


Operations
Congenital anomaly – an abnormality present at birth
The main repair is called a Pull-through or PSARP
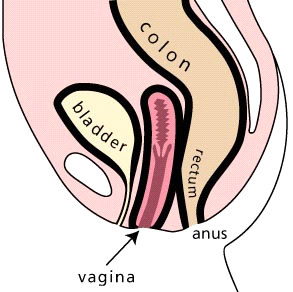
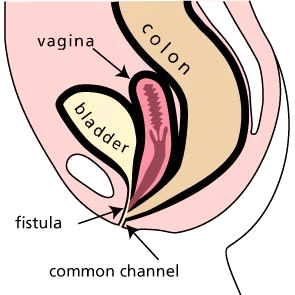
Cloaca – malformation where the colon, bladder and
vagina connect to a single passageway opening out of the
(Posterior-Sagittal-Anorectoplasty)
and
it
is
usually
perineum
performed within the first year of life. This operation
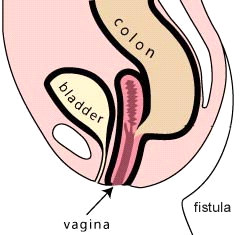
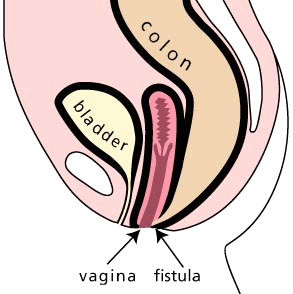
Fistula – an abnormal passage from a normal cavity to
generally takes 3-5 hours, with a post-operative stay of 5-7
the body surface or another cavity.
days.
Genitourinary tract – organs and parts concerned with
Cloaca which is a more complex defect requires a
the kidneys, urinary bladder, and reproductive organs
PSARVUP (Posterior-Sagittal-Anorectovaginourethroplasty)
(vagina, uterus, testes etc)
and usually requires a longer stay and additional recovery
Perineum – the outer area between the vulva and the
time.
anus in a female or between the scrotum and anus in a
Dilatations
male.
Two weeks after the pull-through surgery, you may begin a
program of anal dilatations in order to stretch the child’s new
anus to a normal size. You will begin with a dilator that fits
Adapted from ‘Anorectal Malformations’ by the Pullthru
network.
Anorectal
snugly, and perform the dilatations twice a day. Every 1-2
www.pullthrough.org
weeks the size of the dilator will be increased until the
correct size is reached. At this point the colostomy can be
Disclaimer: Due to the dynamic state of the internet we
Malfor mations
closed. The dilatations continue, but the frequency is
cannot recommend or endorse this website.
gradually decreased until they are no longer required.
Parents Support Group
Colostomy Closure and Nappy Rash
Bowel Group for Kids Inc.
P.O. Box 40
Usually, within 2-3 months of the main repair (PSARP or
Oakdale NSW 2570
A Parent’s Guide
PSARVUP) or adequate dilatation is achieved the colostomy
Ph: 02 4659 6186
is closed. This operation usually requires a stay of 5-6 days.
Throughout this stay, baby will start passing stool through
the new rectum for the first time and they will be frequent
Note: This is general information only and
and loose. During this time, they are susceptible to severe
the situation can vary from case to case.
nappy rash and good bottom care is required with the use of
a skin barrier cream.
There are a variety of barrier creams available and it may
take some trial and error to find one that works well for your
baby. Please ask your nurse for some advice.
It is advisable to start preparing baby’s “bottom” a week/
fortnight prior to this operation. This can be done by placing
Compiled by J Rowe Surgical Nurse Specialist
some stool from baby’s colostomy onto the nappy and
Department of Paediatric Surgery
having baby wear the nappy for 5-10 mins, and/or applying
Starship children’s Hospital
‘skin prep’ wipes to baby’s bottom. This should be done
Level 4
Phone 64 9 307 4949 ext. 6381
several times a day.
Department of Paediatric Surgery
Glossary
Starship Hospital
Anorectal – pertaining to both the anus (ano) and the
Auckland
rectum (rectal)
SSH/WI-3033/007 – updated 01/06
SSH/WI-3033/007 – updated 01/06
SSH/WI-3033/007 – updated 01/06
Introduction
Your baby has been born with an anorectal malformation.
This brochure is intended to provide general information
about anorectal malformations and the operations that are
done to deal with it.
What are Anorectal Malformations?
The term ‘anorectal malformation’ encompasses a wide
range of congenital anomalies involving the rectum, urinary
and reproductive structures with varying degrees of
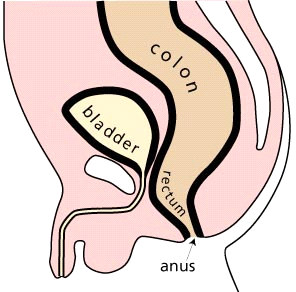
Normal male anatomy
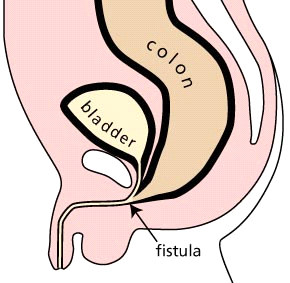
Recto urethral bulbar fistula (Low)
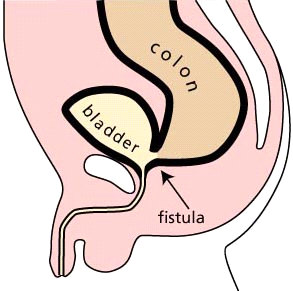
Recto bladder neck fistula (High)
complexity. These are usually referred to as low or high.
Most babies born with anorectal malformations have no anal
opening and may have an abnormal connection between
Colostomy
trial and error in handling the ostomy products. You will be
the rectum and the genitourinary tract or the perineum. This
provided with help from a stoma therapist and the nurses on
There is a large spectrum of defects and each one is different
abnormal connection is called a fistula.
the ward.
from the other. However, there are certain categories or
In females, who have a connection between the rectum,
A referral will be made to a community stoma therapist for
types of defects with similar prognoses and management.
urinary and reproductive tract the word “cloaca” is used.
ongoing help, when you and your baby are discharged
Babies born with a very “low” defect typically require a simple
The type of malformation will influence what surgery baby
home.
operation soon after birth. These children have a good
may require. It will also influence the outcome for your
prognosis for bowel control.
Distal Colostogram
child’s bladder and bowel control.
Babies born with a “high” defect require more complex
Prior to the pull-through operation (main repair), it is
Background/Incidence
treatment. This usually begins with a temporary colostomy on
important to determine the precise defect your baby was
Imperforate anus has been a documented anomaly since
the first day of life. A colostomy is created by dividing the
born with. This will help in terms of prognostic and
antiquity. It has an incidence of 1 in 4000 newborns. Cloaca
large intestine and then bringing the two ends through the
therapeutic implications, as well as helping the surgeon to
has an incidence of 1 in 50 000.
abdominal wall. This procedure provides the child with a
visualise the baby’s anatomy.
Anorectal malformations affect all racial, social, cultural and
temporary way to pass stool.
The distal colostogram is the best study for this, and it
economic groups equally. Studies have not found any
Colostomy Care
consists of injecting contrast material into the distal stoma
definite causes for these birth defects, which are thought to
(closest to the anus) to show the characteristics of the
develop during the 4th to 12th week of gestation.
The usual time between the initial colostomy and the repair
baby’s specific defect. This will show the surgeon how high
surgery is between 3-12 months, but may be longer.
Associated Defects
the rectum is and if there is a fistula connecting to the
Since you are dealing with a small baby, there may be some
urinary tract.
There are a number of associated defects that are
commonly found in a child born with an anorectal
malformation.
Defects of the urinary tract are the most common, and may
require immediate attention.
Other defects which may be present involve the
vertebra
(spine),
anus, heart (
cardiac),
trachea, o
esophagus,
renal
and
limb. This combination of defects is termed
VACTERL.
The severity of these defects vary and your baby will be
investigated for these defects. If present they will be treated
as required.
Normal female anatomy
Vestibular fistula
High Imperforate anus
Typical Cloaca
SSH/WI-3033/007 – updated 01/06
SSH/WI-3033/007 – updated 01/06
SSH/WI-3033/007 – updated 01/06