

Appendix One
1982
Act
MINISTRY OF HEALTH
Information
COVID-19
Health and Disability Sector Official
Resurgence Planning Tool the
under
Version 1.0 11 November 2020
Released
1
Version 1.0 11 November 2020
link to page 3 link to page 3 link to page 4 link to page 5 link to page 6 link to page 7 link to page 9 link to page 11 link to page 12 link to page 12 link to page 12 link to page 13 link to page 13 link to page 13 link to page 13 link to page 15 link to page 16 link to page 18 link to page 30 link to page 41 link to page 42
Appendix One
CONTENTS
Introduction ............................................................................................................................................ 3
Assumptions ....................................................................................................................................... 3
1982
Supporting Material ............................................................................................................................ 4
Te Tiriti o Waitangi ............................................................................................................................. 5
Act
Key Performance Indicators for Achieving Preparedness....................................................................... 6
All of Government and Ministry planning has been informed by common scenarios ........................... 7
Connection between Ministry and the Sector in the event of a Resurgence ......................................... 9
Triggers.................................................................................................................................................. 11
Cross-Cutting Themes ........................................................................................................................... 12
Information
Commitment to Te Tiriti o Waitangi ............................................................................................ 12
Equity ............................................................................................................................................ 12
A scientific evidence base ............................................................................................................ 13
Official
Infection Prevention and Control (IPC) ........................................................................................ 13
Personal Protective Equipment (PPE) .......................................................................................... 13
the
Communications and Engagement .............................................................................................. 13
Resurgence Planning Framework: Prevent, Plan, And Respond ........................................................... 15
under
Strategic Actions: Prevent ................................................................................................................ 16
Strategic Actions: Plan ...................................................................................................................... 18
Strategic Actions: Respond ............................................................................................................... 30
APPENDIX ONE: Scenario-Based Responses per Organisation ............................................................. 41
APPENDIX TWO: Scenarios: Worked Examples .................................................................................... 42
Released
2
Version 1.0 11 November 2020
Appendix One
Introduction
This document has been prepared to assist the Ministry of Health (the Ministry) and district health boards (DHBs) prevent, prepare for and respond to
further community transmission of COVID-19. We know from earlier pandemics, and the current experience of New Zealand and other countries with
1982
COVID-19, that multiple waves of infection can occur. While New Zealand previously achieved and is again on track for elimination, the risk of new cases
potentially seeding further clusters and community transmission remains a very real threat. The Health and Disability Sector Resurgence Planning Tool
provides recommended actions and related information to support preparations for, and effective and timely responses to, the expected community
Act
resurgence of COVID-19. The Planning Tool also provides an outline of how sector organisations engage with the Ministry’s resurgence plan operating
model, in the event of a resurgence or further waves of COVID-19.
It is acknowledged that in many cases, resurgence planning will be well underway, or even complete. Where such plans are already in place, sector
organisations are requested to review them to ensure they are aligned with the relevant content in this document.
Some important points to note:
Information
1. Sector organisations are responsible for their own resurgence planning and this document is designed to support and inform that planning.
2. This document has been developed in conjunction with the COVID-19 National Resurgence Plan, currently being prepared by the COVID-19 All of
Government Response Group in the Department of Prime Minister and Cabinet.
Official
Assumptions
The Ministry’s planning is built on the following assumptions:
the
➢ the Elimination Strategy remains the overarching framework for the health and disability sector
➢ in addition to the community cases detected in Auckland in mid-August 2020, further community cases or clusters of COVID-19 will occur in the
coming months or year - new community cases could be detected at any time and case numbers could rise rapidly
under
➢ the overall size and duration of subsequent waves may well be different from the first wave and the August Auckland community cluster
➢ the severity of the disease and the population groups affected may be similar to the first wave or the August Auckland community cluster, but
ongoing vigilance will be needed to detect and respond to any changes in affected populations and severity
➢ resurgence may occur in conjunction with a concurrent event such as a flood, earthquake or other emergency
➢ all sector organisations will use a CIMS framework in the immediate response to a resurgence
Released
3
Version 1.0 11 November 2020
Appendix One
Supporting Material
This document has been informed by and should be read in conjunction with the following documents, all available on the Ministry’s website. In combination
with this Planning Tool they comprise the framework for health and disability sector preparedness and response to any future community resurgence of COVID-
19:
1982
• Elimination Strategy
Act
• COVID-19 Health and Disability System Response Plan
• Surveillance Plan
• Testing Strategy
• COVID-19 cluster investigation and control guidelines
•
Updated COVID-19 Māori Response Action Plan
Information
• Kia Kaha, Kia Māia, Kia Ora Aotearoa: COVID-19 Psychosocial and Mental Wellbeing Recovery Plan
• Ola Manuia: Pacific Health and Wellbeing Action Plan 2020–2025
• COVID-19 Community Response Framework
•
Official
Getting Through Together: ethical values for a pandemic
• New Zealand Disability Strategy 2016-2026
the
• Mahi Aroha – Carers’ Strategy Action Plan 2019 - 2023
• National Health Emergency Plan: National Reserve Supplies Management and Usage Policies
• New Zealand pandemic response policy for aged residential care 2020 (
planned for publication in November 2020).
under
Released
4
Version 1.0 11 November 2020
Appendix One
Te Tiriti o Waitangi
1982
Te Tiriti o Waitangi principles underpin the Ministry’s resurgence planning. These have been adapted from the recommendations made in the Hauora
Report for Wai 2575, the Health Services and Outcomes Kaupapa Inquiry.
Act
Tino
The guarantee of tino rangatiratanga, which provides for Māori self-determination and mana motuhake in the design, delivery and
Rangatiratanga monitoring of the Covid-19 response to Māori.
Partnership
The principle of partnership, which requires the Crown and Māori to work in partnership in the governance, design, delivery and
monitoring of the Covid-19 response to Māori. Māori must be co-designers, with the Crown, of the Covid-19 response to Māori.
Information
Active
The principle of active protection, which requires the Crown to act, to the fullest extent practicable, to achieve equitable health
protection
outcomes for Māori. This includes ensuring that it, its agents and its Treaty partner are well informed on the extent, and nature of,
both Māori health outcomes and efforts to achieve Māori health equity in the Covid-19 response to Māori.
Options
The principle of options, which requires the Crown to provide for and properly resource kaupapa Māori responses to Covid-19.
Official
Furthermore, the Crown is obliged to ensure that all health and disability services are provided in a culturally appropriate way that
recognises and supports the expression of hauora Māori models of care in the Covid-19 response.
the
Equity
The principle of equity, which requires the Crown to commit to achieving equitable health outcomes for Māori in the Covid-19
response.
under
Released
5
Version 1.0 11 November 2020
Appendix One
Key Performance Indicators for Achieving Preparedness
The following key performance indicators are suggested as a guide for determining preparedness for resurgence activation.
1. Know your organisation’s incident management Operating Model and business continuity plan
1982
2. There is clear accountability, governance and decision-making, including;
a. Relevant Terms of Reference and standard operating procedures in place
Act
b. Financial and operational delegated authorities agreed and ready to go
3. Know how the information flows and how you communicate with stakeholders
4. Identify the right people in the right roles
a. Skill and experience levels are confirmed
b. Training requirements are completed
5. Leadership is aware of and educated on how the model works, and Incident Management Team training is completed (ie, people understand how the
response structure will work and their role within it).
Information
Official
the
under
Released
6
Version 1.0 11 November 2020
Appendix One
All of Government and Ministry planning has been informed by common scenarios
The scenarios below have been created in conjunction with the All of Government (AoG) resurgence planning activity. While the scenarios reflect some of
what the Ministry observed during March to May and subsequently, a scenario-based approach is only illustrative and is not intended to model what any
1982
further outbreaks or waves of infection might look like.
At the most basic level, they are helpful to think about how we would need to prepare and scale up depending on how different types of resurgence might
Act
emerge and play out.
The five scenarios are
not predictions. Rather, they are intended to be used to indicate what actions need to be considered / undertaken, by whom, and
who is accountable for what, in different types of situations.
Scenario 0
• Cases in managed facilities only, no community cases
Information
Elimination achieved, all regions are focused on prevention, preparedness and resurgence planning
elsewhere
Scenario 1
• Up to 10 confirmed cases in a managed facility
Cluster in a managed facility associated with travellers arriving in New Zealand
Official
Scenario 2
• 1 x confirmed cluster (where cluster is 2 or more connected
A case visits a relative in an aged residential care facility and goes on to infect a nurse, a carer and
cases)
the
eight residents. Over two weeks this triggers a single, small, localised cluster of ten cases.
• 1 x 10 cases (over 2 weeks)
• 4 hospitalised, on general ward +
• 1 in ICU
under
Scenario 3
• More than 1 defined cluster, but less than 4
A case goes to a cafe and socialises with a number of people subsequently infecting several
• Crosses more than one PHU area
attendees. Over three weeks this triggers two to three small clusters (including one in residential
• 2-3 x 10-15 cases (20 – 45 cases, over 3 weeks)
disability facility) with up to 45 cases in total across two PHU jurisdictions.
• 2 – 5 hospitalised +
• 1 – 2 in ICU
Released
7
Version 1.0 11 November 2020
Appendix One
Scenario 4
• Confirmed community transmission
Two cases emerge at a similar time, with both attending large events with visitors from across the
• More than 4 and less than 10 confirmed clusters
country (such as a sporting event, a concert or a tangi). Each case infects a large number of people,
• 10 x 20-40+ (200 – 600) cases, over 4 weeks
who subsequently return home across New Zealand. Over four weeks, this triggers outbreaks across
• 40 – 100 hospitalised +
1982
the country, with several locations reporting confirmed community transmission.
• 10 – 25 in ICU
• 3 – 10 deaths
Act
Scenario 5
• More than 10 confirmed clusters
A case goes to a large sporting event and infects a large number of people. The next day attendees
• More than 2 locations with confirmed community
of the sporting event return home across New Zealand. Over eight weeks this triggers more than
transmission
ten confirmed clusters, with several locations reporting confirmed community transmission, with a
• 5,000 cases (over 8 weeks)
particularly large outbreak centred on South Auckland (5,000 cases in total, including 75 deaths).
• 500 hospitalised +
• 150 in ICU
• 75 deaths
Information
Appendix One outlines Scenario-based responses by organisation, including a view of the role of different elements of the sector, including how this
changes as we transition between scenarios and alert levels (noting that any transition between scenarios or alert levels may not be numerically
Official
sequential). These are supported by Appendix Two, which provides worked examples of selected scenarios showing the relationships between the sector
and the Ministry in more detail.
the
under
Released
8
Version 1.0 11 November 2020
Appendix One
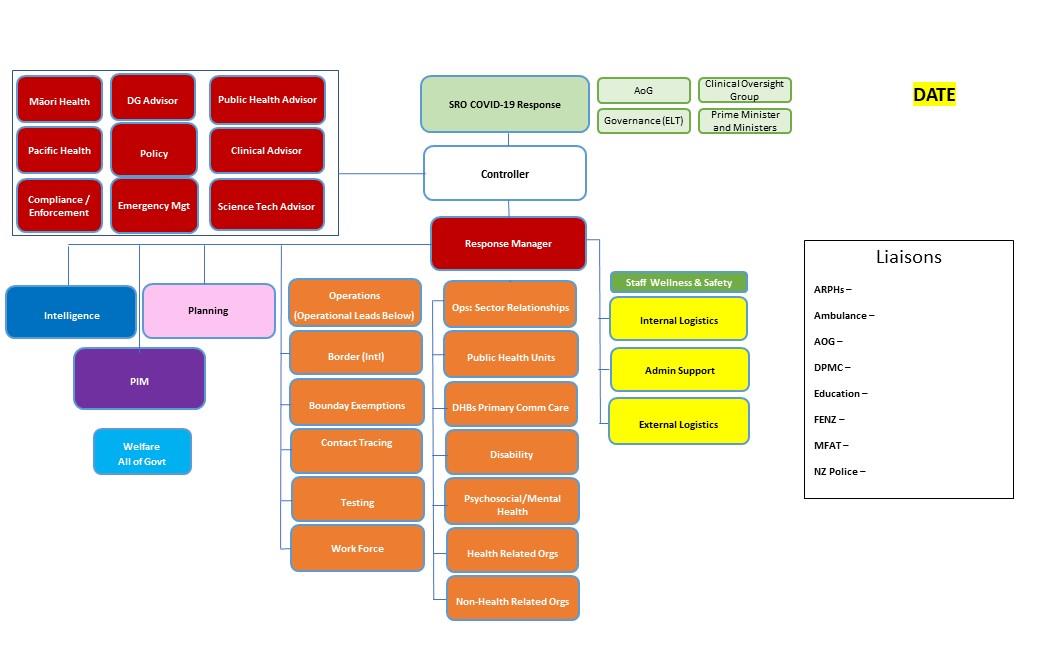
Connection between Ministry and the Sector in the event of a Resurgence
The Ministry of Health’s resurgence operating model for any Incident Management team is CIMS based and updated daily with the individuals assigned to
each function. See template below:
1982
Act
Information
Official
the
under
Released
9
Version 1.0 11 November 2020
Appendix One
The introduction of a new Function, Operations Sector Relationships, has been added specifically to strengthen the relationship and flow of information
between the Ministry and the sector.
1982
The relationship leads have three core objectives:
a. To understand the needs, issues, and concerns of their respective element of the sector and represent that to the Ministry
Act
b. To ensure any advice, guidance or other communication makes its way to the sector in a consistent and timely manner
c. To ensure there is a dedicated and identifiable channel between the Ministry and the sector at all times.
These roles do not replace existing sector bodies, forums or governance groups, but act as a consistent and coordinated conduit to them.
The people filling these roles will have strong sector relationships and networks and may be filled by someone from the sector rather than the Ministry.
Information
Official
the
under
Released
10
Version 1.0 11 November 2020
Appendix One
Triggers
The Ministry continues to monitor and analyse surveillance data from a range of sources in relation to cases, clusters and the potential for, likelihood and
management of, community transmission. The Ministry will inform the health and disability sector and other agencies when agency specific resurgence plans
1982
should be activated or put on stand-by for activation. The sector will generally be informed through a National Health Advisory issued by the Ministry.
There are no pre-determined thresholds or metrics in terms of the types of cases, case numbers or the number or size of community clusters to automatically
Act
trigger activation of resurgence response actions, though activation
could occur as a result of a single, confirmed, community case. Furthermore, other intelligence
may also provide a signal that we have, or may have, undetected community transmission, for example, a person who has travelled from NZ and then tested
positive overseas.
Every signal, case, contact and cluster will be assessed, investigated and managed as appropriate to the circumstances. Strategic response actions, including the
continuation or escalation of the Elimination Strategy, will be calibrated accordingly. Information
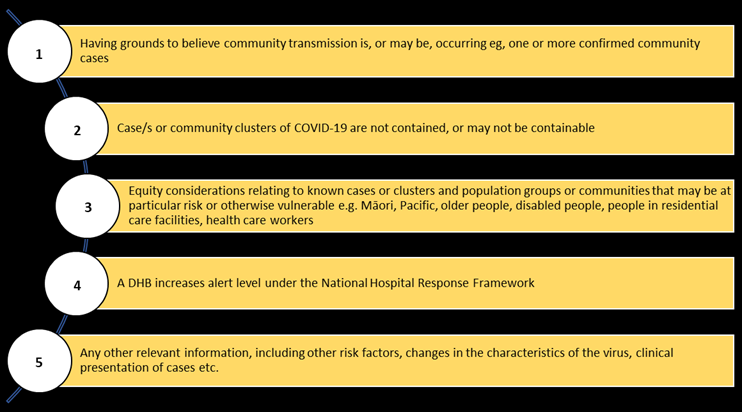
Possible triggers for activating resurgence plans and the
Respond actions of this Planning Tool include:
Official
the
under
Released
11
Version 1.0 11 November 2020
Appendix One
Cross-Cutting Themes
The following themes were identified by the Ministry in its resurgence planning and should be considered when developing operational or organisation-
specific resurgence plans. These themes also reflect lessons identified during the first wave in March and April and the recent August Auckland cluster.
1982
Commitment to Te Tiriti o Waitangi
The health and disability system is committed to fulfilling the special relationship between Māori and the Crown under Te Tiriti o Waitangi (Te Tiriti). The
Act
Ministry, DHBs and PHUs, as stewards of the health and disability system (under Article 1), have the responsibility to enable Māori to exercise authority
over their health and wellbeing (under Article 2) and achieve equitable health outcomes for Māori (under Article 3) in ways that enable Māori to live, thrive
and flourish as Māori.
The principles of Te Tiriti provide the framework for how we will meet our obligations. The Ministry is currently using the principles of Equity, Tino
Rangatiratanga, Options, Partnership and Active Protection, as adapted from the Wai 2575 Stage One Kaupapa Inquiries. These principles are applicable to
the wider health and disability system, including how the health and disability system changes and alter access to services in response to COVID-19.
Information
Equity
Equitable access to health and disability services and health outcomes, including a priority focus on Māori, Pacific, older people, disabled people, people
who experience psychosocial needs, people with existing chronic health conditions, rural communities and other potentially at-risk groups, is central to all
planning and response measures for any significant clusters or further waves. In addition to these priority groups, special consideration must also be given
Official
to health care workers, including those who work in ARC and other residential care settings.
the
COVID-19 creates additional burdens for certain populations who are already significantly affected by adverse social determinants, including Māori, Pacific
and disabled peoples. Beyond controlling COVID-19, it is important to prevent and manage impacts on people, communities and society.
One of the most significant learnings to date has been the need to engage from the outset with at risk populations, particularly Māori, Pacific and older
under
people, and the networks of providers that work most closely with them. Consequently, this plan has been developed in partnership with the Māori, Pacific,
Mental Health and Addictions and Disability directorates and other teams within the Ministry. Many of the strategic actions have been highlighted as
particularly critical to be undertaken with an equity lens, and the Ministry expects that the sector will do so.
While all the actions provided for in this plan should address equity considerations, those items in the tables marked with an asterisk * denote actions
where equity is
especially important. For example, for the Ministry, an asterisk signals the need for early and ongoing engagement with directorates or
Released
12
Version 1.0 11 November 2020
Appendix One
teams that work with and alongside priority groups, including the Māori Health, Disability, and Mental Health and Addictions Directorates, and the Pacific
Health, Health of Older Persons and Long-term Conditions teams.
A scientific evidence base
1982
At every step, actions taken to give effect to the objectives in this Plan should reflect scientific principles and be either based on, or informed by, the best
available evidence. In practice this means referring to and applying knowledge that has been developed through examination of the evidence base and
Act
robust consideration of the suitability for application in the New Zealand context. This includes considering every proposed action in the context of; the
strategic public health approach, the New Zealand health and disability and social system, risk assessment and appetite; and must also be lawful,
proportionate, ethical and consistent with equity considerations.
Care must be taken to ensure that empirical evidence or other relevant information is logical, allows for replicability, distinguishes between correlation and
causation, excludes alternative explanations, and is capable of being falsified through established scientific methods.
Infection Prevention and Control (IPC)
Information
The ongoing maintenance of effective infection prevention and control practices is and will continue to be a priority. This applies to all health care settings,
is relevant to preventing, planning for and responding to any further wave of infections and is essential for the benefit of health care workers, caregivers
and their patients, clients and visitors.
Official
Medical Supplies including Personal Protective Equipment (PPE)
Critical medical supplies and in particular PPE are a vital aspect of the ongoing response to COVID-19. They affect every element of preparedness and
the
response capability. The Ministry continues to purchase, manage, store, distribute and monitor PPE on behalf of DHBs, the health and disability sector,
managed facilities and CBACs. Centralised management aims to ensure equitable access, quality and certainty of supply are maintained and that costs are
met and measured. Given the huge increase in global demand for PPE, PCR testing materials and other supplies, there have been problems in multiple
countries with accessing these goods to meet demand. This is one example of how the international situation will continue to affect New Zealand’s
under
preparedness and response activities and highlights the necessity to consider critical supplies when planning for a further resurgence of COVID-19.
Communications and Engagement
Communicating effectively and engaging with communities have been cornerstones of the response to COVID-19 thus far, and remain crucial to all involved
in preparing for and responding to the pandemic. As a cross-cutting theme, communicating within the Ministry, between stakeholders, to Ministers and to
the general public is critical to a successful response. Some key factors that need to be considered are:
Released
13
Version 1.0 11 November 2020
Appendix One
a. Listening to communities and customising content and delivery of key messages for older people, Māori, Pacific, disabled people, residential care
settings, people who experience psychosocial needs, rural populations and any groups at higher risk of infection or severe outcomes
b. Accessibility: Information about COVID-19 should be accessible for all New Zealanders, and it needs to be translated into alternate formats and key
1982
languages, including Te Reo Māori. For alternate formats: Easy Read, New Zealand Sign Language (NZSL), braille, audio and large print.
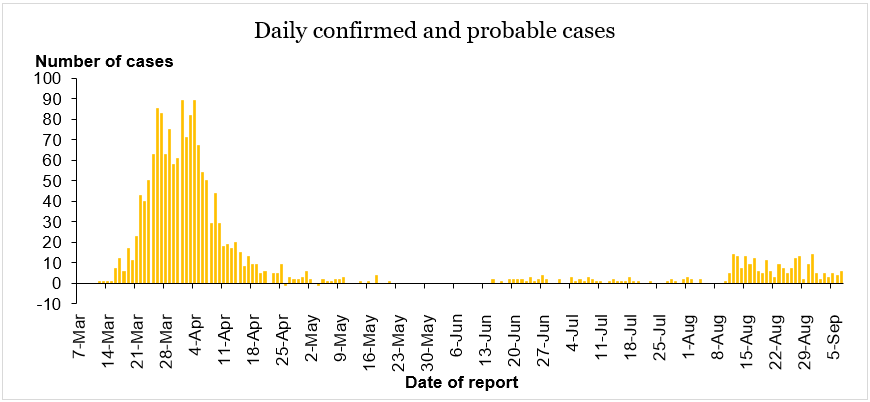
Lessons identified during the first wave (Fig. 1) also highlighted the need for enhanced cross-sector engagement that is proactive, transparent, consistent,
Act
and that transcends organisational boundaries that exist throughout the sector. The Disability Sector Leadership Response Group is a positive example of a
newly established engagement forum that was established to allow for broad sector engagement, and that will continue into business as usual.
Information
Official
the
under
Figure 1. Epidemic curve showing incidence of confirmed and probable COVID-19 cases over time. The first wave of infection (March to April 2020) was
Released
followed by small numbers of cases detected at the border and then the August Auckland community cluster.
14
Version 1.0 11 November 2020
Appendix One
Resurgence Planning Framework: Prevent, Plan, Respond
The Elimination Strategy remains the primary strategic document to guide the response to COVID-19. The Strategy’s four pillars: border control, robust case
detection and surveillance, effective contact tracing and quarantine and strong community support of control measures, should be woven through any
1982
further response from the Ministry and the wider health and disability sector under this Planning Tool.
Within this context the COVID-19 Health and Disability Sector Resurgence Planning Tool is framed around
three strategic objectives:
Act
1. Prevent it
➢ Prevent significant clusters or further waves of COVID-19 infections through the continued implementation of the
Elimination
Strategy, acknowledging that the border is New Zealand’s first line of defence
2. Plan for it
➢ Enhanced domestic surveillance and testing to enable earliest possible detection and monitoring of cases, clusters or community
transmission
➢ Develop scalable Resurgence Action Plans for a significant clusters or further waves of infections
Information
➢ Focus on higher risk groups and priority populations
➢ Ongoing surveillance of the international situation to inform preparedness and minimise disruption to New Zealand health
services
➢ Review and address lessons identified from the first wave and the August Auckland community cluster
Official
3. Respond to it
➢ Immediate escalation of testing coverage, active case finding, contact tracing and isolation / quarantine of cases and contacts
the
➢ Effective / adapted implementation of Ministry, health and disability sector and other agency resurgence action plans
➢ Appropriate clinical management of COVID-19 cases
➢ Maintain essential health and disability services and minimise disruption to business as usual (BaU) services
under
➢ Maintain focus on equity and prioritise services to vulnerable population groups and communities, including Māori, Pacific, older
people, rural communities, disabled people and people who experience psychosocial needs
➢ Response actions to be proportionate, evidence informed and coordinated with all of government response measures.
Response actions are usually followed by
recovery. This will be the case when future clusters are contained and community transmission eliminated.
However, specific recovery guidance is not covered in this document, but may be included in subsequent versions.
Released
15
Version 1.0 11 November 2020
Appendix One
Strategic Action 1:
Prevent
Prevent further waves of COVID-19
1982
Context
1. New Zealand has shown that elimination of COVID-19 can be achieved. This does not mean eradicating the virus permanently from New
Zealand; rather it is being confident we have eliminated chains of transmission in the community for at least 28 days and can effectively
Act
contain any future imported cases from overseas. Even when this Planning Tool is activated for response purposes, the Elimination
Strategy will continue to guide response actions.
Health and disability service providers and the Ministry of Health continue to give effect to the Elimination Strategy to exclude COVID-19, catch it at the
border, contain clusters and prevent further waves of COVID-19. This involves a coordinated and sustained approach to ‘keep it out’, ‘find it’ and ‘stamp it
out’. The four pillars of the Strategy are:
• Border controls: key for stopping the introduction and spread of new cases from overseas
Information
• Robust case detection and surveillance: identify new cases quickly and take appropriate action
• Effective contact tracing and quarantine: an essential part of controlling transmission of the virus
• Strong community support of control measures.
Official
The central preventive measure for eliminating COVID-19 is the first pillar: border controls -
Keep it out. The enhanced public health measures undertaken
at the border, including entry restrictions, managed isolation and quarantine, testing (around days three and twelve) and overall management of the
the
border, are critical to successful to elimination and achieving the objective or preventing further waves.
Keep it out is supported by a
Find it and
Stamp it out approach, using a combination of ongoing disease surveillance; testing and tracing all potential cases,
using enhanced contact tracing; appropriate use of personal protective equipment; rapidly isolating cases and their close contacts; strong community
under
support of control measures, including behaviour change around staying at home with respiratory symptoms, appropriate physical distancing and hygiene
measures, managing the ‘bubble of protection’ for family, whānau, aiga, carers and priority populations including disabled people, using contact tracing
apps; having a sustainable, resilient and agile workforce; and other public health measures as appropriate.
The Elimination Strategy and this COVID-19 Health and Disability Sector Resurgence Planning Tool are complementary. Activities under the Elimination
Strategy will continue to be implemented in the event of a resurgence in COVID-19 leading to the activation of this Plan, and also inform the planning for,
Released
and responses to, significant clusters or further waves of infections in the community.
16
Version 1.0 11 November 2020
Appendix One
Depending on the circumstances, single cases, a small number of linked cases (for example a cluster associated with a traveller arriving from overseas) or a
cluster of unknown origin (for example the August Auckland community cluster) will continue to be managed under the four pillars Elimination Strategy in
the first instance. Elimination activities will also need to continue at scale when Strategic Objective 3 “Respond” of this Resurgence Planning Tool is
activated. See
the Elimination Strategy on the Ministry of Health website for further details.
1982
Act
The following planning and response actions have been developed in order to inform Ministry and sector resurgence plans. Depending on the
circumstances, some will be more relevant or applicable than others.
Information
Official
the
under
Released
17
Version 1.0 11 November 2020
Appendix One
Strategic Action 2:
Plan
The sector needs to continue to prepare for the possibility of significant clusters or further waves of infection. While developing / revising plans to deal with
1982
a resurgence of COVID-19 is critical, associated preparedness activity and the ability to implement the plan, i.e. Respond, are even more so, to help prevent
further outbreaks and to ensure the ability to scale-up a response quickly.
Act
As the World Health Organisation Strategic Framework for Preparedness states, “
When we are prepared, responses are more timely and effective, and we
can limit the human, economic and societal consequences.”
Plans should be prepared for a potential future increase of COVID-19, acknowledging that:
• timing remains uncertain - new community case(s) could be detected at any time and with little or no warning;
•
Information
the overall size, steepness and duration of a subsequent waves may well be different from the first wave and August Auckland cluster;
• the severity of the disease and the population groups affected may be similar to what we have already experienced, but ongoing vigilance will be
needed to detect and respond to any changes in affected / at risk populations and severity.
The first wave of the pandemic in Aotearoa New Zealand lead to a rapid scaling-up of response by the Ministry of Health, the wider health and disability
Official
sector and other government agencies. The key lessons learned during this process should be incorporated into planning that takes place to prepare for a
resurgence in COVID-19.
the
There are a number of reviews that have documented crucial learnings (including in particulat for contact tracing and Aged Residential Care) and each part
of the sector will have critical aspects of the response that have been revised and improved.
under
Released
18
Version 1.0 11 November 2020
Appendix One
Plan for It – subsequent waves of COVID-19
Context
COVID-19 activity in New Zealand has been low since early May 2020, with small numbers of cases being detected and managed at the border from
mid-June. In mid-August 2020, testing detected the first cases of what became the Auckland community cluster. The Ministry activated its
resurgence plan to coordinate the investigation and associated response measures (still ongoing at time of writing).
1982
While mindful of the needs of the wider population, special attention needs to be given to those groups most likely to be susceptible to subsequent
waves of COVID-19. Susceptibility includes both infection and complications, and to disruption of services and supports (e.g. respite and daily cares).
Act
The priority population groups include Māori, Pacific peoples, older people, disabled people, rural communities, people who experience psychosocial
needs, people with existing conditions including immunosuppressive disorders and people in residential care settings. Special consideration must
also be given to health care workers, including those who work in ARC. At present there is no vaccine available for COVID-19 and there is little
evidence of anti-viral treatments being effective for prophylaxis or treatment (although clinical trials are underway). Clinical management will
include supportive treatments, ventilation and treatment of any concurrent bacterial pneumonia.
Planning activity for any increase in case numbers should focus on:
•
Information
ensuring a proportionate, evidence informed and flexible response
• providing a coordinated approach across the health and disability sector and with other sectors
• balancing COVID-19 with other BaU health and disability services
• supporting and maintaining quality health and disability services
Official
• focusing on priority, at-risk populations and improving equity
• communications to engage, empower and build confidence in the wider community.
the
The Ministry of Health and the COVID-19 All of Government Response Group continue to plan for further resurgences of COVID-19 and will
coordinate any response. DHBs are tasked with leading local planning and responses as required. Government agencies are tasked with preparing
responses for the sectors they serve. under
Released
19
Version 1.0 11 November 2020
Appendix One
Key for action tables
1982
Responsibility
For the action tables below, the
Responsibility column indicates the principal stakeholders.
These lists are not exhaustive nor exclusive but provide a guide as to who should lead and be involved. Act
Equity *
An * next to the lead agency is an
equity prompt. Equity should underpin all Ministry of Health work including this Plan. However, the asterisk
denotes actions where equity considerations are
particularly important. For the Ministry this signals the need for engagement with directorates or
teams that work with and alongside priority groups, including the Māori Health, Disability, and Mental Health and Addictions Directorates, and the
Pacific Health, Health of Older Persons, Primary Care, NASO and Long-term Conditions teams.
Information
Planning, co-ordination and reporting
Action
Responsibility
Comments
1. Develop operational resurgence plans to allow for incremental /rapid response escalation:
All agencies*,
All agencies and
Official
including DHBs
a. respond with BaU capacity, prepare for escalation
providers in the
health and
the
b. activate agency surge capacity, prepare for escalation
disability sector
c. activate multi-agency surge capacity, prepare for escalation
must be prepared
d. national / all agency surge capacity
to respond to a
significant cluster
2. Evaluate the effectiveness of the measures used in the first wave and Auckland community cluster and update plans,
under
or further wave of
guidelines, and protocols accordingly
COVID-19
3. Review and where appropriate update business continuity plans and consider critical resource requirements
infections
4. Re-stock, and maintain, essential equipment, including PPE, personal and environmental cleaning products, for all of
the sector, including primary care
5. Promote good hygiene practices, appropriate distancing and sick staff policies
Released
20
Version 1.0 11 November 2020
Appendix One
Planning, co-ordination and reporting
Action
Responsibility
Comments
6. Prepare for a possible escalation in case numbers and severity, including plans for staff absences
1982
7. Ensure that human resources and workforce resilience systems are in place and/or ready to be redeployed
8. Prepare staff resilience, encourage staff leave, medical, dental and wellness appointments, so staff are fit, well, and
Act
rested to respond to further waves. Utilise locums, if necessary, to take leave, and consider mental health needs of
staff, who may be fatigued from first wave.
9. Map key contacts across the sector using organisational charts to enable rapid connections and response, that
a. documents key routes into all priority communities, including ARC, Māori, Pacific and disabled communities
b. identifies a named lead for who would lead resurgence operations
10. DHBs to anticipate how the mental health and wellbeing of communities will or may be affected and develop, review
DHBs
Information
or maintain a psychosocial plan as appropriate
11. Ensure the wider sector has staff with appropriate skills and training ready to be deployed as part of resurgence
Ministry of Health,
operations and/or surge capacity, and there is a policy for redeployment in place.
working with the
sector.
Official
12. Maintain close oversight of legislative instruments and authorisations (e.g. epidemic notice, COVID-19 Public Health
Ministry of Health
Epidemic Notices
Response Act 2020, section 11 orders, waivers/exemptions and any authorisations required for Health Act special
and the C-19PHR
the
powers)
Act require periodic
renewal
13. Ensure an appropriate mechanism is in place to safely and securely share confidential identifiable health information
Ministry of Health
under
14. Ensure a PPE distribution plan is prepared, in accordance with the IPC guidelines, and that includes
Ministry of Health
a. equitable distribution (including who is entitled to receive it from National Supply, and if DHBs will have a
responsibility to distribute);
b. clear points of contact; and
c. purchase and payment mechanisms, if required
Released
21
Version 1.0 11 November 2020
Appendix One
Planning, co-ordination and reporting
Action
Responsibility
Comments
15. Share information with WHO and other international partners e.g. the Communicable Disease Network Australia, and
Ministry of Health
1982
as required under the International Health Regulations 2005
16. Prepare processes and a surge workforce to administer exemptions, if required, for example for individuals wanting to
Ministry of Health
Only relevant if
Act
travel between regions at alert level 1 / 2 and 3 / 4
region(s) are at
levels 3 or 4 and
others at 1 or 2
17. Undertake table top or operational exercises to test resurgence action plans
Ministry of Health-
led, with whole
sector
Information
18. Support the Pandemic Research Programme in conjunction with the Health Research Council
Ministry of Health
19. Coordinate with the National Telehealth Service and Primary Care the response priorities for public advice messaging
Ministry of Health
etc. via digital channels
Official
Intelligence
Action
Responsibility
Comments
the
1. As per COVID-19 Surveillance Plan, enhanced domestic surveillance of:
Ministry of Health
a. cases and clusters notified/managed via EpiSurv and the National Contact Tracing Solution
b. possible community transmission
under
c.
influenza like illness (ILI)
d. community and hospital SARS-CoV-2 viral isolates, including whole genomic sequencing where appropriate
e. serological testing as available
f. influenza vaccine uptake
Released
22
Version 1.0 11 November 2020
Appendix One
Intelligence
Action
Responsibility
Comments
g. National Telehealth Service (NTS) e.g. Healthline phone calls
Ministry of Health
1982
2. Domestic and international surveillance of characteristics of SARS-CoV-2 and COVID-19 (clinical severity, virulence,
Ministry of Health
infectivity, risk groups, genetic changes, clinical management)
Act
3. Monitor and assess information about the effectiveness and other impacts of response interventions, including
Ministry of Health
guidance from international bodies (e.g. WHO) and information from MBIE, MPI, Education etc in order to inform
policy decisions about interventions to be utilised for subsequent responses
4. Further refinement of escalation points with triggers that identify the appropriate response
Ministry of Health
5. Regular reviews of surveillance indicators, the surveillance plan and intelligence reporting as required (e.g., consider
Ministry of Health
Information
‘text mining’)
6. Develop a clear picture of the data that can be accessed, including how and when, and continue strengthening
Ministry of Health
systems for public health data collection (e.g. the quality of ethnicity data) and surveillance
7. Surveillance of international situation to mitigate any impact on supply chain and access to critical clinical supplies
Ministry of Health
Official
8. Enhanced monitoring of health and disability sector capacity during further waves, including primary care capacity and
Ministry of Health
resilience, hospital admissions, ICU occupancy, staff absences, ambulance call outs, Healthline, pharmacies etc., and
the
continue to work with DHBs to optimise data flow into the public health surveillance system
9. Consolidate and review mortality data nationally and review associated processes in liaison with the Chief Coroner’s
Ministry of Health
Office
under
10. Consider modelling likely impact of new cases given experience to date with alert level interventions
Ministry of Health
11. Consider appropriate timing and design of sero-prevalence survey
Ministry of Health,
ESR
12. Continue enhancements of apps (COVID Tracer and Āwhina), including working alongside third-party app providers
Ministry of Health
Released
23
Version 1.0 11 November 2020
Appendix One
Intelligence
Action
Responsibility
Comments
13. Consider reviewing key decisions, protocols and policies to ensure there is an evidence base for public health
Ministry of Health
1982
recommendations
Act
Public health interventions: border
Action
Responsibility
Comments
1. Maintain and review travel restrictions and border controls as mandated under the COVID-19 Public Health Response
Ministry of Health
Act and the Health Act
2. Liaise with agencies coordinating/managing facilities for managed isolation and quarantine for travellers arriving in
Ministry of Health
New Zealand
Information
3. Review and update border management resources
Ministry of Health
4. Provide information to incoming and outgoing travellers on quarantine requirements, relevant symptoms, basic
Ministry of Health
precautions, what to do if travellers become sick, psychosocial resources
Official
5. Work with DHBs to provide consistency for MIQ facilities, including the development of SOPs for standing up a facility,
Ministry of Health,
and establishing communication mechanisms for escalating risks and issues in a timely way
Border agencies
the
6. Be prepared to adjust border controls at short notice
Ministry of Health,
Border agencies
under
7. Review border exemption process for essential health workers
Ministry of Health,
MBIE
Released
24
Version 1.0 11 November 2020
Appendix One
Other public health interventions
Action
Responsibility
Comments
1. Develop and maintain systems to rapidly increase contact tracing capacity if required, including the National
Ministry of Health,
1982
Investigation and Tracing Service
PHUs
2. Continue implementing the National Contact Tracing Solution, including integration of quarantine into the same
Ministry of Health,
Act
platform
PHUs
3. Maintain readiness to implement rapid cluster control measures, particularly in high-risk settings, managed facilities
Ministry of Health,
and communities, including:
PHUs, DHBs
a. identifying key Ministry Cluster Control staff; and
b. ensuring the system machinery is ready to be operationalised immediately, with a ready workforce
4. Plan arrangements for managed isolation and quarantine for community cases (and in some circumstances their
Information Ministry of Health,
household close contacts) who may not be willing or able to self-isolate, including welfare support and psychosocial
DHBs, PHUs
resources
5. Continue seasonal influenza immunisation campaign (March to September annually) and the delivery of the remainder Ministry of Health,
of the National Immunisation Schedule through primary care, with additional communications and logistical support
PHUs, DHBs, PHOs
Official
for any changes in demand, particularly for priority populations including Māori, Pacific, rural communities and
disabled people
the
6. Provide information and resources, including psychosocial resources, to health professionals across all providers and
Ministry of Health,
communities as determined by local needs and planning
PHUs
7. Ensure PHU plans are nationally consistent, so stakeholders are aware of their responsibilities and roles irrespective of
Ministry of Health
under
their location
8. Maintain International Health Regulations core capacity requirements
Ministry of Health,
PHUs
Released
25
Version 1.0 11 November 2020
Appendix One
Health care and emergency response
Action
Responsibility
Comments
1. For consistency of messaging, ensure streamlined communications with one key point of contact, to update NTS-
Ministry of Health,
1982
Healthline, general practice, hospital, ambulance, laboratory staff, aged residential care providers (ARC), Māori and
DHBs, PHUs,
Pacific providers, community pharmacy, lead maternity carers (LMC), family planning and sexual and reproductive
Primary Care,
health services, disability service providers, mental health and addiction providers on current guidance (including on
community care
Act
IPC), policies (including national reserve supplies), and public messages.
and NGO health
and disability
providers
2. Ensure health and disability sector readiness for new cases that may trigger a subsequent wave of infections - address
Ministry of Health,
potential pressure points in resurgence plans covering:
DHBs, PHUs,
primary care
a. Primary care – including coordination with local primary care providers, general practice, pharmacists,
community and
midwives, ambulance etc. regarding IPC protocols, distribution of and access to BAU consumables and
Information NGO health and
national reserve supplies;
disability providers
b. NTS – Healthline aligned and supports frontline service response with clinical advice, health information and
general queries;
c. Capability to establish and then scale up community-based assessment centres (CBACs) and other testing
Official
facilities at short notice;
d. Clear guidance and support for ARC providers, and on DHB obligations and responsibilities for Aged Care;
the
e. Guidance and support to Māori, Pacific, rural communities, mental health, disability, LMC providers;
f. Planning for continuation of care for priority populations, particularly for those with long-term conditions,
e.g. using alternative methods of care provision like mobile outreach teams or mobile medication delivery, or
under
using technology as an enabler;
g. Support for high risk people and communities – including the provision of information on how to access
health services, psychosocial and home support;
Released
26
Version 1.0 11 November 2020
Appendix One
Health care and emergency response
Action
Responsibility
Comments
h. Telehealth services and technology to support relevant aspects of primary care with remote / virtual
1982
solutions, including remote diagnostic capability and specialist care, and staff are trained for technology to be
rapidly deployed when required;
Act
i.
ICUs – including staff training, bed space, ventilators, clinical networks;
j.
Distribution plan for ventilators is completed and implemented, and includes all respiratory equipment and
gases;
k. Laboratory services - including surge capacity for testing (e.g., reagents, testing kits, workforce);
l.
Ensure primary and secondary care has surge capacity, including plans for workforce and improvised health
care facilities, and regularly assess DHB staff capability to ensure skills required are maintained;
Information
m. Capability to care for and support patients at home;
n. Innovative/enhanced arrangements for palliative/hospice care.
3. Resurgence plans to prioritise COVID-19, but also maintain essential health services, and as much BAU health, mental
Ministry of Health,
health and disability services as possible
Primary Care NGOs
Official
4. Collaborate with other DHBs as appropriate to coordinate planning and enhance operational resilience
DHBs
Regional Plans are
the
not required, but
coordination
between DHBs is
5. Maximise resilience of and monitor health sector supply chain.
Ministry of Health,
under
PHARMAC
6. The learnings from the ARC cluster review and DHBs readiness assessments undertaken in alert levels 4 and 3 will be
Ministry of Health,
used in the development of a national outbreak policy for ARC.
ARC, DHBs (PHUs
and health of older
people)
Released
27
Version 1.0 11 November 2020
Appendix One
Communications and community engagement
Action
Responsibility
Comments
1. Prepare, maintain and review Communications Plan, interfacing with the health and disability sector, the public and
Ministry of Health
1982
AoG / DPMC, and maintain communications coordination and consistency of messaging (specific roles, scheduled
sessions with appropriate frequency)
Act
2. Update the public and agencies/providers on the pandemic situation and key messages through regular media reports, Ministry of Health
website, print media, social media, Āwhina app, and other mechanisms as appropriate
3. Activate the Pharmacy services and access to medication communications plan
Ministry of Health
4. Customise delivery of key messages for older people, Māori, Pacific, disabled people, residential care settings,
Ministry of Health,
psychosocial and wellbeing messages for high risk groups and general population, rural populations and any groups at
DHBs, PHUs,
higher risk of infection or severe outcomes
Ministry of Social
Development
Information
5. Information about COVID-19 should be accessible for all New Zealanders, and it needs to be translated into alternate
(alternative
formats and key languages, including Te Reo Māori. For alternate formats (Easy Read, New Zealand Sign Language
formats),
(NZSL), braille, audio and large print):
Department of
a. Write resources in plain English from the outset so that it is easily accessible for the whole audience (and also
Internal Affairs
easier to translate into alternate formats and key languages)
Official
b. Engage with the Ministry of Social Development and Disabled People's Organisations at the beginning of the
the
work to seek advice particularly on how to structure the content so it is accessible
c. Maintain link with the translation team at the Department of Internal Affairs
6. Messaging and communications based on information from ongoing population surveys on knowledge, understanding
Ministry of Health
and practice related to COVID-19
under
7. Coordinate with the National Telehealth Service and Primary Care the response priorities for public advice messaging
Ministry of Health
etc. via digital channels
8. Ensure clear guidance is available on when to use PPE, who should use it, and how to apply it (for both health
Ministry of Health
professionals and the public)
Released
28
Version 1.0 11 November 2020
Appendix One
Communications and community engagement
Action
Responsibility
Comments
9. Disseminate key messages for all sectors, consistent with Ministry of Health plans and communications
All agencies*
1982
10. Regular reviews of communications strategies
All agencies*
Act
Other cross-sectoral actions
Action
Responsibility
Comments
1. All agencies engage with the lead agency (Ministry of Health or AoG), as and when required, through central points of
All agencies
These actions to all
contact, i.e. PIM or COVID Directorate Communications
health sector
agencies and
2. Maintain up-to-date role and contact details of agency staff (including 24/7 and public holiday contacts), and key
Information
agencies in other
contacts in the sector
sectors
3. Keep agency staff and sector updated on the situation and plans
4. Coordinate planning between agencies where required, e.g. emergency management planning collaboration between
Official
ambulance and FENZ
the
under
Released
29
Version 1.0 11 November 2020
Appendix One
Strategic Action 3:
Respond
The following actions have been developed to inform future agency action that is likely to be required when responding to a subsequent waves of infection.
1982
In the event of a resurgence, once the CIMS response model is operational, these actions will inform the iterative Planning and Operations functions of the CIMS model and
will be reviewed, refined and communicated regularly.
Act
Respond to a subsequent wave of COVID-19
Assumptions
➢ new community cases could be detected at any time and case numbers could rise rapidly;
➢ depending on the circumstances, single cases, or even small, contained clusters of linked cases, may continue to be managed under the
Elimination Strategy in the first instance and may or may not trigger full response actions;
➢ the overall size and duration of subsequent waves may well be different from the first wave and the August Auckland cluster;
Information
➢ the severity of the disease and the population groups affected may be similar to the first wave or to the August Auckland cluster, but
ongoing vigilance will be needed to detect and respond to any changes in affected populations and severity.
Key for action tables
Official
This symbol indicates key actions that need to be considered by the agencies as specified.
the
Key decisions and all other actions listed below should be considered in the context of the situation at the time and the possible or likely
evolution of that situation. Such actions may, or may not, be implemented and may be modified as required by the circumstances.
Responsibility
For the strategic action tables below, the
Responsibility column indicates the principal internal (Ministry of Health) and external stakeholders.
under
These lists are not exhaustive nor exclusive but provide a guide as to who should lead and be involved.
Equity *
An * next to the lead directorate or agency is an
equity prompt. Equity should underpin all Ministry of Health work including this Plan. However,
the asterisk denotes actions where equity considerations are
particularly important. For the Ministry of Health this signals the need for
engagement with directorates or teams that work with and alongside priority groups, including the Māori Health, Disability, and Mental Health
and Addictions Directorates, and the Pacific Health, Health of Older Persons, Primary Care, NASO and Long-term Conditions teams.
Released
30
Version 1.0 11 November 2020
Appendix One
Planning, co-ordination and reporting
Action
Responsibility
Comments
1. Alert government agencies to respond or prepare to respond to an increase in cases, clusters and / or community
Ministry of Health
1982
transmission which may lead to a significant cluster or further wave of COVID-19 infections, through agency single
points of contact
This may or may not
be associated with
Act
2. Provide technical advice to inform actions in health and other settings (including Electoral Commission if prior to 17
the use of, or changes
Ministry of Health
October 2020)
to, the COVID-19
Alert Level
3. Maintain or enhance COVID-19 Directorate, consider activating an
Incident Management Team, and / or activate the Ministry of Health
framework.
National Health Coordination Centre (see also 7. Below)
4. Activate COVID-19 resurgence / pandemic action plans, based on Ministry of Health advice
All agencies
Information
5. Lead / coordinate responses for the sectors they serve
All agencies
6. Set response objectives (for example, for a community cluster (a) contain the cluster (b) identify the source).
Ministry of Health
Official
7. Activate emergency management structures (e.g. IMTs, EOCs) and processes, including business continuity plans, as
DHBs, PHUs and other
required
agencies as
appropriate
DHBs and other
the
agencies will decide
whether EOCs need
to be activated in
accordance with local
under
circumstances and
may be directed to do
so by the Ministry
8. Activate the Interagency Pandemic Group, TAG, primary care, Medical Officers of Health/PHU network and ICU
Ministry of Health
Use of e-mail,
advisory groups.
tele/videoconference
s, and face to face
Released
meetings as
31
Version 1.0 11 November 2020
Appendix One
Planning, co-ordination and reporting
Action
Responsibility
Comments
circumstances
require.
1982
9. Engage with Communicable Disease Network Australia and the Australian Health Protection Principal Committee
Ministry of Health
Note other
(particularly if trans-Tasman ‘bubble’ is being planned or in place)
Act
international
‘bubbles’ may also
be planned / in
place
10. Consider activating other pandemic intersectoral work stream groups led by agencies outside the Ministry of Health
Lead agencies for
The lead agency for
each work group
each work group will
provide issue-specific
information for its
Information
members as required
and will decide
whether the work
stream group needs
to be stood up or not.
Official
11. Stand up ambulance liaison officers in NHCC or COVID-19 Directorate / Incident Management Team
Ministry of Health
the
12. Activate processes and workforce, if required, to administer an exemptions regime, for example for individuals
Ministry of Health
wanting to travel between regions at alert level 1 / 2 and 3 / 4
(and/or other agency
as required)
13. If responding using existing agency BAU capacity, prepare to escalate to agency or multi-agency surge capacity
All agencies
under
Released
32
Version 1.0 11 November 2020
Appendix One
Intelligence
Action
Responsibility
Comments
1. As per COVID-19 Surveillance Plan, continue / intensify surveillance as per “plan for it” actions, including monitoring
Ministry of Health,
1982
trends in case and ILI data and reporting to WHO. Review the Plan to ensure it remains fit for purpose
ESR
2. Closely monitor demographic / epidemiological trends in cases and clusters to ensure response measures prioritise
Ministry of Health
Act
affected groups / communities
3. Characterise the event(s), complete ongoing risk assessments, including likely impacts and event evolution
Ministry of Health,
ESR
4. Ensure clear, accurate, and up-to-date intelligence is disseminated across the health system and to DPMC/AoG
Ministry of Health,
ESR
5. Provide regular situation reports and maintain distribution lists
Ministry of Health
Review frequency and
Information
distribution of
situation reports as
required
6. If incidence and / or severity increases, review the need for any additional intelligence and interventions
Ministry of Health
Official
7. Review deaths from COVID-19
Ministry of Health,
Seek to identify
Coroner
changes in pathology,
the
role of co-morbidities
etc.
8. Ensure that equity remains at the centre of policy decisions
Ministry of Health
9. Monitor and report on demand for and capacity of health services including inpatient numbers/capacity, ICU
Ministry of Health, in
under
occupancy, mental health and addiction services, primary care, and ambulance call outs
liaison with DHBs and
PHUs
Released
33
Version 1.0 11 November 2020
Appendix One
Public health interventions
Action
Responsibility
Comments
1. Intensify contact tracing, case finding, case and contact management and cluster control measures
Ministry of Health, in
Local cluster control
1982
2. Activate links with local Māori, Pacific, mental health and disability providers for contact tracing and cluster
liaison with DHBs and
to be PHU-led, with
PHUs
active and close
management
coordination and
Act
3. Review and revise as required information for health professionals on Ministry of Health website
support from the
Ministry. Refer
4. Adopt and adapt further response measures at short notice
COVID-19 Cluster
5. Close coordination between public health unit(s) and Ministry of Health for the management of complex, large or
investigation and
multi-region clusters.
control guidelines.
Medical officer of
6. Review, revise and implement, as required, arrangements for managed isolation and quarantine for persons in-
health powers for
country who may not be willing or able to self-isolate, including welfare support and psychosocial resources
cluster control to be
Information
used in consultation
with the Ministry.
7. Advise NSS, DPMC, Ministers on current and expected future situation, and response measures implemented and
Ministry of Health other
proposed. Note this may or may not include any recommended changes to the current Alert Level (and may also
agencies
Official
include proposed adjustments within the current, or proposed new, Alert Level)
Tailored response
measures may be
implemented locally,
the
regionally or
nationally, and this
may include
differentiated
under
regional Alert Levels
8. Prioritise Māori, Pacific, older people, rural communities and disabled people for services and support
All agencies*
9. Review border controls as required (including any implications for a trans-Tasman and / or Pacific ‘bubble’, if any
Ministry of Health in
such arrangements have been implemented)
liaison with Customs,
MFAT, Ministry of
Tourism etc.
Released
34
Version 1.0 11 November 2020
Appendix One
Public health interventions
Action
Responsibility
Comments
10. Continue seasonal influenza immunisation campaign (March to September annually) and the delivery of the
Ministry of Health,
1982
remainder of the National Immunisation Schedule, with additional communications and logistical support for any
DHBs, PHOs,
changes in demand, particularly for priority populations including Māori, Pacific and disabled people
community pharmacy,
PHUs
Act
11. Continue disease prevention services, e.g., rheumatic fever screening
Ministry of Health,
primary health
organisations, PHUs
Health care and emergency response
Action
Responsibility
Comments
Information
1. Activate resurgence action plans
Ministry of Health,
2.
Consider / implement actions covered in ‘Plan for it’ (see in particular pages 26 to 27)
DHBs, PHOs,
community pharmacies,
Review information
ambulance
for health
professionals on
Official
Ministry of Health
website.
the
3. DHBs to implement appropriate alert level of the Ministry of Health COVID-19 National Hospital Response
DHBs and community
Framework and Community-based providers take appropriate actions under the COVID-19 Community Response
care providers
Framework
under
4. Work alongside primary health services and ambulance to ensure capacity to manage an increase in cases of
Ministry of Health
COVID-19 and those with respiratory symptoms
5. Activate Psychosocial Coordinators, and Pacific and Māori DHB General Managers
DHBs
6. Maximise use of telehealth technology and services (including apps) and Healthline response, and scale up to meet
Ministry of Health other
demand
stakeholders
Released
35
Version 1.0 11 November 2020
Appendix One
Health care and emergency response
Action
Responsibility
Comments
7. Ensure up-to-date guidance is disseminated to the sector and that distribution channels are agreed ahead of time
Ministry of Health
1982
8. Provide guidance on the management / deferral of planned care and elective procedures
Ministry of Health
Act
9. Maintain essential services, and as much BAU health, mental health and disability services as possible
Ministry of Health,
DHBs
10. Prioritise primary care access for vulnerable groups (i.e. Māori, Pacific, older people, those with long-term
Ministry of Health*,
conditions)
DHBs
11. Consider activating improvised health care facilities and surge / re-deployed workforce
Ministry of Health*,
DHBs
Information
12. Consider activating / or coordinate local facilities for managed isolation / quarantine of community cases / contacts DHBs and MBIE
13. Ensure DHBs and other health employers are able to access the surge workforce, including ambulance
Ministry of Health*,
Official
MBIE
14. Provide guidance / advice on clinical placements and minimising health education disruption wherever possible
Ministry of Health*
the
15. Maintain funded temporary accommodation for health workers who cannot return home due to having a
Ministry of Health*,
vulnerable family member in their bubble, or because they are asked to relocate to support the surging of
MBIE
workforce, including for primary care
under
16. Review border exemption process for essential health workers
Ministry of Health*,
MBIE
17. Review, update and disseminate clinical guidance as required, including to health and disability providers, mental
Ministry of Health*
DHBs utilise and
health regulatory services, providers directly contracted by the Ministry, and priority communities
disseminate Ministry
of Health definitions
and guidelines
Released
36
Version 1.0 11 November 2020
Appendix One
Health care and emergency response
Action
Responsibility
Comments
18. Engage with and provide guidance and support to ARC, LMC, general practice, pharmacy and ambulance providers
Ministry of Health* and
1982
DHBs
19. Activate designated testing sites and other testing facilities if required, including liaison and coordination with
Ministry of Health*,
Act
PHOs, Māori and Pacific providers. Note: designated testing sites may need to transition from testing centres to
DHBs
triage role
20. Maximise resilience of, monitor and where necessary, manage the supply chain for health care consumables and
Ministry of Health*,
equipment, particularly critical supplies (essential medicines, devices such as ventilators, testing materials and
DHBs
personal protective equipment)
21. Utilise Healthline to provide information for the public and to assess and triage callers reporting COVID-19
Ministry of Health*,
symptoms
DHBs
Information
22. Promote use of, and use 1737 service for COVID-19 related distress/welfare and psychosocial response
Ministry of Health*
23. Monitor 111 ambulance call volumes, and educate the public to use available websites and Healthline, and only
Ministry of Health*
using 111 for life threatening calls
Official
24. Monitor and report on laboratory, primary care, ambulance including PTS, hospital and intensive care unit
Ministry of Health*,
capability and capacity to Ministry of Health, and take action to anticipate and address bottlenecks
DHBs
the
25. Liaise with ambulance providers to prioritise the use of this service, if required
Ministry of Health*
Only as required by
circumstances
26. Consider surge requirements for PPE. Activate PPE distribution plan, in accordance with the IPC guidelines,
Ministry of Health*
including equitable distribution models (including who is entitled to receive it from National Supply), and purchase
under
and payment mechanisms, if required
27. Activate or intensify actions under specific plans as appropriate eg, psychosocial support, ARC, supply chain, IPC,
DHBs*
regional plans etc
Released
37
Version 1.0 11 November 2020
Appendix One
Communications and community engagement
Action
Responsibility
Comments
1. Update the COVID-19 web page to provide information for the public, health professionals and agencies to guide
Ministry of Health*,
Ongoing
1982
their planning and response
DHBs
2. Release media updates and hold media conferences as required
Act
3. implement and review the Public Information Management Strategy
4. Ensure smooth and timely information sharing with stakeholders, e.g. for change in PPE protocols or case
definitions
5. Work with Māori, Pacific and other health and disability NGO providers to assist them to engage with and support
the communities they serve
6. Continue to disseminate key messages to the public, including:
Ministry of Health*,
All agencies:
Information
a. hygiene and physical distancing
Ministry of Education,
distribute information
MBIE and all other
to their staff, sector
b. known risk factors and symptoms
agencies
and clients through
their normal
c. self-care and caring for others
channels.
Official
d. stay at home if unwell
e. you can still access care from your general practice if you are unwell – it may be a virtual consultation
the
instead of face-to-face targeted wellbeing messaging
f. how to access services and advice for both COVID-19 and non-COVID purposes, noting that service
delivery might be quite different from normal
under
g. call Healthline if concerned
7. Distribute communications material based on the appropriate Alert Level and/or health response, and use
Ministry of Health*
appropriate communications plans, e.g. Pharmacy and Medicines or Primary Care communications plans
Released
38
Version 1.0 11 November 2020
Appendix One
Communications and community engagement
Action
Responsibility
Comments
8. Ensure material is customised, relevant and accessible, and delivery platforms are appropriate to reach older
Ministry of Health*,
Including:
1982
people, Māori, Pacific, disabled people, residential care settings, people who experience psychosocial needs, rural
DHBs, PHUs
- older people
populations and any groups at higher risk of infection or severe outcomes
- people with
Act
9. Information about COVID-19 should be accessible for all New Zealanders, and it needs to be translated into
chronic health
alternate formats and key languages, including Te Reo Māori. For alternate formats (Easy Read, New Zealand Sign
conditions
Language (NZSL), braille, audio and large print):
- Māori, and Pacific
- people who
a. Write resources in plain English from the outset so that it is easily accessible for the whole audience (and
experience
also easier to translate into alternate formats and key languages)
psychosocial need
b. Engage with the Ministry of Social Development and Disabled People's Organisations at the beginning of the
- disabled people
work to seek advice particularly on how to structure the content so it is accessible.
- rural populations
Information
c. Maintain link with the translation team at the Department of Internal Affairs
10. Review / develop and promulgate information targeted to the sectors they serve
All agencies*
11. As required under the International Health Regulations 2005, continue to advise WHO of case numbers and deaths
Ministry of Health
Official
(e.g. via the Ministry website) and any border restrictions implemented that constitute ‘additional measures’
(National IHR Focal
Point)
the
12. Liaise with the Australian Department of Health and Ageing and CDNA
Ministry of Health
13. Communicate as required with foreign governments on the situation overseas and in New Zealand
Ministry of Health,
MFAT
under
14. Advise New Zealanders overseas
MFAT
Safe travel website
Released
39
Version 1.0 11 November 2020
Appendix One
Other cross-sectoral actions
Action
Responsibility
Comments
1. All agencies engage with the lead agency (Ministry of Health or AoG), as and when required, through central points
All agencies
1982
of contact, i.e. PIM or COVID-19 Directorate Communications
2. Ensure agencies can be contacted 24/7 through single points of contact
Act
3. Keep staff and sectors updated
Information
Official
the
under
Released
40
Version 1.0 11 November 2020
Appendix One
APPENDIX ONE: Scenario-Based Responses per Organisation
The following table outlines five scenarios and provides a view of the role of different elements of the sector, including how this changes as we transition between
scenarios (noting that any transition between scenarios or alert levels may not be sequential). These are supported by the detailed worked examples for selected scenarios.
Scenario 1
Scenario 2
Scenario 3
Scenario 4
Scenario 5
(AoG scenario 1)
(AoG scenario 2)
(AoG scenario 3)
(AoG scenario 4)
Cluster in a managed
An imported case visits
A case goes to a cafe and socialises
Two cases occur at a similar time,
A case goes to a major sporting event
facility associated with
an aged residential care
with a number of people subsequently
with both attending large events
and infects a large number of people.
travellers arriving in New
facility and goes on to
infecting several attendees. Over
with visitors from across the country
The next day attendees of the sporting
Zealand
infect a nurse, a carer
three weeks this triggers two to three
(such as a sporting event, a concert
event return home across New
and eight residents. Over
small clusters (including one in
or a tangi). Each case infects many
Zealand. Over eight weeks this triggers
two weeks this triggers a
residential disability facility) with up to
other people, who subsequently
more than ten confirmed clusters, with
single, small, localised
45 cases in total across two PHU
return home across New Zealand.
several locations reporting confirmed
cluster of ten cases.
jurisdictions.
Over four weeks, this triggers
community transmission, with a
outbreaks across the
particularly large outbreak centred on
country, with several locations
South Auckland (5,000 cases in total,
reporting confirmed community
including 75 deaths).
transmission.
High level
All parts of the system
All parts of the system
All parts of the system have roles to
The overall response would be likely
The overall response would be likely to
Responsibility have roles to play but the
have roles to play but
play. While the front-line operational
to be led by AoG/DPMC, with the
be led by AoG/DPMC, with the Ministry
response will be led by the
the immediate response
response will rely on the relevant
Ministry of Health leading the
of Health leading the health sector
local PHU. The Ministry
will be led by the local
PHUs, the overall response would be
health sector response, and
response, and Ministers making the
1982
Resurgence Plan would
PHU. The Ministry
likely to be led by the Ministry of
Ministers making the high-level
high-level decisions about response
not be activated unless
Resurgence Plan would
Health, with AoG and Ministers closely
decisions about response measures.
measures. The Ministry Resurgence
required to mobilise
at least be on standby
monitoring and setting the direction.
The Ministry Resurgence Plan would
Plan would be activated in support of
additional resources.
and may be activated
The Ministry Resurgence Plan would
be activated in support of the
the Elimination Strategy
Act
probably be activated
Elimination Strategy
Sector participants
PHUs
Lead investigation and
Lead investigation and
Lead front-line response measures
Lead front-line response measures
Lead front-line response measures
control measures
control measures
with support and direction from
with support and direction from
with support and direction from
Ministry
Ministry
Ministry
DHBs
Provides hospital care for
Provides hospital care
Provides hospital care for case/s,
Provide hospital care for cases,
Provides hospital care for cases,
case/s if required
for case/s if required
prepares for escalation
activate CBACs and other
activates CBACs and other subsequent
resurgence contingencies, continues
wave contingencies, continues a much
a much BAU services as possible as
BAU services as possible as is
is consistent with COVID demand
consistent with COVID demand
Ministry of
Closely monitors the
Closely monitors the
Leads and coordinates the response
Coordinates with AoG and leads /
Coordinates with AoG and leads /
Health
situation, helps coordinate
situation and prepares
coordinates the health sector
coordinates the health sector response
Information
the PHU response and
for escalation
response
prepares for escalation
Primary Care
BAU
Mainly BAU but assess
Mainly BAU but with contingency
As much BAU as possible within the
As much BAU as possible within the
IPC protocols, PPE
plans either activated or on stand-by
constraints of contingency plans
constraints of contingency plans
supplies and
contingency plans
ARC
BAU
Affected ARC in
Assess and prepare to activate IPC
Activate IPC protocols, PPE supplies
Activate IPC protocols, PPE supplies
isolation, other ARCs
protocols, PPE supplies and
and contingency plans
and contingency plans
Official
assess IPC protocols, PPE
contingency plans
supplies and
contingency plans
AoG
Monitor the situation,
Monitor the situation,
Active monitoring, close coordination
Lead AoG response, working closely
Lead AoG, all of society response,
the
Coordination
coordinate support if
coordinate support,
with Ministry of Health, set general
with Ministry of Health
working closely with Ministry of Health
required (e.g., if foreign
activate, or stand by to
direction, activate or stand by to
nationals are involved)
activate, resurgence
activate resurgence coordination
coordination function
function
What does this mean for:
IPC, including
IPC BAU, PPE provided as
IPC advice scales up, PPE
IPC advice scaled up, PPE provided as
IPC advice scaled up, PPE provided
IPC advice scaled up, PPE provided as
under
PPE and
required.
provided as required.
required, from National Supply.
as required, from National Supply.
required, from National Supply.
ventilators
DHB and primary care
DHB and primary care
DHB and primary care activity:
DHB and primary care activity:
DHB and primary care activity:
activity: BAU. Planning for
activity: BAU. Planning
BAU, considering COVID prioritisation.
COVID prioritisation, BAU continues
Full COVID prioritisation, BAU
ventilator use continues.
and training for
but deprioritised.
continues where possible.
ventilator use continues.
Legal
Primarily managed under
Consider MOoH
Consider MOoH directions/orders if
Consider use of Health Act special
Consider use of Health Act special
the COVID-19 Public
directions/orders if
required for non-compliance by
powers and C-19PHR Act if
powers and C-19PHR Act if necessary
Health Response (Air
required for non-
individual cases/contacts. If more
necessary to support / enforce
to support / enforce control measures
Border) Order 2020, but
compliance by individual
significant powers needed for local
control measures
Health Act powers could
cases/contacts
control e.g. to close a particular
be used for individuals if
premise or cancel a specific event,
Released
required
both Health Act special powers and C-
19PHR Act could be used
Public
Provide updates and
Provide updates and
Provide updates and advice, especially
Provide updates and advice,
Provide updates and advice, especially
messaging
advice, especially to the
advice, especially to the
to affected communities
especially to priority groups
to priority groups
local community
affected community
Māori and
BAU
Engage with / support
Engage with / support communities,
Engage with / support communities,
Engage with / support communities,
Pacific
communities
and receive additional support from
and receive additional support from
and receive additional support from
providers
Ministry, as required
Ministry, as required
Ministry, as required
Healthline
Advised of any change in
Advised of any change in
Advised of any change in messaging or
Advised of any change in messaging
Advised of any change in messaging or
messaging or response
messaging or response,
response, scale up workforce to
or response, scale up workforce to
response, workforce is scaled up and
prepare to scale up
respond
respond
responding
workforce to respond
Ministers /
Immediate and ongoing
Immediate and ongoing
Ongoing updates provided to
Ongoing updates provided to
Ongoing updates provided to Ministers
Cabinet
updates provided to
updates provided to
Ministers, including on potential
Ministers and Cabinet, Ministers
and Cabinet, Ministers and AoG leading
Ministers
Ministers
escalation pathways, and standby
and AoG leading the overall
the overall response
arrangements to scale up response
response
and possible transition to AoG
leadership
41
Version 1.0 11 November 2020
Appendix One
APPENDIX TWO: Scenarios - Selected Worked Examples
SCENARIO 2: LOCAL OUTBREAK, LOCALLY CONTAINED
1982
A case visits a relative in an aged residential care facility and goes on to infect a nurse, a carer and eight residents. Over two weeks this triggers a single, small, localised
cluster of ten cases.
Act
Entity / function
Actions
Comments
Public health unit
• Rapid investigation to identify cases and contacts – isolate/ensure clinical care and quarantine respectively
PHU response using
• Provide advice, agree direction and any additional resources needed with the affected facility, and provide support
existing capacity in
to affected residents, whānau and staff (psychosocial response)
first instance, rapidly
• Update EpiSurv and National Contact Tracing Solution to provide national visibility
scaled up agency
• Ensure affected Māori, Pacific, Mental Health, Disability, Primary and ARC providers are actively engaged in the
surge capacity as
operational response and intelligence
required e.g. for
Information
• Engage with local community e.g. Iwi, schools, retailers, disabled people, community groups
cluster investigation
• Maintain close communication and coordination with the facility, Ministry, DHB, primary care and other providers
and contact tracing
• Medical Officers of Health are prepared to act if required, and the sector understands their legal powers
Primary health
• Vigilance for suspected cases when people visit their GP with flu like symptoms
Work with sector to
Official
care / PHOs
• Coordinate action through PHOs
ensure messaging is
• Activate enhanced IPC and COVID-19 protocols
accurate and timely
• National Telehealth Service is advised of any changes to response required
the
DHB(s)
• Provide additional support to the facility where the outbreak is occurring, including for additional staff or
Clinical care for
facilitating separate staff accommodation if required
patients using agency
• Enhanced community-based testing to detect community transmission (including general practice, designated
BAU capacity and
under
general practice, community based testing centres and where or when necessary local CBAC activation)
agency surge
• Activate enhanced IPC and COVID-19 protocols
capacity for testing
• Evaluate capacity to provide clinical care for inpatients for non-COVID-19 related care
• Increase DHB specific psychosocial supports and messaging for those directly affected, including workforce
• Activate Tumu Whakarae and Pacific GMs
• Link with other sectors, including relevant agencies, e.g. local government, MSD
•
Released
Consider transport needs (and role of ambulance) if patients need moving between facilities
42
Version 1.0 11 November 2020
Appendix One
Entity / function
Actions
Comments
Māori, Pacific, NGO
• If specialised facilities are affected, staff and residents supported in isolation/quarantine
Some situations will
and commercial
• All providers engage with and inform their sectors and communities
require wider
providers including
• All providers maintain vigilance for suspected cases and activate enhanced IPC and COVID-19 protocols
support e.g. if dealing
1982
Iwi, disability,
with an outbreak in
mental health
vulnerable
communities or with
Act
families with
complex and/or
unmet needs
Aged Residential
• Affected facility secured, staff and residents supported in isolation/quarantine
Care
• All providers engage with and inform their sectors and communities
• All providers maintain vigilance for suspected cases and activate enhanced IPC and COVID-19 protocols, including
admission and readmission policies
Information
• Increased targeted psychosocial messaging around increased isolation and the impact of deaths in Aged Residential
Care
Community Care
• Vigilance for suspected cases
Work with NZCOM to
(LMCs, Family
• Activate enhanced IPC and COVID-19 protocols
ensure messaging is
Official
Planning, Carers,
accurate
etc.)
Ministry of Health
• Consider the extent to which the sector response should escalate , including whether to activate the COVID-19
the
Ministry of Health Resurgence Action Plan
• Provide operational support to PHU, DHB and NTS, including NCCS if required
• Closely monitor situation and provide regular updates to the health and disability sector, Ministers, AoG
coordination unit, including advising Ministers and PHUs on the appropriate response, e.g. change in Alert Level, or
under
change in restrictions within Alert Level
• Work with other relevant government agencies to advise on appropriate response measures
• Reporting to WHO, and Australia if trans-Tasman ‘bubble’ implemented
• Sector communications, information coordination, including with stakeholders and NTS
Other sectors
• Limited role, unless required to arrange accommodation, psychosocial and welfare support for people (or their
dependants) in isolation/quarantine
Released
43
Version 1.0 11 November 2020
Appendix One
Entity / function
Actions
Comments
AoG coordination
• Watching brief, support health sector response, prepare to activate or activate if event escalates
unit
Equity actions
• PHUs, DHBs, Ministry and others to prioritise Māori, Pacific, rural, disabled and older people in community-based
Engage with local
1982
testing and other health services
community groups
• Provide accessible information to Māori, Pacific, rural communities, older people, disabled people and people who
and vulnerable
Act
experience psychosocial needs, using appropriate messaging, alternate formats and communication channels
communities early
Public messaging,
• PHU/DHB leads local media engagement, linked with the Ministry
internal
• Ministry leads national media response, coordinates with and supports local PHU media response, updates website,
communications
including messaging for Māori, Pacific, disabled people, people who experience psychosocial needs and other
priority groups
• All key messages and priority information needs to be accessible and produced in alternate formats
• Communications to be focussed through established ARC sector communication channels, DHB GMs planning and
funding, Psychosocial Coordinator, Māori GM (Tumu Whakarae) and Pacific GM
Information
Official
the
under
Released
44
Version 1.0 11 November 2020
Appendix One
SCENARIO 3: LOCAL OUTBREAK, REGIONALLY CONTAINED
A case goes to a cafe and socialises with a number of people subsequently infecting several attendees. Over three weeks this triggers two to three small clusters (including
one in residential disability facility) with up to 45 cases in total across two PHU jurisdictions.
1982
Entity / function
Actions
Comments
Public health unit
• Rapid investigation to identify cases and contacts – isolate/ensure clinical care and quarantine respectively
PHU response using
Act
• Provide advice, and if necessary, direction to the affected facility, and provide support to affected whānau
existing capacity in
(psychosocial response)
first instance, rapidly
• Update EpiSurv and National Contact Tracing Solution to provide national visibility
scaled up agency
• Ensure affected Māori, Pacific, Mental Health, Disability, Primary and ARC providers, and rural communities are
surge capacity as
actively engaged in the operational response and intelligence
required e.g. for
• Engage with local community e.g. Iwi, schools, retailers, disabled people, community groups
cluster investigation
• Maintain close communication and coordination with Ministry, DHB, primary care and other providers on service
and contact tracing
Information
delivery
• Ensure consistent information sharing between PHUs with clusters to allow for coordinated response
• Coordinate with DHBs regarding messaging around continuation of provision of non-COVID-19 related care
• Ensure PPE is distributed equitably and in accordance with IPC guidelines
•
Official
Medical Officers of Health are prepared to act where required, and the sector understands their legal powers
Primary health
• Vigilance for suspected cases when people visit their GP with flu like symptoms
care / PHOs /
• Activate enhanced IPC and COVID-19 protocols
the
Ambulance
• Continuing to provide care for long term conditions
• Primary care links with providers to ensure ongoing care for high complex needs / patients
• National Telehealth Service is advised of any changes to response required
•
under
Consider transport needs (and role of ambulance) if patients need moving between facilities
• Start engaging with DHB and/or Ministry of Health regarding sourcing PPE supplies
DHB(s)
• Provide additional support to the facility where the outbreak is occurring, including for additional staff or facilitating Clinical care for
separate staff accommodation if required
patients using agency
• Enhanced community-based testing to detect community transmission, CBACs and other testing and assessment
BAU capacity and
models are activated or scaled-up where clusters are present
agency surge
• Activate enhanced IPC and COVID-19 protocols
capacity for testing
Released
45
Version 1.0 11 November 2020
Appendix One
Entity / function
Actions
Comments
• Evaluate capacity to provide clinical care for inpatients, and non-urgent outpatients for non-COVID-19 related care
(and role of PTS or ambulance in moving patients between facilities)
• Coordinate messaging around continuation of provision of non-COVID-19 related care
1982
• Increase DHB specific psychosocial supports and messaging for those directly affected, including workforce, and
activate DHB coordinator information sharing (cross-DHB)
•
Act
Activate Tumu Whakarae and Pacific GMs
• Link with other sectors, including relevant agencies, e.g. local government, MSD
• Link with other DHBs where clusters are present
• SitReps are activated
• Ensure PPE is distributed equitably and in accordance with IPC guidelines
Māori, Pacific,
• If specialised facilities are affected, staff and residents supported in isolation/quarantine
Some situations will
NGO and
• All providers engage with and inform their sectors and communities
require wider
commercial
•
Information
All providers maintain vigilance for suspected cases and activate enhanced IPC and COVID-19 protocols
support e.g. if
providers including
• Start engaging with DHB and/or Ministry of Health regarding sourcing PPE supplies
dealing with an
Iwi, disability,
• Indicate needs for funding for future service provision if the scenarios deteriorate
outbreak in
mental health
vulnerable
communities or
Official
with families with
complex and/or
unmet needs
the
Aged Residential
• Affected facility secured, staff and residents supported in isolation/quarantine
Care
• All providers engage with and inform their sectors and communities
• All providers maintain vigilance for suspected cases and activate enhanced IPC and COVID-19 protocols, including
under
admission and readmission policies
• Increased targeted psychosocial messaging around social isolation and the impact of deaths in Aged Residential
Care, including to both residents and the workforce
• Start engaging with DHB and/or Ministry of Health regarding sourcing PPE supplies
Community Care
• Vigilance for suspected cases
Work with NZCOM to
(LMCs, Family
• Activate enhanced IPC and COVID-19 protocols
ensure messaging is
• Start engaging with DHB and/or Ministry of Health regarding sourcing PPE supplies
accurate
Released
46
Version 1.0 11 November 2020
Appendix One
Entity / function
Actions
Comments
Planning, Carers,
etc.)
Ministry of Health
• Consider the extent to which the sector response should escalate, including whether to activate the COVID-19
1982
Ministry of Health Resurgence Action Plan
• Provide operational support to PHU, DHB and NTS, including NCCS if required
•
Act
Closely monitor situation and provide regular updates to the health and disability sector, Ministers, AoG
coordination unit, including advising Ministers and PHUs on the appropriate response, e.g. change in Alert Level, or
change in restrictions within Alert Level
• Work with other relevant government agencies to advise on appropriate response measures
• Reporting to WHO, and Australia if trans-Tasman ‘bubble’ implemented
• Sector communications, information coordination, including with stakeholders and NTS
• Link DHBs with clusters for information sharing and coordinated response
• Coordinate messaging around continuation of provision of non-COVID-19 related care
Information
• Ensure consistent and equitable distribution of PPE in accordance with IPC guidelines
• Ministry will provide clear guidelines for SitRep provision, and how information is shared with the sector
Other sectors
• More active role depending on location and type of cluster. Other agencies will need to be involved, e.g. MSD,
MBIE, Whānau Ora commissioning agencies
Official
AoG coordination
• Watching brief, support health sector response, prepare to activate or activate if event escalates
the
unit
• Anticipate future funding should the situation escalate
Equity actions
• PHUs, PHOs, DHBs, Ministry and others to prioritise Māori, Pacific, disabled, rural and older people in community-
Engage with local
based testing and other health services
community groups
• Provide accessible information to Māori, Pacific, disabled people, older people, rural communities and people who
and vulnerable
under
experience psychosocial needs, using appropriate messaging, alternate formats and communication channels
communities early
Public messaging,
• PHU/DHB leads local media engagement, linked with the Ministry
internal
• Ministry leads national media response, coordinates with and supports local PHU media response, updates website,
communications
including messaging for Māori, Pacific, disabled people, people who experience psychosocial needs and other
priority groups
• All key messages and priority information needs to be accessible and produced in alternate formats
Released
47
Version 1.0 11 November 2020
Appendix One
Entity / function
Actions
Comments
• Communications to be focussed through established ARC sector communication channels, DHB GMs planning and
funding, Psychosocial Coordinator, Māori GM (Tumu Whakarae) and Pacific GM
1982
SCENARIO 4: LOCAL OUTBREAK, NATIONAL SPREAD (WITH COMMUNITY TRANSMISSION)
Two cases emerge at a similar time, with both attending large events with visitors from across the country (such as a sporting event, a concert or a tangi). Each case infects
Act
a large number of people, who subsequently return home across New Zealand. Over four weeks, this triggers outbreaks across the country, with several locations reporting
confirmed community transmission.
Entity / function
Actions
Comments
Public health unit
• Rapid investigation to identify cases and contacts – isolate/ensure clinical care and quarantine respectively
PHU response using
• Provide advice, and if necessary, direction to the affected facility, and provide support to affected whānau
existing capacity in
(psychosocial response)
first instance, rapidly
Information
• Update EpiSurv and National Contact Tracing Solution to provide national visibility
scaled up agency
• Ensure Māori, Pacific, Mental Health, Disability and ARC providers are actively engaged in the operational response surge capacity as
• Engage with local community e.g. Iwi, schools, retailers, disabled people, community groups
required e.g. for
• Maintain close communication and coordination with Ministry, DHB, primary care and other providers
cluster investigation
Official
• Ensure consistent information sharing between PHUs with clusters to allow for coordinated response
and contact tracing
• Coordinate with DHBs regarding messaging around continuation of provision of non-COVID-19 related care
• Ensure PPE is distributed equitably and in accordance with IPC guidelines
the
• Medical Officers of Health act where required, and the sector understands their legal powers
Primary health
• Vigilance for suspected cases when people visit their GP with flu like symptoms
care / PHOs /
• Activate enhanced IPC and COVID-19 protocols
under
Ambulance
• Ensure continued care for long term conditions especially vulnerable populations
• Link with Māori, Pacific, ARC, disability and mental health providers to ensure ongoing care for high complex needs
/ patients and to ensure continued viability of BAU services during changing alert levels
• National Telehealth Service is advised of any changes to response required
• Consider transport needs (and role of ambulance) if patients need moving between facilities
DHB(s)
• If there is a cluster in a facility, provide additional support, including for additional staff or facilitating separate staff
Clinical care for
Released
accommodation if required
patients using agency
48
Version 1.0 11 November 2020
Appendix One
Entity / function
Actions
Comments
• Enhanced community-based testing to detect community transmission, CBACs are activated or scaled-up where
BAU capacity and
clusters are present
agency surge
• Activate enhanced IPC and COVID-19 protocols
capacity for testing
1982
• Evaluate capacity to provide clinical care for inpatients for non-COVID-19 related care, (and role of PTS or
ambulance in moving patients between facilities)
•
Act
Coordinate messaging around continuation of provision of non-COVID-19 related care
• Activate DHB specific psychosocial coordinator, and activate DHB coordinator information sharing (cross-DHB)
• Activate Tumu Whakarae and Pacific GMs
• Link with other sectors, including relevant agencies, e.g. local government, MSD
• Coordinate with other DHBs where clusters are present
• SitReps are activated
• Ensure PPE is distributed equitably and in accordance with IPC guidelines
•
Information
Ask relevant networks with prehospital destination pathways to plan how they will respond. e.g. trauma pathways
Māori, Pacific,
• If specialised facilities are affected, staff and residents supported in isolation/quarantine
Some situations will
NGO and
• All providers engage with and inform their sectors and communities
require wider
commercial
• All providers maintain vigilance for suspected cases and activate enhanced IPC and COVID-19 protocols
support e.g. if
providers including
• Start engaging with DHB and/or Ministry of Health regarding sourcing PPE supplies (NB. PPE distributed by DHBs
dealing with an
Official
Iwi, disability,
will be for publicly funded essential services, not commercial providers)
outbreak in
mental health
• Increasing the psychosocial messaging, gaining continued funding to provide support.
vulnerable
the
communities or
with families with
complex and/or
unmet needs
under
Aged Residential
• Affected facility secured, staff and residents supported in isolation/quarantine
Care
• All providers engage with and inform their sectors and communities
• All providers maintain vigilance for suspected cases and activate enhanced IPC and COVID-19 protocols, including
admission and readmission policies
• Increased targeted psychosocial messaging around increased isolation and the impact of deaths in Aged Residential
Care, and seeking continued funding to provide support
Released
49
Version 1.0 11 November 2020
Appendix One
Entity / function
Actions
Comments
Community Care
• Vigilance for suspected cases
Work with NZCOM to
(LMCs, Family
• Activate enhanced IPC and COVID-19 protocols
ensure messaging is
Planning, Carers,
• Ensure adequate PPE is supplied
accurate
1982
etc.)
Ministry of Health
• Activate the COVID-19 Ministry of Health Resurgence Action Plan
•
Act
Provide operational support to PHU, DHB and NTS, including NCCS if required
• Closely monitor situation and provide regular updates and advice to the health and disability sector, other agencies,
Ministers, DPMC AoG coordination unit, including advising Ministers and PHUs on the appropriate response, e.g.
change in Alert Level, or change in restrictions within Alert Level
• Work with other relevant government agencies to advise on appropriate response measures
• Reporting to WHO, and Australia if trans-Tasman ‘bubble’ implemented
• Sector communications, information coordination, including with stakeholders and NTS
• Link DHBs with clusters together for information sharing and coordinated response
Information
• Coordinate guidance regarding continuation of non-COVID-19 related care
• Ensure consistent and equitable distribution of PPE in accordance with IPC guidelines
• Ministry will provide clear guidelines for SitRep provision to ensure consistency of information, and how
information is disseminated to the sector
Official
• Set up and activate sector advisory networks to ensure top-down, bottom-up information flow
• Update psychosocial planning for restricted movement / isolation
•
the
Understand the funding requirements for providers, e.g. seeking new funding, reprioritisation of existing funds
Other sectors
• More active role depending on location and type of clusters. Other agencies will need to be involved e.g. MSD,
MBIE, Whānau Ora commissioning agencies
under
AoG coordination
• Activated
unit
• Release of new funding to provide further support / resource
• Psychosocial considerations are integrated across the AoG Responses
Equity actions
• PHUs, PHOs, DHBs, Ministry and others to prioritise Māori, Pacific, rural, disabled people, older people and people
Engage with local
who experience psychosocial needs in community-based testing and other health services
community groups
• Provide accessible information to Māori, Pacific, disabled people, rural communities, older people and people who
and vulnerable
Released
experience psychosocial needs, using appropriate messaging, alternate formats and communication channels
communities early
50
Version 1.0 11 November 2020
Appendix One
Entity / function
Actions
Comments
Public messaging,
• PHU/DHB leads local media engagement, linked with the Ministry
internal
• Ministry leads national media response, coordinates with and supports local PHU/DHB media response, updates
communications
website, including messaging for Māori, Pacific, disabled people, people who experience psychosocial needs and
1982
other priority groups
• All key messages and priority information needs to be accessible and produced in alternate formats
•
Act
Communications to be focussed through established ARC sector communication channels, DHB GMs planning and
funding, Psychosocial Coordinator, Māori GM (Tumu Whakarae) and Pacific GM
Information
Official
the
under
Released
51
Version 1.0 11 November 2020
Appendix One
SCENARIO 5: NATIONAL OUTBREAK WITH COMMUNITY TRANSMISSION
A case goes to a large sporting event and infects a large number of people. The next day attendees of the sporting event return home across New Zealand. Over eight
weeks this triggers more than ten confirmed clusters, with several locations reporting confirmed community transmission, with a particularly large outbreak centred on
1982
South Auckland (5,000 cases in total, including 75 deaths).
Entity / function
Actions
Comments
Act
Public health unit
• Rapid investigation to identify cases and contacts –
PHU response using
isolate/ensure clinical care and quarantine respectively
scaled up agency
• Update EpiSurv and National Contact Tracing Solution to provide national visibility
surge capacity as
• Ensure Māori, Pacific, Mental Health, Disabled and ARC providers are actively engaged in the operational response
required e.g. for
• Work in direct partnership with above providers to provide advice, and direction to the affected communities, and
cluster investigation
provide support to affected whānau (psychosocial response)
and contact tracing
• Engage with local community e.g. Iwi, schools, retailers, disabled people, community groups
Information
• Maintain close communication and coordination with Ministry, DHB, primary care and other providers
• Ensure consistent information sharing between PHUs with clusters to allow for coordinated response
• Coordinate with DHBs regarding messaging around continuation of provision of non-COVID-19 related care
• Ensure PPE is distributed equitably and in accordance with IPC guidelines
• Medical Officers of Health act where required, and the sector understands their legal powers
Official
Primary health
• Vigilance for suspected cases when people visit their GP with flu like symptoms
care / PHOs /
• Activate and maintain enhanced IPC and COVID-19 protocols
the
Ambulance
• Ensure continued care for long term conditions especially for vulnerable populations
• Link with Māori, Pacific, ARC, disability and mental health providers, and rural communities, to ensure ongoing care
for high complex needs / patients and to ensure continued viability of BAU services during changing alert levels
• National Telehealth Service is advised of any changes to response required
under
• Consider transport needs (and role of ambulance) if patients need moving between facilities
• Consider ambulance availability to respond to life threatening calls
DHB(s)
• If there is a cluster in a facility, provide additional support, including for additional staff or facilitating separate staff
Clinical care for
accommodation if required
patients using agency
• Enhanced community-based testing to detect community transmission, CBACs are activated or scaled-up where
BAU capacity and
clusters are present
Released
52
Version 1.0 11 November 2020
Appendix One
Entity / function
Actions
Comments
• Activate enhanced IPC and COVID-19 protocols, and psychosocial coordinators, and Māori and Pacific GMs
agency surge
• Provide clinical care for inpatients for non-COVID-19 related care, and coordinate messaging for this service
capacity for testing
provision (and consider how patients may be moved around the country if required, ambulance/PTS may become
1982
overstretched)
• Activate DHB specific psychosocial coordinator, and activate DHB coordinator information sharing (cross-DHB)
•
Act
Activate Tumu Whakarae and Pacific GMs
• Link with other sectors, including relevant agencies, e.g. local government, MSD
• Coordinate with other DHBs where clusters are present
• SitReps are activated
• Support distribution of PPE to essential health services, in accordance with national guidelines
• Surge workforce is accessed through partnership between DHBs, and access is prioritised for vulnerable populations
and workforces
• Activate improvised care facilities, particularly in South Auckland Information
• Ministry of Health monitors and manages ongoing distribution of PPE to all who require
• Arrange accommodation for health workers using MBIE temporary accommodation service
• Ask relevant networks with prehospital destination pathways to plan how they will respond. e.g. trauma pathways
Māori, Pacific,
• Affected facility secured, staff and residents supported in isolation/quarantine
Some situations will
Official
NGO and
• All providers engage with and inform their sectors and communities
require wider
commercial
• All providers maintain vigilance for suspected cases and activate enhanced IPC and COVID-19 protocols
support e.g. if
the
providers including
• Monitor expenditure and link with Ministry of Health
dealing with an
Iwi, disability,
• Increased targeted psychosocial messaging around increased isolation, and seeking continued funding to provide
outbreak in
mental health
support
vulnerable
communities or
under
with families with
complex and/or
unmet needs
Aged Residential
• Affected facility secured, staff and residents supported in isolation/quarantine
Care
• All providers engage with and inform their sectors and communities
• All providers maintain vigilance for suspected cases and activate enhanced IPC and COVID-19 protocols, including
admission and readmission policies
Released
53
Version 1.0 11 November 2020
Appendix One
Entity / function
Actions
Comments
• Increased targeted psychosocial messaging around increased isolation, especial around visiting for vulnerable
communities (in plain English, multiple languages, and in the right places/channels for accessibility)
• Widespread support for the sector on the impact of deaths in Aged Residential Care
1982
Community Care
• Vigilance for suspected cases
Work with NZCOM to
(LMCs, Family
• Activate enhanced IPC and COVID-19 protocols
ensure messaging is
Act
Planning, Carers,
• Ensure adequate PPE is supplied
accurate
etc.)
Ministry of Health
• Activate Resurgence Action Plan
• Provide operational support to PHU and DHB, including NCCS
• AoG has overall responsibility for response
• Work with other relevant government agencies to advise on appropriate response measures
• Closely monitor situation and provide regular updates to the health and disability sector, Ministers, AoG
coordination unit, including advising Ministers and PHUs on the appropriate response, e.g. change in Alert Level, or
Information
change in restrictions within Alert Level
• Reporting to WHO, and Australia if trans-Tasman ‘bubble’ implemented
• Sector communications, information coordination, including with stakeholders and NTS
• Clarify how DHBs can access support for workforce Official
• Link DHBs with clusters together for information sharing and coordinated response
• Coordinate guidance regarding continuation of non-COVID-19 related care
•
the
Monitor and managed ongoing distribution of PPE to all who require and ensure consistent and equitable
distribution in accordance with IPC guidelines
• Ministry will provide clear guidelines for SitRep provision to ensure consistency of information, and how
information is disseminated to the sector
under
• Set up and activate sector advisory networks to ensure top-down, bottom-up information flow
• Update psychosocial planning for restricted movement / isolation
• Understand the funding requirements for providers, e.g. seeking new funding, reprioritisation of existing funds,
Emergency Funding Frameworks
Other sectors
• Arrange accommodation, psychosocial and welfare support for people (or their dependants)
• Mobilise resurgence plans,
•
Released
Coordinate own sectors
54
Version 1.0 11 November 2020
Appendix One
Entity / function
Actions
Comments
• Ensure that in this context, holistic care is provided that addresses the broader determinants of health (socio-
economic support, food deliveries, education support etc.)
AoG coordination
• Activated
1982
unit
• Release of new funding to provide further support / resource
• Ensure that in this context, holistic care is provided that addresses the broader determinants of health (socio-
Act
economic support, food deliveries, education support etc.)
Equity actions
• PHUs, PHOs, DHBs, Ministry and others to prioritise Māori, Pacific, rural, disabled people, older people and people
Engage with local
who experience psychosocial needs in community-based testing and other health services
community groups
• Provide accessible information to Māori, Pacific, disabled people and older people using appropriate messaging,
and vulnerable
alternate formats and communication channels
communities early
Public messaging,
• PHU/DHB leads local media engagement, linked with the Ministry
internal
• Ministry leads national media response, coordinates with and supports local PHU media response, updates website,
communications
including messaging for Māori, Pacific, disabled people, people who experience psychosocial needs and other
Information
priority groups
• All key messages and priority information needs to be accessible and produced in alternate formats
• Communications to be focussed through established ARC sector communication channels, DHB GMs planning and
funding, Psychosocial Coordinator, Māori GM (Tumu Whakarae) and Pacific GM
Official
the
under
Released
55
Version 1.0 11 November 2020