
Document 1
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 15 February 2022
Time:
11:00am to 12:00pm
Location:
Teams: s 9(2)(k)
Chair:
Ian Town
Danny de Lore, David Murdoch, Elizabeth Wilson, Helen Petousis-Harris, James
Members:
Ussher, Nikki Moreland, Owen Sinclair, Peter McIntyre, Sean Hanna, Tony Walls
Andi Shirtcliffe, Brooke Hollingshead, Chriselle Braganza, Daniel Bernal, Edwin
ACT 1982
Ministry of Health Attendees:
Reynolds, Frances Graham, Juliet Rumball-Smith, Mariana Traslosheros Reyes,
Niki Stefanogiannis, Pippa Scott, Sean Driver
Rāwā Mahu Karetai Wood-Bodley, Marion Leighton, Alison Cossar, Amy
Guests:
Alexander, Maria Cotter, Kate Taptiklis, Declan Sua
Ian Frazer, Nikki Turner, Sue Crengle, Caroline McElnay, Fiona Callaghan,
Apologies:
Imogen Roth, John Tait, Patricia Joseph
INFORMATION
Welcome and Previous Minutes
1.0
Ian Town welcomed all Members and Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (08 February 2022) were accepted.
Vaccine Rollout
2.0
An update was provided on the vaccine rollout.
•
First and second doses are high, around 4 million. Most DHBs have reached the target set by
MOH, except Northland.
•
It was noted that paediatric doses were not as high as anticipated, and this was discussed further
in point 3.0.
•
Approximately 2 million booster doses have been administered.
Equity and the Vaccine Rollout
3.0
RELEASED UNDER THE OFFICIAL
•
Representatives from the disability and equity teams at the Ministry of Health summarised some of
the challenges in the vaccine rollout and specifically for 5-11-year-olds, and their approaches to
address these issues.
•
In the vaccine rollout, it has been observed that people living with disabilities have a preference for
going with family or friends to general COVID-19 vaccination centres or events, rather than
attending specialised rollout events, but tailored events are still effective.
•
The significantly lower uptake among tamariki Māori was very concerning to CV TAG, particularly
given the assurances given.
Document 1
•
Approximately 26% of tamariki Māori are vaccinated, which is markedly lower than the national 5–
11-year-old coverage of 45%. Pacific 5-11-years-old have a coverage of around 36%. The rates
varied between regions.
•
Concern was also raised about uptake being lower among Māori 18-49-year-olds. This might be a
consequence of poor access to healthcare in this group because of higher rates of living in
transient housing, higher rates of poverty, and lack of transport.
•
While there are community-led programmes targeting each of these groups, there is stil work
underway to engage these communities through mainstream services. The ability for mainstream
services and the health system as they stand to reach Māori without significant changes was
queried.
•
The equity team identified a gap in availability of vaccination outside of work hours. It is likely that
routinely using schools as vaccination sites and having more clinics/pharmacies open after hours
would increase uptake among tamariki Māori.
1982
•
Funding has also been approved to assist with any workforce capacity issues due to Omicron and
an increase in demand on boosters. Schools have indicated they wil be better placed to engage in
the paediatric roll out in about 2 weeks.
ACT
Booster Doses in 12-17 year-olds
4.0
Draft recommendations on whether 12-17-year-olds should receive booster doses were discussed.
•
Draft recommendations were shared for CV TAG to consider, which proposed boosters only be
administered to those with underlying health conditions, and for those who live with a vulnerable or
immunocompromised household member. These would be offered at 3 months after the primary
course with a broader decision made for this age group at a later date.
INFORMATION
•
It was argued that Māori and Pacific young people need to be included for boosters due to
epidemiology in NZ and the greater risk of severe disease and hospitalisation in this group.
•
Differences between the two age subgroups (16-17yo and 12-15yo) were discussed. It was noted
that there is a small amount of trial data about boosters in 16–17-year-olds, but none for younger
OFFICIAL
ages.
•
It was noted that the UK, US and Australia have recommended that al 16-17-year-olds be offered
THE
boosters. This option could be considered in NZ, with only high-risk 12-15-year-olds offered
boosters.
•
It was noted that there are many 16 and 17 year olds who are out of school or in the workforce
and who may be at high risk of exposure.
UNDER
•
There are limited data about boosters for this age group. Medsafe are expecting an application
soon for boosters in this age group for Pfizer. AstraZeneca is not currently authorised for use in
this age group.
•
The concern around mandates for this group was noted.
•
The purpose o
RELEASED f offering boosters in this age group was queried, as severe disease is already
unlikely. Boosting this age group to reduce transmission would need data to back this up.
•
Reference to the sequencing framework wil be removed as this is now outdated.
•
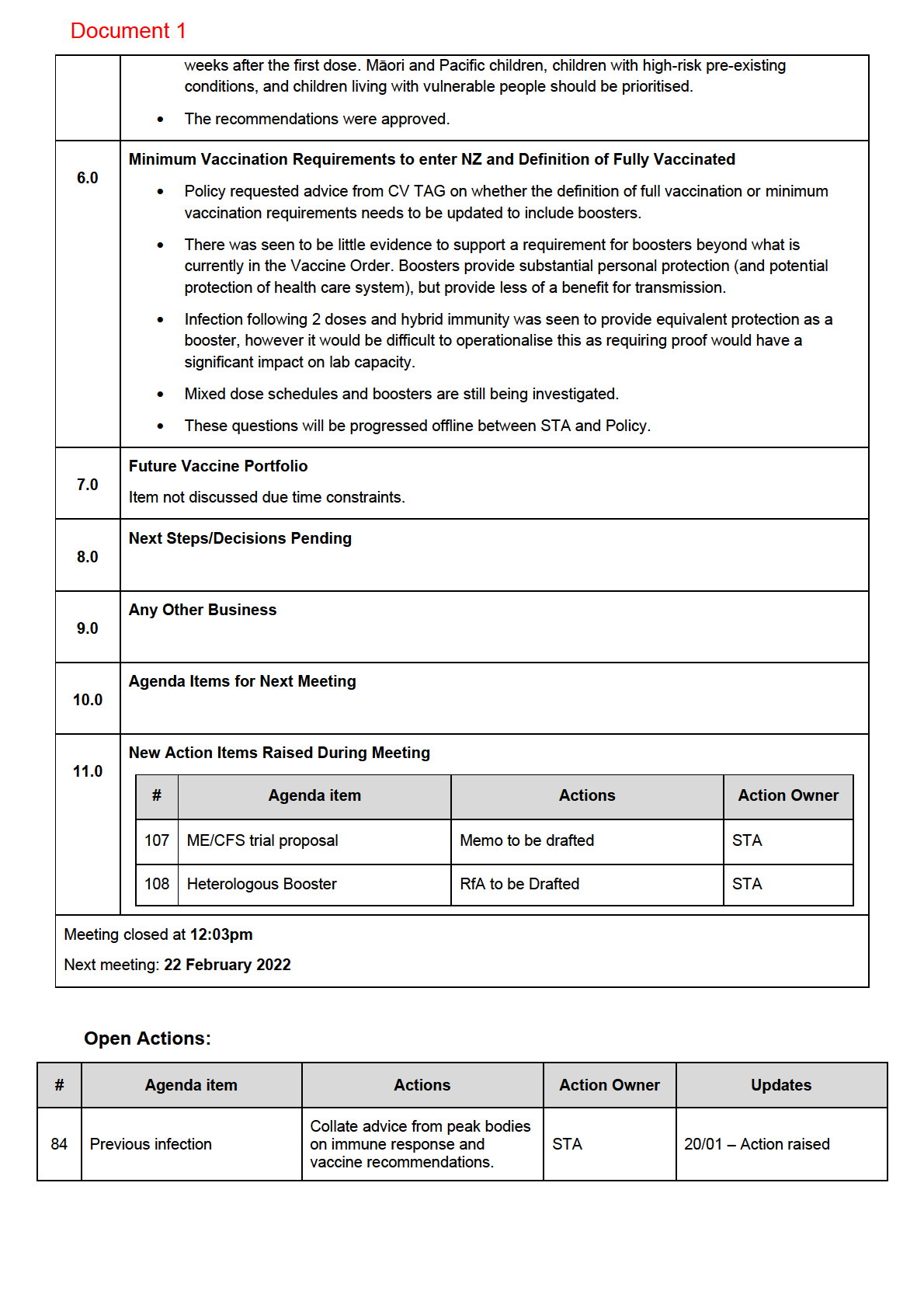
Recommendations wil be redrafted and shared with CV TAG for approval in the coming days.
Dosing interval for 5-11-year-olds
5.0
•
International and local safety data were shared with CV TAG. Revised recommendations were
shared with CV TAG, which proposed that second doses proceed, and that these be given at 8
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 2
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 01 March 2022
Time:
11:00am to 12:00pm
Location:
Teams: s 9(2)(k)
Chair:
Ian Town
Danny de Lore, David Murdoch, Elizabeth Wilson, Helen Petousis-Harris, Ian
1982
Members:
Frazer, James Ussher, Nikki Moreland, Nikki Turner, Owen Sinclair, Peter
McIntyre, Sean Hanna, Sue Crengle, Tony Walls
ACT
Andi Shirtcliffe, Brooke Hollingshead, Caroline McElnay, Chriselle Braganza,
Ministry of Health Attendees:
Daniel Bernal, Edwin Reynolds, Mariana Traslosheros Reyes, Niki
Stefanogiannis, Pippa Scott
Guests:
Alison Cossar, Allison Bennett, Amy Alexander
Apologies:
Fiona Callaghan, John Tait, Juliet Rumball-Smith
INFORMATION
Welcome and Previous Minutes
1.0
Ian Town welcomed all Members and Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (15 February 2022) were accepted.
OFFICIAL
Vaccine Rollout
2.0
THE
An update was provided on the vaccine rollout:
•
Meetings with Vaccine Ministers are now occurring fortnightly, and there was acknowledgement
that the vaccination programme has done what it was intended to do in keeping New Zealanders
safe. Discussions are und
UNDER erway about integrating the COVID-19 vaccination with the wider
National Immunisation Programme (NIP) as influenza season approaches, and an invitation will be
made for the Director of this Programme to speak to CV TAG later in March.
•
Some members of CV TAG had met with the Ministry of Health NIP equity team to discuss actions
underway to improve vaccine uptake among tamariki Māori. School-based programmes will play a
larger role going forward to enable greater access, with the rate of the paediatric rollout slowing
RELEASED
down since schools went back.
•
A soft launch of the booster vaccine for 16-17-year-olds will occur in the coming days, prioritising
those with clinical need in the 16-17-year age group. 12-15-year-olds with clinical need will also
have a pathway available, but a broader rollout will not occur at this stage. However, the focus of
the vaccination programme will remain on tamariki and boosting adults.
Future Vaccine Portfolio
3.0
Document 2
CV TAG were provided with an update on the vaccine portfolio from the Systems Strategy and Policy
team:
•
It was noted that Ministers recently made the decision to maintain an mRNA-based immunisation
programme, and access to mRNA-based vaccines will be maintained. Efforts are ongoing to
confirm maintained access for the latter half of the year, and this will include access to any variant-
specific versions of Pfizer that may become available. In general, large amounts of both the adult
and paediatric doses of Pfizer are currently available.
•
Cabinet has approved Novavax for use as a primary course. Novavax are expected to submit an
application to Medsafe for use as a heterologous booster shortly. The potential for Novavax to be
used as a booster among people who have had an adverse event from their Pfizer primary course
was noted. Discussion about the use of Novavax as a heterologous booster are anticipated,
pending Medsafe approval.
•
Access to a non-mRNA vaccine will also be maintained. Access to a small volume of AstraZeneca
vaccines has been maintained, however the uptake for this vaccine has been very low thus
1982 far.
•
There have been issues with regards to the delivery of Janssen. It is anticipated that there will be
little need for this vaccine and advice has been put forward to Ministers about the p
ACT ossibility of
donating this vaccine.
Novavax as a Heterologous Booster
4.0
CV TAG reviewed the reactogenicity, safety, immunogenicity, and efficacy data on all heterologous
booster schedules:
•
Data is available from the UK COV-BOOST study on Novavax and some smaller studies.
INFORMATION
•
The COV-BOOST trial showed that the use of Janssen, Moderna, Valneva and Curevac following
a primary course of Pfizer or AstraZeneca. Each was well-tolerated, and serious adverse events
were uncommon, however the study cohorts were not large enough to detect rare side effects.
Booster doses of an mRNA vaccine offer the greatest protection, however the use of Novavax as
a booster elicited a modest increase in neutralising titres after a Pfizer course.
OFFICIAL
•
The need for a heterologous booster dose will have to be balanced carefully with the complexity of
implementing different booster vaccines.
THE
•
Half doses of Pfizer may also be a suitable option for those who have side effects after full doses.
Evidence on half doses will be compiled and presented to CV TAG at a future meeting.
•
CV TAG will continue to monitor the evidence in this space and provide recommendations in the
future, pending Medsafe approval of any suitable boosters.
UNDER
Pfizer Second Booster (Fourth dose)
5.0
CV TAG reviewed the data available on second boosters (fourth doses):
•
Data from the UK and US shows that vaccine efficacy against symptomatic infection and severe
disease caused by Omicron wanes over time, and some countries have recommended the
RELEASED
administration of a second booster dose (Israel, the UK, Chile, Hungary, and South Korea). These
have been limited to the elderly or individuals at increased risk (of severe disease or exposure).
•
Data on the safety, reactogenicity and efficacy of second booster doses is currently limited to two
studies from Israel.
•
The rates of confirmed infection and severe disease have been lower after a second booster dose,
however CV TAG noted that the rise in immune responses following a second booster is inferior
when compared to the rise in responses between the second and third dose.
Document 2
•
The data thus far does not support a strong rationale for recommending a second booster at this
point in time.
•
CV TAG will continue to monitor the evidence in this space and provide recommendations in the
future, pending Medsafe approval.
s 9(2)(g)(i)
6.0
1982
ACT
INFORMATION
CV TAG Recommendation Memos
7.0
The latest finalised memos included in agenda for noting:
•
Use of boosters in 12-17-year-olds
OFFICIAL
•
Second dose and interval for 5-11-year-olds
THE
Next Steps/Decisions Pending
8.0
None.
Any Other Business
UNDER
9.0
Clarifications were requested on CV TAG’s recommendations on the use of Novavax as a primary course.
It was confirmed that CV TAG had recommended that the second dose should be administered at least 3
weeks later, and not at 3 weeks later. Coadministration of the vaccine with the influenza vaccine was
considered to be appropriate, with the exception of the adjuvanted flu vaccine.
It was noted that CV TAG earlier recommended that vaccines could be given 4 weeks after infection, but
RELEASED
CV TAG recommended it be given at 12 weeks, and this has not been updated publicly. Clarification will
be sought by the Ministry of Health team.
Agenda Items for Next Meeting
10.0 None.
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 3
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 08 March 2022
Time:
11:00am to 12:00pm
Location:
Teams: s 9(2)(k)
Chair:
David Murdoch
Members:
Danny de Lore, Elizabeth Wilson, Helen Petousis-Harris, Ian Frazer, James
1982
Ussher, Nikki Moreland, Nikki Turner, Owen Sinclair, Sue Crengle, Tony Wal s
Andi Shirtcliffe, Brooke Hollingshead, Caroline McElnay, Chriselle Braganza,
ACT
Ministry of Health Attendees:
Edwin Reynolds, Frances Graham, Juliet Rumball-Smith, Niki Stefanogiannis,
Pippa Scott, Sean Driver
Guests:
Alison Cossar, Amy Alexander, Jennifer Keys, James Entwisle, John Tait, Karin
Van Bart, Laurence Holding, Thomas Teunissen
Apologies:
Daniel Bernal, Fiona Callaghan, Ian Town, Mariana Traslosheros Reyes, Peter
McIntyre, Sean Hanna
INFORMATION
1.0
Welcome and Previous Minutes
David Murdoch welcomed all Members and Attendees and Guests in his capacity as Acting Chair of the
COVID-19 Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (01 March 2022) were accepte
OFFICIAL d.
2.0
CV-ISMB Update
THE
An update was provided on the current process for quantifying the risk of myocarditis by CV-ISMB and the
Ministry’s Post-Event team, and what the current data is tel ing us:
•
New Zealand’s reporting rates are largely in line with international data, with rates of myocarditis
UNDER
and pericarditis higher among younger age groups and after dose two. Most cases have been mild
and self-limiting, though long-term fol ow-up is needed.
•
The Ministry is conducting rapid cycle analyses and self-controlled case studies with respect to
myocarditis, pericarditis, and other adverse events.
•
The Ministry is also conducting a study to examine long-term outcomes after vaccine-induced
myocarditis, wh
RELEASED ich wil look at physical and mental health, physical functioning, and ability of
individuals 12 and over to attend work or school 3 months after a clinical diagnosis of myocarditis.
•
The study has received ethics approval and is expected to be underway with recruitment and
surveying at the end of March. There are currently 300 individuals eligible for the study, with more
expected to be recruited via CARM.
•
The overlap between these studies and that being proposed by the University of Auckland remains
unclear and requires clarification.
Document 3
•
A member highlighted that including post-booster data would be beneficial, as there are individuals
who wil now be 3 months post-booster. However, the limitations on the parameters of the study at
the time of planning limited this.
3.0
Vaccine rollout
This Item was deferred until the next meeting
4.0
Coadministration of COVID-19 vaccines and Flu Vaccines
An update on data relating to the coadministration of all COVID-19 vaccines and flu vaccines was
provided:
•
Data is limited to two publications: the UK ComFlu-COV study and a UK phase 3 trial sub-study.
The studies showed that coadministration is generally well tolerated with no significant safety
concerns. One clinical trial where flu vaccines were coadministered with the Novavax vaccine
showed a lower immune response, but vaccine efficacy was not affected.
1982
•
International peak bodies continue to recommend coadministration, and these include ATAGI,
ACIP, JCVI and NACI.
ACT
•
Previously it was advised that Novavax could be coadministered with other vaccines, with the
exception of the Zostavax vaccine which should be given 7 days later. However, there is also
limited data on coadministering new adjuvanted vaccines. The adjuvanted Novavax vaccine has
been co-administered with FluAd Quad (an adjuvanted flu vaccine), however it is difficult to
detangle the adverse event profile by age in the Novavax sub-study. A member noted the smal
sample size of this study and need for further evidence.
•
Any changes to advice should take this into account.
INFORMATION
•
CV TAG advised an update be made that there should be a 3-day gap between Novavax and
Shingrix or FluAd Quad, as all of these are adjuvanted vaccines. This was not seen to cause equity
issues as they are only available on the private market and therefore have limited use. There was
no dissent to providing this technical update to coadministration advice for these new vaccines.
OFFICIAL
5.0
Myocarditis and Booster Options
•
The Ministry received a letter from IMAC in February requesting CV TAG’s advice on boosters for
THE
mandated workers who had myocarditis after their second dose. Concern was expressed about the
use of AstraZeneca in this population, due to some reports of myocarditis and the link to thrombosis
with thrombocytopaenia (TTS) in age groups under 50.
•
An evidence review on the
UNDER risk of myocarditis after Pfizer and AstraZeneca was presented to CV
TAG.
•
Data from the rol -out of boosters in the US and Israel shows myocarditis rates were lower than
from second doses. AstraZeneca rates were not higher than background rates, though the risk of
TTS must be considered.
•
A member sort clarification from the RfA highlighting that IMAC was not currently recommending
RELEASED
revaccination with Pfizer and have been recommending deferral until now, as is also the policy in
the US. This wil be updated. NACI in Canada suggest that further mRNA doses can be given at
least 90 days post-myocarditis. Australia’s advice is a case-by-case approach, noting the risks of
AstraZeneca.
•
TAG members noted the risk of myocarditis for the vaccine against the risk from COVID-19, which
stil favour getting protection from a booster.
•
There was discussion among CV TAG members on the varying factors and risk associated with
each vaccine booster with regards to previous symptoms, age, sex and infection. It was agreed that
Document 3
if someone had presented with side effects such as myocarditis from Pfizer, they should not have to
have a booster of Pfizer. Acknowledgments were made that there are other options for these
individuals.
•
It was agreed that advice must be nuanced and developed on a case-by-case basis, varying by
individual to support individualised support plans, in order to account for specific risk factors relating
to previous infection, age and sex.
•
Discussions may be needed with the exemptions team to explore possibilities.
•
Individuals should be considered for Novavax if approved as a booster.
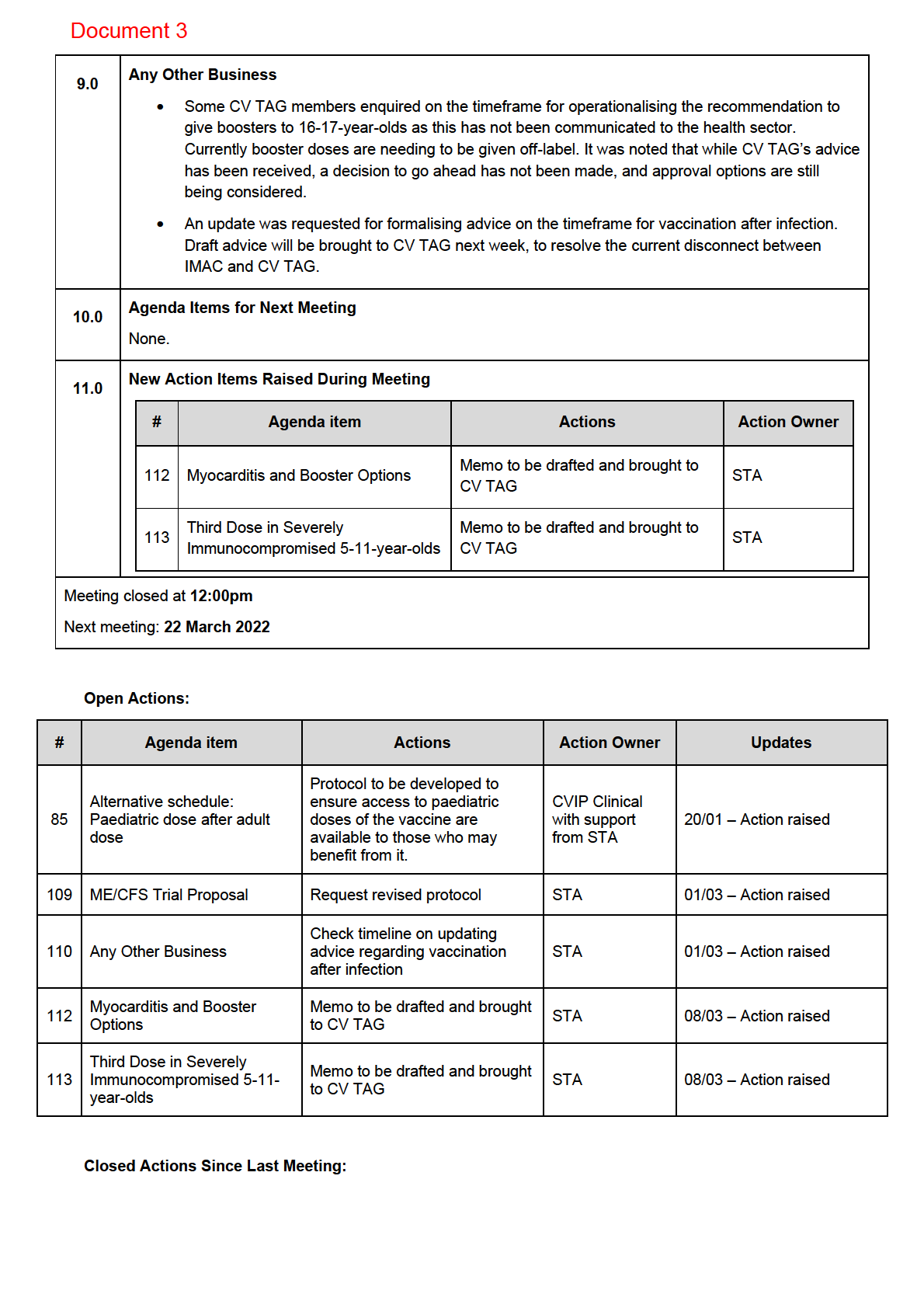
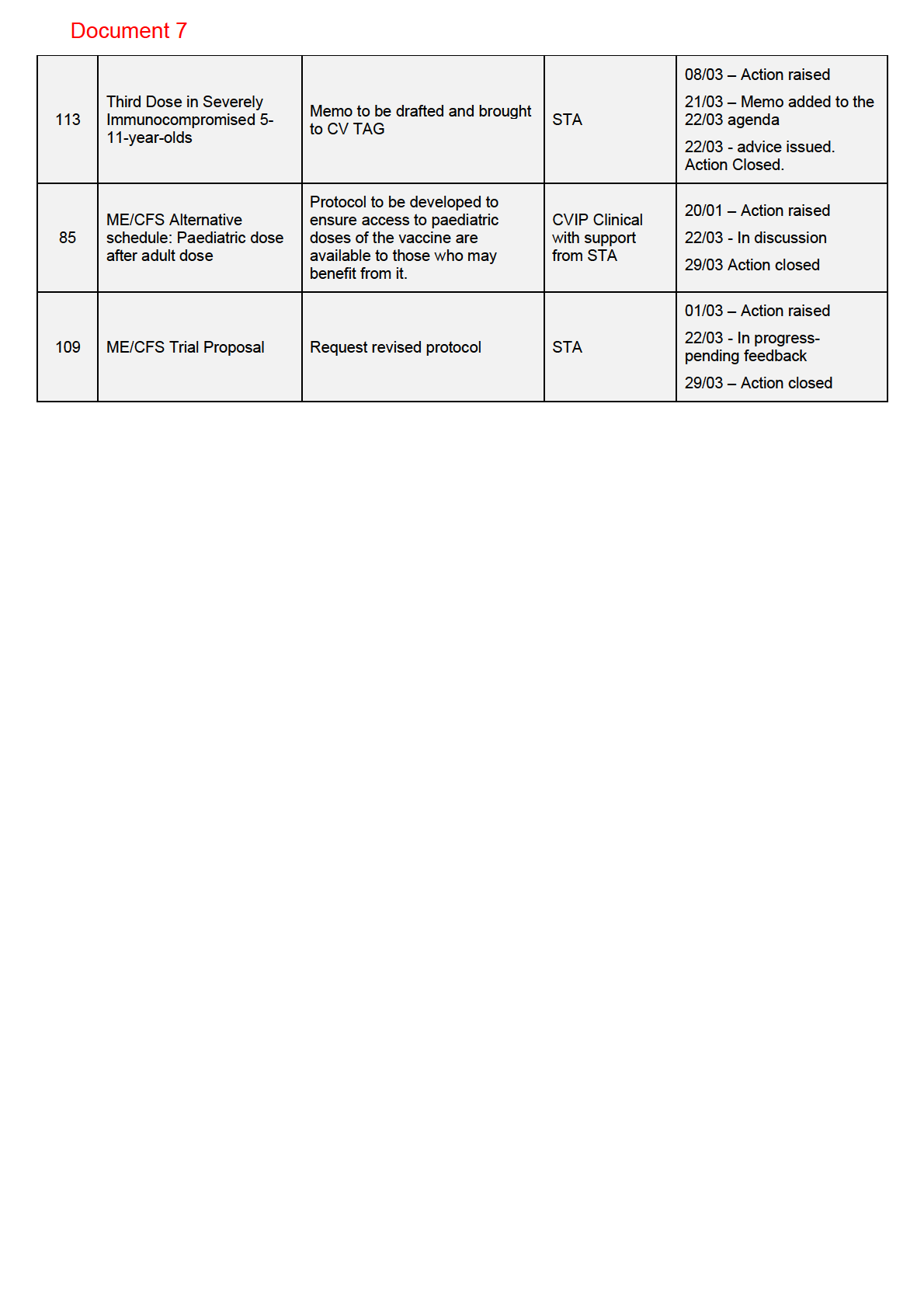
ACTION: STA will draft a memo with CV TAG’s recommendations and circulate.
Third Dose in Severely Immunocompromised 5-11-year-olds
6.0
1982
Advice was requested on the need for a third primary dose in severely immunocompromised 5-11-year-
olds.
•
ACT
A rapid review of the evidence showed no safety data, however based on first principles and the
benefit it has provided to severely immunocompromised older populations, the UK, US, Canada
and Australia have recommended a third primary dose be given. Most of these have been at a 4–8-
week interval, however ATAGI recommended it be given 2-6 months after the first two doses, with
consideration given to timing of treatment.
•
It was noted that generally children have a good immune response, however emerging data
suggests this may wane rapidly against infection, and this would be higher among the severely
immunocompromised.
INFORMATION
•
CV TAG members noted emerging data shows an increased waning of immunity in this age group,
while still protecting against severe disease and discussed how the current interval for children in
NZ might enable greater protection. However, if offered to older immunocompromised individuals it
should be available to this age group as well.
OFFICIAL
•
It was agreed that a third dose should be made available, however this should be limited to those
who need it without clinical discretion to avoid wider availability.
THE
ACTION: STA will draft a memo with CV TAG’s recommendations and circulate.
Pre-print on Pfizer vaccine in 5-11-year-olds
7.0
UNDER
A call was made for initial reaction and comments from a preprint exploring data in New York which shows
that vaccine effectiveness against infection in this age group wanes rapidly:
•
CV TAG noted that protection against severe disease was maintained longer, which is the primary
goal of immunisation. New Zealand’s longer interval between doses suggests duration of protection
may be longer than the 3 weeks in the study. The waning may be due to the smaller dose given.
RELEASED
•
Further data is required before any changes would be made to recommendations however it
emphasises the importance of other public health measures such as mask wearing, ventilation etc.
•
The implications for the public health rationale for vaccinating this age group was raised, noting one
aspect in the decision was preventing further transmission to whānau and within the community.
However, this was only a small factor in decision making.
Next Steps/Decisions Pending
8.0
None.
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 4
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 29 March 2022
Time:
11:00am to 12:00pm
Location:
Teams: s 9(2)(k)
Chair:
Ian Town
David Murdoch, Danny de Lore, Elizabeth Wilson, Helen Petousis-Harris, Ian
1982
Members:
Frazer, James Ussher, Nikki Moreland, Nikki Turner, Owen Sinclair, Peter
McIntyre, Sean Hanna, Sue Crengle, Tony Wal s
ACT
Andi Shirtcliffe, Brooke Hollingshead, Caroline McElnay, Daniel Bernal, Edwin
Ministry of Health Attendees:
Reynolds, Mariana Traslosheros Reyes, Niki Stefanogiannis, Pippa Scott,
Shama Kukkady
Guests:
John Tait, Fran Priddy, Mike Wil iams, Simon Carson, Tara Swadi, Matt Jones,
Laurence Holding, Marion Leighton
Apologies:
Juliet Rumbal -Smith
INFORMATION
1.0
Welcome and Previous Minutes
Ian Town welcomed all Members and Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
OFFICIAL
Minutes of the last meeting (08 March 2022) were accepted.
THE
2.0
Vaccine Rollout
•
An update was provided on the vaccine rol out. Approximately 2.55 mil ion booster doses have
been administered and ~40,400 paediatric 2nd does.
UNDER
•
It was noted that the uptake in 5–11-year-olds has slowed, and thoughts on the reasons for this
were discussed.
•
A member noted that some DHBs predicted a slowing in vaccination rates. The increased
community transmission may be the cause of this as any further vaccination post infection wil be
subject to the 3 months stand down period.
•
Schools were s
RELEASED een as vital to address access and equity issues, and CV TAG noted considerable
variation by DHB on school-based rol outs with further guidance needed.
•
CV TAG encouraged more active use of the National Immunisation Register to recall and follow-
up with children who have had their first dose and not their second.
3.0
Ministry of Health Update on COVID-19 Response
Antibody Testing
Document 4
•
CV TAG were updated on the short and long-term Ministry of Health thinking on serology including
its role in ongoing surveil ance, seroprevalence, and strategic planning. Clinical advice was sought
on the Orbis point-of-care antibody tests being marketed, to be forwarded to Testing TAG.
•
There was concern about the utility of these tests, with members noting that there is no good
immune correlate of protection, there would be no clinical input in interpreting results, nor
guidance on what the results might mean. Pharmacies were not seen as an appropriate setting for
the test with greater supervision needed, and concern was also raised about the implications for
the vaccination programme and public health measures if individuals received these results. It was
also noted this test cannot distinguish between immune response to wild disease and to
vaccination. The high cost and impact of equities was also noted.
4.0
Third Dose for Severely Immunocompromised 5-11-year-olds
•
Draft recommendations were presented to CV TAG for discussion and endorsement on the usage,
timing (8 weeks post second dose) and who is considered severely immunocompromised.
1982
•
While there is no data on the safety or effectiveness of a third primary dose, this can be inferred
from the data in adolescents. Australia, the UK, Canada, and the US have recommended this
ACT
group receive a third primary dose, with timing ranging from 4 to 8 weeks after the second dose.
•
CV TAG recommended a third primary dose be offered to severely immunocompromised 5-11-
year-olds. This would be the same list and at the same interval as was given for adolescents and
adults, with clinical guidance from the IMAC handbook, noting that this may be reviewed over
time.
5.0
Future vaccine portfolio: Use of AstraZeneca
INFORMATION
•
Advice was sought from CV TAG on the requirement to hold any ongoing supply of AstraZeneca
going forward, noting that there are no concerns surround the future supply of Pfizer.
•
There was seen to be a temporary overreliance on AstraZeneca since Novavax has not been
approved as a booster, however it was also noted that there is no long-term data on Novavax, and
therefore if a problem arose, having a smal amount of a vector vaccine with long-term data behind
OFFICIAL
it would give some flexibility to the programme.
•
It was felt that a smal amount wil be retained in the portfolio but Novavax is the primary choice as
THE
an alternative to Pfizer.
6.0
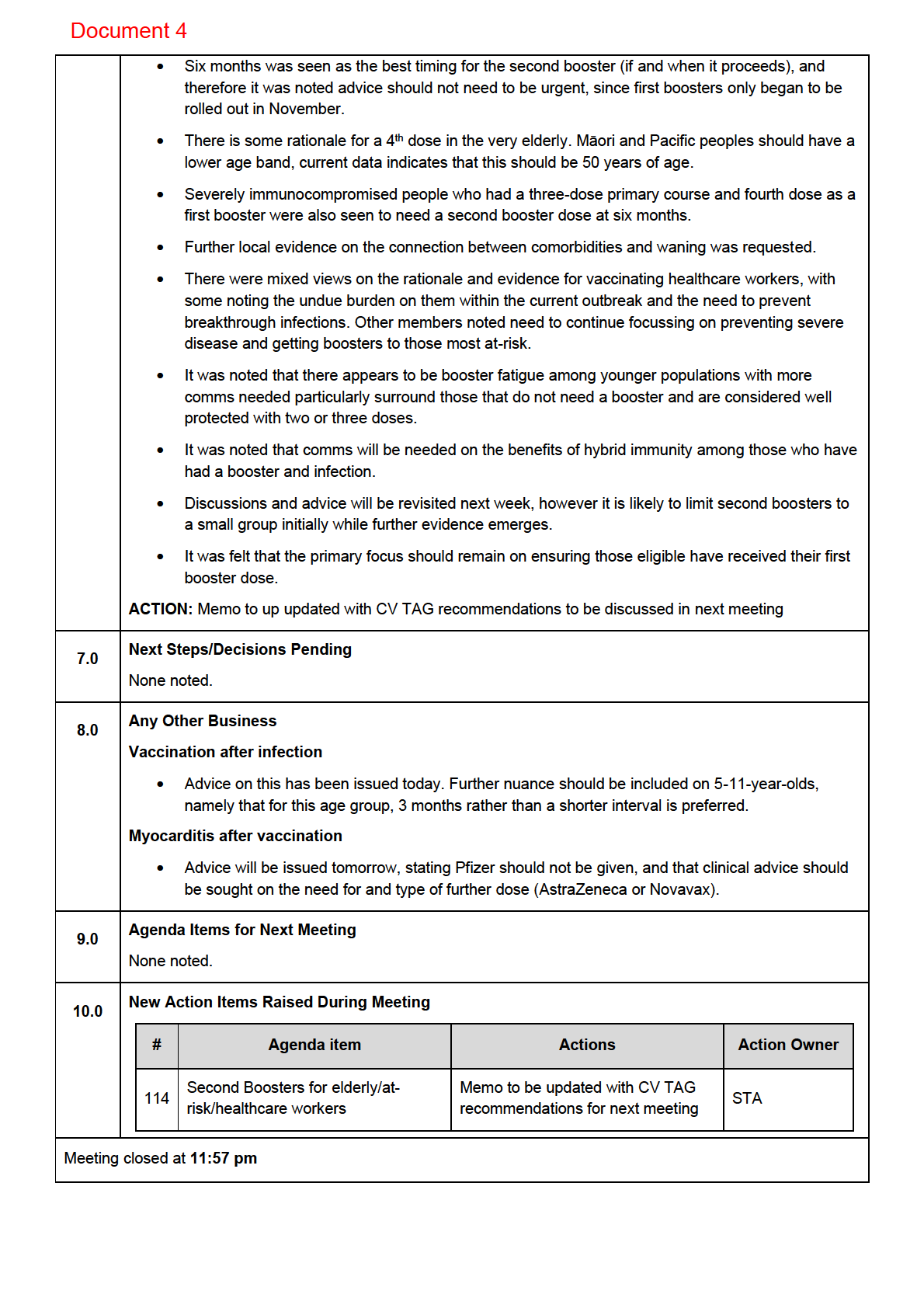
Second Boosters for elderly/at-risk/healthcare workers
•
Draft evidence and recommendations were presented to CV TAG for discussion.
UNDER
•
There is evidence of waning immunity after a first booster dose, and protection appears to wane
faster for the elderly and those living with other health conditions. Māori and Pacific peoples are
also at greater risk of severe disease and hospitalisation. Protection against infection also wanes,
but a fourth dose prevents 30% of cases seen in those who only received three doses.
•
Data on the safety and efficacy of a fourth dose are limited to two studies from Israel, however
RELEASED
these show that a fourth dose is safe and effective in the short term.
•
Some countries have begun rolling out second boosters, however this is mostly limited to the
elderly, very elderly, or immunocompromised. Only Austria is rol ing out a fourth dose to
healthcare workers outside of the Israel trial. The US and Australia have not given advice;
however, it is expected within the next week or two. Countries are giving second boosters four to
six months after third doses.
•
Medsafe are yet to approve a second booster, and there is limited data on pregnant people and
those under 18.
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 5
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 29 March 2022
Time:
11:00am to 12:00pm
Location:
Teams: s 9(2)(k)
Chair:
Ian Town
David Murdoch, Elizabeth Wilson, James Ussher, Nikki Moreland, Nikki Turner,
1982
Members:
Owen Sinclair, Peter McIntyre, Sean Hanna, Sue Crengle, Tony Walls
Brooke Hollingshead, Daniel Bernal, Edwin Reynolds, Mariana Traslosheros
ACT
Ministry of Health Attendees:
Reyes, Niki Stefanogiannis, Pippa Scott, Shama Kukkady, Imogen Roth, Sean
Driver
John Tait, Fran Priddy, Mike Williams, Simon Carson, Tara Swadi, Laurence
Guests:
Holding, Marion Leighton, Alison Cossar, Amy Alexander
Juliet Rumball-Smith, Danny de Lore, Helen Petousis-Harris, Ian Frazer, Andi
Apologies:
Shirtcliffe, Caroline McElnay, Matt Jones
INFORMATION
1.0
Welcome and Previous Minutes
Ian Town welcomed all Members and Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (22 March 2022) were accepted.
OFFICIAL
2.0
Findings of the Ka Matau, Ka Ora study
THE
The findings of the study were shared with CV TAG:
•
The study looked at antibody titres following vaccination 28 days after a second dose of the Pfizer
vaccine. It included 300 individuals aged 16 and over and was oversampled for people over 65,
Māori and Pacific peoples.
UNDER
•
The study looked at differences in immunogenicity in relation to comorbidities, ethnicity and age.
There was a uniformly good response to the vaccine, with high titres of both binding and
neutralising antibodies across different ages and ethnic groups in New Zealand. It was noted that
ethnicity had no impact on immune response in this study
•
The neutralising antibody response to the Omicron variant was reduced, with a less robust
RELEASED
response compared to that against the ancestral, Beta, and Delta strains, similar to what has been
observed internationally.
•
Data about a booster (3rd) dose should be available in approximately 2 months.
3.0
Future of the National Immunisation Programme
The plans for the future National Immunisation Programme were broadly outlined:
•
Learnings from the COVID-19 response will be applied to the wider schedule. It was noted that the
influenza vaccination programme was set to begin this week (April 1st)
Document 5
•
Work is underway to ensure the Programme has a clear presence in the new entities and to
ensure that successful operational delivery structures from the COVID-19 vaccination rollout are
maintained.
•
CV TAG emphasised a need for Treaty and equity obligations to be a focus within the structure.
4.0
Vaccine Rollout
An update was given on the vaccine rollout.
•
Approximately 2.57 million booster vaccines have been administered.
•
The current rate of vaccination in 5–11-year-olds is at 54%. Further work on understanding the
drivers of low uptake is underway.
5.0
Further booster doses for elderly
A summary of the memo was outlined noting the main points and draft recommendations:
1982
•
The ATAGI recommendations and the need for pragmatism from a service delivery point of view
were noted, with an evidence-based approach using data from local hospitalisation risk wherever
ACT
possible.
•
It was noted that the reactogenicity and adverse events among participants in the study. The
vaccine is a reactogenic vaccine, with 78.6% (95%CI: 71.2-84.8) of people who received a second
booster dose reporting a local adverse event, and 42.9% (95%CI: 35-50.7) reporting systemic
adverse events.
•
The faster waning of protection among the elderly was noted, and there was seen to be a need for
protection in age groups aged 65 and older. A younger age band was seen to be needed for Māori
INFORMATION
and Pacific peoples due to the increased risk of severe disease and hospitalisation. Those living in
aged care and disability residential care were also seen to be at risk of increased transmission
and protection and were seen to need a further doses.
•
There was currently seen to be limited and insufficient evidence on the rate of waning in
populations with other health conditions, or in younger age groups who may be at increased risk of
OFFICIAL
workplace exposure e.g. healthcare workers, and it was noted only a couple of countries have
rolled out second boosters to these groups. This evidence will need to be revisited as more data
emerges.
THE
•
The timing of further boosters was discussed. This should be based on local data if possible (from
those hospitalised after a primary schedule and a booster), however this is not currently available.
There is limited data on this, and therefore it could be timed to align with the influenza vaccination
programme, and this option should be considered. Most other countries are recommending a
UNDER
fourth dose from 3-6 months after a third dose, or after infection.
•
The eligibility age for Māori and Pacific peoples for the influenza vaccine should be
consistent with the age for further booster doses of COVID-19 vaccine, and this would require the
National Immunisation Programme bringing down their eligible age to align with that for the
COVID-19 vaccine. This could be an opportunity to increase uptake of the influenza vaccine.
RELEASED
•
It was noted that immunocompromised individuals who received a third primary dose and fourth
dose as a first booster are also at risk of waning protection and should also receive a second
booster, nothing this would be their 5th dose (second booster).
•
Recommendations will be revised and finalised.
6.0
Novavax as a Heterologous Booster
A summary of the draft recommendations was outlined:
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 6
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 26 April 2022
Time:
11:00am to 12:00pm
Location:
Teams: s 9(2)(k)
Chair:
Ian Town
Danny de Lore, Elizabeth Wilson, Helen Petousis-Harris, James Ussher, Nikki
Members:
Moreland, Nikki Turner, Peter McIntyre, Sue Crengle, Tony Walls
Daniel Bernal, Edwin Reynolds, Juliet Rumball-Smith, Mariana Traslosheros
ACT 1982
Ministry of Health Attendees:
Reyes, Pippa Scott, Shama Kukkady, Sean Driver, Kayla Benjamin, Eloise
Williams, Richard Jaine
Guests:
Thomas Teunissen
Ian Frazer, Owen Sinclair, John Tait, Hilary Longhurst, David Murdoch, Sean
Apologies:
Hanna, Andi Shirtcliffe, Brooke Hollingshead, Alison Cossar Allison Bennett
INFORMATION
1.0
Welcome and Previous Minutes
Ian Town welcomed all Members and Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (29 March 2022) were accepted.
2.0
Active Monitoring - Post Vaccine Symptom Check - Update on Results
•
An update was presented by the Post Event team on Pfizer vaccination side-effects in the New
Zealand population. This survey is conducted in addition to CARM and done so through push text
messaging, with a focus on over sampling minority populations.
•
Results:
o Side effects seen in the general population:
▪
A similar number of reported events were seen with the booster compared to the
second primary dose (41% reported for booster and 42% for dose 2)
▪
No increase in myocarditis symptoms were reported after the booster dose relative to
dose 1 and 2 of the primary vaccination cause.
RELEASED UNDER THE OFFICIAL
o Side effects seen in 5–11-year-olds:
▪
A low rate of events was reported with 18% for dose 1 and 24% for dose 2
▪
For most tamariki, the reported side effects were often only minor such as injection site
pain.
▪
A low proportion of children who presented with side effects, missed school (2% after
dose 1 and 4% after dose 2). This was usually only 1 day or less.
Document 6
•
CV TAG noted the wording around “side effects”, suggesting “symptoms” is more appropriate.
Post Event team to follow up with provider about the wording of questions
3.0
COVID-19 Vaccine Independent Safety Monitoring Board Interim Report
•
The ISMB was published last week, this contained an update on NZ cases of myocarditis and
pericarditis.
•
CV TAG noted that New Zealand has reported a disproportionately high number of post
vaccination myocarditis compared to other countries such as US, Australia and Canada.
•
CV TAG members noted this could be due to discrepancies in reporting, case definition and
causality criteria between countries.
•
Specific questions
-
As the “Brighton Celebration Criteria” is being used for anaphylaxis, but is it also being
used for myocarditis?
1982
-
Number of deaths due to myocarditis reported by New Zealand are disproportionate
compared to Australia, US and Canada. Could there be some consultation to clarify
ACT
the criteria used to produce this number compared to other countries?
-
The discrepancies may be due to the detection of cases that are not vaccine
associated due to the higher reporting rates and higher diagnostic suspicion of
myocarditis and pericarditis in general i.e., sensitivity vs specificity and causality.
When considering the patterns following dose 1 and 2, could this be the case as many
alerts sent out are very specific in asking symptoms remotely related to myocarditis
pericarditis (i.e., anxiety)?
INFORMATION
Action: Follow up with Post Event Team whether WHO causality process for adverse events following
immunisation is used in this assessment.
4.0
Vaccine Rollout
An update on the vaccination rollout was given.
OFFICIAL
•
Approximately 2.6 million boosters have been administered with ~23% of 5–11-year-olds are
fully vaccinated.
THE
•
A plateauing has been seen across all age groups of the vaccine roll out. This is most
prominent within the 5–11-year-old age group.
•
Concern was raised that the vaccination numbers across all groups will not see a substantial
UNDER
increase
.
•
The vaccine roll out has been actively supported by Māori providers and schools.
5.0
CV TAG Recommendation Memos
The latest finalised memos were included in the agenda for noting:
RELEASED
Fourth dose for at-risk groups - Second boosters
•
Members noted the importance of increasing the uptake of the first booster dose in high-risk
individuals prior to the second booster dose rollout and consideration of uptake for not just those
over the age of 18 but across multiple age and ethnic groups
•
CV TAG noted that an equity gap has been identified in the uptake of the booster in high-risk
groups. Concern was expressed that the 50 – 65 age group for Māori and Pacific populations are
being left behind for first booster doses, emphasising that a 4th dose would increase the equity gap
seen with the current 1st booster (third dose) roll out.
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 7
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 10 May 2022
Time:
11:00am to 12:00pm
Location:
Teams:s 9(2)(k)
Chair:
Ian Town
Members:
Elizabeth Wilson, James Ussher, Nikki Moreland, Nikki Turner, Owen Sinclair,
Peter McIntyre, Sean Hanna
Andi Shirtcliffe, Chris Hedlund, Edwin Reynolds, Eloise Williams, Juliet Rumball-
ACT 1982
Ministry of Health Attendees:
Smith, Mariana Traslosheros Reyes, Pippa Scott, Shama Kukkady, Sean Driver
(Secretariat)
Guests:
Allison Bennett, Bonnie Jones, Amy Auld
Danny de Lore, David Murdoch, Ian Frazer, Helen Petousis-Harris, Nikki Turner,
Apologies:
Tony Walls Sue Crengle, John Tait, Daniel Bernal, Alison Cossar, Susanna
Chung
INFORMATION
1.0 Welcome and Previous Minutes
Ian Town welcomed all Members and Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (26 April 2022) were accepted.
2.0 Vaccine Rollout
•
Approximately 2.45 million booster doses have been administered to date and ~119,000 tamariki
have been fully vaccinated. Doses continues to increase but incrementally.
•
A stubborn plateau of vaccine uptake is still present in the 5-11 age group.
•
A fourth dose (second booster) is still only available when prescribed by medical practitioners. The
Government is working to establish a legal mechanism for wider availability.
•
It was noted that the equity gap seen throughout the vaccine rollout will require a full system
examination.
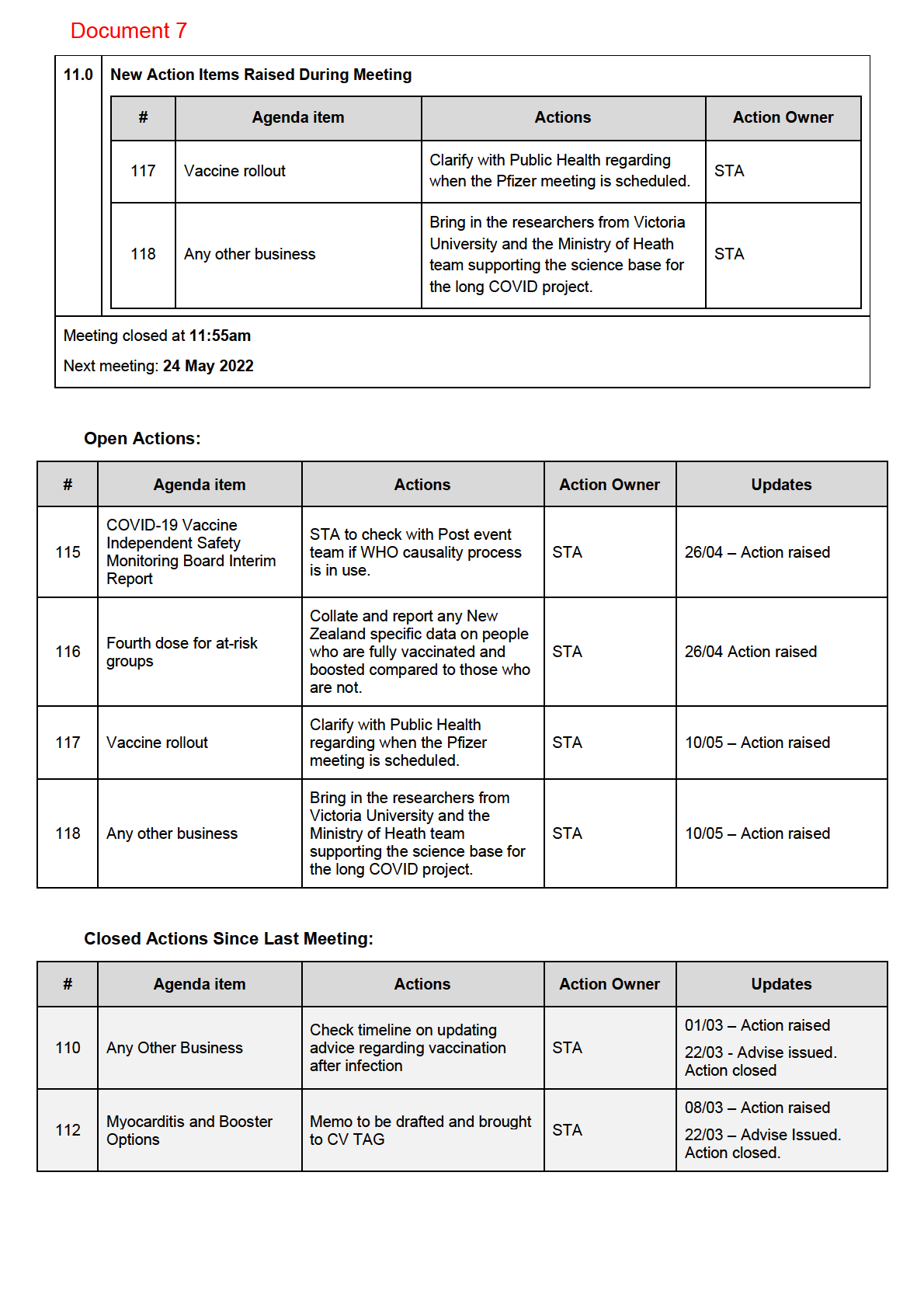
ACTION: Clarify with Public Health regarding when the Pfizer meeting is scheduled.
RELEASED UNDER THE OFFICIAL
3.0 Aging-in the 3rd Primary Dose
•
A brief summary was provided about processes for handling such requests outside of the CV TAG
framework.
4.0 CV-ISMB Interim Report: Response to questions raised last meeting
•
It was noted in the previous CV TAG meeting that New Zealand was potentially overreporting
myocarditis rates compared to other countries. However, it was confirmed that Brighton Collaboration
Document 7
definitions were being used for myocarditis/pericarditis by CV-ISMB, rather than NZ specific
definition.
5.0 Definitions of Fully Vaccinated
•
The definition of up-to-date (fully vaccinated) for vaccination was discussed, with draft guidance
provided around:
• How long after infection SARS-CoV-2 someone is considered up-to-date with vaccination
• The maximum time from a previous dose someone would be considered up-to-date with
vaccination.
• Which overseas schedules (primary and booster) could be considered up-to-date.
•
CV TAG does not currently recommend boosters in those under 18 years of age.
•
Policy, NIP and STA representatives will meet to clarify the purposes for which the definition of ‘up-
1982
to-date’ for vaccination might be used and consequently what the definition should provide. Ongoing
discussion will occur with CV TAG to answer these questions.
ACT
•
A request was made by DPMC for rapid provision of this advice (on 17th May, for same day advice).
This has been postponed until advice is finalised.
6.0 Future Vaccine Strategy
•
The Future Vaccine Strategy work was introduced to CV TAG, outlining questions which will require
input from the group.
•
Follow up meetings to discuss the questions will be arranged with oversight from STA and Policy
teams.
INFORMATION
•
A future meeting was planned between now and the next CV TAG meeting due to the short timeline
with CV TAG members, with initial responses required by 17 May.
•
It was noted that some questions required a public health-based approach and an ‘equity-first’
structure.
OFFICIAL
7.0 CV TAG Recommendation Memos THE
The latest finalised memos were included in agenda for noting:
•
Novavax as a Heterologous Booster has been issued.
8.0 Next Steps/Decisions Pending
UNDER
None.
9.0 Any Other Business
•
CV TAG members requested information about long COVID.
ACTION: Bring in the re
RELEASED searchers from Victoria University and the Ministry of Heath team supporting the
science base for the long COVID project.
10.0 Agenda Items for Next Meeting
None.
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 8
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 24 May 2022
Time:
11:00am to 12:00pm
Location:
Teams: s 9(2)(k)
Chair:
Ian Town
David Murdoch, Nikki Moreland, Nikki Turner, Owen Sinclair, Peter McIntyre,
Members:
Tony Walls
Andi Shirtcliffe, Daniel Bernal, Edwin Reynolds, Eloise Williams, Euan Russel,
ACT 1982
Ministry of Health Attendees:
Juliet Rumball-Smith, Kayla Benjamin, Mariana Traslosheros Reyes, Pippa
Scott, Sean Driver
Guests:
John Tait, Richard Jaine, Susanna Chung, Kris Golding
Danny de Lore, Elizabeth Wilson, Helen Petousis-Harris, Ian Frazer, James
Apologies:
Ussher, Sean Hanna, Sue Crengle, Allison Bennett, Alison Cossar, Amy Auld,
Bonnie Jones, Jim Miller, Shama Kukkady
INFORMATION
1.0
Welcome and Previous Minutes
Ian Town welcomed all Members and Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (10 May 2022) were accepted.
2.0
Vaccine Rollout
• An update was provided on the vaccine rollout. Approximately 2.65 million booster doses have
been administered and ~122,000 2nd paediatric doses, roughly one quarter of all eligible tamariki
are fully vaccinated.
• A stubborn plateau of vaccine uptake is still present in the 5-11 age group.
• A request was made to provide more information around levels in some key populations at risk of
severe COVID-19.
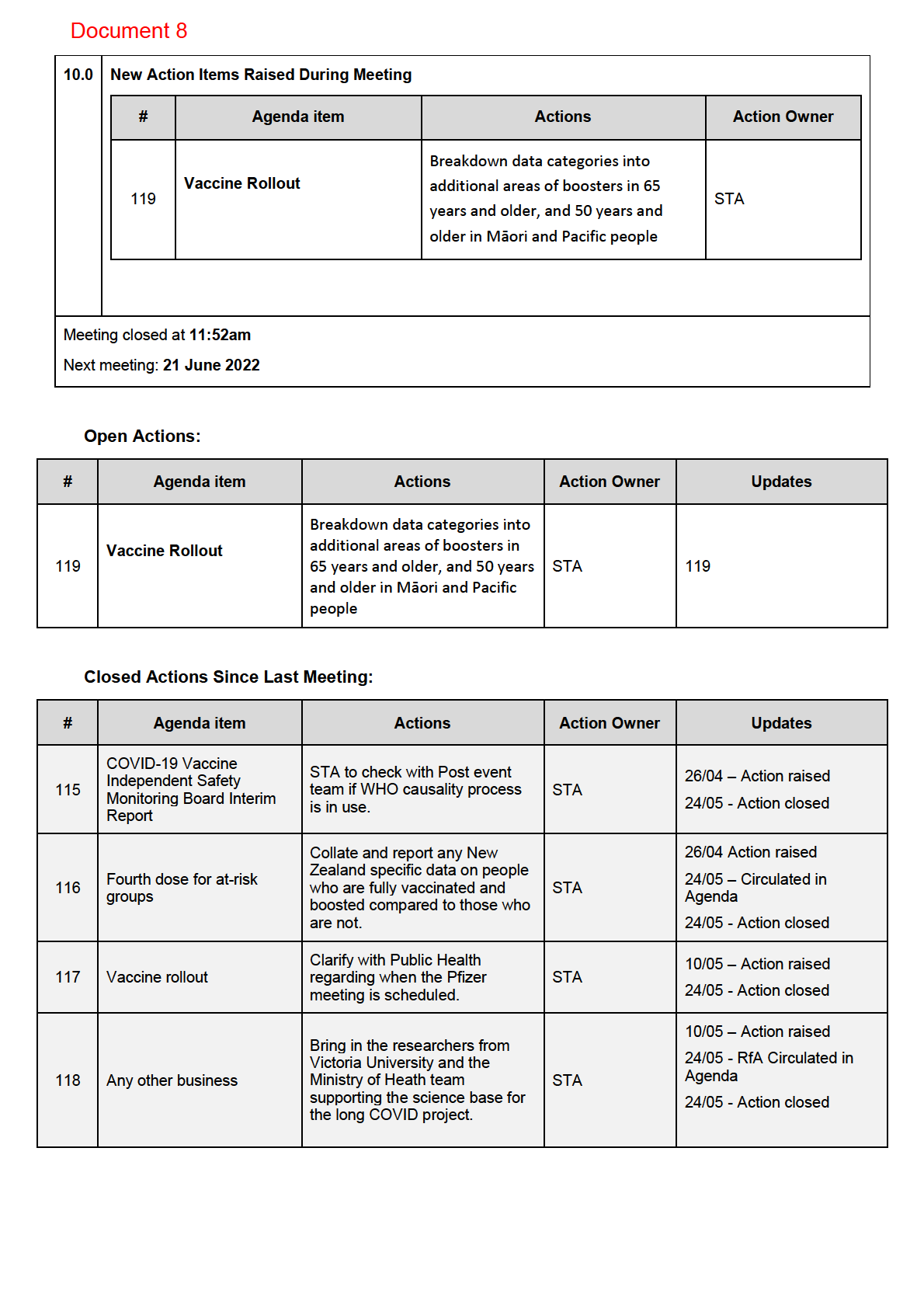
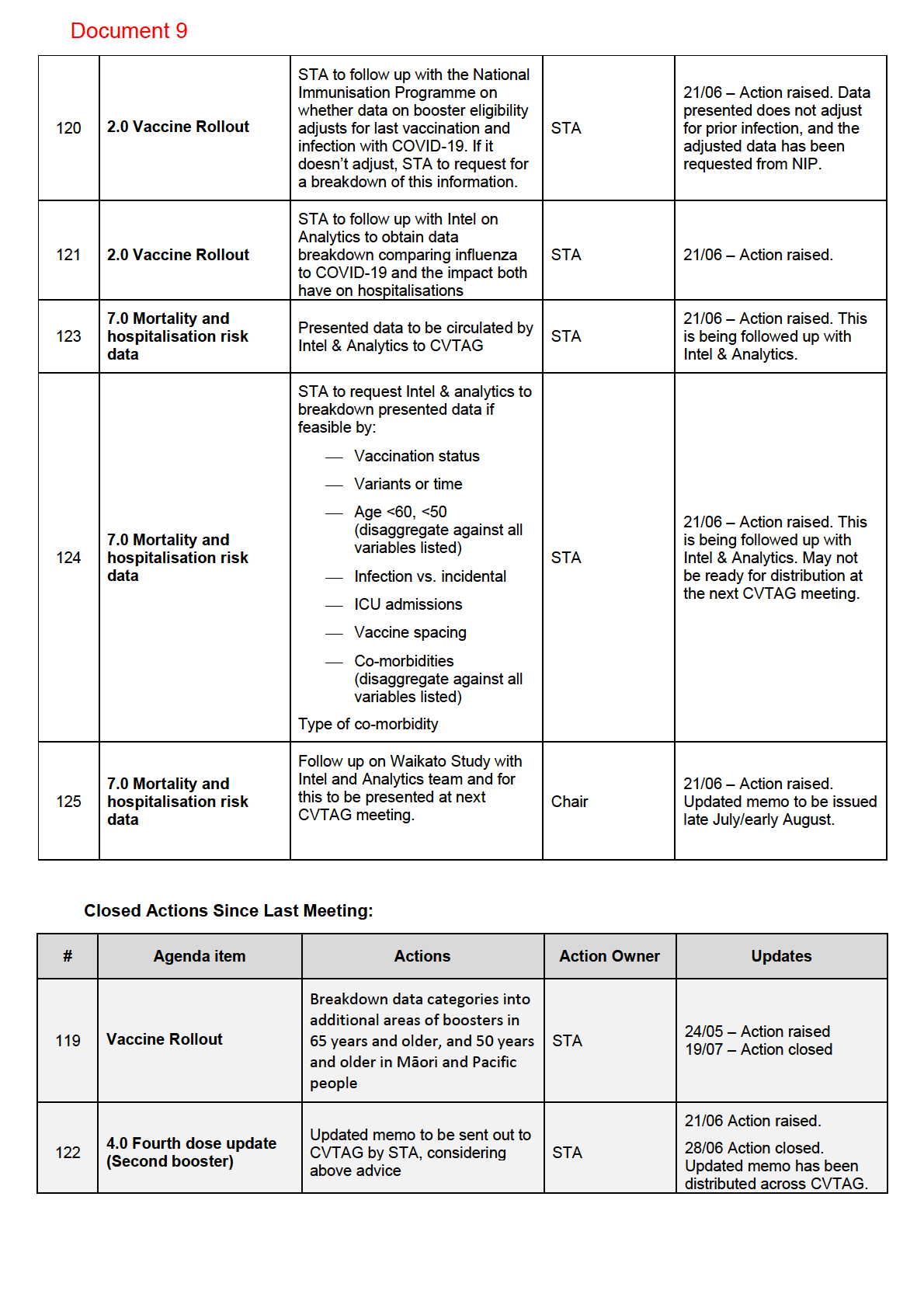
ACTION POINT: Breakdown data in vaccine report to show booster uptake among individuals aged 65 years
and over, and Māori and Pacific people, aged 50 years and over.
RELEASED UNDER THE OFFICIAL
3.0
Development of a National Immunisation Strategy
• Questions relating to the future vaccine strategy have been divided into sections requiring input
from the CV TAG, STA, or assigned to other leads for appropriate response.
• Preliminary answers for questions relevant to CV TAG were shared with the members for feedback.
o
The CV TAG discussed and advised on multiple topics, including the goals of the future
vaccine strategy in capturing the wider picture of long-term health and wellbeing.
Document 8
o
Equity issues in this area are still a concern, noting that there are also still many children yet
to be fully vaccinated. It was noted that an additional meeting with key experts will take
place, in order to facilitate a structured engagement on equity advice on vaccines not just
for COVID-19 but for the future of childhood immunisation in general.
o
There was also discussion on gaps in the current portfolio and the future decisions of what
vaccines to buy and vaccine supply, noting the continuing need to monitory new vaccine
technology and the frequency of future vaccination.
• The need for a meeting with Pfizer was raised. Clarification with Policy team as to when this will be
scheduled.
4.0 Up-to-date vaccination status
• The Request for Advice document on ‘up-to-date vaccination’ was circulated. This document
provides guidance around being ‘up to date’ with vaccination, with considerations including
1982
duration since the last dose of vaccine and recent infection, as well as vaccines received overseas
(e.g. non Medsafe approved vaccines).
ACT
• Members noted that there will be different circumstances for everyone coming from overseas, such
as those who may become due (for their next dose, ie a booster) while in New Zealand while also
noting that different vaccines have different schedules.
• CV TAG discussed the need for clarity and consistency in terminology between ‘overdue’, compared
to ‘maximum limits’, noting that ‘maximum limits’ was associated more with mandate terminology
than having a clinical relevance. For example, a person having completed a primary course, plus a
INFORMATION
booster, would be ‘up to date’, whereas if it’s been over 6 months since they had a primary course,
or COVID-19 infection, they would be considered ‘overdue’.
5.0 NZ Data Detailing Second Booster Eligibility
• CV TAG members noted the discrepancies in booster
OFFICIAL dose up-take and booster eligibility,
particularly in the immunocompromised group. Emphasis was placed on this information being
raised to colleagues and other chann
THE els in the sector. An information awareness plan is in place
that addresses the concern that there is a gap in vaccination here.
6.0 Long COVID Evidence Update
UNDER
• A report on the current long COVID evidence was shared ahead of the meeting with members of
the CV TAG.
• A Ministry of Health lead for this work was identified, and it was noted that a multidisciplinary
group of expert advisors is being formed around this topic.
RELEASED
7.0 Next Steps/Decisions Pending
None.
8.0 Any Other Business
• The CV TAG meeting schedule will move towards meetings every 4-6 weeks (currently fortnightly).
9.0 Agenda Items for Next Meeting
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 9
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 21 June 2022
Time:
11:00am to 12:00pm
Location:
Teams:s 9(2)(k)
Chair:
Daniel Bernal (acting)
Members:
Danny de Lore, Elizabeth Wilson, James Ussher, Nikki Turner, Peter McIntyre,
Sue Crengle, Tony Walls
Ministry of Health Attendees:
Andi Shirtcliffe, Edwin Reynolds, Euan Russell, Juliet Rumball-Smith, Kayla
ACT 1982
Benjamin, Pete Hanl, Sean Driver, Shama Kukkady
Guests:
Antoinette Righarts, John Tait, Kate Taptiklis, Olivia Pearless, Richard Jaine
Alison Cossar, Allison Bennett, David Murdoch, Harriette Carr, Helen Petousis-
Apologies:
Harris, Ian Frazer, Ian Town, Mariana Traslosheros Reyes, Nikki Moreland,
Owen Sinclair, Pippa Scott, Sean Hanna,
INFORMATION
1.0 Welcome and Previous Minutes
Daniel Bernal welcomed all Members and Attendees and Guests in his capacity as acting Chair of the
COVID-19 Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (24 May 2022) were accepted.
s 9(2)(ba)(ii)
CVTAG endorsement of Nuvaxovid as a booster (through email consultation) was discussed, noting:
•
It’s use as a booster should be acceptable
•
This is likely to be considered as an option by a very small sub-set of the population
RELEASED UNDER THE OFFICIAL
•
Acknowledgment of limited safety data, particularly for rare systemic side effects.
•
Use of Nuvaxovid as second booster should be acceptable as pragmatically there is no suggestion of
an increased risk from the first to second booster dose.
2.0 Vaccine Rollout
The latest up take of boosters was presented, including the roll out of 2.6 million booster doses, and a
breakdown by eligibility, ethnicity and age groups (including 50-64 and 65+).
Document 9
CV TAG noted more understanding of the data was needed to understand gaps (e.g., whether booster
eligibility was adjusted for last infection).
Feedback from CVTAG included:
•
The need to address inequities and get more people boosted, particularly for Māori, and those aged
50-64
•
Some noting better picture for Māori and Pacific people than initially envisaged
•
More breakdowns were requested, noting booster eligibility impacted by factors such as last
infection, and duration since primary course
•
Noting of vaccinating against influenza being a key priority (not shown in the data presented, but
commented on as reflection of the current impact on the health system from flu)
ACTIONS:
1982
•
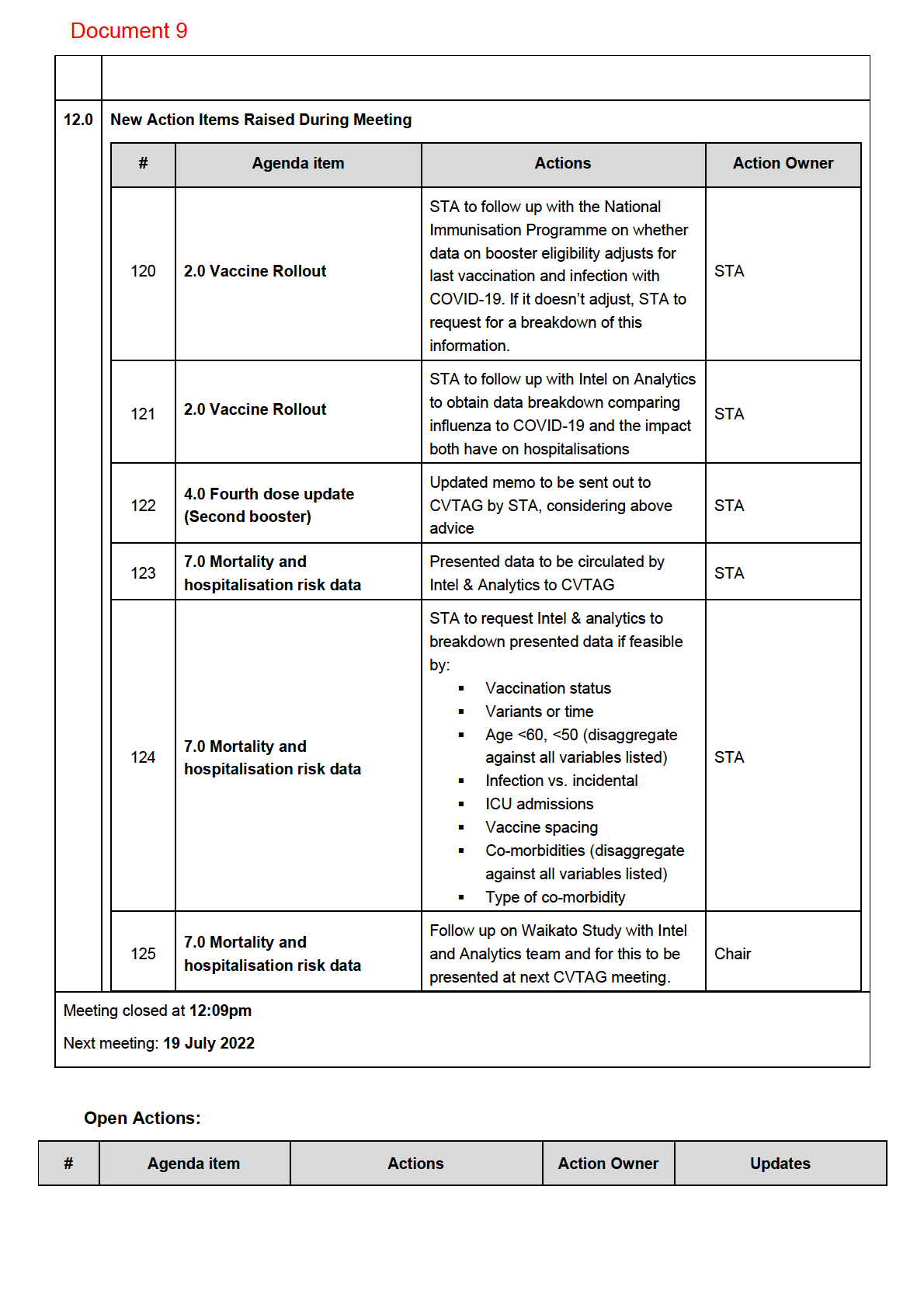
STA to follow up with the National Immunisation Programme on whether data on booster eligibility
adjusts for last vaccination and infection with COVID-19. If it doesn’t adjust, STA to request for a
ACT
breakdown of this information.
•
STA to follow up with Intel on Analytics to obtain data breakdown comparing influenza to COVID-19
and the impact both have on hospitalisations
3.0 Future Vaccine Strategy
Not discussed due to time constraints and will be brought back at a future meeting.
4.0 Fourth Dose Update (Second Booster)
INFORMATION
CVTAG discussed the draft memo, noting:
•
Pragmatically, tolerance and side effects for this booster isn’t expected to be any different to the first
booster, but safety data is very limited
•
Limited understanding of the risks of myocarditis/peric
OFFICIAL arditis among younger age groups should be
considered
THE
•
The booster appears effective on elderly and individuals that are at high risk, but effectiveness
among others is not clear
•
Evidence indicates marginal benefit for otherwise healthy healthcare workers from the second
booster
UNDER
CVTAG recommendations included:
•
Focus should remain on having at-risk populations receiving their first booster dose
•
Advice needs to align with ATAGI recommendations, rather than alignment with influenza roll out.
Keeping as close as possible to the ATAGI recommendations will keep the communications clear
RELEASED
and simple to understand from a technical perspective
•
There was no agreement on acceptability of second boosters for young and healthy healthcare
workers. There was discussion over making this permissible versus providing a “not recommended”
recommendation, but not clear agreement across the group.
•
Otherwise healthy pregnant women should be not recommended due to lack of safety data, aligning
with ATAGI recommendations.
•
The eligibility be considered for all available COVID-19 vaccines.
Document 9
ACTIONS:
•
Updated memo to be sent out to CV TAG, considering above advice
5.0 Booster Eligibility for 12-15s
•
Chair noted MedSafe has provisionally approved the Pfizer booster for 12+
•
Agreement obtained from CVTAG that previous recommendations remain, with insufficient evidence
to recommend boosters for young people aged 12-15, unless clinically very high-risk per past advice
issued.
6.0 Booster Eligibility for 5-11s
Item not addressed due to time constraints and deferred to a later time.
7.0 Mortality and Hospitalisation Risk Data
1982
Data from 1 Feb 2022 was presented on risk of COVID-19 mortality and hospitalisation, including
breakdowns by age and ethnicity.
ACT
CV TAG requested more in-depth breakdown of data including by vaccination status and older age groups.
Similar study currently being undertaken by the University of Waikato was mentioned and a request for this to
be presented at next update was made.
ACTIONS:
•
Presented data to be circulated by Intel & Analytics to CVTAG
INFORMATION
•
STA to request Intel & analytics to breakdown presented data if feasible by:
▪
Vaccination status
▪
Variants or time
▪
Age <60, <50 (disaggregate against all variables listed)
OFFICIAL
▪
Infection vs. incidental
THE
▪
ICU admissions
▪
Vaccine spacing
▪
Co-morbidities (disaggregate against all variables listed)
UNDER
▪
Type of co-morbidity
•
STA to follow up on Waikato Study with Intel and Analytics team and for this to be presented at next
CVTAG meeting.
8.0 Up-to-date vaccination status
CVTAG noted the Request-for-Advice, including update to terminology for what is considered ‘up to date’
RELEASED
9.0 Next Steps/Decisions Pending
None.
10.0 Any Other Business
11.0 Agenda Items for Next Meeting
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 10
Terms of Reference – 1982
COVID-19 Vaccine
ACT
Technical Advisory Group
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
01 March 2021
Document 10
Contents
Introduction ................................................................................................................................ 3
Context........................................................................................................................................ 3
Purpose and Function .................................................................................................................. 4
Membership ................................................................................................................................ 6
Duties and Responsibilities........................................................................................................... 8
Meeting protocols...................................................................................................................... 10
1982
Fees framework ......................................................................................................................... 11
Review of Membership .............................................................................................................. 12
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
2
Document 10
Introduction
The Ministry of Health (the Ministry) is the kaitiaki of the health and disability system in Aotearoa New Zealand.
We do this by providing a fair, effective, and sustainable system that people trust. The Ministry is responsible for
providing active stewardship and leadership across the health and disability system to ensure it provides people
with the highest level of care, regardless of who they are or where they live.
The COVID-19 pandemic has rapidly evolved internationally and in Aotearoa New Zealand. Responding to COVID-
19 in a very rapidly changing environment is a significant ongoing challenge.
1982
The Government's overall public health strategy in respect of the COVID-19 pandemic affecting New Zealand is
elimination. That is, to apply a range of control measures to stop the transmission of COVID-19 in Aotearoa New
Zealand.
ACT
There are four pillars to our elimination strategy, these are:
• border controls
• robust case detection and surveillance
• effective contact tracing and quarantine
• strong community support of control measures
INFORMATION
The Ministry has established the COVID-19 Health System Response Directorate (the Directorate) to give effect
to the elimination strategy. The Ministry is working to ensure the response to COVID-19:
• is evidence-based
OFFICIAL
• is consumer-centred
• is equity-focussed and guided by the Treaty of Waitangi
•
THE
effectively manages clinical and public health issues and risks
• supports an open and transparent culture
• has a continuous quality improvement and safety focus
• monitors and reviews clinical processes and outcomes
UNDER
• guides the development of the Ministry and All of Government strategies to address COVID-19.
Context
RELEASED
In May 2020, Cabinet agreed the COVID-19 Vaccine Strategy [CAB-20-MIN-0382 refers]. The objective is to
secure access to sufficient quantities of safe and effective COVID-19 vaccines, to implement our preferred
immunisation programme at the earliest possible time.
On 10 August 2020, Cabinet agreed to purchase a portfolio of COVID-19 vaccines [CAB-20-MIN-0382 refers]. The
portfolio manages several dimensions of risk and uncertainty, such as:
•
uncertainty about individual vaccine candidate performance or technology platforms
3
Document 10
•
unknown long-term vaccine effectiveness and suitability for particular population groups
•
delays in development, manufacturing, and delivery to purchasers
•
global supply constraints (including in upstream supply chains)
•
the potential for source countries to restrict export of vaccines, and
•
delays or failure to achieve regulatory approval.
To have confidence in the portfolio’s ability to manage risk and support the immunisation programme, we have
deliberately “over-purchased” vaccine stocks.
A diverse portfolio increases the chances of having suitably effective vaccines on hand. It gives our immunisation
programme the best possible range of vaccine options to choose from to protect our population from the risk
and impact of COVID-19.
1982
The purchase of multiple vaccines means that we now must manage:
ACT
a.
variability in efficacy of vaccines for different population groups
b.
potential oversupply of vaccines, if all vaccines in our portfolio successfully gain regulatory
approval and we are required to pay for them
c.
significant overlap in the delivery schedule for multiple vaccines and at significant volumes
d.
complexity of delivery, if we have multiple vaccines available for use and need more than one to
INFORMATION
cover our desired populations due to the volumes available
e.
increased cost, as purchasing multiple vaccines can significantly increase or decrease the overall
cost of the portfolio.
OFFICIAL
Primarily, the impacts of the Portfolio describe above mean that the Ministry of Health will have to advise on
which vaccines to use to support a successful immunisation programme and which not to use, given that we are
THE
likely to have an oversupply of vaccines.
UNDER
Purpose and Function
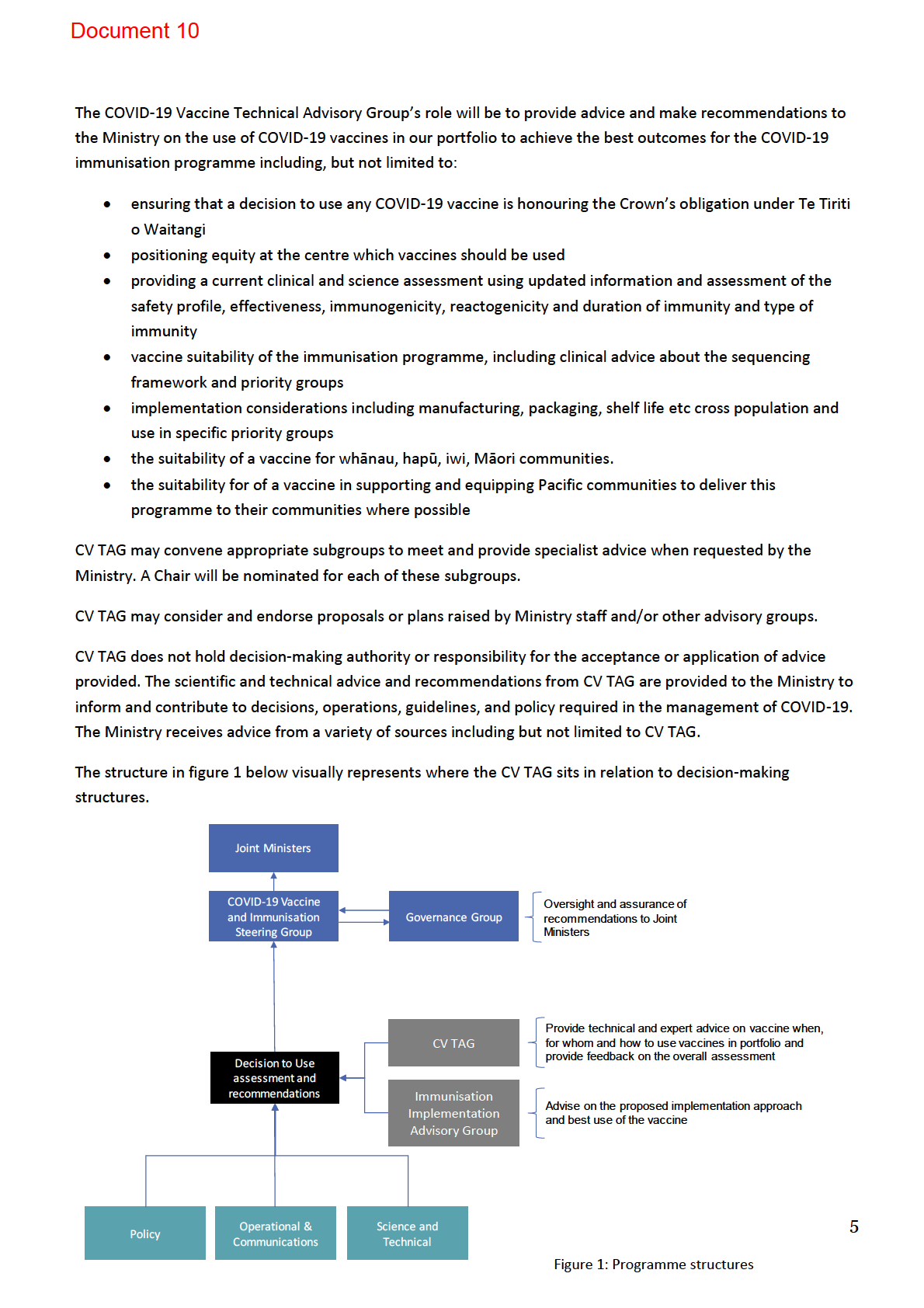
The COVID-19 Vaccine Technical Advisory Group (CV TAG) will provide independent, practical advice to the
Ministry of Health (the Ministry) where requested for the COVID-19 Vaccine and Immunisation Programme,
RELEASED
including for whom a COVID-19 vaccine could be used, if and when a vaccine(s) becomes available as part of the
portfolio of vaccines that have been purchased.
The advice provided by CV TAG will consider updated clinical and technical advice and assessment of vaccine
characteristics and suitability for different priority groups.
The advice provided by the Advisory Group on whether to use or not use a vaccine is independent from
Medsafe’s role in providing regulatory approval. CV TAG provides advice on how to use vaccines in our portfolio
that have achieved regulatory approval from Medsafe.
4
 1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 10
CV TAG is guided by Te Tiriti o Waitangi principles as they apply to the health and disability sector; tino
rangatiratanga, equity, active protection, options, and partnership. This involves the managing of the response
to COVID-19 pandemic through evidence-based approaches with the aim of achieving equity of outcomes, and
contributing to wellbeing for all, including Māori and Pacific peoples.
CV TAG advice differs from that of the Immunisation Implementation Advisory Group (IIAG) in that it focuses on
whether a vaccine is suitable for use and for whom that would best support the immunisation programme. The
IIAG will provide advice on the operational and implementation considerations of vaccine once a decision to use
has been made.
1982
Membership
ACT
The COVID-19 Vaccine Technical Advisory Group is to provide expert, multi-disciplinary expertise on the latest
scientific, clinical, and technical evidence-based, expert advice on COVID-19.
Members of the COVID-19 Vaccine Technical Advisory Group will be asked to:
• provide the Ministry with rapid advice based on the most up to date clinical, scientific, and technical
evidence on COVID-19
INFORMATION
• identify emerging scientific, clinical, or technical issues and inform the Ministry on ways this advice could
be used to design the response to COVID-19 pandemic within Aotearoa New Zealand
• suggest approaches and actions to enact the principles of Te Tiriti o Waitangi and achieve equity for
OFFICIAL
Māori
• advise on ways to reduce inequalities for groups in society negatively impacted by COVID-19, including
THE
but not limited to; ethnicity, dis/ability, geographic location, age, gender, health status, socioeconomic
position, living and working conditions
• identify areas requiring further research, and/or reviews to inform ongoing response.
UNDER
The appointment of Members of CV TAG is based on their personal, technical and specialist expertise. This
includes acknowledgement of Member’s understanding of the systems, structures, stakeholders, and in-depth
specialist knowledge in their respective disciplines, with a view to supporting the effective development and
application of technical advice.
Members will focus on the c
RELEASED ore scientific, technical, and/or clinical basis for advice, referencing the evidence
base alongside the rationale for advice in the context of operational limitations and/or precedent. CV TAG will
comprise equitable Māori representation, alongside representation from Pacific and the disability sector.
Membership of CV TAG will be confirmed through an appointment letter from the Chairperson and a
confirmation response from the Member.
Chairperson
CV TAG will be led by Dr Ian Town, Chief Science Advisor, Ministry of Health
6
Document 10
Members
CV TAG has a standing membership comprised of external (main job is not Ministry employee) technical experts
from disciplines relevant to the response required in the phases and alert levels of the COVID-19 pandemic. The
membership also comprises of equitable Māori representation, alongside representation from Pacific and the
disability sector.
Ex Officio Advisors
Technical experts within the Ministry can also have membership within the group in the capacity of Ex Officio
Advisors as invited by the Chairperson.
Members of CV TAG must agree:
1982
•
to keep all information provided to them strictly confidential and, except as expressly permitted, not
ACT
share, publish, copy in whole or in part or modify or adapt any confidential information in any way
without the Ministry’s prior written consent which may be given or withheld in its absolute discretion.
•
not to use any confidential information for any purpose other than participating in CV TAG activities
without the Ministry’s prior written consent which may be given or withheld in its absolute discretion.
• Where the CV TAG Member wishes to use the information provided for research purposes, a detailed
letter seeking permission to use the data, and describing how the data will be used i
INFORMATION ncluding the ethical
safeguards that will be used to protect the integrity of the data, must be submitted to the Chief Science
Advisor for approval, prior to any research occurring. The Ministry may put conditions on the use of
data, including acknowledgements as appropriate.
• Pre-existing intellectual property rights relating to the pro
OFFICIAL vision of advice remain the property of their
current owner. New intellectual property rights in work created for the Ministry as part of CV TAG
become the property of the Ministry when t
THE hey are created unless otherwise agreed in writing.
•
to declare any real or perceived Conflicts of Interest - CV TAG Members should perform their functions
in good faith, honestly, fairly, impartially, responsibly and avoid situations that might compromise their
integrity or otherwise lead to conf
UNDER licts of interest. The Conflict of Interest form provided by the Ministry
must be completed, returned to [email address].
• The Member must inform the Ministry upon becoming aware of the existence of the possibility of a
conflict arising after completing the form. A register of Conflict of Interest will be recorded and
addressed through the processes outlined above.
RELEASED
• Members of CV TAG are
not authorised to make statements on behalf of the COVID-19 Vaccine
Technical Advisory Group or the Ministry. The Ministry has strict protocols for managing media enquiries
and all such requests should be directed to [email address] and copied to the STA email COVID-
[email address].
• Members have the right to comment to the media on any matter in their professional capacity, as long
as they do not attribute the comment to CV TAG or imply that they are speaking on behalf of CV TAG or
wider Ministry. If a Member is forewarned of being asked to comment to the media, they should advise
7
Document 10
the STA accordingly. If a Member is not forewarned, they should advise the STA immediately after
making comment to the media.
• Members are not authorised to commit COVID-19 Vaccine Technical Advisory Group, any Members of it,
or the Ministry to any financial or legal commitments or to otherwise purport to act as agents for the
Ministry.
Membership of CV TAG will be for a period of 12 months with the option for a further extension as offered
by the Ministry.
A register of membership of CV TAG is maintained and kept within the STA filing system within the Ministry
and accessible to Ministry staff. Names of CV TAG Members and any other information provided by
1982
Members are subject to the Official Information Act 1982 and the Ministry will be required to release such
information on request under that Act unless there are valid reasons for withholding the information under
ACT
the Act.
Duties and Responsibilities
INFORMATION
The duties and responsibilities for the Chairperson, Members and Ex Officio advisors are outlined below.
Duties and responsibilities of the Chairperson of COVID-19 Vaccine Technical Advisory Group
The Chairperson agrees to:
OFFICIAL
• provide leadership and ensure the group retains a focus on its scope as defined in this Terms of
Reference and priorities as determined by t
THE he Ministry
• determine suitability of CV TAG as the recipient of requests for advice, work to be commissioned, tasks,
and facilitators of consultation
• ensure meetings are duly convened and that a quorum of Members is present each meeting
UNDER
• ensure meetings are conducted in an efficient, effective, and focused manner
• ensure the group has the required information to permit provision of advice and to make
recommendations
• consider the principles of Te Tiriti o Waitangi in every action, through ensuring CV TAG is supported to
interact and act with equity as a key consideration, and provides advice that is congruent with these
RELEASED
obligations
• appoint Members to CV TAG based on scientific and technical expertise and the need for effective
representation and tino-rangatiratanga (self-determination and autonomy) of Māori and Pacific peoples
• facilitate communications internally and externally, including; with other key stakeholders as
appropriate; presenting advice and recommendations to decision makers after each meeting; and
summarising any aspects of discussion or advice that should or should not be communicated by
Members
• ensure minutes are taken during meetings and approval given for the minutes as an accurate record of
the summary of the meeting.
8
Document 10
• ensure actions and recommendations are noted and actioned within agreed timeframes
• act as a key contact point for agenda items, responses, absences, and delegations to the meeting, and
will be informed of all activities requested of and undertaken by CV TAG.
Duties and responsibilities of a Member of COVID-19 Vaccine Technical Advisory Group
CV TAG Members are not employees of the Ministry. They agree to:
• familiarise themselves with background material (if any) sent prior to and after meetings
• actively participate in meetings or provide feedback and/or comments as required
• undertake additional activities agreed by the group (such as commenting on advice or guidance,
providing research material, or contacts), and to alert the Chairperson to limitations on availability and
1982
interim delegation arrangements
• share expert knowledge and engage constructively in discussions, acting only in the role they are
ACT
representing and within their scope of expertise
• individually ensure familiarity with, and provide advice that is congruent with the principles and
obligations of Te Tiriti o Waitangi in ensuring the active protection of Māori health, achieving equity
across access, quality of care and outcomes
• ensure that all activity and advice is undertaken with consideration of and respect for equity of
outcomes across all peoples of Aotearoa New Zealand, including but not limited to; ethnicity, dis/ability,
geographic location, age, health, gender and socioeconomic position, living and working conditions
INFORMATION
• lead/facilitate the completion of respectively owned action items within the agreed timeframes
• assume collective responsibility for advice through; working together in a collegial manner; seeking
consensus on provision of advice wherever possible; and noting any unresolved differences of opinion,
limitations of evidence or opportunity for consultation, or concessions made due to time or logistical
OFFICIAL
constraints
• exercise all due professional care and diligence in the performance of their obligations under these
THE
Terms of Reference in accordance with the standards of skill, care, and diligence normally practised by
suitably qualified and experienced persons in performing services of a similar nature.
• to make themselves available for meetings convened for the purpose of providing advice to the Ministry
as described above.
UNDER
Duties and responsibilities of an Ex Officio Advisors of COVID-19 Vaccine Technical Advisory Group
CV TAG Ex Officio Advisors are employees of the Ministry who hold specialist technical positions in a relevant
field. The Ex Officio Advisors are appointed by the Chairperson.
RELEASED
The Ex Officio Advisors agree to:
• represent the Ministry by presenting requests for advice or commissioned pieces of work and providing
relevant background information, context, and communications to support the Members in providing
advice which is shaped for the question or issue at hand
• familiarise themselves with background material (if any) sent prior to meetings
• share expert knowledge and engage constructively in discussions, acting only in the role they are
representing and within their scope of expertise
9
Document 10
• communicate relevant information, activities, decisions, and issues of interest from the Ministry to CV
TAG, and vice versa, through endorsed communication channels and methods
• individually ensure familiarity with and provide advice congruent with the principles and obligations of
Te Tiriti o Waitangi in ensuring the active protection of Māori health and achieve equity across access,
quality of care and outcomes
• ensure that all activity and advice is undertaken with consideration of and respect for equity of
outcomes across all peoples of Aotearoa New Zealand, including but not limited to; ethnicity, dis/ability,
geographic location, age, gender, health, and socioeconomic position, living and working conditions.
Secretariat of COVID-19 Vaccine Technical Advisory Group
1982
The Secretariat is not a Member of CV TAG supports the group and the Chairperson with secretariat duties
ACT
including
• disseminating information required for each meeting
• writing-up the agenda as directed by the Chairperson
• writing the minutes and disseminating these within the group
• update any new Members or additional Members with the Terms of Reference
• receive and store the Conflict of Interest declarations
INFORMATION
• receive fee claims and organise fees payments
• assist the Chairperson with the onboarding arrangements with Members.
OFFICIAL
Meeting protocols THE
Secretariat
The Ministry will ensure adequate secretariat support and other support as may be required from time to time,
UNDER
for CV TAG to carry out their mandate efficiently and effectively.
Meetings coordination
Coordination of the meetings will be managed by the Secretariat through direction of the Chairperson. This will
include all the logistics, documentation, and administration. Members will receive relevant documentation
RELEASED
through email or other digital tools used within the Ministry.
Members must have regular access to electronic and digital tools in which CV TAG meetings are conducted.
Meetings conducted in workplaces must remain confidential and not visual or audible to workplace colleagues.
Delegates
Members will attend all meetings whenever reasonably possible and delegates are not permitted. Apologies
must be in writing (email) to the Chairperson and Secretariat prior to the meeting.
10
Document 10
Other attendees
Guests with relevant expertise may be invited to discuss specific issues and when attending the whole meeting
will abide by the same Terms of Reference.
Non-Members may only attend by invitation of the Chairperson.
Quorum
A meeting quorum for CV TAG requires 50% of standing external Members, including the Chairperson.
The quorum for a meeting is the minimum number of Members required to make the meeting valid. If a meeting
is inquorate, it cannot make recommendations on behalf of the group. It can hold discussions and make
1982
recommendations for later confirmation or rejection by the group.
ACT
Official Information Act requests
All agendas, emails and other communication and information relating to the Network are subject to the Official
Information Act 1982, and the Ministry may be required to release such information on request unless there are
valid reasons for withholding the information under the Act.
INFORMATION
Fees framework
The daily rate has been set in accordance with the Ministry’s Fees Framework and has been approved by the
Director-General of Health and may be paid to Members who are self-employed or privately employed.
OFFICIAL
Members who are paid for their time/employed through the wider state sector (eg they work for Universities,
THE
District Health Boards, Government departments and State agencies) are not personally eligible for a fee,
although on the production of an invoice, the Ministry can reimburse a government funded agency employing
organisation for the Member’s time.
UNDER
The membership register will indicate those Members that are eligible to claim a fee under the Fees Framework
and the level of the fee, based on the above declaration.
A working day of eight hours is the basis of the daily fee is calculation, with hourly pro-rata rates calculated
accordingly. A working day of longer than eight hours does not attract extra payment beyond the daily fee. The
daily fee applies to all work, including the work performed outside of meetings that is required for the group to
RELEASED
carry out its role (e.g. preparation, representing the group at other forums, or administrative work).
All fees and expenses (where agreed) are to be submitted either on a Ministry claim form or as an invoice.
Reasonable expenses are to be agreed in writing in advance and should be supported by tax invoices and/or
receipts.
Payments will be made in accordance with the Ministry’s accounts payable guidelines.
11
Document 10
Work outside of meetings that has been formally commissioned by the Ministry will be formally described in a
written request with anticipated days or hours of work required and the fee rate, which the individual or group
may accept or decline. Additional days or hours of work required must be agreed in writing with the Manager of
STA prior to commencement of the hours worked.
Guidance on organisations that form part of the wider state sector can be found on the SSC website.
For more information, please refer to the Cabinet Fees Framework.
Review of Membership
1982
ACT
Membership of the COVID-19 Vaccine Technical Advisory Group will be reviewed by the Deputy Chief Executive,
COVID-19 Directorate on or before December 2021.
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
12