
Document 1
Memo
Review of COVID-19 Protection Framework settings – 27 July 2022
Date:
1 August 2022
1982
To:
Dr Di Sarfati, Director-General of Health
Copy:
Dr Harriette Carr, Acting Director of Public Health
ACT
Dr Richard Jaine, Deputy Director of Public Health
Dr Robyn Carey, Chief Medical Officer
Dr Ian Town, Chief Science Advisor
Dr Nick Chamberlain, Director, National Public Health Service
Gerardine Clifford-Lidstone, Director, Pacific Health
John Whaanga, Deputy Director-General, Māori Health
INFORMATION
Maree Roberts, Deputy Director-General Strategy, Policy and Legislation
From:
Dr Andrew Old, Deputy Director-General, Public Health Agency
For your:
Decision
OFFICIAL
Purpose
THE
1.
This memo provides you with advice following the 27 July 2022 COVID-19 Protection
Framework Assessment Committee’s (the Committee) regular review of:
a. COVID-19 Protection Framework (CPF) colour settings, and
UNDER
b. isolation and quarantine periods for cases and household contacts.
Background and context
2.
The objective of the CPF is to minimise the impact of, provide protection from, and slow
the transmission of COVID-19. It seeks to minimise COVID-19 hospitalisations and
deaths through vaccination and other public health measures, such as mask use.
RELEASED
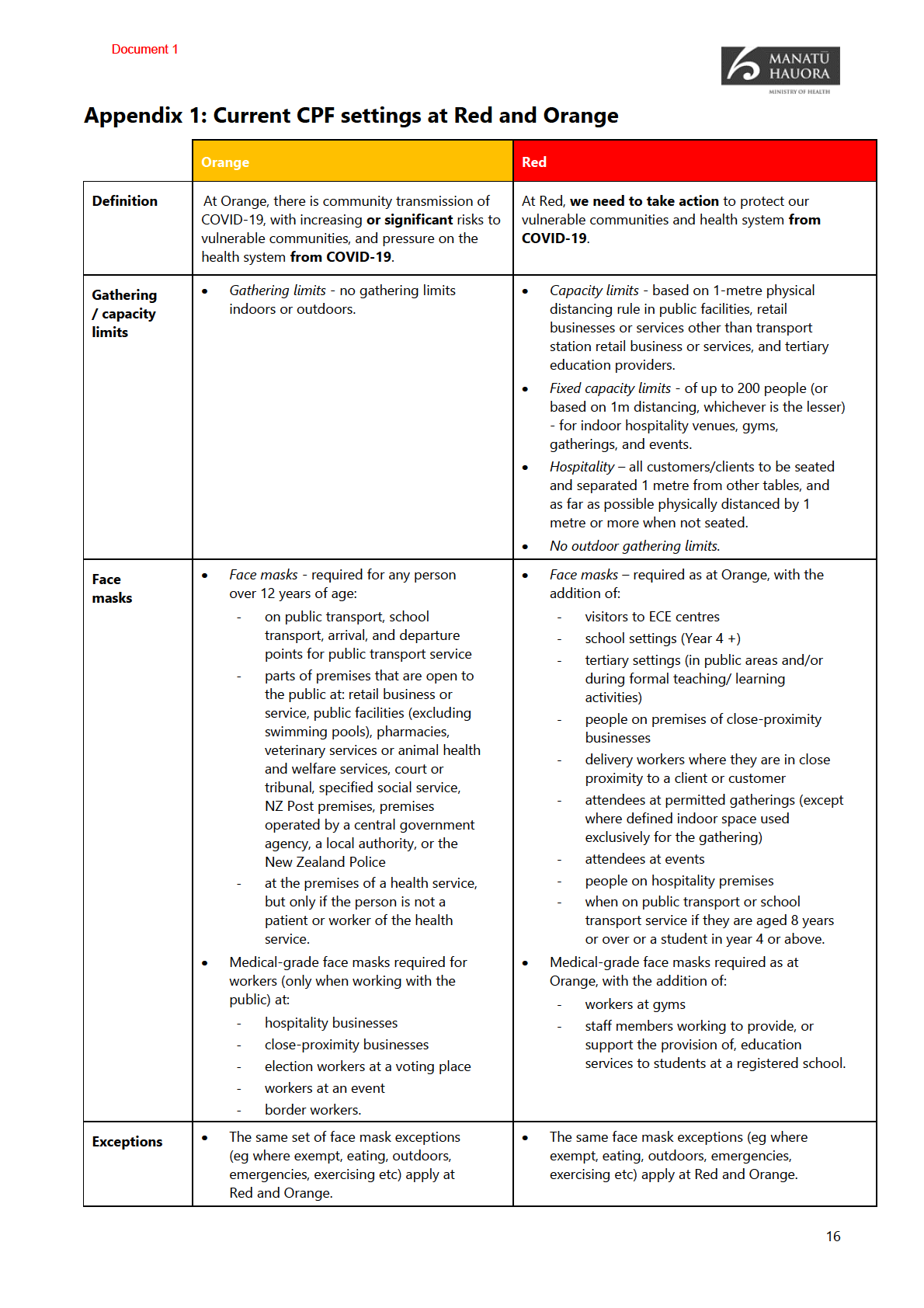
Appendix 1 outlines current measures at the Orange and Red CPF settings.
3.
The purpose of the Committee is to advise you on appropriate CPF levels and other
related matters. Once approved by you, this advice informs overarching Department of
the Prime Minister and Cabinet (DPMC) advice on CPF settings to COVID-19 Ministers.
1

Document 1
The last standard CPF Assessment was held six weeks ago
4.
The last standard CPF Assessment was on 15 June 2022. It recommended that all parts of
the country should remain at Orange; to keep isolation period for cases and household
contacts at 7-days; and to maintain mask settings for schools, airports, and aircraft. A
rapid review of the Red setting measures, and whether mask requirements at Orange or
Red should be strengthened was also recommended (outlined below).
Related work since the last standard CPF Assessment in mid-June
5.
Since the last standard CPF Assessment meeting on 15 June 2022, the following related
1982
pieces of work have been commenced or completed by Manatū Hauora and others:
a.
Winter Package – announced on 14 July 2022, this aims to manage the high case
and hospitalisation rates due to COVID-19 and other winter illnesses. It included
ACT
measures to expand access to therapeutics and vaccination for COVID-19 and flu;
expand eligibility for antivirals, including removing prescription requirements for
eligible groups; and expand access to free rapid antigen tests (RATs) and masks.
b.
Rapid review of Red CPF measures and mask requirements – on 14 July 2022 the
Committee considered whether to expand mask requirements across the Red and
Orange; and/or to reduce gathering limits at Red. No changes were recommended
at that time, but supported work to improve messaging, testing, and ventilation.
INFORMATION
c.
Masks in schools – delivered with the Ministry of Education from 21 July 2022 this
work supports improved mask-wearing in schools and includes a joint advice that all
schools review their mask policies and, if appropriate, require four weeks of indoor
mask wearing where students gather; greater sharing of district infection trend
information to support decision-making; and advice on improving ventilation.
6.
OFFICIAL
This standard CPF review occurred two weeks later than usual. This delay was intended
to enable the Committee to better gauge the early effectiveness of the Winter Package
and other work noted above and provide a better basis for the Committee to consider
THE
whether to maintain the current Orange CPF setting or whether a shift was required.
Current outbreak status
7.
Further detail on the current outbreak and modelling is provided at
Appendix 2.
UNDER
8.
In
the two weeks since 17 July 2022, case rates have decreased by twelve percent.
For the week ending 24 July 2022, the current hospitalisation rate is 15.2 per 100,000, up
seven percent on the prior week.
9.
Current modelling suggests that
COVID-19 cases may have peaked at approximately
11,000 cases in mid-July 2022. However, recent trends may be affected by school
holidays and a reduction of mixing that is affecting testing behaviour and transmission.
RELEASED
10.
Wastewater detections across New Zealand have also tapered slightly and are still
close to the levels during the Omicron peak in March 2022. This indicates that the
number of new cases is reasonably stable.
11.
Case rates across all age groups also plateaued over the past week. However, case rates
are highest for those who are aged 65 or older. Compared to the Omicron peak in
2

Document 1
March 2022, case rates are higher for those who are aged 90+ and close for all other age
groups 50+, while case rates for children and young people are significantly lower.
12.
Overall mortality rates are increasing and are at the highest level for this year. They are likely to continue increasing in the coming weeks due to the trend of mortality
rate rises trending behind case rates rises.
Committee recommendations and rationale
Overall recommendations
1982
13.
Based on the available evidence at this time, and in line with approach agreed by
Cabinet in April 2022 [CAB-22-MIN-0114]1, the CPF Committee recommended that:
ACT
a. all parts of the country should
remain at the Orange CPF setting,
b.
no changes to case isolation and household contact quarantine requirements,
c. to signal what a step down in case isolation and household contact quarantine
requirements would look like, and
d. there be no requirement imposed at this time for people to routinely test if they
have been in contact with someone who has tested positive for COVID-19 or if they
are visiting a vulnerable person.
INFORMATION
14.
These recommendations reflect the Committee’s overall consideration of:
a. the current high levels of COVID-19 infection in the community and burden on
primary and hospital care systems,
b. uncertainty around when the peak will be over, noting a temporary tapering off, and
the risk of a post-school holiday increase,
OFFICIAL
c. the uncertain shape of infections post-peak (lack of confidence in a smooth or rapid
descent from the peak), and
THE
d. the high risk of public confusion and how it might fit within the current winter
wellness and outbreak narrative and behaviours.
Review of CPF colour settings
UNDER
15.
There was consensus within Committee that the whole country should remain at the
Orange CPF setting at this time. The Committee viewed a shift to Red was not warranted
at this time, noting the Winter Package measures and impacts are not yet fully
understood or evidenced to help inform decision making.
16.
The Committee noted that cases do appear to be declining under current settings and
measures. Therefore, we must now consider both what is needed in terms of our current
RELEASED
public health response, but also how that fits with our glide path towards a future post-
winter mostly comprised of only ‘baseline’ measures with fewer ‘reserve’ measures.
1 Cabinet indicated that the health factors used to inform CPF colour decision-making include: the degree of protection
from severe health outcomes from COVID-19 (vaccination coverage, immunity levels and availability of treatments); and
the capacity of the health system to meet demand due to COVID-19.
3

Document 1
More time is needed before we will see the full impact of the Winter Package
17.
Initial indications suggest that the measures within the Winter Package are having a
positive impact supporting existing measures at Orange, in particular:
a.
Greater access to COVID-19 antivirals – since the widening of criteria for COVID-19
antivirals on 18 July 2022 as part of the Winter Package, the volume dispensed in
the week ending 24 July 2022 increased by 65.5 percent on to the week prior (48.7
percent). Nine percent went to Māori and three percent to Pacific People, an
increase on the previous week.
1982
b.
Further increases in take-up of antivirals are expected – with the phased removal of
prescription requirements from 28 July 2022 and more pharmacies distributing (over
400). As antivirals access continues to expand, this in time, may help relieve some
ACT
pressure on GPs and hospitalisations or hospital stays2.
c.
Making second COVID-19 booster shots available - the rollout of a second COVID-19
booster, including to high-risk groups and those aged 50 years and over should
reduce infection rates and hospitalisations and severe health outcomes for
vulnerable people. However, it will take some weeks to see the full impact of this as
uptake by eligible groups increases.
18.
At the same time, other key Winter Package measures being implemented will further
supplement existing measures at Orange, including: INFORMATION
a.
Increasing access to, and supply of, free face masks – to support the effectiveness of
existing mask mandates, with messages encouraging use in other high-risk
contexts3. Since 15 July 2022, 1.8 million P2/N95s (a 41 percent increase in the last
week) and 25 million medical masks have been dispatched for community use.
b.
OFFICIAL
Improving access to RATs – expanding access will make it easier for people to
undertake timely testing and reduce infection as people affected isolate. Since 15
July 2022, 6.5 million RATs have been dispatched across New Zealand.
THE
19.
The Committee noted these encouraging signs but that any impact on case rates or
hospitalisations would be clearer when it next considered the CPF colour setting in mid-
late August 2022 and nearer the end of winter.
Degree of protection from severe hea
UNDER
lth outcomes from COVID-19
20.
The Committee considered that currently there is a reasonably good level of protection
from severe health outcomes due to COVID-19, because:
a. the people most at risk of exposure to COVID-19 and/or severe outcomes are
eligible for a second booster, and roll-out is progressing well to target groups,
b.
RELEASED
there has been a significant increase in the roll-out of antivirals, with further
increases expected, as detailed above,
2 However, current Manatū Hauora evidence shows that most hospitalised individuals are not diagnosed until after
admission to hospital which requires further exploration.
3 Other mask options are available for people who cannot use P2/N95 masks, and a Mask Exemption Pass is available.
4
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 1
31.
However, the modelling of the likely impact of reducing isolation times at the time
(assessed as negligible initially) assumed 100 percent compliance with increased public
health precautions until Day 107. The Committee did not consider the assumptions
underpinning the modelling to be realistic and recommended keeping the issue under
review as the modelling was refined further.
32.
The 15 June 2022 CPF assessment also occurred before a further significant increase in
COVID-19 cases and hospitalisations, which naturally shifted the short-term focus from
options for decreasing self-isolation times, to options for limiting the further pressure on
the health system from more cases and hospitalisations. In this context, in July 2022,
NITC developed a proposal for enhanced public health measures for cases and contacts
1982
in the 3-day period following isolation/quarantine. However, ultimately this was not
progressed as it was considered that the COVID-19 Public Health Response (Protection
ACT
Framework) Order 2021 was the appropriate tool to communicate any requirements.
33.
Going forward, we intend to coordinate all advice on isolation requirements through the
public health risk assessment (eg CPF review) process. This should help avoid duplication
or confusion of advice in relation to these requirements (and guidance) while ensuring
requirements remain proportionate to the public health risk and well connected.
Committee recommendation and rationale
34.
Appendix 4 provides a summary of current settings, and the options considered by the
INFORMATION
Committee, specifically:
a. Option 1: Status quo isolation for cases (7 days); remove quarantine requirement for
household contacts, replace with a daily RAT requirement for 7 days, and
b. Option 2: Reduce the legal isolation requirement for COVID-19 cases to 5 days and
introduce a requirement to test negative on a RAT to release (or a maximum of 7
OFFICIAL
days isolation, whichever comes first); household contacts as in Option 1.
35.
Based on separate advice and options provided by NITC and wider Committee
discussion, on balance it is recomm
THE ended to retain the
status quo isolation and
quarantine settings for now.
36.
However, the Committee also recommended a need
to signal that once a descent from
the BA.5 peak(s) has been confirmed (noting the current wave is driven by new variants,
not by the season).
UNDER
s 9(2)(g)(i)
This change would be followed by further easing of
requirements, indicatively outlined in paragraphs 39-41.
37.
The Committee viewed that any reduction in isolation settings for cases and households
at this time would outweigh the potential benefits. This reflected that:
RELEASED
a. There remains a risk of household contacts being infectious prior to being
symptomatic or returning a positive RAT, leading to a risk of onward transmission
7 Public health precautions were wearing masks outside the home; avoiding high risk settings (as a visitor) eg aged care
facilities, prisons, and hospitals (unless requiring care); and continuing to work from home wherever possible.
7

Document 1
during this period if they do not quarantine8. This reflects the knowledge that viral
loads typically peak early in the course of infection (days 3-4) and a proportion of
household contacts will still test positive following a household index case9.
b. There has been insufficient time to consult with Māori and Pacific stakeholders prior
to changing isolation times. It was noted previous feedback included concerns that:
i. They would prefer to retain the status quo measures over winter – as managing
cases and household contacts together in a bubble is consistent with their
whānau-centred approach (so different isolation or quarantine periods for cases
and household contacts were not supported).
1982
ii. the impact of any change to isolation and quarantine requirements would need
to be modelled (eg in terms of impact on hospitalisations or deaths) prior to a
decision to change the settings, or it could be considered a breach of Te Tiriti.
ACT
c. Any change that might increase cases is not advisable now, because although it
might lead to an increase in the available workforce:
i. while the rate of new cases has slowed in recent weeks, it is not yet sufficiently
clear that trend will continue,
ii. overseas experience suggests that countries are better positioned to deal with
new variants if they have had time to recover from the previous wave, and
INFORMATION
iii. there was widespread recognition that frontline healthcare workers are
currently under a lot of pressure, and that it would be inappropriate to make a
change now that could potentially add to that pressure.
d. Any workforce (and wider) benefits might be somewhat limited
as a parent/guardian
would still need stay home to care for dependants who had COVID-19 (a reasonable
proportion of current workplace absenteeism is
OFFICIAL understood to be due to influenza,
and a reasonable proportion of people remain unable to return to work on day 8)10,
e. There was also a desire to keep public communications as simple and clear as
THE
possible, particularly in relation to the current winter and outbreak narrative.
38.
The Committee also noted that, when it is the right time to make the change to isolation
requirements for household contacts (noting from the above that now is not yet the
right time), the benefits will likely include:
UNDER
a. enabling people to return to work and study, and
b. time spent outside the house would reduce the risk of infection for household
contacts (particularly in crowded houses) although it may increase risk for others
with whom they encountered at work or school11.
RELEASED
8 A person may test negative in the morning, but then become infectious during the day. It is also possible a person may
test negative but be infectious, (ie there may be a delay until they get a positive RAT, which would be inconsequential if
they were quarantining but may lead to onward transmission if they are in the community during the day).
9 Based on early data in New Zealand’s BA.2 wave, 78 percent of household contacts tested positive, but this is unlikely to
be representative of the wider population, as large family groups in houses were over-represented during.
10 Canterbury healthcare worker data showed around 40 percent were not well enough to return to work after 7 days.
11 No modelling has been done on this question to date, and it is unclear if it would be possible. Conceptually, this is more
likely to impact on groups who are less likely to be able to work from home. However, this group may be less likely to
8

Document 1
Signalling direction of travel
s 9(2)(g)(i)
1982
ACT
INFORMATION
OFFICIAL
THE
Other matters related to self-isol
UNDER
ation and quarantine requirements
Not considering a shift to test to release for cases at the current time
42.
The Committee agreed that
a ‘test to release’ option for cases was not appropriate at
this time. For example, it could mean that some people would be required to be in
isolation for longer than they are currently. This was considered not viable without wider
consultation and increased support for those likely affected first. It was acknowledged
RELEASED
that a test to release approach for cases would be useful for cases that remain
asymptomatic, but this could not be implemented in isolation.
Appropriateness of further guidance regarding testing
comply with quarantine settings (due to the impact it may have on employment and income), potentially making a testing
option less risky than requiring quarantine.
9

Document 1
43.
The Committee was asked to consider whether it was appropriate that people test:
a. in the case of non-household contacts, if they have been in contact with someone
who has tested positive for COVID-1912, or
b. if they are visiting a vulnerable person.
44.
In either situation, the Committee is of the view that it would not be appropriate to
either recommend or require testing.
45.
The rationale for this is that both options may identify asymptomatic cases - an
approach not recommended in the Testing Plan. Although this may have benefits in 1982
terms of reducing transmission, any asymptomatic testing (outside of household
contacts) could have several unintended consequences, such as:
a.
ACT
Additional people being (temporarily) taken out of the available workforce.
Although from a science perspective having fewer potentially infectious people at
work could reduce workforce pressures, these people may be late in the course of
their infection. This option would also need to be combined with some form of test
to release, to not inadvertently detain people who are no longer infectious.
b. A negative RAT early in a person’s infectious period does not indicate that they do
not have COVID-19 (and could simply be due to poor technique when the sample is
taken such that a RAT will only test positive when the viral load is very high).
Recommending testing for a person who is visiting a vulnerable person may risk
INFORMATION
exposing the vulnerable person to infectious people who are falsely reassured that
they do not have COVID-19 and so they may forgo precautions such as mask
wearing and physical distancing.
c. People can be at risk of severe illness from COVID-19 from a wide range of factors.
Recommending anyone who is visiting, or spending extended periods of time in
OFFICIAL
contact with, a vulnerable person would significantly increase the amount of
asymptomatic testing.
THE
46.
Emphasising the principle of recommending that people get tested and stay home if
they are symptomatic remains, and particularly if they are planning to be in contact with
vulnerable members of the community.
Equity
UNDER
47.
COVID-19 continues to worsen pre-existing health inequities for many groups,
particularly those underserved by the existing system, despite efforts to equitably
allocate resources. This is often due to overlapping social, clinical, or occupational risk
determinants. Any reduction in CPF settings or in its overall effectiveness as an outbreak
management tool will have a disproportionate effect on those more at-risk in the
RELEASED
population. This includes Māori and Pacific People, disabled, and older people.
48.
As shown above, older people already face an increasing threat during winter across all
four regions, especially for Māori and Pacific Peoples aged 65+. This group is more likely
to be hospitalised. It is expected that the virus will take longer to move through this
12 Note that this requirement was previously in force and was removed in February 2022.
10

Document 1
population due to this group having fewer social interactions. This may lead to a higher
hospitalisation burden over a longer period during winter.
49.
Pasifika continue to be disproportionately affected by COVID-19. Many face other
challenges that compound the impact of COVID-19 i.e. housing-related. Moreover,
Pacific Peoples undergo long-standing inequitable health outcomes and service use,
including considerably less COVID-19 booster and paediatric vaccinations. This is shown
in data that Pasifika with COVID-19 have a mortality rate 4 times greater than European
or Other ethnicities. This is further compounded by the severity of the 2022 flu season.
50.
From 18 July 2022, criteria changes have allowed greater Pasifika and Māori access to 1982
antiviral medication to prevent the more severe health impacts of COVID-19 and
hospitalisation. Following this change there was 65.5 percent increase in the courses of
antiviral medication dispensed over the week ending 24 July 2022.
ACT
51.
Those who suffer high deprivation have a COVID-19 mortality rate 3.1 times higher than
those with low deprivation13. Further, booster uptake is lower in high deprivation areas14.
This emphasises the impact of the pandemic on equitable health outcomes for
economically disadvantaged New Zealanders.
52.
Disabled people and those with underlying medical conditions are also more likely to be
negatively impacted by COVID-19. These people are more likely to be hospitalised or
require medical intervention/support if they test positive with COVID-19. Equally, those
who need assistance with everyday living, are affected when their carers or support
INFORMATION
workers contract COVID-19 and are unable to provide essential support and this issue
has been reflected in feedback from the disability community.
Te Tiriti o Waitangi Analysis
OFFICIAL
53.
Demonstrating a commitment to and embedding the Te Tiriti and achieving Māori
health equity remain a key COVID-19 health response priority. This is heightened by the
threat that COVID-19 poses to Māori and is particularly critical following the release of
THE
the Waitangi Tribunal’s
Haumaru: the COVID-19 Priority Report.
54.
That report found breaches of Tiriti principles of active protection, equity, options, tino
rangatiratanga, and partnership which put Māori at disproportionate risks of infection
and wider COVID-19 impacts. As well as reaffirming those principals as relevant to the
UNDER
COVID-19 response, it noted that the Crown must further support and resource Māori
providers, whānau, hapū, iwi and hapori Māori.
55.
Therefore, the targeted drivers and actions contained in Manatū Hauora’s Māori
Protection Plan released in December 2021 remain relevant. These include actions to
improve Māori vaccination rates, building community resilience to protecting Māori
health and wellbeing, and positioning communities to recover.
RELEASED
56.
While the equity gap has narrowed significantly for first and second vaccination rates for
Māori compared to non-Māori and non-Pacific since December 202115, emerging data
13 Age-standardized and controlled for vaccination status but is affected by lower case reporting in highly deprived areas.
14 This is related to those who are eligible to take up boosters by deprivation status.
15 The second dose equity gap has decreased from 14.2 percent as of 26 December 2021 to 8.2 percent as of 1 April 2022 -
May 2022 COVID-19 Māori Health Protection Plan Monitoring Report.
11

Document 1
continues to highlight the disproportionate impact on Māori. Persistent inequities
remain in infection16 and hospitalisation rates, boosters, and child immunisation rates.
57.
Māori mortality rates of those with COVID-19 are 2.8 times higher than the European or
Other ethnicity group. Data collected in May 2022 shows that Māori are currently
overrepresented in delays for receiving planned care, making up 17 percent of all
patients waiting more than four months. Work is needed across the system to protect
whānau, hapū, iwi and hapori Māori from the impacts of COVID-19.
58.
Given that this memo recommends no changes to existing CPF or isolation settings, the
Māori Protection Plan’s two key drivers remain critical. Related response initiatives 1982
should also have a positive impact for Māori, including the Winter Package measures,
such as free medical and N95 masks to schools, kura, and vulnerable communities,
access to antivirals for those that are eligible17, and COVID-19 and flu vaccinations.
ACT
However the Committee may need to further consider measures to assist Māori if
infection rates and hospitalisations do not improve in the interim.
59.
The first key driver in the Māori Protection Plan’s to boost broader immunisation uptake
will remain integral to protecting Māori health and wellbeing, and includes:
a. work underway to improve vaccination access and uptake for Māori across the
various immunisation programmes, and
b. a focus on supporting vaccination services that meet Māori where they are.
INFORMATION
60.
The second key driver, focused on building the resilience of whānau, hapū, iwi and
hapori Māori, will better position communities to recover from the impact of the
pandemic. This includes through Care in the Community delivering wrap-around and
culturally appropriate services for whānau and a wider community-based model of care
being further developed to support services delivery through winter and beyond.
OFFICIAL
61.
Te Whatu Ora was unable to complete engagement with Māori on the potential changes
to isolation and quarantine requirements. However, given that the Committee does not
recommend changes now but to signal a potential step-down in requirements over time,
THE
it will enable more comprehensive engagement. This is important, as previous
engagement showed strong opposition to any requirement reduction due to the
potential impact on whānau. This engagement also requires Māori-specific impact
modelling to inform their input, which was not available then.
UNDER
62.
Monitoring the COVID-19 impact on Māori is essential to ensure the ongoing response
of the health system gives effect to the principles of Te Tiriti. Manatū Hauora continues
to monitor the impact of COVID-19 on Māori, and this will be formally reported on in
the next COVID-19 Māori Health Protection Plan Monitoring Report in late 2022.
RELEASED
16 Since the Delta outbreak in August 2021, Māori have been 75 percent more likely to contract COVID-19 (201.6 cases per
1,000 Māori compared to 116.4 cases per 1,000 non-Māori non-Pacific). After accounting for age, Māori were 2.4 times
more likely to contract COVID-19 (330.5 cases per 1,000 Māori compared to 136.3 cases per 1,000 non-Māori non-Pacific) -
May 2022 COVID-19 Māori Health Protection Plan Monitoring Report.
17 In the week ending 24 July 2022, nine percent of antiviral courses went to Māori while they accounted for 10 percent of
reported COVID-19 cases.
12

Document 1
s 9(2)(h)
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
13

Document 1
Next Steps
66.
Pending your approval, this memo will be provided to the Department of the Prime
Minister and Cabinet to be included in its overarching advice to COVID-19 Ministers in
the week beginning 1 August 2022 and to the Minister for COVID-19 Response’s office.
Recommendations
It is recommended that you:
1982
1.
Note that on 27 July 2022, the COVID-19 Protection Framework Assessment
Noted
Committee (the Committee) met to consider:
i.
ACT
COVID-19 Protection Framework (CPF) colour settings, and
ii.
isolation and quarantine periods for cases and household contacts.
2.
Note that the Committee considered evidence that showed:
Noted
i.
Current modelling suggests that COVID-19 cases may have peaked at
approximately 11,000 cases in mid-July 2022
ii.
Case rates across all age groups have plateaued over the past week but
are highest for those who are aged 65 years or older
INFORMATION
iii.
The current hospitalisation rate is 15.2 per 100,000, up seven percent
for the week ending 24 July 2022
iv.
Wastewater quantification levels have tapered slightly and are still close
to the levels during the Omicron peak in March 2022
v.
OFFICIAL
Overall mortality rates have increased and are at the highest level for
2022, which is expected to continue in the coming weeks due to the
trend of mortality rate rises trending behind case rates rises.
THE
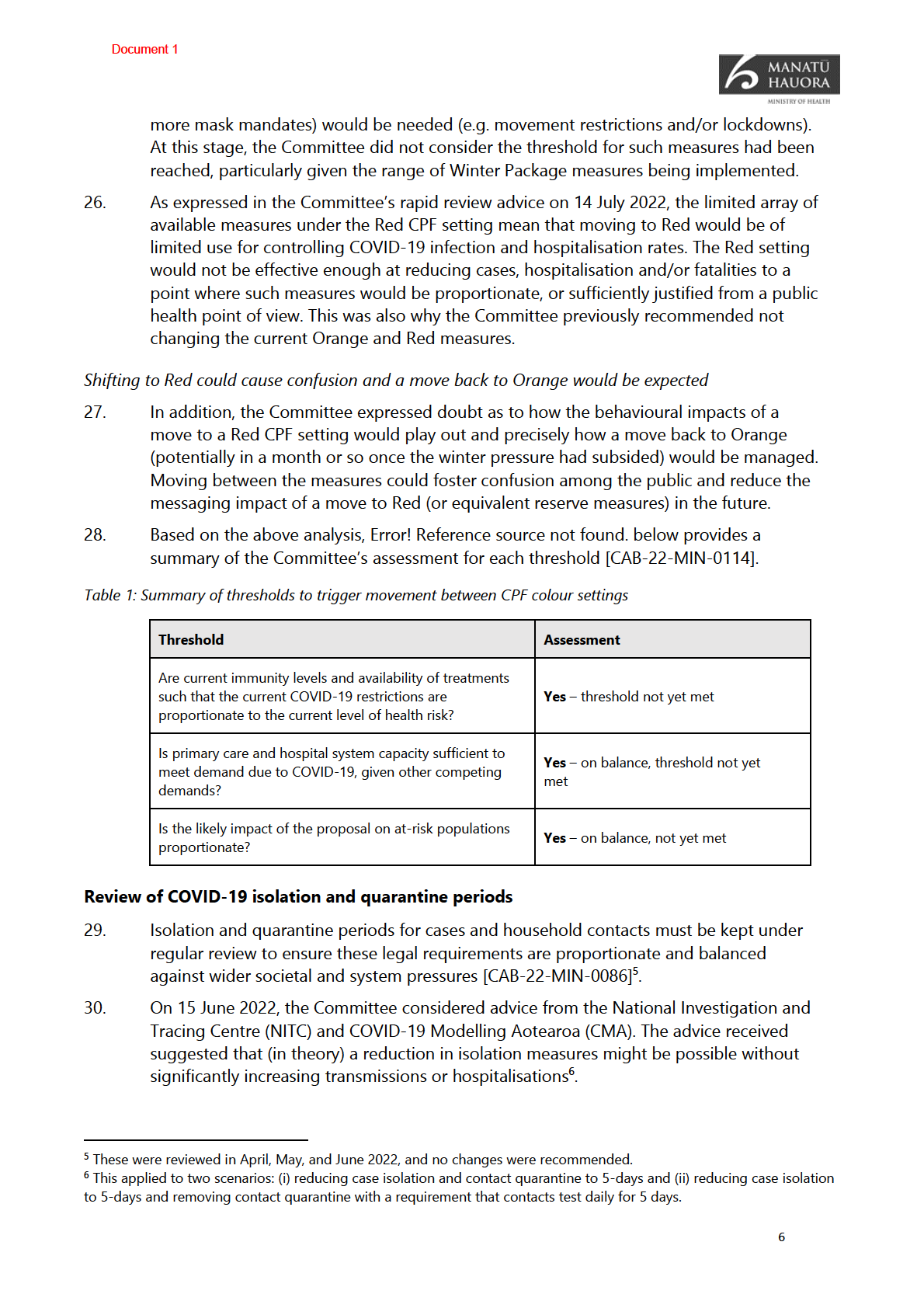
3.
Note that at this time, based on the available evidence and analysis the
Noted
Committee has recommended:
i.
the
entire country should remain at the Orange CPF setting
UNDER
ii.
no changes should be made to isolation and quarantine settings for cases or household contacts
iii.
to signal a clear transition plan with proposed timings for removing
household quarantine requirements and refining isolation advice
iv.
that it would not be appropriate to recommend or require people test:
RELEASED a. if they have been in contact with someone who has tested
positive for COVID-19, or
b. if they are visiting a vulnerable person.
4.
Agree that at this time, based on the available evidence and analysis above:
i.
the entire country should remain at the Orange CPF setting
Yes
14
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 1
Appendix 2: Outbreak analysis and modelling
Current outbreak status
Community cases have increased for the past four weeks but tapered slightly in the last two weeks
1.
For the week ending 24 July 2022, the national weekly case rate was 12.0 per 1,000
population. This is a 12.4 percent decrease from the previous week, which was 13.7 per
1,000 people. This suggests that we may be reaching the peak of the current wave, as
modelling suggests but more time is needed to confirm this.
2.
Comparison of community cases to routine healthcare worker testing continues to 1982
indicate a substantial under reporting of community cases. This suggests that over half
of cases (52 percent) are likely to be not reported (24 per 1,000 vs 12.4 per 1,000).
ACT
3.
In the past week, only one district (Taranaki) experienced an increase in COVID-19 case
rates, mirroring the tapering of case rates in the general population.
Wastewater levels have also tapered slightly and are close to the Omicron peak in March 2022
4.
Wastewater detections of the virus in all regions have plateaued after increasing steadily
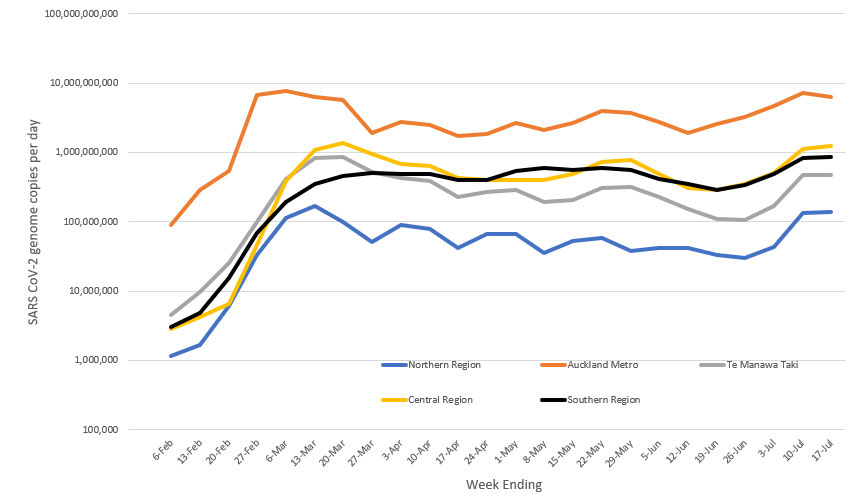
in the past weeks. However as shown in
Figure 1 below, in all regions, the wastewater
levels are like the levels seen in March 2022.
Figure 1 - Regional wastewater trends in SARS-CoV-2 genome quantification weeks 6 February – 17 July 2022
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Case rates across all age groups plateaued over the past week with rates for 65+ increasing
5.
In the week ending 17 July 2022, case rates for all ethnicities aged 65+ increased. Case
rates increased eight percent for Asian, four percent for European or Other, three
percent for Māori and 40 percent for Pacific People.
17

Document 1
6.
In the same period, regional trends of cases across all ethnicities aged 65+ mostly
increased, except in the Northern region with decreased by 3.4 percent. In Te Manawa
Taki cases increased by 13.9 percent, in the Central region by 4.5 percent, and in Te
Waipounamu by 7.8 percent.
These trends continue to be driven by the BA.5 Omicron sub-variant
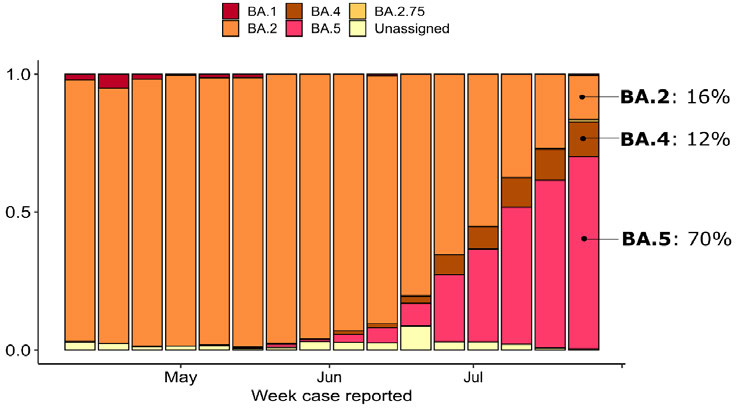
7.
As shown in
Figure 2 below, BA.5 accounts for 70 percent of sequenced community
cases in the past week. It also shows BA.5’s increasing frequency in community samples
over the past few weeks. As expected, in New Zealand is seeing a (relative) growth
advantage of BA.5 over other variants. BA.4 is holding steady at 12 percent.
1982
8.
Modelling continues to suggest BA.5 will account for 90 percent of all community cases
in New Zealand by early August. Its dominance may be due to it having a greater rate of
ACT
reinfecting individuals who have already had earlier COVID-19 variants.
Figure 2- Frequency of Variants of Concern in New Zealand community cases
INFORMATION
OFFICIAL
THE
BA.2.75 is being closely monitored but its impact is not yet well understood
9.
While the new subvariant BA.2.75 appears to be gaining a global foothold there have
been a very small number of reported cases in New Zealand (fewer than 20). Most of
these are linked to the border
UNDER but two have no clear epidemiological link to the border.
10.
It is probable that small numbers of BA.2.75 are transmitting within the New Zealand
community. However, it remains highly uncertain what impact, if any, this will have on
case numbers, reinfection and spread relative to BA.5.
Hospitalisations are likely to continue increasing in the coming weeks 11.
Despite case rates decreasing over the week ending 24 July 2022, over the same week
RELEASED
the national daily average hospital occupancy for inpatients with COVID-19 increased to
15.1 per 100,000 population.
12.
This was an increase of 6.1 percent from the week prior. This may be attributed to the
significantly increased proportion of Pacific People aged 65+ with COVID-19 and of
people aged 65+ more broadly, over the same period.
18

Document 1
13.
Hospital occupancy average rates increased across all regions in the past week, except
for the Northern Region. The Northern region (14.3 per 100,000) decreased by 5.7
percent, Te Manawa Taki (14.4 per 100,000) increased by 23 percent, Central region (15.3
per 100,000) stayed the same in the past week and Te Waipounamu (16.9 per 100,000)
increased by 23 percent.
14.
Tertiary hospital admission positivity has been plateaued with a 7-day rolling average of
4.6 percent (589/ 12,758) for the week ending 24 July. Preliminary analysis indicates a
large majority of cases who are admitted to hospital, test positive and are confirmed as a
case on the day of their hospitalisation.
15.
1982
This means that a large proportion of cases admitted to hospital are not carrying out
their own testing and getting access to therapeutics before their symptoms become
severe. Initiatives are underway to increase access to testing and therapeutics are more
ACT
widely being dispensed, which will help to reduce the numbers of cases being admitted
to hospital.
16.
While the capacity of the health service is currently impacted by winter illness, rates of
COVID-19 infection are primarily being driven by the development of new variants which
are mostly independent of seasonality and their emergence is difficult to predict.
17.
Hospital occupancy average rates increased across all regions in the past week. Northern
region: increased by 31 percent, Te Manawa Taki increased by 11 percent, Central region
increased by 38 percent, and Te Waipounamu increased by 31 percent.
INFORMATION
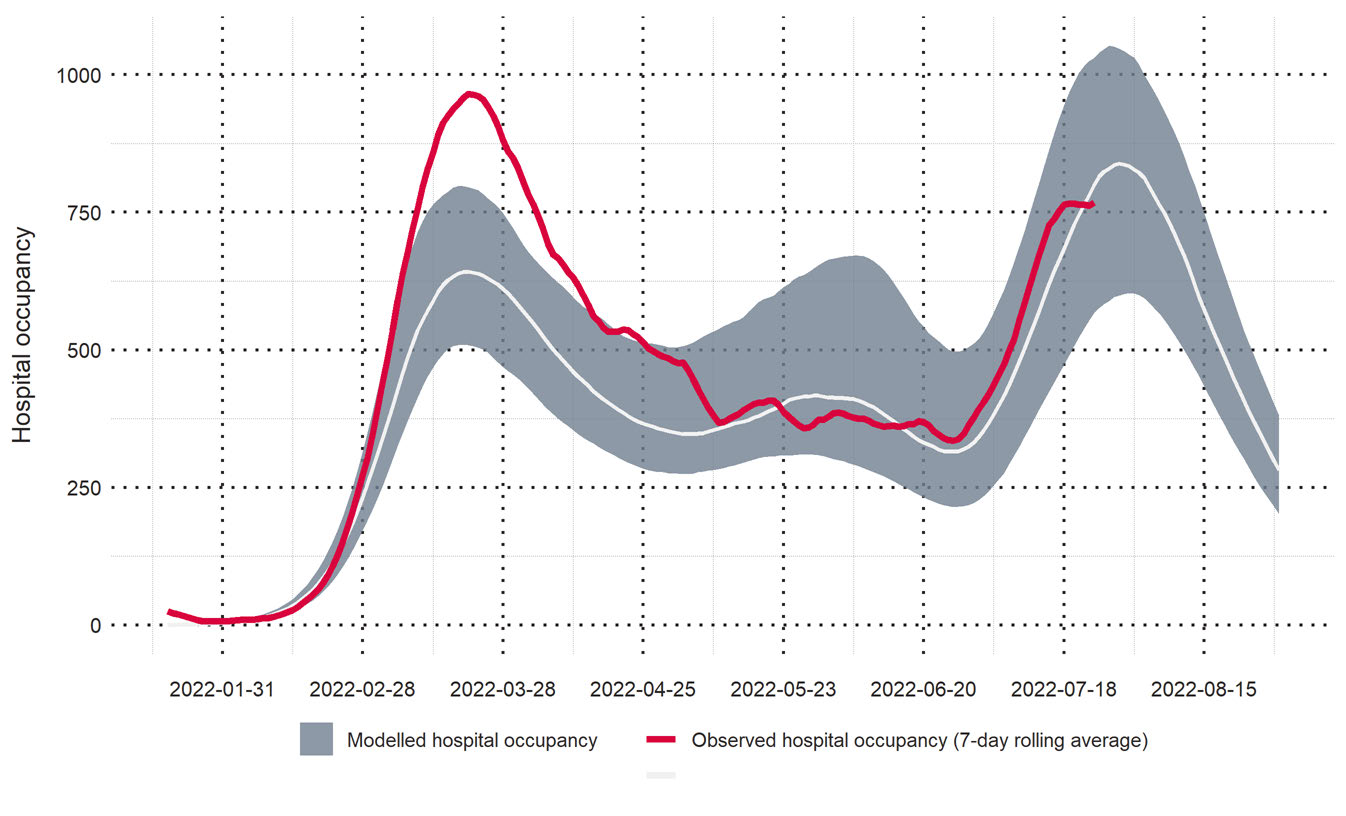
18.
Updated Covid Modelling Aotearoa (CMA) scenarios in
Figure 3 below indicates that
hospital bed occupancy will peak this week at approximately 800 beds occupied a day
(12,000 daily cases). However, it is too soon to confirm whether hospitalisations have
already peaked, as indicated by the grey areas of the predication.
Figure 3 – CMA BA.5 scenarios for hospital occupancy
OFFICIAL
THE
UNDER
RELEASED
19

Document 1
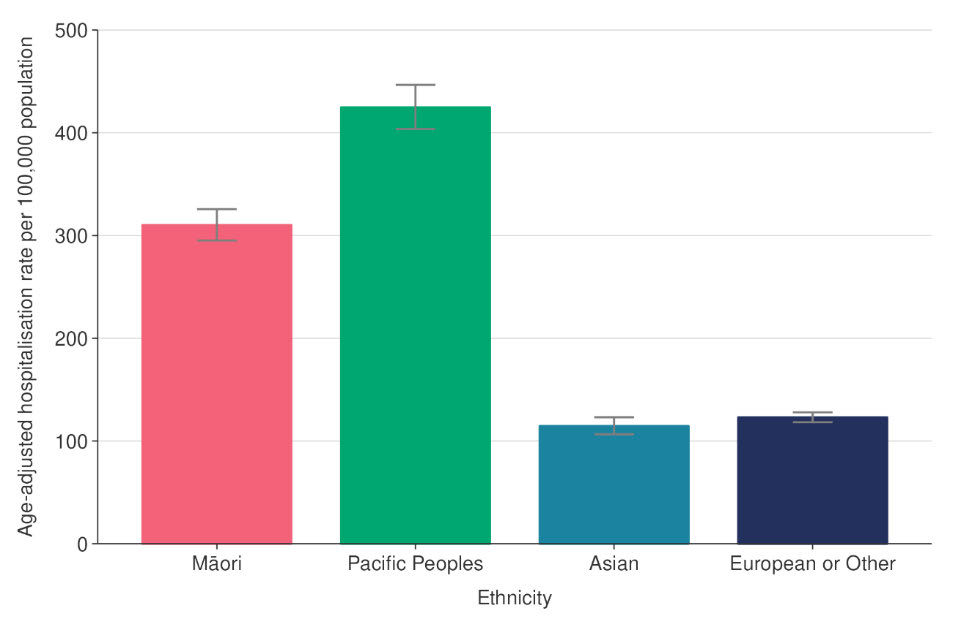
19.
Analysis undertaken to assess hospitalisation risk from COVID-19 has found that Pacific
Peoples have the highest rate of hospitalisation with COVID-19 (424.7 per 100,000)
followed by Māori (310.2 per 100,000) and then Asian and European or Other at the
same level, between 114 and 124 per 100,000. The analysis was age-standardised to
compare ethnic groups with different age structures.
20.
Similarly, total COVID-19 attributed mortality rates by ethnicity, Pacific Peoples have the
highest rate (25.8 per 100,000) followed by Māori (17.8 per 100,000) and then Asian and
European or Other at the same level, between five and eight per 100,000. All the age-
specific rates are higher for Māori and Pacific compared with European and Other.
Figure 4 - Age-standardised cumulative incidence (and 95% confidence intervals) of hospitalisation with COVID-
1982
19 by ethnicity, March 2020 to 24 July 2022
ACT
INFORMATION
OFFICIAL
THE
UNDER
Mortality rates are at their highest level this year and are likely to continue increasing
21.
Mortality rates are likely to continue increasing in the coming weeks due to the trend of
mortality rate rises trending behind case rates rises. As of 20 July 2022, 1,868 people
have died within 28 days of being reported as a case and/or with COVID-19 being
attributed to the cause of death.
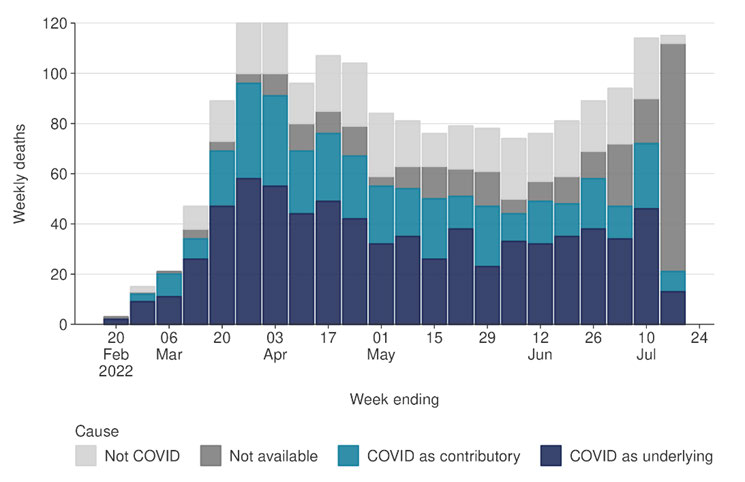
22.
A review of some of these cases indicated COVID-19 was the underlying cause of 861
RELEASED
(50 percent) of deaths and a contributing factor to a further 465 deaths (27 percent).
20

Document 1
Figure 5 – Weekly death attributable to COVID-19 or not
1982
ACT
INFORMATION
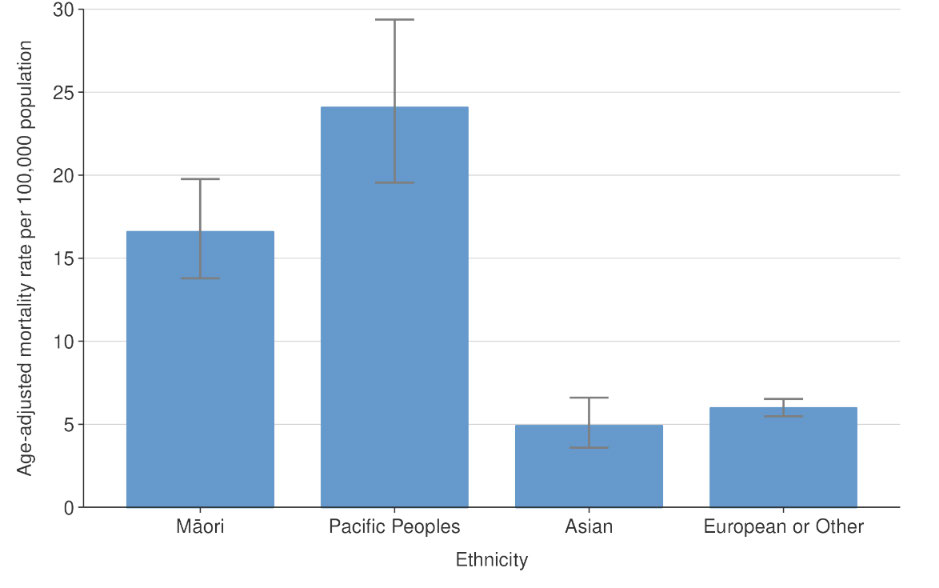
23.
Total deaths rates are lower in Māori (16.5 per 100,000) than European/Other (26.7 per
100,000), despite having higher rates in all age groups. However, Māori and Pacific
mortality rates, after age standardising, were 2.8 and 4.0 times greater, respectively, than
European/Other.
Figure 6 – Age-adjusted mortality rate per 100,000 population by ethnicity
OFFICIAL
THE
UNDER
RELEASED
21

Document 1
Appendix 3: Regional Resilience Leads Feedback
1.
There were varying views from the four regions whether a shift to Red was needed based
on their capacity to respond to COVID-19 and non-COVID-19 demand for health services.
s 9(2)(g)(i)
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
22

Document 1
Appendix 4: Isolation and quarantine settings and options
Current settings
1.
The purpose of Isolation and quarantine requirements for cases and contacts is to reduce
ongoing transmission, by preventing infectious (or potentially infectious) people from
having contact with others within the community.
2.
People who test positive for COVID-19 are required to isolate for 7 days and their
household contacts are required to quarantine for the same period18. Households are
managed as a bubble, counted from the first case’s day 0, with the whole household 1982
released on the case’s day 8. If a household contact tests positive during that period, they
must isolate for a further 7 days from the day they test positive.
3.
ACT
Household contacts who are critical workers in healthcare and other sectors have
established pathways to allow them to continue to work throughout their quarantine
period (if they are well) if service provision is at risk. Cases who are critical healthcare
workers are also able to return to work if well and if service provision is at risk. Other
sectors can apply for a temporary exemption for critical workers who are cases.
Options considered by the Committee
4.
The Committee considered two options for changes to isolation and quarantine settings:
INFORMATION
Option COVID-19 cases
COVID-19 household contacts
Modelling19
1
• Maintain the legal
• Remove the legal requirement for
• 15% - 41%
isolation requirement for
household contacts to quarantine
of cases
COVID-19 cases at 7-
potentially
•
days, with no test-to-
Replace quarantine with a
infectious at
recommendation to employ strong
release requirement.
release
public health pre
OFFICIAL cautions for 7 days
•
•
Average
Recommend that household contacts
time in
test daily with a RAT for 7 days (from
isolation
THE when the first case in the household
(days) – 7
receives a positive result).
days
2
• Decrease to the legal
• Remove the legal requirement for
• 21% - 50%
isolation requirement for
household contacts to quarantine
of cases
UNDER
COVID-19 cases to 5
potentially
•
days, and
Replace quarantine with a
infectious at
recommendation to employ strong
release
• introduce a requirement
public health precautions for 7 days
for one RAT to release (or
•
•
Average
a maximum of 7 days
Recommend that household contacts
time in
test daily with a RAT for 5 days (from
isolation, whichever
isolation
when the first case in the household
comes first).
(days) – 5.7
receives a positive result).
– 6.4 days
RELEASED
18 COVID-19 Public Health response (Isolation and Quarantine) Order 2020
https://www.legislation.govt.nz/regulation/public/2020/0241/latest/LMS401667.html
19 CMA modelling for the two options, impact approximately one month after any change.
23

Document 1
Appendix 5: Current settings for asymptomatic testing for elevated risk
settings or situations
1.
Current settings in relation to asymptomatic testing are as follows:
General public 2.
Test if they are symptomatic. Household contacts and recent arrivals from overseas are
currently the only groups of people who are recommended or required to test
asymptomatically.
Aged Residential Care (ARC)
1982
3.
Residents are initially tested via a RAT and may receive a confirmatory PCR by clinical
discretion. Staff and visitors are advised to stay home if unwell, and staff who are
ACT
asymptomatic contacts are recommended to do a daily RAT prior to starting their shift.
Hospitals including emergency departments
4.
Patients - testing is recommended by clinical discretion as per local hospital guidelines.
5.
Staff – PCR for symptomatic healthcare workers, and daily RAT to work as part of the
CCES/test to return.
Recent review of Testing Plan guidance for each setting
6.
INFORMATION
A group of subject matter experts across the Public Health Agency and Te Whatu Ora
recently reviewed the Testing Plan guidance for each setting and recommended no
changes to test-to-enter for high-risk settings.
7.
Public health advice is that, with the expected high number of cases over the next few
weeks, people should be advised to take all reasonable steps to protect their vulnerable
friends and whānau (eg someone with cancer, frail eld
OFFICIAL erly, or a newborn baby) by staying
home if sick, wearing a mask indoors, coughing into their elbow, physical distancing, and
taking a COVID-19 test if they have any COVID-19 symptoms.
THE
UNDER
RELEASED
24
Document 3
Memo
Public Health Risk Assessment of COVID-19 mandated response measures,
3 October 2022
Date:
12 October 2022
1982
To:
Dr Diana Sarfati, Director-General of Health
From:
Dr Nicholas Jones, Director of Public Health, Public Health Agency
ACT
Dr Andrew Old, Deputy Director-General, Public Health Agency
For your:
Decision
Purpose of report
1.
This memo provides you advice from the Director of Public Health following the 03 October
2022 Public Health Risk Assessment (PHRA). The PHRA considered whether the remaining
mandated (and other) COVID-19 response measures are proportionate to the risk po
INFORMATION sed by
the current outbreak.
2.
This paper seeks your agreement to the recommendations arising from that meeting. The
agreed recommendations will inform a paper on the future management of COVID-19 that
the Minister for COVID-19 Response will take to Cabinet on 17 October 2022.
OFFICIAL
High level summary of key considerations
Previous PHRA recommendations
THE
3.
Advice provided to you fol owing the 17 August 2022 PHRA recommended the removal of
several mandatory measures based on public health advice that they were no longer
proportionate and/or justified. Subsequently, requirements to wear masks in settings other
than healthcare, and quarantine requirements for household contacts were removed, along
UNDER
with testing requirements for international arrivals.
4.
Their removal was considered an appropriate response given New Zealand’s COVID-19
outbreak at that time was waning, with reducing case numbers, hospitalisations, and
deaths. The proportionality of many mandated response measures significantly reduced
due to the changing context of the outbreak at that time.
5.
It was agreed the remaining measures – the retention of case isolation, face masks in
healthcare se
RELEASED ttings and electronic provision of contact details – would be kept under review
and assessed again at the next PHRA. This stepped approach was considered a judicious
way to manage the transition from mandatory measures. It also provided the opportunity
to assess the impacts of these changes across key indicators to determine if it was
appropriate to remove the mandates underpinning two of the four key pillars – masking,
separation, vaccination and isolation – to our COVID-19 response.
1
Document 3
Outcome of 3 October 2022 PHRA
6.
Given the current domestic and international context, the PHRA recommendations
represent a continuation of current measures, with some minor modifications. This
assessment builds on evidence and recommendations from previous assessments
(including the 17 August PHRA, and the CPF Assessments that preceded it).
7.
Key to our ongoing precautionary approach is the need to protect vulnerable populations
and reduce inequities.1 COVID-19 morbidity and mortality data continue to highlight the
disproportionate risks to Māori, Pacific, socio-economically disadvantaged and disabled
communities.
1982
8.
Concerns were expressed that lifting mandates for case isolation and masking in healthcare
facilities, could result in disproportionate impact on these groups. Requiring cases to isolate
remains our most effective measure to reduce transmission of COVID-19, retaining case
ACT
isolation will materially reduce transmission. Its retention also allows for the management
of the response while removing or reducing other measures.
9.
s 9(2)(g)(i)
INFORMATION
10. Five days isolation with test to release is not recommended. Whilst less time in isolation is
undeniably beneficial, this needs to be carefully balanced against the multi-faceted public
messaging associated with introducing a negative test to release requirement, the potential
increase in cases infectious at release, expectations around compliance and the recording
of test to release results.
11. Further changes to border requirements: the removal of the requirement to provide contact
OFFICIAL
details for contact tracing purposes2; and modifications to testing guidance for new arrivals
were also considered.
THE
a. As contact tracing is not currently a feature of the COVID-19 response, the
requirement to collect information for contact tracing purposes is no longer required.
If the response changes, for example in response to a new variant, then contact
tracing information may be sought again. The current requirement for collection via
NZTD can be removed.
UNDER
b. The request to test on arrival currently applies for all passengers. The
recommendation is this is modified to apply specifically to passengers who either
arrive with, or develop symptoms, during their stay.
Outbreak status
Domestical y, at the time of the PHRA, the current outbreak appeared to have stabilised
RELEASED
1 Ministry of Health. 2022. COVID-19 Mortality in Aotearoa New Zealand: Inequities in Risk. Retrieved from
https://www.health.govt.nz/publication/covid-19-mortality-aotearoa-new-zealand-inequities-risk
2 Currently via the New Zealand Traveller Declaration (NZTD).
2
Document 3
12. The PHRA considered data to the week ending 25 September 2022, which showed all
measures used to monitor the COVID-19 epidemic as stable or reducing.
13. However, as of the week ending 7 October 2022, case counts have started to increase
slightly in the context of likely lower reporting/testing and overall lower case ascertainment
(although other key measures, including hospitalisations and deaths, remain stable):
a. there is currently an average of 1,598 new reported1cases per day nationally (7-day
rol ing average to 9 October 2022); this was a 12 percent increase on the previous
week
b. the 7-day rolling average of reported case rates was 32.2 per 100,000 population for 1982
the week ending 9 October; this was 11 percent higher than the previous week, which
was 28.6 per 100,000
ACT
c. hospital occupancy trends from COVID-19 have stabilised in the week ending 09
October and levels of viral particles in wastewater have been relatively constant in the
recent weeks to 02 October. The trend varied somewhat regionally, with some regions
experiencing increases and some decreases.
14. Note that a Ministry of Health COVID-19 hospitalisation data review has identified a coding
error which has resulted in potentially a significant number of COVID hospitalisations not
being captured in the official count. The coding team are working through the issue.
However, the technical issue appears to affect hospitalisations uniformly over time and
appears not to impact trends in the data. Therefore, it is unlikely that the data error has
INFORMATION
impacted current recommendations, as the error is in miscounts distributed across the
entire outbreak period from 2020 to present day and does not indicate a substantial
change in the current risk profile. This error did not impact the daily/weekly reporting of
number in hospital.
Following new data and intel igence over the past week, it is likely that New Zealand will experience a
further wave by the end of 2022
OFFICIAL
15. Model ing developed for and discussed at the PHRA, showed a slow rise through the end of
the year. However, this modelling was based on immune waning alone and not on the
arrival of new variants.
THE
16. It is likely that New Zealand will experience an increase in cases by the end of 2022, either
due to waning, new subvariants, and/or behaviour change. However, data is very
preliminary and as such the impact on cases, hospitalisations and deaths is unknown.
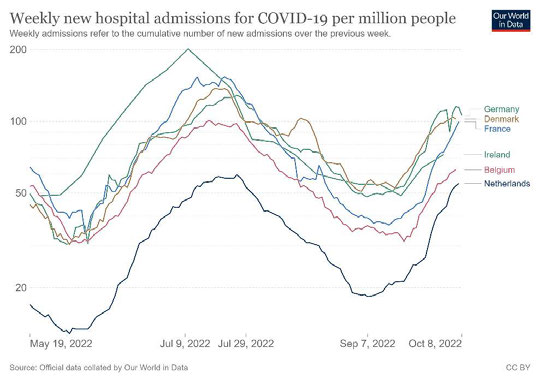
17. As indicated by Figure 1 belo
UNDER w, hospitalisations are rising in many counties in Europe.
RELEASED
3
Document 3
Figure 1: Weekly new hospital admissions for COVID-19 per million people (log scale)
1982
ACT
18. The data from the UK suggests that, at this time, this is due primarily to seasonality factors
(eg, returns to indoor settings, school/office) and immune waning (eg, due to time since
previous Omicron wave and boosting).3 Subvariants are not currently thought to be the
primary driver of the increase in hospitalisations and cases in Europe, due to the prevalence
of these new variants being too low at this time.
19. However, the collection of new subvariants is expected to be associated with an increase in
INFORMATION
cases in the future. The impact of the new variants on hospitalisations is unknown. It would
be expected that booster vaccinations against the new subvariants would still maintain
substantial protection against severe disease and hospitalisation, but no vaccine
effectiveness data is available that is specific to these new subvariants.
There are a number of subvariants circulating domestical y and international y that appear to have a
growth advantage over our predominant variant - BA.5
OFFICIAL
20. The data on subvariants is very uncertain and preliminary. However, bodies such as UKHSA
report with low confidence that new subvariants have a growth advantage and may cause
an increase in cases. Subvariant BA.2
THE .75 appears to show initial signs of increasing in
prevalence across New Zealand in both WGS and wastewater, and we have detected our
first case of BQ1.1 in the last few days. It is unknown what impact the new variants will have
on cases, hospitalisations and deaths.
21. Several subvariants may have a growth advantage over the current predominant variant,
UNDER
BA.5. However, generally a growth advantage of approximately 10 percent or more per day
is thought to be required to be associated with a variant-driven wave of cases. Data are
very preliminary, but it is thought based on European data that the growth advantage of at
least one of the new subvariants (BQ.1.1) is between 10-15 percent. If this is correct, we
would expect to see a rapid increase in the case numbers, sufficient to cause a wave.
a. BQ1.1 is a sub lineage of BA.5 with additional mutations that likely make it more
immune evasive.
RELEASED
b. Similarly, BA.2.75.2 is a sub lineage of BA.2 with immune evasion potential. It is likely
that the immune evasion properties are responsible for the growth advantage.
3 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment data/file/1109820/Technical-Briefing-46.pdf
4
Document 3
However, it is unknown if there will be an increase in hospitalisations or cases due to
BQ.1.1 or any of the new variants, as this has not been observed in international data
to date; only that the growth rate relative to other variants is elevated.
Subvariants such as BA.4.6 and BA.2.75 increased in the community in the most recent data from New
Zealand samples that have undergone whole genome sequencing (WGS)
22. The most recent data from samples that have undergone WGS has found:
a. BA.5. the dominant variant, accounts for ~75 percent of community individual WGS
cases, in the week 17-30 September with BA.4.6 comprising an additional 15 percent. 1982
b. Therefore BA.4 and 5 account for about ~90 percent of cases.
c. BA.2.75 has increased and accounts for ~10 percent.
23.
ACT
Of note since the PHRA, the Institute of Environmental Science and Research (ESR) have
now reported the first detection of BQ1.1 in New Zealand.
New Zealand wastewater testing indicates an increasing proportion of samples are not BA.5
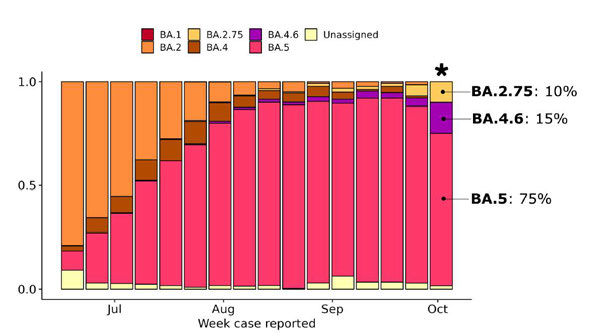
24. As indicated by Figure 2 below, there has been a recent increase in the proportion of
wastewater samples that are (sub)variants other than BA.5.
Figure 2: Frequency of variants/lineages in the past 16 weeks4
INFORMATION
OFFICIAL
THE
25. In summary:
a. Wastewater testing (WWT) estimates of the prevalence of BA.4/5 agrees with that of
individual WGS; BA.4/5 accounts for 90 percent of viral material in the WW (as of 02
October), which gives more confidence that the combined underlying prevalence of
UNDER
BA.5 and BA.4 in the community is likely truly ~90 percent, and is decreasing.
b. WWT is unable to distinguish between BA.4 and BA.5, and therefore cannot identify
increases in prevalence of BA.4.6 specifically.
c. WWT also agrees that there is an increase in BA.2.75; BA.2.75, accounting for ~7
percent of viral material in the WW, which aligns with the 10 percent from individual
RELEASED
4 Frequencies >1% are annotated in the last week. Note, data for the most recent fortnight is preliminary as it will be updated as cases
reported within these weeks are converted into genomes. Data from the week marked with an asterisk represents all sequenced cases,
before this reporting week border-related cases are excluded. Cases classified as Omicron (Unassigned) are typically partial genomes
where it is difficult to be definitive regarding variant/lineage. Source: COVID-19 Genomics Insights (CGI) Report #24, 6 October 2022.
https://www.esr.cri.nz/our-expertise/covid-19-response/covid19-insights/genomics-insights/
5
Document 3
WGS. This indicates that BA.2.75 may be increasing in prevalence in the community.
Monitoring of BA.2.75 includes the monitoring of sublineage BA.2.75.2.
d. BQ.1 has now been detected in New Zealand and would be expected to have a growth
advantage based on overseas experience.
26. WWT for variants is not influenced by the changes in the individual WGS testing patterns.
Recommendations
27. It is recommended that you agree to the following:
1982
Air travel to
1. Remove the requirement for air travellers to New Zealand
Yes
ACT
New
to provide information for COVID-19 contact tracing
Zealand
purposes prior to departure.
2. Note that the Customs (Arriving Passenger and Crew
Noted
Declarations) Amendment Rules 2022 will come into force
on 5 November 2022 requiring air travellers to provide
digital contact and travel history information that can be
shared with Health agencies for contact tracing purposes
as necessary under the Health Act 1956.
INFORMATION
Post-arrival
3. Modify the post-arrival testing guidance for all travellers
Yes
testing
to test if symptomatic only.
Isolation
4. Retain the current requirement for all cases to isolate for 7
Yes
and
days
OFFICIAL
quarantine
Household
5. Continue with guidance for al household contacts to test
Yes
THE
contacts
daily for five days, and if symptomatic beyond those five
days.
Face masks
6. Retain the current face mask requirements for visitors1 on
Yes
the premi
UNDER ses of health services, including aged and
disability-related residential care and disability support
services.
Further work
7. Agree that the variants of concern preparedness work
Yes
to improve
programme include measures to improve equity outcomes
equity
for Māori, Pacific, and disabled communities.
outcomes
RELEASED
Next PHRA
8. Agree any remaining requirements are reviewed at the
Yes
next PHRA.
6
Document 3
9. Agree that a further PHRA will be held in the last week of
Yes
November to again review remaining mandatory
measures.
Next steps
10. Agree to forward this memo to the Department of the
Yes
Prime Minister and Cabinet (DPMC) to contribute to the
paper for Cabinet on 17 October 2022.
11. Note that once you approve this memo, we will provide it
Noted 1982
to Te Whatu Ora, Te Aka Whai Ora, and Whaikaha and
suggest they provide any feedback to DPMC to reflect in
the Cabinet paper noted above.
ACT
12. Note that the advice contained in this memo may inform
Noted
work to change COVID-19 policy settings, such as the
amendment or revocation of COVID-19 orders.
Detailed discussion of the recommendations
Case isolation and requirements for household contacts
INFORMATION
Current requirement
Mandatory 7-day self-isolation of COVID-19 cases
Director Public Health
Retain the current requirement for all cases to isolate for 7 days.
recommendation
Public health rationale
OFFICIAL
Requirements for case isolation and associated supports remain critical
Case isolation remains a cornerstone of our response to limiting transmission
COVID-19 within the community. Isolation of cases can break the chain of
THE
transmission by preventing infectious people from having contact with, and
infecting others within the community.
Without required case isolation and associated supports, it is highly likely that
adherence to guidance to isolate would be lower, leading to more infectious
cases in the community, leading to increased community cases.
UNDER
Removing case isolation and associated supports is likely to increase health
inequities
It is likely that the increase in community cases would affect some
communities and population groups more than others. Specifically:
There is an acknowledged differential exposure to COVID-19 risk related
RELEASED
to socioeconomic status.5 People in lower socioeconomic groups are
more likely to work in jobs with greater risk of exposure, to live in larger
5 Beale S, Braithwaite I, Navaratnam AM Virus Watch Collaborative, et al
Deprivation and exposure to public activities during the COVID-19 pandemic in England and Wales J Epidemiol Community
Health 2022;76:319-326.
7
Document 3
and typical y more crowded houses, and to have underlying risk factors. If
there are more infectious people circulating in a community with more
baseline contacts, this increases the likelihood of onward transmission.
People who are socioeconomically deprived are more likely to face
chal enges in being able to isolate compared to people with greater
access to socioeconomic benefits. This includes differing access to sick
leave, income loss, and potential pressure from employers to return to
work. Earlier return to work comes at the cost of increasing transmission,
which is likely a more significant effect on health outcomes and ability to
work due to illness.
1982
As a result, people who experience higher levels of socioeconomic
deprivation may be more likely to not test, not report results, or break
isolation, potentially causing further cases and further inequities.
ACT
These inequities would likely be exacerbated, rather than mitigated, if
requirements for self-isolation and associated supports (such as Care in
the Community and the Leave Support Scheme) – which are vital for
enabling people in these communities to practically be able to isolate -
were removed.
Feedback from sector stakeholders echoed many of the concerns above:
Compromising equity aims – the Leave Support Scheme (LSS) is closely
tied to isolation mandates. Loss of the LSS would present risks for
INFORMATION
vulnerable populations and workforces with fewer protections.
Coercion to return to work particularly for the most vulnerable - Strong
concern was expressed that if the isolation mandate was removed,
employees may be pressured to return to work even if not fully
recovered. Equity concerns were central to this feedback, particularly
what this change might mean for Māori and Pacific communities.
OFFICIAL
Increased transmission because of relaxed requirements - Removing the
isolation mandate will almost certainly result in increased transmission,
due in part to the message it sends regarding the importance of isolation
THE
and because of the inability of people to isolate due to the two factors
above. Again, equity concerns were raised as any increase in cases will
impact the priority populations most.
COVID-19 continues to pose a substantial public health risk, which is different
UNDER
from other respiratory and communicable diseases
Disease burden: To date, 2,055 deaths have been attributed to COVID-
19 (9 October) out of approximately 1.7 million reported cases. Most of
this burden has fal en on the elderly. The disease burden also falls
disproportionately on Māori and Pacific communities, and those with
prior conditions including disabilities, and those in low socio-economic
conditions, among other groups. With respect to hospitalisation, the
RELEASED
overall population rate is 0.6 per 100,000 (18 September). Older people
have substantially higher hospitalisation rates and, within each age
group, Māori and Pacific communities also have higher hospitalisation
rates.
8
Document 3
Post-infection sequelae: This includes long COVID, and increased risk
factors for a range of other conditions (for example, cardiovascular
disease,6 neurologic and psychiatric disorders,7 changes in brain
structure,8 and diabetes).9 The data on long COVID is developing but
there are still many unknowns and we need to continue to monitor the
risk.
The best way to reduce overall burden and protect vulnerable
communities is via a combination of targeted measures (eg, additional
precautions in Aged Residential Care facilities) and reduction of overal
transmission in the community. Isolation and quarantine measures are 1982
among the most effective public health tools at reducing overall levels
of community transmission.
ACT
A legal requirement to self-isolate is a cornerstone of the public health response
The best practice approach to managing infectious notifiable diseases
transmitted through the droplet or airborne route is to require isolation of
cases during their period of infectivity. This is the most effective tool for
controlling disease transmission. The high transmissibility of COVID-19
reinforces the need for case isolation, which has been a cornerstone of the
public health response throughout the pandemic.
While there has been a reduction of isolation requirements over the course of
the outbreak, we have reached what is probably the minimum threshold for
INFORMATION
self-isolation to remain an effective intervention.
Other control tools, such as requiring masks or physical distancing are
significantly less effective than isolation. Furthermore we note that to be
effective these tools are most effective when utilized across the entire
population. We note also that it is important to see these tools as a suite of
protections that work together. Each tool can be dialled up or down. We have
OFFICIAL
been able to recommend removing or reducing some of those other tools in
part because isolation has remained in place. However, there is no
combination of other mechanisms that would come close to producing the
THE
public health benefit that required self-isolation does.
Available evidence suggests that most people remain willing to isolate
Available data indicates that – currently – most people are willing to isolate,
and do isolate.
UNDER In July, 88 percent of people surveyed indicated they were willing to
isolate if they had COVID-19, were symptomatic, or if a household
member tested positive.10
In an online survey of 1505 adults undertaken 15-20 September 2022,
8% of participants had tested positive for COVID-19 in the past two
RELEASED
6 Xie, Y., Xu, E., Bowe, B. et al. Long-term cardiovascular outcomes of COVID-19. Nat Med 28, 583–590 (2022).
https://doi.org/10.1038/s41591-022-01689-3
7 Wise J. Covid-19: Increased risk of some neurological and psychiatric disorders remains two years after infection, study
finds BMJ 2022; 378 :o2048 doi:10.1136/bmj.o2048
8 Douaud, G., Lee, S., Alfaro-Almagro, F. et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature 604, 697–
707 (2022). https://doi.org/10.1038/s41586-022-04569-5
9 Xie, Y. & Al-Aly, Z. Lancet Diabetes Endocrinol. https://doi.org/10.1016/S2213-8587(22)00044-4 (2022).
10 The Research Agency (TRA). July 2022 DPMC Behaviour & Sentiment Topline.
9
Document 3
weeks and 9% of participants were self-isolating in the same two week
period The survey sample is representative of Aotearoa New Zealand
and suggests that currently adherence to self-isolation is high.
In the same survey, 83% of participants indicated they were likely or
very likely to self-isolate for the 7 day period if they were to test
positive for COVID-19 in the future. This intention remained high
(78%) for participants who had already tested positive for in the past
two weeks.
It is very clear that compliance wil be significantly higher with a mandate than
with a recommendation
1982
Evidence from overseas suggests that a legal requirement to isolate will have
significantly greater adherence than a recommendation to isolate. In the UK,
there was a significant drop in compliance with isolation requirements after th
ACT e
legal requirement to self-isolate was dropped on 24 February 2022. Based on
survey data of people who tested positive for COVID-19, 80 percent were fully
compliant in February, dropping to 64 percent in early March, and 53 percent
in late March.11
This concern is supported by the significant drop in people wearing face masks
on public transport since the removal of the mandate in September – despite it
remaining a recommendation that people do so.
Model ing results (CMA)
INFORMATION
Model ing suggest that the current mandatory isolation policy is approximately
preventing 450 hospitalisations and 50 deaths in the short term compared to
guidance with a reduction to 5 days. Over a year, it is estimated to prevent
1000 hospitalisations and 300 deaths.
When current settings are compared to mandatory with test to release from 5
days, the model estimates that curren
OFFICIAL t settings are preventing 40
hospitalisations and 50 deaths in the short term. Over a year, it is estimated to
prevent 250 hospitalisations and 30 deaths.
THE
Accurate domestic data on the behavioural impact of shifting from mandatory
isolation to guidance is lacking. However, data from the UK infection survey
(based on adherence rates to guidance in the UK) suggests potentially larger
increases in cases and hospitalisations from such a change.
Key limitations of the isolation model are that it assumes RAT sensitivity to be
UNDER
constant over the duration of illness and does not account for increased
sensitivity at day 5. This means that the proportion of cases released who are
infectious may be overestimated. Another limitation is that incomplete
isolation under mandatory requirements is not fully accounted for. Both of
these limitations would tend to overestimate the magnitude of increase
associated with changes to the status quo. Furthermore the modelling does
not account for a new variants which could substantially increase infections.
RELEASED
Model ing results are described in more detail in Appendix 1.
11
https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandwellbeing/bulletins/coronavirusandselfisolationaf
tertestingpositiveinengland/17to26march2022
10
Document 3
It was noted that further change, such as the introduction 5-day self-isolation
plus test to release, is likely to create additional uncertainty and confusion.
People are more likely to adhere if isolation is mandatory. However, we have
no accurate estimate of the proportion of people fol owing the mandatory
required. Behavioural data indicate 88% of those surveyed (July 2022) would
follow isolation rules if they tested positive. Operational providers have
reported that they believe the most critical factor is not whether isolation is
mandatory or recommended, but rather whether people are adequately
supported to do so.
1982
Other comments
System of supports to enable cases to isolate
In order to limit the likelihood of further increases in inequity, it is critical that
ACT
the system of supports that enables people to test, isolate, and reduce risk of
onward transmission are maintained. Specifically:
Leave Support Scheme (LSS) - is closely tied to the retention of
mandatory isolation. While not a consideration for the PHRA, there
was strong support for the retention of the LSS, or a revised support
scheme to replace it. The LSS is regarded as a key enabler to prevent
cases returning to work when they are unwell and/or still infectious.
The LSS is currently under review by Treasury and the Ministry of Social
Development (MSD) – it may be that consideration be given to the
INFORMATION
most appropriate means of providing the necessary supports for
populations which are most negatively impacted by mandatory self-
isolation requirements.
Care in the Community – specifically, it is important that supported
isolation is available for families who need to isolate away from
another vulnerable member of the household.
OFFICIAL
Availability of free masks and RATs for the general public.
Availability of free N95 type masks for people at high risk of severe
outcomes.
THE
Essential Permitted Movements
The Chair requested a paper on Permitted Movements be developed for the
next PHRA meeting, to allow further consideration of the issue. Advice has
been provided to the Minister to al ow parents and caregivers who are cases to
UNDER
drop their dependents off at school. A further category includes allowing
people to return to their usual place of residence to isolate if they are on
holiday elsewhere and can do so safely.
Regulation of point of care testing
Currently, the importation, manufacture, supply, sale, packaging or use of point
of care tests is regulated under the COVID-19 Public Health Response (Point-
of-care Tests) Order 2021. The purpose of this regulation is to ensure that
RELEASED
point of care tests that are relied upon to establish whether a person is subject
to mandatory self-isolation requirements are accurate and reliable.
It is appropriate to maintain the regulation of point of care testing, so long as
mandatory self-isolation requirements remain in place.
11
Document 3
Other countries that have retained some level of required isolation for cases
Legally mandated isolation for a subset of higher-risk workers:
Australia (from 14 October 2022).
Legally mandated isolation with test to release from 5 days: Germany.12
Guidance for household contacts of COVID-19 cases
Current requirement
All household contacts of COVID-19 cases are recommended to test daily for
five days.
1982
Director Public Health
Continue with guidance for all household contacts to test daily for five days,
recommendation
and if symptomatic beyond those five days.
ACT
Public health rationale
The recent removal of quarantine requirements does not appear to have
significantly altered case and hospitalisation numbers. Based on this
experience and the current outbreak context, 5-day daily testing of household
contacts continues to provide a sufficient risk mitigation.
Other comments
Members of the Committee noted the following concerns with the possibility
of changing from the current approach:
change at this time may result in confusion and change fatigue for the
public
INFORMATION
data does not exist on adherence with the status quo. If most contacts
are not following the 5-day testing recommendation a change to
recommending testing on symptom onset may have little impact on
risk.
OFFICIAL
Face masks
Current requirement
The requirements for masks are set out in the COVID-19 Public Health
THE
Response (Masks) Order 2022. The Order specifies that:
masks are legally required for visitors13 in a wide range of health
service settings including primary care, urgent care, pharmacies,
hospitals, aged residential care (ARC), disability-related residential care,
allied health, and other health service settings
UNDER there are exclusions for: patients and people receiving residential care,
health service staff, and visitors to specific health services
(psychotherapy, counselling, mental health and addiction services).
Requirements for patients and workers of health services are determined
local y, based on local assessments in line with Infection Prevention and
Control Guidance.
RELEASED
12 https://handbookgermany.de/en/coronavirus-general-info
13 COVID-19 Public Health Response (Masks) Order 2022, section 5(1)(a): “A person must wear a mask when they are at the premises of a
health service unless the person is a patient or worker of the health service”.
12
Document 3
Director Public Health
Retain the current requirement as described above.
recommendation
Public health rationale
The evidence that mask wearing decreases the rate of transmission of
COVID-19 (and other airborne respiratory viruses) is substantial. An earlier
briefing (HR20221311) provides an overview of the evidence base in
relation to mask use, and mask mandates.
The effectiveness of mask mandates as a public health intervention will
depend on several factors – including the level of community transmission
at the point in time, the nature of the settings in which masking is required, 1982
cultural and geographical norms around masking, correct mask use, and the
extent to which improvements to ventilation/filtration have been enacted as
systemic primary prevention.
ACT
Health service settings have a series of characteristics that elevate the risk
of transmission and/or the risk of severe disease. These settings typical y:
are more likely than other settings to have people present with
undifferentiated viral illness, either because they are seeking help for
symptoms or because they have a co-existing medical emergency
are also more likely to have people present who are vulnerable, either
due to advanced age, underlying conditions, or to being unwell at the
time - facility-level mask requirements lean against inequity, to ensure
that people who are at higher risk can access health services without
INFORMATION
avoidable additional risk14
have variable ability to improve crowding, indoor ventilation and/or air
filtration15
hospital-acquired COVID-19 infections are more likely to have poorer
outcomes than community-acquired COVID-19 infections.16
OFFICIAL
While adherence to mask requirements may be waning or patchy in some
health service settings, it is possible that adherence would drop further
if the mandate was removed. This is evidenced by the decrease in people
masking on publ
THE ic transport in the past month (which has remained
recommended by the Ministry of Health).
Mask requirements lean against inequity, to ensure that people who are
at higher risk can access health services without avoidable additional
risk. A conservative estimate is that one in every six New Zealanders is at
UNDER
14 A conservative estimate is that one in every six New Zealanders is at higher risk of severe illness if they contract COVID-19 (‘Options for
improving respiratory protection against aerosolised viral particles for vulnerable and priority populations’ (HR20220682), 29 April 2022).
Mask mandates in health service settings have two benefits for people in this group: it means that they will (a) be less likely to actually be
infected, and (b) be more likely to feel able to continue to safely access healthcare. In many cases people accessing health services are
unable to choose not to do so.
15 Many health service settings don’t have good design or engineering so that the added value of masks to protect the vulnerable
RELEASED
(patients, staff and visitors) become really important when there is frequent introduction of infection into those environments. This is
especially true of healthcare settings in the community, but also remains a real issue in many hospitals. Many older wards are
predominantly multibed rooms (often 4-6 bed), shared bathrooms and no doors on rooms. In this context, it is often hard to isolate and
improve air filtration.
16 In Victoria, Australia, 7.6 percent of hospital-acquired COVID-19 infections resulted in death, compared to 0.14 percent of reported
cases in the general population in the same period. This demonstrates that infections in hospital settings are associated with significantly
(over 50-fold) higher mortality. Victoria Department of Health. 2022. Chief Health Officer Advice to Premier, 29 August 2022. Retrieved
from https://www.health.vic.gov.au/publications/chief-health-officer-advice-to-premier
13
Document 3
higher risk of severe illness if they contract COVID-19.17 Mask mandates in
health service settings have two benefits for people in this group: it means
that they wil (a) be less likely to actually be infected, and (b) be more likely
to feel able to continue to safely participate in basic activities of daily life,
such as accessing healthcare. In many cases people accessing health
services are unable to choose not to do so.
Removing mask mandates in health service settings may lead to an
increase in cases of hospital-acquired COVID-19. Feedback from two
districts has noted possible links between visitors and hospital-acquired
cases of COVID-19.18 There is still value in trying to prevent infections,
1982
even for highly transmissible variants. While it may not be possible to
get Re to below 1 with highly infectious variants/subvariants, there is still
significant value in trying to prevent infections where possible, as each new
ACT
infection (or reinfection) effectively ‘rolls the dice’ for one or more post-
acute sequelae that are known to occur such as long COVID, and increased
risk of long term (up to 1 year) cardiovascular complications compared to
individuals without COVID-19.19 Long COVID and other post-acute
sequelae have personal costs, but also broader impacts on society, in terms
of outcomes such as increased disability, increased welfare and health costs,
and reduced workforce participation.20
Other comments
Other options considered
If the mask mandate for visitors to health service settings was removed, it
INFORMATION
may create some operational challenges, which would need to be worked
through at a facility level:
If health care facility is still requiring mask use on site (or in certain
higher risk areas within their site) but this is not covered by a
mandate, it may result in security/conflict resolution situation for staff
to manage if members of public do not wish to follow facility rules.
OFFICIAL
Currently, health services can use the Order to compel visitors.
Without mandate, it may be more difficult to deal with a visitor who
refuses to wear a mask, and this may become a more common event.
THE
Evidence that enforcement of mask policy would be more difficult
than mask requirements under an order is limited.
17 The Ministry of Health does not have precise figures for the number of New Zealanders who meet the definition of being at higher risk.
UNDER
However in April 2022, the number of ‘clinically vulnerable’ people (which is defined more narrowly than ‘high risk’) was estimated at
800,000. ‘Options for improving respiratory protection against aerosolised viral particles for vulnerable and priority populations’
(HR20220682), 29 April 2022.
18 “Anecdotal y, visitors have featured in many in-hospital transmission events in many units, especial y geriatrics/rehab wards which
have a high proportion of vulnerable patients. This may have been due to lapses in mask compliance by visitors during the visit (eg,
sharing a cup of tea, or kissing/hugging patient).” “We have had a number of clusters and outbreaks here and when COVID is
everywhere, it is difficult to attribute outbreak sources with any degree of certainty. The relevant ward nurses felt that several of our
events were likely caused by infectious visitors. At the time, mask wearing behaviour by visitors was frankly poor and some visitors
became abusive when asked to wear masks.”
RELEASED
19 See Ballering AV, van Zon SKR, olde Hartman TC, Rosmalen JGM. ’Persistence of somatic symptoms after COVID-19 in the Netherlands:
an observational cohort study’. The Lancet. 2022;400(10350):452-61; and Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes
of COVID-19. Nature Medicine. 2022;28(3):583-90.
20 For example an August 2022 report from the Office for National Statistics in the UK estimated that 1.8 million people living in private
households were experiencing self-reported long COVID (symptoms continuing for more than four weeks after the first suspected COVID-
19 infection that were not explained by something else) see
https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymp
tomsfollowingcoronaviruscovid19infectionintheuk/4august2022.
14
Document 3
Health services would need to consider implications on
patients/residents exposed to visitors, and the potential for an
increase in patients developing hospital-acquired COVID-19 infections.
If the mask mandate for visitors is removed and most visitors are not
wearing masks, one service reported that they may need to consider
implications for staff mask requirements. They considered that it could
be hard to defend mask use around patients if other (non-staff)
people entering the clinical zone are not required to wear them.
Clear public communication is critical under all options
1982
Key to success of any of the options is the clear communication of the
strategy to the public and to healthcare workers.
It is also important to signal that we may need more widespread use of
ACT
masks again if community transmission increases.
Health services situated within other settings
The Committee reaffirmed that where a health service that is situated
entirely within a non-health service (eg, a pharmacy within a supermarket,
or a physio within a gym) the health service is expected to comply with the
Order.
Provision of information using the New Zealand Traveller Declaration for contact
INFORMATION
tracing prior to departure
Current requirement
Air travel ers coming to New Zealand are required to declare, before they
arrive, their contact details and travel history through the NZTD for the sole
purpose of COVID-19 contact tracing, should they need to be urgently
contacted in response to a serious new variant of concern.
OFFICIAL
This requirement is the only substantive remaining health requirement in the
COVID-19 Public Health Response (Air Border) Order 2021.
THE
Director Public Health
Remove the requirement under the Air Border Order, with effect from 05
recommendation
November 2022, for air travellers to New Zealand to provide information
using the NZTD for COVID-19 contact tracing purposes prior to departure.
Public health rationale
The mandatory requirement is not considered proportionate in the current
contex
UNDER t. The requirement relates to a potential future risk and not an
immediate or likely variant requiring action shortly.
However, having air traveller contact details and travel history electronically
collected using the NZTD supports a more efficient and accurate dataset of
passenger information should contact tracing be required.
While the likelihood of needing to stand-up contact tracing of air passengers is
considered low in the current context, the rate at which SARS-CoV-2 continues
RELEASED
to mutate means that we need to ensure our systems remain prepared.
Given the value of this measure, NZ Customs have indicated the requirement
can be continued under the Customs and Excise Act 2018 should there no
longer be a public health rationale to do so.
15
Document 3
Continuing the requirement under Air Border Order until the amended
Customs (Arriving Passenger and Crew Declarations) Rules 2022 comes into
force on 5 November means that there will be a seamless transition and the
ability to contact passengers in the intervening period will be retained.
The most likely scenario where contact tracing may be required would be a
Other comments
new variant that has high severity, high immune escape and low
transmissibility.
Contact tracing is likely to be of limited value in response to a serious new
variant of concern in the absence of other restrictive measures (such as border
closures, pre-departure testing, post-arrival isolation).
1982
Testing of arrivals at the air border
ACT
Current requirement
Air arrivals are encouraged to do a RAT on the day of arrival (0 or 1) and on
day 5 or 6 and to report a positive test result via phone or My Covid-Record. If
positive, they are encouraged to get a free polymerase chain reaction (PCR)
test from a community clinic or GP, so this can be available for whole genome
sequencing.
PHRA recommendation
Modify the post-arrival testing guidance for all travel ers to test if
symptomatic only.
INFORMATION
Director Public Health
Advising all international arrivals at the air border to test on day 0 or 1 and on
recommendation
day 5 or 6, when asymptomatic, is not proportionate given the lower
prevalence of COVID-19 currently circulating globally, the relatively high
impost on travellers, the cost of providing and distributing the RATs at the
airport and the risk of false positives.
Relative effectiveness
OFFICIAL
Post-arrival testing provides additional (early) surveillance of new variants that
may be entering the border. However, the 1-to-2-week lag time from the point
of arrival to having a result from a positive PCR genomically sequenced means
THE
testing at the border is unlikely to detect new variants arriving in the country
before community spread of these variants occurs.
Moreover, based on the drop off in PCR testing numbers, it is assumed
adherence to this guidance is low.
UNDER
Equity
There are equity concerns around the testing performance of large groups of
asymptomatic people because of the testing performance of RATS. For testing
performance of RATS:21 22
the false positivity rate is approximately 1%-2%
RELEASED
21 Ministry of Health. 2022. Approved RATs and how to use them (as at 26 May 2022), viewed on 5 October 2022
https://www.health.govt.nz/covid-19-novel-coronavirus/covid-19-health-advice-public/covid-19-testing/rapid-antigen-testing-
rat#regulatory.
22 Indelicato AM, Mohamed ZH, Dewan MJ, Morley CP. Rapid Antigen Test Sensitivity for Asymptomatic COVID-19 Screening. PRiMER. 2022
Jun 22;6:18. doi: 10.22454/PRiMER.2022.276354. PMID: 35812789; PMCID: PMC9258726. /
16
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 3
decision making. It was requested this updated information be provided at the next
PHRA.
Related to the above, the impacts of long COVID need to be included in the data and
modelling to provide a more comprehensive assessment of the risks and impacts of
COVID-19.
Equity and Te Tiriti considerations
Impact of COVID-19 on vulnerable populations
1982
29. Demonstrating a commitment to the achievement of health equity and Te Tiriti o Waitangi
remains a critical priority in the COVID-19 public health response. COVID-19 has
exacerbated pre-existing health inequities for many groups, particularly those underserved
ACT
by the existing system. This is often due to overlapping social, clinical, and occupational risk
determinants.
30. As shown in Appendix 1, older people are more likely to be hospitalised and this is
reflected in the latest data. As the virus takes longer to move through this population due
to this group having fewer social interactions it may lead to a higher hospitalisation burden
over a longer period.
31. The COVID-19 Mortality in Aotearoa New Zealand: Inequities in Risk report, released
30 September 2022 highlights the disparity of the impacts of the pandemic. Overall
mortality continues to decline. However, after adjusting for age, comorbidities and
INFORMATION
vaccination status, the report showed that the risk of COVID-19 mortality in Māori is 2.2
times higher than that of European and Other group, while for Pacific Peoples the risk was
2.8 times higher.23
32. Pacific Peoples continue to be disproportionately affected by COVID-19. Moreover, they
continue to experience long-standing inequitable health outcomes and service use. Recent
OFFICIAL
data shows Pacific Peoples are the demographic most hospitalised for COVID-19.24
33. Disabled people and those with underlying medical conditions are more likely to be
hospitalised or require medical intervention/support if they test positive with COVID-19.
THE
While deprivation is a proxy, the Committee noted that there is no data and modelling of
hospitalisation and mortality data for disabled communities.
34. While cases and hospitalisations continue to trend downwards overal , several Committee
members expressed strong reluctance to removing self-isolation and mask requirements,
UNDER
without focused modelling on how this would impact Māori, tāngata whaikaha Māori and
disabled people. Current modelling on potential policy changes forecasts impacts such as
case numbers, hospitalisations and mortality for the general population, but it does not
forecast impacts of policy changes for vulnerable groups. The Committee therefore made
its recommendations using the precautionary approach. Development of modelling to
specifically assess equity impacts will assist in addressing this issue.
35. Mandatory self-isolation requirements provide an important safeguard against workers with
RELEASED
COVID-19 returning to work before they have recovered. The Māori Regional Coordination
Hub has indicated that wider consultation should accompany any removal of the self-
23 Ministry of Health. 2022. COVID-19 Mortality in Aotearoa New Zealand: Inequities in Risk. Wellington: Ministry of Health
24 Ibid.
18
Document 3
isolation requirements as it would disproportionately affect the Māori community.
Recommending the retention of self-isolation requirements would help to ensure that
those most vulnerable continue to be able to rest and recover while ill, and do not spread
the virus further among their potentially vulnerable community. Retention of the Leave
Support Scheme will help mitigate these risks.
36. Committee members highlighted that the more distant disproportionate impacts of long
COVID on vulnerable groups must be considered when assessing the public health risk of
stepping down measures. Māori, Pacific Peoples, disabled people and elderly are at greater
risk of developing long COVID and suffering worse health outcomes than the general
population. Māori, for instance, may suffer long COVID for longer than non-Māori. In one 1982
study, 75% of Māori participants had long COVID for more than three months, compared to
only 65% of non-Māori.25
ACT
Stakeholder engagement and key issues and themes emerging
37. Across the board there was strong support for retaining the current mandated measures to
protect vulnerable communities. The move away from the Elimination Strategy and removal
of other mandatory requirements were considered to put these communities at greater risk.
38. The removal of border restrictions and the threat of new variants easily entering the
community is a particular concern for groups with already compromised immunity, limited
access to anti-viral medication and concerns about the relative effectiveness of vaccinations
against new variants.
INFORMATION
39. The changes have caused anxiety in these communities, especial y amongst disabled
people. People are choosing to make individual risk assessments that have resulted in
ongoing isolation or limited interactions with others in their community. Assurances are
also being sought from providers concerning the vaccination of their staff and the ability to
require face masks for home visits.
40.
OFFICIAL
More general y, there is a concern that the community at large may not take the risk of
COVID-19 seriously and put vulnerable populations at greater risk. As noted previously,
there is a strong preference among vulnerable communities for the elimination of COVID-
THE
19. Emerging from this is a desire to build “borders” around these vulnerable populations
through either differentiated public health responses or the retention of current
requirements to ensure that people exercise the behaviours necessary to limit the mortality
and morbidity amongst these populations.
Addressing equity concerns
UNDER
41. It is important that the measures are not viewed in isolation. The new approach to
managing COVID (“prepared, protective, resilient, and stable”) is predicated on using a suite
of voluntary and enforceable measures to address both general and specific risks. A
package of measures could be developed that provides for an effective and proportionate
response to manage the risk of COVID-19 and improve equity outcomes for Māori, Pacific
and disabled communities.
RELEASED
42. For example, based on the feedback received at both the PHRA and from stakeholder
engagement, significant gains can be made through improved communications and
25 Ministry of Health. 2022. Long COVID Evidence Update - 11 August 2022. Wellington: Ministry of Health. 16.
19
Document 3
programmes targeted to those communities. Other system supports like the Leave Support
Scheme could also prove crucial to encouraging the behaviours being sought.
43. Enforceable or mandatory measures can also be re-introduced if the COVID-19 situation
significantly changes. This would be an effective and proportionate response to a
worsening risk profile. While such rights limiting measures may be more controversial than
they have been in the past regarding the social licence, the legal test remains the same.
44. Therefore, it is recommended that a work programme be developed that seeks to lessen
the adverse impacts of COVID-19 on Māori, Pacific and disabled communities. This could
include exploring potential data and modelling improvements for vulnerable populations 1982
recommended by the Committee. It could also encompass the effects of long COVID which
was also recommended that more work be done on. This work will provide assurance to the
Committee and others of:
ACT
a. how we can best meet our Te Tiriti and other obligations
b. provide certainty about our future response to any changes to the risk presented by
COVID-19, and
c. how we might differentiate the measures used to address the risk profiles for different
communities.
s 9(2)(h)
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
20
Document 3
s 9(2)(h)
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
21

Document 3
Next steps
52. Pending your approval, this memo wil be provided to the Department of the Prime
Minister and Cabinet to inform the overarching paper the Minister for COVID-19 Response
wil take to Cabinet on 17 October 2022.
1982
ACT
Signature
Date: 12 October 2022
Dr Nicholas Jones
Director of Public Health
Public Health Agency
Manatū Hauora
INFORMATION
Signature ____________________________________________________
Date: 12 October 2022
OFFICIAL
Dr Andrew Old
Deputy Director-General
Public Health Agency
THE
Manatū Hauora
UNDER
Signature ____________________________________________________
Date: 12 October 2022
Dr Diana Sarfati
Director-General of Health
Manatū Hauora
RELEASED
22
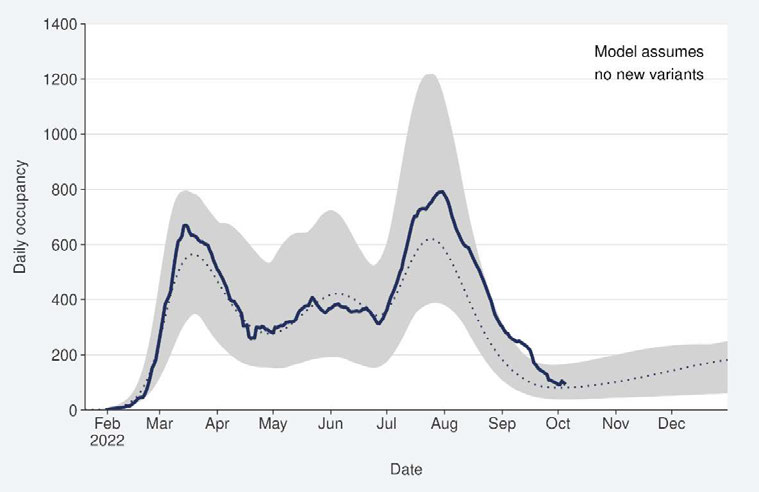
Document 3
Appendix 1: Current outbreak status and summary of modelling
1.
The 7-day rol ing average of reported case rates was 32.2 per 100,000 population for the
week ending 09 October. This was a 11% increase from the previous week, which was 28.6
per 100,000.
2.
All evidence continues to support stabilisation in incidence in the community: reported case
rates and levels of viral ribonucleic acid (RNA) in wastewater have been declining since 10
July but both measures have been relatively constant in the recent weeks to 02 October.
The trend was similar for all regions.
1982
3.
Model ing scenarios suggest that current hospital occupancy is tracking near the higher
range of the prediction for the past two months. It is now tracking closer to the median
projection and is expected to remain stable or slightly increase in the coming months.
ACT
Model ing scenarios account for changes in masking and contact quarantine on 12
September and assume no new variants.
INFORMATION
OFFICIAL
THE
4.
The age-standardised Māori cumulative hospitalisation rate for COVID-19 is 2.1 times
higher than European or Other. Pacific Peoples have the highest cumulative rate of
UNDER
hospitalisation with COVID-19 which is approximately 2.8 times higher than European or
Other.
RELEASED
23
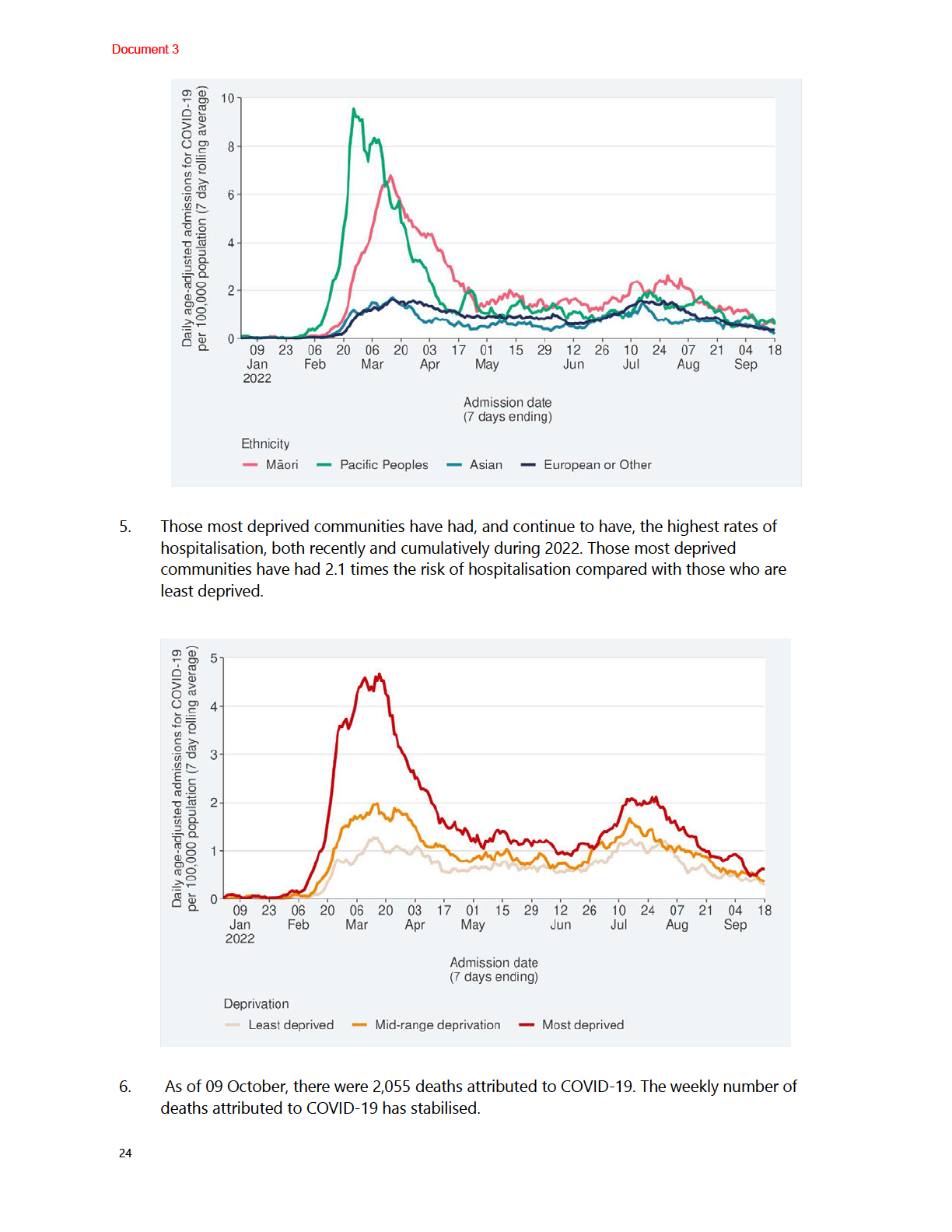
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 3
7.
The modelling results have been produced rapidly to help inform policy advice. They
should be considered as indicative as there are significant uncertainty around the impact of
policy changes and the level of immunity in the population and population behaviour.
8.
Model ing has considered a range of scenarios to reflect this uncertainty by estimating
pessimistic, middle, and optimistic scenarios, reflecting different levels of compliance with
guidance on isolation, specifical y to estimate the effect of shift away from mandated
isolation requirements, should the Epidemic Notice be lifted.
9.
Within the first month, shifting isolation requirements to 5-days guidance no test to
release (TTR) is modelled to increase cumulative hospitalisations by roughly 450 to
1982
1040 and increase deaths by 50 to 170, relative to no change in policy. Over a year, these
increases are 7900 to 8900 for hospitalisations and 1860 to 2160 for deaths.
10. Within the first month, shifting to a requirement to TTR after 5 days for a maximum of 7
ACT
days is modelled to increase hospitalisations by roughly 45 to 640 and increase deaths
by 6 to 120. Over a year, these increases are 7900 to 8050 for hospitalisations and
1870 to 1900 for deaths.
11. Moving to 5-days TTR maximum 7-days guidance is modelled to increase hospitalisations
by roughly 300 to 890 and increase deaths by 40 to 150, relative to no change in policy.
Over a year, these increases are 7900 to 8600 for hospitalisations and 1870 to 2080 for
deaths.
12. Across the scenarios, for-covid hospital occupancy peaks at between 200 and 304 beds,
INFORMATION
compared to a peak of 700 beds in the BA.5 wave. When looking at the high confidence
limit of these estimates, for-covid hospital occupancy still peaks below the BA.5 wave peak
at around 402 beds.
13. Importantly, the model assumes no new variants, therefore the long-term results do not
reflect the likely path of the pandemic. If an immune escape variant should arise, the
estimates for above will change and the modelled results will no longer be valid.
OFFICIAL
14. In general, the short-term peak in cases and hospitalisations can be mitigated by phasing
policy changes over a longer period of time.
THE
15. A note on Rt sensitivity and asymptomatic cases: Given the sensitivity of RATs through
time, a rule that says to only test on the first day of symptoms will miss a large number of
cases. Additional y, 30-40% of infections are asymptomatic.
16. An important caveat is the equity impacts of these changes have not been modelled, in part
due to limited available data
UNDER , but also limitations of the models. However, observations of
prior disease burdens for COVID-19 and based on general observations across public
health, moving some settings from mandates to guidance will likely lead to inequitable
outcomes.
a. Māori and Pacific peoples are more at risk of severe negative health outcomes than
non-Māori non-Pacific Peoples of the same age, and are also more likely to
experience greater disease exposure.
RELEASED
b. Poorer people are at greater risk of severe negative health outcomes than affluent
people of the same age, and are also more likely to experience greater disease
exposure.
c. Shifting to guidance is likely to disproportionately affect those who do not have the
ability to choose to fol ow the guidance. This may include: people in precarious
25
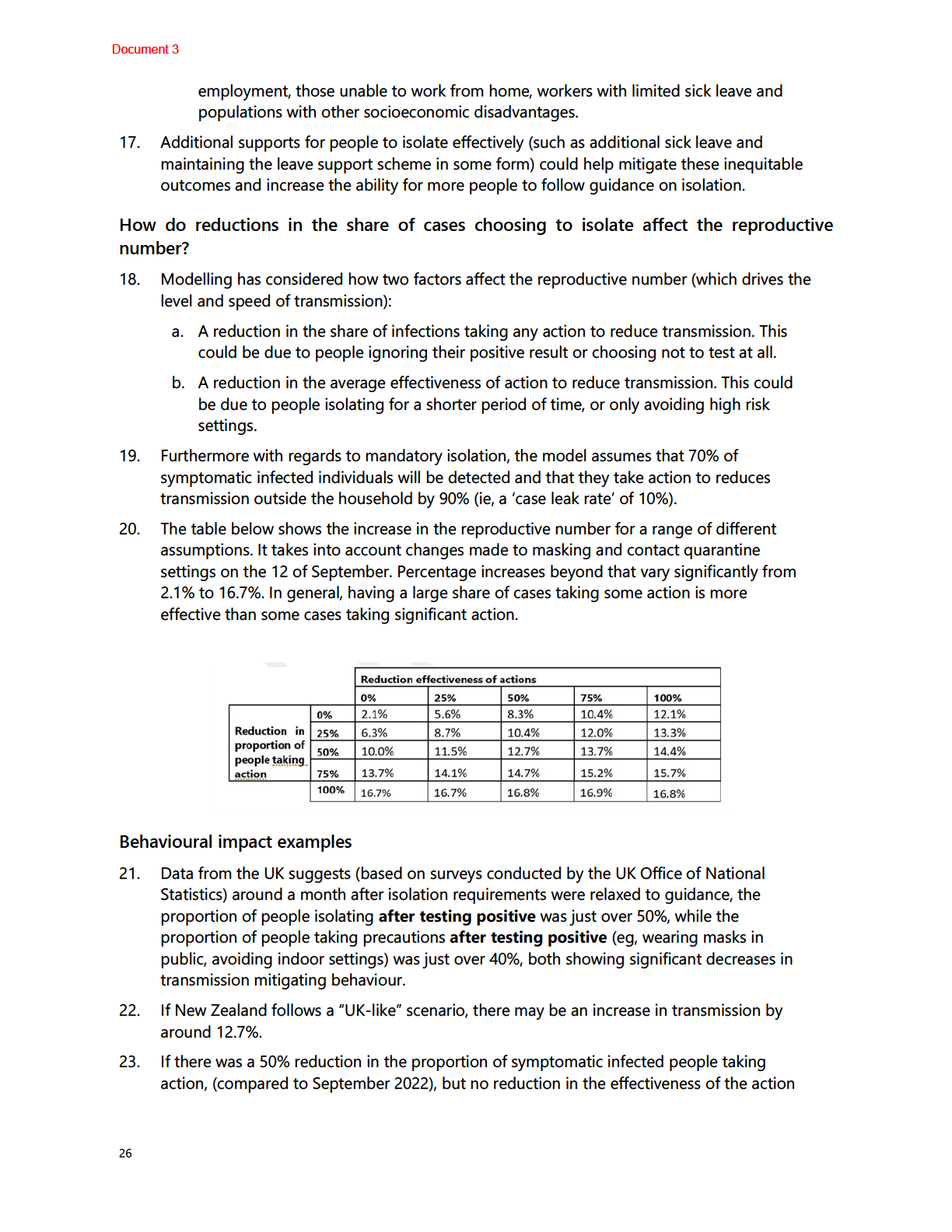
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 3
taken, then we estimate that the effective reproduction number would increase by 10%
(relative to the effective reproduction number in September 2022).
Scenarios considered
24. Model ing has considered adjustments to current mandatory isolation settings as well as
moving to guidance for isolation. For scenarios with mandatory isolation, two changes are
considered: reducing minimum isolation to 5-days with one negative test required before
release and a maximum of 7-days isolation; and reducing isolation to 5-days, with no test
to release. Previous modelling suggests that these scenarios would increase the
reproductive number by 1.4% and 4.2% respectively.
1982
25. Model ing has also considered scenarios where guidance is used for isolation. Because of
the significant uncertainty in how people respond to a removal of mandated case isolation,
ACT
modelling has considered three scenarios:
a. An optimistic scenario, with a 7.8% increase in the reproductive number.
b. A middle scenario, with a 11% increase in the reproductive number.
c. An upper limit scenario, with a 17.5% increase in the reproductive number. This is
slightly higher than the highest increase in the table above, due to small differences in
assumed symptomatic testing rates.
26. Finally, modelling has considered a scenario where no changes are made to case settings,
but guidance for household contacts is changed to testing every 48 hours if symptomatic.
INFORMATION
Compared to the status quo of testing daily for five days, this results in a 3.3% increase in
the reproductive number.
27. Factors that would shift New Zealand towards the optimistic scenario could include:
a. achieving high levels of testing in the community
b. maintaining strong norms that people should work from home if unwell
OFFICIAL
c. high voluntary adherence to mask and case isolation guidance
d. importance of clear communications and assistance (eg, leave support schemes) that
THE
would al ow people to both understand the importance of these, and be able to do
these
e. advice to employers to encourage work from home where possible for unwell people.
Modelling results UNDER
28. Policy changes that increase transmission will tend to have two effects:
a. In the short-term, a large increase in cases, hospitalisations and deaths. The absolute
size of this change will be driven by the level of immunity in the population. This
impact wanes over time as infection-induced immunity increases.
b. In the long-term, a slightly higher steady state level of cases, hospitalisations and
deaths.
RELEASED This impact is smaller in percentage terms but is persistent over time.
29. In general, the short-term peak in cases and hospitalisations can be mitigated by phasing
policy changes over a longer. This smooths out the peak and allows decision makers to
adjust their approach if the path of the outbreak differs from modelled projections.
27
Document 3
30. The table below shows the increase in cases, hospitalisations and deaths under these
scenarios. In the short-term, there is a large relative increase in cases, hospitalisations and
deaths. Relative increases are smaller over the long-term, but larger in absolute terms.
31. Compared to the table presented in the memo on isolation changes, short-term cases,
hospitalisations and deaths tend to be higher across all scenarios, including the baseline.
This partial y reflects the changes are being made on top of policy changes already made in
September. In addition, the policy change is occurring during a plateau in cases, compared
to the downward trend during September.
1982
s 9(2)(g)(i)
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
28
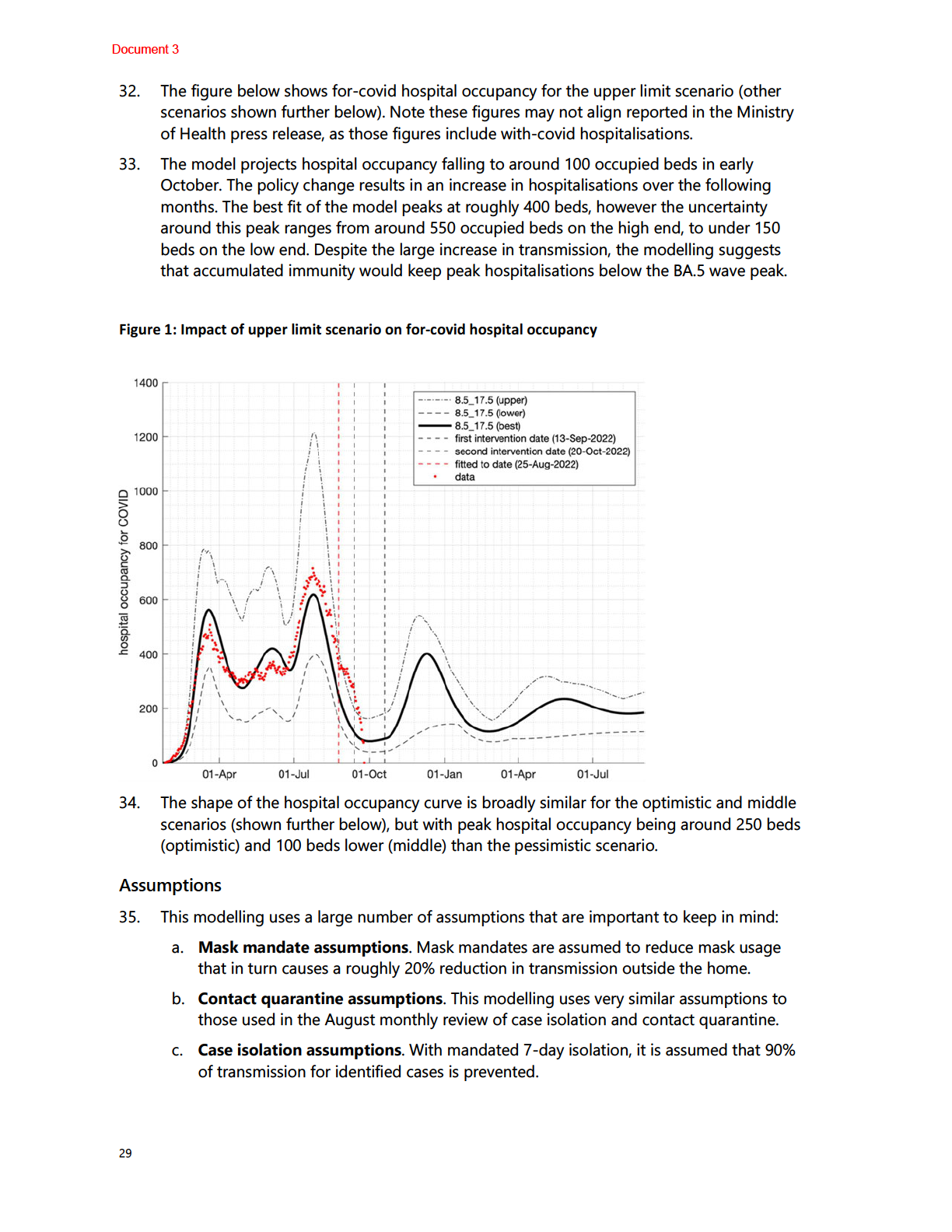
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
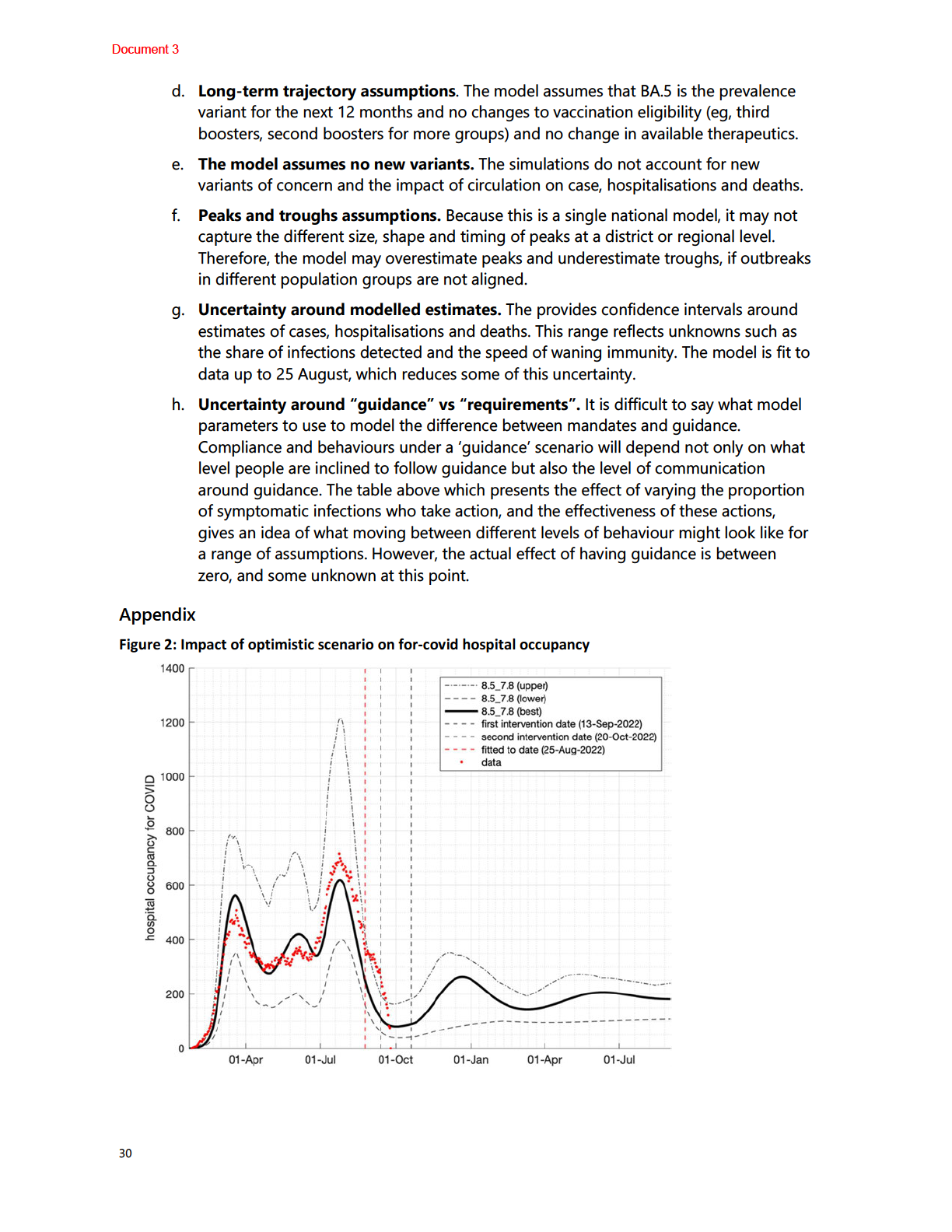
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
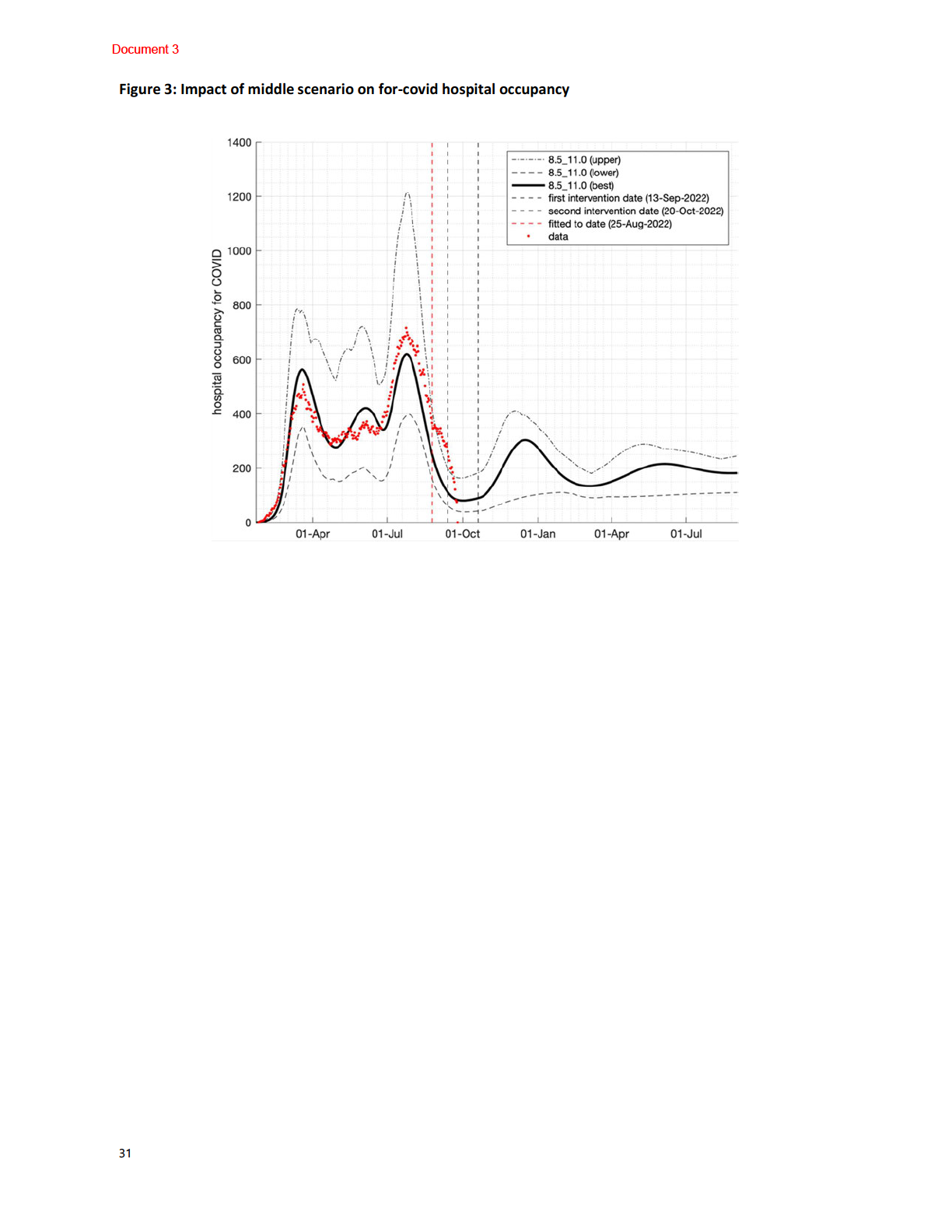
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
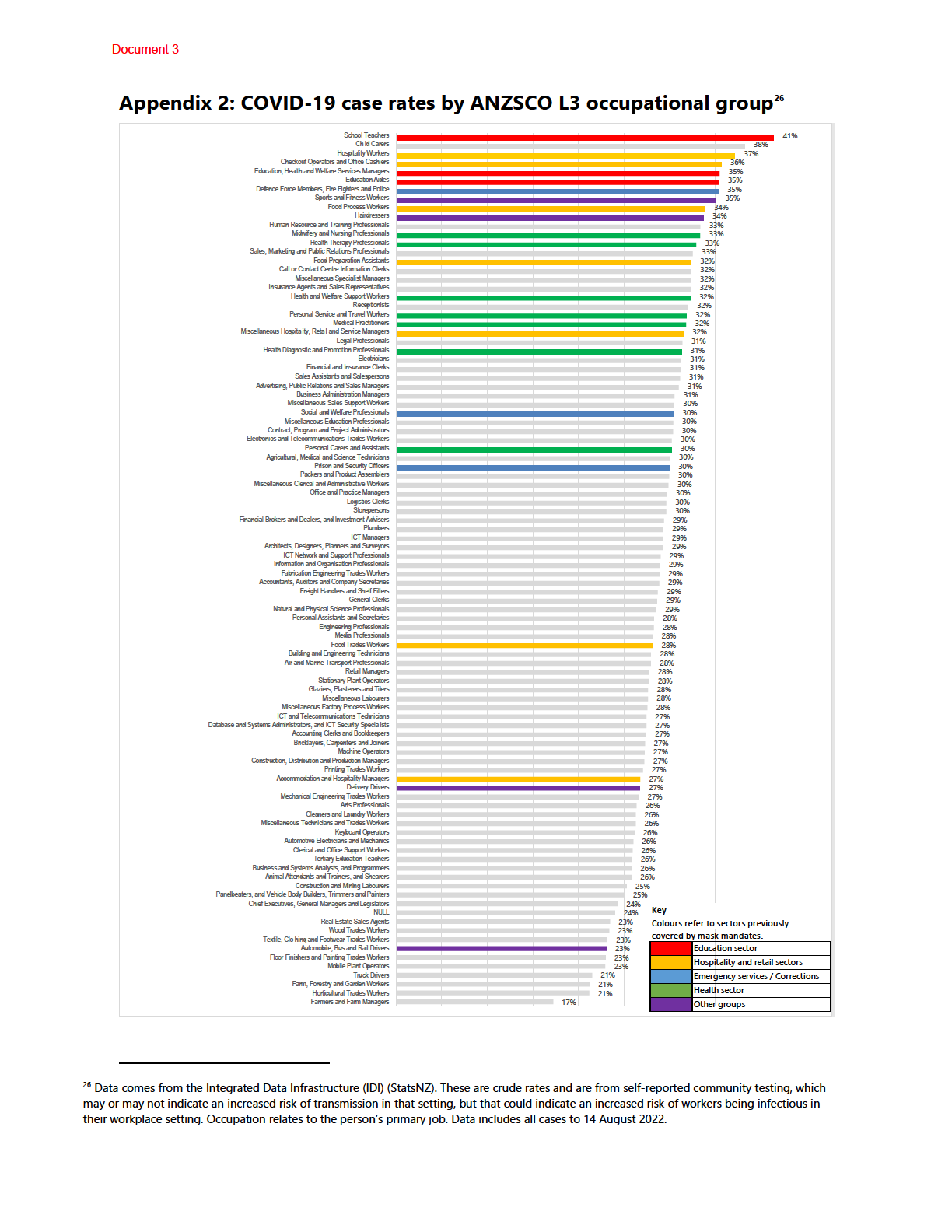
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 3
ENDS.
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED