

Lead Coordination Minister for the Government’s Response to the Royal Commission’s Report into the Terrorist Attack on the Christchurch Mosques
4 July 2022
Harold.
Email:
[FYI request #19134 email]
Ref:
ALOIA186
Dear Harold
Response to your request for official information
Thank you for your request for information under the Of icial Information Act 1982 (the Act)
to the Hon Andrew Lit le, Minister of Health on 19 April 2022, for a list of the following
documents:
“1) Aide Mémoire: Update on New Zealand's Critical and Intensive Care COVID-19
Preparedness [17/09/2021] 2) Aide Mémoire: Update on DHB COVID-19 Readiness [8/10/2021]
3) Briefing: Enhancing national ICU capacity [22/10/2021]
4) Memorandum: Deep Dive on care in community [10/11/2021]
5) Briefing: Care in Community - Cabinet Paper for SWS [11/11/2021]
6) Briefing: Cabinet Paper COVID-19 Care in the Community - health system
readiness and preparation [1/12/2021]
7) Aide Mémoire: Visit to Waikato District Health Board [16/12/2021]
8) Briefing: Follow up from SWC on Care in Community paper [16/12/2021]
9) Briefing: Talking points for Minister Little - Cabinet meeting on 25 January 2022-
COVID-19 Care in the Community [21/01/2022]
10) Briefing: Visit to NRHCC [1/02/2022]
11) Aide Mémoire: COVID-19 Hospital Readiness [11/02/2022]
12) Briefing: Proposal to resource additional critical care beds across Aotearoa New
Zealand [28/02/2022]
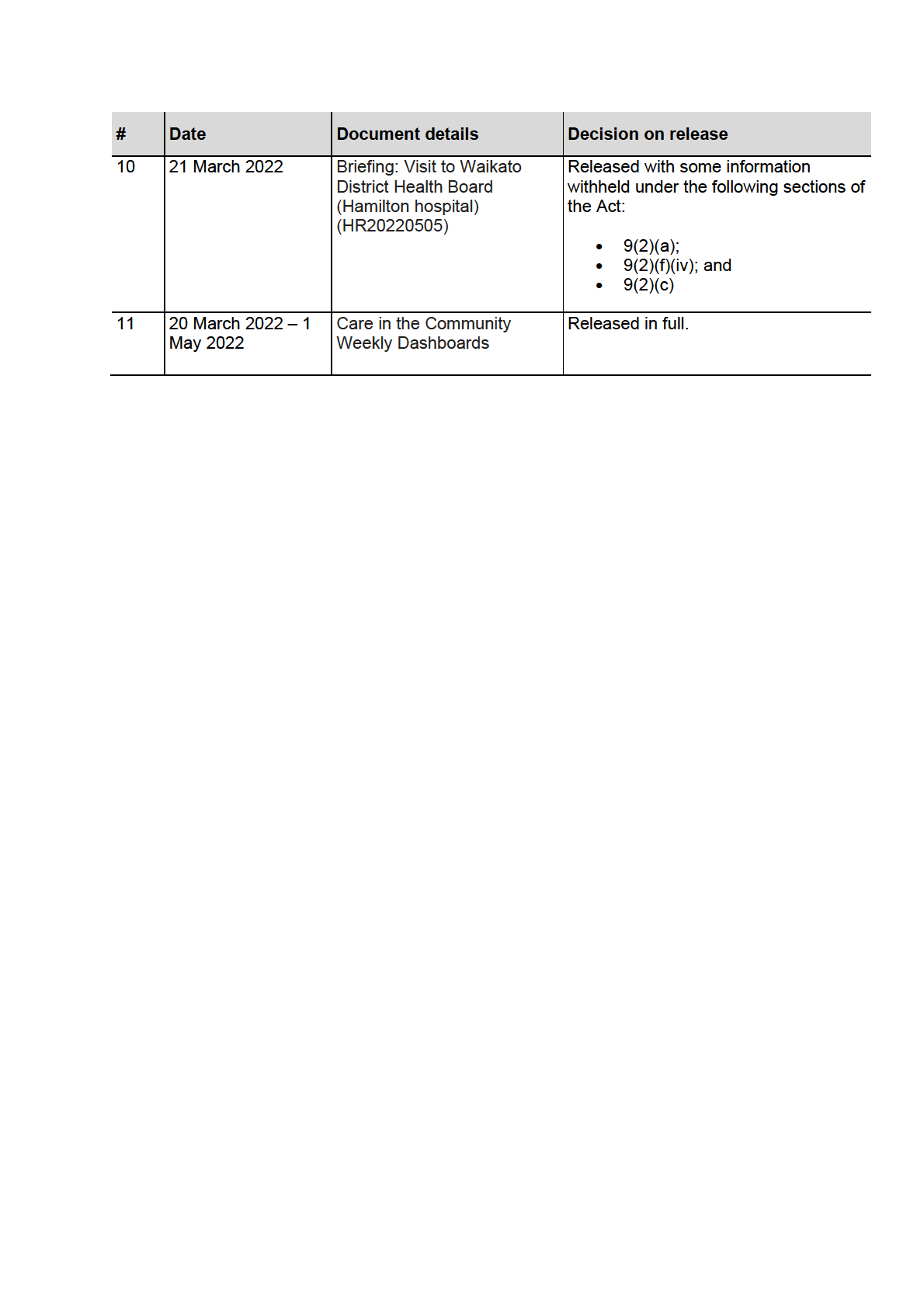
13) Briefing: Visit to Waikato District Health Board (Hamilton hospital) [21/03/2022]
14) And finally, I would like to request copies of all Care in the Community Weekly
Dashboards received by the minister since the beginning of March 2022.”
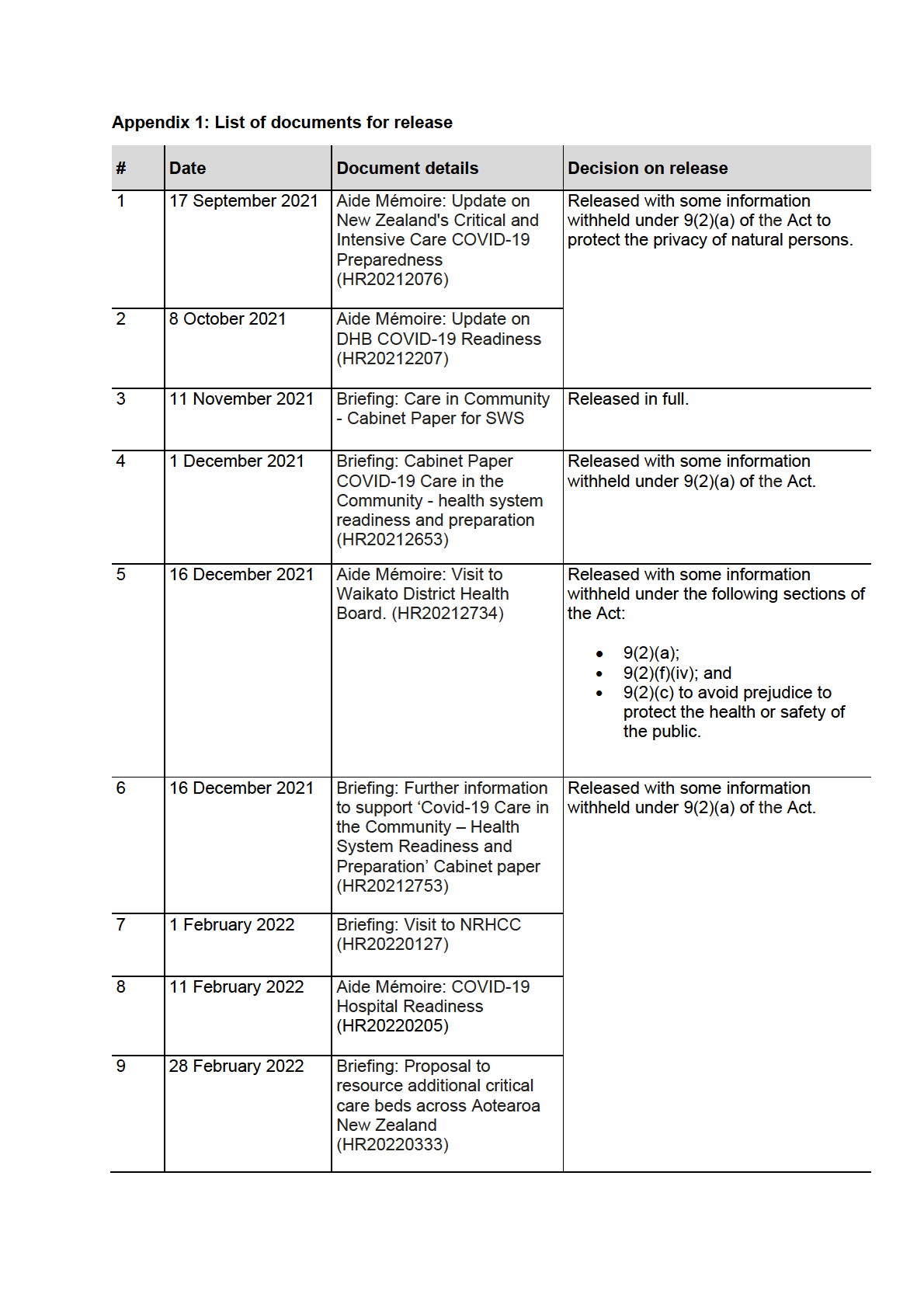
Copies of these briefings, aide-memoire and Care in the Community weekly dashboards are
being released to you as attached and are outlined in Appendix 1 of this letter. Please note,
where information is withheld under section 9 of the Act, I have considered the countervailing
public interest in release in making this decision and consider that it does not outweigh the
need to withhold at this time.
Note the briefing that you have requested titled: “
Enhancing national ICU capacity” was
cancelled, therefore I am refusing this document under section 18(e) of the Act, as the
information requested does not exist.
The document you have requested:
Briefing: Talking points for Minister Little - Cabinet meeting
on 25 January 2022- COVID-19 Care in the Community (HR20220068) is withheld in full under
section 9(2)(g)(i) of the Act, to maintain the effective conduct of public affairs through the free
and frank expression of opinions by or between or to Ministers and officers and employees of
any public service agency.
I was unable to locate the memorandum: “
Deep Dive on care in community” despite
reasonable efforts to locate this paper. As such, this document is refused under 18(e) of the
Act.
Under section 28(3) of the Act, you have the right to ask the Ombudsman to review any
decisions made under this request. The Ombudsman may be contacted by email at:
[email address] or by cal ing 0800 802 602.
Yours sincerely
Hon Andrew Little MP
Minister of Health

Document 1
Aide-Mémoire
Update on New Zealand’s Critical and Intensive Care COVID-19
Preparedness
Date due to MO: 17 September 2021
Action required by:
N/A
Security level:
IN-CONFIDENCE
Health Report number: 20212076
To:
Hon Andrew Little, Minister of Health
ACT 1982
Contact for telephone discussion
INFORMATION
Name
Position
Telephone
Robyn Shearer
Deputy Chief Executive, Sector Support
S9(2)(a)
and Infrastructure
Andrew Connolly
Chief Medical Officer
RELEASED UNDER THE OFFICIAL
Document 1
Update on New Zealand’s Critical and
Intensive Care COVID-19 Preparedness
Security level:
IN CONFIDENCE
Date:
17 September 2021
To:
Hon Andrew Little, Minister of Health
Purpose of the report
1.
This report provides an assessment of New Zealand’s current Intensive Care Unit (ICU)
and other critical care capacity and the ability to scale up capacity in response to a
potential surge in COVID-19 cases.
ACT 1982
2.
The report then outlines steps being taken to establish a baseline of ICU capacity and
capability to support New Zealand hospitals in confidently managing COVID-19 patients
alongside BAU on an ongoing basis.
3.
This includes an assessment of a recent report from Dr Craig Carr, a Dunedin ICU
Intensivist and President of the New Zealand division of the Australian and New Zealand
Intensive Care Society (ANZICS). His report considers ongoing requirement for ICU beds
once New Zealand is ‘opened up’ and promotes investing in portable or modular ICU
INFORMATION
facilities, co-located near hospitals, to enable DHBs to maintain BAU services.
Summary
4.
The New Zealand COVID-19 Alert Level Framework combined with the National Hospital
COVID-19 Escalation Framework has supported New Zealand to prioritise and manage
business as usual (BAU) work and COVID-19 patients at the individual DHB level and, to a
lesser extent, at the regional and national level.
5.
Work was completed in 2020 with DHBs on ICU planning for further COVID-19 surges
following the initial Alert Level Four lockdown period. However, we have gained a great
deal of new knowledge since then about COVID-19, including the new Delta strain and its
increased risks, and from our response measures to date.
6.
At the same time, planning is under way to determine what ICU capacity in necessary to
support BAU and expected COVID-19 and other respiratory hospitalisations once New
Zealand has a sustained high vaccination rate and moves away from level four lockdowns
as its most effective tool for eliminating COVID-19 outbreaks.
7.
In this context, the Ministry has commissioned new
RELEASED UNDER THE OFFICIAL modelling to assist with strengthened
critical care planning going forward.
8.
A paper provided by Dr Craig Carr, includes suggested options for mobile, temporary
COVID-19 dedicated critical care facilities. These options will be considered further in the
context of the new modelling to be provided.
Current context
9.
August 2021 modelling by the joint DHB and Health Infrastructure Unit’s Critical Care
Aide-Mémoire: 20212076
2
Document 1
Service Planning Project confirms New Zealand DHBs have a baseline of 243 fully
resourced ICU capable beds in normal conditions.
10.
Current daily SITREPs have DHBs self-reporting 320 available ICU capable beds. To
achieve this increase, DHBs will be planning on using both fully trained and surge
trained staff and reducing planned care activity.
11.
As part of preparedness planning requirements, in mid-2020, DHBs identified that they
could expand spaces and operate up to 553 ventilated ICU beds once sufficient surge
staff were trained and non-acute hospital activity was minimised.
12.
DHBs also identified that operating at that level for an extended period would put
significant stress on staff and resources as they would also be managing large numbers of
COVID-19 patients in respiratory units and medical wards.
13.
The Delta strain means that New Zealand must stay highly prepared for a COVID-19
resurgence to avoid placing significant pressure on health services until current best
ACT 1982
practice infection control measures are supported by high vaccination coverage.
14.
In addition, demands on the current workforce from Managed Isolation and Quarantine
(MIQ), swabbing, vaccinating, staff self-isolation, and general stress have materially
increased pressure on the health system’s capability to sustain BAU and COVID-19
management in 2021.
15.
While the current Auckland outbreak has overall been handled well by the DHBs, we have
learned that more oversight is needed on DHB workforce preparedness, a
INFORMATION vailability, and
mobility, to provide assurance that sufficient ICU beds can be operated in a sustainable
manner when and where needed under current conditions and going forward.
16.
A range of independent experts have undertaken and released modelling on the number
of hospital and ICU beds needed in New Zealand going forward. This is typically based on
recent Australian information.
17.
The variance in their forecasts around hospitalisations and ICU utilisation largely reflects
assumptions about vaccination rates and infection control measures.
18.
The Ministry has commissioned new COVID-19 modelling to identify ICU and other
hospital and wider health system capacity necessary to manage any late 2021 surge event
and to prepare for ongoing operation of the health system in a more open environment.
Review of Current ICU Capacity Including Workforce
ICU Physical Capacity 2020
19.
There is no national database of ICUs, High Dependency Units (HDUs), or critical care
units (CCUs) across New Zealand.
RELEASED UNDER THE OFFICIAL
20.
At the time of the 2020 COVID-19 outbreak, the Ministry was able to use data in the
recently completed National Asset Management Plan to provide initial numbers,
supplemented by data requests and information collated by ANZICS.
21.
COVID-19 modelling at the time provided guidance on the expected maximum demand
for ICU and HDU at a time when there was no vaccination available and the effectiveness
of community control measures not well established
22.
At the end of April 2020, DHBs reported they had 358 ICU capable beds available and
Aide-Mémoire: 20212076
3
Document 1
had agreed to continue training staff and preparing spaces to be able to surge up to 553
ICU beds if necessary.
23.
The Ministry also directly purchased more ventilators, hi-flow nasal oxygen equipment,
ICU supplies and started upgrading oxygen infrastructure as part of overall
preparedness.
ICU Staffing Capability
24.
A key ICU challenge is demand for nurses within ICU and HDU settings, given the ratio
of specialist nurses to patients (1:1 and 1:2) respectively.
25.
DHBs identified nurses with prior ICU experience and other nurses who could be tra ned
to support a surge response. This includes Post Anaesthetic Care Unit (PACU) nurses,
theatre nurses, surgical and medical ward nurses, emergency department nurses and
anaesthetic technicians.
26.
In addition to identifying and training additional nursing staff, DHBs also planned for
ACT 1982
team-based models of care with one ICU nurse overseeing a pod of non-ICU nurses and
allied health professionals with ratios of experienced ICU nurse to patient varying
between 1:2 and 1:5.
27.
DHBs also proposed asking part time staff to work full time and change from 3 x 8 hour
shifts to 2 x 12 hour. The DHBs noted this could only be sustainable for a short period of
time (around two weeks) as staff would become fatigued.
28.
INFORMATION
Changes to ICU and HDU staffing models comes with recognised mortality risks due to
patients needing close 1:1 monitoring, especially when coming off ventilation.
29.
To support the proposed approach to increase ICU staffing capacity, the Ministry
allocated $2 million of COVID-19 workforce funding to boost DHBs’ ICU surge capacity
by reimbursing DHBs for the costs of releasing staff for training and for the costs
incurred by smaller DHBs when sending staff to larger DHBs for training.
30.
To date, funding has been approved to train 1,220 people across New Zealand. DHBs
have proposed to use this funding to undertake initial ICU surge training to increase the
number of staff that can be utilised to boost ICU surge capacity and for refresher
training for staff who have participated in the initial ICU surge training.
31.
This funding has also been used to develop an e-learning programme. The NZ Critical
Care Pandemic Relief Team Resource e-learning package component is designed for
DHBs to undertake refresher training with those who have participated in the initial ICU
surge training. The e-learning package was finalised and made available to all DHBs on
26 August 2021.
32.
The availability of other medical staff is not conside
RELEASED UNDER THE OFFICIAL red as critical as nurses, as ICU
specialists are able to be supported by anaesthetists and other medical staff who have
relevant experience in theatres and CCUs.
33.
In June 2021, DHBs reported they had 1,417 nurses fully trained to work in ICU and
another 713 non-ICU nurses had received training in preparation for a surge in demand.
34.
Additional focus is now being placed on increasing the ICU and HDU resilience of the
large Auckland Metro DHBs as they are the centre of COVID-19 management, and
scarce staff are being called upon to cover multiple roles.
Aide-Mémoire: 20212076
4
Document 1
ICU Capability Going Forward
35.
The various ICU planning projects operating across the Ministry were brought together
in late 2020 into the joint DHB and Health Infrastructure Unit’s Critical Care Service
Planning Project.
36.
A national critical care service plan will inform future infrastructure requirements over
the next 10-15 years. The plan will describe the delivery framework for critical care
services and provide a forecast of bed capacity required.
37.
As modelling for COVID-19 is progressed, this will be incorporated into the service plan.
38.
Importantly, this work has validated that DHBs have a baseline of only 243 fully
resourced ICU capable beds.
39.
Current daily SITREPs have DHBs self-reporting 320 available ICU capable beds across
ICU and HDU, reflecting their plans to use both fully trained and surge trained staff and
reducing planned care activity.
ACT 1982
40.
Based on the three Auckland metro DHBs’ reported capacity of 131 ICU/HDU beds and
around 60% utilisation, their August 2021 request for out of region ICU staffing support
needs to be better understood in relation to their SITREP reporting.
41.
The Ministry is working with the DHBs to ensure the daily reporting accurately reflects
ICU and HDU beds that could be used for COVID-19 and excludes neonatal and
paediatric intensive care beds.
INFORMATION
42.
The current Auckland outbreak has shown that more oversight and assurance is needed
on DHB workforce preparedness, availability, and mobility, to provide assurance that
sufficient ICU beds can be operated in a sustainable manner when and where needed
under current conditions and going forward.
43.
The Ministry is moving to ensure there is central visibility on the number of nurses now
being actively trained and how they are being deployed through ICUs to get hands on
experience to ensure that the numbers align with stated ICU capacity.
44.
The Ministry has commissioned new COVID-19 modelling to take account of the new
Delta variant context, up to date knowledge of the effectiveness of vaccination and
lockdown measures and other lessons learned from New Zealand’s COVID-19 response
to date.
45.
This will assist in identifying ICU and other hospital and wider health system capacity
necessary to manage any late 2021 surge event and to prepare for ongoing operation of
the health system in a more open environment.
46.
This will include a review of the existing 553 ICU bed capacity forecast.
RELEASED UNDER THE OFFICIAL
Review of Dr Carr’s COVID-19 ICU Model, and Future Modelling
47.
Dr Craig Carr has proposed commissioning external modular ICU capacity alongside
hospitals that could be relocated as necessary and disposed of if no longer needed. He
considers this would allow hospitals to then focus existing capacity on BAU
requirements going forward.
48.
His model presents a scenario where 90% of the population is fully vaccinated.
Aide-Mémoire: 20212076
5
Document 1
49.
The model shows that 160 additional ICU beds are required if current public health
measures were maintained to manage outbreaks and keep the prevalence of COVID-19
in the population at no more than 2 percent.
50.
Significant additional ICU capacity would be required if no additional public health
measures were put in place
51.
The findings are consistent with another model recently presented to the Ministry by
ICU specialists.
52.
As can be seen from the current Delta outbreak, our hospitals are able to cope with a
limited number of COVID-19 ICU hospitalisations, even when public health measures
and adjusted alert levels are in place reducing overall hospital activity.
53.
An outbreak in other regions, or multiple regions, would put additional strain on New
Zealand’s critical care system.
54.
The Ministry is working with Te Pūnaha Matatini (TPM) to develop modelling that
ACT 1982
considers applicable measures and likely effects on ICU and hospital capacity to address
reopening of borders.
55.
Initial work and outputs from this modelling will be complete in time for inclusion in
reports due to Ministers in October 2021.
Expansion of ICU Capacity within Hospital or as external Module
INFORMATION
56.
In the longer term, with a growing and aging population, New Zealand will need to
increase in ICU and HDU capacity in a planned manner.
57.
COVID-19 has heightened the focus on the optimal or essential level of ICU capacity
needed by New Zealand, noting its expense and resource requirements.
58.
To date, New Zealand has focused on increasing ICU capacity within existing hospitals,
or through streaming services between COVID-19 designated acute hospitals and
COVID-19-free planned care hospitals (potentially using private capacity for this
purpose).
59.
The Ministry considers external temporary facilities, as proposed by Dr Carr, should
generally be undertaken as a final response, due to them needing to be integrated into
a range of health services to support COVID-19 patients. There are also additional
infrastructure complexities that would need to be addressed as part of any modular set
up separate from existing hospital sites, for example ensuring reliable electricity and
oxygen supplies.
60.
The Ministry will provide further advice on these options, including a more detailed
breakdown of the relative risk and benefits of the
RELEASED UNDER THE OFFICIAL available infrastructure options, in
October 2021.
Next Steps
61.
The Ministry is actively working on a comprehensive work programme to ensure the
health system can support New Zealanders to actively participate in the community and
move more freely once high vaccination rates are achieved.
62.
The programme will also consider what improvements, if any, need to be made to the
Aide-Mémoire: 20212076
6

Document 1
health system to ensure any future COVID-19 surges can be successfully managed with
acceptable health outcomes, accounting for the current knowledge of the Delta variant
and other lessons learned from our COVID-19 response to date.
63.
Modelling is critical to these preparations, as is central planning, oversight, and
deployment of staff.
64.
While staff capability and leadership are critical determinants, the Ministry is continuing
to review all ICU and HDU requirements to ensure key centres like Auckland are well
prepared.
65.
The Ministry will provide a further briefing to you in October 2021 with more detailed
analysis of critical care needs in the current context and in a scenario of reduction in the
current public health measures as New Zealand looks to re-open to the rest of the
world.
ACT 1982
Robyn Shearer
Deputy Chief Executive
Sector Support and Infrastructure
INFORMATION
Date: 17 September 2021
RELEASED UNDER THE OFFICIAL
Aide-Mémoire: 20212076
7

Document 2
Aide-Mémoire
Update on DHB COVID-19 Readiness
Date due to MO: 8 October 2021
Action required by:
N/A
Security level:
IN CONFIDENCE
Health Report number: 20212207
To:
Hon Andrew Little, Minister of Health
ACT 1982
Contact for telephone discussion
Name
Position
Telephone
Martin Chadwick
Chief Allied Health Professions Officer
S9(2)(a)
INFORMATION
Jess Smaling
Associate Deputy Director-General, DHB
Performance and Support
RELEASED UNDER THE OFFICIAL








Document 2
Update on DHB COVID-19 Readiness
Security level:
IN CONFIDENCE
Date:
8 October 2021
To:
Hon Andrew Little, Minister of Health
Purpose of the report
1.
This report provides assurance of the work already undertaken and advice on next steps for
district health boards (DHBs) to respond to any immediate resurgence and wider system
resilience for when borders are relaxed.
Summary of DHB readiness plans
ACT 1982
2.
DHB readiness planning is a critical workstream in the overall Health System Readiness
programme of work. The work in this area is longstanding, with DHB-led planning activity
having been fast-tracked as part of the initial COVID-19 work in 2020.
3.
DHB plans have been integrated over time based on local testing, and as we have collectively
learned more about the management of COVID-19 in our communities and hospitals.
4.
All DHBs have pandemic preparedness and resurgence plans to guide responses to
community outbreaks and differing alert levels.
INFORMATION
5.
These plans sit alongside national frameworks that provide high level, nationally consistent
guidance to support hospitals, facilities, and community providers to maintain as much service
delivery as safely possible, during any COVID-19 resurgence.
6.
Often when DHB planning is referred to, there is an assumption that this is primarily focused
on our hospital and critical care settings. It is important to note that in our health system, our
DHBs lead, commission and coordinate services across the health care continuum, from public
health, through primary and community settings, and into specialist hospital care. DHB plans
recognise this wider context.
7.
While the approach h s differed across districts depending on local service configurations and
pressures, broadly plans have covered:
Emergency coordination
Psychosocial coordination
Clinical service delivery, including critical care
Infection, prevention, and control
RELEASED UNDER THE OFFICIAL
Managed isolation and quarantine facilities
Testing
Equipment and clinical supplies.
Primary and community care.
8.
Within the primary and community care remit, plans include pharmacy, community residential
care and aged care services, disability and home-based support services, NGOs, Māori and
Pacific community providers, district nursing, community midwifery and allied health.
Aide-Mémoire: 20212207
1

Document 2
9.
Since the latest COVID-19 Delta variant outbreak, the DHB Chief Operating Officers (COOs)
have established a working group to support rapid and practical review of policy development,
advice and actively ensure hospital readiness.
10. The first priority of this group has been to develop a gap analysis of resurgence plans at a
local level for both the community and hospital settings. This rapid review has identified gaps
that DHBs have now been asked to validate to provide revised plans.
11. The key themes reported by the DHBs show:
• All DHBs have articulated plans for ICU and Emergency Departments processes and
service expansion in response to increased alert levels and demand.
• All DHBs have plans to screen and stream patients based on risk factors.
• Almost all DHBs articulated the intent for prioritisation/reprioritisation of surgery, planned
care and outpatient services.
• Planning around services to vulnerable people such as maternity, paediatrics, cancer care,
mental health and assessment treatment and rehabilitation were not universally covered
ACT 1982 .
• Implications for tertiary services such as neurosurgery, cardiac surgery, major trauma,
burns, and spinal services need to be made more visible at a national level.
12. The approach has differed across districts depending on local service configuration and
pressures.
13. The lessons learned from the current outbreak are informing iterations of the plans, including
how local, regional, and national responses are implemented.
INFORMATION
Northern Region Resilience Plan
14. As a result of the recent Delta outbreak and the impact this has had on the Northern Region,
and in particular, the three Auckland DHBs, the Northern Region DHBs are rapidly developing
a Northern Region Resilience Plan.
15. This plan covers sixteen functional areas, from regional provider groups to community care
and public health, supporting the services behind that and all aspects with an equity lens.
Each function will be considered resilient if it has the capacity and capability to support
sustainable responses recurring community resurgences of COVID-19, without limiting the
ability to provide effective non-COVID related health care services
Image 1: Functional areas of Northern Region Resilience Plan
RELEASED UNDER THE OFFICIAL
Aide-Mémoire: 20212207
2

Document 2
16. The plan was presented to the National DHB Chief Executives at their meeting on 6 October
2021 and it was endorsed with agreement that their plan will be used as a template for the Te
Manawa Taki, Central and Southern regions.
Next steps
17. Further work is underway to ensure consistency across DHB’s local planning, and to make sure
any interdependencies in terms of resources, capacity and workforce are acknowledged and
appropriately planned for.
18. The template utilised by the Northern Region provides a platform for an all-region response.
The COOs working group are working closely with the Ministry of Health Emergency
Management group to support and enable a process to rapidly validate existing gaps and
develop and test the plans where the gaps are identified.
19. There is also a need for national work to get a consistent view on prioritisation of health
services should trade-offs need to be made between usual service delivery and management
of COVID-19 patients.
ACT 1982
20. The Ministry will provide you with regular updates on the wider Health System Readiness
programme progress.
INFORMATION
Martin Chadwick
Chief Allied Health Professions Officer
Office of the Chief Clinical Officers
RELEASED UNDER THE OFFICIAL
Aide-Mémoire: 20212207
3
Document 3
In Confidence
Office of the Minister of Health and Office of the Minister for COVID-19 Response
Cabinet Social Wellbeing Committee
COVID-19 Care in the Community
Proposal
1
This paper outlines the evolving model of care for COVID-19 patients in the
community, also referred to as ‘COVID-19 care in the community’ and
explains next steps for scaling up the system.
2
This paper is designed to be read in conjunction with other papers prepared
by the Ministry of Health and Ministry of Social Development that are on the
ACT 1982
Social Wellbeing Committee agenda on 17 November:
• COVID-19 Minimisation and Protection approach – changes to testing,
case investigation and contact tracing (Minister for COVID-19 Response;
Associate Minister of Health).
• COVID-19: A whole of system welfare approach under the COVID
Protection Framework (Minister for Social Development and
INFORMATION
Employment).
Relation to government priorities
3
This paper supports the ongoing response to COVID-19 by setting out the
current state and next steps for caring for COVID-19 patients in the
community.
Executive Summary
4
This paper outlines the current state of the ‘COVID-19 Care in the Community’
operating framework, and highlights areas of development that are being
rapidly scaled up and iteratively worked through to support the increasing
number of cases.
5
New Zealand is now entering the next phase as we near a 90 percent
vaccination rate across the country and we shift our Elimination Strategy to a
minimisation and protection approach with the new COVID-19 Protection
Framework [CAB-21-MIN-0421].
RELEASED UNDER THE OFFICIAL
6
Under the new approach – and with increasing vaccination rates – many
systems and processes which were designed with the goal of stamping out
COVID-19 must now be adjusted to reflect the new goals of minimising the
spread of COVID-19 in the community and protecting those most vulnerable
to the disease.
7
This model will turn the patient experience on its head, from the moment they
test positive with COVID-19. Where previously the initial response was a
1
I N C O N F I D E N C E
Document 3
public health one, focused on containment as the immediate priority, we now
can make the response tailored to the individual’s needs, starting with good
clinical assessment, coupled with public health and welfare assessments. The
Auckland region has already started to turn this model around; other regions
will gradually do so, while maintaining a strong public health response to
contain new cases quickly and efficiently.
8
Our model allows for home isolation of positive cases and contacts and is
called the ‘COVID-19 care in the community’ model, as an alternative to
managed isolation and quarantine (MIQ) for many people, with MIQ and other
accommodation options remaining available for those who need them.
9
The COVID-19 care in the community model will operate as a high-trust
framework that is centrally supported, regionally delivered, and locally led.
The first iteration of the framework was provided to the health sector on 3
ACT 1982
November 2021, and will be regularly updated based on feedback.
10
Central to this approach will be ensuring clinical health, public health, and
welfare needs of a positive case, their whānau, household, and the wider
community are better identified, and that necessary support is connected and
coordinated. The model will help ensure the welfare of a positive case and
others within the household, whilst limiting impacts on the wider health system
and the workforce, and MIQ system capacity.
INFORMATION
11
Ensuring that the model is addressing the needs of individuals and whānau in
an equitable way is critical to its success, particularly given that the current
outbreak is disproportionately affecting Māori and Pacific populations.
12
There will be significant financial investment needed to enable community
health care providers to support COVID-19 patients as case numbers
increase.
13
A more detailed update of the model, with updated financial implications and
metrics for analysis, will be provided to Cabinet early in December 2021.
Background
14
In the New Zealand health system, both before and during the COVID-19
pandemic, most people are cared for at home when they are unwell, with
support from primary, secondary, and tertiary health care as needed.
15
As New Zealand nears 90 percent vaccination rate across the country, our
RELEASED UNDER THE OFFICIAL
Elimination Strategy is shifting to a minimisation and protection approach.
This will see us replacing the Alert Level Framework with the new COVID-19
Protection Framework (CPF) [CAB-21-MIN-0421].
16
The adoption of the CPF framework recognises that our approach to providing
COVID-19 care in the community is changing. Under an Elimination Strategy,
our goal was to eliminate transmission of COVID-19 within the community and
MIQ was a key tool for achieving this. The transition to the CPF framework will
2
I N C O N F I D E N C E
Document 3
see a shift to using self-isolation and quarantine options both in the
community and at the border.
17
This approach acknowledges that we are moving to a setting where, with a
highly vaccinated population and the appropriate set of measures to protect
vulnerable communities, identifying and isolating every case of COVID-19 in
MIQ is not the best use of public health resource.
18
This does not mean that MIQ will not remain a part of the COVID-19 response
toolbox. MIQ will remain necessary where managed care is appropriate, for
example for those who cannot safely isolate at home but do not need hospital
level care, but it will be used proportionately and as required rather than as
the default. Further, the Minister for COVID-19 Response will bring forward a
separate paper to Cabinet on 13 December 2021 concerning the future of
MIQ. This paper will seek agreement to a business case for longer term
ACT 1982
investment in infrastructure and a workforce for MIQ.
19
The option of home isolation will also support our overall strategic direction of
managing expected future COVID-19 waves and allowing us to move more
freely domestically and open internationally without the impact on our health
system becoming unmanageable.
20
Other critical pieces and complementary work includes the MSD-led welfare
INFORMATION
approach and the Housing and Urban Development (HUD) work in alternative
accommodation solutions, which address key components of the COVID-19
care in the community model.
Turning the model on its head
21
Our model for caring for COVID-19 patients in the community must have
elements that are nationally consistent, namely the notification, assessment,
monitoring, and escalation pathways, with variation in the approach to meet
individual needs including any welfare support.
22
At its core, caring for patients at home under this model is necessarily a high
trust model, based on the principles of centrally guided, regionally coordinated,
locally led, to efficiently allocate health resource and enable people to be cared
for in the context of their community. This model does not replace hospital care
where needed but is about providing the right care at the right place at the right
time.
23
Using trusted points of contact, as far as is possible, is also vitally important
RELEASED UNDER THE OFFICIAL
that everywhere around New Zealand, people understand the support available
to them and what is required of them if they test positive. Acknowledging the
need for trusted contact points, the rules and process need to be simple to
understand and navigate for diverse providers and populations across New
Zealand. They need to be supported by their health and social services, but
also by the wider community to do the right thing, and families, friends, and
employers all need to continue our collective efforts.
3
I N C O N F I D E N C E
Document 3
24
Work is underway with the Department of Prime Minister and Cabinet to
develop channels and messages for the public.
First point of contact and assessment of needs following a notification of a positive
COVID-19 case.
25
The priority principle where a positive case is identified is that their initial point
of contact is often the most critical. This initial contact must be delivered if
possible by a known, trusted or connected clinician (such as a general
practitioner) or other community provider who best understands the needs of
the individual and their whānau, and aid in communicating all the relevant
information needed at this key part of the process.
26
The last 20 months have focused on outbreak control response, so first
contact has until recently rightly been through the public health unit (PHU) to
ACT 1982
get into contact tracing and providing initial support. Critical to this is the
assessment of the public health status (contacts, household contacts),
followed by the assessment of the patient’s clinical status (signs and
symptoms), emergent welfare and social needs, within the first 24 hours.
Information is also collected for household contacts and any other close
contacts that may require testing and subsequent support [Table A refers].
Given the highly vaccinated population and an enduring presence of COVID-
19, the focus is now on the individual clinical assessment, followe
INFORMATION d by the
welfare and public health needs to identify those who need urgent clinical
support.
27
The key elements for addressing the needs of a COVID-19 positive patient
will need to cover:
I. A positive COVID-19 test is returned.
II. The laboratory result will be notified to the relevant PHU and regional
coordination hub, and the person’s GP or another primary care provider
(for unenrolled people) and potentially other service providers, e.g. Māori
and Pacific providers.
III. The person will be assessed by their GP or other health professional for
their suitability to recover at home, and notify them to expect a call from
public health for a public health assessment.
IV. The practitioner carrying out the assessment will notify the appropriate
RELEASED UNDER THE OFFICIAL
hub to arrange home care or other support, referral to MIQ or admission
to hospital where applicable.
28
It will be critical that the person doing the initial assessment has access to all
relevant information and is able to view linked data from general practice and
other providers to ensure the assessment takes account of the patient’s
holistic needs.
4
I N C O N F I D E N C E
Document 3
Evolving model of care of COVID-19 cases under the CPF will see a greater
emphasis being put on an initial clinical assessment.
29
As the focus moves away to protection under the CPF, the care in the
community model will evolve to prioritise the initial clinical and holistic
assessment.
30
Additionally, as cases requiring home isolation increase, it will be important to
reserve our limited public health resource for health-related critical functions
such as confirmation of positive cases. It is expected that providers, such as
primary care, could conduct the initial needs assessment. This will require
assurance that key assessment components are robust, regardless of who is
undertaking assessment.
31
The Ministry is working with Māori and Pacific health providers to ensure
ACT 1982
assessments consider cultural needs and nuances at this important stage,
and throughout the home isolation process.
32
The information collected during this assessment will be provided to the
patient’s preferred and trusted primary care provider where one is available.
Table A: Personal/clinical assessment
Initial clinical
Public health
Clinical risk
Suppor
INFORMATION t and
assessment of
assessment
assessment for
cultural needs
COVID-19 signs
COVID-19
assessment
and symptoms
complications and
management
Initial assessment of As per usual
Health history and
Suitability of
current or emerging
processes for public
current medical
accommodation,
need for clinical
health requirements
needs
safety, security, and
support as per usual and statutory
essential needs,
processes for public
responsibilities
whānau needs
health requirements
and statutory
responsibilities
Secure and stabilise
Identify primary and community care needs
and relationships
Determination of suitability of place
Care coordination for whānau
Set-up activities including essential supplies and technology
RELEASED UNDER THE OFFICIAL
Timely and coordinated processes will ensure that appropriate care is provided to
the individual and their household.
33
The assessment will consider clinical and holistic risk in terms of COVID-19
symptoms and any other complications. Patients and their household are
referred to a care setting (eg home, community facility, MIQ, or hospital)
depending on the holistic level of need, including any welfare safety
considerations, and risk of complications [Table B refers]. Consistency in this
5
I N C O N F I D E N C E
Document 3
is necessary so that people in all parts of the country understand what is
required of them.
34
To appropriately triage patients and households, coordination at a local and
regional level is needed. For example, while a patient may not be safe to
disclose that they are experiencing family violence and are therefore not safe
to isolate at home, risks of this type may be identified through information
sharing between providers including local Integrated Safety Response
approaches.
35
Regional and local coordinators will work with the patient’s preferred or
regular primary care provider, where there is one and the provider accepts the
responsibility of COVID-19 care for the patient. If this is not possible, the
coordinator will work to find an alternative primary care provider. At any time
in the process, it is possible for an individual’s or household’s care setting to
ACT 1982
be escalated – for example, where it becomes clear that a patient is not able
to isolate safely at home due to concerns for their health or the health of those
isolating in the household with them. Guidelines will be provided to support
clinicians and other community providers engaging so that they can better
determine it is no longer appropriate for the positive case to be cared for in
the community.
Table B: Levels of care needed and appropriate care setting
INFORMATION
Level One
Level Two
Level Three
Clinical
Asymptomatic or
Moderate symptoms Severe symptoms
assessment
mild symptoms
requiring acute or
palliative care
Risk of
Low risk (e.g., fit,
At risk of
-
complications
young and healthy)
complications
Feasible care
Home Quarantine
Home Quarantine
Hospital or Palliative
Setting
care
COVID-19 care in the Community model
The COVID-19 Care in the Community model will provide support to COVID-19
cases and close contacts to isolate at home.
36
Isolation at home is a well-established part of the health system and an
integral part of the evolving COVID-19 response.
37
The COVID-19 care in the community model
RELEASED UNDER THE OFFICIAL sits within the wider Health
System Preparedness Programme (HSPP) that is underway to ensure the
health system is well prepared to manage an enduring presence of COVID-19
in the community.
38
International evidence and the experience in Auckland and Waikato have
shown that whilst community cases will require management and monitoring
of symptoms, most will not require admission to hospital. The clinical
community is currently looking to experiences from Canada and Australia
which indicate that a primary and community care-led response can reduce
6
I N C O N F I D E N C E
Document 3
pressure on hospital services, when supported with adequate clinical
guidance, patient information system connections, equipment, and workforce.
These lessons are being incorporated into the model outlined in this paper.
39
On 3 November, the Ministry released the first iteration of COVID-19 Care in
the Community Operating Guidelines that looks to provide central support on
the establishment of regionally delivered and locally led systems which
provide both clinical and welfare and wellbeing support to people in the
community.
40
Any COVID-19 positive patients and contacts whose needs are best met in an
MIQ facility will continue to be transferred there, wherever possible. This is
also the case in the event of an individual requiring hospital-level care, they
will be transferred to hospital.
ACT 1982
41
There is also the option for DHB supported isolation facilities for cases and
higher-needs contacts who are assessed to self-isolate unsuccessfully and
where transfer to a MIQ is not feasible or warranted. These facilities provide a
small volume of alternative accommodation solutions (5-10 bubbles of
accommodation).
Primary care services and networks are critical in providing monitoring support and
other health care for patients.
INFORMATION
42
Primary health care, including but not limited to general practice, is well
placed to care for people in the community. This is their core business, and
for many people, their general practice pharmacists, midwives, and other
familiar practitioners are their preferred and trusted health professionals. The
Ministry is working with these sectors to ensure that they can adapt their
services as needed to care for people at home, often via telehealth.
43
These providers also may have a lead role in case management, depending
on the circumstances of the person they are caring for. We need to ensure
people’s health needs are attended to, both in terms of experiencing illness
from COVID 19, but also in terms of continued management of other health
conditions – for example people may need support to collect repeat
prescriptions or attend a scheduled pregnancy consultation.
44
While in most cases, the regular health and welfare checks would be done by
the patient’s or whānau’s regular general practice, in some cases, this will not
be possible, for example approximately 10 percent of COVID-19 cases in
Auckland were not enrolled with a general practice.
RELEASED UNDER THE OFFICIAL
45
Establishing pathways to support whānau who are disengaged from primary
care to enrol and access primary care thus ensuring they receive appropriate
clinical care while isolating at home, will be critical. In these situations, the
DHB would lead the monitoring and connect with local and trusted providers
who can provide support with cases.
46
The exact form of patient welfare checks will vary depending on the context
and needs of the patient and whānau, which may be in-person, or via
7
I N C O N F I D E N C E
Document 3
telehealth or other virtual means. As we continue to roll out greater support in
the community, we expect to be able to provide updated metrics to Cabinet on
the different types of welfare checks being requested, and what further
support, if any, is needed to scale up methods of engagement that best
balance whānau and communities’ needs with provider capacity constraints.
A nationally integrated platform is being developed for providers to share information
47
It is critical that information from key disparate systems is shared where
possible. The current systems development has to date has focused on the
Elimination Strategy and does not, on its own, fit the purpose for the CPF.
48
As a short-term tactical support for the evolving requirements, the current
solutions are being adapted and this includes the National Contact Tracing
(NCTS), National Border (NBS) and Border Clinical Management (BCMS)
ACT 1982
Systems. Health providers will be responsible for inputting their assessments
of each patient into their relevant medical records. However, we need to be
able to feed in the social and welfare information that can be used by relevant
providers.
49
The Ministry is working on developing a national virtual health and telehealth
solutions to integrate information on clinical and welfare needs for cases and
whānau.
INFORMATION
50
The system will build on existing mechanisms used by the COVID Technology
Platform Programme (Vaccination, Borders, Testing and Contact Tracing) to
provide us with assurance people who are self-isolating are being supported
appropriately, through a whole-of-system approach.
51
A fit for purpose solution that supports requirements of Care in the Community
and integrates across PHUs, primary health providers, secondary care
(hospitals) and manaaki/welfare organisations is under development.
52
The Ministry is also working to explore options so that people who are
isolating can be contacted via their preferred channels, for example through
instant messaging services, to reach people more quickly and reduce the risk
of non-response to check-ins. We will also update on this in our December
repo t back.
53
It is also anticipated that the individualised and holistic assessment approach
being developed based on our learnings from the current work in Auckland,
Waikato and Northland will provide the basis for how agencies will ‘check in’
RELEASED UNDER THE OFFICIAL
on status and compliance of those isolating at home and in the community.
Tailoring isolation support services at a regional and local level
54
We understand through our experiences in Auckland and Waikato that the
likelihood of cases and contacts being willing and able to fully comply with
isolation or quarantine arrangements is strongly influenced by the quality of
the relationships that are established at the outset. It is important that upon
8
I N C O N F I D E N C E
Document 3
first contact with the COVID-19 positive person and their whānau, they are
made to feel safe, respected and supported.
55
This underscores the importance of undertaking assessment of personal
health and welfare needs as soon as possible. The programme is developing
key metrics for this stage of the process; examples may include:
• The clinical assessment will happen within 24 hours of a returned positive
test result (95% target)
• Care needs/referral to alternative accommodation within 48 hours
• Interview by public health within 72 hours.
56
Officials will brief Ministers on settled metrics early in December 2021.
ACT 1982
Providing social, welfare, wellbeing, and cultural needs through the whole-of-system
‘welfare approach’
57
The success of the clinical care is dependent on ensuring the holistic and
wrap-around approach is taken to appropriately support the individual who is
required to self-isolate.
58
It is critical within the initial hours following a positive COVID-19 r
INFORMATION esult, to
provide individuals who have high pre-existing needs with appropriate wrap-
around support.
59
The Ministry of Social Development (MSD) is leading the development and
provision of a whole of system approach that will provide welfare and
community-based supports, including food and other essential wellbeing
provisions to support individuals who are required to self-isolate and have
immediate welfare needs.
60
The welfare system approach will ensure that where the initial assessment
has identified that welfare support is required,
the appropriate welfare agency
or provider will be engaged to navigate and support critical wellbeing with
urgency.
61
The principles of ensuring equity in individual and whānau experiences and
enhancing their mana when engaging with services will guide the approach.
We understand from Māori and Pacific providers supporting COVID-19
patients in Auckland that there needs to be a key point of contact for whānau
RELEASED UNDER THE OFFICIAL
to assist them to navigate the system and refer their needs out to appropriate
providers as soon as possible, so that clinical and other care can be well-
integrated.
9
I N C O N F I D E N C E
Document 3
Suitable accommodation will be critical to enable safe self-isolation under the whole
of system welfare approach.
62
While most people who test positive and their immediate household will be
able to safely isolate at home, some of our most vulnerable groups will need
alternative options.
63
We intend that everyone is able to have appropriate accommodation that is
suited to their needs and supports them to isolate safely.
64
The DHB supported isolation facilities could provide a small volume of
alternative accommodation solutions. However, this is limited in scale, not
available in all regions, and will not be able to meet anticipated increased
demands. Table C represents accommodation units currently secured in place
with a contract under the accommodation component of the care in
ACT 1982
community model. The Ministry of Health will continue to work with DHBs and
MBIE to ensure sufficient supply of isolation facilities to mee the anticipated
demand.
Table C: Accommodation units available across the country
DHB
Number of units
Northland
5
Auckland
INFORMATION
7
Waikato
0
Bay of Plenty Lakes
13
Tairāwhiti
6
Hawke’s Bay
10
Taranaki
6
Whanganui
5
Mid Central
5
Wairarapa
3
Capital and Coast Hutt Valley
4
Nelson Marlborough
9
West Coast
0
Canterbury
6
Southern
8
South Canterbury
0
65
HUD, Kāinga Ora, MBIE, and MSD are developing an accommodation
response to support the Ministry of Health’s implementation of home isolation
RELEASED UNDER THE OFFICIAL
and to complement the Welfare response.
66
Under the proposed approach, alternative accommodation would be needed
for COVID-19 positive people who are in accommodation that is unsuitable for
safe self-isolation, where a welfare response cannot manage risks of
spreading the virus, and for COVID-19 patients who are non-compliant with
self-isolation guidelines.
10
I N C O N F I D E N C E
Document 3
Management of ongoing health, social and welfare needs is critical post recovery of
the patient.
67
The primary care team supporting the patient and whānau will continue to be
responsible for regularly monitoring symptoms through the at-risk period of
the illness (typically until day 14). Many people experience ongoing symptoms
and their clinical care will be managed by their primary care team. If these
continue at 6 weeks post-diagnosis, a follow up consultation will be used to
consider whether they need to be referred for secondary care review or
further support services for rehabilitation.
68
The roles and responsibilities need to be clear and understood and we still
have work to do to fine tune the model.
Implementation considerations
ACT 1982
DHB regional resilience plans will be used to implement and assess the progress of
the ‘COVID-19 care in the community’ model.
69
As a result of the recent Delta outbreak and the impact this has had on the
Northern Region, and in particular, the three Auckland DHBs, the Northern
Region DHBs have developed a Northern Region Resilience Plan that
provides a platform for an all-region response.
INFORMATION
70
The plan covers sixteen functional areas, from regional provider groups to
community care and public health, and all aspects have an equity lens, refer
figure one.
71
Each of the four DHB regions has appointed executive leads for progressing
the improvements of identified gaps. The leads meet regularly to progress
regional preparedness and activities and is coordinated by the Health System
Preparedness Programme (HSPP).
72
Each DHB region nationally has or is implementing a governance forum, a
coordination function and dedicated resource to deliver their preparedness
planning. Progress reporting against these plans is provided to the HSPP to
ensure that learnings can be shared and any roadblocks can be removed or
resolved in real time.
The Managing COVID-19 in the Community model will be reviewed regularly as we
progress our learning from regions and communities across New Zealand.
RELEASED UNDER THE OFFICIAL
73
While home isolation as a concept is not new, we consider that consistent
improvement can be made to ensure that the system is working as intended
for patients, whānau, and organisations supporting them. The compressed
timeframes for implementing the CPF will require solutions that need to be
adapted on the basis of the experience that follows, reflecting local conditions
and needs.
74
The clinical operating model and guidance for care in the community are
updated regularly, including further advice on best practice as this comes to
11
I N C O N F I D E N C E
Document 3
light. This means, for example, that key lessons from how home isolation has
worked in Auckland and in the Waikato can be used to support effective home
isolation throughout the rest of New Zealand, should this become necessary.
Copies of the operating model can be made available to Ministers on request.
75
The improvements will be underpinned by rigorous risk assessment and
effective information sharing between providers to ensure that those isolating
have their needs met and are able to access care appropriate to their holistic
level of need. The regional planning is also critical in providing oversight of the
challenges and achievements within regions that will be considered as part of
the continuous learning and improvement process.
76
There are particular complexities around supporting COVID-19 patients who
have other pre-existing conditions. The Ministry is working with relevant parts
of the sector, such as the Royal New Zealand College of General
ACT 1982
Practitioners, to ensure that these complexities are considered when
guidance is being developed and updated.
Interagency support and coordination at central, regional, and local level will be
critical to ensure the success of this programme.
77
Interagency relationships that promote collaboration and coordination will be
critical for the integration and connection of investments and services. This
INFORMATION
applies at all levels of support from centrally supported, regionally delivered,
and locally led.
78
Effective regional coordination is necessary to safely manage each case and
manage health system capacity so that resources can be delivered where
they are most needed. Frameworks have been developed by Pacific health
providers South Seas and The Fono in Auckland to assess patient and
whanau needs, and these are being drawn on to support providers with
culturally competent and appropriate clinical care.
79
PHUs are already building capacity to be able to cope with increasing case
numbers and bringing onboard support via telehealth. However, other
providers, particularly in primary care, will need to offer support in the
assessment process to ensure patients are provided with appropriate support
in timely manner. The Ministry is working on standardised, culturally
appropriate assessment that can support diverse parts of the health workforce
to conduct the assessment.
80
To manage COVID-19 positive people and whānau in the community, more
RELEASED UNDER THE OFFICIAL
rapid notification and involvement of primary care clinical teams is needed,
and a more diverse workforce will be engaged or required. New roles and
responsibilities may be shared across the system, such as more effectively
including allied health workforces. Work is underway to streamline information
sharing and to enable escalation of information to primary care teams where
necessary.
81
Support is needed to empower and enable the workforce to be safe and
effective in their roles, and to ensure sustainability. Flexibility of traditional
12
I N C O N F I D E N C E
Document 3
roles is encouraged, provided that the people engaged have the appropriate
qualifications, competencies, and tools for their work. This includes
community health pathways (developed in tandem with the primary care
clinical model) for primary care teams to use at point of care for guidance on
clinical management.
Metrics and standards are being developed to support the shift from a primarily
public health response to an individual clinical assessment.
82
There are existing metrics for our public health response to COVID-19, for
example requiring cases to be contact traced within the first 48 hours.
83
However, as we transition to a new approach, as stated in paragraph 55, new
metrics have been developed and these will be further considered. The
Ministry will report back on metrics under the new model as part of the
ACT 1982
December 2021 report back to the Cabinet, and iteratively up until then.
Financial Implications
84
There will be financial implications from the evolution of the model for care for
‘COVID-19 care in the community’. However, the work to create an accurate
picture of the funding required is yet to be completed.
85
Initial costings for community-based care assumes that clinical supp
INFORMATION ort for
patients requiring low to moderate level care will be provided through a
combination of general practice teams, established telehealth clinical
services, pharmacy services, and ambulance services. Clinical care is
anticipated to be available and accessible 24/7 to meet the needs of
households. The costing also includes translation services to support clinical
care and digital system integration for clinicians to access patient information.
However, these costs are current best estimates only and the underpinning
assumptions are currently under review with leaders from across the health
sector. Costs for equipment, information technology, accommodation
alternatives and MIQ are excluded from these costs, but will be covered in
other relevant Cabinet papers.
86
More complex care in the community will require a multidisciplinary team
clinical approach that will not only draw upon primary care clinical resources,
but will also require specialist services, and DHB outreach clinical supports,
delivered through the regional and local coordination functions. The costings
for this are currently being worked up.
RELEASED UNDER THE OFFICIAL
87
For the funding period 1 November 2021 to 31 October 2022, we anticipate
approximate costs as set out Table D.
13
I N C O N F I D E N C E
Document 3
Table D: Initial cost estimates for community based care
Sector
Funding (mil ions)
General practice and established telehealth clinical
$420.826
services (telehealth/virtual assessments, monitoring, in-
person assessment)
Community pharmacy (medicines advice, medicines
$18.136
management and delivery)
Paramedic and Ambulance services (patient transport)
$7.170
Translation services to support clinical care
tbc
88
While significant investment is required, providing care for patients and
whānau at home is likely to be more cost-effective than caring for patients in
MIQ or in hospital, and ensures that MIQ and hospital resources are reserved
ACT 1982
for patients and whānau with the most need.
89
We will return to Cabinet with detailed costings for the complete Health
System Preparedness programme of work, including this aspect of COVID-19
Care in the Community early in December 2021.
Legislative Implications
INFORMATION
90
This model operates in a high-trust environment where health is not involved
in compliance.
91
The assessment upfront will identify people at risk of being unable to comply
with the requirements of home isolation, and these people may be transferred
to MIQ or other alternative accommodation.
92
We need a legal framework that will require people to stay at home and will
also provide an escalation framework that will be used for most serious
breaches, taking into account equity and considering diverse and often
complex needs of individuals and communities.
93
Agencies are currently building the legislative and compliance frameworks for
isolation at home. The legal and compliance approach will be based on an
individual’s status, that is, they are COVID-positive or a potential case (a
community contact or a returnee), rather than creating a different framework
for returnees as compared to community members in isolation because of
previous location alone.
RELEASED UNDER THE OFFICIAL
94
We anticipate that once we shift to the CPF, the requirement to isolate at
home will be achieved through amendment to the Isolation and Quarantine
Order rather than continuing the use of s70 Orders as we are now.
95
The compliance framework will consider the post-Elimination context and as
appropriate, adopt a high-trust model. It is anticipated that this framework will
take account of risk assessments of individuals and/or households, to
determine the level and nature of checking that needs to be in place, and will
create a clear pathway and mechanism for escalation (including trigger points)
14
I N C O N F I D E N C E
Document 3
for relevant providers and professionals to follow. Ensuring that communities
retain trust in providers and professionals will also be a key factor in the
design of the framework.
96
Agencies will provide an update to Ministers on this work in late November as
part of the CPF report-back, including more details on the approach, the
frameworks, health and welfare pathways and plans for communicating
expectations to the public.
Impact Analysis
Regulatory Impact Statement
97
The identified potential legislative changes do not require a RIS because all
Orders made under Section 11 of the COVID Act have a standing exemption
ACT 1982
from this process.
Climate Implications of Policy Assessment
98
Not required as it is not anticipated that the work set out in this paper would
have significant emissions impacts.
Population Implications
INFORMATION
99
Māori and Pacific inequities have worsened as a result of the current COVID-
19 outbreak, impacting Māori access to a range of services and resources.
Inequitable COVID-19 vaccination rates between Māori and other ethnicities
means Māori are more vulnerable to contracting COVID-19. They are also at
increased risk of severe COVID-related infections, hospitalisation, requiring
ICU care, and death. It is critically important that care in the community is
delivered in a culturally competent way to reduce additional health risks. This
is being managed by collaborating with Māori and Pacific health providers to
support patients most at-risk from COVID-19.
100
Māori and Pacific populations are also overrepresented among people with
insecure or crowded housing, which may be unsuitable for home quarantine.
Consequently, retaining options for people to be transferred to MIQ or other
community isolation facilities is an important part of reducing inequities in this
work programme. This is also likely to be important for people who are not
safe at home, for example victims of family violence, who are more likely to be
women.
RELEASED UNDER THE OFFICIAL
101
For rural populations, home quarantine reduces the need to travel far from
people’s support networks; providing support by telehealth where available is
likely to be beneficial to rural populations, although it will not always be
possible (for example, in areas with poor phone or internet coverage).
102
There remains significant risk for disabled people - high mortality rates
associated with COVID-19 infections are reported internationally. Significant
distress has been reported by families under current level three restrictions
and there is potential for these issues to be further exacerbated by community
15
I N C O N F I D E N C E
Document 3
isolation and quarantine. Ensuring accessibility of communications and
support will be critical to supporting disabled people to isolate when needed.
The lack of feeling safe is as relevant as being safe and will impact
behaviours, in particular hesitancy in accessing COVID-19 testing. It is
recommended that disabled people and their allies are engaged in a rapid
design approach to ensure the issues for disabled people are understood and
designed into the approach.
Human Rights
103
The changes outlined in this paper have no immediate impact on human
rights, beyond those outlined in relation to the minimisation and protection
approach [CAB-21-MIN-0421 refers].
Consultation
ACT 1982
104
The following agencies were consulted on this paper: Department of Prime
Minister and Cabinet, Ministry of Social Development, Ministry of Business,
Innovation and Employment, the Treasury, Te Puni Kōkiri, Ministry for Pacific
Peoples, Oranga Tamariki, Ministry of Education, Ministry of Housing and
Urban Development, Ministry of Ethnic Communities, Office for Seniors,
Office for Disability Issues, Kāinga Ora.
Communications
INFORMATION
105
All-of-government communications in relation to the implementation of the
COVID Protection Framework will be considered separately by Cabinet.
106
Some operational communicat ons within the health system has already taken
place to allow changes outlined in this paper to be implemented. This includes
updating guidelines around the use of home isolation which have been
distributed to DHBs, PHUs and other health providers.
Proactive Release
107
I intend to proactively release this paper and its associated minute within the
standard 30 business days from the decision being made by Cabinet, with any
appropriate redaction where information would have been withheld under the
Official Information Act 1982.
RELEASED UNDER THE OFFICIAL
16
I N C O N F I D E N C E
Document 3
Recommendations:
The Minister of Health recommends that the Committee:
1
note that the Ministry of Health has developed the COVID-19 care in the
community model to support COVID-19 patients and their households and
whānau to quarantine and isolate at home
2
note that this approach also acknowledges that we are moving to a setting
where, with a highly vaccinated population, managing COVID-19 care in the
community will become the default as we start living with COVID-19
3
note that changes to the model will fundamentally change the patient
experience by moving to a holistic clinical and welfare assessment at the start
of the process, alongside the public health response
ACT 1982
4
note that caring for patients at home is necessarily a high trust model, based
on the principles of centrally guided, regionally coordinated, locally led, to
efficiently allocate health resource and enable people to be cared for in the
context of their community and does not replace hospital care where required
5
note that assessment and triaging of patient and whānau clinical and social
wellbeing needs alongside public health needs will be critical factors
determining the success of the programme
INFORMATION
6
note that the COVID-19 care in the community model will be managed
iteratively, with clinical operating guidelines regularly updated to reflect best
practice as new evidence comes to light
7
note that work is ongoing to address equity considerations in the home
isolation programme, including alternative accommodation options
8
note that the Ministry will report back to Ministers on metrics in the community
care model early in December
9
agree that Ministers will make final decisions on metrics in the community
care
10
note that primary care providers, particularly Māori and Pacific health
providers, are fulfilling a critical role in providing care that effectively meets the
needs of COVID-19 patients and their whānau
11
note that significant financial investment is ne
RELEASED UNDER THE OFFICIAL eded to enable community
health care providers to support COVID-19 patients as case numbers
increase
12
note key enablers for the care in the community model are still being
developed, including interventions which address social, welfare, wellbeing
and cultural needs. Related advice on accommodation, welfare, and MIQ is
being provided to Cabinet
17
I N C O N F I D E N C E
Document 3
13
direct joint Ministers to report back to Cabinet early in December 2021 on the
detailed financial implications of this programme
14
note that there are no implications for primary legislation anticipated, and
work is ongoing on how a compliance framework can be established through
secondary legislation
Authorised for lodgement
ACT 1982
Hon Andrew Little
Minister of Health
INFORMATION
Hon Chris Hipkins
Minister for COVID-19 Response
RELEASED UNDER THE OFFICIAL
18
I N C O N F I D E N C E

Document 4
Health Report
Cabinet Paper: COVID-19 Care in the Community – health system readiness and
preparation
Date due to MO: 1 December 2021
Action required by:
Security level:
IN CONFIDENCE
Health Report number: 20212653
To:
Hon Andrew Little, Minister of Health
Contact for telephone discussion
Name
Position
Telephone
Robyn Shearer
Deputy Chief Executive, Sector Support
S9(2)(a)
and Infrastructure
Russell Simpson
SRO Health System Preparedness
Programme
Minister’s office to complete:
☐ Approved
☐ Decline
☐ Noted
☐ Needs change
☐ Seen
☐ Overtaken by events
☐ See Minister’s Notes
☐ Withdrawn
Comment:

Document 4
Cabinet Paper: COVID-19 Care in the
Community – health system readiness and
preparation
Security level:
IN CONFIDENCE
Date:
1 December 2021
To:
Hon Andrew Little, Minister of Health
Purpose of report
1.
This briefing attaches a draft of the COVID-19 Care in the Community – health system
readiness and preparation Cabinet paper that has been prepared for the Social Wellbeing
Committee on 15 December 2021.
2.
In November, Cabinet directed Ministers to report back on next steps regarding COVID-
19 Care in the Community, including further information on the model of care, metrics for the
programme, and financial implications. [CAB-21-MIN-0492 refers].
3.
This paper requires consultation with your Ministerial colleagues with any feedback by 8
December 2021.
Robyn Shearer
Hon Andrew Little
Acting Chief Executive
Minister of Health
Ministry of Health
Date:
Date: 1/12/2021
HR: 20212653
2

Document 4
Appendix One: Cabinet Paper COVID-19 Care in the
Community

Document 5
Aide-Mémoire
Visit to Waikato District Health Board
Date due to MO: 16 December 2021
Action required by:
N/A
Security level:
IN CONFIDENCE
Health Report number: 20212734
To:
Hon Andrew Little, Minister of Health
Contact for telephone discussion
Name
Position
Telephone
Robyn Shearer
Deputy Chief Executive, Sector Support
S9(2)(a)
and Infrastructure
Jess Smaling
Associate Deputy Director-General, DHB
Performance and Support

Document 5
Aide-Mémoire
Visit to Waikato District Health Board
Date due:
16 December 2021
To:
Hon Andrew Little, Minister of Health
Security level:
IN CONFIDENCE
Health Report number: 20212734
Details of the
Friday 17 December 2021
visit:
12.30pm to 1.45pm
Waikato District Health Board
Waiora Central Business District (CBD) Building
87 Alexandra Street
Hamilton
Organisation
Waikato District Health Board (DHB) serves a population of more than 425,000
and covers more than 21,000 km. It stretches from northern Coromandel to Mt
Ruapehu in the south, and from Raglan on the west coast to Waihi on the
east. 59 percent of the population is defined as living in urban areas, and 41
percent in rural areas. 23 percent of the population is Māori (compared to the
national average of 16 percent).
Purpose of the
On Friday 17 December 2021, you are visiting Waikato DHB to meet with
visit:
frontline staff including the:
• team undertaking the health system preparedness for COVID-19 summer
response
• IT and IMT teams involved in the cybersecurity incident management.
Comment:
You have several events scheduled throughout the day. You will be
accompanied by local Members of Parliament and by a staff member from
your office.
A draft run sheet is provided in Appendix One and Appendix Two identifies key
people.
This aide-mémoire discloses all relevant information.
Robyn Shearer
Deputy Chief Executive
Sector Support and Infrastructure
Document 5
Briefing points to support your visit
1.
This briefing will support your visit to Waikato DHB. The visit is an opportunity to
observe and discuss the region’s preparedness for a COVID-19 summer response, and
the region’s response to the cybersecurity incident.
2.
This has been a challenging year for the DHB, with the ransomware attack, the COVID-19
Delta outbreak and the subsequent lockdown, the nurses and midwives strike and their
third-tier restructure.
3.
During the visit you may like to:
a. Thank the people you meet for their mahi and their resilience.
Waikato District Health Board
4.
Dame Karen Poutasi has been Commissioner at the DHB since May 2019, when then
Minister of Health, Hon Dr David Clark, ordered the replacement of the Board. Dame
Karen works with two Deputy Commissioners, Chad Paraone and Emeritus Professor
Margaret Wilson. Mr. Ken Whelan was appointed to the role of Crown Monitor at
Waikato DHB in August 2018, and the appointment was extended in February 2021 to
an open-ended term.
5.
In the five months to 30 November 2021, the DHB reported a surplus of $0.9 million
compared to its planned year to date deficit of $7.6 million. The underlying results net of
COVID-19 related surpluses and other exceptional expenditure is a deficit of $5.9 million,
which is $1.7 million favourable to plan. The draft (unaudited) actual 2020/21 result
(excluding one-off costs) is a $28.4 million deficit.
6.
Five capital projects have approved crown funding of $111.0 million and $14.9 million
funding is contributed by the DHB. Two of the projects are classified S9(2)(f)(iv) and no
action is required. Three of the projects are classified as S9(2)(f)(iv) by the Health
Infrastructure Unit and risk mitigations are in place.
7.
The Waikato DHB 2021/22 Annual Plan was signed by joint Ministers on 30 September
2021.
8.
The DHB has been part of the Ministry of Health’s (the Ministry) Intensive Support
Programme since April 2021 and is progressing an intensive support plan which covers
the following areas:
•
Mental Health and Addictions Implementation programme in response to the
recently completed ‘Waikato Mental Health and Addictions System Review’.
•
Reduction of child and adolescent mental health services waiting times.
•
Financial sustainability initiatives.
•
Development of more community and primary care services.
Health System Preparedness for COVID-19 Summer Response
9.
Significant work has been undertaken by the health sector to prepare for a surge
response to COVID-19 and implement the Care in the Community model. This includes
DHBs undertaking preparedness plans, regional planning to share skills and resources,
Document 5
and how to coordinate responses. This planning will ensure the country can coordinate
its response to minimise risk and allocate resources to the right place, at the right time.
10.
The Ministry has completed six desktop reviews of DHB resurgence plans, with another
four reviews underway this week, including Waikato DHB. The level of engagement and
cooperation with the review has been outstanding.
11.
The aim of the review is to identify areas of concern for the DHB, to understand the
plan’s strengths, and to identify innovative practices to share with other DHBs. There is
also an opportunity to highlight any additional areas for the DHB to focus their
attention.
12.
Waikato DHB has built a vast amount of experience to effectively respond to COVID-19
within their region, both at the community and hospital level.
13.
There will be the opportunity to thank the Waikato team for their work and for their
participation in the review hosted by the Ministry. You may also wish to ask the
following:
a. What are the challenges and opportunities in supporting their communities?
Specifically, what is working well, what could be working better, are there any
examples of best practice that they would like to share, and what do they need from
the Ministry/Government to support this work?
b.
What are the key things that have been learnt and what has been done to respond
to/address these learnings?
c.
How well are they supporting vulnerable groups in their community?
d. Are they happy with the strength of their preparedness planning?
COVID-19 update
14.
As of 14 December 2021, Waikato DHB reports1:
a. 21 new cases confirmed in the Waikato overnight, with 11 in Te Kūiti, three in
Tokoroa, two in Ōtorohanga, two in Hamilton, one in Te Awamutu, one in
Taumarunui and one in Huntly
b. there are 588 total number of cases (113 active and 475 recovered)
c.
two confirmed cases in hospital
d. Public Health, primary care and manaaki providers are supporting 74 people to
isolate at home
e. 1,393 tests were processed on 13 December and 1,291 vaccinations given
f.
93 percent of the eligible population have received the first dose of vaccine (86
percent Māori, 94 percent Pacific peoples), and 88 percent are fully vaccinated (75
percent Māori, 87 percent Pacific peoples)2.
1 Information sourced from Waikato District Health Board website
https://www.waikatodhbnewsroom.co.nz/2021/12/14/covid-19-public-advisory-14-december-2021/
2 Vaccination rates at Territorial local authority as at 11.59pm 13 December 2021. https://www.health.govt.nz/our-
work/diseases-and-conditions/covid-19-novel-coronavirus/covid-19-data-and-statistics/covid-19-vaccine-data
Document 5
S9(2)(c)
COVID-19 response, S9(2)(c)
, and clinical services
20.
Waikato DHB reports that even though elective and outpatient clinics are now at full-service
levels, they are working on addressing the backlog S9(2)(c)
there
will be an on-going impact on services and staff.
21.
Despite the impact of COVID-19, Waikato DHB’s total planned care interventions
delivery for the year is at 99.3 percent of plan, however, inpatient surgical discharges are
at 91.1 percent of plan.
22.
The DHB has reduced their cardiac waiting list from 95 patients waiting in the week
ending 15 August 2021, to 52 patients waiting in the week ending 12 December 2021.
The maximum target waiting is 73 patients for Waikato DHB, and they have successfully
managed the list.
END.
Document 5
S9(2)(f)(iv)
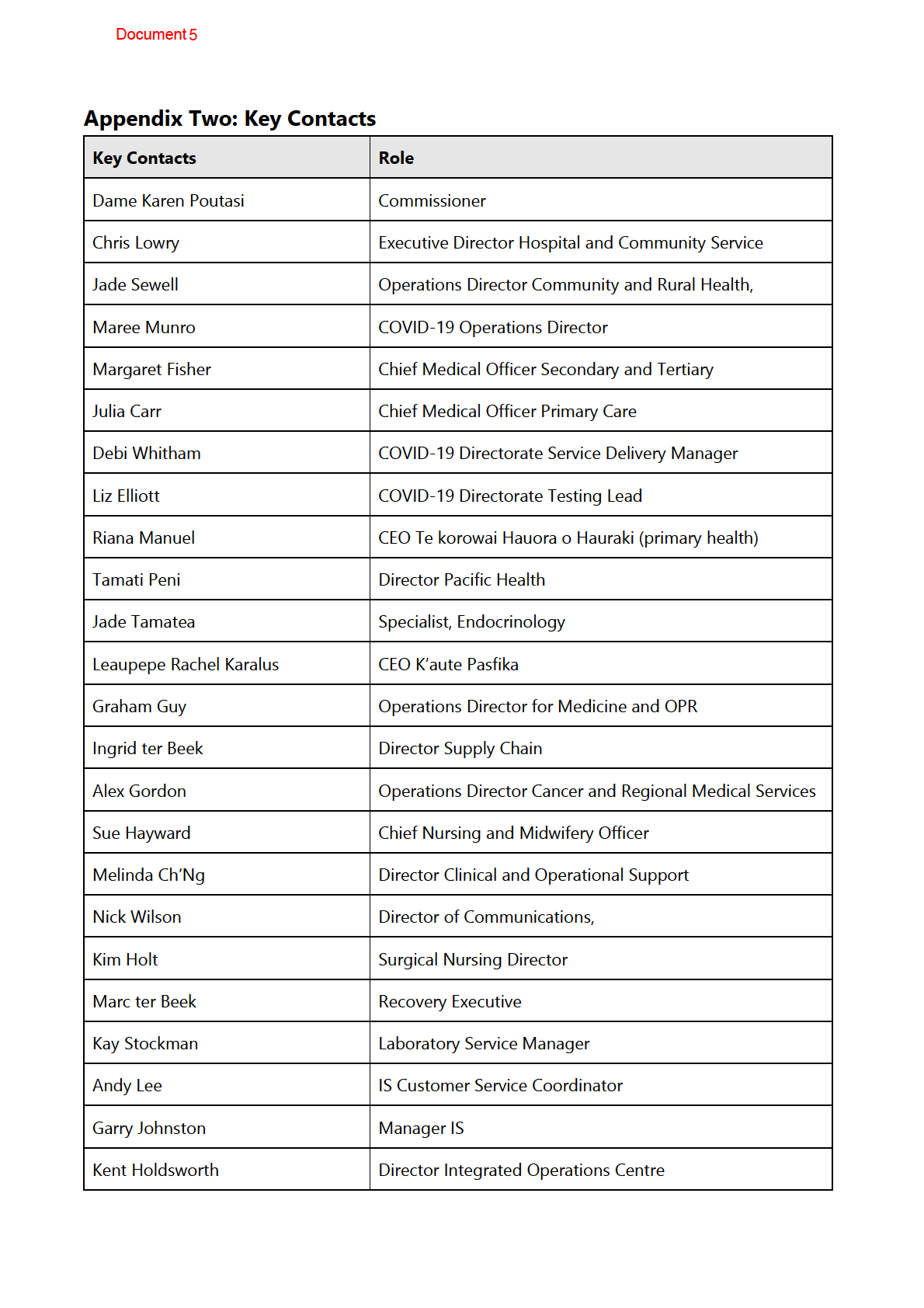
Document 5
Trevor Ecclestone
Manager Emergency Management Planning
Alex Gordon
Operations Director, Cancer Services and Radiology
Alana Ewe-Snow
Manager, Funding and Provider Relations
John Deane
Applications Manager
Max Christopher
Platform Manager
Community and Māori providers
Document 6
Briefing
Further information to support ‘Covid-19 Care in the Community – Health
System Readiness and Preparation’ Cabinet paper
Date due to MO: 16 December 2021
Action required by:
N/A
Security level:
IN CONFIDENCE
Health Report number: 20212753
To:
Hon Andrew Little, Minister of Health
ACT 1982
Contact for telephone discussion
Name
Position
Telephone
INFORMATION
Russel Simpson
Senior Responsible Officer, Health System
S9(2)(a)
Preparedness Programme
Robyn Shearer
Deputy Chief Executive, Sector Support
and Infrastructure
Minister’s office to complete:
☐ Approved
☐ Decline
☐ Noted
☐ Needs change
☐ Seen
☐ Overtaken by events
☐ See Minister’s Notes
☐ Withdrawn
Comment
RELEASED UNDER THE OFFICIAL
Document 6
Further information to support ‘Covid-19
Care in the Community – Health System
Readiness and Preparation’ Cabinet paper
Security level:
IN CONFIDENCE
Date:
16 December 2021
To:
Hon Andrew Little, Minister of Health
ACT 1982
Purpose of report
1.
The purpose of this report is to provide an update on work towards the COVID-19 Care
in the Community model, including funding options, further information on reporting
and metrics, patient privacy and information sharing, and next steps on the housing and
accommodation response.
2.
This report discloses al relevant information and implications.
INFORMATION
Summary
3.
The Cabinet paper ‘Covid-19 Care in the Community – Health System Readiness and
Preparation’ was discussed at the Social Wellbeing Committee on 15 December.
4.
The purpose of the paper was to provide an update on the COVID-19 Care in the
Community model. It also sought decisions on funding and financial implications and
approval of metrics for the model.
5.
We are seeking your decision on rates to be paid to enable general practice and other
primary care providers to providing clinical care to COVID-19 positive patients while they
are isolating home We consider that the appropriate pay rate would incentivise
providers to participate in COVID-19 care in the community, while managing financial
risk.
6.
Reporting on metrics for Care in the Community is being developed iteratively; we wil
have confidence that there is robust data on al metrics by the end of January 2022. Until
that time, reporting on metrics as they become available wil continue to happen
through daily Situational Reporting.
7.
Patient privacy and information sharing must be carefully balanced to protect public
health and maintain trust in the system. Consent to
RELEASED UNDER THE OFFICIAL share patient information is done
when a positive test is returned; we do not consider that it is a good use of health
system resource to seek consent to share information prior to a positive test being
returned.
8.
Al agencies that are involved in the COVID-19 Care in the Community model have a role
to play in identifying and addressing housing needs. The specific roles, responsibilities,
accountabilities and funding streams around housing are continual y being developed as
Document 6
part of the COVID-19 Care in the Community model. This work is progressing but is not
yet at the stage where it can be provided in detail in the current Cabinet paper.
Recommendations
We recommend you:
1
Agree to one of the following funding options for primary care providers
providing COVID-19 care in the community:
a) funding of $241.60 per hour.
Not recommended
Yes/No
OR
ACT 1982
b) funding of $250 per hour.
This is the Ministry’s preferred option.
Yes/No
2
Note that as soon as possible, the Ministry wil transition from an hourly rate
system to one in which available funding is grouped into packages of care
that will incentivise providers to deliver clinical care in a way that meets the
needs of both the patient and their whānau.
3
Note that financial implications the attached Cabinet paper have been
updated to reflect the Ministry’s preferred option, and that officials wil
update this if you choose another funding level.
INFORMATION
4
Note that work is ongoing to integrate data sou ces so that reliable metrics
wil be available by late January 2022.
5
Note that we do not intend to seek consent to share information with
providers of other services that the pat ent may need at the point of seeking
a COVID-19 test.
6
Note that the Ministry is continuing to work with housing agencies to
confirm roles and responsibilities for housing and accommodation in
relation to Care in the Community, and that we wil keep you updated on
this work.
Robyn Shearer
Hon Andrew Little
Deputy Chief Executive
Minister of Health
Sector Support and Infrastructure
Date:
Date:
RELEASED UNDER THE OFFICIAL
Document 6
Further information to support ‘Covid-19
Care in the Community – Health System
Readiness and Preparation’ Cabinet paper
Background
9.
The paper ‘COVID-19 Care in the Community – health system readiness and preparation’
was discussed at the Social Wellbeing Committee’s (SWC) meeting on 15 December
2021. This paper provides an update on the COVID-19 Care in the Community model. It
also seeks decisions on funding and financial implications and approval of metrics for
ACT 1982
the model.
10.
Your office has advised that SWC was not supportive of the proposed hourly rate to
remunerate GPs for providing services to COVID-19 patients. The Ministry wil work with
the Treasury to agree on a revised hourly remuneration rate.
11.
Further minor changes have been made to the paper and an updated version of the
paper is attached as Appendix One. This version wil be considered by Cabinet on 20
December 2021.
INFORMATION
12.
Where further changes have not been able to be incorporated into the Cabinet paper, an
explanation is provided below.
Response to further feedback on Cabinet paper
Reporting against metrics
13.
As noted in the Cabinet paper, metrics are proposed that cover all parts of the patient’s
journey, from positive test through to discharge from isolation and any follow-up care.
Reporting on ome of these metrics is already occurring in the daily COVID-19
Situational Report to Ministers; for the remainder, a dashboard is being developed that
wil be used to report fully at the end of January 2022.
14.
Providing well-coordinated care to patients and whānau wil be digital y enabled
through an updated case management system, adapted from the existing National
Contact Tracing, National Border, and Border Clinical Management Systems, which wil
be able to include inputs from primary and secondary health, as well as social and
RELEASED UNDER THE OFFICIAL
welfare information.
15.
Reporting of the metrics at a national level is dependent on DHBs, PHUs, general
practice and providers using the Border Clinical Management System (BCMS) or directly
through the integration of their patient management systems. Onboarding of DHBs and
PHUs to BCMS is currently under way. Onboarding of DHBs and PHUs to BCMS is
currently under way. Once onboarding and integration is completed, work wil need to
Document 6
be undertaken to guarantee the quality of the data before al metrics can be reported.
This work wil be completed by the end of January 2022.
16.
We could investigate options for DHBs, PHUs and providers to report manual y in the
interim, however, it may not be the best use of Ministry and sector resources at a busy
time of year, and we could not guarantee the quality of the data.
17.
If we can report on any metrics sooner, they wil be incorporated into the Situational
Report.
Consent to share health information with other providers
18.
We do not intend to seek consent to share information with providers of other services
that the patient may need at the point of seeking a COVID-19 test. The rates of testing
far outstrip the number of positive COVID-19 cases. It would not be an effec ive use of
ACT 1982
limited health resources to obtain consent from every person who has a COVID-19 test.
In addition, some forms of testing are now self-administered such as mandatory saliva
testing for border workers.
19.
As outlined in the COVID-19 Care in the Community Framework, the notification of a
positive COVID-19 case result wil be sent to the public health unit (PHU) and the
primary care provider that the patient is enrol ed with (if they are enrol ed with one)
directly from the laboratory as a matter of course.
INFORMATION
20.
As soon as possible when a patient has tested positive for COVID-19, their point of
contact in the health system wil seek informed consent to share relevant information
with providers of other services that the patient may need (for example, a GP sharing
information about a patient’s welfare needs with a social services provider).
21.
Where people do not consent to have their welfare information shared, they are advised
that they can cal the relevant helpline to access support at any time. This is live now and
has been in use since 9 December 2021.
At what point is patient privacy overridden to protect public health?
22.
The PHU or other appropriate provider at the care coordination hub wil assess a COVID-
19 positive person’s situation and the reasons why they are uncontactable or have not
consented to their information being shared. If there are concerns about the person’s
health and welfare, the PHU wil make a decision to share their information with another
provider, the Finder service1, or even escalate to Police in some circumstances.
Housing arrangements
23.
Al agencies that are involved in the COVID-19 Care in the Community model have a role
to play in identifying and addressing housing needs. For example, the health sector wil
RELEASED UNDER THE OFFICIAL
1 The Finder Service is a part of the National Contact Tracing Solution, with the purpose of finding contact details for cases
and disease contacts within NCTS, for any NCTS users working on cases or high priority contacts. In order to do this,
Finders liaise with a number of external and internal sources of information, such as Customs, GP practices, Police and IRD,
as well as the Audit and Compliance team within the Ministry, providing as much detail as has been gathered by case
investigators or contact tracers as necessary.
Document 6
be well-placed to identify housing needs as part of the patient and close contact
assessment process, while the Ministry for Social Development and Kāinga Ora are best
placed to procure and place people in homes.
24.
Pragmatical y, it is also likely that patients and their whānau wil also play a role in
meeting their own housing needs and wil not need support to do so (eg, some
household members temporarily relocating to other premises to create space for
patients to self-isolate safely).
25.
The specific roles, responsibilities, accountabilities and funding streams around housing
are continuing to be developed as part of the COVID-19 Care in the Community model.
This work is progressing but is not yet at the stage where it can be provided in detail in
the current Cabinet paper.
26.
ACT 1982
The Ministry has proposed an interim solution over the summer months, particularly in
relation to regions that are likely to have a high number of visitors. There is a smal
amount of funding (approximately $14 mil ion) in the community self-isolation and
quarantine funding pool that that we propose could be repurposed to support DHBs
with securing alternative accommodation over the summer months.
Next steps
27.
Officials can provide further information on these matters at your request.
INFORMATION
28.
Note that you wil be providing a report back to Cabinet in late February - early March
2022 on the Health System Preparedness Programme, including winter planning at
which time any residual funding needs (including workforce needs) wil have been more
fully assessed and wil be included. Health infrastructure funding is also being sought
separately.
ENDS.
RELEASED UNDER THE OFFICIAL

Document 7
Meeting advice: Minister Little, South Seas, and Northern Regional Health
Coordination Centre
Date due to MO: 01 February 2022
Action required by:
<N/A>
Security level:
IN CONFIDENCE
Health Report number: 20220127
To:
Hon. Andrew Little, Minister of Health
ACT 1982
Contact for telephone discussion
Name
Position
Telephone
Robyn Shearer
Deputy Chief Executive, Sector Support
S9(2)(a)
and Infrastructure
INFORMATION
Geoff Gwynn
Programme Director, Health System
Preparedness
Approved
Decline
Noted
Needs change
Seen
Overtaken by events
Withdrawn
Comment:
RELEASED UNDER THE OFFICIAL

Document 7
Meeting advice: Minister Little, South Seas, and Northern Regional Health
Coordination Centre
Security level:
IN CONFIDENCE
Date:
01 February 2022
To:
Hon Andrew Little, Minister of Health
Purpose of report
1.
ACT 1982
2.
Summary
3.
INFORMATION
4.
5.
Recommendations
RELEASED UNDER THE OFFICIAL
Robyn Shearer
Hon Andrew Little
Deputy Chief Executive,
Minister of Health
Sector Support and Infrastructure
Briefing: HR20220127
1
Document 7
Meeting advice: Minister Little, South Seas, and Northern Regional Health
Coordination Centre
Background / context
1.
2.
ACT 1982
3.
NRHCC
INFORMATION
Overview
4.
5.
6.
7.
Pacific Co ordination Hub
8.
RELEASED UNDER THE OFFICIAL
9.
10.
Briefing: HR20220127
2
Document 7
11.
12.
13.
14.
ACT 1982
Maori Co-ordination
15.
16.
INFORMATION
17.
18.
Key Highlights and Challenges
19.
a.
b.
RELEASED UNDER THE OFFICIAL
c.
d.
e.
Briefing: HR20220127
3

Document 8
Aide-Mémoire
COVID-19 Hospital Readiness
Date due to MO 11 February 2022
Action required by:
N/A
Security level:
UNCLASSIFIED
Health Report number: 20220205
To:
Hon Andrew Little, Minister of Health
Contact for telephone discussion
ACT 1982
Name
Position
Telephone
Robyn Shearer
Deputy Chief Executive, Sector Support
S9(2)(a)
and Infrastructure
Jess Smaling
Associate Deputy-Director General, DHB
Performance and Support
INFORMATION
RELEASED UNDER THE OFFICIAL

Document 8
Aide-Mémoire
COVID-19 Hospital Readiness
Date due:
11 February 2022
To:
Hon Andrew Little, Minister of Health
Security level:
UNCLASSIFIED
Health Report number: 20220205
Details of
14 February 2022
meeting:
ACT 1982
Purpose of
A meeting has been convened by the Prime Minister to discuss COVID-
Meeting:
19 Hospital Capacity and Readiness considering Aotearoa’s increasing
COVID-19 cases.
INFORMATION
Comment:
This Aide-Mémoire covers the fo lowing topics:
1. Critical Care
2. Acute Demand
3. Planned Care
4. Workforce
5. COVID-19 Care in the Community
Robyn Shearer
Deputy Chief Executive
Sector Support and Infrastructure
RELEASED UNDER THE OFFICIAL
2
Aide Memoire: 20220205
Document 8
COVID-19 Hospital Capacity and Readiness
Background
1.
District Health Boards (DHBs) and their supporting networks have completed assurance
activities to determine the current state of Aotearoa’s health sector readiness and
considers the country to be highly prepared for Omicron.
2.
However, there are chal enges to achieving full preparedness. The health sector is
unlikely to meet 100% preparedness. Although it has planned for the implications of
COVID-19, due to externalities, some of those plans wil be unable to be implemented.
3.
These externalities were largely present prior to, but exacerbated by, COVID-19 Some
examples of these are:
a. Shortage with a qualified health workforce.
ACT 1982
b. Existing inequities in the health system.
c. Access to mobile and internet coverage.
d. Supply chains have become increasingly problematic due to COVID-19 influences,
resulting in delays to goods and building supplies. This in turn limits the ability for
DHBs to improve existing infrastructure, and purchase required health infrastructure.
DHB COVID-19 Preparedness Reviews
INFORMATION
4.
As part of its assurance workstream, the Health System Preparedness Programme
conducted desktop reviews of 10 DHBs’ resurgence plans. The purpose of these reviews
was to provide the Ministry with assurance that each DHB had undertaken sufficient
preparedness planning to manage COVID-19 cases in their districts.
5.
To measure preparedness over time and establish an effective continuous improvement
approach to health sector preparedness, baseline data was required. The Ministry
designed an assurance checklist to measure COVID-19 preparedness and circulated it to
DHB Chief Executives in December 2021.
6.
Results of the completed checklist by the 10 DHBs combined identified the fol owing:
a. 63% of identified preparedness activities were complete.
b. 36% of identified preparedness activities were partial y completed.
c. 1% of identified preparedness activities were not started.
7.
With baseline data and the change in approach due to the emergence of the Omicron
variant, an updated checklist was provided to DHBs in January 2022.
RELEASED UNDER THE OFFICIAL
8.
This updated checklist repeated the requirements identified in the December 2021
checklist, and added a subsequent Omicron specific set of criteria.
9.
The results of this checklist identified a national improvement of 10% in completed
preparedness activities, presenting a shift to:
a. 73% of identified preparedness activities to be completed.
b. 27% of identified preparedness activities to be partial y completed.
3
Aide Memoire: 20220205
Document 8
10.
It is acknowledged that hospitals face considerable systemic and structural chal enges,
especial y in the areas of capacity, facilities and workforce, which existed prior to the
onset of the COVID-19 pandemic. The Ministry’s Health System Preparedness
Programme is working closely with DHBs to identify chal enges, share lessons learned
and ways to support DHBs to remediate any issues with their COVID-19 preparedness.
11.
The desktop reviews and resurgence planning checklists provided the Ministry with a
level of assurance that DHBs have plans in place to minimise the impact of COVID-19 on
communities within their district.
12.
DHBs and their supporting networks have done extensive work to prepare their staff,
facilities and communities to address and manage the likely pressures that will come
from the increase of COVID-19 in the community. Some of the measures employed
include:
a. working regional y to plan COVID-19 responses
b. working regionally to share skills
c. working regional y to share resources
d. identifying staffing needs and providing training and refresher courses for staff from
across the organisations to increase the required workforce.
13.
The Ministry is aware that DHBs have identified hospital capacity to be used for COVID-
19 positive patient and have plans in place to use capacity and workforce differently as
required, should a surge in cases occur.
Critical Care
14.
Decisions on prioritising clinical resources and treatment between COVID-19 patients
and planned care and other patients is a key role for the health system. Clearly critical
patients wil always be prioritised first. Unfortunately, this may mean that some services
may see ongoing cancellations or delays.
15.
There are processes in place to support Intensive Care Unit staff to move around the
country if needed. For example, in the early part of the latest outbreak, Intensive Care
Unit staff from around the country were identified, with some travelling to Auckland to
support the response.
16.
This was a pre-emptive strategy to make sure staff had the opportunity to have on the
ground orientation – at that stage the size of the outbreak was unknown, and it was
prudent to make sure staff were available, trained and orientated; and to mitigate any
risk of lower workforce numbers should staff have become close contacts or have been
in places of interest. DHBs have had a significant period of pressure with managing
Respiratory Syncytial Virus (RSV) patients, so this gave flexibility for rostering and staff
welfare.
17.
DHBs continue working on ways to increase intensive-care capacity, including using
“shelled” spaces (areas of hospitals not currently being used) and converting existing
wards to have intensive care capabilities. The Ministry is expecting to approve these
plans in the coming weeks.
Surge planning and response
4
Aide Memoire: 20220205
Document 8
18.
Surge planning has included work to ensure we can maximise the use of our current
capacity of Intensive Care Unit bed spaces and phase up the use of High Dependency
beds, and then Recovery room and other bed spaces.
19.
DHBs are working to best balance the demands of health services, related to both
COVID-19 and other health needs (such as planned care). However, in an escalated
surge situation, there is opportunity to prioritise clinical delivery based on need, and
defer non-urgent, deferrable care that may otherwise draw on health system resources,
including Intensive Care Unit beds.
20.
Hospital bed capacity in Aotearoa changes daily, influenced by district patient demand,
hospital resource and staffing. At present, there are approximately:
a. 250 resourced Critical Care Beds
b. 180 fully COVID-19 capable beds.
21.
In a surge situation, DHBs in Aotearoa can cater for 550 resourced Intensive Care Unit
beds, which can also be converted to al ow further capacity when required. It is
important to note that this is not newly created capacity – it is available capacity being
repurposed. As far as capacity is ‘surged’ for COVID-19 care, the trade-off is capacity for
other ‘business as usual’ health care delivery is being used instead.
22.
Not al patients who have COVID-19 may need to be on a ventilator, or in an Intensive
Care Unit.
23.
DHBs have respiratory equipment for providing a range of oxygen therapies that can be
used by respiratory teams outside of Intensive Care Units. These are critical in the
management of COVID-19 patients.
Funding for Intensive Care Units’ capacity
24.
Cabinet has ear-marked $100 million of capital funding from the COVID-19 Response
and Recovery Fund to accelerate these ICU projects.
25.
The Government wil be upgrading 24 local hospitals this year to support planned and
routine care, to ensure non-COVID-19 patients are safe when COVID-19 patients are
being treated. This includes 23 new Intensive Care Unit and High Dependency Unit beds,
and eight temporary bed conversions to Intensive Care Units.
26.
The three major Intensive Care Unit capacity-increasing projects – North Shore,
Christchurch and Tauranga – remain on target. Tauranga has delivered six High
Dependency Unit beds earlier than planned.
27.
There is another $544 mil ion of operational funding available over three years to fund
ongoing costs like staffing. This funding wil be al ocated to support additional hospital
capacity, including critical care across Aotearoa.
5
Aide Memoire: 20220205
Document 8
Workforce
28.
We have shortages across the range of staff required to support Intensive Care Unit and
High Dependency Unit beds. However, currently our greatest limitation is the nursing
workforce. The level of capability of hospitals nationally differs, with smaller hospitals
not usual y providing higher levels of Intensive Care Unit care. Capability is
geographical y spread, and our staffing reflects this. There are existing networks and
processes in place to support transfer of patients as needed.
29.
DHBs have and continue to train a range of staff groups who can support experienced
Intensive Care Unit staff to manage COVID-19 patients on a temporary basis.
30.
COVID-19 funding of $2 mil ion was al ocated to fund the Intensive Care Unit support
surge training since 2020 - this training builds additional capability for staff to expand
their skillset to support patients with higher ventilation needs but are not the same as a
fully trained and experienced Intensive Care Unit resource. This also includes those that
need refresher training, so is a mix of new and refreshers to boost capacity when
needed.
31.
This initiative will not necessarily mean the optimal ratio of 1:1 staff: patient ratio would
be maintained, but patients would stil receive the best care available – in line with the
historical high quality of care delivered within Aotearoa’s health sector.
32.
Work is underway to increase the permanent critical care nursing workforce. An
international campaign – aimed predominantly at Aotearoa’s trained nurses – has been
launched in February 2022. Other funding approved wil support post graduate study
and increase the number of educators/clinical coaches etc in critical care.
33.
The Health System Preparedness programme has funding of $10 mil ion for short to
medium term health workforce skil s and recruitment initiatives this financial year (to 30
June 2022), of which $3.625 million is designated for the critical care workforce
initiatives. These initiatives include the fol owing.
a. Training for critical care surge support staff - support for the DHBs to train a range
of staff who can provide support to experienced critical care staff to care for COVID-
19 patients on a short-term basis.
b. Recruitment co-ordination function – centralised matching and negotiation of
packages for staff entering New Zealand, including Managed Isolation and
Quarantine places.
c. Recruitment campaign - support for a DHB led campaign to bring New Zealand
trained critical care nurses back.
d. Educators/clinical coaches to support increased student intake numbers – ensuring
that there is increased capability to accept more nurses into critical care study,
potential y with more intakes each year.
e. Scholarship funding for post graduate critical care study -funding for postgraduate
study for a critical care paper for 40 nurses.
f. Funding for increased the Nurse Entry to Practice Programme - increased funding to
support 30 additional nurses into critical care roles.
The health workforce is not immune to COVID-19 either. DHBs are reviewing and testing
their contingency plans to make sure they have approaches in place should their teams
6
Aide Memoire: 20220205
Document 8
become unwell (or are identified as close contacts). This includes considering rostering
and staff cohorting where possible.
Protecting planned care and maximising the use of critical care capacity
34.
Patients requiring complex surgical procedures such as cardiac surgery regularly spend a
short time post-surgery in critical care. National plans have been developed to al ow the
redistribution of patients between units to ensure that the highest priority patients
continue to receive timely care.
35.
Plans are being developed to ensure that during a surge, al critical care capacity is
utilised across Aotearoa in a co-ordinated manner. This wil involve patients being
transferred as necessary to an appropriate bed space.
Protecting critical care capacity
36.
DHBs have increased their capability to manage COVID-19 patients in general (and
specialised) wards – focusing on the provision of oxygen to a patient. Within the Delta
outbreak to date, this has meant a lower percentage of patients have required critical
care than that seen in many other jurisdictions. This is testament to the work of multi-
disciplinary teams.
37.
The availability of new pharmaceuticals to treat COVID-19 is also impacting the number
of patients requiring critical care.
38.
Novel therapeutics for COVID-19 that can be used in the community to reduce the risk
of hospitalisation, Intensive Care Unit admission and death are in the process of
becoming available in New Zealand.1 Planning is in place to develop implementation
plans to rol out these therapeutics in the community, including clear and considered
guidance around where their use should be prioritised.
39.
Increases in the vaccination rate within the population is positively impacting the
number of COVID-19 cases requiring both hospitalisation and critical care.
Acute Demand
40.
There is additional work occurring at the primary-secondary interface to strengthen and
integrate service delivery to al ow primary care to manage people in the community as
they become unwell. These people would otherwise need to go to hospital.
Key points to note are:
a. This is clinical support for acutely unwell people (as distinct from well or mildly
unwell people who are just being monitored).
b. Many current pathways default to hospital Emergency Departments.
c. Integrated services can provide support for primary care to treat people in the
community and avoid hospital.
1 For example, the Monoclonal Antibody treatment casirivumab/imdevimab (Ronapreve) is currently undergoing the approval process
with MedSafe who are awaiting further information from Roche. The initial delivery of 4,800 doses is due to arrive in the country within the
next week.
Regarding oral antiviral treatments, the MedSafe approval process for Phizer’s oral protease inhibitor is underway and Pharmac’s
COVID-19 Therapeutic Technical Advisory Group met in late December 2021 to consider the groups that could be eligible for it.
7
Aide Memoire: 20220205
Document 8
d. Many of these people are COVID-19 positive but wil require treatment for non-
COVID conditions.
e. The clinical Health Pathways platform used by primary care is updated to include
advice, clinical pathways and available options.
41.
Options being explored include:
a. Access to community diagnostics (rather than send patients to hospital for x-rays or
other tests).
b. Mobile or virtual Mobile Digital Technology community teams (including
supporting and upskil ing aged residential care staff).
c. Community infusion clinics (for COVID-19 therapeutics, rehydration and other IV
needs).
d. ‘Hospital in the home’ to avoid hospital admission.
e. Virtual ward rounds to provide secondary care while stil at home.
f. When admitted to hospital, early discharge with secondary support at home
(before being well enough for full discharge back to primary care).
42.
Many of these options are already in place in Auckland and worked well during the Delta
outbreak. Some other regions have pathways in place for certain acute conditions, but
this is not widespread. Work is underway to share these models and provide guidance
for DHBs to al ow acutely unwell patients to be assessed and managed without the need
to go to hospital.
43.
With international borders opening and usual seasonal il nesses anticipated to increase
over the coming winter months, there is work underway to ensure planning is being
carried out for both Omicron and seasonal il ness demands on hospital resources.
The winter season planning considers the fol owing:
a. immunisations for flu and measles
b. pharmacy, community and primary care options
c. surveil ance monitoring
d. emergency management triggers.
Planned Care
44.
The number of Planned Care patients waiting beyond expected timeframes was
increasing prior to March 2020 when COVID-19 lockdowns commenced in New Zealand.
45.
The shift to the ‘Traffic Light’ system has enabled DHBs and private hospital providers to
continue providing health care services under al ‘Traffic Light’ colours. This is a
significant shift from the Alert Level framework, where many procedures (assessments,
diagnostics and surgery) were deferred. Whilst not back to usual planned levels, there
has been a marked increase in delivery of Planned Care services in recent months.
46.
Ongoing communication is important to ensure our health system continues to deliver
as much care as it can safely manage to, and not revert to deferring care unnecessarily.
47.
Strategies to optimise capacity include:
8
Aide Memoire: 20220205
Document 8
a. Additional investment in delivery enabled through COVID-19 Response and
Recovery Fund (CRRF), both in public and private facilities.
b. Changes to care models to reduce the demand on hospital services, i.e., use of
physiotherapists prior to being accepted for orthopaedic surgery.
48.
Advice is provided to the Minister of Health on:
a. the changing quantum of Planned Care impacts in an evolving context
b. the financial impacts of under-delivery of Planned Care
c. other options that could support a reduction in demand or an increase in supply of
services.
49.
Sector leaders (operational and clinical) meet fortnightly, or more regularly as needed, to
discuss emerging service pressures and identify solutions, particularly across tertiary
services.
50.
Regional col aboration can bring new solutions to resource management. Regional
governance leads are focussing this as a priority, and it is anticipated that some of the
existing barriers to col aboration can be overcome more readily through the new Health
NZ organisation model.
51.
Hospitals are no longer able to work in an environment devoid of COVID-19 cases.
Planned Care delivery wil continue to be disrupted as DHBs maintain protocols to
ensure staff and patient safety whilst working in an environment with COVID-19 and
non-COVID-19 patients being treated simultaneously.
52.
Short term immediate priorities for DHBs are increasing capacity, maintaining stability of
and prioritising waiting lists.
COVID-19 Care in the Community
53.
Given the likely pace and scale of a widespread Omicron outbreak, the current Care in
the Community model wil not be able to provide the same high-level of health and
welfare support for people required to isolate. To retain capacity for a primary care led
intensive clinical care pathway for those with the greatest need, a self-service model has
been developed to support low risk patients. This is being built on the fol owing
principles:
a. It wil be equity focused, ensuring that those with the greatest risk wil be able to
access the level of clinical care they need.
b. Non-digital support wil be available for those who are unable to access digital
platforms.
c. Those that can safely self-manage at home wil have a range of guidance to enable
them to do this, including instructions on how to access emergency assessment
should their condition deteriorate at any time.
54.
New functionality across key digital platforms that support the delivery of COVID-19
Care in the Community are under active development, with incremental releases
expected in the coming weeks. Cases wil be able to submit their symptoms, risk factors,
welfare needs, and contact tracing information online rather than via phone. We are also
looking to embed more text message functionality such as positive cases receiving
notification of their test results and information packs with web links via text.
9
Aide Memoire: 20220205
Document 8
55.
A risk stratification tool will allow the health sector to understand its population profiles
and manage resources, such as therapeutics and hospitalisation prioritisation, while also
ensuring that those who can manage their COVID-19 isolation period independently are
enabled to do so. This wil free up primary care and hospital level care resources for
those who need it the most.
ENDS
10
Aide Memoire: 20220205
Document 9
Briefing
Proposal to resource additional critical care beds across Aotearoa New
Zealand
Date due to MO: 28 February 2022
Action required by:
N/A
Security level:
IN-CONFIDENCE
Health Report number: 20220333
ACT 1982
To:
Hon Andrew Little, Minister of Health
Hon Grant Robertson, Minister of Finance
INFORMATION
Contact for telephone discussion
Name
Position
Telephone
Robyn Shearer
Deputy Chief Executive, Sector Support
S9(2)(a)
and Infrastructure
Minister’s office to complete:
☐ Approved
☐ Decline
☐ Noted
☐ Needs change
☐ Seen
☐ Overtaken by events
☐ See Minister’s Notes
☐ Withdrawn
Comment:
RELEASED UNDER THE OFFICIAL
Document 9
Proposal to resource additional critical
care beds across Aotearoa New Zealand
Security level:
IN CONFIDENCE
Date:
28 February 2022
To:
Hon Andrew Little, Minister of Health
Hon Grant Robertson, Minister of Finance
Purpose of the report
ACT 1982
1.
This report outlines a proposal to fund additional critical care beds ac oss Aotearoa
New Zealand and seeks drawdown of the remaining operating funding set aside in the
‘Raising intensive care and inpatient capacity to meet COVID-19 demand’ tagged
contingency of $542.2 mil ion to increase bed capacity. This operating funding is part
of the $544.2 million operating expenditure (and associated $100 mil ion capital
expenditure) announced in December 2021.
2.
The report details the short, medium and long-term al ocation of the funding,
acknowledging a shift from the funding of ‘surge’ (or crisis) capacity to a permanent
INFORMATION
uplift in capacity.
Summary
3.
Since the beginning of the COVID-19 pandemic, district health boards (DHBs) have
developed and maintained plans for managing a surge in critical care patients. This has
involved identifying areas within their hospitals where patients can be managed,
increasing the number of isolation rooms and upgrading airflow, managing stocks of
ventilators and key consumables, preparing to defer non-urgent care, and most
importantly, training a range of staff who can support experienced critical care
personnel to manage patients.
4.
Aotearoa NZ currently has approximately 180 adult and paediatric COVID-19 capable
Intensive Care (ICU)1 beds and approximately 260 funded ICU or High Dependency
Unit (HDU) beds. Approximately 245 of these beds are resourced. Funding of $140
million on an annual basis wil resource an additional 85 (mixture of ICU and HDU)
beds.
5.
The key limiting factor to resourcing additional critical care beds is the nursing
workforce. Funding of $3.6 million (funded through a workforce initiatives al ocation) is
being applied to supporting a recruitment campaign, increasing funding for training
and post graduate study and adding educator/clinical coach time into critical care units
across the country through to 30 June 2022.
RELEASED UNDER THE OFFICIAL
6.
Workforce remains the greatest risk to achieving the increase in capacity over the
timeframe indicated. Other work to standardise qualifications and support training wil
1 These are beds that can be resourced on a 24/7, 1:1 nurse:patient ratio, to care for critically ill, ventilated COVID-19
patients on an ongoing basis.
Document 9
assist in increasing the workforce on a long-term basis. To maintain momentum,
funding of $5.3 mil ion wil be applied to initiatives to increase the permanent
workforce – for recruitment, training and retention – in Year 2.
7.
While the focus wil remain on the nursing workforce in Years 1 and 2, there is the
opportunity to expand the initiatives to other staff groups – predominantly allied
health professionals aligned to critical care.
8.
In April 2020, the OECD published a report titled “Beyond Containment: Health system
responses to COVID-19 in the OECD”. Included in this report were comparisons of both
intensive care and acute bed numbers across OECD countries. Aotearoa NZ was shown
to be particularly low in ICU beds on a population basis.
9.
Published in January 2022, the OECD’s Economic Survey of NZ again identified the
ACT 1982
shortage of ICU capacity and included in its first recommendation that this be
addressed. This proposal therefore focuses on funding a meaningful uplift in resourced
critical care beds across Aotearoa NZ.
10.
In November 2021, Cabinet approved the establishment of the ‘Raising intensive care
and inpatient capacity to meet COVID-19 demand’ tagged contingency to fund the
operating and capital costs associated with solutions to increase ICU and inpatient bed
capacity to meet COVID-19 related pressures on the health system [DEV-21-MIN-0235
refers].
INFORMATION
11.
In December 2021, funding of $100 mil ion was announced to support rapid hospital
improvements to better manage COVID-19, which included the addition of some
ICU/HDU beds as wel as cardiac care and ward beds. At the same time, $544.2 million
was announced to fund increases in hospital bed capacity, both on a surge and
permanent basis.
12.
Transitioning the funding from surge to permanent as it increases over time allows
support for short term peaks in demand to be resourced and also time for the
permanent workforce to increase and the additional funded beds to be appropriately
resourced.
13.
In December 2021, Ministers of Finance and Health (Joint Ministers) approved the
drawdown of part of the operating contingency and the full amount of the capital
contingency to support a preferred programme of rapid capital investments
[HR20212687 refers]. Capital funding of $100 million was drawn down to fund 36
projects of infrastructure upgrades at 24 hospitals across 19 DHBs, with an associated
operating funding of $1 mil ion each year in 2021/22 and 2022/23 to meet the cost of
a team within the Health Infrastructure Unit of the Ministry to support the completion
of the capital projects. The remaining operating balance of the ‘Raising intensive care
and inpatient capacity to meet COVID-19 demand’ tagged contingency is $542.2
million after this drawdown, phased as follows:
RELEASED UNDER THE OFFICIAL
$ million
2021/22 2022/23 2023/24 2024/25 2025/26 &
Total
Outyears
Operating contingency
15.3
106.3
140.2
140.2
140.2
542.2
Document 9
14.
It is proposed the remaining $542.200 million is allocated as follows:
Year
Funding
One-off
Permanent Comments
2021/22
$35.3m(1)
$35.3m surge
Nil
Spread across regions on activity and
costs
population basis to fund surge costs in
both critical care and ward beds
2022/23
$86.3m(1)
$5.3m workforce $81.0m
Agree timing of new beds on regional basis
initiatives
to apply funding(2)
2023/24
$140.2m
Nil
$140.2m
Permanent uplift of 85 critical care beds(3
Outyears $140.2m
Nil
$140.2m
Ongoing permanent uplift of 85 critical care
beds(3)
(1) In 2021/22 and 2022/23, $1 million has been allocated to departmental expenditure to manage the delivery of
ACT 1982
the capital fund ($100 million)
(2) Optimally this would be beds resourced from 1 July (but could include others from later dates)
(3) If regions decided to substitute medical ward beds for critical care beds, the total number of beds would
increase.
15.
Permanent funding would be al ocated to regions, with the requirement to resource a
minimum number of beds. The baseline for the al ocation is the number of beds
currently funded at a unit level. The proposed distribution across the country of the 85
additional funded critical care beds is shown at Appendix 1.
16.
INFORMATION
The expectation is that DHBs would resource existing funded but unresourced beds
before accessing any funding through this al ocation.
17.
From 1 July 2022, the accountability fo this funding will shift to Health NZ (HNZ). The
Ministry of Health (the Ministry) wil ensure that there is joint governance over the
planning and implementation of this funding al ocation and that a smooth transition in
oversight occurs over the next few months.
Recommendations
Minister Minister
of of
Health Finance
We recommend you:
a)
Note that on 22 November 2021, Cabinet approved the establishment of the
“Raising intensive care and inpatient capacity to meet COVID-19 demand”
tagged contingency to fund operating and capital costs associated with
solutions to increase ICU and inpatient bed capacity to meet COVID-19-
related pressures on the health system [DEV-21-MIN-0235 refers]
b)
Note that Cabinet authorised the Ministers of Finance and Health to jointly
approve the drawdown from this tagged contingency and approve any
RELEASED UNDER THE OFFICIAL
changes to appropriations subject to the fol owing conditions:
a. the need for funding is evidenced by reliable and accepted
modelling
b. the solution can realistical y be implemented within the short to
medium term to reflect the acute need of the COVID-19 response
Document 9
c. critical enablers (e.g. capital solutions, workforce, logistics,
administration) have been provided for and coordinated across the
Ministry of Health and applicable District Health Boards (or Health
New Zealand regions)
c)
Note in December 2021, Joint Ministers approved the drawdown of $100
million in capital and $2 million in operating ($1 million each year in
2021/22 and 2022/23) from the “Raising intensive care and inpatient
capacity to meet COVID-19 demand” tagged contingency [HR20212687
refers] and the remaining balance of the contingency is $542.2 mil ion in
operating funding only, profiled as fol ows:
ACT 1982
$ million
2021/22 2022/23 2023/24 2024/25 2025/26
&
Outyears
Operating contingency
15.3
106.3
140.2
140 2
140.2
d)
Agree the remaining $542.2 mil ion operating funding held in contingency
Yes/No Yes/No
INFORMATION
should be rephased across years, to increase funding for surge costs in the
2021/22 year and allocated as fol ows to fund a minimum of 85 additional
inpatient beds:
Year
Funding
One-off
Permanent Comments
2021/22
$35.3m(1)
$35.3m
Nil
Spread across regions on activity
surge
and population basis to fund
costs
surge costs in both critical care
and ward beds
2022/23
$86.3m 1)
$5.3m
$81.0m
Surge as above. Agree timing of
workforce
new beds on regional basis to
initiatives
apply funding(2)
2023/24
$140.2m
Nil
$140.2m
Permanent uplift of 85 critical care
beds(3)
Outyears
$140.2m
Nil
$140.2m
Ongoing permanent uplift of 85
critical care beds(3)
(1) In 2021/22 and 2022/23, $1 mil ion has been al ocated to departmental expenditure to
RELEASED UNDER THE OFFICIAL
manage the delivery of the capital fund ($100 million)
(2) Optimally this would be beds resourced from 1 July (but could include others from later
dates)
(3) If regions decided to substitute medical ward beds for critical care beds, the total number of
beds would increase.
Document 9
e)
Note the transition in funding from surge funding to permanent funding
over Years 1 and 2.
f)
Agree to fully draw down the remaining $542.2 million from the “Raising
intensive care and inpatient capacity to meet COVID-19 demand” tagged
Yes/No Yes/No
contingency to give effect to the policy decision in recommendation d above,
exhausting this contingency.
g)
Approve the fol owing changes to appropriations to provide for that
decision, with a corresponding impact on the operating balance and net core
Yes/No Yes/No
crown debt:
$m - increase/(decrease)
ACT 1982
Vote: Health
2021/22 2022/23 2023/24 2024/25 2025/26 &
Minister of Health
Outyears
Non-Departmental Output
Expense:
Health and Disability Support
4 97
Services - Auckland DHB
Health and Disability Support
1.54
Services - Bay of Plenty DHB
INFORMATION
Health and Disability Support
2.70
Services - Canterbury DHB
Health and Disability Support
1.43
Services - Capital & Coast DHB
Health and Disability Support
6.36
Services – Counties-Manukau DHB
Health and Disability Support
1.02
Services - Hawke's Bay DHB
Health and Disability Support
0.77
Services - Hutt Val ey DHB
Health and Disability Support
0.67
Services - Lakes DHB
Health and Disability Support
1.03
Services - MidCentral DHB
Health and Disability Support
0.89
Services - Nelson Marlborough DHB
Health and Disability Support
1 25
Services - Northland DHB
RELEASED UNDER THE OFFICIAL
Health and Disability Support
0.35
Services - South Canterbury DHB
Health and Disability Support
1.74
Services - Southern DHB

Document 9
Health and Disability Support
0.33
Services - Tairāwhiti DHB
Health and Disability Support
0.67
Services - Taranaki DHB
Health and Disability Support
2.34
Services - Waikato DHB
Health and Disability Support
0 29
Services - Wairarapa DHB
Health and Disability Support
6.32
Services - Waitematā DHB
Health and Disability Support
ACT 1982
0 22
Services - West Coast DHB
Health and Disability Support
0.43
Services - Whanganui DHB
Delivering Hospital and Specialist
-
86.30
140.20
140.20
140.20
Services
Total Operating
35.30
86.30
140.20
140.20
140.20
h)
Note that funding in 2022/23 and outyears is being appropriated into the
INFORMATION
non-departmental output appropriation
‘Delivering Hospital and
Specialist Services’ that has been established as part of the Health and
Disability System Reforms from 1 July 2022 [HR 20212335 refers].
i)
Agree that the changes to appropriations for 2021/22 above be included in
the 2021/22 Supplementary Estimates and that, in the interim, the increase
Yes/No Yes/No
be met from Imprest Supply.
j)
Note that quarterly reports wil be provided to Ministers on progress towards
resourcing additional hospital capacity.
RELEASED UNDER THE OFFICIAL
Robyn Shearer
Hon. Andrew Little
Deputy Chief Executive
Minister of Health
Sector Support and Infrastructure
Date:
Document 9
Date:
Hon Grant Robertson
Minister of Finance
Date:
ACT 1982
INFORMATION
RELEASED UNDER THE OFFICIAL
Document 9
Introduction
1.
The practice of intensive care medicine (or critical care) involves caring for the sickest
and most badly injured patients. As the name implies, it involves concentrated support
for each patient, often requiring one-on-one nursing support over extended periods –
particularly if the patient needs mechanical ventilation to keep them alive.
2.
Critical care is provided in multiple settings, including ICU, HDU and paediatric and
neonatal ICU. Critical care staff also provide support to and assessment of patients in
hospital wards and co-ordinate and staff the transport of critical y il patients both within
and between hospitals.
3.
In addition to acute and urgent care, critical care manages a high volume of planned
ACT 1982
care patients (cardiac and others) who require specialised care immediately after their
surgery.
4.
In line with other areas of the health sector, critical care is unable to meet the increasing
demands of a growing and ageing population, increasing clinical complexity and the
improved ability to treat critically ill patients.
5.
Over the past ten years (to 2020/21), there have been over 200,000 admissions to critical
care units and over 13 mil ion hours of care across adult and paediatric units.
6.
In terms of activity through critical care units, the most common diagnoses relate to
INFORMATION
cardiovascular disease, traumatic injuries, respiratory and digestive diseases and tumours
(both malignant and benign).
7.
The majority of critical care is provided to patients over the age of 65. In terms of
ethnicity, Māori and Pasifika have relatively higher rates of utilisation of critical care – in
line with higher rates of admission to hospital general y. This reflects the higher health
needs of these groups and is positive from an access perspective.
8.
In April 2020, the OECD published a report titled “Beyond Containment: Health system
responses to COVID-19 in the OECD”. Included in this report were comparisons of both
intensive care and acute beds numbers across OECD countries. Comparisons between
OECD countries is not exact. Health systems, health funding, bed definitions and
counting and models of care are not standardised. However, the data suggests that
Aotearoa NZ is particularly low in ICU beds on a population basis. Published in January
2022, the OECD’s Economic Survey of NZ again identified the shortage of ICU capacity
and included in its first recommendation that this be addressed.
Current context
9.
In December 2021, capital expenditure funding of $100 million was announced to
support rapid hospital improvements to better manage COVID-19. As part of this
funding, 18 permanent and 8 temporary ICU/HDU beds, 5 cardiac care beds and 75
ward beds were to be commissioned.
RELEASED UNDER THE OFFICIAL
10.
At the same time, $544.2 mil ion was announced to fund increases in hospital bed
capacity, both on a surge and permanent basis.
11.
Since the beginning of the COVID-19 pandemic, DHBs have developed and maintained
plans for managing a surge in critical care patients. This has involved identifying areas
Document 9
within their hospitals where patients can be managed, increasing the number of
isolation rooms and upgrading airflow, managing stocks of ventilators and key
consumables and most importantly, training a range of staff who can support
experienced critical care personnel to manage patients.
12.
To support and inform this work, a Critical Care Sector Advisory Group (CCSAG) was
established in September 2021 and has been meeting regularly. In addition, during
2021 the Health Infrastructure Unit led a long-term service planning process to identify
critical care capacity needs, which also had significant sector and clinical input.
13.
This plan provides a robust basis for equitable investment in critical care across
Aotearoa NZ – to be co-ordinated on a regional level. The plan is based on ensuring
Aotearoa NZ has sufficient ICU/HDU capacity to maintain business as usual (BAU) plus
ACT 1982
meet future demand based on a growing aging population and the need to improve
equitable outcomes. This funding wil move the sector towards that goa
Proposal
14.
The aim of the funding is to lift the overal capacity of the hospital system, to allow it to
continue normal operations and lessen the effects on planned care, while stil responding
to surges/crises as they occur. It is acknowledged that the increment in capacity enabled
by this funding wil not eliminate the need for the system to prepare, train and redeploy
staff to respond to short term increases in service demand or crises. Winter res
INFORMATION piratory
il nesses and events such as Whakaari/White Island wil always require a specific and
targeted response. The Aotearoa NZ health sector has always responded well to these
situations.
Link to capital programme ($100 million) to support rapid infrastructure and capacity
improvements
15.
The 36 projects being funded in hospitals across the country include the development of
additional critical care and general ward beds – on both a surge and permanent basis. As
these come on-line, they will provide vital surge capacity and also allow improved
separation of COVID-19 patients, thereby reducing the risk of cross infection of other
patients and staff. This wil enable business as usual activity such as planned care
procedures to continue at an increased level.
16.
These beds wil be funded as required on a surge basis from the operating expenditure
in Year 1.
17.
Unless regions decide to apply funding to general inpatient beds rather than critical care
beds, none of the 75 inpatient ward beds nor 5 cardiac care beds being commissioned
under the Rapid Hospital Improvement Projects (RHIP) wil be directly funded through
this allocation.
18.
In addition, 16 of the 26 (temporary and permanent) critical care beds being
RELEASED UNDER THE OFFICIAL
commissioned through the RHIP wil not be directly funded. These beds wil be available
as surge capacity and wil be stood up as BAU beds as the population need increases
over time.
19.
With specific reference to critical care bed capacity across the country, there are already
a number of existing beds that are not funded across the country. Long term planning of
Document 9
capacity would suggest that while al beds being added through the RHIP fund wil be
required in the long term, permanent funding should be applied equitably across al
beds – both existing and new. Allocating beds on an equitable basis wil require some
infrastructure improvements that are not funded via the RHIP. However, confirmation has
been obtained that these modifications can be made on the same timeframes, so the
beds wil be available by 1 July 2023.
Transitioning from surge funding to permanent funding
20.
The Ministry has funded DHBs to train staff who can support experienced critical care
staff to manage COVID-19 patients. Further funding from this allocation will be utilised in
Year 2 to ensure new and refresher training continues.
ACT 1982
21.
In the short term, the focus for the surge funding in Year 1 will be on ensuring resources
can be applied to manage COVID-19 surges within hospitals and supporting the
additional staffing costs (backfilling, additional shifts, shifting staff between hospitals)
needed to deliver care.
22.
Therefore, the proposal includes a rephasing of funding between Years 1 and 2
(supported by Treasury), to account for the expected costs in 2021/22 relating to the
Omicron surge. The fol owing table shows the proposed shift in timing for the funding.
Year
Current phasing Proposed phasing Comments
of funding
of funding
INFORMATION
2021/22 $15.3m
$35.3m
All funding allocated as surge
2022/23 $106.3m
$86.3m
Mixture of workforce initiatives and
permanent funding
2023/24 $140.2m
$140.2m
All funding allocated to permanent uplift
Outyears $140.2m
$140.2m
All funding allocated to permanent uplift
23.
The full funding of $35.3 million in 2021/22 will be available to DHBs on a regional basis
to fund surge costs. It is proposed to al ocate 50 percent of the funding to the three
Auckland metro DHBs, as they have managed (and wil continue to manage) the majority
of COVID-19 patients requiring hospitalisation and al ocate the remaining 50 percent to
regions on a population-based funding formula.
24.
The COVID-19 financial tracker wil be enhanced to capture costs that can be identified
for reimbursement from this funding.
25.
As COVID-19 evolves to become endemic, preparedness for surges wil be managed in
the same manner as influenza, RSV, etc and therefore part of a hospital’s usual planning
processes.
26
The funding in 2022/23 wil be a mixture of workforce initiative funding ($5.3 million) and
funding ($81 million) for the first al ocation of permanent additional beds.
27.
The Ministry will work with regions to identify by 30 April 2022, the phasing and timing
RELEASED UNDER THE OFFICIAL
of the first tranche of additional beds across 2022/23, with a minimum of 45 beds
available by 31 December 2022.
28.
From 1 July 2023, al funding ($140.2 million) will be allocated to permanent additional
beds. The Ministry wil work with regions by 30 June 2022 to confirm the final allocation
of beds from 1 July 2023.
Document 9
Focus on critical care (ICU/HDU) beds
29.
As previously noted, the OECD report noted NZ as low in both acute beds and critical
care beds, but particularly low on the latter.
30.
Funding specific increases in general ward beds is more difficult as their staffing and
availability is regularly flexed to meet demand and patient acuity. The planning approach
used for ICU/HDU needs to also be applied more general y to ward beds, to inform
future system wide investment decisions in those areas.
31.
As it is proposed that the funding wil transition from surge funding to permanent
funding from 2023/24 onwards, the surge funding available in the interim periods will be
available to be applied across both ICU/HDU and ward beds. Regions wil also have the
opportunity to switch funding into ward beds if they can justify this as a higher priority.
ACT 1982
32.
Improving access to ICU/HDU beds also wil support improved flow and outcomes across
a wide range of hospital services. In particular, in tertiary centres where planned
procedures regularly require critical care post-surgery, it has been estimated that around
10 percent of major surgery has been postponed due to lack of an ICU/HDU bed.
33.
Applying the full funding (from 2023/24 onwards) to an increment in critical care
capacity (ca 85/ca 260 or around 30 percent) wil have a greater relative effect than
spreading it across ward beds (ca 320/ca 7500 or around 4 percent) due to the relatively
high cost of providing critical care beds, their discrete nature, and ease of counting.
INFORMATION
34.
The need for an increase in critical care capacity was identified well before the pandemic
but has received much attention in that light. Whether Omicron or future variants
(combined with new treatments etc) result in relatively fewer patients requiring critical
care does not eliminate the need for investment in this area.
35.
Long term planning suggests a population need of around 400 critical care beds by
2035/36 for business as usual (BAU) activity. This funding – if all applied to critical care –
wil ensure there is a 50 percent increment towards that number. Making this partial step
also al ows for a review of the planning before additional beds are added, to reflect
update population projections, patient flows and clinical practice changes.
36.
In this regard, the Ministry has engaged with interim Health NZ to ensure that this
proposal is in line with other long-term planning around location of services, links with
tertiary and quaternary services and equity considerations.
Resourcing the additional beds with a focus on nursing workforce
37.
Critical care patients require the most complex, intensive and costly care within the
health system. A range of staff groups from medical specialists through nursing to allied
health and administration are directly involved in the delivery of critical care. Patients
also access high volumes of radiology, laboratory services and pharmaceuticals.
Maintenance of high-tech equipment requires specialised staff as well.
RELEASED UNDER THE OFFICIAL
38.
While a number of the staff groups have ongoing shortages, it is deficits in nursing
rosters that has resulted in beds remaining unresourced.
39.
As part of COVID-19 funding announced in December 2021 for Care in the Community,
$10 million was allocated to workforce initiatives with $3.6 million specifically targeted to
Document 9
the critical care nursing workforce. This initiative funding is separate to this proposal,
which is to directly resource additional bed capacity.
40.
This funding has been al ocated for the period to 30 June 2022 to:
a. Support for the international recruitment campaign launched in February 2022 (the
initial campaign being funded by DHBs) – to provide candidate care and liaise with
DHBs. This funding also covers an evaluation process to inform future campaigns.
b. Additional educators and clinical coaches in critical care units across all DHBs – this
funding wil be al ocated on a regional basis.
c. Additional funding for postgraduate study for nurses completing courses related
to critical care.
d.
ACT 1982
Initiatives to encourage nurses to choose critical care as a career option.
41.
This proposal includes an allocation of $5.3 million in Year 2 to continue the initiatives
noted above, as well as seeking other opportunities to support nurses to train in critical
care and to potential y expand the initiatives to other staff groups – predominantly allied
health professionals – aligned to critical care.
42.
Phasing the permanent increase in critical care capacity over the period to 1 July 2023
will allow time for staffing numbers to be increased and therefore beds to be
appropriately resourced.
INFORMATION
43.
Until the allocation of beds across units is finalised and the mix of ICU and HDU beds is
known, the total number of additional nurses required to staff them is unclear. It is likely
that this number wil be 200-300 once al beds are operational. Recruiting to these
numbers may affect other services also seeking to recruit and retain staff.
Supporting change with enhanced data collection
44.
Historical y central y col ected data on critical care activity such as occupancy has been
ad hoc and intermittent.
45.
As part of ongoing work around both critical care and COVID-19 reporting, the Ministry
is mandating the use of the Critical Health Resource Information System (CHRIS), which
is run by the Australia and New Zealand Intensive Care Society (ANZICS). Most large (and
some smaller) units already provide data into this system on a daily basis.
46.
This system has been modified over time to col ect data on al hospital COVID-19
patients and ventilator use.
47
As well as providing access by way of personal logins for Ministry staff, a daily extract wil
be available to be used as a common data source. This wil also reduce the need for
DHBs to provide manual data, which is prone to human error.
RELEASED UNDER THE OFFICIAL
Calculating the cost of a resourced bed
48.
To identify the cost of a resourced critical care and general medical ward bed, a data
request was sent to DHBs asking them to provide both marginal and fully absorbed costs
for the different bed types.
Document 9
49.
While there was the anticipated range of costs across different levels of critical care beds
– relative to the complexity of the patient, the same was not the case for medical ward
beds.
50.
The range of costs is summarised in the table below.
Critical care bed
Tertiary DHB
Low
High
Average
Marginal cost
$1,424,813
$1,521,920
$1,474,831
Fully absorbed cost
$1,899,750
$2,175,785
$2,015,294
$1,745,063 Mid way
Medium DHB
ACT 1982
Marginal cost
$714,810
$1,281,442
$998,297
Fully absorbed cost
$940,933
$1,601,802
$1,291 418
$1,144,858 Mid-way
Small DHB
Marginal cost
$575,941
$911,337
$755,155
Fully absorbed cost
$735,638
$1,171,390
$968,561
$861,858 Mid-way
Medical ward bed
Low
High
Average
INFORMATION
Marginal cost
$178,779
$443,033
$300,851
Fully absorbed cost
$235,334
$590,711
$384,383
$342,617 Mid-way
51.
Based on relative size and populations, the majority of critical care beds wil be al ocated
to medium sized and tertiary (or similarly managed) units. Therefore, the funding
al ocation has been based on $1.75 million for a tertiary unit and $1.2 million for other
units.
52.
If a region decides to al ocate funding to ward beds rather than critical care, there is an
expectation that, based on funding of $350,000 per ward bed, either three or five ward
beds would be substituted for a critical care bed.
53.
While this funding represents only a marginal increase in the context of overal DHB
revenue, directly funding critical care beds al ows them to increase resourcing in other
areas.
54.
Funding critical care units at the higher end of the cost structure wil al ow them to build
capability as well as capacity. Critical care units deliver a range of services in addition to
patient care, such as flight co-ordination for patient transfers and outreach services into
general wards to support assessment of at-risk patients.
55.
Effective and efficient delivery of critical care is dependent on the ability to transfer
RELEASED UNDER THE OFFICIAL
patients quickly and safely to an appropriate unit. Regions wil need to consider this in
their deliberations over the location of additional beds. There is a long-term work
programme around the future delivery of pre and interhospital transfers and has not
been considered as part of this funding.
Document 9
Allocation of permanent additional beds
56.
The proposed al ocation is based on the fol owing principles:
a. The al ocation of surge funding in the short term wil be applied to hospitals on as
‘as needed’ basis, with an al ocation at a regional level.
b. The proposal for the permanent al ocation of funding wil be based on long term
service planning – this planning is currently only available for critical care capacity.
c. The new funding provides the ability to rebase capacity in line with the findings of
the national modelling work. Using an al ocation based on long term planning
addresses existing inequities across regions in the funding of critical care beds.
d. Al ocating the funding at a regional level al ows regions to consider their col ective
ACT 1982
capacity and determine a different view of priority investment in their region. This
may involve substitution of critical care beds for general ward beds.
e. The al ocation is in line with Health NZ’s recognition of and focus on the need to
configure capacity more effectively.
57.
The long-term service plan for critical care – undertaken by the Health Infrastructure Unit
in the Ministry – is based on historical utilisation, patient flows and patient
demographics. Using this baseline information, the plan uses population projections,
adjusts for such things as increasing length of stay and optimal occupancy rates and
INFORMATION
projects the need for critical care bed needs at a unit level out to 2035/36.
58.
The plan had significant input from critical care clinicians and other stakeholders during
its development.
59.
While the proposed al ocation uses his report as the basis for this interim stepped
increase in capacity, there have been some practical adjustments such as not decreasing
the number of beds from current capacity.
60.
The proposal uses currently funded beds as the baseline – not resourced beds –
acknowledging that DHBs have responsibility to resource beds to the level included in
their financial planning. Critical care units wil not receive their al ocated funding until
they can confirm that they are able to resource the beds on an ongoing basis.
61.
In proposing the al ocation, we have engaged with HNZ and they wil take leadership of
final allocations in 2022/23 and outyears and implementation of this initiative. However,
to give assurances around what this funding wil achieve, we can confirm that there wil
be a minimum of 85 additional critical care beds.
62.
The Ministry wil work with regions to identify the phasing of additional bed capacity
during 2022/23 – to ensure the $81 million available in that year is fully utilised.
63.
The proposed al ocation of beds to be funded on a permanent basis from 1 July 2023 at a
facility and regional level is at Appendix A.
RELEASED UNDER THE OFFICIAL
Consultation
64.
The fol owing groups have been consulted in determining the al ocation of this funding:
a. Interim Health NZ
b. The Treasury
Document 9
c. The Ministry’s Critical Care Sector Advisory Group
d. Other Ministry departments including the Health Infrastructure Unit, Health
Workforce, Finance and the Office of the Chief Clinical Officers
e. Regional CE leads on capital expenditure
f. All DHBs receiving funding for additional beds – either critical care or general ward
– from the $100 million capital funding.
Chal enges, risks and mitigation
Workforce – notably nursing
65.
ACT 1982
As is the case for al health sector providers currently, the key challenge for critical care
is the availability of staff – be that surge support or increasing the permanent
workforce.
66.
As previously noted, we have funded initiatives targeted at attracting new nurses to
critical care, attracting trained nurses to (and back to NZ) and supporting them
through their training. DHBs and the Ministry are also cons dering options to support
staff retention.
67.
Clear communication around funding intentions al ows DHBs to commit to recruitment
processes across al staff groups.
INFORMATION
68.
The Ministry wil work specifical y with DHBs that have a stepped increase in capacity,
to ensure they have appropriate plans to resource both staffing and other operating
costs as required.
Additional capital funding requirements
69.
As a result of the $100 million being specifical y targeted to COVID-19 related projects,
while the operating expenditure is aimed at equitable capacity increases, a number of
DHBs will need additional financial support to allow structural alterations, as well as
funding the purcha e of additional beds and related equipment.
70.
The Ministry will work with DHBs and (interim) HNZ to ensure that the 85 beds are
available by 1 July 2023.
Accountability and monitoring
71.
With the health reforms currently being implemented, the responsibility for allocating
funding and working with the DHBs to ensure the beds are available and resourced on
the timeframes outlined in this paper will shift to HNZ. Similarly, the accountability for
maintaining a minimum number of critical care beds and planning for future
requirements wil belong to HNZ.
72.
The Ministry wil ensure that there is joint governance over the planning and
RELEASED UNDER THE OFFICIAL
implementation of this funding allocation and that a smooth transition in oversight
occurs over the next few months.
Document 9
Appendix A: Proposed al ocation of additional critical care beds
Share of
Currently additional
Region
Facility
funded
beds New total
Northern
Whangārei
8
1
9
North Shore / Waitākere
14
4
18
Auckland CVICU
22
10
32
Auckland DCCM
17
9
26
Starship PICU
22
7
29
ACT 1982
Middlemore
18
4
22
101
35
136
Te Manawa Taki Tauranga
10
4
14
Whakatane
4
4
Rotorua
4
3
7
Gisborne
3
2
5
Taranaki
5
1
6
Waikato
28
1
29
INFORMATION
54
11
65
Central
Wellington
22
9
31
Hawke's Bay
11
3
14
Hutt
4
2
6
Palmerston North
6
1
7
Wairarapa
6
6
Whanganui
3
3
52
15
67
South Island
Christchurch
21
12
33
Nelson
7
7
Wairau
4
4
Timaru
4
2
6
Dunedin
9
10
19
Southland
6
6
Greymouth
4
4
55
24
79
Total
262
85
347
NB: additional physical beds – 4 at Waitematā, 3 at Coun
RELEASED UNDER THE OFFICIAL ties Manukau, 2 at Bay of Plenty, 9 at
Canterbury and 2 at Nelson Marlborough – are held as surge capacity and for long term need.

Document 10
Aide-Mémoire
Visit to Waikato District Health Board
Date due to MO: 21 March 2022
Action required by:
N/A
Security level:
IN CONFIDENCE
Health Report number: 20220505
To:
Hon Andrew Little, Minister of Health
Contact for telephone discussion
Name
Position
Telephone
Jess Smaling
Acting Deputy Director-General, DHB
S9(2)(a)
Performance and Support
Stuart Powell
Chief Advisor, DHB Performance and
Support

Document 10
Aide-Mémoire
Visit to Waikato District Health Board
Date due:
21 March 2022
To:
Hon Andrew Little, Minister of Health
Security level:
IN CONFIDENCE
Health Report number: 20220505
Details of the
Tuesday 22 March 2022
visit
8.00am-9.30am
Waikato Hospital
183 Pembroke Street
Hamilton
Organisation
Waikato District Health Board (DHB) serves a population of more than
425,000 and covers more than 21,000 km2. It stretches from northern
Coromandel to Mt Ruapehu in the south, and from Raglan on the west
coast to Waihi on the east. Fifty-nine percent of the population is
defined as living in urban areas, and 41 percent in rural areas. Twenty-
three percent of the population is Māori (compared to the national
average of 16 percent).
Purpose of the
On Tuesday 22 March, you are visiting Waikato DHB to meet with frontline
visit
staff and senior staff leading Waikato DHB’s COVID-19 response S9(2)(c)
Comment:
You will be accompanied by a staff member from your office. As per the
COVID-19 protocols only one staff member will be allowed to visit the
premises with you.
A run sheet for the visit is provided in Appendix One.
This aide-mémoire discloses all relevant information.
Jess Smaling
Acting Deputy Director-General
DHB Performance and Support
Aide-Mémoire: 20220505
1
Document 10
Briefing points to support your visit
1.
This briefing will support your visit to Waikato DHB. This is a fol ow-on from your visit on
17 December 2021 (HR 20212734 refers). It provides an opportunity to observe on the
ground pressures to respond to COVID-19 and S9(2)(c)
2.
During the visit you may like to:
a. Thank the people you meet for their ongoing mahi and their resilience.
Waikato District Health Board
3.
Dame Karen Poutasi has been Commissioner at the DHB since May 2019, when then
Minister of Health, Hon Dr David Clark, ordered the replacement of the Board. Dame
Karen works with two Deputy Commissioners, Chad Paraone and Emeritus Professor
Margaret Wilson. Mr Ken Whelan was appointed to the role of Crown Monitor at Waikato
DHB in August 2018, and the appointment was extended in February 2021 to an open-
ended term.
4.
Waikato DHB’s YTD results for the eight months ended 28 February 2022 is a deficit of
$5.3 million against a YTD budgeted deficit of $8.5 million. The underlying BAU deficit net
of Covid-19 surpluses and the impact of uninsured cyber-attack costs is a net deficit of
$9.8 million. The DHB is forecasting to end the current financial year with a net deficit well
below its budgeted deficit of $30 million (BAU).
5.
Waikato DHB has five infrastructure projects with approved Crown funding totalling $111
million. The Wairora building seismic upgrade and Farmers building projects are classified
S9(2)(f)(iv) by the Health Infrastructure Unit (HIU) and are on track. The Linear Accelerators,
Tokoroa Hospital reconfiguration and Adult Mental Health Facility projects are classified as
S9(2)(f)(iv) by the HIU and risk mitigations are in place. A business case for the Linear
Accelerators was received in January 2022 and a Health Report is being prepared for the
Director-General of Health’s approval. A concept plan was agreed in December 2021 for
the Tokoroa Hospital reconfiguration and project deliverables have been established. The
DHB is preparing the Adult Mental Health Facility detailed business case and is on track
for the Capital Investment Committee consideration in the April 2022 meeting.
6.
The Waikato DHB 2021/22 Annual Plan was signed by joint Ministers on 30 September
2021.
7.
A summary of key service performance indicators for Waikato DHB shows the fol owing:
As of 13 March 2022, the cardiac waiting list is within the total maximum waiting
with 64 patients listed for surgery (total maximum waiting target 75). 13 out of 64
patients are waiting outside their expected treatment timeframes.
Emergency Department (ED) - 67.1 percent of patients (target 95 percent) are being
admitted, discharged or transferred within six hours. The DHB has been below 70
percent for most of the last two quarters of 2021.
Planned Care Interventions are at 100.0 percent delivery against plan with 93.9
percent inpatient surgical discharges and 96.3 percent caseweights.
Aide-Mémoire: <HR#>
2
Document 10
ESPI 2 - 22 services are not meeting ESPI 2 (First Specialist Assessment)
expectations, with 4,252 patients waiting longer than four months.
ESPI 5 - 15 services are not meeting ESPI 5 (Treatment) expectations, with 2,054
patients waiting longer than four months.
CT performance - 69.4 percent of patients waiting less than six weeks for their scan
against a 95 percent target. The DHB has been below target the last 12 months.
MRI performance - 61.5 percent of patients waiting less than six weeks for their scan
against a 90 percent target. The DHB has been below target the last 12 months.
Improvement Action Plan (IAP) Funding - Waikato DHB have an approved IAP which
is addressing part of the waiting lists in orthopaedics, improving waiting list
management, and the commencement of extra clinics on weekends to reduce long
waiters.
8.
You may like to take the opportunity to:
a. Thank them for achieving 96% of expected Planned Care caseweighted discharges in
this extremely challenging environment.
b. Discuss the chal enges of ensuring patients that need to be seen or treated urgently
continue to receive their services whilst dealing with the Omicron surge.
9.
The DHB has been part of the Ministry of Health’s (the Ministry) Intensive Support
Programme since April 2021 and is progressing an intensive support plan which covers
the following areas:
Mental Health and Addictions Implementation programme in response to the
recently completed ‘Waikato Mental Health and Addictions System Review’.
Reduction of child and adolescent mental health services waiting times.
Financial sustainability initiatives.
Development of more integrated community and primary care services.
COVID-19 Response
10.
Across the Te Manawa Taki Region (Waikato DHB, Taranaki DHB, Lakes DHB, Bay of Plenty
DHB and Tairawhiti DHB) all the five DHBs have worked well via their Care in Community
hubs to support people and their whānau with COVID-19 and to ensure an equitable
response.
11.
The region reports workforce and capacity as their primary pressure point. This is due to
staffing shortages, increase in sick leave being taken, inability to recruit and to staff
leaving due to workload pressures noted as a factor. The workforce issue is raised across
the full continuum of care – primary care, hospital services, vaccination and testing
programmes, older persons care, disability support services, pharmacy and mental health
and addiction services.
12.
The region also expressed concern that the initial Self-Assessment form that COVID-
positive patients are asked to fill out is too long and will further compound equity issues.
The Ministry at the beginning of March 2022 reduced the length of the form which now
takes on average five-ten minutes to fill out. Continuous improvements are being done to
make the form more user friendly.
Aide-Mémoire: <HR#>
3
Document 10
13.
In addition, the region is concerned about the rol out, implementation, training and
delivery timeframes of the data and digital space. The upgrades were difficult to keep up
with and created a lot of manual work in-between the changes. The concern was that
whānau may ‘fall through the cracks’. In response to these concerns the Ministry has:
A team dedicated to support the implementation of the data and digital solutions
available for care providers and the community care hubs. The team provides a
range of drop-in sessions for end users and hubs, regional education sessions, GP-
specific education and regular updates on data and digital changes and upcoming
enhancements.
Conducted a review of all the hubs to ascertain their level of preparedness, take
learnings from other hubs and align possible regional and localised solutions.
Conducted several sessions to address issues relating to technology access and
reporting needs.
Recruited four Regional Health Liaisons who coordinate the preparedness and
operations of the response, share lessons learned and continually review and
streamline processes.
14.
RATs col ection sites and provider channels are enabling at least 94.8% of the population
to access RATs within a 20 minute drive.
15.
RATs are being provided into the Waikato community via the collection sites and Tainui
Waikato is providing a parallel channel into community providers and their communities.
Tainui Waikato is part of a National Māori Provider Distribution Channel supporting the
distribution of RATs to Māori and vulnerable communities. The Ministry stood this up
three weeks ago to advance equitable access for Māori and prioritised populations.
16.
Pacific Health & Disability Providers now have access through several channels to order
supply of RATS and PPE from the Ministry and pul from the DHB’s and the Māori
Providers Distribution Channels.
17.
PPE supply has suffered from the domestic freight and courier challenges due to
absenteeism caused by the outbreak. Recent feedback to the Ministry is that PPE is
flowing into the providers.
18.
Throughout the visit you may like to take the opportunity to ask:
a. What are the things that are working wel , that we absolutely need to continue doing,
and what are the things that are working less wel , that we need to resolve?
19.
Throughout the visit you may like to comment that:
a. People are working in an extremely dynamic and demanding environment and that
you recognise the chal enges that places on, not just them and their col eagues, but
also their loved ones and wider whānau.
b. You acknowledge staff fatigue at this time and thank staff who have stepped up to fill
some of the critical roles.
Aide-Mémoire: <HR#>
4
Document 10
COVID-19 Situation Update
20.
As of 20 March 2022, Waikato DHB reports1
a.
1339 new community cases
b. 10,449 active cases
c.
93.5% of the population is fully vaccinated
d. 68.6% of the population aged 18 and over has received a booster dose
e. 83 cases are in the hospital
f.
4 cases are in ICU/HDU
S9(2)(c)
1 https://www.waikatodhbnewsroom.co.nz/2022/03/20/covid-19-public-advisory-20-march-2022/
Aide-Mémoire: <HR#>
5
Document 10
S9(2)(c)
25.
You may like to take the opportunity to ask:
a. If there are any ongoing clinical and operational chal enges they face after resuming
normal operations?
26.
You may like to take the opportunity to:
a. Thank them for progressing the remediation programme in this chal enging
environment.
b. Thank staff for their effort during the incident and continuing to provide services to
the community and the Te Manawa Taki region.
END.
Aide-Mémoire: <HR#>
6
Document 10
S9(2)(f)(iv)
Aide-Mémoire: <HR#>
7