Document 1
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 25 January 2022
Time:
11:00am to 12:00pm
Location:
Teams: S9(2)(k)
Chair:
Ian Town
Danny de Lore, David Murdoch, Elizabeth Wilson, Helen Petousis-Harris, James
Members:
Ussher, Nikki Moreland, Nikki Turner, Owen Sinclair, Pete McIntyre, Sean
Hanna, Sue Crengle, Tony Wal s
ACT 1982
Andi Shirtcliffe, Brooke Hollingshead, Caroline McElnay, Daniel Bernal, Juliet
Ministry of Health Attendees:
Rumball-Smith, Mariana Traslosheros Reyes, Niki Stefanogiannis, Phoebe
Currie, Liam McConnell, Chriselle Braganza
Guests:
John Tait; Ian Frazer, Edwin Reynolds, Fiona Cal aghan, Imogen Roth, Pippa
Apologies:
INFORMATION
Scott
1.0
Welcome and Previous Minutes
Ian Town welcomed all Members and Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (20 January 2022) were accepted subject to the following changes to item 10.
• It was requested that item 10 be amended to include boosters for 12-17-year-olds who are high-
risk, and boosters for 12-17-year-olds in general population.
2.0
Interval for Boosters
• The calls from some commentators to shorten the interval for a booster to 3 months were
discussed.
• Immunity does not wane at the same pace for all, and therefore it was argued that any changes to
recommendations should not be applied to al and should be based on age and risk factors.
• People aged over 50 or with high-risk conditions w
RELEASED UNDER THE OFFICIAL ere likely to benefit from a shorter interval,
however this age eligibility would need to be lower for Māori and Pacific peoples (e.g., 35-40) due
to the increased risk of hospitalisation, severe disease, and death. Some emerging evidence
shows a shorter interval between the second dose and the booster may lead to lower vaccine
effectiveness against symptomatic infection than longer intervals.
• Preliminary results from the VAANZ study were shared, which noted that 28 days post-second
dose, neutralisation against Omicron was low, demonstrating the importance of boosters.
Neutralisation against Delta remained high. However, it was noted that this was only one part of
the immune response. It has been requested that this data be shared with the Ministry.
Document 1
• Recommendations wil be drafted and shared with CV TAG for approval.
3.0
Heterologous Schedules for Booster Doses
• The Ministry of Health Policy team have requested advice be developed on heterologous booster
schedules, in case of supply issues with Pfizer.
• A rapid review conducted by STA on the data for safety, reactogenicity, and immunogenicity of
heterologous booster schedules was shared with CV TAG, looking at the use of AstraZeneca,
Janssen, Moderna or Novavax fol owing a Pfizer primary course.
• For participants primed with Pfizer, there were more local and systemic reactions after
AstraZeneca, Janssen, and Moderna, with these mostly being malaise and fatigue, however rates
were under 5%.
• Moderna appears to be the most reactogenic for those vaccinated with Pfizer, and alongside
Pfizer has a risk of myocarditis. However, Pfizer and Moderna offer the greatest protection as
boosters in terms of increasing neutralising antibody and T cell responses.
• Heterologous boosts increased antibody titres to a larger extent than homologous boosts, th
ACT 1982 ough
Pfizer as a booster protects slightly better and it was noted that Pfizer as a booster remains a
good option.
• No boosters were more or less impacted by variants, but Pfizer and Moderna increased
neutralising antibodies against Omicron.
• One possibility raised was that mRNA vaccines could be recommended for elderly and high-risk
populations due to the need for an increased immune response, with Novavax or Janssen an
option for younger populations.
INFORMATION
• A supply of Novavax wil also be important for a smal group who have had severe reactions to
Pfizer, or for those hesitant for an mRNA vaccine.
• This topic wil be kept under rolling review by STA for when advice is requested from the
programme. This advice wil also become relevant as more people return to New Zealand with
varying vaccine schedules.
4.0
Booster doses for pregnant people at 4 months
• Draft recommendations to endorse changes to the timing of boosters in pregnant people were
shared with CV TAG. Changes to this advice were made at pace based on updates to
international guidance, noting that formal advice and endorsement from CV TAG would be sought.
• There have been no adverse events or safety signals from the rol out of the vaccine in pregnant
people despite large numbers being vaccinated, and the risk of COVID-19 in this population is
clear. It was agreed that this should be brought forward from 6 months to align with the timing for
the general population.
• A formal memo with CV TAG’s updated recommen
RELEASED UNDER THE OFFICIAL dations wil be issued.
5.0
4th Dose (first booster) for severely immunocompromised people
• Draft recommendations to endorse changes to the timing of boosters in severely
immunocompromised people were shared with CV TAG. Changes to this advice were made at
pace based on updates to international guidance, noting that formal advice and endorsement from
CV TAG would be sought.
• Data on the safety and efficacy of a fourth dose (first booster) for severely immunocompromised
people who received three primary doses is emerging and promising. A longer interval for a
booster dose in this population may cause harm, given the rapid degree of waning protection
Document 1against Omicron. Formal advice on boosters has not been given for this group who are more at
risk, and therefore a booster dose at 4 months was seen as beneficial.
• A formal memo with CV TAG’s recommendations wil be issued.
6.0
4th Dose (second booster) for high-risk populations
This item was not discussed.
7.0
5–11-year-olds safety data
An update on the vaccination rollout of boosters and paediatric doses was given:
• A breakdown of doses administered by age and ethnicity was requested by CV TAG, and this wil
be a formal agenda item next week for discussion.
• Some smal groups have filed affidavits to halt the rol out programme but have not been
successful. The Ministry team have been providing advice to Crown law, and if CV TAG members
are approached about the injunction, they are welcome to refer queries to the Ministry of Health.
• Concern was also raised that insufficient vaccinators feel confident to administer the paediatric
ACT 1982
vaccine, and further mentoring is required. This would be exacerbated in provincial and rural areas
where access to the paediatric formulation and trained vaccinators was understood to be lower.
Pharmacists have also never vaccinated this population.
• A school-based rollout targeting Decile 1 to 4 schools was seen as an option to reach more Māori
and Pacific 5-11-year-olds, alongside an increase in communication relevant to communities.
• Some CV TAG members mentioned that parents are requesting their children have access to a
second dose earlier than 8 weeks, and formal communication or guidance from the Ministry was
INFORMATION
requested prior to the formal safety review in February. No children should be receiving second
doses.
• Some high-risk children may benefit from an earlier second dose, so these children could be
prioritised, however, clear guidance on which groups are considered high risk is required.
• A statement on 5-11-year-olds and the protection provided by two doses is being written by the
Science and Technical Ad isory team to pre-empt calls for booster doses in this age group.
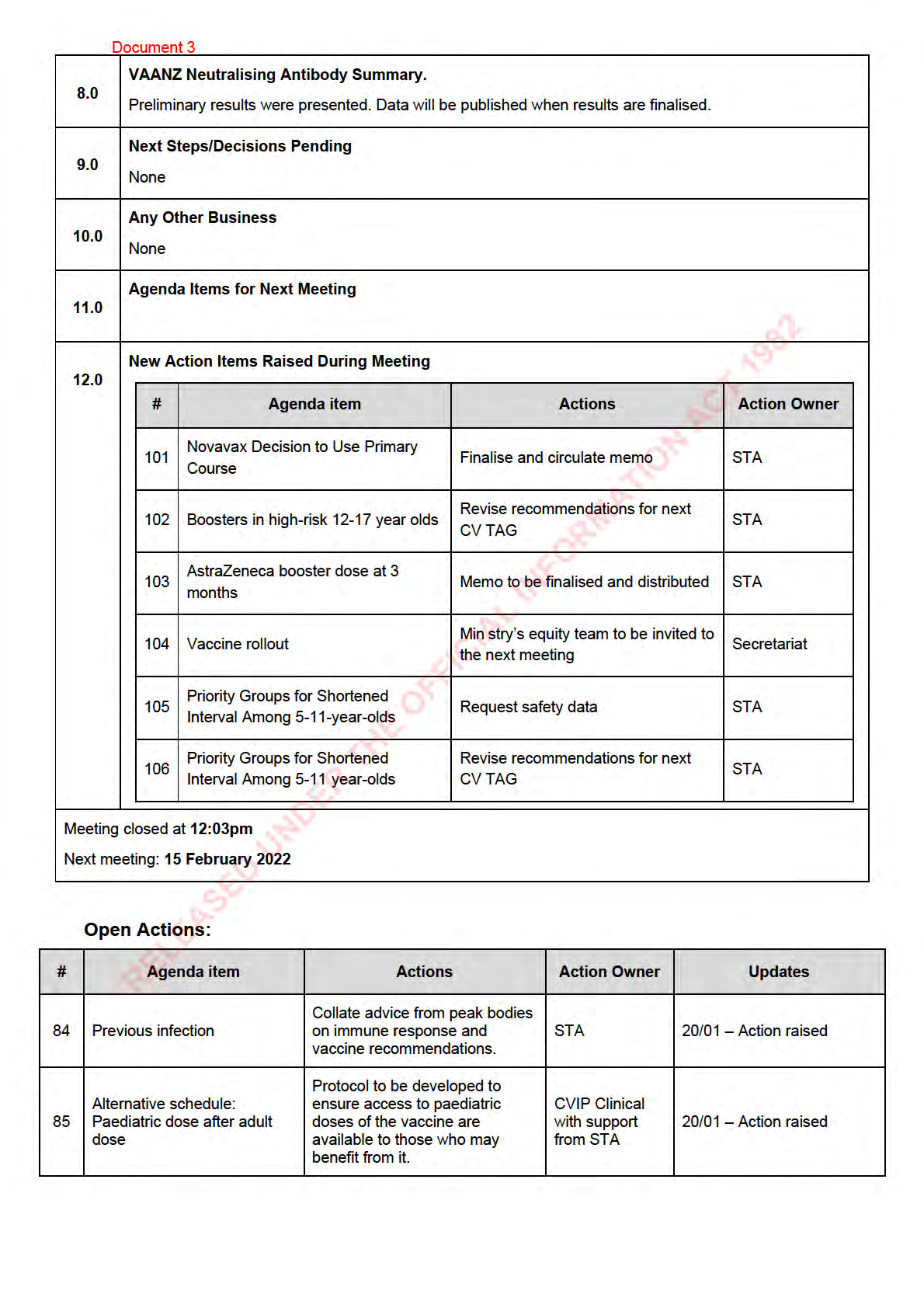
8.0
Next Steps/Decisions Pending
None.
9.0
Any Other Business
Booster rol out
An update was provided on the booster rol out.
• Over one mil ion doses have now been administered.
• A breakdown of doses administered by age and ethnicity was requested by CV TAG, and this wil
RELEASED UNDER THE OFFICIAL
be a formal agenda item next week for discussion.
• Concern was raised that if eligibility for boosters fol ows the original sequencing framework then
this wil reproduce inequities. Forecasting and model ing for doses (from Matt Jones) wil be
shared with CV TAG for discussion.
Dosing errors
Document 1
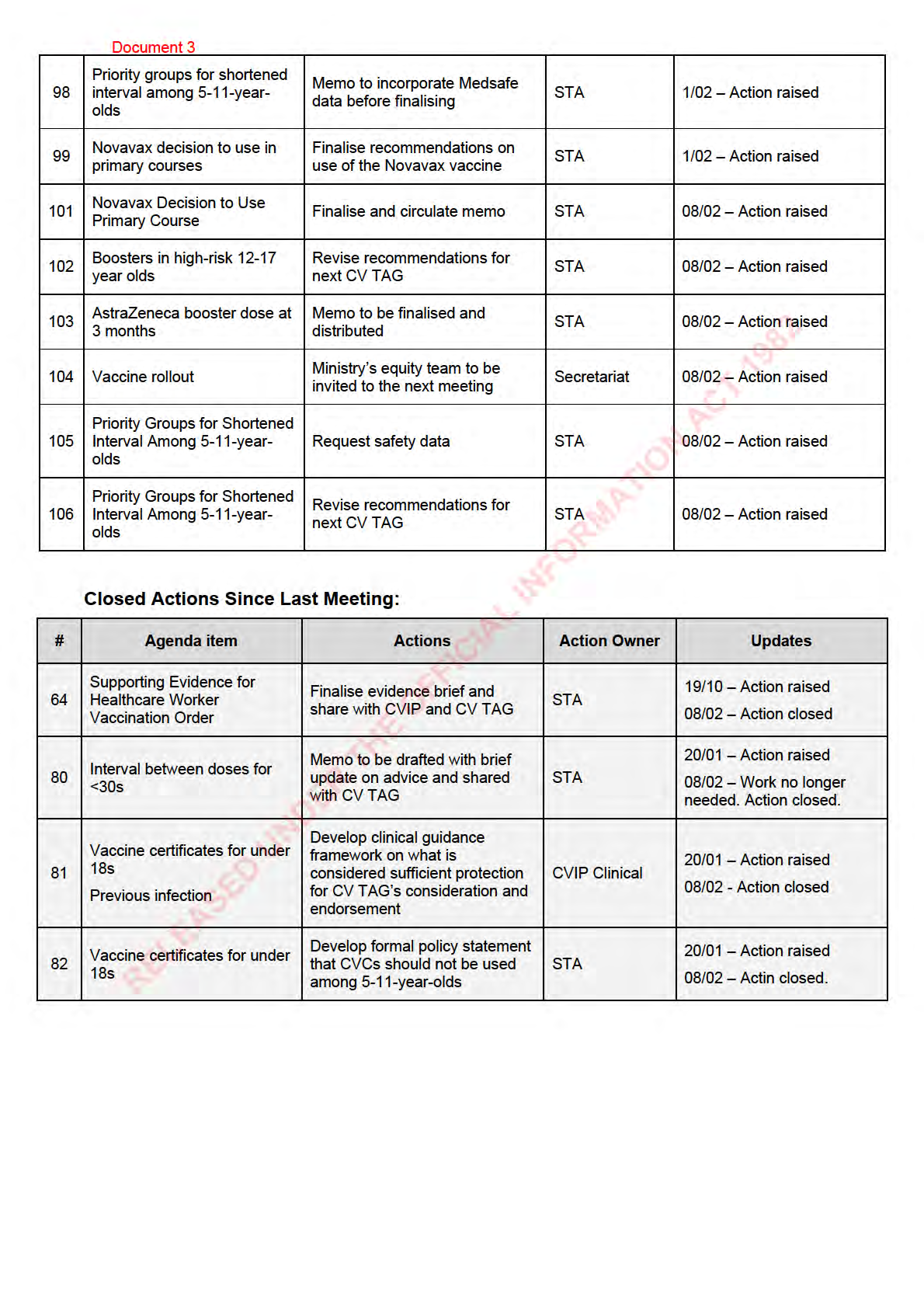
Supporting Evidence for
Finalise evidence brief and
64 Healthcare Worker
STA
19/10 – Action raised
share with CVIP and CV TAG
Vaccination Order
Memo to be drafted with brief
Interval between doses
80
update on advice and shared
STA
20/01 – Action raised
for <30s
with CV TAG
Develop clinical guidance
Vaccine certificates for
framework on what is
81 under 18s
considered sufficient protection
CVIP Clinical
20/01 – Action raised
Previous infection
for CV TAG’s consideration and
endorsement
Develop formal policy statement
Vaccine certificates for
82
that CVCs should not be used
STA
20/01 – Action raised
under 18s
among 5-11-year-olds
ACT 1982
Collate advice from peak bodies
84 Previous infection
on immune response and
STA
20/01 – Action raised
vaccine recommendations.
Protocol to be developed to
Alternative schedule:
ensure access to paediatric
CVIP Clinical with
85 Paediatric dose after adult doses of the vaccine are
20/01 – Action raised
support from STA
dose
available to those who may
INFORMATION
benefit from it.
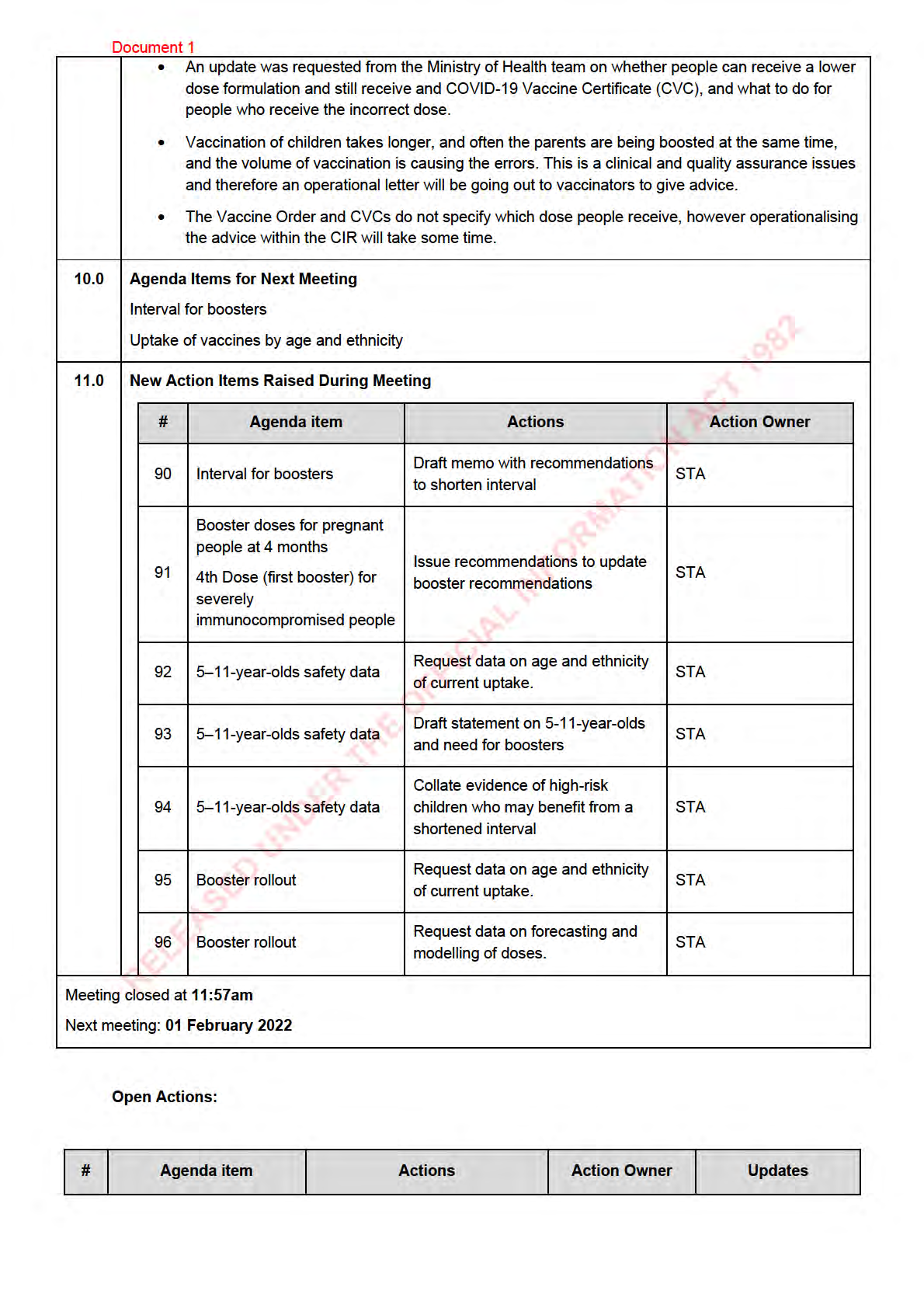
Send updated comment for
mRNA Injections and
87
statement to include comment
STA
20/01 – Action raised
Aspiration
on blood and myocarditis
Draft memo with
90 Interval for boosters
recommendations to shorten
STA
25/01 – Action raised
interval
Booster doses for
pregnant people at 4
months
Issue recommendations to
91 4th Dose (first booster) for update booster
STA
25/01 – Action raised
severely
recommendations
immunocompromised
people
RELEASED UNDER THE OFFICIAL
5–11-year-olds safety
Request data on age and
92
STA
25/01 – Action raised
data
ethnicity of current uptake.
5–11-year-olds safety
Draft statement on 5-11-year-
93
STA
25/01 – Action raised
data
olds and need for boosters
Collate evidence of high-risk
5–11-year-olds safety
94
children who may benefit from a STA
25/01 – Action raised
data
shortened interval

Document 2
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 01 February 2022
Time:
11:00am to 12:00pm
Location:
Teams: S9(2)(k)
Chair:
Ian Town
Danny de Lore, David Murdoch, Elizabeth Wilson, James Ussher, Nikki Turner,
Members:
Owen Sinclair, Peter McIntyre
ACT 1982
Andi Shirtcliffe, Daniel Bernal, Edwin Reynolds, Imogen Roth, Juliet Rumbal -
Ministry of Health Attendees:
Smith, Mariana Traslosheros Reyes, Niki Stefanogiannis, Pippa Scott, Matt
Jones, Liam McConnel , Amy Auld, Alison Cossar, Frances Graham
Guests:
John Tait, Anna Brooks
Apologies:
Helen Petousis-Harris, Ian Frazer, Nikki Moreland, Sean Hanna, Sue Crengle,
Tony Wal s, Brooke Hol ingshead Caroline McElnay, Fiona Cal aghan
INFORMATION
1.0
Welcome and Previous Minutes
Ian Town welcomed all Members and Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (25 January 2022) were accepted.
2.0
Vaccine Rollout
An update was provided on the vaccine rol out. Approximately 1.3 mil ion booster doses have been
administered. The paediatric vaccine rollout wil need to be accelerated in the light of Omicron.
3.0
Proposal to allow the lower dose (Paediatric) formulation in some people with ME
A brief overview was provided on the proposal. There is a significant number of people with ME in NZ,
many of whom have chosen not to vaccinate. International data shows that up to 20% have reported
severe adverse events, mostly severe relapse. The proposal outlined giving paediatric doses by
prescription to ME patients on the basis of Pfizer’s initial dose finding studies showing less reactogenicity
with a 10µg dose than a 30µg dose, and reasonable immu
RELEASED UNDER THE OFFICIAL nogenicity.
CV TAG discussed the proposal and there was general support. However, it was noted that there is no
guarantee that this wil meet eligibility criteria for a vaccine certificate under the current legislation and
legal review of the proposal would be beneficial.
A formal proposal and request for endorsement wil be sent by the applicant to the Chair for consideration.
4.0
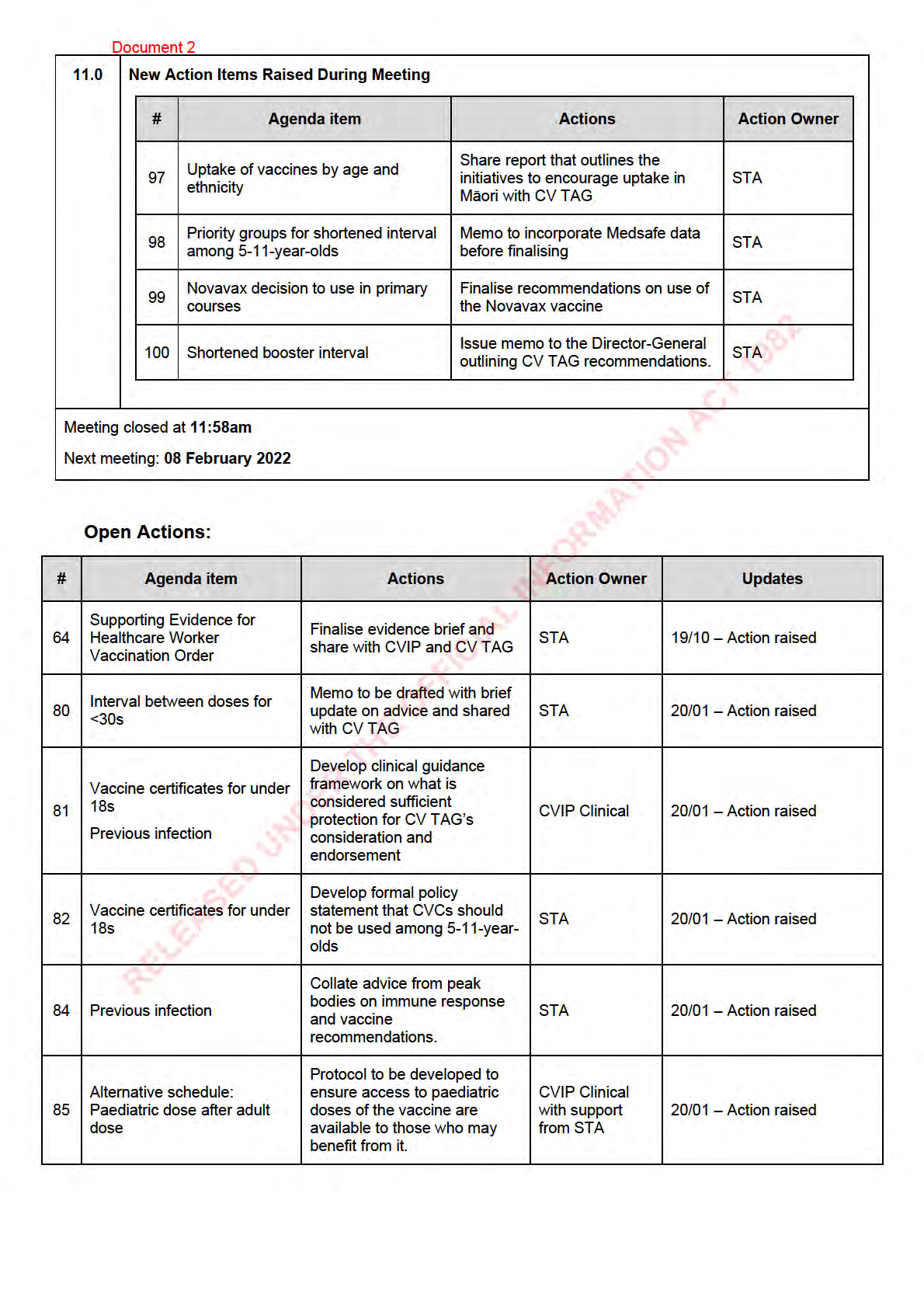
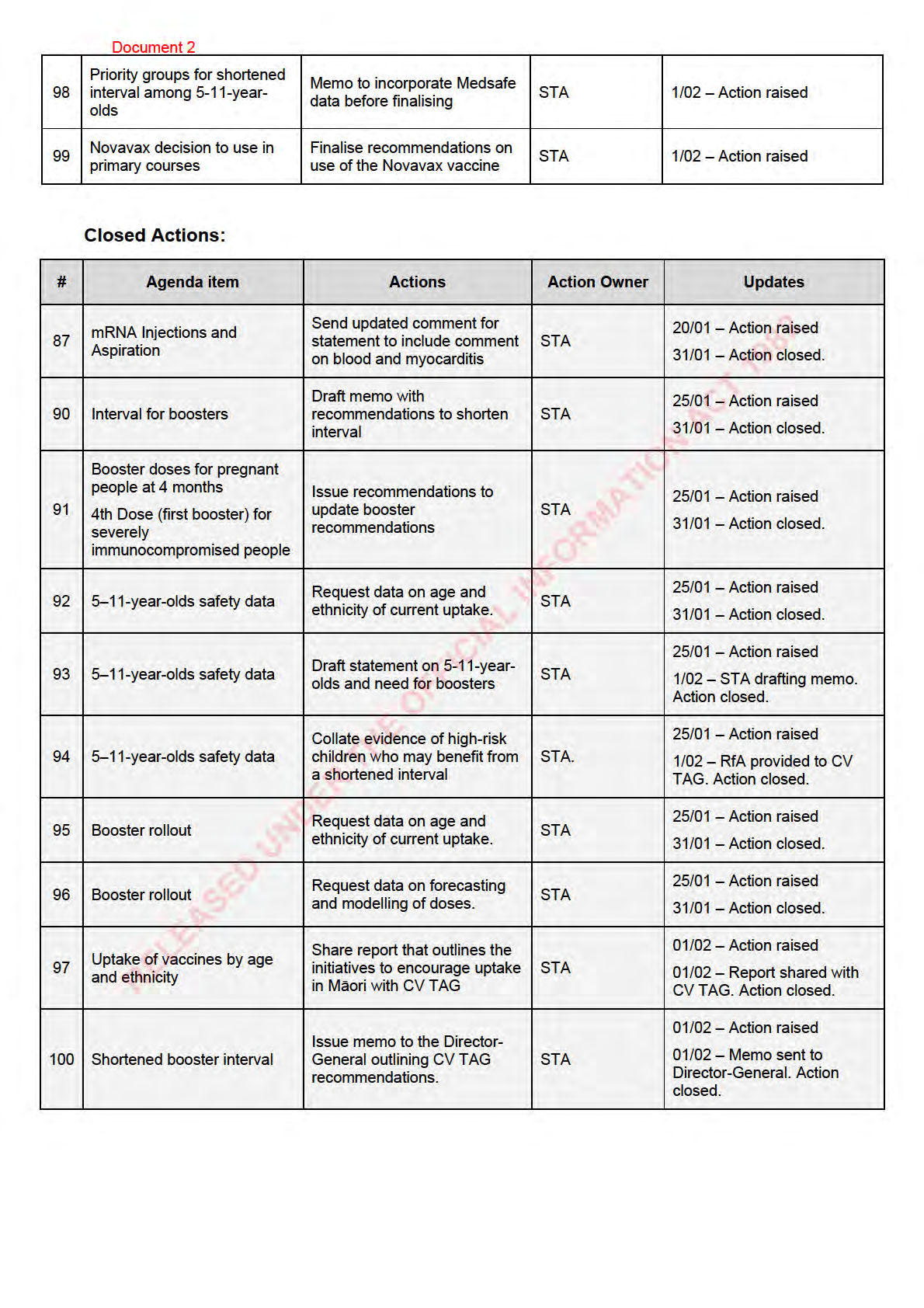
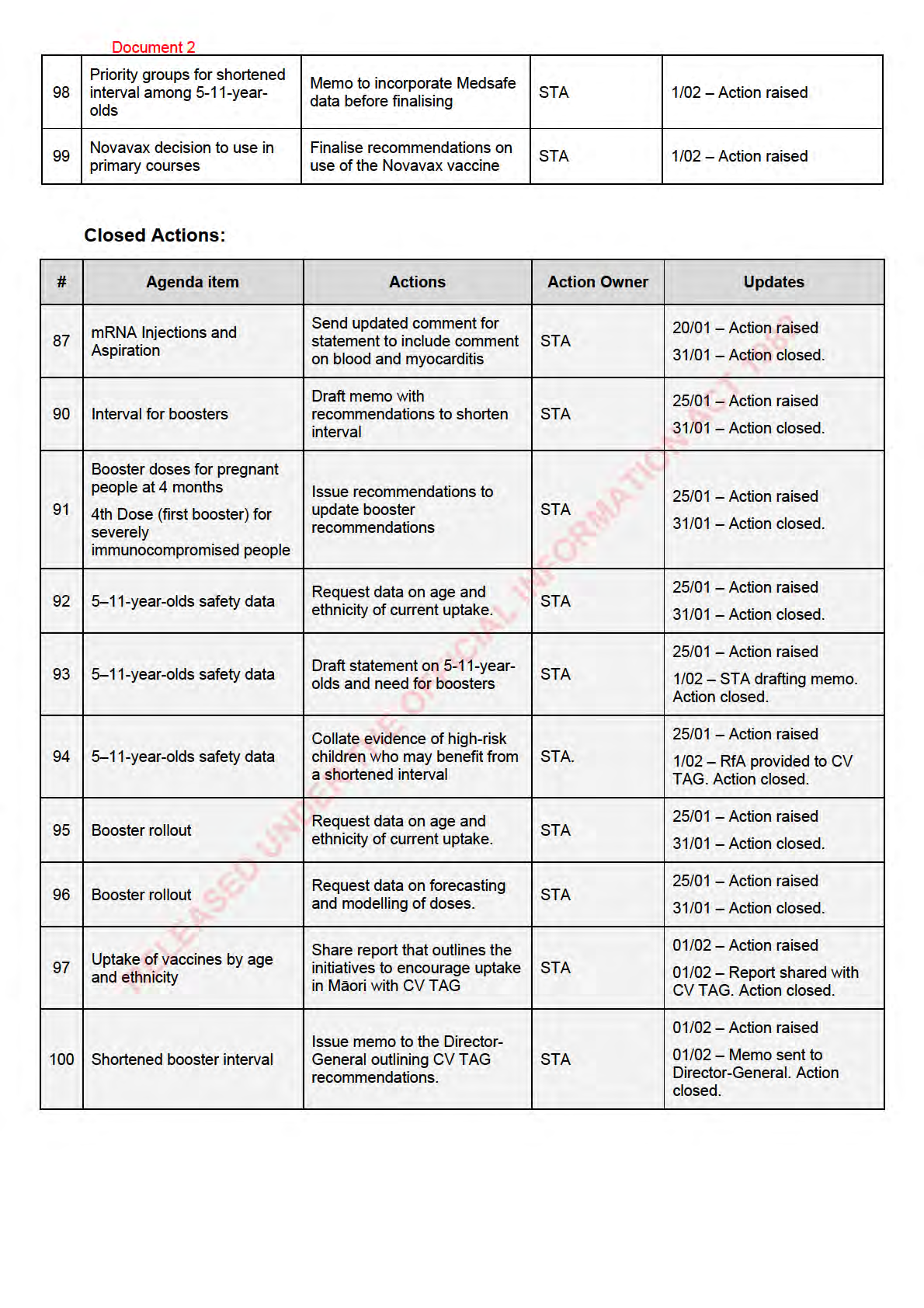
Uptake of vaccines by age and ethnicity
Document 2
The data on vaccine uptake by age and ethnicity was presented to CV TAG. It was noted that booking
numbers are continuing to rise for boosters.
CV TAG was encouraged by the booster uptake in Māori, however the uptake was lower in younger ages.
Concern was noted on the low booster uptake in elderly Pacific peoples and the low vaccine uptake in the
Pacific community in general.
CV TAG also expressed concern that first dose uptake in 5-11 year-olds is substantial y lower for Māori
compared to NZ European. There was discussion about school-based vaccination programmes being a
suitable option to increase access and uptake.
The low paediatric first dose uptake should be addressed with urgency, as wel as the lower uptake in
Pacific peoples.
A report that outlines the initiatives to encourage uptake in Māori wil be shared with CV TAG and the
Chair wil express the concerns noted during the discussion at the Steering Group.
5.0
Priority groups for shortened interval among 5-11-year-olds
The vaccination rollout in 5-11-year-olds was discussed and it was noted that no significant safety
concerns have been identified to date It was noted that in general, immunogenicity tends to be high
ACT 1982 er with
a longer interval and we want to provide children with the best chance for prolonged immunity.
CV TAG re-iterated their recommendation that the dose interval for 5–11-year-olds be 8 weeks to provide
long term protection. This topic wil be under ongoing review by CV TAG, and consideration wil be wil be
given as to whether there are any priority groups that should receive an earlier second dose.
A formal memo wil be issued to the Director-General following next week’s meeting.
6.0
Novavax decision to use in primary courses
INFORMATION
Novavax safety and efficacy data were reviewed, and it was noted that submission to Medsafe is only for
primary course vaccination, so there wil only be few people in New Zealand eligible for this.
A memo outlining CV TAG recommendations wil be drafted and discussed at the next meeting.
7.0
Shortened booster interval
The recommendations for a shortened booster interval were discussed, including who should be
prioritised. It was noted that the Ministry wil work with providers to make sure priority populations in their
areas are targeted appropriately.
CV TAG recommend that the booster interval be shortened to 3 months (including for
immunocompromised and pregnant people), with priority groups as fol ows: Māori and Pacific people aged
18 years and over those aged 65 years or over; residents of aged care and disability facilities; frontline
healthcare workers, border workers, or essential workers whose ability to work is critical for infrastructure
and supply chains; anyone aged 18 years and over with comorbidities.
A memo wil be sent to the Director-General outlining these recommendations.
8.0
Next Steps/Decisions Pending
RELEASED UNDER THE OFFICIAL
None
9.0
Any Other Business
None
10.0 Agenda Items for Next Meeting

Document 3
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 08 February 2022
Time:
11:00am to 12:00pm
Location:
Teams: S9(2)(k)
Chair:
Ian Town
Danny de Lore, David Murdoch, Elizabeth Wilson, Helen Petousis-Harris, James
Members:
Ussher, Nikki Moreland, Owen Sinclair, Peter McIntyre, Sean Hanna, Sue
Crengle, Tony Walls
ACT 1982
Ministry of Health Attendees:
Brooke Hollingshead, Daniel Bernal, Edwin Reynolds, Frances Graham, Juliet
Rumball-Smith, Mariana Traslosheros Reyes, Pippa Scott, Sean Driver
Guests:
Hil ary Longhurst, Ali Mirjalili, Tom Hil s
Apologies:
Ian Frazer, Nikki Turner, Andi Shirtc iffe, Caroline McElnay, Chriselle Braganza
Fiona Cal aghan, Imogen Roth, Niki Stefanogiannis
INFORMATION
Welcome and Previous Minutes
1.0
Ian Town welcomed all Members and Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (01 February 2022) were accepted.
Vaccine Rollout
2.0
An update was provided on the vaccine rol out.
• Approximately 1.6 mil ion booster doses have been administered.
• Equity concerns in the paediatric rollout were highlighted. A conversation wil be organised
between CV TAG and the CVIP equity team/ Māori health providers.
BMI Needle Length Study
3.0
Initial results of the study were reported:
• Based on an ethnically diverse sample who were predominantly young and male with few
comorbidities, the standard 25mm needle was ass
RELEASED UNDER THE OFFICIAL essed as insufficient length for intramuscular
vaccine deposition in around 15% of participants. Only a smal percentage of these were
vaccinated with the longer needle.
• Measuring arm circumference or noting BMI helped to identify who may need a longer needle.
However, antibody levels were comparable in this study (general y young and healthy people)
between those who likely received intramuscular administration and those who likely received
subcutaneous administration.
• The researchers wil fol ow up with IMAC in respect of any operational changes.
Document 3
Novavax Decision to Use Primary Course
4.0
Draft recommendations for the decision to use the Novavax vaccine as a primary course were discussed:
• It was noted that only a small group remain in New Zealand who have not had a primary course,
and there are also limited data on the use of the Novavax vaccine in heterologous schedules.
• There may be some benefit to people covered under Vaccine Orders, or people who have had an
adverse reaction to Pfizer as a first dose.
• Use as a booster dose was not discussed as Medsafe are yet to consider the Novavax vaccine for
use as a booster.
• Recommendation for use as a primary vaccine course was agreed by CV TAG.
Booster Doses in 12-17 year-olds
5.0
Draft recommendations on whether 12-17-year-olds should receive booster doses were discussed.
• The available (limited) data, and recommendations from other jurisdictions were discussed. It was
noted that peak bodies international y have varied recommendations, which sometimes differ for
ACT 1982
younger and older ages within this age-group.
• There was agreement that comorbidities and epidemiology of COVID-19 should be used to guide
recommendations in this age group.
• It was agreed that 12-17-year-olds with medical comorbidi ies should be offered booster
vaccination. Other risk factors such as ethnicity and social determinants were also advocated for,
with Māori and Pacific peoples being disproportionately impacted by COVID-19 and severe
disease thus far in the pandemic.
INFORMATION
• Issues surrounding mandates for this age-g oup were also re-iterated.
• A discussion is required with Medsafe on use of boosters in this age group, as boosters are
currently only approved for those 18 years of age and older.
• These recommendations wil be finalised within the next week.
AstraZeneca Booster Dose at 3 Months
6.0
It was agreed that the interval between primary vaccination and boosters could also be brought forward to
3 months for the AstraZeneca vaccine.
Priority Groups for Shortened Interval Among 5-11 year-olds
7.0
A discussion of the safety of second doses and any need for a shortened interval occurred:
• Data available for this age group are limited. But general safety signals have been reassuring to
dat.
• Medsafe/ CARM/ ISMB processes and data wil be summarised for the next memo draft.
• Consideration was given to shortening the interval
RELEASED UNDER THE OFFICIAL in this age group, and whether it would help to
address the current Omicron outbreak. However it was considered there is a strong rationale to
continue recommending the 8 week interval between doses for this group, based on the generally
lower severity of disease in this age group, the protection provided by the first dose, and
potentially better protection and reduced side effects with a longer interval.
• It was noted that, because Medsafe approval is for a 3-week interval in this age group, there is no
basis to refuse a shorter interval if individual parents were to insist.