 From:
From:
Lydia Verschaffelt <[email address]>
Sent:
Friday, 13 August 2021 1:55 pm
To:
[email address]
Subject:
FW: Formal Complaint from NZDSOS
Attachments:
RESPONSE-TO-MEDSAFE_FINAL-PDF.pdf; Re: Response to your correspondence from Minister
Hipkins (CH203993); Formal Complaint from NZDSOS; CH203993.pdf
Kia ora
We just wanted to pass on the correspondence that Minister Hipkins has received from the below group, NZDSOS.
We understand that you’re likely very aware of this group already. They wrote to several Members of Parliament
and the Minister has provided a response but will not be engaging further. The Ministry of Health has offered to
discuss the group’s concerns with them and we just wanted to ensure the Council is aware of this dialogue.
Have a good weekend.
Ngā mihi,
Lydia
Lydia Verschaffelt |
Health Private Secretary
Office of Hon Chris Hipkins Minister for COVID‐19 Response | Minister of Education | Minister for the Public Service | Leader of the House
Parliament Buildings, Private Bag 18041, Wellington 6160, New Zealand
From: NZ Doctors Speak Out with Science [mailto:[email address]]
Sent: Friday, 6 August 2021 11:06 PM
To: Ashley Bloomfield <[email address]>
Cc: A Little Office (MIN) <[email address]>; C Hipkins (MIN) <[Chris Hipkins request email]>; Rt Hon Jacinda
Ardern <[email address]>; Chris James <[email address]>
Subject: Formal Complaint from NZDSOS
Dear Dr. Bloomfield;
Further to our previous email please find attached the document titled "
Rebuttal to Prof. P. McIntyre and
Dr. Ian Town response to NZDSOS concerning Pfizer Comirnaty"
The document can also be downloaded from our website:
https://nzdsos.com/wp-content/uploads/2021/06/RESPONSE-TO-MEDSAFE_FINAL-PDF.pdf
Steering Committee – NZDSOS
Matt Shelton, Tracy Chandler, Cindy de Villiers, Mark Bailey, Jacques Imbeau, Simon Thornley, Tessa Jones.
1

Sent with ProtonMail Secure Email.
2
 Rebu%al to Prof. P. McIntyre and Dr. Ian Town response to NZDSOS
concerning Pfizer Comirnaty
Rebu%al to Prof. P. McIntyre and Dr. Ian Town response to NZDSOS
concerning Pfizer Comirnaty
On June 14 2021 Mr. Chris James from Medsafe replied to NZDSOS:
“Dear NZ Doctors Group
Thank you for your recent emails providing your views on COVID-19, COVID-19 vaccines and
therapeuMc opMons.
In response to the scienMfic and evidence base aspects of your correspondence I have asked Dr Ian
Town, Chief Science Advisor Ministry of Health, for advice. Please find aSached a copy of the
expert advice commissioned by Dr Town.
This response does not address the issues detailed in your leSer to MCNZ. We will leave you to
discuss these with the Medical Council directly.
Dr Town is happy to discuss any aspects of the aSached informaMon if you wish to.
Kind regards
Chris”
Copy of the document Mtled
COVID Issues Rebu%al_FINAL.pdf is aSached
-------------------------------------------
NZDSOS has considered carefully the comments from Professor McIntyre and Dr. Ian Town, who
we will refer to as the “authors” when not specifically addressing them by name. We have found
significant deficiencies in their argument. Below we explain why.
On the exaggerated disease burden and comparison with influenza
The authors refer to a Lancet arMcle 1 which compares hospitalised cases of COVID-19 to
hospitalised cases of influenza from earlier years, and finds a relaMve risk of death 2.9 Mmes higher
in the COVID-19 compared to the influenza paMents.
There are several reasons that this arMcle is unsuitable for comparing the fatality of COVID-19 from
influenza. This arMcle does not address the issue of the infecMon fatality raMo for individuals at a
populaMon level of exposure to the virus. The comparison of age fatality does not compensate for
the poorer metabolic profile of the covid-19 paMents who have twice the prevalence of overweight
and obesity than the influenza group. In addiMon, a study over the same period showed that early
venMlaMon in French paMents, a policy in some centres at the Mme, resulted in a 74% increase in
mortality for those who were venMlated early compared to those venMlated at higher levels of lung
dysfuncMon. 2 This finding was similar to that demonstrated in the UK 3 and was also confirmed in
interviews with North American intensivists. 4 It is, therefore, now clear that at least some of the
high mortality observed early in the COVID-19 crisis was due to over treatment, rather than the
virus itself. The authors make no menMon of this in their response.
It is also now widely recognised that the early infecMon fatality rates of COVID-19 published by the
World Health OrganisaMon were overstated, as they were confused with case-fatality rates and
inappropriate comparisons of staMsMcs were made. 5 The authors claim that Ioannidis does not
make a comparison directly with influenza, yet he does in one paper cited by our group. 6
“
At a very broad, bird’s eye view level, worldwide the IFR [infec:on fatality rate] of COVID-19 this
season may be in the same ballpark as the IFR of influenza (0.1%, 0.2% in a bad year).”
The authors claim that our group has mis-represented Ioannidis’ studies. It is clear, however, that
this is implied by his work, as Ioannidis himself states.
On the Safety and efficacy of COVID-19 vaccines
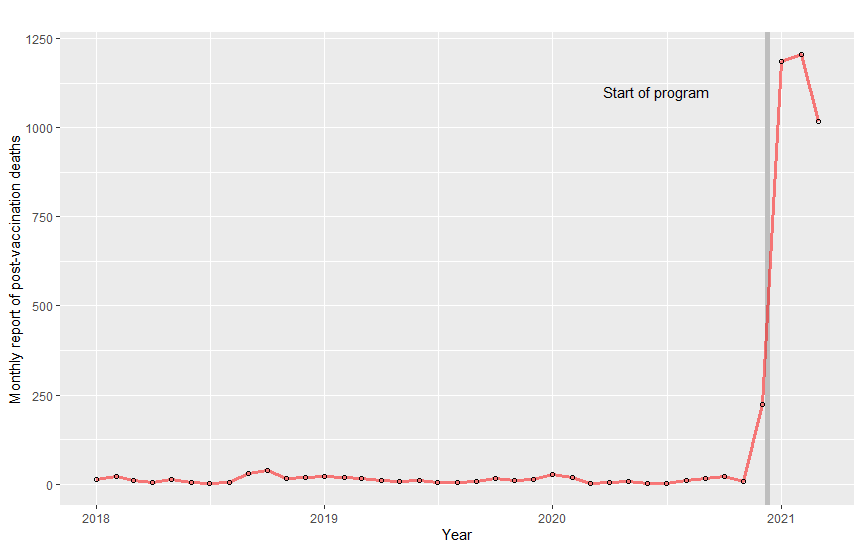
The VAERS database has had a 100-fold increase in the monthly incidence of post-vaccine deaths,
compared with earlier trends (
Figure 1).
Figure 1. Line plot of monthly counts of post-vaccinaMon death reports from VAERS (all ages,
2018 to present). VerMcal line indicates start date of US covid-19 vaccinaMon programme.
In line with our groups concerns, the authors dismiss this trend as aSributable to the majority of
vaccines occurring in subjects over the age of 65 years who are themselves at increased risk of
death.
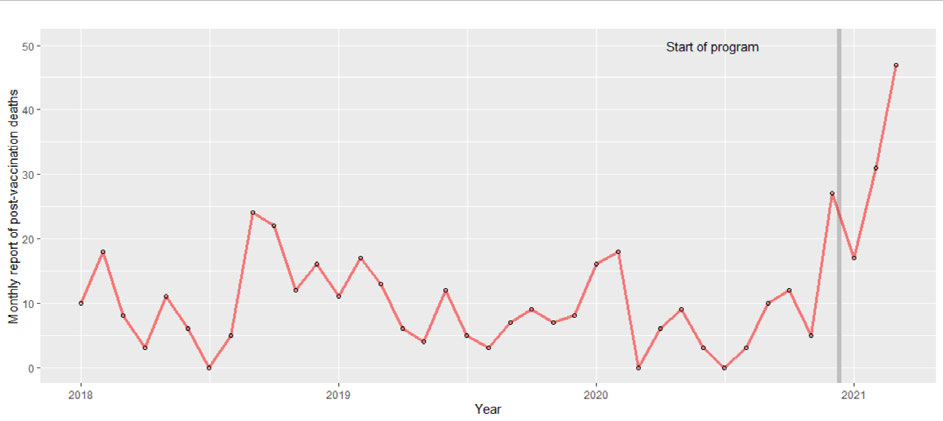
Trends of increased reports of post vaccine deaths are occurring in people who have received the
COVID-19 vaccine younger than 65 years, with a spike of deaths, five-fold higher than compared to
background observed in people aged 0 to 45 years aier COVID-19 vaccine, compared to
background monthly rates (
figure 2). Although many more people have been vaccinated in 2021
than in earlier years, people under the age of 45 years are at extremely low risk of sudden death,
and a five-fold increase must surely be cause for concern and warrant further invesMgaMon and
cauMon in recommending vaccinaMon to younger age groups. Although, we acknowledge that
VAERS is an early warning system, and the system accepts all reports made to it, it surely must now
be clear that this early warning system has sounded, and that further invesMgaMons must be made
to improve public confidence in vaccine safety. Considering the extremely low fatality of COVID-19
for this age group (~50/100,000 or 0.05%) 7, any harm aSributable to the vaccine for this younger
age group deserves close scruMny. EsMmates also show systemaMc under-reporMng of adverse
effects, when VAERS reporMng rates are compared to the results of controlled studies. 8
The authors lack of concern in these warning signals reflects what we believe is an overwhelming
belief on behalf of the government and aligned academics in the safety of the vaccine despite data
indicaMng otherwise. This refusal to acknowledge such trends underscores why we as pracMMoners
have wriSen the leSer outlining our concerns to the government that such warning signals are
being ignored.
The authors also fail to acknowledge that earlier catastrophic predicMons about COVID-19 have not
materialised. InsisMng that COVID-19 is a much greater threat than it actually is can only serve to
insMll fear in the populaMon and jusMfy drasMc measures that otherwise could not be sustained.
The Ministry of Health has consistently avoided any public menMon of any evidence that could help
reduce fear of COVID-19 and has acMvely worked at undermining and suppressing any valid
alternaMve treatments that could both help further reduce the morbidity of COVID-19 and negate
the validity of provisional consents/emergency use authorisaMon for the experimental mRNA
vaccines.
Figure 2. Line plot of monthly counts of post-vaccinaMon death reports, aged less than 45 years
from VAERS (2018 to present). VerMcal line indicates start date of US COVID-19 vaccinaMon
programme.
The authors then assert that the vaccine has saved lives from COVID-19 by comparing projected
deaths in the UK with observed. This is not convincing evidence, since modelled projecMons of
deaths from COVID-19 have been consistently inaccurate throughout the pandemic. 9 The best
informaMon from trials does not show a convincing benefit for reduced overall mortality or
COVID-19 deaths from the vaccine. 10 In fact, since the manufacturers of vaccines themselves state
that since death from COVID-19 is so rare, such a trial that examines this issue will be prohibiMvely
expensive and not feasible. 11 It is concerning that the government is relying on extremely weak,
speculaMve evidence to indicate that the Pfizer vaccine will prolong survival as a result of its use.
Asser@on that there is “no evidence of adverse effects” from the vaccine
The authors assert that there is ‘no evidence of adverse effects’ from the vaccine. This posiMon is
not consistent with even the trial evidence which highlighted several severe adverse events in the
experimental group. Considering the trends in VAERS data and Eurosurveillance, surely the
government’s posiMon cannot be so naïve? Importantly, the Norwegian Health authoriMes have
concluded that the Pfizer vaccine was likely to be responsible for a cluster of deaths in rest home
residents early in their vaccine programme. 12 Others have noted case-series of vaccine induced
thrombosis and thrombocytopenia aier the COVID-19 Pfizer and AstraZeneca vaccines. 13 A recent
pre-publicaMon release from the Official Journal of the American Academy of Pediatrics reports on
seven cases of acute myocardiMs or myopericardiMs in healthy male adolescents who presented
with chest pain all within four days aier the second dose of Pfizer-BioNTech COVID-19 vaccinaMon.
14
While the link between these adverse events and the vaccine has not been definiMvely established,
it is worrying that this is not raised at all by the authors in their bold claim of no evidence of
adverse events from the vaccine. Clearly the VAERS data and emerging case-series are signals that
the safety of these products should be closely examined and risk-benefit analyses carried out.
On concerns about other poten@al adverse effects:
1- O
n the concern that permanent altera:on of DNA may occur.
The science on this is sMll unfolding and we are concerned that the authors claim a definiMve
statement on this topic. The first reference the authors provide is the Centers for Disease Control
and PrevenMon website which is aimed at providing the public with a simple overview of the
mRNA injecMon. The second reference (and diagram) only shows the “
proposed sequence of
events leading to the generaMon of adapMve immune responses upon mRNA vaccinaMon”. From
this the authors appear to conclude that it would be impossible for the injected mRNA to become
integrated into our DNA because mRNA does not work that way. A study published in the 25 May
2021 by MIT and Harvard scienMsts 15 didn’t prove specifically that the mRNA from the current
COVID-19 vaccines is being integrated into our DNA but it did show, quite convincingly, that a
viable cellular pathway exists whereby snippets of SARS-CoV-2 viral RNA could become integrated
into our genomic DNA. A more recent publicaMon has also revealed that human cells can write
RNA sequences into DNA. 16 As stated by Richard Pomerantz, PhD, associate professor of
biochemistry and molecular biology at Thomas Jefferson University, the study “will help us
understand the significance of having a mechanism for converMng RNA messages into DNA in our
own cells.” 17
Clearly further research is needed on this topic before injecMng people with an experimental gene
therapy that could alter the recipient’s DNA.
2-
On the concerns about immune suppression and exaggerated ac:va:on from pathogenic
priming, ADE and vaccine interference.
This concern was clearly idenMfied by a plethora of mRNA vector researchers and scienMsts and
was the subject of a published paper in early mid 2020 18:
“Because some Middle East respiratory
syndrome (MERS) and SARS-CoV-1 vaccines have shown evidence of disease enhancement in some
animal models, this is a par:cular concern for SARS CoV-2 vaccines…Con:nuous monitoring of this
risk during clinical trials in an epidemic context will be needed."
It is far from reassuring that this issue is being currently studied and monitored during the ongoing
clinical trials scheduled to end in May 2023. The point we are making is simple: the people of New
Zealand are not experimental subjects to study a novel vaccine based on gene therapy. At the very
least if they are to be enrolled in a massive clinical trial it should be clearly disclosed, the risks
explained and parMcipaMon should be enMrely voluntary, free of any propaganda and/or coercion,
implied or otherwise.
3-
Concerns about the spike proteins causing endothelial cell mitochondrial damage.
The authors menMon that the quoted study refers to endothelial cell damage by infecMon, not
vaccinaMon. They then state that “
In human mRNA vaccine recipients, spike protein is produced
intracellularly through mRNA transcrip:on in the ribosome and then displayed on the surface of
the an:gen presen:ng cell to induce B cells to produce an:body to spike protein – this is en:rely
different and protec:ve.” They fail to take into account recent evidence demonstraMng that spike
proteins produced by human host cells via mRNA coding do not remain “
displayed on the an:gen
producing cell” but can be released and rather freely circulate in the blood of individuals who have
received one or two mRNA injecMons. Free SARS-CoV-2 Spike Protein S1 ParMcles that allows the
spike proteins to bind to ACE-2 are also present. We quote the researcher of this recently
published study: “
We hypothesize that the cellular immune responses triggered by the T-cell
ac:va:on, which would occur days a]er the vaccina:on, lead to the direct killing of cells
presen:ng spike protein and an addi:onal release of spike into the blood stream. The mechanisms
underlying release of free S1 and the subsequent detec:on of the intact spike protein remain
unclear and require further studies.” 19
Recently disclosed Pfizer animal studies 20 have shown that surrogate lipid nanoparMcles (LNP-
mRNA) were not only found at the injecMon site but also in various organs of test animals,
including the liver, the ovaries, adrenal glands, spleen etc... This means that various types of cells,
in addiMon to muscle cells, could be induced to produce spike proteins following the injecMon. If
the same thing happens in vaccinated humans and these cells are then destroyed by the immune
system of the vaccinee, this would explain freely circulaMng spike proteins and S1 aier injecMon of
Comirnaty.
Again a definiMve statement by the authors is being quesMoned by recent research.
4-
Concern about ‘the concept of shedding (presumably of spike protein) a]er vaccina:on,
affec:ng unvaccinated bystanders, par:cularly in the form of hormonal disrup:on and/or cloang
abnormali:es in females of all ages’.
The authors are quick to dismiss the possibility of shedding as not scienMfically credible. They also
dismiss the possibility of environmental exposure to the study intervenMon (mRNA encapsulated in
lipid nanoparMcles - LNPs) as menMoned by the manufacturer as “rouMne part of good clinical
pracMce guidelines for phase 1 and 2 studies and does not imply any concern about transmission.”
We have shown earlier evidence of wide biodistribuMon of the LNPs in the Pfizer animal study. We
have also explained that the spike proteins and S1 are freely circulaMng in the blood stream aier
injecMon with mRNA.
So what is the level of certainty with regards to the possibility of environmental exposure?
Is the hypothesis that NLP and the spike proteins freely circulaMng in the blood stream of
individuals who have received the vaccine, could possibly be excreted in bodily fluids such as
saliva, sweat, semen and breast milk, far-fetched?
Can we summarily rule out that credible hypothesis simply because of the lack of knowledge due
to the lack of proper research?
In Pfizer PF-07302048 (BNT162 RNA-Based COVID-19 Vaccines) Protocol C4591001 21 on pages
67-68 the manufacturer took specific precauMons to exclude pregnant woman in the following
situaMons:
“
•A male par:cipant who is receiving or has discon:nued study interven:on exposes a female
partner prior to or around the :me of concep:on.
A female is found to be pregnant while being exposed or having been exposed to study interven:on
due to environmental exposure. Below are examples of environmental exposure during pregnancy:
• A female family member or healthcare provider reports that she is pregnant a]er having been
exposed to the study interven:on by inhala:on or skin contact.
• A male family member or healthcare provider who has been exposed to the study interven:on by
inhala:on or skin contact then exposes his female partner prior to or around the :me of
concep:on. “
And
Exposure During BreasYeeding:
An exposure during breasseeding occurs* if:
•
A female par:cipant is found to be breasdeeding while receiving or a]er discon:nuing study
interven:on.
• A female is found to be breasdeeding while being exposed or having been exposed to study
interven:on (ie, environmental exposure). An example of environmental exposure during
breasdeeding is a female family member or healthcare provider who reports that she is
breasdeeding a]er having been exposed to the study interven:on by inhala:on or skin contact.
*Note that Pfizer does not say exposure “
could” or “
may occur”, they rather state that exposure
“
occurs”.
Whether or not Pfizer was simply following good clinical pracMce guidelines (as claimed by the
authors) and had no concern about transmission cannot be definiMvely determined by reading the
above excerpts from the trial protocol. However, in light of other scienMfic evidence discussed
above, the wording is clearly jusMfied.
5-
Concern that ‘through molecular mimicry of synci:n-1, and with reports of increased
miscarriages, there is concern in pregnancy and for fer:lity’.
There remains significant concerns for ferMlity and pregnancy due to the large number of
uncertainMes surrounding the mRNA injecMons. We believe it was a gross oversight by the
European Medicines Agency’s Assessment report about Comirnaty 22 where they stated that,
“
Several literature reports indicate that LNP-formulated RNAs can distribute rather
nonspecifically to several organs such as spleen, heart, kidney, lung and brain. In line with this,
results from the newly transmifed study 185350, indicate a broader biodistribu:on pafern with
low and measurable radioac:vity in the ovaries and testes,” but then dismissed safety concerns
based on, “the absence of toxicological findings in gonads” and the relaMvely low concentraMons
found in the gonads.
The Pfizer biodistribuMon studies themselves were not included in the EMA’s report and have only
recently been disclosed. FerMlity issues remain a serious concern as the studies reveal that
distantly injected mRNA can indeed reach the gonads.
Any mRNA reaching the gonads (and/or
uterus) with subsequent generaMon of spike proteins is a concern, hence the implicaMons for the
effects on human ferMlity for both males and females remains unknown at this stage. AddiMonally
there were no biodistribuMon studies done with the actual Pfizer injecMon being administered to
humans.
Similarly, there ought to have been proper clinical trials to rule out possible effects on the syncyMn
proteins that
do share a remarkable homology with the SARS spike protein. These placental
implantaMon and immune-suppressing proteins are themselves the result of viral inserMons into a
common mammalian ancestor aeons ago (HERV-W, the human endogenous retrovirus W). Some
work has been done in animals proving the effects of interfering with these proteins, but Pfizer and
Moderna are only now running studies in pregnant women. InteresMngly they are only recruiMng
women from 24 weeks, well aier successful syncyMo-trophoblasMc aSachment has successfully
occurred. Of course, the results will be in only aier the women have delivered their babies,
reminding of the adage “absence of evidence of harm is not evidence of absence of harm.”
We discuss this further in point 10.
6-
Concern about ‘the poten:al for autoimmune reac:ons, or impaired or exaggerated infec:on
responses, years a]er vaccina:on that short or even medium-term trials would not disclose’.
By definiMon the authors cannot possibly have any knowledge about these potenMal long-term
responses. These are ongoing clinical trials and no long-term data is now available. 23 It is unclear
why they refer to an Australasian Society for Clinical Immunology and Allergy guide sheet as the
ASCIA also have no possible knowledge of any long term data. It is equally unclear why the authors
refer to a study in mice where they claim, “
mRNA vaccines may offer benefit in the treatment of
mul:ple sclerosis.” The mouse study involved induced experimental autoimmune
encephalomyeliMs and is not relevant to the concerns that we have raised about potenMal long-
term immunopathology in humans.
7-
Concern about ‘the poten:al for spike protein-as-prion disease’ in the distant future.
While we accept that Classens asserMons lacks validaMon from peers, we find quesMonable the use
of VegSource.com and Facebook as validaMon for their dismissal of Classen's concerns about
potenMal prion pathology.
8-
Concern that ‘vaccinated people may not have prolonged or broad-based immunity, including to
the many new variants of concern, and have higher death rates when exposed’.
The authors suggest that “
protec:on from the vaccine against severe disease to the variants is well
preserved” however a published study by researchers from Pfizer has shown that vaccine
effecMveness is reduced for many of these variant strains. The vaccine was only 2/3 as effecMve
against the South African strain as against the original strain 24 and Pfizer CEO, Albert Bourla, said
on 15 April 2021 that while more research is needed, it is likely that people who receive Covid-19
vaccines will need booster shots within a year aierward, and then annual vaccinaMons, to
maintain protecMon against the virus as it evolves. 25
The medical media is awash with reports of so-called ‘breakthrough cases following vaccinaMon’
and in April 2021 the CDC has moved to issue instrucMons that PCR tesMng of possible cases in the
vaccinated is to use a cycle threshold of up to 28 only, here: hSps://www.cdc.gov/vaccines/
covid-19/health-departments/breakthrough-cases.html . This would seem a clear aSempt to
minimize cases, given the ‘standard’ cycle thresholds used have been from 35 to 45. Further they
have now stopped even recording these cases, unless they result in hospitalisaMon or death. This
cannot allow for valid comparisons and can only be seen as a plan to falsely aSribute lower “case”
numbers to the vaccines.
9-
Concern that ‘the symptoms, oxida:ve stress and inflammatory phenotype of “long covid”
syndrome may be produced solely by the spike protein, without presence of whole virus’.
There are valid concerns regarding spike protein toxicity. Yuichiro Suzuki et al presented a strong
argument that the spike protein by itself can cause a signaling response in the vasculature with
potenMally widespread consequences. 26,27,28 Furthermore, they suggested that a similar effect
could happen in response to the mRNA vaccines, and they warned of potenMal long term
consequences for both children and adults who received COVID-19 vaccines based on the spike
protein. 29 The S1 subunit can promote loss of barrier integrity, suggesMng that the spike protein
acMng alone triggers a pro-inflammatory response in brain endothelial cells. 30
We would be remiss to highlight the lack of knowledge by the authors on this issue. ExpectaMons
based on assumpMons cannot be enough to brush aside valid concerns.
10-
Concern that ‘the effects on children (two reports on VAERS of deaths of young children in
clinical trials), pregnancy, fer:lity, the elderly and infirm, interac:ons with medica:ons, other
chronic condi:ons, have not been studied’.
The authors provide no reassurance that the experimental vaccines have been studied in these
groups and concede that, “
it is true that evidence is only accumula:ng now about COVID-19
vaccines including Comirnaty when given to people with a range of chronic condi:ons including
immunocompromising condi:ons, pregnant women and those who are very frail.” However they
proceed to make the sweeping claim that, “
the benefits of vaccina:on have been universally
determined to greatly exceed the risks.” They go on to say, “
A]er hundreds of millions of doses, no
evidence of adverse effects has emerged.” Neither of these claims are backed up with suitable
evidence.
There is evidence that the COVID-19 vaccine can cause damage, as discussed above. The potenMal
impact on male ferMlity of the spike protein generated endogenously by the vaccine could also
negaMvely impact the male testes, as the ACE2 receptor is highly expressed in Leydig cells in the
testes. 31 Several studies have now shown that the coronavirus spike protein is able to gain access
to cells in the testes via the ACE2 receptor, and disrupt male reproducMon. 32,33 A paper involving
postmortem examinaMon of tesMcles of six male COVID-19 paMents found microscopic evidence of
spike protein in intersMMal cells in the testes of paMents with damaged tesMcles. 34
We argue that our analysis provided above of the virulence of the virus (very low) and the
alarming spike in VAERS deaths leads to the complete opposite conclusion and the COVID-19
vaccines should be proscribed immediately unless for experimental use with full informed consent.
Therapies for COVID-19 that may prevent or successfully treat disease
The authors reject the descripMon of mRNA vaccines as gene therapy when it has been shown that
it is quite possible for RNA to be reverse transcribed into the DNA of the host cell. The syntheMc
mRNA itself is based on geneMc technology. Their denial that it is a gene therapy is also in
contradicMon to common parlance as the largest online open source encyclopaedia clearly lists
mRNA as a subtype of gene therapy including reference to BioNTech products. 35
The definiMon of gene therapy is rapidly evolving to include mRNA gene therapy, regardless of its
ability to be reverse-transcribed into cell DNA.
The severity of COVID-19 compared to influenza has been discussed above.
While the authors repeat the usual informaMon provided by authoriMes and their chosen “experts”
against the use of alternaMve treatments to COVID-19, they overlook that the government took
steps to restrict access to such medicaMon early in the pandemic and decided not to approve
them. Meanwhile, Medsafe demonstrated unusual speed in neglecsully granMng provisional
consent to the Pfizer Comirnaty injecMon for the enMre populaMon of NZ above the age of 16 years.
This decision was found to be illegal, aier which, the government quickly changed the legislaMon,
with no new risk assessment offered. So we are far from impressed by what is “recommended”.
As an example, for IvermecMn there is an abundance of evidence for beneficial effects in
prevenMng fatality aier COVID-19 infecMon, including meta-analysis 36,37,38,39,40,41,42 and other
reviews. 43,44,45,46,47
In looking for signals as to the worthiness of IvermecMn research, the authors defer to the WHO – a
private organisaMon that has been found severely wanMng in many aspects of the pandemic, and
whose biggest funders during the pandemic (China and the Gates FoundaMon) can hardly be said
to be financially and poliMcally neutral. The authors should read the research themselves and trust
their own judgement. We have supplied the references again and summarise below. Intellectual
laziness will be no defence in any future enquiry should New Zealand experience a significant
outbreak with lives lost needlessly due to suppression of clinical proof of IvermecMn’s efficacy, or if
the vaccine is acknowledged to be harmful and it emerges that it was never jusMfied as “the only
way out of the pandemic”. Indeed, this single fact - the seemingly collecMve denial by major public
health bodies of a lifesaving cure for COVID-19 illness – tesMfies to the apparent triumph of profits
and poliMcs over scienMfic medicine. The casual treatment of our concerns as some sort of
‘rebuSal tennis’ by the authors does nothing to reassure the public that they are being properly
guarded.
A summary of some facts about IvermecMn are as follows:
•
A meta-analysis of 3 trials, assessing 738 parMcipants, found that IvermecMn prophylaxis
among health care workers and COVID-19 contacts reduces the risk of COVID-19 infecMon
by 86%.
•
A meta-analysis of 13 trials, assessing 1892 parMcipants, found that IvermecMn reduced the
risk of death by an average of 68% compared with the control group.
•
IvermecMn has a well-established safety profile with billions of doses used worldwide for
parasiMc infecMons. Various WHO documents on parasiMc infecMons refer to IvermecMn
long safety record.
•
IvermecMn is affordable, and can be distributed by various means, e.g. post, and self-
administered. It can therefore effecMvely reach tradiMonally ‘hard-to-reach’ and vulnerable
populaMons such as undocumented migrants, homeless, the elderly living alone or in care
homes, those lacking transport to reach health faciliMes, and those who lack access to
adequate health care for other reasons.
The weight of medical and scienMfic opinion
The authors aSempt to discredit scienMfic arguments by calling into quesMon the background
knowledge of the highly qualified professionals who made them speaks for itself and does not
require further comment.
Summary
The authors claim that our concerns are not well founded has not been established by their
response and we have presented further evidence rebuyng these asserMons and reinforcing our
posiMon.
For such a rapidly developed and sMll experimental pharmaceuMcal the bar should be set
extremely low for recognising signals of potenMal and actual harm, and invesMgaMng any concerns
with alacrity and vigour, given the mass populaMon being targeted - soon to include children, if
New Zealand conMnues to follow the same path as the United Kingdom, United States, Canada etc.
We have clearly outlined that there are safe and viable alternaMves to the novel mRNA injecMons.
We also emphasise newer and alarming informaMon (of more deaths, heart inflammaMon in young
people, and Dr Tess Lawrie’s call to stop the roll-out based on her group’s assessment of the UK’s
Yellow Card system 48) that has emerged since our leSer to Medsafe in May 2021 and that has
prompted us to write statements on informed consent and on injecMng children. Our leSers have
been sent widely to the government, media and our medical bodies, with supporMng references. 49
The extent and mechanisms of harm that are emerging from the injecMon deserve the utmost
open-minded, rapid and willing assessment to enable the necessary acMon.
At NZDSOS we believe strongly that there is no urgent need for the use of this experimental
vaccine in the New Zealand populaMon and its use should be halted immediately.
References
1- Piroth L, CoSenet J, Mariet A-S, et al. Comparison of the characterisMcs, morbidity, and mortality
of COVID-19 and seasonal influenza: a naMonwide, populaMon-based retrospecMve cohort study.
The Lancet Respiratory Medicine 2021;9(3):251-59. doi: 10.1016/s2213-2600(20)30527-0
2- Dupuis C, Bouadma L, de Montmollin E, et al. AssociaMon Between Early Invasive Mechanical
VenMlaMon and Day-60 Mortality in Acute Hypoxemic Respiratory Failure Related to Coronavirus
Disease-2019 Pneumonia.
Cri:cal Care Explora:ons 2021;3(1):e0329. Doi:
10.1097/cce.0000000000000329
3- Ferrando-Vivas P, Doidge J, Thomas K, et al. PrognosMc Factors for 30-Day Mortality in CriMcally
Ill PaMents With Coronavirus Disease 2019: An ObservaMonal Cohort Study.
Cri:cal Care Medicine 2021;49(1)
4. Ledford H. Why do COVID death rates seem to be falling?
Nature 2020:190-92.
5. Roth S, Clausen L, Möller S. COVID-19. Scenarios of a superfluous crisis.
Kybernetes 2020
6- Ioannidis JP. The infecMon fatality rate of COVID-19 inferred from seroprevalence data.
MedRxiv 2020
7- Spiegelhalter D. Use of “normal” risk to improve understanding of dangers of covid-19.
BMJ 2020;370:m3259. doi: 10.1136/bmj.m3259
8- Rosenthal S, Chen R. The reporMng sensiMviMes of two passive surveillance systems for vaccine
adverse events.
American journal of public health 1995;85(12):1706-09.
9- Ioannidis JP, Cripps S, Tanner MA. ForecasMng for COVID-19 has failed.
Interna:onal journal of
forecas:ng 2020
10- Polack FP, Thomas SJ, Kitchin N, et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19
Vaccine.
New England Journal of Medicine 2020;383(27):2603-15. doi: 10.1056/NEJMoa2034577
11- Doshi P. Will covid-19 vaccines save lives? Current trials aren’t designed to tell us.
BMJ 2020;371:m4037. doi: 10.1136/bmj.m4037
12- Torjesen I. Covid-19: Pfizer-BioNTech vaccine is “likely” responsible for deaths of some elderly
paMents, Norwegian review finds.
BMJ: Bri:sh Medical Journal (Online) 2021;373
13- Lee EJ, Cines DB, Gernsheimer T, et al. Thrombocytopenia following Pfizer and Moderna SARS-
CoV-2 vaccinaMon.
American Journal of Hematology 2021
14- Mayme Marshall, Ian D. Ferguson, Paul Lewis, et al. SymptomaMc Acute MyocardiMs in Seven
Adolescents Following Pfizer-BioNTech COVID-19 VaccinaMon. Pediatrics June 2021, e2021052478;
DOI: hSps://doi.org/10.1542/peds.2021-052478
hSps://pediatrics.aappublicaMons.org/content/early/2021/06/04/peds.2021-052478
15- Liguo Zhang, Alexsia Richards, Andrew Khalil, Emile Wogram, HaiMng Ma, Richard A. Young,
Rudolf Jaenisch. Reverse-transcribed SARS-CoV-2 RNA can integrate into the genome of cultured
human cells and can be expressed in paMent-derived Mssues. Proc Natl Acad Sci U S A. 2021 May
25;118(21)
16- Chandramouly G, et al. Polθ reverse transcribes RNA and promotes RNA-templated DNA repair.
Science Advances 2021;24(7)
17- New Discovery Shows Human Cells Can Write RNA Sequences Into DNA – Challenges Central
Principle in Biology hSps://scitechdaily.com/new-discovery-shows-human-cells-can-write-rna-
sequences-into-dna-challenges-central-principle-in-biology/
18- Paul-Henri Lambert, et al. Consensus summary report for CEPI/BC March 12-13, 2020 meeMng:
Assessment of risk of disease enhancement with COVID-19 vaccines. Vaccine. 2020 Jun 26; 38(31)
19- Alana F Ogata, Chi-An Cheng, Michaël Desjardins, Yasmeen Senussi, , Megan Powell, ewis
Novack, Salena Von, Xiaofang Li, Lindsey R Baden, David R Walt. CirculaMng SARS-CoV-2 Vaccine
AnMgen Detected in the Plasma of mRNA-1273 Vaccine Recipients.
Clinical Infec:ous Diseases,
ciab465, Published: 20 May 2021 hSps://doi.org/10.1093/cid/ciab465
20- PFIZER CONFIDENTIAL - SARS-CoV-2 mRNA Vaccine (BNT162, PF-07302048) . 2.6.4 Summary of
pharmacokineMc study . hSps://www.pmda.go.jp/drugs/2021/
P20210212001/672212000 30300AMX00231 I100 1.pdf
21- PFIZER PF-07302048 (BNT162 RNA-Based COVID-19 Vaccines) Protocol C4591001. hSp://
82.221.129.208/pfizervax.pdf
22- Assessment report Comirnaty -EMA 19 February 2021 hSps://www.ema.europa.eu/en/
documents/assessment-report/comirnaty-epar-public-assessment-report en.pdf
23- Study to Describe the Safety, Tolerability, Immunogenicity, and Efficacy of RNA Vaccine
Candidates Against COVID-19 in Healthy Individuals - ClinicalTrials.gov IdenMfier NCT04368728:
hSps://clinicaltrials.gov/ct2/show/results/NCT04368728?view=results
24- Liu, Y., Liu, J., Xia, H., Zhang, X., Fontes-Garfias, C. R., Swanson, K. A. ... Shi, P.-Y. (2021).
Neutralizing AcMvity of BNT162b2-Elicited Serum. N Engl J Med 384: 1466-1468. hSps://doi.org/
10.1056/NEJMc2102017.
25-
Jared S. Hopkins. Annual Covid-19 Vaccine Booster Shots Likely Needed, Pfizer CEO Says. The
Wall Street Journal. Updated April 15, 2021 7:57 pm ET
hfps://www.wsj.com/ar:cles/annual-
covid-19-vaccine-booster-shots-likely-needed-pfizer-ceo-says-11618520527 26- Suzuki, Y. J. (2020). The Viral Protein Fragment Theory of COVID-19 Pathogenesis. Medical
Hypotheses 144: 110267. hSps://doi.org/10.1016/j.mehy.2020.110267.
27- Suzuki, Y. J., Nikolaienko, S. I., Dibrova, V. A., Dibrova, Y. V., Vasylyk, V. M., Novikov, M. Y. ...
Gychka, S. G. (2021).SARS-CoV-2 Spike Protein-Mediated Cell Signaling in Lung Vascular Cells.
Vascular Pharmacology 137: 106823. hSps://doi.org/10.1016/j.vph.2020.106823.
28- Suzuki, Y.J., Nikolaienko, S.I., Dibrova, V.A., Dibrova, Y.V., Vasylyk, V.M., Novikov, M.Y. ... Gychka,
S.G. (2020). SARS-CoV-2 Spike Protein-Mediated Cell Signaling in Lung Vascular Cells. Vascular
Pharmacology 137: 106823. hSps://www.doi.org/10.1016/j.vph.2020.106823.
29- Suzuki, Y. J. & Gychka, S. G. (2021). SARS-CoV-2 Spike Protein Elicits Cell Signaling in Human
Host Cells: ImplicaMons for Possible Consequences of COVID-19 Vaccines. Vaccines 9: 36.
hSps://doi.org/10.3390/vaccines9010036.
30- Buzhdygana, T. P., DeOrec, B. J., Baldwin-Leclair, A., Bullock, T. A., McGary, H. M. ... Ramirez, S.
H. (2020). The SARS-CoV-2 Spike Protein Alters Barrier FuncMon in 2D StaMc and 3D Microfluidic in-
Vitro Models of the Human Blood-Brain Barrier. Neurobiology of Disease 146: 105131. hSps://
doi.org/10.1016/j.nbd.2020.105131.
31- Verma, S., Saksena, S. & Sadri-Ardekani, H. (2020). ACE2 Receptor Expression in Testes:
ImplicaMons in Coronavirus Disease 2019 Pathogenesis. Biology of ReproducMon 103(3): 449-451.
hSps://doi.org/10.1093/biolre/ioaa080.
32- Navarra, A., Albani, E., Castellano, S., Arruzzolo L., & Levi-Sey P. E. (2020). Coronavirus
Disease-19 InfecMon: ImplicaMons on Male FerMlity and ReproducMon. FronMers in Physiology 11:
574761. hSps://www.doi.org/10.3389/fphys.2020.574761.
33- Wang, Z.& Xu, X. (2020). ScRNA-seq Profiling of Human Testes Reveals the Presence of the
ACE2 Receptor, a Target for SARS-CoV-2 InfecMon in Spermatogonia, Leydig and Sertoli Cells. Cells
9: 920. hSps://doi.org/10.3390/cells9040920.
34- Achua, J. K., Chu, K. Y., Ibrahim, E., Khodamoradi, K., Delma, K. S., Ramsamy, R. ... Arora, H.
(2021). Histopathology and Ultrastructural Findings of Fatal COVID-19 InfecMons on TesMs. The
World Journal of Men's Health 39(1): 65-74. hSps://doi.org/10.5534/wjmh.200170.
35- Gene therapy - Wikipedia hSps://en.wikipedia.org/wiki/Gene therapy
36- Kory, P.
et al. (2021). Review of the Emerging Evidence DemonstraMng the Efficacy of
IvermecMn in the Prophylaxis and Treatment of COVID-19. To appear in
American Journal of
Therapeu:cs, May-June 2021
37- Hill, A.
et al. (2021). Meta-analysis of randomized trials of ivermecMn to treat SARS-CoV-2
infecMon.
Research Square preprint. DOI: 10.21203/rs.3.rs-148845/v1
38-Cobos-Campos, R.
et al. (2021). PotenMal use of IvermecMn for the treatment and profilaxis.
Clinical Research and Trials, 7, 1-5. DOI: 10.15761/CRT.1000333 (over-ridden)
39- Bryant, A., Lawrie, T.A., Dowswell, T., Fordham, E.J., Mitchell, S., Hill, S.R. & Tham, T.C. (2021).
IvermecMn for prevenMon and treatment of COVID-19 infecMon: a systemaMc review and meta-
analysis.
OSF preprint, hSps://osf.io/k37i/ DOI: 10.31219/osf.io/k37i
40- Castañeda-Sabogal, A.
et al. (2021). Outcomes of IvermecMn in the treatment of COVID-19: a
systemaMc review and meta-analysis.
medRxiv preprint, DOI: 10.1101/2021.01.26.21250420
41- Nicolas, P., Maia, M. F., Bassat, Q., Kobylinski, K. C., Monteiro, W. & Rabinovich, N. R. (2020).
Safety of oral ivermecMn during pregnancy: a systemaMc review and meta-analysis.
The Lancet
Global Health, 8, E92 – E100. doi: hSps://doi.org/10.1016/S2214-109X(19)30453-X .
42- Navarro, M. et al. (2020). Safety of high-dose ivermecMn: a systemaMc review and meta-
analysis.
Journal of An:microbial Chemotherapy, DOI: 10.1093/jac/dkz524
43- Crump, A. (2017). IvermecMn: enigmaMc mulMfaceted ‘wonder’ drug conMnues to surprise and
exceed expectaMons.
The Journal of An:bio:cs,
70, 495-505. doi: 10.1038/ja.2017.11
44- Heidary, F. & Gharebaghi, R. (2020). IvermecMn: a systemaMc review from anMviral effects to
COVID-19 complementary regimen.
The Journal of An:bio:cs, 73, 593–602. doi: 10.1038/
s41429-020-0336-z
45- Nardelli, P.
et al. (2021). Crying wolf in Mme of Corona: the strange case of ivermecMn and
hydroxychloroquine. Is the fear of failure withholding potenMal life-saving treatment from clinical
use?
Signa Vitae, DOI: 10.22514/sv.2021.043
46- Schmith, V. D., Zhou, J. (J. & Lohmer, L. R. (2020). The Approved Dose of IvermecMn Alone is not
the Ideal Dose for the Treatment of COVID-19.
Clinical Pharmacology and Therapeu:cs, DOI:
hSps://doi.org/10.1002/cpt.1889
47- Caly, L.
et al. (2020). The FDA-approved drug ivermecMn inhibits the replicaMon of SARS-CoV-2
in vitro.
An:viral Research,
178, 104787. DOI: hSps://doi.org/10.1016/j.anMviral.2020.104787
48- Lawrie, T., Urgent preliminary report of Yellow Card data up to 26th May 2021 to MHRA, hSp://
medisolve.org/yellowcard urgentprelimreport.pdf
49- hSps://nzdsos.com/2021/06/14/informed-consent/
 From:
From:
NZ Doctors Speak Out with Science <[email address]>
Sent:
Friday, 6 August 2021 10:41 pm
To:
Lydia Verschaffelt-Parliament; C Hipkins (MIN)
Cc:
A Little Office (MIN); Rt Hon Jacinda Ardern; Ashley Bloomfield; Chris James
Subject:
Re: Response to your correspondence from Minister Hipkins (CH203993)
Attachments:
Reply to Chris Hipkins 6 August 2021 Final.pdf
6 August 2021
Dear Mrs. Verschaffelt;
Please find attached our letter in reply to Minister Hipkins:
-------------------------
Chris Hipkins – Minister for Covid-19 Response
emails: [Chris Hipkins request email]
[email address]
C.C: mailto:[email address] ; mailto:[email address],
mailto:[email address]; mailto:[email address]
RESPONSE TO YOUR LETTER DATED 6 AUGUST 2021 – Ref. CH203993
Dear Minister Hipkins;
Please find attached our letter in reply to your own received this morning.
Sincerely;
NZDSOS – Steering Committee:
Matt Shelton, Tracy Chandler, Cindy de Villiers, Mark Bailey, Jacques Imbeau, Simon Thornley, Tessa Jones
Sent with ProtonMail Secure Email.
‐‐‐‐‐‐‐ Original Message ‐‐‐‐‐‐‐
On Friday, August 6th, 2021 at 1:53 PM, Lydia Verschaffelt <[email address]> wrote:
Kia ora
1

Please find attached a letter to you from Hon Chris Hipkins, Minister for COVID‐19 Response.
Ngā mihi
Lydia Verschaffelt |
Health Private Secretary
Office of Hon Chris Hipkins
Minister for COVID‐19 Response | Minister of Education | Minister for the Public Service | Leader of the House
Parliament Buildings, Private Bag 18041, Wellington 6160, New Zealand
2

6 August 2021
Chris Hipkins – Minister for Covid-19 Response
emails: [Chris Hipkins request email]
[email address]
C.C: mailto:[email address] ; m
ailto:[email address] ,
m
ailto:[email address] ; mailto:[email address]
RESPONSE TO YOUR LETTER DATED 6 AUGUST 2021 – Ref. CH203993
Dear Minister Hipkins;
Thank you for your letter received today 6 August 2021 in reply to our correspondence of 28 June and 6 July
2021. We did reply to Dr. Town and are still waiting for a response.
Thank you also for the confirmation that the current mass injection programme with the Pfizer Comirnaty
vector is indeed part of large ongoing clinical trials. Therefore every individual injected with this vector is a
'de facto' part of these large clinical trials i.e a large scale experiment using a novel genetic therapy agent. It
appears that your government has failed to make that important fact very clear to all those who have either
agreed or been coerced into having the injections.
Since, by your own admission, what is currently unfolding in New Zealand is part of large ongoing clinical
trials, the government is bound to follow the ethical rules related to clinical trials and make sure that ALL
adverse events are actually reported and that all participants are closely monitored.
We have been informed of multiple instances where patients are told that their adverse event is not related
to the injections. Many are having to insist that it be reported to CARM; many patients and doctors are also
unable to report it themselves as the CARM website has been crashing repeatedly. This is in contravention of
the ethical guidelines of clinical trials. In an experiment such as the one your government is conducting, it is
the responsibility of the one conducting the trial to accurately record
all adverse events and to prove that
such adverse events are NOT caused by the experiment. . https://www.linkedin.com/pulse/four-big-mistakes-
clinical-trials-adverse-event-vera-madzarevic-phd-
Another very important matter that needs to be raised is the issue of the isolation of the “SARS-CoV-2” virus.
Obviously all the health measures and restrictions imposed by your government since March 2020 are
justified by the existence of an alleged novel coronavirus called SARS-CoV-2. Since this is the fundamental
basis for the NZ government actions, can you please provide material evidence that the SARS-CoV-2 virus has
been
isolated directly from an infected patient.
Please do not send us evidence of a so-called ‘isolate’ from an
in vitro tissue culture exposed to a sample from
a patient that was given the diagnosis of “COVID-19” — someone said to have “COVID-19” after a positive
Polymerase Chain Reaction “test” that has no established diagnostic specificity for the said clinical disease.
That kind of circular reasoning does not establish the proof of the alleged virus “SARS-CoV-2”. So, a simple
request to you to provide the fundamental evidence behind the unprecedented measures that have been
carried out on the New Zealand population.
Finally Minister, you have made various contradictory statements to the media around the vaccine being
mandatory. On July 10th 2021 you stated everyone would be vaccinated, “by whatever means necessary,” and
yet this week you have said such claims are disinformation. Many Kiwis are being vaccinated after threats by
their employers, and others as they suspect the unvaccinated will be victimised and marginalised by the
government for their refusal. Are they correct? As doctors, how are we to advise such patients when they are
trying to make an important treatment decision on medical grounds, with these threats of human rights
abuses in the background? An unambiguous statement either way is very important, for obvious reasons
Sincerely;
NZDSOS – Steering Committee:
Matt Shelton, Tracy Chandler, Cindy de Villiers, Mark Bailey, Jacques Imbeau, Simon Thornley, Tessa Jones
 From:
From:
NZ Doctors Speak Out with Science <[email address]>
Sent:
Friday, 6 August 2021 10:40 pm
To:
Ashley Bloomfield
Cc:
A Little Office (MIN); C Hipkins (MIN); Rt Hon Jacinda Ardern; Chris James
Subject:
Formal Complaint from NZDSOS
Attachments:
Complaint to Director General of Health Final.pdf
Dear Dr. Bloomfield;
Please find attached a formal complaint.
Steering Committee – NZDSOS
Matt Shelton, Tracy Chandler, Cindy de Villiers, Mark Bailey, Jacques Imbeau, Simon Thornley, Tessa Jones.
Sent with ProtonMail Secure Email.
1

6 August 2021
Dr. Ashley Bloomfield
Director General Of Health
Ministry of Health
Email: mailto:[email address]
C.C: mailto:[email address] ; mailto:[Chris Hipkins request email] ;
ma
ilto:[email address] , mailto:[email address]
FORMAL COMPLAINT FROM NZDSOS
Dear Director General of Health;
We have previously written multiple letters to Mr. Chris James of Medsafe with copies to you,
the Minister of Health, the Minister for Covid-19 Response and to the Prime Minister. In
addition we have provided a detailed response to Medsafe in the form of a document titled
“Rebuttal to Prof. P. McIntyre and Dr. Ian Town response to NZDSOS concerning Pfizer
Comirnaty”, which is fully referenced. (Copy attached)
We are fully aware that Medsafe has given provisional consent to Comirnaty, how this was
undertaken and that you have further approved it for children from the age of 12. Presumably
the government has already requested that Medsafe investigate the same down to infants, and
that you endorse the same, as well as the targeting of pregnant women, as we write?
To repeat, do you understand that Pfizer's trial (the one with no children, pregnant women,
old or infirm patients etc) actually showed an absolute risk reduction of less than 1%, by
simple maths, and that the number of deaths in each group was NOT statistically different?
Irrespective of contradictions in the medical press around efficacy, serious adverse events to
Pfizer Comirnaty are increasing at an unprecedented pace. We are receiving reliable reports
that seem to far exceed those released on the Medsafe website. Once our legal advice is
finalised we will provide an unofficial list of suspicious deaths post-vaccine that demand
urgent and proper consideration by Medsafe, in the context of the extremely large experiment
being visited on our citizens by Pfizer - with the government’s consent, and waiver of any
liability. We are hearing over and over from patients whose genuine concerns are dismissed
and, given the extremely large reporting of deaths and serious injuries overseas, it is frankly
appalling that our medical system has not been prepared and optimized to watch for and
report the remotest chance of harmful effects here at home.
On the contrary, we believe the coup carried out against informed consent and the threats
made to doctors who depart from the ‘safe and effective’ narrative have combined to fatally
damage the role of doctors as sentinel gatekeepers, apparently unable to watch for public
harm from a brand new and under-researched medication. We repeat, the apparent lack of
consideration for ethical or humanitarian factors is truly horrifying. What happened to the
precautionary principle? We have dismantled tenets of good medical practice in order to mass
vaccinate for an influenza-level disease.
Recent news from Israel has demonstrated the poor effectiveness of this product, where 50%
of people infected with the ‘Delta’ variant had been fully inoculated with Pfizer Comirnaty, and
that 62% of new UK Covid-19 cases have received both inoculations. Public Health England
have reported a 6 fold increased mortality in those infected by the Delta variant who had been
vaccinated compared to unvaccinated Delta cases. It is clear that there is something badly
amiss with many of the patterns we are observing. We are therefore lodging a formal
complaint to you as Director General of Health and urgently request that:
You provide material evidence that the SARS-CoV-2 virus has been directly
isolated from any individual and proven to be infectious and able to cause
disease.1
The provisional consent of Pfizer Comirnaty be rescinded until such time.
That all restrictions and public health measures related to SARS-CoV-2 and the
allegedly related disease called COVID-19 be lifted until such time.
You accept the strength of evidence for medical treatment strategies, in
particular for Ivermectin, as advanced by Drs Tess Lawrie of BIRD and Pierre
Kory of Front Line Critical Care Alliance. (Your sworn affidavit dismissed the
therapeutic potential but we have since provided references to up-skill your
knowledge in this area, and call on you to make Ivermectin a key part of NZ’s
response strategy, to wit the remarkable success of countries like Mexico, India
and some in South America). Further we request you liaise with your peers in Fiji
to facilitate Ivermectin’s use there.
We respectfully remain at your disposal awaiting your prompt reply.
Sincerely,
Steering Committee – NZDSOS
Matt Shelton, Tracy Chandler, Cindy de Villiers, Mark Bailey, Jacques Imbeau, Simon Thornley,
Tessa Jones.
1. NB: References to papers that purport to demonstrate the ‘isolation’ of “SARS-CoV-2” are not proof of the virus
if they involve indirect techniques such as observing cytopathic effects
in vitro in mixed tissue cultures, using the
Polymerase Chain Reaction to amplify genetic fragments of unproven provenance, or genomic sequencing
through Massive parallel sequencing (aka “Next-generation sequencing”) of unpurified samples.
 From:
From:
s 9(2)(a)
Sent:
Tuesday, 17 August 2021 2:38 pm
To:
Lydia Verschaffelt-Parliament
Cc:
s 9(2)(a)
Subject:
RE: Formal Complaint from NZDSOS
Kia ora Lydia
Thank you for providing this to us, we appreciate being kept in the loop.
Ngā mihi
s 9(2)(a)
s 9(2)(a)
M
m
m
Te Kaunihera Rata o Aotearoa |
Medical Council of New Zealand
s 9(2)(a)
|0800 286 801
www.mcnz.org.nz | s 9(2)(a)
This email may contain legally privileged or confidential information which is intended for the use of the
addressee only. If you receive this mail in error, please delete it from your system immediately and
notify us at either the above email address or on +64 4 384 7635.
1