Regulatory Impact Statement
Reducing Road Trauma: Random Drug Testing for Drivers
Agency Disclosure Statement
1.
The Ministry of Transport (the Ministry) has prepared this Regulatory Impact Statement
(RIS). It follows a recent review of New Zealand’s drug-driving enforcement regime and
analyses options that might offer improved road safety through changes to the
enforcement regime.
2.
The review provided an opportunity to examine how to reduce the harm resulting from
drug-driving in New Zealand at a reasonable cost, through changes to the enforcement
regime.
3.
The origin of the review is the Safer Journeys Action Plan 2013-15, which includes an
action for investigating opportunities to strengthen the existing drug-driving enforcement
t 1982
model in New Zealand.
Limitations of the review
4.
Data on the issue of drug-driving in New Zealand is limited, as no study clearly shows
the extent of drug-driving in New Zealand. Instead, the Ministry estimated the size of
New Zealand’s drug-driving problem using an independently peer reviewed cost-benefit
analysis. This analysis took into account several data sources, such as international
research, and crash data. These sources included data from New Zealand’s crash
analysis system (CAS)1, data from an Environmental Science and Research (ESR) study
of drivers who died in road crashes in New Zealand2 and data from the United Kingdom.
These data sources were used, respectively, to provide low, central and high estimates
of the social cost of New Zealand’s drug-driving problem.
5.
Where possible, the Ministry has sought to estimate the impact of the proposed changes
on offenders and the Justice sector, including the NZ Police, the courts and the prison
under the
system. The Ministry’s data on the costs of different options came from several sources
including the NZ Police, the New Zealand Transport Agency (NZTA), the Department of
Corrections and the Ministry of Justice. The Ministry’s cost-benefit analysis was
dependent on this data.
6.
The cost-benefit analysis report can be found on the Ministry’s website:
http://www.transport.govt.nz/Drug-Driving-CBA.The report canvasses in detail the
methodology employed to estimate the size of the drug-driving problem in New Zealand,
and determine the costs and benefits of various enforcement options. The key findings in
that analysis are summarised in this RIS.
Out of scope of the review
7.
The review did not look directly at drug-driving penalties, as this was addressed as part
of the drink-driving sanctions review. However, the penalty regime is an intrinsic
component of some options, as the nature of those options raise issues about whether
criminal penalties can be justified given the nature of the evidence able to be collected.
Released
Official Information Ac
1 In New Zealand all traffic crashes data reported by police are recorded in CAS.
2 In New Zealand, all toxicological analyses are carried out by one laboratory, ESR, in Wellington.
When a driver is killed in a crash, a blood sample may be sent for analysis.
1
8.
New Zealand’s approach to drug-driving has so far been to reduce the harm resulting
from impaired driving at a reasonable cost, rather than to design regimes as a drug
control strategy designed to punish drivers for using illicit substances.
Withheld under section 9(2)(a)
Adviser
Ministry of Transport
March 2016
under the
Released
Official Information Act 1982
2
Status Quo
New Zealand’s current drug-driving regime
9.
New Zealand’s current drug-driving regime was introduced in 2009. The approach to
drug-driving enforcement is based on both proving a person is impaired and cannot drive
safely, and has drugs present in their blood.
10.
The current drug-driving enforcement regime identifies drug impairment using a
behavioural test. This helps to improve road safety, ensuring impaired drivers are taken
off the road and prosecuted. However, this is only the case if Police are able to identify
impaired drivers and establish good cause to suspect they have used a drug. Good
cause to suspect can be established by a Police officer through a driver’s personal
demeanour, or if they witness behaviours such as erratic driving or swerving across
lanes. This approach is set out in the Land Transport Act 1998.
11.
A Police officer must have good cause to suspect a driver has used a drug or drugs
t 1982
before that driver can be tested. Good cause may be formed based on a driver’s manner
of driving or demeanour when they are stopped and spoken to by Police.
12.
If a Police officer can determine good cause, a driver can be required to undergo a
behavioural test called a Compulsory Impairment Test (CIT). The CIT is designed to
determine whether a driver’s capacity to drive a motor vehicle is impaired. A trained
Police officer carries out the test, which comprises eye, walk and turn, and one-leg-stand
assessments. For safety reasons CITs cannot be done by the roadside, so drivers are
usually brought back to a Police station to be tested for impairment.
13.
The CIT is useful because there is a less predictable relationship between the amount of
drugs in a driver’s body and the effect on their driving ability. These relationships are
much better understood for alcohol. There is also a wide range of drugs that are used
that can act on different neural pathways in the central nervous system and are
metabolised in different ways and over different lengths of time. Further, the wide range
of potentially impairing drugs, including many prescription drugs, means that screening
under the
technology can only test for a limited range of drugs. The CIT is also able to address
when drivers have used multiple drugs at once.
14.
However, the CIT can be quite demanding on Police resources and on drivers, taking on
average around 52 minutes to complete including transportation time. Police officers also
need special training to be able to conduct the test. Stakeholders have expressed
concern about the subjective nature of the CIT; however, a high proportion (90 percent)
of blood samples taken after a CIT has not been completed satisfactorily test positive for
the presence of a qualifying drug or drugs. From November 2009 to December 2013,
1004 blood tests were taken, of which 903 tested positive for qualifying drugs.
15.
The NZ Police advise that each year around 200 blood samples are analysed following
drivers completing a CIT unsatisfactorily. While the Police do not have data on how
many drivers satisfactorily complete CITs, or how many CITs are conducted overall, the
number of drivers is likely to be low given the high threshold required for determining
good cause to suspect.
Released
16.
As there are limits to the number of tests that can be practically carried out, New
Zealand’s regime is successful in prosecuting and removing visibly impaired drivers from
the roads, but does not provide the conditions for general deterrence.
Official Information Ac
3
17.
If a driver’s performance on this test is unsatisfactory, a Police officer can require the
driver to undergo a blood test for a qualifying drug. These are drugs categorised under
Schedule 1, 2, and parts of Schedule 3 of the Misuse of Drugs Act 1975, as well as
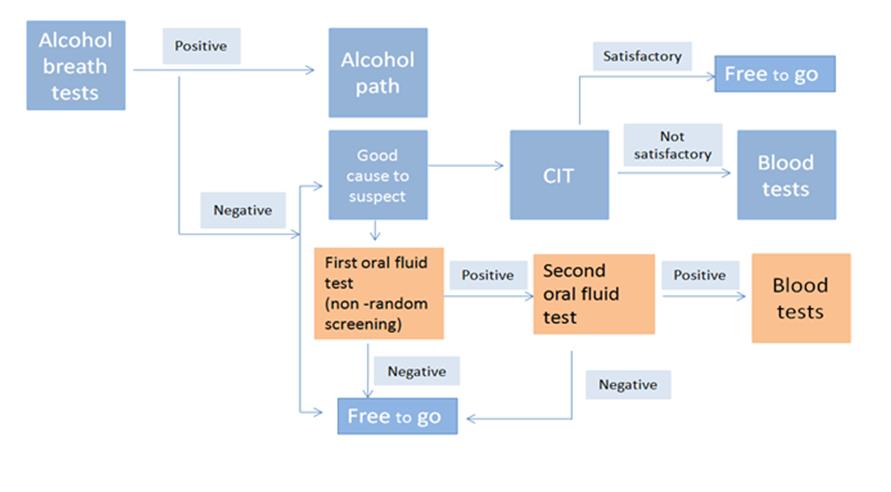
prescription medicines.
18.
Section 57A of the Land Transport Act (the Act) states it is an offence to drive while
impaired, with evidence in the blood of a qualifying drug. Both illegal drugs and
prescription medicines can impair a person’s ability to drive safely. Therefore, New
Zealand’s current drug-driving regime relies on two elements - unsatisfactory
performance on a CIT and a subsequent blood specimen that indicates the presence of
at least one qualifying drug in the driver’s blood.
19.
However, the law provides a defence for a person who can prove that they have a
current and valid prescription for the drug from a health practitioner and were using the
drug in accordance with the health practitioner’s or manufacturer’s instructions.
20.
The regime also includes a presence-based offence. Section 58(1)(b) of the Act applies
t 1982
to drivers who are hospitalised because of a crash. Because of their injuries, these
drivers cannot undergo a CIT. If the driver’s blood test, taken in a hospital, shows the
presence of a Class A drug (for example, methamphetamine), they can be prosecuted.
Drivers can be prosecuted for a wider range of qualifying drugs under the impairment
offence.
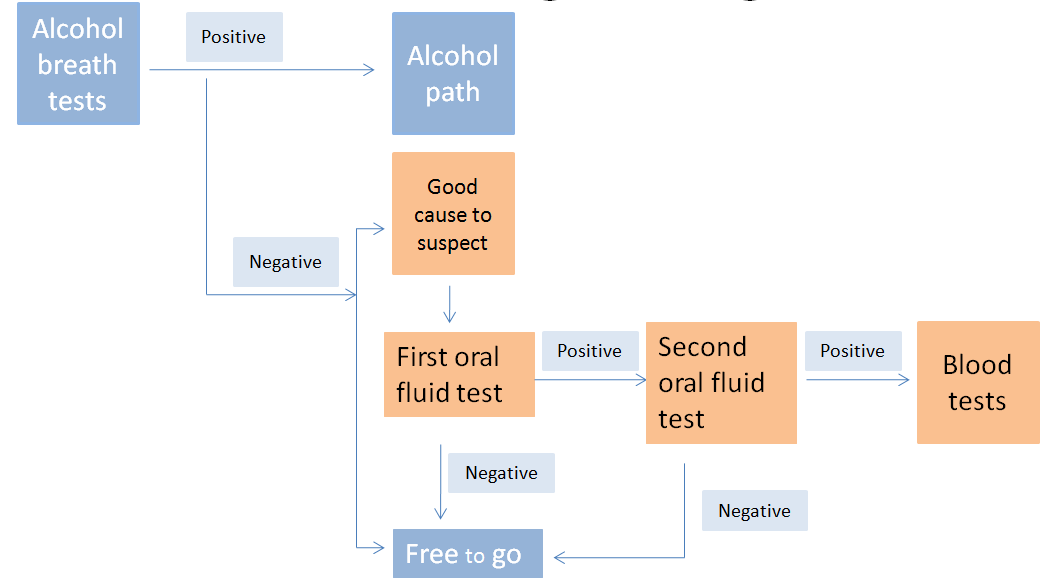
Problem definition
21.
Specific data on the issue of drug-driving in New Zealand is limited, as studies do not
clearly show the extent of the issue. Instead, the Ministry assessed the size of the drug-
driving problem by using several data sources, including New Zealand crash data, which
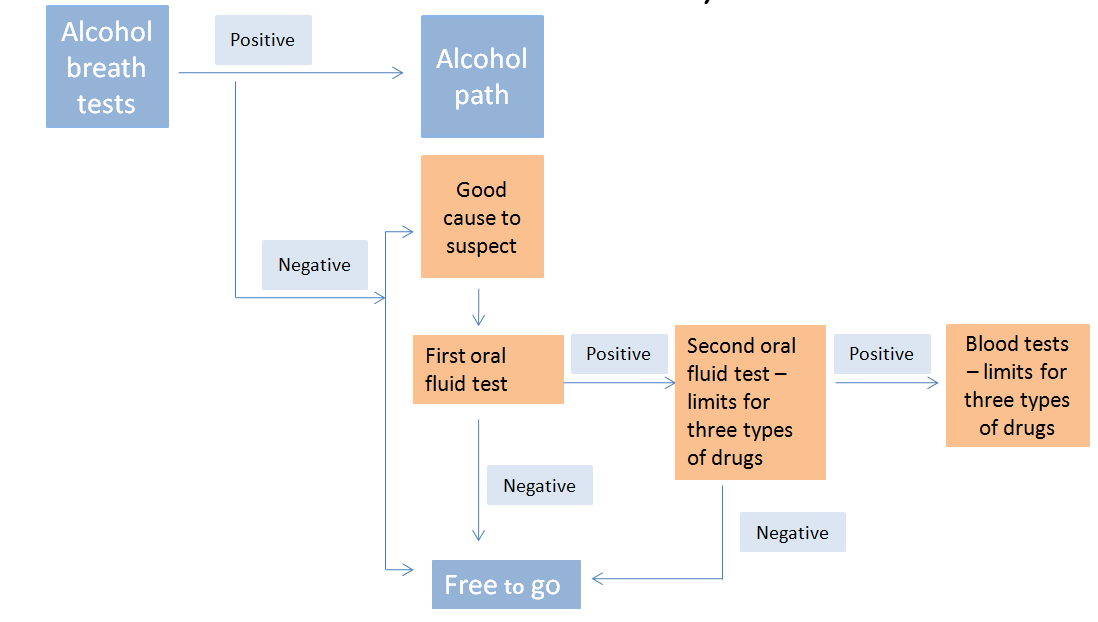
has been compiled in a cost-benefit analysis.
22.
The method involved three different data sources to estimate the scale of New Zealand’s
drug-driving problem. These sources included data from New Zealand’s crash analysis
system (
CAS) that includes all traffic crash data reported by the Police, data from the
under the
United Kingdom, and a 2014 New Zealand Environmental Science and Research (
ESR)
study of drivers killed in road crashes.
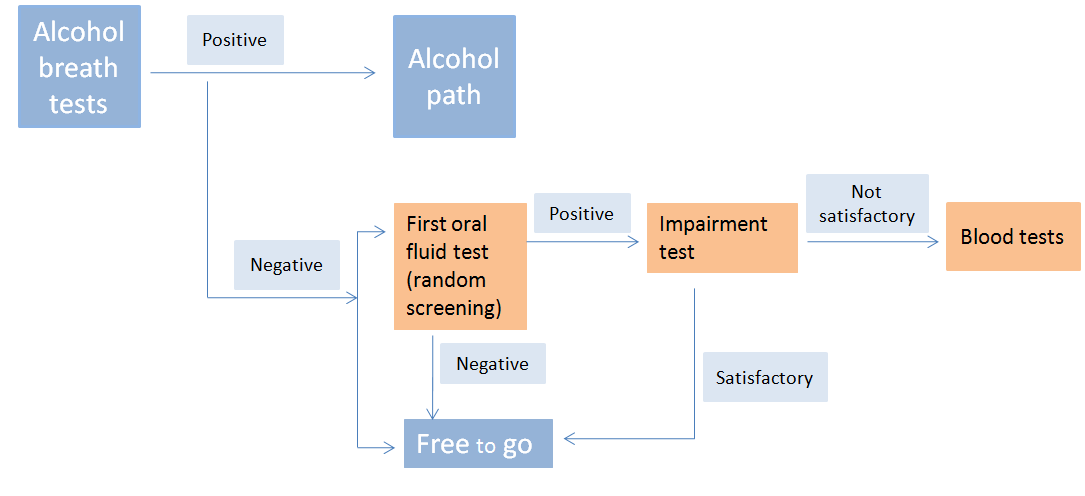
23.
In order to build up the estimates of social cost, estimates of the numbers of crashes with
drug-driving needed to be prepared. The approach assumes that the factors that
formulate trends in drink driving accidents (where costs can be relatively easily
estimated) are similar to the factors that formulate trends in drug-driving accidents. The
analysis uses a ratio of drug related fatal crashes to alcohol related fatal crashes to
estimate the number of crashes with drug-driving.
24.
The ratios used were obtained based on the data from the CAS, the studies in the UK,
and the ESR study in New Zealand. This allowed, low, medium and high estimates of the
social cost to be prepared. The accompanying independently reviewed cost benefit
analysis report sets out the methodology in detail, and identifies the research on which it
was based.
Released
25.
Unlike alcohol, there is no comprehensive data showing the relationship between the
dosages of various drugs, the level of impairment and crash risk. The World Health
Organisation notes a meta-analysis that compiled information from 66 studies showed an
increase in the risk of crashes for 11 different drugs3. However, it is not possible to
Official Information Ac
disaggregate the social cost and attribute it to particular drugs and dosages, when taken
on their own or in combination with others.
3 Global Status Report on Road Safety 2015; World Health Organization: p.40
4
26.
The Ministry’s cost-benefit analysis estimates the social cost of drug-driving at between
$96.8 million and $731.4 million per annum, with a central estimate of $250.5 million.
This is equivalent to 23 people dying, 112 serious crashes, and 304 minor crashes per
year. The cost-benefit analysis only provides indicative estimates of the costs and
benefits of potential policy changes. The analysis is subject to a range of unknowns and
uncertainties. Simulation analysis has been carried out to provide a more robust picture
of the likely range of benefits and costs of the policy proposals.
More about the New Zealand data used in the cost benefit analysis
27.
ESR study of deceased drivers analysed the blood samples of 1,046 drivers, who died in
motor vehicle crashes between 2004 and 2009, for alcohol and drugs. 48 percent of
those drivers tested positive for alcohol, drugs, or both.
28.
The study found that of the 500 drivers who tested positive:
27 percent4 had just alcohol in their system
t 1982
19 percent had just cannabis in their system
28 percent had used both alcohol and cannabis
25 percent had used a combination of drugs, which may have included alcohol
and/or cannabis.
29.
The level of drug-use found in the blood samples taken from dead drivers is not
comparable to the level of drug-use found in the general population, as impaired drivers
are more likely to have a road crash resulting in a fatality. The data also does not
indicate whether a driver with drugs in their system was impaired. The type of drug, the
size of the dosage and the length of time a drug has been in a driver’s body and their
physiology all have a bearing on the degree to which a driver is affected. That a driver is
found to have consumed a drug is not necessarily an indication that their driving was
impaired.
under the
30.
In addition, the Ministry does not have data on the number of people who may be driving
while impaired by prescription drugs, or the number of people who may use drugs at the
same time as alcohol. The impairment caused by some combinations of drugs, or the
mixing of drugs and alcohol (such as cannabis and alcohol) can be much greater than
each on their own.
CAS data
Using CAS data, the Ministry was able to examine a number of fatal crashes occurring
where a driver had consumed drugs. Although the numbers are small and subject to
fluctuation, we can see that the number of fatal crashes occurring where drivers have
consumed drugs is now higher than in the 1990s (see below).
Released
Official Information Ac
4 The percentages in this list do not add up to 100 percent, due to rounding.
5
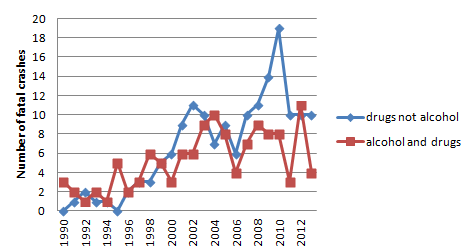
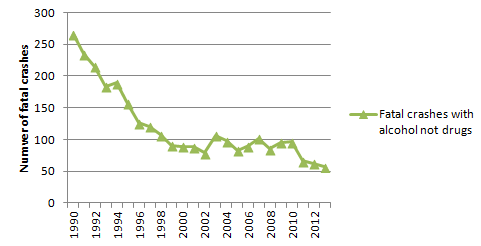 Figure 1: Fatal crashes with qualifying drugs (or combined with alcohol) 1990-2013
Figure 1: Fatal crashes with qualifying drugs (or combined with alcohol) 1990-2013
t 1982
31.
In comparison, the numbers of fatal crashes per annum, where drivers have consumed
alcohol, is now less than in the 1990s (see Figure 2 below). It is important to note that
the numbers of crashes involving alcohol are much higher than the numbers of crashes
recorded where drivers had consumed drugs.
Figure 2: Fatal crashes with alcohol (no drugs) 1990-2013
under the
32.
The numbers of drug-related crashes recorded in the CAS are probably underreported,
due to drugs not being routinely tested for. Current operational practice is that if alcohol
is observed at a high level over the limit, other tests are not carried out. On the other
hand, those that are recorded may not have been caused by drugs.
Released
Official Information Ac
6
Other data that indicates the level of drug-driving in New Zealand
33.
There are several studies pointing to the prevalence of the use of certain drugs generally
and in driving. The Ministry of Health’s 2007/08 New Zealand Alcohol and Drug Use
survey found the most commonly used recreational drugs in the 12 months before the
survey were cannabis (14.6 percent), BZP party pills (5.6 percent), MDMA (2.6 percent),
and amphetamines (2.1 percent). In that year, buying BZP party pills was legal, so the
number of people using BZP has likely dropped since then.
34.
A new question about driving while affected by drugs with or without alcohol was
introduced in 2014 to the Ministry’s Public Attitudes to Road Safety survey. Nine percent
of participants said they had driven while affected by prescription or pharmacy drugs,
including two percent combined with alcohol. Four percent said they had driven while
affected by other drugs (whether legal or not), including two percent combined with
alcohol.
35.
This was a self-report survey. As self-report surveys are voluntary and based on self-
t 1982
reported drug use. The survey sample may not represent real drug use. A driver may
also be objectively impaired, without feeling that this is the case, or vice versa. In
addition, the question asked whether drivers felt ‘affected’ by drugs, rather than
‘impaired’. While we cannot be certain about how drivers interpreted the question, being
‘affected’ by drugs does not mean that one is impaired.
36.
The Ministry of Health’s Cannabis Use 2012/13: New Zealand Health survey found that
11 percent of adults reported using cannabis in the 12 months before the survey. Of this
11 percent, 36 percent of cannabis users reported driving under the influence of
cannabis in the last 12 months. This equates to around 133,000 adults. Men were 1.5
times more likely than women to have driven under the influence of cannabis in the last
12 months.
Problems with New Zealand’s current drug-driving enforcement regime
37.
The current regime does take some drug-impaired drivers off the road after the fact, but
under the
does not appear to be deterring the behaviour in the first place. As outlined by social
costs estimated in the cost-benefit analysis, it is apparent that a drug-driving problem
exists in New Zealand and that this problem is causing a cost to New Zealanders and to
society in general. New Zealand’s drug-driving enforcement regime does not create the
conditions for general deterrence as compared, for example, to New Zealand’s random
drink-driving testing regime. General deterrence involves deterring the general motoring
population from driving while drugged. General deterrence relies on highly visible Police
enforcement and the perceived likelihood of being caught, as well as the consequences
that follow for a drugged driver. Random breath testing has been found to be very
effective in deterring and, therefore, reducing drink-driving.
38.
Establishing good cause to suspect can be difficult for the Police. A Police officer must
explicitly identify a reason to suspect a driver. CITs also involve a degree of subjectivity
and, therefore, require well-trained officers, and are time consuming. For these reasons,
the number of impairment tests are low. NZ Police advise that around 200 tests are
unsatisfactorily completed per annum, but do not hold data on how many CITs are
Released
conducted overall. So, while the sanctions facing a drugged driver are severe, there is
neither sufficiently visible enforcement nor enough tests to have a significant deterrence
effect.
Official Information Ac
7
39.
Given the limitations inherent in New Zealand’s current drug-driving regime, coupled with
the prevalence of fatal crashes which involved drug-driving in New Zealand, it appears
there is an opportunity to improve the drug-driving enforcement regime in New Zealand.
Objectives
40.
In March 2010, the Government released Safer Journeys New Zealand’s Road Safety
Strategy 2010-2020. Safer Journeys established a vision of a “safe road system
increasingly free of death and serious injury” and adopted the ‘Safe System’ approach to
achieve this.
41.
A Safe System approach looks across the road system to achieve safe roads and road
sides, safe vehicles, safe speeds and safe road use. A Safe System approach to road
safety recognises that even responsible people sometimes make mistakes and poor
decisions when travelling on the roads. It therefore looks to institute policies that
proactively mitigate the risk of a crash and reduce the severity of consequences in the
event of a crash.
t 1982
42.
Safer Journeys identified alcohol and drug-impaired driving as an area of high concern.
Safer Journeys included an action for investigating opportunities to strengthen the
existing drug-driving enforcement model in New Zealand, through a review.
43.
The main objective of a drug-driving enforcement regime is to reduce the harms caused
by drug-driving. To be successful, a drug-driving enforcement regime, needs to:
remove impaired drivers from the road
prosecute and sanction drugged drivers
deter drivers from driving drugged.
44.
It is also desirable, as in any regulatory regime, that it should:
under the
apply best practice enforcement techniques and technologies
achieve a net benefit from any changes and avoid unintended consequences.
Options and impact analysis
International regimes
45.
The Ministry investigated drug-driving regimes in a number of countries. The Ministry’s
review found countries consistently use impairment-based regimes, often in parallel with
other approaches. One of the main reasons for this is the very large range of impairing
drugs, both illegal and prescription, which cannot be identified easily through the
roadside testing of body fluids. However, the Ministry also found that several countries
have an impairment-based regime similar to that of New Zealand’s regime but also make
use of a presence-based approach. A presence based approach uses screening devices
to test for the presence of drugs using bodily fluids.
Released
46.
The Ministry then identified the United Kingdom’s and Victoria, Australia’s regimes as
regimes that should be examined in more depth. Both regimes are quite different from
each other, but both use a presence-based approach, in parallel with a regime similar to
New Zealand’s.
Official Information Ac
8
Victoria’s drug-driving regime
47.
Victoria’s regime consists of two separate testing regimes that run in parallel. In addition
to running a good-cause, impairment-testing regime, Victoria uses another regime that is
a random presence based drug testing model.
48.
The regime tests for at least one of three drugs in an oral fluid sample and this alone is
sufficient evidence of an offence. The strategic principle behind this type of operation is
general deterrence of drug-driving, to raise the perceived risk of an illegal drug-driver
being caught for this offence, not necessarily to detect illegal drug-driving on a larger
scale than could be achieved by targeted drug-driving enforcement operations. While
this is a random testing regime, it is applied in a targeted way, with operations set up on
arterial routes for long-haul truck drivers, near nightclubs for all drivers, and in areas
associated with high levels of drug-use.
49.
Testing is conducted by randomly intercepting small groups of drivers passing through
Police alcohol checkpoints. All drivers intercepted are first screened for alcohol. If the
t 1982
driver fails this test, the officer then follows their alcohol enforcement process.
50.
If the driver passes the alcohol-screening test, a preliminary oral fluid test is conducted to
detect the presence of cannabis, methamphetamines or ecstasy. A device called
DrugWipe II is used to detect the presence of the three drugs in an oral fluid sample
obtained by the driver swiping the top of their tongue against a test pad on the device.
51.
If the device shows the presence of any one of the three drugs, then a second, different,
oral fluid test is taken. The driver places a swab attached to a stick under their tongue
and collects an oral fluid sample. It is then swiped against the test pad on the testing
device. If the device shows the presence of any one of three drugs, the oral fluid sample
is sent away to a forensic laboratory for confirmatory analysis.
52.
Victoria was the first jurisdiction to introduce roadside drug testing of drivers, and has
provided the blueprint for the legislation and enforcement methods in other Australian
jurisdictions.
under the
53.
As outlined in an article by Dr Baldock (Centre for Automotive Safety Research,
University of Adelaide) a number of Australian jurisdictions have undertaken reviews of
their roadside drug testing programs. These reviews have focussed on process
evaluations (training, equipment, relationships between stakeholders etc) and analysis of
data relating to enforcement and detection. Key variables have included the number of
screening tests, the number of confirmed positives for different drugs, and the overall
detection rate. However, the overall detection rates are difficult to determine, given the
use of targeted operations and the discretion to choose particular drivers from a line of
vehicles at checkpoint sites. This means that detection rates would be affected by
operational factors to a greater degree than any changes in the rate of offending among
the driving population.
54.
Surveys of drivers have been used to measure deterrence. Variables measured have
included perceived likelihood of detection for drug-driving, social disapproval of drug-
driving, anxiety about drug-driving, and self reported frequency of drug-driving.
Released
55.
Reviews of Victoria’s roadside drug testing regime have been uniformly positive and
supportive.
Official Information Ac
9
56.
The best measure of effectiveness would be the reduction in the number of drug related
road crashes; however no reviews that the Ministry is aware of have included crash-
based data analysis, which is unfortunate. To undertake such an evaluation, it would be
necessary to compare rates of crash-involved drivers testing positive to the prescribed
drugs before and after the introduction of random roadside drug testing. Such an
evaluation would pose a number of methodological challenges.
57.
The major implication of the lack of crash-based evaluation of Victoria’s random roadside
drug testing regime is that there is no concrete indicator of the road safety benefit of this
form of enforcement.
58.
However, a paper written by Professor Max Cameron of Monash University’s Accident
Research Centre has aimed to develop an analogy between random drug testing and the
early years of random breath testing in Australia. This analogy is used to predict the
likely effects on drug-driving among killed drivers as the number of random drug tests is
increased.
t 1982
59.
Relationships between the annual number of random drug tests conducted in Victoria
between 2005 and 2009 and the percentage of killed drivers with drugs in their blood
stream were able to be calibrated. The calibrated relationships were then used in
conjunction with an estimate of the cost per random drug test to determine the cost
effectiveness of random drug testing.
60.
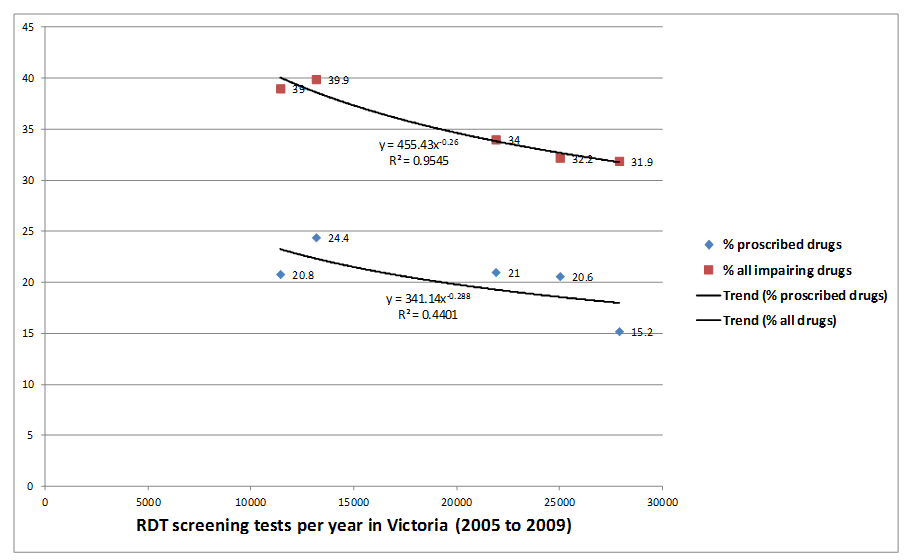
The relationship between the annual number of random oral fluid tests and the annual
percentage of killed drivers with at least one of the proscribed drugs is shown in the
figure below. An even stronger relationship is apparent between the number of random
oral fluid tests and the percentage of killed drivers with any impairing drug (including the
three proscribed drugs). This suggests an association between random drug testing and
the deterrence of both proscribed and non-proscribed impairing drugs taken by drivers.
Figure 3: Relationships between percentage of killed drivers with proscribed drugs, or
any impairing drug, versus number of drivers screened by random oral fluid tests at
random drug testing in Victoria
under the
Released
Official Information Ac
10
61.
The study concluded that there was a reasonable analogy between random drug testing
and random breath testing. From this, the researchers considered it appropriate to use
the relationships illustrated in Figure 3 above to predict the likely effects on driver
fatalities as random drug testing levels are increased. The conclusion of the paper
suggests that best-practice random drug testing has the potential to achieve significant
general deterrence of drug-driving.
United Kingdom’s drug-driving regime
62.
The United Kingdom has two drug-driving enforcement regimes running in parallel. The
first regime is very similar to New Zealand’s current impairment-based regime.
63.
In March 2015, the United Kingdom introduced a new regime that allowed Police officers
to test drivers for drug use, using an oral fluid test, as well as setting specific limits for
eight illegal, and nine medicinal drugs. The limits apply both when Police officers perform
a field impairment test, and when they perform an oral fluid test.
t 1982
64.
The limits for the eight illegal drugs are extremely low and are effectively zero tolerance
limits. The limits for the nine medicinal drugs are set at levels where drivers would be
expected to be impaired, and are well above the therapeutic levels for these drugs.
65.
The drug-driving regime used by the United Kingdom requires Police officers to have
belief that a driver has used drugs. If a Police officer believes a driver has used drugs,
they are able to use an oral fluid test to test for cannabis and cocaine. The UK is
currently only doing roadside oral fluid tests for those two drugs. Even if a driver passes
this test, if a Police officer still believes they are impaired, they can require the driver to
undergo a field impairment test.
66.
If either the oral fluid screening test or the field impairment test indicates a driver has
used drugs, or is impaired, the Police officer can then take a blood or urine sample to
test for drugs.
67.
For the other illegal drugs and for the medicinal drugs, the United Kingdom currently
under the
uses an impairment-based regime.
68.
The Ministry’s analysis of other countries regimes led us to believe there were two
questions that needed to be answered when designing a drug-driving enforcement
regime:
Is a behavioural impairment-based approach or a presence-based approach
preferable?
Should presence alone be sanctioned?
Should a regime have a good-cause to suspect (non-random) or a random
testing approach?
Different methods of testing drivers for drugs
69.
The most plausible mechanism for drug-driving enforcement to reduce societal costs is
Released
through a deterrent effect from increased law enforcement. It is assumed that individuals’
behaviour could be affected by increased testing at the roadside and by word of mouth of
people who have been tested. The reduced prevalence of impairment due to the change
in individuals’ behaviour would lead to reduced injury and non-injury crashes and,
Official Information Ac
therefore, lower social costs.
11
70.
The Ministry investigated two drug-driving testing methods – behavioural impairment-
based testing and presence-based testing:
A behavioural impairment-based approach involves a behavioural test to identify
that a driver is impaired. In New Zealand, this test is the CIT.
A presence-based approach requires a Police officer to determine whether a
driver had used drugs through bodily fluid testing (i.e. urine, oral fluids including
saliva, or blood).
71.
In practice, drug enforcement regimes use a combination of these methods, placing
weight on one or the other depending on the policy objectives of the regime. The reason
for this is that each of the methods have advantages and disadvantages. Behavioural
impairment testing works well to identify visibly impaired drivers, but there are limitations
in the number of tests that can be conducted. Further, it is possible for drivers to be
affected by drugs without visible impairment. Drug use can affect drivers and the ability
to drive safely by:
t 1982
Slowing down reaction time – this can be crucial in an emergency situation
Dulling the thinking process making it difficult to multi-task – an essential skill
necessary for safe driving
Causing a distorted view of time and distance – reducing a drivers ability to drive
safely and identify driving hazards
Stimulating the nervous system leading to:
o reduced attention span
o over-confidence in driving skills that is not supported by an actual
improvement in driving ability
under the
o the sudden onset of fatigue as the stimulant effects wear off
o altering a driver’s view and experience of reality, with their actions and
responses quite different to what is actually needed. They may be
unaware of how much their driving skills are impaired.
72.
Presence based testing through oral fluid screening tests presents a more practical
method of identifying a larger group of drivers who have taken drugs and consequently
may be impaired. However, presence alone does not necessarily prove that driving
ability is impaired.
Behavioural impairment-based testing regimes
73.
The focus of New Zealand’s current drug-driving enforcement regime is to identify drug
impairment using a behavioural test. This helps improve road safety, by ensuring visibly
impaired drivers are taken off the road and successfully prosecuted, provided the Police
can identify them and establish good cause to suspect a driver has used a drug or drugs.
Released
74.
The behavioural test is useful because it is difficult to link the presence or amount of
drugs in a person’s body with their fitness to drive. Further, a behavioural test does not
rely on identifying a specific drug impairing a driver before a blood sample is taken for
Official Information Ac
evidential purposes.
12
75.
CITs consist of a number of tests, including an eye assessment, a walk and turn
assessment and a one-leg stand assessment. As those being tested are likely to be
impaired, these tests cannot be done at the roadside safely, so drivers are usually
brought back to a Police station to be tested for impairment. In addition, distractions at
the roadside could result in a Police officer incorrectly determining a person is impaired.
76.
The CIT, as conducted in New Zealand, appears to be effective in identifying impairment
in drivers. Around 90 percent of those who unsatisfactorily complete the CIT are found to
have qualifying drugs in their blood which suggests, but does not prove, that the
impairment was caused by the drugs present.
77.
However, a CIT can take a long time and thus impose costs on both drivers and on
Police time and resources. Further, not all Police officers are trained to carry out a CIT
and so are not able to perform a CIT. The option of redesigning the CIT has not been
considered, as the current process is considered best practice.
78.
Blood testing remains the most accurate method for identifying a broad range of drugs,
t 1982
including prescription drugs, but is not feasible at the roadside.
Presence-based testing regimes
79.
The main alternative to impairment-based testing is to test for the presence of drugs
using roadside screening devices. Relying solely on presence-based testing would be a
departure from New Zealand’s current impairment-based approach (although there is a
presence-based offence for hospitalised drivers who cannot undergo the CIT).
80.
A screening test of a driver’s oral fluids is the most practical and least invasive roadside
drug screening method available. Oral fluid testing devices are available, and used in
other countries, but do have limitations. These devices work by detecting the presence of
a drug in an oral fluid sample obtained by the driver swiping the top of their tongue
against a test pad on the device. Using such a device requires a driver to be stopped for
around five minutes. This is much longer than the time taken to administer a passive
breath alcohol test, which generally only takes a few seconds.
under the
81.
In 2009, Cabinet agreed that New Zealand should not consider moving to a random
roadside drug testing regime until performance-based issues with oral fluid screening
devices (in terms of the limited range of drugs that they are able to detect, their lack of
accuracy, and the slow time to produce a result) have been satisfactorily resolved.
Reliability of oral fluid screening devices
82.
Roadside screening devices used to test for the presence of drugs can only identify a
limited number of drugs. The devices are relatively slow and expensive compared to
alcohol testing devices and cannot determine the amount of drugs in a person’s body. As
more drugs are tested for using oral fluid testing devices, the time needed for testing and
the cost increases. The number of drugs that can be tested for is currently limited. The
devices used by the Australian State of Victoria take around five minutes and tests for
methamphetamine, THC (the active ingredient in cannabis) and MDMA (ecstasy) only.
83.
Roadside drug testing can detect THC for several hours after use. The exact time can
Released
vary, depending on the amount and potency of the cannabis used and the individual’s
metabolism. Inactive THC residue in the body of a driver from use in previous days or
weeks is not detected by the oral fluid screening tests.
Official Information Ac
13
84.
ESR has indicated that blood samples taken from drivers who do not satisfactorily
perform the CIT show the drugs most commonly used by impaired drivers are cannabis
and methamphetamine. While drivers sometimes report taking MDMA, blood samples
indicate that drivers will think they have taken ecstasy, when actually taking a different
type of drug.
85.
Some oral fluid screening devices can also be susceptible to temperature and humidity
fluctuation. In addition, while the accuracy of oral fluid screening devices has improved
over recent years, the oral fluid screening devices that are currently available can
produce false positive results. This is when the device incorrectly indicates the presence
of a drug in an oral fluid sample when it is absent. Part of the reason false positives can
occur is due to operator error, for example if a Police officer does not follow the device’s
operating instructions precisely.
86.
Nevertheless, over the last 3-4 years oral fluid screening devices have improved in
sensitivity, in particular, their ability to detect THC (the active ingredient of cannabis).
The availability of devices has also increased, with a number of different testing options
t 1982
now available. Police anticipates that there will continue to be developments in the drug
testing space, which will deliver quicker and more effective technology in the future.
87.
While most drug screening devices still take around 3-4 minutes to produce a result for a
small number of drugs (between 3-5), technology is improving. Already, there are more
sensitive testing options becoming readily available. For example, the Drager DrugCheck
3000 can detect THC and offers two measurement options: fast or sensitive. The fast
mode displays a quantity of 40 ng/ml or more after just one minute. The sensitive model
permits detection of 15 ng/ml THC after three minutes. Given that cannabis use is still
higher than any other drug, the fast mode does offer some benefit.
88.
Police advise that these new devices reduce the risk of operator error, thereby mitigating
some of the risk of returning a false positive result.
89.
Compared to breath alcohol screening, the cost of oral fluid screening remains high
(currently at around $35-$45 per test for a disposable device) depending on the device
under the
used. While the unit cost per oral fluid test is high, disposable devices can be used at the
roadside without the need for an external power source. They do not incur any on-going
servicing costs such as those associated with calibration, or any down-time while the
device is being serviced.
90.
If the trends relating to improvements in screening devices continue, there may be better
and more cost effective devices available by the time the Police would be tendering for
devices (if proposals are endorsed by the Government and Parliament). Furthermore,
any improvements in screening devices will be closely monitored by Police, to ensure the
greatest operational efficiency.
91.
Officer training in the correct use of the device and careful monitoring of false positive
rates in the administration of roadside screening tests is critically important. This is to
reduce the risk of detaining innocent drivers for further evidential testing, and to maintain
public perception of integrity and fairness of the testing process.
Released
92.
Accurate up-to-date data on the rate of false positive in other jurisdictions and on
particular testing devices has been difficult to obtain. An Australian study conducted prior
to 2009 noted that overall drug positive rate was 1 in 50 drivers tested in the State of
Victoria. Of the samples tested positive at the roadside, only two percent were found not
Official Information Ac
to contain drugs in the laboratory (false positives). However, this was some time ago and
testing procedures have since improved. Another study in Victoria has quoted a false
positive rate of 0.8% for the oral fluid testing devices employed there.
14
93.
Other jurisdictions have addressed the issue of false positives by improving the handling
of testing equipment, and subsequently the rate of false positives has declined.
94.
To provide further reassurance on testing accuracy, a two-step testing process could be
used, like in Victoria, Australia. In addition, blood tests also have the ability to confirm
presence of drugs.
95.
Blood specimens can be used to detect the presence of drugs and do not produce false
positive test results. In New Zealand, blood samples could continue to be collected using
the same process and equipment that is currently used to collect blood specimens from
drivers for alcohol or drug analysis. It would be analysed by ESR using the same
equipment, processes and standards of accuracy that currently apply to the analysis of
evidential blood specimens for drugs under the current drug-driving enforcement regime.
Blood results will not produce false positive results.
Tolerance limits
t 1982
96.
Many countries operate a zero tolerance policy in presence-based regimes because it is
difficult to link driving impairment with the level of drug or combinations of a drug found in
a driver’s system, and there is a wide range of drugs to be addressed.
97.
A small number of jurisdictions are setting per se limits5 for some drugs. However, there
is debate on the validity of such limits in terms of whether they reflect levels of
impairment or crash risk. Testing for compliance with a range of drug limits would be
complex and very expensive. Blood tests would need to be conducted, as there are no
current drug screening devices capable of establishing the amount of drugs in a person’s
body.
98.
A benefit of presence-based regimes using screening devices is that it makes large-
scale roadside testing possible, which helps with general deterrence. Presence-based
testing can remove impaired drivers from the road and sanction them for presenting a
danger to other road users. However, it is a blunter tool than impairment-based testing,
and there is a risk that drivers who are not road safety risks are sanctioned. This is
under the
unlikely to happen under a behavioural impairment-based regime, such as New
Zealand’s current regime.
Criminal-based sanctions or infringement penalties?
99.
If a presence-based regime is introduced, a question exists about whether drivers found
to be driving with drugs in their system only – which is currently not an offence - receive
criminal sanctions or infringement penalties. Criminal sanctions would involve a driver
being prosecuted in court and facing serious penalties similar to those that apply to
serious drink-driving offences. An infringement does not result in a criminal conviction.
100.
Criminal sanctions would act as a strong deterrent to drug-driving. However, a presence-
based regime would not indicate whether a driver was impaired, and as such would not
show conclusively whether that driver was a road safety risk.
101.
The current drug-driving laws focus on the harm caused by driving whilst impaired by a
drug. Without conclusive evidence that the presence of a drug has affected a person’s
Released
ability to drive, the imposition of a criminal sanction is likely to be unjustified. Therefore,
the imposition of an infringement rather than a criminal offence appears more
appropriate where the focus is purely on the presence of drugs.
Official Information Ac
5 the limit above which driving is illegal
15
102.
A disadvantage of criminal-based sanctions is the workload and cost they will place on
the Justice sector. Infringement penalties would result in much lower costs to the Justice
sector, as infringements do not generally result in a court hearing unless the driver
requests a defended hearing.
103.
However, having an infringement regime could lead to a risk of this offence being
perceived as minor. This would depend on the infringement penalties applied. An
infringement fee coupled with demerit points could offer a reasonable deterrent,
commensurate with the nature of the offence. Infringement penalties would also not put
as much pressure on the justice sector as criminal-based sanctions. Infringements also
offer a swifter way of sanctioning drivers than a court prosecution.
Random or non-random testing
104.
The Ministry investigated random and non-random approaches to testing drivers for
drugs:
t 1982
A non-random (good cause to suspect) approach requires Police officers to
determine that they have good cause to believe a driver has used a drug or drugs
before conducting any further drug tests. Non-random testing has the benefit of
removing drivers who are obviously impaired from the road.
Random testing involves stopping cars randomly such as at a booze bus random
testing checkpoint and, for practical reasons, typically requires using an oral fluid
testing device to test drivers for the presence of drugs. Random testing has the
benefit of deterring the general population from drug-driving.
Non-random (good cause to suspect) drug testing
105.
Non-random testing is reliant on a Police officer first having good cause to suspect the
use of a drug before they can begin any testing process. Under this type of regime,
Police officers are not permitted to detain and test drivers who are not yet suspected of
having committed an offence. This type of regime therefore carries a reduced risk of
under the
subjecting innocent drivers to unnecessary testing. When Police are able to determine
good cause to suspect, this regime is effective in removing drug-impaired drivers from
the road.
106.
Regimes based on good cause to suspect do have weaknesses. NZ Police state there is
a high evidentiary threshold for establishing good cause to suspect. This threshold
means it is likely there are a number of drug-impaired drivers who are not being tested.
107.
Reliance on good cause to suspect has a limited effect on deterring people who take
drugs from driving, particularly when compared to random drug testing regimes. This is
because a good-cause to suspect approach is unlikely to test sufficient numbers of
people from the general driving population to be a deterrent from using drugs and
driving.
Random drug testing
108.
Random drug-driving testing is a regime where a Police officer can stop any driver who
Released
is driving a motor vehicle on a public road and drug test them, without first needing good
cause to suspect the driver has used a qualifying drug or drugs. New Zealand already
operates a random testing regime for alcohol known as Compulsory Breath Testing
Official Information Ac
(CBT).
16
109.
The best conditions for deterrence involve Police officers carrying out significant
numbers of tests on a random basis. This creates an effect known as general
deterrence, and is an important feature of New Zealand’s current drink-driving regime.
110.
General deterrence would apply when the mere threat of being caught and sanctioned
deters the majority of drivers from committing an offence. High levels of general
deterrence are achieved only if the roadside testing of drivers is conducted at sufficiently
intense levels, and in a sufficiently visible manner such as at checkpoints, to increase
public perception of the risk that they will be caught if they drive after having used drugs.
Currently, New Zealand’s drug-driving enforcement regime does not benefit from a
general deterrence effect, as drivers are not being tested for drugs in sufficiently high
numbers. International evidence shows that when drivers know they are unlikely to ‘get
away with it’, they are much less likely to risk drug-driving.
111.
While random testing has been used in New Zealand for drink-driving enforcement for
many years, cost and practicality are a major issue for random drug testing. Selecting
drivers randomly and requiring them to undergo a CIT would be impractical due to the
t 1982
length of time a driver would be stopped while being tested (around 52 minutes,
including travel time to a Police station).
112.
Random-testing regimes usually determine who should undergo evidential testing using
a roadside screening test. This test replaces the need for a Police officer to have good
cause to suspect a driver has used a drug or drugs. As noted above, roadside drug
screening devices have limitations.
Options considered and criteria assessed against
Six options considered
113.
The Ministry considered six options to improve the drug-driving enforcement regime, as
well as retaining the status quo. These options are variations on both random, or non-
random testing, and presence-based, or impairment-based approaches. Many of the
options build on New Zealand’s current drug-driving enforcement regime, and take into
under the
account regimes used in other countries.
114.
The six options were designed after consideration of the strengths and weaknesses of
different approaches to enforcement and how various regimes, if implemented in a New
Zealand setting, might reduce the harm caused by drug-driving; feedback from
engagement with various stakeholder groups; and whether it would be practical to
implement the various regimes in New Zealand.
115.
Random behavioural testing has not been included as an option, as it would be
impractical and unjustified, due to the length of time a driver would need to be stopped
for testing. According to NZ Police data, a CIT takes approximately 52 minutes per test
(including travel time).
116.
All options, except for option 3, assume that the Police would retain the power to conduct
CITs with good cause to suspect, as drivers may be impaired by drugs that cannot be
tested for with an oral fluid screening device.
Released
Official Information Ac
17
Feasible number of tests
117.
Each option was assessed using the feasible number of tests the Police would be able to
conduct under that option. For non-random regimes, where the Police must have good
cause to suspect a driver has used drugs, the number chosen was 1000 tests. This
number is five times the current tests undertaken. We believe this number is attainable
with extra resourcing. While a higher number of tests would be preferable, these regimes
are based on Police identifying sufficient numbers of people to put through the testing
process. Random testing regimes enable a larger number of drivers to be screened. The
feasible number used was 45,000 tests. This is seen as a credible number of tests to
create deterrence and therefore achieve road safety benefits. In 2013, Victoria
conducted 42,000 screening tests, although there are plans to increase the number of
screening tests to 100,000 by 2016.
Criteria assessed against
118.
The analysis considers the options below against the following criteria:
t 1982
Meets the objectives of drug-driving enforcement – meets the objectives as set out in
the objectives section of this RIS
Impacts on drivers – the impacts on the freedom and private benefits of individuals
Public acceptability – whether the public is likely to accept and adhere to a particular
policy option
Impacts on the Courts and Corrections – the impacts on the integrity, cost and
efficiency of the justice system when processing drivers
Operational feasibility – the practicality for the NZ Police to implement the regime in a
way that is consistent with the intention of the regime.
Trade offs to be considered
under the
119.
The analysis in this RIS is designed to allow decision makers to consider the trade offs
that need to be made when deciding to change the drug driving enforcement regime.
The key trade offs are between:
estimated road safety benefits
the impacts on drivers including potential inconsistencies with the New Zealand
Bill of Rights Act 1990 and
the practicalities of implementing any new enforcement regime.
120.
Decision makers will need to weigh up the road safety benefits of particular options and
the potential impacts on drivers.
Education option not considered further
Released
121.
Public education is an alternative to enforcement. The NZTA currently uses public
education through a range of communications media, including YouTube, Facebook and
Twitter, to converse with drivers about driving while under the influence of drugs. While
the Ministry recognises that outcomes of the drug-driving enforcement regime overlap
Official Information Ac
with the NZTA’s focus on promoting road safety, it considers public education to be a
tool that gives effect to the drug-driving policies in place. It is likely to be more effective
when it accompanies changes to the drug-driving regime. As such, we do not consider
18
that additional investment in education will be effective in addressing drug-driving, except
as an adjunct to any change in enforcement approach.
122.
The Ministry of Transport and other relevant agencies (in particular the NZTA) will
continue to work on non-legislative enhancements to the drug-driving regime [EGI Min
(12) 7/2].
Option 1: Status quo (with increased testing)
123.
Option 1 would maintain the compulsory drug-driving impairment tests under the current
regime, but increase the number of tests undertaken. This option would also maintain the
blood test for evidence. While more Police resources would be deployed to help ensure
drug-drivers are taken off the road, it is difficult to determine the number of increased
tests that would be undertaken as this option does require a Police officer to have good
cause to suspect a driver has used a drug, or drugs. Under option 1, the drug-driving
enforcement regime remains unchanged from the status quo.
t 1982
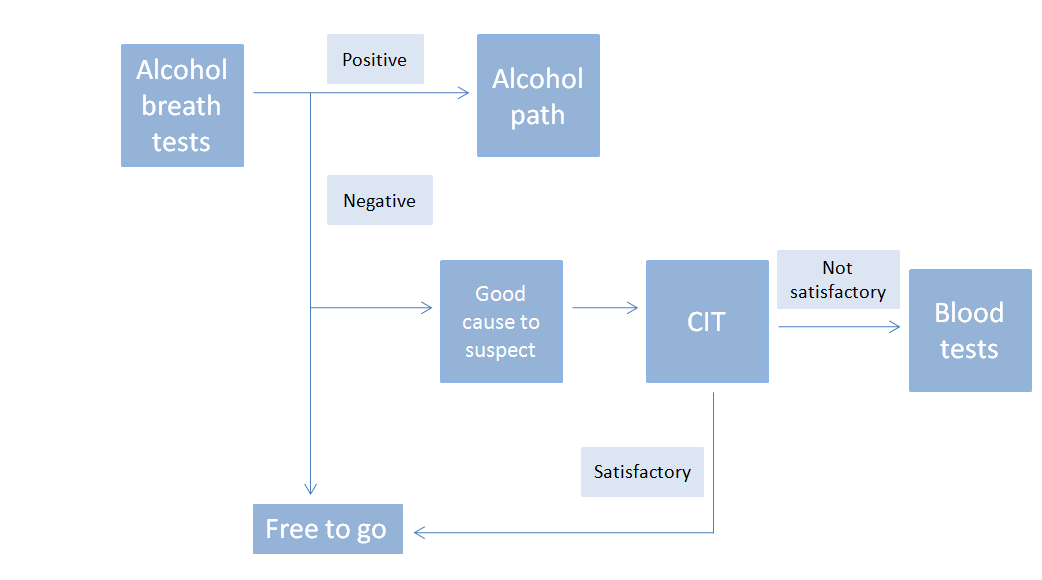
124.
Under this option, if good cause to suspect exists, the officer will require the driver to
undergo a CIT. If a driver’s performance on the CIT is unsatisfactory, a Police officer can
require the driver to undergo a blood test for a qualifying drug.
125.
The following diagram outlines the testing process under option 1.
Diagram 1: Testing process under option 1
under the
126.
Assuming 1000 tests were completed, option 1 has a central BCR of 0.27. This option
would have some road safety benefits, through removing drivers who are obviously
impaired from the road.
Option 2: Existing model for CIT in addition to random oral fluid testing (preferred option
and similar to that used in Victoria, Australia)
Released
127.
Option 2 would introduce a random oral fluid testing approach. This model is based
largely on the approach used in the Australian State of Victoria since 2004.
Official Information Ac
19
128.
Random testing would most likely be applied by intercepting small groups of drivers
passing through Police alcohol checkpoints. First, drivers would be screened for alcohol.
If the driver failed this test, the officer would then follow the drink-driving enforcement
process. If the driver passed the alcohol screening test, a preliminary oral fluid test for
drugs may follow.
129.
While subject to further investigation and procurement procedures, it is likely that Police
would use an oral fluid screening device designed to detect the presence of three
qualifying drugs (cannabis, methamphetamine or MDMA). This test requires a driver to
swipe the top of their tongue against a test pad on the device.
130.
A positive result on the first oral fluid test would result in a second oral fluid test on a
different device. The second oral fluid testing device would have a higher rate of
accuracy than the initial test, at an increased cost and time. If this device shows the
presence of any one of three drugs, then a blood test would follow. The blood sample
would be sent to a forensic laboratory for confirmatory analysis.
t 1982
131.
The random component of this regime has no requirement for Police to prove
impairment. The presence of any specified drug detected in the evidential analysis would
be sufficient proof of an offence.
132.
There is the risk that drivers are prosecuted whether impaired or not, and some of whom
may not be a road safety risk. In Australia, the State of Victoria deals with this by only
issuing infringement offences for presence-based tests if it is a driver’s first offence.
Criminal offences apply if drivers are found drug-driving a second time. Similar to the
Victorian regime, option 2 assumes an infringement offence for those who fail the blood
test following the random screening pathway.
133.
The following diagram outlines the process that would be followed under option 2. The
diagram below assumes that a Police officer would first undertake an alcohol screening
test before undertaking an oral fluid test for drugs. This is because in an operational
setting, this is the most likely path that would be followed. However, a Police officer
would have the ability to take an oral fluid test without first having taken an alcohol
under the
breath test.
Released
Official Information Ac
20
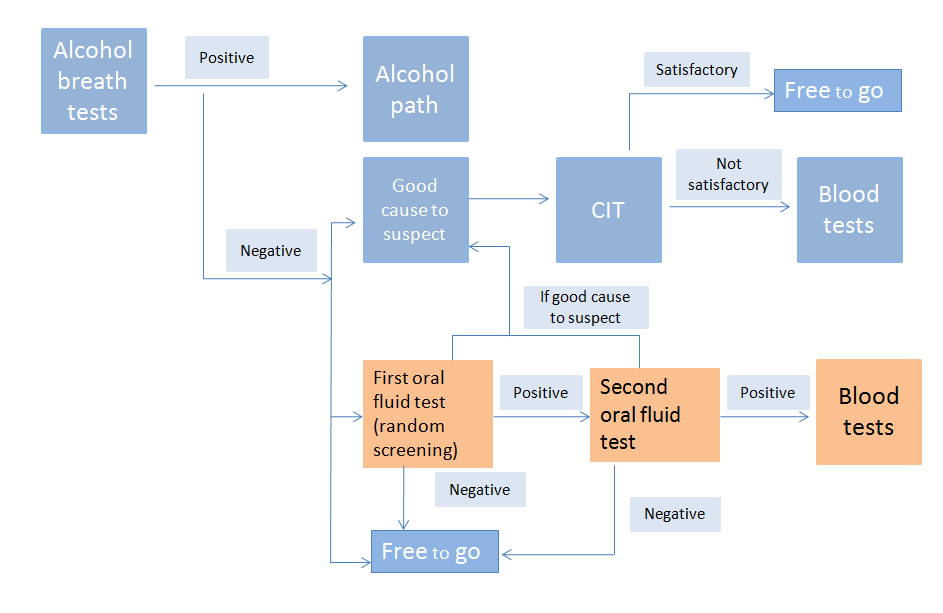 Diagram 2: Testing process under option 2
Diagram 2: Testing process under option 2
t 1982
134.
Assuming 45,000 tests were done, option 2 has a central BCR of 5.15. This option has
positive road safety benefits, and is cost effective and practical. Unlike non-random
options, it creates deterrence without the need to prosecute a large number of drivers.
However, because it is a random testing regime it will have negative impacts on private
freedoms, as drivers who have not taken drugs will undergo drug screening, which
requires them to provide an oral fluid sample. In comparison to alcohol screening, the
under the
initial screening drug test is considerably more time consuming.
135.
The two parallel regimes (oral fluid testing and the CIT) could produce quite different
outcomes for a driver depending on which testing method the officer used. For example,
a driver subjected to the oral fluid test could receive a much lesser penalty than if they
went through the impairment regime and received a criminal conviction. In addition, the
availability of two different drug testing processes could lead to two drivers, both
impaired, facing different legal consequences. The testing process would depend on
which testing process the Police officer chose at the time. However, there is a higher
evidentiary threshold for the impairment testing process because a Police officer must
first have good cause to suspect a driver has used a drug and prove impairment through
the CIT. Such a potential inconsistency is difficult to reconcile if it is considered desirable
to introduce a random testing regime, which results in the need to run parallel regimes.
136.
A possible mitigation to this concern is to allow the Police, under certain conditions, to
switch from the random testing process to the impairment testing process. This would
apply, if after starting the random testing process, a Police officer formed good cause to
Released
suspect a driver had used drugs. For example, a driver passes the first oral fluid testing
process but admits to Police they have taken drugs or they appear to be under the
influence of drugs. This mitigation would create an opportunity for a driver to face the
Official Information Ac
more serious criminal penalty if they are impaired, regardless of which testing process
the officer started with. This approach would also reduce the risk of an impaired driver
avoiding a sanction if they had used a drug that the oral fluid screening device was
unable to detect.
21
137.
To avoid allegations that the drug testing process is capricious or unreasonable, the law
could require the Police officer to complete the process for the infringement offence once
a driver had failed two oral fluid screening tests, rather than permitting a switch to occur
to the impairment process. In addition, once a switch to the impairment process had
taken place, the Police officer should not be allowed to switch back to the oral fluid
testing process.
138.
The switching approach provides an opportunity for a driver to face the more serious
impairment offence if they are impaired regardless of which testing process the officer
started with. It would also reduce the risk of an impaired driver avoiding a sanction if they
had used a drug that the oral fluid screening device was unable to detect.
139.
There are two possible approaches to sanctioning those drivers who commit a presence-
based offence under this option:
Infringement offence with an infringement fee and demerit points (and no criminal
conviction results)
t 1982
Criminal offence with criminal penalties equivalent to existing criminal penalties
for the current impairment offence.
Advantages and disadvantages of an infringement offence
140.
Applying an approach where there is no conclusive evidence of impairment required,
runs a risk of directing road traffic enforcement and court resources to dealing with
drivers who do not necessarily present a road safety risk. There is the risk that drivers
are prosecuted whether impaired or not, and some of whom may not be a road safety
risk. This risk would be mitigated by using an infringement regime, rather than criminal
prosecution. An infringement does not result in a criminal conviction.
141.
Infringement penalties would offer much lower costs to the Justice sector than criminal
penalties, as infringements do not generally result in a court hearing unless the driver
requests a defended hearing. Infringements also offer a swifter way of sanctioning
under the
drivers than a court prosecution.
142.
Introducing an infringement regime could lead to a risk of drug-driving being perceived
as a minor offence. This would depend, in part on the infringement penalties applied. An
infringement fee coupled with demerit points could offer a reasonable deterrent,
commensurate with the nature of the offence and the social harm caused. In New
Zealand’s random alcohol testing regime, infringement penalties are applied to drivers
under the age of 20 who are between 0 and 150 micrograms (mcg) of alcohol per litre of
breath. Infringement penalties are also issued to drivers aged 20 and over who have
breath alcohol levels between 250 and 400mcg of alcohol per litre of breath. In both
cases, the penalty is a $200 infringement fee and 50 demerit points. Because driver
licences are suspended for three months after 100 or more demerit points have been
accumulated within a 2-year period, 50 demerit points is a strong deterrent. It would be
sensible to apply these penalties to sanction drivers found to have drugs in their system.
Advantages and disadvantages of a criminal offence
Released
143.
As described above, criminal sanctions would act as a strong deterrent to drug-driving.
However, a presence-based approach would not indicate whether a driver was impaired,
and as such would not show conclusively whether that a driver was a road safety risk.
Official Information Ac
144.
The current drug-driving laws focus on harm caused by driving whilst impaired by a drug.
Without conclusive evidence that the presence of a drug has affected a person’s ability
to drive, an infringement offence is preferred over a criminal offence.
22
145.
A disadvantage of the criminal-based sanctions is the workload and cost they will place
on the court system. Based on Police screening 45,000 drivers a year, the Ministry
estimates the cost to the Ministry of Justice would be around $560,000 per year. There
will also be a cost to the Department of Corrections for handling more community home
detention and related sentences, which would be around $6.22 million per year.
Preferred approach for offences
146.
The Ministry’s cost-benefit analysis looked at criminal-based sanctions and infringement
sanctions for option 2. The BCR for an infringement offence is 5.15, while the BCR of the
criminal offence is 2.01. This reflects the added cost involved with a criminal offence to
the Justice Sector and Department of Corrections. On balance, the Ministry prefers
setting the level of penalty at an infringement while noting Police officer would have the
ability to switch to the impairment process, which involves criminal penalties. Option 2 is
compared to other options on this basis.
Option 3: Non-random roadside testing (replacing current CITs with oral fluid testing)
t 1982
147.
Option 3 would replace the CIT with non-random roadside oral fluid testing. If a Police
officer found good cause to suspect that a driver had used a drug an oral fluid testing
process would follow. If there was a positive result on the initial oral fluid test, the driver
would be required to undertake a second oral fluid test. The oral fluid tests used in option
3 would be the same as those used in option 2, and would be subject to a competitive
procurement process.
148.
Police would take a blood sample if a driver failed both the screening tests, and would
send the sample to a laboratory for evidential testing. If a driver had evidence of a
specifying drug in their bloodstream, they would be prosecuted. The following diagram
outlines the process for testing under option 3.
Diagram 3: Testing process under option 3
under the
Released
Official Information Ac
23
149.
Assuming 1000 tests were carried out, option 3 has a central BCR of 0.29. This option
would have some road safety benefits, through removing drivers who are obviously
impaired from the road.
150.
A major problem with this option is that due to the limited number of drugs an oral fluid
device can test for, if the driver passes a screening test but is still visibly impaired, they
would be free to go. In this instance, an impaired driver who poses a safety threat could
potentially not be removed from the road.
151.
Testing which relies on good cause to suspect is appropriate from a New Zealand Bill of
Rights Act 1990 perspective. This is due to testing being limited to drivers who are
potentially impaired, with impairment identified before prosecution. Option 3 is a
presence-based regime, which means that drivers who are not impaired may be
prosecuted.
Option 4: Non-random roadside testing but with limits (similar to UK model)
t 1982
152.
Option 4 would introduce non-random roadside oral fluid testing, similar to option 3.
Under this option, a blood sample would be taken if a driver failed the oral fluid tests.
However, the blood sample sent to a laboratory would be tested to determine if the
amount of drugs identified by the oral fluid test exceeds a specified limit.
153.
The following diagram outlines the process for testing under option 4.
Diagram 4: Testing process under option 4
under the
Released
154.
Assuming 1000 tests were carried out, option 4 has a central BCR of 0.27. The benefits
and disadvantages of this option are similar to option 3. However, it presupposes an
ability to link the amount of drugs in a person’s body with their level of impairment. If this
could be done, it would mitigate the risk of drivers being prosecuted who were not
Official Information Ac
impaired. In the Ministry’s view, this is not yet possible. Further, the evidential testing of
blood to test whether the amount of the drug exceeds the legal limit would be
prohibitively expensive.
24
155.
Like option 3, the problem with this option is that due to the limited number of drugs an
oral fluid device can test for, if the driver passes a screening test but is still visibly
impaired, they could not be taken off the road.
156.
Like all other non-random options, testing which relies on good cause to suspect is valid
from a Bill of Rights Act 1990 perspective. This is due to testing being limited to drivers
who are potentially impaired, with impairment being identified before prosecution can
proceed.
Option 5: Random roadside oral fluid testing in conjunction with CIT
157.
Option 5 would introduce a random roadside oral fluid testing regime. However, unlike
option 2, a CIT would be undertaken rather than a second oral fluid test, following a
positive result on an initial oral fluid test. Blood tests would also be required following an
unsatisfactory result from the CIT.
158.
The following diagram outlines the process for testing under option 5.
t 1982
Diagram 5: Testing process under option 5
under the
159.
Assuming 45,000 random tests were undertaken, option 5 has a central BCR of 2.16.
This option potentially couples the benefits of a random testing regime with the benefits
of the existing good cause to suspect regime. It has positive road safety benefits, as it
does not require a second, more expensive evidential oral fluid test to confirm a person
has taken drugs. It also ensures those who are a risk to others’ safety are correctly
identified and stopped from driving.
160.
The Ministry believes that this option would be less difficult to justify than option 2 from a
Bill of Rights Act 1990 perspective, as drivers are being shown to be impaired before
being prosecuted.
Released
Official Information Ac
25
161.
Police do not support this option, due to operational feasibility of the regime. This is due
to a number of factors, such as the real potential for oral fluid screening tests to lead to a
bias in the administration of the CIT, and the considerable resource requirements
associated with the proposal. It would take an average of one hour for drivers who fail
the first oral test to complete the CIT before a decision is made to progress the blood
sample. This has considerable implications for Police, involving the removal of an officer
from the frontline for at least an hour, with no definable outcome. Police does not believe
that the policy objective of delivering high levels of testing can be achieved through this
regime, and therefore the benefits will not be fully realised.
Option 6: Non-random roadside testing without limits
162.
Option 6 would allow Police to either require a driver to undergo a CIT or alternatively, a
roadside oral fluid test once forming good cause to suspect. If the first oral fluid test
indicates a positive result, a second oral fluid test would follow. If a positive result were
obtained for a second time, a blood test would follow.
t 1982
163.
The following diagram outlines the process for testing under option 6.
Diagram 6: Testing process under option 6
under the
164.
Assuming 1000 tests were carried out, option 6 has a central BCR of 0.24. This option
has similar benefits to options 3 and 4, with some road safety benefits, through removing
drivers who are obviously impaired from the road.
165.
In addition, there is likely to be a bias in favour of using an oral fluid screening pathway,
given the complexities inherent in the CIT and the resources required. However, a CIT
Released
gives Police a way of testing for many drugs that oral fluid testing would not identify.
166.
Like all other non-random testing options, which rely on good cause to suspect, this
option is valid from a Bill of Rights Act 1990 perspective. This is due to testing being
Official Information Ac
limited to drivers who are potentially impaired, with impairment being identified before
prosecution can proceed.
26
link to page 28
167.
There is the risk that drivers are prosecuted whether impaired or not, some of whom may
not be a road safety risk. This risk could be mitigated to some extent by using an
infringement regime, rather than criminal prosecution.
168.
Table 1 below compares the options against the assessment criteria. Option 2, followed
closely by option 5, offers the best fit against the criteria.
t 1982
under the
Released
Official Information Ac
27
Table 1: Multi criteria analysis - options to amend drug-driving enforcement regime assessed against criteria6
Option
Objectives of drug-driving
Impacts on drivers
Public acceptability
Impacts on the
Operational
Benefit cost
enforcement (to reduce
(assessment based on
Courts &
feasibility
ratio
(
=preferred)
harms caused by drug-
limited information due
Corrections
driving; provide deterrence
to lack of a full public
effect; and remove impaired
consultation)
drivers from road and
sanction them)
1: Current enforcement
Small reduction in harms caused
approach with increased
by drug-driving.
Will affect very few drivers as
testing. Testing process
it relies on good cause to
Court time
Current system but
Deterrent effect limited.
0.27
outlined in diagram 1.
Same as status quo.
suspect. Unlikely to cause
increased –impact
would require additional
t 1982
Removes visibly impaired drivers
concern as it is involves the
on justice system.
trained officers.
from the road, if identified, and
same enforcement regime.
sanctions them.
2: Existing model for CIT
Significant reduction in harms
in addition to random
caused by drug-driving.
Police have indicated
oral fluid testing
Infringement
Will affect a significant number
their support of random
(similar to Victorian
Negative impact on private freedom
offence means
Deters drug drivers.
of drivers, as any driver may
oral fluid testing
model) . Testing process
by detaining people not yet
there will be a
be tested. Oral fluid testing
alongside the current
5.15
outlined in diagram 2.
Removes potentially impaired
suspected of committing an
limited impact on
may be considered invasive.
CIT regime. Police
drivers from the road provided
offence. Risk of sanctioning
court time or
Presence-based offence may
would need to change
they prove positive for a drug
people who are not impaired.
processing. Police
cause concern.
operational practices,
screened by the testing device
will face costs.
including training.
Drivers are sanctioned but at a
lower level than criminal offending.
3: Non-random roadside
Small reduction in harms caused
Will affect very few drivers as
testing
by drug-driving.
it relies on good cause to
(replacing current CIT).
Deterrent effect limited.
suspect. Testing method may
Testing process outlined
Court and
Police would need to
be considered more invasive
in diagram 3.
Risk of sanctioning those who
processing time
change operational
It would not remove visibly
0.28
under the
than CIT, however the time
are not visibly impaired.
increased –impact
practices, including
impaired drivers but would remove
taken for the test will be
on justice system.
training.
potentially impaired drivers from
significantly improved (5
the road provided they prove
minutes compared to 52
positive for a drug screened by the
minutes).
testing device.
6 A benefit cost ratio has been provided in addition to the multi criteria analysis table for comprehensiveness. Each of the criteria may or may not be monetised in the cost benefit
analysis.
28
Released
Official Information Ac
Option
Objectives of drug driving
Impacts on drivers
Public acceptability
Impacts on the
Operational
Benefit cost
enforcement (to reduce
(assessment based on
Courts &
feasibility
ratio
(
=preferred)
harms caused by drug-
limited information due
Corrections
driving; provide deterrence
to lack of a full public
effect; and remove impaired
consultation)
drivers from road and
sanction them)
4: Existing model for CIT
Small reduction in harms caused
in addition to non-
by drug-driving.
Setting of limits is
random roadside testing
Deterrent effect limited.
Will affect very few drivers
problematic and testing
with limits
There is a risk of sanctioning
Court and
as it relies on good cause
devices expensive.
t 1982
(similar to UK model).
As well as removing visibly
people who are not impaired as
processing time
0.27
to suspect. Testing method
Police would need to
Testing process outlined
impaired drivers, removes
different people are affected
increased –impact
may be considered more
change operational
in diagram 4.
potentially impaired drivers from
differently by drugs.
on justice system.
invasive than CIT.
practices, including
the road if they prove positive for a
training.
drug screened by the testing
device and sanctions them.
5: Existing model for CIT
Significant reduction in harms
in addition to random
caused by drug-driving.
Police have indicated
roadside screening
Deters drug drivers.
Court and
this option is
followed by a CIT.
Negative impact on private
Will affect a significant number
processing time
operationally unsound.
Testing process outlined
Removes impaired drivers from
freedom by detaining people
2.16
of drivers, as any driver may
increased –
Police would need to
in diagram 5.
the road if they prove positive for a
not yet suspected of committing
be tested.
medium impact on
change operational
drug screened by the testing
an offence.
justice system.
practices, including
device and do not perform a
training.
satisfactory CIT. Drivers are
sanctioned at a criminal level.
6: Existing model for
Some reduction in harms caused
CIT in addition to non-
by drug-driving.
random roadside testing
under the
without limits. Testing
Deterrent effect limited.
Will affect very few drivers as
Court and
Police would need to
process outlined in
it relies on good cause to
Risk of sanctioning those
processing time
change operational
As well as removing visibly
0.25
diagram 6.
suspect. Testing method may
who are not impaired.
increased –impact
practices, including
impaired drivers, removes
be considered more invasive
on justice system.
training.
potentially impaired drivers from
than CIT.
the road if they prove positive for a
drug screened by the testing
device, and sanctions them.
Key:
Significantly better than status quo
Negligible difference, or no change from status quo, or unknown
Significantly worse than status quo
29
Released
Official Information Ac
Cost benefit analysis
169.
A cost benefit analysis has been prepared for the six policy options using studies and
data from both New Zealand and overseas. The costs and benefits are estimated over
10 years, which are stated as present values of the sums of the incremental costs and
benefits respectively, in comparison to the status quo.
Benefits and costs analysed through the cost benefit analysis
170.
The benefits captured through the cost benefit analysis are as follows:
Safety benefits. The relationship between the drug-driver testing rate per 1000
licensed drivers and the percentage of drivers that are killed because of drug-
driving has been used to estimate the reduction in social costs of road crashes,
therefore the benefits. It is assumed the same level of benefits will be seen
regardless of the testing method used. Therefore, the savings in social costs is
the same for all options regardless of the testing method used.
t 1982
Other benefits not estimated/included and likely limitations. Due to limited
information available, the cost benefit analysis does not include health effects
from changes in enforcement level. However, we do not believe that this impact
would be large enough to alter the conclusion of the analysis. Higher level of
enforcement is expected to reduce drug impaired driving but not necessarily drug
consumption. However, the costs of achieving this benefit vary markedly between
options.
171.
The costs captured through the cost benefit analysis are as follows:
Unit test costs. These unit costs are costs per test mainly covering the Police’s
time on testing, the cost of the devices for oral fluid tests and the lab analysis for
evidence.
Cost to enforcement-related agencies – Police, Ministry of Justice, NZTA,
under the
Department of Corrections. This includes the resource costs to departments.
Apart from costs to the Ministry of Justice and Department of Corrections, there
could also be impacts on the legal aid system. Due to a lack of information, the
impact on legal aid has not been included in this analysis.
Costs to individuals. In addition to travel time costs, there are the time costs
related to appearances at court and time taken for disqualified drivers to apply for
limited licences. Further, there would be resource costs for individuals related to
vehicle impoundment.
Cost of changing testing methods. Under some of the proposed options below,
the current impairment tests would be replaced by roadside oral fluid tests. The
related costs differences are mainly due to the difference in the unit costs for
Police and time costs for individuals.
Other costs not estimated/included (including costs to wider society). Other costs
Released
not included in the cost benefit analysis are economic impacts of traffic delays
resulting from road crashes, reduced travel and costs to businesses. They have
not been included in the analysis, either due to a lack of information, or because
they are not expected to be significant.
Official Information Ac
30
link to page 31
172.
Table 2 below outlines the results of the cost benefit analysis for each of the six options
considered. It summarises the estimated net present value (NPV) and BCR of each
option, assuming 45,000 tests take place each year for each of the random testing
options, and 1000 tests take place each year for the good cause to suspect options.
Table 2: Summary of BCR results for each option
Option
Option
Option
Option
Option
Option
1000
45,000
1000
1000
1000
45000 tests
tests
tests
tests
tests
tests
1
2
3
4
5
6
Net present value
1982
High estimates
-8.42
839.30
-6.48
-7.74
756.70
-9.41
Central estimates
-28.10
248.10
-26.16
-27.42
165.51
-27.22
Low estimates
-34.82
46.21
-32.87
-34.14
-36.38
-33.30
the Act
Benefit - cost ratio
High estimates
0.78
15.03
0.82
0.79
6.31
0.74
Central estimates
0.27
5.15
0.28
0.27
2.16
0.25
Low estimates
0.09
1.77
0.10
0.09
0.74
0.09
173.
If the net present value (i.e. present value of benefits minus present value of costs) is
under
positive, and subsequently the BCR (i.e. present value of benefits divided by present
value of costs) is greater than one, the associated option is deemed to deliver net
benefits to the nation.
174.
Further detail on the cost benefit analysis can be found in the document
Safety
impairment project: Increase the level of drug-driving enforcement in New Zealand –
Cost benefit analysis.
Information
Results of the cost benefit analysis
175.
These results indicate the benefits from a reduction in the number of deaths and injuries
will outweigh the increased resource costs to departments and individual costs for
options 2 and 5. This holds under all high and central estimates, and low estimates for
option 2. The central estimate BCRs for options 2 and 5 are 5.15 and 2.16 respectively.
176.
Under options 1, 3, 4 and 6, while the benefits are larger than the costs under high
estimates, this does not hold true under central and low estimates, with BCRs lower than
Released
1, and negative net present values.
177.
This implies that when considering uncertainties, options 2 and 5 would deliver net
benefits to society, but the others would not.
Official
31
link to page 32
Preferred option
178.
Based on the results of the multi criteria analysis and cost benefit analysis, option 2 and
option 5 were scrutinised in more detail by the Ministry.
179.
Table 3 below outlines the strengths and weaknesses of the two drug-driving testing
models, when considered side-by-side.
Table 3: Strengths and weaknesses of each random testing option
Option 2 (preferred option) -
Option 5 - Impairment-based random
Presence-based random drug
drug testing model (45,000 tests)
testing model (45,000 tests)
1982
Road safety
Estimated reduction of 10.8 alcohol-
Estimated reduction of 10.8 alcohol-
impact
related fatalities per annum
related fatalities per annum
Good impact on road safety through
Good impact on road safety, through
deterring drug-users from drug-driving
deterring drug-users from drug-driving
BCR – Central
5.15
2.16
Act
estimate
the
Cost for 45,000
$52.65 million over 10 years
$142.41 million over 10 years
tests
Operational
NZ Police have stated they support
NZ Police have stated this regime would
acceptability
this regime. This is due to:
have considerable operational risks. This
is due to:
Ability to deliver higher levels
of testing across the general
Potential for first oral fluid testing
driving behaviour, delivering
result to bias the administration
greater general deterrent
of the CIT
under
value in line with policy
The time taken to process a
objectives
driver to the point of having a
Still have the option to pursue
blood sample taken is expected
impairment offences through
to be at least one hour. Officers
the current CIT process
are removed from the frontline
The time taken to process a
environment during this time.
driver to the point of having a
Concern regarding undue
blood sample taken is
detention due to the first oral
expected to be around 15
fluid screening test returning an
Information
minutes representing less
inaccurate test result.
impact on motorists and
Because of the resources
Police resources
required to support this regime,
Police may not be able to deliver
the higher level of testing the
proposal assumes, therefore
undermining the assumed
benefits of the BCR, which are
based on 45,000 tests per
Released
annum
Impacts on
The regime would impact these
The regime would impact these sections
private benefits
sections of the Bill of Rights Act 1990:
of the Bill of Rights Act 1990:
Official
and freedoms
unreasonable search and
unreasonable search and
seizure
seizure
32
arbitrary arrest or detainment
arbitrary arrest or detainment
the right to be presumed
the right to be presumed
innocent until proved guilty
innocent until proved guilty
according to law.
according to law.
The Ministry of Justice is particularly
The Ministry of Justice is particularly
concerned with this regime in relation
concerned with this regime, in relation to
to the right to be presumed innocent,
arbitrary detainment, as a false positive
as presence of a drug would not
on oral fluid screening test could lead to
necessarily indicate impairment.
a driver being detained for an unduly
long amount of time (an average CIT
takes 52 minutes).
Public
The public may be in favour of this
The public may be in favour of this policy
acceptability
policy given feedback from
given feedback from representative
representative groups, however open
groups, however open public
1982
public consultation has not been
consultation has not been undertaken.
undertaken. There may be some risks
Presence-based testing may be
due to the presence of drugs being
considered more invasive than the
tested for, rather than impairment, as
current regime. The length of time taken
drivers may be sanctioned when not
as a result of the CIT stage may be seen
impaired and presence-based testing
as undesirable.
may be considered more invasive
Act
than the current regime.
the
Impacts on
If a criminal offence is used for
This regime would result in an increase
Justice sector
prosecution, this regime would result
in drivers processed by the Justice
in a larger increase in drivers
sector.
processed by the Justice sector than
an impairment regime. This is
because there may be drivers
identified who have drugs in their
system but who are not impaired.
under
They would not be prosecuted in an
impairment regime.
180.
Both options provide similar road safety impacts. Police has advised that option 5 has
considerable operational risks and is operationally unsound, and may explain why it is
not used in any other jurisdiction.
Information
181.
A major concern of the Police is that the oral fluid analysis could pre-empt the outcome
of the CIT, whereby a positive oral fluid test could lead some officers negatively
assessing the performance of the CIT. The risk here is that the impartiality of the CIT
may be undermined by the positive test result that precedes it. This could lead to
significant legal challenges, which may undermine the robustness of the whole system.
182.
Another problem with option 5 is a scenario where the initial fluid test may test positive
for the active ingredient of cannabis (THC), which may pre-empt an unsatisfactory CIT.
Released
The subsequent blood sample analysis may test negative for THC, but may test positive
for other qualifying drugs. This brings about a question that could be raised in court:
where if the oral fluid test constitutes the good cause to suspect that the driver is
operating a motor vehicle while under the influence of THC, but this is not supported by
Official
the evidence (the blood sample), is there good cause to suspect and prosecute for other
qualifying drugs?
33
183.
Police is also concerned about the resource implication for option 5. Every time a driver
fails the first oral fluid test, the officer must transport the driver to an accessible station
(or any such appropriate place), administer the test, and then transport the driver back.
For the duration of this process, the officer is removed from the frontline, and therefore
cannot administer any further random oral fluid tests. This will impact on the delivery of
the proposed testing levels, and consequently, impact on the assumed benefits of the
option.
184.
Given the Police are the key implementing agency for drug-driving enforcement, weight
must be given to its concerns. For the reasons outlined above, in addition to the results
of the multi criteria analysis and cost benefit analysis, option 2 is the preferred option.
185.
In order to implement the preferred option, the Land Transport Act 1998 will need to be
amended to introduce random drug testing.
1982
Risks associated with the preferred option
186.
The following concerns have been expressed in relation to the Bill of Rights Act 1990
about the proposal to introduce a presence based random testing regime.
Section 21 – the right to be secure against unreasonable search and seizure.
Act
Random testing removes the need for reasonable grounds to be established
the
before a person is tested for drugs.
Section 22 – the right not to be arbitrarily arrested or detained. Detention is
considered arbitrary if it is capricious, unreasoned or without good cause. A
preliminary oral fluid test taking around five minutes is likely to constitute a
detention and the removal of the need for good cause would likely make such a
detention arbitrary.
Section 25 (c) – the right to be presumed innocent until proved guilty according to
law. The prosecution bears the legal burden of proving every element of an
offence to the required standard of proof, and disproving any potentially available
under
defence. Shifting the onus of proof onto the defendant will limit section 25(c) of
the Bill of Rights Act 1990.
187.
The Ministry of Justice has stated it is unlikely that the limits to section 21 and 22 are
justified under section 5 of the Bill of Rights Act. It believes the limits on rights are more
than reasonably necessary, as the proposals do not include an appropriate threshold to
meet before detaining and undertaking an invasive search of potentially innocent people.
Information
188.
The Ministry of Justice has also stated that the proposed drug testing regime appears to
shift the burden of proof to the defendant to demonstrate an offence has not been
committed. It believes it is unlikely the limit on section 25(c) is justified under section 5 of
the Bill of Rights Act 1990, stating that punishing people who are not impaired is not
rationally connected to the objective of the policy and the lack of any per se limit from
which to infer impairment also means that rights are not minimally impaired.
Ministry of Transport comment
Released
189.
These are similar to human rights issues which have arisen for random alcohol testing,
which was found to be inconsistent with the Bill of Rights Act by the then Attorney-
General when it was introduced in 1991.
Official
34
190.
The human rights implications of the preferred option are significant and must be
considered in detail by decision makers. These are summarised below:
Under the preferred option in this paper, any driver may be required to undergo a
presence based bodily fluid test, irrespective of whether they are presumed to be
driving while impaired. Many people in New Zealand may consider this is a more
invasive method of testing than the current behavioural impairment test, which
does not require any sampling of bodily fluids.
The preferred option will take away individual freedoms in the form of time.
Current oral fluid testing devices take up to 5 minutes to produce a result, which
may be considered a significant amount of time detain a driver when they are not
yet suspected of committing an offence.
While the technology used in presence based drug testing devices has improved
1982
and continues to improve, the possibility of false positive results does exist. While
a blood test can correctly identify for the presence of drugs, the possibility of
putting an innocent person through a number of confirmatory tests does exist
under the preferred option.
191.
The false positive rate of the proposed regime is unknown and will only be identified if
Act
the regime is implemented and the appropriate data recorded. The cost benefit analysis
the
completed for the proposed regime estimated a total false positive rate of 1.5 percent.
This includes all false positive results that would occur along the testing process. A
smaller number of the total false positive tests would arise at the evidential blood testing
stage. This rate is based off data from Victoria about the current rate of false positive
results on oral fluid testing devices, in conjunction with some assumptions made on the
likely analogy between New Zealand’s current CIT regime and proposed regime.
192.
Of the total random oral fluid tests administered in Victoria, 6.2% result in a positive
result. On the second oral fluid test, 5.4% of the total number of tests initially
administered result in a positive result (here some false positive test results have already
been picked up - 0.8 percent). The cost benefit analysis prepared by the Ministry
under
assumes the same level of false positives just mentioned. Drivers whose tests show a
positive result on the second oral fluid test will go to an evidential blood test. The cost
benefit analysis also estimates that 87 percent of these blood tests return a positive
result. This is based on the expected analogy between the current CIT regime (where
blood tests have a 90 percent positive rate) and the proposed regime. Another way of
looking at this, is that the cost benefit analysis assumes that two oral fluid tests will be
about as effective as a CIT in determining impairment, or the presence of drugs.
Information
193.
Like other outputs of the cost benefit analysis, the estimated total false positive rate is
based on assumptions that cannot be validated. There is a danger in using an analogy
between the current CIT regime and the proposed regime for a level of false positive
results, as there are significant differences between the two regimes.
194.
In addition to the human rights implications mentioned above, there are constitutional
concerns with the introduction of the preferred presence-based infringement regime,
given that the infringement regime is not calibrated against evidence of any impairment
Released
and therefore conclusive evidence of road safety risk. The concern is that the
introduction of an infringement offence which will sit alongside the current criminal
offence for drug-driving could lead to unequal treatment of individuals before the law.
Official
35
195.
The proposed changes may result in unequal treatment before the law in two situations;
firstly where Police discretion is exercised in requiring an individual to undertake the
behavioural impairment based test and face a criminal sanction, and secondly where
Police discretion is exercised to require a driver to undergo the presence-based test and
face an infringement offence without the ability to demonstrate they are not impaired.
196.
Where a person passes a CIT, they would not then be required to undertake an oral fluid
screening test, and therefore cannot be found to have committed an infringement
offence, even though they may have consumed drugs.
197.
This could also lead to a situation where two people, both impaired, may face different
legal consequences based on the test administered by the Police officer at the time.
There is a concern that the oral fluid test will be considered an easy option and that
Police may use even when a person appears to be impaired.
1982
198.
The introduction of an infringement offence which runs alongside a similar criminal
offence is not unfamiliar in New Zealand law. There are two drink-driving infringement
offences within the Land Transport Act 1998 that run alongside similar criminal offences,
these apply in the following situations:
For drivers under the age of 20 who are detected as having between 0 and 150
Act
micrograms (mcg) of alcohol per litre of breath; and
the
For drivers aged 20 and over who are detected as having a breath alcohol level
between 250 and 400 mcg of alcohol per litre of breath.
199.
The penalty for both offences is a $200 infringement fee and 50 demerit points. Where a
driver is found to be over the upper limit in both instances, they will instead face a
criminal sanction, which may include a period of imprisonment or a fine, and
disqualification from holding or obtaining a driver’s licence for a period of time. However,
comparing the preferred drug-driving regime with these infringement regimes does have
limitations.
under
200.
The final assessment of the consistency of the proposals with the Bill of Rights Act will
be undertaken by the Attorney-General when a Bill to implement the random testing
regime is available.
Consultation
201.
The Ministry undertook a targeted consultation process rather than a general public
consultation. The Ministry held a Stakeholder Workshop on 12 May 2015. Attendees
Information
included a range of government departments, treatment providers, and several interest
groups such the NZ Automobile Association and the NZ Drug Foundation. Thirty
stakeholder groups were invited to this workshop, and four took the opportunity to
provide written feedback on the proposals.
202.
Stakeholders felt drug-driving affects all ages, and involves both prescription and illicit
drugs. They were also concerned by the low number of drug tests being done under New
Zealand’s current regime. Some stakeholders were concerned about presence-based
Released
testing, as the mere presence of a drug or drugs in a specimen does not mean a person
is impaired.
203.
There was no consensus on the best way forward. Some stakeholders favoured
Official
adopting the Australian regime while others were opposed due to inconsistencies of this
regime with the Bill of Rights Act 1990.
36
204.
Police have been consulted on the review and have provided significant feedback over
the course of the drug-driving review. Police support the Ministry’s preferred option.
Police has indicated that it believes as technology continues to improve, the Ministry’s
preferred option may be even more cost effective in the future.
205.
The Ministry of Justice has provided feedback on the drug-driving review, particularly on
its human rights implications. This feedback has been incorporated into this regulatory
impact statement. It also noted that additional costs will add to existing Ministry of Justice
budget pressures and could affect the provision of existing services unless additional
funding is secured.
206.
The NZ Automobile Association did a survey of around 2500 of its members in 2009.
This survey found that 89 percent of members surveyed supported introducing roadside
saliva testing for drugs. However, this survey did not explain the process that is involved
with oral fluid drug-screening tests or the time it would take to screen a driver’s oral fluid
1982
for drugs. The NZ Automobile Association advises that his level of support remains
consistent with a rolling survey that the Association conducts quarterly, where members
are asked if they support or oppose introducing a saliva based drug test to detect drug-
driving. In the last survey, of around 900 members, 83.9 percent expressed support.
Conclusion and recommendation
the Act
207.
A review was undertaken by the Ministry to determine how to minimise harm resulting
from drug-driving in New Zealand at a reasonable cost through changes to the
enforcement regime. The key tasks of the review were to identify the extent of New
Zealand’s drug-driving problem and to determine whether New Zealand’s current drug-
driving enforcement model should remain as the Government’s preferred model.
208.
The drug-driving review process involved analysing the existing regime, studying
international regimes, gathering data, holding discussions with stakeholders, developing
options and undertaking a cost benefit analysis.
209.
A cost benefit analysis prepared for the review found that drug-driving in New Zealand
under
imposes an estimated social cost of between $96.8 million and $731.4 million per
annum, with a central estimate of $250.5 million. This translates to approximately 23
people dying, 112 serious crashes, and 304 minor crashes per year.
210.
A number of potential enforcement models have been scrutinised. These models
included New Zealand’s current regime, three regimes based on good cause to suspect,
and two random testing regimes.
Information
211.
While the analysis of these potential regimes is subject to a range of unknowns and
uncertainties, the cost benefit analysis prepared has used best practice methods to
provide a more robust picture of the likely range of benefits and costs of the various
regimes. Under current operational practices and data collection methods, it is not
possible to further analyse the extent of the drug-driving problem in New Zealand and its
associated harms. The operational cost and ethical issues that come along with
collecting the types and volume of data needed to more fully realise the extent of the
drug-driving problem in New Zealand, means that this is not possible.
Released
212.
Having estimated the likely scale of the social cost of drug-driving in New Zealand, a
further investment in drug-driving enforcement is justified. A benefit-cost analysis
indicates that a random drug testing regime is the most cost-effective method of reducing
Official
the cost of drug-driving. One the reasons that random drug testing is cost effective, is the
deterrent effect it has on the driving population. There were two possible approaches to
random testing considered. The first approach modelled on Victoria, Australia. The
second approach involves a random roadside oral fluid screening test followed by a CIT.
37
213.
The most cost effective approach is the Victoria model. This has been employed
successfully in Australia since 2004. While many factors contribute to road safety,
Victoria has a superior road safety record to New Zealand. The Victorian model has
been adopted by most Australian states, with some variations.
214.
The human rights implications of the Ministry’s preferred option are significant and must
be considered fully by decision makers. Under the preferred option, a drug-screening
device that uses bodily fluid testing will be used on drivers not yet suspected of driving
while impaired, or under the influence of drugs. These drug testing devices take longer
(up to five minutes) to produce a test result, when compared against current roadside
alcohol testing devices (30 seconds), which will result in a driver being detained for
longer. As well as the time required, the need to take an oral fluid sample may also be
considered more invasive than a passive alcohol screening test.
215.
In addition, oral fluid screening devices can be susceptible to producing false positive
1982
results, largely as a result of operator error. To mitigate the risk of false positive test
results, the preferred option will use a second oral fluid test. Furthermore, an evidential
blood test would correct any false positives on presence-based tests. This would enable
an individual to establish that they are not impaired before facing any sanction. However,
false positive results may subject innocent drivers to unnecessary confirmatory tests, if
the preferred option is implemented. This includes the possibility of an innocent driver
Act
having to undergo a blood test and wait several days, or longer, for the results to be
the
confirmed by a laboratory.
216.
As it is difficult to link driving impairment with the level of drug or combinations of a drug
found in a driver’s system the preferred option wil operate a zero tolerance policy. This
approach is a shift from the status quo enforcement regime, which is based on proving a
person is impaired and cannot drive safely, and has drugs present in their blood.
217.
This approach will sanction people without any consideration given as to whether they
are in fact visibly impaired or conclusively pose a safety risk. However, given that there is
difficulty in establishing limits relating to an individual’s fitness to drive, in the absence of
evidence of behavioural impairment, by virtue of the presence of the particular drug or
under
drugs, it will be considered that the driver presents a risk to road safety, although less of
a risk than a driver who is conclusively impaired. The recommended approach seeks to
mitigate this risk by creating an infringement offence rather than a criminal offence, i.e.
the offence would not result in a criminal conviction. Nonetheless, it is still a sanction.
218.
The other random drug testing option considered would have similar road safety
benefits. It would also mitigate some of the human rights issues associated with the
preferred option because it includes a CIT. However, the Police do not support this
Information
option because, in its view, it is not operationally feasible, and would not deliver against
the policy objectives because of this. Given the Police’s responsibility for implementing
any regime, considerable weight must be placed on the Police’s view. This option would
also be significantly more expensive. As a result, this option is not recommended
219.
In summary, there is a trade-off that needs to be made by decision makers when
deciding whether to change the drug-driving enforcement regime in New Zealand to a
presence based random drug driving regime. This trade-offs involves:
Released
estimated road safety benefits
inconsistencies with the New Zealand Bill of Rights Act 1990 and
Official
the practicalities of implementing any new enforcement regime.
38
220.
If decision makers decide to place an emphasis on estimated road safety benefits, the
Ministry recommends choosing the preferred option in this paper. However, if decision
makers decide that the preferred option in this paper will impinge too greatly on drivers'
rights, they may choose not to implement the preferred option in this paper.
221.
If decision makers decide to implement the Ministry’s preferred enforcement regime, it is
recommended that 45,000 random tests are administered annually. The Ministry’s
independently reviewed cost benefit analysis estimates that 45,000 random tests could
prevent 10.8 drug-related fatalities per annum at a cost of around $7 million per annum.
222.
The recommended option in this paper will ensure that drivers are deterred from using
drugs and then driving, therefore reducing the harms caused by drug-driving. While the
Ministry and the NZ Police have considered other options, the Ministry considers that
they do not offer the level of benefit that the preferred option will offer.
1982
Implementation plan and risks
223.
A random drug testing regime requires visible enforcement, publicity, and a much larger
number of tests than a non-random regime, particularly if the regime is designed to
create a deterrence effect.
Act
224.
The preferred option proposes beginning a new drug-driving regime with 15,000 random
the
drug tests in the first year. This number would increase to 30,000 tests in the second
year and 45,000 tests in the third year of the regime. A measured roll out of the regime
wil help to ensure the new regime integrates smoothly with New Zealand’s current drink-
driving and drug-driving enforcement regimes.
225.
It may take some time to begin the regime. The Police would need to identify and make
provision for any additional operational requirements. They would also need to develop
and implement an appropriate training programme for Police officers in the use of the
device and identify a suitable oral fluid screening device via a competitive tendering
process. The Minister of Police would need to approve any new devices by Notice in the
Gazette. The implementation process would take at least six months.
under
226.
There will also be implications for the NZTA, which would need to promote and explain
any changes.
227.
The proposals set out in this paper will have financial implications for the Crown.
Changes to the testing regime for drug-driving will result in higher costs for the NZ Police
and the Justice sector to allow further tests to be undertaken. This may require new
funding or funding to be diverted from elsewhere.
Information
228.
The additional government costs and savings were estimated as part of the Ministry’s
cost benefit analysis. Assuming a random regime comprising of an oral-fluid screening
test and a CIT is used, total net government costs were estimated at $2.4 million in the
first year, assuming 15,000 random drug-tests were used in the first year. This would rise
to $4.7 million in the second year for 30,000 tests, and $7 million in the third year for
45,000 tests. These costs include Police training.
229.
Over 65 percent of the additional costs fall on the NZ Police, and result from the random
Released
drug screening process, including the cost of purchasing drug screening devices. Drug-
driving and drunk-driving enforcement costs are met from the National Land Transport
Fund under the Road Policing Programme of the National Land Transport Programme.
Official
The Road Policing Programme of around $300 million per annum would need to be
varied to accommodate this expenditure. The NZ Police currently spend around $42
million per annum on alcohol and drug enforcement.
39
link to page 40 link to page 40
230.
However, there will also additional costs for the NZTA, Ministry of Justice (Courts) and
Department of Corrections due to a larger number of drug-driving offences. These costs
would normally be met through departmental appropriations. The Department of
Corrections advises any increase in costs cannot be met out of its baseline funding
.
231.
Table 4 sets out the potential financial implications.
Table 4: Potential financial implications
Potential
Cost ($m)
Cost ($m)
Cost ($m)
financial
(GST excl)
(GST excl)
(GST excl)
implications
Year 1 (15000
Year 2 (30000
Year 3 (45000
tests)
tests)
tests)
NZ Police
2.65
4.91
6.83
1982
NZTA
0.00
0.00
0.01
Ministry of
0.04
0.07
0.10
Justice
Department of
0.00
0.01
0.01
Corrections
One-off costs
1.85
-
-
Act
Total financial
the
4.55
5.00
6.95
implications
Arrangements for monitoring, evaluation and review
232.
The Ministry recommends that it, the NZ Police and the NZTA closely monitor the
impacts of any changes to drug-testing policy. While the NZ Police record data on the
number of blood samples analysed following drivers completing a CIT unsatisfactorily, it
does not record how many drivers satisfactorily complete CITs, or how many CITs are
conducted overall.
under
233.
In order to examine the effectiveness of the preferred policy option in this paper, the
Ministry believes the following data, on New Zealand’s good cause to suspect regime
and random testing regime would be helpful for evaluating the new regime. Further
discussion with NZ Police on the feasibility of collecting this data and prioritising them will
be required:
Information
Released
Official
40
Good cause to suspect
Random testing
Number of compulsory
Number of individuals being tested
impairment tests
Number of false positives on first and
Number of blood tests
second oral fluid screening tests
Number of positive drug
Number of blood tests
tests
Number of positive blood tests
The types of drugs being
found
The types of drugs being found
Number of Police with up
Number of offence notices issued
to date training
Number of defended hearings
Number of Police trained
Number of Police trained
1982
Number of defended
Public perception of likelihood of being
hearings
stopped and tested
Types of offences and
Public perception of dangers of drug-
numbers
driving
Act
the
234.
After the legislation has come into force and 3 years of data are available, the Ministry
will provide a report to the Minister of Transport on the effectiveness of proposed
measures.
235.
Effectiveness wil be evaluated through the public’s perception of the likelihood of being
stopped and tested for drug-driving, and their perception of the dangers of drug-driving.
Overtime, success would involve a decline in detection rates of drug-driving. However,
three years is unlikely to be a sufficient length of time to realise the full benefits of the
regime, especially as this period coincides with the implementation phase of the policy.
under
236.
Due to the high level of interest in these proposed changes, their impact will also be
scrutinised by stakeholders, the public and the media.
Information
Released
Official
41