

Quarantine & Isolation
Capability
Self-Quarantine Framework
RNZ Re-visited
RELEASED UNDER THE
A consolidation of the lessons learnt from the MIQ self-isolation pilot and the reconnecting New Zealand framework.
OFFICIAL INFORMATION ACT 1982
Version 0.2 - Final
29 July 2022

 Document Control
Document Control
Formal approval of this document is the prerogative of the Chief Executive of the Ministry of Business, Innovation and
Employment (MBIE).
Version
Date
Description
Consultation
0.1
29 June 2022
Development of the Self-
Document Creation.
Quarantine Plan
For review.
0.2
1 July 2022
Review and revision of the plan
Reviewed by Programme Director and Project
Lead.
Feedback incorporated.
0.2
21 July 2022
Final review and endorsement
Programme Director and Project Lead
program director
0.2
26 July 2022
Incorporate NZ Customs, NZ
GM & DCE consultation
Police, Health feedback. Final
review GM MIQ and DCE
Document Location
REF
Last Save
Location
127722050
4 July 2022
https://mako.wd.govt.nz/otcs/llisapi.dll?func=ll&objaction=overview&objid=127722050
Document Security
RELEASED UNDER THE
This document is the property of the New Zealand Government and contains official information protected by law. It is
classified as
IN CONFIDENCE. The document is to be safeguarded in accordance with the Protective Security requirements
that can be found at protectivesecurity.govt.nz.
OFFICIAL INFORMATION ACT 1982
IN CONFIDENCE
Page 2 of 17
link to page 2 link to page 2 link to page 2 link to page 3 link to page 4 link to page 5 link to page 5 link to page 5 link to page 6 link to page 6 link to page 7 link to page 7 link to page 8 link to page 9 link to page 10 link to page 11 link to page 13 link to page 14 link to page 14 link to page 16 link to page 16 link to page 17 link to page 17 link to page 17

 Contents
Document Control ......................................................................................................... 2
Document Location ........................................................................................................ 2
Document Security ........................................................................................................ 2
Contents ........................................................................................................................ 3
Glossary ......................................................................................................................... 4
Overview ....................................................................................................................... 5
Objective ............................................................................................................................................................................. 5
Assumptions ........................................................................................................................................................................ 5
Important context for the self-quarantine framework ....................................................................................................... 6
Public Health view on application of the framework .......................................................................................................... 6
The Self-Quarantine System Components ...................................................................... 7
Reconnecting New Zealanders Medium Risk Pathway ....................................................................................................... 7
Compliance Strategy ........................................................................................................................................................... 8
Self-Isolation Pilot for Business Travellers .......................................................................................................................... 9
Traveller Health Declaration System ................................................................................................................................. 10
End to End Self Quarantine Framework ....................................................................... 11
Implementation Challenges and Opportunities ............................................................ 13
APPENDIX 1 ............................................................................................................................................. 14
Contents
Document Control ......................................................................................................... 2
Document Location ........................................................................................................ 2
Document Security ........................................................................................................ 2
Contents ........................................................................................................................ 3
Glossary ......................................................................................................................... 4
Overview ....................................................................................................................... 5
Objective ............................................................................................................................................................................. 5
Assumptions ........................................................................................................................................................................ 5
Important context for the self-quarantine framework ....................................................................................................... 6
Public Health view on application of the framework .......................................................................................................... 6
The Self-Quarantine System Components ...................................................................... 7
Reconnecting New Zealanders Medium Risk Pathway ....................................................................................................... 7
Compliance Strategy ........................................................................................................................................................... 8
Self-Isolation Pilot for Business Travellers .......................................................................................................................... 9
Traveller Health Declaration System ................................................................................................................................. 10
End to End Self Quarantine Framework ....................................................................... 11
Implementation Challenges and Opportunities ............................................................ 13
APPENDIX 1 ............................................................................................................................................. 14
Self-Isolation Pilot – Summary of Trial .................................................................................................... 14
APPENDIX 2 ............................................................................................................................................. 16
Standard Operating Procedures – Self Isolation Pilot ............................................................................ 16
APPENDIX 3 ............................................................................................................................................. 17
Location Monitoring Border Arrivals Self Isolating Under the Medium Pathways – Minister Briefing
Paper ....................................................................................................................................................... 17
RELEASED UNDER THE
OFFICIAL INFORMATION ACT 1982
IN CONFIDENCE
Page 3 of 17

 Glossary
Glossary
AoG
All of Government
BAU
Business As Usual
COVID-19
Illness caused by the novel SARS-CoV-2 virus
Facility
A contracted hotel for persons to stay as directed by the government for a period of
quarantine or isolation
Isolation
Isolation separates sick people with a contagious disease from people who are not sick.
P&C
People and Culture
MAKO
MBIE electronic document storage system
MBIE
Ministry of Business, Innovation and Employment
MIQF
Managed Isolation & Quarantine Facility
MoH
Ministry of Health
MOU
Memorandum of Understanding
NPHS
National Public Health Service
OGAs
Other government agencies
RELEASED UNDER THE
QIC
Quarantine and Isolation Capability
Quarantine
Separates and restricts the movement of people who were exposed to a contagious
disease to see if they become sick. These people may have been exposed to a disease and
do not know it, or they may have the disease but do not show symptoms.
OFFICIAL INFORMATION ACT 1982
Self-Quarantine
Quarantine that occurs at a person’s home or other approved location, not at a
government approved facility
SOP
Standard Operating Procedure
IN CONFIDENCE
Page 4 of 17


TKM
Te Kawa Mataaho Public Service Commission
Overview
Objective
The purpose of this document is to consolidate knowledge and information sources that MBIE have obtained on self-
quarantine for border arrivals since late 2020. It also revisits the Self Quarantine framework agreed across government to
implement the first step of Reconnecting New Zealanders.
The self-quarantine response in early 2020 as the first step to respond to the COVID-19 pandemic was delivered by Ministry
of Health (MoH). The later design in 2022 of Reconnecting New Zealanders (RNZ) was led by DPMC with MBIE coordinating
government agencies to provide an end to end framework, including a minimal compliance model for enforcement of
Regulation breaches. MBIE did not have responsibility for delivery of any of the elements included in the framework,
including the compliance enforcement strategy, other than building the model.
In late 2021 MBIE designed, led, and implemented a pilot for self-isolation for business travellers. The design of the self-
isolation pilot was agreed by Cabinet as part of RNZ work programme and MBIE was the lead agency for delivering the pilot.
This document is not intended to design an All of Government self-quarantine framework. Instead, it presents the previously
developed RNZ framework for self-isolation with the responsibility for delivery sitting with the Government agencies
responsible for the functional area.
This report is for information only and collates all information related to self-quarantine into one resource document to
inform future decision making on self-quarantine, if required. Whilst this document provides information related to MBIE-led
self-quarantine, there are other resources and learnings from health-led self-quarantine that would also be valuable i.e., the
domestic self-quarantine and self-isolation response (Care in the Community).
Note that this plan provides a framework for Self-Quarantine using the standard definitions. Previous activities in this space
have referred to Self-Isolation however we are no longer using this terminology to better align with correct health system
definitions.
Assumptions
The following assumptions exist in relation to the Self-Quarantine framework:
•
RELEASED UNDER THE
Self-quarantine is for persons legislated to do so on arrival into New Zealand, this is likely to include those at risk of
having been exposed prior to or during international travel
•
All inbound travellers would be required to self-quarantine for an agreed period (7-14 days previously) on arrival at
New Zealand’s border, to limit the spread of a future Covid-19 variant. This quarantine period would be established
based on public health advice.
•
The self-quarantine framework may be considered in the following scenarios:
̵
Self-quarantine only
OFFICIAL INFORMATION ACT 1982
̵
Self-quarantine while the Quarantine and Isolation Capability (QIC) is being implemented (QIC replaces self-
quarantine after 3-4 weeks)
̵
Self-quarantine or QIC pathway - hybrid model (some travellers being directed to self-quarantine and some
travellers being directed to a MIQ facility)
IN CONFIDENCE
Page 5 of 17


•
The conditions for which self-quarantine as an appropriate response framework may change over time and is
contingent on balancing the risk posed by the Covid or other disease variant and the government strategy.
Important context for the self-quarantine framework
MBIE do not have the resources or expertise in place to develop a new AoG self-quarantine system on behalf of government.
The reconnecting New Zealanders AoG framework for self-isolation blueprint, included in this document, details how the
plan was intended to be operationalised when self-isolation for border returnees was first introduced in early 2022, it is
therefore a starting point. This framework was built on a high trust, low touch, diminishing health risk model at the time it
was implemented.
Public Health view on application of the framework
Consistent with the Variants of Concern Strategic Framework, the threshold for using elimination approach measures
including the use of managed quarantine, and self-quarantine is particularly high. In most situations Health would prefer to
use domestic public health measures that have been shown to be effective during the course of the pandemic, and apply
these to arrivals. This reflects both the increased level of immunity in the community, and the changing nature of social
license. This also reflects the increased transmissibility that we are likely to see with new Variants of Concern.
An elimination approach is only likely to be used where a range of the following factors are present:
̵
If there were indications of very high clinical severity and likely high fatality rates
̵
Transmissibility levels that could be managed with strong border measures
̵
There are high levels of immune escape and current immunity levels are likely to be ineffective
̵
There would be clear benefits that could be realised in the time that the measures could be sustained
̵
For a health system that is already under pressure, a new variant of concern is likely to place the health system
under extreme pressure
̵
Where at-risk communities are likely to be severely affected.
If a decision were made to close the border in response to a variant of concern (VOC) and commence the stand-up of the QIC
to manage returnees, then in the intervening four weeks there would be a requirement to implement some form of self-
quarantine/isolation, unless the borders were fully shut to all incoming travellers (unless the borders were fully shut to all
incoming travellers, which has never been done – not even during 2020 and the full Elimination Strategy).
The starting point for running self-quarantine at the border as an interim measure would be the current self-isolation
settings, where arrivals are required to test using rapid antigen tests on day 0/1 and day 5/6. Arrivals who currently test
positive are required to self-isolate for 7 days.
RELEASED UNDER THE
Self-quarantine for arrivals would likely include:
a.
self-quarantine until they return a negative test on day 0/1 or day 5/6.
b.
the framework designed for the Reconnecting New Zealanders Strategy (RNZ)
c.
support from Care in the Community networks where appropriate.
OFFICIAL INFORMATION ACT 1982
However, there are a range of considerations and factors that would inform the public health advice regarding the
appropriate settings for self-quarantine for international travellers in any situation, including:
1.
Public health risk context: what is the public health risk posed by international travellers, relative to the domestic
public health risk? It is likely that given our current border settings, any high-risk VOC will already have seeded in the
country and circulating by the time it is identified as a high risk VOC. Additionally, the international risk relative to
domestic risk is likely to change rapidly as the VOC becomes more prevalent in Aotearoa New Zealand (i.e., the
IN CONFIDENCE
Page 6 of 17


international risk is likely to diminish relative to domestic risk fairly rapidly). This means that self-quarantine settings
will need to adjust rapidly to reflect this changing risk profile, in order to remain proportionate and justifiable.
2.
Purpose/Intent: what is the purpose/intent of implementing a self-quarantine pathway? This is intrinsically linked to
the public health risk context – if the VOC is already seeded and circulating in the country, implementing self-
quarantine for international travellers is likely to have limited value in preventing onward transmission of the VOC to
the community. In such a situation, the intent is more likely to be to limit new seeding events, to slow the spread of
the VOC. This means that some degree of risk or ‘leakage’ associated with the self-quarantine settings and pathway
is more acceptable (e.g., the use of public transport to travel to a self-quarantine location, with appropriate
mitigations such as mask use).
3.
Other public health measures: what other public health measures are in place, or can be strengthened, to mitigate
risk? There are a suite of public health measures available that can be implemented and/or strengthened to reduce
the impact that a VOC may have on the community. These may complement self -quarantine for international
arrivals. These measures include implementing pre-departure testing, strengthening contact tracing (criteria and
resource challenges) for cases infected with the VOC, and adjusting quarantine/isolation periods and testing
frequency to reflect changing risk tolerances. The deployment of additional public health measures may mean that a
high-trust self-quarantine model is an acceptable approach to achieving the purpose of implementing self-
quarantine, in a given public health risk context.
Ultimately, the public health advice regarding which self-quarantine settings are appropriate in any situation will need to
consider the public health risk posed by international travellers to the community relative to the domestic risk, the intent of
implementing self-quarantine requirements for travellers, via air and maritime borders, and the range of other public health
measures that are in place (or could be deployed/strengthened) in response to the risk posed by the VOC.
The Self-Quarantine System Components
The starting point for running self-quarantine at the border as an interim measure would be the current settings, where
arrivals are required to test using rapid antigen tests on day 0/1 and day 5/6. Arrivals who currently test positive are required
to self-isolate for 7 days. Self-quarantine for arrivals would likely draw on these provisions, for example they may need to
self-isolate until they return a negative test on day 0/1 or day 5/6. We would also draw on the framework designed for the
Reconnecting New Zealanders Strategy (RNZ) and be supported by Care in the Community where appropriate.
Reconnecting New Zealanders Medium Risk Pathway
RELEASED UNDER THE
The RNZ strategy set out a staged approach for reopening our air and maritime borders based on passenger risk. The
requirements for each pathway that have evolved throughout the pandemic has a clear plan for self-quarantine as part of the
medium risk pathway for travellers and outlined core requirements that travellers had to meet to be eligible. The
requirements at the time being:
•
Proof of having completed a primary course of COVID-19 vaccination
•
Completion of a pre departure test before travel
OFFICIAL INFORMATION ACT 1982
•
A passenger declaration about travel history
•
Taking and reporting the results of a Rapid Antigen Test (RAT) on day 0/1 and 5/6
•
A requirement to self-quarantine for seven days, and
•
A final negative test before ending quarantine and entering the community.
IN CONFIDENCE
Page 7 of 17


Compliance monitoring for testing requirements was undertaken by the MoH through automated email and text reminders.
No follow up phone calls were conducted unless a traveller registered a positive result. Testing requirements were subject to
change.
Infringement offences were created for failing to complete required test (MOH) / inaccurately report test (MOH) / fail to
remain in quarantine location (serious breaches NZ Police). There were no proactive enforcement measures in place and no
compliance monitoring. There was only a reactive response available in cases of serious reported breaches.
As part of the Reconnecting New Zealanders pathways, work was also undertaken to:
•
identify appropriate settings for groups to enter quarantine together in specific circumstances
•
allow eligible sports and cultural groups to train or rehearse together
•
identify special circumstances where people may leave.
Compliance Strategy
Self-isolation under RNZ was set up as a high trust, low touch model and created infringement offences specific to self-
isolation. However, no agency had the capacity to perform the enforcement function, other than NZ Police in instances
where there was a high public health risk.
In summary that RNZ model provided:
•
NZ Police have powers to make further enquiries to determine if there had been a breach of self-quarantine
requirements. NZ Police proposed a graduated enforcement approach for those breaches which are prioritised as
presenting significant public health risks, balanced against other operational demands
•
Customs enforced infringement offences that were detected at the border relating to breaches of pre departure
testing, unvaccinated travellers, non-completion of the required traveller declaration and breaches committed by a
carrier bringing persons to New Zealand who did not meet entry requirements
•
Health had responsibility for Infringement offences for failing to complete testing requirements or inaccurately
reporting test results.
Enforcement Limitations
High trust models have served New Zealand well throughout this pandemic. Most returnees did the right thing to help
protect the New Zealand community by complying with their self-isolation requirements.
RELEASED UNDER THE
The monitoring of those in self-quarantine needs to be consistently applied, but also proportionate to the public health risk
posed by non-compliance. This approach was challenging because the public health risk posed by non-compliance is highly
dynamic and can shift rapidly as the domestic risk situation evolves (e.g., within days sometimes). Parity between border
cases and community cases also needs to be proportionate, unless border arrivals present a higher risk. Then there is a
justification for differential treatment.
There are a number of limitations with the RNZ compliance model including:
•
Travel to self-quarantine destination from the airport allows the returnee to mix with NZ community members e.g.
OFFICIAL INFORMATION ACT 1982
bus, taxi, uber, domestic air travel, family collection
•
Public Health Advice may require a test at the airport on arrival into New Zealand. If the advice requires health staff
administered or supervised staffing for this would need to be provided, as would a location for this activity to occur.
This proposal was explored in RNZ but discounted given the operational challenges to deliver. Alternatively for self-
administered testing compliance checking would still need to be staffed.
IN CONFIDENCE
Page 8 of 17


•
The process for returnees who test positive on arrival into New Zealand is that the returnee travels to their place of
self quarantine and then self-quarantines under the care in the community framework, like any domestic cases. The
only difference is that the traveller is asked to get a PCR test to enable whole genome sequencing, for the MOH
surveillance work.
•
There is currently a reliance on returnees completing a NZ Traveller Declaration (NZTD) prior to travel, which includes
information on how contact can be made with the traveller once in New Zealand, including physical address, phone
number and email address. There is no mention in the current version of NZTD of a location for self-quarantine.
Without this information being collected and made available compliance activities are not possible.
•
Should self-quarantine information be collected there is no verification process or resourcing to confirm the address
information given in the NZTD, so false/incorrect addresses or unsuitable addresses for self quarantine such as shared
accommodation addresses could be provided.
•
There is no monitoring to ensure compliance with the requirement to remain at the reported address1. Whilst options
have been considered, none have been agreed to be suitable for self-quarantine purposes.
•
A returnee can self-quarantine with others who are not subject to any restriction on movement unless the returnee
tests positive.
•
A tool for the public to report non-compliance of self-quarantine requirements was created, however a resource to
receive, triage or action these reports needs to be identified for implementation.
•
NZ Police may undertake enforcement action if a breach poses a significant public health risk.
Self-Isolation Pilot for Business Travellers
A self-isolation pilot for business travellers was designed and implemented to test some of the processes for isolation in the
community as an alternative to managed isolation and quarantine for low to medium risk international business travellers.
This pilot was part of the RNZ work programme to plan for a phased border reopening.
The self-isolation pilot covered:
•
The border system and processes
•
The delivery of services in self-isolation
•
Monitoring, compliance, and enforcement
•
The participant experiences
•
The experience of other stakeholders.
RELEASED UNDER THE
The pilot was designed to include up to 150 travellers arriving at Auckland or Christchurch between 30 October and
18 December 2021. Businesses were asked to submit expressions of interest (EOI) in the pilot via an online portal.
Information was collected through this process to check that applicants met the strict eligibility criteria and therefore could
be considered low-medium risk.
79 participants successfully completed self-isolation through the pilot programme from 30 October to 18 December 2021.
OFFICIAL INFORMATION ACT 1982
1 A cross agency Cabinet paper on ‘location monitoring’ of border arrivals using the self-isolation model under the medium risk pathway can be found at
Appendix 2.
IN CONFIDENCE
Page 9 of 17


Key findings from the pilot can be found in Appendix 1. One of the most significant findings was that none of the processes
included in the pilot could be scaled up.
Traveller Health Declaration System
Everyone travelling to New Zealand by air must now complete a New Zealand Traveller Declaration (NZTD) prior to check-in
at the airport.
The information collected, which includes COVID-19 vaccination status, is used to let travellers know what they need to do
when they arrive in New Zealand: such as self-test on arrival or enter self-quarantine.
Returnees need to complete a NZTD and be issued with a Traveller Pass to board their flight to New Zealand and must show
their pass on arrival in New Zealand.
The complexity of digital and operational systems that the NZTD needs mean that it is being developed in stages. The first
version came into effect in March 2022. Changes are made to the system as requirements for returnees change and alerts
are sent to returnees to inform them of these changes. These alerts are not automated and require a manual process to
identify email addresses and send notifications of any pending changes.
The New Zealand Customs Service is administering this system and programme of work.
RELEASED UNDER THE
OFFICIAL INFORMATION ACT 1982
IN CONFIDENCE
Page 10 of 17

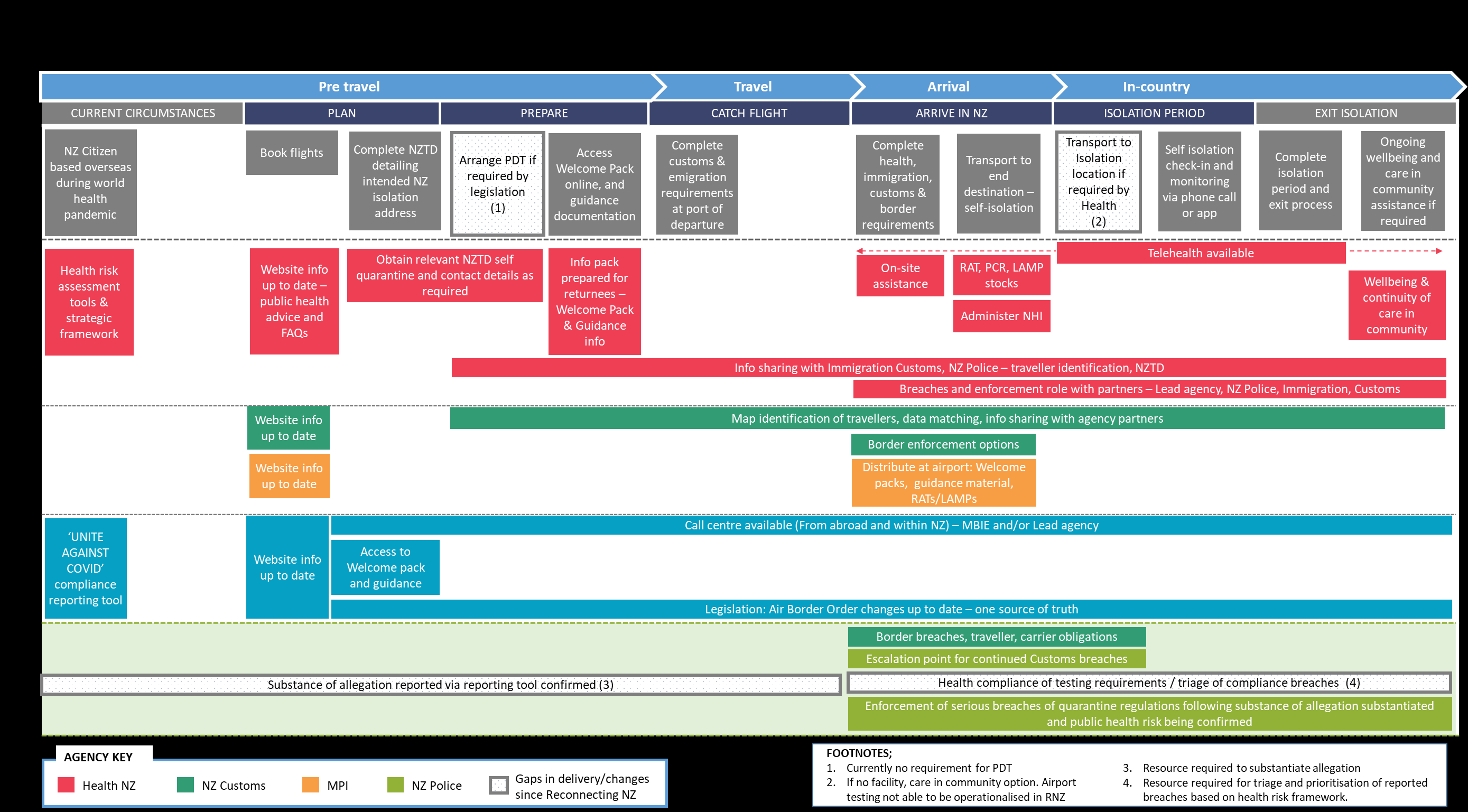
 End to End Self Quarantine Framework
End to End Self Quarantine Framework
Please see below the
End-to-End Self Quarantine framework. This is the RNZ model with modifications to represent advances
in technology i.e., availability of LAMP, and introduction of NZTD and inclusion of the Health and Wellness framework and
use of telehealth services. Testing modalities will be directed by public health.
The model proposes no more than what was previously agreed by agencies as part of the RNZ border opening, and the 72-
hour period when the model and requirement to self-isolate was operational. This model represents a point in time
agreement by agencies to perform certain functions. Further work is needed to understand if these agencies have the
capacity to operationalise in a future environment, or any options for improvement.
RELEASED UNDER THE
OFFICIAL INFORMATION ACT 1982
IN CONFIDENCE
Page 11 of 17



RELEASED UNDER THE
OFFICIAL INFORMATION ACT 1982
Page 12 of 17

 Implementation Challenges and Opportunities
Implementation Challenges and Opportunities
The challenges in implementing a self-quarantine model to address any of the variant scenarios are:
•
The integrity, reporting and availability of reliable pre departure testing
•
NZTD further development is needed to capture information to support a self-quarantine model to ensure quarantine
addresses are recorded accurately and can be shared with enforcement agencies
•
Privacy Impact Assessment (PIA) for information sharing that allows Health access to the information is in place
currently, however if changes are to be made to the information that the system collects, the purpose it is collected
for and who it is to be shared with, a new PIA will be required.
•
Border enforcement options for travellers that have not completed NZTD has a significant dependency on NZ Customs
•
A process and resource is required to determine if the self-quarantine location is suitable, i.e., internet connection for
monitoring, family in location, health risk posed by travel? Self-quarantine location address not validated
•
Border testing of arrivals. It is necessary to allow the returnee to travel to place of self-quarantine? LAMP or RAT
testing at the border options. Identification of the resource and location to perform this function is needed. This
process was considered and discounted as part of RNZ given the challenges to operationalise.
o Airport location required for testing before scheduled onward travel, Auckland, and Christchurch airport
authorities’ dependency
o Resource required to supervise testing and recording into Health data base. dependency on National Public
Health Service (NPHS)
•
Returnee travel to location to start self-quarantine. Public transport required. Issues arise if the returnee cannot
reach destination in single day i.e., stop over required as driving or ferry crossing needed
•
Arrive at location and commence self-quarantine and compliance testing. Dependency on testing monitoring by NPHS
•
Compliance monitoring tool for reporting of breaches by Members of Public on the Unite Against COVID-19 website
requires resourcing for the triage and prioritisation process, based on public health risk model.
•
Rules governing movement once the returnee commences self-quarantine must be simple and easy to enforce if a
breach is identified. In RNZ there were a large number of exemptions allowing a person to leave their address
permitted in the various orders. These exemptions cannot necessarily be distinguished by a member of the public
reporting a breach.
•
There is no dedicated agency to investigate reported breaches. NZ Police commitment in RNZ was to investigate
established, serious breaches. Resourcing would be required to complete investigative functions before referral to NZ
RELEASED UNDER THE
Police.
•
Not every returnee crossing the border has a place to quarantine i.e., a home, or if they do, it may be unsafe to do so
due to vulnerable people living there. There needs to be alternate options identified for these people.
OFFICIAL INFORMATION ACT 1982
IN CONFIDENCE
Page 13 of 17

 APPENDIX 1
Self-Isolation Pilot – Summary of Trial
APPENDIX 1
Self-Isolation Pilot – Summary of Trial
79 participants successfully completed self-isolation through the pilot programme from 30 October to 18 December 2021.
Regarding the Application Process
•
A two-stage expression of interest and ballot successfully identified 81 participants to trial home isolation as an
alternative to MIQ, for a closely monitored approach to self-isolation. 79 individuals participated in the pilot
•
The strict criteria adopted for the pilot per Cabinet’s agreement, including the requirement to isolate close to the port
of arrival, meant that options for participation were severely limited for travellers living outside Auckland. There were
few international flights scheduled into Christchurch (none from Australia and only from Singapore).
Regarding the Arrival Process and Transfer to self-isolation
•
The processes to identify and separate self-isolating travellers from travellers going to managed isolation and
quarantine (MIQ) worked effectively and smoothly
•
Airports put in place systems that would cater for the number of people expected to participate in the pilot. The small
size of the pilot limited the extent to which systems were fully tested, as the highest number of arrivals was four on
any flight
•
In Auckland, Rapid Antigen Testing was done for all pilot participants. The test extended the transfer time in the
airport by 14-15 minutes for each individual
•
It is the view of the airports that undertaking COVID-19 testing at the border at scale is not operationally viable
because of space constraints to safely accommodate large numbers of people being tested on-site, and the risks and
costs of delays to passenger disembarkation if arrival halls are not cleared quickly
•
Overall, the use of commercial transport providers to drive participants to their place of self-isolation was highly
successful with few incidents
Regarding the participant experience of self-isolation
•
The opportunity to travel internationally for business was valued by participants
•
Most participants were satisfied or very satisfied with their self-isolation experience
RELEASED UNDER THE
•
Most participants found the self-isolation experience easy. The key themes in the participant feedback were that the
number of tests, the length of the required self-isolation was perceived as excessive, and that the challenges became
harder after the first few days, including being bored and lonely and separated from loved ones.
Regarding Health checks during self-isolation
•
During their stay in self-isolation, regular saliva-PCR tests were taken. In Christchurch where health workers
OFFICIAL INFORMATION ACT 1982
supervised the collection of the tests there were no insufficient samples. In Auckland, where tests were unsupervised,
there were a small number (six) of insufficient tests. The implications of these observations need to be considered
alongside experience from other situations where saliva testing is used.
•
The pilot faced operational challenges from implementing a targeted programme at the same time as the nation-wide
introduction of three days home isolation for travellers after seven days of MIQ, and increased demand for health
IN CONFIDENCE
Page 14 of 17


support to deliver health checks for self-isolating community cases. In a wider roll-out the priority and mechanism for
health checks for returnees will need to be weighed against other demands due to cases in the community.
Regarding Monitoring during self-isolation
•
Monitoring of pilot participation was effective, with no breaches identified. However, the participant views on
monitoring were varied, with some welcoming the daily interactions with the monitoring staff and others finding the
phone calls intrusive.
•
More advanced technological methods for tracking, using GPS tracking devices and other technologies were
advocated for by some participants.
•
From the perspective of the monitoring company the approach was a high-trust model, which relied on establishing a
good relationship between the participant and the monitoring staff. This view aligns with participant views that it
would be possible to evade the monitoring if you wanted to.
Regarding data collection and information sharing
•
Multiple agency involvement requires that information is speedily, efficiently, and securely shared to facilitate a clear
self-isolation pathway for travellers. Given the small scale of the pilot, the processes used were mostly manual.
•
The model of self-isolation will determine the extent of information collection and sharing required, but to handle
large volumes of travellers it will not be feasible to use manual processes. Manual processes are not only resource
heavy but also introduce privacy and security risks as it is not possible to track and monitor all data access and use.
•
Overall, while manual in nature, the information sharing processes put in place for the pilot worked well to ensure
that all partner agencies received the information required for their part in the process.
Regarding Communications
•
Communications using multiple methods were necessary to engage with stakeholders such as the airports and health
services, iwi, partner agencies and pilot participants. The communications were effective because they used multiple
digital channels, and because they could be revised to take account of the changes to the pilot requirements and in
response to feedback as the pilot progressed.
RELEASED UNDER THE
OFFICIAL INFORMATION ACT 1982
IN CONFIDENCE
Page 15 of 17

 APPENDIX 2
Standard Operating Procedures – Self Isolation Pilot
Links to developed standard operating procedures developed by MBIE for the self-isolation pilot,
APPENDIX 2
Standard Operating Procedures – Self Isolation Pilot
Links to developed standard operating procedures developed by MBIE for the self-isolation pilot,
however we do not recommend these are used are as follows:
SIP Transport SOP.docx
Manage participant compliance monitoring v1.0.docx
Urgent issues after hours (1).docx
SIP Arrival in NZ SOP.docx
Manual eligibility check SOP V0.3 final.docx
SIP Allocate Voucher SOP.docx
Identify eligible applications SOP final.docx
Manage compliance exceptions v1.0 final.docx
Manage exit SOP.docx
RELEASED UNDER THE
OFFICIAL INFORMATION ACT 1982
IN CONFIDENCE
Page 16 of 17

 APPENDIX 3
Location Monitoring Border Arrivals Self Isolating Under the Medium Pathways – Minister
APPENDIX 3
Location Monitoring Border Arrivals Self Isolating Under the Medium Pathways – Minister
Briefing Paper
LINK: 2122-2166 SIGNED location monitoring border arrivals self-isolating unde... (2).pdf
RELEASED UNDER THE
OFFICIAL INFORMATION ACT 1982
IN CONFIDENCE
Page 17 of 17