Standard (NZS 8156:2008) that an
This is Part 1.
Ambulance Service
“shall be aware of, and where
appropriate, contribute to, regional and/or national large
scale contingency planning and be able to operate in
Released
accordance with such plans including…. AMPLANZ”.
Ambulance New Zealand has approved policy to clarify:
“…the mandate of AMPLANZ and to ensure that
Ambulance NZ and Ambulance Services understand their
roles and responsibilities with regards to the development,
maintenance, and operationalisation of AMPLANZ”.
1An Ambulance Service is defined in NZS8156:2008 Section 1.5 page 12.
4
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)




















1.5 The Ambulance Sector
(ACC)-contracted fixed wing and rotary air ambulance
Trust. The area of coverage of the land-based services
The primary role for the ambulance sector is to deliver
and the bases of the air ambulances are noted in
pre-hospital health care. This includes triage, treatment
Figure 1.
and transport and pre-hospital emergency and non-
acute care. Response to major emergencies is also
Ambulance communications and clinical control
considered part of the sector’s primary role. Beyond
services are managed by the two land based
the emergency functions, Ambulance Services are
ambulance services. The services are provided by St
continuing to develop their role in the primary health
John Clinical Control Services (CCS) and WFA Central
care sector.
Communications. The St John CCS is currently run
from two Clinical Control Centres in Auckland and
There are two land-based emergency Ambulance
Christchurch. The WFA Central Communications is
Services and 11 Accident Compensation Corporation
based in Wellington.
1982
Figure 1
Act
Information
Land based ambulance services
St John
Wellington Free Ambulance
Air ambulance services
Official
Helicopters
Fixed Wing Aircraft
the
under
Released
PART 1 SEPT 2016
5
Ambulance Services are required to comply with the
Appendix 2 lists the key legislation and plans that
Ambulance Standard (NZS 8156: 2008).
guide Ambulance Service emergency planning.
In addition, there are multiple services that provide
patient transfer services, private hire services, support
2.2 The 5 ‘Rs’
to public events and specialist operational support to
The New Zealand integrated approach to emergency
other emergency services.
management can be described by the four areas of
activity, known as the ‘4Rs’ 4.
2.0 Frameworks and Concepts of
These are
Emergency Management
Reduction: identifying and analysing long-term
risks to human life and property from natural or
2.1 Legislation and National Emergency
non-natural hazards; taking steps to eliminate
these risks if practicable, and, if not, reducing the
Management Plans
1982
magnitude of their impact and the likelihood of
The ambulance sector in New Zealand, unlike many
their occurring
services internationally, does not have its own
Act
Readiness: developing operational systems and
legislation that guides and regulates the provision of
capabilities before an emergency occurs
ambulance services.
Response: actions taken immediately before, during
That said, Ambulance Services are health sector
or directly after an incident or emergency to save
organisations and therefore have responsibilities
lives and property, and to help communities recover
within, for example, the Health Act 1956 and
New Zealand Public Health and Disability Act 2000.
Recovery: the coordinated efforts and processes
used to bring about the immediate, medium-
In the context of emergency management, the
term and long-term holistic regeneration of an
ambulance sector must comply with, for example, the
organisation and community following an emergency.
Civil Defence Emergency Management Act 2002 and
Information
Epidemic Preparedness Act 2006.
For the purposes of AMPLANZ, a ‘5th R’ is identified
as critical:
Ambulance services shall be aware of their
responsibilities under these legislations as well as
Relationships: the development and maintenance of
other health, safety and workplace legislation.
communications, coordination and understanding of
capacity and capability between ambulance service
There are two key national plans that relate to
managers and key personnel in health service
Official
emergency management. These are the:
agencies, civil defence and welfare agencies, lifeline
National Civil Defence Emergency Management
organisations and private sector agencies, as well as
Plan 2015
traditional emergency service partners.
the
National Health Emergency Plan 2015 (NHEP).
2.3 CIMS (New Zealand Coordinated
The NHEP, in particular, refers to the requirement of
Ambulance Services to:
Incident Management System5)
“...provide triage, initial treatment and transportation
The purpose of CIMS is to provide structure and
under
as outlined in the Ambulance Major Incident and
coordination in the management of incidents with
Emergency Plan...” (AMPLANZ) 2
the aim of improving efficiency and effectiveness
in management response. CIMS is New Zealand’s
And:
approach to incident management and it provides a
“...if regional ambulance resources are overwhelmed,
framework to manage a range of diverse incidents from
ambulance services will open the National Crisis
routine incidents to major emergencies.
Coordination Centre (NCCC). The NCCC will coordinate
CIMS is a seamless approach based on the following
with the National Health Coordination Centre and other
Released
principles across all responding organisations:
national emergency management structures ... as
required. The NCCC will also coordinate the (national)
Common structures, roles, and responsibilities
ambulance response.” 3
Common terminology
The Ministry of Health (MoH) is the lead agency
Modular and scalable
for national health and disability sector emergency
planning and response coordination.
2National Health Emergency Plan 2015. Page 23.
3National Health Emergency Plan 2015. Page 23.
4http://www.civildefence.govt.nz/cdem-sector/cdem-framework/the-4rs/
6
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)

1982
Act
Responsive to community needs
All Ambulance Services are required to be familiar with
CIMS and have personnel trained to the appropriate
Integrated response coordination
level to manage incidents in line with CIMS. CIMS
Consolidated action planning
manuals shall be available to all Ambulance Service
personnel.
Integrated information management and
communications
2.4 Concept of Ambulance Emergency
Resource coordination
Management
Information
Designated response facilities
Manageable span of control
2.4.1 The Responsibilities of Ambulance Services in
To coordinate the effective use of all of the available
a Major Incident
resources, agencies need a formalised management
structure that lends consistency, fosters efficiency and
The role of the ambulance sector in response to a
Official
provides direction across the 4Rs. The CIMS structure
major incident is to deliver and maintain appropriate
is built on the functions:
pre-hospital clinical care. In a mass casualty incident,
ambulance will lead the operational health response
CONTROL: Coordinates and controls the response
to the incident at the scene/s and manage the triage,
the
INTELLIGENCE: Collects and analyses information
treatment and transport of patients to appropriate
and intelligence related to context, impact and
receiving hospitals or health facilities. In all
consequences; also distributes intelligence outputs
emergencies impacting the health of the communities,
Ambulance Services will manage and coordinate their
PLANNING: Leads planning for response activities
response with the DHBs and other emergency services
under
and resource needs
to manage demands on the healthcare system.
OPERATIONS: Provides detailed direction,
Below are key responsibilities of Ambulance Services
coordination, and supervision of response
in a major incident.
elements on behalf of the Control function
Responsibilities of an Ambulance Service in all
LOGISTICS: Provides personnel, equipment,
emergencies:
supplies, facilities, and services to support
response activities
To save life in conjunction with other Emergency
Services
Released
PUBLIC INFORMATION MANAGEMENT: Develops
and delivers messages to the public, directly and
To notify and liaise with the other Emergency
through the media, and liaises with the community
Services
if required
To initiate and maintain an Ambulance Service
WELFARE: Coordinates the delivery of emergency
Command and Control structure lead by an
welfare services and resources to affected
Ambulance Service Controller
individuals, families/whānau, and communities
5The New Zealand Coordinated Incident Management System (CIMS), 2nd edition. 2014. Safer communities through integrated emergency
management. Pages 4–6.
PART 1 SEPT 2016
7
To protect the health, safety and welfare of all
To assume responsibility for casualty
ambulance staff generally, and all health workers
decontamination, in conjunction with the Fire
on the scene. Also ensure that the actions of
Service
Ambulance and health staff do not put others
To provide the Fire Service with clinical advice and
at risk.
assistance to support on-site decontamination
To supply sufficient ambulances and staff for
To maintain adequate emergency ambulance cover
the incident
throughout the Ambulance Service’s operational
To provide a communications system between
area for the duration of the major incident
ambulance and DHBs (including hospitals)
To progressively release activated hospital(s) and
To provide Ambulance Liaison Officer/s to the
health facilities and ultimately issue a message
partner agencies as appropriate for the incident
indicating the completion of casualty evacuation.
To reduce to a minimum, the disruption of the
1982
normal work of the Service by implementing
2.4.2 A structured and consistent approach
Business Continuity Plans, as appropriate,
AMPLANZ is aligned with CIMS, important
ensuring the restoration of normality at the
New Zealand emergency management concepts and
Act
earliest opportunity.
with key national emergency plans.
Responsibilities of an Ambulance Service for Mass
AMPLANZ also notes that to effectively manage large
Casualty Incidents in particular:
and complex incidents, the processes and procedures
used by ambulance services need to be established
To provide a structure to support the triage,
and understood within the services and also by partner
treatment and transport of casualties from the
agencies.
scene by establishing an Ambulance Control
Point, Casualty Clearing Point and Ambulance
Major incidents, such as mass casualty events, are
Loading Point
infrequent and consequently any procedures required
Information
to manage such incidents shall follow the same basic
To provide a Senior Ambulance Officer at the scene
processes as for smaller and less complex incidents.
to act as Ambulance Commander (AC)
Therefore essential processes, such as assigning
To be part of the Scene Incident Management Team
initial response roles and responsibilities, incident
(IMT) to ensure a coordinated response to the
escalation, notifications, situation reports, triage etc
incident
are the same no matter what the size or complexity of
the incident.
Official
To identify, notify and communicate with appropriate
receiving hospital(s), health facilities and DHBs
of the prevailing situation and the categories and
2.4.3 Whole of Organisation and Sector
the
estimated times of arrival of casualties
AMPLANZ is designed to ensure that all parts of the
To triage all patients prior to evacuation from
ambulance sector and the individual services are
the scene
involved in the response, recovery and development of
readiness of the sector. This will then contribute to the
To manage all medical resources deployed to the
resilience of the health sector.
scene for the treatment and care of casualties
under
Within an Ambulance Service there are roles and
To determine the priorities for the evacuation
responsibilities of first-responding crews, for ambulance
of casualties, ensuring even and simultaneous
service management and also for key support staff in
dispatch to the receiving hospital(s) and health
non- operational or core support positions.
facilities
Across the sector, guidance is given to further integrate
To organise transportation for casualties to the
the individual service’s response and planning at
receiving hospital(s) and health facilities, and any
the tactical and operational levels and also in the
necessary secondary transfers between hospital
coordination of all ambulance services with national
Released
To acquire additional ambulance resources, as
agencies, such as MoH.
necessary through the use of the Ambulance
Service’s national coordination mechanisms
To forward to the receiving hospital(s) and health
facilities, Medical Officer(s) of Health and DHB(s),
any information acquired at the scene relating to
chemical, biological or radiation (CBR) hazards and
possible contamination of casualties or rescuers
and advise of the potential for self-presenting
patients
8
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
AMPLANZ Part 2:
Consistent Operations at the Scene
For all Ambulance Services staff working directly at or with the scene
September 2016
1982
Act
Content
Information
Part 1: Introduction to AMPLANZ and Emergency Management for the
Ambulance Sector
Part 2: Consistent Operations at the Scene
1.0 Introduction
10
3.6 Summary of scene roles and responsibilities
21
Official
2.0 Readiness and Reduction
10
3.7 Site Set up
22
2.1 Planning and development
10
3.8 Coordination with Health, Emergency Services and
2.2 Training and education
10
other Agencies
25
3.8.1 Health
25
the
3.0 Response
10
3.8.2 Emergency Services and other Agencies
25
3.1 Activations, Level of Response, and Notifications
10
3.9 Media
25
3.1.1 Escalation
11
3.10 Resources and Equipment
26
3.1.2 Definition and Types of Incident
12
3.1.3 Response Matrix Tool
13
3.10.1 Major Incident Vests
26
3.1.4 Risk Assessment and Response
13
3.11 Specialist Operations
26
under
3.2 Role of the First Crew
14
3.11.1 Activation of Ambulance Specialist Operations
27
3.11.2 Pre-hospital Responses by DHBs and other organisations
27
3.3 Triage
14
3.11.3 Activation of Responses by DHBs and other organisations
3.4 Communications and information management
16
27
3.4.1 On-scene communications
16
4.0 Recovery
27
3.4.2 METHANE
16
4.1 Ambulance Debrief Processes and Tools
28
3.4.3 Notifications to Health Partners
18
4.1.1 Debrief aims and requirements
28
3.4.4 Information Management tools
18
4.1.2 Debrief and Reporting tools
28
3.4.5 Integration with the Incident Management Team
19
Part 3: Ambulance Service Approach
Released
3.5 Command Structure and Scene Management
19
3.5.1 Simple Command Structure
19
Part 4: National Crisis Coordination Centre
3.5.2 Comprehensive Command Structure
19
Appendices
1.0 Introduction
complete CIMS 2 training, with refresher training
every five years
AMPLANZ is divided into four parts plus an overview
document. This is Part 2 and focuses on the activities
All ambulance operations managers, CCCS
to be undertaken by responding crews, the duty
managers and relief managers to complete CIMS 4
management, the CCCS and those operational officers
training with refresher training every five years
directly involved at the scene, in coordination with
Senior ambulance managers and officers (District
other responding agencies.
Operations Managers, Territory Managers etc.) who
This document should be read in conjunction with
will be required to fill Ambulance Commander or
Part 1: Introduction to AMPLANZ and Emergency
Operations Manager roles to complete ‘Ambulance
Management for the Ambulance Sector.
Critical Incident Management’ training or similar (to
be developed)
Appendix 1 has a Glossary of Terms and Abbreviations.
Emergency Management Continuing Clinical
1982
2.0 Readiness and Reduction
Education Modules for ambulance officers shall be
developed and maintained to develop skills and
competencies in key aspects of the Ambulance
2.1 Planning and development
Act
Service major incident readiness and response
The Ambulance Service is responsible for the
Ambulance and Communications staff effectively
development and maintenance of:
practice their skills in ambulance and multi-agency
Relationships with other emergency services,
major incident or emergency exercises
including the DHBs, civil defence and key public
Operational Staff who are required to undertake
and private sector agencies that may require an
Specialist Operations will receive appropriate
ambulance major incident response or will impact
specific training. There shall be a national
an ambulance response
alignment, in conjunction with partner agencies, to
Business Continuity Management will be integrated
ensure consistent training in all specialist areas.
Information
into the service; from station level through to core
Training needs analysis is required to further enhance
support departments, such as IT or Finance
the appropriateness of emergency management
Risk analysis processes in their area to ensure
training and education within an Ambulance Service.
priority operational risks are mitigated
Training and education in emergency management
Predetermined or tactical response plans including
for Ambulance Services shall also align appropriately
their integration with other emergency services
with competency frameworks and guidelines of other
Official
and partner agencies. This will include the timely
emergency service partners, as well as with Civil
communication of these plans from the CCCS to
Defence and Emergency Management Agencies.
responding ambulance officers and management
the
The provision of appropriate and consistent
3.0 Response
equipment and materials required for responding to
a major incident. These will be in the form of kits
3.1 Activations, Level of Response1, and
and caches of materials and equipment.
Notifications
under
It is also an Ambulance Service responsibility to
develop its own exercises and / or to take part in
This section outlines the Ambulance activation
multi-agency exercises that clearly test aspects of
mechanisms and levels of response required for an
the service’s major incident response procedures and
incident in the community that may require escalation
plans and enables review and learning to be reflected
to the national level.
in modifications of these procedures. See Part 3
Section 2 for further details.
The aim is to ensure that every major incident is
managed appropriately as early as possible in the
2.2 Training and education
response. This will improve patient outcomes and will
Released
All operational ambulance staff shall have a basic
ensure that the responding ambulance officers are
level of emergency management training from
supported quickly and effectively.
their primary qualifications. To further enhance an
The classification of the type of incident is essential to
Ambulance Service emergency response, ambulance
ensure that appropriate activations and notifications
officers and managers shall have the appropriate
occur. Once an incident has been classified it triggers
level of training for the role they may be required to
certain actions that must be taken by the affected
undertake at the scene of a major incident. Such
training should include, but is not limited to:
Ambulance Service. This will enable quick decision-
making to determine the level of coordination required.
All emergency ambulance staff and CCCS staff to
1This section draws on Ambulance Victoria (AV) Emergency Response Plan 2009. AV’s generous support is acknowledged.
10
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
The major variables that govern the type of response
To allow the identification of correct response levels,
from an Ambulance Service include:
two tools have been developed:
Time to respond to the incident (travel, triage, treat
An Escalation Flow Chart that notes the actions of
and transport)
all ambulance parties in the initial escalation
The complexity of the incident
A Response Matrix to be used by the CCCS.
The number of patients.
3.1.1 Escalation
There are four levels of response:
The Escalation Flow Chart – Figure 1 – provides an
Normal Operations
overview of the actions by the CCCS and the Ambulance
Duty Operational Manager2 in the initial stages of a
Level 1: medium impact on normal operations
major incident. This outlines when to use the Response
Level 2: high impact on normal operations
Matrix and the initial assessment, as well as clearly
Level 3: severe impact on normal operations.
defining the actions to be undertaken by the CCCS and
Duty Manager, based on the level of incident.1982
Figure 1: Escalation Flow Chart
Duty Operations Manager
Communicator and/or Dispatcher
CCCS Duty Manager
Act
(or Ops Management Team/AMb Service Exec on-call)
Use Response Matrix to establish
Duty Ops Manager with
initial estimated response level
CCCS DM:
Incident
received
Undertake initial assessment
Review initial resourcing / initial
response plan
Decide if declaration required
Possible or Actual
and at what Level
Incident identified as possibly
Major Incident or
Ensure Amb Service Exec is
outside of normal operations
Emergency?
informed
Call appropriate Ops
Management Teleconf with
YES
Information
agenda to
Brief management team and
Escalate to CCCS Duty Manager
YES
To develop Ambulance Action
Plan
Escalate to Duty Ops
Request a Major Incident page
Manager – Is He/She
be sent to DHBs if appropriate
contactable?
Immediately dispatch appropriate
resources as per SOP
NO
Official
Page appropriate Ambulance Service
Management Team group
Request and receive a
“Possible Major Incident” Message to
YES
METHANE Report
initiate Teleconference
the
CCCS DM must call the Service
NO
Exec on-call
under
LEVEL 1
Major Incident Declared?
Managed by Duty Ops Manager
YES
LEVEL 2
Page “Declared Major Incident”
Managed by Duty Ops Manager
Level 1, 2 or 3 to appropriate
unless otherwise advised by Amb
NO
Major Incident (MI) Paging Group
Service Exec
Normal Operations
LEVEL 3
Released
Managed by Duty Ops Manager unless
otherwise advised by Amb Service Exec
Continual reassessments based
Page incident updates to
on SITREPS
appropriate MI Group as required
Support the incident via EOC,
CCCS, NCCC etc
NO
Page “Stand Down” to
YES
Stand-down issued?
appropriate MI Paging Group
2Duty Operational Manager is a generic position title that covers a number of positions used across the sector such as Operations Team
Manager, Shift Supervisor, Duty District Manager etc.
PART 2 SEPT 2016
11
3.1.2 Definition and Types of Incident
A major incident or emergency for ambulance is defined as:
Any occurrence that presents serious threat to the health of the community, disruption to the service or
causes (or is likely to cause) such numbers or types of casualties as to require special arrangements to
be implemented by appropriate responding agencies including:
Ambulance Services
District Health Boards (including, for example, hospitals, primary care, and public health)
The Ministry of Health.
AMPLANZ has adopted a set of descriptors for types of incidents applicable to all hazards. These incident
1982
descriptors relate to the ability to access patients, involvement of a lead agency or a comprehensive CIMS
structure and the complexity of the response and its impact on normal services.
Act
Time to respond, triage, treat and transport is another factor that will impact on patient care and normal service
delivery. Therefore this will need to be taken into account in the decision-making process.
Figure 2: Types of Incidents
Type of Incident Description
Complex
Incident that is not routine or it is an infrequently used procedure (e.g. CBR, Airport
emergency, major Civil Defence Emergency Management (CDEM) event (tsunami))
Information
Controlled
Incident that has a lead agency (e.g. Police, Fire, Health, CDEM etc) or comprehensive
CIMS structure in place or a large number of personnel are deployed
Official
Restricted
Where access to patients is difficult owing to hazardous, environmental or security
factors
the
Open
Where there are no issues regarding the access to or egress from patients
Simple
Incident where normal or routine Ambulance procedures apply
under
Released
12
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
3.1.3 Response Matrix Tool
The initial assessment of an incident is the responsibility of the CCCS Duty Manager using the response matrix
below in Figure 3.
Figure 3: Response Matrix
>21
Level 2
Level 2
Level 2
Level 3
Level 3
11–20
Level 2
Level 2
Level 2
Level 3
Level 3
1982
6–10
Level 1
Level 1
Level 2
Level 2
Level 2
Act
Normal
3–5
Level 1
Level 1
Level 2
Level 2
Operations
Normal
Normal
0–2
Level 1
Level 1
Level 2
Operations
Operations
Numbers of
Simple/
Simple/
Simple/
Complex/
Patients
Restricted/
Type of
Open
Restricted
Controlled
Information
Controlled
Incident
Time
<1hr
1–2hr
2–4hr
4–8hr
>8hr
Official
How to use the Response Matrix
1. Estimate the total likely ‘Time’ or duration of the incident for ambulance (travel, triage, treatment and transport)
and plot on the Response Matrix
the
2. Determine the ‘Type of Incident’ from Figure 2 and plot it on the Response Matrix
3. Determine the Severity of the Incident by comparing the time estimate to the Type of Incident, and select the
greater (i.e. further to the right of the matrix)
4. Determine the likely number of patients and plot against the Severity of the Incident on the Response Matrix
under
5. The Duty Operational Manager will be informed and will respond according to approved Standard Operating
Procedures. If the local Duty Operations Manager is not available then CCCS Duty Manager will contact the
Local Operations Management Team and the Ambulance Service Exec to escalate the incident.
3.1.4 Risk Assessment and Response
Once an incident has been classified using the Response Matrix Tool and determined to be outside of normal
business, the CCCS will inform the Ambulance Service Duty Operational Manager.
Released
Ambulance Service Duty Operational Manager, in consultation with the CCCS Manager, will then be required to
confirm that a major incident has occurred and will declare a major incident for ambulance at the appropriate
level. This will be done using information from the incident scene, the CCCS, partner agencies and other reliable
sources. To assist with decision-making the Ambulance Service Duty Operational Manager will need to consider:
The type of incident
The possible time for ambulance to respond (travel, triage, treat and transport) and therefore for patients to
reach definitive care
The location of the incident, relative to ambulance resources and health facilities
PART 2 SEPT 2016
13
The number and status of patients
Coordinate the deployment of resources at the
scene
The availability of ambulance resources
Provide Sitreps using the METHANE format.
Environmental factors, such as weather and time of day
Summary of Triage Officer Role
Health and safety of responding ambulance resources
Assess and triage the number and type of patients
The need to coordinate with other services and the
impact of their operations, in particular, the health
Obtain triage tags and apply triage tags
services.
Inform Ambulance Operations Manager (AOM) of
numbers and status of patients
Begin to coordinate the removal of triaged patients
3.2 Role of the First Crew
to the Casualty Clearing Point(s) (when set up)
1982
The actions of the first-arriving ambulance crew at
Begin to allocate the clinical priority for patients
an incident are crucial to establishing an appropriate
until a Treatment Officer is appointed. (See Section
response to an incident. These are summarised below.
3.6 for role description of the Treatment Officer)
Act
Primary Roles
For full task cards for the members of the first crew –
see Appendix 4.
Ensure the scene is safe. Use ‘STEP 1, 2, 3’ as
appropriate. See Appendix 3
All ambulances will carry Ambulance Major Incident
Folders to assist the first crew. See Part 2 Section
Complete a scene ‘walk around / size up’
3.4.4.
Provide an immediate and initial Incident Situation
Report (Sitrep) utilising the following METHANE3
3.3 Triage
format to the CCCS
The aims of triage, wherever it is done, are not only
Identify and make contact with the Officers in
to deliver the right patient to the right place at the
Information
Charge of other responding services and begin the
right time so that they receive the optimum treatment
coordination process
but also to ‘do the most for the most’, accepting that
Adopt Operations Manager and Triage Officer roles
valuable medical resources are directed to those with
and put on the appropriate Major Incident vests
the greatest clinical need.
Conduct initial triage of the scene
The principles of triage shall be used whenever:
Official
Provide further and regular Sitreps following the
“The number of casualties exceeds the number of
METHANE format to the CCCS
skilled rescuers available”.
Meet, brief and allocate roles to incoming
The first triage decision will be made at the scene,
the
ambulance crews
likely where the patient is found. This will be done
using a primary triage process as outlined in Figure 5.
Provide a handover to a more senior Officer when/if
This is a process performed by the designated triage
requested.
officer at the scene. The Triage Officer should be the
Summary of Operations Manager Role
highest clinically qualified officer available.
under
Ensure scene safety
The process is rapid, taking seconds to complete.
Triage enables the Triage Officer to prioritise patient
Complete scene assessment and reconnaissance
treatment and transport. Patients will be labelled and,
Establish appropriate sites and roles for scene
where appropriate, grouped according to their status.
management
Maintain liaison with responding agencies
Released
3 METHANE is a pneumonic for a standard situation report. See AMPLANZ Part 2 Section 3.4.2 and Figure 5
14
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
Figure 5: Primary Triage Algorithm
YES
MOBILE?
Delayed
Green T3
NO
Dead
Black T0
1982
NO Act
NO
BREATHING?
OPEN
BREATHING?
AIRWAY
YES
YES
Information
DIFFICULTY
YES
BREATHING?
NO
Official
RADIAL
No
Immediate
PULSE PRESENT?
the
Red T1
Yes
under
OBEYS
No
Urgent
COMMANDS?
Yes
Yellow T2
Figure 4 notes a casualty category of ‘Mobile’. This is defined as a person with minor injuries who is able to
walk or be moved without assistance from medical personnel to a designated ‘green’ triage area, where they
Released
will be reassessed.
It is the responsibility of the Triage Officer to ensure that the appropriate label or tag (black, red, yellow or green) is
attached to the patient and that patients are directed to the appropriate location.
The triage tools, including tags, to be used by all Ambulance Services are outlined in Appendix 5.
(Note the triage
tags are under review.)
Triage is an ongoing and dynamic process. Following the primary triage, further triage decisions at the scene are
taken at the Casualty Clearing Point (secondary triage). It is also important to recognise that changing clinical
conditions may require re-labelling and further documentation. Ambulance Personnel will use best endeavors to
access all health information available at the scene including personal medical information adjuncts while noting
the time and resource challenges of triaging and treating in a major incident.
PART 2 SEPT 2016
15
3.4 Communications and information
When communicating, all sections are used in the
report. Where information is unknown, that section is
management
stated as being unknown or that an estimate is being
The most significant factor that will contribute to
provided.
successful command and control of an incident is
‘Number of patients unknown, but is estimated to be
effectiveness of the communications systems and
approximately 50’
protocols. These include:
‘Hazard identification has not yet been completed, but
On-scene communications within the Ambulance
heavy rain looks imminent’.
Service and within the Incident Management Team
If any section of the report is missing, the receiver
Communications between the responding crews,
requests the information from the originator.
the Ambulance Commander and the CCCS
The recognised status changes affected are:
The detail and timeliness of information given to the
1982
Incident Controller, to the CCCS and to health partners
Standby notification (warning of a Possible,
unconfirmed Major Incident)
The tools available to the Ambulance Commander
and CCCS to manage the information, including
Declaration (Confirmed Major Incident or “Not” a
Act
sitreps, action planning and resource requests.
Major Incident)
Update to Major Incident Level (A level or
3.4.1 On-scene communications
information change)
On-scene communications will initially be from the first
Stand-down (Notification that an Agency can stand
arriving ambulance, until a specialised communications
down or that the ‘whole of incident’ stand-down is
vehicle or a senior officer’s car is on scene and able to
given.
act as an Ambulance Command Point.
Standby: The First Crew arriving at the incident is
The on-scene communications point must establish
required to provide an initial sitrep as soon as possible
Information
immediate communications with the CCCS. Continuous
(within 5mins of arriving at scene). This can be an
communications must be maintained at all times.
incomplete METHANE report to the CCCS and the “M”
The principal radio communications system on-site
may be a “Standby” if the situation is unclear.
is the ambulance radio network, through the site
As soon as possible a full sitrep shall then be
communications point. A Communications Officer shall
communicated using the METHANE Report and clearly
be appointed by the Ambulance Commander in complex
stating at the beginning:
Official
incidents. All communications from the scene to the
CCCS will be managed by the Communication Officer.
Declaration4: Major Incident Declarations are
communicated using a METHANE report. The
All responding crews and management must switch to
declaration starts the report with words clearly stating,
the
the on-site communications network (for example, VHF
for Example:
‘Major Incident Declared’.
simplex or UHF) on arrival at the incident scene.
Or, if it is NOT a major incident and a declaration is NOT
Incident and Ambulance Action Plans should
required at scene, then clearly state “M. This is not a
include the establishment of command, control
major incident”. The rest of the METHANE report should
and local operational networks: for both radio and
be used.
under
telephone communications; on-site and off site. It is
recommended that provision be made for ground to air
Updates and changes: These are communicated using
communication capability.
a METHANE report providing the up-to-date information.
It is not necessary to repeat all previously stated
Ambulances may only communicate with the CCCS
information during an update. Where there has been
once they have left the site, with the exception of the
no change state, for example “M., E., T., H., A., all no
break down of the communications system on-site.
change. N. Number of casualties has increased to 15,
all Triage Green. E., no change.”
Declared”.
Released
3.4.2 METHANE
Ambulance Stand-down: It is important that these are
Standardised communications are required around any
also communicated using a METHANE report to provide
notification or status change of major incidents. These
a clear understanding of the situation and prevent
communications need to be readily understood and
confusion. For instance, it would cause great confusion
meet the needs of all agencies. A METHANE report is
to a receiving hospital to receive a stand-down message
the internationally recognised tool for this and is utilised
while patients were still in transit. In-transit patients are
in this plan. See Figure 5.
4Note: Any Ambulance Officer is able to ‘Declare’ a Major Incident based on a thorough scene assessment and / or validated information from
the Public and / or Emergency Services Partners.
16
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
covered in the numbers section. Examples of an inclusion in a stand-down METHANE report from the scene:
“All
patients have departed the scene for Hospital” Or
“35 patients have departed the scene for Hospital. 25 non-injured
have been moved by bus to the Rembrandt Motel by Police”.
Figure 5: METHANE Report
M
Major incident status. Standby / declared / confirmed / stand-down
It is important that each phase or change is communicated immdediately
through the command and communication chain
1982
Act
E
Exact location of the incident
GPS / grid references and / or known landmarks can be helpful
to other parties and agencies
T
Type of incident involved
Information
H
Official
Hazards that have been identified or the potential for them
the
A
Access and egress pathway to the scene is advised
under This should also apply for a Safe Forward Point, Staging Area,
or Assembly Area.
N
Number and approximate status of patients
Released
E
Emergency Services already present, and those needed
Extra Ambulance resources needed
PART 2 SEPT 2016
17
3.4.3 Notifications to Health Partners
1 set of triage tags / labels
The Ambulance Services are required to communicate
1 Ambulance Operations Manager vest
and coordinate with the local, regional and national
1 Triage Officer vest
health services regarding the transport of patients
Appropriate ambulance tactical plans for the local
to the most appropriate health facilities. DHBs and
area
the appropriate hospitals therefore require timely
notification and accurate details of the incident.
The Ambulance Incident Command Notebook should
be used by all First Crews arriving on scene in major
The CCCS will develop and maintain procedures that:
incidents, and then by Ambulance Operations Managers
Inform the DHBs of possible and declared major
in the majority of Level 1 or 2 incidents where simple
incidents. This will be achieved by paging / texting
management structures are in place. The notebook
information to DHB Operational Points of Contact5
provides:
Facilitate teleconference/s between the Ambulance
At the Front (multiple copies of): METHANE reports,
1982
Service, receiving DHB/s and the CCCS to enable
formats for command structures and communications
efficient information transfer. The teleconference
networks, maps, Ambulance Action Plans (AAP), patient
numbers will be communicated to the DHBs on or
tracking, decision / communications logs, debrief
Act
prior to a declaration of a major incident.
checklist and Commanders report.
The leader of the teleconference will be the
At the Back: Aide de memoire for responding
Ambulance Commander, Ambulance Operations
ambulances and managers as to their initial roles,
Manager and / or the Ambulance Service Duty
including triage algorithms.
Executive (Ambulance Service Controller) depending
See Appendix 6 for an example of notebook pages.
on availability and scale of the incident. The format
There is ongoing developments relating to electronic
of the teleconference shall follow a METHANE report
patient information management. As tools come on line,
plus information such as arrival times at the receiving
Ambulance Services will incorporate these appropriately
health facilities. The teleconference will be a short
into their Major Incident Management.
Information
briefing (5-10 minutes maximum). In-depth planning or
clinical discussions should be held separately.
Level 2–3 incidents
It is the responsibility of the DHBs to maintain their
For more complex and prolonged incidents (Level 2 or
operational points of contact and to ensure information
3) or where there is a comprehensive management
is cascaded to the appropriate operational staff and
structure in place for ambulance and also the incident as
executive management within their organisations.
a whole, then an Ambulance Incident Command Board
Official
shall be used. The command board has the following:
For incidents with large numbers of casualties,
communications notifying the hospital of every arriving
Event and Communications Log forms
ambulance and status of patients being transported,
the
Incident and Ambulance Organisation Chart
may be suspended. This is owing to resource
Situation Report forms (based on METHANE)
constraints in the receiving hospitals.
Patient / Casualty Tracking forms
3.4.4 Information Management tools
Ambulance Action Plan form
Ambulance Staff Tracking form
under
At the scene, in the CCCS and in the ASEOC (Ambulance
Ambulance Resource Tracking form
Service Emergency Operations Centre), comprehensive
information management is required to ensure that
Small whiteboard/s plus pens.
coordination between partners, communication
See Appendix 6 for examples of forms.
regarding resource provision and the appropriate and
safe transport of casualties is maintained.
Emergency Management Information Systems (EMIS)
Level 1–2 incidents
The Ministry of Health and the Ministry of Civil Defence
and Emergency Management both have EMIS (for
Released
To assist with this, the First Crew on scene, the
example, E.Sponder). Ambulance Services currently
Ambulance Operations Manager and the Ambulance
access and utilise the Health EMIS.
Commander are provided with tools to provide quick
reference to procedures and specific responses
For complex and prolonged responses, the use of an
information, and access to appropriate forms.
EMIS may be required at the scene by the Incident
Management Team. Should this occur, the Ambulance
These tools will be held in Ambulance Major Incident
Commander will need to request the appropriate
Folders in all ambulances. These folders will contain:
resources from the ASEOC. For example, a laptop with
An Ambulance Incident Command Notebook
mobile communications etc.
5The DHB Operational Points of Contact may differ from the DHB Single Point of Contact as specified in the NHEP. They may include
emergency department clinicians or managers, duty managers, emergency planners, telephonists and/or executive managers. It is a DHB
decision as to who should receive communications from the CCCS.
18
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
3.4.5 Integration with the Incident Management Team
Figure 6: Simple Command Structure
It is a requirement of CIMS that the information
systems of all responding agencies be integrated to
provide a single set of information. This will enable
Incident Controller
the Incident Controller to maintain a comprehensive
or Lead Agency
overview of the situation and therefore enable the
Officer In Charge
development of appropriate incident action plans. To
facilitate this, the Ambulance Commander will:
Provide the Incident Controller with regular and
Ambulance
comprehensive Ambulance Sitreps
Operations
Manager
Action specific orders from the Incident Controller
relating to the overall management of the incident
CCCS
1982
while ensuring that appropriate patient care and
ambulance staff safety is maintained
Provide the Incident Controller with the Ambulance
Treatment Act
Triage Officer/s
Action Plan (AAP) and modify the AAP if necessary
Officer/s
for the improvement management of the incident
while ensuring that appropriate patient care and
ambulance staff safety is maintained
Control: provides coordination across agencies
Inform the Incident Controller of changes to
Command / Control: directs the operational
Ambulance resourcing
response within an Ambulance Service at the
scene
Request, through the Incident Controller, any non-
ambulance resources required by Ambulance
Communications
Services.
Information
The physical placement of the Ambulance Commander
CIMS components of control, logistics and planning
with the Incident Management Team will facilitate the
/ intelligence are undertaken by the Ambulance
communication and coordination within the incident.
Operations Manager (AOM) and Operations are
undertaken by the Triage and Treatment Officers.
3.5 Command Structure and Scene
Ambulance roles such as transport, communications
Official
Management
etc, will be undertaken as part of other roles. The
Safety Officer role is the responsibility of the AOM.
This section provides ambulance managers with
the
a guideline as to the roles required and scale of
structure that may need to be set up to manage two
3.5.2 Comprehensive Command Structure
examples of incidents. These examples note the
A Command Structure for long duration Controlled
modular and expandable nature of CIMS.
and / or Complex Incidents (Level 2 or 3), or simple /
restricted incidents equivalent to Level 1 or 2 (short
under
3.5.1 Simple Command Structure
duration but with large numbers of casualties) will
require the Ambulance Commander or Operations
A simple command structure for normal operations
Manager to decide how the Ambulance and CIMS
and Level 1 incidents or Open, Simple, Restricted or
roles will be implemented and therefore the staffing
Controlled incident of short duration (< 4hrs) and a
required. This will need constant reassessment as part
small number of patients (< 6 patients). See Figure 6.
of the ambulance incident action planning processes.
See Figure 7 for the structure.
It is recognised that the ability of an Ambulance
Released
Service to fill all roles or functions in a full CIMS
structure may be limited. Therefore roles may need
to be prioritised and / or combined to match the
personnel available.
PART 2 SEPT 2016
19
There are a number of priority roles that need to be in
5. Longer-term logistics and planning and intelligence.
place immediately by ambulance officers, then roles may
The following roles are discretionary and will be
be able to be combined with priority roles, and others
requested and deployed by the Ambulance Commander
that may wait until more resources arrive. As a guide, the
depending on the complexity (type, duration and scale)
priority of responsibilities and roles should be:
of the incident: Communications Officer, Aviation
1. Incident management and coordination with partner
Coordination, and Administration Officer.
agencies, including safety and communications
The Ambulance Commander will have to decide quickly
2. Triage
to request support from the ASEOC via the CCCS to
3. Treatment
enable appropriate resources to be deployed from the
4. Immediate transport (loading / parking) and
most appropriate Ambulance Service.
logistical management
Figure 7: Complex Command Structure
1982
Act
Ambulance
Incident
Service
CCCS
Controller
Controller
CIMS Incident Management Team
Ambulance Service EOC (ASEOC)
Ambulance
Information
Admin Officer
Commander
Planning &
Safety Officer
Intelligence Officer
Official
Communications
Logistics Officer
Ambulance
Officer
Operations
the Manager
Aviation
Sector Officer
Sector Officer
under
Coordinator
Sector 1
Sector 2
Transport
Triage
Officer
Officer/s
Treatment
Officer/s
Released Sector 1
Sector 2 (all roles not shown)
Control: provides coordination across agencies
Command / Control: directs the operational response within an Ambulance Service at the scene
Communications
Priority roles in dark colours, other roles to be combined with priority roles or resourced depending on the incident
and resource availability. This is a Commander decision.
20
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)

1982
Act
3.6 Summary of scene roles and
Triage Areas and is responsible to the AOM or Sector
Officer.
responsibilities
Ambulance Treatment Officer: Responsible for
Key scene roles are summarised below. Task cards for
coordinating patient treatment, liaising closely with the
all roles are in Appendix 7.
Transport Officer and the Triage Officer. To delegate
Ambulance Commander (AC): The officer responsible
tasks to all medical and other personnel at the Casualty
Information
for scene management, all medical resources for
Clearing Post. To report to the AOM or Sector Officer.
complex and prolonged incidents. The AC will be
Ambulance Transport Officer: The officer responsible
part of the Incident Management Team (IMT) when
for all transport, loading and parking management in
an IMT has been established for controlled or
consultation with the AOM. Responsibilities include:
complex incidents (Level 2 or 3 Incidents). The AC is
allocating vehicles for transport, according to patient
responsible for the safety of all health and ambulance
priority, ensuring that suitable access and egress is
Official
personnel on scene for this scale of incident. This
available into the ambulance loading point at or near
is an incident management role and therefore shall
the Casualty Clearing Point (CCP), for the efficient use
not have patient care responsibilities. The AC is
of vehicles, establishing an appropriate ambulance
the
responsible to the Ambulance Service Controller.
parking area. Reports to the AOM or Sector Officer.
Ambulance Operations Manager (AOM): The officer
Ambulance Administration Officer: This officer will
delegated with the responsibility to manage operational
be assigned to the Ambulance Commander at the
activities of the incident at the point of patient contact
scene. The responsibilities will be to maintain the
and the site role most commonly established for open
AC’s decision and communications log, communicate
under
simple, restricted or minor controlled incidents (Level 1
on behalf of the AC, if appropriate, and act as the
or 2 incidents). This is an incident management role and
communications officer (if no specific person is
therefore shall not have patient care responsibilities.
appointed). There may be an Administration Officer
The AOM is to take on the role of Ambulance Safety
attached to the AOM if resources allow.
Officer if one is not appointed.
Ambulance Communications Officer – on-site:
Ambulance Sector Officer/s: A major incident may be
The officer who establishes, and is responsible for,
sufficiently large to divide into sectors. A Sector Officer
effective communications on-site. May be deployed
is responsible for managing a sector of an incident.
from the CCCS or from the local Ambulance Service.
Released
They are responsible to the Ambulance Operations
Ambulance Logistics Officer:
Manager.
This role is responsible
for the systems and management relating to control,
Ambulance Safety Officer: The officer responsible for
monitoring and re-supply of all personnel, materials
ensuring the overall safety of ambulance and other support
and equipment at major incidents.
personnel at the incident scene. Reports directly to the AC
when established or more commonly to the Ambulance
Responsible to the AC and may only be required for
Operations Manager. Will work very closely with the lead
prolonged controlled or complex (Level 2 or 3) incidents.
agency or Incident Safety Officer if established.
This role will also work closely to the Incident Logistics
Ambulance Triage Officer: Responsible for the triage of
Manager in such incidents.
all patients in an incident or sector. In command of all
PART 2 SEPT 2016
21
The Ambulance Logistics support will be provided by
The ICP is where the Incident Controller and
the ASEOC in the majority of incidents.
members of the Incident Management Team direct
Aviation Coordinator: This role will be provided by the Air
responsibilities during an emergency situation.
Ambulance Service and is responsible for landing zones
Every incident will have an ICP. The ICP is critical
and safety of operations. This role is responsible to the
to command and control and is the point where the
Operations Manager/Commander for the coordination of
Incident Controller will manage the whole incident.
all aviation resources at the incident scene.
For smaller incidents, the ICP may move with the
Ambulance Planning and Intelligence Officer(s):
Incident Controller. For larger incidents, the ICP may be
These roles are responsible for assembling, maintaining
a vehicle (fire appliance, police car or command unit),
and analysing all information available relating to the
trailer, tent or building.
ambulance and wider incident response. This will include:
Ambulance Command Point (ACP)
Resource summaries
1982
The Ambulance Command Point is responsible for
Analysis that will identify and prioritise issues of
managing all ambulance activities at the scene and
concern
ideally should be co-located with, or very near, the ICP.
Act
Development or revision Ambulance Action Plan
‘Ambulance Command Point’ will initially be the first
(AAP) objectives and actions for approval by the AC.
ambulance vehicle on the scene, using a red flashing light.
The only ambulance or health response vehicle to display a
Depending on the scale of the incident and the
flashing light will be the scene Ambulance Command Point
ambulance staff available these roles may be two
where it is safe to do so and where it does not conflict with
persons or combined.
other agency protocols (e.g. airport emergency plan).
Responsible to the AC and may only be required at the
scene for prolonged controlled or complex (Level 2 or
Sectors
3) incidents. This Officer(s) will also work closely to the
For complex and large scale incidents it may be
Incident Planning and Intelligence Managers in such
necessary to divide a scene into sectors. This aids
Information
incidents.
the management and accountability of the incident
In the majority of incidents, the Planning and Intelligence
by breaking down the span of control and allowing
roles will be provided by the ASEOC and will be
individual operations.
responsible to the Ambulance Service Controller.
Sectors may be defined by the Incident Controller for
Medical, Nursing and allied Health personnel:
overall use, or by individual agency commanders for their
Official
Appendix 7 also contains task cards for both PRIME6
agency’s needs. Several numbering variations exist for
doctors and nurses as well as for those health
sectorisation and common sense and logic should be
personnel who may volunteer or be assigned by their
applied, along with an understanding of the conventions
the
organisation to assist at the scene.
that apply to other agencies. See Appendix 8 for examples.
Ambulance Liaison: It will be important that
A sector can also be established to fulfil a special
communication is maintained directly with the receiving
purpose or field of operation. For example, a large
emergency departments, hospitals or DHBs, and / or
Forward Triage Area may be considered a sector. Often
the partner agencies, such as CDEM. The Ambulance
the combined area of CCP and transport facilities is
under
Service Controller will appoint Liaison Officers to the
defined as a sector with a Sector Officer managing the
appropriate facilities for the particular incident. A
Treatment Officer and Transport Officer and associated
Liaison Manager may be required if there are a number
incident facilities.
of liaison points in place. This role is based in the
Ambulance command within a sector lies with the Sector
ASEOC to support the Ambulance Service Controller
Officer who reports to the Ambulance Operations Manager.
with the information flow to and from partner EOCs.
See Part 3 and Appendix 15 for task cards etc for the
Assembly Area
Liaison Managers or Officers.
The Assembly Area is where resources are organised
Released
3.7 Site Set up
and prepared for deployment. It may include the
provision of crew welfare and maintenance facilities.
There are consistent site or scene locations or
An Assembly Area would normally be located away from
facilities required by CIMS as well as those specialist
an incident at an established facility, for example, an
facilities required by Ambulance. Below is a summary
ambulance station. Assembly Areas are for support
of these facilities and their roles. See Figure 8.
rather than being operational.
Incident Control Point (ICP)
6PRIME = Primary Response In Medical Emergencies.
22
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)

1982
Act
Staging Areas
Forward Triage
Staging Areas are locations where resources are
Forward triage is carried out in the field to identify and
gathered before being despatched to a Safe Forward
triage patients in a priority order to their removal to a
Point or directly to an incident area. As an incident grows,
Casualty Clearing Point. In large scale incidents, where
there may need to be more than one Staging Area.
there are a number of sectors, forward triage may be
Staging Areas:
required in each.
Provide a safe location for resources awaiting
Triage wristbands / tags should be attached in the field,
Information
assignment
where possible, and re-assessed when patients enter
the triage area.
Keep track of resources
Casualty Clearing Point (CCP)
Provide a check-in area for all arriving personnel
This area is made up of two areas:
Allow the Incident Management Team to plan for
resource use
Triage Area: This is normally a point positioned at
Official the entrance of the CCP. It is essential this area
Must be located in a safe area
does not become blocked – a continual flow of
Should have separate entrance and exit routes
patients is essential. Patients should be re-triaged
the
at this point (and tagged if not already attached)
Should be large enough to accommodate
prior to their flow through to the appropriate
anticipated levels of resources
priority sections in the treatment area. Uninjured
Reduce traffic congestion.
patients and the deceased must be removed to two
separate areas and not enter the treatment area.
Ambulance Parking Area
under
Treatment Area: This must be a safe area large
The place designated at the scene of a major incident
enough to accommodate the anticipated number
(forward of the Assembly Point) where ambulances can
of casualties. It should be between the Triage Point
park, thus avoiding congestion at the entrance to the
and the ambulance loading area and should be
scene or at the Ambulance Loading Point. These areas
separated into three sections:
are also suitable for staff briefings, refreshments and
re-stocking of equipment. This area may be part of an
Triage 1
Red
Incident Staging Area.
Triage 2
Yellow
Released
Safe Forward Point (SFP)
Triage 3
Green
The SFP is a safe facility or location near the incident
Specific priority areas should be designated by some colour
from which forward operations can be supported.
identification e.g. coloured flags, tarpaulins or signage.
Landing Zone (LZ) or Helipad (HP)
There may be more than one CCP.
Specific area that has been identified for safe arrival,
Ambulance Loading Point (ALP)
landing and departure of helicopters. Consideration needs
to be given to night operation requirements (i.e. lighting).
This is an area (preferably of hard standing) in close
proximity to the CCP, where ambulances can manoeuvre
and load patients.
PART 2 SEPT 2016
23
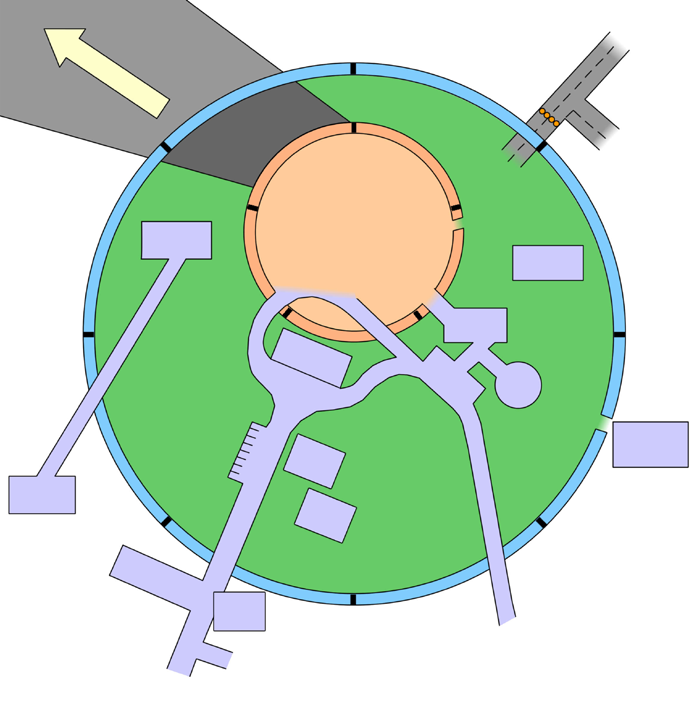

Figure 8: Major Incident Footprint
Scene Access and Egress
It is expected that the majority of casualties will be transported by road.
A considerable number of emergency and support vehicles will be travelling to and from the scene.
It is recommended that the Ambulance Commander/Ambulance Operations Manager, in liaison with the Police and
Fire Commanders, establish clearly marked entry points and exit points to avoid congestion and improve vehicle flow.
All keys should remain in the ambulances unless specified otherwise.
1982
Act
W
Cordon
ind dir
ec
Road
tion
Closures
Cordon
Possible need
D
for E
iversions
vacuation
er
Uninjur
ut
Incident Site
ed
Information
Evacuation
O
Assembly
Point
escue
nner I
Forward
Reception
Triage + R
Area
Pocil
Casualty
Official
e
Clearing
/ F
Point
tion
ir
S
e
afe F
/
or
R
w
P
ar
A
e
oin
d
mbulanc
Evacua
s
t
Loading PT
cu
the
e
e
Helipad
Ambulances
Staging Area
Welfare, Friends
Inciden
C
and Relatives
Con
t
tr
under
ol
asualt
Point
y E
Welfare
v
Assistance
Ambulanc
acua
Command e
P
tions
oint
Ambulanc
Parking A e
rea
Exit
Scene
Only
Released
Access
Control
Ambulance Route
to Hospital/s
Assembly
Area
24
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
3.8 Coordination with Health,
It will also be necessary to coordinate with non-health
organisations and perhaps access their resources and
Emergency Services and other Agencies
expertise. It is necessary for senior ambulance officers
In mass casualty incidents it is unlikely that any single
to be fully briefed on:
agency will have the required resources to meet the
The role, capacity and capability of the emergency
needs of a response. The CIMS approach provides for
services and non-government organisations (NGOs)
coordination across all responding agencies.
e.g. Salvation Army and NZ Red Cross, private
sector organisations and Civil Defence Emergency
3.8.1 Health
Management Organisations
A mass casualty incident may impact severely on
The communication channels with these
the local, regional and national health system. The
organisations to be able to access appropriate
coordination of patient transport, according to priority,
resources.
1982
to the most appropriate health facility is therefore
An Ambulance Service is responsible to ensure that
critical. All senior ambulance officers who may fulfil the
Ambulance Commanders and Operations Managers
Ambulance Commander or Operations Manager roles
have access to contact points for appropriate agencies
at scene are to be fully briefed on:
Act
that have access to specialist support services7.
Capacity and capability of the local and regional
receiving health facilities
3.9 Media
Emergency plans of the local DHBs as they impact
Media representatives will arrive at the scene following
on Ambulance Service
a major incident. Media will also go to hospitals and
any other site where there is a possibility of acquiring
The communication channels with receiving health
information on the incident.
facilities or DHBs to coordinate patient transport
An Ambulance Service will receive inquiries from
The communication channels with Regional Health
the news media seeking information on the incident
Information
Coordination and / or National Health Coordination
including the numbers of injured and deceased etc.
structures.
Ambulance officers will be aware of and follow their
An Ambulance Service is responsible to ensure that
organisation’s media policies. For all incidents, an
Ambulance Commanders and Operations Managers
Ambulance Service Public Information Manager (PIM)
have access to appropriate contact points for the local
will be available to coordinate inquiries from the media
and regional health facilities and services.
with appropriate other agencies. This person will be
Official
For all Level 2 and 3 incidents, the DHBs will be
based initially at the Ambulance Service EOC.
informed via the notifications system as part of the
For large scale incidents, where there is a clear CIMS
activation of the ambulance response. DHBs can
the incident management team in place, all media inquiries and
choose to be informed for Level 1 incidents. See Part 2
the release of information to the media will be managed by
Sections 3.1 and 3.4.
the Incident Public Information Manager responsible to the
Incident Controller. Public Information Management will also
3.8.2 Emergency Services and other Agencies
be part of the CIMS Incident Action Plan.
under
All senior ambulance officers, who may be appointed
For smaller incidents, the lead agency (for example,
to the Ambulance Commander or Operations Manager
Police or Fire) may request all news releases be
roles at the scene, will need to have access to
directed to their Public Information Managers or a
information on tactical ambulance responses for
Senior Officer.
specific hazards in their operational area. These will
be in the form of ambulance tactical plans and will
In all cases Ambulance Services will coordinate media
be developed in coordination with other responding
inquiries and release of information with the Incident
agencies and the ‘owners’ of the plans (for example,
Controller’s Public Information Manager.
an airport company, stadium event management etc).
Released
These plans will be developed by the Ambulance
Service and be accessible from the CCCS CAD system,
with appropriate accessible backup copies.
7Note: This does not necessarily mean an Ambulance Service maintaining lengthy lists of agencies etc. For example, many CDEM
organisations have agreements with the NGOs and contacts with private sector service providers.
PART 2 SEPT 2016
25
3.10 Resources and Equipment
and emergency services partners. All areas of
operations require specific and specialised education
All potential Ambulance Commanders and Operations
and awareness. Many of these areas are used as part
Managers shall be made aware of the resources and
of local normal business but may also be required as
equipment that may be available in their service area.
part of a major incident response. These include:
These may include:
Land Search and Rescue
Ambulance major Incident cache of medical
materials and equipment
Marine Search and Rescue
DHB medical materials etc that may be accessible
Mines Rescue
to a pre-hospital response
High Angle Rescue
Specialist materials, equipment, services and
Helicopter response.
personnel from a partner emergency service or
1982
support agency that may be accessible to a pre-
There are a number of national Special Operations
hospital response. For example, urban search and
Teams that may be deployed regionally or nationally.
rescue (USAR) equipment, CDEM logistics.
Below are summaries of their current roles.
Act
There will be a defined procedure for an Ambulance
Special Emergency Response Teams (SERT)
Commander or Operations Manager to request
These teams are required to respond rapidly at the
resources as part of METHANE reports and Ambulance
request of partner emergency services, Ambulance
Action Plans sent to the CCCS and the ASEOC.
Service management and CCCS. SERT are deployed
Ambulance officers shall be regularly trained in the
nationally. SERT Officers are under the command of
deployment and use of ambulance major incident
the lead agency at the Scene, but remain under the
caches. These will also be used in major public events
control of the Ambulance Service. SERT operate with
to improve familiarity with the materials and equipment.
the following groups or areas:
In all emergency, PTS and event ambulances, there
Police Armed Offenders Squad (AOS)/Special Tactic
Information
is an Ambulance Major Incident Folder. This folder
Group (STG): The SERT team is trained to operate
contains role task cards, triage tags, aid memoires etc.
with these two groups. The distinction has been that
See Part 2 Section 3.4.4. These folders will form part
Armed Offenders Squad (AOS) carries out all armed
of the ambulance manifest and be audited as such.
incidents and the STG deal with hostage situations
and counter-terrorist activity. SERT trains with both
To assist managers in the Ambulance Commander or
of these groups and is regarded as part of the Police
Ambulance Operations Manager roles a number of Official
operation. The role is to provide clinical care in
tools have been developed. These include:
the hot/warm zone (see Appendix 1 for definition),
Ambulance Incident Command Notebook: See Part 2
SERT officers wear the same protective equipment
the
Section 3.4.4 and Appendix 6.
as the police and use police radios during AOS/STG
operations.
Ambulance Incident Command Boards: See Part 2
Section 3.4.4 and Appendix 6.
Land Search and Rescue (SAR): SERT often support
Police by providing medical care to all searching
3.10.1 Major Incident Vests
personnel and the lost or injured party when found.
under
These can be very labour intensive with a number of
There are standard vests to identify ambulance
hazards. Care of the searching staff is the major role,
incident management and roles at the scene of a
including assessing and treating reactively and also
major incident.
monitoring staff during prolonged searches.
These need to be consistent across all Ambulance
Marine Operations: SERT works closely with Police
Services to ensure all ambulance roles are clearly
on security and mass casualty incidents at sea.
identified.
Specific training includes water rescue and patient
See Appendix 9 for the details.
retrieval. SERT are also involved with the inter-service
Released
preparation and operation to intercept illegal ‘boat
3.11 Specialist Operations
people’ with the role being to assess the health of
passengers, organise evacuation, in the event of
To be able to access patients quickly, Ambulance
serious illness or injury and help in a decision-making
Services have developed skills and strong
role to quarantine the vessel if necessary. As with AOS
relationships with other emergency services and
operations, SERT officers also provide care to Police if
agencies to undertake specialist operations. There is
required.
a mix of local and national approaches to meeting the
needs of patients, the local operational environment
26
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
Urban Search and Rescue USAR
3.11.2 Pre-hospital Responses by DHBs and other
There are currently four USAR teams and these are
organisations
deployed nationally. The ambulance sector provides
There are Ambulance response procedures for PRIME8
the USAR Team Medics. This role is firstly to ensure
Doctors and Nurses as part of a pre-hospital response.
health and welfare of the USAR staff. The treatment
and extrication of trapped patients would be completed
There are currently few formal pre-hospital medical
with consultation and active participation of the USAR
responses developed as part of DHB or hospital
Medic. USAR Medics may also be members of SERT.
emergency plans. DHB and hospital emergency plans
USAR Team Medics, when deployed, are under the
need to consider the deployment of these resources
command of the USAR Officer incharge.
in support of the pre-hospital response and formalise
the notification, activation, roles and responsibilities,
Chemical Biological Radiological (CBR)
training and equipping of these resources.
CBR trained officers work as part of AOS operations (as
There is also a NZ Red Cross volunteer pre-hospital
1982
part of SERT) and / or Fire Service hazardous materials
response capability that may be deployed if requested.
(HazMat) operations (as part of the Ambulance CBR
The Ambulance Commander may request specialist
Team). Both are deployed nationally. All officers are
medical and nursing resources to assist with the
Act
trained to Level 3 Chemical Protection, which involves
general pre-hospital response and to undertake
the wearing of a chemical resistant splash suits and
specialist procedures. There are clear doctor and
self-contained breathing apparatus progressing to
nurse task cards as well as other task role cards in
use of chemical suits. CBR Officers are trained in
Appendix 7.
decontamination procedures for both walking and
stretcher patients and the problems associated with
Note: In a pre-hospital response, all specialist medical,
both. Level 2 protection is used at ‘clandestine labs’
nursing and first aid resources working at the scene
(Clan labs) in association with ballistic equipment as
will be under command of the Ambulance Commander
part of an AOS operation.
or Operations Manager.
Information
CBR trained officers working in a HazMat operation
are under the command and control of the Ambulance
3.11.3 Activation of Responses by DHBs and other
Commander or Ambulance Operations Manager on
organisations
scene. In an AOS operation, the CBR trained officers are
Requests for health or medical support (from a
under the command of the lead agency at the scene.
DHB, for example) shall be done by the Ambulance
Ambulance Rescue
Commander directly to the agency concerned and in
Official
coordination with the Incident Controller.
There is currently one rescue squad, trained in 4WD,
High Angle rescue, basic rescue techniques and
Requests for non-health support (from the Salvation
the
swift water rescue. Team members are activated by
Army, for example) or from a voluntary agency (from
CCCS and respond urgently to all cases. Specialist
the NZ Red Cross, for example) shall be done by the
equipment includes 4WDs, ropes, abseiling hardware,
Ambulance Commander to the Incident Controller.
PFDs (Personal Flotation Devices), throw bags,
stretchers with mule wheel, winches, and an A-Frame
4.0 Recovery
for high angle rescue.
under
The process of recovery for an Ambulance Service
is defined as the re-establishment of normal service
3.11.1 Activation of Ambulance Specialist Operations
delivery after a major incident. This process should
A specialist response shall be activated in the
start as soon as possible in the response phase
following ways:
and be aligned with Ambulance Service business
continuity plans. Ambulance Services will be required to
By the Ambulance Commander or Ambulance
contribute to the overall recovery of the health services
Operations Manager at scene in consultation with
and community. It may also be that, dependent on
the lead agency or Incident Controller. This will be
the incident, there may be a new ‘normality’ for the
Released
done through the CCCS using normal processes
community. Ambulance Services will have to realign
and possibly in consultation with local Ambulance
themselves appropriately as part of the recovery
Service management.
OR
process.
By Police or Fire directly via the CCCS for SERT,
All logs and notes made during the incident will need
USAR or CBR resources. The CCCS will inform
to be correlated in case of possible public inquiries as
Ambulance Service management.
to the effectiveness of the overall management of the
response.
8PRIME = Primary Response In Medical Emergencies.
PART 2 SEPT 2016
27
It is envisaged that even in a moderately sized major
Crews lacking expertise or skills
incident there will be an effect on staff, supplies,
Equipment failures
equipment, finance and vehicles. Areas requiring
consideration for recovery will include, but should not be
Significant impact on non-operational
limited to:
departments of the Ambulance Service
Staff welfare/debriefs
External criticism or triggers impacting
perceptions of the ambulance response
Rosters
Or other issues that may trigger a response
Leave
from the Ambulance Service’s Reportable
Operational review and learning
Events Management System.
Development of new models of operation where
and when required
4.1.2 Debrief and Reporting tools
1982
Consumables (medical/fuel)
An Ambulance Commander and staff who worked at
the scene or in the CCCS as part of the response, will
Equipment
be required to take part in one or more of the following
Act
Vehicles (servicing repairs etc)
processes:
Finance and cost recovery.
Hot or Scene debrief
Ambulance Service management is responsible for
This is the lowest level of debrief but may be the most
ensuring that the majority of the above areas are
important. All responding ambulance officers and
managed. This may require the appointment of a
communications staff should take part in this debrief.
Recovery Manager. See Part 3.
This is a relatively informal process and should follow
the debrief template as noted in the Ambulance
4.1 Ambulance Debrief Processes
Incident Command Notebook. This should occur as
Information
and Tools9
soon as possible following the incident. See Appendix
6.
4.1.1 Debrief aims and requirements
Ambulance Commander’s After Action Report
The aim of the debrief process is two-fold:
For a significant incident, the AC will be required to
complete an After Action Report. The aim here is to
To identify and acknowledge where the response
communicate the findings from the incident scene,
Official
went well and ensure that these experiences are
including learning and acknowledging excellence.
shared
This report will contribute to the wider Ambulance
To identify where improvements in the response
Service debrief and reporting process. This should be
the
is required and develop a plan of action to ensure
completed within one month of the incident. An After
that learning occurs.
Action Report Template is in Appendix 10.
An incident debrief and / or reporting is required:
Ambulance Service Debrief
Following all Level 2 and 3 incidents
This process will be managed by the Ambulance
under
A level 1 incident (or where a major incident should
Service Controller and may be delegated to an
have been declared) where there has been one or
Ambulance Service Recovery Manager (if appointed).
more of the following:
This process will be more formal and will draw in all
relevant staff; operations, communications (CCCS),
Injury to or safety issues for Ambulance Officers
and non-operations. This debrief should occur within
Poor clinical outcomes of patients possibly
two months of the incident. The guidelines and
attributable to the Ambulance scene
documentation for this level of debrief are in Part 3.
management
Released
Communications failures or issues
Failure of SOPs or Tactical Plans that have
impacted on response
Ineffective coordination between responding
agencies
9This section draws on the NZFS Incident Management – Command and Control Technical Manual Aug 2009. Section 6 pages 1–19. The
NZFS Special Operations support is gratefully acknowledged.
28
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
AMPLANZ Part 3:
Ambulance Service Approach
For Ambulance Service Managers working in all areas of the emergency management cycle
September 2016
1982
Act
Content
Part 1: Introduction to AMPLANZ and Emergency Management for the
Ambulance Sector
Information
Part 2: Consistent Operations at the Scene
Part 3: Ambulance Service Approach
1.0 Introduction
30
3.5 Ambulance Service Emergency Response Management Structure 34
2.0 Readiness and Reduction
30
3.5.1 Simple Ambulance Service Emergency Response Management
Structure
34
2.1 Risk Management and Planning
30
3.5.2 Comprehensive Ambulance Service Emergency Response
2.1.1 Business Continuity Planning
30
Management Structure
34
Official
2.1.2 Ambulance Tactical Planning
30
3.5.3 CCCS Incident Management Structure
36
2.1.3 Inter-agency Planning
3.6 Ambulance Operations and CCCS roles and responsibilities
38
Inter-Ambulance Service Cooperation
31
2.2 Exercising
31
3.7 Ambulance Non-operational staff: roles and responsibilities
40
the
2.3 Training and education
32
3.8 Coordination with health, emergency services and other agencies
40
2.4 Review and Audit
32
3.8.1 Health coordination
41
3.0 Response
32
3.8.2 Emergency Services and Other Agencies
41
3.1 Activations, Level of Response, and Notifications
32
3.9 Media
41
under
3.2 Activation based on national and regional warnings
32
3.10 Ambulance Service Resources and Emergency Operations Centre 42
3.3 Communications
32
3.10.1 Ambulance Service Resources
3.3.1 From an Ambulance Commander:
32
3.10.2 Air Desk
42
3.3.2 From a health or CDEM EOC
32
3.10.3 Ambulance Service Emergency Operations Centre
42
3.3.3 Ambulance Operations Management briefing
33
4.0 Recovery
42
3.3.4 Major Incident Notifications within Ambulance Services and to
4.1 Ongoing Impact of the Incident
42
partner agencies
33
3.3.5 Call back
33
4.2 Operations and CCCS: Roles and Responsibilities in Recovery
43
3.4 Information management
33
Released
3.4.1 Tools
33
4.3 Non Operational Staff: Roles and Responsibilities in Recovery 43
3.4.2 Emergency Management Information Systems (EMIS)
33
4.4 Ambulance Debrief and Reporting Processes
43
3.4.3 Integration with the Incident Management Team
33
4.4.1 Debrief aims and requirements
43
4.4.2 Hot or scene debrief
43
4.4.3 Ambulance Service Debrief
43
4.4.4 Ambulance Service Major Incident Report
43
Part 4: National Crisis Coordination Centre
Appendices
1.0 Introduction
and agencies such as New Zealand Fire Service
(NZFS) are required to develop tactical or operational
AMPLANZ is divided into four parts plus an overview
response plans by law. The key preparedness activity
document. This is Part 3 and focuses on the activities
by Ambulance Services will be to ensure appropriate
to be undertaken by Ambulance Service Management
tactical response plans are developed, exercised and
in all areas of the emergency management cycle.
communicated in coordination with other response
This document should be read in conjunction with
agencies and the owners of the facilities.
Part 1: Introduction to AMPLANZ and Emergency
Management for the Ambulance Sector and Part 2:
2.1.1 Business Continuity Planning
Consistent Operations at the Scene.
Ambulance Services are required to have
2.0 Readiness and Reduction
comprehensive business continuity policies
management (BCM) and processes in place that
include the development and management, as well
1982
2.1 Risk Management and Planning
as testing, of plans. AS/NZS 5050:2010 and ISO/TS
22317:2015 are appropriate references for BCM Plans
All Ambulance Services are required to identify, analyse,
shall be developed for all stations, service departments
Act
treat and monitor all risks facing their organisations.
(operations and support or core department) ensuring
An Ambulance Service’s risk management policies and
they are integrated across the service. Where risks are
frameworks should be based on AS/NZS ISO 31000
identified, the Ambulance Service will develop a strategy
Risk Management Principles and Guidelines1.
to treat these risks.
The major incidents covered by the AMPLANZ are
Business Continuity Plans (BCPs) shall be fully
normally considered as having risk of:
accessible to and understood by the appropriate staff
low likelihood of occurrence
across the Ambulance Service.
high impact on normal business.
Appendix 11 provides examples of templates for
Information
AMPLANZ certainly does not cover all aspects of risk
station and department level BCPs.
management in an Ambulance Service. It focuses
on the requirement to ensure that ‘normal’ services
2.1.2 Ambulance Tactical Planning
can be maintained and Ambulance Services are
Noting the risk context of AMPLANZ, there is a need
able to respond safely and appropriately to known
to prioritise the mitigation of hazards according to the
hazards in the community. Therefore the focus here
possible risk to the community, Ambulance Services
is on business continuity, tactical plans and their Official
and the health sector. To assist with prioritisation, the
prioritisation, and coordination of plans.
Ambulance Service will need to consider the following:
For example: There are complex hazards that may
Complexity, and therefore coordination
the
require a health and therefore ambulance response. A
requirements, of the incident. Issues that may
number of these hazards, such as earthquakes, tsunami
further complicate the response include:
or floods, require significant national multi-agency
coordination and response and need Civil Defence and
Communications issues
Emergency Management lead planning. The nature and
Requirements for specialist trained ambulance
under
scale of the ambulance response would depend on the
staff or services (e.g. SERT, CBR, mines rescue)
impact of the ‘event’ on the community. The Ambulance
Services tactical response would be based on ensuring
Risk to responding staff if not informed or
the ambulance management and communications are
trained in preparation for the incident
in place to support the community response as the
The need for a multi Ambulance Service or
incident unfolds. The welfare of staff and patients are
emergency service response
central. The key preparedness activity by Ambulance
Services would be based on appropriate and tested
Possible duration of the incident
business continuity plans.
Number of patients and their acuity
Released
There are known hazards in the local area which may
Impact on local health services
require a specific ambulance response. These may
include, for example, bus accidents, viral outbreaks,
Local Ambulance Service capacity and capability.
incidents at large factory or business premises, airports,
It is necessary for an Ambulance Service to develop,
tunnels, health and age-care facilities, petro-chemical
maintain and test ambulance tactical response plans
plants, and stadia etc. All plant, facility or infrastructure
for known hazards. Tactical plans shall complement
owners are required to manage their risks appropriately,
1This Standard supersedes NZS 4360:2004 Risk Management. NZS 4360 noted in NZS 8156 Section 3.5 page 19.
30
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
the Activation and Escalation Processes outlined in
As part of this, Ambulance Services will need to
Part 2 Section 3.1 and cover:
ensure the:
Location details for the site or hazard area
Notifications systems in place are clearly specified
Maps or plans
including Ambulance to DHB but also DHB to
Ambulance
Initial response actions by CCCS and Ambulance
Managers
Role of medical staff in the pre-hospital setting is
clearly specified
Critical Information for the safety of crews and others
Integration of all DHB provider arms with the
Key Personnel details for the site authority or
Ambulance response, including specifically Public
hazard area
Health and Primary Care.
Details of hazards
There is a requirement also for an alignment of the
1982
Review dates and responsibilities.
Ambulance Service plans with the National plans such
as the National Mass Casualty Transport Plan.
Evidence of agreement with the site authority.
Emergency Service, CDEM and private sector emergency
Tactical plans will be easily accessible to the CCCS
Act
dispatchers and responding ambulance management
planning
and crews at the time of the response. This shall include
CDEM Groups have completed risk analysis of their
appropriate electronic access as well as hard copies.
regions and are developing contingency plans for
Appendix 12 provides a template for local tactical plans.
the management of those risks and coordination in
a response. These include, for example, initial and
ongoing response, welfare and lifelines.
2.1.3 Inter-agency Planning
Inter-Ambulance Service Cooperation
Police and Fire also have responsibilities to lead the
response planning for significant hazards where they
There are a number of hazards and therefore risks
are the lead agencies.
Information
shared between Ambulance Services that require a
There are also private sector agencies that are
combined response from all.
required to plan for major incidents in their operational
For example: the northern Rimutaka Tunnel Train
areas.
Incident (Wairarapa) may require a tactical response
Ambulance Services are required to coordinate
combining the resources of the Wellington Free
their tactical plans with the lead agencies as part
Ambulance, St John, a number of air ambulance Official
of the overall health response. This shall include
providers and possibly NZDF. There may be a
clear agreements for cost recovery with the incident
requirement to activate national coordination
controller.
mechanisms within the ambulance sector. A number of
the
DHBs are also likely to be involved.
2.2 Exercising
Therefore Ambulance Services are required to identify
hazards, plan responses (management, clinical,
A complete Ambulance Service Response, including
communications, coordination), and test plans for
the set up and activation of an ASEOC, shall be
such hazards. The aim will be to build an appropriate
exercised in at least one major CDEM (Tier 3–42)
under
response, build inter-service operational relationships
exercise as well as at least one major emergency
and develop coordination mechanisms.
services or health exercise each year.
Communication and activations systems shall be
Health Emergency Planning
tested as appropriate for all exercises where there
Ambulance Services are required to integrate their
is a likelihood of a significant ambulance and health
emergency management planning with that of the
response.
DHBs Likewise, the DHB Operational Planning
All exercises shall be evaluated and results reported
Frameworks (OPF) notes that a DHB will ensure that
Released
internally within the Ambulance Service. Lessons will
all ambulance providers have plans and resources in
be identified and shared. Processes will be developed
place to ensure that their emergency responses are
to incorporate changes into the appropriate level
integrated, coordinated and exercised with the DHB’s
of planning within the sector. This shall include the
Health Emergency Plan (HEP).
annual AMPLANZ review by Ambulance New Zealand.
2Ministry of Civil Defence Emergency Management (MCDEM) Tier 3 exercises test territorial local authority (TLA) and CDEM group (CDEMG)
operations. MCDEM Tier 4 exercises test National Crisis Management Centre (NCMC), CDEMG and TLA operations. Both of these will require
a service and national response from Ambulance.
PART 3 SEPT 2016
31
2.3 Training and education
3.0 Response
To enable a complete and effective Ambulance Service
emergency response, appropriate members of the
3.1 Activations, Level of Response, and
ambulance management team shall be trained in their
Notifications
initial response roles, the functioning and role of the
ASEOC (Ambulance Service Emergency Operations
The activation, levels of response and notifications for
Centre). Such training shall include, but is not limited to:
an Ambulance Service are detailed in AMPLANZ Part 2
Section 3.1.
CIMS 2 (minimum)
Emergency Coordination Centre or Operations
3.2 Activation based on national and
Centre management
regional warnings
Leadership and On-call management roles for
1982
middle and senior management required as part of
The Ministry of Health and the Ministry of Civil Defence
or in support of an ambulance response
and Emergency Management will send out notifications
to all emergency management stakeholders in the
Specific training as developed / run by key
health sector and the wider CDEM sector.
Act
partners, such as the Regional CDEM Groups,
DHBs, MoH or MCDEM on specific roles E.g.
The CCCS are the single points of contact for the
Controllers’ course, Liaison Managers’ inductions
Ambulance Services.
Emergency Management Information System (EMIS)
The types of national notifications are noted in Appendix
log in and basic use
13. The CCCS will receive these notifications and is
responsible for cascading them to the Ambulance Sector.
Specific in-house training on the set up and
procedures of the local ASEOC.
The CCCS will inform all Ambulance Services and the
appropriate level of response, service management
Potential staff of an ASEOC shall include key managers
and/or national coordination will be determined.
and also support staff to undertake data entry and
Information
administration support functions.
There are also Regional CDEM group or local authority
notifications. The CCCS will receive these notifications
Training needs analysis is required to further enhance
and cascade appropriately to the Ambulance Services.
the appropriateness of emergency management
Local Ambulance Service Management may also receive
training and education within an Ambulance Service.
notification directly from local authorities and will ensure
Training and education in emergency management
that the CCCS is informed.
Official
for Ambulance Services shall align appropriately
Note: If there is an ambulance major incident response
with competency frameworks and guidelines of other
required, this will be activated and escalated using the
emergency service partners, as well as with Civil
the process noted in Part 2 Section 3.1 and usually before
Defence and Emergency Management Agencies.
MoH or MCDEM alerts have been received.
2.4 Review and Audit
3.3 Communications
The Ambulance Service Major Incident and Emergency
under
plans, and the related operational procedures, shall
3.3.1 From an Ambulance Commander
be audited and reviewed as part of the Ambulance
The Ambulance Service Management will receive
Service’s quality management systems to ensure the
METHANE reports from the scene as soon as possible
notification, activation and management of a full and
via the CCCS. For complex and / or long duration
coordinated ambulance service response.
incidents, the Ambulance Commander will also develop
AMPLANZ will be reviewed annually to take into account
Ambulance Action Plans to be part of the overall
local and internationally significant development and
Incident Action Plan approved by the Incident Controller.
lessons identified or learnt. There will be a formal
See Part 2 Section 3.4.1.
Released
review of AMPLANZ no later than every three years.
The Ambulance New Zealand Standards and
3.3.2 From a health or CDEM EOC
Accreditation Committee has national responsibility for
review of AMPLANZ on behalf of the Ambulance New
In a health or CDEM emergency (e.g. pandemic
Zealand trustees.
or natural disaster etc), the Ambulance Service
Management will receive sitreps, resource and
information requests, and action plans. The Ambulance
Service will be required to maintain communications
remotely, or via a Liaison Manager, with the lead
32
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
agency and to contribute to briefings, provision of
3.4.2 Emergency Management Information Systems
intelligence and action plans as appropriate.
(EMIS)
3.3.3 Ambulance Operations Management briefing
The Ministry of Health and the Ministry of Civil Defence
Emergency Management both have EMIS. At the
All Ambulance Services shall maintain a procedure
Ambulance Service level, the current EMIS is able to be
to ensure that all local senior operations managers
accessed and utilised.
and appropriate non-operations managers receive a
Ambulance Services shall develop and use the EMIS, in
briefing on the incident, be allocated roles/tasks, as
coordination with the MoH, DHBs and other response
appropriate, and develop the initial ambulance response.
and emergency management agencies. The Ambulance
This briefing should be separate to and before the CCCS
Service will use the EMIS to ensure appropriate
briefing teleconference noted in Part 3 Section 3.3.4.
intelligence, planning and operational information,
This briefing is likely to be completed by teleconference.
relating to the incident, is integrated and transparent
1982
across local and national responding agencies.
3.3.4 Major Incident Notifications within Ambulance
The CCCS shall ensure that the key information
Services and to partner agencies
captured in the CAD is linked to the EMIS. Information
Act
available in the EMIS should also be easily accessible
See Appendix 14 for a guideline on the Ambulance
to key staff to inform decision-making with in the CCCS
Service staff and health partner agencies who should
and ASEOC.
receive notifications of Level 1, 2 or 3 major incidents.
Ambulance Services shall also work towards ensuring
The CCCS will maintain a Standard Operating
that EMIS access is integrated into scene management.
Procedure to notify (via page/text) and then brief (via
short teleconference):
DHB operational points of contact
3.4.3 Integration with the Incident Management Team
Ambulance Service management who were not
Information
required to be part of the briefing noted in Section
It is a requirement of CIMS that the information
3.3.3 above.
systems of all responding agencies be integrated
to provide a single set of information. This will
Other appropriate response agencies (e.g. CDEM)
enable the Local or Regional Controller to maintain a
It is the responsibility of the Ambulance Services
comprehensive overview of the situation and therefore
and the CCCS to maintain contact lists and test
enable the development of appropriate incident action
Official
this notification system according to the Standard
plans. To facilitate this, the Ambulance Service will:
Operating Procedures.
Provide the Controller with regular and
comprehensive Ambulance sitreps
the
3.3.5 Call back
Action specific orders from the Controller relating
All Ambulance Services shall maintain a procedure to
to the overall management of the incident while
ensure that all required operations and non-operations
ensuring that appropriate patient care and
staff are able to be called back to assist in the
ambulance staff safety is maintained
operational response as appropriate.
under
Provide the Controller with the Ambulance Action
Plan (AAP) and modify the AAP if necessary for
3.4 Information management
the improved management of the overall incident
while ensuring that appropriate patient care and
3.4.1 Tools
ambulance staff safety is maintained
To assist with the management of information
Inform the Controller of changes to Ambulance
during an incident, an Ambulance Service shall have
resourcing
appropriate tools to be used by duty management
Request, through the Controller, any non-ambulance
Released
initially and then staff required to support a complex or
resources required by Ambulance
prolonged response. These tools may include:
For complex and multi-Ambulance Service
Communication and Decision Logs
responses, where there is national coordination
Sitrep / METHANE reports
(see part 4), ensure the Ambulance sitreps, AAPs,
and ambulance resource status/requirements are
Ambulance Action Plan (AAP)
communicated to the Controller, the health EOC
Resource tracking reports
within the responding DHBs and National Health
Coordination Centre (NHCC).
Mapping.
ePRF
PART 3 SEPT 2016
33
3.5 Ambulance Service Emergency Response Management Structure
This section provides Ambulance Service Managers with a guideline on the roles required and scale of the
management structure that may need to be set up to manage two types of incident. These examples note the
modular and expandable nature of CIMS.
3.5.1 Simple Ambulance Service Emergency Response Management Structure
Simple command structure for Level 1 incidents or Open, Simple, Restricted or Controlled incident of short
duration (< 4hrs) and a small number of patients (< 10 patients). See Figure 1.
Figure 1: Simple Ambulance Service Emergency Response Management Structure
1982
Ambulance
Service
Act
Executive Team
Duty Operations
Executive Officer
Ambulance Public
(Ambulance Service
Information
Controller – ASC)
Manager (PIM)
Information
Incident
CCCS
Controller
Ambulance
Official
Commander
or Operations
Manager
the
Scene management (all roles not shown)
Control: provides coordination across agencies
Command / Control: directs the operational response within an Ambulance Service at the scene
under
Communications
This follows ‘business as usual’ management. In this case the majority of incidents will require minimal
communications with, or coordination by, the Ambulance Service Controller (ASC). The ASC will be undertaken by
the Duty Operations Executive Officer3 on the declaration of a major incident of the Ambulance Service. Where
there is an impact on normal operations, direction will be provided by the ASC.
The CIMS roles of Control, Logistics and Planning / Intelligence are undertaken by the ASC according to the
requirements of the Ambulance Commander or Operations Manager at the scene. The ASC will decide if he/she
requires extra support to undertake these roles.
Released
The CCCS will follow business as usual management procedures across its national virtual structure to ensure
management of the incident and normal service delivery.
Media inquiries will be managed by the Ambulance Public Information Manager (PIM) in coordination with incident
lead agency media officer (e.g. Police or Fire). Release of Ambulance Information will also be approved by the ASC.
Ambulance Service Executive Team shall receive timely updates of the incident from the ASC and may be
requested to undertake specific tasks depending on the impact of the incident on the whole organisation.
3Business As Usual titles vary across the services at this level and include: Duty Operations Executive On-Call, Duty National Executive,
District Duty Manager, On Call Manager or Executive etc.
34
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)


1982
Act
3.5.2 Comprehensive Ambulance Service Emergency
Service Controller, unless formally agreed otherwise.
Response Management Structure
The response shall be managed from an Ambulance
A clear Ambulance Service command and control
Service Emergency Operations Centre (ASEOC), a
structure will be required for long duration Controlled
CCCS Major Incident Room or virtually, depending on
Information
and / or Complex Incidents (Level 2 or 3) or for
the scale, duration and complexity of the incident(s).
a single or multiple simple / restricted incidents
CIMS roles or functions will be implemented within
equivalent to Level 1 or 2 (short duration but with
the ASEOC and therefore increased staffing will be
large numbers of casualties). There will be similar
required. This will need constant reassessment as
management requirements for conplex business
part of the ambulance action planning processes. See
continuity incidents.
Figures 2 & 3 and Part 3 Section 3.6 for summaries
Official
The Ambulance Service Controller (ASC) role is to lead
of the ASEOC roles and responsibilities.
the Ambulance response management structure that
It is recognised that the ability of a local part of an
provides strategic direction, support and coordination
Ambulance Service to fill all roles within the full CIMS
the
for Ambulance Commanders in complex or multiple
structure in an ASEOC with individual managers
incidents / emergencies. The ASC is responsible to
is limited, particularly for long duration, complex
the Ambulance Service Executive Team.
incidents. That said, all CIMS roles will need to be
The Ambulance Service Executive Team delegates
undertaken. To do this, CIMS roles may have to be
authority to the ASC to manage the operational
shared between managers. How this issue is managed
under
response of the Ambulance Service in a major
by the Ambulance Service is the responsibility of the
incident. The Executive Team will maintain strategic
ASC. It may be necessary to request support from
oversight of the response and will provide guidance as
neighbouring Ambulance Services or other services to
required. The ASC will ensure that the Executive Team
ensure the appropriate roles are undertaken effectively
is informed of the incident developments.
for the duration of an incident. A request may be made
via national coordination mechanisms.
For a large, complex incident, where local ambulance
resources are insufficient, there may be a requirement
for a national coordination mechanism (see part 4)
Released
that enables access to resources and expertise from
across New Zealand. All Ambulance Services shall
have in place a clearly defined mechanism to assist
with the coordination of ambulance resources from
outside the area affected by the incident. Should
national coordination be required, operational control
of the response remains with the local Ambulance
PART 3 SEPT 2016
35
Figure 2: Comprehensive Ambulance Service Emergency Response Management Structure
Ambulance
Service
Executive Team
Recovery
Manager
Ambulance
1982
Service
Controller
Clinical/
Technical
Advisors
Act
EOC or
Administration
Response
Officers
Manager
ASEOC Human
ASEOC
ASEOC
ASEOC Public
ASEOC Logistics
ASEOC Planning
ASEOC Liaison
Resource
Operations
Intelligence
Information
Manager
Manager
Manager
Manager
Manager
Manager
Manager (PIM)
Information
Supplies, ICT,
Ambulance
Equipment
Liaison
Contractors
Officers to:
– ED
CCCS
– Health/
Official
Field Operations
Communication
Hospital EOC
(Commander etc)
& Clinical Control
– CDEM EOC /
Services
ECC
– Police EOC
the
– etc
Field / External incident
under
Control: provides coordination across agencies
Command / Control: leads and supports the operational response within an Ambulance Service
Communications
A similar structure may be used to manage complex internal or business continuity incidents that impact on patients
and services. For example extensive communications failure. The type of incident will dictate which managers
Released
undertake the key roles in the structure such as Ambulance Service Controller and ASEOC Operations Manager. See
Figure 3 for an example structure. Note that the structure may be modified depending on the incident type.
36
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)

1982
Act
Figure 3: Comprehensive Ambulance Service Emergency Response Management Structure for
Internal or Business Continuity Incident
Ambulance
Service
Executive Team
Information
Recovery
Manager
Ambulance
Service
Controller
Clinical/
Official
Technical
Advisors
EOC or
Administration
Response
Officers
Manager
the
ASEOC Human
ASEOC
ASEOC
ASEOC Public
under
ASEOC Logistics
ASEOC Planning
ASEOC Liaison
Resource
Operations
Intelligence
Information
Manager
Manager
Manager
Manager
Manager
Manager
Manager (PIM)
Ambulance
Supplies, ICT,
Liaison
Equipment
Officers to:
– ED
Released
CCCS
– Health/
Technical
Field Operations /
Communication
Hospital EOC
Services (as
Other Dept
& Clinical Control
– CDEM EOC /
required)
Services
ECC
– Police EOC
– etc
Internal or Business Continuity Incident
impacting on Ambulance Services
PART 3 SEPT 2016
37
3.6 Ambulance Operations and CCCS
ASEOC Operations Manager
roles and responsibilities
Reports to the ASC
There are key responsibilities for all roles required in
Manages and supports the responding managers
the ASEOC structure during an emergency response.
(e.g. Ambulance Commander/s)
The more complex the response and the longer the
Assesses and evaluates the incident operations,
duration of the incident, the greater the demand on the
including progress, resource requirements and priority
management structure.
Provides information to the ASC and other sections
Again it is noted that roles may be combined depending
of the ASEOC
on staff availability and the workload to manage the
response. In a short duration incident, the Ambulance
Contributes to the development of the Ambulance
Service Controller may be able to undertake the majority
Action Plan
of the ASEOC roles, including operations, planning and
Implements the Ambulance Action Plan in
1982
logistics while Public Information Management and
coordination with the responding managers and
Liaison may be delegated.
their teams.
Act
See Appendix 15 for Task Cards for ASEOC roles.
ASEOC Intelligence Manager
Ambulance Service Controller (ASC)
Reports to the ASC
Responsible for the Ambulance Service emergency
Maintain a log to record activities
operational response
Liaises and / or integrates with the Intelligence
Sets the objectives for the Ambulance Service
Sections of the Lead Agency, other responding
Response
agencies, other internal ambulance sources and
Reports to the Ambulance Service Executive Team
nationally as required
Coordinates with the National Crisis Coordination
Gathers, collates and analyses response
Information
Centre (if activated)
information
Responsible for the activation for the ASEOC and
Develops and distributes intelligence products such
the appropriate ongoing resourcing
as situation reports, situation maps etc. to ensure
a common operating pictures
Contributes to and approves Ambulance Action Plan
(AAP)
Maintain information communication sources in the
Official EOC – e.g. whiteboards, maps, etc.
Responsible for the management of the ‘Business
as Usual Activities’ alongside the emergency
Contribute to response and contingency plans
the
response (but may be delegated to another
through the provision of accurate current situational
executive)
awareness and possible future scenarios
Responsible for the quick operational recovery of
Contributes to the development of the Ambulance
normal service delivery following the incident (may
Action Plan
be delegated to a Recovery Manager).
ASEOC Planning Manager
under
Ambulance Service Executive Team
Reports to the ASC
Delegates the operational Ambulance response to
Maintain a log to record activities
the ASC
Develop the Ambulance Action Plan based on
Maintain executive oversight of the response
the Ambulance Controller’s objectives, current
Provide strategic guidance and support to the ASC
situational awareness and resource availability
Will decide to activate or request activation of the
Develop an action planning process (meetings,
Released
Ambulance National Crisis Coordination Centre
teams, timelines etc.) appropriate for the incident
(NCCC). See Part 4
Develop contingency plans based possible incident
Assist the ASC, where appropriate and when
developments as required
requested, with Public and Internal information
Develop long term plans as appropriate including
management and Business Continuity of the
the planning for and transition to recovery
Service.
Forecast the immediate, medium and long term
resource requirements as appropriate for the
38
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
incident, and include these requirements in the
ASEOC EOC or Response Manager
Ambulance Plans for approval by the ASC
Reports to the ASC
Integrate the Ambulance Plans with those of the
Lead Agency and Support Agencies as appropriate
Ensures efficient flow of information in the ASEOC
Supports the ASEOC functional Managers to
ASEOC Logistics Manager
perform their role
Reports to the ASC
Coordinates the internal function of the ASEOC
Liaises with Logistics Sections in the lead agency,
Ensures the staffing needs of the ASEOC are met
other responding agencies, and nationally as
required
Monitors the health and welfare of ASEOC staff
Responds to the priority logistical needs identified
Ensures appropriate administrative support is in
by Operations and noted in the AAP
place for the ASEOC
1982
Work with and delegates to the appropriate
ASEOC Clinical / Technical Advisors
departments of the Ambulance Service to meet
Reports to the ASC
the priority response needs of the incident; for
Act
example: Human Resources, IT, medical and
Provides advice to the ASC on clinical, technical or
non- medical supply, catering, fleet, refuelling,
management issues relating to the response and
mechanical, and traffic support
subsequent recovery
Develops a communications plan for the
May be required to coordinate with DHBs to
management of the incident. This should be
obtain hospital bed status information etc and
done in liaison with the CCCS and the Ambulance
communicate this information to the ASEOC
Service IT department
Operations Manager and ASEOC Liaison Manager
Contributes to the development of the Ambulance
Role may be filled by Service Clinical Advisors and
Action Plan.
/ or Emergency Planning Advisors, depending on
Information
the requirement.
ASEOC Public Information Manager (PIM)
ASEOC Administration Officer/s
Reports to the ASC
Staff allocated to support the ASC or other managers
Liaises with Public Information sections in the lead
as required. Tasks will include:
agency, other responding agencies and nationally
Official
as required
Maintaining a communications and decisions log
for their manager
Maintains an Ambulance Service media contact
point for the incident
Maintaining currency of information in the ASEOC
the
on whiteboards or by other means
Coordinates all media and information releases with
the Lead Agency Public Information management
Monitoring and disseminating information received
via the MoH EMIS.
Advises the ASC on Public Information Management
strategies
Ambulance Service Recovery Manager
under
Develops and maintains up–to- date internal
Appointed early in the response (shared with P&I or
information for Ambulance staff as required.
Logistics Manager during the response)
ASEOC Liaison Manager & Officers
Engage with Roster Administrators, HR, peer
support agencies, Fleet Managers/Service agents,
Report to the ASC
Suppliers and Finance Officers to plan for the quick
Responsible for maintaining information flow and
return to normal service and readiness
contact with key partner agencies. For example:
Report to the ASC during the response and the
Released
CDEM EOC, DHB or receiving hospital/s
Ambulance Service Operations Manager during
Manage key Liaison Officers roles, such as
the recovery.
Ambulance Liaison – ED, Ambulance Liaison –
Health, Ambulance Liaison – Non-health (if required)
May be based in the ASEOC or at the EOC of a
partner agency.
PART 3 SEPT 2016
39

1982
Act
3.7 Ambulance Non-operational staff:
It will be the ASEOC Liaison Manager who will have
the responsibility for maintaining the relationship
roles and responsibilities
with coordination mechanisms within partner
All Ambulance Services have human resources working
agencies during a response. This will include: sharing
in support of front line ambulance staff and also
information, requesting resources if required, inputting
Information
undertaking other business activities. The scale and
into a multi-agency action plan. There may be a
focus of these departments varies from service to
number of Liaison Officers working with this Manager,
service.
depending on the incident. See Appendix 16 for task
cards.
The management of a complex or long duration
incident will require tasks to be undertaken by non-
It is recognised that Ambulance Services have limited
operations staff.
resources to provide liaison across a number of
Official
different agencies. Therefore the Ambulance Service
To make the best use of the capability and capacity
Controller will have to prioritise the placement of
of these staff, managers will need clarity of the tasks
direct ambulance liaison according to the incident’s
the
that may be required. Managers will also prepare their
complexity, duration and impact on ambulance
teams appropriately.
operations, health services and the wider community.
All support services shall have business continuity
In an MCI the key roles to be filled will be the Liaison
plans in place and these shall include their response
Officer – ED and the Liaison Officer – Health.
during a complex and long duration major incident that
under
impacts on the ambulance service and therefore will
3.8.1 Health coordination
also impact on the work of the support service. The
A mass casualty incident or health emergency may
type of response may include (but not limited to):
impact severely on the local, regional and national
realignment of normal business
health system. The coordination of patient transport,
provision of staff to an ASEOC
according to priority, to the most appropriate health
facility is therefore critical. All senior ambulance
actioning on specific tasks as required by the
officers who may fulfil the key roles in the ASEOC shall
Ambulance Service Controller.
be fully briefed on:
Released
3.8 Coordination with health, emergency
Capacity and capability of the local and regional
receiving health facilities
services and other agencies
Capacity and capability of the local and regional
In a complex mass casualty incident or major
Ambulance Services including air ambulance (rotary
emergency, it is unlikely that any single agency will
and fixed wing) with the support of the Air Desk
have the required resources to meet the needs
(see section 3.10.2)
of a response. The CIMS approach provides for
Emergency plans of the local DHBs as they impact
coordination across all responding agencies.
the Ambulance Services
40
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
The communication channels with receiving health
Ambulance managers need to maintain relationships
facilities or DHBs to coordinate patient transport
with such organisations.
The communication channels with Regional Health
An Ambulance Service is responsible to ensure that its
Coordination structures.
Ambulance Service Controller has access to contact
An Ambulance Service is responsible to ensure that
points for appropriate agencies.
ASEOC have access to appropriate contact points for
the local and regional health facilities and services.
3.9 Media
For all Level 2 and 3 incidents, DHBs will be informed
Media representatives will arrive at the scene following
via the notifications system as part of the activation
a major incident. Media will also go to hospitals and
of the ambulance response. DHBs will receive Level 1
any other site where there is a possibility of acquiring
notifications. The MoH Regional Emergency Management
information on the incident including the numbers of
Advisors and 0800 GET MOH will be informed for Level
injured and deceased etc.
1982
2 and 3 incidents. See Part 3 Section 3.3 and Appendix
Ambulance officers will be aware of and follow their
14. Procedures are in place to hold an initial briefing
organisation’s media policies. For all incidents, an
teleconference with partner agencies and neighbouring
Ambulance Service Public Information Manager (PIM)
Ambulance Services, based on the scale of the incident.
Act
will be available to coordinate inquiries from the media
This will be facilitated by the CCCS Manager and managed
with appropriate other agencies. This person will be
by the Ambulance Commander, Ambulance Service
based initially at the Ambulance Service EOC.
Controller or their delegate.
For large scale incidents, where there is a clear
Ambulance Services will also coordinate their actions
CIMS incident management team in place, all media
in line with the National Mass Casualty Transport Plan.
inquiries, and the release of information to the media,
will be managed by the Incident Public Information
3.8.2 Emergency Services and Other Agencies
Manager responsible to the Incident Controller. Public
Ambulance Managers working in an ASEOC will need
Information Management will also be part of the CIMS
Information
to have access to information on tactical ambulance
Incident Action Plan.
responses for specific hazards in their areas. These
For smaller incidents, the lead agency (for example,
will be in the form of ambulance tactical plans and
Police or Fire) may request all news releases be directed
developed in coordination with other responding
to their Public Information Managers or Senior Officers.
agencies and the ‘owners’ of the plan (for example,
an airport company, stadium event management etc).
It is a priority for the Ambulance Service Controller to
Official
These plans will be developed by the Ambulance
ensure consistent management of public and internal
Service and be accessible from the CCCS CAD system,
information is in place as quickly as possible.
with appropriate accessible backup copies.
the 3.10 Ambulance Service Resources and
It will also be necessary to coordinate with non-health
organisations and perhaps access their resources and
Emergency Operations Centre
expertise. In CIMS approach, the Ambulance Liaison
or Logistics Manager will have the responsibility for
3.10.1 Ambulance Service Resources
requesting such resources if required. That said, it is
under
necessary for senior ambulance officers to be fully
Ambulance Service Managers who may be required
briefed on:
to undertake the ASC role or other key roles in the
ASEOC, such as Logistics or Operations Managers,
• The role, capacity and capability of the emergency
shall make themselves aware of the resources and
services, NZ Defence Force, NGOs such as
equipment that may be used in their immediate service
Salvation Army and NZ Red Cross, private sector
areas during a major incident. These may include:
organisations and Civil Defence Emergency
Management Organisations
Ambulance Major Incident cache of medical
materials and equipment
• The communication channels with the above
Released
organisations to enable access to appropriate
DHB medical materials that may be accessible to a
resources.
pre-hospital response
Note: An Ambulance Service does not need to
Specialist materials, equipment, services and
maintain extensive lists of agencies etc. Other
personnel from a partner emergency service or
agencies maintain contracts and contacts lists
support agency that may be required by a pre-
for support services: for example, many CDEM
hospital response. For example, USAR equipment,
organisations have agreements with NGOs and
CDEM logistics.
contacts with private sector service providers.
PART 3 SEPT 2016
41
All Ambulance Services are required to maintain major
situation, plans and resource requirements.
incident equipment and materials, with efficient means
The Ambulance Service shall have a space
of deployment, to ensure a major incident in their
appropriately set up or able to be set up as an ASEOC
service area could be appropriately resourced. These
within 30 minutes of a major incident being declared.
materials and equipment will be nationally consistent
kits or caches to ensure interoperability between
See Appendix 16 for the specification guideline on the
Ambulance Services.
set up of the ASEOC.
The CCCS CAD will maintain current information on
The CCCS is required to maintain an ‘Incident Room’ in
the majority of ambulance resources available for
each Centre to enable the communications management
deployment. The status of ambulance resources shall
of a major incident to be separated from normal service
be in a form that is immediately accessible to national
delivery, when appropriate. The CCCS Incident Rooms
coordination mechanisms, if required. For example,
will require similar specifications as the ASEOC.
this may be via the health EMIS. This will include the
1982
location and detail of Major Incident Caches in urban
4.0 Recovery
centres and Station Kits in strategic rural stations.
The ambulance or event services, including NZ Defence
4.1 Ongoing Impact of the Incident
Act
Force (NZDF) or NZ Red Cross, not normally deployed by
the CCCS, will maintain their resource status, capacity
The process of recovery for an Ambulance Service
and capability in a form that is immediately accessible
is defined as the re-establishment of normal service
to the CCCS or to national coordination structures if
delivery after a major incident. This process should
required. For example, this may be via the health EMIS
start as soon as possible in the response phase
or Liaison Officers, in the case of the NZDF.
and be aligned with Ambulance Service business
continuity plans. Ambulance Services will be required to
contribute to the overall recovery of the health services
3.10.2 Air Desk
and community. It may also be that, depending on
The National Air Desk will aim to:
the incident, there may be a new ‘normality’ for the
Information
community. Ambulance Services may have to realign
Resource appropriate rotary & fixed wing aircraft
themselves appropriately as part of the recovery process.
Dispatch & coordinate both rotary & fixed wing aircraft
All logs and notes made during the incident at the
Recommend appropriate airport to use for staging
Ambulance Service level will need to be correlated
point between rotary & fixed wing aircraft
and stored in case of possible inquiries into the
management of an incident.
Official
Coordinate with road dispatchers transfer of patients
to hospitals from air
It is envisaged that even in a moderately sized major
incident there will be an effect on the Ambulance
Ensure that air coverage is still maintained in the
Service. Areas requiring consideration for recovery will
the
other regions and
include, but should not be limited to:
If required provide an on the ground air coordinator
Staff welfare/debriefs
3.10.3 Ambulance Service Emergency Operations
Rosters and leave
under
Centre
Operational review and learning
For smaller incidents, an ASEOC may be able to operate
Consumables (medical/fuel)
‘virtually’ from the CCCS Incident Room or from a
Equipment (repair, servicing, review and
partner agency EOC. However, ASEOC will be physically
replacement)
required for complex or long duration incidents.
Vehicles (servicing, repairs etc)
The role of the ASEOC is to:
Finance and cost recovery.
Coordinate the ambulance response to a major
Released
incident with the Ambulance Commander(s) and the
Recovery roles have been built into the role
CCCS
descriptions for response managers at the service
level as well as for key non-operational staff.
Plan for future resource requirements of a major
incident
For complex incidents that have impacted significantly
on the ongoing functioning of the Ambulance Service, a
Manage the impact of the incident/s on normal
Recovery Manager may be required to concentrate on
service delivery
rebuilding or modification of the service in the post-
Ensure that all key stakeholders, both internal
incident environment. Note: the Recovery Manager is a
and external, are informed of the current incident
role not necessarily a position.
42
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
4.2 Operations and CCCS: Roles and
External criticism or triggers impacting the
perceptions of the ambulance response
Responsibilities in Recovery
Or other issue that may trigger a response from
All role descriptions in Appendix 15 have recovery
the Ambulance Service’s Reportable Events
actions included. A role description of the Recovery
Management System.5
Manager is included.
4.4.2 Hot or scene debrief
4.3 Non Operational Staff: Roles and
This is the lowest level of debrief but may be the most
Responsibilities in Recovery
important. All responding ambulance officers and
Each Ambulance Service shall ensure Business
communications staff should take part in this debrief.
Continuity Plans for non-operationals departments’
This is a relatively informal process and should follow
BCPs or support services include both response
the debrief template as noted in the Ambulance
1982
actions as well as recovery actions. An example of
Incident Command Notebook and in Appendix 17.
a recovery action may be: The Ambulance Service
This should occur as soon as possible following
Financial Officer will be required to correlate and report
the incident. It will be managed by the Ambulance
Act
on all direct incident costs to enable cost recovery. This
Commander, the ASC or the Recovery Manager.
should be completed in a specific timeframe.
4.4.3 Ambulance Service Debrief
4.4 Ambulance Debrief and Reporting
This process will be managed by the Ambulance
Processes4
Service Controller and may be delegated to a Recovery
Manager. This process will be more formal and will
draw in all relevant staff; operations, communications
4.4.1 Debrief aims and requirements
(CCCS), non-operations/support and Ambulance
The aim of the debrief process is two-fold:
Service Executive as appropriate. This should be
Information
completed within two months of the incident. The
To identify and acknowledge where the response
guidelines and documentation for this level of debrief
went well and ensure that these experiences are
are in Appendix 17.
shared
The outcome of this debrief will inform an inter-agency
To identify where improvements in the response
debrief if required.
is required and develop a plan of action to ensure
Official
that learning occurs.
4.4.4 Ambulance Service Major Incident Report
An incident debrief and / or reporting is required:
The aim of this report is to communicate the findings
Following all Level 2 and 3 incidents the
relating to the ‘whole-of-service’ response. It will
A level 1 incident (or where a level 1 incident
include learning and acknowledgement of excellence.
should have been declared) where there has been
This should be completed within six months of the
one or more of the following:
incident. The Ambulance Service Major Incident Report
will include:
Injury to or safety issues for Ambulance Officers
under
Poor clinical outcomes of patients possibly
The Ambulance Commander’s After Action Report
attributable to the Ambulance scene
(See Part 2).
management
The Ambulance Service Debrief
Communications failures or issues
The Inter-agency Debrief
Failure of SOPs or Tactical Plans that have
impacted on response
Specific information, experience, lessons
identified and recommendations from operations,
Ineffective coordination between responding
communications, non-operations/support
Released
agencies
departments (including financial costs to the
Crews lacking expertise or skills
service) or other source not covered in the above
Equipment failures
debriefs.
Significant impact on the non-operational
An Ambulance Service Major Incident Report Template
departments of the Ambulance Service
is in Appendix 17.
The reporting process will be coordinated by the
Ambulance Service Recovery Manager (if appointed).
4This section draws on the NZFS Incident Management – Command and Control Technical Manual Aug 2009. Section 6 pages 1–19. The
NZFS Special Operations support is gratefully acknowledged.
5See NZS8156 Section 3.7 page 20.
PART 3 SEPT 2016
43
1982
Act
Information
Official
the
under
Released
44
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
AMPLANZ Part 4:
National Crisis Coordination Centre
For Ambulance Service Managers to use as the framework for the development and use
of the National Crisis Coordination Centre
1982
SEPTEMBER 2016
Act
Content
Information
Part 1: Introduction to AMPLANZ and Emergency Management for the
Ambulance Sector
Part 2: Consistent Operations at the Scene
Part 3: Ambulance Service Approach
Official
Part 4: National Crisis Coordination Centre
1.0 Introduction
46
3.4 Information Management
48
1.1 Requirement for National Coordination
46
3.4.1 Tools
48
3.4.2 Emergency Management Information Systems (EMIS)
48
the
2.0 Readiness and Reduction
46
3.5 Structure and roles and responsibilities
48
2.1 Response Planning
46
3.6 Coordination with health, emergency services and other agencies
2.2 Exercising
46
48
2.3 Training and education
47
3.7 Media
49
2.4 Review and Audit
47
under
3.8 Resources
49
3.0 Response
47
4.0 Recovery
49
3.1 Notification
47
4.1 Ongoing Impact of the Incident
49
3.1.1. Escalation of a local incident
47
3.1.2. National warnings
47
4.2 Recovery Roles and Responsibilities
49
3.2 Activation
48
4.3 Debrief and Reporting Processes
49
4.3.1 Debrief aims and requirements
49
3.3 Communications
48
4.3.2 Major Incident Reporting
49
Appendices
Released
1.0 Introduction
Ambulance Service in the response and recovery
phases of the emergency
This is Part 4 of AMPLANZ and provides a framework
Provide a sustainable support structure, with
for the development and management of the National
trained personnel and appropriate infrastructure, to
Crisis Coordination Centre (NCCC) and its associated
be able to operate 24/7 if required.
procedures, for use in a major emergency where
national ambulance sector coordination may be required.
The operational control of the ambulance response
shall always remain with the local Ambulance Service
This document should be read in conjunction with
unless the local service requests control be formally
Part 3: Ambulance Service Approach
handed to another Ambulance Service.
1.1 Requirement for National
2.0 Readiness and Reduction
Coordination
2.1 Response Planning
1982
It is a clear requirement of the National Health
The majority of operational and tactical response
Emergency Plan that the ambulance sector shall
““...
planning is undertaken by individual Ambulance
coordinate... via the National Crisis Coordination Centre....”1
Services, the CCCS and their local emergency
Act
management agencies and neighbouring Ambulance
There are two broad scenarios where a degree of
Services. This is outlined in Part 3 Section 2.
national coordination may be required, these are:
The NCCC shall be written into specific ambulance
1. When there is an event affecting the nation (i.e.
operational and tactical plans as appropriate.
pandemic, major environmental disaster) and the
The ambulance sector contribution to national health
National Health Coordination Centre (NHCC) or
emergency planning may be undertaken in a number
National Crisis Management Centre (NCMC) has
of ways, including:
been placed on standby, opened or activated
Meeting the obligations set out in legislation (e.g.
2. When one or more of Ambulance Services are
CDEM Act) for Ambulance Services, DHB, MoH
overwhelmed and require support from other
Information
or other national agencies. Individual Ambulance
ambulance services, or perhaps national health
Services may be contracted and funded to
or national Civil Defence resources. Such an
coordinate the emergency planning and capability
emergency is likely, but not exclusively, to be a
development of the ambulance sector. For example,
protracted event and require an ongoing response
(chemical, biological and radiological) CBR capability
lasting a number of days and where recovery lasts
development
a number of weeks before normal services can be
Official
Aligning of Ambulance Service plans with national
resumed.
plans, such as the National Mass Casualty
The level of the national coordination will be
Transport Plan
the
dependent on the incident complexity, duration, scale
Cooperation between services for specific known
and location.
pre-planned events or known threat (e.g. Rugby
It is also noted, that an Ambulance Service will be
World Cup 2011, VIP tours / meetings etc)
required to focus on the immediate Operational and
Using the NCCC in planning for exercises, pre-
Tactical response to a local or regional incident. The
planned events or known threats, where it is
under
provision and coordination of external Ambulance
necessary that national coordination will be required
resources is best managed through a separate
Individual Ambulance Services contributing to
coordination mechanism. Therefore It has been
specific issues relating to emergency response
agreed that St John will maintain the National Crisis
planning. For example; revision of the New Zealand
Coordination Centre (NCCC) for its own national
Influenza Pandemic Action Plan.
coordination and all ambulance service coordination.
The choice of the approach used will depend on the
This is broadly defined as a mechanism that, with
planning issue, priority for individual services, capability
supporting procedures, is able to:
in the sector and the resources available to assist the
Released
Receive requests from the responding Service or
sector.
part Service that has been overwhelmed
Coordinate the provision of requested ambulance
2.2 Exercising
resources from other Ambulance Services or
The NCCC shall be involved in at least one major (Tier
nationally
3–42) exercise each year. The communication and
Liaise and coordinate with key National Emergency
activation procedures shall be tested as appropriate
Management Agencies on behalf of the responding
for all regional (Tier 3) exercises.
1NHEP 2015 page 12.
2MCDEM Tier 3 exercises test TLA and CDEMG operations. MCDEM Tier 4 exercises test NCMC, CDEMG and TLA operations. Both of these
will require a National response from St John.
2
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)

1982
Act
All activations of the NCCC for an exercise or a real
Training and education in emergency management
event shall be evaluated and lessons will be identified
for Ambulance Services shall align appropriately
and shared with the Ambulance Services. The key
with competency frameworks and guidelines of other
learnings shall then form part of the annual AMPLANZ
emergency service partners, as well as with Civil
Information
review and the reviews of an Ambulance Service’s own
Defence and Emergency Management Agencies.
Major Incident and Emergency Plan.
2.4 Review and Audit
2.3 Training and education
The Ambulance Service Major Incident and Emergency
To enable the NCCC to undertake its role, all potential
plans, and the related operational procedures,
Official
personnel who may be required to work at this level
including national coordination mechanisms, to ensure
shall be trained appropriately. It is noted that the
the notification, activation and management of a full
training requirements to assist in national coordination
and coordinated Ambulance Service response, shall
are similar to those required for an Ambulance Service
be audited and reviewed as part of the Ambulance
the
Emergency Operations Centre (ASEOC). Such training
Service’s quality management systems.
should include, but is not limited to:
AMPLANZ will be reviewed annually to take into account
CIMS 2 (minimum)
local and internationally significant development and
lessons identified or learnt. There will be a formal
Emergency Coordination Centre or Operations
review of AMPLANZ no later than every three years. The
under
Centre management
Ambulance New Zealand Standards and Accreditation
Leadership and On-call management roles for
Committee has the national responsibility for the review
middle and senior management required as part of
of AMPLANZ on behalf of Ambulance New Zealand
or in support of an ambulance response
trustees.
Specific training as developed / run by key
3.0 Response
partners, such as MoH or MCDEM. e.g. MCDEM
Controllers course, NHCC and NCMC Liaison
Released
Officer Inductions
3.1 Notification
EMIS login and basic use
3.1.1. Escalation of a local incident
Specific in house training on the set up and
The notification and escalation processes to be
procedures of the facility from where the national
used are outlined in Part 2 Section 3.0. This notes
coordination mechanism may operate.
when an Ambulance Service’s national coordination
Training needs analysis is required to further enhance
mechanisms should be informed, placed on standby
the appropriateness of emergency management
or activated depending on the incident.
training and education within an Ambulance Service.
PART 4 SEPT 2016
3
3.1.2. National warnings
appropriate intelligence, planning and operational
information relating to the incident is integrated and
MoH and the MCDEM will send out National
transparent locally, regionally and nationally.
Warning notifications to all emergency management
stakeholders in the health sector and the wider
CDEM sector.
3.5 Structure and roles and
The types of national notifications are noted in Appendix
responsibilities
13. The CCCS will receive these notifications and is
In developing a mechanism to access ambulance
responsible for cascading these to Ambulance Services.
resources from other services or nationally, or from
It is the responsibility of each Ambulance Service
national partner agencies, St John will ensure that a
to respond appropriately to these notifications and
clear coordination structure is in place and the roles
develop their responses, including the degree to which
within that structure have defined responsibilities.
inter-service or national coordination is required.
The coordination structure shall be based on CIMS and
1982
therefore shall include the following functions or roles:
3.2 Activation
National Ambulance Controller
There will be a clear procedure as to how to activate
Act
Operations
the NCCC and this shall be communicated to the
Ambulance sector and key partner agencies.
Planning
3.3 Communications
Intelligence
Logistics
The CCCS shall be the Ambulance sector ‘single point
of contact’ for partner agencies (for example: the MOH
Public Information Management
and MCDEM) to notify Ambulance Services of potential
Liaison
or actual events or to access Ambulance resources.
Technical advice
Information
An Ambulance Service shall ensure it has the ability
access or provide resources, support or coordination
Human Resources
at any time as part of its national coordination
Note the modular and expandable nature of CIMS.
mechanism. An Ambulance Service’s key points of
That is, all roles will need to be carried out to meet
contact shall be communicated across the sector.
the requirements of the incident and the requests of
the responding Ambulance Service.
Official
3.4 Information Management
Each function shall have clear role descriptions in the
form of task cards or similar.
3.4.1 Tools
the The facility or location where the coordination functions
The NCCC will have access to and use similar tools
occur will normally be outside of the immediate
in a service’s ASEOC. It will be required to produce
geographic area where the incident has occurred.
information for national partner agencies and to
Coordination functions may be managed ‘virtually’ or
appropriately action requests from the NHCC or
from an ASEOC depending on the scale, duration and
NCMC. These tools shall include but are not limited
under
complexity of the emergency.
to:
The detailed structure of the NCCC will be noted in
Communication and Decision Logs
the St John Major Incident & Emergency Plan. It will
Sitreps
be communicated nationally to all ambulance services
Ambulance Coordination Plan template
and partner agencies.
Resource tracking reports
Access to Mapping.
3.6 Coordination with health,
Released
emergency services and other agencies
3.4.2 Emergency Management Information Systems
The NCCC will liaise with national agencies. These
(EMIS)
include:
MoH and MCDEM both have EMIS. At the Ambulance
National Health Coordination Centre NHCC (MoH)
Service level, the EMIS is currently accessed and
utilised appropriately.
National Crisis Management Centre NCMC
(MCDEM)
The EMIS shall be utilised to provide the NHCC and
NCMC with the overall status of the ambulance sector.
National Welfare Coordination Group
The NCCC will need to access the EMIS to ensure
4
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
National Fire Service Headquarters
4.0 Recovery
National Police Headquarters.
4.1 Ongoing Impact of the Incident
To facilitate this coordination, ambulance managers
undertaking coordination roles shall maintain current
The process of recovery for an Ambulance Service
operational relationships with key staff in these
is defined as the re-establishment of normal service
national agencies. This will require appropriate
delivery after a major incident. This process should
security clearance for key ambulance managers.
start as soon as possible in the response phase
and be aligned with Ambulance Service business
As noted in Part 4 Section 3.5 above, the liaison
continuity plans. Ambulance services will be required
functions may be required to one or more of the above
to contribute to the overall recovery of the health
organisations. It is recognised that there are limited
services and community. It may also be the case
human resources to provide liaison across a number
that, depending on the incident, there may be a new
of different agencies and therefore a process of
‘normality’ for the community. Ambulance Services
1982
prioritisation will be required according to the incident’s
may have to realign themselves appropriately as part
complexity, duration and the impact on ambulance
of the recovery process.
operations, health services and the wider community.
Act
At the national level ambulance recovery coordination
To perform the liaison function appropriately will
following a complex and nationally significant
require timely access to Ambulance Service Sitreps,
emergency shall be based on the requirements of the
intelligence as well as action plans. There will also
local Ambulance Services and / or the needs of the
need to have an understanding of the ambulance
health sector locally, regionally and nationally.
sector’s current resource status and immediate and
future resource requirements. This may be done most
The Ambulance Services shall consider recovery
effectively by an Emergency Management Information
functions as part of the NCCC.
System (EMIS).
Part 3 has outlined the range of recovery issues for an
The NCCC shall assist with the implementation of key
Ambulance Service.
Information
health sector emergency plans such as the National
Mass Casualty Transport Plan.
4.2 Recovery Roles and Responsibilities
3.7 Media
All key functions to be carried out as part of the NCCC
(see Part 4 Section 3.5 above) shall have recovery
Media representatives will arrive at the scene
actions noted as part of role descriptions. A role
following a major incident. Media will also go to
description of the Recovery Coordinator shall be
Official
hospitals and any other sites where there is a
considered.
possibility of information on the incident including the
numbers of injured and deceased etc.
4.3 Debrief and Reporting Processes
the
All staff shall be aware of and follow their
organisation’s media policies.
4.3.1 Debrief aims and requirements
For all incidents, an Ambulance Service Public
The aim of the debrief process is two-fold:
Information Manager will be available to manage
To identify and acknowledge where the response
under
local inquiries from the media with appropriate
went well and ensure that these experiences are
other agencies.
shared
At a national level, the NCCC will be required to
To identify where improvements in the response
contribute with media releases by the NHCC and other
is required and develop a plan of action to ensure
similar national agencies. It is the NHCC that will
that learning occurs.
coordinate all Public Information for the Health Sector
as a whole.
An Ambulance Service shall have debrief processes as
specified in Part 3 Section 4.4. The NCCC shall have
Released
3.8 Resources
similar processes in place.
The NCCC shall specify what resources will be required
4.3.2 Major Incident Reporting
to support a local operational Ambulance response
An Ambulance Service shall have reporting processes
for a sustained period. These will include, but are not
as specified in Part 3 Section 4.4. The NCCC shall
limited to, appropriate and trained Human Resources to
have similar processes in place to capture lessons to
fulfil key functions specified above, appropriate facilities
assist future planning and service improvement.
(for example, an ASEOC) and tools.
All logs and notes made during the incident in the NCCC
level will need to be correlated and stored in case of
possible inquiries into incident management.
PART 4 SEPT 2016
5
Appendices
Appendix 1: Glossary of Terms and Abbreviations
Appendix 2: References
Appendix 3: STEP 1-2-3 scene approach rule
Appendix 4: Task Cards for First Responding Ambulance to a possible
major incident
1982
Appendix 5: Triage Tools and Tags (Review continuing)
Appendix 6: Information Management Tools
Act
Appendix 7: Ambulance Scene Task Cards
Appendix 8: Sector numbering – examples
Appendix 9: Vest and role labels
Appendix 10: Ambulance Commander After Action Report Template
Information
Appendix 11: Business Continuity Plan example template
Appendix 12: Tactical Plan Template Official
Appendix 13: MCDEM and MoH alerts
Appendix 14: Ambulance MI Notifications List (Guideline)
the
Appendix 15: Major Incident Task Cards for an Ambulance Service EOC (ASEOC)
Appendix 16: Guideline for ASEOC set up
under
Appendix 17: ASEOC & NCCC Debrief and Reporting Tools
Released
6
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
Notes:
1982
Act
Information
Official
the
under
Released
PART 4 FEB 2016
7
Notes:
1982
Act
Information
Official
the
under
Released
8
NEW ZEALAND AMBULANCE MAJOR INCIDENT AND EMERGENCY PLAN (AMPLANZ)
Notes:
1982
Act
Information
Official
the
under
Released
PART 4 FEB 2016
9


1982
Act
Information
Official
the
under
Released
Document Outline