HAWKES BAY DISTRICT HEALTH BOARD
Manual:
Operational Policy Manual
Doc No:
HBDHB/OPM/002
Date Issued:
May 2002
Date Reviewed: April 2019
Approved:
Executive Director – People &
Event Management Policy
Quality
Signature:
Kate Coley
Page:
1 of 9
PURPOSE
The purpose of the event management system at Hawkes Bay DHB is to:
1. Identify, report and analyse all events1 that cause harm or have to the potential to cause
harm to staff, patients and anyone else affected by the HBDHB’s activities.
2. Set out the system for the DHB to, review and improve the systems that assure clinical safety
and personnel health and safety to reduce risk for staff, patients and others.
3. To contribute to improved quality, safety, experience and efficiency of health and disability
services through:
early identification, reporting and review of events
sharing lessons learned through the review process so preventable events are not
repeated
transparency, open communication and accountability.
4. Provide information to inform organisational improvement activities.
PRINCIPLES
The fundamental role of the event management system is to enhance consumer and staff safety
by learning from events and near misses that occur in Hawke’s Bay District Health Board
(HBDHB). The following principles underpin this policy:
1. The National Adverse Events Reporting Policy for New Zealand Health and Disability
Services (Health Quality and Safety Commission, 2017) is the foundation for this policy.
2. Open communication is essential to the event reporting and review process. Consumers,
their families/whanau and staff are legally and ethically entitled to transparent, truthful and
open communication at all times following an event and throughout any subsequent review.
3. Affected people are encouraged and supported to participate in the review process. Where
appropriate the health consumer, families/whanau and staff involved in the adverse event
will be offered the opportunity to share their story as part of the review process. Review
findings and recommendations will be shared with people involved in the review.
4. Reviews of events will result in actions to improve the quality and safety of health care.
Health consumers, families/whanau and staff will be assured that when events and near
misses occur, action is taken. Action focuses on learning, improving safety, reliability and
reducing the possibility of recurrence.
5. Analysis of trends informs continuous learning and system changes. Reporting is only of
value if it is accompanied by meaningful analysis which leads to recommendations for
1 The term event is used throughout this policy to mean a near miss/good catch or actual incident which has the
potential to cause harm, or has caused harm to a patient, staff member, contractor or visitor to Hawkes Bay DHB.
This is a Controlled Document. The electronic version of this document is the most up-to-date and in the
case of conflict the electronic version prevails over any printed version. This document is for internal use
only and may not be relied upon by third parties for any purpose whatsoever.
© 2019 Hawke’s Bay District Health Board
Event Management Policy
Page 2 of 9
April 2019
Doc No HBDHB/OPM/002
system changes designed to prevent recurrence of events. Lessons learned must be
disseminated.
6. Event reporting is encouraged through a no blame culture. Consumers and staff must be
encouraged to report events in the interests of improvement and without fear of retribution.
Events that are reported will be investigated with a focus on determining the underlying
system failures and not attributing blame to individuals. Leaders must ensure a fair and just
culture prevails so individuals are not held accountable or punished for system failures.
7. Event review practice will emphasise culturally safe participants. The cultural viewpoint and
practices of a consumer and their whanau or staff members are considered when they are
involved in the event review process.
8. Events that involve a criminal act, or substance abuse by any individual(s) employed by
HBDHB, a deliberate unsafe act, or a deliberate consumer harm will be managed in a
separate process and will involve the relevant regulatory authorities.
9. RADAR (electronic risk reporting system) will be readily accessible to all staff.
SCOPE
This policy applies to all HBDHB staff, including honorary or unpaid employees, temporary
employees, students, volunteers, contractors and any other persons working for, or providing
services to Hawkes Bay DHB.
Exclusions
This policy does not apply in the following cases:
1. Complaints; made by persons receiving care and treatment from HBDHB are covered by the
Consumer Feedback Policy – HBDHB/OPM/001.
2. Employment relationship issues and events affecting any employee in health and disability
service settings in New Zealand. These are managed under the Employment Relations Act
2000 (and regulations) that aim to build productive employment relationships through the
promotion of good faith in all aspects of the employment environment and the employment
relationship.
3. Intentional harm. In any of the following situations the event must be reported through the
events system, however it will be investigated differently.
A criminal act
A deliberately unsafe act
Substance abuse by any individual(s) employed by HBDHB
Deliberate patient harm or abuse
4.
Whenever it is discovered any event has any element of intentionality it will be reviewed
through one or a combination of the following systems:
Event system = just culture i.e. focuses on systems, process issues but has zero
tolerance for reckless behaviour.
Conflict resolution = debriefing, meetings and/or arrangements/agreements made
between parties in conflict
Performance management
Disciplinary action - refer to Disciplinary Policy
This is a Controlled Document. The electronic version of this document is the most up-to-date and in the
case of conflict the electronic version prevails over any printed version. This document is for internal use
only and may not be relied upon by third parties for any purpose whatsoever.
© 2019 Hawke’s Bay District Health Board
Event Management Policy
Page 3 of 9
April 2019
Doc No HBDHB/OPM/002
EVENT REPORTING AND MANAGEMENT
HBDHB will design and review the policy and system for reporting and reviewing events to comply
with guidelines set out by the New Zealand Health Quality and Safety Commission.
The procedure for reporting and reviewing events at HBDHB is set out in the accompanying
Event Management Guideline – OPM123.
All events including near misses must be submitted into RADAR (electronic risk management
system) within 24 hours of the event.
The employee who first becomes aware of the event; or the employee most involved in the event;
or the employee to whom the event is reported is responsible for completing and submitting the
event form
Any reported near miss or event resulting in harm to a patient must be documented in the
patient’s health record with a reference to the original event notification form number and any
actions taken.
Any staff member involved in an event will be supported to access assistance as required through
the DHB Human Resources team, Occupational Health team and/or their professional or
industrial body.
If an event is regarded as “notifiable” to Worksafe NZ, the Health and Safety Advisor (or delegate)
must be advised immediately. Worksafe website:
https://worksafe.govt.nz/ The Directorate leadership team with overall responsibility for an event is identified by where the
event occurred and can be further quantified by where the improvement work needs to occur.
For example if a patient goes to radiology from a surgical ward and falls while in Radiology, the
review and communication of the event is the responsibility of the Radiology Department and not
Surgical Services.
The Directorate leadership team is responsible for disclosing information and communicating
with consumers, their whanau and/or representative and staff.
The Directorate leadership team is responsible for finalising the review prior to CREAG and for
the action of recommendations following review.
Al events on the Health Quality and Safety Commission ‘Always Report and Review2’ list will be
reported and reviewed.
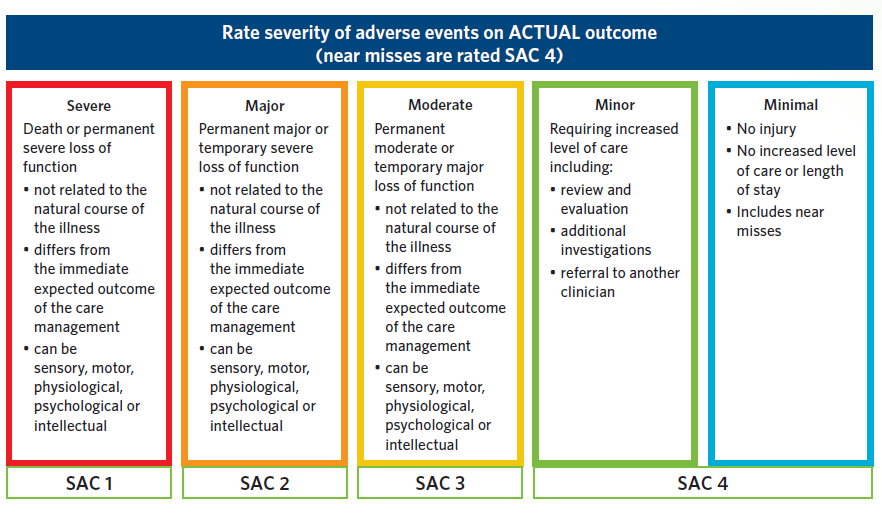
The Severity Assessment Code (SAC) table is used to determine the severity of any event.
Severity is based on
actual outcome
(see Appendix 1). Severity Assessment Code (SAC) 1 and 2 events (Adverse Events)
Note: see Appendix 1 for event severity definitions.
A formal review will be undertaken of all SAC1 and SAC2 adverse events (AE), including mental
health events, and any events on the Always Report and Review list using a recognised event
review methodology (e.g. London protocol or Root Cause analysis etc).
Recommendations or actions generated through the review of any AE are designed to eliminate,
control, or accept the root causes/causal factors identified for the adverse event.
2 HQSC Always Report and Review This is a Controlled Document. The electronic version of this document is the most up-to-date and in the
case of conflict the electronic version prevails over any printed version. This document is for internal use
only and may not be relied upon by third parties for any purpose whatsoever.
© 2019 Hawke’s Bay District Health Board
Event Management Policy
Page 4 of 9
April 2019
Doc No HBDHB/OPM/002
Monitoring to evaluate the impact of recommended actions on care, services and outcomes will
be undertaken at 6 and 12 months after the completion of the action.
SAC 1 and SAC 2 events (collectively referred to as adverse events (AE)) will be reported to the
Heath Quality and Safety Commission (HQSC) within 15 working days from the date the adverse
event is reported.
A summary of the findings and recommendations from any AE, using the Adverse Event Brief
Part B template, is sent to the Health Quality and Safety Commission within 70 working days
from the date the adverse event is reported. This summary must include an outline of the actions
agreed by the Clinical Risk Event Advisory Group, the plan for implementation of the actions or
the reasons for not implementing the recommendations.
The Patient Safety and Clinical Compliance Service will ensure reporting to HQSC is completed.
SAC 3 and 4 Events
Note: see Appendix 1 for event severity definitions.
The area manager or delegate is responsible for reviewing all SAC3 and 4 events and providing
a robust report, including recommendations for system improvements.
When no recommendations are generated through the review, the review report must note the
fact.
Reviews of SAC3 and 4 events and good catch/near misses must be undertaken and closed
within 30 working days.
The area manager or their delegate is responsible for monitoring corrective actions generated
through the review of SAC 3 and 4 events and maintaining an audit register.
The area manager or their delegate is responsible for analysing trends and for reporting identified
system problems through organisational escalation pathways.
OPEN COMMUNICATION IN AN EVENT REVIEW The directorate leadership team is responsible for disclosing information and communicating with
consumers, their whanau and/or representative and staff in line with the Open Communication
Policy OPM/111.
ACCOUNTABILITY in and EVENT INVESTIGATION - a Fair and Just Culture
HBDHB aims to maintain a fair and just organisational culture where people trust they will be
treated with respect.
Maintaining and promoting a fair and just culture relies on:
acceptance that management systems can be improved;
recognition that people can and do make mistakes;
understanding that people/groups at all levels may develop unhealthy /unsafe patterns of
behaviour; and
knowledge that reckless conduct will not be tolerated.
This is a Controlled Document. The electronic version of this document is the most up-to-date and in the
case of conflict the electronic version prevails over any printed version. This document is for internal use
only and may not be relied upon by third parties for any purpose whatsoever.
© 2019 Hawke’s Bay District Health Board
Event Management Policy
Page 5 of 9
April 2019
Doc No HBDHB/OPM/002
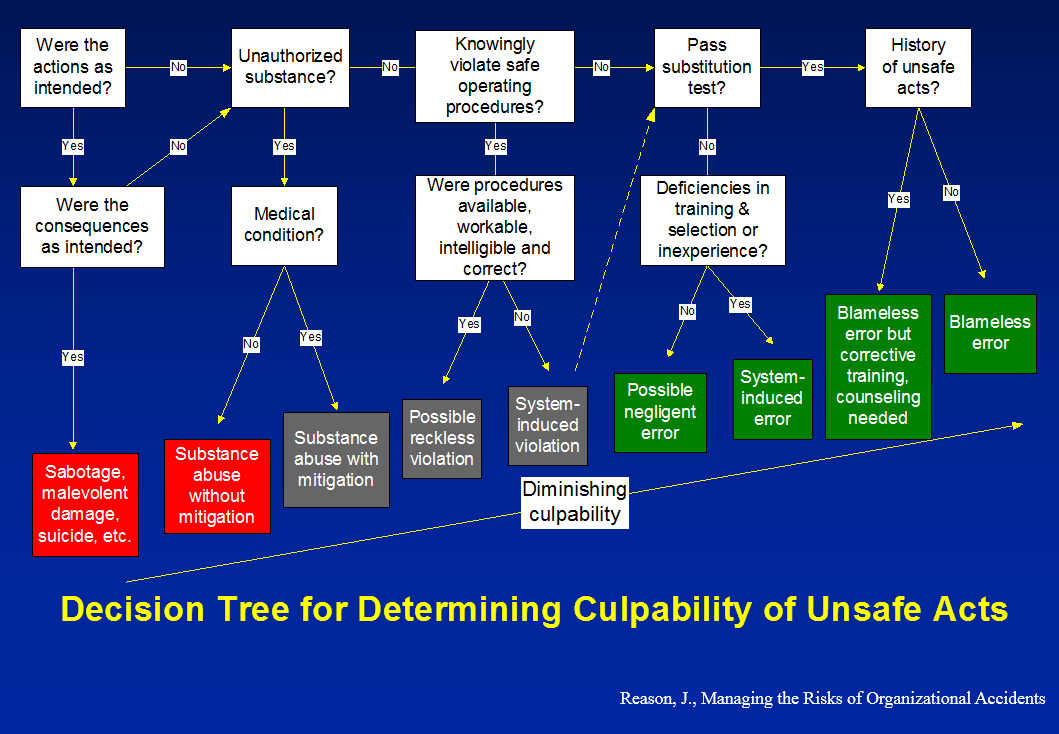
Hawke’s Bay DHB supports the use of James Reason’s
Decision Tree for Determining Culpability
of Unsafe Acts including the
Substitution Test (but not limited to) to determine whether actions
were reasonable and appropriate and if behaviour is risky, reckless or unintentional
(see
Appendix 2).
FEEDBACK IN AN EVENT REVIEW
1. Any person who submits an event form and any staff involved in an event must be given
feedback by their manager (or delegate), describing investigation findings, outcomes and
recommendations unless they have specified “no feedback required”.
2. RADAR allows the submitter of an event to log into that event and check the progress via the
File Submission Tracker page.
3. Lessons learned from event review will be shared with staff through quality reports,
department meetings, internal committees and staff newsletters etc.
DOCUMENTATION IN AN EVENT REVIEW
Storage and retention of information related to events
The original event form, all related documentation and correspondence must be filed securely in
the event management system and associated systems for a minimum of 15 years.
Copies of event forms involving employees will be kept
indefinitely by the OH&S Team for ACC
purposes and in compliance with the Health and Safety at Work Act 2015.
Each event notification form will be sequentially numbered to enable easy access, tracking and
identification.
System Assurance
Documentation of any event review may be audited.
Periodic audits by the system administrators will evaluate compliance with event management
policies and procedures. The event management contingency plan will be activated in the event
of failure of the event management system.
All documentation, including the event form, investigation, identified causal / contributing factors,
recommendations, action plans and evaluation of implemented changes
must be saved in a way
that enables ready access for audit.
Protection of Information Where a patient or external agency requests information related to an event, the request must
be forwarded to the HBDHB Privacy Officer/s who will determine the appropriate person or
department to respond to the request.
Information gained from the event notification is confidential to HBDHB except where disclosure
is required by law, e.g. notification of accidents to WorkSafe New Zealand, NZ Police, HBDHB's
risk insurer or under the Privacy Act 1993, Health Information Privacy Code 1994 or Official
Information Act 1992 (subject to withholding grounds).
This is a Controlled Document. The electronic version of this document is the most up-to-date and in the
case of conflict the electronic version prevails over any printed version. This document is for internal use
only and may not be relied upon by third parties for any purpose whatsoever.
© 2019 Hawke’s Bay District Health Board


Event Management Policy
Page 6 of 9
April 2019
Doc No HBDHB/OPM/002
MEASUREMENT CRITERIA
Directorate Leadership Teams are responsible for monitoring
all event recommendations,
actions, trends, evaluating changes and disseminating lessons learned to staff.
All adverse events, recommendations and trends are monitored and analysed by HBDHB Clinical
Governance Committees. The Clinical Governance Committees include but are not limited to
Clinical Risk & Event Advisory Group, Pharmacy and Therapeutic Advisory Group, Patient Safety
and Risk Management Committee.
ASSOCIATED DOCUMENTS
Clinical Risk and Event Advisory Group Terms of Reference
Critical Incident Stress Management Defusing Debriefing Policy - EPM/031
Consumer Feedback Policy – OPM/001
Disciplinary Policy - PPM/012
Event Management Guideline – OPM/123
Event Management Process Flowchart (Appendix 1) – OPM123
Event Reporting and Consumer Feedback Training Guides
Open Communication Policy – OPM/111
Health and Disability Code of Rights
Health and Safety Policy – OPM/019
Health and Safety at Work Act 2015 and associated regulations
Health & Safety Standard 4801
ISO 31000
National Adverse Events Reporting Policy (2017) and associated documents
https://www.hqsc.govt.nz/our-programmes/adverse-events/
New Zealand Standard 8134:2008 Health and Disability Services (General) Standard
Retention Schedule - General Disposal Authority for District Health Boards
REFERENCES
Health Quality and Safety Commission (HQSC).
Health and Disability Services' National
Reportable Events Policy. Wellington; 2017
Frankel A, Haraden C, Federico F, Lenoci-Edwards J.
A framework for Safe, Reliable, and
Effective Care. White Paper. Cambridge, MA: Institute for Healthcare Improvement and Safe &
Reliable Healthcare; 2017.
Reason J.
Managing the Risk of Organizational Accidents. Aldershot, Hants, England: Ashgate
1997
Vincent C, Patient Safety. Second Edition. Wiley-Blackwell. BMJIBooks. 2010
DEFINITIONS
Adverse Event An event with negative or unfavourable reactions or results that are unintended, unexpected or
unplanned13 (also referred to as ‘incident’ or ‘reportable event’). In practice this is most often
understood as an event which results in harm or has the potential to result in harm to a consumer.
This is a Controlled Document. The electronic version of this document is the most up-to-date and in the
case of conflict the electronic version prevails over any printed version. This document is for internal use
only and may not be relied upon by third parties for any purpose whatsoever.
© 2019 Hawke’s Bay District Health Board
Event Management Policy
Page 7 of 9
April 2019
Doc No HBDHB/OPM/002
Consumer For the purposes of this Policy a consumer can also be a client, patient or resident. It is the
person who uses/receives health and disability services, or their representative.
Near Miss
This is an event which, under different circumstances, could have caused harm to a consumer
but did not, and which is indistinguishable from an adverse event in all but outcome.
Open Communication
Open communication or open disclosure, refers to the timely and transparent approach to
communicating with, engaging with and supporting consumers and their whānau when adverse
events occur.
RADAR (Report, Analyse, Determine, Act, Resolve)
The electronic risk management system where events, complaints, complements and
organisational risk is reported, managed and monitored.
Review
A review is another name for a formal process that is carried out by the health or disability service
provider to analyse an adverse event or near miss and develop recommendations based on the
findings. There are a variety of review methodologies.17 Reviews can be undertaken at different
levels, depending on the adverse event (e.g. comprehensive, concise, desk-review or single
aggregated review of similar events).
Severity Assessment Code (SAC) The SAC is a numerical rating which defines the severity of an adverse event and as a
consequence the required level of reporting and review to be undertaken for the event.18
Whānau The family or extended family/group of people who are important to the consumer.
KEY WORDS
Adverse
Event
Incident
SAC
Notifiable
RADAR
For further information please contact the Patient Safety Advisor.
This is a Controlled Document. The electronic version of this document is the most up-to-date and in the
case of conflict the electronic version prevails over any printed version. This document is for internal use
only and may not be relied upon by third parties for any purpose whatsoever.
© 2019 Hawke’s Bay District Health Board
Event Management Policy
Page 8 of 9
April 2019
Doc No HBDHB/OPM/002
Appendix 1
Severity Assessment Code (SAC) Rating Tool*
*Extract from National Adverse Events Reporting Policy (2017).
This is a Controlled Document. The electronic version of this document is the most up-to-date and in the case of conflict the electronic version prevails over any
printed version. This document is for internal use only and may not be relied upon by third parties for any purpose whatsoever.
© 2019 Hawke’s Bay District Health Board
Event Management Policy
Page 9 of 9
April 2019
Doc No HBDHB/OPM/002
Appendix 2
James Reason’s Decision Tree for determining culpability of
unsafe acts including the Substitution Test
This is a Controlled Document. The electronic version of this document is the most up-to-date and in the case of conflict the electronic version prevails over any
printed version. This document is for internal use only and may not be relied upon by third parties for any purpose whatsoever.
© 2019 Hawke’s Bay District Health Board