Document one
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 13 April 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
David Murdoch, Edwin Reynolds, Elizabeth Wilson, Helen Petousis-Harris, Ian
Members:
Frazer, James Ussher, Nikki Moreland, Nikki Turner, Peter McIntyre, Pippa
Scott, Sean Hanna
Ministry of Health Attendees:
Caroline McElnay, Daniel Bernal, Juliet Rumbal -Smith, Fiona Cal aghan,
Chriselle Braganza
Guests:
Janelle Duncan, Sarah Emerson
Apologies:
Andi Shirtcliffe, John Taylor, Matire Harwood, Shayma Faircloth, Sue Crengle,
Tony Walls, Kath Blair, Al ison Bennett, Kris Golding
1.0
Welcome and previous minutes
Ian Town welcomed all Members, Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (23 March 2021) were accepted.
The Chair noted that the CV TAG membership and minutes wil be released as part of an OIA
request.
2.0
Science Updates
CV TAG members were asked to note any errors or concerns about these documents to the
Secretariat. An amendment to the wording in section 3.9 of the Pfizer Science Overview document
was proposed: change “blood clotting issue” to “thrombocytopenia” to avoid any confusion.
under the Official Information Act 1982
The Ministry is maintaining a line of sight on any unusual events with respect to the Pfizer vaccine.
The DG has asked for daily updates about Pfizer, including any concerning matters in the adverse
events reported following vaccination and in the literature.
3.0
Research in Children
The document wil continue to be updated regularly. It wil be relevant for briefing Minsters on the
likely time that children aged 12-15 years can be considered for vaccination. Medsafe has contacted
Pfizer for data submissions on this topic.
Released
4.0
Vaccine Rollout
There has been a cal for public reporting about the vaccine rollout and the Ministry has developed a
one-page summary on the current progress. The document focusses on the rol out thus far, but a
forward-looking plan wil be available shortly, once DHBs have lodged their rol out plans. The scaling
Document one
of smal to large confidence-building events is imminent and the national public relations campaign
wil start on Monday 19 April.
A summary of the rol out was provided to CV TAG members. The Ministry is working with DHBs to
address gaps in the private sector, for example, those who would not normal y expect be covered
through a DHB arrangement but need to be vaccinated at the same time as others.
Some issues were raised during this discussion:
•
There was a concern that adverse event reporting was disconnected especially between the
CIR and the CARM processes.
•
There have been previous discussions around active approaches to monitoring, such as
sending out an SMS text to people after they have received the vaccine to gain feedback on
any issues. To date this technology has not been implemented in NZ. Australia has offered
to share their cloud-based technology with NZ, and it would be good to implement this
system before scaling up our rollout. This would al ow for more trust in the reporting system
instead of relying on the passive system that is currently in place.
The Chair suggested that these issues be escalated directly with the Director of the COVID-19
Immunisation Programme.
5.0
Overlap Influenza Campaign
The Minister has made a clear decision against pausing the influenza programme, but this comes
down to the sequencing and timing, which wil vary across the country. For example, the COVID-19
vaccine is being rol ed out in Counties Manukau and thus wil be administered first, followed by
influenza. However, in other parts of the country, people would have time to receive the influenza
vaccine first, followed by the COVID-19 vaccine.
Discussion included:
•
Work is being undertaken around establishing clear communication with primary care
colleagues and a flexib e framework is being developed to aid with decision making.
•
The priority is to administer the COVID-19 vaccine without delay, which means that the
influenza vaccine programme may need to be delayed
•
The Ministry has provided sequencing advice to primary care. Feedback from Counties
Manukau DHB identified the need for more flexibility. The messaging has been softened to
reflect that the COVID-19 vaccine appointment is a priority, however, if the person does not
have an appointment for the COVID-19 vaccine, they can get a flu vaccine. The influenza
programme is also developing a tool for flu vaccine providers that contains a poster with a
flowchart providing clear instructions on which vaccine should be administered in which
under the Official Information Act 1982
order.
6.0
CV ISMB Memo Update
The post-event pil ar team provided an update on the COVID-19 Vaccine Independent Safety
Monitoring Board (CV ISMB) meetings. During the last ISMB meeting on 31 March, Medsafe
provided detailed safety information on the vaccine rol out. This included an overview of the serious
and non-serious events. The Board has reviewed diagnostic criteria for anaphylaxis events. The
ISMB also noted concern around how the second dose wil be administered for people who
Released
experienced serious side effects after the first dose, and how this information wil be communicated.
The ISMB meeting also raised the fol owing questions:
•
Consideration of vaccinating high-risk children: The Chair noted that the CV TAG have
provided advice against vaccinating children as there is not enough data currently available
to support use in children.
Document one
•
Model ing studies on whether there is a need for a booster dose: The Chair noted that this
item wil be added as an item for further work.
Discussion included:
•
The monitoring through CARM and Medsafe is different from needing clinical feedback when
an issue occurs. A clinical framework is required and wil be developed by the Ministry.
•
The adverse events post event are dealt with in primary care. There is a need for a
conversation between IMAC, the Ministry, and Healthline to support the escalation of
unusual events to clinical advisors and a potential need for setting up a virtual clinic for
those that need fol ow up.
•
If someone experiences a severe reaction that requires closer observation, when receiving
their second dose, they should be referred to the larger, well-established DHBs that have
the required clinical oversight.
•
The requirements for additional care haven’t been articulated for people who experience
serious events or have other complications. It has been suggested that operational clinical
leads around the country nominate a clinical lead to participate in a working group. It would
be good to have support from the sector to lead discussions on where patients go, what
equipment workforce is required for good care, and what this would look like for al proposed
models. This discussion wil start on Thursday 15 April and it is anticipated that this will be
sector lead and Ministry facilitated.
•
Every DHB has a responsibility to ensure that the programme is safely delivered, including
seeking senior health professionals’ advice on who should get vaccinated.
7.0
48h Testing Advice
CV TAG recommendations have been implemented into the testing advice, which wil go out in the
next 24 hours.
8.0
Interchangeability of COVID-19 Vaccines
Key points of discussion:
•
Given that ATAGI has ecommended the COVID-19 Pfizer vaccine is preferred over the
AstraZeneca vaccine for adults aged under 50 years, it is unclear what should be done with
people who have had one dose of the AstraZeneca vaccine and are now not eligible for it.
People in Australia might refuse to take the second AstraZeneca dose but some of these are
frontline workers, so a ruling is required.
•
The status of vaccination wil need to be recorded appropriately on the CIR to avoid people
being recal ed for an additional dose of Pfizer. This wil be noted on the memo going out to
under the Official Information Act 1982
the CVIP.
CV TAG members recommended that where a single dose of another two-dose regimen vaccine is
documented, a single dose of the Pfizer vaccine should be given at least 4 weeks after the first
vaccine dose.
Post-meeting note: ATAGI has recommended people who have had the first dose of the
AstraZeneca vaccine without any serious adverse effects can be given the second dose, including
adults under 50 years.
Released
9.0
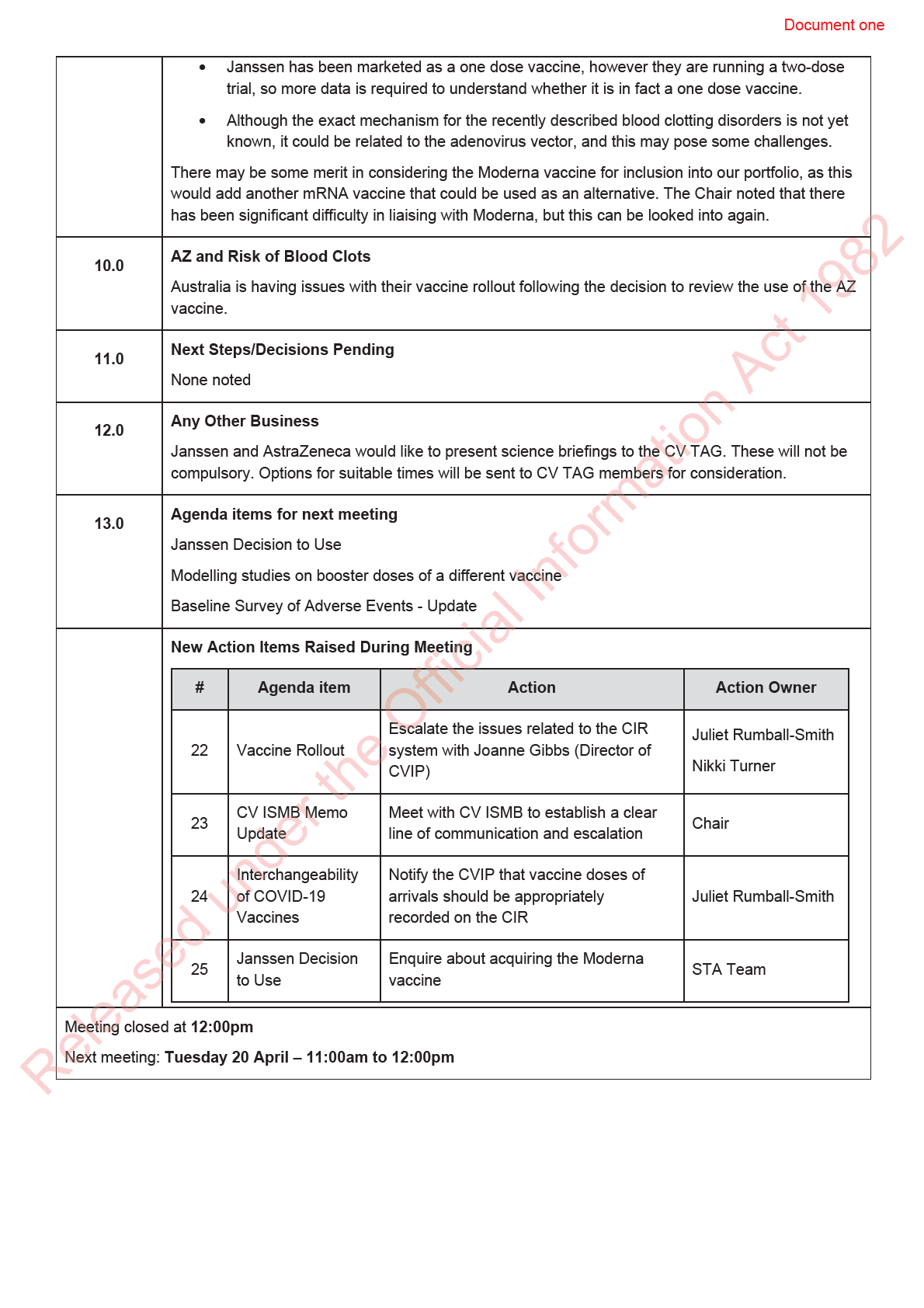
Janssen Decision to Use
The Chair noted that the Decision to Use for Janssen wil fol ow a careful approach to allow for policy
and science advice to consider which populations may be more suited to receive this vaccine
CV TAG noted that:

Document two
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 27 April 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
Members:
David Murdoch, Edwin Reynolds, Elizabeth Wilson, Helen Petousis-Harris, Ian
Frazer, Nikki Moreland, Nikki Turner, Peter McIntyre, Pippa Scott, Sue Crengle
Ministry of Health Attendees:
Andi Shirtcliffe, Daniel Bernal, Juliet Rumball-Smith, Fiona Callaghan, Chriselle
Braganza, Shayma Faircloth
Guests:
Apologies:
Caroline McElnay, James Ussher, John Taylor, Matire Harwood, Sean Hanna,
Tony Walls
1.0
Welcome and previous minutes
Ian Town welcomed all Members, Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (13 April 2021) were accepted.
2.0
Science Updates
CV TAG was requested to send any updated information for inclusion into the documents.
It was noted that data on vaccination of immunocompromised individuals is beginning to emerge.
The updated Cancer Control Agency guidance includes material on the vaccination of
immunocompromised individuals taking in to account the timing of vaccination with respect to
treatment, the COVID-19 risk, and the ability of immunocompromised individuals to produce an
immune response. This updated guidance wil be shared with CV TAG.
under the Official Information Act 1982
3.0
Research in Children
Pfizer has been invited to submit data on children to Medsafe to inform a decision by the Medicines
Assessment Advisory Committee.
4.0
Vaccine Rollout
The daily vaccine report was presented to CV TAG. There are approximately 400,000 doses in
storage, but these wil be utilised quickly once the rollout is ramped up in June/July. A supply of
Released
stored doses is required so that the vaccine can be deployed rapidly in the event of an outbreak.
Key points:
•
Al DHBs have been asked for their individual rol out plans as different approaches are being
taken according to locations and their population.
Document two
•
The rollout is somewhat short of meeting the daily medium-term target of 5,000 doses per
day but there has been good progress towards people receiving their second dose.
•
A request was received for administrative and IT purposes to define a maximum allowable
time interval between doses. The suggestion based on current evidence and
recommendations from ATAGI and the US CDC is for six weeks. It is recommended that the
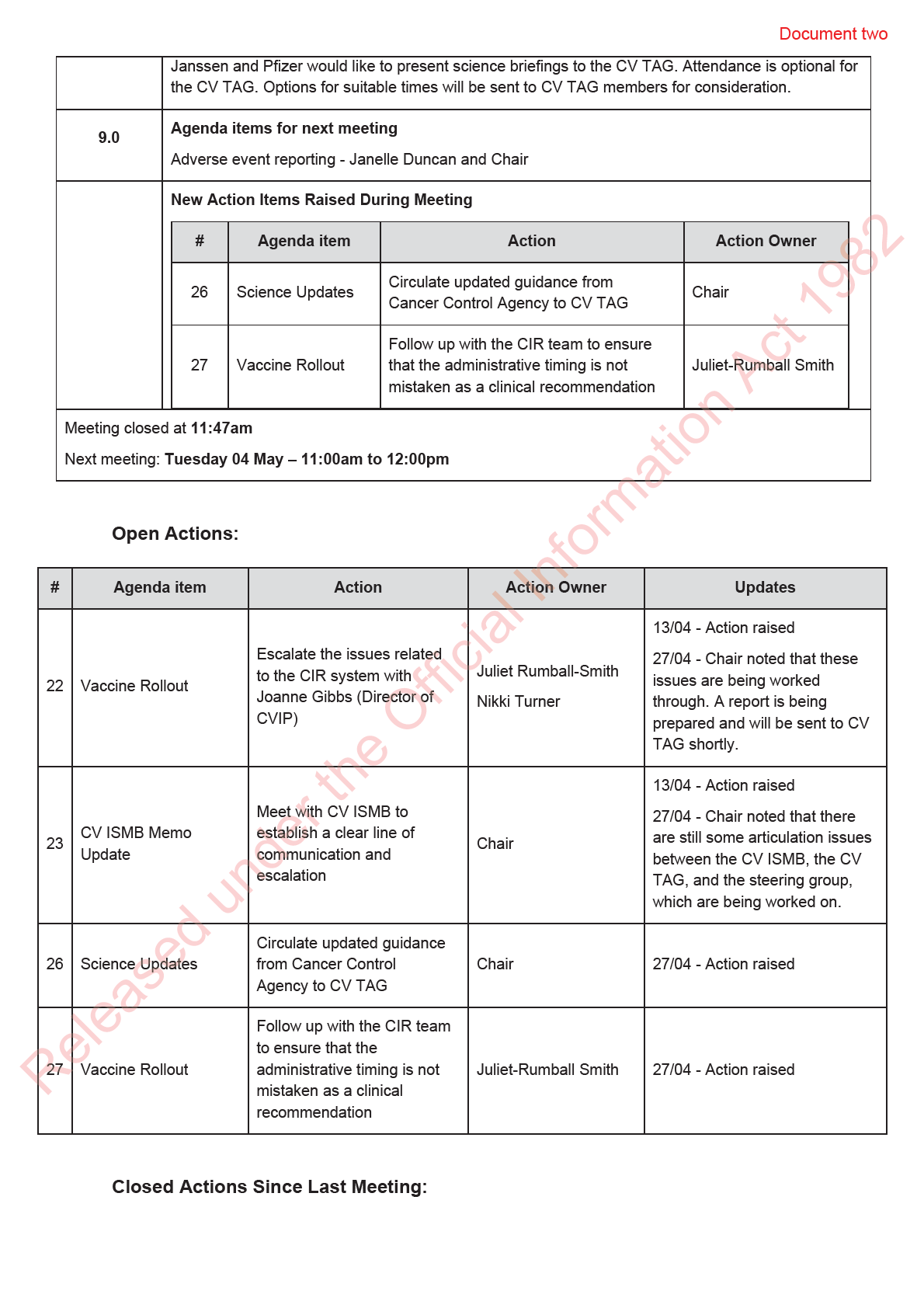
second dose be given as close to the three-week time as possible. The Ministry will work
with the CIR team to ensure that this administrative upper limit on the interval between
doses isn’t interpreted as a clinical recommendation.
5.0
Baseline Survey of Adverse Events
The study wil pause their work on anaphylaxis and focus on some of the original priorities, including
thrombotic issues. Chart reviews wil be conducted to evaluate the accuracy of the data with respect
to capturing adverse events. The protocols of the study wil be published after the advisory group
have provided feedback.
Key points:
•
Data for thrombotic events was collected for Medsafe, however this was not broken down by
sub-population. Work is ongoing regarding case definition. This work is being undertaken in
collaboration with a haematologist.
•
Funding from the Global Vaccine Data Network (GVDN) wil al ow for col aboration and
evaluation of baseline rates. At this stage, it is not known whether the methodology for
estimating the rates are harmonised across studies.
•
CV TAG noted that in most countries the benefits of vaccination far outweigh the risk of rare
side effects.
6.0
Serological Survey Protocol
A brief overview was provided on the seroprevalence study by the University of Auckland. The study
evaluated blood samples collected by the NZ blood service between December 2020 and January
2021. As the study was based on a convenience sample, there are issues of bias, however, there
was good geographical spread and a broad age range (16-88 years). Immunoassays were carried
out to evaluate the level of COVID 19 antibodies. 18 positive samples were detected, of which six
were matched to previously confirmed cases. The studies were carried out blinded and showed that
the serological testing algorithms worked well. The study found eight previously undiagnosed cases
and a low seroprevalence of ~ 0.1%, suggesting a very low amount of undetected community
transmission.
Key points:
•
It was highlighted that the more vulnerable Māori and Pacific populations were
underrepresented in this study. This was recognised as a limitation of the study.
under the Official Information Act 1982
•
It has been shown that anti-spike IgG antibodies last for several months after infection.
•
The upcoming VAANZ study that has previously been discussed with the CV TAG wil be
specifical y recruiting Māori and Pacific populations to address the gap in immunogenicity
data for these populations.
•
CV TAG noted that at this stage there is no need for further seroprevalence studies in NZ,
given the low rate of infection and that it is highly unlikely that a large number of infections
were undetected.
Released
7.0
Next Steps/Decisions Pending
None noted
8.0
Any Other Business

Document three
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 11 May 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
David Murdoch, Edwin Reynolds, Elizabeth Wilson, Helen Petousis-Harris, Ian
Members:
Frazer, James Ussher, Nikki Moreland, Nikki Turner, Peter McIntyre, Pippa
Scott, Sean Hanna, Tony Walls
Ministry of Health Attendees:
Caroline McElnay, Daniel Bernal, Juliet Rumbal -Smith, Chriselle Braganza,
Shayma Faircloth; Christian Marchel o
Guests:
Janelle Duncan; Niki Stefanogiannis
Apologies:
Andi Shirtcliffe, Fiona Cal aghan, John Taylor, Matire Harwood, Tim Hanlon, Sue
Crengle
1.0
Welcome and previous minutes
Ian Town welcomed all Members, Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (27 April 2021) were accepted subject to the fol owing correction being
made to Item 6.0 Serological Survey Protocol (added text in red):
18 positive samples were detected, of which six were matched to previously confirmed cases. The
studies were carried out blinded and showed that the serological testing algorithms worked well.
There were 4 seropositive samples with notable 2020 travel to high-risk areas suggesting infection
outside NZ. The study found an additional eight previously undiagnosed cases and a low
seroprevalence of ~ 0.1%, suggesting a very low amount of undetected community transmission.
under the Official Information Act 1982
2.0
Science Updates
The Chair summarised key points from the briefing that was held with Janssen the previous evening.
Janssen provided an overview of the Phase 1, 2, and 3 studies, fol owed by a detailed breakdown of
adverse events, including thrombotic thrombocytopenic disorders. Janssen noted that their decision
to market the vaccine as a single dose was deliberate and strategic given the positive Phase 1
results but studies using a second dose are underway. The vaccine also shows promising results
against variants of concern. Future studies in adolescents, children, and pregnant persons were also
outlined.
Released
The Ministry’s policy team wil be looking at potential use of the Janssen vaccine in NZ in the
following weeks, as the vaccine is under consideration by Medsafe. If approval is granted, a
discussion wil be held with CV TAG around the use of the Janssen vaccine, similar to the process
following approval of the Pfizer vaccine.
Updates on the Pfizer vaccine were highlighted:
Document three
•
The emergency use authorisation has been extended by the FDA to include use in ages 12-
15 years.
•
Phase 1 studies on a prototype vaccine targeting variants of concern wil be commencing
soon.
•
More data is emerging around the effectiveness of a single dose and general y suggest that
two doses are more effective than one.
•
Data is emerging around the vaccine’s effect on transmission, with studies in household
settings showing that the vaccine reduced onwards transmission.
•
Revised manufacturing target to 3 bil ion doses produced by end of 2021.
•
Data is emerging for pregnant persons, with no safety signals detected in this population yet
but only a smal number have been vaccinated.
AstraZeneca has begun preclinical studies for a prototype vaccine targeting variants. Due to the
blood clotting issues, trials in children have been suspended temporarily until this can be
investigated further.
Novavax has released results showing that the vaccine has around 50% efficacy against the B.1.351
(South African) variant. They are currently developing a prototype vaccine targeting this variant.
Novavax have also extended their Phase 3 trial to include children aged 12-17 years.
3.0
Research in Children
Canada and US have extended Pfizer’s emergency use approval to include ages 12-15. Pfizer are
also seeking extension of the EMA approval.
Pfizer wil be submitting data to Medsafe shortly for extension of the approval to 12-15 years. The
Medicines Assessment Advisory Committee (MAAC) meeting in June wil consider this information
and the CVIP are looking at timing of administration via high school events, which may land in Q3
and Q4. This wil have to be managed carefully as the timing may coincide with other events such as
the examination period.
4.0
Vaccine Rollout
The daily vaccine report was presented to CV TAG. Approximately 373,000 doses have been
administered, of which 114,000 were second doses. The first mass vaccination event is being
planned for deployment in late June, with an event company hired to organise this event. The
Ministry has been working with primary care colleagues and has recommended that a site must be
able to administer around 30 doses per day to be established as a primary care vaccination centre.
This wil allow approximately 30% of primary care teams to begin vaccinating when supply is
available for the wider rollout. Other col eagues wil be encouraged to refer their patients to the
under the Official Information Act 1982
nearest site.
5.0
Update on Adverse Event Reporting (CIR system)
Post-event workstream provided an overview of the work that is being undertaken as part of the
adverse events reporting process. An updated paper was provided to CV TAG that covered the
reporting of adverse events following immunisation (AEFI), an uplift to the Centre for Adverse
Reactions Monitoring (CARM) system, and the development of a clinical protocol for the
management of consumers who experience an adverse event fol owing the first dose.
Released
Key points:
•
The level of work is unprecedented; usual y CARM receives about 5,000 reports a year but
have already received around 2,600 reports since the beginning of the COVID-19 vaccine
rollout.
Document three
•
Reports submitted to CARM are triaged according to seriousness and are escalated for
medical assessment. This includes serious adverse events, adverse events of special
interest (AESI), and those that may be part of a suspected signal.
•
The post-event workstream prepares a daily report on reported adverse events and a
weekly update with any signals that are being investigated.
•
Four signals are currently being investigated: thrombosis with thrombocytopenia syndrome
(TTS), appendicitis, herpes zoster, and myocarditis.
•
Medsafe reports on adverse events weekly but there is currently a lag time of a month to
allow for identification of any causality. The reports are published every Wednesday on the
Medsafe website to align with other communications.
•
The COVID-CARM application was released on 30th March, which took CARM from being
paper-based to digitised. While this hasn’t changed from a consumer’s perspective,
background processes have changed significantly and allow the whole process to be digital.
It was highlighted that this application was implemented as an interim solution while a new
and more suitable database is being explored.
•
A clinical protocol in being developed for administering the second dose to people who
experienced an adverse event following the first dose. An initial meeting was held with
DHBs, Immunisation Advisory Centre (IMAC), and HealthPathways to discuss this. A follow
up meeting is occurring tomorrow to progress the draft protocol further.
•
It was noted that the implementation of an active monitoring has been approved in principle
by the steering group, with further work on the proposal underway.
CV TAG noted that the need for an active SMS based monitoring system has been highlighted as an
important aspect of the New Zealand surveil ance system in previous meetings (formerly the COVID-
19 Vaccine Strategy Science and Technical Advisory group to MBIE) and that this system should
have been implemented months ago. The active monitoring system is key to building community
confidence in the vaccine, to increase uptake, and to undertake risk assessments. There was strong
support from the CV TAG for the active SMS based reporting system to be implemented
immediately.
6.0
Ring Vaccination
An overview was provided on the paper that was prepared by policy and public health teams within
the Ministry. The paper outlines previous discussions with CV TAG, which concluded that the
COVID-19 vacc ne should not be used for post-exposure prophylaxis but can be used for ring
vaccination. For implementation purposes, further advice and clarification is required around the
definition and purpose of ring vaccination during a COVID-19 outbreak.
Key points of discussion:
under the Official Information Act 1982
1. CV TAG accepted the definition of ring vaccination as described in the paper. However, the
preference is to move away from using the term ‘ring vaccination’ and instead use ‘targeted
vaccination’. It was noted there are ‘details within the details’ that are more difficult to define,
i.e., defining the ‘rings’ or persons to be targeted.
2. Targeted vaccination should be implemented alongside other public health measures and
not as a standalone measure. A protocol should be developed and ready for implementation
if we have an outbreak. The use of targeted vaccination can reduce harm and increase
Released community confidence and vaccine uptake.
3. A question was raised as to what the trigger point would be for deploying targeted
vaccination. There is no international data on using the COVID-19 vaccine for targeted
vaccination to inform this decision. The situation in New Zealand means that there may be
an opportunity to get some data. It is difficult to differentiate between post-exposure
Document three
prophylaxis and targeted vaccination because some close contacts wil likely end up being
included in the target group.
4. It was noted that NZ is already taking a targeted approach by starting vaccinations with
border workers in the sequencing framework. It has been communicated with DHBs that
targeted vaccination is in our 'toolbox’, but the Ministry has not been able to provide
specifics on how this would be implemented.
5. There wil be communities with low vaccine coverage, and we wil need a protocol to ensure
increased coverage while maintaining equity in an outbreak setting. The wider border
opening may lead to potential outbreaks in some communities.
6. Targeted vaccination has a place as part of our suite of public health interventions d ring an
outbreak where there wil be an increased demand for vaccination. The Ministry wil work on
general supply chains, staffing, and logistics. A judgement call will have to be made by
senior officials within the Ministry as to when targeted vaccination is required. This work will
be led by the public health team.
CV TAG endorsed the approach of targeted vaccination and the development of a protocol as part of
the contingency plan.
7.0
Next Steps/Decisions Pending
None
8.0
Any Other Business
•
Vaccine rol out in Australia: The vaccine programme is progressing smoothly, with
approximately 10% of the population vaccinated with at least one dose. The vaccine is being
rolled out at immunisation centres, as well as general practices, and there are no vaccine
shortages.
•
Timing of flu vaccine: A discussion was had about whether the Ministry can endorse that it is
acceptable to have a four week gap between the two doses of the Pfizer vaccine, following
questions received via the IMAC 0800 line on timing of the flu vaccine. It was noted that
changing the Ministry’s view on the interval between doses would have significant implications
for the booking system, the CIR, and distribution and volume planning. The current public
messaging is that doses should be spaced at least 21 days apart. Any further endorsement or
permissive statements may lead to confusion, especially since the advice has been to prioritise
the COVID-19 vaccine.
9.0
Agenda items for next meeting
None noted
under the Official Information Act 1982
New Action Items Raised During Meeting
None
Meeting closed at
12:01pm Next meeting:
Tuesday 18 May – 11:00am to 12:00pm
Released

Document four
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 25 May 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
David Murdoch, Elizabeth Wilson, Helen Petousis-Harris, James Ussher, John
Members:
Taylor, Nikki Moreland, Nikki Turner, Peter McIntyre, Pippa Scott, Sue Crengle,
Tony Walls
Ministry of Health Attendees:
Caroline McElnay, Daniel Bernal, Edwin Reynolds, Fiona Cal aghan, Juliet
Rumball-Smith, Chriselle Braganza, Shayma Faircloth
Guests:
Ali Mirjalili, Tom Hil s, Kris Golding, Al ison Bennett, Tim Hanlon
Apologies:
Andi Shirtcliffe, Ian Frazer, Matire Harwood, Sean Hanna
1.0
Welcome and previous minutes
Ian Town welcomed all Members, Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (11 May 2021) were accepted.
The Chair noted that key messages from CV TAG meetings are provided as a verbal update to the
Vaccine Steering Group and are also reported to Ministers.
2.0
Science Updates
Updates on the Pfizer vaccine were highlighted:
•
The US FDA has authorised storage of the undiluted vaccine at fridge temperatures for up to
a month.
under the Official Information Act 1982
•
The vaccine received ful regulatory approval in Switzerland, Japan, and Brazil.
•
The vaccine has been approved for use in ages 12-15 in the US, Singapore, and the UAE.
•
Preliminary data on extended dose intervals showed that a 12-week interval was associated
with increased antibody titres but decreased T cell responses, compared to a 3-week
interval. However, it is not clear what role each of these responses play in long term
protection.
•
Preliminary evidence on mixed vaccine schedules with Pfizer and AstraZeneca showed that
Released heterologous vaccine schedules were more reactogenic than homologous schedules.
•
Data from Public Health England indicated that the Pfizer and AstraZeneca vaccines were
effective against the B.1.1.7 (UK) and B.1.617.2 (Indian) variants.
Document four
•
The CEO of Pfizer has stated that there may be a need for booster doses, however, no data
have been released on antibody waning. It is also not clear whether “booster” refers to a
third shot of the original vaccine or a second-generation vaccine targeting variants of
concern.
•
Events of myocarditis post-vaccination are being evaluated by regulators, including the EMA
and FDA. Preliminary evidence suggests that rates are low in the US, UK and the EU (~1
per million) and Israel (~6 per mil ion).
Key points of discussion:
•
CV TAG noted that the Pfizer storage temperature is an important issue as we move into the
wider rol out and an expedited approval process for changing the storage conditions may be
beneficial.
•
The WHO Strategic Advisory Group of Experts (SAGE) are evaluating whethe there is a
differential degree of risk of thrombotic thrombocytopenia syndrome for Janssen versus
AstraZeneca, however, no recommendations have been made. Given the increased risk of
thrombosis in pregnancy, some counties have specifically recommended against
administering adenoviral-vector vaccines to pregnant persons.
•
The Janssen vaccine is being studied in 400 pregnant women
CV TAG members were asked to send any new research, updates, or changes to the Secretariat.
3.0
Research in Children
Key points:
•
Medsafe are considering an extension of the Pfizer provisional approval to include ages 12-
15.
4.0
Vaccine Rollout
The daily vaccine report was presented to CV TAG. Over half a mil ion doses have been
administered, with the delivery of vaccines to nearly 200 different sites around NZ progressing
smoothly as the rollout continues.
It was highlighted that it would be beneficial to report the proportion of eligible Māori population that
have been vaccinated. The Chair noted this is a critical part of the equity reporting framework and
this matter has been relayed to DHBs. Issues with the 2018 census are making this difficult to map.
5.0
Research P oject on BMI and Immunogenicity
Researchers from Auckland provided an overview of the proposed study to evaluate the effect of
BMI and arm size on intramuscular vaccine delivery and immunogenicity. The study will investigate
under the Official Information Act 1982
vaccine delivery into the deltoid muscle by using ultrasound to measure the distance from the skin to
the muscle. Patient finger prick blood samples wil then be analysed for immunogenicity. This will
help to understand the appropriate needle length required for different BMIs.
Key points of discussion:
•
Vaccinators general y decide on which needle length to use by ‘eyebal ing’ patient size.
There is little data currently available on which part constitutes the deltoid muscle in people
with higher BMIs. There has also been some trouble with accessing longer needles that may
be needed for people with extremely high BMIs. This is a concerning issue, particularly for
Released Pacific populations, who may have different arm morphology.
•
Two options were presented for sampling in the study: finger-prick sampling, which is quick
and easy, and can be analysed using spike immunogenicity assays; or venous blood
Document four
sampling, which can allow for more in-depth analysis but is not very practical. CV TAG
recommended the finger-prick option.
•
It was highlighted that it would be useful to compare the proposed method with the approach
that is currently used in order to evaluate the method.
•
It was strongly suggested that researchers ensure that they recruit a sufficient number of
participants from Māori, Pacific and other race/ethnicity populations.
•
It was highlighted that the vaccine rol out is about to expand to Group 3, which includes
those with BMI >40. This wil have relevance towards determining whether the targets of the
study are achievable in the proposed timeframe.
•
It was noted that data on skin thickness is relatively easily to col ect via ultrasound and this
may be shared sooner, however, serology results wil take longer.
CV TAG approved the general approach of the study and requested that the research be shared as
it becomes available. CV TAG members were requested to submit any further suggestions about the
protocol to the Secretariat for provision to researchers of the study.
6.0
Pfizer Decision to use Tier 3
The policy team sought advice from CV TAG regarding any updates for the Decision to Use the
Pfizer COVID-19 vaccine, as Aotearoa-New Zealand moves to vaccinating Tier 3. This is to ensure
that due process is being fol owed and assess whether there is any additional information that needs
to be considered before proceeding with the wider rollout.
Key points:
•
Updated information from the global rollout is being tracked regularly in the science update
documents, and there has not been any evidence to indicate a concern about using Pfizer
for the wider rollout.
•
To date, the safety data from Aotearoa-New Zealand are consistent with the known safety
profile, including in ethnic populations and those with co-morbidities.
•
The COVID-19 Vaccine Independent Safety Monitoring Board (CV ISMB) has been
reviewing adverse events following immunisation and is satisfied with the safety profile of
Pfizer. There are some safety signals being evaluated but there is a high degree of
confidence that these events are consistent with the global rollout.
•
Regarding the reduction in reporting rates for adverse events, it was highlighted that this is
normal because rates generally reduce as vaccinators become more experienced and
confident. The message to the sector is to continue to report anything unexpected and
concerning.
under the Official Information Act 1982
CV TAG agreed that the safety and effectiveness data, to date, regarding the Pfizer COVID-19
vaccine are consistent with previous evidence, with no concerns being raised about using this
vaccine for the wider rollout to group three. CV TAG recommended that no changes are required to
the Decision to Use Pfizer.
7 0
Pregnancy Advice
Prior to the meeting, CV TAG were provided with a literature review on COVID-19 vaccines and
pregnancy and a proposed revised recommendation prepared by IMAC... It was highlighted that
Released
pregnancy is an immune-compromised state, with pregnant persons at higher risk of severe
outcomes from COVID-19 infection. There have been no toxicity issues identified with the COVID-19
vaccine in preclinical studies and there are no first-principle reasons to exclude pregnant persons
from being offered the COVID-19 vaccine. Moreover, emerging real-world data are showing that the
Document four
Pfizer vaccine in safe in pregnant persons. Based on this, CV TAG were requested to revise the
current recommendation for COVID-19 vaccines in pregnancy to reflect the latest data.
Key points:
•
The messaging around pregnancy needs to be clear as the vaccine rollout moves into tier 3,
which may include pregnant women.
•
Data on the safety of the COVID-19 vaccine in pregnant persons have been reported and
international bodies have recommended the COVID-19 vaccine during pregnancy.
•
Without a clear recommendation, it may be difficult to pivot advice rapidly, in the event of an
outbreak, to allow pregnant persons to be vaccinated.
CV TAG agreed that the current recommendation needs to be revised to provide more clarity. It was
noted that this wil be followed up with an engagement process with various stakeholders. CV TAG
members were requested to send any further comments regarding the revised recommendation over
the next few days. The final revised recommendation wil be put forward to the COVID Immunisation
programme for implementation.
8.0
Long-term effects of Pfizer vaccine
This item was not discussed due to time constraints.
7.0
Next Steps/Decisions Pending
None
9.0
Any Other Business
Update on active monitoring: The steering group has provided approval in principle to proceed
with the implementation of an active monitoring system. The process is currently in the technical
assessment phase. The Post Event team are expecting a way forward shortly.
10.0
Agenda items for next meeting
Long-term effects of Pfizer vaccine
11.0
New Action Items Raised During Meeting
None
Meeting closed at
12:00pm Next meeting:
Tuesday 08 June – 11:00am to 12:00pm
under the Official Information Act 1982
Open Actions:
None
Closed Actions Since Last Meeting:
None
Released

Document five
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 08 June 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
Members:
David Murdoch, Edwin Reynolds, Elizabeth Wilson, Helen Petousis-Harris, Ian
Frazer, James Ussher, Nikki Moreland, Nikki Turner, Pippa Scott, Sean Hanna
Ministry of Health Attendees:
Andi Shirtcliffe, Caroline McElnay, Daniel Bernal, Fiona Cal aghan, Chriselle
Braganza, Shayma Faircloth
Guests:
Kris Golding, Tim Hanlon
Apologies:
Al ison Bennett, Juliet Rumball-Smith Matire Harwood, Peter McIntyre, Sue
Crengle, Tony Walls
1.0
Welcome and previous minutes
Ian Town welcomed all Members, Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (25 May 2021) were accepted.
2.0
Science Updates
Updates on the COVID-19 vaccines were highlighted:
•
Pfizer published the Phase 3 trial data from 12-15 year-olds.
•
Israel Health Ministry has concluded that the cases of myocarditis, predominantly in younger
males, fol owing the Pfizer vaccine are probably linked to the vaccine. The US and EU
regulators have stated that a causal link is yet to be established.
under the Official Information Act 1982
•
The rate of thrombosis with thrombocytopenia Syndrome is approximately 1 case in 100,000
for the AstraZeneca vaccine and 1 case in 300,000 for the Janssen vaccine.
•
Preliminary data from the UK reported that the Novavax vaccine has an overal efficacy of
89.7% which is higher than the previously reported efficacy of 60% from South African trials
where the B.1.351 variant was prevalent.
•
Preliminary data suggests that an 8-week interval between two doses of the mixed schedule
of AstraZeneca and Pfizer vaccines leads to high immunogenicity.
Released
It was noted that the AstraZeneca science overview document wil be provided to CV TAG shortly.
CV TAG members were asked to send any new research, updates, or changes to the Secretariat.
3.0
Research in Children
Key points:
Document five
•
Pfizer published the Phase 3 trial data from 12-15 year-olds. In general, safety and efficacy
results from the 1,131 children enrol ed were consistent with the Phase 3 trial in adults.
4.0
Vaccine Rollout
The daily vaccine report was presented to CV TAG. The rollout is proceeding at pace, with
approximately 750,000 doses administered.
5.0
Research Prioritisation Framework
Post-event workstream presented the proposed prioritisation framework for research on surveil ance
questions of importance to NZ.
Key points:
•
Medsafe is interested in any safety concerns and wil not contribute to research support but
wil provide guidance and technical expertise as required.
•
A research workshop will be run held to further these discussions.
Key points of discussion:
•
CV TAG generally supported the prioritisation framework and recommended that equity
considerations be weaved into al criteria in the framework
6.0
Decision to Use Pfizer for 12 -15 years
The policy team sought advice from CV TAG regarding the Decision to Use the Pfizer COVID-19
vaccine for 12-15 year-olds. Medsafe are expected to make a decision on regulatory approval this
week, with advice going to Cabinet thereafter. CV TAG discussed the results from the Phase 3 trials
in children aged 12-15 years for the Pfizer vaccine
Key points of discussion:
•
Myocarditis should be watched closely as a potential safety signal. Any benefits of
administering the vaccine to children should be evaluated against the risks. If the aim is to
reduce the spread of infection, then 12-15 year-olds are not a high priority at this stage,
except those that are vulnerable and at high risk.
•
Children with severe neurodisabilities in institutional care are a vulnerable population in
countries with high prevalence of the disease. This group has been listed as a priority
population in the UK.
•
There should be a clear reason to vaccinate children at a population level. The potential role
of transmission in schools wil have to be evaluated against the potential risks of vaccination
in children. The Science and Technical team are setting up a sub-TAG on testing in children
to understand whether there is a requirement to test more in children and this information
under the Official Information Act 1982
wil feed into the discussion on the decision to use.
•
There is some very early informal discussion in Australia on vaccinating children as they
may have played a role in transmission of the virus during the current Victoria outbreak.
•
Some countries have recommended deferring vaccination of children until there is more
equitable coverage global y in the elderly, healthcare workers, and the general adult
population that are at higher risk from COVID-19 than children.
CV TAG wil provide recommendations in the form of a memo to inform the decision to use the Pfizer
Released
vaccine for 12-15 year-olds, including an evaluation of the risks and the benefits. CV TAG noted that
they would also like to review any conditions recommended by Medsafe, prior to finalising their
recommendations.
Document five
7.0
Upcoming decisions on Janssen and AZ
The policy team noted that Medsafe decisions on the AstraZeneca and Janssen vaccines are
expected shortly and CV TAG wil be consulted for advice on decision to use both of these vaccines.
8.0
Next Steps/Decisions Pending
None
9.0
Any Other Business
Update on use of COVID-19 vaccines in pregnancy: The Ministry has been
working with
RANZCOG to update the recommendations for pregnancy. The recommendations from RANZCOG
are consistent with that of the Ministry, IMAC, and Australian authorities, and state that the Pfizer
vaccine can be administered at any stage during pregnancy.
Concerns over Pfizer vaccine rollout: CV TAG members are drafting a response to address
concerns that were raised in a letter to Medsafe from a general practitioners’ group, regarding the
Pfizer COVID-19 vaccine safety and efficacy.
10.0
Agenda items for next meeting
Update on VAANZ study
11.0
New Action Items Raised During Meeting
None
Meeting closed at
11:36am Next meeting:
Tuesday 15 June – 11:00am to 12:00pm
Open Actions:
None
Closed Actions Since Last Meeting:
None
under the Official Information Act 1982
Released

Document six
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 22 June 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
David Murdoch, Edwin Reynolds, Elizabeth Wilson, Helen Petousis-Harris, Ian
Members:
Frazer, James Ussher, Nikki Moreland, Nikki Turner, Peter McIntyre, Pippa
Scott, Sean Hanna, Sue Crengle, Tony Walls
Andi Shirtcliffe, Caroline McElnay, Daniel Bernal, Fiona Cal aghan, Juliet
Ministry of Health Attendees:
Rumball-Smith, Chriselle Braganza, Shayma Faircloth, Niki Stefanogiannis,
Brooke Hollingshead
Guests:
Kris Golding, Al ison Bennett, Tia Narvaez
Apologies:
1.0
Welcome and previous minutes
Ian Town welcomed all Members, Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (08 June 2021) were accepted.
2.0
Science Updates
CV TAG members were asked to send any new research, updates, or changes to the Secretariat.
3.0
Research in Children
This item was discussed later as part of Item 6.
under the Official Information Act 1982
4.0
Vaccine Rollout
The daily vaccine report was presented to CV TAG. Nearly a mil ion doses have been administered
around New Zealand. The focus is now on equity distribution for Māori and Pacific populations as
internal data shows underperformance in some regions. The Ministry will work with DHBs to facilitate
higher uptake.
Key points:
•
CV TAG suggested that it would be good for the reporting be done in column percent to
Released allow for the denominator to represent each ethnic population. This would identify any
inequity more accurately. It was noted that the Ministry is working on achieving more
accurate reporting and this matter wil be followed up.
Document six
•
CV TAG suggested that a literature review of social drivers may be useful to understand the
requirements for higher coverage in younger people (aged 16 and above). It was noted that
the Ministry’s Behavioural Insights team are looking into these studies.
5.0
Decision to Use Janssen
The Policy team sought advice from CV TAG regarding the decision to use the Janssen COVID-19
vaccine.
Key points of discussion:
•
CV TAG discussed a potential precaution for younger age groups, given the safety signal
observed in the US for thrombosis with thrombocytopenia syndrome (TTS). There is lack of
clarity on whether the frequency of TTS with the Janssen vaccine is similar to that with
AstraZeneca.
•
It is stil unclear whether this is a true one-dose vaccine. Janssen is conducting trials testing
two doses of the vaccine and this data wil shed light on whether a second boost dose is
required for better protection.
•
This vaccine might be less effective against circulating variants of concern. However, it
depends what the objectives of vaccination are. For example, viral vectored vaccines seem
effective at reducing hospitalisation and death but if the aim is to reduce viral infection, then
vectored vaccines seem inferior, particularly after one dose
•
Only a smal supply of Janssen may be required in New Zealand as a potential alternative to
the Pfizer vaccine for some individuals.
•
The option to donate the majority of the Janssen vaccine to countries in need should be
considered, when it becomes available
Overall, CV TAG felt that there is little gain in using the Janssen vaccine, given that it has lower
efficacy than the Pfizer vaccine and noting the safety signals. It wil be challenging to communicate
the benefits versus the risk of this vaccine in New Zealand, where we have little community
transmission. CV TAG were asked to send any additional comments to the Chair and Secretariat for
incorporation into the recommendations.
6.0
Decision to Use Pfizer for 12 -15 years
Medsafe has provisionally approved the Pfizer COVID-19 vaccine for 12-15 year-olds. The Policy
team sought advice from CV TAG regarding the decision to use the Pfizer vaccine in this age group.
Key points o discussion:
•
Children in this age group are at low risk for poor outcomes if they contract COVID-19.
However, achieving target coverage wil require immunisation of younger age groups. We
under the Official Information Act 1982
wil need geographic as well as demographic, e.g., ethnicity, coverage.
•
No safety signals have been observed in this specific age group but there are limited data
available to date.
•
It would be advisable to delay until more safety data is available, especially with regards to
potential safety signals such as myocarditis, which have been reported in some overseas
rollouts eg, Israel
•
No subgroups were identified for prioritisation (with the exception of a smal number of
Released children undergoing cancer treatment or under specialist care) or for precautions, at this
stage.
•
New Zealand is in a low prevalence COVID-19 environment and other groups in the
Sequencing Framework are a higher priority because of the risk of severe health outcomes.

Document seven
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 29 June 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
Andi Shirtcliffe, David Murdoch, Edwin Reynolds, Elizabeth Wilson, Helen
Members:
Petousis-Harris, Ian Frazer, James Ussher, Nikki Moreland, Nikki Turner, Peter
McIntyre, Pippa Scott, Sean Hanna, Sue Crengle, Tony Walls
Ministry of Health Attendees:
Daniel Bernal, Fiona Callaghan, Juliet Rumball-Smith, Chriselle Braganza,
Shayma Faircloth, Niki Stefanogiannis; Brooke Hol ingshead
Guests:
Tim Hanlon; Jared Green, Kris Golding
Apologies:
Caroline McElnay
1.0
Welcome and previous minutes
Ian Town welcomed all Members, Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (22 June 2021) were accepted subject to the fol owing correction being
made to Item 7.0.
•
Antibody testing may be useful for monitoring immune responses of incoming workers and
this can also be used to validate vaccine certificates, however it is not recommended at this
stage.
2.0
Myocarditis after Pfizer Vaccination
•
Advice on the Decision to Use Pfizer for 12-15-year-olds was issued to Cabinet, however a
decision has been deferred pending advice from CV TAG on myocarditis.
under the Official Information Act 1982
•
The FDA have added a warning for myocarditis and pericarditis to the Pfizer and Moderna
vaccine data sheets, after observing a series of cases following vaccination. It is seen most
predominantly in adolescent and young adults, particularly males aged <30 years, and after
the second dose. CV TAG discussed the current evidence and risks.
Key points of discussion:
•
The University of Auckland is leading a project estimating background rates of adverse
events in New Zealand, including myocarditis, and is expected to report findings within the
Released next 7-10 days. Data on the ethnic breakdown of cases was requested to be included.
•
CV TAG noted concern about the potential risk of myocarditis has grown and a sense of
urgency to develop options, e.g., for alternative vaccine schedules, and advice.
Document seven
•
While evidence is stil emerging, IMAC clinicians are already fielding requests on
myocarditis. It was noted that because the issue is relatively rare, the true risk may not be
known for some time until the vaccine rollout internationally has progressed further.
•
There is a need to communicate safety information to inform the public and present a
balanced assessment of the risk and benefits. Science communicators who can appeal to a
range of different ethnicities wil be important.
•
Further information is needed on vaccine hesitancy among young adults and men <30 and
how this may be impacted by a potential safety signal, to inform how the commentary would
be managed.
•
Possible options raised by CV TAG included:
o Considering using only a single dose among people who are at higher risk (e.g.
young males <30, people with a history of myocarditis) until further evidence is
available. It was noted that Israel is actively considering this option
o Heterologous vaccine schedules (e.g., offering Janssen or another vaccine – when
available - as a second dose).
o Considering the ongoing use of Pfizer in young males <30 until further evidence
emerges. It was noted that many within this population would have been captured
under groups 1-3. Data on the numbers in each of these groups, as wel as when
they are expected to be vaccinated, is needed from CVIP.
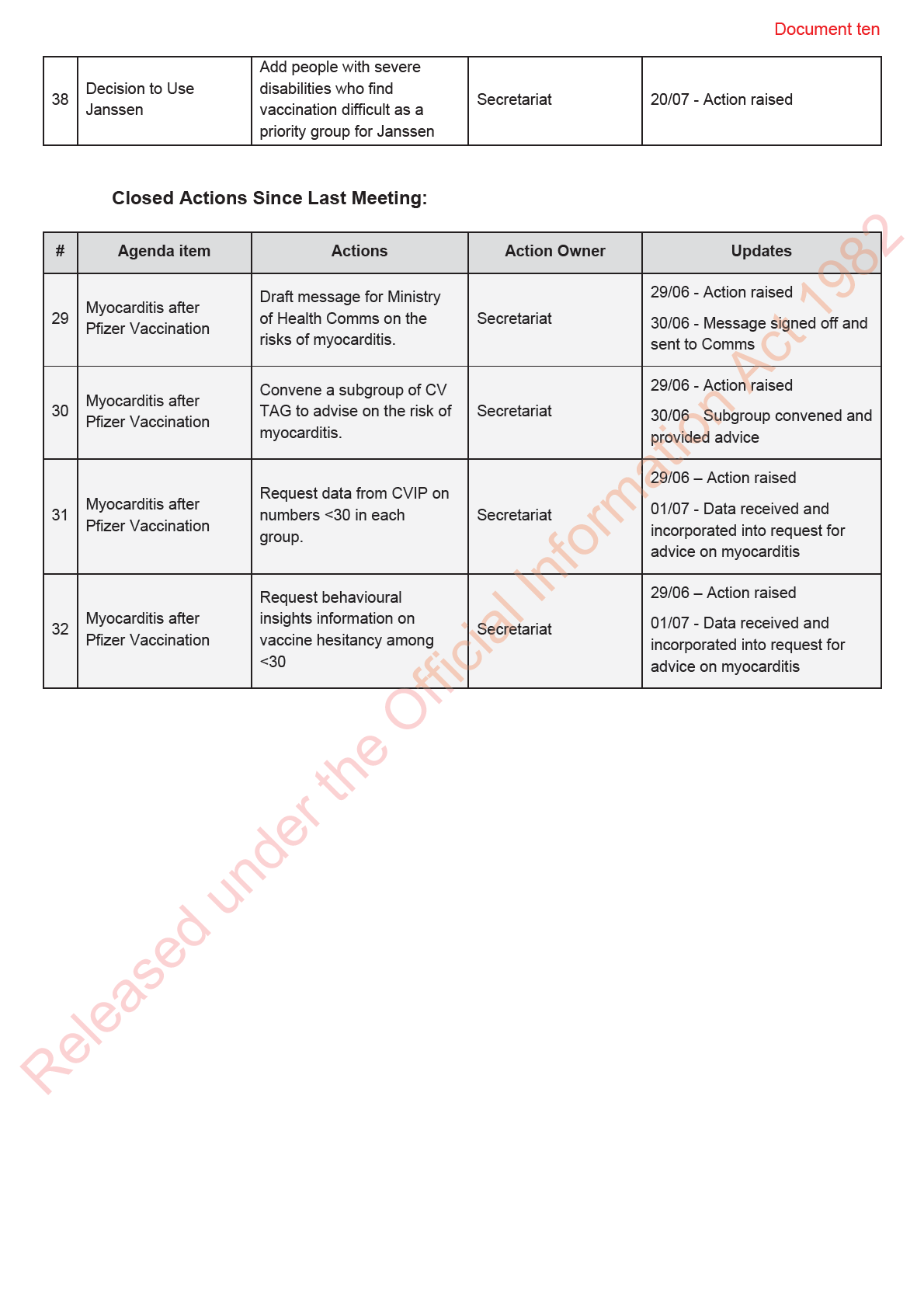
It was agreed that a subgroup would be convened to draft advice which wil be presented to the CV
TAG next week (06 July) to inform recommendations around using the Pfizer vaccine in younger
people.
3.0
COVID-19 Vaccination in the Frail Elderly
•
CV TAG were informed that there have been two recent incidences of frail elderly individuals
passing away shortly fol owing administration of the Pfizer vaccination. Each was showing
serious progressive decline prior to vaccination, and there was a concern from the family
and general practitioner that the vaccination may have played a role in their death.
•
The Ministry of Health and Medsafe have received requests for advice on this issue, and
therefore it was considered important to develop guidance to be proactive, ensure
consistency, and to support and empower health professionals to make decisions.
•
CV TAG reviewed the science advice, ethics document and draft recommendations on
administering the COVID-19 vaccine in the frail elderly.
•
Draft recommendations for consideration by CV TAG are summarised below:
under the Official Information Act 1982
o The COVID-19 Vaccine Immunisation Programme (CVIP) recommends that all
eligible adults, including the frail and elderly with several comorbidities are offered
vaccination against COVID-19 provided that there are no contra-indications to
vaccine administration, to provide protection for both the individual as well as their
surrounding community. This is consistent with advice provided by ATAGI/DHHS
(Australia).
o CVIP endorses individual clinical risk/benefit appraisal and shared decision making
between clients, whānau, surrogate decision makers, and clinicians on the
Released individual.
Key points of discussion:
•
It was noted that this is not a problem specific to the COVID-19 vaccine; evaluating the
benefits and risks of therapies and interventions in the frail elderly is a common occurrence.

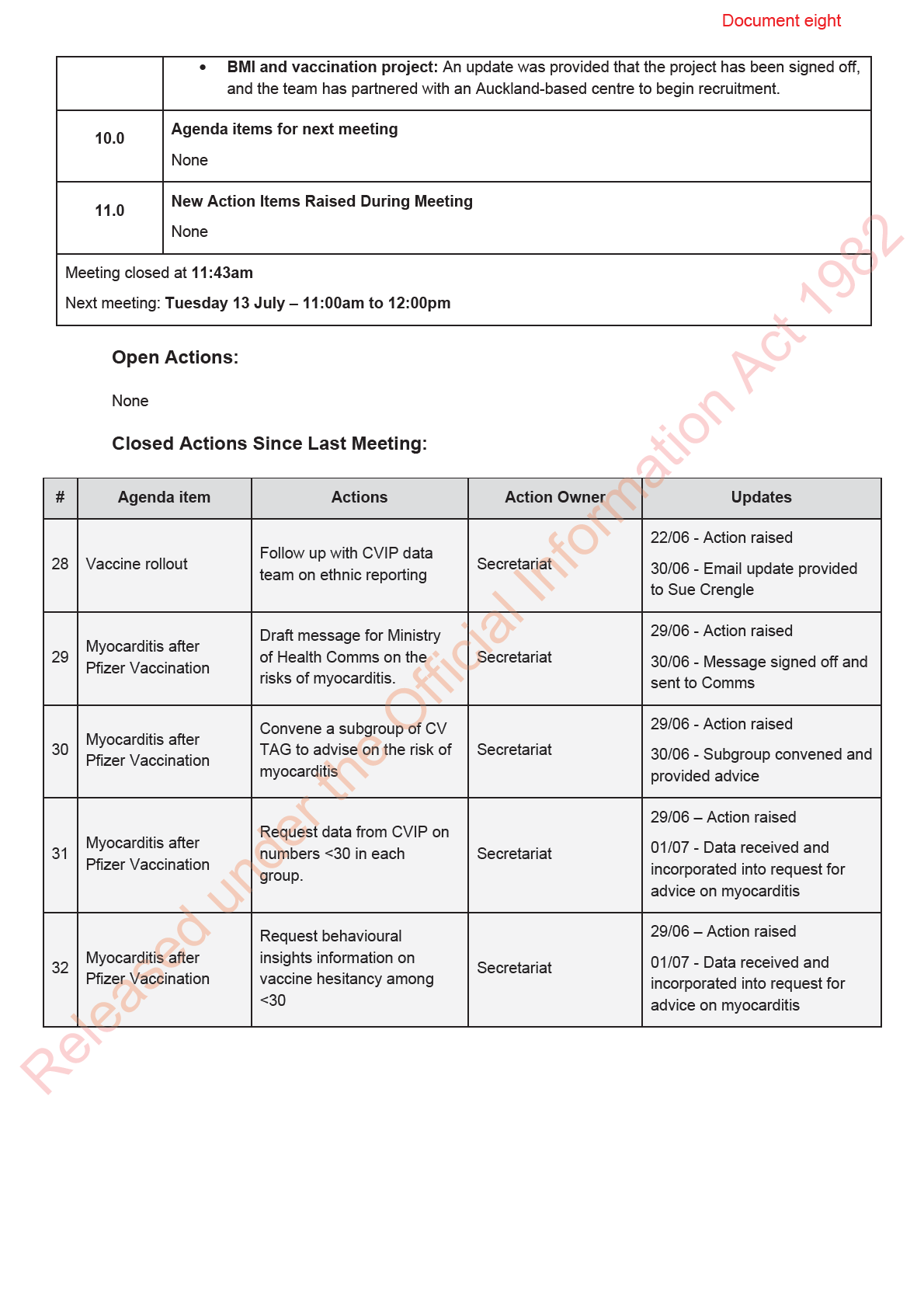
Document eight
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 06 July 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
Members:
David Murdoch, Elizabeth Wilson, Helen Petousis-Harris, James Ussher, Nikki
Moreland, Peter McIntyre, Pippa Scott, Tony Walls
Ministry of Health Attendees:
Caroline McElnay, Edwin Reynolds, Fiona Callaghan, Juliet Rumbal -Smith,
Chriselle Braganza, Shayma Faircloth, Niki Stefanogiannis,
Guests:
Janelle Duncan
Apologies:
Andi Shirtcliffe, Daniel Bernal, Ian Frazer, Nikki Turner, Sue Crengle, Sean
Hanna
1.0
Welcome and previous minutes
Ian Town welcomed all Members, Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (29 June 2021) were accepted subject to the fol owing correction being
made to Item 2.0 (in red):
•
There is a need to communicate safety information to inform the public and present a
balanced assessment of the risk and benefits. Science communicators who can appeal to a
range of different ethnicities, genders, and ages wil be important.
2.0
Science Updates
Key points:
under the Official Information Act 1982
•
Evidence is emerging to indicate that a heterologous regimen consisting of AstraZeneca as
the first dose and Pfizer as the second dose induces robust immune responses.
•
Preliminary data are available with regards to immune correlates of protection, however,
more data are required to make reliable inferences about efficacy.
•
Preliminary data are available for a third dose of AstraZeneca, and third doses in those who
are immunocompromised.
3.0
Research in Children
Released
This item was discussed as part of Item 6.0
4.0
Vaccine Rollout
A batch of 150,000 doses of Pfizer arrived ahead of schedule this week, with the next delivery
expected next week. Further batches are expected to arrive late July, as the immunisation
Document eight
programme to scales up. Nearly 500,000 people have been administered two doses of the vaccine
to date.
5.0
Janssen – Decision to use
The Janssen COVID-19 vaccine has been granted provisional approval by Medsafe. No precautions
were added, but a warning regarding potential risk of thrombosis and thrombocytopenia has been
included. CV TAG’s recommendations for the decision to use the Janssen vaccine wil be provided
to the immunisation programme.
6.0
Myocarditis after Pfizer Vaccination
CV TAG discussed advice provided by the STA and a subgroup of CV TAG, on the current evidence
on events of myocarditis/pericarditis post vaccination, and related questions.
Key points:
•
Previous studies of US military personnel, that evaluated the risk of myocarditis fol owing the
smallpox vaccine, indicated that myocarditis was a potential safety issue, with cases usually
occurring within a few days of vaccination.
•
Events of myocarditis tend to be associated with the second dose of mRNA COVID-19
vaccines, although some cases occur after the first dose. The rate of myocarditis tends to be
higher in males and younger age groups, particularly in males aged 16-30.
•
There is limited information, to date, on the long-term outcomes and severity of myocarditis
following vaccination. Of the 29 cases in the Vaccine Safety Datalink (VSD) reported in the
US, 24 (83%) were hospitalised with a median stay of 1 day (range 0-13 days), including two
who were admitted to the ICU. Al cases were discharged, and nearly al cases had
resolution of symptoms at follow up.
•
Overall, emerging evidence suggests that myocarditis is a largely self-limiting and rare event
following mRNA vaccination, with the rate for Pfizer in the US being approximately 0.8 per
100,000 in 12-39 year-olds within 21 days following the second dose.
•
CV TAG discussed possibility of alternative vaccination schedules that might mitigate the
risk in younger age groups. However, any change in dosing schedule will require Medsafe
approval.
•
CV TAG discussed potential recommendations, including advice for those with rheumatic
heart disease, those with a previous history of myocarditis, or those who develop
myocarditis fol owing the first dose.
A subgroup of the CVTAG will meet 08 July to draft recommendations. The recommendations will be
finalised by the end of week and discussed at the next CV TAG ful meeting.
under the Official Information Act 1982
7.0
VAANZ Research Update
An update was provided on the VAANZ study evaluating immunogenicity of the Pfizer vaccine in the
Aotearoa New Zealand population, with equity as a key priority. The study has enrolled around 113
individuals (of the total 300) to date. Approximately 30% are Māori and 40% are Pacific Peoples.
8.0
Next Steps/Decisions Pending
None
Released
9.0
Any Other Business
•
Advice for vaccination in the frail elderly: Recommendations have been finalised and
shared with the relevant peak bodies.

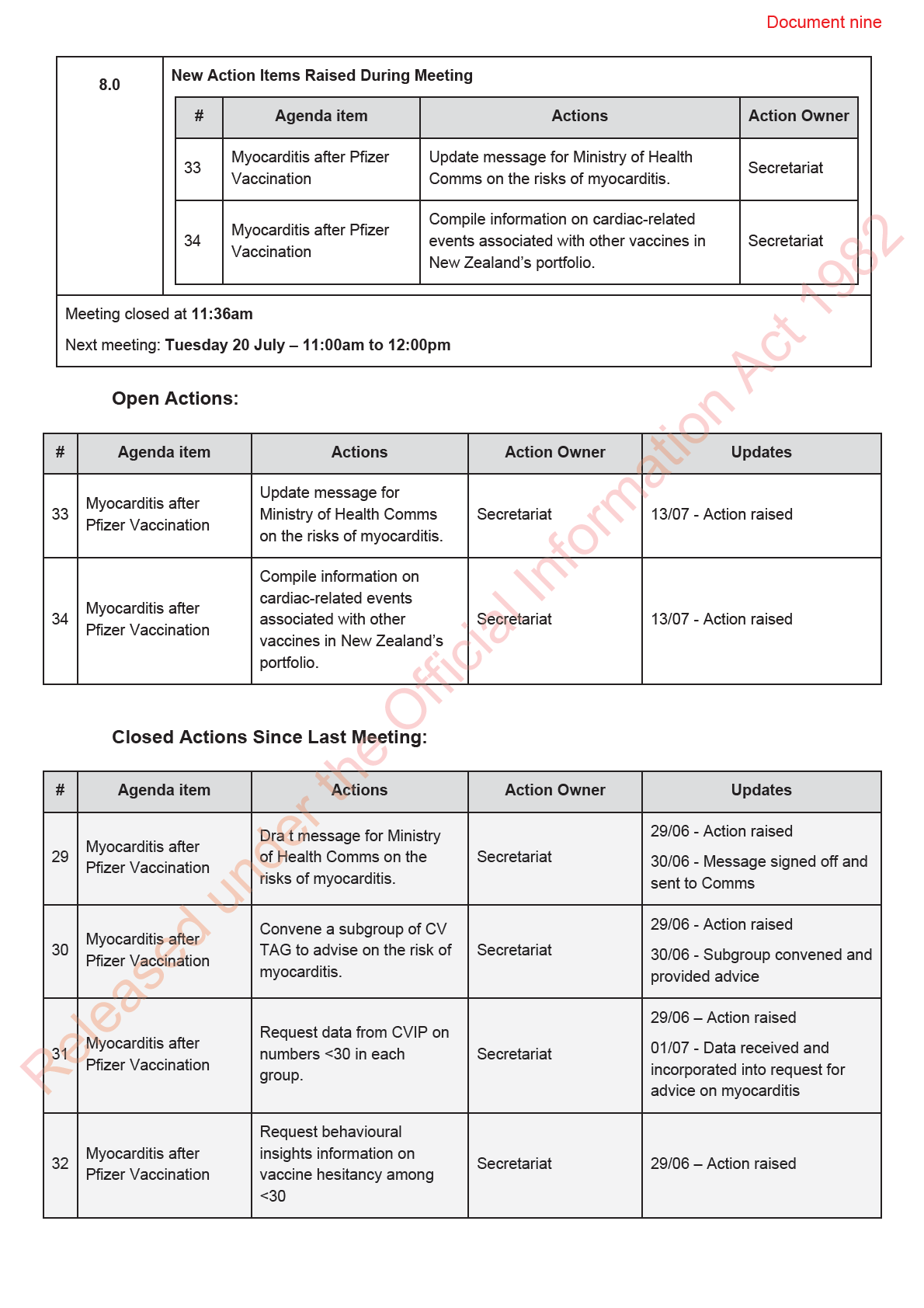
Document nine
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 13 July 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
Members:
David Murdoch, Elizabeth Wilson, Helen Petousis-Harris, James Ussher, Nikki
Moreland, Peter McIntyre, Pippa Scott, Sue Crengle,
Ministry of Health Attendees:
Andi Shirtcliffe, Daniel Bernal, Edwin Reynolds, Fiona Callaghan, Juliet Rumbal -
Smith, Chrisel e Braganza, Shayma Faircloth, Brooke Hollingshead
Guests:
Bryan Mitchelson
Apologies:
Nikki Turner, Niki Stefanogiannis, Tony Walls, Sean Hanna, Ian Frazer, Caroline
McElnay
1.0
Welcome and previous minutes
Ian Town welcomed all Members, Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (06 July 2021) were accepted.
2.0
Vaccine Rollout
The vaccine rollout continues to scale up. The focus wil progressively move to the general
population (Group 4), and there wil be a corresponding shift in communications to focus on getting
everyone vaccinated. The national booking system will go live soon.
3.0
Children Priority Groups
This item was not discussed and wil be carried over to next week.
under the Official Information Act 1982
4.0
Myocarditis Recommendations
•
Draft recommendations on the risk of myocarditis after mRNA vaccination were presented to
CV TAG.
•
It was noted that, this is a developing issue, and there are stil several uncertainties in the
data.
•
Based on preliminary US data, the risk of myocarditis after Pfizer vaccination is
Released approximately 1 in 25,000 for males 12-29 years, and 1 in 240,000 for females 12-29 years.
For individuals 30 and over, the corresponding risks decrease to approximately 1 in 400,000
for males, and 1 in a mil ion for females. While the risk for females is lower than for males, it
is stil greater for younger people, and therefore any recommendation should be applied to
all people aged under 30.
Document nine
•
The New Zealand context of having no community transmission is important to consider, as
the risk of COVID-19 is currently low and this effects the benefit:risk assessment.
•
CV TAG noted that cardiac-related events after vaccination are being reported to CARM,
and the Independent Safety Monitoring Board (ISMB) is reviewing reported cases.
•
Emerging evidence suggests one dose of the vaccine appears to be highly immunogenic,
and provides greater protection in younger compared to older age groups, and therefore
may provide sufficient protection in the interim, until further evidence emerges on second
dose options.
•
CV TAG progressed to summarise an initial draft of the approach:
o The second dose of Pfizer vaccination could be deferred in individuals aged 29
years and under until further information is available about the risk, long-term
outcomes of myocarditis and/or pericarditis, and protection offered by one dose for
this age group.
o People 29 years of age and younger who require regular clinical re iew by a
cardiologist are advised to discuss the risks and benefits of the first dose of COVID-
19 vaccine for their specific situation with their healthcare team
o People aged 30 years and over should stil receive two doses of the vaccine, 21
days apart as the risk of myocarditis and/or pericarditis post vaccination is less than
1 in 400,000 and risks of severe disease and sequelae due to COVID-19, including
myocarditis, are substantial y higher in this age group compared to people aged 29
years and under.
o Anyone who develops confirmed myocarditis and/or pericarditis after the first dose
should not receive a second dose of the Pfizer COVID-19 vaccine. CV TAG wil
consider alternative options for a second dose of COVID-19 vaccination in this
group at a future date as evidence emerges from overseas safety monitoring.
o CV TAG wil continue to monitor all relevant effectiveness and safety data closely
and advise on the need and options for the second dose for individuals aged 29
years and under at a future date. Options for the second dose may include: 1)
proceeding with the second dose of the Pfizer COVID-19 vaccine after a longer
interval between doses; 2) not administering a second dose; 3) administering a
second dose of an alternative COVID-19 vaccine.
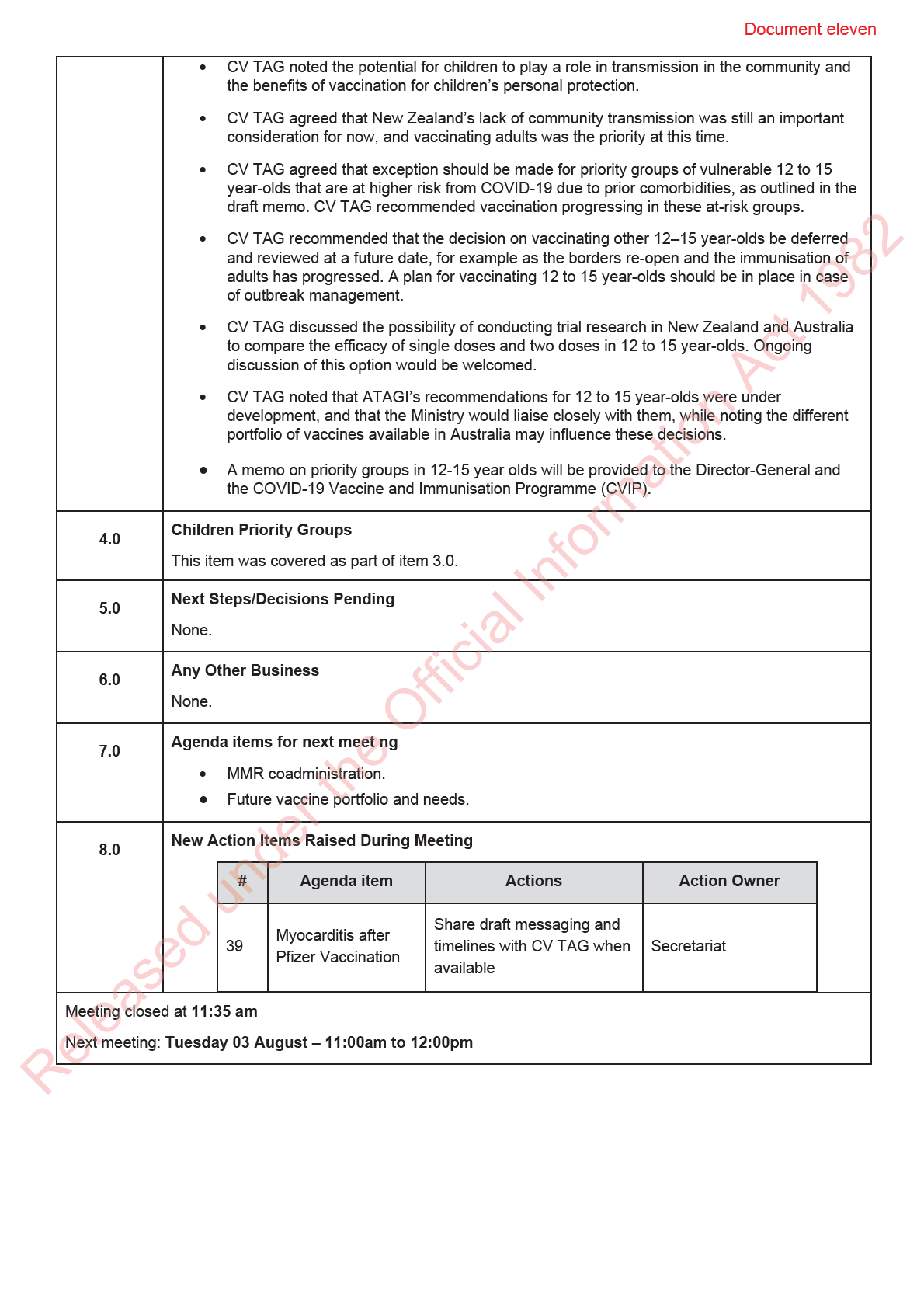
•
A memo with these recommendations is being prepared and wil be shared with CV TAG for
feedback. Public-facing communications will be drafted for CVIP Communications. Options
wil need to remain agile as further evidence emerges.
•
Cardiac related events associated with alternative vaccine schedules wil be explored by the
Science and Technical Advisory team, as wil the use of other options.
•
Given that vaccinating the whānau together is a key approach for delivering the vaccine to
Māori, further discussion wil be needed on the equity implications of these
under the Official Information Act 1982
recommendations.
•
The Director-General wil need to be consulted about the options and the CVIP team wil
need to consider the implications for the programme.
5 0
Next Steps/Decisions Pending
None.
Released
6.0
Any Other Business
None.
7.0
Agenda items for next meeting
Children Priority Groups.

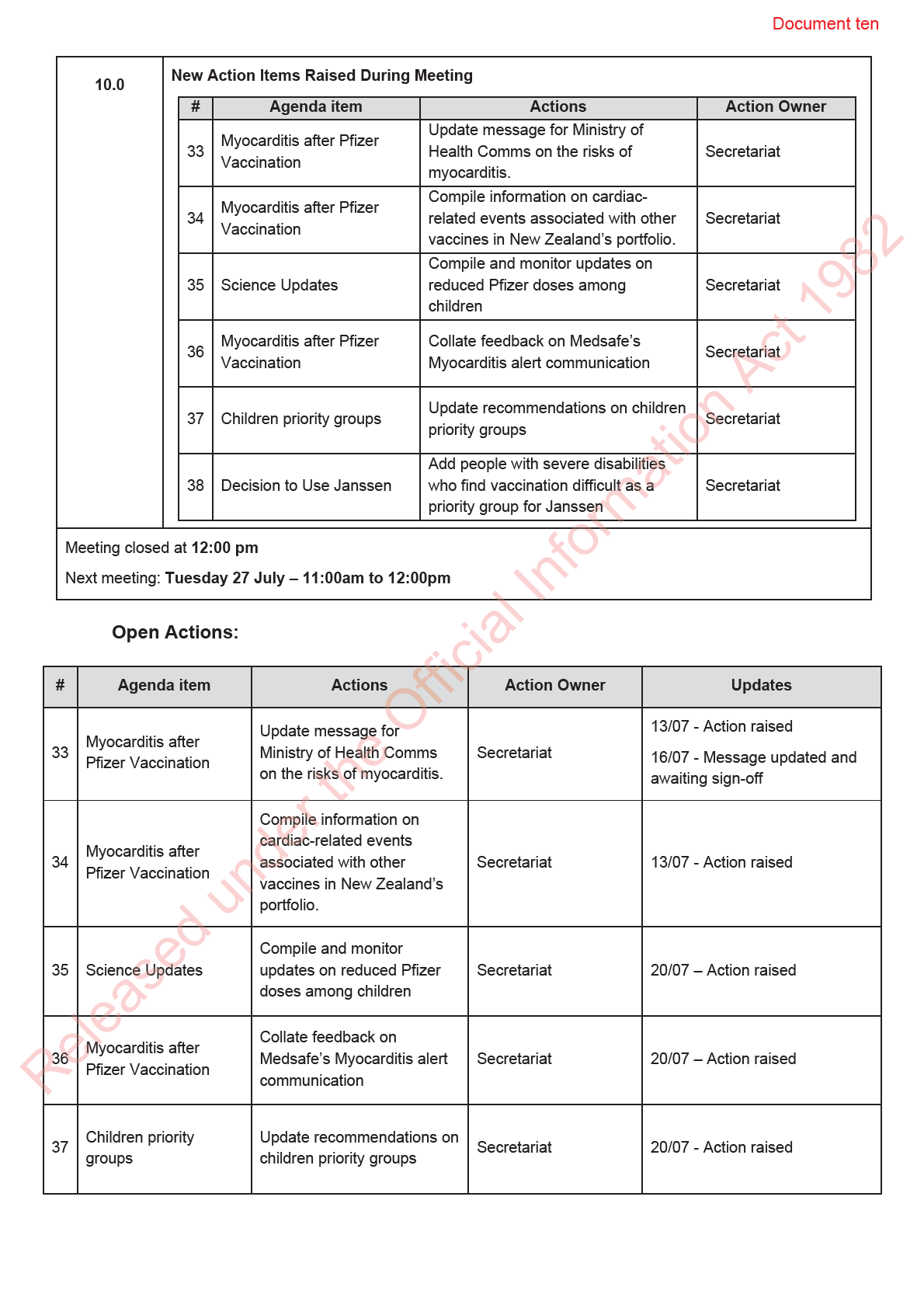
Document ten
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 20 July 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
Members:
David Murdoch, Elizabeth Wilson, Ian Frazer, Nikki Turner, Peter McIntyre,
Pippa Scott, Sean Hanna, Sue Crengle, Tony Wal s
Ministry of Health Attendees:
Caroline McElnay, Daniel Bernal, Edwin Reynolds, Fiona Cal aghan, Brooke
Hollingshead
Guests:
Bryan Mitchelson, Janel e Duncan
Andi Shirtcliffe, James Ussher, Shayma Faircloth, Helen Petousis-Harris, Nikki
Apologies:
Moreland, Juliet Rumbal -Smith, Niki Stefanogiannis, Chris James, Derek
Fitzgerald, Susan Kenyon
1.0
Welcome and previous minutes
Ian Town welcomed all Members Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (13 July 2021) were accepted.
2.0
Science Updates
Updates on the COVID-19 vaccines were highlighted:
•
The US Food and Drug Administration and European Medicines Agency have added
warnings to the vaccine data sheets for Janssen and AstraZeneca on Guillain-Barré
syndrome.
under the Official Information Act 1982
•
Evidence on single dose effectiveness was added to the science updates.
•
It was noted that Pfizer is trialling lower doses among young people aged under 12.
3.0
Research in Children
This item was not discussed.
4.0
Vaccine Rollout
Released
The daily vaccine report was presented to CV TAG. The rollout is proceeding at pace, and larger
deliveries of Pfizer are expected each month. The Ministry is on track to move into the next round of
invitations (Group 4 from 28th July).
5.0
Myocarditis Recommendations Update
Document ten
•
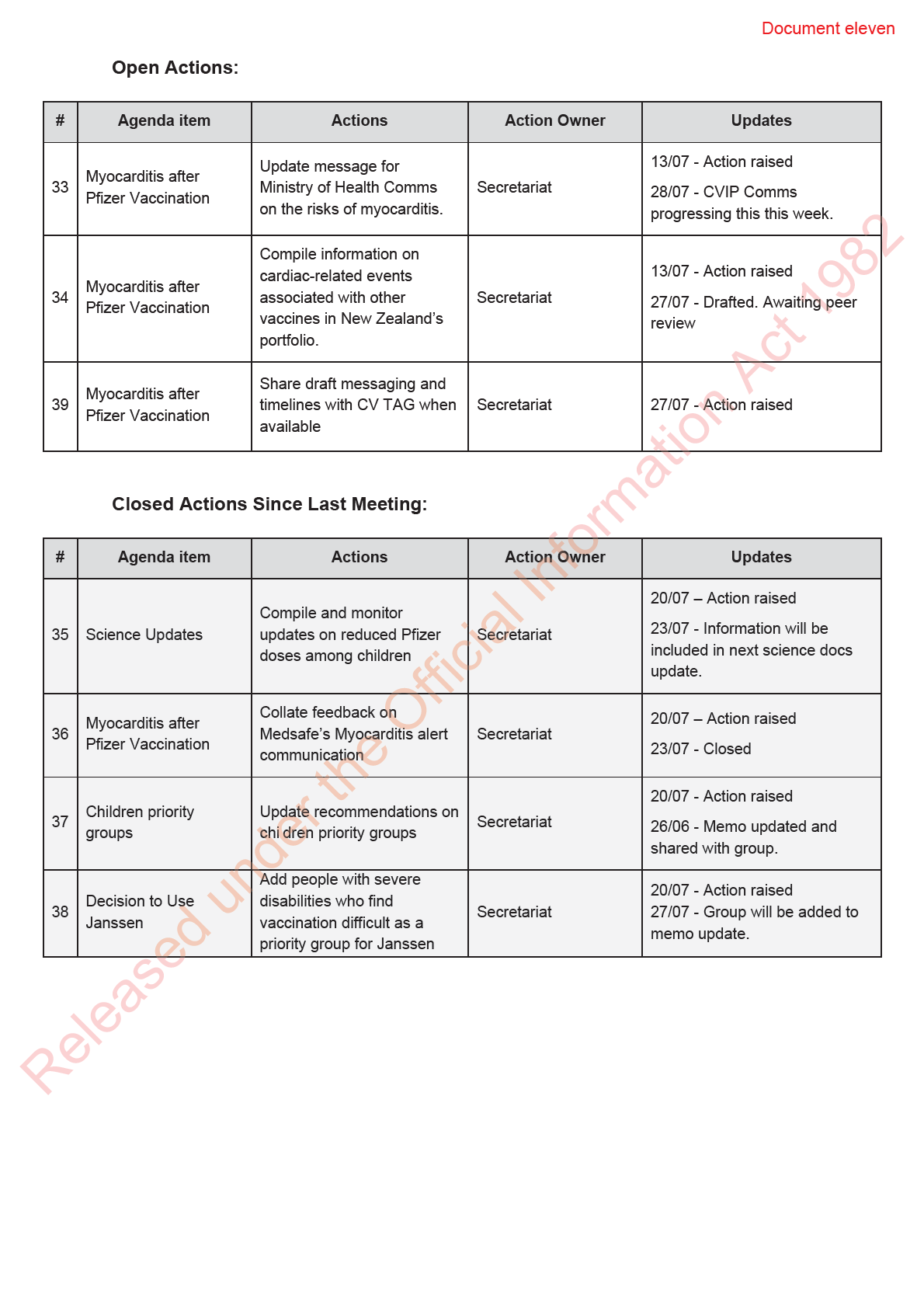
A Medsafe alert on myocarditis wil be published later this week. The draft communication
was shared with CV TAG, and feedback wil be col ated by the Secretariat to share back to
Medsafe.
•
CV TAG discussed the background rates of myocarditis, and rates post-Pfizer vaccination,
internationally and in Aotearoa New Zealand.
o It was agreed that the US rates provided the best available baseline for
comparisons with Aotearoa New Zealand.
o The US data is broken down further by gender, age group and follow-up time, and
notes a risk of 1 in 25,000 for males aged 12-29 within 7 days of the second dose,
and 1 in 238,000 for females aged 12-29 within 7 days of the second dose, for
mRNA vaccines.
o Severity measures should also be incorporated into the presentation of the data, for
example hospitalisation and/or ICU admission rates, if data are available.
•
Draft recommendations on the risk of myocarditis after Pfizer vaccination were discussed.
o CV TAG noted that there is some evidence that young people aged 16 to 29 years
have a strong immune response after one dose, however that two doses provide the
best protection. A delayed schedule for the second dose was discussed. Whether
this potentially reduces the risk of myocarditis, in addition to the severity of other
adverse events, is unknown.
o CV TAG recommended that for people aged 16 to 29 years the second dose be
administered at least 8 weeks after the first.
o It was noted that this would have practical implications for the booking system,
planning mass vaccination events, and public risk communications.
•
A memo with these recommendations wil be updated and provided to the Director-General
and CVIP.
6.0
Children Priority Groups
•
Draft recommendations for potential priority groups among children were shared with the
group, to inform the Decision to Use for 12- to 15-year-olds
• Priority groups over eas have included children who are about to under long-term
immunosuppression, immunocompromised, in long-term residential care, requiring
transplants or who have neurologic disabilities or gastrointestinal (multi-system medically
vulnerable) conditions. Risk factors for COVID-19 such as obesity, respiratory disease, and
ethnicity should also be taken into account.
•
CV TAG noted that the New Zealand’s lack of community transmission was an important
consideration for now, and vaccinating adults was the priority at this time.
under the Official Information Act 1982
•
STA will revise draft recommendations and share with CV TAG.
7.0
Next Steps/Decisions Pending
None.
8.0
Any Other Business
It was noted that Janssen could be an option for people with severe disabilities who find vaccination
difficult, and therefore this group should be added to the ‘Decision to Use Janssen’ memo.
Released
9.0
Agenda items for next meeting
MMR and flu vaccine scheduling and co-administration was discussed. The STA are currently
drafting advice on this for CV TAG’s consideration, and it is scheduled for discussion at CV TAG’s
meeting on Tuesday 3 August.

Document eleven
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 27 July 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
Members:
Elizabeth Wilson, James Ussher, Nikki Moreland, Nikki Turner, Peter McIntyre,
Sue Crengle, Tony Wal s
Andi Shirtcliffe, Caroline McElnay, Edwin Reynolds, Fiona Callaghan, Juliet
Ministry of Health Attendees:
Rumball-Smith, Niki Stefanogiannis, Brooke Hollingshead, Shayma Faircloth,
Pippa Scott
Guests:
Kris Golding
Apologies:
David Murdoch, Helen Petousis-Harris, Ian Frazer, Sean Hanna, Daniel Bernal
1.0
Welcome and previous minutes
Ian Town welcomed all Members, Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (20 July 2021) were accepted.
2.0
Myocarditis Recommendations Update
The final memo on Myocarditis after Pfizer mRNA vaccination was shared with CV TAG and
discussed.
•
The final memo included input and advice from Medsafe.
•
The Director-General has received the recommendations, and an implementation plan is
currently being prepared within the Ministry, once the recommendations have been agreed
by Ministers
under the Official Information Act 1982
•
CV TAG discussed the data supporting longer dosing intervals for Pfizer; Data showed
higher immunogenicity was associated with an extended dosing interval (median 10 weeks)
compared to the usual 3-4 weeks.
•
CV TAG discussed the recommended dosing interval for people under 30 years. CV TAG
discussed the while an 8-week interval is recommended for this age group, administering
the second dose between 6 and 12 weeks is acceptable, and that the exact timing is a
programming decision.
Released •It was agreed that all changes must communicated in a way to provide clarity.
3.0
Decision to Use Pfizer 12-15 year-olds
CV TAG reviewed the memo on the Decision to Use Pfizer for 12- to 15-year-olds (dated 24 June
2021).

Document twelve
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 3 August 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
Members:
David Murdoch, Ian Frazer, James Ussher, Jono Hoogerbrug, Nikki Moreland,
Nikki Turner, Peter McIntyre, Sue Crengle, Tony Walls
Ministry of Health Attendees:
Andi Shirtcliffe, Brooke Hollingshead, Daniel Bernal, Edwin Reynolds, Fiona
Callaghan, Shayma Faircloth,
Guests:
Christian Marchello, Kris Golding
Caroline McElnay, Elizabeth Wilson, Helen Petousis-Harris, Juliet Rumball-
Apologies:
Smith, Niki Stefanogiannis, Sean Hanna
1.0
Welcome and previous minutes
Ian Town welcomed all Members, Attendees and Guests in his capacity as Chair of the COVID-19
Vaccine Technical Advisory Group (CV TAG).
Minutes of the last meeting (27 July 2021) were accepted.
2.0
Science Updates The Chair advised that in future, the science documents on the vaccines and research in children
wil be moved to the back of the materials as an appendix. The documents wil be updated for the
fortnightly meetings, however the agenda wil include a discussion prompt once a month.
3.0
Research in children
Item covered under 2.0, and the same discussion prompt wil apply for future meetings.
under the Official Information Act 1982
4.0
Myocarditis Recommendations Update
The Chair updated CV TAG on progress with the final recommendations on myocarditis.
•
The Director-General has accepted the recommendations. An announcement and
implementation plan for extending the dosing interval is forthcoming.
•
It wil result in significant programmatic changes and has important equity considerations,
however the emphasis on distributing first doses to priority groups has been noted and
accepted.
Released
5.0
Decision to Use Pfizer 12- to 15-year-olds and Children Priority Groups
•
The chal enges posed by the Delta variant and emerging data on differences in clinical
severity among children were discussed with respect to vaccination in children.
Document twelve
•
Earlier advice had been that a broader decision on vaccinating 12- to 15-year-olds should be
deferred.
•
Aotearoa New Zealand’s lack of community transmission was noted as an important
consideration in making this decision.
•
An exception should be made for priority groups of 12- to 15-year-olds that are at higher risk
from COVID-19 due to prior comorbidities, as are outlined in the draft memo, which CV TAG
supported.
•
Vaccinations as part of outbreak management, for example in schools, was also considered
an exception.
•
Opportunities provided by mass vaccination events and vaccinating whānau together were
noted as important considerations.
•
The Decision to Use for 12 to 15-year-olds and memo on priority groups will be provided to
the Director-General and the COVID-19 Vaccine and Immunisation Programme (CVIP).
6.0
Dosing interval for Pfizer
•
The Request for Advice (RfA) on this topic was reviewed.
•
The data on improved immune responses with a delayed interval was noted as promising.
•
It was noted that, in the event of an outbreak, there would be reduced protection for those
who have only had one dose. CV-TAG therefore encouraged surge capacity to be built into
the programme in case of an outbreak.
•
Exceptions to the longer intervals among immunosuppressed people (e.g., with solid
tumours) was discussed, and the Science and Technical Advisory team wil progress
consultation and discussion on these exceptions.
•
The RfA on evidence on the dosing intervals wil be shared with the Director-General.
7.0
Future Vaccine Portfolio
•
The Ministry’s Policy team has requested CV TAG advice on considerations for ongoing
purchasing for New Zealand’s vaccine portfolio from a scientific perspective.
•
The RfA prepared by the Science and Technical Advisory Team on this topic was reviewed.
Data on immunity, ’booster’ doses, safety concerns and the impact of variants was
discussed.
•
Data on long-term immunogenicity and antibody levels are stil emerging, however initial
data suggests immunity is long-lasting (at least 8 months for antibody levels). Currently
there are no precise correlates of protection, however the presence of neutralising
under the Official Information Act 1982
antibodies is a useful measure.
•
Further evidence on immunogenicity and clinical outcomes are awaited.
•
It was noted that there may be other factors impacting purchasing outside of scientific or
clinical evidence, and that some countries have begun purchasing booster doses.
•
Local immunogenicity data needs to be incorporated into the Request for Advice, and it was
noted that VAANZ would be collecting some further local information in their clinical trial
currently underway.
Released •Within the wider portfolio, it was noted that a formal application had not yet been received by
Medsafe from Novavax.
•
Evidence regarding heterologous vaccine schedules is emerging, and wil be a consideration
for those individuals who require an alternative to Pfizer.
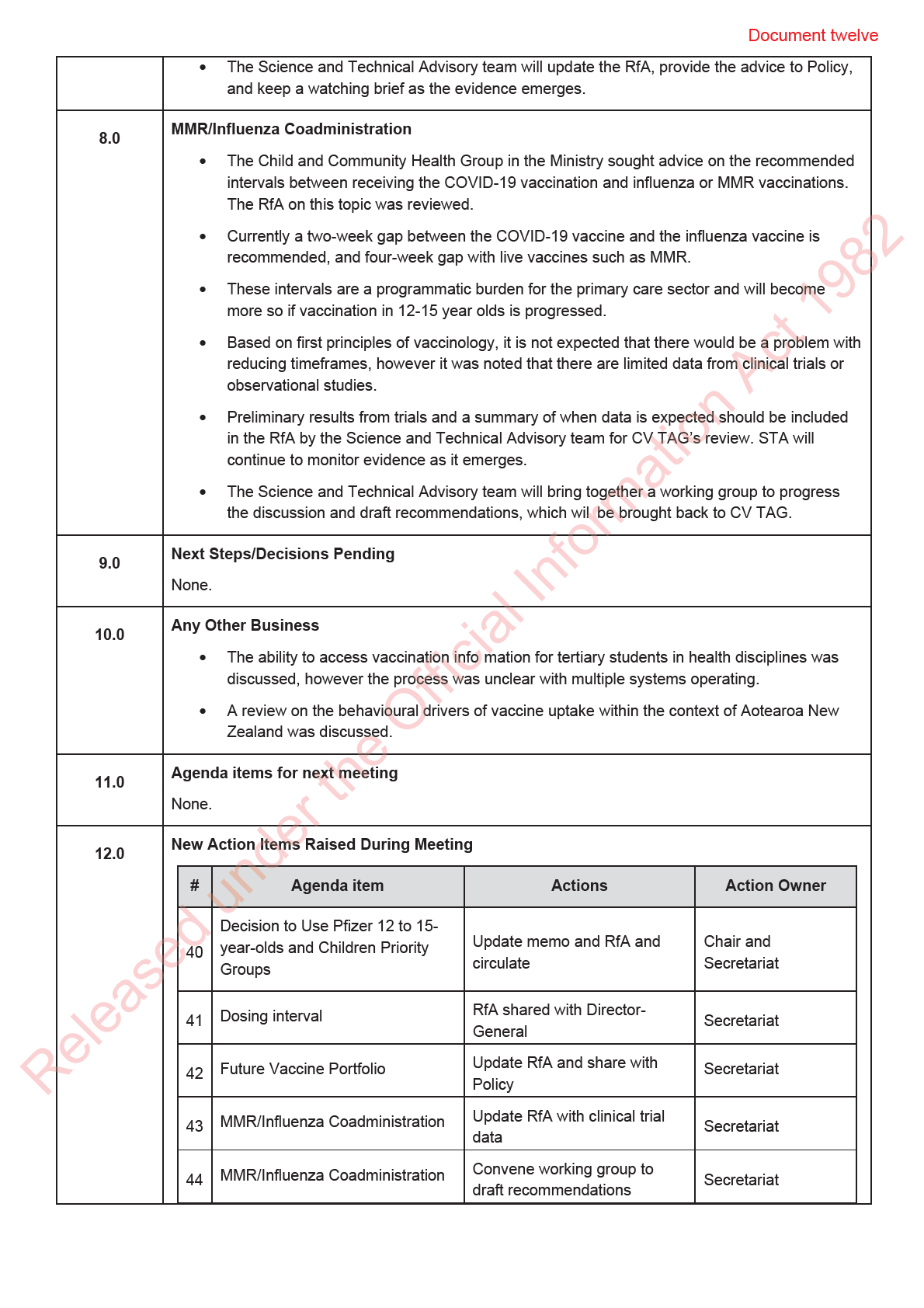
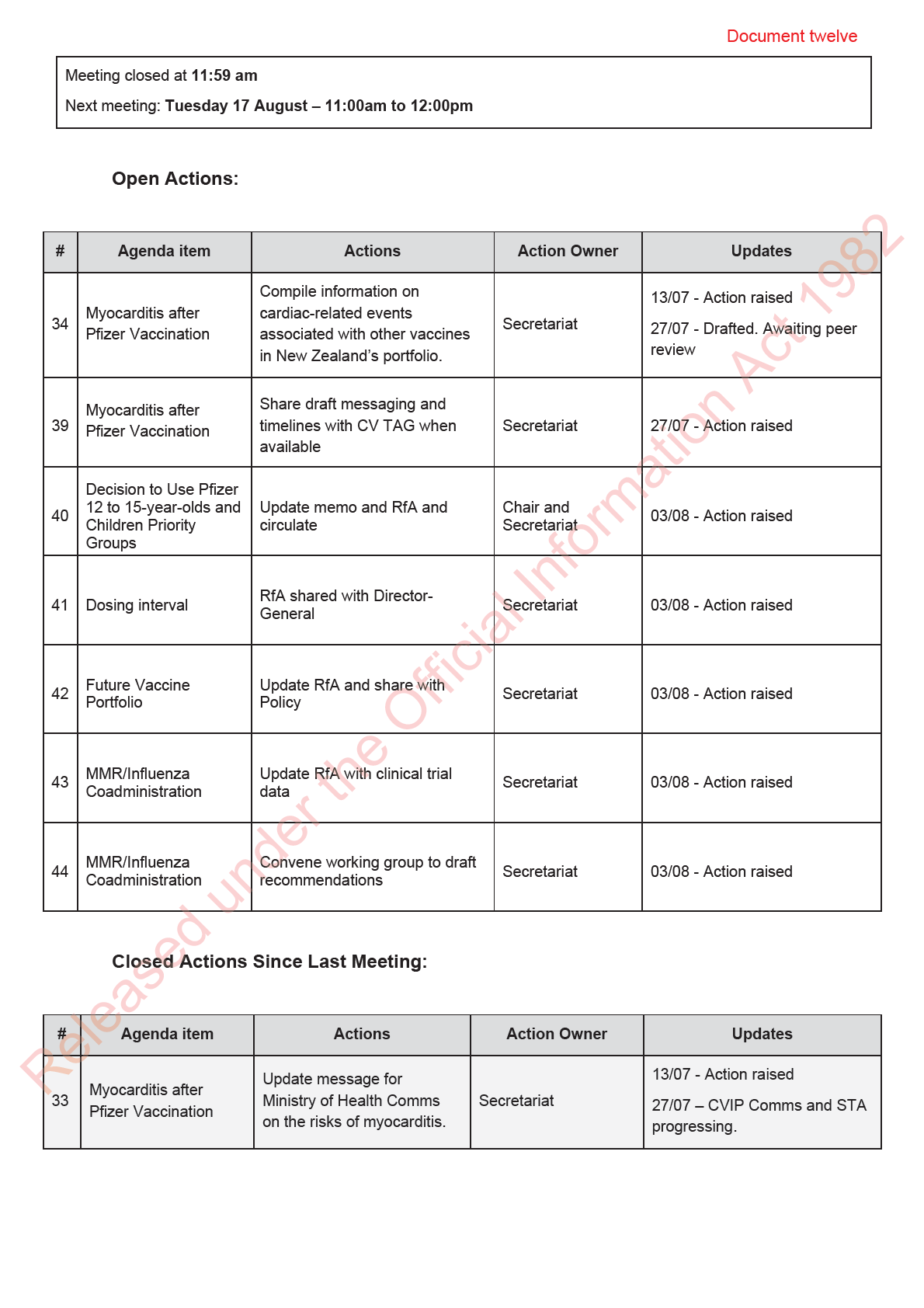

Document thirteen
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 17 August 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
1982
Elizabeth Wilson, Helen Petousis-Harris, James Ussher, Nikki Moreland, Nikki
Members:
Turner, Peter McIntyre, Sean Hanna, Sue Crengle, Tony Wal s
Andi Shirtcliffe, Brooke Hollingshead, Daniel Bernal, Edwin Reynolds, Fiona
Ministry of Health Attendees:
Callaghan, Juliet Rumbal -Smith, Niki Stefanogiannis, Shayma Faircloth, Pippa
Scott
Guests:
Christian Marchello, John Tait, Kris Golding, Rachel Eyre, Tia Narvaez
Apologies:
Caroline McElnay, David Murdoch Ian Frazer
1.0
Welcome and previous minutes
Ian Town welcomed all Members and Attendees in his capacity as Chair of the COVID-19 Vaccine
Technical Advisory Group (CV TAG) Mr John Tait, Chair of the Vaccine ISMB was welcomed.
Minutes of the last meeting (03 August 2021) were accepted.
2.0
Science Updates Updates on the COVID-19 vaccines were highlighted:
•
There are reports that the US intends to grant ful approval of Pfizer in early September.
•
The US Food and Drug Administration have amended their emergency use authorisations
for Pfizer and Moderna to al ow for the use of a third dose in certain immunocompromised
people, specifically, solid organ transplant recipients or those who are diagnosed with
conditions that are considered to have an equivalent level of immunocompromise.
under the Official Info
•
Pfizer have released preliminary data on third doses in adults showing increased
neutralising antibody titres.
•
More data on the safety of vaccination among pregnant women has been released.
3.0
Research in children
Updates on COVID-19 vaccine research among children were highlighted:
Released •CV TAG requested information on whether any post-marketing larger summaries have been
released relating to children. Some initial data from the CDC were shared, and this wil be
included in future updates.
4.0
Vaccine Rollout Update
Document thirteen
The daily vaccine report was presented to CV TAG. The rollout is proceeding at pace and ramping
up to deliver 50,000+ doses per day. Supplies are now steady. The 2020 Health Service Utilisation
is being used as the population denominator in order to monitor vaccination data by ethnicity.
5.0
Dosing Interval for Pfizer
The Chair shared that the extension of the interval between doses was accepted by the Director-
General and announced by the Prime Minister last week and was framed as providing greater
population protection. The changes to the booking website have been implemented and this has
freed up appointments for more first doses around New Zealand.
6.0
S9(2)(f)(iv)
1982
7.0
Decision to Use Pfizer 12- to 15-year-olds
•
CV TAG’s recommendation that vaccination of 12- to 15-year-olds proceeds has been
relayed to the Director-General and Vaccine Ministers.
•
Advice on promoting vaccination in whānau groups has been incorporated.
•
CV TAG requested the benef ts of personal and family protection should be emphasised,
rather than indirect benefits such as population protection.
•
The importance of vaccinating vulnerable groups among 12- to 15-year-olds was raised and
discussed. It was noted that 12- to 15-year-olds considered Group 3 wil be prioritised
through another pathway and given codes to book.
8.0
MMR/Influenza Coadministration A draft memo reviewing evidence on coadministration of the COVID-19 vaccine with other vaccines
(e.g. MMR/Influenza/HPV) was shared with CV TAG for discussion.
•
CV TAG discussed the immunisation programme in the context of concern about RSV
outbreaks and impact on staffing, lagging vaccination rates for MMR and HPV, and
under the Official Info
knowledge of the prior impact of measles outbreaks on Māori and Pasifika.
•
CV TAG encouraged that al intervals between COVID-19 vaccines and other vaccines (with
the exception below) be removed, and same-day coadministration be allowed. Such
intervals were seen as a barrier to uptake of both the COVID-19 vaccine and other
vaccinations.
•
An exception to same-day coadministration should be made for the live-attenuated shingles
vaccine (Zostavax), where a 7-day interval is stil required.
Released •It was noted that younger people produce a good immune response to the COVID-19
vaccine and therefore even if this immune response is reduced by coadministration, it would
stil likely provide excellent protection.
•
The science on coadministration wil continue to be monitored by the Science and Technical
Advisory team.
Document thirteen
•
The advice memo wil be updated to reflect this messaging and shared with CVIP.
9.0
Other COVID-19 Vaccines that New Zealand Could Recognise for Border Workers
•
The Ministry’s Policy team have requested CV TAG’s advice on which other vaccines (in
addition to Pfizer) should be recognised among border workers, and how to approach
incomplete vaccinations among border workers.
•
Medsafe has advised that the Ministry should adopt vaccines provisional y approved or
authorised through emergency use provisions by:
1. Medsafe themselves and
2. Regulators in countries with similar regulatory systems to New Zealand, including
the Australian Therapeutic Goods Administration, the US Food and Drug
1982
Administration, Health Products and Food Branch of Health Canada, United
Kingdom Medicines and Healthcare products Regulatory Agency, and the European
Medicines Agency.
•
The current advice is that if someone is partially vaccinated and only has a single-dose of a
two-dose course regimen from overseas, they should have a dose of Pfizer after at least
four weeks. It was noted that there should be no upper limit on when the second dose can
be administered, and courses did not have to be repeated if there had been a long interval.
They also advised against the use of serology/antibody testing to check protection.
•
CV TAG noted that any guidance to border workers could potentially apply more general y to
all overseas arrivals.
•
Sinopharm and Sinovac vaccines were discussed, with mention of recipients of these
possibly needing a booster dose of Pfizer to provide sufficient protection. However, it was
noted that a complete review of the evidence on protection offered by other vaccines and
incomplete vaccination schedules is needed to inform the discussion.
•
The Science and Technical Advisory team wil conduct a review of the evidence and share
this with CV TAG for discussion at a future meeting.
10.0
Next Steps/Decisions Pending
None.
11.0
Any Other Business
None.
12.0
Agenda items for next meeting
None. under the Official Info
13.0
New Action Items Raised During Meeting
#
Agenda item
Actions
Action Owner
Updates
Compile information on
cardiac-related events
13/07 - Action raised
Myocarditis after
34
associated with other
Secretariat
Pfizer Vaccination
27/07 - Drafted. Awaiting
Released
vaccines in New
peer review
Zealand’s portfolio.
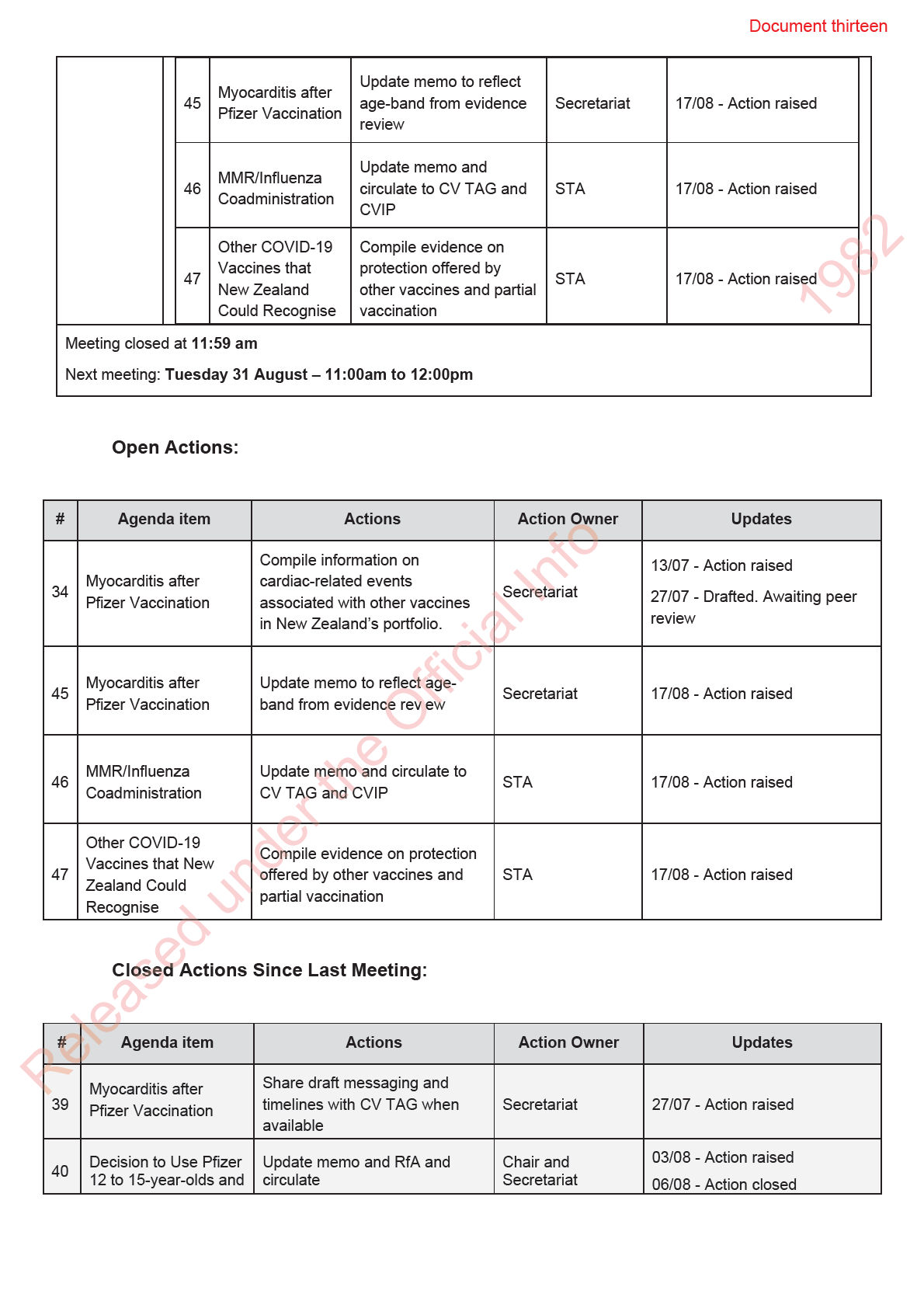
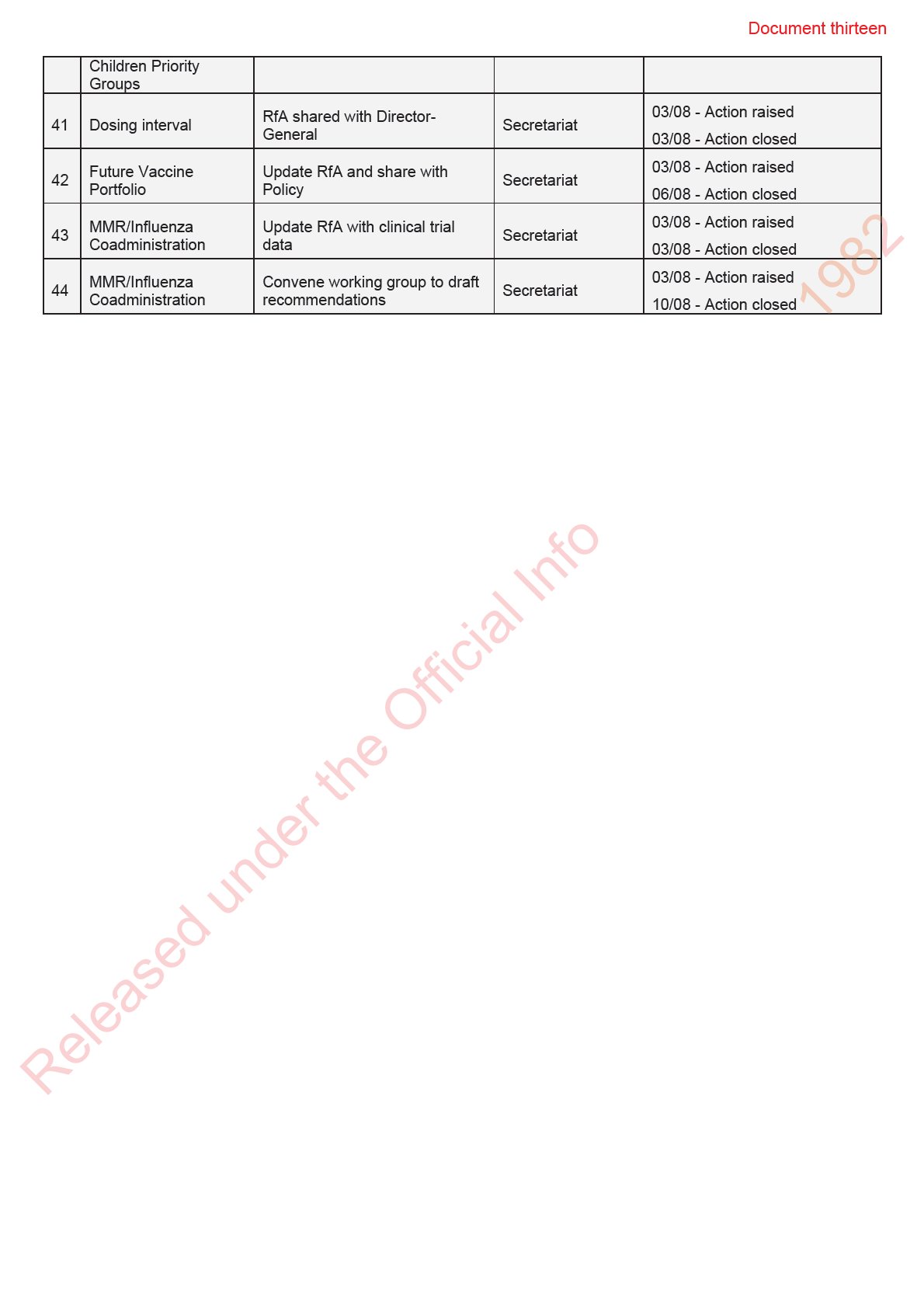

Document fourteen
MINUTES: COVID-19 Vaccine Technical Advisory Group
Date:
Tuesday 31 August 2021
Time:
11:00am to 12:00pm
Location:
Out of Scope
Chair:
Ian Town
Members:
Elizabeth Wilson, James Ussher, Helen Petousis-Harris, Ian Frazer, Nikki
Moreland, Nikki Turner, Peter McIntyre, Sue Crengle, Tony Wal s
Andi Shirtcliffe, Brooke Hollingshead, Daniel Bernal, David Murdoch, Edwin
Ministry of Health Attendees:
Reynolds, Fiona Callaghan, Juliet Rumball-Smith, Niki Stefanogiannis, Pippa
Scott, Shayma Faircloth
Guests:
John Tait, Kris Golding
Apologies:
Caroline McElnay, Sean Hanna
1.0
Welcome and previous minutes
Ian Town welcomed all Members and Attendees in his capacity as Chair of the COVID-19 Vaccine
Technical Advisory Group (CV TAG), including Mr John Tait, Chair of the Vaccine ISMB.
Minutes of the last meeting (17 August 2021) were accepted.
2.0
Vaccine Rollout Update
The daily vaccine report was presented to CV TAG:
•
The rollout is proceeding at pace with high demand for vaccines. Drivers include more primary
care providers d ive-through models, and reduced waiting time post vaccination.
•
Over one mil ion people are now fully vaccinated, and vaccines wil be open to everyone from 1
September.
under the Official Information Act 1982
•
The high demand for vaccines means additional supplies may be needed from mid-September
onwards, and discussions are underway on how to source these.
•
Additional funding is being provided to support Māori and Pacific provider-led vaccination and
wraparound services.
3.0
MMR/Influenza Coadministration
An update on CV TAG’s advice on the coadministration of the COVID-19 vaccine with other vaccines was
given:
Released
•
Finalised CV TAG advice recommending that the interval between administering the COVID-19
vaccines and other vaccines be removed (with the exception of the shingles vaccine Zostavax)
has been shared with CVIP.
•
Advice will be formal y announced a Steering Group.
Document fourteen
4.0
Myocarditis after Pfizer Vaccination
The recent death of a woman with myocarditis post-vaccination was discussed with CV TAG:
•
ISMB determined that vaccination was one of the causal factors.
•
It was noted that this myocarditis following vaccination is extremely rare.
•
The case is under review by a coroner and the case report wil be published providing greater
detail.
5.0
Third Dose
This item was discussed with the agenda item below.
6.0
Pfizer Dosing Error A draft protocol was shared with CV TAG for providing guidance for incidents where a vaccination may
have been missed:
•
The protocol is intended to be generic clinical guidance that can be applied to multiple situation
and wil also inform guidance for the potential missed vaccination incident at Highbrook.
•
It was discussed that smal er incidents should be managed under individualised clinical
management plans, and a broader approach was needed for larger groups, with an al owance for
clinical discretion.
•
For large groups, in general, third doses wil be offered to al of those potentially affected.
•
Serology is of limited use for large groups due to high false negatives. Serology could be
considered with smaller groups and if first dose was missed.
•
Further evidence on the link between dosing intervals and reactogenicity was requested from the
Science and Technical Advisory team.
•
The memo wil be updated and shared with CVIP.
• The group also noted generally that there is good evidence on the safety and immunogenicity
associated with administering third doses to the immunocompromised.
7.0
Other COVID-19 Vaccines that New Zealand Could Recognise for Border Workers Draft recommendations were shared with CV TAG on which vaccines could be recognised for work at the
border:
•
The group noted the need for high degrees of protection for Border Workers to reduce the risk of
onward transmission
under the Official Information Act 1982
•
It was discussed that, in general, New Zealand should recognise vaccines approved by Medsafe
and Medsafe-recognised regulators: TGA, EMA, FDA, MHRA, Health Canada, and EU member
states.
•
One exception to the above is that border workers that have received the single-dose adenovirus
vaccine from Janssen/J&J, and no further COVID-19 vaccination, would require one dose of
Pfizer to increase their level of protection.
•
Under this approach, as of 31 August, the fol owing vaccines would be recognised for border
Released
work: Pfizer, AstraZeneca (approved by Medsafe); Moderna, Covishield (approved by Medsafe-
recognised bodies); and Janssen/J&J plus one dose of Pfizer.
•
Partial and ful vaccination with vaccines not recognised by these authorities should be given a
single booster dose of the Pfizer vaccine.